
Submitted:
04 July 2025
Posted:
07 July 2025
You are already at the latest version
Abstract
Background: Knee osteoarthritis is highly prevalent and leads to disabling chronic pain, often worsened by overweight and sedentary lifestyles. Objective: To present the DESTRA protocol, a novel, evidence-based, integrated approach to improve pain, functionality, and metabolic health. Methods: Description of six pillars combining an-ti-inflammatory nutrition, targeted exercise, sleep hygiene, injectable therapies, mi-cronutrient supplementation, and behavioral adherence strategies. Results (expected): Improvement in pain (VAS, WOMAC), functional scores, body composition, and pa-tient autonomy. Conclusion: DESTRA may represent a reproducible, scalable, and safe framework for treating knee osteoarthritis in overweight patients.
Keywords:
knee osteoarthritis
; chronic pain
; multidisciplinary protocol
; weight management
; injectable therapies
; orthobiologics
; sleep hygiene
; functional rehabilitation
1. Introduction
Osteoarthritis (OA) of the knee is one of the most prevalent musculoskeletal conditions worldwide, with a major impact on quality of life, work capacity, and social participation [1,2]. Knee OA is particularly relevant among middle-aged women with overweight or obesity, combining joint degeneration with systemic inflammatory alterations that perpetuate pain and functional decline [1,3]. Chronic pain in knee OA is a multidimensional phenomenon involving not only nociceptive mechanisms, but also central sensitization, biomechanical overload, low-grade systemic inflammation, and behavioral factors [4,5].
Current standard treatments for knee OA — including isolated exercise programs, anti-inflammatory medications, intra-articular injections, or weight loss interventions — often fail to achieve lasting symptom relief or sustainable functional recovery [6,7]. Fragmented approaches ignore the complex interactions between metabolism, inflammation, sleep quality, micronutrient status, and movement capacity, all of which influence pain modulation and tissue healing [8,9].
Emerging evidence shows that obesity, metabolic syndrome, and poor sleep patterns exacerbate inflammatory pathways, increase pain perception, and reduce adherence to rehabilitation interventions [9,10,11]. Furthermore, dietary patterns, gut microbiota alterations, and vitamin deficiencies may negatively affect articular cartilage homeostasis and the neuromodulatory balance involved in chronic pain processing [12,13]. Thus, addressing knee OA from an integrated, multidomain perspective appears essential to restore patients’ function and autonomy.
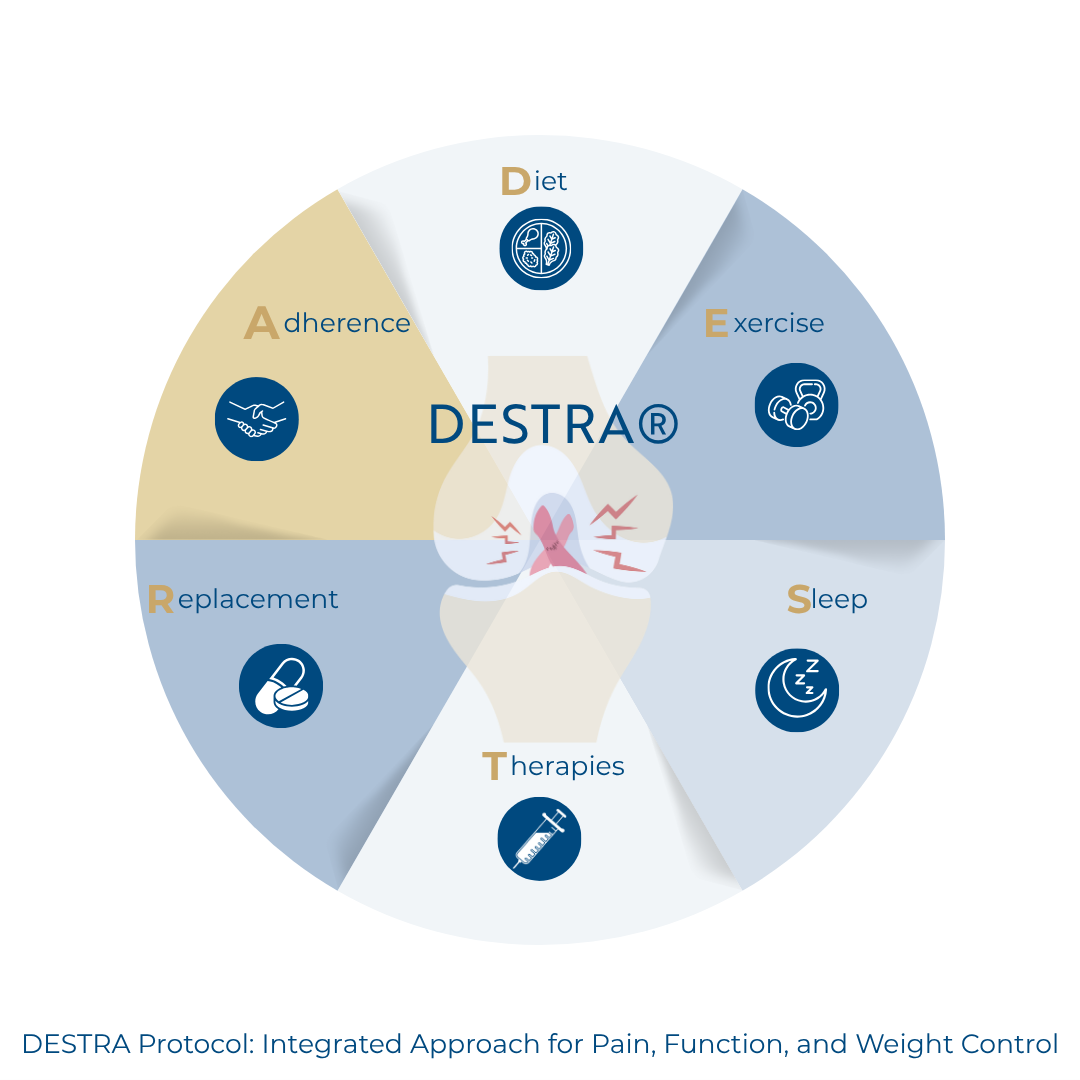
Inspired by comprehensive frameworks such as the SDIMMMER protocol in regenerative medicine — which systematically maps metabolic, nutritional, and lifestyle factors to optimize outcomes [14] — the DESTRA protocol was developed to deliver a structured, replicable, and evidence-based approach to pain management and functional rehabilitation in knee osteoarthritis. DESTRA combines six pillars: (1) anti-inflammatory nutrition, (2) pain-adapted and progressive exercise, (3) sleep hygiene, (4) injectable and orthobiologic therapies including GLP-1/GIP analogs and biologicals like BMA, PRF, and PRP, (5) micronutrient supplementation, and (6) behavioral adherence strategies.
The DESTRA protocol is designed to move beyond mere symptom suppression. Its goal is to create a therapeutic ecosystem that supports weight control, improves tissue repair capacity, rebalances pro- and anti-inflammatory mediators, and promotes active patient participation in the treatment journey. We hypothesize that this integrative framework can help mitigate pain, improve joint function, and sustain long-term results in overweight patients with knee osteoarthritis who are not immediate surgical candidates.
Accordingly, this article aims to describe the rationale, structure, and implementation pathways of the DESTRA protocol, providing a standardized model to be tested in future clinical trials and disseminated in evidence-based orthopedic practice.
2. Materials and Methods
2.1. Study Framework and Target Population
The DESTRA protocol was designed as a practical, integrative, and replicable framework to address chronic pain, functional loss, and metabolic dysfunction in patients with knee osteoarthritis who are overweight or obese, and not immediate surgical candidates. Its target population includes adults, predominantly women aged 38 to 65 years, with symptomatic knee OA and body mass index above 27 kg/m², experiencing functional limitations and persistent pain for more than three months.
The DESTRA method combines six interdependent pillars aiming to optimize joint physiology, modulate pain, and promote weight reduction through a personalized, multidisciplinary approach. The pillars are designed to address both local articular dysfunction and systemic contributors such as low-grade inflammation, sleep disturbance, and micronutrient deficiencies.
2.2. DESTRA Protocol Components
A schematic overview of the DESTRA pillars is provided in Figure 1 (to be designed), and summarized in Table 1 (to be designed). Each pillar is described below.
Pillar 1: Anti-Inflammatory Nutrition
- Individualized anti-inflammatory dietary plans prioritizing foods rich in omega-3 fatty acids, antioxidants, fiber, and phytonutrients.
- Reduction of ultra-processed foods, added sugars, saturated fats, and pro-inflammatory dietary patterns.
- Incorporation of Mediterranean or plant-forward strategies tailored to patient preferences and cultural context.
- Nutritional counseling to ensure adherence and manage expectations.
- The goal is to reduce systemic inflammation, improve gut microbiota balance, and support weight loss, indirectly modulating pain pathways.
Pillar 2: Pain-Adapted and Progressive Exercise
- Functional exercises supervised with attention to pain thresholds, joint protection, and neuromuscular control.
- Progressive loading respecting arthrogenic inhibition and central sensitization phenomena.
- Low-impact aerobic activities, aquatic therapy, and lower limb strength training.
- Strategies to prevent kinesiophobia and restore proprioception.
- Periodic reassessments to personalize progressions based on pain, functional capacity, and tolerance.
Pillar 3: Sleep Hygiene
- Assessment of sleep patterns using validated tools.
- Sleep hygiene education with consistent sleep–wake times, reduced evening screen exposure, and improved bedroom conditions.
- Screening for sleep disorders requiring referral.
- Emphasis on sleep’s role in regulating pain perception, cortisol balance, and metabolic health.
Pillar 4: Injectable and Orthobiologic Therapies
- GLP-1 and GIP receptor analogs to support weight loss and decrease inflammation.
- Orthobiologics (Viscosupplementation with hyaluronic acid, BMA, PRF, iPRF, PRP) following clinical indications and performed with ultrasound guidance.
Pillar 5: Micronutrient Supplementation
- Assessment of nutritional and vitamin status (vitamin D, B complex, iron, magnesium, zinc, among others).
- Laboratory testing according to evidence-based guidelines.
- Personalized supplementation plans to correct deficiencies that may contribute to fatigue, mood changes, and delayed tissue repair.
Pillar 6: Behavioral and Adherence Strategies
- Use of motivational interviewing and coaching techniques to encourage lifestyle changes.
- Educational materials and support groups for empowerment and engagement.
- Periodic follow-up consultations to track progress and overcome barriers.
- Application of gamification principles (e.g., goal setting, rewards, progress visualization) to promote sustained adherence.
2.3. Implementation Roadmap
The DESTRA protocol is intended to be delivered over a minimum of 12 weeks, with multidisciplinary evaluations at baseline, mid-point (6 weeks), and final assessment (12 weeks). Clinicians may adapt the timeline based on individual progress and tolerability.
Key process markers to monitor include:
- pain scores (e.g., VAS, WOMAC)
- functional status (e.g., KOOS, timed up-and-go test)
- weight and body composition
- sleep quality metrics
- biochemical markers (inflammatory profile, vitamin levels)
Electronic medical records and standardized forms will document adherence, adverse events, and clinical evolution to ensure reproducibility and future research opportunities.
3. Discussion
Knee osteoarthritis represents a complex interplay between mechanical joint degeneration, systemic low-grade inflammation, neuroplastic pain sensitization, and behavioral or lifestyle determinants. Patients with overweight or obesity are disproportionately affected due to increased joint overload, higher levels of inflammatory adipokines, and a greater prevalence of sleep disorders, micronutrient deficiencies, and sedentary behaviors [1,2,3,4].
Fragmented approaches frequently fail to deliver sustainable symptom relief or functional recovery. Chronic pain may persist despite intra-articular injections if systemic inflammation and poor muscle conditioning are not addressed [5,6,7].
The DESTRA protocol was developed to respond to these multidimensional challenges. By combining anti-inflammatory nutrition, progressive exercise, sleep hygiene, micronutrient optimization, advanced injectable therapies including GLP-1/GIP analogs, and behavioral strategies, DESTRA creates a therapeutic ecosystem that promotes joint homeostasis and patient autonomy.
Its modular and flexible structure facilitates adaptation to individual needs and real-world clinical resources, while standard outcome tracking supports future prospective validation. Challenges such as resource allocation and interdisciplinary training may be anticipated, but the benefits of integrating these pillars justify efforts toward implementation and evaluation in randomized studies.
4. Conclusions
The DESTRA protocol provides an innovative and replicable model to manage pain, dysfunction, and excess weight in patients with knee osteoarthritis. By addressing multiple interrelated domains, DESTRA goes beyond symptomatic relief, encouraging sustainable changes in joint health and patient behavior..
References
- Katz JN, Arant KR, Loeser RF. Diagnosis and treatment of hip and knee osteoarthritis: a review. JAMA. 2021;325(6):568–578. [CrossRef]
- Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745–1759. [CrossRef]
- Bliddal H, Leeds AR, Christensen R. Osteoarthritis, obesity and weight loss: evidence, hypotheses and horizons — a scoping review. Obes Rev. 2014;15(7):578–586. [CrossRef]
- Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis Cartilage. 2019;27(11):1578–1589. [CrossRef]
- Kittelson AJ, George SZ. Physical therapy for knee osteoarthritis: why does it fail, and what might change that? J Orthop Sports Phys Ther. 2022;52(1):3–7. [CrossRef]
- McAlindon TE, Bannuru RR, Sullivan MC, et al. OARSI guidelines for the non-surgical management of knee osteoarthritis, update 2022. Osteoarthritis Cartilage. 2022;30(4):383–406. [CrossRef]
- Fernandes L, Hagen KB, Bijlsma JW, et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann Rheum Dis. 2013;72(7):1125–1135. [CrossRef]
- Whibley D, AlKandari N, Kristensen K, et al. Sleep and pain: a systematic review of the bidirectional relationship. Pain. 2019;160(8):1699–1704. [CrossRef]
- Koyanagi A, Garin N, Olaya B, et al. Chronic conditions and sleep problems among adults aged 50 years or over in nine countries: a multicountry study. PLoS One. 2014;9(12):e114742. [CrossRef]
- Gallo VS, Jean Y, Lohrmann D. Impact of weight loss interventions on knee osteoarthritis: a systematic review. Orthop Nurs. 2020;39(2):94–100. [CrossRef]
- Nicholas MK, Molloy AR, Tonkin LE, Beeston L. Manage chronic pain: do more, not less. Pain Rep. 2022;7(4):e1017. [CrossRef]
- Ramires LC, Santos GS, da Fonseca LF, et al. The association between gut microbiota and osteoarthritis: does the disease begin in the gut? Int J Mol Sci. 2022;23(3):1494. [CrossRef]
- Charles-Messance H, Mitchelson KAJ, De Marco Castro E, Sheedy FJ, Roche HM. Regulating metabolic inflammation by nutritional modulation. J Allergy Clin Immunol. 2020;146(4):706–720. [CrossRef]
- Lana JF, Lana JVB, Santos GS, et al. SDIMMMER: a proposed clinical approach to optimize cellular physiology in regenerative medicine. Life. 2024;14(10):1287. [CrossRef]
Figure 1.
DESTRA Protocol Flowchart.
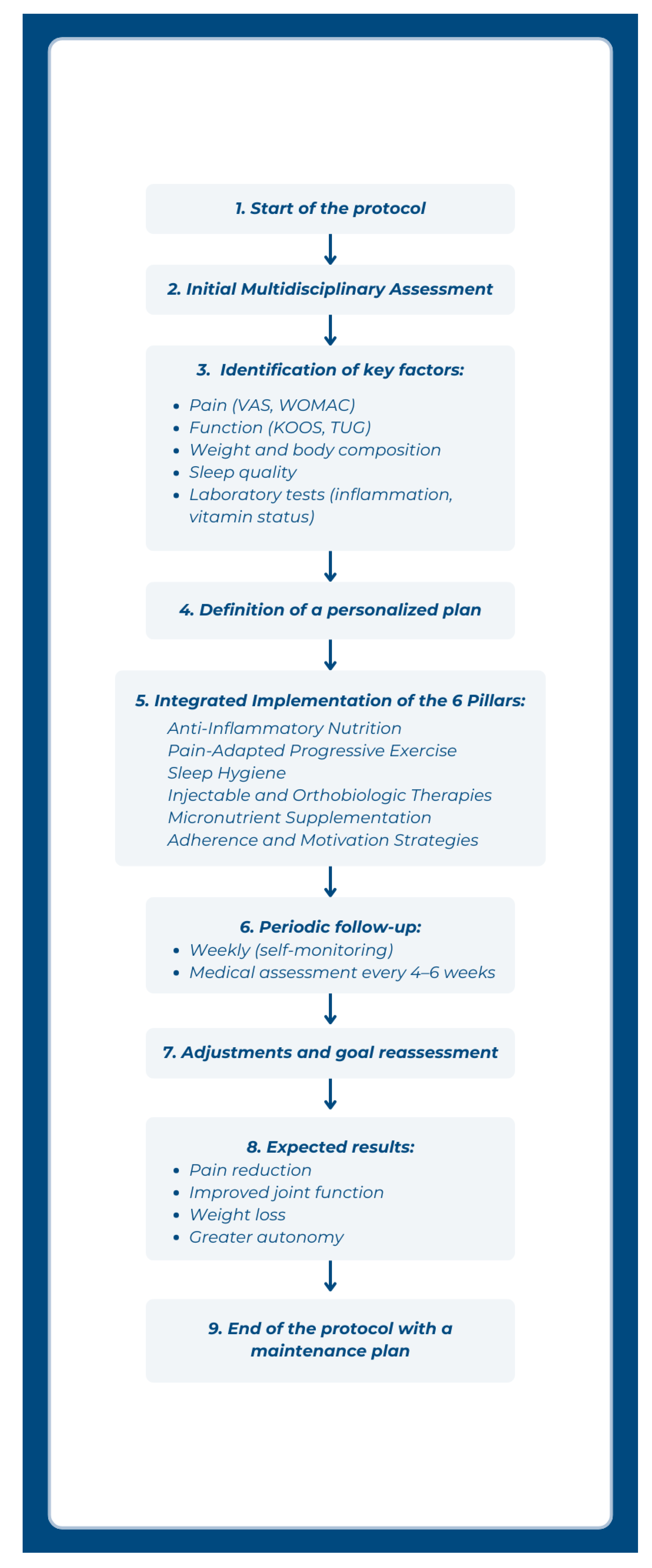

Table 1.
DESTRA Protocol Overview.
| Pillar | Description | Key Objectives |
|---|---|---|
| 1. Anti-Inflammatory Nutrition | Personalized meal plans emphasizing omega-3, antioxidants, fiber, and low glycemic load; avoidance of ultra-processed foods and pro-inflammatory items | Reduce systemic inflammation; support microbiota; promote weight loss |
| 2. Pain-Adapted Progressive Exercise | Structured functional exercise with progressive loading respecting pain thresholds; includes aerobic, strength, and proprioceptive training | Restore joint function; improve neuromuscular control; counteract kinesiophobia |
| 3. Sleep Hygiene | Assessment and education on sleep patterns; establishing consistent habits and environmental adjustments | Optimize hormonal balance; reduce pain sensitization; improve recovery |
| 4. Injectable and Orthobiologic Therapies | Viscosupplementation, GLP-1/GIP analogs, orthobiologics (BMA, PRF, iPRF, PRP) | Enhance pain control; promote joint homeostasis; stimulate regeneration |
| 5. Micronutrient Supplementation | Targeted correction of deficiencies (vitamin D, B complex, magnesium, iron, zinc) | Improve tissue repair; support mood and energy; modulate inflammation |
| 6. Behavioral and Adherence Strategies | Coaching, motivational interviewing, patient education, support groups, gamification | Sustain engagement; reinforce autonomy; improve treatment adherence |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



