Submitted:
14 July 2025
Posted:
15 July 2025
You are already at the latest version
Abstract
Ventricular tachycardia (VT) remains a major cause of morbidity and mortality in patients with structural heart disease. While catheter ablation has become a cornerstone in VT management, recurrence rates remain substantial due to limitations in electroanatomic mapping (EAM), particularly in cases of deep or heterogeneous arrhythmogenic substrates. Cardiac imaging, especially when multimodal and integrated with mapping systems, has emerged as a critical adjunct to enhance procedural efficacy, safety, and individualized strategy.
This comprehensive review explores the evolving role of various imaging modalities, including echocardiography, cardiac magnetic resonance (CMR), computed tomography (CT), positron emission tomography (PET), and intracardiac echocardiography (ICE), in the preprocedural and intraprocedural phases of VT ablation. We highlight their respective strengths in substrate identification, anatomical delineation, real-time guidance. While limitations persist, including costs, availability, artifacts in device carriers, and lack of standardization, future advances are likely to redefine procedural workflows.
Keywords:
imaging
; catheter ablation
; ventricular tachycardia
; cardiac magnetic resonance
; computed tomography
; intracardiac echocardiography
1. Introduction
Ventricular tachycardia (VT) remains a significant cause of cardiovascular morbidity and mortality, particularly in patients with structural heart disease[1].
Catheter ablation has emerged as a crucial treatment modality for this potentially life-threatening arrhythmia due to increasing evidences of its superiority over antiarrhythmic drugs [2,3,4,5,6]. However, despite technological advancements and increasing operator experience, the recurrence rate following ablation procedures remains not negligible [3].
Electroanatomic mapping (EAM), the gold standard for arrhythmogenic substrate characterization, has some limitations. Activation mapping is effective only if the arrhythmia is inducible, sustained, and well-tolerated. The evaluation of low-voltage areas depends on factors such as catheter tip orientation, tissue contact, and far-field effects from healthy myocardium. Additionally, substrate mapping and pace-mapping are less reliable when the arrhythmogenic substrate is located intramyocardially [7].
In recent years, cardiac imaging has assumed an increasingly relevant role in enhancing both the efficacy and safety of VT ablation procedures.
The expert consensus statement on VT ablation recommends integrating pre-procedural imaging for accurate identification of potential arrhythmogenic substrates and procedural planning [3].
Multimodal imaging techniques, including transthoracic and intracardiac echocardiography (ICE), cardiac magnetic resonance imaging (CMR), computed tomography (CT), Positron Emission Tomography (PET), have shown to be invaluable tools in the periprocedural evaluation of patients undergoing VT ablation. These advanced imaging-based approaches provide:
- Detailed characterization of the arrhythmogenic substrate
- Optimal planning of access strategies
- Real-time guidance during the procedure
- Assessment of ablation efficacy
The integration of imaging-derived information with EAM systems has led to a more precise and tailored approach to VT ablation. This synergy has significantly increased our understanding of the complex substrates underlying VT and has enabled more targeted and effective ablation strategies.
This review aims to critically examine the current role and future perspectives of various imaging modalities in facilitating and optimizing VT ablation procedures. We will explore the strengths and limitations of each imaging technique, discuss their integration into clinical practice, and highlight emerging technologies that promise to further refine our approach to VT ablation.
2. Pre-Procedural Imaging Assessment
Transthoracic echocardiography (TTE) represents an unexpensive and widely available imaging tool. It can provide a wide range of information regarding biventricular function, dimensions and valvular physiology. Reduced left ventricular ejection fraction (LVEF) and functional right ventricular indexes have been associated with extensive substrates and worse prognosis in patients with ischaemic heart disease or cardiomyopathies undergoing VT ablation [8,9]. In case of VT originating from the valvular apparatus, pre-procedural echocardiography could provide important clues regarding the anatomical structures involved (Figure 1, panel B and C). The presence of regional left or right ventricular wall motion abnormalities (i.e. segmental a-dyskinesia, regional wall thinning) could suggest the presence of underlying pathological substrate. However, detection of regional dysfunction is affected by significant inter-operator variability and low reproducibility. Over the years, speckle tracking techniques have demonstrated higher sensitivity in detecting subtle cardiac wall motion abnormalities compared to standard echocardiography [10]. Impaired echocardiographic endocardial and epicardial strain values have been associated with pathological bipolar and unipolar EAM areas in patients with ischemic heart disease undergoing ventricular arrhythmia ablation [11]. Deformation imaging analysis is able to reveal subtle pathological substrate in patients with cardio myopathies and impaired strain values have been associated with worse outcomes in subjects affected by arrhythmogenic cardiomyopathy (AC) or sarcoidosis [12,13,14].
Cardiac magnetic resonance (CMR) can provide comprehensive biventricular functional assessment together with multiparameter tissue characterization, a crucial factor in patients with arrhythmic phenotypes [1]. Left and right ventricular ejection fraction are established predictors of short and long-term adverse outcomes after VT ablation [3,15,16,17]. T2-weighted sequence and T2 mapping techniques can detect oedema in patients with inflammatory cardiomyopathies, thereby guiding dedicated diagnostic and therapeutic pathways. Late gadolinium enhancement (LGE) could be an expression of fibrosis, inflammation or expanded extracellular volume (Figure 1, panel D and E). LGE localization and pattern can provide crucial clues in the differential diagnosis between ischemic, genetic and acquired cardiomyopathies (Figure 2, panel B and C) [1,9] and it is crucial in setting up the procedural workflow. Presence and extent of LGE have been extensively associated with adverse arrhythmic events in patients with coronary disease and cardiomyopathies. Moreover, LGE location can suggest a preferential access (endocardial, epicardial or combined) depending on the predominant underlying substrate [18]. Over the years, high-resolution late gadolinium enhanced-CMR (LGE-CMR) has emerged as a novel non-invasive tool for detecting CC before the procedure through pixel signal intensity (PSI) analysis [19,20,21].
Although the clinical benefits of CMR have been widely investigated, it is only in recent years that evidence has emerged demonstrating its safe use and feasibility in the majority of patients with implantable cardioverter defibrillators (ICDs)[22,23]. Beyond safety concerns, a significant obstacle to the utilization of CMR-provided information in device carriers has long been represented by metal induced hyperintensity artifacts [24,25] on LGE images, which can appear similar to the hyperenhancement of scar tissue. These artifacts especially occur at regions of the heart that are close to the device generator, such as the anterior and lateral wall, and the outflow tracts [26]. Device-related artifacts also appear on cine and perfusion cardiac MR images, even if usually less important than those on LGE sequences. Luckily, over the last years novel LGE-CMR wideband (WB) sequences have been developed to attenuate these artifacts [27,28,29,30,31]. Roca-Luque et al. demonstrated that WB analysis can effectively detect arrhythmogenic CCs even in patients with ICD undergoing VT ablation [28]. Patel et al [32] recently evaluated a large population of ICD patients undergoing CMR with a WB technique, revealing that 36% had a new or changed diagnosis, and 28% experienced management changes, especially those with VT. Patients with LGE had worse outcomes, with a higher incidence of major adverse cardiac events (MACEs). Overall, LGE CMR proved to be highly valuable for clinical decision-making and prognosis in ICD patients.
Tissue characterization of the RV by CMR is hampered by the reduced thickness of the free wall and LGE identification is often difficult. CMR-derived feature tracking analysis could detect mild RV abnormalities and has been associated with pathological epicardial and endocardial EAM voltages in patients with arrhythmogenic cardiomyopathy, even in the absence of overt LGE [33]. Catheter Ablation of ventricular arrhythmias have been increasingly performed in patients with severe LV or RV dysfunction, often necessitating intensive care unit support and temporary LV or RV mechanical support. Therefore, novel scores, such as the PAINES2D (Pulmonary disease, Age, Ischemic cardiomyopathy, NYHA class, Ejection fraction, Storm, Scar volume, Diabetes), have been developed to predict the risk of hemodynamic decompensation after VT ablation [34]. In this setting, CMR can provide important prognostic information, such LVEF, right ventricular function and scar extent for periprocedural planning in high-risk subjects undergoing complex procedures.
Contrast-enhanced computed tomography (CT) has increasingly been used in many cardiovascular disorders, including coronary artery, valvular and pericardial diseases [35,36]. Multidetector CT (MDCT) can provide accurate information regarding wall thickness, myocardial perfusion and fat deposition [35,37]. MDCT can identify scar tissue and border zone which are commonly targeted during VT ablation procedures [38,39,40]. Lipomatous metaplasia can be detected in patients with coronary artery disease and cardiomyopathies [41,42,43,44] and it may play a significant role in promoting scar-related re-entry by affecting current leak and conduction velocity [45,46]. Moreover, MDCT can reveal other important prognostic elements, such as coronary artery plaques and unrecognized intracardiac thrombosis. Careful assessment of coronary anatomy and periprocedural multimodality imaging are crucial in case of an epicardial approach to reduce the risk of complications. Notably, MDCT can represent an appealing option for subjects with ICD affected by VT, even in cases when CMR is contraindicated or impaired by artifacts.
Positron emission tomography (PET) can provide crucial insights about metabolic cardiac pathways, especially in the presence of cardiac inflammation by use of 18F-fluorodeoxyglucose (FDG) or other tracers [18,47]. Inflammatory processes detected in patients undergoing PET before ablation led to identification of specific aetiologies (such as lymphocytic myocarditis and sarcoidosis) and improved the therapeutical management (Figure 2, panel D and E). Specifically, 18-FDG PET has emerged as a pivotal imaging tool for identifying cardiac and extracardiac sarcoidosis and it can help in planning optimal diagnostic and therapeutic pathways in these patients [48]. In this setting, RV uptake has been associated with worse prognosis in subjects with cardiac sarcoidosis [49]. It is to note that FDG-PET can reveal the presence of unrecognized cardiac inflammation, even in patients with arrhythmogenic cardiomyopathies carrying pathogenetic or likely pathogenetic variants [50]. Therefore, identification of inflammatory processes could potentially lead to the use of immunomodulatory therapies in patients with high arrhythmic burden and optimize the timing of catheter ablation (Figure 2). Even if less accurate than other imaging modalities, 18-FDG PET can identify metabolic heterogeneous zone. The burden of heterogeneous zone has been associated to poor prognosis in patients undergoing VT ablation [51].
3. Intraprocedural Imaging: Focus on Intracardiac Echocardiography
Intracardiac echocardiography (ICE) has emerged as an invaluable tool in the field of interventional electrophysiology, particularly in the context of VT ablation[52]. This advanced imaging modality offers real-time, high-resolution visualization of cardiac structures, enabling precise catheter navigation and improved procedural outcomes by simply positioning the ultrasound probe in the right atrium and ventricle [53]. Unlike transoesophageal echocardiography, ICE can be performed by the operator, without the need for general anaesthesia and oesophageal intubation [54]. The commonly used technology is phased-array ICE, which consists of a 64-element transducer mounted at the distal end of an 8- or 10-French steerable catheter. This catheter can be deflected in four directions (anterior, posterior, right, and left) and generates a wedge-shaped image displayed on a standard ultrasound workstation. Compared to mechanical rotational systems, phased-array ICE offers several advantages, including greater depth of penetration (up to 15 cm), enhanced maneuverability, and the capability to acquire Doppler and color flow imaging [54,55].
Intracardiac echocardiography-derived anatomical data can be merged with EAM Systems. In the CARTOSOUND module (CARTO, Biosense Webster, Inc., Diamond Bar, California, USA), a specially adapted ICE catheter (Soundstar) with an embedded positional sensor is employed. The device acquires several planar images at different angles within the cardiac chamber, and the inner wall is outlined either manually or through automated edge-detection algorithms (Figure 3, panel A). These contours are then assembled by the software to form a dynamic three-dimensional model, onto which electrical mapping data is subsequently superimposed. Intracavitary structures can be acquired as separate objects. A green marker is used to display the real-time location of the catheter tip when it intersects the ultrasound beam [54]. This integration allows for a more comprehensive understanding of the cardiac chambers anatomical features and enhances the precision of catheter navigation during ablation procedures (Figure 3).
The utility of ICE in VT ablation spans multiple domains, including anatomical delineation, substrate characterization, catheter-tissue contact assessment, and complication monitoring (Figure 1, panel F; Figure 3).
3.1. Anatomical Delineation and Catheter Navigation
ICE provides visualization of cardiac chambers, valvular structures, and intracardiac masses, facilitating accurate catheter positioning and navigation. In the context of VT ablation, ICE allows to obtain detailed imaging of the ventricular anatomy, including critical structures. By delineating the coronary cusps and identifying the origin of the coronary arteries, ICE may eliminate the need for coronary angiography in cases of arrhythmias originating from the coronary cusps. The term of “fourth dimension” has been proposed for intracavitary structures such as papillary muscles, false tendons, and the moderator band [56], which can serve as arrhythmogenic foci and are difficult to target during ablation due to their complex 3D geometry, not easily understandable with EAM alone. ICE allows accurate real time visualization of the anatomical landmarks of these structures, enabling operators to navigate complex anatomies with greater confidence and precision (Figure 1, panel F) [57,58,59,60]. EHRA Expert consensus on catheter ablation of ventricular arrhythmias recommend ICE (Class I, LOE B-NR) to identify and target the papillary muscles and to assess for catheter stability [3].
3.2. Substrate Characterization
One of the most significant advantages provided by ICE in VT ablation is its ability to visualize in real time the potential arrhythmogenic substrate. Even without offering the substrate characterization capabilities of MR and CT, ICE can identify areas of myocardial scarring (Figure 3, panel A), that serve as the substrate for reentrant VT circuits [61,62,63]. These regions typically appear as areas of increased echogenicity, wall thinning, or akinesis. Furthermore, ICE can detect intramural and epicardial substrates, guiding the procedural approach. This capability is particularly valuable in cases of non-ischemic cardiomyopathy [64,65].
3.3. Catheter-Tissue Contact Assessment
Optimal catheter-tissue contact is crucial for effective energy delivery and lesion formation during VT ablation. ICE provides real-time visualization of the catheter tip in relation to the myocardium, allowing operators to ensure adequate contact before and during radiofrequency energy application. This feature is especially useful when ablating in areas with complex anatomy or in regions where catheter stability may be challenging, such as papillary muscles. ICE is of critical importance during ablation in the right and left ventricular outflow tracts, as it allows for direct visualization of the valvular apparatus and enables accurate tagging of their position within the EAM system [54,66,67,68].
3.4. Complication Preventing and Monitoring
ICE plays a vital role in enhancing the safety profile of VT ablation procedures by enabling real-time monitoring for potential complications (fig). It allows for early detection of pericardial effusion, which can be a harbinger of cardiac perforation (Figure 3, panel B). Additionally, ICE can visualize microbubble formation during radiofrequency energy delivery, which may precede steam pops and tissue overheating [69]. The ability to detect these complications in their nascent stages allows for prompt intervention, potentially mitigating more severe sequelae. Furthermore, the ability to visualize cardiac chambers, access routes, and anatomical alterations in real-time before positioning the ablation catheter can guide the operator in avoiding manipulations of the ablation catheter in areas at risk of complications [70,71]. In Figure 3 panel C is showed a case of ischemic VT ablation in which the visualization of a large aortic plaque led the operator to avoid the retrograde transaortic approach and to perform the procedure using only the transseptal approach instead.
3.5. Reduction in Fluoroscopy Exposure
The use of ICE in VT ablation procedures has been associated with a significant reduction in fluoroscopy time and radiation exposure for both patients and operators. In some cases, ICE guidance has enabled the performance of “zero-fluoroscopy” VT ablation procedures, which is particularly beneficial for young patients or pregnant women. [66,67,68,72]
3.6. Procedural Outcomes and Clinical Impact
Despite the above-mentioned advantages offered by ICE, randomized studies on clinical impact are still lacking. A large retrospective analysis showed that the use of ICE during VT ablation was associated with a lower likelihood of 12-month VT-related readmissions and repeat ablations compared to procedures performed without ICE [73]. In a nationwide Japanese database the ICE group showed a lower prevalence of cardiac tamponade than non-ICE group with no additional clinical advantages [74].
3.7. Future Perspectives
The CARTOSOUND FAM module is a new deep learning imaging algorithm integrated with ICE for 3D reconstruction of cardiac anatomy without the need to manually annotate ultrasound (US) contours. This module is currently available for left atrium reconstruction [75,76]. If successfully applied to the ventricular chambers in the future, it could improve workflow efficiency and reduce operator dependency, as already highlighted in atrial fibrillation ablation.
The NuVision NAV is a 10 F ultrasound imaging catheter with a 4D ICE ultrasound transducer which conveys 3D location information that is integrated with the CARTO Navigation System (Biosense Webster), allowing for high-quality multiplanar reconstruction with minimal catheter manipulation. 4D ICE in a preclinical swine model demonstrated its ability to provide real-time multiplanar imaging and volumetric acquisition for guiding complex electrophysiology procedures. The technology allowed accurate electroanatomic reconstructions with minimal catheter movement and facilitated precise ablation of ventricular structures [77]. Potential benefits include reduced procedural time and improved safety.
These technological advancements are expected to further enhance the utility of ICE in VT ablation, providing electrophysiologists with more sophisticated tools for navigating complex cardiac structures.
4. Intraprocedural Imaging: Focus on CT and CMR
Integration of advanced imaging modalities, particularly MDCT and CMR, into EAM systems represents one of the major technological advancements in the field of transcatheter ablation in recent years. Integration of MDCT and CMR provides crucial information for procedural planning, substrate characterization, and real-time guidance during ablation.
Late gadolinium enhancement cardiac magnetic resonance (LGE-CMR) has emerged as a powerful tool for identifying and characterizing myocardial scar, which serves as the substrate for re-entrant VT circuits. LGE-CMR can delineate not only the core scar but also the heterogeneous border zone tissue, which has been shown to well correlate with areas of slow conduction and VT isthmuses identified on EAM.
Compared with MR, MDCT offers superior spatial resolution, allowing detailed assessment of the myocardial structure [53]. As a consequence, MDCT provides detailed anatomical information, including coronary artery and venous anatomy, valve apparatus, left phrenic nerve, which is particularly valuable in case of epicardial approach, for enhancing procedural safety [78]. Furthermore, CT can identify areas of epicardial fat, which may affect local electrogram characteristics and ablation efficacy. Even if MDCT provides high spatial resolution, it exhibits a lower contrast-to-noise ratio within myocardial tissue that can result in less accurate scar characterization, compared to MR [18], essential during VT ablation. In the past decade, various studies investigated the utility of importing anatomical and substrate information obtained from CT and CMR into the EAM system. The integration software initially available provided the integration of anatomic features of cardiac chambers, but the segmentation of coronary arteries and left phrenic nerve and, more important, the characterization of scar, were not supported.
After promising evidence gathered in small preliminary studies [79,80,81] a growing interest in imaging integration emerged, thanks also to the development of dedicated software enabling the integration of crucial patient specific data on cardiac anatomy and structural substrate.
In the study by Komatsu et al [40] the integration of MDCT wall thickness (WT) with 3D electroanatomic maps was useful to focus mapping and ablation on the culprit regions in postinfarction VT. A significant correlation was found between the areas of WT <5 mm and endocardial low voltage, but no such correlation was found in the epicardium. The vast majority (87%) of areas of low voltage and local abnormal ventricular activities (LAVA) were located in areas with WT < 5 mm or at its border and very late LAVA (>100 msec after QRS complex) were almost exclusively detected within the thinnest area (< 3 mm), showing a correlation between regional myocardial WT and low-voltage regions and distribution of LAVA critical for the generation and maintenance of postinfarction VT. However, despite a good correlation, WT <5 mm was consistently smaller than endocardial low-voltage area.
Yamashita et al [82] first reported the systematic use of imaging integration with CT or CMR in a substantial number of patients (116) undergoing catheter ablation of VT scar related of various etiologies. Image processing was obtained with a dedicated software, and all segmented structures were exported in the form of 3D meshes and loaded into 3D mapping systems.
Imaging integration allowed the identification of 89% of critical isthmuses and 85% of local abnormal ventricular activities (LAVA). CMR proved to be superior to CT in detecting arrhythmic substrates, but its use was limited to 30 patients due to exclusions criteria, like the presence of implanted defibrillators. CT, on the other hand, offered higher spatial resolution, enabling detailed visualization of cardiac structures, including the phrenic nerve and coronary arteries, which influenced epicardial ablation strategies in a significant number of cases. Imaging also prompted additional mapping in over half of the patients and epicardial access in a third, with CMR producing significantly fewer false positives compared to CT. Key messages of this study are that CMR is superior to CT in detecting arrhythmic substrates, although its feasibility is limited to patients without implanted devices. CT, on the other hand, excels in providing detailed anatomical resolution, allowing for precise identification of cardiac structures, but it is less accurate in identifying arrhythmic substrates.
Despite these limitations, MDCT remains a valuable alternative to CMR, provides important information for identification and characterization of arrhythmogenic substrate in postinfarction VT and can help focus mapping and ablation on the culprit regions [83].
Lipomatous metaplasia plays a role in the arrhythmogenic substrate of both ischemic and non-ischemic cardiomyopathies. This pathological process, characterized by the replacement of myocytes with adipose tissue within fibrotic scars [41,42,43,44], alters the electrophysiological properties of the myocardium, favoring slow conduction, promoting reentry circuits, and increasing overall susceptibility to ventricular arrhythmias. Differentiating adipose metaplasia from dense scar is important for precise substrate-based ablation strategies. In this context, the integration of CT into EAM systems represents a valuable tool. CT allows for high-resolution differentiation between adipose tissue and fibrosis (Figure 4). When combined with CMR, which provides detailed tissue characterization LGE, CT enhances the accuracy of substrate identification. The multimodal approach leveraging CT and CMR integration into mapping systems can refine procedural planning and optimize ablation outcomes by distinguishing adipose metaplasia from scar tissue, ultimately improving guidance for mapping and ablation [45,46,84,85].
The remarkable potential of CMR to characterize scar tissue and to facilitate catheter ablation has been confirmed by various studies including an increasing number of patients in recent years.
PSI techniques can provide a comprehensive picture of the extent, transmurality and heterogeneity of the underlying arrhythmic substrate by use of automatic LGE analysis. CCs are often located in the border zone area of the scar with a complex tridimensional architecture [86]. Recently, the evolution of these techniques has provided additional information regarding the true arrhythmogenic potential of CCs in terms of their ramifications and transmurality [86]. Moreover, CMR-based analysis has been able to detect CCs demonstrated by double extra stimulus testing even in areas with apparently normal EAM voltages [87].
In a prospective, experimental non randomized study of 54 patients, color-coded PSI maps were obtained from a high-resolution 3Tesla LGE-CMR study and were imported into the navigation system to aid the VT substrate ablation [88]. The heterogeneous tissue channels (HTCs) depicted in the PSI were correlated to EAM information. In this study, the gold standard was the identification of channels through EAM, while HTCs in the scar were considered true positives if confirmed by mapping, showing a 77% of concordance. Channels identified by mapping but not by CMR were classified as false negatives (23%). There was also a 16% rate of false positives, where CMR identified an arrhythmogenic substrate not confirmed by mapping, and no ablation was performed in these cases. Compared to the control group, the integration of CMR with mapping resulted in reduced radiofrequency applications, increased non-inducibility rates, and improved arrhythmia-free survival during follow-up. Interestingly, false positives identified by CMR had more events at follow-up, suggesting that in some cases CMR might define the arrhythmogenic substrates even better than electronatomic mapping.
Patients with cardiac devices were excluded in the studies presented so far. In the following years, the utilization of wideband sequences has enabled overcoming this limit.
Based on intriguing results obtained with CMR aided scar dechanneling [88], the same group evaluated the feasibility and potential benefit of VT substrate ablation entirely guided by CMR imaging in a subsequent study [89]. The authors prospectively compared a purely CMR-guided method using PSI maps alone with two historical approaches: standard EAM without CMR and EAM combined with CMR-derived PSI maps.
CMR-guided approach significantly shortened the procedure time, reduced fluoroscopy and lowers the rate of inducible VT after ablation compared to the other methods. Over 12 months of follow-up, patients treated with CMR guidance showed fewer arrhythmia recurrences than those undergoing ablation with no CMR, with no differences between CMR aided and guided ablation. The study highlights the safety, efficiency, and improved outcomes of integrating advanced CMR imaging into VT substrate ablation, offering a promising direction for optimizing the management of scar-related arrhythmias.
The VOYAGE trial [90] is an ongoing prospective, randomized, multi-center open-label study with control group involving a total of eight centers. The primary objective is to analyze the outcome of CMR guided and aided approaches of VT ablation in terms of effectiveness at 12 months in comparison to a control group (standard of care VT ablation). The primary endpoint is defined as any VT recurrences during a 12-months follow-up. The enrollment is concluded and the results are expected in next few months. In Figure 5 and Figure 6 are shown two examples of CMR aided and guided VT ablation, respectively.
5. Limitations
Despite the promising advancements in multimodal imaging for VT ablation, several limitations must be acknowledged. The use of ICE entails an additional procedural cost that may limit its widespread adoption. Image acquisition and processing can be time-consuming and technically demanding, requiring dedicated expertise and software integration, which may not be available in all centers. Moreover, while imaging modalities such as CT and PET offer high anatomical and metabolic detail, additional radiation exposure must be considered, especially in younger patients. The presence of implantable cardiac devices still represents a challenge for cardiac CMR despite the advent of wideband sequences, which are not widely available in many centers. The heterogeneity of imaging protocols, lack of standardization across centers, and relatively small sample sizes in many studies reduce the generalizability of current evidences.
6. Conclusions
Cardiac imaging has revolutionized the approach to VT ablation by offering precise anatomical and substrate characterization, improving procedural planning, and enhancing safety and efficacy. The integration of advanced imaging modalities with EAM enables a tailored, patient-specific strategy that may improve long-term outcomes, particularly in complex substrates. Although limitations persist, technological advancements such as the development of more automated image analysis tools, improved real-time integration capabilities, deep-learning-based anatomical reconstructions, promise to overcome current barriers. Future large prospective studies will be instrumental in defining the optimal role of imaging in VT ablation workflows and guiding the standardization of protocols. In the evolving field of electrophysiology, multimodal imaging is increasingly recognized as a key enabler of precision medicine.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Zeppenfeld, K.; Tfelt-Hansen, J.; De Riva, M.; Winkel, B.G.; Behr, E.R.; Blom, N.A.; et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. 2022, 43, 3997–4126. [Google Scholar] [CrossRef]
- Della Bella, P.; Baratto, F.; Vergara, P.; Bertocchi, P.; Santamaria, M.; Notarstefano, P.; et al. Does Timing of Ventricular Tachycardia Ablation Affect Prognosis in Patients With an Implantable Cardioverter Defibrillator? Results From the Multicenter Randomized PARTITA Trial. Circulation. 2022, 145, 1829–1838. [Google Scholar] [CrossRef] [PubMed]
- Cronin, E.M.; Bogun, F.M.; Maury, P.; Peichl, P.; Chen, M.; Namboodiri, N.; et al. 2019 HRS/EHRA/APHRS/LAHRS expert consensus statement on catheter ablation of ventricular arrhythmias. EP Eur. 2019, 21, 1143–1144. [Google Scholar]
- Arenal, Á.; Ávila, P.; Jiménez-Candil, J.; Tercedor, L.; Calvo, D.; Arribas, F.; et al. Substrate Ablation vs Antiarrhythmic Drug Therapy for Symptomatic Ventricular Tachycardia. J Am Coll Cardiol. 2022, 79, 1441–1453. [Google Scholar] [CrossRef] [PubMed]
- Tung, R.; Xue, Y.; Chen, M.; Jiang, C.; Shatz, D.Y.; Besser, S.A.; et al. First-Line Catheter Ablation of Monomorphic Ventricular Tachycardia in Cardiomyopathy Concurrent With Defibrillator Implantation: The PAUSE-SCD Randomized Trial. Circulation. 2022, 145, 1839–1849. [Google Scholar] [CrossRef]
- Sapp, J.L.; Tang, A.S.L.; Parkash, R.; Stevenson, W.G.; Healey, J.S.; Gula, L.J.; et al. Catheter Ablation or Antiarrhythmic Drugs for Ventricular Tachycardia. N Engl J Med. 2024, NEJMoa2409501. [Google Scholar] [CrossRef]
- Berruezo, A.; Penela, D.; Jáuregui, B.; Soto-Iglesias, D. The role of imaging in catheter ablation of ventricular arrhythmias. Pacing Clin Electrophysiol. 2021, 44, 1115–1125. [Google Scholar] [CrossRef]
- Ujeyl, A.; Inada, K.; Hillmann, K.; Wohlmuth, P.; Kato, M.; Tedrow, U.; et al. Right Heart Function Prediction of Outcome in Heart Failure Patients After Catheter Ablation for Recurrent Ventricular Tachycardia. JACC Heart Fail. 2013, 1, 281–289. [Google Scholar] [CrossRef]
- Arbelo, E.; Protonotarios, A.; Gimeno, J.R.; Arbustini, E.; Barriales-Villa, R.; Basso, C.; et al. 2023 ESC Guidelines for the management of cardiomyopathies. Eur Heart J. 2023, 44, 3503–3626. [Google Scholar] [CrossRef]
- Collier, P.; Phelan, D.; Klein, A. A Test in Context: Myocardial Strain Measured by Speckle-Tracking Echocardiography. J Am Coll Cardiol. 2017, 69, 1043–1056. [Google Scholar] [CrossRef]
- Trivedi, S.J.; Campbell, T.; Stefani, L.D.; Thomas, L.; Kumar, S. Strain by speckle tracking echocardiography correlates with electroanatomic scar location and burden in ischaemic cardiomyopathy. Eur Heart J - Cardiovasc Imaging. 2021, 22, 855–865. [Google Scholar] [CrossRef] [PubMed]
- Joyce, E.; Ninaber, M.K.; Katsanos, S.; Debonnaire, P.; Kamperidis, V.; Bax, J.J.; et al. Subclinical left ventricular dysfunction by echocardiographic speckle-tracking strain analysis relates to outcome in sarcoidosis. Eur J Heart Fail. 2015, 17, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Taha, K.; Kirkels, F.P.; Teske, A.J.; Asselbergs, F.W.; van Tintelen, J.P.; Doevendans, P.A.; et al. Echocardiographic Deformation Imaging for Early Detection of Genetic Cardiomyopathies: JACC Review Topic of the Week. J Am Coll Cardiol. 2022, 79, 594–608. [Google Scholar] [CrossRef] [PubMed]
- Kirkels, F.P.; Lie, Ø.H.; Cramer, M.J.; Chivulescu, M.; Rootwelt-Norberg, C.; Asselbergs, F.W.; et al. Right Ventricular Functional Abnormalities in Arrhythmogenic Cardiomyopathy: Association With Life-Threatening Ventricular Arrhythmias. JACC Cardiovasc Imaging. 2021, 14, 900–910. [Google Scholar] [CrossRef]
- Berte, B.; Sacher, F.; Venlet, J.; Andreu, D.; Mahida, S.; Aldhoon, B.; et al. VT Recurrence After Ablation: Incomplete Ablation or Disease Progression? A Multicentric European Study. J Cardiovasc Electrophysiol. 2016, 27, 80–87. [Google Scholar] [CrossRef]
- Shen, L.; Liu, S.; Zhang, Z.; Xiong, Y.; Lai, Z.; Hu, F.; et al. Catheter ablation of ventricular tachycardia in patients with arrhythmogenic right ventricular cardiomyopathy and biventricular involvement. Europace 2024, 26, euae059. [Google Scholar] [CrossRef]
- John, L.A.; John, I.I.; Tedford, R.J.; Gregoski, M.J.; Gold, M.R.; Field, M.E.; et al. Substrate Imaging Before Catheter Ablation of Ventricular Tachycardia. JACC Clin Electrophysiol. 2023, 9, 1684–1693. [Google Scholar] [CrossRef]
- Chery, G.; Khoshknab, M.; Nazarian, S. Imaging to Facilitate Ventricular Tachycardia Ablation. JACC Clin Electrophysiol. 2024, 10, 2277–2292. [Google Scholar] [CrossRef]
- Fernández-Armenta, J.; Berruezo, A.; Andreu, D.; Camara, O.; Silva, E.; Serra, L.; et al. Three-Dimensional Architecture of Scar and Conducting Channels Based on High Resolution ce-CMR: Insights for Ventricular Tachycardia Ablation. Circ Arrhythm Electrophysiol. 2013, 6, 528–537. [Google Scholar] [CrossRef]
- Estner, H.L.; Zviman, M.M.; Herzka, D.; Miller, F.; Castro, V.; Nazarian, S.; et al. The critical isthmus sites of ischemic ventricular tachycardia are in zones of tissue heterogeneity, visualized by magnetic resonance imaging. Heart Rhythm. 2011, 8, 1942–1949. [Google Scholar] [CrossRef]
- Piers, S.R.D.; Tao, Q.; De Riva Silva, M.; Siebelink, H.M.; Schalij, M.J.; Van Der Geest, R.J.; et al. CMR–Based Identification of Critical Isthmus Sites of Ischemic and Nonischemic Ventricular Tachycardia. JACC Cardiovasc Imaging. 2014, 7, 774–784. [Google Scholar] [CrossRef]
- Padmanabhan, D.; Kella, D.K.; Deshmukh, A.J.; Mulpuru, S.K.; Mehta, R.A.; Dalzell, C.M.; et al. Safety of thoracic magnetic resonance imaging for patients with pacemakers and defibrillators. Heart Rhythm. 2019, 16, 1645–1651. [Google Scholar] [CrossRef]
- Russo, R.J.; Costa, H.S.; Silva, P.D.; Anderson, J.L.; Arshad, A.; Biederman, R.W.W.; et al. Assessing the Risks Associated with MRI in Patients with a Pacemaker or Defibrillator. N Engl J Med. 2017, 376, 755–764. [Google Scholar] [CrossRef]
- Schwitter, J.; Gold, M.R.; Al Fagih, A.; Lee, S.; Peterson, M.; Ciuffo, A.; et al. Image Quality of Cardiac Magnetic Resonance Imaging in Patients With an Implantable Cardioverter Defibrillator System Designed for the Magnetic Resonance Imaging Environment. Circ Cardiovasc Imaging. 2016, 9, e004025. [Google Scholar] [CrossRef]
- Mesubi, O.; Ahmad, G.; Jeudy, J.; Jimenez, A.; Kuk, R.; Saliaris, A.; et al. Impact of ICD artifact burden on late gadolinium enhancement cardiac MR imaging in patients undergoing ventricular tachycardia ablation. Pacing Clin Electrophysiol PACE. 2014, 37, 1274–1283. [Google Scholar] [CrossRef]
- Sasaki, T.; Hansford, R.; Zviman, M.M.; Kolandaivelu, A.; Bluemke, D.A.; Berger, R.D.; et al. Quantitative Assessment of Artifacts on Cardiac Magnetic Resonance Imaging of Patients With Pacemakers and Implantable Cardioverter-Defibrillators. Circ Cardiovasc Imaging. 2011, 4, 662–670. [Google Scholar] [CrossRef]
- Rashid, S.; Rapacchi, S.; Vaseghi, M.; Tung, R.; Shivkumar, K.; Finn, J.P.; et al. Improved Late Gadolinium Enhancement MR Imaging for Patients with Implanted Cardiac Devices. Radiology [Internet]. /: 1 [cited 2025 Mar 2]; Available from: https, 2025. [Google Scholar]
- Roca-Luque, I.; Van Breukelen, A.; Alarcon, F.; Garre, P.; Tolosana, J.M.; Borras, R.; et al. Ventricular scar channel entrances identified by new wideband cardiac magnetic resonance sequence to guide ventricular tachycardia ablation in patients with cardiac defibrillators. EP Eur. 2020, 22, 598–606. [Google Scholar] [CrossRef]
- Bhuva, A.N.; Kellman, P.; Graham, A.; Ramlall, M.; Boubertakh, R.; Feuchter, P.; et al. Clinical impact of cardiovascular magnetic resonance with optimized myocardial scar detection in patients with cardiac implantable devices. Int J Cardiol. 2019, 279, 72–78. [Google Scholar] [CrossRef]
- Hilbert, S.; Weber, A.; Nehrke, K.; Börnert, P.; Schnackenburg, B.; Oebel, S.; et al. Artefact-free late gadolinium enhancement imaging in patients with implanted cardiac devices using a modified broadband sequence: current strategies and results from a real-world patient cohort. Eur Eur Pacing Arrhythm Card Electrophysiol J Work Groups Card Pacing Arrhythm Card Cell Electrophysiol Eur Soc Cardiol. 2018, 20, 801–807. [Google Scholar] [CrossRef]
- Do, D.H.; Eyvazian, V.; Bayoneta, A.J.; Hu, P.; Finn, J.P.; Bradfield, J.S.; et al. Cardiac magnetic resonance imaging using wideband sequences in patients with nonconditional cardiac implanted electronic devices. Heart Rhythm. 2018, 15, 218–225. [Google Scholar] [CrossRef]
- Patel, H.N.; Wang, S.; Rao, S.; Singh, A.; Landeras, L.; Besser, S.A.; et al. Impact of wideband cardiac magnetic resonance on diagnosis, decision-making and outcomes in patients with implantable cardioverter defibrillators. Eur Heart J - Cardiovasc Imaging. 2023, 24, 181–189. [Google Scholar] [CrossRef]
- Zghaib, T.; Ghasabeh, M.A.; Assis, F.R.; Chrispin, J.; Keramati, A.; Misra, S.; et al. Regional Strain by Cardiac Magnetic Resonance Imaging Improves Detection of Right Ventricular Scar Compared With Late Gadolinium Enhancement on a Multimodality Scar Evaluation in Patients With Arrhythmogenic Right Ventricular Cardiomyopathy. Circ Cardiovasc Imaging. 2018, 11, e007546. [Google Scholar] [CrossRef]
- Santangeli, P.; Muser, D.; Zado, E.S.; Magnani, S.; Khetpal, S.; Hutchinson, M.D.; et al. Acute Hemodynamic Decompensation During Catheter Ablation of Scar-Related Ventricular Tachycardia: Incidence, Predictors, and Impact on Mortality. Circ Arrhythm Electrophysiol. 2015, 8, 68–75. [Google Scholar] [CrossRef]
- Pontone, G.; Rossi, A.; Guglielmo, M.; Dweck, M.R.; Gaemperli, O.; Nieman, K.; et al. Clinical applications of cardiac computed tomography: a consensus paper of the European Association of Cardiovascular Imaging—part I. Eur Heart J - Cardiovasc Imaging. 2022, 23, 299–314. [Google Scholar] [CrossRef]
- Pontone, G.; Rossi, A.; Guglielmo, M.; Dweck, M.R.; Gaemperli, O.; Nieman, K.; et al. Clinical applications of cardiac computed tomography: a consensus paper of the European Association of Cardiovascular Imaging—part II. Eur Heart J - Cardiovasc Imaging. 2022, 23, e136–61. [Google Scholar] [CrossRef]
- Sasaki, T.; Calkins, H.; Miller, C.F.; Zviman, M.M.; Zipunnikov, V.; Arai, T.; et al. New insight into scar-related ventricular tachycardia circuits in ischemic cardiomyopathy: Fat deposition after myocardial infarction on computed tomography--A pilot study. Heart Rhythm. 2015, 12, 1508–1518. [Google Scholar] [CrossRef]
- Tian, J.; Jeudy, J.; Smith, M.F.; Jimenez, A.; Yin, X.; Bruce, P.A.; et al. Three-Dimensional Contrast-Enhanced Multidetector CT for Anatomic, Dynamic, and Perfusion Characterization of Abnormal Myocardium To Guide Ventricular Tachycardia Ablations. Circ Arrhythm Electrophysiol. 2010, 3, 496–504. [Google Scholar] [CrossRef]
- Esposito, A.; Palmisano, A.; Antunes, S.; Maccabelli, G.; Colantoni, C.; Rancoita, P.M.V.; et al. Cardiac CT With Delayed Enhancement in the Characterization of Ventricular Tachycardia Structural Substrate. JACC Cardiovasc Imaging. 2016, 9, 822–832. [Google Scholar] [CrossRef]
- Komatsu, Y.; Cochet, H.; Jadidi, A.; Sacher, F.; Shah, A.; Derval, N.; et al. Regional Myocardial Wall Thinning at Multidetector Computed Tomography Correlates to Arrhythmogenic Substrate in Postinfarction Ventricular Tachycardia: Assessment of Structural and Electrical Substrate. Circ Arrhythm Electrophysiol. 2013, 6, 342–350. [Google Scholar] [CrossRef]
- Baroldi, G.; Silver, M.D.; De Maria, R.; Parodi, O.; Pellegrini, A. Lipomatous metaplasia in left ventricular scar. Can J Cardiol. 1997, 13, 65–71. [Google Scholar]
- Su, L.; Siegel, J.E.; Fishbein, M.C. Adipose tissue in myocardial infarction. Cardiovasc Pathol Off J Soc Cardiovasc Pathol. 2004, 13, 98–102. [Google Scholar] [CrossRef]
- Ichikawa, Y.; Kitagawa, K.; Chino, S.; Ishida, M.; Matsuoka, K.; Tanigawa, T.; et al. Adipose tissue detected by multislice computed tomography in patients after myocardial infarction. JACC Cardiovasc Imaging. 2009, 2, 548–555. [Google Scholar] [CrossRef]
- Schmitt, M.; Samani, N.; McCann, G. Images in cardiovascular medicine. Lipomatous metaplasia in ischemic cardiomyopathy: a common but unappreciated entity. Circulation. 2007, 116, e5–e6. [Google Scholar]
- Xu, L.; Khoshknab, M.; Berger, R.D.; Chrispin, J.; Dixit, S.; Santangeli, P.; et al. Lipomatous Metaplasia Enables Ventricular Tachycardia by Reducing Current Loss Within the Protected Corridor. JACC Clin Electrophysiol. 2022, 8, 1274–1285. [Google Scholar] [CrossRef]
- Xu, L.; Zahid, S.; Khoshknab, M.; Moss, J.; Berger, R.D.; Chrispin, J.; et al. Lipomatous Metaplasia Facilitates Slow Conduction in Critical Ventricular Tachycardia Corridors Within Postinfarct Myocardium. JACC Clin Electrophysiol. 2023, 9, 1235–1245. [Google Scholar] [CrossRef]
- Tung, R.; Bauer, B.; Schelbert, H.; Lynch, J.P.; Auerbach, M.; Gupta, P.; et al. Incidence of abnormal positron emission tomography in patients with unexplained cardiomyopathy and ventricular arrhythmias: The potential role of occult inflammation in arrhythmogenesis. Heart Rhythm. 2015, 12, 2488–2498. [Google Scholar] [CrossRef]
- Sharma, R.; Kouranos, V.; Cooper, L.T.; Metra, M.; Ristic, A.; Heidecker, B.; et al. Management of cardiac sarcoidosis: A clinical consensus statement of the Heart Failure Association, the European Association of Cardiovascular Imaging, the ESC Working Group on Myocardial & Pericardial Diseases, and the European Heart Rhythm Association of the ESC. Eur Heart J. 2024, 45, 2697–2726. [Google Scholar]
- Tuominen, H.; Haarala, A.; Tikkakoski, A.; Kähönen, M.; Nikus, K.; Sipilä, K. FDG-PET in possible cardiac sarcoidosis: Right ventricular uptake and high total cardiac metabolic activity predict cardiovascular events. J Nucl Cardiol. 2021, 28, 199–205. [Google Scholar] [CrossRef]
- Tessier, R.; Marteau, L.; Vivien, M.; Guyomarch, B.; Thollet, A.; Fellah, I.; et al. 18F-Fluorodeoxyglucose Positron Emission Tomography for the Detection of Myocardial Inflammation in Arrhythmogenic Left Ventricular Cardiomyopathy. Circ Cardiovasc Imaging. 2022, 15, e014065. [Google Scholar] [CrossRef]
- Miller, B.; Vunnam, R.; Mesubi, O.; Smith, M.F.; Chen, W.; Mahat, J.B.; et al. Metabolic heterogeneous zone assessed by18 FDG-PET is predictive of postablation mortality in patients with ventricular tachycardia. J Cardiovasc Electrophysiol. 2021, 32, 2238–2245. [Google Scholar] [CrossRef]
- Kanawati, J.; De Silva, K.; Bhaskaran, A.; Turnbull, S.; Zhou, J.; Kotake, Y.; et al. Intracardiac echocardiography techniques to identify ventricular arrhythmia substrate. Heart Rhythm O2. 2022, 3, 602–612. [Google Scholar] [CrossRef]
- Muser, D.; Lavalle, C.; Guarracini, F.; Sassone, B.; Conte, E.; Magnani, S.; et al. Role of cardiac imaging in patients undergoing catheter ablation of ventricular tachycardia. J Cardiovasc Med. 2021, 22, 727–737. [Google Scholar] [CrossRef]
- Enriquez, A.; Saenz, L.C.; Rosso, R.; Silvestry, F.E.; Callans, D.; Marchlinski, F.E.; et al. Use of Intracardiac Echocardiography in Interventional Cardiology: Working With the Anatomy Rather Than Fighting It. Circulation. 2018, 137, 2278–2294. [Google Scholar] [CrossRef]
- Marrouche, N.F.; Martin, D.O.; Wazni, O.; Gillinov, A.M.; Klein, A.; Bhargava, M.; et al. Phased-Array Intracardiac Echocardiography Monitoring During Pulmonary Vein Isolation in Patients With Atrial Fibrillation: Impact on Outcome and Complications. Circulation. 2003, 107, 2710–2716. [Google Scholar] [CrossRef]
- Madhavan, M.; Asirvatham, S.J. The Fourth Dimension: Endocavitary Ventricular Tachycardia. Circ Arrhythm Electrophysiol. 2010, 3, 302–304. [Google Scholar] [CrossRef]
- De Sensi, F.; Addonisio, L.; Cresti, A.; Limbruno, U. Anatomical reconstruction of right ventricular structures with intracardiac echocardiography during ablation of premature contractions from moderator band. Indian Pacing Electrophysiol J. 2024, 24, 155–157. [Google Scholar] [CrossRef]
- Sadek, M.M.; Benhayon, D.; Sureddi, R.; Chik, W.; Santangeli, P.; Supple, G.E.; et al. Idiopathic ventricular arrhythmias originating from the moderator band: Electrocardiographic characteristics and treatment by catheter ablation. Heart Rhythm. 2015, 12, 67–75. [Google Scholar] [CrossRef]
- Kautzner, J.; Peichl, P. Papillary Muscle Ventricular Tachycardia or Ectopy: Diagnostics, Catheter Ablation and the Role of Intracardiac Echocardiography. Arrhythmia Electrophysiol Rev. 2019, 8, 65–69. [Google Scholar] [CrossRef]
- Proietti, R.; Rivera, S.; Dussault, C.; Essebag, V.; Bernier, M.L.; Ayala-Paredes, F.; et al. Intracardiac echo-facilitated 3D electroanatomical mapping of ventricular arrhythmias from the papillary muscles: assessing the ‘fourth dimension’ during ablation.
- Bunch, T.J.; Weiss, J.P.; Crandall, B.G.; Day, J.D.; Dimarco, J.P.; Ferguson, J.D.; et al. Image Integration Using Intracardiac Ultrasound and 3D Reconstruction for Scar Mapping and Ablation of Ventricular Tachycardia. J Cardiovasc Electrophysiol. 2010, 21, 678–684. [Google Scholar] [CrossRef]
- Hussein, A.; Jimenez, A.; Ahmad, G.; Mesubi, O.; Klein, T.; Gurm, G.; et al. Assessment of Ventricular Tachycardia Scar Substrate by Intracardiac Echocardiography. Pacing Clin Electrophysiol. 2014, 37, 412–421. [Google Scholar] [CrossRef]
- Qian, P.C.; Tedrow, U.B. Intracardiac Echocardiography to Guide Catheter Ablation of Ventricular Arrhythmias in Ischemic Cardiomyopathy. Card Electrophysiol Clin. 2021, 13, 285–292. [Google Scholar] [CrossRef]
- Bala, R.; Ren, J.F.; Hutchinson, M.D.; Desjardins, B.; Tschabrunn, C.; Gerstenfeld, E.P.; et al. Assessing Epicardial Substrate Using Intracardiac Echocardiography During VT Ablation. Circ Arrhythm Electrophysiol. 2011, 4, 667–673. [Google Scholar] [CrossRef]
- Barrett, C.; Tzou, W.S. Utility of Intracardiac Echocardiography for Guiding Ablation of Ventricular Tachycardia in Nonischemic Cardiomyopathy. Card Electrophysiol Clin. 2021, 13, 337–343. [Google Scholar] [CrossRef]
- Lamberti, F.; Di Clemente, F.; Remoli, R.; Bellini, C.; De Santis, A.; Mercurio, M.; et al. Catheter ablation of idiopathic ventricular tachycardia without the use of fluoroscopy. Int J Cardiol.
- Kautzner, J.; Haskova, J.; Lehar, F. Intracardiac Echocardiography to Guide Non-fluoroscopic Electrophysiology Procedures. Card Electrophysiol Clin. 2021, 13, 399–408. [Google Scholar] [CrossRef]
- Rivera, S.; Vecchio, N.; Ricapito, P.; Ayala-Paredes, F. Non-fluoroscopic catheter ablation of arrhythmias with origin at the summit of the left ventricle. J Interv Card Electrophysiol. 2019, 56, 279–290. [Google Scholar] [CrossRef]
- Hasegawa, K.; Yoneda, Z.T.; Martines-Parachini, J.R.; Powers, E.M.; Davogustto, G.E.; Hu, T.Y.; et al. Can Intracardiac Echocardiography Reduce Steam Pops During Half-Normal Saline Irrigated Radiofrequency Ablation? Circ Arrhythm Electrophysiol [Internet]. 2024 Jun [cited 2025 Mar 17];17(6). Available from: https://www.ahajournals.org/doi/10.1161/CIRCEP.123. 0126. [Google Scholar]
- Peichl, P.; Wichterle, D.; Čihák, R.; Aldhoon, B.; Kautzner, J. Catheter Ablation of Ventricular Tachycardia in the Presence of an Old Endocavitary Thrombus Guided by Intracardiac Echocardiography: ABLATION IN PRESENCE OF THROMBUS. Pacing Clin Electrophysiol. 2016, 39, 581–587. [Google Scholar] [CrossRef]
- Raczka, F.; Granier, M.; Cung, T.T.; Davy, J.M. Intracardiac thrombus: a good indication of ultrasound image integration system (CartosoundTM) for radiofrequency ablation. Europace. 2010, 12, 591–592. [Google Scholar] [CrossRef]
- Enriquez, A.; Sadek, M.; Hanson, M.; Yang, J.; Matos, C.D.; Neira, V.; et al. Feasibility, Efficacy, and Safety of Fluoroless Ablation of VT in Patients With Structural Heart Disease. JACC Clin Electrophysiol. 2024, 10, 1287–1300. [Google Scholar] [CrossRef]
- Field, M.E.; Gold, M.R.; Reynolds, M.R.; Goldstein, L.; Lee, S.H.Y.; Kalsekar, I.; et al. Real-world outcomes of ventricular tachycardia catheter ablation with versus without intracardiac echocardiography. J Cardiovasc Electrophysiol. 2020, 31, 417–422. [Google Scholar] [CrossRef]
- Kitamura, T.; Nakajima, M.; Kawamura, I.; Kaszynski, R.H.; Ohbe, H.; Sasabuchi, Y.; et al. Safety and effectiveness of intracardiac echocardiography in ventricular tachycardia ablation: a nationwide observational study. Heart Vessels. 2021, 36, 1009–1015. [Google Scholar] [CrossRef]
- Di Biase, L.; Zou, F.; Lin, A.N.; Grupposo, V.; Marazzato, J.; Tarantino, N.; et al. Feasibility of three-dimensional artificial intelligence algorithm integration with intracardiac echocardiography for left atrial imaging during atrial fibrillation catheter ablation. Europace. 2023, 25, euad211. [Google Scholar] [CrossRef]
- Akerström, F.; Drca, N.; Jensen-Urstad, M.; Braunschweig, F. Feasibility of a novel algorithm for automated reconstruction of the left atrial anatomy based on intracardiac echocardiography. Pacing Clin Electrophysiol. 2022, 45, 1288–1294. [Google Scholar] [CrossRef]
- Blumenthal, C.J.; Hsue, W.; Chen, T.; Zhang, D.; Brem, E.; Garcia, F.C.; et al. Preclinical Experience Using 4D Intracardiac Echocardiography to Guide Cardiac Electrophysiology Procedures. J Cardiovasc Electrophysiol. 2025, 36, 480–486. [Google Scholar] [CrossRef]
- Mahida, S.; Sacher, F.; Dubois, R.; Sermesant, M.; Bogun, F.; Haïssaguerre, M.; et al. Cardiac Imaging in Patients With Ventricular Tachycardia. Circulation. 2017, 136, 2491–2507. [Google Scholar] [CrossRef]
- Wijnmaalen, A.P.; Van Der Geest, R.J.; Van Huls Van Taxis, C.F.B.; Siebelink, H.M.J.; Kroft, L.J.M.; Bax, J.J.; et al. Head-to-head comparison of contrast-enhanced magnetic resonance imaging and electroanatomical voltage mapping to assess post-infarct scar characteristics in patients with ventricular tachycardias: real-time image integration and reversed registration. Eur Heart J. 2011, 32, 104–114. [Google Scholar] [CrossRef]
- Tian, J.; Jeudy, J.; Smith, M.F.; Jimenez, A.; Yin, X.; Bruce, P.A.; et al. Three-dimensional contrast-enhanced multidetector CT for anatomic, dynamic, and perfusion characterization of abnormal myocardium to guide ventricular tachycardia ablations. Circ Arrhythm Electrophysiol. 2010, 3, 496–504. [Google Scholar] [CrossRef]
- Andreu, D.; Berruezo, A.; Ortiz-Pérez, J.T.; Silva, E.; Mont, L.; Borràs, R.; et al. Integration of 3D Electroanatomic Maps and Magnetic Resonance Scar Characterization Into the Navigation System to Guide Ventricular Tachycardia Ablation. Circ Arrhythm Electrophysiol. 2011, 4, 674–683. [Google Scholar] [CrossRef]
- Yamashita, S.; Sacher, F.; Mahida, S.; Berte, B.; Lim, H.S.; Komatsu, Y.; et al. Image Integration to Guide Catheter Ablation in Scar-Related Ventricular Tachycardia. J Cardiovasc Electrophysiol. 2016, 27, 699–708. [Google Scholar] [CrossRef]
- Takigawa, M.; Duchateau, J.; Sacher, F.; Martin, R.; Vlachos, K.; Kitamura, T.; et al. Are wall thickness channels defined by computed tomography predictive of isthmuses of postinfarction ventricular tachycardia? Heart Rhythm 2019, 16, 1661–1668. [Google Scholar] [CrossRef]
- Parollo, M.; Mazzocchetti, L.; Cori, A.D.; Segreti, L.; Lucia, R.D.; Grifoni, G.; et al. Lipomatous metaplasia as the most reliable computed tomography predictor for functional substrate localization in scar-related ventricular tachycardia. Heart Rhythm. 2023, 20, 1593–1594. [Google Scholar] [CrossRef]
- Di Cori, A.; Pistelli, L.; Parollo, M.; Zaurino, N.; Segreti, L.; Zucchelli, G. Approaching Ventricular Tachycardia Ablation in 2024: An Update on Mapping and Ablation Strategies, Timing, and Future Directions. J Clin Med. 2024, 13, 5017. [Google Scholar] [CrossRef]
- Sanchez-Somonte, P.; Garre, P.; Vázquez-Calvo, S.; Quinto, L.; Borràs, R.; Prat, S.; et al. Scar conducting channel characterization to predict arrhythmogenicity during ventricular tachycardia ablation. EP Eur. 2023, 25, 989–999. [Google Scholar] [CrossRef]
- Acosta, J.; Andreu, D.; Penela, D.; Cabrera, M.; Carlosena, A.; Korshunov, V.; et al. Elucidation of hidden slow conduction by double ventricular extrastimuli: a method for further arrhythmic substrate identification in ventricular tachycardia ablation procedures. EP Eur. 2018, 20, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Andreu, D.; Penela, D.; Acosta, J.; Fernández-Armenta, J.; Perea, R.J.; Soto-Iglesias, D.; et al. Cardiac magnetic resonance–aided scar dechanneling: Influence on acute and long-term outcomes. Heart Rhythm. 2017, 14, 1121–1128. [Google Scholar] [CrossRef]
- Soto-Iglesias, D.; Penela, D.; Jáuregui, B.; Acosta, J.; Fernández-Armenta, J.; Linhart, M.; et al. Cardiac Magnetic Resonance-Guided Ventricular Tachycardia Substrate Ablation. JACC Clin Electrophysiol. 2020, 6, 436–447. [Google Scholar] [CrossRef] [PubMed]
- Lilli, A.; Parollo, M.; Mazzocchetti, L.; De Sensi, F.; Rossi, A.; Notarstefano, P.; et al. Ventricular tachycardia ablation guided or aided by scar characterization with cardiac magnetic resonance: rationale and design of VOYAGE study. BMC Cardiovasc Disord. 2022, 22, 169. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
A 35-years old female with mitral valve prolapse presented an elevated ventricular arrhythmic burden and underwent cardiological evaluation. Panel A: resting ECG showing the presence of PVCs with right bundle branch block-like morphology (qR in lead V1) and superior axis. Panel B: echocardiography showed the presence of bileaflet mitral valve prolapse with mitral annular disjunction (yellow arrow). Panel C: reduced strain values in the lateral wall at speckle tracking echocardiography. CMR demonstrated the presence of significant midwall LGE in inferolateral segments (Panel D, red arrow) and in the postero-medial papillary muscle (Panel E, orange arrow). Panel F: after ineffective anti arrhythmic treatments, the patient underwent PVCs ablation at the posterior-medial papillary muscle. Adequate contact between the ablation catheter and the papillary muscle was assured through ICE. PVC, premature ventricular complex; CMR, cardiac magnetic resonance; LGE, late gadolinium enhancement; ICE, intracardiac echocardiography.
Figure 1.
A 35-years old female with mitral valve prolapse presented an elevated ventricular arrhythmic burden and underwent cardiological evaluation. Panel A: resting ECG showing the presence of PVCs with right bundle branch block-like morphology (qR in lead V1) and superior axis. Panel B: echocardiography showed the presence of bileaflet mitral valve prolapse with mitral annular disjunction (yellow arrow). Panel C: reduced strain values in the lateral wall at speckle tracking echocardiography. CMR demonstrated the presence of significant midwall LGE in inferolateral segments (Panel D, red arrow) and in the postero-medial papillary muscle (Panel E, orange arrow). Panel F: after ineffective anti arrhythmic treatments, the patient underwent PVCs ablation at the posterior-medial papillary muscle. Adequate contact between the ablation catheter and the papillary muscle was assured through ICE. PVC, premature ventricular complex; CMR, cardiac magnetic resonance; LGE, late gadolinium enhancement; ICE, intracardiac echocardiography.
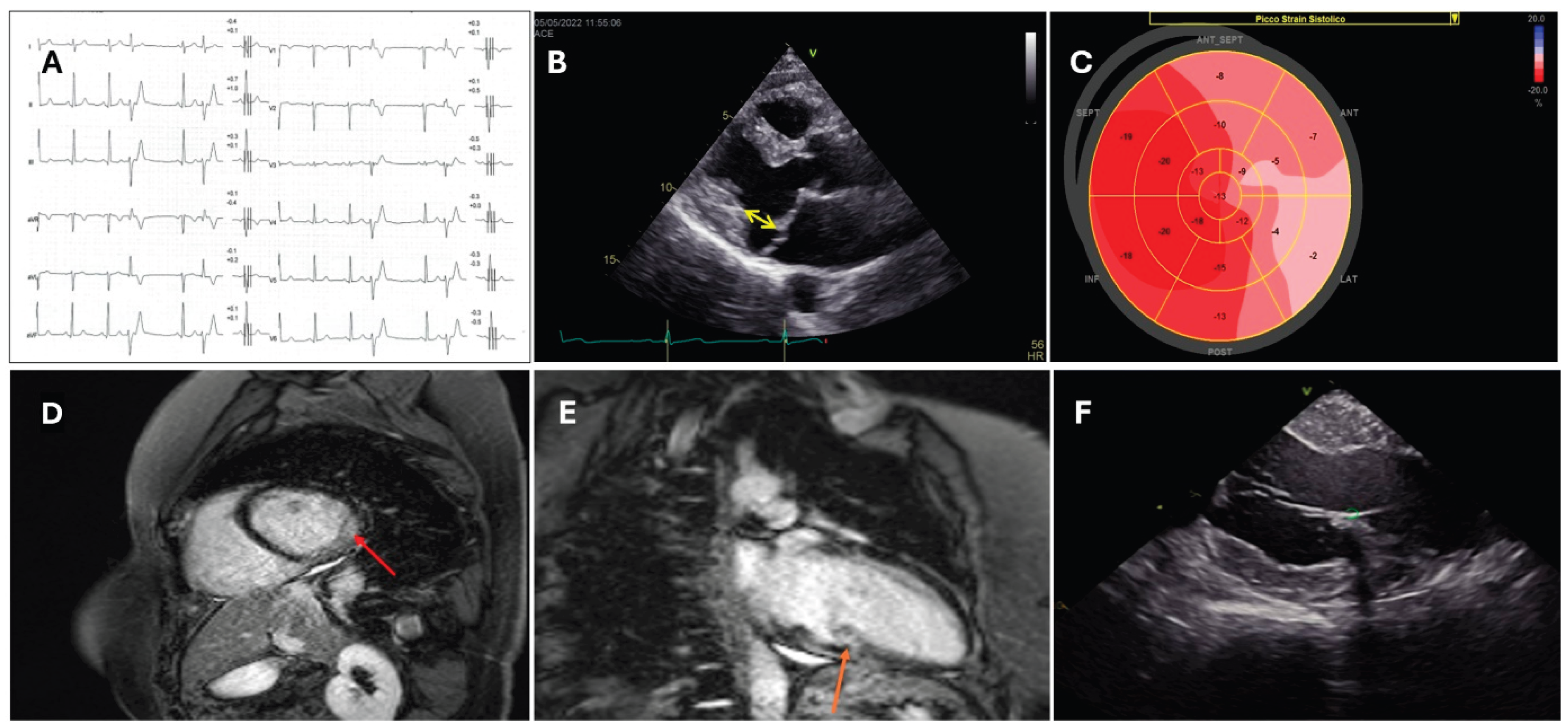
Figure 2.
Figure 2. A: a 55-years old male was admitted to our Cardiology unit for catheter ablation of symptomatic PVCs and NSVT. Coronary angiography did not show any significant lesion. B and C: CMR demonstrated the presence of patchy LGE in the interventricular septum and inferolateral wall. D: intense 18-FDG uptake was detected by PET scan in the interventricular septum and inferolateral wall. E: 18-FDG PET revealed the presence of pathological uptake in the apical right pulmonary lobe. F: inflammatory infiltrates and non-caseating granulomas were identified at histology after pulmonary lymphonodes biopsy, compatible with pulmonary sarcoidosis. After steroid therapy, the patient experienced significant symptomatic improvement and reduction of the arrhythmic burden; therefore, catheter ablation was postponed. PVCs, premature ventricular complexes; NSVT, non-sustained ventricular tachycardia; CMR, cardiac magnetic resonance; LGE, late gadolinium enhancement; 18-FDG PET, 18-fluorodeoxyglucose positron emission tomography.
Figure 2.
Figure 2. A: a 55-years old male was admitted to our Cardiology unit for catheter ablation of symptomatic PVCs and NSVT. Coronary angiography did not show any significant lesion. B and C: CMR demonstrated the presence of patchy LGE in the interventricular septum and inferolateral wall. D: intense 18-FDG uptake was detected by PET scan in the interventricular septum and inferolateral wall. E: 18-FDG PET revealed the presence of pathological uptake in the apical right pulmonary lobe. F: inflammatory infiltrates and non-caseating granulomas were identified at histology after pulmonary lymphonodes biopsy, compatible with pulmonary sarcoidosis. After steroid therapy, the patient experienced significant symptomatic improvement and reduction of the arrhythmic burden; therefore, catheter ablation was postponed. PVCs, premature ventricular complexes; NSVT, non-sustained ventricular tachycardia; CMR, cardiac magnetic resonance; LGE, late gadolinium enhancement; 18-FDG PET, 18-fluorodeoxyglucose positron emission tomography.
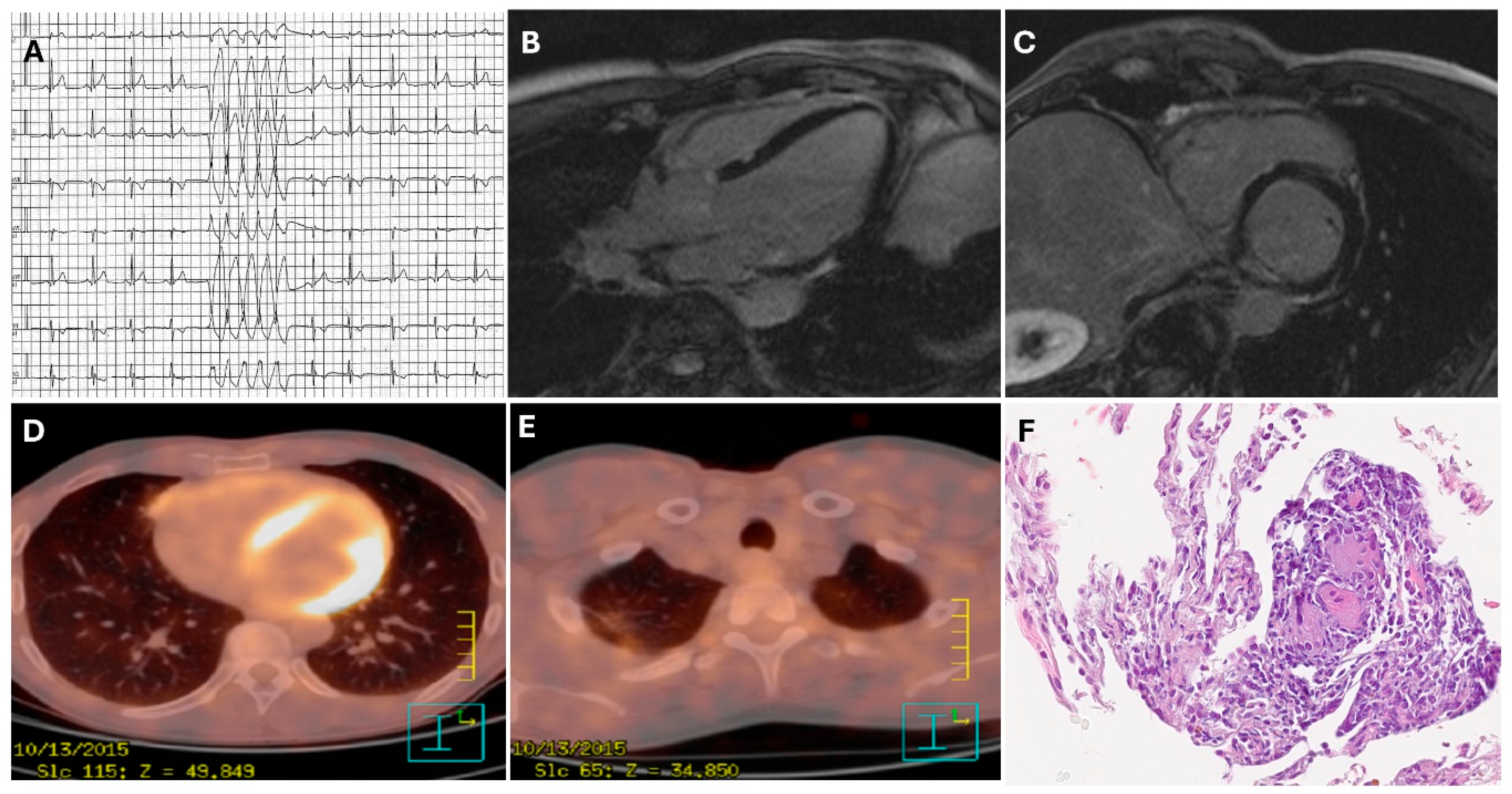
Figure 3.
Examples of applications of ICE in VT ablation: A) 3D reconstruction of the left ventricle obtained with the ICE probe positioned in the right ventricle, showing a subendocardial scar area on the lateral wall (red arrows); B) Intraprocedural detection of pericardial effusion; C) Identification of a large aortic plaque at sino-tubular junction which prompted the operator to avoid the transaortic approach and proceed exclusively via the transseptal route. ICE, intracardiac echocardiography; VT, ventricular tachycardia.
Figure 3.
Examples of applications of ICE in VT ablation: A) 3D reconstruction of the left ventricle obtained with the ICE probe positioned in the right ventricle, showing a subendocardial scar area on the lateral wall (red arrows); B) Intraprocedural detection of pericardial effusion; C) Identification of a large aortic plaque at sino-tubular junction which prompted the operator to avoid the transaortic approach and proceed exclusively via the transseptal route. ICE, intracardiac echocardiography; VT, ventricular tachycardia.
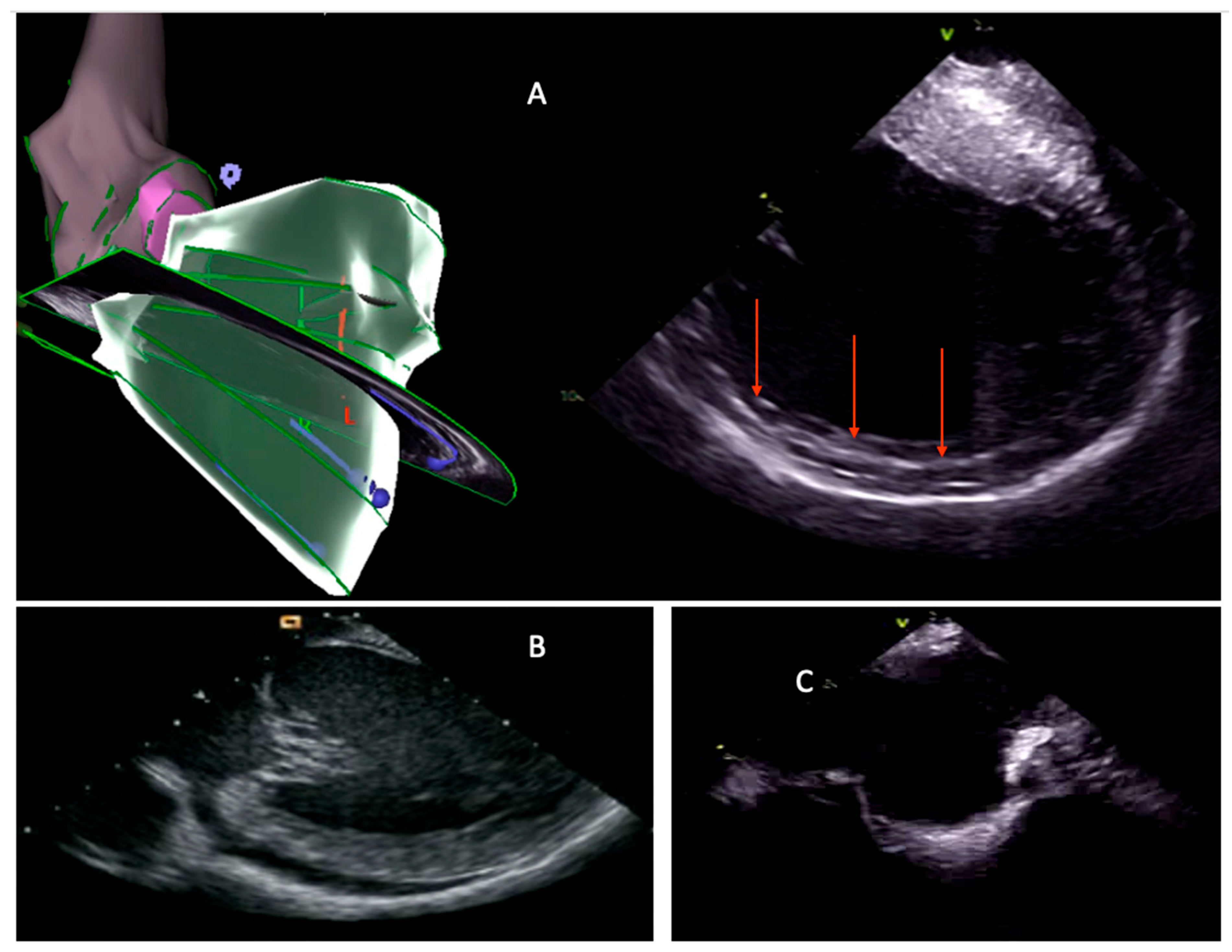
Figure 4.
MDCT from an ischemic patient post-processed with a dedicated software (ADAS 3D). Three-dimensional reconstruction of aorta (pink) and left ventricle with lipomatous metaplasia (transparent black) and wall thickness analysis. LV wall thickness is shown as a colour map (from blue > 6 mm to red < 1 mm). LV, Left Ventricle; MDCT, Multidetector CT.
Figure 4.
MDCT from an ischemic patient post-processed with a dedicated software (ADAS 3D). Three-dimensional reconstruction of aorta (pink) and left ventricle with lipomatous metaplasia (transparent black) and wall thickness analysis. LV wall thickness is shown as a colour map (from blue > 6 mm to red < 1 mm). LV, Left Ventricle; MDCT, Multidetector CT.
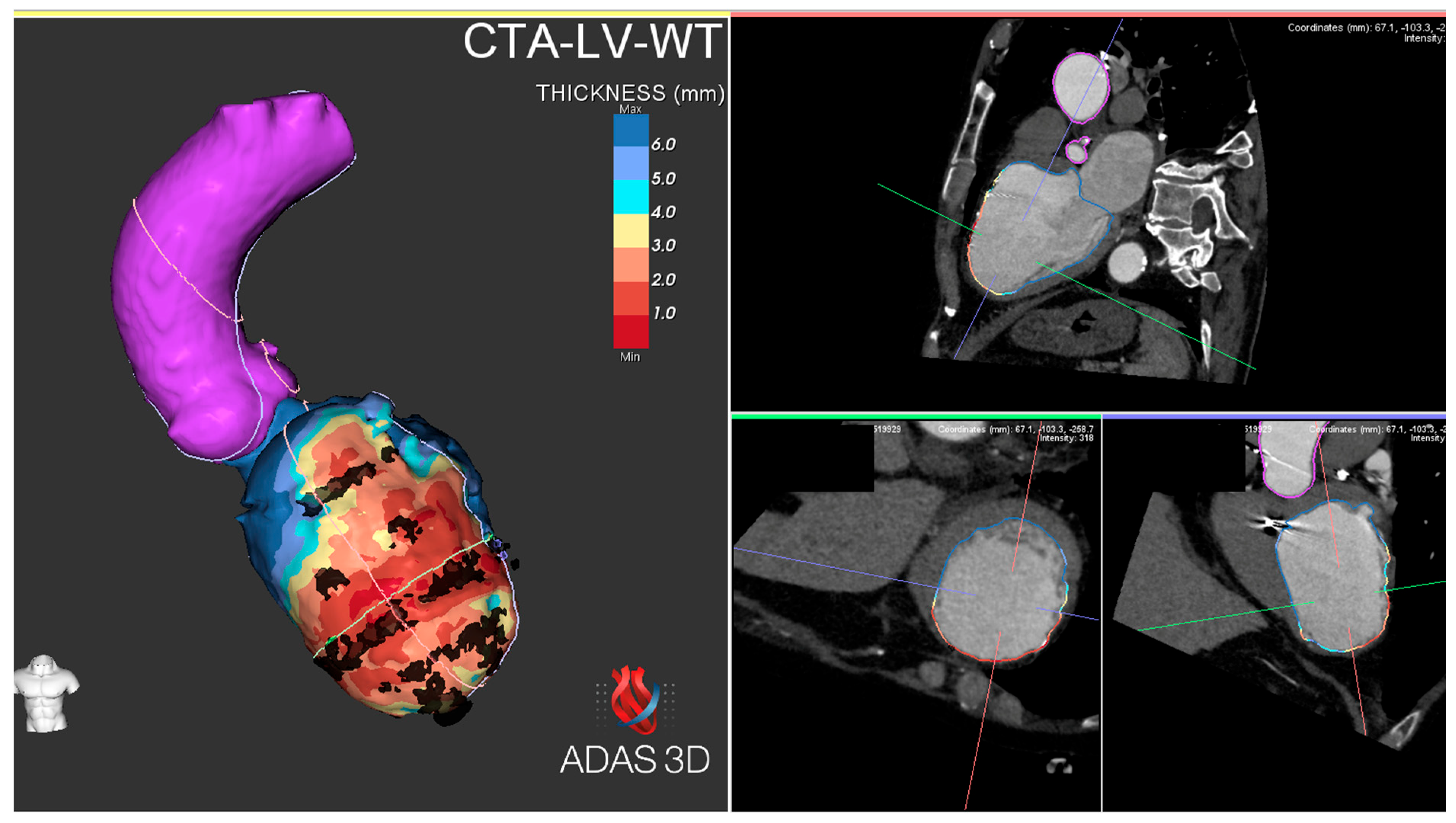
Figure 5.
A patient with previous myocardial infarction experienced multiple ICD shocks due to recurrent episodes of VT. The pre-procedural CMR was of insufficient quality (Panel A); however, the use of wideband sequences (Panel B) enabled clear visualization and characterization of an inferolateral scar. The scar was successfully imported into the EAM system using ADAS 3D software. Panel C displays a posterior view of the bipolar voltage map with standard thresholds for dense scar (<0.5 mV) and border zone (<1.5 mV). Panel D shows the corresponding projection of the color-coded LGE-CMR-derived PSI map (red = dense scar, blue = normal tissue, cream/orange = border zone). Putative conducting corridors were identified and annotated with yellow (10% layer) and blue (20% layer) lines and were superimposed onto the voltage map. Following substrate ablation targeting LAVAs local abnormal ventricular activities (LAVAs) identified by EAM, VT was still inducible. The critical isthmus, exhibiting a diastolic potential (Panel E and F), was located in a region previously identified as a HTC on the PSI map (panel D, yellow circle). Application of radiofrequency energy resulted in prompt termination of the VT (Panel G). ICD, implanted cardioverter defibrillator; VT, ventricular tachycardia; CMR, cardiac magnetic resonance; EAM, electroanatomic mapping; LGE, late gadolinium enhancement; PSI, pixel signal intensity; LAVA, local abnormal ventricular activities; HTC, heterogeneous tissue channel.
Figure 5.
A patient with previous myocardial infarction experienced multiple ICD shocks due to recurrent episodes of VT. The pre-procedural CMR was of insufficient quality (Panel A); however, the use of wideband sequences (Panel B) enabled clear visualization and characterization of an inferolateral scar. The scar was successfully imported into the EAM system using ADAS 3D software. Panel C displays a posterior view of the bipolar voltage map with standard thresholds for dense scar (<0.5 mV) and border zone (<1.5 mV). Panel D shows the corresponding projection of the color-coded LGE-CMR-derived PSI map (red = dense scar, blue = normal tissue, cream/orange = border zone). Putative conducting corridors were identified and annotated with yellow (10% layer) and blue (20% layer) lines and were superimposed onto the voltage map. Following substrate ablation targeting LAVAs local abnormal ventricular activities (LAVAs) identified by EAM, VT was still inducible. The critical isthmus, exhibiting a diastolic potential (Panel E and F), was located in a region previously identified as a HTC on the PSI map (panel D, yellow circle). Application of radiofrequency energy resulted in prompt termination of the VT (Panel G). ICD, implanted cardioverter defibrillator; VT, ventricular tachycardia; CMR, cardiac magnetic resonance; EAM, electroanatomic mapping; LGE, late gadolinium enhancement; PSI, pixel signal intensity; LAVA, local abnormal ventricular activities; HTC, heterogeneous tissue channel.
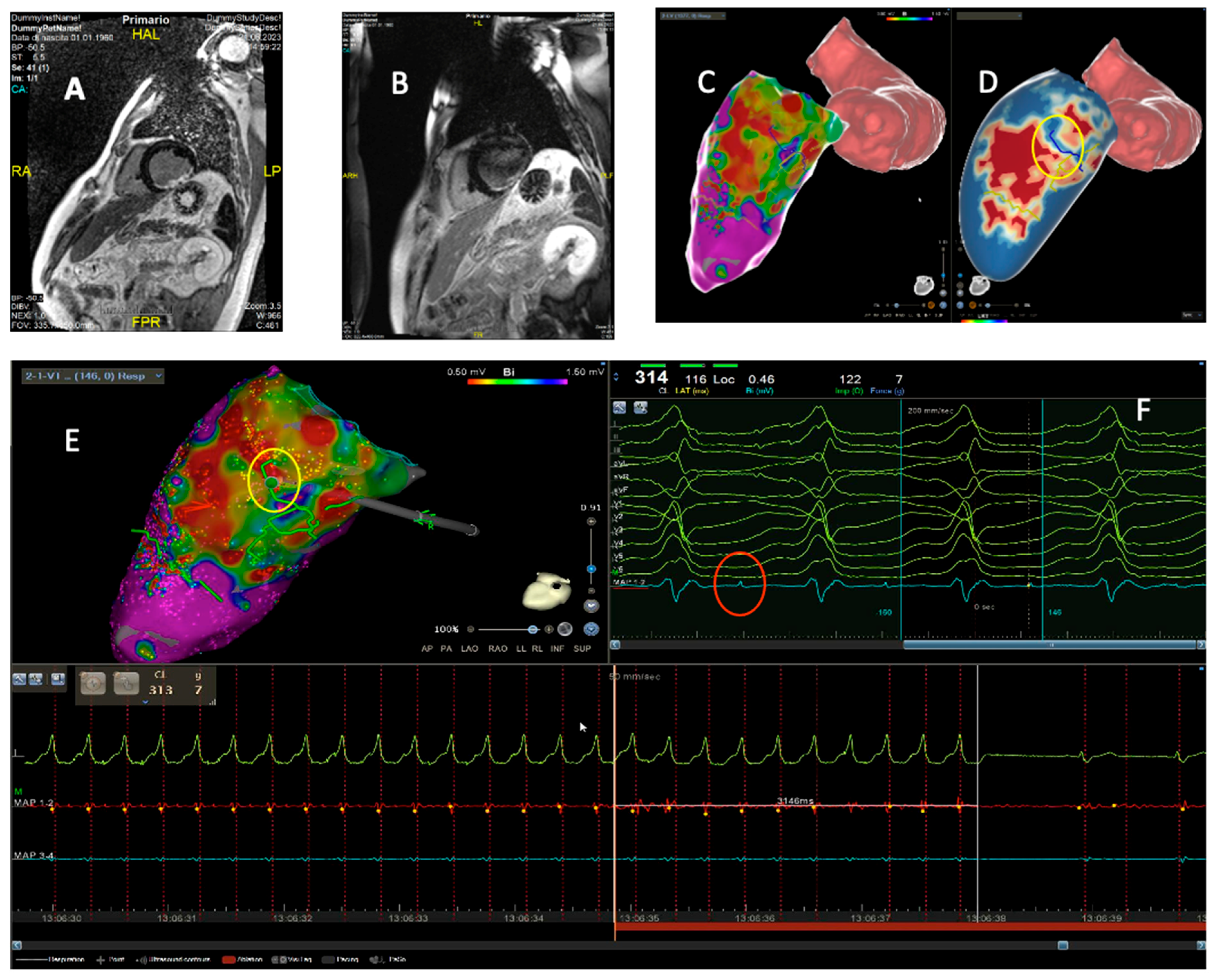
Figure 6.
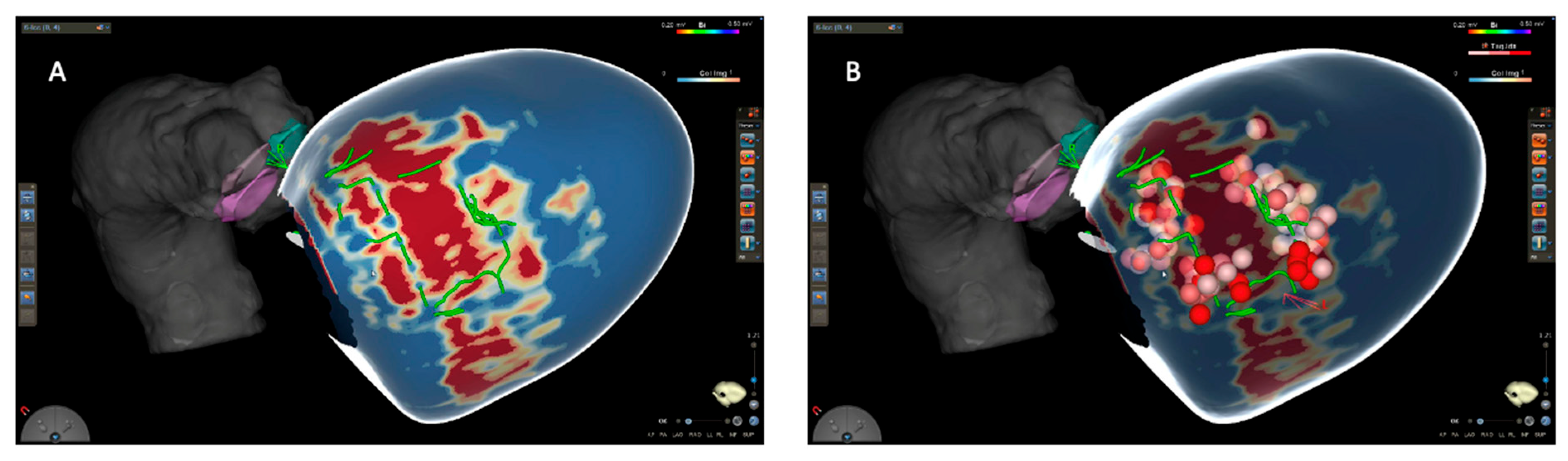
CMR-guided VT ablation. Patient with previous inferolateral MI and recurrent episodes of VT. A) figure shows color-coded LGE-CMR-derived PSI map. Blue: normal myocardium, red: dense scar. Green lines indicate putative HTC. B) Dots indicate lesions set at the entrance and within the HCT. At the end of the procedure VT was no more inducible. After 36 months of follow-up, no arrhythmia recurrences occurred. CMR, cardiac magnetic resonance; MI, myocardial infarction; VT, ventricular tachycardia; LGE, late gadolinium enhancement; PSI, pixel signal intensity; HTC, heterogeneous tissue channel.
Figure 6.
CMR-guided VT ablation. Patient with previous inferolateral MI and recurrent episodes of VT. A) figure shows color-coded LGE-CMR-derived PSI map. Blue: normal myocardium, red: dense scar. Green lines indicate putative HTC. B) Dots indicate lesions set at the entrance and within the HCT. At the end of the procedure VT was no more inducible. After 36 months of follow-up, no arrhythmia recurrences occurred. CMR, cardiac magnetic resonance; MI, myocardial infarction; VT, ventricular tachycardia; LGE, late gadolinium enhancement; PSI, pixel signal intensity; HTC, heterogeneous tissue channel.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



