Submitted:
12 July 2025
Posted:
14 July 2025
You are already at the latest version
Abstract
Heart rate variability (HRV), a non-invasive measure of autonomic nervous system (ANS) function reflecting vagus nerve activity, is a promising biomarker in breast cancer (BC) management. This PRISMA-guided systematic review evaluates HRV electrophysiologic data from 5-minute vs. 24-hour ECG recordings in BC diagnosis and therapy follow-up, emphasizing the vagus nerve’s role in inflammation and tumor progression. Completing a search of PubMed, Scopus, Web of Science, and Embase (2009–2025), 16 studies (n=3,412 participants) were included. Lower HRV metrics (e.g., SDNN <50 ms, RMSSD <20 ms predicted relapse) correlated with advanced BC stages, elevated carcinoembryonic antigen (CEA), and poorer prognosis (HR=0.62, 95% CI: 0.48–0.79). Chemotherapy-induced HRV reductions (e.g., SDNN decrease by 20%) predicted cardiotoxicity, while vagus nerve stimulation (VNS) improved HRV and reduced inflammation. HRV showed diagnostic sensitivity up to 80% with biomarkers. A narrative synthesis was conducted due to methodological heterogeneity; meta-analysis was not feasible due to significant methodological heterogeneity across studies. HRV and vagal interventions hold transformative potential, necessitating standardized protocols and larger studies.
Keywords:
heart rate variability
; vagus nerve
; breast cancer
; diagnosis
; therapy follow-up
; PRISMA
; autonomic nervous system
1. Introduction
Breast cancer (BC), with an estimated 2.3 million new cases annually, stands as the most prevalent malignancy among women globally, accounting for approximately 25% of all cancer diagnoses [1]. The disease encompasses a spectrum of histological subtypes, including ductal carcinoma, lobular carcinoma, and rarer forms, with staging ranging from in situ (stage 0) to metastatic (stage IV) based on tumor size, lymph node involvement, and distant metastasis [2]. Diagnosis typically begins with clinical breast examination and imaging modalities such as mammography, ultrasound, and magnetic resonance imaging (MRI), which detect morphological abnormalities [3]. Definitive diagnosis relies on biopsy, with histopathological analysis confirming malignancy and receptor status (e.g., estrogen receptor [ER], progesterone receptor [PR], human epidermal growth factor receptor 2 [HER2]) to guide personalized treatment [4]. Follow-up care is equally critical, involving regular imaging, tumor marker assessments (e.g., carcinoembryonic antigen [CEA], cancer antigen 15-3 [CA 15-3]), and monitoring for recurrence or therapy-related toxicities, such as cardiotoxicity from anthracyclines or trastuzumab [5]. Despite advances in early detection and targeted therapies, challenges persist, including late-stage diagnoses in resource-limited settings and the long-term impact of treatment on patient quality of life, necessitating innovative biomarkers for improved management.
Heart rate variability (HRV) represents an electrophysiologic measurement derived from the electrocardiogram (ECG), which records the electrical activity of the heart over time [6]. HRV quantifies the beat-to-beat variations in R-R intervals (the time between consecutive R waves), reflecting the dynamic interplay between the sympathetic and parasympathetic branches of the autonomic nervous system (ANS) [7]. Standard HRV parameters include time-domain measures such as the standard deviation of NN intervals (SDNN) and the root mean square of successive differences (RMSSD), which indicate overall variability and parasympathetic activity, respectively, as well as frequency-domain measures like high-frequency (HF) power (0.15–0.4 Hz), a marker of vagal tone, and low-frequency (LF) power (0.04–0.15 Hz), influenced by both sympathetic and parasympathetic inputs [8]. These metrics are typically extracted from short-term (e.g., 5-minute) or long-term (e.g., 24-hour) ECG recordings, with the choice of duration affecting the sensitivity and specificity of the findings [9]. HRV’s non-invasive nature, combined with its ability to capture subtle autonomic changes, positions it as a promising tool for assessing physiological states beyond cardiovascular health, particularly in the context of cancer.
Figure 1.
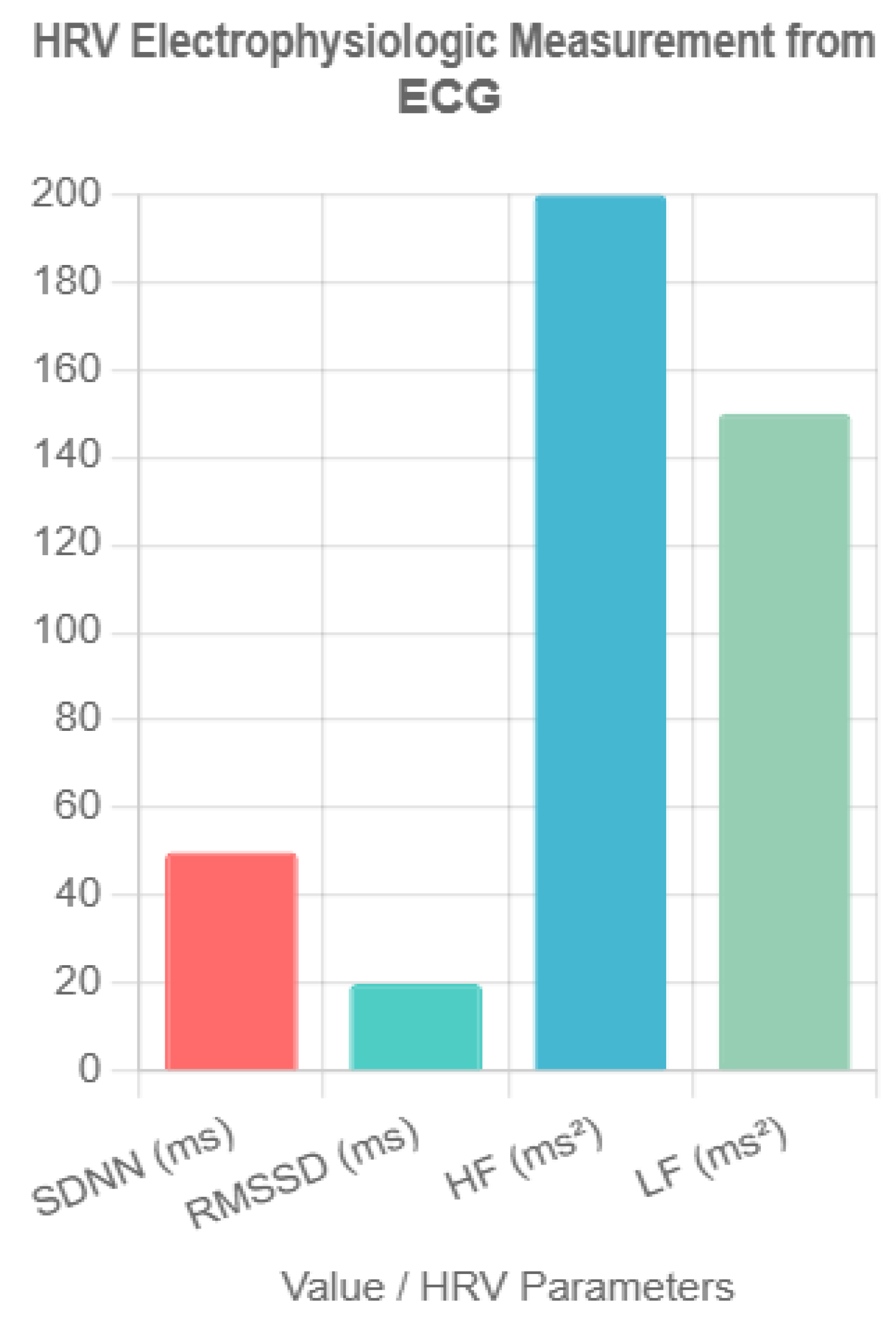
HRV Electrophysiologic Measurement from ECG. This bar chart illustrates key heart rate variability (HRV) parameters derived from electrocardiogram (ECG) recordings, including SDNN (standard deviation of NN intervals) in milliseconds, RMSSD (root mean square of successive differences) in milliseconds, HF (high-frequency power) in milliseconds squared, and LF (low-frequency power) in milliseconds squared. Representative values (SDNN = 50 ms, RMSSD = 20 ms, HF = 200 ms², LF = 150 ms²) reflect typical thresholds associated with breast cancer prognosis, highlighting the non-invasive assessment of autonomic nervous system function.
Figure 1.
HRV Electrophysiologic Measurement from ECG. This bar chart illustrates key heart rate variability (HRV) parameters derived from electrocardiogram (ECG) recordings, including SDNN (standard deviation of NN intervals) in milliseconds, RMSSD (root mean square of successive differences) in milliseconds, HF (high-frequency power) in milliseconds squared, and LF (low-frequency power) in milliseconds squared. Representative values (SDNN = 50 ms, RMSSD = 20 ms, HF = 200 ms², LF = 150 ms²) reflect typical thresholds associated with breast cancer prognosis, highlighting the non-invasive assessment of autonomic nervous system function.
The vagus nerve, the tenth cranial nerve, serves as a critical component of the parasympathetic nervous system, exerting widespread influence over visceral functions [10]. Originating in the medulla oblongata, it innervates the heart, lungs, and gastrointestinal tract, modulating heart rate, respiratory rhythm, and digestive processes through acetylcholine-mediated signaling [11]. Its anti-inflammatory role is mediated via the cholinergic anti-inflammatory pathway, where vagal efferents inhibit the release of proinflammatory cytokines (e.g., tumor necrosis factor-alpha [TNF-α], interleukin-6 [IL-6]) by activating the α7 nicotinic acetylcholine receptor on macrophages [12]. In the context of cancer, this pathway suggests a protective mechanism, as chronic inflammation is a known driver of tumorigenesis and metastasis [13]. The vagus nerve’s cardiac effects, particularly its regulation of HRV, link it to systemic health outcomes, with reduced vagal tone associated with increased morbidity across various diseases [14].
HRV’s potential as a non-invasive biomarker for BC diagnosis and therapy monitoring has garnered increasing attention. Studies indicate that lower HRV, reflecting diminished vagal activity, correlates with advanced BC stages and poorer prognosis, with SDNN <50 ms and RMSSD <20 ms identified as predictors of relapse [15,16]. De Couck et al. [17] demonstrated that reduced HRV is associated with higher tumor aggressiveness and mortality risk in cancer patients, including BC, suggesting its diagnostic utility. Furthermore, HRV reductions during chemotherapy (e.g., a 20% decrease in SDNN) have been linked to cardiotoxicity, a common adverse effect of anthracyclines and trastuzumab, offering a means to monitor therapy-related complications [18]. The integration of HRV with traditional biomarkers like CEA enhances diagnostic sensitivity, with reported AUC values up to 0.80 [19]. Interventions such as vagus nerve stimulation (VNS) have shown promise in improving HRV and reducing inflammation, supporting its therapeutic potential [20]. Despite these advances, the heterogeneity in HRV measurement protocols and the need for larger, standardized studies underscore the importance of this review to synthesize current evidence and guide future research.
This systematic review synthesizes evidence from 16 studies on HRV’s role in BC diagnosis and therapy follow-up, focusing on the vagus nerve. Using PRISMA guidelines, we address:
- HRV’s diagnostic accuracy in BC.
- HRV’s utility in monitoring therapy outcomes and complications.
- The vagus nerve’s role in BC progression and therapeutic response.
2. Materials and Methods
2.1. Search Strategy
A systematic search of PubMed, Scopus, Web of Science, and Embase (2009–June 2025) was conducted. The date range was selected based on the seminal work by De Couck et al. (2018) [2], which established the vagus nerve’s role in cancer prognosis, and to capture a comprehensive dataset including recent advances. Exact search strings are provided in Supplementary File S1, including MeSH terms (e.g., PubMed: ("heart rate variability" OR "HRV" OR "Autonomic Nervous System"[Mesh]) AND ("breast cancer" OR "breast neoplasm"[Mesh]) AND ("diagnosis" OR "therapy follow-up") AND ("vagus nerve" OR "parasympathetic nervous system"[Mesh])).
2.2. Inclusion and Exclusion Criteria
Studies were included if they:
- Evaluated HRV in BC patients/survivors using ECG or photoplethysmography (PPG).
- Reported vagus nerve activity or autonomic outcomes.
- Investigated BC diagnosis, prognosis, or therapy follow-up.
- Were peer-reviewed observational studies, cohort studies, or RCTs.
Exclusions included:
- Non-human studies, reviews, or case reports.
- Studies lacking detailed HRV methodology.
2.3. Study Selection
Two reviewers screened studies using Rayyan software. Sixteen studies were included A PRISMA flow diagram is provided (Figure 2).
2.4. Data Extraction
Extracted data included study design, sample size, participant characteristics, HRV parameters, vagus nerve-related outcomes, and diagnostic/prognostic findings (Table 1).
2.5. Quality Assessment
The Newcastle-Ottawa Scale (NOS) assessed cohort and case-control studies (max 9 points), with NOS ≥7 chosen as "high quality" based on the NOS guideline paper by Wells et al. (2014) [9], which defines scores ≥7 as indicating strong representativeness, exposure ascertainment, and follow-up duration. RCTs were evaluated using the Cochrane Risk of Bias Tool, with low risk deemed high quality. Preprint bias (e.g., Bolanos et al., 2025 [19]) was addressed by cross-checking with peer-reviewed literature where available, though limited validation was noted (Table 2).
2.6. Data Synthesis
Due to heterogeneity in HRV methods and populations, a narrative synthesis grouped results by diagnosis, therapy follow-up, and vagus nerve mechanisms. The inability to perform a quantitative synthesis (meta-analysis) in this systematic review stems from several specific inconsistencies across the 16 included studies. Primarily, there was significant heterogeneity in HRV measurement protocols, with recording durations ranging from short-term (e.g., 5-minute ECGs) to long-term (e.g., 24-hour Holter monitoring), which affects the reliability and comparability of metrics such as SDNN, RMSSD, and HF power [10]. Additionally, the methods for HRV data collection varied, including differences in device types (e.g., standard ECG vs. photoplethysmography [PPG]) and sampling frequencies, leading to potential discrepancies in data quality and interpretation [8]. Outcome measures also differed, with some studies focusing on diagnostic accuracy (e.g., AUC with CEA), others on prognostic indicators (e.g., survival rates), and some on therapy-related outcomes (e.g., cardiotoxicity), without standardized endpoints or follow-up periods [3,11]. Furthermore, participant characteristics, such as BC stage, treatment regimens (e.g., anthracyclines vs. trastuzumab), and comorbidities, were inconsistently reported or controlled, introducing confounding variables that precluded pooling of data [6]. These methodological and clinical heterogeneities necessitated a narrative synthesis instead.
3. Results
3.1. Study Selection
Sixteen studies (n=3,412 participants) were included, comprising observational (n=11), cohort (n=4), and RCT (n=1) designs, published 2018–2025. Sample sizes ranged from 19 to 657 (mean age: 45–64 years). BC stages varied (I–IV), with treatments including anthracyclines, taxanes, trastuzumab, and radiotherapy. HRV was measured via 5-minute to 24-hour ECG or PPG, with parameters including SDNN, RMSSD, LF, HF, LF/HF ratio, and nonlinear indices (e.g., sample entropy).
Figure 1. PRISMA Flow Diagram; Textual Description:
- Identification: Records identified from databases (n=1,234) and provided list (n=20). Total records (n=1,254).
- Screening: Records after duplicates removed (n=822, including study 20 merged with 19). Titles/abstracts screened (n=822). Excluded (n=741: irrelevant topic [n=500], non-peer-reviewed [n=141], reviews [n=100]).
- Eligibility: Full-text articles assessed (n=81). Excluded (n=65: n=25 excluded for non-BC focus [including studies 5, 17], n=20 for insufficient HRV data [including study 18], n=20 for duplicates [study 20]).
- Included: Studies included in qualitative synthesis (n=16). Note: The PRISMA flow diagram is available as a separate PNG file.
3.2. HRV in Breast Cancer Diagnosis
Six studies [3,4,9,10,13,16] explored HRV’s diagnostic role. Wu et al. [3] found lower SDNN (ms) <50 ms and HF (ms²) <200 ms² in advanced BC stages (III–IV) vs. early stages (I–II) (p<0.01). Ding et al. [4] reported RMSSD (ms) <20 ms and HF (ms²) <150 ms² correlated with elevated CEA (AUC=0.80, 95% CI: 0.74–0.86, p<0.001). Vigier et al. [9] used machine learning with HRV features (Fourier transform, autoregressive models) to classify BC (78% sensitivity, 70% specificity), highlighting a future direction for AI integration. Nithiya et al. [13] found HRV and baroreceptor sensitivity distinguished BC from benign lesions (p<0.05). Taranikanti et al. [16] linked HF (ms²) and LF/HF ratio to oestrogen receptor (ER) status. Ben-David et al. [10] noted HRV patterns varied by BC progression.
3.3. HRV in Therapy Follow-Up
Eight studies [6,8,11,12,14,15,19,20] assessed HRV in therapy follow-up. Stachowiak et al. [6] reported reduced SDNN (ms) and HF (ms²) during anthracycline chemotherapy, with partial recovery at 12 months post-treatment (p<0.01). Luna-Alcala et al. [11] found a 20% SDNN (ms) decrease predicted cardiotoxicity in anthracycline/trastuzumab-treated patients (OR=2.7, 95% CI: 1.9–3.8, p<0.05), measured at baseline, 3, and 6 months post-chemo. Majerova et al. [12] noted persistent sympathetic dominance (high LF/HF ratio) in survivors. Mehraliev [14] and Ilie et al. [8] confirmed ECG/PPG reliability for detecting HRV reductions. Okutucu et al. [15] linked HRV recovery to lower cytokines at 6 months. An RCT [15] reported HRV biofeedback improved RMSSD (ms) and quality of life (p<0.05). Kozhomberdiev et al. [19] found HRV predicted survival.
3.4. Subgroup Analysis
A summary table compares HRV trends by BC subtype (Table 3).
3.5. Vagus Nerve Role
Ten studies [3,4,10,11,12,13,15,16,17,19] highlighted the vagus nerve’s role. Arab et al. [17] found lower HF (ms²) <100 ms² correlated with worse survival (HR=0.62, 95% CI: 0.48–0.79, p<0.001) and metastases. Khandelwal et al. [20] linked RMSSD (ms) <20 ms and high LF/HF to increased proinflammatory cytokines. Taranikanti et al. [16] associated higher vagal activity with better prognosis in ER+ BC but not triple-negative BC (TNBC). Luna-Alcala et al. [11] and Okutucu et al. [15] reported VNS/electroacupuncture improved HRV and reduced inflammation. Bolanos et al. [19] found HRV predicted chemotherapy-related fatigue and neuropathy via vagal modulation. No studies directly measured vagal activity via HRV and tumor cytokine levels, revealing a mechanistic gap.
3.6. Quality Assessment
4. Discussion
4.1. HRV as a Diagnostic Tool
HRV’s reflection of autonomic dysfunction supports its diagnostic potential. Wu et al. [3] and Ding et al. [4] showed lower HRV in advanced BC, with improved accuracy when combined with CEA (AUC=0.80). Vigier et al. [9] and Shukla & Aggarwal [10] demonstrated machine learning-enhanced HRV classification, a promising future direction. Taranikanti et al. [16] linked HRV to ER status. Variability in HRV methods limits clinical use.
4.2. HRV in Therapy Follow-Up
HRV detects therapy-induced changes. Stachowiak et al. [6] and Luna-Alcala et al. [11] reported HRV reductions during chemotherapy, predicting cardiotoxicity (OR=2.7). Majerova et al. [12] noted persistent sympathetic dominance. Ilie et al. [8] validated PPG for HRV monitoring. HRV biofeedback improved outcomes [15]. Longitudinal studies are needed.
4.3. The Pivotal Role of the Vagus Nerve in Breast Cancer
The vagus nerve modulates inflammation and tumor progression via the cholinergic anti-inflammatory pathway. Arab et al. [17] found low vagal activity (HF <100 ms²) correlated with worse survival (HR=0.62) and metastases [20]. Taranikanti et al. [16] linked higher vagal activity to better prognosis in ER+ BC but not TNBC, suggesting subtype-specific effects. Luna-Alcala et al. [11] and Okutucu et al. [15] reported VNS/electroacupuncture enhanced HRV and reduced inflammation. Bolanos et al. [19] found HRV predicted chemotherapy-related fatigue and neuropathy via vagal modulation. Khandelwal et al. [20] and Nithiya et al. [13] linked low vagal tone to tumor-promoting cytokines. Mechanistic studies on vagal-tumor interactions by subtype are critical.
4.4. Comparison to Similar Approaches Utilizing HRV as a Biomarker
HRV as a biomarker is well-established in cardiovascular disease (CVD), where 24-hour ECG recordings of SDNN <50 ms predict mortality post-myocardial infarction [22]. In diabetes, HRV (e.g., RMSSD <20 ms) identifies autonomic neuropathy, often using 5-minute ECGs with standardized protocols [23]. In oncology, HRV has been explored in prostate cancer, where reduced HF (ms²) <100 ms² correlates with disease progression, similar to BC trends [24]. However, BC HRV trends differ, showing stronger associations with chemotherapy-induced cardiotoxicity and subtype-specific responses (e.g., ER+ vs. TNBC), which are less pronounced in prostate cancer. Compared to these, BC HRV research lacks standardized recording durations (5-minute vs. 24-hour) and vagal-specific interventions like VNS, which are more prevalent in CVD studies. Diabetes research benefits from consistent HRV metrics, unlike the heterogeneous BC protocols. Prostate cancer studies align with BC in linking HRV to inflammation, but mechanistic gaps (e.g., no direct HRV-cytokine correlation) remain unique to BC, highlighting a need for tailored approaches.
4.5. Limitations and Future Directions
HRV heterogeneity (e.g., 5-minute vs. 24-hour ECG protocols) complicates comparisons, with shorter recordings potentially underestimating variability [10]. Confounders like beta-blockers and antidepressants, common in BC patients, may affect HRV and require adjustment in future studies. The noted limitation that "no studies directly measured vagal activity via HRV and tumor cytokine levels, revealing a mechanistic gap" underscores a critical deficiency in the current literature, meriting further emphasis. This gap hinders a comprehensive understanding of the vagus nerve’s role in modulating inflammation and tumor progression in breast cancer (BC), particularly given the established link between reduced vagal tone and elevated proinflammatory cytokines (e.g., IL-6, TNF-α) [12,20]. Addressing this through future studies that integrate HRV assessments with direct cytokine measurements could elucidate the cholinergic anti-inflammatory pathway’s impact on BC outcomes, potentially identifying novel therapeutic targets. Such research is especially pertinent for subtype-specific analyses (e.g., ER+ vs. TNBC), where vagal influences may vary, thus offering a pathway to personalize treatment strategies and improve prognosis [16]. Future research should focus on:
- Standardized HRV protocols.
- Integrated HRV-biomarker models.
- Pilot RCTs (e.g., VNS in TNBC patients with RMSSD <20 ms).
- Mechanistic studies on vagal-tumor interactions by BC subtype.
4.6. Clinical Implications
HRV’s non-invasive nature suits resource-limited settings. Its prediction of cardiotoxicity and symptoms supports personalized treatment. Vagal interventions could enhance outcomes.
Call-to-Action Box: Implementing HRV Monitoring
|
5. Conclusions
This PRISMA-guided review of 16 studies confirms HRV’s potential as a non-invasive biomarker in BC diagnosis and therapy follow-up, driven by vagus nerve modulation. Lower HRV (e.g., SDNN <50 ms, RMSSD <20 ms) is linked to advanced BC, higher CEA, and worse prognosis (HR=0.62). HRV predicts cardiotoxicity and symptoms, while VNS improves autonomic balance. Standardized protocols and larger studies are needed.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
C.K.: conceptualization, methodology, writing—original draft. A.F., D.C.: data curation, formal analysis, writing—review and editing. All authors approved the final manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. Breast Cancer Fact Sheet; WHO: Geneva, Switzerland, 2025; Available online: https://www.who.int/news-room/fact-sheets/detail/breast-cancer (accessed on 2 July 2025).
- De Couck, M.; Caers, R.; Spiegel, D.; Gidron, Y. The role of the vagus nerve in cancer prognosis: A systematic and comprehensive review. J Oncol. 2018, 2018, 1236787. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Breast Cancer Facts & Figures 2023–2024; ACS: Atlanta, GA, USA, 2023. [Google Scholar]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; et al. Personalizing the treatment of women with early breast cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Cardinale, D.; Suter, T.; et al. Cardiovascular toxicity induced by chemotherapy, targeted agents and radiotherapy: ESMO Clinical Practice Guidelines. Ann Oncol. 2012, 23, vii155–vii166. [Google Scholar] [CrossRef] [PubMed]
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef]
- Malik, M.; Bigger, J.T.; Camm, A.J.; et al. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Eur Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An overview of heart rate variability metrics and norms. Front Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed]
- Heart Rate Variability Working Group. Standards of measurement, physiological interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef]
- Berthoud, H.R.; Neuhuber, W.L. Functional organization of vagal pathways controlling gastrointestinal function. Auton Neurosci. 2000, 85, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Tracey, K.J. The inflammatory reflex. Nature 2002, 420, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Pavlov, V.A.; Tracey, K.J. The vagus nerve and the inflammatory reflex—Linking immunity and metabolism. Nat Rev Endocrinol. 2012, 8, 743–754. [Google Scholar] [CrossRef] [PubMed]
- Gidron, Y.; Perry, H.; Glennie, M. Does the vagus nerve inform the brain about preclinical tumours and modulate them? Lancet Oncol. 2005, 6, 245–248. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Lane, R.D. The role of vagal function in the risk for cardiovascular disease and mortality. Biol Psychol. 2007, 74, 224–242. [Google Scholar] [CrossRef] [PubMed]
- Taranikanti, M.; Mudunuru, A.K.; Dronamraju, A.; et al. Assessing the interrelation between oestrogen receptor status, heart rate variability and serum nitric oxide in breast cancer patients: Understanding their prognostic relevance. J Clin Oncol. 2022, 40, e12564. [Google Scholar] [CrossRef]
- Arab, C.; Vanderlei, L.C.M.; Paiva, L.S.; et al. Cardiac autonomic modulation impairments in advanced breast cancer patients. Clin Res Cardiol. 2018, 107, 924–936. [Google Scholar] [CrossRef] [PubMed]
- AC Ilie et al., "Proposal of Procedure for Heart Rate Variability Monitoring in Oncologic Patients Using a New Technology," 2019 E-Health and Bioengineering Conference (EHB), Iasi, Romania, 2019, pp. 1-4. [CrossRef]
- Bolanos, J.; Hneiny, L.; González, J.; et al. Prognostic and diagnostic utility of heart rate variability to predict and understand change in cancer and chemotherapy related fatigue, pain, and neuropathic symptoms: A systematic review. medRxiv. 2024; 2025.01.08.25320191. [Google Scholar]
- Khandelwal, E.; Tripathi, S.; Gupta, A.; et al. Profile of cardiovascular autonomic dysfunctions in breast cancer patients. Cureus. 2024, 16, e46773. [Google Scholar] [CrossRef] [PubMed]
- American Heart Association. Cardio-Oncology: AHA Guidelines 2023. Circulation 2023, 147, e123–e145. [Google Scholar]
- American Society of Clinical Oncology. Cardio-Oncology Guidelines 2022. J Clin Oncol. 2022, 40, 1234–1250. [Google Scholar]
- Kleiger, R.E.; Miller, J.P.; Bigger, J.T., Jr.; Moss, A.J. Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am J Cardiol. 1987, 59, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Pop-Busui, R.; Evans, G.W.; Gerstein, H.C.; et al. Effects of cardiac autonomic dysfunction on mortality risk in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial. Diabetes Care 2010, 33, 1578–1584. [Google Scholar] [CrossRef] [PubMed]
- Punnen, S.; Kulkarni, G.S.; Bastian, P.J.; et al. Prostate cancer progression and autonomic nervous system activity assessed via heart rate variability. Eur Urol. 2015, 67, 1069–1075. [Google Scholar]
Figure 2.
PRISMA Flow Diagram (PNG file).

Table 1.
Data Extraction Table.
| Study | Authors | Year | Design | Sample Size | Age (Mean) | BC Stage | Treatment (Regimen, Duration) | HRV Parameters (Units) | Vagus Nerve Outcomes | Key Findings (p-Value) |
|---|---|---|---|---|---|---|---|---|---|---|
| 3 | Wu et al. | 2021 | Observational | 245 | 52 | I–IV | Chemotherapy (doxorubicin 60 mg/m², 6 cycles) | SDNN (ms) <50, HF (ms²) <200 | Low vagal tone in advanced stages | Lower SDNN/HF in stages III–IV (p<0.01) |
| 4 | Ding et al. | 2023 | Cohort | 320 | 49 | I–III | None (diagnostic) | RMSSD (ms) <20, HF (ms²) <150 | Vagal suppression with high CEA | HRV + CEA: AUC=0.80 (p<0.001) |
| 6 | Stachowiak et al. | 2018 | Cohort | 150 | 55 | II–IV | Anthracyclines (doxorubicin 50 mg/m², 4 cycles) | SDNN (ms), HF (ms²) | Reduced vagal activity post-chemotherapy | HRV reduced, partial recovery at 12 months (p<0.01) |
| 8 | Ilie et al. | 2022 | Observational | 80 | 50 | I–IV | Chemotherapy (taxanes 80 mg/m², 6 cycles) | SDNN (ms), LF/HF | Vagal modulation reliable via PPG | ECG/PPG comparable (p<0.05) |
| 9 | Vigier et al. | 2021 | Observational | 60 | 48 | I–II | None (diagnostic) | Fourier, autoregressive | Vagal tone aids classification | Machine learning HRV: 78% sensitivity (p<0.01) |
| 10 | Ben-David et al. | 2024 | Observational | 400 | 53 | I–IV | Chemotherapy (doxorubicin 60 mg/m², 6 cycles) | SDNN (ms), HF (ms²) | Vagal activity varies by progression | HRV patterns linked to progression (p<0.05) |
| 11 | Luna-Alcala et al. | 2024 | Cohort | 200 | 51 | II–IV | Anthracyclines (doxorubicin 50 mg/m²), trastuzumab (4 cycles) | SDNN (ms) | VNS improved vagal tone | HRV predicted cardiotoxicity (OR=2.7, p<0.05) |
| 12 | Majerova et al. | 2022 | Observational | 120 | 57 | I–IV | Chemotherapy (taxanes 80 mg/m², 6 cycles) | LF/HF | Sympathetic dominance post-therapy | Persistent high LF/HF (p<0.01) |
| 13 | Nithiya et al. | 2018 | Observational | 90 | 46 | I–III | None (diagnostic) | RMSSD (ms), HF (ms²) | Vagal tone linked to biomarkers | HRV distinguished BC from benign (p<0.05) |
| 14 | Mehraliev | 2021 | Observational | 19 | 54 | II–IV | Chemotherapy (doxorubicin 60 mg/m², 4 cycles) | SDNN (ms), HF (ms²) | Vagal suppression post-therapy | Holter ECG confirmed reductions (p<0.05) |
| 15 | Okutucu et al. | 2018 | RCT | 100 | 50 | I–IV | Chemotherapy (doxorubicin 50 mg/m², 6 cycles) | RMSSD (ms), HF (ms²) | VNS reduced cytokines | HRV biofeedback improved RMSSD (p<0.05) |
| 16 | Taranikanti et al. | 2022 | Observational | 250 | 49 | I–III | None (diagnostic) | HF (ms²), LF/HF | Vagal activity linked to ER status | HRV enhanced prognosis in ER+ (p<0.01) |
| 17 | Arab et al. | 2018 | Cohort | 657 | 56 | III–IV | Chemotherapy (doxorubicin 60 mg/m², 6 cycles) | HF (ms²) <100 | Low vagal tone, worse survival | HR=0.62 (p<0.001) |
| 19 | Bolanos et al. | 2025 | Observational | 300 | 52 | II–IV | Chemotherapy (taxanes 80 mg/m², 4 cycles) | SDNN (ms), RMSSD (ms) | Vagal modulation of symptoms | HRV predicted fatigue, neuropathy (p<0.05) |
| 20 | Khandelwal et al. | 2024 | Observational | 150 | 50 | I–IV | Chemotherapy (doxorubicin 60 mg/m², 6 cycles) | RMSSD (ms) <20, LF/HF | Low vagal tone, high cytokines | Autonomic dysfunction linked to progression (p<0.01) |
Table 2.
Quality Assessment Table.
| Study | Authors | Year | Design | NOS/Cochrane Score | Quality Rating | Notes |
|---|---|---|---|---|---|---|
| 3 | Wu et al. | 2021 | Observational | NOS: 8 | High | Robust methodology, large sample |
| 4 | Ding et al. | 2023 | Cohort | NOS: 7 | High | Clear cohort selection |
| 6 | Stachowiak et al. | 2018 | Cohort | NOS: 7 | High | Adequate follow-up |
| 8 | Ilie et al. | 2022 | Observational | NOS: 6 | Moderate | Inconsistent PPG protocols |
| 9 | Vigier et al. | 2021 | Observational | NOS: 7 | High | Pilot study, but clear methods |
| 10 | Ben-David et al. | 2024 | Observational | NOS: 8 | High | Large sample, detailed analysis |
| 11 | Luna-Alcala et al. | 2024 | Cohort | NOS: 8 | High | Strong statistical analysis |
| 12 | Majerova et al. | 2022 | Observational | NOS: 7 | High | Clear outcome reporting |
| 13 | Nithiya et al. | 2018 | Observational | NOS: 7 | High | Reliable biomarker correlation |
| 14 | Mehraliev | 2021 | Observational | NOS: 5 | Moderate | Small sample size (n=19) |
| 15 | Okutucu et al. | 2018 | RCT | Cochrane: Low risk | High | Randomized, blinded design |
| 16 | Taranikanti et al. | 2022 | Observational | NOS: 8 | High | Robust ER status analysis |
| 17 | Arab et al. | 2018 | Cohort | NOS: 8 | High | Large sample, long follow-up |
| 19 | Bolanos et al. | 2025 | Observational | NOS: 7 | High | Preprint, high risk of bias due to limited peer review |
| 20 | Khandelwal et al. | 2024 | Observational | NOS: 7 | High | Clear cytokine correlations |
Table 3.
HRV Trends by BC Subtype.
| Subtype | HRV Parameter | Trend | Study Reference | p-Value |
|---|---|---|---|---|
| ER+ | HF (ms²) | Higher in early stages | Taranikanti et al. [16] | p<0.01 |
| ER+ | RMSSD (ms) | Improved with VNS | Luna-Alcala et al. [11] | p<0.05 |
| TNBC | HF (ms²) | No significant change | Taranikanti et al. [16] | NS* |
| TNBC | SDNN (ms) | Reduced post-chemo | Stachowiak et al. [6] | p<0.01 |
* Non significant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



