Submitted:
10 July 2025
Posted:
11 July 2025
You are already at the latest version
Abstract
BACKGROUND
This review aims to summarize the imaging features on cross-sectional imaging mo-dalities of metastases to the gastrointestinal tract (GI) with a linitis plastica (LP) pat-tern and to present a series of cases from different primary tumours. Challenging questions concerning their diagnosis will be discussed in detail, including their differ-ential diagnosis.
The term LP is to describe the macroscopic appearance of any hollow organ with dif-fuse mural tumour infiltration, responsible for the loss of parietal distensibility. Pri-mary LP, however rare, may be found throughout the GI tract. First described in the stomach, which represents the most frequent location, it is associated with undifferen-tiated adenocarcinoma with poorly cohesive cells, often presenting signet ring fea-tures.
In addition to primary GI LP, LP-like metastases may occur in association with prima-ry tumours arising beyond the GI tract, namely breast (especially the lobular type), urinary bladder and prostate carcinomas.
MAIN TEXT
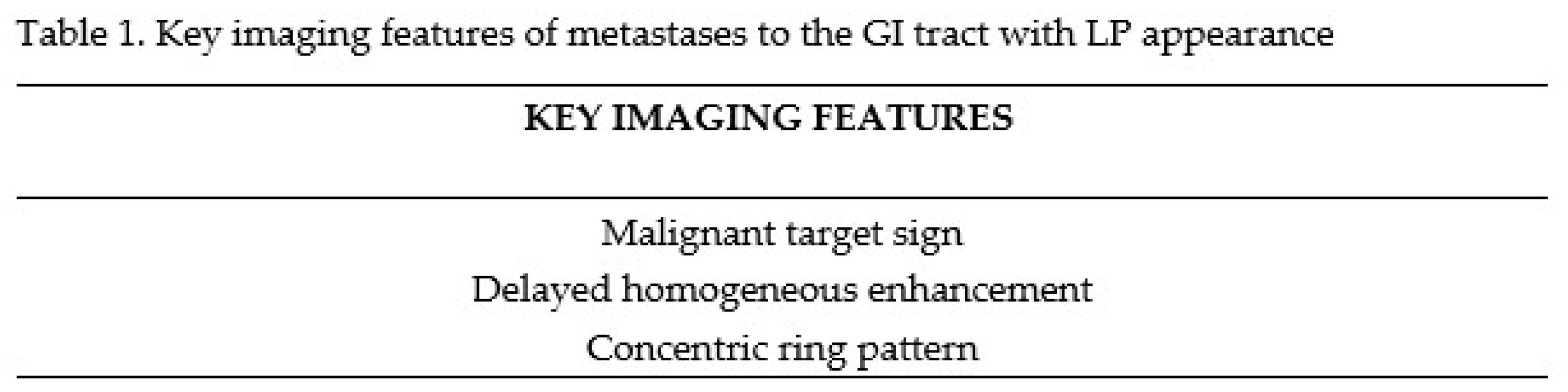
LP-like GI metastases appear as circumferential and enhancing thickenings of the GI, with an exaggerated zonal anatomy and a narrowed lumen. As a result of the diffuse parietal tumour infiltration that frequently preserves the mucosa, the infiltrated sub-mucosa and serosa appear disproportionately expanded with increased enhancement compared to the muscularis propria (MP). This appearance constitutes the malignant target sign, which is to be differentiated from its non-tumoral counterpart, the benign target sign, where the low density intervening and most prominent layer is the edem-atous submucosa.
A homogeneous enhancement with loss of layer differentiation at the delayed phase and a concentric ring pattern on MR have also been described as key imaging features, in addition to associated findings, such as secondary intestinal occlusion and concom-itant peritoneal carcinomatosis (PC).
CONCLUSIONS
GI metastases with LP pattern cause a diagnostic challenge as they may mim-ic primary tumours as well as benign conditions such as inflammatory/infectious dis-eases.
Achieving the correct diagnosis is crucial, as patient management differs. Since the mucosa may be spared, endoscopies and biopsies are frequently negative. Thus, alt-hough immunohistochemistry (IHC) studies are essential, radiologists play a para-mount role in suggesting LP-like GI metastases and proposing deep and extensive bi-opsies to obtain substantial representative tissue to confirm the diagnosis.
Moreover, in the event of an unknown primary tumour, recognition of the LP pattern may be extremely helpful in suggesting possible primary tumours.
Keywords:
Linitis plastica
; gastro-intestinal metastases
; target sign
MAIN TEXT
LP-like GI metastases appear as circumferential and enhancing thickenings of the GI, with an exaggerated zonal anatomy and a narrowed lumen. As a result of the diffuse parietal tumour infiltration that frequently preserves the mucosa, the infiltrated submucosa and serosa appear disproportionately expanded with increased enhancement compared to the muscularis propria (MP). This appearance constitutes the malignant target sign, which is to be differentiated from its non-tumoral counterpart, the benign target sign, where the low density intervening and most prominent layer is the edematous submucosa. A homogeneous enhancement with loss of layer differentiation at the delayed phase and a concentric ring pattern on MR have also been described as key imaging features, in addition to associated findings, such as secondary intestinal occlusion and concomitant peritoneal carcinomatosis (PC).
CONCLUSIONS
GI metastases with LP pattern cause a diagnostic challenge as they may mimic primary tumours as well as benign conditions such as inflammatory/infectious diseases.
Achieving the correct diagnosis is crucial, as patient management differs. Since the mucosa may be spared, endoscopies and biopsies are frequently negative. Thus, although immunohistochemistry (IHC) studies are essential, radiologists play a paramount role in suggesting LP-like GI metastases and proposing deep and extensive biopsies to obtain substantial representative tissue to confirm the diagnosis.
Moreover, in the event of an unknown primary tumour, recognition of the LP pattern may be extremely helpful in suggesting possible primary tumours.
Keywords: Linitis plastica 1, gastro-intestinal metastases 2, target sign 3.
1. Background
Metastases to the GI tract are traditionally considered to be rare. However, the high incidence with which they have been described at autopsy exams, up to 35% in patients with breast cancer for instance, suggests otherwise [1].
Amongst metastases to GI tract, a particular group with LP-like features has also been reported [2].
The expression LP-like refers to its similarity on cross-sectional imaging with primary LP. LP was first introduced in 1779 as a medical term to describe a gastric condition containing scirrhous tissue [3]. The origin of its name is related to the bands of filamentous tissue found within the submucosa, which resemble fibers of linen [4]. A series of scattered definitions followed throughout the years [4,5] until it was stated in 1953 that it corresponded to a cancerous gastric subtype, characterized by a large proportion of fibrous scar tissue [6], and an ominous prognosis [7].
Diagnosis of LP-like metastases to the GI constitutes a challenge throughout the diagnostic process. Focusing on cross-sectional imaging, achieving a correct diagnosis is often difficult given the relative unlikelihood of an isolated GI metastasis compared with a second primary tumour [8]. Metastases with a LP pattern may also mimic a series of benign conditions, making the right diagnosis even more challenging. Despite the defy, it is crucial to accomplish the correct diagnosis as patient management and prognosis may differ considerably.
To the best of our knowledge, a series of cases presenting metastases to the GI tract with a LP pattern from different primary tumours has not yet been reported. Therefore, our aim is to illustrate the findings on cross-sectional imaging of this particular metastatic appearance with a review of the literature. Furthermore, we will also discuss how to distinguish this condition from other malignant and benign causes, which may appear with similar imaging patterns.
2. Main text
Given that LP-like metastases resemble primary LP, a brief rational description of gastric LP will introduce the subject, followed by the description of their key imaging features.
2.1. Primary gastric tumour with LP appearance
The primary gastric tumour originates from the fundic gland cells deep within the mucosa and proceed to disseminate centrifugally into the submucosa, the MP, and the serosa with a desmoplastic reaction pattern [9], resulting in a diffuse infiltration of the gastric wall. Tumour cells are scattered within the stroma rather than replacing it, as any mass-forming tumour would. Thus, the stomach preserves its layered pattern, but it appears strikingly thickened due to the described phenomena: deep infiltrative tumour and exuberant desmoplastic reaction.
Although the term has been broadly used as interchangeable with scirrhous, Lauren or signet ring cell carcinoma, LP does not correlate to a single pathology entity, and it should only be used to describe the macroscopic characteristics of the tumour [10,11,12,13]. It is principally associated with a poorly differentiated adenocarcinoma, whose poorly cohesive cells trigger fibroblasts [4,14], which explains the disproportionate desmoplastic reaction. This process leads to a stiff and shrunken stomach, with significant luminal narrowing and a leather bottle appearance [15] . Signet ring cells, with a large quantity of cytoplasmic mucin and an eccentrically displaced nucleus [14] may also be present, in a variable percentage.
In 1933, it was discovered that the mucosa was frequently preserved or minimally involved in LP [16]. Abundant neo-vascularization, although abnormal and non-functional, has been recently described thanks to advanced endoscopic techniques and it has been postulated that it is secondary to the mechanical compression induced by the extensive reactive fibrosis within the submucosa [17]. At a later stage, rural folds may most frequently disappear, with rigidity and flattening of the mucosa, or become swelled, with a waffle-like appearance [18].
2.1.1. Primary GI tumours with LP appearance: Cross-sectional imaging
Gastric LP is featured on cross-sectional imaging as a diffusely infiltrated stomach with regular concentric wall thickening and a characteristic exaggeration of the normal zonal anatomy. Obliteration of gastric folds, rigidity, and limited distensibility are also key features.
This concentric appearance of the thickened gastric layers share similarity with the “target sign” described by Balthazar on contrast-enhanced computer tomography (CE-CT) for inflammatory and ischemic bowel diseases (Figure 1). Three concentric rings were observed within the intestinal wall showing high-, low- and high-attenuation. The low-attenuation ring corresponded to the submucosa, which, as a result of edema, inflammatory infiltration, blood products or fat appeared as the most prominent layer [19,20]. This sign proved to be useful in differentiating benign from malignant conditions [21]. However, scirrhous gastric tumours were cited as an exception to this rule as they could also present the “target sign” [21,22].
In addition to the stomach, undifferentiated and poorly differentiated small bowel (SB) and colorectal primary tumours may also appear with a LP pattern [10,23,24,25,26,27,28,29]. Cross- sectional imaging features include tumour infiltration of a frequently long segment of the bowel (>5cm) involving full wall thickness, preserving its layers and leading to a rigid and contracted bowel segment [24] (Figure 2).
2.2. Metastases to the GI tract with LP appearance
Metastases to the GI with a LP appearance are more frequent than primary LP [30,31]. Generally speaking, metastases to the GI tract from a primary LP are bound to show the same imaging features [31,32,33]. However, certain non-gastrointestinal primary tumours have also been found to metastasize to the GI tract in this fashion.
Breast cancer is the second most common primary tumour responsible for gastrointestinal metastases, following melanoma [34]. Although invasive lobular carcinoma (ILC) accounts only for 5%-15% of all breast cancer cases [35], it is the subtype most frequently associated with GI metastases with an incidence as high as 40%, compared to 2% invasive carcinoma of no special type NST (the most recent denomination for the invasive ductal carcinoma) [36].
ILC metastases to the GI tract mirror the way ILC diffusely spreads within the breast and thus commonly appear with a LP pattern [37, 38]. This characteristic presentation is related to tumour genomic changes which result in the loss of E-cadherin, the molecule responsible for cell-to-cell adhesion [39].
In addition to the stomach, which remains the hollow organ most frequently affected [38,40], the rectum, the colon and the small bowel may also be involved. Current incidences are difficult to establish since published data vary, probably due to the limited number of patients included in the series [37, 40, 41].
LP-like metastases to the GI tract from prostate and bladder cancers are far less frequent, with only 13 cases of rectal metastases reported for both tumours [42].
Other tumours that may also metastasize with a LP pattern, even more rarely, are lung, pancreaticobiliary and ovarian carcinomas [20, 43, 44]. Whereas gallbladder carcinoma has been traditionally included in this list, no published case reports have been currently found.
2.2.1. Imaging features
Regardless of their origin and their location, LP-like metastases have been reported to show the same imaging characteristics. Unlike mass-like metastases, they appear more infiltrative as regular, symmetrical and concentric thickened segments with a narrowed lumen [31, 32].
The dissemination pattern of GI LP-like metastases has a key role in the interpretation of imaging features. Indeed, the most affected layer is the submucosa. This may be explained by the fact that the main dissemination route seems to be hematogenous and that most of the arterial, venous and lymphatic vessels that supply the mucosa and MP originate from plexi located within the submucosa (Figure 3). Once in the submucosa, metastatic deposits may extend both circumferentially and continuously via the lymphatic channels [1]. An alternative route is the longitudinal intramural spread, favored by the milking force associated with the peristaltic and anti-peristaltic movements [45].
2.2.1.1. Malignant target sign
This imaging feature is a distinct variant of the benign “target sign” and is highly suggestive of LP-like metastases on CE-CT [20,44]. The submucosa is usually the most affected layer as it corresponds to the point of departure of the metastatic infiltration. Moreover, it contains loose connective tissue. These two characteristics allow it to be the layer containing the greatest tumour burden, and it shows a highly enhancing appearance. As the tumour extends centrifugally, tumour cells reach the MP, which is composed of tightly packed muscle cells, so tumoral infiltration will not be as striking as within the submucosa. The next layer involved is the serosa, which contains a layer of vascularized connective tissue, more distensible than the MP (Figure 4). Therefore, following intravenous contrast administration, the alternation of the submucosa, which appears remarkably thickened and enhancing, the MP, which appears as the least enhancing and least thickened layer and the serosa, variably thickened and enhancing, but to a greater degree compared to the MP, constitute the “malignant target sign” of the metastatic bowel (Figure 5). However, it is important to note that the “malignant target sign” is not a diagnostic requirement. Indeed, in our experience, the malignant target sign is not frequently found within the stomach.
2.2.1.2. Homogeneous delayed enhancement
A very specific imaging feature of LP-like metastases is the homogeneous enhancement at a 2 minute-delayed phase on contrast-enhanced cross-sectional imaging, where layers cease to be discernible (Figure 6). This appearance correlates with the abundant desmoplastic reaction associated with LP, which is known for its progressive enhancement [46].
2.2.1.3. Concentric ring pattern
LP-like metastases within the GI tract will appear as a thickened segment with preservation of zonal anatomy. Stratified layers will not only be preserved but, due to intervening tumoral tissue and desmoplastic reaction, the distinction between them will appear exaggerated. Layers may be depicted on magnetic resonance (MR) as a concentric ring pattern on T2 weighted- and diffusion-weighted images as a characteristic imaging finding [47,48,49,50,51] (Figure 7) (Table 1).
2.2.1.4. Length
The length of the affected GI segment varies from rather long in the sigmoid, rectum and anus to segmental in the small bowel and colon [46]. Likewise, gastric involvement may be focal or more frequently diffuse (Figure 8).
Kim et al. observed in their series of patients with primary colorectal carcinoma with LP features that when the rectum was involved, disease frequently reached the anal verge [24], probably secondary to the longitudinal intramural spread mentioned earlier. We have also found this feature quite frequently in LP-like metastases to the rectum (Figure 9).
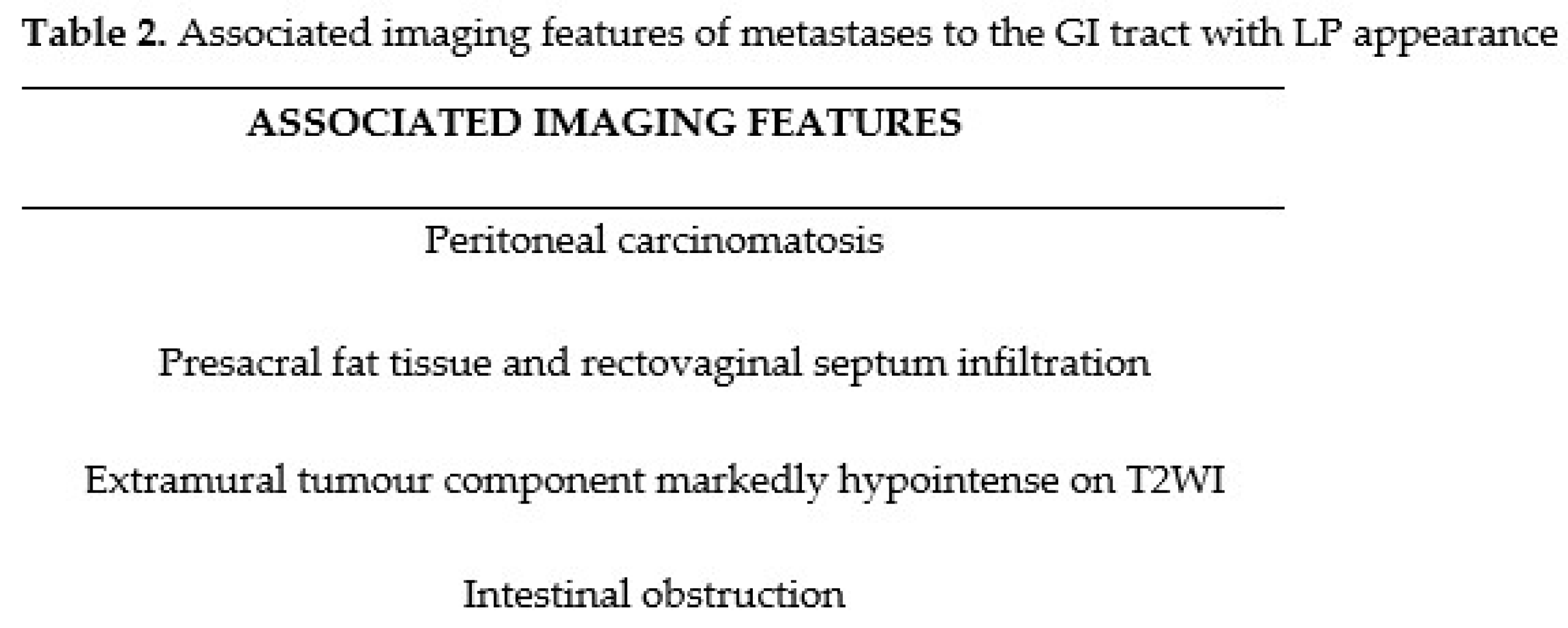
2.2.2. Associated imaging features (Table 2)
2.2.2.1. Peritoneal carcinomatosis
Concomitant PC is frequently encountered, eg. in up to 50-80% of LP-like metastases to the rectum at diagnosis [44]. A characteristic presentation has been described in ILC with rectal LP-like metastases, which includes marked parietal thickening of the bladder and vagina, as well as bilateral hydronephrosis, due to peritoneal involvement (Figure 10) [52].
2.2.2.2. Presacral fat tissue and rectovaginal septum infiltration, and T2 weighted imaging (T2WI) hypointense extramural tumour component
For anorectal LP-like metastases from ILC, two additional imaging features have been reported: the infiltration of the presacral fat tissue and rectovaginal septum (Figure 11) [53] and the presence of an extramural component of the tumour, markedly hypointense on T2WI, probably related to the intense desmoplastic reaction (Figure 12) [47]. However, these features may be extrapolated to other primary tumours as we have found an extramural component markedly hypointense on T2-WI associated with rectal LP-like metastases from bladder carcinoma.
2.2.2.3. Intestinal obstruction
2.3. Diagnostic challenges
LP-like metastases to the GI tract constitute a challenge throughout the diagnostic steps. Therefore, to achieve the correct diagnosis it is mandatory to integrate patient information, including previous clinical history, with imaging and pathologic findings.
3.1. Anamnesis
Several considerations need to be highlighted to avoid misleading conclusions when interpreting GI abnormalities suspicious of malignancy on cross-sectional imaging modalities.
Taking in consideration that the time lapse between the diagnosis of the primary tumour and the occurrence of GI metastases tends to be long (up to a 30-year interval in breast carcinoma) [57], this critical part of information concerning the patient´s oncologic history may occasionally be lost or missed. Therefore, a complete anamnesis represents a key point for a correct diagnosis.
Moreover, the low frequency with which GI metastases are encountered and the fact that they may appear as the only site of disease recurrence, with no signs of active disease elsewhere, may lead to a low index of suspicion [58].
In addition to GI metastases from a known primary tumour, in a low percentage of cases, 3-5%, they may occur from an unknown primary malignancy [59]. In this setting, ICH is indeed fundamental to identifying the primary tumour, but acknowledgement of a LP pattern on cross-sectional imaging may also be extremely helpful in narrowing the list of possible primary tumours and thus guiding the diagnosis (Figure 15).
3.2. Clinical presentation
LP-like metastases to the GI may be clinically silent initially. Although they may be responsible for intestinal obstruction, as previously described, they are most associated with nonspecific GI symptoms that may be attributed to ongoing treatment in an oncologic patient or to other non-malignant GI disorders [60,61].
3.3. Imaging findings
LP-like GI metastases may be challenging to identify due to their infiltrating behavior, as they appear as smooth bowel thickenings on CT [37] and may be mistaken for peristaltic movements.
The frequent possibility of concomitant PC constitutes an additional diagnostic problem. For metastases involving a retroperitoneal bowel segment, the diagnosis is relatively easy. However, in intraperitoneal locations, it may be challenging to differentiate them from peritoneal deposits. What appears to be useful is the absence of peritoneal disease and ascites, which indicate that the lesion is not secondary to peritoneal dissemination. However, it is extremely difficult to correctly rule out peritoneal deposits on cross-sectional imaging.
The differentiation becomes more conspicuous thanks to the key imaging features previously described. In the event of GI tract infiltration secondary to deposits within the serosa, there will be no preservation of the zonal anatomy, so the malignant target sign and the concentric ring pattern will not be found. Moreover, tumoral infiltration in PC is centripetal, the tumour burden will be predominant within the superficial layers. The enhancing behavior will vary, depending principally on the histological characteristics of the primary tumour.
3.4 Pathology
Based on the histological characteristics, it is not always possible to distinguish a GI metastasis with a LP pattern from a peritoneal deposit invading the GI wall. In this setting, imaging may play a paramount role in distinguishing serosal deposits (peritoneal carcinomatosis) from subserosal metastases.
In daily practice, metastatic disease to the GI often remains pathologically unconfirmed (Figure 12). GI metastases often appear at the end-stage of the disease [62], when the patient's clinical condition is poor and the likelihood of agreeing to an endoscopic investigation is presumably reduced. Moreover, endoscopy may be falsely negative, as metastatic disease to the GI tract is primarily submucosal [63] and the mucosa is frequently spared. Superficial biopsies may be negative, rendering it necessary to obtain deep and extensive biopsies when LP-like GI metastases are suspected [64]. Additionally, it is generally difficult to obtain a whole pathological specimen. In fact, in a high number of patients who undergo exploratory laparoscopy, immediate closure occurs due to the widespread disease. Furthermore, even when feasible, metastasectomy does not improve patient prognosis, and surgical intervention is usually limited to palliation in patients who present with GI obstruction or perforation.
2.4. Differential diagnosis
2.4.1. Malignant causes.
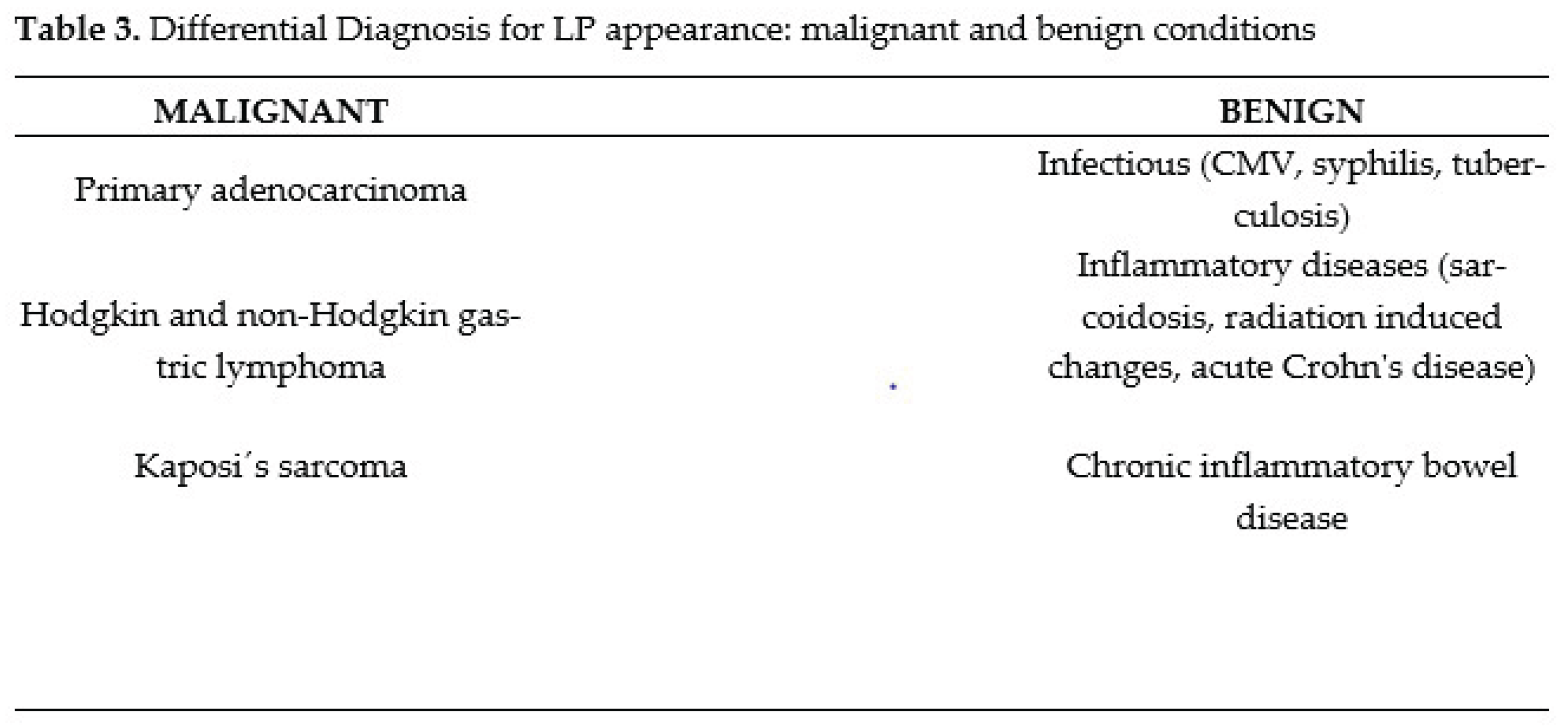
The main differential diagnosis is represented by primary adenocarcinomas of the GI with a LP appearance, which most commonly are undifferentiated or poorly differentiated. IHC is diriment, as conventional histological examinations may fall short on the diagnosis. For instance, ILC may contain a large number of signet ring cells, which, combined with the typical mucosal-preserved pattern of spread, may cause an overlap between metastatic disease to the stomach and a gastric LP primary tumour (Figure 16).
Thus, IHC is essential for the diagnosis: metastatic ILC is usually positive for CK7, ER, PR and GCDFP 15 and negative for vimentin, while CK 20 and CEA are almost always present in primary gastrointestinal tumours and absent in breast carcinomas [65,66]. However, the value of CT and MR in supporting the diagnosis of secondary LP should not be underestimated: although a second primary tumour may occur, metastasis should be suspected first if LP pattern is detected (Figure 17-18).
Figure 18.
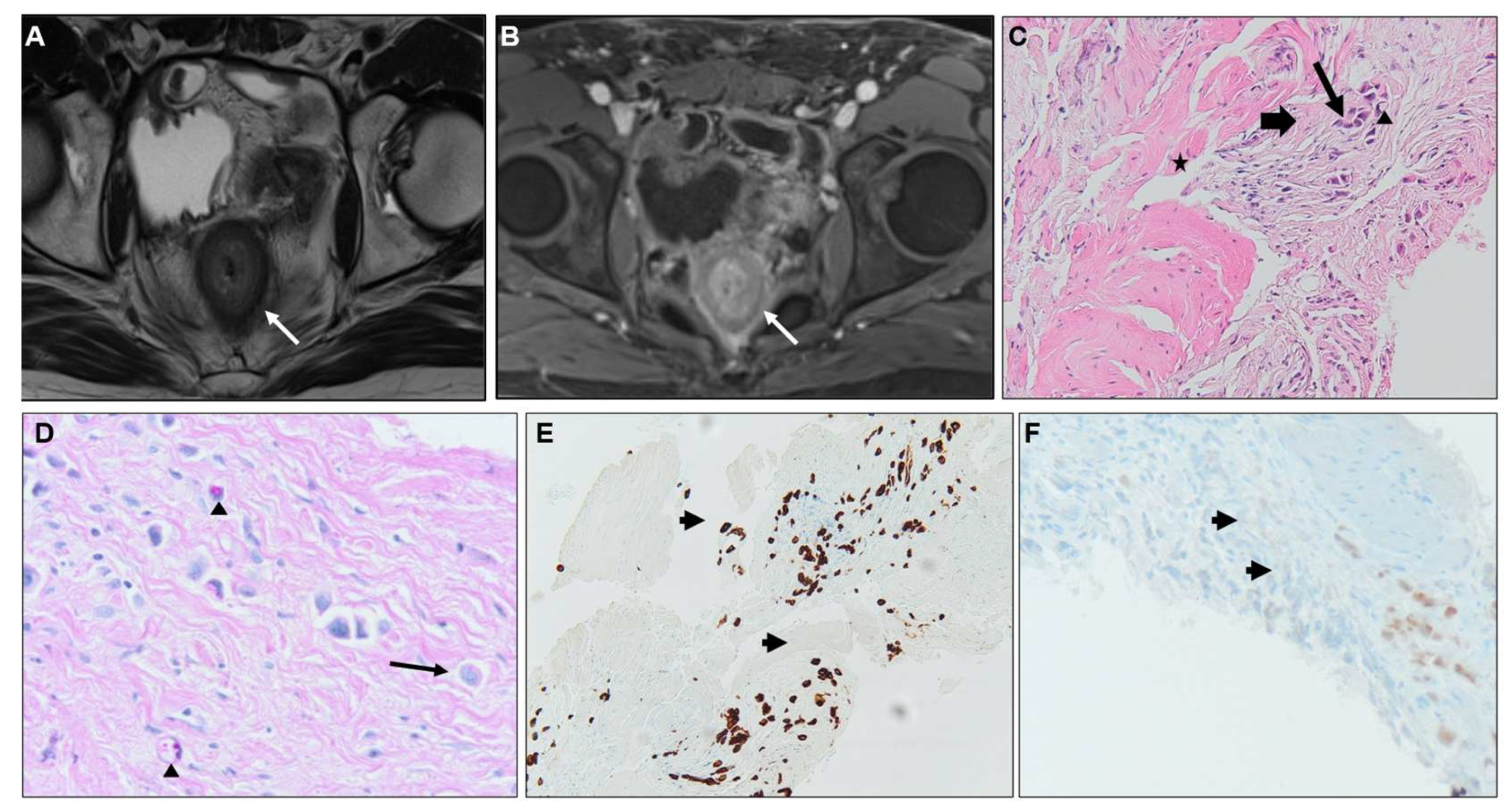
A) Axial T2WI, B) Axial CE-GRE-T1WI, C) 100X Hematoxylin and eosin (H&E) IHC, D) 100X PAS special stain, E) 40X CK7 IHC, F) 40X Gata3 IHC. Patient with bladder adenocarcinoma (plasmocytoid variant with independent cells), treated with surgery and chemotherapy, with suspicion of rectal metastasis on a follow up MR: concentric ring pattern on T2WI (arrow in A) and the malignant target sign (arrow in B). IHC staining followed fine needle biopsy. H&E staining (C) shows tumour infiltration of the rectal MP. Normal muscle cells (*) surrounded by desmoplastic tissue (arrow) containing atypical cells (fine arrow) and scarce signet ring cells (arrowhead). PAS special stain (D) is generally positive in adenocarcinoma of various sites (mucin is PAS+). Notice signet ring cells (arrowheads) and the plasmacytoid aspect of tumour cells (fine arrow ) as plasmacytoid urothelial carcinoma is a variant of infiltrating urothelial carcinoma characterized by tumour cells that have striking morphologic and immunohistochemical resemblance with plasma cells.CK7 IHC (E) staining tumour cells (arrows). CK7 is a membranous / cytoplasmic marker generally expressed in urothelial carcinoma and negative in colorectal carcinoma. Gata3 IHC (F) marking tumour cells (arrows). Gata3 is a nuclear marker with expression in many epithelial neoplasms, including most urothelial carcinomas, primary and metastatic. It is not present in rectal carcinoma. The histological and IHC profile confirmed that the rectal lesion was a metastasis of the primary tumour of the bladder.
Figure 18.
A) Axial T2WI, B) Axial CE-GRE-T1WI, C) 100X Hematoxylin and eosin (H&E) IHC, D) 100X PAS special stain, E) 40X CK7 IHC, F) 40X Gata3 IHC. Patient with bladder adenocarcinoma (plasmocytoid variant with independent cells), treated with surgery and chemotherapy, with suspicion of rectal metastasis on a follow up MR: concentric ring pattern on T2WI (arrow in A) and the malignant target sign (arrow in B). IHC staining followed fine needle biopsy. H&E staining (C) shows tumour infiltration of the rectal MP. Normal muscle cells (*) surrounded by desmoplastic tissue (arrow) containing atypical cells (fine arrow) and scarce signet ring cells (arrowhead). PAS special stain (D) is generally positive in adenocarcinoma of various sites (mucin is PAS+). Notice signet ring cells (arrowheads) and the plasmacytoid aspect of tumour cells (fine arrow ) as plasmacytoid urothelial carcinoma is a variant of infiltrating urothelial carcinoma characterized by tumour cells that have striking morphologic and immunohistochemical resemblance with plasma cells.CK7 IHC (E) staining tumour cells (arrows). CK7 is a membranous / cytoplasmic marker generally expressed in urothelial carcinoma and negative in colorectal carcinoma. Gata3 IHC (F) marking tumour cells (arrows). Gata3 is a nuclear marker with expression in many epithelial neoplasms, including most urothelial carcinomas, primary and metastatic. It is not present in rectal carcinoma. The histological and IHC profile confirmed that the rectal lesion was a metastasis of the primary tumour of the bladder.
Other primary tumours that may appear as a LP are both Hodgkin and non-Hodgkin gastric lymphomas [67,68]. Differentiating imaging features of gastric lymphomas are the less pronounced contrast enhancement and a certain degree of preserved gastric distension due to the lack of desmoplastic response [69].
2.4.2. Benign causes.
Several benign conditions may also mimic gastric LP-like metastases, namely infectious such as CMV [72], syphilis [73] , tuberculosis [74] and inflammatory diseases including sarcoidosis, radiation induced changes and acute Crohn's disease [74,75]. (Table 3)
However, the identification of the benign target sign, with a hypoenhancing edematous submucosa, will ease the diagnosis. Inflammatory changes within surrounding fat and long length of a solitary involved segment, traditionally associated with benign causes [20] will be helpful imaging features, whereas short and multiple segments would favour GI metastases. The length criterion, however, should be taken in with caution as it may vary, and it should be noted that both short and long segments may be affected [78].
Chronic inflammatory bowel disease, with fibrous components and homogeneous wall enhancement on a delayed phase may not be that easy to distinguish, especially considering that malignant transformation in the setting of an inflammatory bowel disease may occur [79].
Despite the challenge, it is crucial to achieve the correct diagnosis as patient management and prognosis differ. While surgical resection is the first option for non-metastatic primary gastric, small bowel and colorectal carcinomas, it should also be considered in certain cases of solitary resectable GI metastases, especially within the stomach [80] or the rectum [42]. These cases require careful evaluation by a multidisciplinary tumour board since the decision depends on the clinical condition of the patient and the underlying primary tumour [42].
In a palliative setting, international guidelines recommend endocrine systemic treatment for metastases from breast cancer [81,82], while radiotherapy may be used in selected cases of rectal metastases.
3. Conclusions
While metastases to the GI tract presenting with a LP pattern are uncommon, their diagnosis holds great importance and acknowledgment of the characteristic appearance on cross-sectional imaging is mandatory for their correct diagnosis.
Although IHC is essential to achieve the correct diagnosis, the value of CT and MR in supporting the diagnosis of secondary LP should not be underestimated. It is the paramount role of the radiologist to suggest the diagnosis and to recommend performing deep and repeated biopsies since the mucosa is frequently spared.
Moreover, in the event of an unknown primary tumour, recognition of the LP pattern may be extremely helpful in suggesting possible primary tumours.
Author Contributions
A.V.S. Designing and writing manuscript, literature review, images and schemes. E.C.L. Literature review, references and image editing. M.G.G. Histology knowledge and imaging. L.M. Radiotherapy knowledge about patient management. C.M. Histology knowledge and imaging. A.M.B. Colonoscopy knowledge and imaging. C.K. Surgical knowledge about patient management. M.A.B. Designing and critical revision of manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This work was in part supported by a grant from the Association Jules Bordet
Institutional Review Board Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| ADC | apparent diffusion coefficient |
| CE | contrast enhanced |
| CT | computer tomography |
| CK7 | cytokeratin 7 |
| DWI | diffusion weighted imaging |
| GI | gastrointestinal |
| GRE-T1WI | gradient recalled echo T1 weighted images |
| H&E | hematoxylin and eosin |
| IHC | immunohistochemistry |
| ILC | invasive lobular carcinoma |
| LP | linitis plastica |
| MP | muscularis propria |
| MPR | multiplanar reconstruction |
| MR | magnetic resonance |
| SB | small bowel |
| PC | peritoneal carcinomatosis |
| T2WI | T2 weighted imaging |
References
- Feczko, P.J.; Collins, D.D.; Mezwa, D.G. Metastatic disease involving the gastrointestinal tract. Radiol Clin North Am. 1993, 31, 1359–73. [Google Scholar] [CrossRef] [PubMed]
- Cormier, W.J.; Gaffey, T.A.; Welch, J.M.; Welch, J.S.; Edmonson, J.H. Linitis plastica caused by metastatic lobular carcinoma of the breast. Mayo Clin Proc. 1980, 55, 747–53. [Google Scholar] [PubMed]
- Mastoraki, A.; Papanikolaou, I.S.; Sakorafas, G.; Safioleas, M. Facing the challenge of managing linitis plastica-review of the literature. Hepatogastroenterology 2009, 56, 1773–8. [Google Scholar] [PubMed]
- Agnes, A.; Estrella, J.S.; Badgwell, B. The significance of a nineteenth century definition in the era of genomics: linitis plastica . World J Surg Oncol. 2017, 5, 15(1)-123. [CrossRef] [PubMed]
- Lyle, H.H. VIII.Linitis Plastica (Cirrhosis of Stomach): With a Report of a Case Cured by Gastro-Jejunostomy. Ann Surg. 1911, 54, 625–68. [Google Scholar] [CrossRef] [PubMed]
- Stout, A.P. Tumors of the stomach, Armed Forces Institute of Pathology, Washington DC, USA, 1953; pp. 1- 134.
- Consul, N.; DiSantis, D.J.; Dyer, R.B. The “leather bottle” stomach. Abdom Radiol (NY) 2018, 43, 2210–1. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, N.; Ulahannan, M.J.; Mandile, M.A.; Cayten, C.G.; Pitchumoni, C.S. Increased risk of colorectal cancer following breast cancer. Ann Surg 1986, 203, 307–10. [Google Scholar] [CrossRef] [PubMed]
- Christodoulidis, G.; Koumarelas, K.E.; Kouliou, M.N.; Samara, M.; Thodou, E.; Zacharoulis, D. The Genomic Signatures of Linitis Plastica Signal the Entrance into a New Era: Novel Approaches for Diagnosis and Treatment. Int J Mol Sci [Internet] 2023. [CrossRef]
- Balthazar, E.J.; Rosenberg, H.D.; Davidian, M.M. Primary and metastatic scirrrhous carcinoma of the rectum. AJR Am J Roentgenol 1979, 132, 711–5. [Google Scholar] [CrossRef] [PubMed]
- Mariette, C.; Carneiro, F.; Grabsch, H.I.; van der Post, R.S.; Allum, W.; de Manzoni, G.; et al. Consensus on the pathological definition and classification of poorly cohesive gastric carcinoma. Gastric Cancer 2019, 22, 1–9. [Google Scholar] [CrossRef] [PubMed]
- El-Nakeep, S.; Kasi, A. Linitis Plastica. StatPearls Publishing, Treasure Island, Florida, USA, 2023.
- Piessen, G; Messager, M; Leteurtre, E; Jean-Pierre, T; Mariette, C. Signet ring cell histology is an independent predictor of poor prognosis in gastric adenocarcinoma regardless of tumoral clinical presentation. Ann Surg. 2009, 250, 878–87. [Google Scholar]
- WHO Classification of Tumours of the Digestive System. 2010. International Agency for Research on Cancer (IARC). WHO Classification of Tumours of the Digestive System. 4th ed. Lyon: IARC; 2010.
- Landry, R.M. Linitis Plastica: A Clinical and Pathological Study of the Various Diseases which May Produce the Leather Bottle Stomach 1950, 140 p.
- Howard, C.P. Linitis plastica: a study of ten cases. QJM 1933, 2, 59–78. [Google Scholar]
- Fornasarig, M.; Capuano, A.; Maiero, S.; Pivetta, E.; Canzonieri, V.; Belluco, C.; et al. pCLE detects mucosal neoplastic vascular pattern in gastric linitis plastica. Clin Exp Med. 2023, 23, 547–51. [Google Scholar] [CrossRef] [PubMed]
- Muraoka, S.; Tsuchida, K.; Iwasaki, M.; Izawa, N.; Jinnai, H.; Komatsubara, T.; et al. A case report of gastric linitis plastica diagnosed by endoscopic ultrasound-guided fine needle aspiration. Medicine 2017, 96, e8937. [Google Scholar] [CrossRef] [PubMed]
- Meyers, M.A.; Oliphant, M.; Teixidor, H.; Weiser, P. Metastatic carcinoma simulating inflammatory colitis. Am J Roentgenol Radium Ther Nucl Med 1975, 123, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Gollub, M.J.; Schwartz, M.B.; Shia, J. Scirrhous metastases to the gastrointestinal tract at CT: the malignant target sign. AJR Am J Roentgenol 2009, 192, 936–40. [Google Scholar] [CrossRef] [PubMed]
- Balthazar, E.J. CT of the gastrointestinal tract: principles and interpretation. AJR Am J Roentgenol 1991, 156, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Balthazar, E.J.; Siegel, S.E.; Megibow, A.J.; Scholes, J.; Gordon, R. CT in patients with scirrhous carcinoma of the GI tract: imaging findings and value for tumor detection and staging. AJR Am J Roentgenol 1995, 165, 839–45. [Google Scholar] [CrossRef] [PubMed]
- Laufman, H.; Saphir, O. Primary linitis plastica type of carcinoma of the colon. AMA Arch Surg 1951, 62, 79–91. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Ha, H.K.; Cho, K.S.; Yu, E.; Kim, J.C.; Yoo, C.S.; et al. CT features of primary colorectal signet-ring cell carcinoma. J Comput Assist Tomogr 2001, 25, 225–30. [Google Scholar] [CrossRef] [PubMed]
- Rao, T.R.; Hambrick, E.; Abcarian, H.; Salgia, K.; Recant, W.M. Colorectal linitis plastica. Dis Colon Rectum 1982, 25, 239–44. [Google Scholar] [CrossRef] [PubMed]
- Brosnan, C.; Hannan, E.; Duggan, W.; Mullen, D.; Buckley, M.; Stafford, A.T. Primary colorectal linitis plastica presenting as rapid acute deterioration: a diagnostic dilemma. Ann R Coll Surg Engl 2020, 102, e187–9. [Google Scholar] [CrossRef] [PubMed]
- Shirouzu, K.; Isomoto, H.; Morodomi, T.; Ogata, Y.; Akagi, Y.; Kakegawa, T. Primary linitis plastica carcinoma of the colon and rectum. Cancer 1994, 74, 1863–8. [Google Scholar] [CrossRef] [PubMed]
- Yen, H.H.; Chen, Y.Y.; Soon, M.S. Primary linitis plastica of the jejunum. Gastrointest Endosc 2006, 63, 503–4. [Google Scholar] [CrossRef] [PubMed]
- Raskin, M.M.; Viamonte, M.; Viamonte, M.Jr. Primary linitis plastica carcinoma of the colon. Radiology 1974, 11, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Papp, J.P.Jr.; Levine, E.J.; Thomas, F.B. Primary linitis plastica carcinoma of the colon and rectum. Am J Gastroenterol 1995, 90, 141–5. [Google Scholar] [PubMed]
- Jang, H.J.; Lim, H.K.; Kim, H.S.; Cho, E.Y.; Lee, S.J.; Kim, K.A.; et al. Intestinal metastases from gastric adenocarcinoma: helical CT findings. J Comput Assist Tomogr 2001, 25, 61–7. [Google Scholar] [CrossRef] [PubMed]
- Fisher, E.R.; Brown, C.H. Linitis plastica carcinoma of the stomach with extensive metastases simulating a colonic lesion. Gastroenterology 1952, 20, 503–8. [Google Scholar] [CrossRef] [PubMed]
- Kondo, K.; Usui, Y.; Matsukawa, M.; Yamada, S.; Negoro, T.; Kan, T.; et al. An autopsy case of gastric metastasis simulating linitis plastica carcinoma from primary linitis plastica carcinoma of the rectu]. Gan No Rinsho 1988, 34, 1996–2001. [Google Scholar] [PubMed]
- Eljabu, W.; Finch, G.; Nottingham, J.; Vaingankar, N. Metastatic deposits of breast lobular carcinoma to small bowel and rectum. Int J Breast Cancer 2011, 2011, 413949. [Google Scholar] [CrossRef] [PubMed]
- Dixon, J.M.; Anderson, T.J.; Page, D.L.; Lee, D.; Duffy, S.W. Infiltrating lobular carcinoma of the breast. Histopathology 1982, 6, 149–61. [Google Scholar] [CrossRef] [PubMed]
- Lamovec, J.; Bracko, M. Metastatic pattern of infiltrating lobular carcinoma of the breast: an autopsy study. J Surg Oncol 1991, 48, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Winston, C.B.; Hadar, O.; Teitcher, J.B.; Caravelli, J.F.; Sklarin, N.T.; Panicek, D.M.; et al. Metastatic lobular carcinoma of the breast: patterns of spread in the chest, abdomen, and pelvis on CT. AJR Am J Roentgenol 2000, 175, 795–800. [Google Scholar] [CrossRef] [PubMed]
- El-Hage, A.; Ruel, C.; Afif, W.; Wissanji, H.; Hogue, J.C.; Desbiens, C.; et al. Metastatic pattern of invasive lobular carcinoma of the breast-Emphasis on gastric metastases. J Surg Oncol 2017, 115, 359. [Google Scholar] [CrossRef] [PubMed]
- McCart Reed, A.E.; Kutasovic, J.R.; Lakhani, S.R.; Simpson, PT. Invasive lobular carcinoma of the breast: morphology, biomarkers and ’omics. Breast Cancer Res 2015, 30, 17:12. [Google Scholar]
- McLemore, E.C.; Pockaj, B.A.; Reynolds, C.; Gray, R.J.; Hernandez, J.L.; Grant, C.S.; et al. Breast cancer: presentation and intervention in women with gastrointestinal metastasis and carcinomatosis. Ann Surg Oncol 2005, 12, 886–94. [Google Scholar] [CrossRef] [PubMed]
- Ambroggi, M.; Stroppa, E.M.; Mordenti, P.; Biasini, C.; Zangrandi, A.; Michieletti, E.; et al. Metastatic breast cancer to the gastrointestinal tract: report of five cases and review of the literature. Int J Breast Cancer, 2012. [Google Scholar]
- Janjic, O.; Labgaa, I.; Hübner, M.; Demartines, N.; Joliat, G.R. Metastasis to the rectum: A systematic review of the literature. Eur J Surg Oncol 2022, 48, 822–33. [Google Scholar] [CrossRef] [PubMed]
- Lior, T.; Chin Ng, S.; Ng, M.K. A rare case of linitis plastica of the colon from ovarian carcinoma. J Surg Case Rep 2019, 2019(3), rjz089. [Google Scholar] [CrossRef] [PubMed]
- Ha, H.K.; Jee, K.R.; Yu, E.; Yu, C.S.; Rha, S.E.; Lee, I.J.; et al. CT features of metastatic linitis plastica to the rectum in patients with peritoneal carcinomatosis. AJR Am J Roentgenol 2000, 174, 463–6. [Google Scholar] [CrossRef] [PubMed]
- Fernet, P.; Azar, H.A.; Stout, A.P. Intramural (tubal) spread of linitis plastica along the alimentary tract. Gastroenterology 1965, 48, 419–24. [Google Scholar] [CrossRef] [PubMed]
- Burgain, C.; Germain, A.; Bastien, C.; Orry, X.; Choné, L.; Claudon, M.; et al. Computed tomography features of gastrointestinal linitis plastica: spectrum of findings in early and delayed phase imaging. Abdom Radiol 2016, 41, 1370–7. [Google Scholar] [CrossRef] [PubMed]
- Lau, L.C.; Wee, B.; Wang, S.; Thian, Y.L. Metastatic breast cancer to the rectum: A case report with emphasis on MRI features. Medicine 2017;96,e6739.
- Rudralingam, V.; Dobson, M.J.; Pitt, M.; Stewart, D.J.; Hearn, A.; Susnerwala, S. MR imaging of linitis plastica of the rectum. AJR Am J Roentgenol 2003, 181, 428–30. [Google Scholar] [CrossRef] [PubMed]
- Mazza, S.; Laurenza, C.; Elvo, B.; Tanzi, G.; Ungari, M.; Soro, S.; et al. Rectal linitis plastica as the first presentation of metastatic lobular breast cancer: an endoscopic ultrasound diagnosis. Clin J Gastroenterol 2022, 15, 1072–7. [Google Scholar] [CrossRef] [PubMed]
- Mommersteeg, M.C.; Kies, D.A.; van der Laan, J.; Wonders, J. Linitis plastica of the rectum secondary to prostate carcinoma. BMJ Case Rep 2022, 15. [Google Scholar] [CrossRef] [PubMed]
- Dresen, R.C.; Beets, G.L.; Rutten, H.J.T.; Engelen, S.M.E.; Lahaye, M.J.; Vliegen, R.F.A.; et al. Locally advanced rectal cancer: MR imaging for restaging after neoadjuvant radiation therapy with concomitant chemotherapy. Part I. Are we able to predict tumor confined to the rectal wall? Radiology 2009, 252, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, G.; Manno, A.; Mulè, A.; Verbo, A.; Rizzo, G.; Sermoneta, D.; et al. Gastro-intestinal symptoms as clinical manifestation of peritoneal and retroperitoneal spread of an invasive lobular breast cancer: report of a case and review of the literature. BMC Cancer 2006, 19, 193. [Google Scholar] [CrossRef] [PubMed]
- Ruymbeke, H.; Harlet, L.; Stragier, B.; Steenkiste, E.; Ryckx, M.; Marolleau, F. Anorectal metastasis from breast carcinoma: a case report and review of the literature. BMC Res Notes 2018, 11, 268. [Google Scholar] [CrossRef] [PubMed]
- Taal, B.G.; den Hartog Jager, F.C.; Steinmetz, R.; Peterse, H. The spectrum of gastrointestinal metastases of breast carcinoma: II. The colon and rectum. Gastrointest Endosc 1992, 38, 136–41. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Zhang, J. Gastric cancer with large bowel obstruction as the first presentation: A case report. Oncol Lett 2013, 6, 1377–9. [Google Scholar] [CrossRef] [PubMed]
- Tariq, T.; Turk, A.; Reaume, M.; Muddasani, A.; Parmar, M. Blocked by a Ring: A Case of Gastric Linitis Plastica Presenting as Large Bowel Obstruction Secondary to Rectal Stenosis. ACG Case Rep J 2019, 6:e00007.2. 57.
- Benfiguig, A.; Anciaux, M.L.; Eugène, C.I.; Benkémoun, G.; Etienne, J.C. Gastric metastasis of breast cancer occurring after a cancer-free interval of 30 years. Ann Gastroenterol Hepatol 1992, 28, 175–7. [Google Scholar]
- Fizazi, K.; Greco, F.A.; Pavlidis, N.; Daugaard, G. ; Oien, K; ; Pentheroudakis, G. et al. Cancers of unknown primary site: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2015 26 Suppl 5,v133–8. [Google Scholar]
- Fayemi, A.O.; Ali, M.; Braun, E.V. Metastatic carcinoma simulating linitis plastica of the colon. A case report. Am J Gastroenterol 1979, 71, 311–4. [Google Scholar] [PubMed]
- Meyers, M.A. Intraperitoneal spread of malignancies and its effect on the bowel. Clin Radiol 1981, 32, 129–46. [Google Scholar] [CrossRef] [PubMed]
- Haberstich, R.; Tuech, J.J.; Wilt, M.; Rodier, J.F. Anal localization as first manifestation of metastatic ductal breast carcinoma. Tech Coloproctol 2005, 9, 237–8. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.; Howell, A.; Chrissohou, M.; Swindell, R.I.; Hudson, M.; Sellwood, R.A. A comparison of the metastatic pattern of infiltrating lobular carcinoma and infiltrating duct carcinoma of the breast. Br J Cancer 1984, 5, :23–30. [Google Scholar] [CrossRef] [PubMed]
- Ferri, L.E.; Onerheim, R.; Emond, C. Linitis plastica as the first indication of metastatic lobular carcinoma of the breast: case report and literature review. Can J Surg 1999, 42, 466–9. [Google Scholar] [PubMed]
- Hsieh, P.S; Yeh, C.Y.; Chen, J.R. Changchien, CR. Ileocecal breast carcinoma metastasis. Int J Colorectal Dis 2004, 19, 607–8. [Google Scholar] [CrossRef] [PubMed]
- Tot, T. The role of cytokeratins 20 and 7 and estrogen receptor analysis in separation of metastatic lobular carcinoma of the breast and metastatic signet ring cell carcinoma of the gastrointestinal tract. APMIS 2000, 108, 467–72. [Google Scholar] [CrossRef] [PubMed]
- Levine, M.S.; Pantongrag-Brown, L.; Aguilera, N.S.; Buck, J.L.; Buetow, P.C. Non-Hodgkin lymphoma of the stomach: a cause of linitis plastica. Radiology 1996, 201, 375–8. [Google Scholar] [CrossRef] [PubMed]
- Ozyilkan, O.; Ozyilkan, E. ; Gastric Hodgkin’s disease presenting with radiological appearance of linitis plastica. Am J Gastroenterol 1999, 94, 3661–2. [Google Scholar] [CrossRef] [PubMed]
- Lo Re, G.; Federica, V.; Midiri, F.; Picone, D.; La Tona, G.; Galia, M.; et al. Radiological Features of Gastrointestinal Lymphoma. Gastroenterol Res Pract 2016, 2016, 2498143. [Google Scholar] [CrossRef] [PubMed]
- Cervia, J.S. Gastric Kaposi’s sarcoma without skin lesions presenting as linitis plastica. Gastrointest Endosc 1992, 38, 96. [Google Scholar] [CrossRef] [PubMed]
- Hadjiyane, C.; Lee, Y.H.; Stein, L.; Jayagopal, S.; Shih, H.; Pellecchia, C. Kaposi’s sarcoma presenting as linitis plastica. Am J Gastroenterol 1991, 86, 1823–5. [Google Scholar] [PubMed]
- Murray, J.G.; Evans, S.J.; Jeffrey, P.B.; Halvorsen, R.A.Jr. Cytomegalovirus colitis in AIDS: CT features. AJR Am J Roentgenol 1995, 165, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Abdu, R.A.; Carter, K.; Pomidor, W.J. Gastric syphilis mimicking linitis plastica. Arch Surg 1993, 128, 103–4. [Google Scholar] [CrossRef] [PubMed]
- Rubesin, S.E.; Levine, M.S.; Laufer, I. Double-contrast upper gastrointestinal radiography: a pattern approach for diseases of the stomach. Radiology 2008, 246, 33–48. [Google Scholar] [CrossRef] [PubMed]
- Calafat, P.; de Diller, A.B.; Sanchez, C. Breast carcinoma metastasis in ileum-colon and gallbladder simulating inflammatory diseases. Rev Fac Cien Med Univ Nac Cordoba 1999, 56, 123–7. [Google Scholar] [CrossRef] [PubMed]
- Macari, M.; Balthazar, E.J. CT of bowel wall thickening: significance and pitfalls of interpretation. AJR Am J Roentgenol 2001, 176, 1105–16. [Google Scholar] [CrossRef] [PubMed]
- Macari, M.; Megibow, A.J.; Balthazar, E.J. A pattern approach to the abnormal small bowel: observations at MDCT and CT enterography. AJR Am J Roentgeno 2007, 188, 1344–55. [Google Scholar] [CrossRef] [PubMed]
- DiPiro, P.J.; Tirumani, S.H.; Cruz, G.P.; Ramaiya, N.H.; Lester, S.C.; Shinagare, A.B. Lobular breast cancer: patterns of intraabdominal metastatic spread on imaging and prognostic significance. Abdom Radiol 2019, 44, 362–9. [Google Scholar] [CrossRef] [PubMed]
- Hristova, L.; Soyer, P.; Hoeffel, C.; Marteau, P.; Oussalah, A.; Lavergne-Slove, A.; et al. Colorectal cancer in inflammatory bowel diseases: CT features with pathological correlation. Abdom Imaging 2013, 38, 421–35. [Google Scholar] [CrossRef] [PubMed]
- Dória, M.T.; Maesaka, J.Y.; Filho, S.N.; Silveira, T.P.; Boufelli, G.; Siqueira, S.A.C.; et al. Gastric metastasis as the first manifestation of an invasive lobular carcinoma of the breast. Autops Case Rep 2015, 5, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Manohar, P.M.; Davidson, N.E. Updates in endocrine therapy for metastatic breast cancer. Cancer Biol Med 2021, 19, 202–12. [Google Scholar] [CrossRef] [PubMed]
- Ethier, SP. Using functional genomics and artificial intelligence to reverse engineer human cancer cells; Cambridge Scholars Publishing: Newcastle upon Tyne, UK; 2023; p. 161. [Google Scholar]
Figure 1.
A) Scheme of the layers of the normal gastrointestinal tract (GI). B) Scheme representing the target sign in benign conditions: the submucosa appears thickened and the most prominent low-attenuation layer as a result of edema, inflammatory infiltration, blood products or fat. C) Axial contrast-enhanced (CE)-CT: benign target sign (arrow) in the context of enteritis secondary to radiotherapy.
Figure 1.
A) Scheme of the layers of the normal gastrointestinal tract (GI). B) Scheme representing the target sign in benign conditions: the submucosa appears thickened and the most prominent low-attenuation layer as a result of edema, inflammatory infiltration, blood products or fat. C) Axial contrast-enhanced (CE)-CT: benign target sign (arrow) in the context of enteritis secondary to radiotherapy.
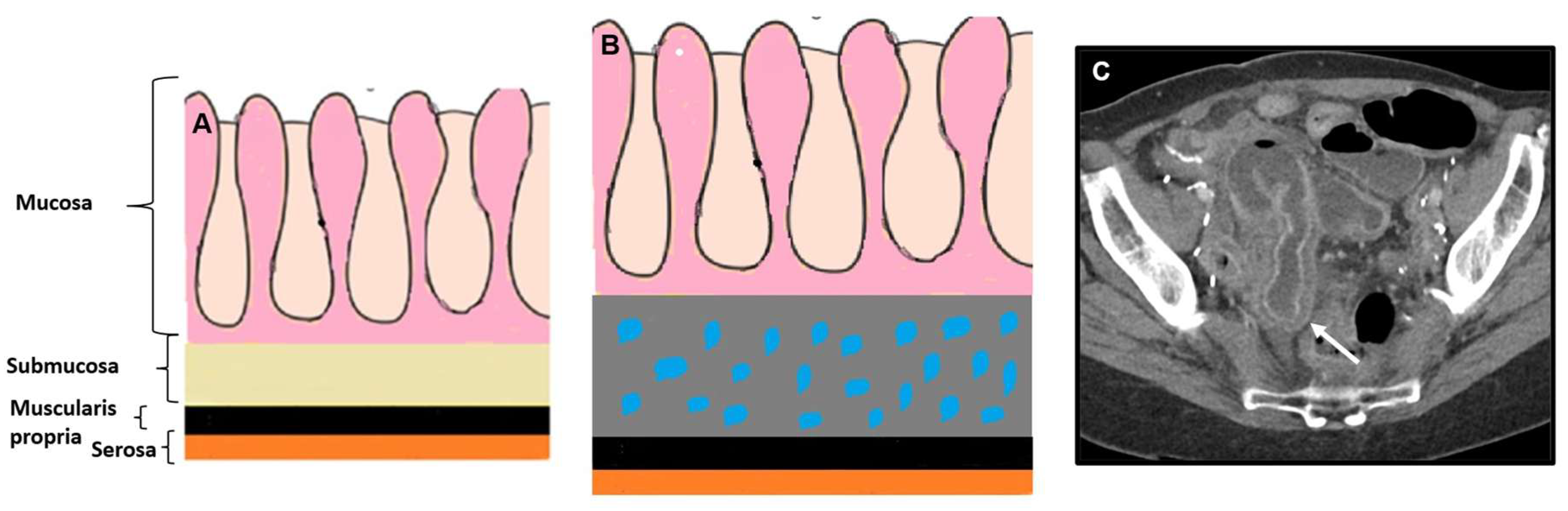
Figure 2.
Primary GI tumours with LP-pattern. Tumour infiltration of the bowel wall with a full wall thickness involvement, preserving its layers and leading to a rigid and contracted bowel segment. A) CE-CT Coronal MPR. Undifferentiated tumour of the duodenum (arrow). B) Axial CE-CT. Undifferentiated tumour of the ascending colon (arrow). C) CE-CT Coronal MPR. Undifferentiated tumour of the sigmoid colon (arrow). D) Axial CE-CT. Undifferentiated tumour of the rectum (arrow)..
Figure 2.
Primary GI tumours with LP-pattern. Tumour infiltration of the bowel wall with a full wall thickness involvement, preserving its layers and leading to a rigid and contracted bowel segment. A) CE-CT Coronal MPR. Undifferentiated tumour of the duodenum (arrow). B) Axial CE-CT. Undifferentiated tumour of the ascending colon (arrow). C) CE-CT Coronal MPR. Undifferentiated tumour of the sigmoid colon (arrow). D) Axial CE-CT. Undifferentiated tumour of the rectum (arrow)..
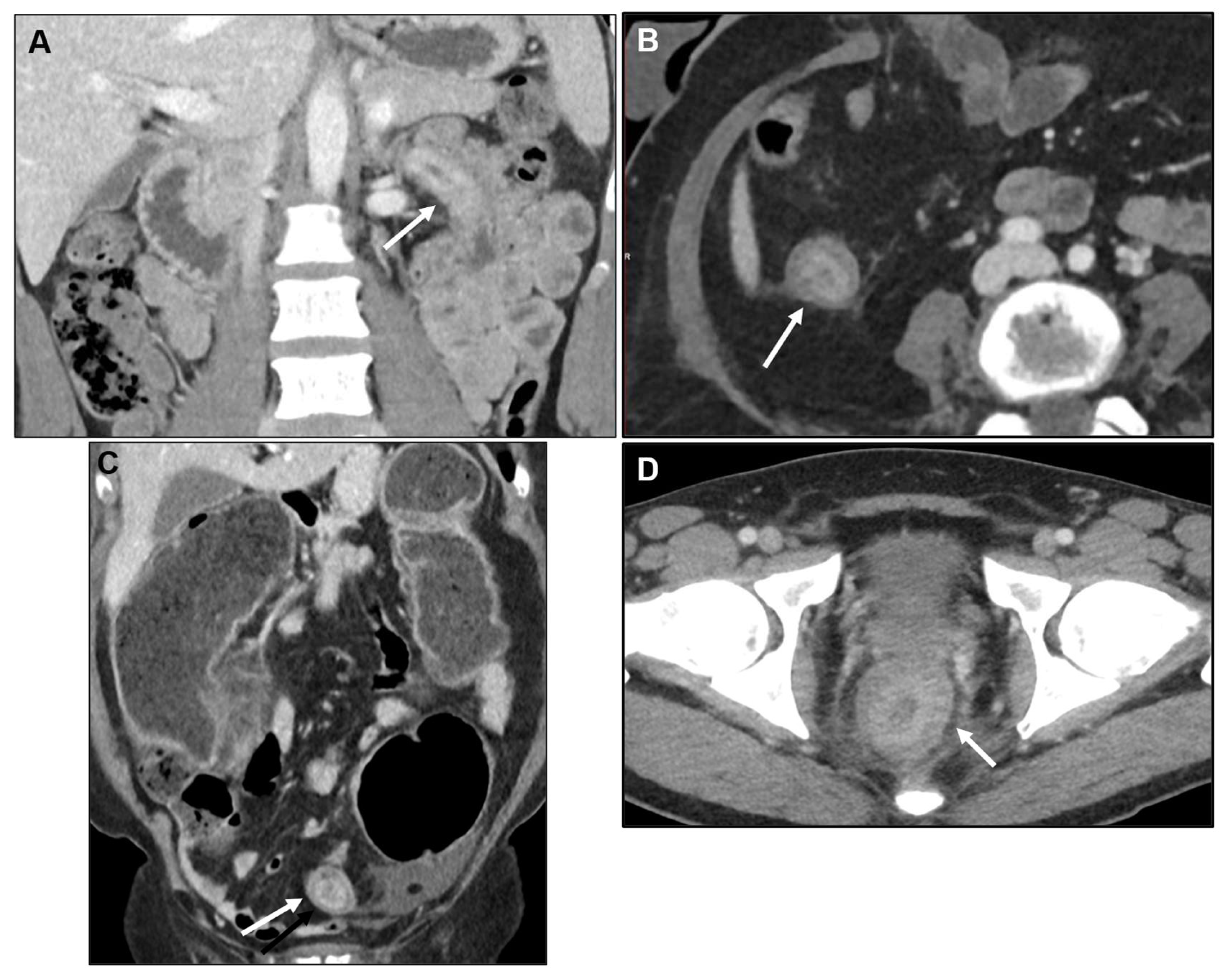
Figure 3.
Scheme representing layers of the GI tract and its vasculature. Most of the arterial, venous and lymphatic vessels that supply the mucosa and muscularis propria (MP) originate from plexi located within the submucosa (*).
Figure 3.
Scheme representing layers of the GI tract and its vasculature. Most of the arterial, venous and lymphatic vessels that supply the mucosa and muscularis propria (MP) originate from plexi located within the submucosa (*).
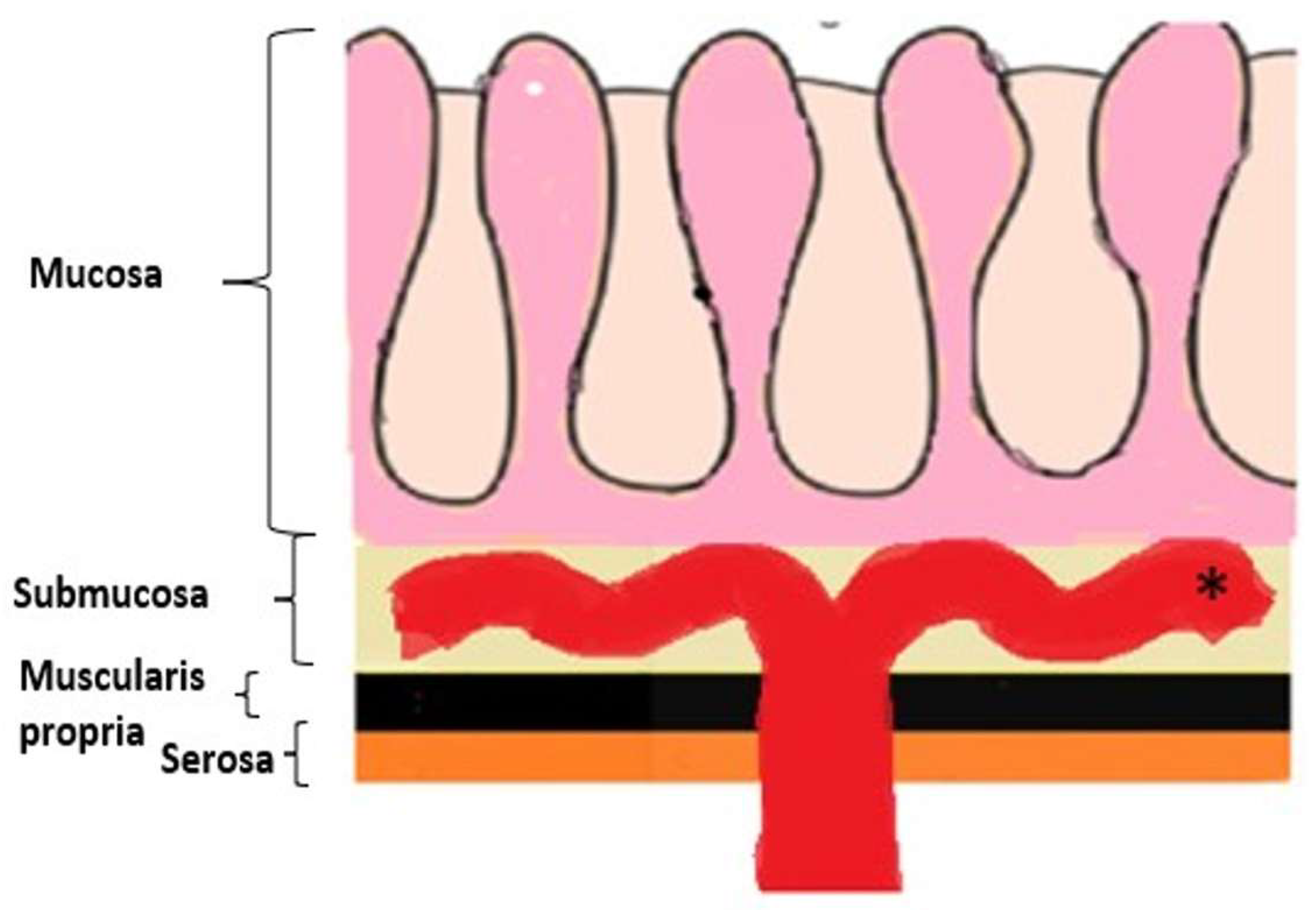
Figure 4.
A) Scheme of the layers of the normal GI tract. B) Scheme representing the centrifugal infiltration of LP-like metastases within the bowel wall. The submucosa is usually the most affected layer as it corresponds to the point of departure of the metastatic infiltration and it contains loose connective tissue. As the tumour extends centrifugally, the next involved layer is the MP, which is composed of tightly packed muscle cells, so tumour infiltration will not be as striking as within the submucosa. The next involved layer is the serosa, which contains a layer of vascularized connective tissue, more distensible than the MP.
Figure 4.
A) Scheme of the layers of the normal GI tract. B) Scheme representing the centrifugal infiltration of LP-like metastases within the bowel wall. The submucosa is usually the most affected layer as it corresponds to the point of departure of the metastatic infiltration and it contains loose connective tissue. As the tumour extends centrifugally, the next involved layer is the MP, which is composed of tightly packed muscle cells, so tumour infiltration will not be as striking as within the submucosa. The next involved layer is the serosa, which contains a layer of vascularized connective tissue, more distensible than the MP.
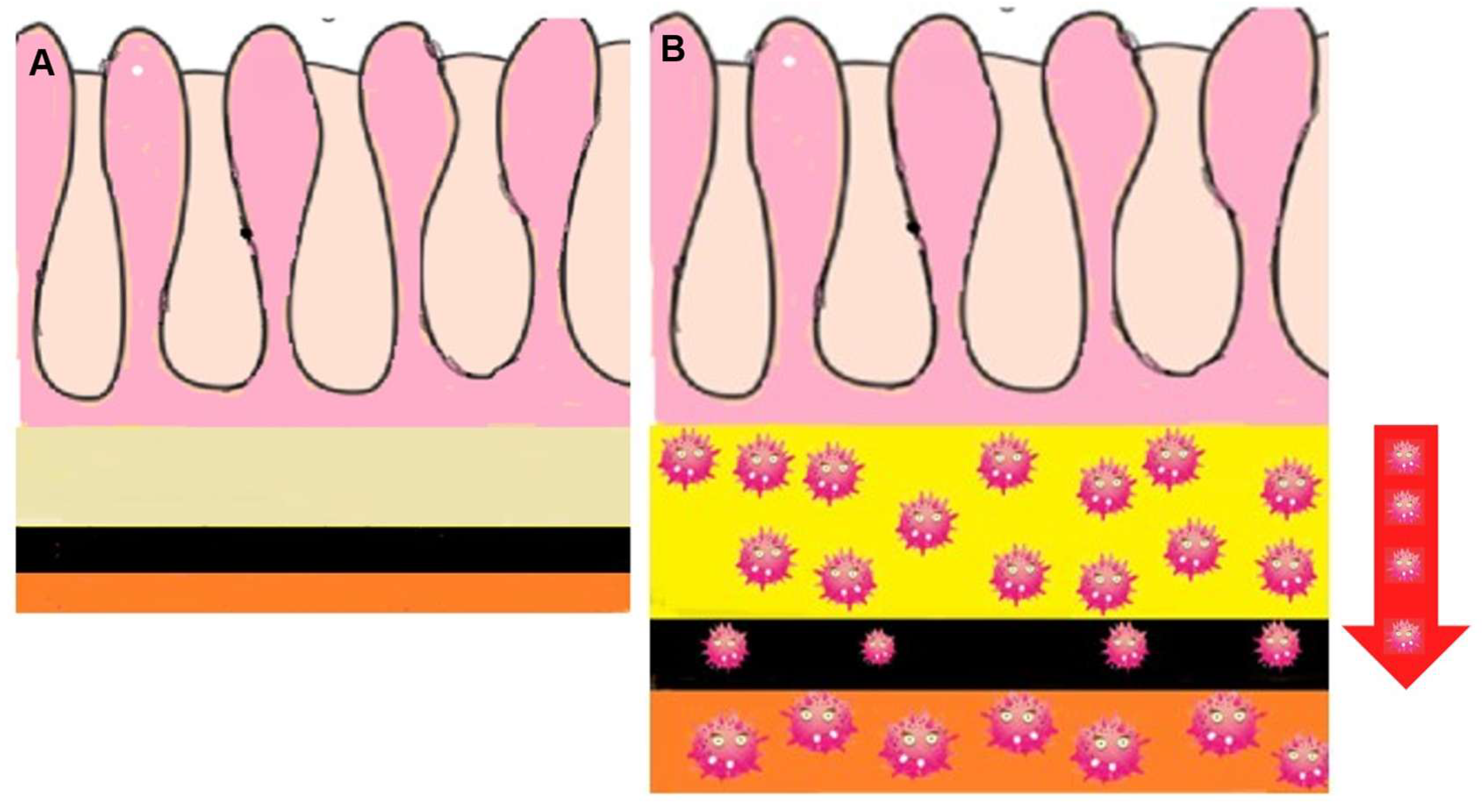
Figure 5.
Malignant target sign. A) Axial CE-CT. Metastasis to the caecum from invasive lobular carcinoma (ILC). B) Axial CE-GRE-T1WI. Rectal metastasis from breast adenocarcinoma.
Figure 5.
Malignant target sign. A) Axial CE-CT. Metastasis to the caecum from invasive lobular carcinoma (ILC). B) Axial CE-GRE-T1WI. Rectal metastasis from breast adenocarcinoma.
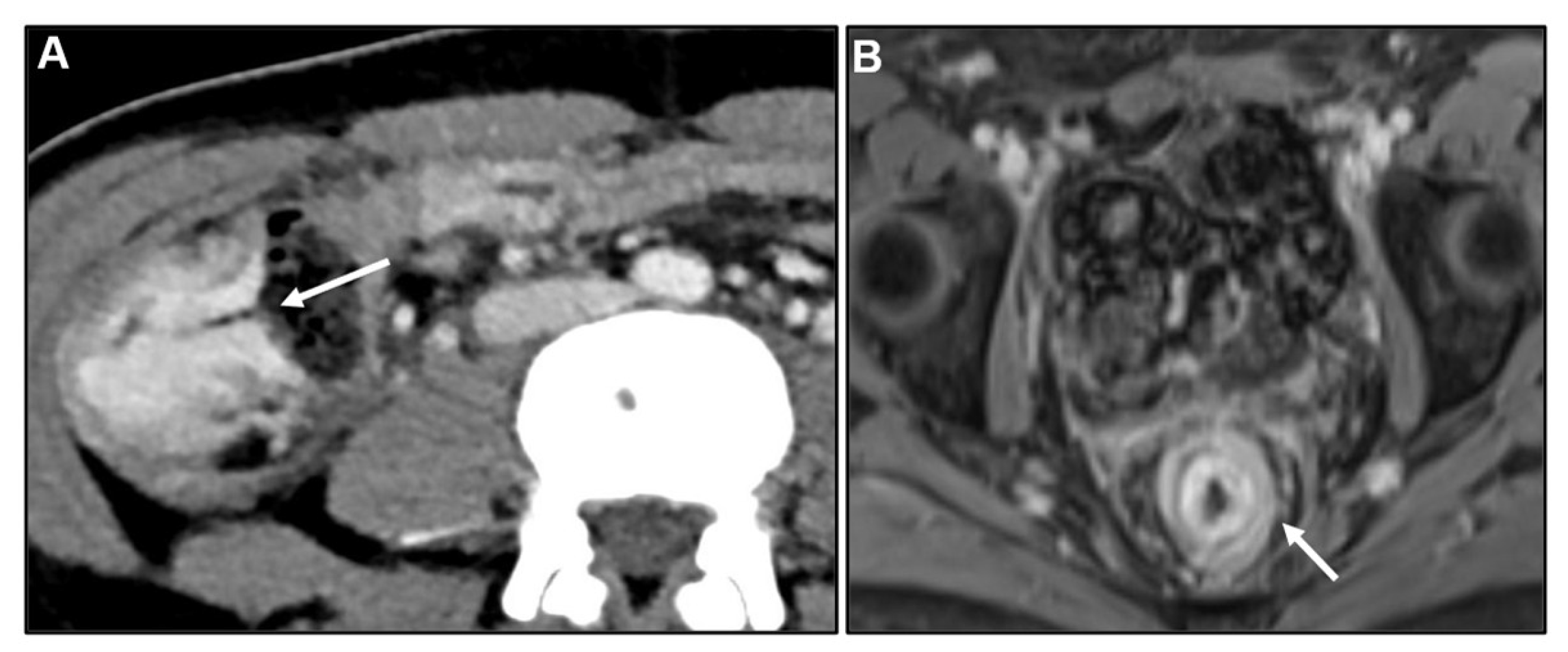
Figure 7.
Concentric ring pattern on T2 weighted imaging (T2WI) and diffusion weighted imaging (DWI). Metastatic infiltration will appear as a thickened wall with preservation of zonal anatomy. Stratified layers are preserved, and the distinction between them appears exaggerated. On T2WI and DWI, the characteristic finding is a concentric ring pattern as in A) Axial T2WI and in B-C) DWI and corresponding apparent diffusion coefficient (ADC). Rectal metastasis from breast adenocarcinoma (concentric ring pattern, arrow).
Figure 7.
Concentric ring pattern on T2 weighted imaging (T2WI) and diffusion weighted imaging (DWI). Metastatic infiltration will appear as a thickened wall with preservation of zonal anatomy. Stratified layers are preserved, and the distinction between them appears exaggerated. On T2WI and DWI, the characteristic finding is a concentric ring pattern as in A) Axial T2WI and in B-C) DWI and corresponding apparent diffusion coefficient (ADC). Rectal metastasis from breast adenocarcinoma (concentric ring pattern, arrow).
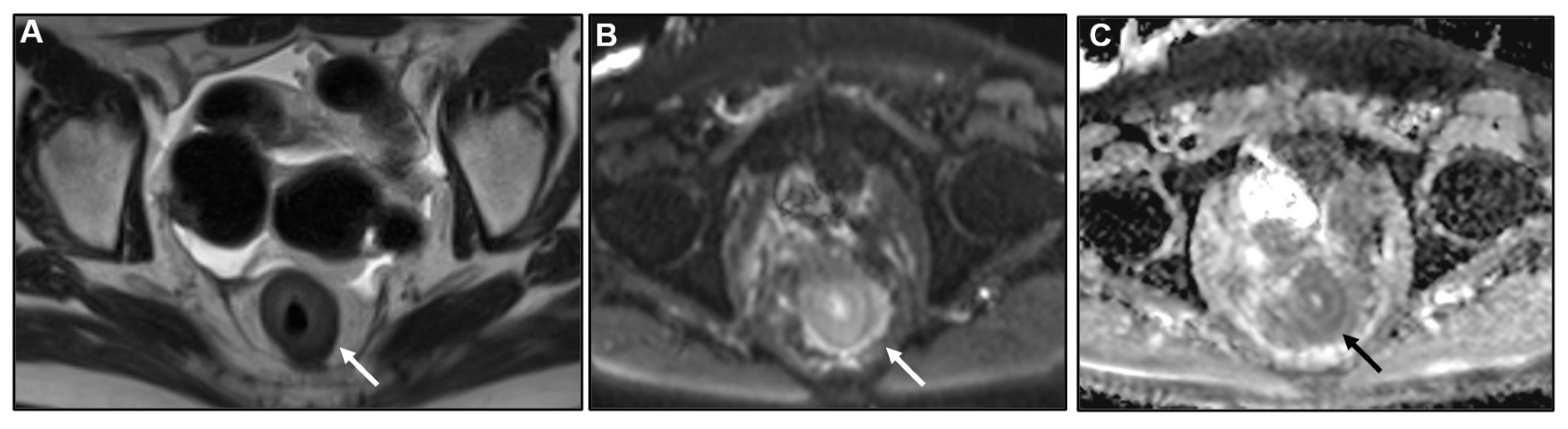
Figure 8.
Appearance of different lengths of the segments involved. A) Axial T2WI. Metastasis to the small bowel (SB) (arrow) from invasive lobular carcinoma (ILC). B) Axial CE-CT. Metastasis to the transverse colon (arrow) from ILC. C) Coronal MPR CE-CT. Metastasis to the ascending (arrow) and descending colon (arrowhead) from gastric adenocarcinoma. D) Axial CE-CT. Metastasis to the sigmoid colon (arrow) from ILC.
Figure 8.
Appearance of different lengths of the segments involved. A) Axial T2WI. Metastasis to the small bowel (SB) (arrow) from invasive lobular carcinoma (ILC). B) Axial CE-CT. Metastasis to the transverse colon (arrow) from ILC. C) Coronal MPR CE-CT. Metastasis to the ascending (arrow) and descending colon (arrowhead) from gastric adenocarcinoma. D) Axial CE-CT. Metastasis to the sigmoid colon (arrow) from ILC.
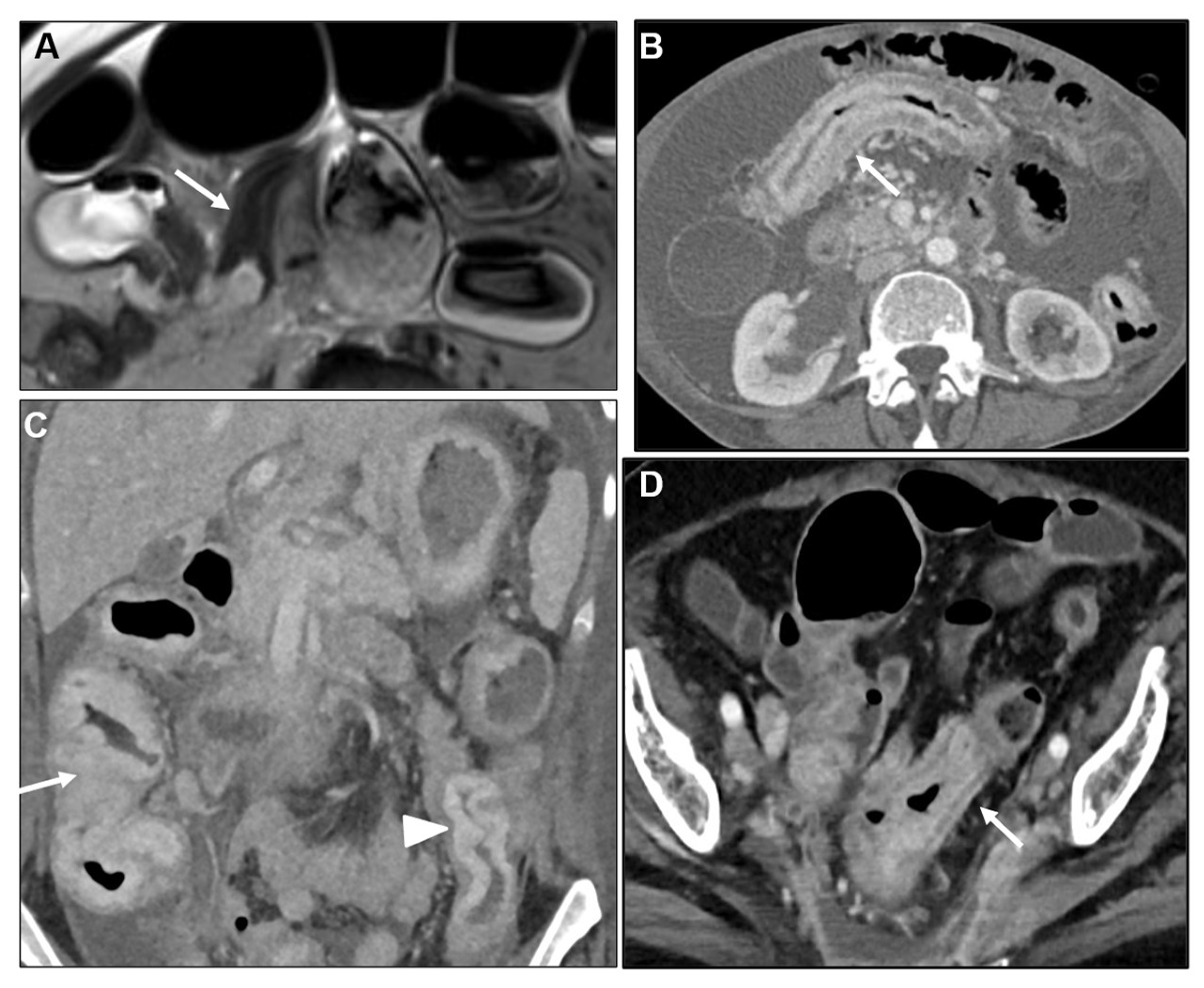
Figure 9.
A-B) Axial CE-GRE-T1WI. Metastasis to the rectum (arrow in A) from breast adenocarcinoma with extension to the anal verge (arrow in B), probably secondary to longitudinal intramural spread linked to peristaltic-antiperistaltic movements.
Figure 9.
A-B) Axial CE-GRE-T1WI. Metastasis to the rectum (arrow in A) from breast adenocarcinoma with extension to the anal verge (arrow in B), probably secondary to longitudinal intramural spread linked to peristaltic-antiperistaltic movements.
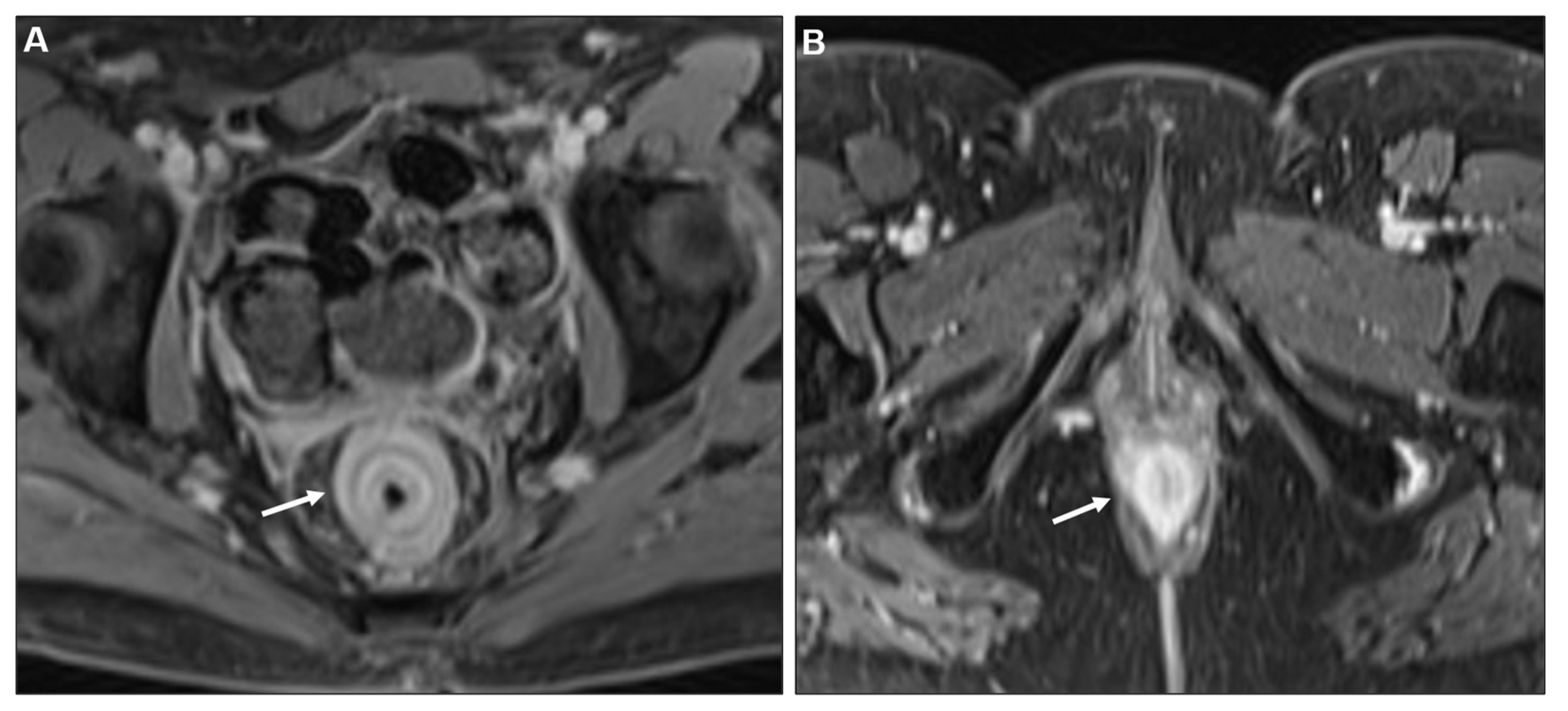
Figure 10.
Concomitant peritoneal carcinomatosis (PC). A) Axial CE-CT B) Axial CE-GRE-T1WI. LP-like metastases from ILC to the rectum (thick arrows) and sigmoid (thin arrows) and concomitant PC with deposits on top of the bladder (* in A) and around the uterus (arrowhead in A), ascites (* in B) and enhancing parietal peritoneum (arrowhead in B). .
Figure 10.
Concomitant peritoneal carcinomatosis (PC). A) Axial CE-CT B) Axial CE-GRE-T1WI. LP-like metastases from ILC to the rectum (thick arrows) and sigmoid (thin arrows) and concomitant PC with deposits on top of the bladder (* in A) and around the uterus (arrowhead in A), ascites (* in B) and enhancing parietal peritoneum (arrowhead in B). .
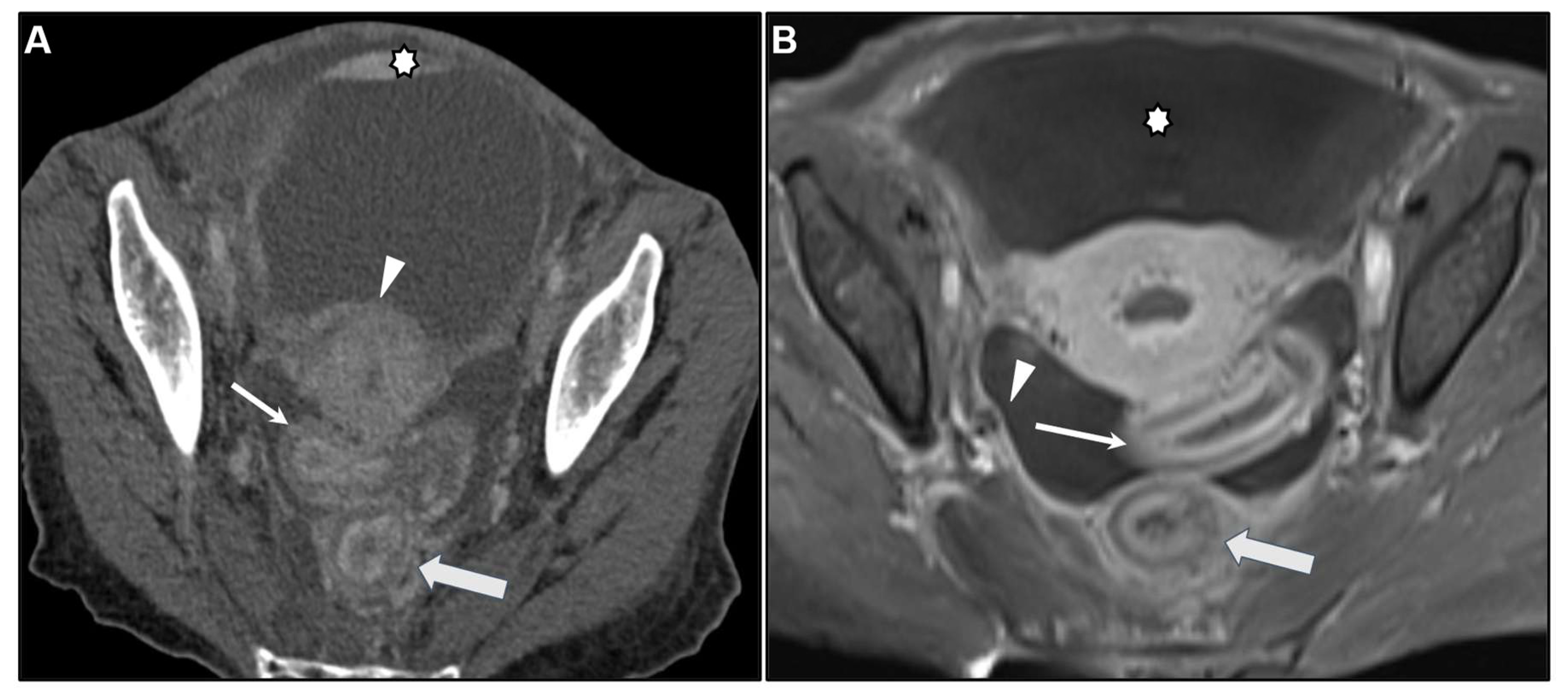
Figure 11.
Infiltration of the rectovaginal septum. A) Axial CE-GRE-T1WI. LP-like rectal metastases (arrow in A) from breast adenocarcinoma with infiltration of the rectovaginal septum (arrowhead in A). B) Corresponding colonoscopy reveals an extrinsic stenosis of the anus and rectum with rigid walls.
Figure 11.
Infiltration of the rectovaginal septum. A) Axial CE-GRE-T1WI. LP-like rectal metastases (arrow in A) from breast adenocarcinoma with infiltration of the rectovaginal septum (arrowhead in A). B) Corresponding colonoscopy reveals an extrinsic stenosis of the anus and rectum with rigid walls.
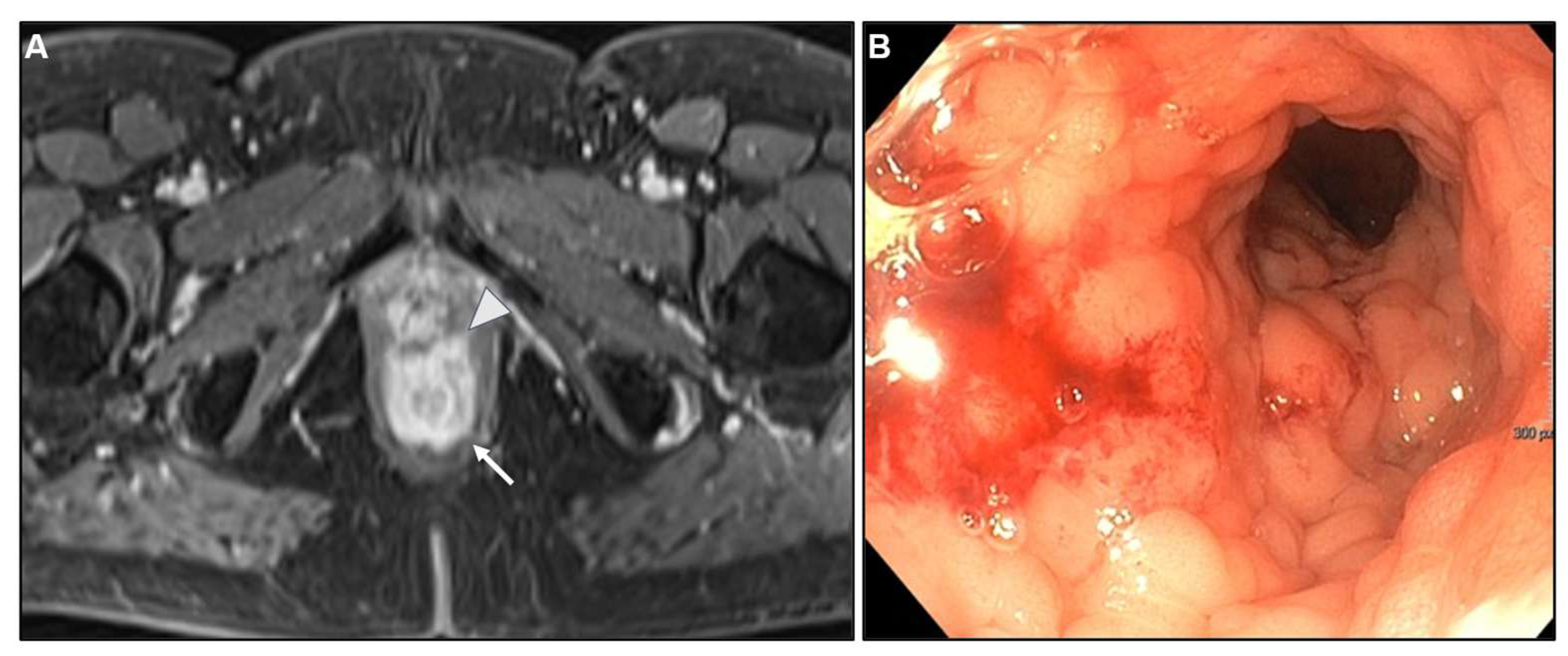
Figure 12.
Extramural tumour component markedly hypointense on T2WI. A) Axial T2WI, B) Axial CE-GRE-T1WI, C) DWI, D) ADC, E) Colonoscopy. Patient with bladder adenocarcinoma treated with surgery and chemotherapy. Note the irregular contour with T2WI markedly hypointense extramural tumour component (arrowhead in A) due to the intense desmoplastic reaction. Observe the concentric ring pattern of the rectum, more conspicuous on DWI (arrow in C-D) and the malignant target sign (arrow in B). E) Extrinsic rectal tumour infiltration was identified during colonoscopy, with luminal occlusion, probably due to metastases from bladder adenocarcinoma. Biopsy results were negative for malignancy. Patient underwent surgery for colostomy. During surgery exploration, peritoneal metastases were found. Patient died shortly afterwards, and diagnosis could not be confirmed.
Figure 12.
Extramural tumour component markedly hypointense on T2WI. A) Axial T2WI, B) Axial CE-GRE-T1WI, C) DWI, D) ADC, E) Colonoscopy. Patient with bladder adenocarcinoma treated with surgery and chemotherapy. Note the irregular contour with T2WI markedly hypointense extramural tumour component (arrowhead in A) due to the intense desmoplastic reaction. Observe the concentric ring pattern of the rectum, more conspicuous on DWI (arrow in C-D) and the malignant target sign (arrow in B). E) Extrinsic rectal tumour infiltration was identified during colonoscopy, with luminal occlusion, probably due to metastases from bladder adenocarcinoma. Biopsy results were negative for malignancy. Patient underwent surgery for colostomy. During surgery exploration, peritoneal metastases were found. Patient died shortly afterwards, and diagnosis could not be confirmed.
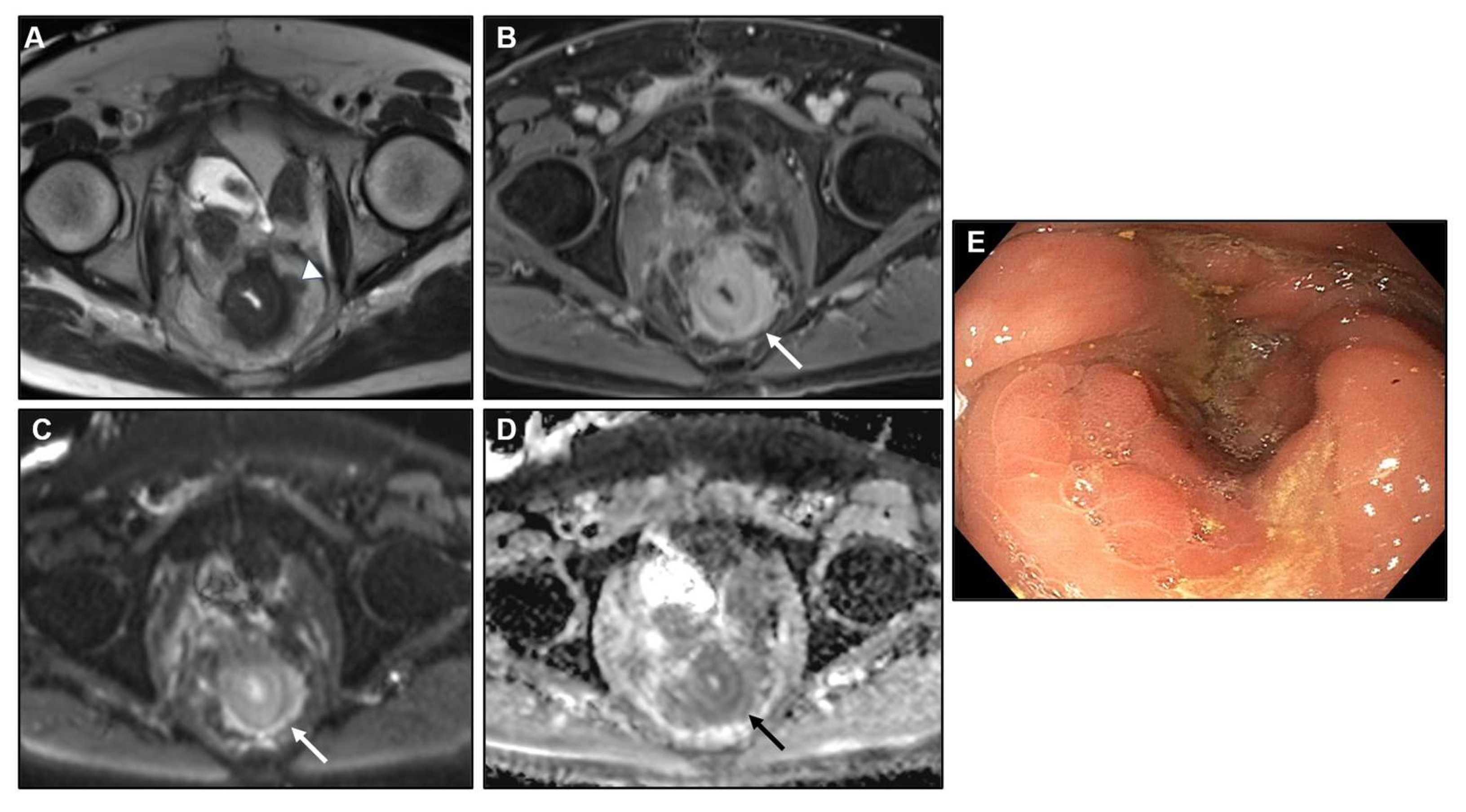
Figure 13.
Bowel obstruction. A) Axial CE-CT, B) MPR CE-CT. Patient with bladder adenocarcinoma with rectal metastasis (arrow in A) presenting as a colonic obstruction (* in B). C) Axial CE-CT. Patient with metastases from ILC to the SB (arrows) and the ascending colon (arrowhead) causing occlusion at multiple sites.
Figure 13.
Bowel obstruction. A) Axial CE-CT, B) MPR CE-CT. Patient with bladder adenocarcinoma with rectal metastasis (arrow in A) presenting as a colonic obstruction (* in B). C) Axial CE-CT. Patient with metastases from ILC to the SB (arrows) and the ascending colon (arrowhead) causing occlusion at multiple sites.
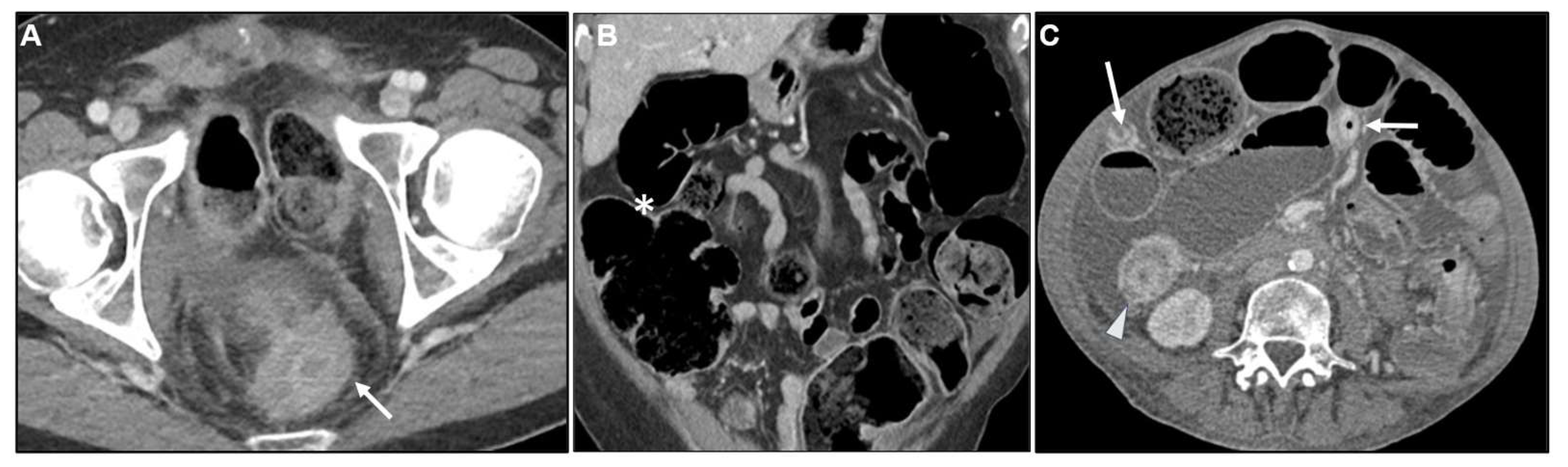
Figure 14.
Bowel obstruction. A) Axial CE-CT, B) Axial T2WI, C) Coronal T2WI, D) Axial CE-GRE-T1WI. Patient with poorly differentiated gastric adenocarcinoma, with a LP appearance (focal form) (arrow in A). Patient achieved complete remission and, two years after the diagnosis, presented with a colon obstruction with a LP-like pattern at the transition point within the distal transverse colon (arrow in B-D). The LP pattern is best depicted on axial images, with concentric thickening of layers and a malignant target sign after contrast injection (arrow in D). The patient underwent surgery, where peritoneal deposits were also found, not depictable on imaging. A metastasis to the transverse colon from gastric adenocarcinoma was confirmed at immunohistochemistry (IHC) following biopsy.
Figure 14.
Bowel obstruction. A) Axial CE-CT, B) Axial T2WI, C) Coronal T2WI, D) Axial CE-GRE-T1WI. Patient with poorly differentiated gastric adenocarcinoma, with a LP appearance (focal form) (arrow in A). Patient achieved complete remission and, two years after the diagnosis, presented with a colon obstruction with a LP-like pattern at the transition point within the distal transverse colon (arrow in B-D). The LP pattern is best depicted on axial images, with concentric thickening of layers and a malignant target sign after contrast injection (arrow in D). The patient underwent surgery, where peritoneal deposits were also found, not depictable on imaging. A metastasis to the transverse colon from gastric adenocarcinoma was confirmed at immunohistochemistry (IHC) following biopsy.
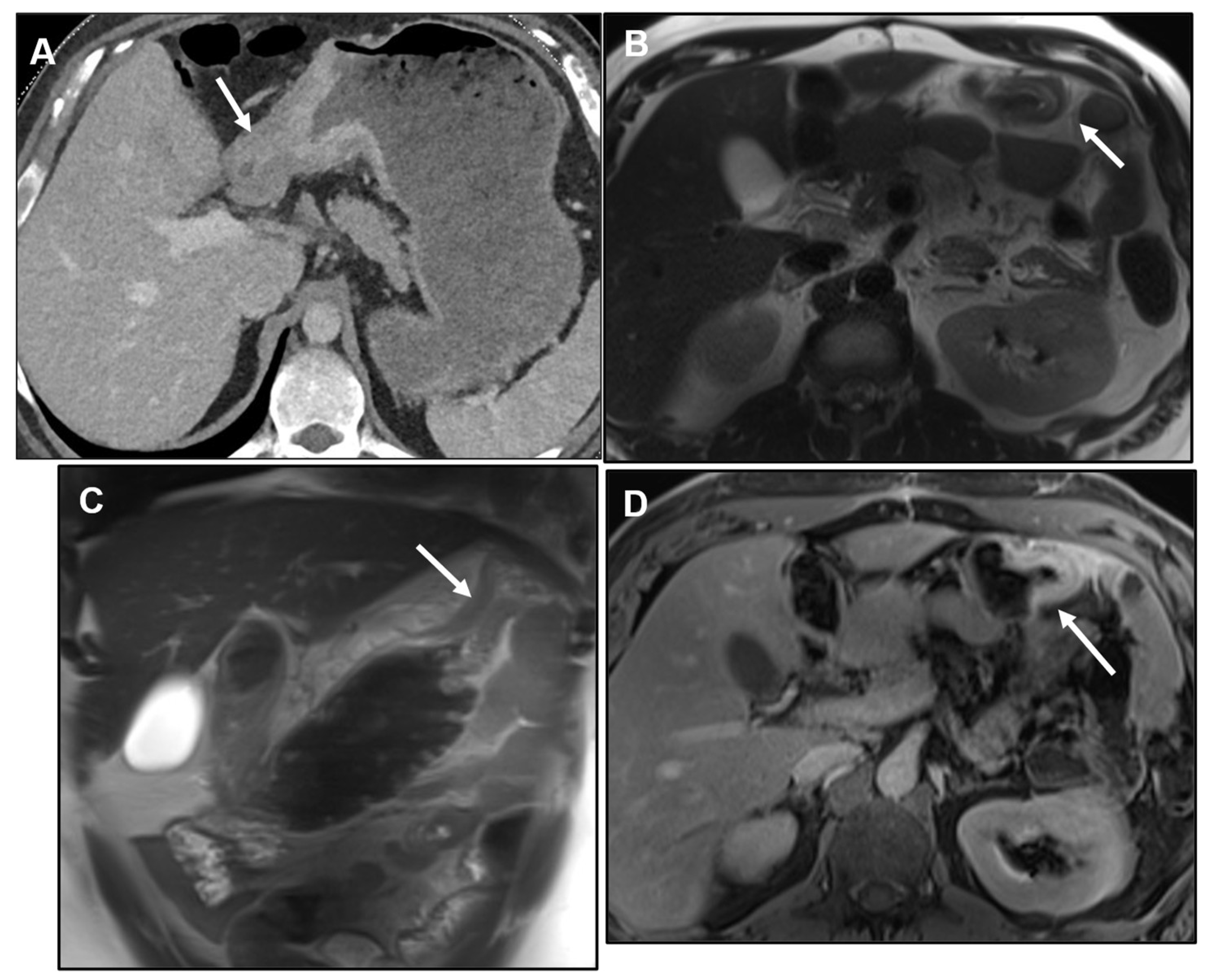
Figure 15.
A) Axial T2WI, B) DWI, C) Axial CE-GRE-T1WI. Female patient with bladder adenocarcinoma, treated with surgery and chemotherapy. On a follow-up MR, a thickened rectum was noted: observe the concentric ring pattern on T2WI (arrow in A) and the malignant ring sign after intravenous contrast administration (arrow in C). Patient was thought to have rectal metastasis from known primary tumour, but IHC concluded that the origin was occult breast adenocarcinoma.
Figure 15.
A) Axial T2WI, B) DWI, C) Axial CE-GRE-T1WI. Female patient with bladder adenocarcinoma, treated with surgery and chemotherapy. On a follow-up MR, a thickened rectum was noted: observe the concentric ring pattern on T2WI (arrow in A) and the malignant ring sign after intravenous contrast administration (arrow in C). Patient was thought to have rectal metastasis from known primary tumour, but IHC concluded that the origin was occult breast adenocarcinoma.
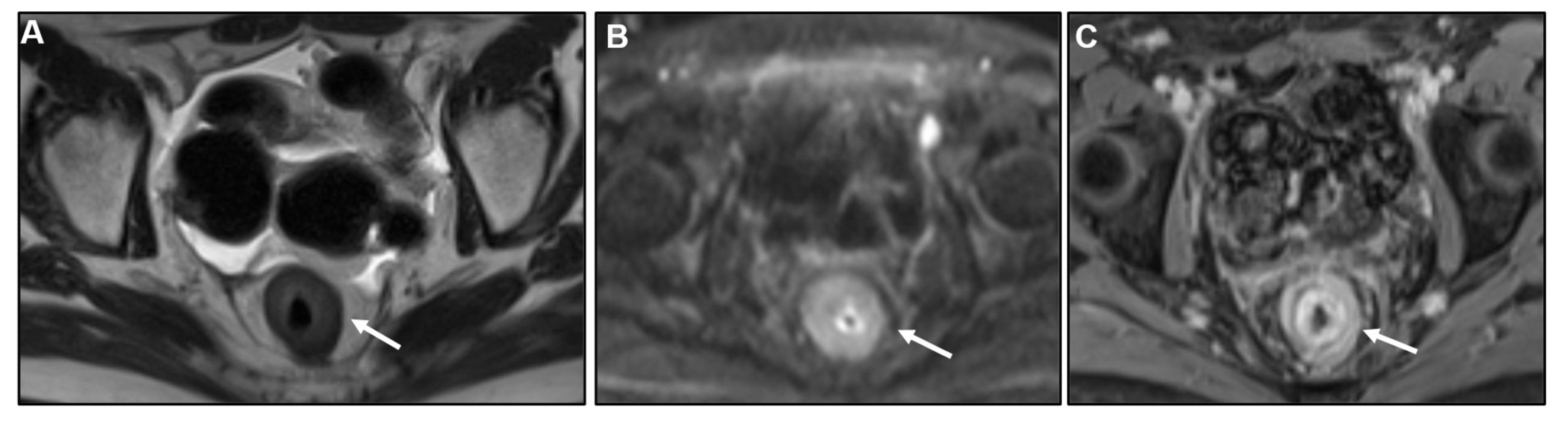
Figure 16.
A) CE-CT coronal MPR, B) DWI, C) Axial T2WI. Patient with ILC undergoing chemotherapy and malaise. Observe the diffusely thickened and shrunken stomach, with a LP pattern and loss of gastric folds. Differential diagnosis included primary adenocarcinoma and metastasis from ILC. IHC following deep biopsy concluded gastric metastasis from ILC.
Figure 16.
A) CE-CT coronal MPR, B) DWI, C) Axial T2WI. Patient with ILC undergoing chemotherapy and malaise. Observe the diffusely thickened and shrunken stomach, with a LP pattern and loss of gastric folds. Differential diagnosis included primary adenocarcinoma and metastasis from ILC. IHC following deep biopsy concluded gastric metastasis from ILC.
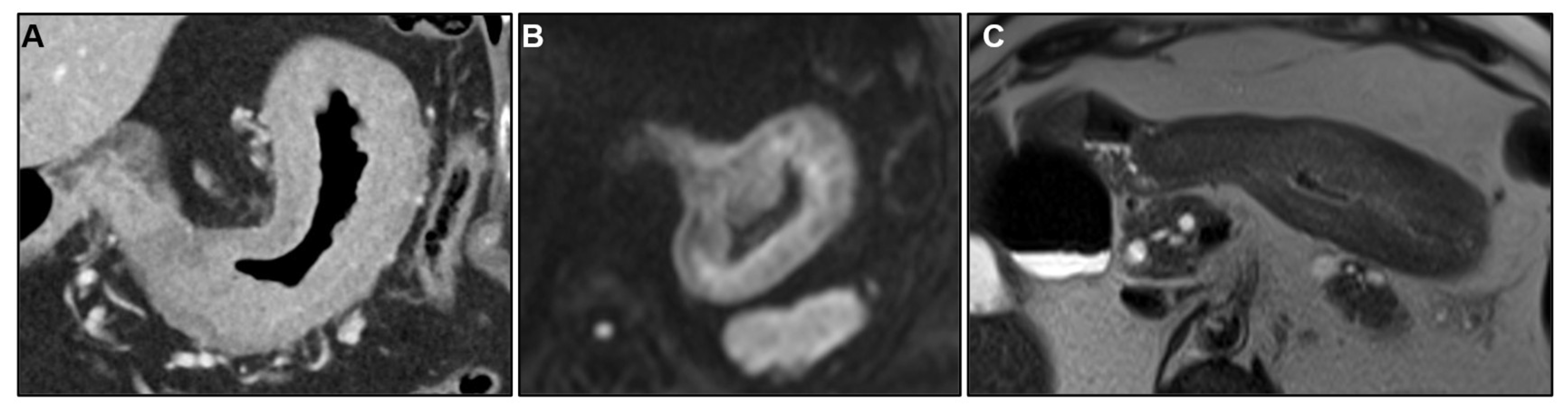
Figure 17.
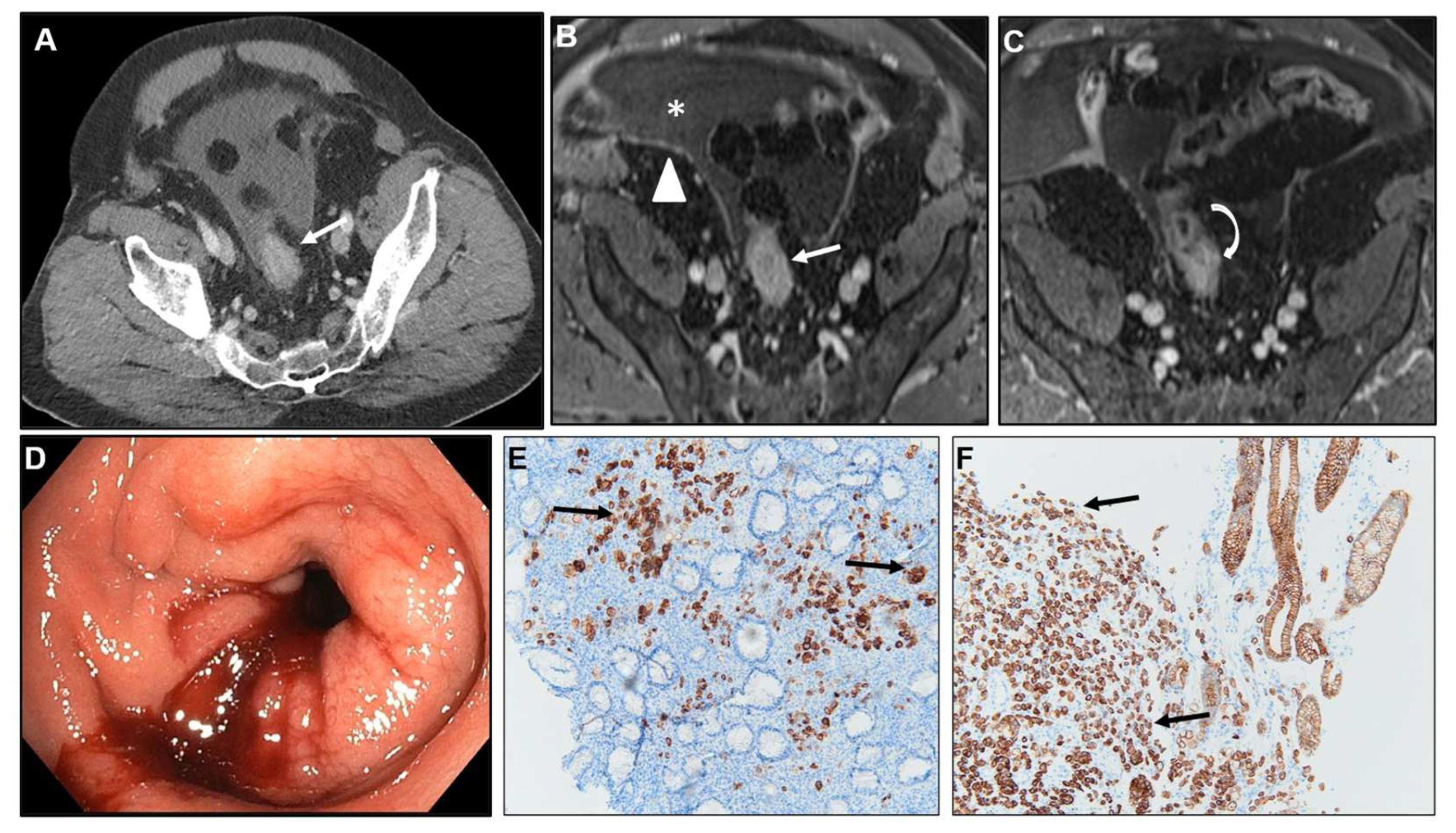
A) Axial CE-CT, B-C) Axial CE-GRE-T1WI, D) Colonoscopy, E) 40X Cytokeratin 7 (CK7) IHC staining tumour cells within the sigmoid lesion, F) 40X CK7 IHC staining tumour cells within the gastric primary tumour. Patient with signet ring cell gastric adenocarcinoma who underwent surgery and subsequently developed PC. Sigmoid lesion with a LP-pattern discovered on a follow-up CT (arrow in A). Notice the malignant target sign (arrow in B), abrupt transition of thickness (curved arrow in C). Ascites (* in B) and deposits within the parietal peritoneum (arrowhead in B). During colonoscopy (D), the mucosa appeared edematous and erythematous, and a stenosis was found at 20cm from the anal verge with no identified lesion. Deep biopsies were performed. IHC confirmed metastasis from gastric adenocarcinoma. Observe atypical cells infiltrating the lamina propria of the rectum (in this case the mucosa was infiltrated), stained by CK7, both within the sigmoid lesion (black arrows in E) and the gastric primary tumour (black arrows in F). CK7 is a keratin, a membranous / cytoplasmic marker with expression in many normal epithelia and epithelial tumours, generally present in upper GI tumours but not colorectal carcinomas. Thus, IHC confirmed the gastric tumour as the origin of the sigmoid metastasis.
Figure 17.
A) Axial CE-CT, B-C) Axial CE-GRE-T1WI, D) Colonoscopy, E) 40X Cytokeratin 7 (CK7) IHC staining tumour cells within the sigmoid lesion, F) 40X CK7 IHC staining tumour cells within the gastric primary tumour. Patient with signet ring cell gastric adenocarcinoma who underwent surgery and subsequently developed PC. Sigmoid lesion with a LP-pattern discovered on a follow-up CT (arrow in A). Notice the malignant target sign (arrow in B), abrupt transition of thickness (curved arrow in C). Ascites (* in B) and deposits within the parietal peritoneum (arrowhead in B). During colonoscopy (D), the mucosa appeared edematous and erythematous, and a stenosis was found at 20cm from the anal verge with no identified lesion. Deep biopsies were performed. IHC confirmed metastasis from gastric adenocarcinoma. Observe atypical cells infiltrating the lamina propria of the rectum (in this case the mucosa was infiltrated), stained by CK7, both within the sigmoid lesion (black arrows in E) and the gastric primary tumour (black arrows in F). CK7 is a keratin, a membranous / cytoplasmic marker with expression in many normal epithelia and epithelial tumours, generally present in upper GI tumours but not colorectal carcinomas. Thus, IHC confirmed the gastric tumour as the origin of the sigmoid metastasis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



