
Submitted:
03 July 2025
Posted:
04 July 2025
You are already at the latest version
Abstract
Background/Objectives: Inflammation-based markers have emerged as potential prognostic tools in hepatocellular carcinoma (HCC), but comparative data with classical prognostic factors in untreated HCC are limited. This study aimed to evaluate and compare the prognostic performance of inflammatory and conventional markers using Harrell’s concordance index (C-index). Methods: This retrospective study included 250 patients with untreated HCC. Prognostic variables included age, BCLC stage, Milan criteria, MELD score, AFP, albumin, Charlson comorbidity index, and the inflammation-based markers neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR), systemic inflammation response index (SIRI), and systemic immune-inflammation index (SIII). Survival was analyzed using Cox regression. Predictive performance was assessed using the C-index, Akaike information criterion (AIC), and likelihood ratio tests. Results: Among classical markers, BCLC showed the highest predictive performance (C-index: 0.717), while NLR ranked highest among inflammatory markers (C-index: 0.640), above the MELD score and Milan criteria. In multivariate analysis, NLR ≥2.3 remained an independent predictor of overall survival (HR: 1.859; 95% CI: 1.321–2.615; p < 0.001), along with BCLC stage, albumin, Charlson index, and Milan criteria. Including NLR in the model modestly improved the C-index (from 0.781 to 0.794) but significantly enhanced model fit (Δ–2LL = 12.605; p < 0.001; lower AIC). Conclusions: NLR is an accessible, cost-effective, and independent prognostic marker for overall survival in untreated HCC. It shows discriminative power comparable to or greater than most conventional predictors and may complement classical stratification tools for HCC.
Keywords:
hepatocarcinoma
; prognostic factors
; neutrophil-to-lymphocyte ratio
1. Introduction
According to GLOBOCAN 2022 estimates, liver cancer accounted for approximately 865,000 new cases and over 750,000 deaths globally, ranking as the third leading cause of cancer-related mortality—following lung and colorectal cancers—and the sixth most commonly diagnosed malignancy [1]. Hepatocellular carcinoma (HCC) represents the predominant histological subtype, comprising 75–85% of all liver cancer cases. Chronic infection with hepatitis B or C virus remains a major etiological factor, contributing to an estimated 21–55% of cases worldwide [2]. Additional risk factors include exposure to aflatoxins, excessive alcohol intake, metabolic conditions such as obesity and diabetes, tobacco use, non-alcoholic fatty liver disease (NAFLD), as well as male sex and older age[3]. The relative importance of these risk factors varies by geographic region.
The American Association for the Study of Liver Diseases indicates that cirrhosis, regardless of its etiology, is the main risk factor, and that the epidemiological transition is shifting the burden toward older individuals with metabolic risk factors, although viral hepatitis remains relevant in endemic areas[4]. Moreover, the incidence in women is increasing in relation to NAFLD/NASH, approaching that of men within this subgroup, although the overall burden remains higher in males[5].
Although it has improved in recent decades, the 5-year overall survival rate for patients still remains around 22%[6].
The prognosis of patients with hepatocellular carcinoma is determined by tumor-related characteristics, liver function, the patient’s general condition, and serum biomarkers [7,8]. Among these, the most relevant and consistently reported factors in the literature include: advanced age, male sex, and alcoholic liver disease [9]; the Barcelona Clinic Liver Cancer (BCLC) staging system [10]; the Child-Pugh classification, Model for End-Stage Liver Disease (MELD) score[11]; elevated serum alpha-fetoprotein (AFP) levels [12]; the Milan criteria [13], and albumin[14].
It is worth noting that, despite the recent publication of several studies on the subject[15,16,17,18], inflammatory biomarkers are not commonly included in the classical lists of prognostic factors for hepatocellular carcinoma[7,13,19] o son mencionados muy superficialmente[20]. Nevertheless, there is increasing evidence that the presence of systemic inflammation in cancer patients, including those with HCC, is associated with poorer prognosis in terms of disease progression and survival [21,22].
In this sense, several hematological parameters derived from a simple peripheral blood sample have been proposed as inflammatory prognostic markers: neutrophil-to-lymphocyte ratio (NLR)[23], platelet-to-lymphocyte ratio (PLR)[24], monocyte-to-lymphocyte ratio (MLR)[25], serum C-reactive protein[26], C-reactive proteine to albumine ratio[27] , Systemic Inflammation Response Index (SIRI)[28], Systemic Immune-inflammation Index (SIII)[29], and others more complex as modified Glasgow Prognostic Score[30]. Recent studies have highlighted that these biomarkers may be helpful in revealing the underlying inflammatory state. Moreover, most of them, to a lesser or greater degree, have been reported as good prognostic markers in a large number of neoplasms, including untreated [12,15,31,32,33,34] and treated HCC[35,36].
However, few studies have directly compared the prognostic utility of inflammatory biomarkers, either against one another or in relation to established prognostic factors, in patients with hepatocellular carcinoma. This study aimed to evaluate and compare the prognostic value for overall survival of the most accessible inflammatory markers (NLR, PLR, MLR, SIRI, and SII), adjusting for conventional prognostic variables as potential confounders in a well-defined cohort of patients with untreated HCC
2. Materials and Methods
2.1. Design and Study Population
An observational retrospective study was conducted on a cohort of 250 consecutive non-selected patients diagnosed with hepatocellular carcinoma between 2011 y 2020 in our institution. The setting was a tertiary care hospital that serves a population of approximately 400,000 inhabitants. Exclusion criteria included those patients whose clinical records or follow-up was incomplete or not available. The number and characteristics of these excluded patients were not collected.
2.2. Management of the Patients
All patients included in the study were diagnosed with HCC through one or two dynamic imaging radiological tests (liver contrast-enhanced ultrasound, contrast-enhanced computed tomography and/or Magnetic Resonance Imaging with contrast) or a clear histological or cytological diagnosis of hepatocellular carcinoma. Histological samples were obtained by means of percutaneous fine needle aspiration cytology, core needle biopsy and/or resection specimens.
Once the diagnosis was established, staging was determined according to the Barcelona Clinic Liver Cancer (BCLC) classification[10]. Following these criteria, treatment was then proposed. In early stages BCLC 0-A was treated with curative intent by liver resection, ablation or liver transplantation, while in the other more advanced stages the intent was no longer curative and treatment was applied by transcatheter arterial chemoembolization (TACE), systemic treatment or simply palliative measures.
2.3. Follow-Up
The patients were entered into the study with the date of the day on which the first definitive treatment was applied after diagnosis. All of them were followed up by periodic visits to the hospital outpatient clinic. In the long term, it was possible to determine whether the patient was still alive or had died and the date of exitus by consulting the hospital and/or primary care databases. The overall mean follow-up time for the entire cohort was 20.4 months, while for surviving patients it was 48.4 months.
2.4. Study Variables
Clinical data were extracted from patients’ medical records, entered into a database, and subsequently analyzed. The following variables were evaluated:
Baseline characteristics. Age and sex at the time of the diagnosis.
Comorbidity. The Charlson Comorbidity Index was calculated for each patient. This index includes 19 medical conditions, each weighted from 1 to 6 points, with total scores ranging from 0 to 37, depending on the presence and severity of comorbid diseases. A score of 0 indicates the absence of comorbidities. Generally, scores of 1–2 indicate low comorbidity, 3–4 moderate comorbidity, and scores greater than 4 indicate high comorbidity[37]. In this study, the index was not adjusted for age or for the presence of AIDS, as no patients in the cohort had this condition.
Assessment of Underlying Liver Disease. The etiology of liver disease (alcohol-related, viral, mixed, or other), Child–Pugh classification, and the MELD score [38] were determined and recorded.
Laboratory data. At the time of diagnosis, the following laboratory values were recorded: absolute neutrophil, lymphocyte, monocyte, and platelet counts; and alpha-fetoprotein (AFP) levels.
Inflammation-Based Prognostic Markers (Pretreatment). The neutrophil-to-lymphocyte ratio was calculated by dividing the absolute neutrophil count by the absolute lymphocyte count (N/L). The platelet-to-lymphocyte ratio (PLR) was obtained by dividing the platelet count by the lymphocyte count (P/L). The monocyte-to-lymphocyte ratio (MLR) was calculated as M/L. The Systemic Inflammation Response Index (SIRI) was defined as the product of the neutrophil and monocyte counts divided by the lymphocyte count (N × M / L)[28]. The Systemic Immune-Inflammation Index (SIII) was calculated by multiplying the neutrophil and platelet counts and dividing the result by the lymphocyte count (N × P / L)[39].
Conventional prognostic factors. Patients were staged into five groups (0, A, B, C, or D) according to the Barcelona Clinic Liver Cancer classification [10]. Additional prognostic factors included the Milan criteria [40], serum albumin levels (g/dL), and serum AFP levels (ng/mL).
Therapeutic options. All treatment modalities received by the patients were documented. These included ablation therapy (percutaneous ethanol injection, radiofrequency ablation, or microwave ablation), transarterial chemoembolization (TACE), surgical resection, liver transplantation, systemic therapy, and/or palliative care measures.
Outcome variable. Long-term survival was considered the primary outcome. Survival time was defined as the interval between the date of inclusion in the study (i.e., the date of initial treatment) and the date of death, regardless of whether the cause of death was related to the neoplasm.
2.5. Statistical Analysis
The data were entered and analyzed using SPSS statistical package v. 29.0 (IBM Corporation, Armonk, NY, USA), and the RStudio software (v. 4.5.1). Figures were performed using the software Jamovi (v. 2.6.26).
Descriptive analysis. A descriptive analysis of the study sample was conducted. Categorical variables were summarized using frequencies and percentages. For numerical variables, results were expressed as mean ± standard deviation or median with interquartile range, depending on the distribution of the data. The Kolmogorov–Smirnov test was used to assess the normality of distributions. Survival analysis was performed using the Kaplan–Meier method.
Univariate analysis. A univariate Cox proportional hazards regression was conducted to evaluate the association between each predictor variable, including inflammatory markers, and overall survival. The Log-Rank test was used to compare survival curves.
Subsequently, the discriminative ability of each classical prognostic factor for hepatocellular carcinoma, along with the inflammatory markers, was assessed. For this purpose, Harrell’s concordance index (C-index) [41,42] was calculated using univariate Cox regression models. The C-index reflects the probability that, for a random pair of patients, the one with the worse predicted prognosis according to the model will indeed die before the other. C-indices were reported along with their standard errors and 95% confidence intervals, using the “rcorr.cens()” function from the Hmisc package in R. This approach also allowed for the identification of the most accurate survival predictor among the inflammatory markers. The C-index ranges from 0.5 (no predictive ability) to 1.0 (perfect discrimination), with higher values indicating superior performance in distinguishing between patients with different survival outcomes.
Given the pronounced skewness observed in the distribution of the numerical variables, these were analyzed as categorical variables using specific cutoff values. The cutoffs applied were: 2.3 for NLR, 100.0 for PLR, 0.30 for MLR, 1.0 for SIRI, and 400.0 for SIII. These thresholds were obtained by rounding the values identified using the Youden index and by referencing previously published literature. Accordingly, NLR values were categorized as <2.3 or ≥2.3; PLR as <100 or ≥100; MLR as <0.30 or ≥0.30; SIRI as <1.0 or ≥1.0; and SIII as <400 or ≥400 for all subsequent analyses.
Multivariate Analysis and Model Comparison. A multivariate Cox proportional hazards regression model was constructed, in which the best survival predictor among the inflammatory markers was adjusted for classical prognostic factors of hepatocellular carcinoma, including age, Charlson comorbidity index, BCLC classification, Milan criteria, MELD score, serum AFP, and serum albumin levels. The objective was to determine which variables remained independent prognostic factors for overall survival.
To evaluate and compare model performance, the concordance index (C-index), Akaike Information Criterion (AIC), and the likelihood ratio test were calculated for models with and without inclusion of the NLR.
To assess the model’s overall discriminative ability, the C-index was computed. Two multivariate models were fitted: one including the NLR and another excluding it. The C-indices of both models were compared, and the statistical significance of the difference was evaluated using the z-score formula for differences between independent means, incorporating the pooled standard error.
To evaluate model fit while considering complexity, the AIC was also calculated. A lower AIC value indicates a better balance between goodness-of-fit and parsimony. This metric was used to compare the full model including the NLR with a reduced model excluding it.
In addition, the likelihood ratio test was performed to determine whether the inclusion of NLR significantly improved the model’s explanatory power. This test is based on the difference in the –2 log-likelihood (–2LL) values between the two models.
The strength of association was expressed using hazard ratios (HRs) with their corresponding 95% confidence intervals (CIs). Each C-index was reported along with its 95% CI and standard error (SE). A two-sided p-value of < 0.05 was considered statistically significant.
3. Results
3.1. Baseline Characteristics
Of the 250 patients included in the study, 195 (78%) were men and 55 (22%) were women (p < 0.001), resulting in a male-to-female ratio of 3.5:1 (p < 0.001). The mean age was 68.0 ± 10.4 years.
The underlying cause of liver disease was alcohol-related in 80 patients (32.0%), viral in 78 (31.2%), mixed etiology in 29 (11.6%), and other causes in 32 patients (12.8%). In 19 patients (7.6%), no evidence of underlying liver disease was found, and in another 12 cases (4.8%), the etiology could not be determined.
Regarding the treatment received, ablation was the most frequently used initial therapy with curative intent, performed in 94 patients (37.6%). An additional 27 patients (10.8%) received ablation either as a bridge to liver transplantation or as a second-line treatment. TACE was used as the first-line treatment in 31 patients (12.4%) and as a second-line option in 14 additional cases. Liver transplantation was initially proposed for 35 patients, but only 13 ultimately underwent the procedure. Surgical resection was offered as the initial treatment in 8 patients (3.2%). Systemic therapy was administered as the first-line treatment in 19 patients (7.6%) and as a second- or third-line option in 37 patients (14.8%). In 84 cases (33.7%), patients were referred for palliative care as the initial therapeutic approach.
The overall survival curve is presented in Figure 1. At the end of follow-up, only 43 patients (17.2%) were still alive, while the remaining 207 patients (82.8%) had died. Regardless of disease stage and treatment modality, the overall probability of survival at 1, 3, and 5 years was 49.8%, 27.6%, and 12.7%, respectively. The estimated mean survival was 27.1 months (SE: 2.6; 95% CI: 22.0–32.2), and the estimated median survival was 11.9 months (IQR: 1.6–37.0).
3.2. Univariate Cox Regression Analysis
The baseline characteristics of the study population and the results of the univariate Cox regression analysis for survival are presented in Table 1. Figure 2 displays the unadjusted Kaplan–Meier survival curves according to baseline NLR levels. Patients with elevated NLR values had an estimated 5-year survival probability of 4.8%, compared to 21.0% in those with NLR values below 2.30 (p < 0.001).
3.3. C-Index–Based Evaluation of Prognostic Variables
The individual C-index values for each prognostic variable are presented in Table 2. According to this index, the three strongest predictors of survival in untreated hepatocellular carcinoma were the BCLC classification (C-index: 0.717; SE: 0.017; 95% CI: 0.750–0.864), serum albumin level (C-index: 0.713; SE: 0.020; 95% CI: 0.674–0.752), and comorbidity as measured by the Charlson score (C-index: 0.672; SE: 0.019; 95% CI: 0.635–0.709). Among the inflammatory markers, the NLR was the best predictor (C-index: 0.640; SE: 0.016; 95% CI: 0.609–0.671), ranking fourth overall, above the Milan criteria and the MELD score.
3.4. Multivariate Cox Regression Analysis
In the multivariate Cox regression analysis (Figure 3), the inflammatory marker NLR (≥ 2.3) remained an independent prognostic factor for overall survival in patients with untreated hepatocellular carcinoma, with a hazard ratio (HR) of 1.859 (95% CI: 1.321–2.615; p < 0.001). This association persisted after adjustment for classical prognostic variables, including BCLC stage (HR: 1.661; p < 0.001), serum albumin level (HR: 0.554; p < 0.001), Charlson comorbidity index (HR: 1.116; p = 0.006), and Milan criteria (HR: 0.637; p = 0.023). In contrast, age, AFP level, and MELD score did not reach statistical significance in the model. The overall model test was significant (χ² = 152.566; df = 8; p < 0.001), indicating good overall model fit.
The Child-Pugh classification was not included as a covariate in the multivariable analysis, as it was deemed redundant with other variables already incorporated into the model: albumin, MELD score, and BCLC staging system. Including Child-Pugh alongside these parameters could lead to collinearity and reduce model parsimony.
The multivariable model that included the NLR yielded a C-index of 0.794 (SE: 0.016; 95% CI: 0.763–0.825), whereas the model excluding NLR (Figure 4) showed a C-index of 0.781 (SE: 0.018; 95% CI: 0.746–0.816) (Figure 4). Although the absolute C-index was slightly higher when the inflammatory marker was included, the difference between the two models did not reach statistical significance (z = 0.54; p = 0.59).
However, the comparison of the –2 log-likelihood (–2LL) values revealed a significant improvement in model fit. The model including NLR had a –2LL of 1343.129, compared to 1355.734 for the model without NLR, resulting in a statistically significant difference in log-likelihood (Δ–2LL = 12.605; p < 0.001).
Finally, the full multivariable Cox model that included NLR also demonstrated superior fit based on the Akaike Information Criterion (AIC). The AIC for the model with NLR was 1359.1, compared to 1369.7 for the model without it. This difference supports the inclusion of NLR as a relevant prognostic factor, reflecting an improved balance between model complexity and explanatory power.
4. Discussion
This study demonstrates that assessing the inflammatory status of patients with untreated hepatocellular carcinoma at the time of diagnosis may serve as a valuable tool for predicting overall survival. Among all the inflammatory markers evaluated in this cohort, the neutrophil-to-lymphocyte ratio emerged as the strongest predictor of survival.
In the multivariate analysis, NLR remained an independent prognostic factor after adjustment for classical non-inflammatory prognostic variables. Regarding its discriminative capacity, NLR ranked fourth according to Harrell’s concordance index (C-index) when compared with both inflammatory and non-inflammatory markers, surpassing even the MELD score and the Milan criteria. These findings position NLR as a relevant prognostic marker, with greater discriminative power than several classical parameters commonly used in the stratification of hepatocellular carcinoma.
Moreover, although the inclusion of NLR in the Cox regression model was associated with a modest increase in the C-index, it led to a statistically significant improvement in overall model performance. These results suggest that NLR provides independent prognostic value and enhances the explanatory capacity of the model, even if its contribution to individual-level discrimination is limited.
The role of neutrophils in the progression of solid tumors, including hepatocellular carcinoma, and their potential as therapeutic targets has been widely studied [22]. HCC is recognized as an inflammation-related cancer in which non-resolving inflammation contributes to both tumor development and progression. Neutrophils play a central role in shaping the immune microenvironment of these tumors. A high density of intratumoral neutrophils, commonly referred to as tumor-associated neutrophils (TANs) [43], has been identified within the tumor microenvironment. Elevated TAN infiltration has been associated with worse recurrence-free, cancer-specific, and overall survival. Moreover, TANs may exert both anti-tumorigenic and pro-tumorigenic effects, a duality that carries important therapeutic implications[44]. Within this context, the NLR may serve as a useful prognostic indicator of tumor progression.
Several previously published studies have examined the prognostic significance of inflammatory markers in patients with hepatocellular carcinoma[34].
Regarding NLR, most studies have demonstrated a significant association with overall survival in univariate analyses[32,45,46,47,48,49,50,51,52]. However, only a few of them[45,47], identified NLR as an independent prognostic factor in multivariate models. In some cohorts, this association could not be confirmed[53], likely due to limited sample size. Analyses using ROC curves have yielded inconsistent results: while some studies reported excellent areas under the curve (AUC)[52], others produced paradoxical findings[54]. Nevertheless, several meta-analyses[15,16,18,33,55,56], have concluded that NLR is clearly an effective prognostic factor in patients with HCC, particularly among East Asian populations, where the incidence of the disease is higher.
These studies appear to exhibit considerable heterogeneity in the cutoff values used to define elevated NLR, which complicates standardization and direct comparison of results across different cohorts. Indeed, in the reviewed series, cutoff values ranged from 1.7[50] to 4.2[51]. In our study, a cutoff of 2.3 was applied. Nevertheless, regardless of the specific threshold used, most studies—including several meta-analyses—have found a statistically significant association between elevated NLR and reduced overall survival.
Regarding other inflammatory markers, several studies, including three meta-analyses[17,57,58,59], have demonstrated that elevated platelet-to-lymphocyte ratio (PLR) is independently associated with poorer overall survival and a higher risk of recurrence in patients with HCC[46,47,49,50,51,60]. Both the monocyte-to-lymphocyte ratio (MLR) and the lymphocyte-to-monocyte ratio (LMR) have also been evaluated as prognostic factors in HCC patients. Some studies have shown that elevated preoperative MLR levels are associated with worse survival outcomes[50,61]. Conversely, patients with higher preoperative LMR values appear to have a better prognosis[46,62,63]. However, other series have failed to confirm the prognostic utility of these markers in HCC[51].
A well-established association has also been observed between the systemic inflammation response index (SIRI) and the prognosis of untreated hepatocellular carcinoma. Several studies and meta-analyses have shown that elevated SIRI values[64], as well as other systemic inflammation indices such as the systemic immune-inflammation index (SIII)[65], are independently associated with worse overall survival and increased tumor aggressiveness in patients with hepatocellular carcinoma, regardless of treatment status, even in advanced-stage disease without specific therapy[66,67].
Finally, other inflammatory markers such as serum C-reactive protein (CRP)[31], the C-reactive protein to albumin ratio[68], the gamma-glutamyl transpeptidase to platelet ratio (GPR)[48], and the aspartate aminotransferase-to-lymphocyte ratio (ALR)[49], have also been linked to survival, although they were not included in the present study.
It is important to emphasize that the magnitude of a variable’s association with survival, typically expressed as the hazard ratio in most studies, is not equivalent to its individual predictive power, either alone or within the context of a regression model. In such cases, the concordance index (C-index) is more commonly used. In survival analysis, the hazard ratio quantifies the effect of a predictor on the risk of the event occurring, indicating how much the hazard changes with each unit increase in the predictor[69]. The C-index, on the other hand, measures the model’s discriminatory ability by estimating the proportion of correctly ordered patient pairs based on predicted survival times. While the HR provides insight into the strength and direction of associations, the C-index evaluates the overall predictive accuracy of the model in distinguishing survival outcomes[70].
Several studies have also employed receiver operating characteristic (ROC) curves to evaluate the prognostic utility of inflammatory markers in relation to hepatocellular carcinoma[49,51,52,54]. The reported areas under the curve ranged from 0.479[51] to 0.811[52], generally indicating poor performance, except for the latter series. In our study, we did not use ROC curve analysis, as it treats mortality as a binary outcome rather than accounting for survival time. This limitation may lead to an underestimation of the true prognostic value of the variables.
As in the previously mentioned studies, all inflammatory markers analyzed in our cohort were significantly associated with overall survival in the univariate analysis. The same was observed for the classical prognostic variables included in the analysis. However, when evaluating the predictive power of each variable using the concordance index (C-index), only a few surpassed the threshold of 0.6. These included the MELD score, Milan criteria, NLR, Charlson comorbidity index, serum albumin, and BCLC classification. Among all variables, the BCLC classification showed the highest prognostic accuracy for untreated hepatocellular carcinoma, with a concordance index (C-index) of 0.717. Among the inflammatory markers, NLR yielded the highest C-index (0.640). The remaining inflammatory markers—PLR, MLR, SIRI, and SIII—showed individual predictive power below 0.6 according to the C-index. For this reason, only NLR was included as the representative inflammatory marker in the multivariate analysis. Assessing whether the low predictive performance observed for the other inflammatory markers was due to the selection of cutoff values for the numerical variables was beyond the scope of this study.
In addition to its statistical significance in the multivariate Cox model, the inclusion of NLR improved the overall model fit as evidenced by a reduction in AIC. While the increase in discriminative ability (as measured by the concordance index) was modest and did not reach statistical significance, the AIC reflected a more favorable trade-off between model complexity and explanatory strength. Moreover, the inclusion of NLR in the multivariable Cox regression model led to a significant improvement in model fit, with a significant reduction in –2 log-likelihood. This statistically significant change indicates that the model including NLR better captures survival-related variability in untreated hepatocellular carcinoma.
These findings support the utility of NLR as an easily accessible prognostic marker, with predictive power potentially comparable to that of classical tools used in the prognostic stratification of hepatocellular carcinoma. This parameter should be routinely included in standard hematological reports and considered among the general prognostic factors for patients with hepatocellular carcinoma.
A key strength of this study lies in the comparative analytical approach, which incorporates Harrell’s concordance index (C-index), the Akaike Information Criterion (AIC), and the likelihood ratio test. This multifaceted methodology provides a more nuanced and comprehensive evaluation of the predictive performance of individual variables, complementing traditional estimates based solely on hazard ratios.
Limitations of this study include its single-center and retrospective design. Additionally, the potential for bias must be acknowledged due to the exclusion of other possible confounding factors related to hepatocellular carcinoma prognosis, particularly in the molecular and genetic domains. Nevertheless, we believe that these findings are highly applicable to routine clinical practice in the management of patients with hepatocellular carcinoma.
5. Conclusions
The NLR may be considered as one of the most relevant prognostic markers for overall survival in patients with untreated hepatocellular carcinoma. Given its simplicity, accessibility, and clinical relevance, NLR should be integrated into prognostic assessments for hepatocellular carcinoma. Future studies are warranted to validate these findings in larger, multicenter cohorts and to explore the added value of combining NLR with molecular and genetic markers for more refined risk stratification.
Author Contributions
Conceptualization, J.M.G, N.A.L. and C.R.H.S.; methodology, J.M.G.; validation, F.C.B., P.P.S. and C.R.H.S.; formal analysis, J.M.G..; investigation, N.A.L. and I.M.M; resources, N.A.L. and I.M.M; data curation, N.A.L. and I.M.M.; writing—original draft preparation, N.A.L., I.M.M, and J.M.G.; writing—review and editing, J.M.G.; visualization, J.M.G. and I.M.M.; supervision, J.M.G.; project administration, N.A.L.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Hospital Universitario de Gran Canaria Dr. Negrín. Approval Code: 2021-443-1. Approval date: 23 November 2021.
Informed Consent Statement
Patient consent was waived as the study involved only anonymized data and did not require informed consent, given that no direct patient intervention or identifiable information was involved.
Data Availability Statement
Underlying data not included in this article are available from the corresponding author upon reasonable request in accordance with local and national regulations.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HCC | Hepatocellular carcinoma |
| BCLC | Barcelona Clinic Liver Cancer |
| AFP | Alpha-fetoprotein |
| MELD | Model for End-Stage Liver Disease |
| NLR | Neutrophil-to-lymphocyte ratio |
| PLR | Platelet-to-lymphocyte ratio |
| MLR | Monocyte-to-lymphocyte ratio |
| SIRI | Systemic Inflammation Response Index |
| SIII | Systemic Immune-inflammation Index |
| TACE | Transcatheter arterial chemoembolization |
| C-index | Harrell’s concordance index |
| AIC | Akaike Information Criterion |
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global Cancer Statistics 2022: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2024, 74, 229–263. [Google Scholar] [CrossRef]
- de Martel, C.; Georges, D.; Bray, F.; Ferlay, J.; Clifford, G.M. Global Burden of Cancer Attributable to Infections in 2018: A Worldwide Incidence Analysis. Lancet Glob Health 2020, 8, e180–e190. [Google Scholar] [CrossRef]
- Wang, J.; Qiu, K.; Zhou, S.; Gan, Y.; Jiang, K.; Wang, D.; Wang, H. Risk Factors for Hepatocellular Carcinoma: An Umbrella Review of Systematic Review and Meta-Analysis. Ann Med 2025, 57. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.G.; Llovet, J.M.; Yarchoan, M.; Mehta, N.; Heimbach, J.K.; Dawson, L.A.; Jou, J.H.; Kulik, L.M.; Agopian, V.G.; Marrero, J.A.; et al. AASLD Practice Guidance on Prevention, Diagnosis, and Treatment of Hepatocellular Carcinoma. Hepatology 2023, 78, 1922–1965. [Google Scholar] [CrossRef]
- Tan, D.J.H.; Setiawan, V.W.; Ng, C.H.; Lim, W.H.; Muthiah, M.D.; Tan, E.X.; Dan, Y.Y.; Roberts, L.R.; Loomba, R.; Huang, D.Q. Global Burden of Liver Cancer in Males and Females: Changing Etiological Basis and the Growing Contribution of NASH. Hepatology 2023, 77, 1150–1163. [Google Scholar] [CrossRef]
- Siegel, R.L.; Kratzer, T.B.; Giaquinto, A.N.; Sung, H.; Jemal, A. Cancer Statistics, 2025. CA Cancer J Clin 2025, 75. [Google Scholar] [CrossRef] [PubMed]
- Giannini, E.G.; Farinati, F.; Ciccarese, F.; Pecorelli, A.; Rapaccini, G.L.; Di Marco, M.; Benvegnù, L.; Caturelli, E.; Zoli, M.; Borzio, F.; et al. Prognosis of Untreated Hepatocellular Carcinoma. Hepatology 2015, 61, 184–190. [Google Scholar] [CrossRef]
- Nevola, R.; Ruocco, R.; Criscuolo, L.; Villani, A.; Alfano, M.; Beccia, D.; Imbriani, S.; Claar, E.; Cozzolino, D.; Carlo Sasso, F.; et al. Predictors of Early and Late Hepatocellular Carcinoma Recurrence. World J Gastroenterol 2023, 29, 1243–1260. [Google Scholar] [CrossRef] [PubMed]
- Yilma, M.; Houhong Xu, R.; Saxena, V.; Muzzin, M.; Tucker, L.Y.; Lee, J.; Mehta, N.; Mukhtar, N. Survival Outcomes Among Patients With Hepatocellular Carcinoma in a Large Integrated US Health System. JAMA Netw Open 2024, 7, e2435066. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC Strategy for Prognosis Prediction and Treatment Recommendation: The 2022 Update. J Hepatol 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Kim, K.M.; Shim, S.G.; Sinn, D.H.; Song, J.E.; Kim, B.S.; Kim, H.G. Child-Pugh, MELD, MELD-Na, and ALBI Scores: Which Liver Function Models Best Predicts Prognosis for HCC Patient with Ascites? Scand J Gastroenterol 2020, 55, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Ota, M.; Komeda, K.; Iida, H.; Ueno, M.; Kosaka, H.; Nomi, T.; Tanaka, S.; Nakai, T.; Hokutou, D.; Matsumoto, M.; et al. The Prognostic Value of Preoperative Serum Markers and Risk Classification in Patients with Hepatocellular Carcinoma. Ann Surg Oncol 2023, 30, 2807–2815. [Google Scholar] [CrossRef]
- Brown, Z.J.; Tsilimigras, D.I.; Ruff, S.M.; Mohseni, A.; Kamel, I.R.; Cloyd, J.M.; Pawlik, T.M. Management of Hepatocellular Carcinoma: A Review. JAMA Surg 2023, 158, 410–420. [Google Scholar] [CrossRef] [PubMed]
- Jeng, L.-B.; Chan, W.-L.; Teng, C.-F. Prognostic Significance of Serum Albumin Level and Albumin-Based Mono- and Combination Biomarkers in Patients with Hepatocellular Carcinoma. Cancers (Basel) 2023, 15, 1005. [Google Scholar] [CrossRef]
- Lin, S.; Hu, S.; Ran, Y.; Wu, F. Neutrophil-to-Lymphocyte Ratio Predicts Prognosis of Patients with Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. Transl Cancer Res 2021, 10, 1667–1678. [Google Scholar] [CrossRef]
- Min, G.T.; Li, Y.M.; Yao, N.; Wang, J.; Wang, H.P.; Chen, W. The Pretreatment Neutrophil-Lymphocyte Ratio May Predict Prognosis of Patients with Liver Cancer: A Systematic Review and Meta-Analysis. Clin Transplant 2018, 32. [Google Scholar] [CrossRef]
- Ma, W.; Zhang, P.; Qi, J.; Gu, L.; Zang, M.; Yao, H.; Shi, X.; Wang, C.; Jiang, Y. Prognostic Value of Platelet to Lymphocyte Ratio in Hepatocellular Carcinoma: A Meta-Analysis. Sci Rep 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Chen, H.; Chen, Z.; Tan, J.; Wu, F.; Li, X. Prognostic Value of Neutrophil-to-Lymphocyte Ratio in Patients with Hepatocellular Carcinoma Receiving Curative Therapies: A Systematic Review and Meta-Analysis. BMC Cancer 2025, 25, 571. [Google Scholar] [CrossRef]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular Carcinoma. The Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef]
- Pinto Marques, H.; Gomes da Silva, S.; De Martin, E.; Agopian, V.G.; Martins, P.N. Emerging Biomarkers in HCC Patients: Current Status. Int J Surg 2020, 82, 70–76. [Google Scholar] [CrossRef]
- Balkwill, F.; Mantovani, A. Inflammation and Cancer: Back to Virchow? The Lancet 2001, 357, 539–545. [Google Scholar] [CrossRef]
- Arvanitakis, K.; Mitroulis, I.; Germanidis, G. Tumor-Associated Neutrophils in Hepatocellular Carcinoma Pathogenesis, Prognosis, and Therapy. Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic Role of Neutrophil-to-Lymphocyte Ratio in Solid Tumors: A Systematic Review and Meta-Analysis. JNCI: Journal of the National Cancer Institute 2014, 106. [Google Scholar] [CrossRef]
- Li, B.; Zhou, P.; Liu, Y.; Wei, H.; Yang, X.; Chen, T.; Xiao, J. Platelet-to-Lymphocyte Ratio in Advanced Cancer: Review and Meta-Analysis. Clinica Chimica Acta 2018, 483, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Mo, D.C.; Liu, X.; Lv, Y.J.; Qin, Y.Q.; Xie, G.S. Is Monocyte-to-Lymphocyte Ratio the Best Systematic Inflammatory Biomarker for the Prognosis of Gastrointestinal Stromal Tumors? J Surg Oncol 2019, 119, 1024–1025. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.-S.; Kim, S.Y.; Moon, A. C-Reactive Protein Signaling Pathways in Tumor Progression. Biomol Ther (Seoul) 2023, 31, 473–483. [Google Scholar] [CrossRef]
- Xu, H.; Ma, Y.; Deng, F.; Ju, W.; Sun, X.; Wang, H. The Prognostic Value of C-Reactive Protein/Albumin Ratio in Human Malignancies: An Updated Meta-Analysis. Onco Targets Ther 2017, Volume 10, 3059–3070. [Google Scholar] [CrossRef]
- Qi, Q.; Zhuang, L.; Shen, Y.; Geng, Y.; Yu, S.; Chen, H.; Liu, L.; Meng, Z.; Wang, P.; Chen, Z. A Novel Systemic Inflammation Response Index (SIRI) for Predicting the Survival of Patients with Pancreatic Cancer after Chemotherapy. Cancer 2016, 122, 2158–2167. [Google Scholar] [CrossRef]
- van ’t Land, F.R.; Aziz, M.H.; Michiels, N.; Mieog, J.S.D.; Bonsing, B.A.; Luelmo, S.A.C.; Homs, M.Y.V.; Groot Koerkamp, B.; Papageorgiou, G.; van Eijck, C.H.J. Increasing Systemic Immune-Inflammation Index During Treatment in Patients With Advanced Pancreatic Cancer Is Associated With Poor Survival: A Retrospective, Multicenter, Cohort Study. Ann Surg 2023, 278, 1018–1023. [Google Scholar] [CrossRef]
- Proctor, M.J.; Morrison, D.S.; Talwar, D.; Balmer, S.M.; Fletcher, C.D.; O’reilly, D.S.J.; Foulis, A.K.; Horgan, P.G.; Mcmillan, D.C. A Comparison of Inflammation-Based Prognostic Scores in Patients with Cancer. A Glasgow Inflammation Outcome Study. Eur J Cancer 2011, 47, 2633–2641. [Google Scholar] [CrossRef]
- Hashimoto, K.; Ikeda, Y.; Korenaga, D.; Tanoue, K.; Hamatake, M.; Kawasaki, K.; Yamaoka, T.; Iwatani, Y.; Akazawa, K.; Takenaka, K. The Impact of Preoperative Serum C-reactive Protein on the Prognosis of Patients with Hepatocellular Carcinoma. Cancer 2005, 103, 1856–1864. [Google Scholar] [CrossRef]
- Gomez, D.; Farid, S.; Malik, H.Z.; Young, A.L.; Toogood, G.J.; Lodge, J.P.A.; Prasad, K.R. Preoperative Neutrophil-to-Lymphocyte Ratio as a Prognostic Predictor after Curative Resection for Hepatocellular Carcinoma. World J Surg 2008, 32, 1757–1762. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Wu, F.; Du, L.; Dong, Y.; Lin, S. Significant Association between High Neutrophil-Lymphocyte Ratio and Poor Prognosis in Patients with Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. Front Immunol 2023, 14, 1211399. [Google Scholar] [CrossRef]
- Giannone, F.; Slovic, N.; Pessaux, P.; Schuster, C.; Baumert, T.F.; Lupberger, J. Inflammation-Related Prognostic Markers in Resected Hepatocellular Carcinoma. Front Oncol 2023, 13, 1267870. [Google Scholar] [CrossRef]
- Minici, R.; Venturini, M.; Guzzardi, G.; Fontana, F.; Coppola, A.; Piacentino, F.; Torre, F.; Spinetta, M.; Maglio, P.; Guerriero, P.; et al. A Multicenter International Retrospective Investigation Assessing the Prognostic Role of Inflammation-Based Scores (Neutrophil-to-Lymphocyte, Lymphocyte-to-Monocyte, and Platelet-to-Lymphocyte Ratios) in Patients with Intermediate-Stage Hepatocellular Carcinoma (HCC) Undergoing Chemoembolizations of the Liver. Cancers (Basel) 2024, 16, 1618. [Google Scholar] [CrossRef]
- Halazun, K.J.; Hardy, M.A.; Rana, A.A.; Woodland IV, D.C.; Luyten, E.J.; Mahadev, S.; Witkowski, P.; Siegel, A.B.; Brown, R.S.; Emond, J.C. Negative Impact of Neutrophil-Lymphocyte Ratio on Outcome after Liver Transplantation for Hepatocellular Carcinoma. Ann Surg 2009, 250, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J Chronic Dis 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Qi, X.; Guo, X. Child-Pugh Versus MELD Score for the Assessment of Prognosis in Liver Cirrhosis: A Systematic Review and Meta-Analysis of Observational Studies. Medicine 2016, 95. [Google Scholar] [CrossRef]
- van ’t Land, F.R.; Aziz, M.H.; Michiels, N.; Mieog, J.S.D.; Bonsing, B.A.; Luelmo, S.A.C.; Homs, M.Y.V.; Groot Koerkamp, B.; Papageorgiou, G.; van Eijck, C.H.J. Increasing Systemic Immune-Inflammation Index During Treatment in Patients With Advanced Pancreatic Cancer Is Associated With Poor Survival: A Retrospective, Multicenter, Cohort Study. Ann Surg 2023, 278, 1018–1023. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver Transplantation for the Treatment of Small Hepatocellular Carcinomas in Patients with Cirrhosis. N Engl J Med 1996, 334, 693–700. [Google Scholar] [CrossRef]
- Brentnall, A.R.; Cuzick, J. Use of the Concordance Index for Predictors of Censored Survival Data. Stat Methods Med Res 2018, 27, 2359–2373. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F.E.; Lee, K.L.; Mark, D.B. Multivariable Prognostic Models: Issues in Developing Models, Evaluating Assumptions and Adequacy, and Measuring and Reducing Errors. Stat Med 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Shen, M.; Hu, P.; Donskov, F.; Wang, G.; Liu, Q.; Du, J. Tumor-Associated Neutrophils as a New Prognostic Factor in Cancer: A Systematic Review and Meta-Analysis. PLoS One 2014, 9, e98259. [Google Scholar] [CrossRef]
- Gregory, A.D.; Houghton, A.M.G. Tumor-Associated Neutrophils: New Targets for Cancer Therapy. Cancer Res 2011, 71, 2411–2416. [Google Scholar] [CrossRef]
- Lu, S.D.; Wang, Y.Y.; Peng, N.F.; Peng, Y.C.; Zhong, J.H.; Qin, H.G.; Xiang, B. De; You, X.M.; Ma, L.; Li, L.Q. Preoperative Ratio of Neutrophils to Lymphocytes Predicts Postresection Survival in Selected Patients with Early or Intermediate Stage Hepatocellular Carcinoma. Medicine (United States) 2016, 95. [Google Scholar] [CrossRef]
- Zheng, J.; Seier, K.; Gonen, M.; Balachandran, V.P.; Kingham, T.P.; D’Angelica, M.I.; Allen, P.J.; Jarnagin, W.R.; DeMatteo, R.P. Utility of Serum Inflammatory Markers for Predicting Microvascular Invasion and Survival for Patients with Hepatocellular Carcinoma. Ann Surg Oncol 2017, 24, 3706–3714. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Bai, N.; Hu, X.; OuYang, X.W.; Yao, L.; Tao, Y.; Wang, Z. Preoperative Inflammatory Markers of NLR and PLR as Indicators of Poor Prognosis in Resectable HCC. PeerJ 2019, 7, e7132. [Google Scholar] [CrossRef] [PubMed]
- Dai, T.; Deng, M.; Ye, L.; Liu, R.; Lin, G.; Chen, X.; Li, H.; Liu, W.; Yang, Y.; Chen, G.; et al. Prognostic Value of Combined Preoperative Gamma-Glutamyl Transpeptidase to Platelet Ratio and Fibrinogen in Patients with HBV-Related Hepatocellular Carcinoma after Hepatectomy. Am J Transl Res 2020, 12, 2984. [Google Scholar]
- Wu, W.; Wang, Q.; Han, D.; Li, J.; Nie, Y.; Guo, D.; Yang, L.; Tao, K.; Zhang, X.; Dou, K. Prognostic Value of Preoperative Inflammatory Markers in Patients with Hepatocellular Carcinoma Who Underwent Curative Resection. Cancer Cell Int 2021, 21, 500. [Google Scholar] [CrossRef]
- Silva, J.P.M.; Coelho, F.F.; Cassenote, A.J.F.; Jeismann, V.B.; Fonseca, G.M.; Kruger, J.A.P.; de Meira Júnior, J.D.; Nahas, S.C.; Herman, P. Preoperative Inflammatory Markers as Prognostic Predictors after Hepatocellular Carcinoma Resection: Data from a Western Referral Center. BMC Surg 2022, 22, 329. [Google Scholar] [CrossRef]
- Zhou, J.; Yang, D. Changes in Inflammatory Markers Predict the Prognosis of Resected Hepatocellular Carcinoma with Child–Pugh A. Current Oncology 2022, 29, 5800–5809. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Li, X.; Geng, M.; Ye, X.; Liu, H.; Liu, Y.; Wan, G.; Wang, X. Pretreatment Neutrophil-Lymphocyte Ratio: An Independent Predictor of Survival in Patients with Hepatocellular Carcinoma. Medicine (United States) 2015, 94, e639. [Google Scholar] [CrossRef]
- Sullivan, K.M.; Groeschl, R.T.; Turaga, K.K.; Tsai, S.; Christians, K.K.; White, S.B.; Rilling, W.S.; Pilgrim, C.H.C.; Gamblin, T.C. Neutrophil-to-lymphocyte Ratio as a Predictor of Outcomes for Patients with Hepatocellular Carcinoma: A Western Perspective. J Surg Oncol 2014, 109, 95–97. [Google Scholar] [CrossRef]
- Li, S.C.; Xu, Z.; Deng, Y.L.; Wang, Y.N.; Jia, Y.M.; Ding, J. Higher Neutrophil-Lymphocyte Ratio Is Associated with Better Prognosis of Hepatocellular Carcinoma. Medicine (United States) 2020, 99, E20919. [Google Scholar] [CrossRef]
- Xiao, W.-K.; Chen, D.; Li, S.-Q.; Fu, S.-J.; Peng, B.-G.; Liang, L.-J. Prognostic Significance of Neutrophil-Lymphocyte Ratio in Hepatocellular Carcinoma: A Meta-Analysis. BMC Cancer 2014, 14, 117. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Li, J.; Deng, H.; Li, H.; Su, C.; Guo, X. Neutrophil-to-Lymphocyte Ratio for the Prognostic Assessment of Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis of Observational Studies. Oncotarget 2016, 7, 45283–45301. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Si, G.; Zhu, F.; Hui, J.; Cai, S.; Huang, C.; Cheng, S.; Fathy, A.H.; Xiang, Y.; Li, J. Prognostic Role of Platelet to Lymphocyte Ratio in Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. Oncotarget 2017, 8, 22854–22862. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Cai, J.; Li, H.; Zeng, K.; He, L.; Fu, H.; Zhang, J.; Chen, L.; Yao, J.; Zhang, Y.; et al. Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio as Prognostic Predictors for Hepatocellular Carcinoma Patients with Various Treatments: A Meta-Analysis and Systematic Review. Cell Physiol Biochem 2017, 44, 967–981. [Google Scholar] [CrossRef]
- Hu, D.-H.; Yu, S.-M. Association between Platelet to Lymphocyte Ratio (PLR) and Overall Survival (OS) of Hepatocellular Carcinoma (HCC): A Meta-Analysis. Cell Mol Biol 2017, 63, 30–32. [Google Scholar] [CrossRef]
- Kim, H.; Choi, H.Z.; Choi, J.M.; Kang, B.M.; Lee, J.W.; Hwang, J.W. Sarcopenia with Systemic Inflammation Can Predict Survival in Patients with Hepatocellular Carcinoma Undergoing Curative Resection. J Gastrointest Oncol 2022, 13, 744–753. [Google Scholar] [CrossRef]
- Wang, Q.; Qiao, W.; Liu, B.; Li, J.; Yuan, C.; Long, J.; Hu, C.; Zang, C.; Zheng, J.; Zhang, Y. The Monocyte to Lymphocyte Ratio Not Only at Baseline but Also at Relapse Predicts Poor Outcomes in Patients with Hepatocellular Carcinoma Receiving Locoregional Therapy. BMC Gastroenterol 2022, 22, 98. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.X.; Ruan, D.Y.; Li, Y.; Wu, D.H.; Ma, X.K.; Chen, J.; Chen, Z.H.; Li, X.; Wang, T.T.; Lin, Q.; et al. Lymphocyte-to-Monocyte Ratio Predicts Survival of Patients with Hepatocellular Carcinoma after Curative Resection. World J Gastroenterol 2015, 21, 10898–10906. [Google Scholar] [CrossRef]
- Lin, S.; Lin, Y.; Fang, Y.; Mo, Z.; Hong, X.; Ji, C.; Jian, Z. Clinicopathological and Prognostic Value of Preoperative Lymphocyte to Monocyte Ratio for Hepatocellular Carcinoma Following Curative Resection. Medicine 2021, 100, e24153. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Tang, Z. Prognostic and Clinicopathological Significance of Systemic Inflammation Response Index in Patients with Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. Front Immunol 2024, 15. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Huang, Y.; Lin, T. Prognostic Impact of Elevated Pre-Treatment Systemic Immune-Inflammation Index (SII) in Hepatocellular Carcinoma. Medicine 2020, 99, e18571. [Google Scholar] [CrossRef]
- Hu, B.; Yang, X.R.; Xu, Y.; Sun, Y.F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.M.; Qiu, S.J.; Zhou, J.; et al. Systemic Immune-Inflammation Index Predicts Prognosis of Patients after Curative Resection for Hepatocellular Carcinoma. Clin Cancer Res 2014, 20, 6212–6222. [Google Scholar] [CrossRef]
- Fu, H.; Zheng, J.; Cai, J.; Zeng, K.; Yao, J.; Chen, L.; Li, H.; Zhang, J.; Zhang, Y.; Zhao, H.; et al. Systemic Immune-Inflammation Index (SII) Is Useful to Predict Survival Outcomes in Patients after Liver Transplantation for Hepatocellular Carcinoma within Hangzhou Criteria. Cell Physiol Biochem 2018, 47, 293–301. [Google Scholar] [CrossRef]
- Lin, N.; Li, J.; Ke, Q.; Wang, L.; Cao, Y.; Liu, J. Clinical Significance of C-Reactive Protein to Albumin Ratio in Patients with Hepatocellular Carcinoma: A Meta-Analysis. Dis Markers 2020, 2020. [Google Scholar] [CrossRef]
- Uno, H.; Claggett, B.; Tian, L.; Inoue, E.; Gallo, P.; Miyata, T.; Schrag, D.; Takeuchi, M.; Uyama, Y.; Zhao, L.; et al. Moving Beyond the Hazard Ratio in Quantifying the Between-Group Difference in Survival Analysis. J Clin Oncol 2014, 32, 2380–2385. [Google Scholar] [CrossRef]
- McLernon, D.J.; Giardiello, D.; Van Calster, B.; Wynants, L.; van Geloven, N.; van Smeden, M.; Therneau, T.; Steyerberg, E.W.; McLernon, D.J.; Giardiello, D.; et al. Assessing Performance and Clinical Usefulness in Prediction Models with Survival Outcomes: Practical Guidance for Cox Proportional Hazards Models. Ann Intern Med 2023, 176, 105–114. [Google Scholar] [CrossRef]
Figure 1.
Kaplan–Meier overall survival curve for the entire cohort of patients with hepatocellular carcinoma.
Figure 1.
Kaplan–Meier overall survival curve for the entire cohort of patients with hepatocellular carcinoma.
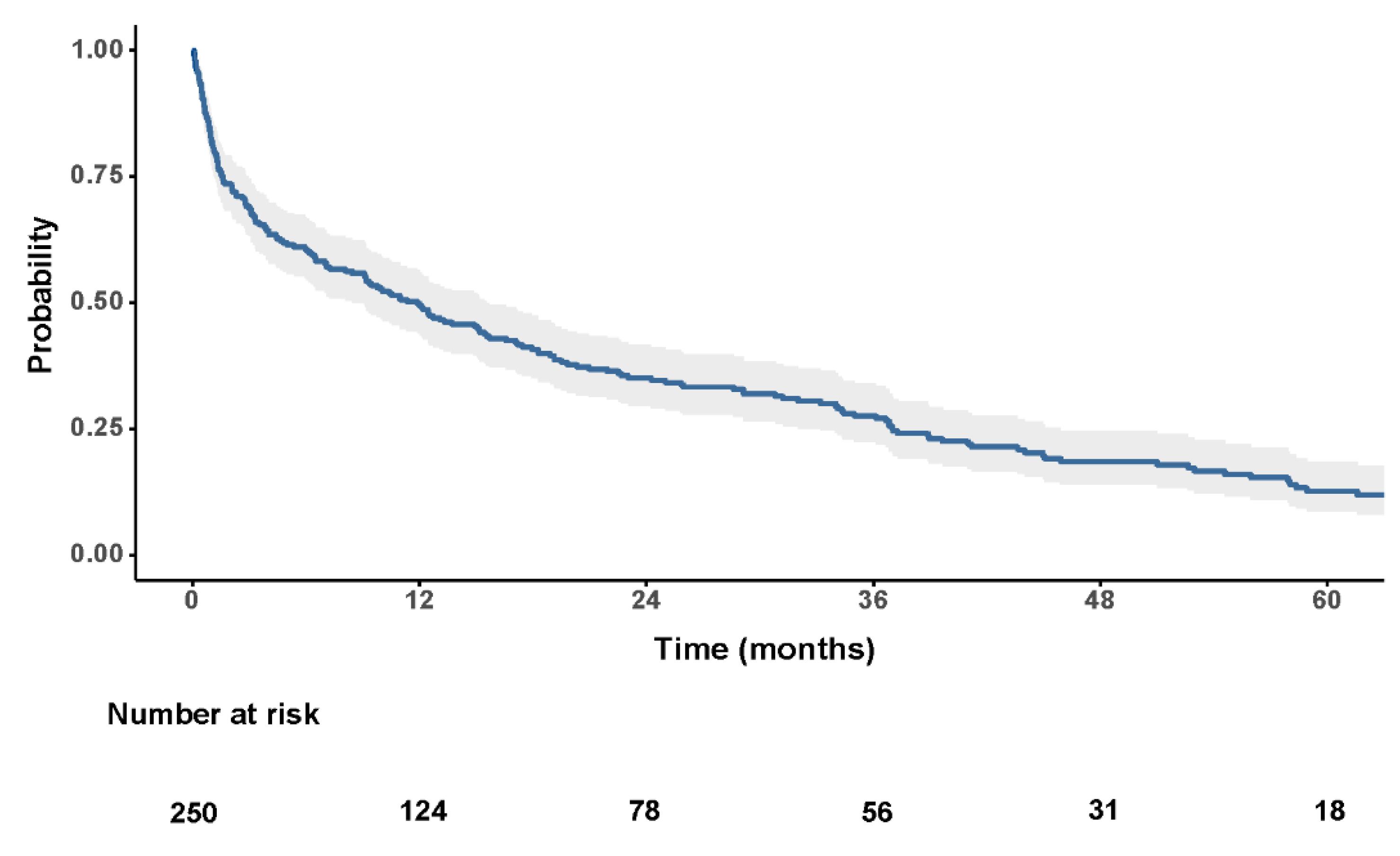
Figure 2.
Unadjusted survival curves for patients with baseline neutrophil-to-lymphocyte ratio (NLR) < 2.30 (blue) and patients with baseline NLR ≥ 2.30 (red) (p < 0.001).
Figure 2.
Unadjusted survival curves for patients with baseline neutrophil-to-lymphocyte ratio (NLR) < 2.30 (blue) and patients with baseline NLR ≥ 2.30 (red) (p < 0.001).
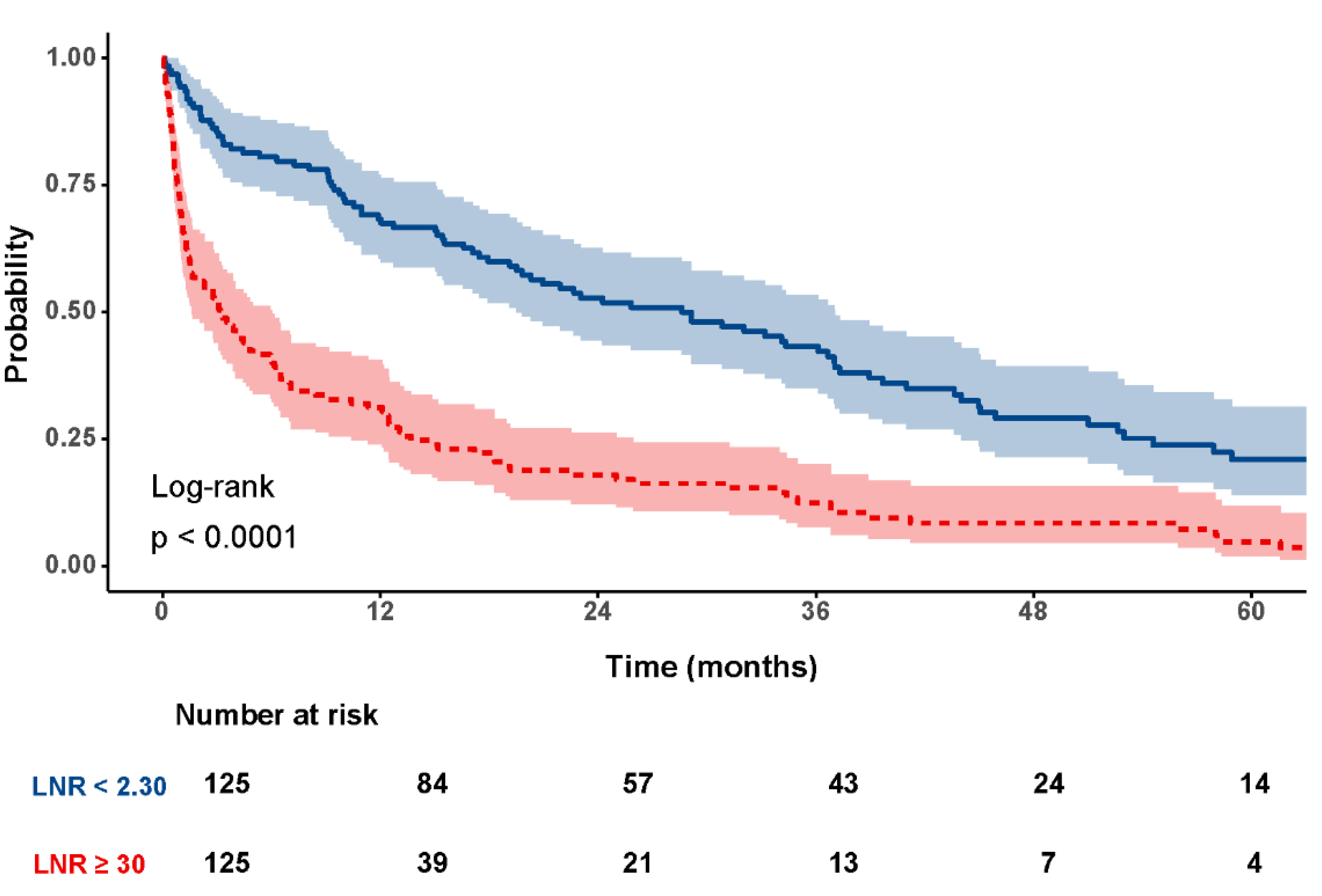
Figure 3.
Forest plot of the multivariate Cox regression model including the neutrophil-to-lymphocyte ratio (NLR) as a covariate for overall survival in patients with untreated hepatocellular carcinoma.
Figure 3.
Forest plot of the multivariate Cox regression model including the neutrophil-to-lymphocyte ratio (NLR) as a covariate for overall survival in patients with untreated hepatocellular carcinoma.

Figure 4.
Forest plot of the multivariate Cox regression model excluding the neutrophil-to-lymphocyte ratio (NLR) for overall survival in patients with untreated hepatocellular carcinoma.
Figure 4.
Forest plot of the multivariate Cox regression model excluding the neutrophil-to-lymphocyte ratio (NLR) for overall survival in patients with untreated hepatocellular carcinoma.
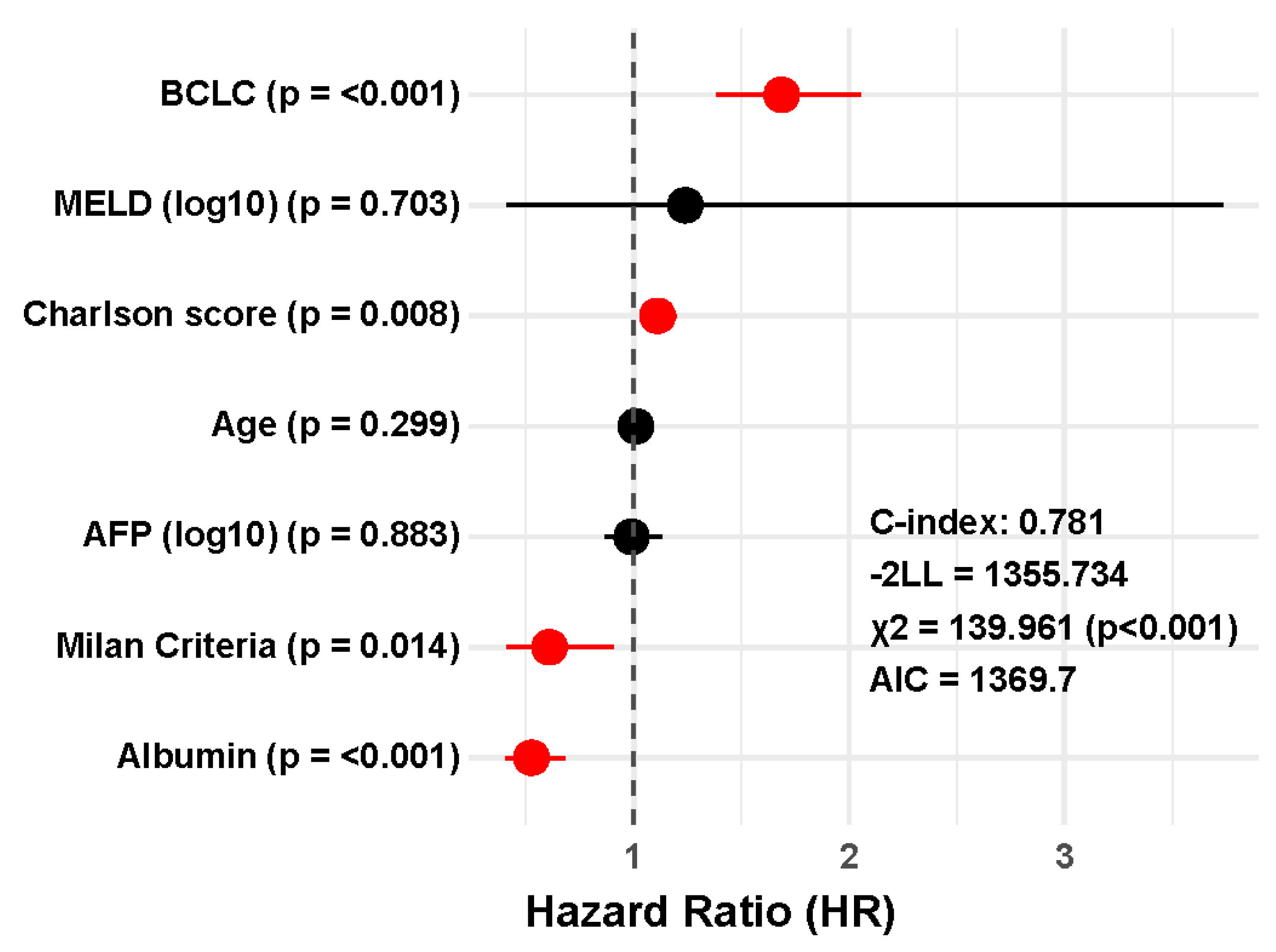

Table 1.
Baseline characteristics of the study population and results of the univariate Cox regression analysis for overall survival.
Table 1.
Baseline characteristics of the study population and results of the univariate Cox regression analysis for overall survival.
| Variable | n (%) | Univariate Analysis (HR – CI 95%) |
p |
|---|---|---|---|
| Age (mean ± SD) | 68 (±10,4) | 1.03 (1.01 – 1.05) | <0.001* |
| Sex: - men - women |
195 (78,0) 55 (22,0) |
0.91 (0.65 – 1.26) | 0.561 |
| Charlson score (median – IQR) | 7 (6,0 – 9,0) | 1.27 (1.20 – 1.34) | <0.001* |
| Diabetes mellitus: - No - Yes |
133 (53.2) 117 (46.8) |
1.16 (0.89 – 1.53) | 0.277 |
| OH Chirrosis: - No - Yes |
170 (68.0) 80 (32.0) |
1.13 (0.85 – 1.52) | 0.397 |
| AFP (Log10) (ng/mL) (median – IQR) | 10.27 (3.15 – 428.46) | 1.33 (1.19 – 1.48) | <0.001* |
| Albumin (g/dL) (median – IQR) | 3,4 (2,8 – 4,0) | 0.46 (0.37 – 0.56) | <0.001* |
| Child classification: A B C |
127(50,8) 75 (30,0) 26 (10,4) |
2.49 (2.01 – 3.08) | <0.001* |
| Milan criteria: - No - Yes |
105 (42,0) 143 (57,2) |
0.36 (0.26 – 0.48) | <0.001* |
| BCLC classification: 0 A B C D |
11 (4,4) 101 (40,4) 49 (19,6) 57 (22,8) 32 (12,8) |
2.10 (1.93 – 2.40) | <0,001* |
| MELD score (median – IQR) | 10,04 (7,90 – 13,63) | 1.07 (1.04 – 1.10) | <0.001* |
| NLR (median – IQR) | 2,34 (1,5 – 3,9) | 1.12 (1.08 – 1.15) | <0.001* |
| PLR (median – IQR) | 94,92 (61,57 – 139,37) | 1.02 (1.01 – 1.03) | <0.001* |
| MLR (median – IQR) | 0.40 (0.28 – 0.59) | 1.21 (1.02 – 1.43) | 0.028* |
| SIRI (median – IQR) | 1.22 (0.74 – 2.49) | 1.07 (1.05 – 1.09) | <0.001* |
| SIII (Log10) (median – IQR) | 318.2 (160.0 – 587.3) | 2.30 (1.64 – 3.22) | <0.001* |
BCLC: Barcelona Clinic Liver Cancer; NLR: Neutrophil-to-lymphocyte ratio; PLR: Platelet-to-lymphocyte ratio; MLR: Monocyte-to-lymphocyte ratio; SIRI: Systemic Inflammation Response Index; SIII: Systemic Immune-inflammation Index. IQR: Interquartile Range.
Table 2.
Individual C-index values, ordered from highest to lowest, for each prognostic variable of overall survival in untreated hepatocellular carcinoma.
Table 2.
Individual C-index values, ordered from highest to lowest, for each prognostic variable of overall survival in untreated hepatocellular carcinoma.
| Prognostic factor | C-index (Standar Error) | CI 95% |
| BCLC | 0.717 (0.017) | 0.684 – 0.750 |
| Albumine | 0.713 (0.020) | 0.674 – 0.752 |
| Charlson score | 0.672 (0.019) | 0.635 – 0.709. |
| NLR | 0.640 (0.016) | 0.609 – 0.671 |
| Milan criteria | 0.639 (0.016) | 0.608 – 0.670 |
| MELD score | 0.626 (0.023) | 0.581 – 0.671 |
| PLR | 0.605 (0.018) | 0.570 – 0.640 |
| SIII | 0.603 (0.018) | 0.568 – 0.638 |
| Age | 0.595 (0.022) | 0.537 – 0.623. |
| SIRI | 0.593 (0.0 18) | 0.558 – 0.628 |
| AFP | 0.592 (0.025) | 0.543 – 0.641 |
| MLR | 0.585 (0.017) | 0.552 – 0.618 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



