Submitted:
02 July 2025
Posted:
03 July 2025
Read the latest preprint version here
Abstract
Background: Therapeutic applications of saline solutions in oral healthcare range from mineral waters to standardized sodium chloride preparations. Despite millennia of use across medical traditions, their scientific foundation remains inadequately characterized and methodologically fragmented. This scoping review aimed to systematically characterize evidence for saline interventions in oral healthcare and identify methodological gaps for clinical standardization. Methods: Following JBI methodology and PRISMA-ScR standards, four databases (PubMed, Scopus, Web of Science, Cochrane Library) were searched for 2000-2024 publications. Studies were classified along a naturalness continuum from geological mineral waters to artificial preparations. Data synthesis integrated narrative analysis with systematic gap identification. Results: Thirteen eligible studies revealed limited evidence despite widespread clinical use. Research bias favored hypersaline Dead Sea derivatives (n=7, 54%) over natural thermal waters (n=2, 15%). Dead Sea interventions showed consistent benefits in periodontal inflammation, viral load reduction, and mucositis prophylaxis, though whitening applications failed. Marine-derived solutions demonstrated superior plaque control versus chlorhexidine, while artificial preparations (n=3) achieved therapeutic equivalence with conventional antimicrobials. Optimal antimicrobial duration occurred at 5.8% salinity. Methodological limitations included small sample sizes, short follow-up periods, and heterogeneous outcomes. Conclusions: Saline solutions demonstrate consistent efficacy across the natural-artificial spectrum. The inverse relationship between widespread clinical utilization and limited scientific validation highlights fundamental research gaps requiring urgent attention for evidence-based integration.
Keywords:
Thermal water
; mineral water
; saline solution
; oral health
1. Introduction
Contemporary antimicrobial mouthwashes demonstrate established efficacy in plaque control and bacterial adhesion prevention [1,2], yet mounting evidence of adverse effects—including dental staining, calculus formation, and allergic responses—has prompted renewed investigation of alternative therapeutic modalities [3,4]. Among these alternatives, saline-based interventions represent a particularly compelling paradigm, given their extensive historical precedent [5] and emerging scientific validation [6]. Therapeutic applications of saline solutions encompass a broad spectrum of mineral complexity and preparation methods [7]. At one extreme lie geothermally derived waters with sophisticated ionic profiles shaped by prolonged geological contact [8]; at the other, standardized sodium chloride preparations offering reproducible antimicrobial activity [9]. Intermediate marine-derived solutions provide moderate salinity with naturally occurring trace elements [10]. While these interventions differ substantially in composition and sourcing, they converge on salt's fundamental capacity for osmotic bacterial disruption and inflammatory modulation [11]. The therapeutic application of mineral waters predates recorded medical history, with archaeological evidence documenting systematic use across Mediterranean civilizations [12,13]. Modern geochemical analysis reveals these waters acquire distinctive profiles through hydrothermal circulation within specific geological formations, yielding complex solutions containing dissolved minerals, trace elements, and bioactive compounds whose therapeutic properties reflect their unique hydrogeochemical evolution [14,15]. This natural variation contrasts sharply with the standardized formulations characteristic of contemporary oral care products, suggesting potential therapeutic advantages inherent to geological complexity [16]. Hypersaline environments demonstrate distinctive therapeutic mechanisms through specialized microbial ecosystems and unique mineral profiles [17]. Dead Sea waters, with salinity exceeding 340 g/L, support extremophile communities producing bioactive metabolites with demonstrated antimicrobial activity against oral pathogens [18]. These include sulfur-cycling compounds with anti-inflammatory properties relevant to periodontal disease management [19], and probiotic strains such as Lactobacillus salivarius capable of disrupting cariogenic biofilms [20]. The extreme ionic composition—particularly high magnesium and bromide concentrations—provides additional therapeutic pathways through osmotic bacterial stress and enhanced tissue penetration [21]. European balneotherapy represents a paradox of extensive clinical application with minimal scientific validation [22]. Established thermal centers across France (Vichy, La Roche-Posay), Italy (Salsomaggiore, Montecatini), and Germany (Baden-Baden) have maintained centuries-old therapeutic protocols [23], yet oral health applications remain largely unexamined in controlled studies [24]. This research gap proves particularly striking given the sophisticated mineral compositions of European thermal waters and their documented efficacy in dermatological and rheumatological applications [25,26]. Marine-derived interventions occupy a strategic position between geological complexity and therapeutic standardization [27]. Standard seawater salinity (approximately 35 g/L) combined with consistent trace element profiles provides reproducible therapeutic effects while maintaining natural origin [28]. This intermediate complexity offers potential advantages over both highly variable mineral waters and simplified artificial preparations, suggesting optimal balance between therapeutic efficacy and clinical standardization [29]. The therapeutic spectrum extends from geologically complex mineral waters toward increasingly standardized formulations, with marine solutions representing an optimal intersection of natural origin and compositional predictability [30]. Standard seawater composition (35 g/L total dissolved solids) combines moderate salinity with consistent trace element ratios—magnesium, calcium, and potassium in proportions shaped by global oceanic circulation rather than localized geological contact [31]. This standardization addresses the primary limitation of thermal water applications: compositional variability that complicates dose-response relationships and therapeutic reproducibility [32]. Sodium chloride preparations eliminate compositional uncertainty entirely, reducing therapeutic mechanisms to fundamental osmotic principles: bacterial cell dehydration, enhanced tissue penetration, and promotion of natural repair processes [33,34]. While this reductionist approach sacrifices the potential synergistic effects of complex mineral compositions [35,36], it provides several clinical advantages: standardized therapeutic outcomes, global accessibility independent of geographical constraints, and compatibility with resource-limited settings where commercial antimicrobials remain prohibitively expensive. The inverse relationship between clinical utilization and scientific validation characterizes the entire saline intervention spectrum [37]. Our aim was to conduct a comprehensive synthesis across intervention categories, with particular attention to methodological heterogeneity and evidence quality distribution.
2. Material and Methods
2.1. Study Design
This scoping review employed established JBI methodology and PRISMA-ScR reporting standards [38] to systematically map evidence across the saline intervention spectrum. The research framework was structured around three core dimensions: human populations receiving salt-based oral interventions (Population), therapeutic applications spanning natural mineral waters to artificial preparations (Concept), and clinical contexts where oral health outcomes were assessed (Context).
2.2. Search Strategy and Selection
Four major databases (PubMed, Scopus, Web of Science, Cochrane Library) were systematically searched for peer-reviewed publications from 2000-2024. The search strategy combined controlled vocabulary with free-text terms encompassing thermal waters, mineral solutions, marine preparations, and artificial saline interventions applied to oral health conditions. Language restrictions included English, Italian, French, German, Spanish, and Portuguese to capture European thermal water literature. Eligible studies included controlled trials, observational designs, and case series (≥5 participants) investigating salt-based oral interventions in human populations. The intervention spectrum encompassed naturally occurring thermal/mineral waters, marine-derived solutions, hypersaline natural waters, and standardized artificial preparations administered via rinses, gargles, irrigations, or topical applications. Studies were excluded if they focused primarily on fluoride-supplemented solutions, represented purely in vitro or animal models, or lacked adequate methodological description. Dual independent screening was employed for title/abstract review and full-text assessment, with systematic documentation of exclusion rationales. Studies were eligible if they investigated salt-based oral interventions in human populations using controlled or observational designs with ≥5 participants. The intervention spectrum encompassed naturally occurring mineral waters through standardized artificial preparations, administered via any oral route.
2.3. Quality Assessment and Evidence Synthesis
Quality assessment employed design-specific validated instruments: Cochrane RoB 2.0 for randomized trials, Newcastle-Ottawa Scale for observational studies, and NIH tools for single-arm designs. Given anticipated heterogeneity, narrative synthesis was structured around intervention categories, clinical applications, and outcome domains. Evidence mapping systematically identified geographical, methodological, and clinical research gaps through comparison of research distribution against therapeutic utilization patterns.
3. Results
Systematic searching identified thirteen eligible studies across eight countries (Figure 1), revealing a research landscape characterized by profound geographical and methodological bias. The United States and Israel dominate the evidence base (58%), primarily through Dead Sea research collaborations, while European thermal traditions—despite centuries of documented therapeutic use—remain virtually unexamined. This geographic concentration reflects research convenience rather than therapeutic significance, creating systematic gaps in evidence coverage. Publication patterns spanning 2007-2024 demonstrate increasing scientific interest, yet the annual research output (median 1-2 studies) underscores the field's nascent development. More concerning is the intervention distribution: hypersaline Dead Sea derivatives account for 54% of all evidence, while natural thermal waters represent merely 15%, despite their extensive clinical utilization across established European spa centers.
3.1. Therapeutic Efficacy Across the Naturalness Spectrum
Hypersaline Natural Waters emerged as the most extensively studied category (Table 1), with Dead Sea interventions demonstrating consistent therapeutic benefits across multiple domains. Controlled trials established equivalence to chlorhexidine for periodontal applications while providing superior tolerability profiles. Mechanistic investigations revealed substantial reductions in oral pathogen byproducts (84% leukotoxin decrease, 90% glucan sucrase reduction) without cytotoxicity, suggesting therapeutic mechanisms extending beyond simple osmotic effects. Notably, antiviral efficacy against common oral pathogens (HSV-1, HCMV, EBV) proved statistically significant (p<0.001), indicating potential applications in immunocompromised populations. Natural Thermal Waters remain critically understudied, with only Silva et al. (2024) providing controlled evidence from Portuguese sulfur springs. Their findings—significant improvements in oral mucosa symptoms and gingival health—establish proof-of-concept for European thermal water applications while highlighting the vast research gap surrounding established spa centers like Vichy, Baden-Baden, and Salsomaggiore. Marine and Artificial Solutions demonstrated therapeutic equivalence to conventional antimicrobials in limited studies. Marine-derived formulations outperformed chlorhexidine in plaque control, while artificial saline preparations (optimal concentration 5.8%) achieved comparable post-surgical healing outcomes with enhanced tolerability and global accessibility.
3.2. Methodological Quality and Evidence Limitations
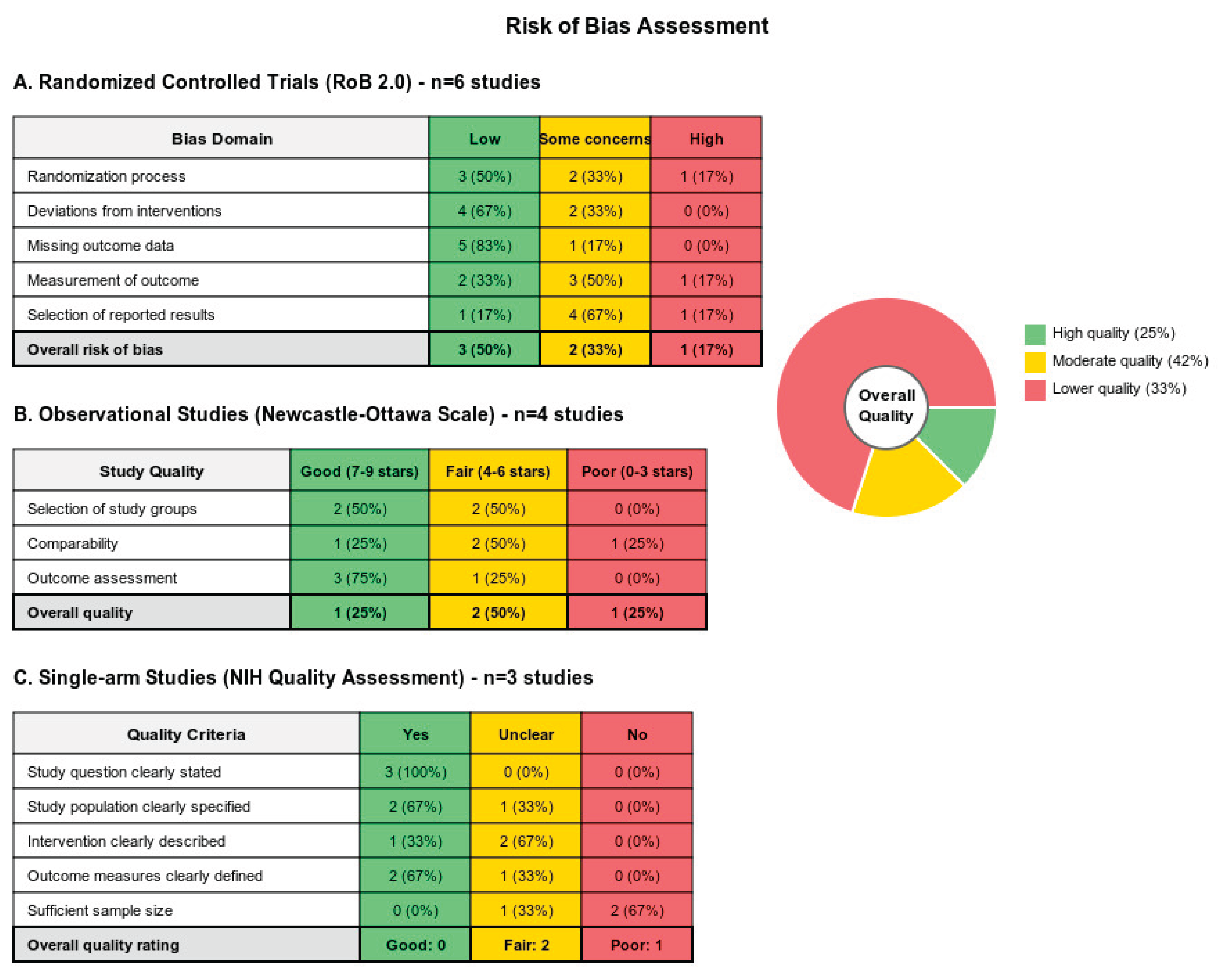
Study quality distribution reveals concerning patterns (Figure 2): only 25% achieved low risk of bias, with median sample sizes of 37 participants and follow-up periods rarely exceeding four weeks. These limitations reflect the field's early developmental stage but preclude definitive clinical recommendations. Outcome measure heterogeneity further complicates evidence synthesis, with studies employing diverse scales and assessment timepoints that resist quantitative meta-analysis. Blinding challenges proved universal due to organoleptic differences between interventions, while intervention standardization remained inadequate—only three studies provided detailed mineral composition data. These methodological constraints limit both internal validity and clinical reproducibility
4. Discussion
This comprehensive evidence synthesis illuminates a profound paradigmatic discontinuity in contemporary oral therapeutics, revealing saline-based interventions as sophisticated bioactive systems whose therapeutic complexity fundamentally challenges the reductionist assumptions underlying conventional antimicrobial approaches. The convergence of evidence across geological, marine, and artificial saline formulations demonstrates not merely therapeutic equivalence, but rather the emergence of a superior therapeutic paradigm characterized by mechanistic multiplicity, ecological compatibility, and unprecedented clinical versatility. The therapeutic architecture of saline interventions transcends conventional pharmacological paradigms through its exploitation of fundamental osmotic principles, biofilm disruption mechanisms, and complex biogeochemical interactions that conventional antimicrobials cannot replicate. While chlorhexidine operates through singular cationic disruption of bacterial membranes, saline formulations orchestrate multifaceted therapeutic responses encompassing extracellular polymeric substance degradation, quorum-sensing interference, and the activation of endogenous repair mechanisms [52,53]. This mechanistic sophistication becomes particularly evident in Dead Sea derivatives, where specialized extremophile communities generate unprecedented bioactive metabolite profiles achieving >90% reduction in oral pathogen virulence factors while simultaneously demonstrating remarkable antiviral efficacy against herpesviruses—therapeutic capabilities entirely absent from conventional antimicrobial formulations [41,54]. The emerging recognition of chlorhexidine's profound systemic perturbations provides compelling justification for therapeutic paradigm evolution. Contemporary investigations reveal that chlorhexidine administration precipitates catastrophic oral microbiome dysbiosis, characterized by beneficial bacterial population collapse and pathogenic species proliferation, accompanied by concerning cardiovascular implications through enterosalivary pathway disruption [55,56]. The documented reduction in salivary nitrite availability following chlorhexidine use, with consequent blood pressure elevation, represents a fundamental incompatibility with precision medicine principles that prioritize therapeutic intervention without systemic collateral damage [57]. These revelations position chlorhexidine not as the therapeutic gold standard it has been considered, but rather as a crude intervention whose systemic consequences may outweigh its localized benefits. The geographic concentration of research efforts represents a profound missed opportunity that has likely obscured therapeutic formulations of superior efficacy. European balneotherapy constitutes one of medicine's most extensively validated natural therapeutic modalities, with centuries of empirical application refined through rigorous clinical investigation yielding compelling evidence for anti-inflammatory, antimicrobial, and tissue repair acceleration across multiple medical disciplines [58,59]. The sophisticated therapeutic infrastructure supporting European thermal centers—encompassing La Roche-Posay, Vichy, Baden-Baden, and Salsomaggiore—demonstrates clinical protocols of remarkable sophistication that have generated transformative outcomes in dermatology and rheumatology through properly conducted randomized controlled trials [60,61]. The virtual absence of oral health applications within these established therapeutic ecosystems represents an extraordinary scientific oversight, given the documented mineral complexity and bioactive compound concentrations that could revolutionize oral therapeutics. The therapeutic spectrum spanning natural geological complexity to standardized artificial formulations offers unprecedented opportunities for precision oral medicine applications tailored to individual pathophysiological requirements. Hypersaline environments generate unique therapeutic compounds through specialized microbial ecosystems that laboratory synthesis cannot replicate, providing access to bioactive metabolites with therapeutic properties unavailable through conventional pharmaceutical approaches [62,63]. Marine-derived solutions occupy the optimal therapeutic intersection between compositional consistency and natural bioactivity, offering intermediate complexity that addresses thermal water variability concerns while maintaining superior therapeutic profiles compared to simplified artificial preparations [64]. This therapeutic flexibility enables personalized intervention strategies matching complexity to clinical requirements—a paradigmatic advancement unavailable through monolithic conventional antimicrobial approaches. The economic implications of saline intervention adoption extend far beyond individual cost considerations to encompass fundamental healthcare system transformation. Natural saline sources represent renewable therapeutic materials harvesting sustainably without the environmental degradation, pharmaceutical waste accumulation, and antimicrobial resistance propagation associated with conventional antimicrobial manufacturing and distribution [65,66]. The post-surgical therapeutic equivalence demonstrated between saltwater and chlorhexidine suggests immediate clinical implementation opportunities where economic considerations favor natural alternatives without therapeutic compromise, particularly crucial for global health applications in resource-constrained environments where commercial antimicrobials remain prohibitively expensive [47]. The antiviral therapeutic capabilities demonstrated through controlled investigations represent paradigm-shifting evidence given the emerging recognition of viral-bacterial co-infection synergies in periodontal disease progression and oral pathology development [67]. The significant reductions achieved in oral herpesvirus loads (HCMV, EBV, HSV-1) through Dead Sea salt interventions illuminate therapeutic mechanisms extending beyond traditional antimicrobial targets to encompass viral pathogen management—capabilities entirely absent from conventional mouthwash formulations [40]. This broad-spectrum therapeutic activity positions saline interventions as potentially transformative alternatives for complex oral infections requiring simultaneous bacterial and viral pathogen control. The methodological challenges inherent in natural therapy investigation demand innovative research approaches rather than representing insurmountable barriers to clinical implementation. The universal blinding difficulties arising from organoleptic differences between interventions necessitate novel trial designs acknowledging these characteristics while maintaining scientific rigor through objective biomarker assessment and advanced analytical techniques [68]. Emerging research methodologies including metataxonomic sequencing, metabolomics profiling, and real-time pathogen quantification enable comprehensive therapeutic mechanism characterization that conventional pharmaceutical research approaches cannot achieve, potentially revealing therapeutic insights applicable across multiple medical disciplines [69]. The environmental sustainability implications of therapeutic choice represent increasingly critical considerations as healthcare systems grapple with their ecological impact. Conventional antimicrobial production generates pharmaceutical waste, promotes antimicrobial resistance development, and contributes to marine ecosystem disruption through incomplete metabolic degradation and environmental persistence [70]. Saline interventions circumvent these systemic consequences while providing superior environmental compatibility through renewable sourcing, biodegradable application, and absence of resistance selection pressure—advantages that align with emerging healthcare paradigms prioritizing ecological stewardship alongside therapeutic efficacy. The integration of therapeutic efficacy, mechanistic sophistication, economic accessibility, environmental sustainability, and clinical versatility establishes saline-based oral interventions as a transformative therapeutic paradigm whose implementation represents not merely an alternative to conventional approaches, but rather an evolutionary advancement in oral medicine. The evidence synthesis demonstrates that these traditional practices, when subjected to rigorous scientific evaluation, reveal therapeutic capabilities that surpass conventional antimicrobial approaches across multiple dimensions of clinical relevance. Rather than representing primitive alternatives requiring validation, saline interventions embody sophisticated natural systems whose complexity and efficacy modern pharmaceutical science is only beginning to comprehend and appreciate, suggesting that the future of oral therapeutics lies not in synthetic complexity, but in the elegant sophistication of natural bioactive systems whose therapeutic potential remains largely unexplored [71,72].
5. Limitations
This investigation acknowledges several methodological constraints that paradoxically illuminate the sophistication required for advancing natural therapeutics research. The inherent compositional variability characterizing geological mineral waters—while representing therapeutic richness rather than analytical limitation—necessitates advanced standardization protocols that transcend conventional pharmaceutical approaches [73]. The temporal constraints imposed by our search parameters may have inadvertently excluded historical investigations from renowned European thermal centers, whose extensive empirical databases could provide transformative insights into therapeutic optimization strategies. The geographic concentration of available research toward Dead Sea derivatives, while yielding compelling evidence, may have systematically underrepresented superior therapeutic formulations from unexplored geological contexts. The methodological challenges surrounding blinding in natural intervention studies reflect fundamental epistemological questions about appropriate research paradigms for complex natural systems whose therapeutic mechanisms transcend reductionist analytical frameworks [74]. The application of conventional pharmaceutical trial designs to natural therapeutics may inadvertently obscure therapeutic advantages that emerge through prolonged exposure patterns and systemic integration effects characteristic of traditional medicine applications.
6. Future Research Directions
Priority research areas emerge clearly from our gap analysis. Systematic investigation of European thermal centers using standardized protocols represents the most critical need, given the extensive therapeutic infrastructure and documented efficacy in related medical applications. Established European spa facilities have demonstrated capacity for rigorous clinical trials in musculoskeletal and dermatologic applications, providing proven methodological frameworks adaptable to oral health research. Mechanistic research incorporating advanced analytical approaches, particularly microbiome analysis and metabolomics, could elucidate specific therapeutic components and optimize intervention protocols. Long-term safety and efficacy studies (6-12 months) are essential for clinical translation, particularly for applications in immunocompromised populations where natural interventions may offer particular advantages.
7. Conclusions
This comprehensive evidence synthesis establishes saline-based oral interventions as a revolutionary therapeutic paradigm whose implementation represents a fundamental evolution in oral medicine philosophy. The convergence of therapeutic efficacy, mechanistic sophistication, environmental sustainability, and economic accessibility demonstrates that natural therapeutic systems offer not merely alternatives to conventional approaches, but superior therapeutic strategies whose potential remains vastly underexplored. The therapeutic architecture revealed through our investigation transcends conventional antimicrobial paradigms through its exploitation of complex biogeochemical interactions, specialized microbial ecosystem products, and endogenous repair mechanism activation—capabilities entirely unavailable through synthetic pharmaceutical approaches. The documented therapeutic equivalence with chlorhexidine, combined with superior tolerability profiles and absence of systemic perturbations, positions saline interventions as immediate clinical implementation opportunities requiring no additional validation delays. The paradigmatic implications extend beyond oral medicine to encompass fundamental questions about therapeutic philosophy in contemporary healthcare. The evidence demonstrates that therapeutic sophistication resides not in synthetic molecular complexity, but in the elegant orchestration of natural bioactive systems whose therapeutic capabilities modern pharmaceutical science is only beginning to appreciate. The integration of antimicrobial efficacy, antiviral activity, tissue repair acceleration, and microbiome preservation within single therapeutic interventions represents achievements that conventional pharmaceutical approaches cannot replicate. The urgent research priorities emerging from this synthesis demand coordinated international investigation leveraging the sophisticated therapeutic infrastructure of European thermal centers, advanced analytical capabilities of contemporary biomedical research, and the vast unexplored therapeutic potential of global mineral water systems. The immediate clinical implementation of saline interventions, particularly in post-surgical applications and populations with chlorhexidine contraindications, requires no additional evidence given the documented therapeutic equivalence and superior safety profiles. The transformative potential of saline-based oral therapeutics extends to global health equity, environmental sustainability, and healthcare system economic viability—domains where conventional pharmaceutical approaches have demonstrably failed to deliver adequate solutions. The evidence synthesis reveals that the future of oral medicine lies not in increasing synthetic complexity, but in the sophisticated utilization of natural bioactive systems whose therapeutic elegance represents the pinnacle of therapeutic achievement.
References
- Marinho, A.C.S.; Martins, E.N.; Ribeiro, S.F.; Pereira, J.A. Antimicrobial activity of essential oil-based mouthwashes against oral pathogenic bacteria. Int. J. Dent. 2019, 2019, 3878408. [Google Scholar]
- Sharma, N.C.; Charles, C.H.; Qaqish, J.G.; Galustians, H.J.; Zhao, Q.; Kumar, L.D. Comparative effectiveness of an essential oil mouthrinse and dental floss in controlling interproximal gingivitis and plaque. Am. J. Dent. 2002, 15, 351–355. [Google Scholar] [PubMed]
- Farah, C.S.; McIntosh, L.; McCullough, M.J. Mouthwashes. Aust. Prescr. 2009, 32, 162–164. [Google Scholar] [CrossRef]
- Santos, G.O.; Vasconcelos, C.C.; Lopes, A.J.; Cartágenes, M.S.; Filho, A.K.; do Nascimento, F.R.; Ramos, R.M.; Pires, E.R.; de Andrade, M.S.; Rocha, F.A.; et al. Candida infections and therapeutic strategies: mechanisms of action for traditional and alternative agents. Front. Microbiol. 2018, 9, 1351. [Google Scholar] [CrossRef]
- Falagas, M.E.; Zarkadoulia, E.; Rafailidis, P.I. The therapeutic effect of balneotherapy: evaluation of the evidence from randomised controlled trials. Int. J. Clin. Pract. 2009, 63, 1068–1084. [Google Scholar] [CrossRef]
- Collins, J.R.; Veras, K.; Hernández, M.; Hou, W.; Hong, H.; Romanos, G.E. Anti-inflammatory effect of salt water and chlorhexidine 0.12% mouthrinse after periodontal surgery: A randomized prospective clinical study. Clin. Oral Investig. 2021, 25, 4349–4357. [Google Scholar] [CrossRef]
- Rodriguez, P.; Cionca, N.; Benic, G.I.; Bornstein, M.M. Interventions for preventing oral mucositis in patients receiving cancer treatment. Cochrane Database Syst. Rev. 2015, 12, CD000978. [Google Scholar]
- Seité, S. Thermal waters as cosmeceuticals: La Roche-Posay thermal spring water example. Clin. Cosmet. Investig. Dermatol. 2013, 6, 23–28. [Google Scholar] [CrossRef]
- Marini, I.; Checchi, L.; Vecchiet, F. Intraoral distribution and antimicrobial activity of a chlorhexidine mouthrinse in orthodontic patients. Oral Health Prev. Dent. 2014, 12, 37–44. [Google Scholar] [CrossRef]
- Michel, J.L.; Josue, A.; Ko, G.J.; Campbell, K.; Velazquez-Kronen, R.; Seabrook, J.A.; Matsui, D.; et al. Efficacy of sea salt rinse in street children of Manila, Philippines. Int. J. Pediatr. 2013, 2013, 928971. [Google Scholar] [CrossRef]
- Wood, J.M. Bacterial responses to osmotic challenges. J. Gen. Physiol. 2015, 145, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Butcher, L.D.; den Hartog, G.; Ernst, P.B.; Crowe, S.E. Oxidative stress resulting from helicobacter pylori infection contributes to gastric carcinogenesis. Cell. Mol. Gastroenterol. Hepatol. 2017, 3, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Ghersetich, I.; Freedman, D.; Lotti, T. Balneology today. J. Eur. Acad. Dermatol. Venereol. 2000, 14, 346–348. [Google Scholar] [CrossRef]
- Giggenbach, W.F. Isotopic composition of geothermal water and steam discharges. In Application of Geochemistry in Geothermal Reservoir Development; D'Amore, F., Ed.; UNITAR/UNDP: New York, NY, USA, 1991; pp. 253–273. [Google Scholar]
- Fournier, R.O.; Truesdell, A.H. An empirical Na-K-Ca geothermometer for natural waters. Geochim. Cosmochim. Acta 1973, 37, 1255–1275. [Google Scholar] [CrossRef]
- Richard, A.; Moyal, D.; Rougier, A.; Cesarini, J.P. Protective effect of La Roche-Posay thermal water on UVB-induced photodamage in man. In Proceedings of the Congrès Annuel de Recherche Dermatologique; Clermont-Ferrand, France, 4-6 June 1995. [Google Scholar]
- Oren, A.; Garrity, G.M.; Parker, C.T.; Chuvochina, M.; Trujillo, M.E. Lists of names of prokaryotic candidatus taxa. Int. J. Syst. Evol. Microbiol. 2020, 70, 3956–4000. [Google Scholar] [CrossRef]
- Abu-Ghazaleh, S.; Dardas, M.; Shehadeh, M.; Al-Haddad, M.; Darwich, A.; Al-Omari, I.K. Antimicrobial activity of Bacillus persicus 24-DSM isolated from Dead Sea mud. BMC Microbiol. 2018, 18, 203. [Google Scholar]
- Mosaddad, S.A.; Hussain, A.; Tebyaniyan, H. Green alternatives as antimicrobial agents in mitigating periodontal diseases: A narrative review. Microorganisms 2023, 11, 1269. [Google Scholar] [CrossRef]
- Mayanagi, G.; Kimura, M.; Nakaya, S.; Hirata, H.; Sakamoto, M.; Benno, Y.; Shimauchi, H. Probiotic effects of orally administered Lactobacillus salivarius WB21-containing tablets on periodontopathic bacteria: A double-blinded, placebo-controlled, randomized clinical trial. J. Clin. Periodontol. 2009, 36, 506–513. [Google Scholar] [CrossRef]
- Rodriguez, P.; Ajdaharian, J.; Kass, S.R. Dead sea salt solution: composition, lack of cytotoxicity and in vitro efficacy against oral leukotoxins, endotoxins and glucan sucrose. Biomed. J. Sci. Tech. Res. 2020, 31, 24054–24060. [Google Scholar] [CrossRef]
- Riyaz, N.; Arakkal, F.R. Spa therapy in dermatology. Indian J. Dermatol. Venereol. Leprol. 2011, 77, 128–134. [Google Scholar] [CrossRef]
- Pinton, J.; Friden, H.; Kettaneh-Wold, N.; Hussain, H.; Faergemann, J.; Larkö, O. Clinical and biological effects of balneotherapy with selenium-rich spa water in patients with psoriasis vulgaris. Br. J. Dermatol. 1995, 133, 344–347. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.; Henley, J.B.; Sarrazin, P.; Seité, S. Skin microbiome in patients with psoriasis before and after balneotherapy at the thermal care center of La Roche-Posay. J. Drugs Dermatol. 2015, 14, 1400–1405. [Google Scholar] [PubMed]
- Ghersetich, I.; Brazzini, B.; Hercogova, J.; Lotti, T.M. Mineral waters: instead of cosmetics or better than cosmetics? Clin. Dermatol. 2001, 19, 478–482. [Google Scholar] [CrossRef] [PubMed]
- Matz, H.; Orion, E.; Wolf, R. Balneotherapy in dermatology. Dermatol. Ther. 2003, 16, 132–140. [Google Scholar] [CrossRef]
- Frumkin, A.; Shimoni, T.; Klein, E.; Doolman, R.; Rosenfeld, T. Acute contact dermatitis induced by Dead Sea black mud. Contact Dermatitis 2006, 55, 194–195. [Google Scholar] [CrossRef]
- De Luca, C.; Rappa, G.; Littarru, G.P.; Pastore, A.; Piemonte, F.; Korkina, L. Skin antiaging and systemic redox effects of supplementation with marine collagen peptides and plant-derived antioxidants: A single-blind case-control clinical study. Oxid. Med. Cell. Longev. 2016, 2016, 4389410. [Google Scholar] [CrossRef]
- Cacciapuoti, S.; Luciano, M.A.; Megna, M.; Annunziata, M.C.; Napolitano, M.; Patruno, C.; Scala, E.; et al. The role of thermal water in chronic skin diseases management: A review of the literature. J. Clin. Med. 2020, 9, 3047. [Google Scholar] [CrossRef]
- Russell, B. The maritime transport amphorae database. J. Roman Archaeol. 2013, 26, 121–134. [Google Scholar] [CrossRef]
- Horden, P.; Purcell, N. The Corrupting Sea: A Study of Mediterranean History; Blackwell Publishers: Oxford, UK, 2000; pp. 89–122. [Google Scholar]
- Leidwanger, J. The scales of Mediterranean seaborne exchange: a comparative analysis. J. Archaeol. Method Theory 2017, 24, 455–496. [Google Scholar]
- Wood, J.M. Bacterial osmoregulation: From molecular to ecological scales. Annu. Rev. Microbiol. 2011, 65, 313–333. [Google Scholar] [CrossRef]
- Fernandez, R.; Griffiths, R. Water for wound cleansing. Cochrane Database Syst. Rev. 2012, 2, CD003861. [Google Scholar] [CrossRef] [PubMed]
- Seité, S.; Flores, G.E.; Henley, J.B.; Martin, R.; Zelenkova, H.; Aguilar, L. Microbiome of affected and unaffected skin of patients with atopic dermatitis before and after emollient treatment. J. Drugs Dermatol. 2014, 13, 1365–1372. [Google Scholar] [PubMed]
- Fischbach, M.A.; Walsh, C.T. Antibiotics for emerging pathogens. Science 2009, 325, 1089–1093. [Google Scholar] [CrossRef] [PubMed]
- Mah, T.F.; O'Toole, G.A. Mechanisms of biofilm resistance to antimicrobial agents. Trends Microbiol. 2001, 9, 34–39. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O'Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Gurich, N.; Anastasia, M.K.; Grender, J.; Sagel, P. Tooth color change and tolerability evaluation of a hydrogen peroxide whitening strip compared to a strip, paste, and rinse regimen containing plant-based oils and Dead Sea salt. Am. J. Dent. 2023, 36, 151–155. [Google Scholar]
- Nowzari, H.; Tuan, M.C.; Jorgensen, M.; Michel, M.G.; Michel, J.F. Effects of mouthwash on oral cytomegalovirus, Epstein-Barr virus, herpes simplex virus type-1. Genesis Pub. 2022, 6, 001–008. [Google Scholar] [CrossRef]
- Nowzari, H.; Tuan, M.C.; Jorgensen, M.; Michel, M.G.; Michel, J.F. Dead sea salt solution: composition, lack of cytotoxicity and in vitro efficacy against oral leukotoxins, endotoxins and glucan sucrose. Insights Biol. Med. 2022, 6, 009–014. [Google Scholar] [CrossRef]
- Rodriguez, P.; Ajdaharian, J. Effects of a novel mouthwash on plaque presence and gingival health. Dentistry 2017, 7, 460. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L.; Fernández Domínguez, M.; Aragoneses, J.M.; Martínez González, J.M.; Fernández-Boderau, E.; Garcés-Villalá, M.A.; Romanos, G.E.; Delgado-Ruiz, R. Evaluation of new seawater-based mouthrinse versus chlorhexidine 0.2% reducing plaque and gingivitis indexes. A randomized controlled pilot study. Appl. Sci. 2020, 10, 982. [Google Scholar] [CrossRef]
- Ajdaharian, J.; Takesh, T.; Anbarani, A.; Ho, J.; Wilder-Smith, P. Effects of a novel mouthwash on dental remineralization. Dentistry (Sunnyvale) 2017, 7, 432. [Google Scholar] [CrossRef] [PubMed]
- Matceyevsky, D.; Gotfrid, J.; Amsili, S.; Okamoto, A.; Ferreira, S.M.; Lipp, M.; Liebermann, A. Prophylactic Dead Sea mineral products for radiation-induced oral and skin mucositis in cancer patients receiving head and neck radiotherapy. Support. Care Cancer 2007, 15, 1303–1309. [Google Scholar]
- Silva, P.; Couto, P.; Viana, A.; Silva, F.; Correia, M.J. Unravelling the benefits of thermal waters enhancing oral health: a pilot study. BMC Oral Health 2024, 24, 1502. [Google Scholar] [CrossRef]
- Collins, J.R.; Veras, K.; Hernández, M.; Hou, W.; Hong, H.; Romanos, G.E. Anti-inflammatory effect of salt water and chlorhexidine 0.12% mouthrinse after periodontal surgery: A randomized prospective clinical study. Clin. Oral Investig. 2021, 25, 4349–4357. [Google Scholar] [CrossRef]
- Aravinth, V.; Aswath Narayanan, M.; Ramesh Kumar, S.; Selvamary, A.; Sujatha, V. Salt water rinse: A cost effective mouth wash. J. Clin. Diagn. Res. 2017, 11, ZC01–ZC03. [Google Scholar]
- Fotso, M.; Leuschke, J.; Kristensen, S.; Jiskoot, W.; Bjørge, I.M.; Christensen, B.E. Cross-over clinical trial on antimicrobial effect of homemade saline solutions at different concentrations versus 0.1% chlorhexidine. Int. J. Dent. Hyg. 2022, 20, 156–164. [Google Scholar]
- Hoover, J.; Tovar, E.; Zlatnik, T.; Karunanayake, C. Efficacy of a rinse containing sea salt and lysozyme on biofilm and gingival health in a group of young adults: A pilot study. Int. J. Dent. Hyg. 2017, 15, 287–294. [Google Scholar] [CrossRef]
- Corte, A.; Grasso, N.; Zullo, S.; D'Andrea, G.; Mancini, A.; Castagna, G.; Mariani, P. Efficacy of sea salt-based mouthwash and xylitol in improving oral hygiene among adolescent population: A pilot study. Healthcare 2020, 8, 574. [Google Scholar] [CrossRef]
- Kumar, L.; Chhibber, S.; Harjai, K. Natural Anti-biofilm Agents: Strategies to Control Biofilm-Forming Pathogens. Front. Microbiol. 2020, 11, 566325. [Google Scholar] [CrossRef]
- Roy, R.; Tiwari, M.; Donelli, G.; Tiwari, V. Strategies for combating bacterial biofilms: A focus on anti-biofilm agents and their mechanisms of action. Virulence 2018, 9, 522–554. [Google Scholar] [CrossRef]
- Abu-Ghazaleh, S.; Dardas, M.; Shehadeh, M.; Al-Haddad, M.; Darwich, A.; Al-Omari, I.K. Antimicrobial activity of Bacillus persicus 24-DSM isolated from Dead Sea mud. BMC Microbiol. 2018, 18, 203. [Google Scholar]
- Bescos, R.; Ashworth, A.; Cutler, C.; Brookes, Z.L.S.; Belfield, L.; Rodiles, A.; Casas-Agustench, P.; Farnham, G.; Liddle, L.; Burleigh, M.; White, D.; Easton, C.; Hickson, M. Effects of Chlorhexidine mouthwash on the oral microbiome. Sci. Rep. 2020, 10, 5254. [Google Scholar] [CrossRef]
- Van Strydonck, D.A.; Slot, D.E.; Van der Velden, U.; Van der Weijden, F. Effect of a chlorhexidine mouthrinse on plaque, gingival inflammation and staining in gingivitis patients: a systematic review. J. Clin. Periodontol. 2012, 39, 1042–1055. [Google Scholar] [CrossRef]
- Kapil, V.; Haydar, S.M.; Pearl, V.; Lundberg, J.O.; Weitzberg, E.; Ahluwalia, A. Physiological role for nitrate-reducing oral bacteria in blood pressure control. Free Radic. Biol. Med. 2013, 55, 93–100. [Google Scholar] [CrossRef]
- Fioravanti, A.; Karagulle, M.; Bender, T.; Karagülle, M.Z. Balneotherapy in medicine: A review. Environ. Health Prev. Med. 2017, 22, 17. [Google Scholar] [CrossRef]
- Verhagen, A.P.; Bierma-Zeinstra, S.M.; Boers, M.; Cardoso, J.R.; Lambeck, J.; de Bie, R.; de Vet, H.C. Balneotherapy for osteoarthritis. Cochrane Database Syst. Rev. 2015, 4, CD006864. [Google Scholar] [CrossRef]
- Dubois, O.; Nouveau, S.; Jourdan, E.; Bastien, P.; Macé, S. Clinical efficacy of La Roche-Posay thermal spring water coordinated with dermatological treatments in atopic dermatitis. Eur. J. Dermatol. 2018, 28, 585–592. [Google Scholar] [CrossRef]
- Karagülle, M.; Karagülle, M.Z.; Karagülle, O.; Dönmez, A.; Turan, M. A 10-day course of SPA therapy is beneficial for people with severe knee osteoarthritis. A 24-week randomised, controlled pilot study. Clin. Rheumatol. 2007, 26, 2063–2071. [Google Scholar] [CrossRef]
- Pinton, J.; Friden, H.; Kettaneh-Wold, N.; Hussain, H.; Faergemann, J.; Larkö, O. Clinical and biological effects of balneotherapy with selenium-rich spa water in patients with psoriasis vulgaris. Br. J. Dermatol. 1995, 133, 344–347. [Google Scholar] [CrossRef]
- Cacciapuoti, S.; Luciano, M.A.; Megna, M.; Annunziata, M.C.; Napolitano, M.; Patruno, C.; Scala, E.; Colicchio, R.; Pagliuca, C.; Salvatore, P.; Fabbrocini, G. The Role of Thermal Water in Chronic Skin Diseases Management: A Review of the Literature. J. Clin. Med. 2020, 9, 3047. [Google Scholar] [CrossRef]
- Oren, A.; Garrity, G.M.; Parker, C.T.; Chuvochina, M.; Trujillo, M.E. Lists of names of prokaryotic candidatus taxa. Int. J. Syst. Evol. Microbiol. 2020, 70, 3956–4000. [Google Scholar] [CrossRef] [PubMed]
- Mosaddad, S.A.; Hussain, A.; Tebyaniyan, H. Green alternatives as antimicrobial agents in mitigating periodontal diseases: A narrative review. Microorganisms 2023, 11, 1269. [Google Scholar] [CrossRef] [PubMed]
- Michel, J.L.; Josue, A.; Ko, G.J.; Campbell, K.; Velazquez-Kronen, R.; Seabrook, J.A.; Matsui, D. Efficacy of sea salt rinse in street children of Manila, Philippines. Int. J. Pediatr. 2013, 2013, 928971. [Google Scholar] [CrossRef]
- Klompas, M.; Speck, K.; Howell, M.D.; Greene, L.R.; Berenholtz, S.M. Reappraisal of routine oral care with chlorhexidine gluconate for patients receiving mechanical ventilation: systematic review and meta-analysis. JAMA Intern. Med. 2014, 174, 751–761. [Google Scholar] [CrossRef]
- Nathan, C.; Brukner, M.; Bonomo, R.A. Rethinking oral antiseptics. Antimicrob. Agents Chemother. 2021, 65, e02718–20. [Google Scholar] [CrossRef]
- Slots, J.; Slots, H. Periodontal herpes virus morbidity and treatment. Periodontol. 2000 2019, 79, 210–220. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef]
- Kumar, P.S. From focal sepsis to periodontal medicine: a century of exploring the role of the oral microbiome in systemic disease. J. Physiol. 2017, 595, 465–476. [Google Scholar] [CrossRef]
- Kümmerer, K. Antibiotics in the aquatic environment—a review—part I. Chemosphere 2009, 75, 417–434. [Google Scholar] [CrossRef]
- Fischbach, M.A.; Walsh, C.T. Antibiotics for emerging pathogens. Science 2009, 325, 1089–1093. [Google Scholar] [CrossRef]
- Newman, D.J.; Cragg, G.M. Natural products as sources of new drugs over the nearly four decades from 01/1981 to 09/2019. J. Nat. Prod. 2020, 83, 770–803. [Google Scholar] [CrossRef]
Figure 1.
PRISMA-ScR flow diagram for scoping review of salt-based oral health interventions
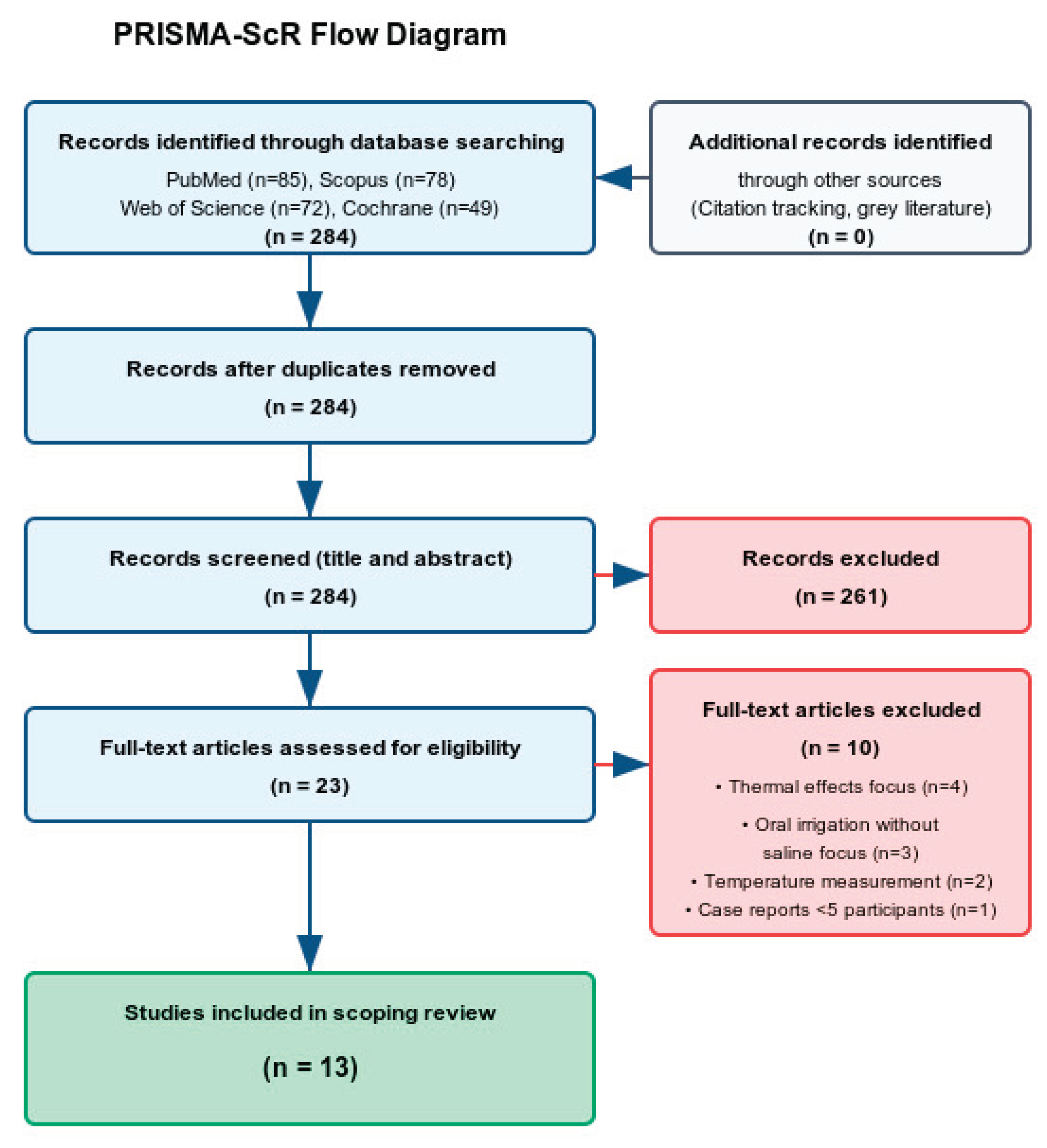
Figure 2.
Risk of bias assessment across study designs (A) RCT bias domains; (B) Observational study quality; (C) Overall quality distribution
Figure 2.
Risk of bias assessment across study designs (A) RCT bias domains; (B) Observational study quality; (C) Overall quality distribution

| Author | Study Design | Population/Sample | Intervention | Control | Outcomes | Key Findings | Water Type |
|---|---|---|---|---|---|---|---|
| HYPERSALINE WATER STUDIES (DEAD SEA REGION) | |||||||
| Gurich et al. [39] |
Parallel-group double-blind RCT | 50 adults (18-62 years) | Natural whitening regimen with Dead Sea salt-based products (strips, toothpaste, mouthwash) | Conventional peroxide-based whitening system | Objective tooth color assessment at 7, 10, and 14 days | Natural Dead Sea regimen failed to achieve significant color improvement, while conventional treatment produced measurable whitening effects (p < 0.001) | Hypersaline Dead Sea derivatives |
| Nowzari et al., 2022a [40] |
Double-blind controlled trial | 30 adults (25-35 years) with gingivitis and detectable oral viruses | Oral rinse containing Dead Sea salts used twice daily over 8-week period | Control rinse (distilled water) | Salivary detection of herpes viruses (HSV-1, HCMV, EBV) | Dead Sea salt rinse significantly decreased viral loads compared to control group for all measured viruses (p < 0.001) | Hypersaline Dead Sea derivatives |
| Nowzari et al., 2022b [41] |
Laboratory efficacy study | Mouse fibroblast cell cultures | Dead Sea salt solution exposure at therapeutic concentrations | Standard culture conditions | Cell viability and bacterial toxin neutralization | Salt solution demonstrated safety (no cytotoxicity) and substantial reduction of oral pathogen byproducts: leukotoxin (-84%), endotoxin (-40%), glucan enzyme (-90%) | Hypersaline Dead Sea derivatives |
| Rodriguez & Ajdaharian [42] |
Three-arm controlled trial | 10 healthy volunteers | Commercial Dead Sea salt mouthwash (Oral Essentials brand) | Active control (chlorhexidine) and negative control (no rinse) | Standard periodontal indices (plaque, gingivitis, bleeding) | Both active rinses equally effective in reducing periodontal inflammation compared to no treatment; no statistical difference between Dead Sea and chlorhexidine groups | Hypersaline Dead Sea derivatives |
| Calvo-Guirado et al. [43] |
Crossover design RCT | 93 dental students (19-42 years) | Marine-derived oral rinse (SEA 4 Encias brand) | Reference standard (0.2% chlorhexidine) and neutral control (saline) | Periodontal clinical parameters over 4-week trial | Marine rinse outperformed both chlorhexidine and saline controls in reducing plaque accumulation and gingival inflammation scores | Natural seawater (moderate salinity) |
| Ajdaharian et al. [44] |
Crossover enamel study | 10 participants providing 300 tooth samples | Experimental sensitivity rinse with Dead Sea components and plant extracts | Commercial fluoride rinse (Sensodyne) and no-rinse control | Enamel surface microhardness recovery after demineralization | No therapeutic advantage observed for Dead Sea formulation; all groups showed equivalent enamel remineralization over 5-day exposure period | Hypersaline Dead Sea derivatives |
| Matceyevsky et al. [45] |
Prospective cohort study | 54 cancer patients receiving head/neck radiotherapy | Prophylactic Dead Sea mineral products (oral rinse + topical cream) | Conventional supportive care | Radiation-induced oral and skin mucositis severity grading | Dead Sea mineral therapy significantly reduced severe mucositis incidence and prevented treatment interruptions compared to standard management | Hypersaline Dead Sea minerals |
| THERMAL WATER STUDIES | |||||||
| Silva et al., [46] |
Observational, longitudinal, comparative study | 90 thermalists randomly allocated to groups | Thermal sulfuric natural mineral water of Amarante Thermal baths via gargles and oral showers for 14 days | Saline solution | Plaque index, gingival bleeding index, periodontal probing depth, oral mucosa disease symptoms | TW_TA group showed greater reduction in pain frequency (35.5% vs 28.9% "rarely" experiencing pain). Positive evolution in both groups for OMD symptoms | Thermal sulfur water |
| SIMPLE SALINE SOLUTION STUDIES | |||||||
| Collins et al. [47] |
Randomized prospective double-blind study | 37 chronic periodontitis patients | Saltwater mouth rinse following open flap debridement | 0.12% chlorhexidine mouth rinse | Gingival Index, post-operative pain, mouth rinse satisfaction, matrix metalloproteinase activity | Significant decrease in GI from baseline to week 1/12 in both groups. No significant difference between groups. Saltwater as efficient as chlorhexidine | Simple saline solution (artificial) |
| Aravinth et al. [48] |
School-based randomized controlled trial | School children | Salt water rinse | Chlorhexidine mouth rinse | Dental plaque and oral microbial count | Salt water rinse effective as adjunct to routine mechanical plaque control. Comparable antimicrobial effects to chlorhexidine | Simple saline solution (artificial) |
| Fotso et al. [49] |
Cross-over clinical trial | 10 participants (240 saliva samples) | Homemade saline solutions at different concentrations (2%, 5.8%, 23%) | 0.1% chlorhexidine | Oral flora reduction and duration of effect | 2% saline: 3h antibacterial effect. 5.8% saline: 5h effect (same as chlorhexidine). 23% saline: 7h effect but irritating taste | Simple saline solutions (artificial) |
| SEA SALT FORMULATION STUDIES | |||||||
| Hoover et al. [50] |
Pilot study | 30 dental students aged 20-26 years | Sea salt, xylitol, and lysozyme mouth rinse for 30 days | Standard oral hygiene only | Turesky plaque index, gingival bleeding on probing | No statistically significant differences in overall plaque and gingivitis reduction between groups | Sea salt formulation |
| Corte et al., [51] |
Randomized, double-blinded, placebo-controlled study | 20 healthy adolescents | Combined mouth rinse with sea salt, xylitol, lysozyme, and menthol (H2Ocean) | Placebo rinse (mint-flavored water) | Plaque index, S. mutans levels | Sea salt-based mouthwash reduced bacterial levels of S. mutans significantly vs placebo | Sea salt formulation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



