Submitted:
09 July 2025
Posted:
09 July 2025
You are already at the latest version
Abstract
Aim: Cytomegalovirus (CMV) infection is prevalent in patients with ulcerative colitis (UC), particularly in severe, steroid-refractory cases, yet its role in disease exacerbation remains debated. This retrospective cohort study included 110 patients with moderate-to-severe UC (as per Truelove and Witts criteria) who underwent colonoscopy and CMV testing. The primary objective was to investigate the correlation between tissue CMV DNA positivity, quantified via PCR, and endoscopic activity scores (Mayo and Rachmilewitz), alongside associations with inflammatory markers and recent steroid use. Materials and Methods: A retrospective cohort study included 110 UC patients from a university clinic (January 2021–April 2024). Patients underwent colonoscopy with tissue and blood PCR for CMV detection. Endoscopic activity was assessed using Mayo and Rachmilewitz scores. Results: Our results showed that 37% of patients were tissue CMV-DNA over 250 copies, with significantly higher Mayo scores (8.7 vs. 7.6, p=0.02), Rachmilewitz scores (8.6 vs. 7.4, p=0.03), erythrocyte sedimentation rates (54.3 vs. 42.8, p=0.04), and serum CMV levels (878.9 vs. 71.4, p=0.008). Correlation analysis revealed positive associations between tissue CMV copy number and sedimentation rates (r=0.22, p=0.01), serum CMV (r=0.37, p=0.0001), Mayo scores (r=0.18, p=0.05), and Rachmilewitz scores (r=0.25, p=0.008). Logistic regression analysis indicated a 12-fold increased risk of CMV positivity with recent steroid use (p=0.030). Conclusion: This study directly examines tissue CMV-DNA positivity and endoscopic activity degrees. Our findings suggest that the presence of CMV in colonic tissue may increase the endoscopic activity score in moderate to severe ulcerative colitis. These results underscore the need for routine CMV screening and larger prospective studies to clarify this interaction.
Keywords:
cytomegalovirus
; ulcerative colitis
; endoscopic activity
; Rachmilewits index
; Mayo score
; PCR
; steroid use
; inflammation
1. Introduction
Cytomegalovirus (CMV), a double-stranded DNA virus from the Herpesviridae family, can present asymptomatically, with systemic symptoms, or as tissue-invasive disease. The gastrointestinal tract is frequently affected, accounting for 30% of tissue-invasive cases in immunocompetent patients [1]. A high prevalence of CMV infection has been identified in patients with ulcerative colitis, particularly in severe corticosteroid-refractory cases, where the infection rate ranges from 20% to 40% based on diagnoses made using antigenemia and histological examination of tissue biopsies [2,3]. In immunocompetent individuals, CMV colitis is predominantly asymptomatic or manifests as a self-limiting condition [1,4]. However, it can potentially progress to a chronic infection or establish a lifelong carrier state characterized by intermittent viral reactivation [5]. CMV reactivation is commonly observed in cases of severe ulcerative colitis or patients exhibiting resistance to corticosteroid therapy. Nonetheless, it remains unclear whether CMV plays a causative role in exacerbating ulcerative colitis or merely represents an incidental finding associated with severe disease states [6,7]. On the other hand, some studies have suggested that there may be a close relationship between inflammation promoting viral expression and viral replication exacerbating inflammation [8]. The optimal approach for diagnosing CMV colitis remains unclear; however, Haematoxylin and Eosin (H&E) staining, immunohistochemistry (IHC), and tissue PCR are considered the preferred methods for detecting CMV in colonic tissue. These techniques are deemed more reliable for assessing CMV involvement in colitis than antigenemia testing, IgM serology, or CMV DNA PCR analysis [7,9]. Conversely, the delayed results of methods such as H&E staining in patients with acute severe ulcerative colitis may postpone the initiation of treatment for CMV-complicated colitis, potentially leading to serious complications [10,11]. Therefore, the European Crohn's and Colitis Organization (ECCO) guidelines recommend initiating of antiviral therapy in patients identified with CMV reactivation [12]. The Mayo Scoring System and the Rachmilewitz Index are commonly used tools for assessing the activity of UC [13,14]. These indices help in evaluating disease severity and guiding treatment decisions [15,16]. Some studies, albeit indirectly, have demonstrated that histologically confirmed CMV infection in colonic tissue is associated with increased inflammatory activity and elevated endoscopic activity scores in patients with UC [3,6,17,18]. However, there is a limited number of studies examining the direct impact of CMV detection through PCR in tissue samples on inflammatory and endoscopic severity. This study aims to compare the quantitative levels of CMV DNA, measured via PCR in tissue samples from ulcerative colitis patients experiencing moderate to severe flares—classified according to the Truelove and Witts criteria—with their corresponding endoscopic activity scores. Furthermore, we seek to evaluate the potential correlation between the presence of CMV and disease severity in this context.
2. Material and Method
This study was approved by the Ethics Committee of XXX on April 4, 2024 (approval number: 2024000169-1; file number: 2024/169). Since the study was designed as a retrospective analysis, an informed consent form was not necessary.
2.1. Patient Selection
Between January 2021 and April 2024, a total of 231 patients diagnosed with moderate-to-severe colitis according to the Truelove and Witts criteria were identified at the university's Gastroenterology Clinic. Of these, 110 ulcerative colitis patients who underwent colonoscopy or flexible rectosigmoidoscopy and had tissue and blood PCR samples collected for histopathological and CMV analysis were included in the study. Among the remaining 121 patients, 71 had undergone colonoscopy or rectosigmoidoscopy within the preceding 6 months, and thus, repeat procedures were not performed. Four patients were clinically critical, requiring hospitalization and intravenous steroid and supportive therapy, leading to their exclusion from the study results. The remaining patients were excluded because they either did not consent to the endoscopic procedure or the procedure could not be performed (Figure 1). The demographic characteristics of the patients, age at diagnosis, follow-up durations, laboratory findings at the time of admission, daily defecation frequencies, quantitative results of serum CMV PCR tests, endoscopic Mayo Clinical and Rachmilewitz scores, tissue biopsy results, and quantitative results of tissue CMV PCR tests were recorded.
2.2. Endoscopic Procedures and Tissue Sampling
All endoscopic procedures were performed using the Fujinon EC-760R standard colonoscope by gastroenterologists with at least 2 years of experience in the field. After determining the Modified Mayo Score and Rachmilewitz endoscopic activity index of patients clinically suspected of having moderate or severe colitis according to Truelove and Witts criteria (Table 1) [14,16]. Biopsy samples were collected. For PCR analysis, a single bite sufficient to fill the forceps was taken using standard disposable colonoscopic forceps (2.8 mm Micro-Tech Endoscopy USA) and transferred to the PCR laboratory in serum saline under appropriate conditions and speed. In samples of similar sizes obtained from colon tissue, a threshold value of 250 copies of CMV DNA as detected by RT-PCR is accepted as indicative of a positive presence of CMV [19]. For other histochemical analyses, multiple samples were collected using the same forceps and sent for pathological examination in 4% formalin solution.
2.3. Statistics
Participants from the active ulcerative colitis group were divided into two groups: those with CMV colitis and those without. The study investigated whether there were differences between the two groups in terms of basic laboratory values, inflammatory markers, endoscopic and clinical disease activity scores, steroid use, and the amount of steroids used. Distribution analysis of the variables was performed using the Kolmogorov-Smirnov test. For parametric variables, independent sample t-tests were applied, while for non-parametric variables, the Mann-Whitney U test was used. Pearson's chi-square test was employed to compare categorical variables between the groups. The confidence interval (CI) was set at 95%, and a significance level of P < .05 was considered statistically significant. Power analysis was conducted using nQuery Advisor version 7, and statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) version 26.
3. Results
Patients were divided into two groups based on whether their tissue CMV PCR test results were positive (n=41) or negative (n=69). The study evaluated the presence of CMV in colon tissue samples and CMV DNA copy numbers, examining their relationships with endoscopic activity grades, quantitative serum CMV DNA PCR values, CRP, and sedimentation levels in both groups, as well as their association with stool frequency (Table 2).
A comparison was made between patients with CMV-positive ulcerative colitis (UC) and CMV-negative UC. No significant difference was observed in age (p = 0.93), diagnosis age (p = 0.38), white blood cell count (WBC) (p = 0.8), C-reactive protein (CRP) (p = 0.5), or daily defecation between the two groups. The proportion of females was significantly higher in the CMV-negative UC group (56%) compared to the CMV-positive UC group (42%) (p = 0.001). There was no significant difference in the proportion of males between the two groups (p=0.8). Follow-up time was significantly longer in the CMV-negative UC group (88 weeks) compared to the CMV-positive UC group (59.4 weeks) (p = 0.02). Erythrocyte sedimentation rate (ESR) was significantly higher in the CMV-positive UC group (54.3) compared to the CMV-negative UC group (42.8) (p = 0.04). CMV PCR serum levels were significantly elevated in the CMV-positive UC group (878.9) compared to the CMV-negative UC group (71.4) (p = 0.008). Rachmilewitz EAI was significantly higher in the CMV-positive UC group (8.6) compared to the CMV-negative UC group (7.4) (p = 0.03). Mayo score was significantly higher in the CMV-positive UC group (8.7) compared to the CMV-negative UC group (7.6) (p = 0.02). The correlation analysis between tissue CMV DNA copy number and various parameters is shown in Table 3.
Table 2 presents the correlation analysis of CMV-PCR tissue copy number with various parameters using the non-parametric Spearman method. The analysis revealed no statistically significant correlation between WBC and CMV-PCR tissue copy number. Similarly, daily defecation (r = 0.1, p = 0.29), age (r = 0.01, p = 0.8), diagnosis age (r = 0.1, p = 0.27), and CRP (r = 0.13, p = 0.16) showed no significant correlation with CMV-PCR tissue copy number. However, a statistically significant positive correlation was observed between sedimentation rates and CMV-PCR serum (r = 0.22, p = 0.01). Furthermore, CMV PCR serum exhibited a significant positive correlation (r = 0.37, p = 0.0001). A statistically significant correlation was also found for a Mayo Score (r = 0.18, p = 0.05) and Rachmilewitz EAI (r = 0.25, p = 0.008).
Logistic regression analysis was performed to determine the association between CMV DNA detection in tissue samples and the use of steroids or anti-TNF drugs in the preceding year (Table 4).
Logistic regression analysis was performed to identify predictors of CMV PCR positivity in tissues. The results, as shown in Table 2, indicated that steroid usage within the last 3 months was a significant predictor of CMV PCR positivity (p = 0.030). The odds ratio (Exp(B)) for steroid usage was 12.191, suggesting that individuals who used steroids in the last 3 months had approximately 12 times higher odds of CMV PCR positivity compared to those who did not. The 95% confidence interval for the odds ratio ranged from 1.281 to 116.032. Mayo Score (p = 0.472), Rachmilewitz (p = 0.440), Anti-TNF usage (p = 0.555), CRP (p = 0.735), and Sedim (p = 0.460) were not significantly associated with CMV PCR positivity in this model.
4. Discussion
The association between cytomegalovirus (CMV) infection and inflammatory bowel disease continues to be a debated topic. CMV infection is commonly observed in ulcerative colitis (UC) and may be detrimental. Diagnosis of CMV reactivation necessitates in situ detection of viral markers via immunohistochemistry or nucleic acid amplification, with quantification of infection density being crucial. While CMV reactivation may be considered an innocent bystander in refractory UC exacerbations, accumulating evidence suggests a deleterious role [7,15,20]. The existing data remain inconclusive regarding whether CMV exacerbates inflammation in individuals with severe colitis or merely represents an opportunistic finding associated with severe disease [21]. Small, retrospective studies and varying definitions for disease severity and CMV disease often limit the interpretation of existing results. CMV colitis is rare in patients with Crohn's disease or mild-to-moderate ulcerative colitis. In patients with severe and/or steroid-refractory ulcerative colitis, local reactivation of CMV can be detected in approximately 21-36% of cases in actively inflamed colon tissue [11,22,23,24]. Also CMV infection may represent a significant factor in the development of therapeutic resistance in IBD, particularly in cases of severe UC [25]. In our study, consistent with the existing literature, tissue CMV DNA positivity was detected in 37% of moderate-to-severe UC patients based on samples obtained with endoscopic procedures.
In patients with IBD, mucosal damage can compromise the intestinal mechanical barrier, potentially predisposing them to viral infections [26]. Consequently, these patients may exhibit a heightened systemic inflammatory response. It is established that patients with severe ulcerative colitis demonstrate elevated laboratory parameters indicative of an inflammatory response compared to those with inactive disease [27]. Furthermore, some studies indicate that in endoscopically active ulcerative colitis, the presence of CMV in tissue samples is associated with higher levels of inflammatory response parameters such as Erythrocyte Sedimentation Rate ESR and CRP compared to those without detectable CMV [2,22,28]. In our findings, despite similar clinical and endoscopic features between the two groups, we did not observe a significant difference in WBC count and CRP levels, which are indicative of acute inflammation. However, we demonstrated that ESR, a marker of more prolonged inflammation, was statistically significantly higher in patients with tissue CMV positivity. The similarity in clinical findings at the time of patient enrollment may explain the lack of difference in acute-phase inflammatory markers. Furthermore, the presence of CMV in tissue may have increased chronic inflammation over the long term, thereby elevating ESR.
The endoscopic evaluation of mucosal damage plays a crucial role in assessing the severity of UC. While both established and novel biomarkers, including fecal calprotectin and histopathological scoring, offer supplementary insights into biological disease activity, endoscopy remains the gold standard for an objective evaluation of the disease [29]. Consequently, routine endoscopic procedures for evaluating disease status are advocated in the clinical management guidelines by the American College of Gastroenterology, the international consensus statement known as STRIDE (Selecting Therapeutic Targets in Inflammatory Bowel Disease), and by regulatory authorities within the context of clinical trials [30]. The primary objective of our study was to investigate the relationship between the presence and copy number of CMV, detected by tissue rtPCR, and the degree of endoscopic activity in patients with moderate to severe UC. To achieve this aim, we employed the Mayo and Rachmilewitz scoring systems, which have been in use for nearly three decades and are well familiar to clinicians [29]. In our study, we evaluated the effect of tissue CMV PCR presence on the degree of endoscopic activation using various statistical methods. The average Mayo clinical score in tissue CMV positive patients was found to be 8.7, while in CMV negative patients, this value was 7.6. This difference is statistically significant. Additionally, the Rachmilewitz EAI score was determined to be 8.6 in CMV positive patients and 7.4 in CMV negative patients. This difference was also statistically significant. Correlation analysis demonstrated a positive correlation between the tissue CMV copy number and both the Mayo and Rachmilewitz scores. Our findings indicate that there is a higher disease activity in patients who are CMV tissue PCR positive. On the other hand, to understand whether high activity indices serve as indicators of tissue CMV positivity, logistic regression analysis was performed; however, it was observed that neither the elevation of the Mayo score nor the Rachmilewitz score had a significant effect on predicting tissue CMV positivity. The literature contains a limited number of studies examining CMV positivity and endoscopic findings during ulcerative colitis flare-ups [31,32,33]. Suzuki et al. reported that the sensitivity of irregular ulceration for detecting positive CMV was 100%, while the specificity of wide mucosal defects was 95%. Additionally, punched-out and longitudinal ulcerations demonstrated relatively high sensitivity and specificity, exceeding 70% for each, and Yang et al. also reported similar findings [31,33]. In the literature, no study has been found that directly examines both CMV tissue DNA positivity and the degree of endoscopic activity as in our study. Only one study involving 25 patients with CMV PCR positivity in tissue reported endoscopic activity scores before and after treatment. In that study, the median Rachmilewitz score prior to treatment was found to be 10 (7–12), similar to our findings. Additionally, no significant difference was observed between the endoscopic activity scores during the flare and after treatment in these patients [6].
Cytomegalovirus (CMV) infection has been implicated as a contributing factor in the relapse of IBD [33]. This association has been predominantly noted in patients with UC, particularly among those undergoing high-dose corticosteroid therapy [34]. In our study, logistic regression analysis was conducted to predict tissue CMV PCR positivity, which demonstrated no association with anti-TNF use. However, steroid use within the preceding three months was found to be significantly associated with tissue CMV DNA positivity, resulting in a 12-fold increase in risk.
In contemporary medical research, sufficient diagnostic criteria related to CMV copy numbers for confirming the presence of CMV infection in ulcerative colitis or in colon tissue under immunosuppressive conditions have yet to be developed [19]. In our study, cases were classified as CMV-positive solely based on tissue CMV DNA copy numbers exceeding 250. Among the 41 patients meeting this criterion, histopathological examination revealed features consistent with classic CMV infection in only 3 cases. Although a copy number of 250 or higher in tissue, coupled with clinical findings, is often deemed sufficient for diagnostic purposes by certain guidelines, numerous sources continue to prioritize histopathological evidence for confirming CMV positivity [35,36,37]. Consequently, to reflect this nuance, we employed the term "patients with tissue CMV DNA positivity" rather than "patients with CMV infection" in our analysis.
Our study has several limitations. Primarily, it was designed as a single centered, retrospective cohort study. A total of 110 patients were included; this sample size may limit the generalizability of the results and could have reduced the statistical power of the study. Furthermore, its single-center nature hinders the extrapolation of findings to a broader population. Endoscopic scoring systems such as the Mayo and Rachmilewitz scores, which rely on the endoscopist's observations and expertise, may introduce potential bias despite the established validity of these systems. Finally, the limited number of similar studies in the literature poses challenges in comparatively validating our findings.
In conclusion, this study highlights the significant association between CMV presence and the severity of UC, underscoring the importance of proactive diagnostic and therapeutic strategies. Our analysis demonstrated that CMV DNA positivity in tissue samples is associated with higher Modified Mayo Clinical and Rachmilewitz endoscopic activity scores, elevated erythrocyte sedimentation rates, and increased serum CMV levels, with a 12-fold greater risk observed in patients with recent steroid use. Clinically, routine CMV screening, particularly in steroid-refractory cases, appears crucial for enabling timely antiviral treatment and improving patient outcomes. Although limitations such as the retrospective design, single-center nature, and small sample size may restrict the generalizability of our findings, future research should involve larger, multi-center prospective studies to better elucidate the interaction between CMV infection and UC progression.
Author Contributions
OK: Conceptualized and performed the primary research activities and led the writing of the manuscript. HE: Managed the arrangement of statistical data and contributed to the writing process. EI: Handled data collection and processing. UA and MU: Provided assistance with manuscript writing and performed critical revisions. AB: Conducted critical revisions and performed the final review.
Conflicts of Interest and funding statement
There is no conflict of interest and funding related to manuscript.
Ethical statement
This study was reviewed and approved by the Ondokuz Mayıs University Clinical Research Ethics Committee at 04.04.2024 (application number: 2024000169-1; file number: 2024/169). All procedures were conducted in accordance with the ethical guidelines and regulations set forth by the committee, ensuring the protection of participants' rights, privacy, and welfare. Informed consent was obtained from all participants prior to their involvement, and the study adhered to relevant national and international ethical standards, including the Declaration of Helsinki.
Data Availability Statement
The data can be found in the data repository of the Gastroenterology Department at Ondokuz Mayıs University Faculty of Medicine. If you wish to request access to the data, please contact us at abektas@omu.edu.tr or ufukavcioglu@yahoo.com, or please visit https://hastane.omu.edu.tr/tr/bolumlerimiz/boeluemler-liste/gastroenteroloji .
References
- Yeh, P.-J.; Wu, R.-C.; Chen, C.-L.; Chiu, C.-T.; Lai, M.-W.; Chen, C.-C.; Chiu, C.-H.; Pan, Y.-B.; Lin, W.-R.; Le, P.-H. Cytomegalovirus diseases of the gastrointestinal tract in immunocompetent patients: A narrative review. Viruses 2024, 16, 346. [Google Scholar] [CrossRef] [PubMed]
- Domènech, E.; Vega, R.; Ojanguren, I.; Hernández, Á.; Garcia-Planella, E.; Bernal, I.; Rosinach, M.; Boix, J.; Cabré, E.; Gassull, M.A. Cytomegalovirus infection in ulcerative colitis: a prospective, comparative study on prevalence and diagnostic strategy. Inflammatory bowel diseases 2008, 14, 1373–1379. [Google Scholar] [CrossRef] [PubMed]
- Mourad, F.H.; Hashash, J.G.; Kariyawasam, V.C.; Leong, R.W. Ulcerative colitis and cytomegalovirus infection: from A to Z. Journal of Crohn's and Colitis 2020, 14, 1162–1171. [Google Scholar] [CrossRef]
- Yeh, P.-J.; Wu, R.-C.; Chiu, C.-T.; Lai, M.-W.; Chen, C.-M.; Pan, Y.-B.; Su, M.-Y.; Kuo, C.-J.; Lin, W.-R.; Le, P.-H. Cytomegalovirus diseases of the gastrointestinal tract. Viruses 2022, 14, 352. [Google Scholar] [CrossRef]
- Sager, K.; Alam, S.; Bond, A.; Chinnappan, L.; Probert, C. cytomegalovirus and inflammatory bowel disease. Alimentary pharmacology & therapeutics 2015, 41, 725–733. [Google Scholar]
- Ozdemir, B.; Atay, A.; Kayhan, M.A.; Ozin, Y.O.; Gokce, D.T.; Altunsoy, A.; Guner, R. Tissue quantitative RT–PCR test for diagnostic significance of cytomegalovirus infection in patients with inflammatory bowel disease and treatment response: Cytomegalovirus infection in patients with inflammatory bowel disease. Medicine 2023, 102, e34463. [Google Scholar] [CrossRef]
- Lawlor, G.; Moss, A.C. Cytomegalovirus in inflammatory bowel disease: pathogen or innocent bystander? Inflammatory bowel diseases 2010, 16, 1620–1627. [Google Scholar] [CrossRef]
- Jentzer, A.; Veyrard, P.; Roblin, X.; Saint-Sardos, P.; Rochereau, N.; Paul, S.; Bourlet, T.; Pozzetto, B.; Pillet, S. Cytomegalovirus and inflammatory bowel diseases (IBD) with a special focus on the link with ulcerative colitis (UC). Microorganisms 2020, 8, 1078. [Google Scholar] [CrossRef]
- Esen, S.; Saglik, I.; Dolar, E.; Cesur, S.; Ugras, N.; Agca, H.; Merdan, O.; Ener, B. Diagnostic utility of cytomegalovirus (CMV) DNA quantitation in ulcerative colitis. Viruses 2024, 16, 691. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Yamakawa, T.; Hirano, T.; Kazama, T.; Hirayama, D.; Wagatsuma, K.; Nakase, H. Current diagnostic and therapeutic approaches to cytomegalovirus infections in ulcerative colitis patients based on clinical and basic research data. International Journal of Molecular Sciences 2020, 21, 2438. [Google Scholar] [CrossRef]
- Hazır-Konya, H.; Avkan-Oğuz, V.; Akpınar, H.; Sağol, Ö.; Sayıner, A. Investigation of cytomegalovirus in intestinal tissue in a country with high CMV seroprevalence. The Turkish Journal of Gastroenterology 2021, 32, 123. [Google Scholar] [CrossRef] [PubMed]
- Magro, F.; Gionchetti, P.; Eliakim, R.; Ardizzone, S.; Armuzzi, A.; Barreiro-de Acosta, M.; Burisch, J.; Gecse, K.B.; Hart, A.L.; Hindryckx, P. Third European evidence-based consensus on diagnosis and management of ulcerative colitis. Part 1: definitions, diagnosis, extra-intestinal manifestations, pregnancy, cancer surveillance, surgery, and ileo-anal pouch disorders. Journal of Crohn's and Colitis 2017, 11, 649–670. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, A.; Ford, A.C. Poor correlation between patient-reported and endoscopic components of the Mayo score in ulcerative colitis. Gastroenterology 2016, 150, 1037–1039. [Google Scholar] [CrossRef] [PubMed]
- Rachmilewitz, D. Coated mesalazine (5-aminosalicylic acid) versus sulphasalazine in the treatment of active ulcerative colitis: a randomised trial. British Medical Journal 1989, 298, 82–86. [Google Scholar] [CrossRef]
- Ikeya, K.; Hanai, H.; Sugimoto, K.; Osawa, S.; Kawasaki, S.; Iida, T.; Maruyama, Y.; Watanabe, F. The ulcerative colitis endoscopic index of severity more accurately reflects clinical outcomes and long-term prognosis than the Mayo endoscopic score. Journal of Crohn's and Colitis 2016, 10, 286–295. [Google Scholar] [CrossRef]
- Schoepfer, A.M.; Beglinger, C.; Straumann, A.; Trummler, M.; Renzulli, P.; Seibold, F. Ulcerative colitis: correlation of the Rachmilewitz endoscopic activity index with fecal calprotectin, clinical activity, C-reactive protein, and blood leukocytes. Inflammatory bowel diseases 2009, 15, 1851–1858. [Google Scholar] [CrossRef]
- Levin, A.; Yaari, S.; Stoff, R.; Caplan, O.; Wolf, D.G.; Israeli, E. Diagnosis of cytomegalovirus infection during exacerbation of ulcerative colitis. Digestion 2017, 96, 142–148. [Google Scholar] [CrossRef]
- Lee, H.-S.; Park, S.H.; Kim, S.-H.; Kim, J.; Choi, J.; Lee, H.J.; Kim, W.S.; Lee, J.-M.; Kwak, M.S.; Hwang, S.W. Risk factors and clinical outcomes associated with cytomegalovirus colitis in patients with acute severe ulcerative colitis. Inflammatory bowel diseases 2016, 22, 912–918. [Google Scholar] [CrossRef]
- Park, S.C.; Jeen, Y.M.; Jeen, Y.T. Approach to cytomegalovirus infections in patients with ulcerative colitis. The Korean journal of internal medicine 2017, 32, 383. [Google Scholar] [CrossRef]
- Pillet, S.; Roblin, X.; Cornillon, J.; Mariat, C.; Pozzetto, B. Quantification of cytomegalovirus viral load. Expert review of anti-infective therapy 2014, 12, 193–210. [Google Scholar] [CrossRef]
- Römkens, T.E.; Bulte, G.J.; Nissen, L.H.; Drenth, J.P. Cytomegalovirus in inflammatory bowel disease: A systematic review. World journal of gastroenterology 2016, 22, 1321. [Google Scholar] [CrossRef]
- Wang, W.; Chen, X.; Pan, J.; Zhang, X.; Zhang, L. Epstein–Barr virus and human cytomegalovirus infection in intestinal mucosa of Chinese patients with inflammatory bowel disease. Frontiers in Microbiology 2022, 13, 915453. [Google Scholar] [CrossRef]
- Ren, K.; Yong, C.; Wang, Y.; Wei, H.; Zhao, K.; He, B.; Cui, M.; Chen, Y.; Wang, J. Cytomegalovirus Pneumonia in Inflammatory Bowel Disease: Literature Review and Clinical Recommendations. Infection and Drug Resistance 2023, 6195–6208. [Google Scholar] [CrossRef]
- Kandiel, A.; Lashner, B. Cytomegalovirus colitis complicating inflammatory bowel disease. Official journal of the American College of Gastroenterology| ACG 2006, 101, 2857–2865. [Google Scholar] [CrossRef]
- Liu, C.-C.; Ji, S.; Ding, Y.; Zhou, L.; Liu, X.; Li, W. Cytomegalovirus infection and steroid-refractory inflammatory bowel disease: possible relationship from an updated meta-analysis. Irish Journal of Medical Science (1971-) 2018, 187, 935–942. [Google Scholar] [CrossRef]
- Sánchez de Medina, F.; Romero-Calvo, I.; Mascaraque, C.; Martínez-Augustin, O. Intestinal inflammation and mucosal barrier function. Inflammatory bowel diseases 2014, 20, 2394–2404. [Google Scholar] [CrossRef]
- Saez, A.; Herrero-Fernandez, B.; Gomez-Bris, R.; Sánchez-Martinez, H.; Gonzalez-Granado, J.M. Pathophysiology of inflammatory bowel disease: innate immune system. International Journal of Molecular Sciences 2023, 24, 1526. [Google Scholar] [CrossRef] [PubMed]
- Altunal, L.; Ozel, A.; Ak, C. Cytomegalovirus reactivation in ulcerative colitis patients: Early indicators. Nigerian Journal of Clinical Practice 2023, 26, 765–770. [Google Scholar] [CrossRef] [PubMed]
- Yao, H.; Najarian, K.; Gryak, J.; Bishu, S.; Rice, M.D.; Waljee, A.K.; Wilkins, H.J.; Stidham, R.W. Fully automated endoscopic disease activity assessment in ulcerative colitis. Gastrointestinal Endoscopy 2021, 93, 728–736. e721. [Google Scholar] [CrossRef] [PubMed]
- Peyrin-Biroulet, L.; Sandborn, W.; Sands, B.E.; Reinisch, W.; Bemelman, W.; Bryant, R.V.; D'Haens, G.; Dotan, I.; Dubinsky, M.; Feagan, B. Selecting therapeutic targets in inflammatory bowel disease (STRIDE): determining therapeutic goals for treat-to-target. Official journal of the American College of Gastroenterology| ACG 2015, 110, 1324–1338. [Google Scholar] [CrossRef]
- Yang, H.; Zhou, W.; Lv, H.; Wu, D.; Feng, Y.; Shu, H.; Jin, M.; Hu, L.; Wang, Q.; Wu, D. The association between CMV viremia or endoscopic features and histopathological characteristics of CMV colitis in patients with underlying ulcerative colitis. Inflammatory bowel diseases 2017, 23, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, Y.; Ando, T.; Hirooka, Y.; Watanabe, O.; Miyahara, R.; Nakamura, M.; Yamamura, T.; Goto, H. Characteristic endoscopic findings and risk factors for cytomegalovirus-associated colitis in patients with active ulcerative colitis. World journal of gastrointestinal endoscopy 2016, 8, 301. [Google Scholar] [CrossRef]
- Shieh, A.C.; Guler, E.; Tirumani, S.H.; Dumot, J.; Ramaiya, N.H. Clinical, imaging, endoscopic findings, and management of patients with CMV colitis: a single-institute experience. Emergency radiology 2020, 27, 277–284. [Google Scholar] [CrossRef]
- Suzuki, H.; Kato, J.; Kuriyama, M.; Hiraoka, S.; Kuwaki, K.; Yamamoto, K. Specific endoscopic features of ulcerative colitis complicated by cytomegalovirus infection. World journal of gastroenterology: WJG 2010, 16, 1245. [Google Scholar] [CrossRef]
- Tun, G.S.; Raza, M.; Hale, M.F.; Lobo, A.J. Polymerase chain reaction for detection of mucosal cytomegalovirus infection in patients with acute ulcerative colitis. Annals of gastroenterology 2018, 32, 81. [Google Scholar] [CrossRef]
- Erürker Öztürk, T.; KIYICI, M.; Gülten, M.; DOLAR, M.; Gürel, S.; NAK, S.; Eren, F. Importance of using tissue PCR to diagnose CMV colitis in ulcerative colitis. Dicle Tıp Dergisi 2023, 50. [Google Scholar] [CrossRef]
- Jena, A.; Mishra, S.; Singh, A.K.; Sekar, A.; Sharma, V. Cytomegalovirus in ulcerative colitis: an evidence-based approach to diagnosis and treatment. Expert Review of Gastroenterology & Hepatology 2022, 16, 109–120. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of the participants; CMV PCR: cytomegalovirus polymerase chain reaction.
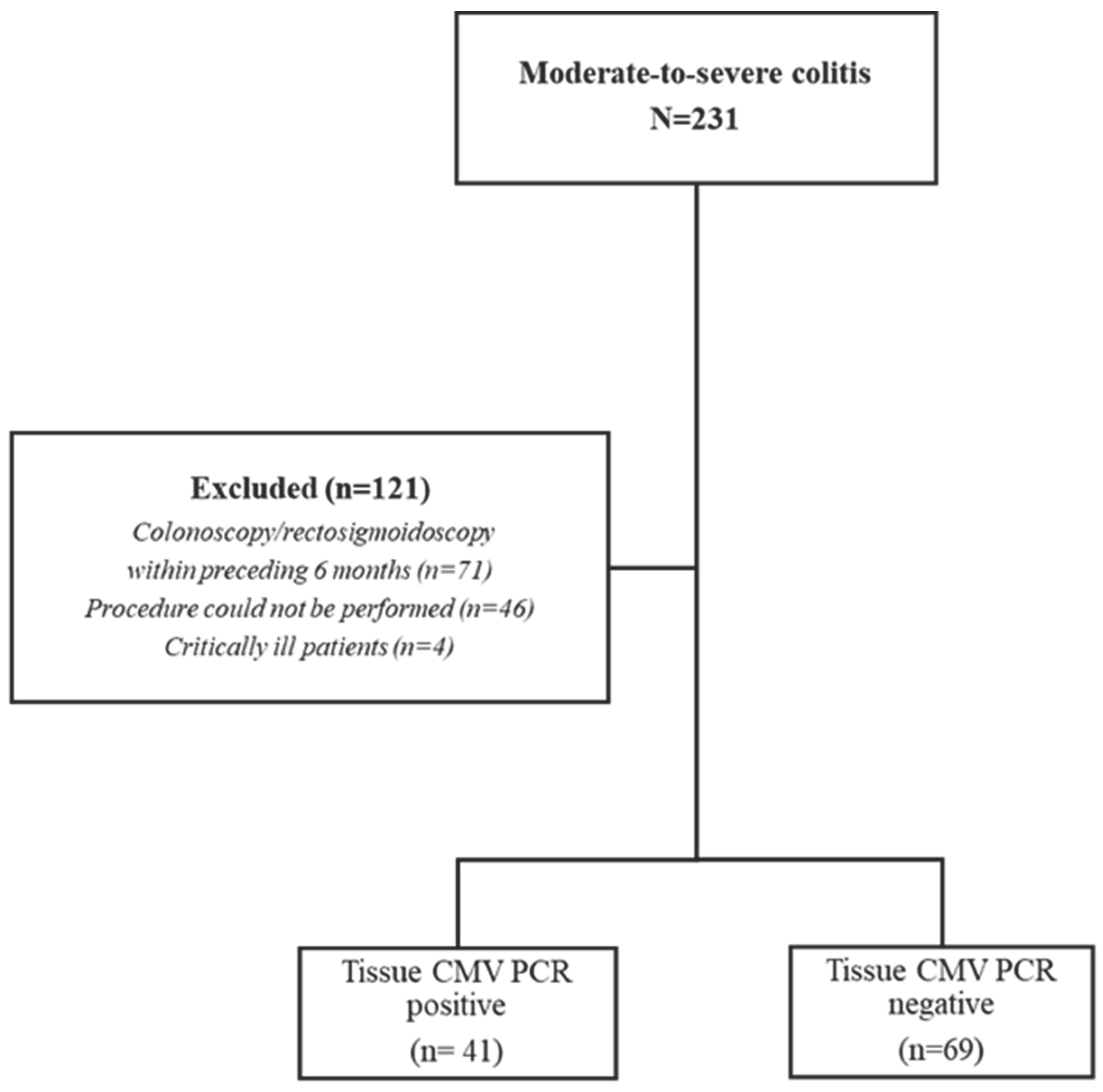

Table 1.
Modified Mayo Score and Rachmilewitz Endoscopic Activity Index.
| Modified Mayo Score | ||||
| Score | 0 | 1 | 2 | 3 |
| Stool frequency | Normal |
1-2 more than normal | 3-4 more than normal | 4-5 more than normal |
| Rectal bleed | No bleed |
Streaks of blood with stool less than half the time | Obvious blood most of the time | Blood alone |
| Endoscopic findings | Normal | Mild | Moderate | Severe |
| Physician Global Assessment | Normal | Mild | Moderate | Severe |
| Rachmilewitz Endoscopic Activity Index | ||||
| Score | 0 | 2 | 4 | |
| Granulation scattering reflected light | No | Yes | ||
| Vascular appereance | Normal | Faded/disturbed | Completely absent | |
| Fragility of mucosa | None | Contact bleeding | Spontaneous bleeding | |
| Mucosal damage (mucus, fibrin, exudate, erosion, ulcer) | None | Slight | Pronounced | |
Table 2.
Comparison of some parameters between CMV + and CMV - active ulcerative colitis patients.
| CMV positive UC (n=41) |
CMV negative UC (n=69) |
p value | |
| Age (year) | 45.6±19.9 | 45.9±117.53.9 | 0.93 |
|
Female, n (%) Male, n (%) |
21 (42%) 20 (58%) |
21 (31%) 48 (69%) |
0.001* 0.8 |
| Diagnosis age | 40.9±19.8 | 37.6±17.9 | 0.38 |
| Follow up time (weeks) | 59.4±60.7 | 88±72.2 | 0.02 |
| WBC | 10.1±10.8 | 9.6±4.2 | 0.8 |
| CRP | 39.9±44.6 | 33.8±51 | 0.5 |
| ESR (sedim) | 54.3±28.9 | 42.8±28.3 | 0.04 |
| Daily defecation | 10.1±6 | 9.5±7.1 | 0.6 |
| CMV PCR serum | 878.9±2473 | 71.4±316.6 | 0.008 |
|
Rachmilewitz EAI |
8.6±2.6 | 7.4±3.1 |
0.03 |
|
Mayo Score |
8.7±2.4 |
7.6±3.5 |
0.02 |
Abbreviations: WBC: white blood cell, ESR: erythrocyte sedimatation rate.
Table 3.
Correlation analysis of CMV-PCR tissue copy number with different parameters (non-parametric Spearman).
Table 3.
Correlation analysis of CMV-PCR tissue copy number with different parameters (non-parametric Spearman).
| Correlation | r | p |
| WBC | -0.16 | 0.09 |
| Daily defecation | 0.1 | 0.29 |
| Age | 0.01 | 0.8 |
| Diagnosis age | 0.1 | 0.27 |
| CRP | 0.13 | 0.16 |
| Sedim | 0.22 | 0.01 |
| CMV PCR serum | 0.37 | 0.0001 |
| Mayo Score | 0.18 | 0.05 |
| Rachmilewitz Endoscopic Activity Index | 0.25 | 0.008 |
Table 4.
Logistic regression analysis for prediction of the CMV PCR positivity in tissues.
| B | Wald | p | Exp(B) | 95% C.I.for EXP(B) | |||
| Lower | Upper | ||||||
| Results | Mayo Score | -0.15 | 0.51 | 0.47 | 0.85 | 0.55 | 1.31 |
| Rachmilewitz | 0.18 | 0.59 | 0.44 | 1.2 | 0.75 | 1.91 | |
| Anti TNF usage | -0.7 | 0.34 | 0.55 | 0.49 | 0.04 | 5.18 | |
| Steroid usage in last 3 months | 2.5 | 4.73 | 0.03 | 12.1 | 1.2 | 116.03 | |
| CRP | -.003 | 0.11 | 0.73 | 0.99 | 0.97 | 1.01 | |
| Sedim | 0.01 | 0.54 | 0.46 | 1.01 | 0.97 | 1.05 | |
| Constant | -4.7 | 4.63 | 0.03 | 0.009 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



