Submitted:
08 July 2025
Posted:
10 July 2025
You are already at the latest version
Abstract
During pregnancy a mother experiences increased metabolic demands to meet the needs of the fetus. A mismatch between these demands and nutrient intake can result in a host of developmental abnormalities to the fetus and health risks to the mother. Several studies have reported strong correlations between deficiency of the essential mineral, magnesium (Mg2+), and many pregnancy complications, including intrauterine growth restriction, preeclampsia, gestational diabetes, and preterm delivery. Mg2+ also impacts fetal programming and disease presentation in childhood and adulthood, showing that aberrant Mg2+ levels in utero have far reaching consequences. Unfortunately, there is no established clinical range of normal serum Mg2+ levels, which makes it challenging to identify mothers and/or fetuses at risk of adverse effects. In this review, we evaluated recently published data to identify a range of serum Mg2+ concentrations that may reflect chronic Mg2+ insufficiency (0.7- 0.85 mmol/L). We then evaluated independent studies that reported on the relationship between Mg2+ levels and pregnancy outcomes to assess whether this cutoff may help identify patients at risk for adverse events and inform therapeutic strategies. Our literature review showed that chronic Mg2+ insufficiency coupled with a molar ratio of calcium (Ca2+) to Mg2+ greater than 3 may indicate increased risk to mother or fetus. Given the high social and economic burdens of pregnancy complications, nutritional supplementation that includes Mg2+ at all stages of pregnancy may be a safe and cost-effective way to mitigate the risk of adverse outcomes for mother and child.
Keywords:
magnesium
; calcium
; pregnancy
; lactation
; fetus
; supplement
; birth defects
1. Introduction
Calcium & Magnesium – Two Major Mineral Nutrients
Calcium (Ca2+) and magnesium (Mg2+) are both essential minerals that play vital roles in many physiologic processes. Mg2+ and Ca2+ work together to support each other’s absorption and utilization. Maintaining a proper ratio (i.e., balance) between these minerals is necessary for each of them to carry out their individual roles, which are discussed below.
Ca2+ is the most abundant mineral in the human body with nearly all (99%) of it contained as insoluble calcium phosphates within the skeleton and teeth. The remainder, which is found as ionized Ca2+ in the circulatory system, intra- and extracellular fluids, and various tissues, is vital to maintaining the skeleton, transmitting nerve impulses, and regulating hormone secretion, vascular tone, cellular signaling, blood clotting, and cardiac and skeletal muscle function [1]. Ca2+ participates in the structural stabilization of biomolecules and membranes and controls the catalytic activity of hundreds of enzymes [2,3]. With respect to pregnancy and lactation, Ca2+ triggers new life at fertilization, controls several developmental processes, and may also regulate diverse cellular processes during differentiation including metabolism, proliferation, secretion, contraction, synaptic transmission, learning and memory [4].
Mg2+ is the fourth most abundant mineral in the human body, behind Ca2+, sodium (Na), and potassium (K), and the second most abundant intracellular cation following K [5,6,7,8]. Like Ca2+, most of the body’s Mg2+ is found in the skeleton (50-60%) with the remainder contained in the muscles and tissues (40-50%). Less than 1% is found in the circulatory system, with the largest fraction of this 1% contained in erythrocytes. Mg2+ plays crucial roles in diverse physiological processes [5,6,7,8]. It is critical to the stability of all polyphosphate compounds and their roles in many enzymatic reactions. These reactions facilitate the hydrolysis of phosphate esters (ATPases), and the transfer of phosphoryl groups (kinases and phosphatases) in virtually every metabolic pathway [7]. Mg2+ serves as a cofactor in over 600 enzyme systems that govern a variety of physiological activities, including glucose metabolism, protein synthesis, muscle and nerve transmission, neuromuscular conduction, blood glucose management, and blood pressure regulation [5,6,7,8]. It also plays an important role in signal transduction, most likely as a second messenger [11], and is required for the active transport of Ca2+ and K ions across cell membranes, making it essential for proper immune responses, antioxidant synthesis, vitamin D synthesis and activation, nerve impulse transmission, muscular contraction, vasomotor tone, and proper heart rhythm [7,9,10].
In this review we evaluated how maternal levels of Ca2+ and Mg2+ during pregnancy affect health outcomes of the fetus. We focused on these two minerals because they are critical for proper fetal growth and development, and disruptions to their maternal levels are strongly associated with poor outcomes. The goal of this literature analysis was to determine if a cutoff concentration of Mg2+, which may reflect chronic latent Mg2+ deficiency, could potentially inform on adverse health risks to mother and/or baby early in pregnancy (first and second trimester). Conditions that occur late in pregnancy (third trimester) have been widely reported on and therefore were not the focus of this review.
2. Materials and Methods
The PRISMA-S search protocol was used to search scientific and clinical databases, as well as private collections, to identify and analyze almost 2,000 publications [108]. Searches included terms such as “pregnancy,” “lactation,” “calcium,” “magnesium,” “fetus,” “maternal,” “serum,” and related search terms. Results were published on or before May 1, 2025. We screened over 1,500 results and selected 107 core articles after removing duplicates, as well as secondary, non-English, and irrelevant studies.
3. Results
Reported levels of serum Ca2+ and Mg2+ during pregnancy and lactation
Pregnancy and lactation are times of high Ca2+ and Mg2+ demand [12,13]. Approximately 25-30 g of Ca2+ and 0.8 to 1 g of Mg2+ are transferred from mother to the fetal skeleton by the end of a normal pregnancy. Typically, the fetus accumulates 2-3 mg Ca2+/day during the first trimester [12]. During the second and third trimesters the rate of accumulation increases to 250 mg Ca2+/day and over 300 mg Ca2+/day, respectively.
Less is known about the rates of Mg2+ accumulation by the fetus. Historical data suggest that about 80% of fetal mineral content is accumulated during the third trimester, as Ziegler’s 1976 study reported that the rate of Mg2+ transfer increases from 1.8 mg/day to 5-7.5 mg/day over the last five weeks of pregnancy [13]. However, more recent clinical data from Larsson et al. clearly show that maternal Mg2+ transfer to the placenta and fetus takes place in parallel with Ca2+ transfer and begins early in the first trimester (Table 1) [14]. It is our stance that Larson’s tabulated data is particularly important because they were gathered from a defined population in a single laboratory over time, and thus less susceptible to the variability introduced by inter-laboratory analyses of diverse populations [15]. The question then, of whether these data could be applicable to the population at large, can be answered by other reports by Cai et al. (China) and Hansu and Cikim (Turkey), which suggest the trends summarized in Table 1 are pregnancy in women around the world [16,17].
Some have asserted that the changes in Mg2+ levels reported by Larsson et.al. reflect its dilution caused by increases in plasma volume during pregnancy. This idea is not supported by data published by De Jorge et al., which shows Mg2+ concentrations show a similar pattern of changes throughout pregnancy (Table 2) [19].
In another study, Rigo et al. confirm that Larsson’s findings on the mineral levels in the mother also inform Mg2+ levels in the fetus [20]. Here, a systematic literature review and meta-analysis of serum Mg2+ levels in newborns was conducted with the goal of quantifying normal and tolerable concentration ranges during the neonatal period. In this review they also highlighted factors that influence Mg2+ levels and how maternal Mg2+ levels during pregnancy relate to serum Mg2+ in the neonate at birth. Their literature review showed that mothers who did not receive dietary Mg2+ supplementation during pregnancy gave birth to neonates with Mg2+ levels (0.76 (95% CI: 0.52, 0.99) mmol/L) similar to those of their mother during pregnancy (0.74 (95% CI: 0.43, 1.04) mmol/L). However, neonate levels increased during the first week of life (0.91 (95% CI: 0.55, 1.26) mmol/L) before returning to their baseline levels (0.74 (95% CI: 0.43, 1.04) mmoL/L). This pattern was also seen in mothers who received dietary Mg2+ supplementation during pregnancy. In this group the average neonatal serum Mg2+ concentration was higher at 1.29 mmol/L (95% CI: 0.50, 2.08), which rose to 1.44 mmol/L (95% CI: 0.61, 2.27) during the first week of life. It should be noted that despite the low average Mg2+ levels in mothers who did not receive dietary supplements, some individuals in this group gave birth to newborns with Mg2+ levels as high as 2.0 mmol/L. Serum Mg2+ levels > 2.5 mmol/L have been linked to an increased risk of mortality, admission into intensive care, hypotonia, hypotension, and respiratory depression [21,22,23]. However, in Rigo’s study, serum Mg2+ levels of 2.0 mmol/L were shown to be well tolerated by neonates.
Maternal transfer of minerals continues during lactation [24]. Breastmilk contains higher levels of Ca2+ and Mg2+ at the start of lactation, which start to decline after approximately 6 months (Table 3) [25,26,27]. Assuming a daily neonatal intake of about 800 mL of breast milk, this fluid provides 225-240 mg Ca2+/day early in lactation and 200-210 mg Ca2+/day later in lactation to support continuing neonatal growth and development. Likewise, Mg2+ content in this volume of breast milk is 27 mg/day early in lactation and decreases to 18 mg/day later in lactation.
The data generated by Gates et. al. (Table 3) also reveal insight into how mineral deficiencies in mothers of preterm infants are reflected in the quality of their breastmilk [27]. Their preterm children had an average gestational age of 28.2 ± 2.8 weeks and average birth weight of 1,098 g (vs. normal term birth weight of about 3,200 g). The volumes of breast milk each day increased from an average of 171.8 mL (day 7) to 224.2 mL (day 21) and then decreased slightly to 210.3 mL. In addition to the shortfall in milk supply by these mothers as compared to mothers who carry to term, the Ca2+ content in their breastmilk was initially low and decreased during lactation. In contrast, both the Mg2+ and phosphorus content of their breastmilk paralleled the contents of breastmilk provided by mothers of full term babies.
Another Perspective: The Molar Ratio of Serum Ca2+ to Serum Mg2+ and Impacts on Fetal and Maternal Outcomes
Larsson’s data on Ca2+ and Mg2+ levels from pregnancy to postpartum (Table 1) may also be considered from another perspective: the molar ratio of serum Ca2+ to serum Mg2+ (Table 4).
Both clinical guidelines and published data show that the risk of adverse effects on mother and/or fetus is minimal when both serum Ca2+ and serum Mg2+ are high in the reference ranges (Table 4, HiCa:HiMg column).2 In contrast, these same documents raise minor concerns when serum Ca2+ is low in the reference ranges. For example, Tsakiridis et al. reviewed the most recently published guidelines for antenatal nutrition issued by five international regulatory or medical authorities [28]. They found that most of these authorities recommended Ca2+ supplementation in populations with low dietary Ca2+ intake. Clinical data suggested that supplementation benefitted women at risk for preeclampsia and reduced the risk of gestational hypertension, neonatal mortality, and preterm birth in women with low dietary Ca2+ intake. The data were sufficient to prompt the recommendation that Ca2+ consumption be highly encouraged during pregnancy, especially during the second and third trimester.
Likewise, Adams et al. summarized evidence for the benefits associated with supplementation of Ca2+ and Mg2+ [29]. They identified clear associations between low serum Ca2+ and risk of preeclampsia, eclampsia, and pregnancy-induced hypertension, supporting the benefits of supplementation. Less definitive correlations between the effects of supplementation and preterm birth or maternal mortality were identified. Maternal Ca2+ supplementation was also related to reductions in neonatal hypertension, low birth weight, and neonatal intensive care unit admission. The authors concluded that Ca2+ supplementation of 550 mg of elemental Ca2+ daily should be recommended for U.S. women, with a need for higher levels of supplementation if the woman had a low intake of milk, vegetables, or milk-based foods or was at high risk of preeclampsia, preterm birth, and/or gestational hypertension. It was speculated that supplementation could help reduce the risk of other conditions associated with low Ca2+ intake including preterm birth, low birth weight, neonatal mortality, and Autism Spectrum Disorder.
Despite the value of Ca2+ in maintaining skeletal integrity [30,31], neither Adams nor other recent reviewers identified a relationship between low serum Ca2+ and maternal bone health. For example, Tihtonen et al. screened 3,555 records in 11 databases and analyzed data from seven randomized controlled trials (RCTs) including 1,566 pregnant women [32]. No advantage of Ca2+ supplementation was found on maternal bone mineral density after delivery or during breast-feeding, even when dietary Ca2+ intake was low. Further, the conclusion was not modified even when the dose of Ca2+ or concomitant vitamin D administration was considered. Similarly, Cai et al. screened supplementation reports in multiple databases and analyzed five randomized controlled trials including 567 lactating women [33]. Their meta-analysis indicated that Ca2+ supplementation does not provide clinically important benefits for bone mineral density in lactating women. However, both groups of investigators noted confounding elements, in that there was adequate dietary intake before supplementation in some studies, and others did not measure baseline Ca2+ intake. These findings suggested that advising lactating women to meet the current recommended Ca2+ intakes (with supplementation if dietary intake is low) is warranted unless new high-certainty evidence to the contrary from robust clinical trials becomes available.
Conversely, when the serum Mg2+ concentration is low (Table 4, LoCa:LoMg and HiCa:LoMg columns), the published literature is rife with adverse consequences.
Adverse Effects Associated with Maternal Chronic Mg2+ Insufficiency Early in Pregnancy
Instead of describing reduced Mg2+ as a “deficiency,” we will use the term “chronic insufficiency” to define a metabolic state where the serum mineral concentration is in the lowest quartile of its normal range (Table 1) for a period of at least 3 months. Recent reports suggest that chronic Mg2+ insufficiency enhances the risks of adverse events for mother and child (Table 5). We will focus our attention on examples of adverse events that occur early in pregnancy (Table 6), because adverse effects that occur late in pregnancy are widely recognized.
4. Interim Summary & Action Steps
Pregnancy and lactation are stressful periods of increased metabolic demands associated with changes in the mother’s physiology and social environment and developmental requirements of the child. Clinicians recognize that many women fail to consume adequate vitamins and minerals necessary to support a healthy pregnancy. When this is the case, supplementation of key vitamins and minerals may be required. Optimizing endometrial wellbeing may also help to prevent common pregnancy complications, including adverse effects on both early and late fetal development, as well as compromised mineral and complex oligosaccharide levels in breast milk.
For a mineral such as iron, the U.S. Food and Drug Administration has provided specific recommendations for provision with folate. In contrast, no specific recommendations for prenatal Ca2+ or Mg2+ supplementation have been established. This is a significant shortcoming, since inadequate stores or intake of these two essential mineral nutrients can have adverse effects on the mother, such as hypertension, complications of labor, and extended disability and recovery time after delivery. Furthermore, the fetus can be affected, resulting in abnormal organ and tissue development, intrauterine growth retardation, congenital malformations, reduced immunocompetence, preterm delivery, and lifelong, increased risk of metabolic disturbances such as type 2 diabetes, metabolic syndrome/obesity, hypertension, and chronic kidney disease.
5. What Constitutes the Reference Range for These Minerals?
Serum Ca2+ is routinely monitored, and the reference range for Ca2+ (2.2-2.7 mmol/L) is relatively consistent around the world [1]. Consequently, Ca2+ levels are readily available to clinicians, providing guidance in patient care. In contrast, Mg2+ is often viewed as a micromineral that has little significance until serious adverse events (e.g., preeclampsia, eclampsia, high risk of premature birth) prompt administration of tocolytics such as intravenous magnesium sulfate. Also, the interpretation of serum Mg2+ levels presents a number of practical problems. First, serum Mg2+ may not be routinely monitored, although clinical instruments for such monitoring are readily available [56]. Interlaboratory variability further complicates interpretation of existing data [57,58]. Equally problematic is the observation that there is little consensus on reference values and the units in which they are reported. Serum Mg2+ values are reported in mg/dL, mmol/L, or mEq/L. In addition, serum Mg2+ values may be determined as total Mg2+ or ionized Mg2+. As a result of these differences, no standardized reference range for serum Mg2+ has been established, which has led to a wide variety of reference ranges being reported (Table 7).
Serum Mg2+ concentration shows little variation as a consequence of tight physiological regulation, and clinicians have concluded that its serum concentration may not provide the most informative picture of Mg2+ status in an individual [73,74]. Nonetheless, if chronically low serum Mg2+ is a concern, defining ranges of serum Mg2+ concentrations that will support the health of both normal subjects and patients remains a challenge that merits attention [75,76]. Indeed, the German Society for Magnesium Research e.V. recently proposed a value of 0.85 mmol/L to define the lower limit of serum Mg2+ concentration associated with lower risks to good health [77,78].
Are the dietary requirements for calcium and magnesium adequately met?
The recommended daily Ca2+ intake in the general adult population ranges between 500 and 1,300 mg daily [1,79]. Surprisingly, the Recommended Daily Allowances (RDAs) for pregnant and lactating women (1,000-1,300 mg Ca daily) fall within the same range. Maternal sources of both Ca2+ and Mg2+ include increased uptake from the diet, increased renal uptake and recirculation, and bone resorption. In fact, bone resorption is so extensive that the loss of Ca2+ during pregnancy and 6 months of lactation is equivalent to 4-5% of the mother’s total skeletal calcium content (about 1,200 g Ca2+) [1]. (Bone loss is expected to be more extensive if a mother bears twins or triplets.)
As Weaver, Heaney and others have noted, most of the Ca2+ in the American diet comes from dairy products [80]. (N.B. Dairy products do not include oat, soy or other plant-derived “milk.”) Changes in the Western diet indicate that diet alone may not be sufficient to meet maternal needs for Ca2+ during pregnancy and lactation. As a result, in 2020, the World Health Organization issued an updated guideline for Ca2+ supplementation before and during pregnancy [81]. The committee concluded that low-certainty evidence suggests that starting Ca2+ supplementation before and/or early in pregnancy (compared to placebo or no treatment) may include the possibility of a risk reduction for preeclampsia and eclampsia, particularly for those women with greater than 80% compliance with calcium supplementation. They also noted “that the acceptability of Ca2+ supplementation by women may vary – while women may value nutritional interventions that can lead to a healthy baby and a positive pregnancy experience, Ca2+ tablets can be large, have a powdery texture and be unpalatable to consume. Feasibility may also be limited in settings where Ca2+ is not always available due to logistical or staff constraints or cost. In addition, limited access to pre-conception healthcare services may be a barrier to the provision of Ca2+ supplements prior to pregnancy.”
The recommended daily Mg2+ intake in the general adult population ranges between 310 and 420 mg, whereas pregnant women have a recommended daily Mg2+ intake of 350–400 mg [82]. Maternal sources of Mg2+ include uptake from the diet, renal uptake and recirculation, and bone resorption. In addition, some evidence suggests altered tissue distribution and an increased renal output of Mg2+ during pregnancy [83]. Unlike Ca2+, Mg2+ uptake is not significantly affected by vitamin D. Dietary surveys confirm that dietary Mg2+ remains below recommended levels in Europe and the United States. According to several recent reports, these diets include between 30% and 50% less Mg2+ than the daily recommended dosage [84,85]. Many authorities state, however, “magnesium deficiency is extremely rare [87].”
Likewise, both the Australian Government Department of Health and World Health Organization guidelines state that there is insufficient evidence to conclude whether dietary Mg2+ supplementation during pregnancy is beneficial, even for leg cramps [28]. Other government authorities are silent about Mg2+. Adams et al. and other investigators provide weak recommendations for Mg2+ supplementation [29]. “Overall, because U.S. women have average magnesium intake that is 22% less than the RDA, and because levels decrease during pregnancy, we recommend supplementing with 350 mg because 345 mg was found be sufficient to keep magnesium levels stable, and supplementation studies with doses of 345–500 mg were found to be beneficial. This recommendation appears likely to reduce the rate of pregnancy-induced hypertension, maternal hospitalization, preterm birth, low birth weight, and low Apgar scores, and could possibly help with other conditions as well [29].”
Defining an Action Range for Mg2+
By considering all this information together with recent reports by Čabarkapa et al., Liebscher and Liebscher, Escobedo-Monge et al., and Rosanoff et al., an action range for Mg2+ (i.e., a concentration range that may prompt clinical intervention) can be reasonably defined as 0.7 to 0.85 mmol serum mg/L [87,88,89]. Čabarkapa’s prospective study, which included 403 pregnant women > 18 years old, with singleton pregnancies, provides particularly relevant data [87]. Between 11- and 14-weeks’ gestation, a single blood sample was collected from every study participant and concentrations of urea, creatinine, uric acid, Mg2+, free beta subunit of human chorionic gonadotrophin, plasma protein A related to pregnancy, and C-reactive protein were measured. All subjects were followed through the rest of pregnancy. 61 of the study participants developed pre-eclampsia and were retrospectively compared to a group of 342 participants who experienced uncomplicated pregnancies and normal outcomes. Serum Mg2+ levels were significantly lower in PEKT mothers compared to the TNT group (0.69 ± 0.18 vs. 0.85 ± 0.08 mmol/L; p < 0.001). The level of serum Mg2+ had the strongest significant positive correlation (p < 0.05) with the week of gestational outcomes (R = 0.442), weight (R = 0.416), and Apgar score (R = 0.343) of the newborns, and the strongest significant negative correlation with the number of miscarriages (R = −0.413), serum creatinine levels (R = −0.471), and the number of pregnancies (R = −0.326). The week of gestational outcome was predicted with the greatest reliability by the serum Mg2+. A serum Mg2+ level ≤ 0.81 mmol/L in the first trimester predicted preeclampsia with a sensitivity of 77.0% and specificity of 71.6%. When serum creatinine levels were considered in conjunction with serum Mg2+, it was found that creatinine levels > 53 µmol/L detected preeclampsia with a sensitivity of 93% (preeclampsia 62.3 µmol/L vs. normal 49.2 µmol/L; p < 0.001). Thus, in late first trimester, Ca2+, Mg2+ and creatinine levels appear to be biomarkers associated with risk of preeclampsia later in pregnancy.3
6. Potential for Reducing Risks
If our working hypothesis has validity, high Ca2+: Mg2+ molar ratios (i.e., values in the range > 3, see Table 4) and serum Mg2+ concentration in the lowest quartile of the reference range (0.7 - 0.85 mmol/L) may present increased risk for complications during pregnancy and lactation (Figure 1). “Moving the needle” by increasing maternal serum Mg2+ concentration to ≥ 0.85 mmol/L is a potential action step. How can this be accomplished? Actions such as the following may reduce the risks associated with chronic Mg2+ insufficiency.
Diet and education
As a first action step, let us echo the words of Murphy et al. [90]. “Adequate consumption of nutrients that support infant neurodevelopment is critical among pregnant women and women of childbearing age.” Their review of the potential effects of socioeconomic inequalities on nutrient gaps in these life stages is particularly informative. They analyzed data from 2007–2018 NHANES related to usual intake (foods and dietary supplements) of neurodevelopment-related nutrients among women of childbearing age and pregnant women (20–44 years). Usual intake was compared across household food security, poverty-to-income ratio (PIR), and household participation in federal food and nutrition assistance programs. Women in households that participated in the Supplemental Nutrition Assistance Program had a significantly lower intake of multiple nutrients relative to those who did not participate. For example, 50% had intakes below the estimated average requirement (EAR) for vitamin A (versus 32%), 42% were below the EAR for calcium (versus 33%) and 65% were below the EAR for magnesium (versus 42%). Similar gradients were observed by PIR and household food security, and among pregnant women wherein gaps were more evident in those experiencing socioeconomic inequalities. The use of dietary supplements attenuated shortfalls for most nutrients. These findings highlight a critical need to support the nutritional requirements for women of childbearing age and pregnant women.
As Henriksen and others have pointed out, a mixed diet including whole grain cereals, milk and dairy products, vegetables, starchy roots, berries, meat and fish constitutes the best sources of Mg2+ [80,91]. Magnesium concentrations are especially high in dark chocolate, and nuts. “Hard” water contains more Mg2+ than “soft” water and drinking either “hard” or mineral water can contribute 10–20 mg/day to the total Mg2+ intake.
Supplementation
Numerous clinical trials have tested whether the risk the pregnancy complications mentioned herein can be mitigated by supplementing the diet with Mg2+ alone or with a combination of Mg2+ and Ca2+. Unfortunately, the results are conflicting and have often been judged to be of low evidentiary value [92,93,94,95,96,97,98,99]. When statistical analyses fail to establish causal relationships, authors may conclude that serum mineral levels were “adequate” [99].
On the other hand, since Mg2+ is involved in roughly 80% of physiological processes, establishing causal relationships between serum Mg2+ and risks associated with chronic Mg2+ insufficiency through statistical analyses of data from large clinical trials may be an unrealistic expectation. For example, well-designed trials typically include large cohorts of women having a wide range of serum Mg2+ levels. Mechanistically, those with sufficient Mg2+ will not benefit from supplementation, since absorption will be limited naturally; their lack of responsiveness will skew subsequent statistical analyses unless the data are stratified. Some of the trial designs include supplementation that is started during pregnancy and is of short duration. This may be “too little and too late,” since some studies suggest twelve weeks or more of supplementation may be needed to restore intracellular Mg2+. Moreover, Larsson’s data (Table 1) show that Mg2+ is utilized from start to finish of pregnancy [14]. Finally, the course of supplementation may be inadequate.
This last comment is illustrated by comparison of the outcomes of two randomized clinical trials in which nominal supplemental doses of 300 mg of magnesium citrate were administered daily to pregnant women at risk for adverse events [100,101]. The BRAMAG study was carried out at three centers in Brazil [100]. Over 800 women were enrolled, each with a singleton pregnancy and at least one risk factor for adverse events. The 407 women in the treatment group received a tablet containing 300 mg of magnesium citrate daily from the 12th to the 20th week of gestation.4 Preeclampsia or eclampsia, severe hypertension, placental abruption, and stroke or death were monitored in the mothers. Preterm birth, stillbirth, neonatal death or NICU admission after birth, and small for gestational age birthweights were monitored in the offspring. Data from the 407 study participants who received magnesium citrate compared to data from 422 participants who were given placebo. 75 neonates (18.4%) in the magnesium supplement arm and 76 neonates (18.0%) in the placebo arm developed at least one of the adverse effects listed above – an adjusted odds ratio (aOR) of 1.10 (95% CI 0.72–1.68). The most common outcome among neonates was preterm birth (9.3%). 49 (12.0%) women in the magnesium arm and 41 women (9.7%) in the placebo arm developed at least one of the pregnancy complications listed above – an aOR of 1.29 (95% CI 0.83–2.00). The most common complication was pre-eclampsia prior to 37 weeks’ gestation (9.3%) and severe gestational hypertension prior to 37 weeks’ gestation (4.9%). Of note, the risk of placental abruption was lower in the magnesium group (9 events [2.2%]) compared to the placebo arm (21 events [5.0%]), equivalent to an adjusted OR of 0.43 (95% CI 0.20 to 0.95). The authors concluded, “Oral magnesium citrate supplementation did not appear to reduce adverse perinatal or maternal outcomes in high-risk singleton pregnancies.”
Conversely, in a separate study that was carried out in Turkey, the effects of Mg2+ supplementation in women with serum Mg2+ concentrations in the lowest quartile of the normal range were evaluated [101]. The study included 120 pregnant women at 12-14 weeks’ gestation. Participants had an average age of 29 years and normal weight. Most study participants had a history of gestational diabetes mellitus, preeclampsia, preterm birth, and stillbirth. Participants with Mg2+ serum levels higher than 1.9 mg/dl were considered a control group (Group A, n = 60). Participants with Mg2+ levels lower than this were considered to have hypomagnesemia and were divided into Groups B and C (n = 60 for both). Each participant received a daily multimineral tablet containing 100 mg Mg2+ until delivery. Group A had an average serum Mg2+ level of 0.86 mmol/L. Groups B and C had an average serum Mg2+ level of 0.71 mmol/L. Group C received an additional tablet daily for one month during pregnancy that contained 200 mg Mg2+ as magnesium citrate in an effervescent formulation. The data showed that supplemental Mg2+ significantly reduced maternal preeclampsia (P = 0.018), preterm birth (P = 0.044), gestational diabetes (P = 0.003), and leg cramps (P < 0.001) for the mother, as well as a reduced risk of intrauterine growth restriction (IUGR) (P < 0.001), low birth weight (P = 0.002), and Apgar score under 7 (P = 0.006) for the child. The investigators concluded, “Mg2+ supplement during pregnancy likely decreases the probability of occurrence of many complications of pregnancy.”
7. Discussion
In summary, available data affirm the importance of maintaining adequate maternal mineral nutrition before and during pregnancy and during lactation. Adequate Ca2+ and Mg2+ may be particularly important to both mother and child, given the broad spectrum of physiological roles of these two key minerals.
Taken together, a growing body of data suggests that maternal counseling about risks associated with serum Mg2+ of 0.70 to 0.85 mmol/L and serum Ca2+ in the reference range should be considered prior to and early in pregnancy. Straightforward actions such as counseling to improve a mother’s diet, adding necessary supplements both before, during and after pregnancy, have proven valuable and cost-effective in the past and will continue to do so [102,103,104].
Although these actionable insights could potentially mitigate a wide variety of birth defects and complications, we acknowledge this review’s limitations. Randomized controlled trial outcomes reported heterogeneous findings, which highlight the need for additional high-quality prospective studies aimed at evaluating the clinical outcomes of chronic Ca2+ and Mg2+ insufficiency, defining the optimal serum Mg2+ levels, and testing supplementation strategies.
Based on the information available in the scientific literature, we conclude that nutritional supplementation at all stages of pregnancy may be a safe and cost-effective way to reduce the risk of pregnancy complications and adverse outcomes for mother and child [105,106,107]. Future large-scale studies, including randomized trials, will be required to confirm this working hypothesis.
References
- National Institutes of Health. Calcium Fact Sheet for Health Professionals. https://ods.od.nih.gov/factsheets/Calcium-HealthProfessional/. Accessed 8 August 2024.
- Weaver CM, Heaney RP, Eds. Calcium in Human Health. Humana Press, Totowa, NJ. 2006.
- Elíes, J.; Yáñez, M.; Pereira, T.M.C.; Gil-Longo, J.; MacDougall, D.A.; Campos-Toimil, M. An Update to Calcium Binding Proteins. Adv Exp Med Biol. 2020, 1131, 183–213. [Google Scholar] [CrossRef] [PubMed]
- Kalkwarf, HJ. Calcium in pregnancy and lactation. Chapter 18, pp. 297-309 in: Calcium in Human Health, Weaver CM, Heaney RP, Eds. Humana Press, Totowa, NJ, 2006.
- Touyz, R.M.; de Baaij, J.H.; Hoenderop, J.G.; Ingelfinger, J.R. Magnesium Disorders. New Engl. J. Med. 2024, 390, 1998–2009. [Google Scholar] [CrossRef] [PubMed]
- Kothari, M.; Wanjari, A.; Shaikh, S.M.; Tantia, P.; Waghmare, B.V.; Parepalli, A.; Hamdulay, K.F.; Nelakuditi, M. A Comprehensive Review on Understanding Magnesium Disorders: Pathophysiology, Clinical Manifestations, and Management Strategies. Cureus 2024, 16, e68385. [Google Scholar] [CrossRef] [PubMed]
- Kröse, J.L.; de Baaij, J.H.F. Magnesium biology. Nephrol. Dial. Transplant. 2024, 39, 1965–1975. [Google Scholar] [CrossRef]
- Mathew, A.A.; Panonnummal, R. ‘Magnesium’-the master cation-as a drug—possibilities and evidences. BioMetals 2021, 34, 955–986. [Google Scholar] [CrossRef]
- Snoke JE, Yanari S, Bloch K. Synthesis of glutathione from gamma-glutamylcysteine. J Biol Chem. 1953, 201, 573–586. [CrossRef] [PubMed]
- Yanari, S.; Snoke, J.E.; Bloch, K. Energy sources in glutathione synthesis. J. Biol. Chem. 1953, 201, 561–571. [Google Scholar] [CrossRef]
- Stangherlin, A.; O’nEill, J.S. Signal Transduction: Magnesium Manifests as a Second Messenger. Curr. Biol. 2018, 28, R1403–R1405. [Google Scholar] [CrossRef]
- Kovacs, C.S. Maternal Mineral and Bone Metabolism During Pregnancy, Lactation, and Post-Weaning Recovery. Physiol. Rev. 2016, 96, 449–547. [Google Scholar] [CrossRef]
- Ziegler, E.; Odonnell, A.; Nelson, S.; Fomon, S. Body-composition of reference fetus. Growth 1976, 40, 329–341. [Google Scholar]
- Larsson, A.; Palm, M.; Hansson, L.; Axelsson, O. Reference values for clinical chemistry tests during normal pregnancy. BJOG: Int. J. Obstet. Gynaecol. 2008, 115, 874–881. [Google Scholar] [CrossRef]
- Yan, Y.; Pu, Y.; Zeng, J.; Zhang, T.; Zhou, W.; Zhang, J.; Wang, J.; Zhang, C.; Chen, W.; Zhang, C. Evaluation of serum electrolytes measurement through the 6-year trueness verification program in China. Clin Chem Lab Med. 2020, 59, 107–116. [Google Scholar] [CrossRef]
- Cao, X.; Wu, M.; Zhang, G.; Lin, L.; Tu, M.; Xiao, D.; Zhong, C.; Zhang, H.; Yang, S.; Liu, J.; et al. Longitudinal plasma magnesium status during pregnancy and the risk of gestational diabetes mellitus: a prospective cohort study. Environ. Sci. Pollut. Res. 2023, 30, 65392–65400. [Google Scholar] [CrossRef]
- Hansu, K.; Cikim, I.G. Vitamin and mineral levels during pregnancy. Front. Public Heal. 2022, 68, 1705–1708. [Google Scholar] [CrossRef]
- National Institutes of Health, Office of Dietary Supplements. Phosphorus: Fact sheet for professionals. https://ods.od.nih.gov/factsheets/Phosphorus-HealthProfessional/.
- De Jorge, F.B.; Delascio, D.; De Ulhoa Cintra, A.B.; Antunes, M.L. Magnesium concentration in the blood serum of normal pregnant women. Obstet Gynecol. 1965, 25, 253–4. [Google Scholar] [PubMed]
- Rigo, J.; Pieltain, C.; Christmann, V.; Bonsante, F.; Moltu, S.J.; Iacobelli, S.; Marret, S. Serum Magnesium Levels in Preterm Infants Are Higher Than Adult Levels: A Systematic Literature Review and Meta-Analysis. Nutrients 2017, 9, 1125. [Google Scholar] [CrossRef]
- Tan, L.; Xu, Q.; Li, C.; Liu, J.; Shi, R. High-Normal Serum Magnesium and Hypermagnesemia Are Associated With Increased 30-Day In-Hospital Mortality: A Retrospective Cohort Study. Front. Cardiovasc. Med. 2021, 8. [Google Scholar] [CrossRef]
- Cheungpasitporn, W.; Thongprayoon, C.; Chewcharat, A.; Petnak, T.; Mao, M.A.; Davis, P.W.; Bathini, T.; Vallabhajosyula, S.; Qureshi, F.; Erickson, S.B. Hospital-Acquired Dysmagnesemia and In-Hospital Mortality. Med Sci. 2020, 8, 37. [Google Scholar] [CrossRef]
- Carrillo, I.G.; Vega, A.; Goicoechea, M.; Shabaka, A.; Gatius, S.; Abad, S.; López-Gómez, J.M. Impact of Serum Magnesium Levels on Kidney and Cardiovascular Prognosis and Mortality in CKD Patients. J. Ren. Nutr. 2021, 31, 494–502. [Google Scholar] [CrossRef]
- Krebs, N.F.; Reidinger, C.J.; Robertson, A.D.; Brenner, M. Bone mineral density changes during lactation: maternal, dietary, and biochemical correlates. Am. J. Clin. Nutr. 1997, 65, 1738–1746. [Google Scholar] [CrossRef]
- Sánchez, C.; Fente, C.; Barreiro, R.; López-Racamonde, O.; Cepeda, A.; Regal, P. Association between Breast Milk Mineral Content and Maternal Adherence to Healthy Dietary Patterns in Spain: A Transversal Study. Foods 2020, 9, 659. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Solomons, N.W.; E Scott, M.; Koski, K.G. Minerals and Trace Elements in Human Breast Milk Are Associated with Guatemalan Infant Anthropometric Outcomes within the First 6 Months. J. Nutr. 2016, 146, 2067–2074. [Google Scholar] [CrossRef] [PubMed]
- Gates, A.; Marin, T.; De Leo, G.; Waller, J.L.; Stansfield, B.K. Nutrient composition of preterm mother’s milk and factors that influence nutrient content. Am. J. Clin. Nutr. 2021, 114, 1719–1728. [Google Scholar] [CrossRef]
- Tsakiridis, I.; Kasapidou, E.; Dagklis, T.; Leonida, I.; Leonida, C.; Bakaloudi, D.R.; Chourdakis, M. Nutrition in Pregnancy: A Comparative Review of Major Guidelines. Obstet. Gynecol. Surv. 2020, 75, 692–702. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.B.; Sorenson, J.C.; Pollard, E.L.; Kirby, J.K.; Audhya, T. Evidence-Based Recommendations for an Optimal Prenatal Supplement for Women in the U.S., Part Two: Minerals. Nutrients 2021, 13, 1849. [Google Scholar] [CrossRef] [PubMed]
- Ciosek, Ż.; Kot, K.; Kosik-Bogacka, D.; Łanocha-Arendarczyk, N.; Rotter, I. The Effects of Calcium, Magnesium, Phosphorus, Fluoride, and Lead on Bone Tissue. Biomolecules 2021, 11, 506. [Google Scholar] [CrossRef]
- Kovacs, C.S. The Skeleton Is a Storehouse of Mineral That Is Plundered During Lactation and (Fully?) Replenished Afterwards. J. Bone Miner. Res. 2017, 32, 676–680. [Google Scholar] [CrossRef]
- Tihtonen, K.; Korhonen, P.; Isojärvi, J.; Ojala, R.; Ashorn, U.; Ashorn, P.; Tammela, O. Calcium supplementation during pregnancy and maternal and offspring bone health: a systematic review and meta-analysis. Ann. New York Acad. Sci. 2021, 1509, 23–36. [Google Scholar] [CrossRef]
- Cai, G.; Tian, J.; Winzenberg, T.; Wu, F. Calcium supplementation for improving bone density in lactating women: a systematic review and meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2020, 112, 48–56. [Google Scholar] [CrossRef]
- Neelamegham, S.; Mahal, L.K. Multi-level regulation of cellular glycosylation: from genes to transcript to enzyme to structure. Curr. Opin. Struct. Biol. 2016, 40, 145–152. [Google Scholar] [CrossRef]
- Durin, Z.; Houdou, M.; Legrand, D.; Foulquier, F. Metalloglycobiology: The power of metals in regulating glycosylation. Biochim. et Biophys. Acta (BBA) - Gen. Subj. 2023, 1867, 130412. [Google Scholar] [CrossRef]
- Foulquier, F.; Legrand, D. Biometals and glycosylation in humans: Congenital disorders of glycosylation shed lights into the crucial role of Golgi manganese homeostasis. Biochim. et Biophys. Acta (BBA) - Gen. Subj. 2020, 1864, 129674. [Google Scholar] [CrossRef] [PubMed]
- Lönnerdal, B.; Hernell, O. An Opinion on “Staging” of Infant Formula. J. Pediatr. Gastroenterol. Nutr. 2016, 62, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Hegar, B.; Wibowo, Y.; Basrowi, R.W.; Ranuh, R.G.; Sudarmo, S.M.; Munasir, Z.; Atthiyah, A.F.; Widodo, A.D.; Supriatmo, *!!! REPLACE !!!*; Kadim, M.; et al. The Role of Two Human Milk Oligosaccharides, 2′-Fucosyllactose and Lacto-N-Neotetraose, in Infant Nutrition. Pediatr. Gastroenterol. Hepatol. Nutr. 2019, 22, 330–340. [Google Scholar] [CrossRef]
- Sibley, C.P.; Brownbill, P.; Dilworth, M.; Glazier, J.D. Review: Adaptation in placental nutrient supply to meet fetal growth demand: Implications for programming. Placenta 2010, 31, S70–S74. [Google Scholar] [CrossRef] [PubMed]
- Runnels, L.W.; Komiya, Y. TRPM6 and TRPM7: Novel players in cell intercalation during vertebrate embryonic development. Dev. Dyn. 2020, 249, 912–923. [Google Scholar] [CrossRef]
- Komiya, Y.; Su, L.-T.; Chen, H.-C.; Habas, R.; Runnels, L.W. Magnesium and embryonic development. Magnes. Res. 2014, 27, 1–8. [Google Scholar] [CrossRef]
- Watanabe, M.; Shinohara, A.; Matsukawa, T.; Chiba, M.; Wu, J.; Iesaki, T.; Okada, T. Chronic magnesium deficiency decreases tolerance to hypoxia/reoxygenation injury in mouse heart. Life Sci. 2011, 88, 658–663. [Google Scholar] [CrossRef]
- Burton, G.J.; Jauniaux, E. The human placenta: new perspectives on its formation and function during early pregnancy. Proc. R. Soc. B: Biol. Sci. 2023, 290, 20230191. [Google Scholar] [CrossRef]
- Schlegel, R.N.; Cuffe, J.; Moritz, K.; Paravicini, T. Maternal hypomagnesemia causes placental abnormalities and fetal and postnatal mortality. Placenta 2015, 36, 750–758. [Google Scholar] [CrossRef]
- Rosner, J.; Gupta, M.; McGill, M.; Xue, X.; Chatterjee, P.; Yoshida-Hay, M.; Robeson, W.; Metz, C. Magnesium deficiency during pregnancy in mice impairs placental size and function. Placenta 2016, 39, 87–93. [Google Scholar] [CrossRef]
- Kocylowski, R.; Grzesiak, M.; Gaj, Z.; Lorenc, W.; Bakinowska, E.; Barałkiewicz, D.; von Kaisenberg, C.S.; Lamers, Y.; Suliburska, J. Associations between the Level of Trace Elements and Minerals and Folate in Maternal Serum and Amniotic Fluid and Congenital Abnormalities. Nutrients 2019, 11, 328. [Google Scholar] [CrossRef]
- World Health Organization. https://www.who.int/news-room/spotlight/why-we-need-to-talk-about-losing-a-baby. Accessed 1 October 2024.
- Sami, A.S.; Suat, E.; Alkis, I.; Karakus, Y.; Guler, S. The role of trace element, mineral, vitamin and total antioxidant status in women with habitual abortion. J. Matern. Neonatal Med. 2019, 34, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.-I.; Cardenas, A.; Rifas-Shiman, S.L.; Zota, A.R.; Hivert, M.-F.; Aris, I.M.; Sanders, A.P. Non-essential and essential trace element mixtures and kidney function in early pregnancy – A cross-sectional analysis in project viva. Environ. Res. 2022, 216, 114846–114846. [Google Scholar] [CrossRef]
- Stenhouse, C.; Suva, L.J.; Gaddy, D.; Wu, G.; Bazer, F.W. Phosphate, Calcium, and Vitamin D: Key Regulators of Fetal and Placental Development in Mammals. Adv Exp Med Biol. 2022, 1354, 77–107. [Google Scholar] [CrossRef]
- Rothen, J.-P.; Rutishauser, J.; Arnet, I.; Allemann, S.S. Renal insufficiency and magnesium deficiency correlate with a decreased formation of biologically active cholecalciferol: a retrospective observational study. Pharm. Weekbl. 2022, 45, 240–244. [Google Scholar] [CrossRef]
- Leonard, S.A.; Siadat, S.; Main, E.K.; Huybrechts, K.F.; El-Sayed, Y.Y.; Hlatky, M.A.; Atkinson, J.; Sujan, A.; Bateman, B.T. Chronic Hypertension During Pregnancy: Prevalence and Treatment in the United States, 2008–2021. Hypertension 2024, 81, 1716–1723. [Google Scholar] [CrossRef] [PubMed]
- Brandt, J.S.; Ananth, C.V. Chronic Hypertension: A Neglected Condition but With Emerging Importance in Obstetrics and Beyond. Hypertension 2024, 81, 1724–1727. [Google Scholar] [CrossRef] [PubMed]
- Rosanoff, A.; Costello, R.B.; Johnson, G.H. Effectively Prescribing Oral Magnesium Therapy for Hypertension: A Categorized Systematic Review of 49 Clinical Trials. Nutrients 2021, 13, 195. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. RE: Petition for a qualified health claim for magnesium and reduced risk of high blood pressure (hypertension) (docket No. FDA-2016-Q-3770). January 10, 2022. https://www.fda.gov/media/155304/download?attachment.
- Saris, N.-E.L.; Mervaala, E.; Karppanen, H.; Khawaja, J.A.; Lewenstam, A. Magnesium: An update on physiological, clinical and analytical aspects. Clin. Chim. Acta 2000, 294, 1–26. [Google Scholar] [CrossRef]
- Holmberg, M.J.; Granfeldt, A.; Andersen, L.W. Bicarbonate, calcium, and magnesium for in-hospital cardiac arrest – An instrumental variable analysis. Resuscitation 2023, 191, 109958. [Google Scholar] [CrossRef] [PubMed]
- Bohn, M.K.; Bailey, D.; Balion, C.; Cembrowski, G.; Collier, C.; De Guire, V.; Higgins, V.; Jung, B.; Ali, Z.M.; Seccombe, D.; et al. Reference Interval Harmonization: Harnessing the Power of Big Data Analytics to Derive Common Reference Intervals across Populations and Testing Platforms. Clin. Chem. 2023, 69, 991–1008. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.I.; Brown, P.W. The Effects of Magnesium on Hydroxyapatite Formation In Vitro from CaHPO4 and Ca4(PO4)2O at 37.4°C. Calcif. Tissue Int. 1997, 60, 538–546. [Google Scholar] [CrossRef]
- Lowenstein, F.W.; Stanton, M.F. Serum magnesium levels in the United States, 1971-1974. J. Am. Coll. Nutr. 1986, 5, 399–414. [Google Scholar] [CrossRef] [PubMed]
- Mejía-Rodríguez, F.; Shamah-Levy, T.; Villalpando, S.; García-Guerra, A.; Humarán, I.M.-G. Iron, zinc, copper and magnesium deficiencies in Mexican adults from the National Health and Nutrition Survey 2006. Salud Publica De Mex. 2013, 55, 275–284. [Google Scholar] [CrossRef]
- Misra, P.S.; Nessim, S.J. Clinical aspects of magnesium physiology in patients on dialysis. Semin. Dial. 2017, 30, 438–445. [Google Scholar] [CrossRef]
- Costello, R.B.; Elin, R.J.; Rosanoff, A.; Wallace, T.C.; Guerrero-Romero, F.; Hruby, A.; Lutsey, P.L.; Nielsen, F.H.; Rodriguez-Moran, M.; Song, Y.; et al. Perspective: The Case for an Evidence-Based Reference Interval for Serum Magnesium: The Time Has Come. Adv. Nutr. 2016, 7, 977–993. [Google Scholar] [CrossRef]
- Rosanoff, A. Perspective: US Adult Magnesium Requirements Need Updating: Impacts of Rising Body Weights and Data-Derived Variance. Adv. Nutr. Int. Rev. J. 2020, 12, 298–304. [Google Scholar] [CrossRef]
- Yamanaka, R.; Shindo, Y.; Oka, K. Magnesium Is a Key Player in Neuronal Maturation and Neuropathology. Int. J. Mol. Sci. 2019, 20, 3439. [Google Scholar] [CrossRef]
- Workinger, J.L.; Doyle, R.P.; Bortz, J. Challenges in the Diagnosis of Magnesium Status. Nutrients 2018, 10, 1202. [Google Scholar] [CrossRef]
- Leenders, N.H.J.; Vervloet, M.G. Magnesium: A Magic Bullet for Cardiovascular Disease in Chronic Kidney Disease? Nutrients 2019, 11, 455. [Google Scholar] [CrossRef] [PubMed]
- Zhan, Y.; Chen, R.; Zheng, W.; Guo, C.; Lu, L.; Ji, X.; Chi, Z.; Yu, J. Association Between Serum Magnesium and Anemia: China Health and Nutrition Survey. Biol. Trace Element Res. 2014, 159, 39–45. [Google Scholar] [CrossRef] [PubMed]
- van de Wal-Visscher, E.R.; Kooman, J.P.; van der Sande, F.M. Magnesium in Chronic Kidney Disease: Should We Care? Blood Purif. 2018, 45, 173–178. [Google Scholar] [CrossRef]
- Glasdam, S.-M.; Glasdam, S.; Peters, G.H. The Importance of Magnesium in the Human Body: A Systematic Literature Review. Adv. Clin. Chem. 2016, 73, 169–193. [Google Scholar] [CrossRef] [PubMed]
- Akizawa, Y.; Koizumi, S.; Itokawa, Y.; Ojima, T.; Nakamura, Y.; Tamura, T.; Kusaka, Y. Daily Magnesium Intake and Serum Magnesium Concentration among Japanese People. J. Epidemiology 2008, 18, 151–159. [Google Scholar] [CrossRef]
- Severino, P.; Netti, L.; Mariani, M.V.; Maraone, A.; D’aMato, A.; Scarpati, R.; Infusino, F.; Pucci, M.; Lavalle, C.; Maestrini, V.; et al. Prevention of Cardiovascular Disease: Screening for Magnesium Deficiency. Cardiol. Res. Pr. 2019, 2019, 1–10. [Google Scholar] [CrossRef]
- Møller, A.S.; Bressendorff, I.; Nordholm, A.; Egstrand, S.; Jørgensen, N.R.; Klausen, T.W.; Olgaard, K.; Hansen, D.; Jacobsen, A.A. Diurnal variation of magnesium and the mineral metabolism in patients with chronic kidney disease. Bone Rep. 2021, 15, 101130. [Google Scholar] [CrossRef]
- Razzaque, M.S. Magnesium: Are We Consuming Enough? Nutrients 2018, 10, 1863. [Google Scholar] [CrossRef]
- Rosanoff, A.; Weaver, C.M.; Rude, R.K. Suboptimal magnesium status in the United States: are the health consequences underestimated? Nutr. Rev. 2012, 70, 153–164. [Google Scholar] [CrossRef]
- Rosanoff, A.; West, C.; Elin, R.J.; Micke, O.; Baniasadi, S.; Barbagallo, M.; Campbell, E.; Cheng, F.-C.; Costello, R.B.; Gamboa-Gomez, C.; et al. Recommendation on an updated standardization of serum magnesium reference ranges. Eur. J. Nutr. 2022, 61, 3697–3706. [Google Scholar] [CrossRef]
- Micke, O.; Vormann, J.; Kraus, A.; Kisters, K. Serum magnesium: time for a standardized and evidence-based reference range. Magnes Res. 2021, 34, 84–89. [Google Scholar] [CrossRef]
- Micke, O.; Vormann, J.; Classen, H.-G.; Kisters, K. Magnesium: Bedeutung für die hausärztliche Praxis – Positionspapier der Gesellschaft für Magnesium-Forschung e. V. DMW - Dtsch. Med. Wochenschr. 2020, 145, 1628–1634. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Wang, X.-F.; Li, D.-Y.; Chen, Y.-C.; Zhao, L.-J.; Liu, X.-G.; Guo, Y.-F.; Shen, J.; Lin, X.; Deng, J.; et al. The good, the bad, and the ugly of calcium supplementation: a review of calcium intake on human health. Clin. Interv. Aging 2018, 13, 2443–2452. [Google Scholar] [CrossRef]
- Weaver CM, Heaney RP. Food sources, supplements, and bioavailability. Chapter 9, pp. 129-142 in: Calcium in Human Health, Weaver CM, Heaney RP, Eds. Humana Press, Totowa, NJ, 2006.
- World Health Organization. WHO recommendation on calcium supplementation before pregnancy for the prevention of pre-eclampsia and its complications. Geneva: World Health Organization; 2020.
- National Institutes of Health. Magnesium Fact Sheet for Professionals. https://ods.od.nih.gov/factsheets/Magnesium-HealthProfessional/?print=1. Accessed 8 August 2024.
- Spätling, L.; Classen, H.G.; Kisters, K.; Liebscher, U.; Rylander, R.; et al. Supplementation of magnesium in pregnancy. J Preg Child Health. 2017, 4, 302. [Google Scholar] [CrossRef]
- Parazzini, F.; Di Martino, M.; Pellegrino, P. Magnesium in the gynecological practice: a literature review. Magnes. Res. 2017, 30, 1–7. [Google Scholar] [CrossRef]
- Tian, Z.; Qu, S.; Chen, Y.; Fang, J.; Song, X.; He, K.; Jiang, K.; Sun, X.; Shi, J.; Tao, Y.; et al. Associations of the magnesium depletion score and magnesium intake with diabetes among US adults: an analysis of the National Health and Nutrition Examination Survey 2011-2018. Epidemiology Heal. 2024, 46, e2024020. [Google Scholar] [CrossRef] [PubMed]
- Repke, J.T. Calcium, Magnesium, and Zinc Supplementation and Perinatal Outcome. Clin. Obstet. Gynecol. 1991, 34, 262–267. [Google Scholar] [CrossRef]
- Čabarkapa, V.; Bogavac, M.; Jakovljević, A.; Pezo, L.; Nikolić, A.; Belopavlović, Z.; Mirjana, D. Serum magnesium level in the first trimester of pregnancy as a predictor of pre-eclampsia – a pilot study. Hypertens. Pregnancy 2018, 37, 144–153. [Google Scholar] [CrossRef]
- Escobedo-Monge, M.F.; Barrado, E.; Parodi-Román, J.; Escobedo-Monge, M.A.; Torres-Hinojal, M.C.; Marugán-Miguelsanz, J.M. Magnesium Status and Ca/Mg Ratios in a Series of Children and Adolescents with Chronic Diseases. Nutrients 2022, 14, 2941. [Google Scholar] [CrossRef]
- Rosanoff, A.; West, C.; Elin, R.J.; Micke, O.; Baniasadi, S.; Barbagallo, M.; Campbell, E.; Cheng, F.-C.; Costello, R.B.; Gamboa-Gomez, C.; et al. Recommendation on an updated standardization of serum magnesium reference ranges. Eur. J. Nutr. 2022, 61, 3697–3706. [Google Scholar] [CrossRef]
- Murphy, R.; Marshall, K.; Zagorin, S.; Devarshi, P.P.; Mitmesser, S.H. Socioeconomic Inequalities Impact the Ability of Pregnant Women and Women of Childbearing Age to Consume Nutrients Needed for Neurodevelopment: An Analysis of NHANES 2007–2018. Nutrients 2022, 14, 3823. [Google Scholar] [CrossRef]
- Henriksen, C.; Aaseth, J.O. Magnesium: a scoping review for Nordic Nutrition Recommendations 2023. Food Nutr. Res. 2023, 67. [Google Scholar] [CrossRef] [PubMed]
- Farias, P.M.; Marcelino, G.; Santana, L.F.; de Almeida, E.B.; Guimarães, R.d.C.A.; Pott, A.; Hiane, P.A.; Freitas, K.d.C. Minerals in Pregnancy and Their Impact on Child Growth and Development. Molecules 2020, 25, 5630. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Yu, Y.; Zhu, T.; Lin, X.; Jing, X.; Zhang, J. Oral Magnesium Supplementation for the Prevention of Preeclampsia: a Meta-analysis or Randomized Controlled Trials. Biol. Trace Element Res. 2021, 200, 3572–3581. [Google Scholar] [CrossRef] [PubMed]
- Makrides, M.; Crosby, D.D.; Shepherd, E.; A Crowther, C.; Bain, E.; Cochrane Pregnancy and Childbirth Group. Magnesium supplementation in pregnancy. Cochrane Database Syst. Rev. 2014, 2019, CD000937. [Google Scholar] [CrossRef]
- Liu, J.; Song, G.; Zhao, G.; Meng, T. Effect of oral magnesium supplementation for relieving leg cramps during pregnancy: A meta-analysis of randomized controlled trials. Taiwan. J. Obstet. Gynecol. 2021, 60, 609–614. [Google Scholar] [CrossRef]
- Gunabalasingam, S.; Slizys, D.D.A.L.; Quotah, O.; Magee, L.; White, S.L.; Rigutto-Farebrother, J.; Poston, L.; Dalrymple, K.V.; Flynn, A.C. Micronutrient supplementation interventions in preconception and pregnant women at increased risk of developing pre-eclampsia: a systematic review and meta-analysis. Eur. J. Clin. Nutr. 2022, 77, 710–730. [Google Scholar] [CrossRef]
- Doyle, L.; Flynn, A.; Cashman, K. The effect of magnesium supplementation on biochemical markers of bone metabolism or blood pressure in healthy young adult females. Eur. J. Clin. Nutr. 1999, 53, 255–261. [Google Scholar] [CrossRef]
- Zubero, M.B.; Llop, S.; Irizar, A.; Murcia, M.; Molinuevo, A.; Ballester, F.; Levi, M.; Lozano, M.; Ayerdi, M.; Santa-Marina, L. Serum metal levels in a population of Spanish pregnant women. Gac. Sanit. 2021, 36, 468–476. [Google Scholar] [CrossRef]
- McCowan, L.M.; Figueras, F.; Anderson, N.H. Evidence-based national guidelines for the management of suspected fetal growth restriction: comparison, consensus, and controversy. Am. J. Obstet. Gynecol. 2018, 218, S855–S868. [Google Scholar] [CrossRef]
- de Araújo, C.A.L.; Ray, J.G.; Figueiroa, J.N.; Alves, J.G. BRAzil magnesium (BRAMAG) trial: a double-masked randomized clinical trial of oral magnesium supplementation in pregnancy. BMC Pregnancy Childbirth 2020, 20, 1–7. [Google Scholar] [CrossRef]
- Tarjan, A.; Zarean, E. Effect of Magnesium Supplement on Pregnancy Outcomes: A Randomized Control Trial. Adv. Biomed. Res. 2017, 6, 109. [Google Scholar] [CrossRef] [PubMed]
- Dalton, L.M.; Fhloinn, D.M.N.; Gaydadzhieva, G.T.; Mazurkiewicz, O.M.; Leeson, H.; Wright, C.P. Magnesium in pregnancy. Nutr. Rev. 2016, 74, 549–557. [Google Scholar] [CrossRef]
- Kinnunen, T.; Liu, Y.; Koivisto, A.; Virtanen, S.; Luoto, R. Effects of dietary counselling on micronutrient intakes in pregnant women in Finland. Matern. Child Nutr. 2021, 17, e13203. [Google Scholar] [CrossRef] [PubMed]
- Orlova, S.; Dikke, G.; Pickering, G.; Djobava, E.; Konchits, S.; Starostin, K. Magnesium level correlation with clinical status and quality of life in women with hormone related conditions and pregnancy based on real world data. Sci. Rep. 2021, 11, 1–10. [Google Scholar] [CrossRef]
- Yelverton, C.A.; Rafferty, A.A.; Moore, R.L.; Byrne, D.F.; Mehegan, J.; Cotter, P.D.; Van Sinderen, D.; Murphy, E.F.; Killeen, S.L.; McAuliffe, F.M. Diet and mental health in pregnancy: Nutrients of importance based on large observational cohort data. Nutrition 2022, 96, 111582. [Google Scholar] [CrossRef] [PubMed]
- Crawford, S.A.; Brown, A.R.; Camargo, J.T.; Kerling, E.H.; Carlson, S.E.; Gajewski, B.J.; Sullivan, D.K.; Valentine, C.J. Micronutrient Gaps and Supplement Use in a Diverse Cohort of Pregnant Women. Nutrients 2023, 15, 3228. [Google Scholar] [CrossRef]
- Prabhu, K.; Dastidar, R.G.; Aroor, A.R.; Rao, M.; Shetty, S.; Poojari, V.G.; Bs, V. Micronutrients in Adverse Pregnancy Outcomes. F1000Research 2024, 11, 1369. [Google Scholar] [CrossRef]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B.; PRISMA-S Group. PRISMA-S: An extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Syst. Rev. 2021, 10, 1–19. [Google Scholar] [CrossRef]
- Hsiao, P.-J.; Liao, C.-Y.; Kao, Y.-H.; Chan, J.-S.; Lin, Y.-F.; Chuu, C.-P.; Chen, J.-S. Comparison of fractional excretion of electrolytes in patients at different stages of chronic kidney disease. Medicine 2020, 99, e18709. [Google Scholar] [CrossRef]
Figure 1.
Thermograph of relationships between serum Mg2+ and health. The color green reflects concentrations that typically fall within the normal range; red reflects concentrations that are associated with adverse effects. Yellow shading reflects concentrations which may be associated with increased risks of adverse effects in individuals under physiological stress, as in pregnancy and lactation.
Figure 1.
Thermograph of relationships between serum Mg2+ and health. The color green reflects concentrations that typically fall within the normal range; red reflects concentrations that are associated with adverse effects. Yellow shading reflects concentrations which may be associated with increased risks of adverse effects in individuals under physiological stress, as in pregnancy and lactation.
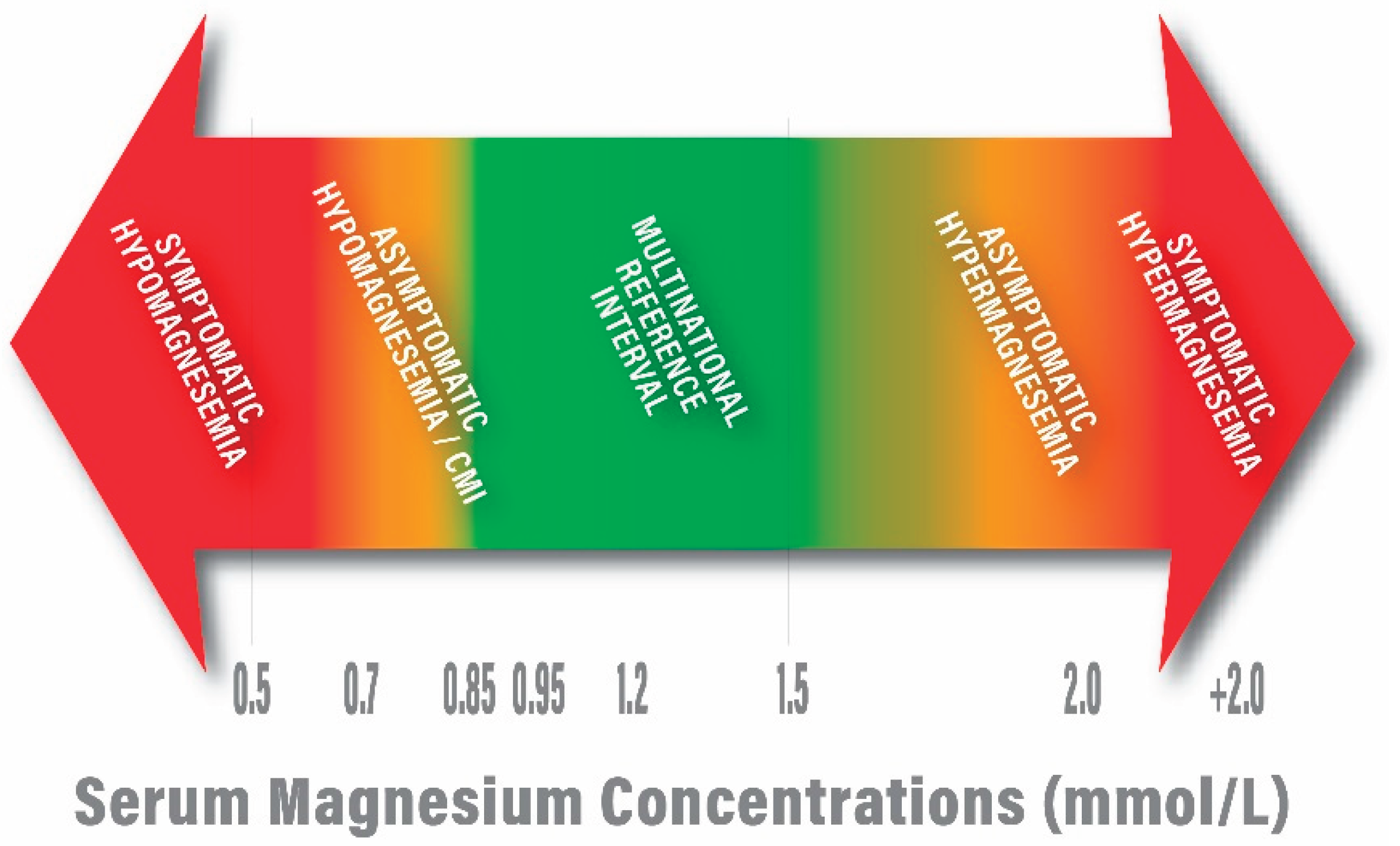

Table 1.
Changes in mean serum concentrations of key minerals during pregnancy (Larsson [14]).
Table 1.
Changes in mean serum concentrations of key minerals during pregnancy (Larsson [14]).
| Period | Calcium (mmol/L) | Magnesium (mmol/L) | Phosphate (mmol/L)1 | |||
|---|---|---|---|---|---|---|
| Lower Limit* | Upper Limit* | Lower Limit* | Upper Limit* | Lower Limit* | Upper Limit* | |
| Week 7–17 | 2.18 (2.12–2.23) | 2.53 (2.50–2.57) | 0.70 (0.69–0.71) | 0.96 (0.88–1.059) | 0.85 (0.80–0.90) | 1.65 (1.43–1.86) |
| Week 17–24 | 2.08 (2.04–2.11) | 2.45 (2.41–2.50) | 0.66 (0.65–0.66) | 0.87 (0.84–0.90) | 0.84 (0.74–0.95) | 1.45 (1.41–1.48) |
| Week 24–28 | 2.04 (1.99–2.08) | 2.40 (2.36–2.43) | 0.63 (0.63–0.63) | 0.91 (0.86–0.97) | 0.81 (0.67–0.95) | 1.47 (1.43–1.51) |
| Week 28–31 | 2.07 (2.03–2.11) | 2.41 (2.33–2.49) | 0.63 (0.63–0.64) | 0.91 (0.88–0.94) | 0.77 (0.70–0.85) | 1.44 (1.38–1.49) |
| Week 31–34 | 2.05 (1.99–2.10) | 2.38 (2.37–2.40) | 0.64 (0.64–0.64) | 0.90 (0.84–0.97) | 0.84 (0.72–0.95) | 1.42 (1.35–1.49) |
| Week 34–38 | 2.04 (1.96–2.11) | 2.41 (2.39–2.43) | 0.57 (0.50–0.65) | 0.87 (0.84–0.90) | 0.85 (0.80–0.90) | 1.50 (1.43–1.57) |
| Predelivery | 1.98 (1.91–2.05) | 2.46 (2.42–2.50) | 0.64 (0.63–0.65) | 0.94 (0.91–0.96) | 0.89 (0.86–0.92) | 1.50 (1.43–1.57) |
| Postpartum | 2.06 (1.90–2.22) | 2.57 (2.51–2.63) | 0.68 (0.66–0.71) | 0.99 (0.92–1.06) | 1.00 (0.89–1.12) | 1.80 (1.62–1.99) |
* Mean and (90% Confidence Interval).
Table 2.
Effects of plasma volume on serum magnesium concentrations (De Jorge [19]).
Table 2.
Effects of plasma volume on serum magnesium concentrations (De Jorge [19]).
| Gestation (Days) | Gestation (Weeks) | No. of Women | Mean [Mg], mEq/L | SD | Plasma Volume (mL) | Corrected Conc. Mg (mEq/L) | Conc. Mg (mmol/L) |
|---|---|---|---|---|---|---|---|
| ~30 | ~4 | 5 | 1.873 | 0.104 | 2644 | 1.834 | 0.92 |
| 31-60 | 4-9 | 12 | 1.826 | 0.103 | 2643 | 1.787 | 0.89 |
| 61-90 | 9-13 | 28 | 1.728 | 0.091 | 2770 | 1.773 | 0.89 |
| 91-120 | 13-17 | 29 | 1.694 | 0.139 | 3047 | 1.912 | 0.96 |
| 121-150 | 17-21 | 23 | 1.599 | 0.177 | 3305 | 1.957 | 0.98 |
| 151-180 | 21-26 | 23 | 1.558 | 0.104 | 3550 | 2.048 | 1.02 |
| 180-210 | 26-30 | 17 | 1.488 | 0.101 | 3769 | 2.077 | 1.04 |
| 211-240 | 30-34 | 9 | 1.526 | 0.121 | 3820 | 2.159 | 1.08 |
| 240-270 | 34-39 | 5 | 1.392 | 0.173 | 3658 | 1.882 | 0.94 |
| Normal Value | 2.087 | 0.067 | 2.087 | 1.04 |
Table 3.
Mineral content of whole milk of mothers.
| Category | Mineral content, mmol/L | Source | ||
|---|---|---|---|---|
| Ca | P | Mg | ||
| A. Mothers who carried to term | ||||
| Human (Early lactation) | 7.4 | 3.9 | 1.4 | Sánchez [25] |
| Human (Late lactation) | 6.3 | 3.9 | 1.4 | |
| Human (Early lactation) | 6.9 | - | 1.0 | Li [26] |
| Human (Late lactation) | 6.6 | - | 0.9 | |
| Human (Established feeding) | 6.7 | - | 1.5 | |
| Human | 7 | 4.7 | 1.3 | Sanchez [26] |
| B. Mothers who delivered prematurely | ||||
| Human (Day 7 post-partum) | 6.1 | 4.7 | 1.3 | Gates [27] |
| Human (Day 14 post-partum) | 5.6 | 4.6 | 1.2 | |
| Human (Day 21 post-partum) | 5.5 | 4.4 | 1.2 | |
| Human (Day 28 post-partum) | 5.3 | 4.1 | 1.4 | |
| The values in this table are means and do not reflect the reported standard deviations, confidence intervals, or the ranges of concentrations found. | ||||
Table 4.
Molar ratios of Ca:Mg during pregnancy. The ratios are calculated as ratios of the means cited by Larsson [14].
Table 4.
Molar ratios of Ca:Mg during pregnancy. The ratios are calculated as ratios of the means cited by Larsson [14].
| Period | Molar Ratio Ca:Mg | |||
|---|---|---|---|---|
| LoCa:LoMg | HiCa:LoMg | HiCa:HiMg | LoCa:HiMg | |
| Week 7–17 | 3.11 | 3.61 | 2.64 | 2.27 |
| Week 17–24 | 3.15 | 3.71 | 2.82 | 2.39 |
| Week 24–28 | 3.24 | 3.81 | 2.64 | 2.24 |
| Week 28–31 | 3.29 | 3.83 | 2.65 | 2.27 |
| Week 31–34 | 3.20 | 3.72 | 2.64 | 2.28 |
| Week 34–38 | 3.58 | 4.23 | 2.77 | 2.34 |
| Predelivery | 3.09 | 3.84 | 2.62 | 2.11 |
| Postpartum | 3.03 | 3.78 | 2.60 | 2.08 |
Table 5.
Increased risks associated with low maternal serum Mg2+.
| For mother with chronic Mg2+ deficiency | For child |
|---|---|
| Poor embryonic development Poor placental development Spontaneous abortion Declines in renal health Hypertension |
Inadequate intrauterine growth and development (Fetal Growth Restriction) Spontaneous pre-term birth |
| Late pregnancy complications (Not a focus of this review) | |
| Declines in mental health during pregnancy Pre-eclampsia and related side effects Placental abruption Declines in immune health Gestational diabetes Early time of delivery (pre-term delivery) Post-partum depression Post-partum recovery of bone mineral density |
Retarded organ development/fetal programming Congenital abnormalities Poor skeletal development |
Table 6.
Examples of Increased Risks Potentially Associated with Low Maternal Serum Mg2+ Early in Pregnancy.
Table 6.
Examples of Increased Risks Potentially Associated with Low Maternal Serum Mg2+ Early in Pregnancy.
| Risk: Failure to appropriately glycosylate lipid intermediates and proteins |
|
| Risk: Inability to meet nutrient demands retards embryonic development [39] |
|
| Risk: Aberrations in placental development |
|
| Risk: Spontaneous abortion |
|
| Risk: Declines in renal health |
|
| Risk: Inadequate biosynthesis of active Vitamin D3 |
|
| Risk: Essential Hypertension |
|
Table 7.
Reference values for serum magnesium concentration in adults.
| 0.68-0.88 mmol/L [Martin 59] |
| 0.70 – 0.96 mmol/L [Lowenstein and Stanton 60] |
| 0.70 – 0.95 mmol/L [Mejía-Rodriguez 61] |
| 0.71 – 0.94 [Nordic reference interval, Larsson 14] |
| 0.7 – 1.0 mmol/L [a U.S. standard; Misra 62] |
| 0.85 – 0.96 mmol/L [Costello 63; Rosanoff 64] |
| 0.5 – 1.05 mmol/L [a Japanese standard; Yamanaka 65] |
| 0.7 – 1.0 mmol/L [Workinger 66] |
| 0.7 – 1.05 mmol/L [a European standard; Leenders 67] |
| 0.84 – 1.05 mmol/L [Zhan 68] |
| 0.7 – 1.1 mmol/L [Van de Wal-Visscher 69; Glasdam 70] |
| 0.54 – 1.19 mmol/L [Akizawa 71] |
| 0.76 – 1.15 mmol/L [a European standard; Severino 72] |
| 1. | Phosphorus data are included for reference. Phosphorus and calcium are interrelated because hormones, such as vitamin D and parathyroid hormone (PTH), regulate the metabolism of both minerals. In addition, phosphorus and calcium make up hydroxyapatite, the main structural component in bones and tooth enamel. In adults, normal phosphate concentration in serum or plasma is 2.5 to 4.5 mg/dL (0.81 to 1.45 mmol/L) [18]. |
| 2. | The reference ranges for serum calcium and serum magnesium vary but generally range from 2.2-2.7 mmol/L and 0.7-1.0 mmol/L, respectively. |
| 3. | Data related to serum creatinine concentrations in Stage 1 and 2 chronic kidney disease patients show increases in serum creatinine when kidney function is compromised [109]. Thus, the association of increased serum creatinine with risk of pre-eclampsia may reflect early changes in kidney function. |
| 4. | Magnesium citrate contains 11% magnesium by weight. If 300 mg of magnesium citrate was administered, the magnesium content was 34 mg. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



