
Submitted:
04 July 2025
Posted:
07 July 2025
You are already at the latest version
Abstract
Background/Objectives: Preschool hearing screening is justified by the risk of late-onset hearing loss, the high prevalence of otitis media with effusion in school-aged children, and the critical timing just before children begin formal reading and learn to write. This study describes the results of the annual preschool hearing screening program in Campo Maior from 2007 to 2025 (nineteen years) and correlates the audiological referral to the otoscopy findings by the otolaryngologists. Methodology: Retrospective study using clinical records from nineteen years of preschool hearing screening. Results: Screening identified 310 children (29% of 1,068 screened) requiring referral to an ENT specialist. Of the 217 referred children evaluated by ENT, 198 (91,2%) had confirmed pathology or healthcare needs of medical intervention. A statistically significant positive association (r=0.254, p< 0,05) existed between abnormal otoscopy findings and Type B or C2 tympanograms (versus Type A or C1). Hearing loss occurring with Type A tympanograms (0.8% unilaterally, 0.3% bilaterally) may suggest sensorineural hearing loss. Conclusion: This study reinforces the importance of universal preschool audiological screening for all children, particularly for children facing geographic barriers to healthcare. Community-based interventions facilitated by social solidarity associations can play a crucial role in mitigating healthcare access disparities across populations.
Keywords:
hearing screening
; tympanogram
; children
; preschool
1. Introduction
As children grow and develop, they acquire skills that go beyond understanding and producing oral language. They also develop abilities related to written language, such as recognizing the concept of written words, engaging in attentive listening during read-aloud activities, and becoming familiar with vocabulary and syntactic structures that are less common in spoken language. Additionally, the practice of sharing ideas contributes to this process. Together, these experiences support children's literacy development and effective language use [1,2,3].
Most reading acquisition theories converge in recognizing that it develops through phases, including the pre-alphabetic phase, the partially alphabetic phase, the alphabetic phase, and the consolidated alphabetic phase [4,5].
The child must begin by learning how the orthographic system of their language relates to the phonemes that make up speech [5,6].
The quality of a child's hearing is of special relevance in learning to read, especially during the partially alphabetic phase and the alphabetic phase. In the partially alphabetic phase, because, in addition to knowing the name and sound of the letters, the child must acquire the ability to detect the different phonemes that constitute the word (phonemic awareness). In the alphabetic phase, because the child must acquire the ability to decode, that is, they must acquire knowledge of the grapheme-phoneme correspondences that enable the connection between orthography and the auditory lexicon stored in their memory [4,5].
The way one interprets what is heard, especially speech, depends on the knowledge about what is being said, the complexity of the information, and the ability to use context to fill in what was not heard, so that the information makes sense [7].
In schools, children spend most of their time listening; in other words, they listen to learn, and paradoxically, they even listen to learn how to read. It is known that acoustic conditions influence speech perception, particularly that of words, linguistic units whose identification is hindered by a continuous sound that masks their boundaries. If this is true for adults, it is even more evident in children, as humans only reach adult-level performance in adverse acoustic conditions at the ages of 12–14 years [8,9].
Classrooms are intended for learning. Most learning is mediated through speech. Based on these two statements, we can conclude that students need to hear the information being transmitted to them clearly. This clarity will depend on the student’s hearing and the acoustic conditions of the classroom [7,8].
Because the auditory system of children is not fully mature, and some low-intensity phonemes are emitted below 20 dB in rapid speech, and children are still learning the relationships between different speech sounds and therefore need redundancies to hear them clearly and create solid perceptions and representations, several authors argue that normal hearing in children is below 16 dB rather than 21 dB as in adults. They also state that children are continuously learning new concepts, and their hearing serves as the foundation for this learning [10,11,12].
The detection or even prevention of hearing loss and possible psychosocial disorders associated with it should be carried out during the neonatal, preschool, and school periods, aiming at the earliest possible identification of auditory function alterations and thus minimizing their consequences for the individual's school and socio-professional inclusion [13].
Although newborn hearing screening in Portugal is fully implemented, World Health Organization reports the almost double incidence of hearing loss in preschool age, comparing with the perinatal period, due to middle ear pathology and also the appearance of late onset permanent hearing loss [13].
Around the age of five, hearing loss, whether conductive or sensorineural, often goes unnoticed because it may be unilateral and/or fluctuating or because its onset was late due to genetic, traumatic, infectious, or other causes, and it did not significantly affect the acquisition of speech and language [14,15].
On the other hand, various studies indicate there is a peak prevalence of middle ear pathologies at the age of five, notably otitis media with effusion [16].
The diagnosis of otitis media with effusion can be incidental or stem from discomfort and behavioural changes in the child. It is rarely identifiable by parents or educators as it can be unilateral and usually does not present inflammatory signs or symptoms. The average hearing loss associated with these conditions ranges from 25–30 dB. Additionally, 90% of children experience at least one episode of otitis media with effusion before starting school [17,18].
The late onset hearing loss, the prevalence of otitis media with effusion, and the proximity to the start of formal learning of reading and writing justify the implementation of pre-school screening [15].
The goals of a pre-school hearing screening program include, early and reliable detection and identification of hearing problems; Adequate access to professional care for all children suspected of having a hearing loss or auditory processing disorders including children whose parent(s) or other caregiver(s) do not have the resources to pay for the care [14,15,19].
The primary target population for pre-school hearing screening is all children aged 4–7 years and is not oriented to those children with diagnosed hearing loss and who are under current professional management of the loss [15].
This screening will produce over referrals. For the benefit of children undergoing hearing screenings, false positives are preferable to false negatives [15].
Regarding the tests to be used in screening, the different recommendations mention otoscopy, tympanometry, and a hearing screening, which are quick tests and well accepted by children [13,14,20].
The otoscopy checks for the presence or absence of cerumen or any impossibility of performing tympanometry and/or hearing screening (e.g., transtympanic tube) [14].
A tympanogram is a test that indirectly assesses the compliance of the tympanic membrane and the pressure within the middle ear. Its sensitivity (ability to detect middle ears with effusion – type B tympanogram), according to studies, ranges from 49% to 99%, while its specificity (ability to diagnose normal middle ears – type A tympanogram) is approximately 100% in most studies [21].
Hearing screening, using the hear/not-hear criterion, aims to increase sensitivity in detecting audiological changes/hearing impairment not only at the middle ear level but also at the inner ear level. The hear/not-hear criterion can be defined as the child's ability to respond to the recommended screening levels at the tested frequencies in both ears [13]. According to several authors, the tested frequencies are generally 1, 2, and 4 kHz, with 0.5 kHz being tested when the tympanogram is not used in screening and environmental noise allows it [13,22].
Access to health care should be a universal right and for the World Health Organization, the economic and social circumstances of individuals should not condition their maximum health potential [23].
In Portugal, according to the Health Regulatory Authority, regardless of the quality in which the user accesses health care or the entity responsible for its financing or charges, the constituent legislator enshrined in the Constitution of the Portuguese Republic basic principles of a democratic regime, which must be respected: the principles of universality and equality. Portugal enshrines in Article 64 of the Constitution of the Portuguese Republic the fundamental right to health protection. Healthcare services must be provided close to the place of residence to reduce costs associated with time spent and travel undertaken. In certain geographical locations characterized by isolation and remoteness, there must be local collaboration between health institutions, healthcare professionals, local authorities, and the social sector, always ensuring the technical requirements that guarantee the effectiveness of the services provided [24,25].
Coração Delta, a Social Solidarity association whose mission is to drive and promote projects and programs in the areas of education, special education, health, and social intervention, stands as one of the excellent examples of collaboration between the social sector and health institutions and professionals in an inland municipality of Portugal, Campo Maior [26].
Campo Maior is a Portuguese border town located in the Alto Alentejo region, in the district of Portalegre. In 2023, the resident population was 7,916 inhabitants, of which 1,125 were aged between 0 and 14 years [27]. Access to Audiology and Otolaryngology services is extremely limited in that region, leading to delayed referrals for specialized care.
The present study aims to describe the results of the annual preschool audiological screening conducted in the Municipality of Campo Maior from 2007 to 2025 (nineteen years) and to correlate the audiological referral to the otoscopy findings by the otolaryngologists.
2. Materials and Methods
The audiological screening of the children was conducted, in all instances, in the presence of their legal guardian or a duly authorized representative. Currently, legal guardians sign an informed consent form authorizing the transfer of data to the Coração Delta Association.
This retrospective study using clinical records from nineteen years of preschool hearing screening study was carried out in compliance with established ethical principles and in full accordance with the General Data Protection Regulation (GDPR – Regulation (EU) 2016/679). Anonymity and confidentiality of all participant data were strictly maintained, in line with best practices for research involving human subjects and the Declaration of Helsinki.
2.1. Participants
Over a nineteen-year period, a total of 1,068 children from the Municipality of Campo Maior were screened prior to entering the first grade of primary school in the upcoming academic year. Among the screened children, 534 were male and 534 were female. Most of the children, specifically 828 (77.5%), were aged five, while the remaining 240 (22.5%) were aged six.
2.2. Procedure
Annually, Coração Delta staff contact all preschools in the municipality of Campo Maior to identify children transitioning to the first grade of primary education. After identification, the respective legal guardians are contacted and invited to express their interest in their child’s participation in the screening. Once the interest is confirmed, the legal guardians are informed about the date, time, and location of the screening. To facilitate family participation, the screening has always been scheduled for Saturdays, ensuring greater availability for involvement.
The screening was conducted annually, in March (53,2%), April (27,6%), May (8,2%), or June (11,0%), by a team consisting of two professors and four students from the Audiology Bachelor's degree program at the Coimbra Health School and two Otolaryngologists (ENT). The evaluations took place in two rooms prepared to ensure minimal ambient noise.
Each year, two otoscopes, two impedance meters, and two audiometers, all properly calibrated, were used.
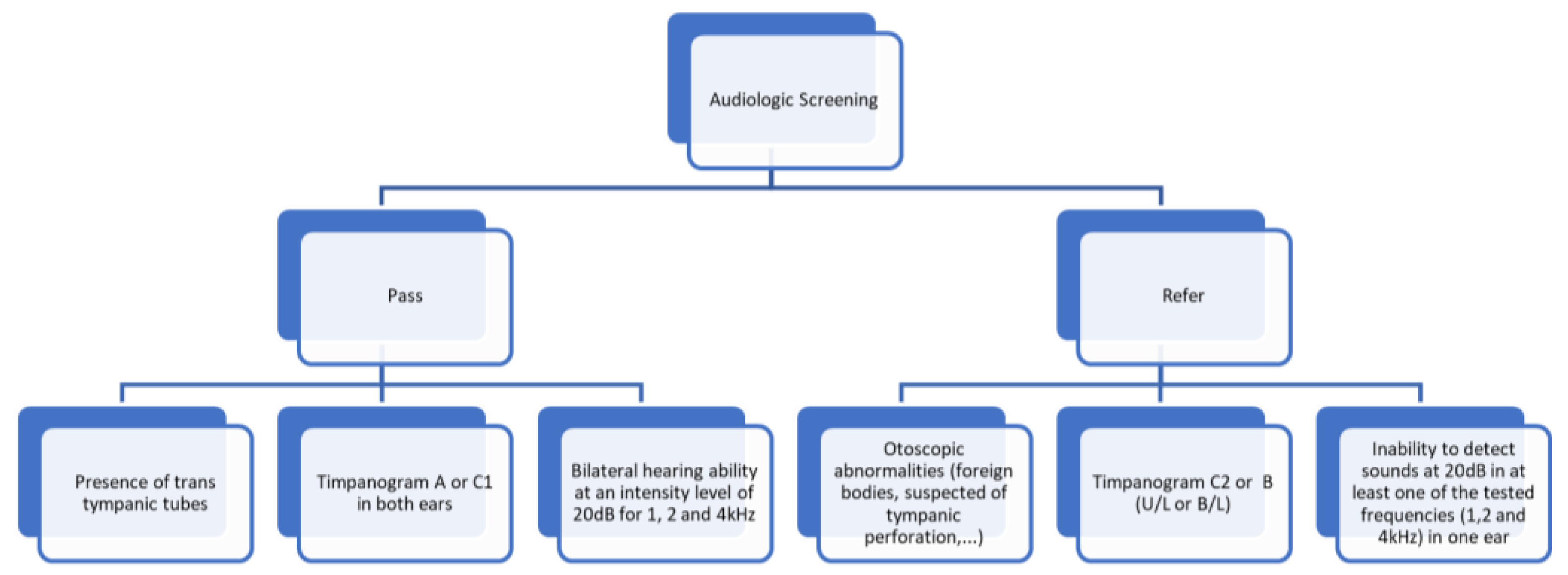
Children were screened according to the following protocol: otoscopy, tympanogram, and hearing screening at an intensity of 20 dB in 1, 2 and 4kHz.
The child successfully passed the screening under the following conditions:
- -
- The presence of trans tympanic tubes, accompanied by a recommendation to continue consulting their Otorhinolaryngologist (ENT).
- -
- A tympanogram results classified as type A or C1 in both ears.
- -
- Bilateral hearing ability at an intensity level of 20dB for frequencies of 1, 2, and 4 kHz.
The child was referred for further evaluation based on the following criteria:
- -
- Observed alterations during otoscopy, such as the presence of foreign bodies or suspected perforations.
- -
- A tympanogram results classified as type C2 or B in one or both ears.
- -
- Inability to detect sounds at 20dB in at least one of the tested frequencies in one ear.
Figure 1.
Screening Protocol.
The referred children were promptly seen by an ENT specialist at the screening site, upon their request.
2.3. Statistical Analysis
Descriptive statistics summarized discrete variables as frequencies and percentages. Spearman's correlation assessed associations between variables, with statistical significance defined as p < 0.05.
3. Results
3.1. Screening Results
Among the 1,068 children who were screened, 310 (29%) did not pass the screening and were subsequently referred to an ENT specialist. Of those referred, unilateral changes were observed in 137 children (12.8%), while 173 children exhibited bilateral changes (Figure 2). The most common findings were alterations in the tympanogram, occurring unilaterally in 104 children (9.7%) and bilaterally in 81 children (7.6%) (Table 1). 7.7% of the children presented with a type B tympanogram in both ears. Hearing loss was associated with the presence of a type B tympanogram, occurring in the right ear in 49.1%, 29.8%, and 39.5% of cases at 1, 2, and 4 kHz, respectively. In the left ear, it occurred in 44.6%, 31.5%, and 38.7% of cases at 1, 2, and 4 kHz, respectively. Tympanostomy tubes were present in only 12 (1.2%) of the screened children.
In 2021, due to Covid-19, 87 children from 2020 and 2021 were screened. That year, only 11.5% of the children did not pass the screening. Up until that moment, the referral percentage was 29.5%. After 2021, the referral percentage increased to 34.2%. In 2022, there was a significant increase in referrals, with 38.9% of the children being referred.
3.2. Medical Referral
The ENT observation at the time of the screening process was conducted for 217 children, representing 70% of the referrals from the screening and early treatment was ensured whenever possible (wax removal, toilette of middle ear discharge, prescription of medical treatment). All the children confirmed to have otoscopic or audiological findings were referred to a formal hospital evaluation. Of these, 123 children (56.7%), were directed to a follow-up evaluation by the ENT specialty, while only 19 children (8.8%) did not receive any type of medical referral (Table 2).
3.3. Association of Medical Otoscopy Findings with Tympanogram Types
Table 3 shows the relationship between the tympanogram results of 434 ears and the otoscopy performed by an ENT physician. Among the ears examined, 204 were considered normal and 109 had otitis media with effusion. Additionally, one ear was identified with a perforation and 29 with Eustachian tube dysfunction. Type B and Type C2 tympanograms were the ones with the highest percentage of associated pathology (80.9% for Type B and 46.5% for Type C2).
A statistically significant positive association was observed between abnormal medical otoscopy findings and Type B or C2 tympanograms versus Type A or C1 tympanograms (r = 0.254; p < 0.001; N = 434) and between abnormal medical otoscopy findings and Type B tympanograms versus Type A tympanograms (r = 0.566; p < 0.001; N = 215).
A statistically significant positive association was too observed between abnormal medical otoscopy findings and Type B versus Type A or C1 or C2 tympanograms (r = 0.456; p < 0.001; N = 434)
4. Discussion
Among 1,068 children screened, 310 (29%) failed the screening and were referred for ENT evaluation on site. Subsequent assessment by ENT specialists of 217 referred children confirmed 198 (91,2%) cases with pathology or healthcare needs requiring medical intervention.
Abnormal medical otoscopy findings significantly predict Type B/C2 tympanograms (vs. Type A/C1), with a moderate positive correlation (r=0.254). This confirms tympanometry's sensitivity to middle ear effusion and other otoscopically detectable pathologies. These findings are consistent with those reported by Anwar et al. (2016), who observed a tympanogram sensitivity of 85.85% and a specificity of 72.22% in the identification of otitis media with effusion. Similarly, Fiellau-Nikolajsen (1980) reported a sensitivity of 91% and a specificity of 84%, further reinforcing the diagnostic utility of tympanometry in the assessment of middle ear conditions [28,29].
Regarding hearing loss, it is more frequently associated with type B tympanograms than with type A. In fact, a type B tympanogram is indicative of otitis media with effusion, and the literature reports that this condition can cause mild to moderate hearing loss [17,18].
Hearing loss associated with a Type A tympanogram (0.8% unilateral and 0.3% bilateral) is likely indicative of sensorineural hearing loss, potentially of mild to moderate severity, which had not yet been detected by the ages of 5 or 6. These findings suggest a higher prevalence of sensorineural hearing loss compared to that reported by Brodie et al. (2022), who identified a prevalence of 0.2% in a screening of children aged 2 to 6 years, and by Lü et al. (2011), who reported a prevalence of 0.75 per 1000 (95% CI: 0.38–1.12) in children aged 3 to 6 years [30,31].
These findings confirm that preschool hearing screening is justified, given that: the incidence of late onset hearing loss, the high prevalence of otitis media with effusion, and its critical importance preceding formal reading and writing learning. Most identifiable conditions can be resolved through medical or surgical intervention, which typically restores hearing thresholds to normal levels. Early identification is fundamental for establishing proper foundational literacy skills – the foundation of all lifelong learning.
As a study limitation, we can mention the absence of data on the follow-up of these children, whether at the medical level (medication and surgery), or at the audiological level with confirmation of hearing loss, specifically the suspected cases of sensorineural hearing loss. However, the authors of this study found that, often with financial support from Coração Delta, most of the referred children received a correct and timely response to their problem.
This study confirms the importance of preschool screening for all children, especially those from more vulnerable populations, such as those geographically distant from healthcare services. Community intervention promoted by social solidarity associations can play a crucial role in mitigating disparities in access to healthcare services among diverse populations.
Author Contributions
Conceptualization, M.S. and L.M.; methodology, M.S.; formal analysis, CR and LM and M.S.; investigation, C.M.; resources, D.G. and M.B. and M.S.; data curation, J.P and J.T. and J.M and M.P. and M.S.; writing—original draft preparation, L.M. and C.R. and M.S.; writing—review and editing, C.R. and M.S.; visualization, L.M.; supervision, M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Declaration of generative AI and AI-assisted technologies in the writing process: During the preparation of this work the author(s) used Copilot in order to translate. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Davidse, Neeltje J., et al. Cognitive and Environmental Predictors of Early Literacy Skills. Read Writ. 2011, Vol. 24, pp. 395-412. [CrossRef]
- Rayner, Keith, et al. How Psychological Science Informs the Teaching of Reading. Psychological Science in the Public Interest. 2001, Vol. 2, pp. 31-74. [CrossRef]
- Hand, E D, Lonigan, C J e Puranik, C S. Prediction of kindergarten and first-grade reading skills: Unique contributions of preschool writing and early-literacy skills. Reading and Writing. 2024, Vol. 37, 1, pp. 25-48. [CrossRef]
- Ehri, Linnea C. Development of Sight Word Reading: Phases and Findings. [ed.] Margaret J. Snowling e Charles Hulme. The Science of Reading: a Handbook. Singapore : Blackwell Publishing, 2007, pp. 135-154.
- Share, D. L. Blueprint for a universal theory of learning to read: The Combinatorial Model. Blueprint for a universal theory of learning to read: The Combinatorial Model. 2025, Vol. 60, 2. [CrossRef]
- Furgoni, A, Martin, C D e Stoehr, A. A cross linguistic study on orthographic influence during auditory word recognition. Sci Rep . 2025, Vol. 15, p. 8374. [CrossRef]
- Boothroyd, Arthur. Speech Perception in the Classroom. [autor do livro] Joseph J. Smaldino e Carol Flexer. Handbook of Acoustic Accessibility - Best Practices for Listening, Learning, and Literacy in the Classroom. New York - Stuttgart : Thieme, 2012, pp. 18-33.
- Klatte, Maria, Wegner, Marlis e Hellbruck, Jurgen. Noise in School Environment and Cognitive Perfomance in Elementary School Children. Part B - Cognitive Psychological Studies. Forum Acusticum 2005. [Online] 2005. [Citação: 15 de Maio de 2010.] http://intellagence.eu.com/acoustic2008/cd1/data/fa2005-budapest/paper/682-0.pdf.
- Gordon, K R e Grieco-Calub, T M. Children build their vocabularies in noisy environments: The necessity of a cross-disciplinary approach to understand word learning. Wiley Interdiscip Rev Cogn Sci. Mar-Apr de 2024, Vol. 15, 2, p. e 1671. [CrossRef]
- McFadden, Brittany e Pittman, Andrea. Effect of minimal hearing loss on children’s ability to multitask in quiet and in noise. Lang Speech Hear Serv Sch. July de 2008, Vol. 39 (3), pp. 342–351. [CrossRef]
- Porter, Heather e Bess, Fred H. Children with Unilateral Hearing Loss. 2011, pp. 175-192.
- Tharpe, Anne Marie. Permanent Minimal and Mild Bilateral Hearing Loss in Children: Implications and Outcomes. [autor do livro] Richard Seewald e Anne Marie Tharpe. Comprehensive Handbook of Pediatric Audiology. University of Western Ontario, London, Ontario, Canada : Plural Publishing, Inc., 2011, pp. 193-202.
- World Health Organization. Hearing screening: considerations for implementation. 2021. ISBN 978-92-4-003276-7 (electronic version), ISBN 978-92-4-003277-4 (print version).
- American Speech-Language-Hearing Association. Panel on Audiologic Assessment. Guidelines for Audiologic Screening. Rockville, MD : The Association, 1997.
- Skarżyński, Henryk e Piotrowska, Anna . Screening for Pre-School and School-Age Hearing Problems: European Consensus Statement. International Journal of Pediatric Otorhinolaryngology. 2012, Vol. 76, 1, pp. 120–121. [CrossRef]
- Zielhuis, G. A., Rach, G. H. e Broek, Van P. den. The Occurrence of Otitis Media with Effusion in Dutch Pre-School Children. Clinical Otolaryngology & Allied Sciences. Apr. de 1990, Vol. 15, pp. 147-153. [CrossRef]
- Rosenfeld, R M, et al. Clinical Practice Guideline: Otitis Media with Effusion (Update). Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2016, Vol. 154, 1 Suppl, pp. S1–S41.
- Vanneste , P e Page , C. Otitis media with effusion in children: Pathophysiology, diagnosis, and treatment. A review. J Otol. Jun de 2019, Vol. 14, 2, pp. 33-39. [CrossRef]
- Mackey, A R, Persson, A e Uhlén, I. Pre-school hearing screening is necessary to detect childhood hearing loss after the newborn period: a study exploring risk factors, additional disabilities, and referral pathways. International journal of audiology . 2025, Vol. 64, 1, pp. 80-88. [CrossRef]
- American Academy of Audiology. Clinical Practice Guidelines: Childhood Hearing Screening. 2011.
- Hunter, Lisa L e Blankenship, Chelsea M. Middle ear measurement. [autor do livro] Anne Marie Tharpe e Richard Seewald. Comprehensive Handbook of Pediatric Audiology. 2. s.l. : Plural Publishing, 2017, pp. 449-473.
- Dows, M e Northern, J. Hearing in Children. 6. London : Williams&Wilkins, 2014.
- Dahlgren G, Whitehead M. Concepts and Principles for Tackling Social Inequities in Health: Levelling Up Part I and Part II. Copenhagen: WHO Regional Office for Europe, 2006.
- Entidade Reguladora da Saúde. Direito à proteção da saúde – O Serviço Nacional de Saúde – Universalidade. Porto, Portugal : s.n., 2021.
- Furtado, Cláudia e Pereira, João. Equidade e Acesso aos Cuidados de Saúde- Documento de Trabalho. Escola Nacional de Saúde Pública, Universidade Nova de Lisboa : s.n., 2010.
- Coração Delta - Associação de Solidariedade Social. Coração Delta - Associação de Solidariedade Social. Coração Delta - Associação de Solidariedade Social. [Online] 2 de junho de 2025. https://www.coracaodelta.com.
- Instituto Nacional de Estatística. Instituto Nacional de Estatística. Instituto Nacional de Estatística. [Online] 2 de junho de 2025. https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_main.
- Anwar, K, et al. Otitis media with effusion: Accuracy of tympanometry in detecting fluid in the middle ears of children at myringotomies. Pak J Med Sci. doi: 10.12669/pjms.322.9009, Mar-Apr de 2016, Vol. 32, 2, pp. 466-70. [CrossRef]
- Fiellau-Nikolajsen, M. Tympanometry and middle ear effusion: a cohort-study in three-year-old children. International journal of pediatric otorhinolaryngology. 1980, Vol. 2, 1, pp. 39-49. [CrossRef]
- Brodie, K D, et al. Outcomes of an Early Childhood Hearing Screening Program in a Low-Income Setting. JAMA otolaryngology-- head & neck surgery. 2022, Vol. 148, 4, pp. 326–332. [CrossRef]
- Lü, J, et al. Screening for delayed-onset hearing loss in preschool children who previously passed the newborn hearing screening. International journal of pediatric otorhinolaryngology. 2011, Vol. 75, 8, pp. 1045–1049. [CrossRef]
Figure 2.
Screening results.


Table 1.
Test results.
| N | % | |
|---|---|---|
| U/L Tympanogram | 104 | 9,7 |
| U/L Hearing Screening | 9 | 0,8 |
| U/L Tympanogram + Hearing Screening | 24 | 2,2 |
| B/L Tympanogram | 81 | 7,6 |
| B/L Hearing Screening | 3 | 0,3 |
| B/L Tympanogram+Hearing Screening (U/L) | 31 | 2,9 |
| B/L Tympanogram+Hearing Screening (B/L) | 51 | 4,8 |
| B/L Hearing Screening+Tympanogram (U/L) | 7 | 0,7 |
Legend: U/L – unilateral; B/L - bilateral.
Table 2.
Medical referral.
| N | % | |
|---|---|---|
| ENT Consultation | 123 | 56.7 |
| Monitoring | 30 | 13.8 |
| Medication | 20 | 9.2 |
| Discharge | 19 | 8.8 |
| Other Consultation(s) | 16 | 7.4 |
| Wax Removal | 5 | 2.3 |
| Speech Therapy | 4 | 1.8 |
| Total | 217 | 100.0 |
Table 3.
Otoscopy and Tympanogram Results: Comparative Analysis.
| Medical Otoscopy | Type A (N = 42) | Type C1 (N = 60) | Type C2 (N = 159) | Type B (N = 173) |
|---|---|---|---|---|
| Normal | 36 (86.4%) | 50 (83.3%) | 85 (53.5%) | 33 (19.1%) |
| Otitis Media with Effusion | 2 (4.8%) | 3 (5.0%) | 13 (8.2%) | 91 (52.6%) |
| Acute Otitis Media | 1 (2.4%) | 0 (0.0%) | 3 (1.9%) | 8 (4.6%) |
| Tympanic Depression | 0 (0.0%) | 3 (5.0%) | 23 (14.5%) | 11 (6.4%) |
| Cerumen | 2 (4.8%) | 2 (3.3%) | 11 (6.9%) | 22 (12.7%) |
| Tympanosclerosis | 0 (0.0%) | 0 (0.0%) | 2 (1.3%) | 0 (0.0%) |
| Tympanic Perforation | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (0.6%) |
| Eustachian Tube Dysfunction | 1 (2.4%) | 2 (3.3%) | 19 (11.9%) | 7 (4.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



