Submitted:
14 July 2025
Posted:
16 July 2025
You are already at the latest version
Abstract
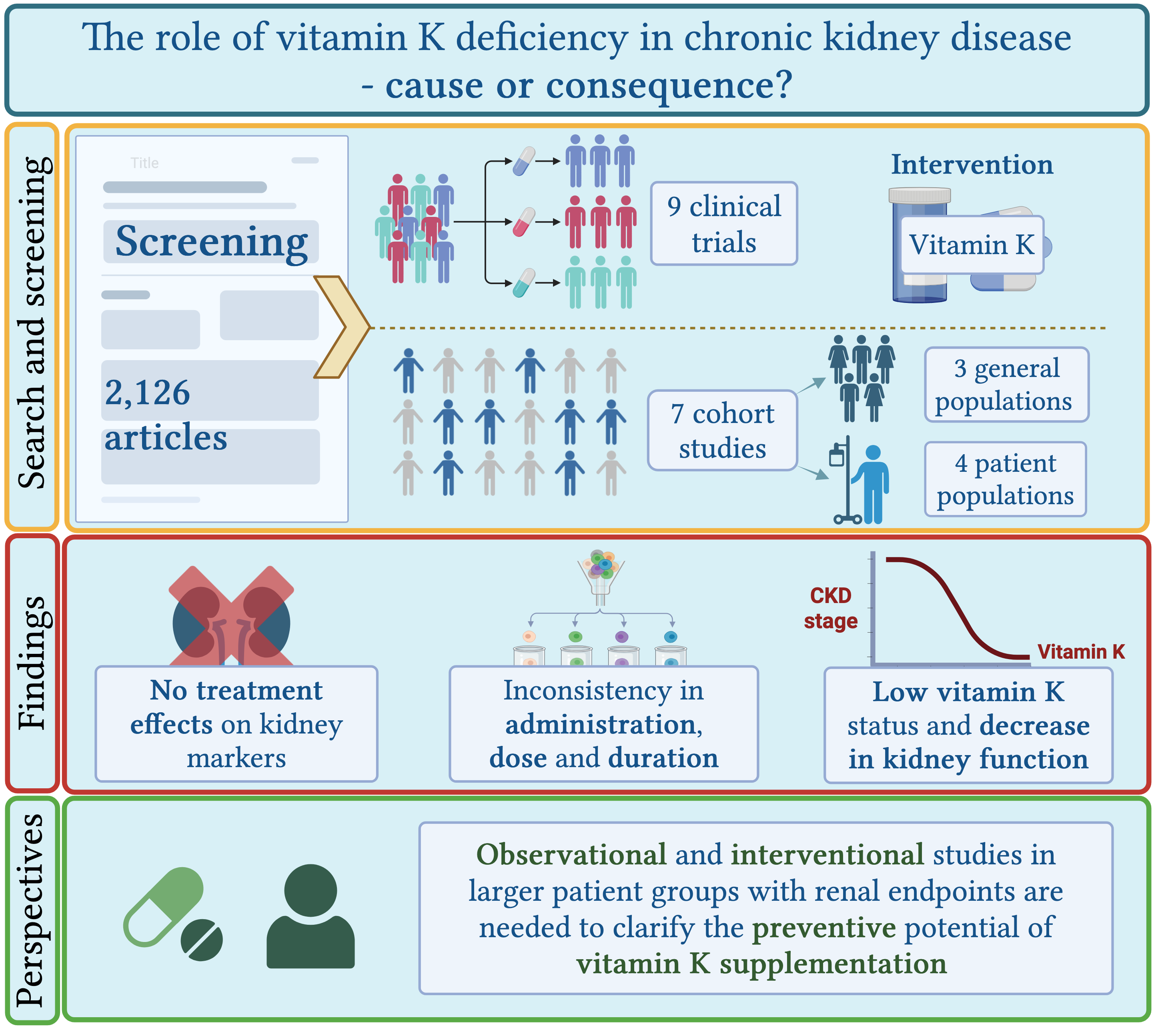
Background/objectives: Chronic kidney disease (CKD) affects up to 15% of the global population and is driven by vascular and interstitial damage, most prevalent in persons with hypertension and diabetes. Vitamin K, a necessary cofactor for activation of vitamin K-dependent proteins may modulate these processes. It is well established that vitamin K deficiency associates with CKD, but the therapeutic effects of supplementation on kidney function are still uncertain. We aimed to review the current evidence on the effect of vitamin K deficiency and supplementation on any marker of renal function and kidney disease, across general adult populations and CKD patient populations. Methods: A search was conducted in PubMed, targeting terms related to vitamin K status and CKD. Studies were included if they reported data on vitamin K status or supplementation in relation to kidney function outcomes. Results: A total of 16 studies were included. Nine interventional studies were included and confirmed that vitamin K supplementation improves biomarkers of vitamin K status but showed no consistent beneficial effects on renal function. Seven observational studies across populations found significant associations between vitamin K status and decline in kidney function, however, associations often attenuated after adjustments. Conclusion: No clear effect of supplementation was observed on the reported kidney markers in patient populations. A clear as-sociation between low vitamin K status and impaired kidney function was confirmed. Study het-erogeneity makes comparability and generalisability of the results difficult. Our review highlights the need for more cohort studies and clinical trials in general or patient populations.
Keywords:
Vitamin K
; chronic kidney disease
; supplementation
1. Introduction
Chronic kidney disease (CKD) is estimated to have a global prevalence of up to 15%, making it a major public health burden[1]. CKD is a collective term for several diseases causing progressive decline of glomerular filtration rate (GFR). There are multiple risk factors for developing CKD, with the most prevalent being vascular and interstitial damage, particularly caused by diabetes and hypertension[2].
Research has already established a high prevalence of vitamin K deficiency in CKD patients. This is believed to be partly due to dietary restrictions, medication-induced, and possibly an impaired vitamin K recycling in CKD patients[3,4]
Some of the early vascular changes in hypertension leading to damage in the kidneys are thickening of tunica media and reduced luminal diameter causing increased vascular resistance. The vascular modelling is particularly present in the small resistance arteries, such as the proximal arteries of the kidneys[5]. The increased resistance results in shear stress on the endothelium promoting endothelial dysfunction and upregulation of pro-inflammatory cytokines leading to activation of several transcription factors, including nuclear factor kappa beta (NF-kB) and bone morphogenic protein 2 (BMP2). This initiates a phenotype switching in the vascular smooth muscle cells (VSMC) from a contractile to a pro-inflammatory and osteogenic phenotype. The differentiation of VSMCs increases calcification and along with increased vascular shear stress mediate kidney damage [6,7].
Diabetes is another prominent risk factor for CKD. Approximately 40% of individuals with type 2 diabetes (T2D) and 30% with type 1 diabetes (T1D) develop diabetic kidney disease [8]. T2D is a chronic metabolic condition characterized by insulin resistance and hyperglycaemia, and T1D is an autoimmune disease attacking the insulin producing beta cells of the pancreas [9,10]. The pathophysiology behind diabetic nephropathy includes renal structure changes leading to glomerular hyperfiltration, albuminuria and decline in GFR. In addition to these structural changes, metabolic alterations result in glomerular hypertrophy, inflammation of the renal interstitium, and fibrosis[8].
Vitamin K is a group of fat-soluble molecules with phylloquinone (vitamin K1) particularly present in green leafy vegetables and the menaquinones (MKs), also referred to as vitamin K2, present in fermented foods and animal-based products including dairy products[11]. Vitamin K2 consists of subtypes MK4-MK13 and both vitamin K1 and vitamin K2 exert their effect through gamma glutamate carboxylase, activating vitamin K dependent proteins (VKDP). There is no generally accepted standard for how to measure vitamin K status. However, measurement of blood levels of the inactive (uncarboxylated) VKDPs, dephospho-uncarboxylated matrix Gla protein (dp-ucMGP) and Protein Induced by Vitamin K Absence (PIVKA), are thought to provide a better measure of vitamin K status compared to direct measurement of circulating vitamin K vitamers, which have a short half-life in blood. Several studies have found a strong decreasing effect of vitamin K supplementation on dp-ucMGP levels in a dose dependent manner, as a reflection of improved vitamin K status [12,13].
In particular, the two VKDPs, MGP and growth arrest-specific gene 6 (GAS-6) are believed to play a role in the pathogenesis of CKD. GAS-6 is expressed in the endothelium, VSMC and bone marrow. It has a wide range of effects on haemostasis and inflammation, suppressing the pro-inflammatory cytokine NF-kB[14]. MGP is expressed by VSMC and chondrocytes[6]. It is a potent inhibitor of vascular calcification by binding BMP-2 thus protecting against VSMC differentiation. Furthermore, MGP’s chemical structure binds calcium crystals preventing calcium depositing in the vascular tissue[9].
Studies have found associations between low vitamin K status and CKD, as plasma dp-ucMGP levels have been found to increase with the stage of the disease[15]. This is believed to be both due to decreased vitamin K intake due to a potassium-restrictive diet, adverse effects of medications, and disease-related impaired vitamin K metabolism[16]. As CKD patients are also at markedly increased risk of arterial calcification, there is an interest in investigating vitamin K supplementation as a therapeutic intervention in CKD patients[17]. One scoping review highlighted the potential of vitamin K as a therapeutic target in CKD, though optimal dosing remains unclear[18]. Supplementation in haemodialysis patients reduced dp-ucMGP levels and slowed vascular calcification progression, especially in those with existing calcifications[19]. However, a review from 2021 concluded that there is no strong evidence that vitamin K supplementation slows progression of calcification in CKD patients, but that the supplementation is safe and improves serum markers[17].
Vitamin K also shows potential as a nephroprotective measure by regulating the tissue damaging pathogeneses. Few studies have investigated the effect of vitamin K on glycaemic status, inflammation, and insulin resistance. A study from 2018 found that supplementation with vitamin K1 reduced the activation of the NF-kB pathway and secretion of pro-inflammatory cytokines. Furthermore, they found that, within a patient population with T2D, there was a strong association between low levels of vitamin K1 and increased insulin resistance. Vitamin K1 supplementation was found to reduce insulin resistance and enhance glycaemic status in both mice and patients with T2D, supporting the potentially preventive properties of vitamin K in subjects with T2D[20]. A review from 2016 found that supplementation with vitamin K1 reduced the expression of the pro-inflammatory cytokine IL-6, contributing to the potential anti-inflammatory properties of vitamin K[21].
A recent cross-sectional general population study in adults found that increasing levels of plasma dp-ucMGP were linked to central obesity, diabetes, hyperlipidaemia, and reduced kidney function[22]. Thus, one doubling of dp-ucMGP was associated with ten times (OR 9.83, 95% CI 5.49–17.59) increased risk of reduced kidney function. Interestingly, within the subgroup of hypertensive participants the association between lower vitamin K status and increased risk of reduced kidney function was even higher[22]. In conclusion, these studies suggest a potential role of vitamin K in kidney disease. However, the exact mechanisms and clinical importance of vitamin K in kidney disease are still not clear. While CKD and impaired kidney function seems to be associated with vitamin K deficiency, less is known about whether vitamin K deficiency is associated with progression of CKD and whether improvement of vitamin K status, e.g. by supplementation, can prevent or change the course of CKD.
We aimed to perform a scoping review investigating the current evidence on the effect of vitamin K deficiency and supplementation on renal function across general adult populations and CKD patient populations.
The introduction should briefly place the study in a broad context and highlight why it is important. It should define the purpose of the work and its significance. The current state of the research field should be carefully reviewed and key publications cited. Please highlight controversial and diverging hypotheses when necessary. Finally, briefly mention the main aim of the work and highlight the principal conclusions. As far as possible, please keep the introduction comprehensible to scientists outside your particular field of research. References should be numbered in order of appearance and indicated by a numeral or numerals in square brackets—e.g., [1] or [2,3], or [4,5,6]. See the end of the document for further details on references.
2. Materials and Methods
This scoping review was conducted in agreement with Joanna Briggs Institute’s methodology using the PRISMA extension for scoping reviews (PRISMA-ScR)[23]. A protocol including an initial limited search was conducted prior to the final literature search. The final search strategy was based on biomarkers and terms relating to CKD and renal function in one mesh term category and biomarkers and terms relating to vitamin K in the second (Appendix, Table A1 and Table A2).
We utilised PubMed database to identify studies that investigated the effect of vitamin K supplementation or vitamin K deficiency on markers of kidney function, progression of kidney disease or kidney transplantation. We included studies on general adult populations, with normal kidney function, and CKD patient population, with or without other known diseases. The search included cohort studies or clinical trials, published in English regardless of date of publication or geographical location.
All identified articles/citations were uploaded into Covidence, and duplicates were removed[24]. Titles and abstracts were independently screened by two reviewers, M.K. Torbensen and V.T. Wegge, and selected articles were full text screened. Disagreements were resolved through discussion. Final articles for inclusion were additionally examined by an experienced third reviewer, J.A. Lauridsen (Figure B1). We used and modified a Covidence data extraction tool. The extracted data included information on participants, study design and key findings relevant to this scoping review’s objective.
The reference list of all included sources of evidence was screened for potential additional studies by screening cross-references.
3. Results
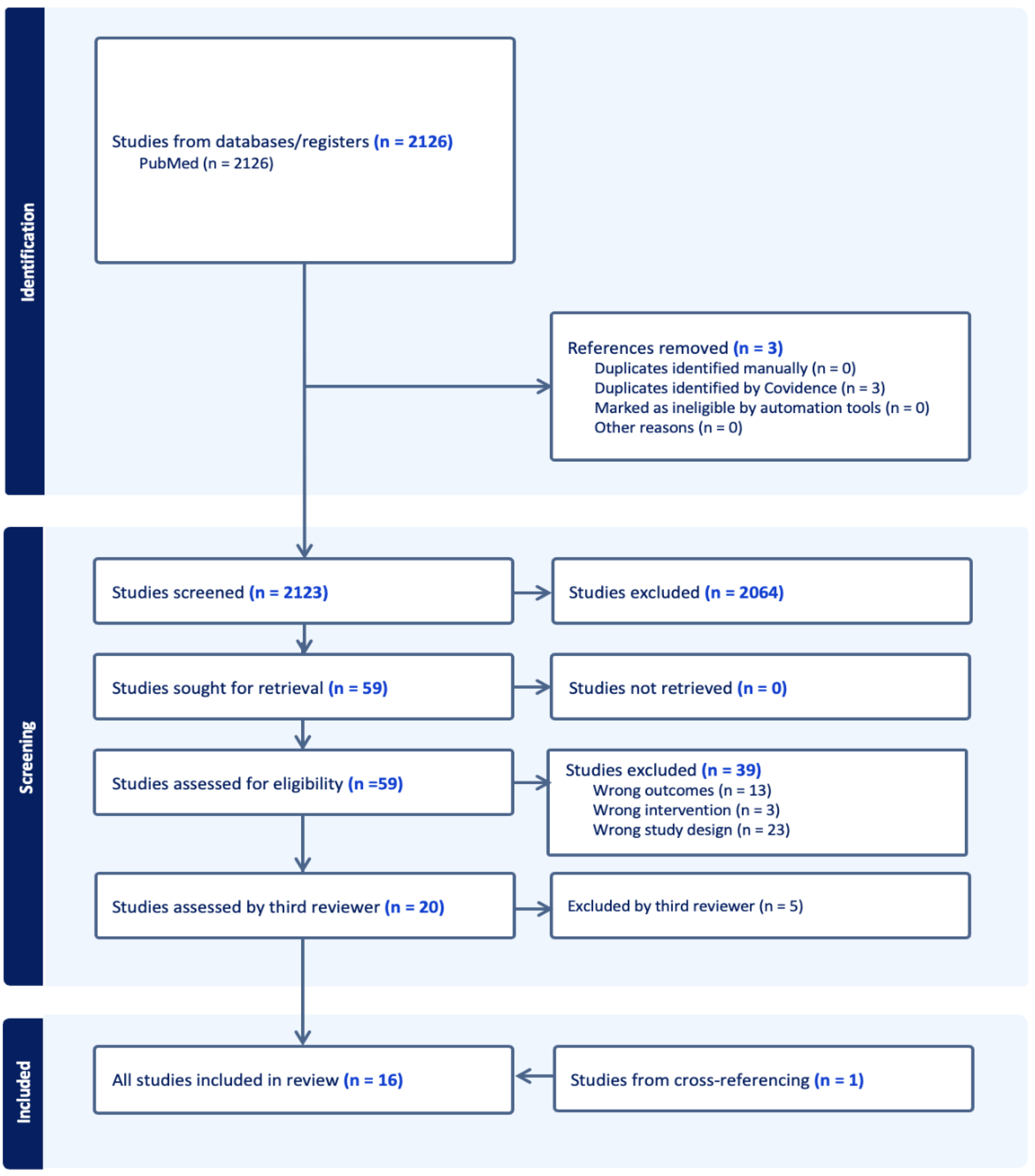
Our literature search identified 2,126 studies from the PubMed database of which three were duplicates. Through title and abstract screening, 2,064 articles were deemed irrelevant to the present review, leaving 59 articles for full text screening. Following full text screening, a total of 39 articles were excluded, 13 due to non-relevant outcomes, three studies due to wrong interventions, 23 due to non-relevant study designs. We cross-referenced the 59 articles and found one article not yet included in our search. The third reviewer screened the final 20 articles which led to exclusion of five articles due to non-relevant study design. Thus 15 articles were included from the literature search and one from cross referencing, leaving 16 articles for final extraction (Figure B1). The 16 articles consisted of nine clinical trials (Table C1) and seven cohort studies (Table C2). The clinical trials consisted of eight randomized controlled trials (RCTs) and one non-controlled trial in patients. Three studies were conducted in populations of kidney transplant recipients (KTR), three in patients with varying degree of chronic kidney disease (CKD 3-5), and three in haemodialysis (HD) patients. The cohorts consisted of three studies in adult general populations, and four in patient populations (KTR (two studies), T1D (one study) and CKD patients (one study)). Nine of the 16 included studies had one or more primary outcomes relating to kidney function (transplant failure (two studies), decline in kidney function, incident CKD or progression of CKD (five studies)). 13 studies had dp-ucMGP, ucMGP or MGP levels, as measurements for vitamin K status. Four studies had uncarboxylated osteocalcin (ucOC) and/or ucOC/OC ratio as marker, one study had phylloquinone levels as a marker and finally two studies had no measurement for vitamin K status. Two studies had a primary outcome relating to association of dp-ucMGP levels and kidney function (one study) or dp-ucMGP levels and dietary intake of vitamin K1 and vitamin K2 (one study). The remaining studies included secondary outcomes relating to kidney function.
3.1. Experimental Studies
3.1.1. Chronic Kidney Disease
Three RCTs in CKD patients investigated effects of vitamin K supplementation on the progression of kidney disease. Witham et al. performed a RCT that found no treatment effect on the estimated glomerular filtration rate (eGFR) or urine albumin-creatinine ratio (UACR) after 400 µg/day MK-7 supplementation for 12 months in 159 adult patients with CKD (n=80 intervention, n=79 placebo)[25]. In two separate RCTs, Kurnatowska et al. found that dp-ucMGP levels declined significantly following supplementation with 90 µg/day MK-7 + 10 µg vitamin D for 270±12 days compared to the control group receiving only vitamin D supplementation. They included 42 stage 3-5 patients in 2015 (n=29 intervention, n=13 placebo) and 38 stage 4-5 patients in 2016 (n=26 intervention, n=12 placebo). The trial from 2015 found a significant between-groups difference in eGFR after intervention, with decline in eGFR in the intervention group, though this group had a lower eGFR at baseline when compared to the placebo group, they did not adjust for the baseline difference. They also found a significant rise in creatinine in the intervention group which was borderline significant in the between-groups difference. The trial in 2016 showed a strong inverse association between eGFR and dp-ucMGP levels, and found correlations between dp-ucMGP levels, creatinine, and proteinuria, but no significant between-group change in eGFR between the supplementation and placebo groups [26,27]
3.1.2. Kidney Transplant Recipients
Lees et al. performed a RCT examining the effect of 5 mg menadiol diphosphate (vitamin K analogue) thrice weekly for 12 months on the kidney outcomes proteinuria, eGFR and urine protein creatinine ratio in 90 KTR (n=45 intervention, n=45 placebo). They observed no treatment effect on eGFR or proteinuria [28]. Eelderink et al. also reported no significant change in kidney function (eGFR or creatinine clearance) in their RCT following 360 µg/day MK-7 treatment for 12 weeks in 40 patients (n=20 intervention n=20 placebo)[29]. Mansour et al. performed a non-controlled clinical trial supplementing 60 KTR patients (no control group) with 360 µg/day MK-7 for 8 weeks. They found a small, but statistically significant increase in serum creatinine, indicating a decline in kidney function, although no adjustments were made for this outcome[30].
3.1.3. Haemodialysis Patients
Three RCTs in HD populations assessed serum creatinine after different supplementation strategies. Naiyarakseree et al. performed an intervention with supplementation of 375 µg/day MK-7 for 24 weeks in 96 patients (50 intervention, n=46 control group), Oikonomaki et al. supplemented 200 µg/day MK-7 for 12 months in 102 patients (n=58 intervention, n=44 control group) and Macias-Cervantes supplemented 10 mg intravenous vitamin K1 thrice weekly for 12 months in 60 patients (n=30 intervention, n=30 placebo). All three studies had creatinine as the only marker of kidney function, and none of the studies showed a significant between-groups difference following intervention[31,32,33].
3.2. Cohort Studies
3.2.1. General Adult Populations
Three cohort studies in the general adult population examined associations between vitamin K status and kidney function. Groothof et al. assessed a cohort of 3,969 adults with a mean follow-up period of 7.1 years. In the crude analyses, Groothof et al. found strong associations between high dp-ucMGP levels at baseline and incident CKD and microalbuminuria, but these associations disappeared when adjusting for baseline eGFR[34]. O’Seaghdha et al. assessed 1,442 adults with a mean follow-up of 7.8 years. They found a higher risk of CKD and microalbuminuria with higher vitamin K1 levels (four quartiles of phylloquinone levels) at follow-up. These associations remained significant after multivariable adjustment including eGFR[35]. Wei et al. assessed 1,009 adults with a median follow-up 8.9 years. They identified an inverse association between dp-ucMGP levels and eGFR, with high baseline dp-ucMGP levels (indicating low vitamin K status) predicting eGFR decline, though adjustment for baseline eGFR was not specified[36].
3.2.2. Cohort Studies in Kidney Transplant Recipient
Two cohort studies examined kidney transplant recipients. Van Ballegoijen et al. assessed 461 KTR with stable kidney function with a median follow-up period of 9.8 years. They found that elevated dp-ucMGP levels (dp-ucMGP >1057 pmol/L) in combination with both low and high vitamin D levels was associated with higher hazard ratios for death censored graft failure (defined as return to dialysis therapy or re-transplantation), compared to the group with lower dp-ucMGP levels (dp-ucMGP <1057 pmol/L) both in crude and when adjusting for age, sex, any cyclic variation, current smoking status, body mass index, triglycerides, average blood glucose levels, systolic blood pressure, year of transplantation, dialysis duration and eGFR[37]. Keyzer et al. assessed 518 KTR for a mean period of 9.8 years. They reported an association between higher quartiles of dp-ucMGP and transplant failure (defined by return to dialysis therapy or re-transplantation), though the association reduced with adjustment models and finally became non-significant after adjusting for baseline eGFR[38].
3.2.3. Cohort Study in Type 1 Diabetes Patients
In a cohort of 638 patients with T1D followed for 5-7 years, Nielsen et al. found that higher quartiles of dp-ucMGP (low vitamin K status) were associated with markedly increased risk of incident end stage kidney disease (ESKD). This association remained in crude and partially adjusted models but was lost after adjusting for baseline eGFR, albuminuria and T1D-duration[39].
3.2.4. Cohort Study in Chronic Kidney Disease Cohort
Roumeliotis et al. followed 66 type 2 diabetic CKD patients for 7 years, reporting positive correlation between dp-ucMGP levels and proteinuria. They found an inverse correlation between dp-ucMGP levels and both baseline and follow-up eGFR. Higher dp-ucMGP levels (≥656 pmol/L) were associated with 4.02 times higher longitudinal risk of a ≥30% reduction in eGFR or progression to ESKD in a multivariate model adjusted for T2D-duration, serum albumin and proteinuria[40].
4. Discussion
Vitamin K supplementation in eight RCTs and one non-controlled trial consistently reduced dp-ucMGP levels in CKD patients, KTR, and HD patients, but no beneficial changes in eGFR, creatinine, or proteinuria were observed. Two studies showed a significant decline in kidney function after intervention. In the general adult populations, three cohort studies reported associations between low vitamin K status, measured as high dp-ucMGP levels, and indicators of impaired kidney function in terms of reduced eGFR, increased risk of incident CKD and microalbuminuria. While some of these associations attenuated after adjusting for baseline kidney function, others remained significant even after multivariable adjustment[35,36,37]. In kidney transplant recipients, one study reported a significant association between high dp-ucMGP levels (low vitamin K status) and graft failure after full adjustment, while others found no difference or attenuated effects after adjustment. Among patients with T1D or CKD, higher dp-ucMGP levels were associated with increased risk of ESKD and eGFR decline. The associations attenuated in the T1D group after adjustments and whilst the CKD group’s association remained significant, they reported a very limited adjustment model.
The nine experimental studies differed with regards to type, administration, dose, and duration of vitamin K supplementation. Across the studies they used vitamin K1, MK-7 or menadiol diphosphate either as oral tablets or intravenous administration. The dosages varied from 90µg to 400µg daily with a duration of intervention ranging from 8 weeks to 12 months. The heterogeneity of the studies limits the comparability and generalizability of the results. Only one of the studies were designed to investigate progression of CKD and progression of kidney function as a primary outcome, though with the lowest dose of supplementation. CKD often is a slowly progressing disease[41], making investigation of healthy subjects or patients in early stages of CKD difficult in clinical trials. This makes cohort studies in a general population more feasible for this research question. Another possibility for examining the potential preventive effects of vitamin K supplementation on CKD would be to include patients with diabetes or hypertension, as the incidence of CKD is higher within these groups. An experimental study in rats from 2015 showed a nephroprotective effect of vitamin K1 supplementation after streptozotocin-induced destruction of the beta cells in pancreas. Supplementation had significant beneficial effects on insulin levels, blood glucose, creatinine, albumin-creatinine ratio, urea and uric acid. It also showed a neutralization effect on histopathological change, and immunohistochemical changes in the kidneys of the vitamin K supplemented rats. The pro-inflammatory NF-kB was expressed widely in the streptozotocin induced rats and completely absent in the supplemented rats[42]. These results could point towards vitamin K being a protective factor against the adverse effects of diabetes on kidney function.
Of the eight included RCTs and one non-controlled clinical trial, six out of nine studies employed plasma dp-ucMGP as a marker of vitamin K status. These six studies all demonstrated significant lowering of dp-ucMGP levels in the intervention groups, demonstrating biological effect. However, no studies reported any significant or tendencies of improvements in renal endpoints such as eGFR, proteinuria, or creatinine, and two studies found significant increase in creatinine after intervention, indicating worsening of kidney function. This could suggest that supplementation of vitamin K does not prevent progression of kidney disease. Two studies even indicated a decrease in kidney function, but both studies had limitations, one did not include a control group and the other appeared to have marked differences in baseline characteristics between the intervention and control group. Arguably, it also points to gaps in the literature and the need for more studies. E.g., the dose and duration employed in the studies may have been insufficient to influence renal outcomes beneficially. The results could also mean that the beneficial effects of vitamin K supplementation are limited in these patient populations due to their pre-existing kidney disease and impaired vitamin K function. Several factors likely play a role in development of functional vitamin K deficiency. A study by Kaesler et al. have found that the pharmacokinetics of vitamin K (K1, MK-4 and MK-7) are altered in patients with uraemia, a complication to CKD. In their prospective clinical trial, they observed changes in high density lipoprotein (cholesterol) particles in patients with uraemia causing reduced uptake of MK-7, impairment of the vascular protective function and potentially contributing to calcification of the arteries. Furthermore, in the same study, clinical trials in CKD rats showed altered vitamin K recycling, an essential part of the vitamin K cycle[16]. These findings could indicate that CKD patients may not benefit from vitamin K supplementation due to decreased bioavailability and reuse of vitamin K. Whether these barriers may be overcome by increasing the dose of vitamin K in interventional studies is not known.
The general adult populations studies reported associations between low vitamin K status and several kidney disease outcomes, however, in several of the studies, these associations became non-significant after adjustment for baseline eGFR. The fact that most studies lost significance after adjusting for baseline eGFR could either point to the baseline kidney function driving the effect of vitamin K on the progression of kidney disease or potentially mediating the effect. In case of the latter, adjusting increases the risk of missing a potential therapeutic effect of vitamin K supplementation. In general, the studies were not consistent in their approach when accounting for potential confounders. This could point to the interplay between vitamin K and kidney function being complex and further analyses are required to uncover the effects.
5. Conclusions
In this scoping review we investigated the role of vitamin K in the decline in kidney function and progression of CKD. While observational studies provided evidence of a temporal association of low vitamin K status and decrease in kidney function, interventional studies did not suggest that vitamin K supplementation could prevent decline in kidney function markers. The populations and study settings in the interventional studies differed on several parameters including sample size and type, administration, dose and duration of vitamin K supplementation. Study heterogeneity makes comparability and generalisability of the results difficult. Our results indicate the interplay between vitamin K and kidney function is complex and in need of further studies to uncover whether vitamin K supplementation could prevent decline of kidney function in patients or even prevent development of CKD in high-risk groups. Both observational and interventional studies in larger patient groups with renal endpoints are needed to clarify the preventive and therapeutic potential of vitamin K supplementation
Author Contributions
J.A. Lauridsen conceived the idea for the scoping review. M.K. Torbensen and V.T. Wegge contributed equally to this paper in developing the protocol, conducting the literature search and screening, extracting and charting the data, and drafting the manuscript. A. Linneberg provided expert feedback throughout the writing process and critically revised the manuscript. J.A. Lauridsen provided guidance in every step of the process, on the methodology, assisted as third reviewer, and supervised the project. Conceptualization, M.K. Torbensen, V.T. Wegge and J.A. Lauridsen; methodology, M.K. Torbensen, V.T. Wegge and J.A. Lauridsen; validation, A. Linneberg, and J.A. Lauridsen; investigation, M.K. Torbensen and V.T. Wegge; resources A. Linneberg and J.A. Lauridsen; data curation M.K. Torbensen and V.T. Wegge; writing—original draft preparation, M.K. Torbensen and V.T. Wegge; writing—review and editing, A. Linneberg and J.A. Lauridsen; visualization, M.K. Torbensen and V.T. Wegge; supervision, J.A. Lauridsen; project administration, M.K. Torbensen, V.T. Wegge and J.A. Lauridsen. All authors have contributed to the interpretation of findings, critical revision of the manuscript, have read and agreed to the published version of the manuscript.
Funding
J.A. Lauridsen is funded by a grant from Independent Research Fund Denmark (grant number F-12815–03-14–01).
Data Availability Statement
No new data was created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments). Where GenAI has been used for purposes such as generating text, data, or graphics, or for study design, data collection, analysis, or interpretation of data, please add “During the preparation of this manuscript/study, the author(s) used [tool name, version information] for the purposes of [description of use]. The authors have reviewed and edited the output and take full responsibility for the content of this publication.”
Conflicts of Interest
A. Linneberg has received investigational products from Kappa Bioscience AS for an intervention trial (The InterVitaminK Trial; clinicatrials.gov identifier NCT05259046) using vitamin K2 supplements as the active intervention. The remaining authors declare no personal or financial conflict of interest. The remaining authors declare no personal or financial conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CKD | Chronic kidney disease |
| GFR | Glomerular filtration rate |
| NF-kB | Nuclear factor kappa beta |
| BMP2 | Bone morphogenic protein 2 |
| VSMC | Vascular smooth muscle cell |
| T2D | Type 2 diabetes |
| T1D | Type 1 diabetes |
| MKs | Menaquinones |
| VKDP | Vitamin K dependent protein |
| Dp-ucMGP | Dephospho-uncarboxylated matrix Gla protein |
| PIVKA | Protein induced by vitamin k absence |
| GAS-6 | Growth arrest specific protein 6 |
| OR | Odds ratio |
| CI | Confidence interval |
| RCT | Randomized controlled trial |
| KTR | Kidney transplant recipients |
| HD | Haemodialysis |
| Uc-OC | Uncarboxylated osteocalcin |
| OC | Osteocalcin |
| eGFR | Estimated glomerular filtration rate |
| UACR | Urine albumin creatinine ratio |
| ESKD | End stage kidney disease |
Appendix A. Search Strategy

Table A1.
Search terms related to chronic kidney disease and related biomarkers.
| MeSH terms | Kidney failure, chronic | Renal insufficiency, chronic | Renal insufficiency | Glomerulosclerosis focal segmental | Glomerular filtration rate | Estimated glomerular filtration rate | eGFR | Proteinuria | Albuminuria |
Renal Dialysis |
Dialysis |
|||
| Entry terms | Renal failure, chronic | Chronic renal insufficiencies | Renal insufficiencies | Segmental glomerulosclerosis focal | Filtration rate, glomerular | Proteinurias | Albuminurias | Dialyses, renal | Dialyses | |||||
| Chronic renal Failure | Renal insufficiencies, chronic | Kidney insufficiency | Glomerulo-nephritis, focal sclerosing | Filtration rates, Glomerular | Renal dialyses | |||||||||
| End-stage kidney disease | Chronic kidney insufficiency | Insufficiency, kidney | Focal sclerosing glomerulo-nephritides | Glomerular filtration rates | Dialysis, renal | |||||||||
| Disease, end-stage kidney | Chronic kidney insufficiencies | Kidney insufficiencies | Focal sclerosing glomerulonephritis | Rate, glomerular filtration | Hemodialysis | |||||||||
| End stage kidney Disease | Kidney insufficiencies chronic | Kidney failure | Glomerulo-nephritides, focal sclerosing | Rates, glomerular filtration | Hemodialyses | |||||||||
| Kidney disease, end-Stage | Chronic renal insufficiency | Failure, kidney | Sclerosing glomerulo-nephritides, focal | Dialysis, extracorporeal | ||||||||||
| ESRD | Kidney insufficiency, chronic | Failures, kidney | Sclerosing glomerulonephritis focal | Dialyses, extracorporeal | ||||||||||
| End-stage renal disease | Chronic kidney diseases | Kidney failures | Glomerulosclerosis focal | Extracorporeal dialyses | ||||||||||
| Disease, end-stage renal | Chronic kidney disease | Renal failure | Focal glomerulosclerosis | Extracorporeal dialysis | ||||||||||
| End stage renal disease | Disease, chronic kidney | Failure, renal | Focal segmental glomerulosclerosis | |||||||||||
| Renal disease, end-stage | Diseases, chronic kidney | Failures, renal | Hyalinosis, segmental glomerular | |||||||||||
| Renal disease, end stage | Kidney disease, chronic | Renal failures | Glomerular hyalinosis, segmental | |||||||||||
| Renal failure, end-stage | Kidney diseases, chronic | Hyalinosis, segmental | ||||||||||||
| End-stage renal failure | Chronic renal diseases | Segmental hyalinosis | ||||||||||||
| Renal failure, end stage | Chronic renal disease | Segmental glomerular hyalinosis | ||||||||||||
| Chronic kidney failure | Disease, chronic renal | |||||||||||||
| Diseases, chronic renal | ||||||||||||||
| Renal disease, chronic | ||||||||||||||
| Renal diseases, chronic | ||||||||||||||
| Abbreviations: eGFR, estimated glomerular filtration rate; ESRD, end-stage renal disease; MeSH, Medical Subject Headings; | ||||||||||||||
Table A2.
Search terms related to vitamin K and biomarkers of vitamin K status.
| MeSH terms | Carboxyprothrombin | Vitamin K1 | Vitamin K2 | Menaquinone 7 | Matrix Gla Protein | Dp-ucMGP | ucMGP | Osteocalcin | Vitamin K |
| Entry terms | Decarboxyprothrombin | Phyto-nadione | Mena-quinone | Menaquinone K7 | Gla protein, matrix | Desphospho-uncarboxylated matrix GLA protein, human | 4-Carboxyglutamic protein, bone | ||
| Des(gamma-carboxy)prothrombin | Phyllo-quinone | Vitamin K quinone | Vitamin MK 7 | Matrix gamma-carboxyglu-tamic acid protein | Dephosphory-lated uncarboxylated matrix Gla protein | 4 Carboxyglutamic protein, bone | |||
| Des-gamma-carboxy prothrombin | Phyto-menadione | Vitamin K2 | Menaquinone-7 | Bone 4-carboxy- glutamic protein |
|||||
| Descarboxylated prothrombin | Vitamin K1 | Mena-quinones | Vitamin K2(35) | Protein, bone 4-carboxyglutamic | |||||
| Descarboxyprothrombin | Konakion | 1,4-naphthalenedione, 2-(3,7,11,15,19,23,27-heptamethyl-2,6,10,14,18,22,26-octacosaheptaenyl)-3-methyl-, (all-E)- | Bone gamma-carboxyglutamic acid protein | ||||||
| Non-carboxylated factor II | Phyllohydro-quinone | Bone gamma carboxyglutamic acid protein | |||||||
| PIVKA II | Aqua-mephyton | Bone Gla protein | |||||||
| PIVKA-II | Protein, bone Gla | ||||||||
| protein induced by vitamin K absence or antagonist-II | Calcium-binding protein, vitamin K-dependent | ||||||||
| Des-gamma-carboxyprothrombin | Calcium binding protein, vitamin K dependent | ||||||||
| DCP (prothrombin) | Gla protein, bone | ||||||||
| Acarboxy prothrombin | Vitamin K-dependent bone protein | ||||||||
| protein induced by vitamin K absence or antagonists | Vitamin K dependent bone protein | ||||||||
| PIVKA | |||||||||
| Prothrombin precursor | |||||||||
| Isoprothrombin | |||||||||
| Abbreviations: DCP, Des-gamma-carboxy prothrombin; dp-ucMGP, dephospho-uncarboxylated matrix Gla protein; uc-MGP, uncarboxylated matrix Gla protein; PIVKA, protein induced by vitamin K absence or antagonist; | |||||||||
Appendix B
Figure B1.
PRISMA flowchart of included/excluded studies.
Appendix C. Extracted Data
Table C1.
Clinical trials.
| Author | Country | Title | Study design | Population description | Sample size | Intervention | Kidney outcome (Primary/secondary) | Vitamin K measurements/outcomes |
| Lees et al. 2021 | United Kingdom | The ViKTORIES trial: A randomized, double-blind, placebo-controlled trial of vitamin K supplementation to improve vascular health in kidney transplant recipients. | RCT | KTR with functioning kidney transplant for 1 year or more. | 90 | Vitamin K (menadiol diphosphate) 5 mg orally x3 weekly for 12 months + Placebo (n=45 intervention, n=45 placebo). | Secondary: No treatment effect on eGFR or urine protein-creatinine ratio between intervention group and placebo. | Dp-ucMGP: Significant lowering in intervention group to placebo. |
| Eelderink et al. 2023 | Netherlands | Effect of vitamin K supplementation on serum calcification propensity and arterial stiffness in vitamin K-deficient kidney transplant recipients: A double-blind, randomized, placebo-controlled clinical trial. | RCT | KTR with eGFR>20 and vitamin K deficiency (plasma dp-ucMGP >500 pmol/L). | 40 | Vitamin K2 (MK-7) 360 μg/day for 12 weeks + placebo (n=20 intervention, n=20 placebo). | Secondary: No treatment effect on eGFR. | Dp-ucMGP, ucOC, ucOC/cOC ratio: all showed significant lower score in treatment group compared with placebo. |
| Naiyarakseree et al. 2023 | Thailand | Effect of Menaquinone-7 Supplementation on Arterial Stiffness in Chronic Hemodialysis Patients: A Multicenter Randomized Controlled Trial. | RCT | Chronic HD patients with arterial stiffness (cfPWV ≥ 10 m/s). | 96 | Vitamin K2 (MK-7) 375 µg/daily for 24 weeks, no placebo (n=50 intervention, n=46 control). | No significant differences or changes in serum creatinine after 12 and 24 weeks. | No vitamin K measurements. |
| Witham et al. 2020 | United Kingdom | Vitamin K Supplementation to Improve Vascular Stiffness in CKD: The K4Kidneys Randomized Controlled Trial. | RCT | CKD patients stage 3b or 4 (defined as an eGFR of >15 ml/min and <45 ml/min). | 159 | vitamin K2 (MK-7) 400 µg tablet/day for 12 months + placebo (n=80 intervention, n=79 placebo). | eGFR, urinary protein-creatinine ratio and serum creatinine: No significant differences in intervention group to placebo. | Significantly lowered osteocalcin and log-transformed dp-ucMGP between intervention and placebo. |
| Kurnatowska et al. 2015 | Poland | Effect of vitamin K2 on progression of atherosclerosis and vascular calcification in nondialyzed patients with chronic kidney disease stages 3-5. | RCT | CKD stage 3-5 with eGFR <60 for at least 6 months. | 42 | Vitamin K2 (MK-7) 90 µg/day + 10 µg vitamin D for 270±12 days + placebo 10µg vitamin D/day (n=29 intervention, n=13 placebo). | Significant rise in serum creatinine in intervention group. Significant group difference in eGFR after intervention (decline in eGFR in intervention group). | Significant decrease in dp-ucMGP in intervention group, but no significant difference to placebo. Significant decrease in osteocalcin in treatment group, significant increase in placebo group, but no significant difference between the groups. Borderline significant increase in MGP for treatment group, no significant difference to placebo. |
| Oikonomaki et al. 2019 | Greece | The effect of vitamin K2 supplementation on vascular calcification in haemodialysis patients: a 1-year follow-up randomized trial. | RCT | ESRD patients on haemodialysis. | 102 | Vitamin K2 (MK-7) 200 µg/day for 12 months, no placebo (n=58 intervention, n=44 control). | No significant change or difference in serum creatinine. | Significant decrease in ucMGP in intervention group at 12 months follow-up and significant difference to placebo group. |
| Macias-Cervantes et al. 2024 | Mexico | Effect of vitamin K1 supplementation on coronary calcifications in hemodialysis patients: a randomized controlled trial. | RCT | Chronic haemodialysis patients. 58.3% (n=35) with diabetic nephropathy being the primary etiology of chronic kidney disease. The median duration of haemodialysis was 48 months (12–204). | 60 | Vitamin K1 10 mg IV x3 weekly, after haemodialysis session, for 12 months, placebo (n=30 intervention, n=30 placebo). | Secondary: Serum creatinine: No significant changes between groups at follow-up. | No vitamin K measurements. |
| Kurnatowska et al. 2016 | Poland | Plasma Desphospho-Uncarboxylated Matrix Gla Protein as a Marker of Kidney Damage and Cardiovascular Risk in Advanced Stage of Chronic Kidney Disease. | RCT | CKD patients stage 4-5 with a coronary calcification score (CACS) of ≥10 Agatston units. | 38 | Vitamin K2 (MK-7) 90 µg/day + 10 µg vitamin D for 270±12 days. Placebo with vitamin D 10 µg (n=26 intervention, n=12 placebo). | Primary: Association between plasma dp-ucMGP and kidney function (serum creatinine, eGFR and proteinuria): No significant change in eGFR in either group after substitution. Strong inverse association between eGFR and dp-ucMGP. Positive correlation between dp-ucMGP, creatinine and proteinuria. | Dp-ucMGP: Significant decrease from baseline to follow-up in intervention group, compared to placebo? Osteocalcin: Significant difference between groups at follow-up. |
| Mansour et al. 2017 | Lebanon | Vitamin K2 supplementation and arterial stiffness among renal transplant recipients-a single-arm, single-center clinical trial. | Non-Controlled clinical trial | KTR patients with functional renal graft. | 60 | Vitamin K2 (MK-7) 360 μg/day for 8 weeks, no control group (n=60 intervention). | Secondary: Serum creatinine: Borderline significant increase from baseline to follow-up. | Dp-ucMGP: Significant decrease from baseline to follow-up. |
|
Table C1: Data table of included clinical studies. Abbreviations: CKD, chronic kidney disease; cOC, carboxylated osteocalcin; dp-ucMGP, dephospho-uncarboxylated Matrix Gla-Protein; eGFR, Estimated glomerular filtration rate; ESKD, end stage kidney disease; KTR, kidney transplant recipients; MGP, matrix Gla protein; MK-7, menaquinone 7; Q1-Q4, quartiles 1-4; RCT, randomized controlled trial; T1D, type 1 diabetes; T2D, Type 2 diabetes; ucMGP, uncarboxylated matrix Gla protein; ucOC, uncarboxylated osteocalcin. | ||||||||
Table C2.
Clinical trials.
| Author | Country | Title | Study design | Aim of study/purpose | Population description | Sample size | Follow up (years) | Kidney Outcome (Primary/Secondary) | Vitamin K measurements |
| Van Ballegooijen et al. 2019 | Nether-lands | Joint association of vitamins D and K status with long-term outcomes in stable kidney transplant recipients. | Cohort study | The association of both vitamins D and K status, and vitamin D treatment with all-cause mortality and death-censored graft failure. |
Adult kidney transplant recipients. Stable kidney function, median 6.1 years post transplantation, mean age of 52 years, 53% male. | 461 | Median 9.8 | Primary: Associations of combined vitamin D and dp-ucMGP levels with graft failure(return to dialysis therapy or re-transplantation), showed significantly. Higher eGFR in the groups with low dp-ucMGP levels. | dp-ucMGP <1057pmol/L or ≧ 1057pmol/L. |
| Keyzer et al. 2015 | Nether-lands | Vitamin K status and mortality after kidney transplantation: a cohort study. | Cohort study | Investigating if Vitamin K defficiency increase risk of all cause mortality and transplant failure after kidney transplantation. | Kidney transplant recipients with stable kidney function, 56% male, mean age 51 years, median of 6 years after kidney transplantation. | 518 | Median 9.8 | Primary: Highest quartile showed significant increase in transplant failure in three adjustment models, association was lost after adjustment for baseline kidney function. | dp-ucMGP Quartiles Q1: <734pmol/L, Q2: 734-1038 pmol/L, Q3: 1039-1535 pmol/L and Q4: >1535 pmol/L. |
| Wei et al. 2017 | Belgium | Desphospho-uncarboxylated matrix Gla protein is a novel circulating biomarker predicting deterioration of renal function in the general population. | Cohort study | Does dp-ucMGP predict a decrease in eGFR. | Flemish from the FLEMENGHO family-based population study, present analysis covered period from 1996-2015, 50.6% women, white europeans. | 1009 | Median 8.9 | Primary: Association between eGFR and plasma dp-ucMGP. with significant decline in eGFR between low and high levels of dp-ucMGP. | dp-ucMGP low: mean 2.42 µg/L (1.87–3.06) and high mean 5.08 ug/L (4.22–6.30). |
| Nielsen et al. 2025 | Den-mark | The associations between functional vitamin K status and all-cause mortality, cardiovascular disease and end-stage kidney disease in persons with type 1 diabetes | Cohort study | To assess the association of dp-ucMGP with mortality, cardiovascular disease and progression to ESKD in persons with T1D | Data from a cohort of persons with T1D followed up at Steno Diabetes Center Copenhagen, Denmark. 55% male. | 667 | Approximately 5-7 | Primary: Progression of ESKD. Lost significance in multivariable adjustment model four after adjusting for baseline eGFR and urinary albumin excretion rate. | dp-ucMGP quartiles (pmol/L): 316.5 (302.0–336.0) 386.0 (370.0–398.0) 457.0 (433.5–478.0) 611.0 (551.0–775.0). |
| O'Seaghdha et al. 2012 | USA | Phylloquinone and vitamin D status: associations with incident chronic kidney disease in the Framingham Offspring cohort. | Cohort study | Investigating if deficiencies of vitamins D and K may be associated with incident CKD and/or incident albuminuria in general population. | Framingham Heart Study participants (mean age 58 years; 50.5% women), free of CKD (eGFR<60 ml/min/1.732). |
1442 | Median 7.8 | Primary: Significantly higher incidence of CKD in the highest quartile of phylloquinone. Secondary: Significant association between higher quartiles of phylloquinone and incident albuminuria, but a borderline significance in the highest quartiles. | Phylloquinone levels stratified into 4 quartiles (nmol/L): 0.05-0.55, 0.56-0.98, 0.99-1.77 and 1.78-35.02. |
| Groothof et al. 2020 | Nether-lands | Functional vitamin K status and risk of incident chronic kidney disease and microalbuminuria: a prospective general population-based cohort study. | Cohort study | To assess the association between. circulating dp-ucMGP and incident CKD |
Inhabitants from the city of Groningen, mean age 52.3 years, mainly Caucasian. | 3969 | Median 7.1 | Primary: Incident CKD or microalbuminuria. The association of plasma dp-ucMGP with incident CKD disappeared following adjustment for the confounding effect of baseline eGFR. The association to proteinuria in males disappeared after adjustment for age. | Dp-ucMGP levels stratified in four quartiles (pmol/L) Males: <245, 245–381, 382–550 and >550. Females: <193, 193-341, 342–513 and >513. |
| Roumeliotis et al. 2020 | Greece | The Association of dp-ucMGP with Cardiovascular Morbidity and Decreased Renal Function in Diabetic Chronic Kidney Disease. | Cohort study | Investigating the association between dp-ucMGP and mortality, CV disease, and decreased renal function in a cohort of patients with diabetic CKD. | Diabetic CKD patients, divided into two groups: dp-ucMGP over and under 656 pM Mean age 67.4 (dp-ucMGP <656 pM) Mean age 69.7 (dp-ucMGP >656 pM) Almost all male in both groups. |
66 | Median 7 | Primary: Significantly higher risk of eGFR decline or progression to ESKD which remained after adjustment for T2D, proteinuria and serum albumin. | Dp-ucMGP < 656 pmol/L and Dp-ucMGP ≥ 656 pmol/L. |
|
Table C2: Data table of included cohort studies. Abbreviations: CKD, chronic kidney disease; dp-ucMGP, dephosphorylated-uncarboxylated matrix Gla-protein; eGFR, estimated glomerular filtration rate; ESKD, end stage kidney disease; Q1-Q4, quartiles 1-4; T1D, type 1 diabetes; T2D, type 2 diabetes; ucMGP, uncarboxylated matrix Gla-protein. | |||||||||
References
- Hill NR, Fatoba ST, Oke JL, Hirst JA, O’Callaghan CA, Lasserson DS, et al. Global Prevalence of Chronic Kidney Disease – A Systematic Review and Meta-Analysis. PLoS One 2016;11. [CrossRef]
- Düsing P, Zietzer A, Goody PR, Hosen MR, Kurts C, Nickenig G, et al. Vascular pathologies in chronic kidney disease: pathophysiological mechanisms and novel therapeutic approaches. J Mol Med (Berl) 2021;99:335. [CrossRef]
- Shea MK, Booth SL. Vitamin K, Vascular Calcification, and Chronic Kidney Disease: Current Evidence and Unanswered Questions. Curr Dev Nutr 2019;3. [CrossRef]
- Dai L, Li L, Erlandsson H, Jaminon AMG, Qureshi AR, Ripsweden J, et al. Functional vitamin K insufficiency, vascular calcification and mortality in advanced chronic kidney disease: A cohort study. PLoS One 2021;16. [CrossRef]
- Rizzoni D, Agabiti-Rosei E. Structural abnormalities of small resistance arteries in essential hypertension. Intern Emerg Med 2012;7:205–12. [CrossRef]
- Oates JC, Russell DL, Van Beusecum JP. Endothelial cells: potential novel regulators of renal inflammation. American Journal of Physiology-Renal Physiology 2022;322:F309–21. [CrossRef]
- Shioi A, Morioka T, Shoji T, Emoto M. The Inhibitory Roles of Vitamin K in Progression of Vascular Calcification. Nutrients 2020;12:583. [CrossRef]
- Alicic RZ, Rooney MT, Tuttle KR. Diabetic kidney disease: Challenges, progress, and possibilities. Clinical Journal of the American Society of Nephrology 2017;12:2032–45. [CrossRef]
- Lacombe J, Guo K, Bonneau J, Faubert D, Gioanni F, Vivoli A, et al. Vitamin K-dependent carboxylation regulates Ca2+ flux and adaptation to metabolic stress in β cells. Cell Rep 2023;42. [CrossRef]
- Moore DJ, Leibel NI, Polonsky W, Rodriguez H. Understanding the different stages of type 1 diabetes and their management: a plain language summary. Curr Med Res Opin 2025;41:13–24. [CrossRef]
- Bhikadiya D, Bhikadiya K. Calcium Regulation And The Medical Advantages Of Vitamin K2. South East Eur J Public Health 2024:1568–79. [CrossRef]
- Roumeliotis S, Dounousi E, Salmas M, Eleftheriadis T, Liakopoulos V. Vascular Calcification in Chronic Kidney Disease: The Role of Vitamin K- Dependent Matrix Gla Protein. Front Med (Lausanne) 2020;7:154. [CrossRef]
- Chen HG, Sheng LT, Zhang YB, Cao AL, Lai YW, Kunutsor SK, et al. Association of vitamin K with cardiovascular events and all-cause mortality: a systematic review and meta-analysis. Eur J Nutr 2019;58:2191–205. [CrossRef]
- Van Der Meer JHM, Van Der Poll T, Van’t Veer C. TAM receptors, Gas6, and protein S: roles in inflammation and hemostasis. Blood 2014;123:2460–9. [CrossRef]
- Thamratnopkoon S, Susantitaphong P, Tumkosit M, Katavetin P, Tiranathanagul K, Praditpornsilpa K, et al. Correlations of Plasma Desphosphorylated Uncarboxylated Matrix Gla Protein with Vascular Calcification and Vascular Stiffness in Chronic Kidney Disease. Nephron 2017;135:167–72. [CrossRef]
- Kaesler N, Schreibing F, Speer T, Puente-Secades S de la, Rapp N, Drechsler C, et al. Altered vitamin K biodistribution and metabolism in experimental and human chronic kidney disease. Kidney Int 2022;101:338–48. [CrossRef]
- Grzejszczak P, Kurnatowska I. Role of Vitamin K in CKD: Is Its Supplementation Advisable in CKD Patients? Kidney Blood Press Res 2021;46:523–30. [CrossRef]
- Bellone F, Cinquegrani M, Nicotera R, Carullo N, Casarella A, Presta P, et al. Role of Vitamin K in Chronic Kidney Disease: A Focus on Bone and Cardiovascular Health. Int J Mol Sci 2022;23:5282. [CrossRef]
- Taher M, Wafa E, Sayed-Ahmed N, el Dahshan K. Correlation Between Matrix Gla Protein Level and Effect of Vitamin K2 Therapy on Vascular Calcification in Hemodialysis Patients. Nephrology Dialysis Transplantation 2023;38. [CrossRef]
- Dihingia A, Ozah D, Baruah PK, Kalita J, Manna P. Prophylactic role of vitamin K supplementation on vascular inflammation in type 2 diabetes by regulating the NF-κB/Nrf2 pathway via activating Gla proteins. Food Funct 2018;9:450–62. [CrossRef]
- Manna P, Kalita J. Beneficial role of vitamin K supplementation on insulin sensitivity, glucose metabolism, and the reduced risk of type 2 diabetes: A review. Nutrition 2016;32:732–9. [CrossRef]
- Lauridsen JA, Leth-Møller KB, Møllehave LT, Kårhus LL, Dantoft TM, Kofoed KF, et al. Investigating the associations between uncarboxylated matrix gla protein as a proxy for vitamin K status and cardiovascular disease risk factors in a general adult population. Eur J Nutr 2025;64:1–9. [CrossRef]
- Peters, MDJ; Godfrey, C; McInterney, P; Munn, Z; Tricco, AC; Khalil, H. Scoping Reviews (2020). Aromataris E, Lockwood C, Porritt K, Pilla, B; Jordan, Z; editors. JBI Manual for Evidence Synthesis. JBI; 2024. Available from: https://synthesismanual.jbi.global. Last accessed: 20/05/2025; n.d. [CrossRef]
- Covidence 2025. Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org. Last accessed: 25/05/2025; n.d.
- Witham MD, Lees JS, White M, Band M, Bell S, Chantler DJ, et al. Vitamin K Supplementation to Improve Vascular Stiffness in CKD: The K4Kidneys Randomized Controlled Trial. J Am Soc Nephrol 2020;31:2434–45. [CrossRef]
- [Kurnatowska I, Grzelak P, Masajtis-Zagajewska A, Kaczmarska M, Stefańczyk L, Vermeer C, et al. Plasma Desphospho-Uncarboxylated Matrix Gla Protein as a Marker of Kidney Damage and Cardiovascular Risk in Advanced Stage of Chronic Kidney Disease. Kidney Blood Press Res 2016;41:231–9. [CrossRef]
- Kurnatowska I, Grzelak P, Masajtis-Zagajewska A, Kaczmarska M, Stefańczyk L, Vermeer C, et al. Effect of vitamin K2 on progression of atherosclerosis and vascular calcification in nondialyzed patients with chronic kidney disease stages 3-5. Pol Arch Med Wewn 2015;125:631–40. [CrossRef]
- Lees JS, Rankin AJ, Gillis KA, Zhu LY, Mangion K, Rutherford E, et al. The ViKTORIES trial: A randomized, double-blind, placebo-controlled trial of vitamin K supplementation to improve vascular health in kidney transplant recipients. Am J Transplant 2021;21:3356–68. [CrossRef]
- Eelderink C, Kremer D, Riphagen IJ, Knobbe TJ, Schurgers LJ, Pasch A, et al. Effect of vitamin K supplementation on serum calcification propensity and arterial stiffness in vitamin K-deficient kidney transplant recipients: A double-blind, randomized, placebo-controlled clinical trial. Am J Transplant 2023;23:520–30. [CrossRef]
- Mansour AG, Hariri E, Daaboul Y, Korjian S, A EA, Protogerou AD, et al. Vitamin K2 supplementation and arterial stiffness among renal transplant recipients-a single-arm, single-center clinical trial. J Am Soc Hypertens 2017;11:589–97. [CrossRef]
- Naiyarakseree N, Phannajit J, Naiyarakseree W, Mahatanan N, Asavapujanamanee P, Lekhyananda S, et al. Effect of Menaquinone-7 Supplementation on Arterial Stiffness in Chronic Hemodialysis Patients: A Multicenter Randomized Controlled Trial. Nutrients 2023;15. [CrossRef]
- Oikonomaki T, Papasotiriou M, Ntrinias T, Kalogeropoulou C, Zabakis P, Kalavrizioti D, et al. The effect of vitamin K2 supplementation on vascular calcification in haemodialysis patients: a 1-year follow-up randomized trial. Int Urol Nephrol 2019;51:2037–44. [CrossRef]
- Macias-Cervantes HE, Ocampo-Apolonio MA, Guardado-Mendoza R, Baron-Manzo M, Pereyra-Nobara TA, Hinojosa-Gutiérrez LR, et al. Effect of vitamin K1 supplementation on coronary calcifications in hemodialysis patients: a randomized controlled trial. J Nephrol 2025;38:511–9. [CrossRef]
- Groothof D, Post A, Sotomayor CG, Keyzer CA, Flores-Guerero JL, Hak E, et al. Functional vitamin K status and risk of incident chronic kidney disease and microalbuminuria: a prospective general population-based cohort study. Nephrol Dial Transplant 2021;36:2290–9. [CrossRef]
- O’Seaghdha CM, Hwang SJ, Holden R, Booth SL, Fox CS. Phylloquinone and vitamin D status: associations with incident chronic kidney disease in the Framingham Offspring cohort. Am J Nephrol 2012;36:68–77. [CrossRef]
- Wei FF, Trenson S, Thijs L, Huang QF, Zhang ZY, Yang WY, et al. Desphospho-uncarboxylated matrix Gla protein is a novel circulating biomarker predicting deterioration of renal function in the general population. Nephrol Dial Transplant 2018;33:1122–8. [CrossRef]
- Van Ballegooijen AJ, Beulens JWJ, Keyzer CA, Navis GJ, Berger SP, H de BM, et al. Joint association of vitamins D and K status with long-term outcomes in stable kidney transplant recipients. Nephrology Dialysis Transplantation 2020;35:706–14. [CrossRef]
- Keyzer CA, Vermeer C, Joosten MM, Knapen MH, Drummen NE, Navis G, et al. Vitamin K status and mortality after kidney transplantation: a cohort study. Am J Kidney Dis 2015;65:474–83. [CrossRef]
- Nielsen CFB, Thysen SM, Kampmann FB, Hansen TW, Jørgensen NR, Tofte N, et al. The associations between functional vitamin K status and all-cause mortality, cardiovascular disease and end-stage kidney disease in persons with type 1 diabetes. Diabetes Obes Metab 2025;27:348–56. [CrossRef]
- Roumeliotis S, Roumeliotis A, Stamou A, Leivaditis K, Kantartzi K, Panagoutsos S, et al. The Association of dp-ucMGP with Cardiovascular Morbidity and Decreased Renal Function in Diabetic Chronic Kidney Disease. Int J Mol Sci 2020;21:6035. [CrossRef]
- Schlackow I, Simons C, Oke J, Feakins B, O’Callaghan CA, Richard Hobbs FD, et al. Long-term health outcomes of people with reduced kidney function in the UK: A modelling study using population health data. PLoS Med 2020;17:e1003478. [CrossRef]
- Sai Varsha MKN, Raman T, Manikandan R, Dhanasekaran G. Hypoglycemic action of vitamin K1 protects against early-onset diabetic nephropathy in streptozotocin-induced rats. Nutrition 2015;31:1284–92. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



