Submitted:
01 July 2025
Posted:
02 July 2025
You are already at the latest version
Abstract
(1) Background: Cardiovascular disease (CVD) and edentulism are major public health challenges with shared risk factors and overlapping inflammatory pathways. (2) Methods: This study investigates the association between complete tooth loss and cardiovascular disease in a nationally representative sample of U.S. adults using data from the 2015–2018 National Health and Nutrition Examination Survey (NHANES). A cross-sectional analysis was conducted among adults aged ≥30 years, incorporating clinically assessed dental status and self-reported CVD outcomes. Weighted multivariate logistic regression models were conducted to investigate the relationship between complete edentulism and different cardiovascular conditions adjusted for age, sex, race/ethnicity, education, income, BMI, and diabetes status. 3) Results: Individuals with cardiovascular conditions, including coronary heart disease, heart attack, stroke, and congestive heart failure, had higher odds of complete edentulism compared to those without cardiovascular conditions, with odds ratios ranging from 1.60 to 1.85 (p < 0.01). Older age, lower educational attainment, and lower income were also associated with higher odds of tooth loss. (4) Conclusions: This study contributes further to the existing evidence of oral-systemic health link, showing that individuals with cardiovascular conditions are more likely to be edentulous.
Keywords:
Cardiovascular disease
; endodontics
; missing tooth
; tooth loss
; NHANES
; Cross sectional study
1. Introduction
Oral diseases such as dental caries, periodontitis are the most prevalent oral conditions worldwide [1,2]. It It is one of the leading public health concerns because of their widespread presence and their significant contribution to the global disease burden, which significantly increased between 1990 and 2015 [1,2]. Despite the advancement in medical and dentistry, the outcome of oral conditions has not improved over the last three decades [2,3,4]. Oral conditions continue to be a persistent challenge to health systems in most countries [2,3,4]. The number of people suffering from untreated oral diseases rose from an estimated 2.5 billion people in 1990 to 3.5 billion people in 2015 [2,3,4].
Tooth loss, whether partial or complete, is a noncommunicable condition influenced by various biological, behavioral, and socioeconomic factors [5,6,7]. Tooth loss is a long-term indicator of one’s lifetime experience with dental disease [5,6,7,8]. As stated earlier, tooth loss (full or partial) substantially increases chewing problems, resulting in the ingestion of a high-fat, low-fiber diet [9,10]. Physical pain, psychological distress, functional impairment, and diminished quality of life are some of the major consequences of tooth loss, all leading to considerable healthcare costs [9,10]. Moreover, evidence shows that the loss of multiple teeth has been associated with multiple systemic health outcomes and various chronic conditions [7,8]. These include hypertension [11], diabetes mellitus [12], peripheral arterial disease [13], cardiovascular and cerebrovascular diseases [14], heart failure, stroke, and mortality [15], angina pectoris [16], overweight and obesity [17], chronic kidney disease [18], chronic obstructive pulmonary disease [19], dementia [20], depression [21], cognitive decline [22], and certain malignancies such as liver [23] and pancreatic cancer [24], as well as with the presence of multi-morbidity, defined as the coexistence of two or more chronic conditions [25,26,27]. From an epidemiological perspective, it is estimated that between 60% and 80% of the elderly population are affected by at least one chronic condition [28]. The interplay between adverse oral conditions, age, and chronic illness is one of the most significant challenges facing healthcare systems worldwide, with high prevalence among older people [28].
With increasing life expectancy, the impact of poor oral health on the quality of life in older adults has become an important public health concern [29,30]. This issue is particularly critical in low- and middle-income countries, where the management of dental caries and periodontal diseases often relies on tooth extraction rather than preventive or restorative approaches [29,30].
Cardiovascular disease (CVD) and oral diseases are among the most prevalent chronic conditions globally, and both are a major public health and economic concern [31]. In 2018, the Centers for Disease Control and Prevention (CDC) estimated that CVD accounted for $147 billion in lost productivity in the United States, with total costs including morbidity and mortality, projected to reach $1.1 trillion by 2035 [31]. Cardiovascular disease account for nearly one-third of all global deaths, and over 800,000 Americans experience new or recurrent coronary events each year, according to the American Heart Association (AHA) [32,33].Emerging studies have reported a link between oral and cardiovascular health; however, existing studies have relied on small or region-specific samples, limiting the generalizability of their findings to broader populations. There are few studies that control for socioeconomic and demographic variables comprehensively while still showing an independent effect of CVD on complete edentulism [34,35,36,37]. In addition, it is unclear, based on current knowledge which of various CVD subtypes (e.g., CHF vs. stroke) are most positively associated with edentulism [38].
To address this gap, the present study aims to evaluate the association between cardiovascular disease and complete edentulism using data from the 2015-2018 National Health and Nutrition Examination Survey (NHANES), which provides clinically assessed dental measures and comprehensive demographic, behavioral, and health-related variables. We hypothesize that individuals with cardiovascular disease are more likely to be completely edentulous, potentially due to the influence of systemic and local inflammation.
2. Materials and Methods
2.1. Study Population
This cross-sectional study utilized data from the National Health and Nutrition Examination Survey (NHANES), a nationally representative program conducted by the Centers for Disease Control and Prevention (CDC) [39]. NHANES collects comprehensive health, nutritional, and dental data through structured interviews, surveys, clinical examinations, and laboratory investigations. The study population included adults aged 30 years and older from the 2015–2016 and 2017-2018 NHANES cycles. Inclusion criteria required participants to have complete data on tooth loss, cardiovascular disease (CVD) status, and other confounding covariates. Participants with missing data on these variables were excluded from the analysis. Since 1999, the NHANES has provided nationally representative data on health con- ditions, diseases, and associated risk factors in the U.S. This study employs a rigorous methodology, incorporating surveys, laboratory analyses, and clinical assessments to generate comprehensive public health insights [39]. A multistage, stratified, and clustered probability sampling strategy is used by NHANES, ensuring that the collected data are representative of the civilian, non-institutionalized U.S. population. NHANES (National Health and Nutrition Examination Survey) is a program conducted by the National Center for Health Statistics (NCHS) that collects data prospectively through standardized protocols during its cross-sectional survey cycle. All the participants signed written informed consent form. We analyzed already collected, publicly available data of 2015–2016 and 2017-2018 NHANES dataset and we used it as a secondary data. This study was conducted in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. The study analyzed publicly available NHANES data from 2017 to 2018 and was classified as non-human research, making it exempt from an International Review Board (IRB) review. Nationally representative estimates reflecting the broader U.S. population were obtained by applying survey weights and accounting for NHANES’ complex sampling design.
2.2. Definition of the Dependent Variable: Complete Tooth Loss
The primary outcome variable in this study was complete edentulism, defined as the absence of all natural permanent teeth, including third molars. This variable was operationalized as a binary construct, with “0” indicating individuals with dentition and “1” indicating individuals with complete tooth loss. According to the American Association of Oral and Maxillofacial Surgeons (AAOMS), edentulism refers to the loss of one or more functional teeth and is typically classified as either partial or complete, depending on the extent of tooth loss; common causes include dental caries, periodontal disease, and trauma [40]. For the purposes of this analysis, only individuals with complete edentulism were classified as cases and compared to those with preserved dentition. This binary classification enabled the assessment of the relationship between complete edentulism and cardiovascular disease within a cross-sectional epidemiologic framework.
2.3. Description of Independent Variable: Cardiovascular Diseases
CVD status was determined from self-reported physician diagnoses of coronary heart disease, heart attack (myocardial infarction), stroke and congestive heart failure. These conditions were analyzed individually and also grouped into a combined ‘heart disease’ category for broader analysis. CVD status was coded as a binary variable (Yes/No), with “Yes” assigned to individuals reporting at least one of the listed diagnoses, and “No” to those reporting none.
2.4. The Potential Confounding Variable
In this study, several demographic and health-related variables were categorized for analysis. These factors were adjusted for during the analysis. Age was grouped into 19–44, 45–59, and ≥60 years and was analyzed as a continuous variable. was classified as a binary variable (male or female) while race was treated as a nominal variable with categories including Non-Hispanic White, Non- Hispanic Black, Hispanic, Non-Hispanic Asian, and other races. Education level was divided into three categories: less than high school, high school/GED and more than high school education. Income level (ratio of family income to federal poverty level) as a categorical ordinal variable was categorized into <100%FPL, 100%-99%FPL, 200%-399%FPL, 400%+FPL.
Body mass index (BMI) was categorized into underweight, normal, overweight, obese and analyzed as categorical ordinal variable. Diabetes status was assessed using a single question, “Have you ever been told by a doctor or health professional that you have diabetes or sugar diabetes?” and responses were categorized into two groups: “no” for no diabetes and “yes” or “borderline” for the presence of diabetes or pre-diabetes.
2.5. Statistical Methods
Statistical analysis was conducted using descriptive statistics to summarize the sample characteristics. To compare groups with and without tooth loss, chi-square tests were used for categorical variables, while t-tests were used for continuous variables. To assess the relationship between tooth loss and CVD, a weighted multivariate binary logistic regression model was utilized, adjusting for potential confounding factors such as age, sex, education, race, body mass index, income level and diabetes status. Logistic regression models were applied to estimate odds ratios (ORs) with 95% confidence intervals (CIs) for the association between tooth loss and CVD, adjusting for the identified confounders. A p-value of less than 0.05 was considered statistically positive. All statistical analyses were performed using STATA 17 software (StataCorp LLC, College Station, TX, USA).
3. Results
Table 1 summarizes the weighted characteristics of the study population by complete edentulism status. Of the 11,287 participants, 1,763 (15.62%) were completely edentulous. The proportion of complete tooth loss was higher among those with heart disease (1.76%) compared to those without (6.42%) (P < 0.0001). Participants with a history of myocardial infarction had a complete tooth loss rate of 0.78%, while the rate among those without was 7.42% (P < 0.0001). Those with coronary heart disease had a rate of 0.74% compared to 7.39% among those without (P < 0.0001). For individuals with congestive heart failure, the rate was 0.58%, while it was 7.61% among those without (P < 0.0001). Stroke was linked to an edentulism rate of 0.64%, compared to 7.61% in those without stroke (P < 0.0001). Gender distribution showed similar proportions: 6.65% in males and 6.78% in females (P = 0.53). Edentulism was highest among White participants (7.41%), followed by Black (6.70%), Hispanic (2.72%), Asian (2.10%), and Others (1.87%) (P = 0.00017). Age differences were observed, with higher rates among older age groups, ranging from 0.28% in participants aged 6–11 to 3.14% in those above 60 years (P < 0.0001). Participants with lower education levels (0–11 years) had an edentulism rate of 2.13%, compared to 1.35% among those with more than a high school education (P < 0.0001). Edentulism was most frequent in the lowest income group (<100% FPL) at 30.42%, and it decreased with higher income levels (P < 0.0001). Among BMI categories, edentulism was observed at 2.52% among obese individuals and 1.97% among those with normal BMI (P < 0.0001). Diabetes status showed an edentulism rate of 1.24% among participants with diabetes and 10.99% among those without, with no notable difference across groups (P = 0.0976).
Table 2 displays weighted logistic regression results for factors related to complete tooth loss. Participants with a history of myocardial infarction had higher odds of tooth loss (OR = 1.78; 95% CI: 1.27–2.49; P = 0.001), while sex was not associated (OR = 1.04; 95% CI: 0.86–1.26; P = 0.648). Compared to younger adults, odds were higher among those aged 45–59 (OR = 2.23; 95% CI: 1.61–3.09) and ≥60 (OR = 4.31; 95% CI: 2.88–6.46) (P < 0.001 for both). Odds were lower among those with a high school diploma/GED (OR = 0.64; 95% CI: 0.50–0.82; P = 0.001) and more than high school education (OR = 0.40; 95% CI: 0.31–0.50; P < 0.001) compared to those with less education. Compared to individuals <100% FPL, lower odds were observed in the 200–399% (OR = 0.54; 95% CI: 0.37–0.78; P = 0.002) and ≥400% (OR = 0.38; 95% CI: 0.25–0.57; P < 0.001) FPL groups. No difference was found for the 100–199% FPL group (OR = 0.92; 95% CI: 0.69–1.23; P = 0.592). Compared to Hispanic individuals, odds of tooth loss were higher among Non-Hispanic White (OR = 1.54; P = 0.027), Black (OR = 1.62; P = 0.010), Asian (OR = 1.99; P = 0.005), and Other racial/ethnic groups (OR = 2.50; P = 0.001). Diabetes was not associated with tooth loss, with odds ratios of 1.13 (diagnosed; P = 0.367) and 1.12 (borderline; P = 0.631).
Table 3 presents the logistic regression results examining the association between heart disease (CHD, MI, CHF, or stroke) and complete tooth loss. Individuals with heart disease had higher odds of tooth loss (OR = 1.70; 95% CI: 1.35–2.14; P < 0.001). Sex was not associated (OR = 1.04; 95% CI: 0.86–1.25; P = 0.664). Participants aged 45–59 years had higher odds compared to younger individuals (OR = 2.19; 95% CI: 1.59–3.02; P < 0.001), and those aged 60 and above had even higher odds (OR = 4.06; 95% CI: 2.72–6.07; P < 0.001). For education, individuals with a high school diploma or GED had lower odds than those with less than high school education (OR = 0.65; 95% CI: 0.50–0.83; P = 0.001), and those with education beyond high school had even lower odds (OR = 0.40; 95% CI: 0.32–0.50; P < 0.001). Regarding income, participants in the 200–399% FPL group had lower odds than those in the <100% FPL category (OR = 0.54; 95% CI: 0.37–0.78; P = 0.002), as did those in the ≥400% FPL group (OR = 0.38; 95% CI: 0.26–0.58; P < 0.001). The 100–199% FPL group showed no difference (OR = 0.92; 95% CI: 0.69–1.22; P = 0.566). Compared to Hispanic individuals, the odds of complete tooth loss were higher among Non-Hispanic White (OR = 1.49; 95% CI: 1.02–2.19; P = 0.039), Non-Hispanic Black (OR = 1.57; 95% CI: 1.09–2.26; P = 0.017), Non-Hispanic Asian (OR = 1.99; 95% CI: 1.24–3.19; P = 0.006), and Other race/ethnicities (OR = 2.45; 95% CI: 1.48–4.06; P = 0.001). Diabetes was not associated with tooth loss (OR = 1.08; 95% CI: 0.82–1.42; P = 0.558) nor was borderline diabetes (OR = 1.06; 95% CI: 0.65–1.74; P = 0.785). For BMI, compared to underweight participants, the odds were 0.71 for normal weight (95% CI: 0.23–2.18; P = 0.542), 0.83 for overweight (95% CI: 0.26–2.64; P = 0.747), and 0.73 for obese individuals (95% CI: 0.24–2.20; P = 0.574).
Table 4 displays the logistic regression results for the association between coronary heart disease (CHD) and complete tooth loss. Participants with CHD had higher odds of tooth loss (OR = 1.60; 95% CI: 1.16–2.20; P = 0.005). No association was observed for sex (OR = 1.03; 95% CI: 0.85–1.24; P = 0.721). Compared to younger adults, those aged 45–59 years had higher odds (OR = 2.26; 95% CI: 1.63–3.12; P < 0.001) and those aged 60 and above showed even greater odds (OR = 4.35; 95% CI: 2.90–6.52; P < 0.001). Individuals with a high school diploma or GED had lower odds than those with less than high school education (OR = 0.66; 95% CI: 0.51–0.85; P = 0.003), and those with more than high school education had lower odds as well (OR = 0.40; 95% CI: 0.31–0.51; P < 0.001). Regarding income, participants in the 200–399% FPL range had lower odds than those in the <100% FPL group (OR = 0.53; 95% CI: 0.37–0.78; P = 0.002), as did those in the ≥400% FPL category (OR = 0.37; 95% CI: 0.25–0.56; P < 0.001). The 100–199% FPL group showed no difference (OR = 0.93; 95% CI: 0.70–1.23; P = 0.617).Compared to Hispanics, higher odds were seen in Non-Hispanic White (OR = 1.52; 95% CI: 1.03–2.24; P = 0.035), Non-Hispanic Black (OR = 1.62; 95% CI: 1.13–2.34; P = 0.010), Non-Hispanic Asian (OR = 1.99; 95% CI: 1.25–3.17; P = 0.005), and Other racial/ethnic groups (OR = 2.55; 95% CI: 1.54–4.21; P = 0.001). Diabetes was not associated with complete tooth loss (OR = 1.13; 95% CI: 0.85–1.52; P = 0.365) nor was borderline diabetes (OR = 1.08; 95% CI: 0.65–1.78; P = 0.751).For BMI, odds were 0.71 among individuals with normal weight (95% CI: 0.23–2.17; P = 0.537), 0.82 among those overweight (95% CI: 0.25–2.61; P = 0.731), and 0.74 among those with obesity (95% CI: 0.24–2.25; P = 0.593) compared to underweight participants.
Table 5 shows the logistic regression model examining the association between congestive heart failure (CHF) and complete tooth loss. Participants with CHF had higher odds of tooth loss (OR = 1.85; 95% CI: 1.29–2.67; P = 0.002). Sex showed no association (OR = 1.01; 95% CI: 0.84–1.23; P = 0.840). Compared to younger adults, odds were higher among those aged 45–59 years (OR = 2.26; 95% CI: 1.64–3.11; P < 0.001) and ≥60 years (OR = 4.42; 95% CI: 2.92–6.68; P < 0.001). Those with a high school diploma or GED had lower odds of tooth loss than those with less education (OR = 0.64; 95% CI: 0.50–0.83; P = 0.001), and those with more than high school education had even lower odds (OR = 0.39; 95% CI: 0.31–0.50; P < 0.001). For income, individuals in the 200–399% FPL group had lower odds than those below 100% FPL (OR = 0.53; 95% CI: 0.37–0.78; P = 0.002), as did those in the ≥400% FPL group (OR = 0.38; 95% CI: 0.25–0.57; P < 0.001). No difference was observed for the 100–199% FPL group (OR = 0.92; 95% CI: 0.69–1.22; P = 0.556). Compared to Hispanic individuals, odds of tooth loss were higher among Non-Hispanic White (OR = 1.54; 95% CI: 1.04–2.27; P = 0.029), Non-Hispanic Black (OR = 1.59; 95% CI: 1.10–2.30; P = 0.014), Non-Hispanic Asian (OR = 1.97; 95% CI: 1.23–3.15; P = 0.006), and Other racial groups (OR = 2.61; 95% CI: 1.58–4.32; P < 0.001). Diabetes was not associated with tooth loss (OR = 1.12; 95% CI: 0.84–1.50; P = 0.404) nor was borderline diabetes (OR = 1.06; 95% CI: 0.64–1.74; P = 0.814). For BMI, the odds were 0.71 for normal weight (95% CI: 0.23–2.21; P = 0.552), 0.83 for overweight (95% CI: 0.26–2.67; P = 0.751), and 0.74 for obese individuals (95% CI: 0.24–2.22; P = 0.581) compared to underweight participants.
Table 6 presents regression results for the association between stroke and complete tooth loss. Participants with a history of stroke had higher odds of tooth loss (OR = 1.64; 95% CI: 1.17–2.29; P = 0.005), while sex was not associated (OR = 1.01; 95% CI: 0.84–1.23; P = 0.849).Compared to younger adults, odds were higher among those aged 45–59 years (OR = 2.26; 95% CI: 1.64–3.12; P < 0.001) and ≥60 years (OR = 4.44; 95% CI: 2.95–6.69; P < 0.001). Participants with a high school diploma had lower odds than those with less education (OR = 0.64; 95% CI: 0.50–0.83; P <0.001), and those with education beyond high school had even lower odds (OR = 0.40; 95% CI: 0.31–0.50; P < 0.001). Lower odds were observed in the 200–399% FPL group (OR = 0.54; 95% CI: 0.37–0.78; P = 0.002) and the ≥400% FPL group (OR = 0.38; 95% CI: 0.25–0.57; P < 0.001), with no difference in the 100–199% FPL group (OR = 0.92; 95% CI: 0.69–1.23; P = 0.601).Compared to Hispanic individuals, the odds of tooth loss were higher among Non-Hispanic White (OR = 1.55; 95% CI: 1.05–2.27; P = 0.027), Non-Hispanic Black (OR = 1.60; 95% CI: 1.11–2.32; P = 0.013), Non-Hispanic Asian (OR = 2.01; 95% CI: 1.26– 3.20; P = 0.005), and Other racial/ethnic groups (OR = 2.58; 95% CI: 1.56–4.29; P = 0.001). Diabetes was not associated with tooth loss (OR = 1.12; 95% CI: 0.85–1.49; P = 0.390), nor was borderline diabetes (OR = 1.06; 95% CI: 0.65–1.72; P = 0.787). For BMI, compared to underweight individuals, the odds of tooth loss were lower in the normal (OR = 0.68; 95% CI: 0.22–2.09; P = 0.499), overweight (OR = 0.80; 95% CI: 0.25–2.53; P = 0.698), and obese (OR = 0.72; 95% CI: 0.24–2.17; P = 0.557) categories.
4. Discussion
The present study investigated the association between cardiovascular disease and tooth loss in a large, nationally representative sample of U.S adults. Our analysis demonstrated a positive association between complete tooth loss and all major types of cardiovascular disease, including heart attack, coronary heart disease, stroke, and congestive heart failure. Congestive heart disease was found to have the strongest association with tooth loss. This study is among the few that have comprehensively examined the association between complete edentulism and various cardiovascular disease subtypes within a U.S. population, while accounting for a wide range of demographic and health-related confounders. A cross-sectional study in (2021) conducted a population-based survey in older Mexican adults support our findings of the association between complete edentulism and chronic diseases, including cardiovascular and cerebrovascular events [41]. Additionally, a case control study in (2022) reported that patients under 70 years old who had experienced myocardial infarction showed positively higher rates of edentulism, implicating tooth loss as a correlate of cardiovascular pathology [42]. Furthermore, a 7-Year follow-up prospective single cohort study in (2024) examined cardiovascular patients undergoing full-arch implant-prosthetic rehabilitation and noted the high prevalence of edentulism in this group, framing it within the broader context of systemic health [43].
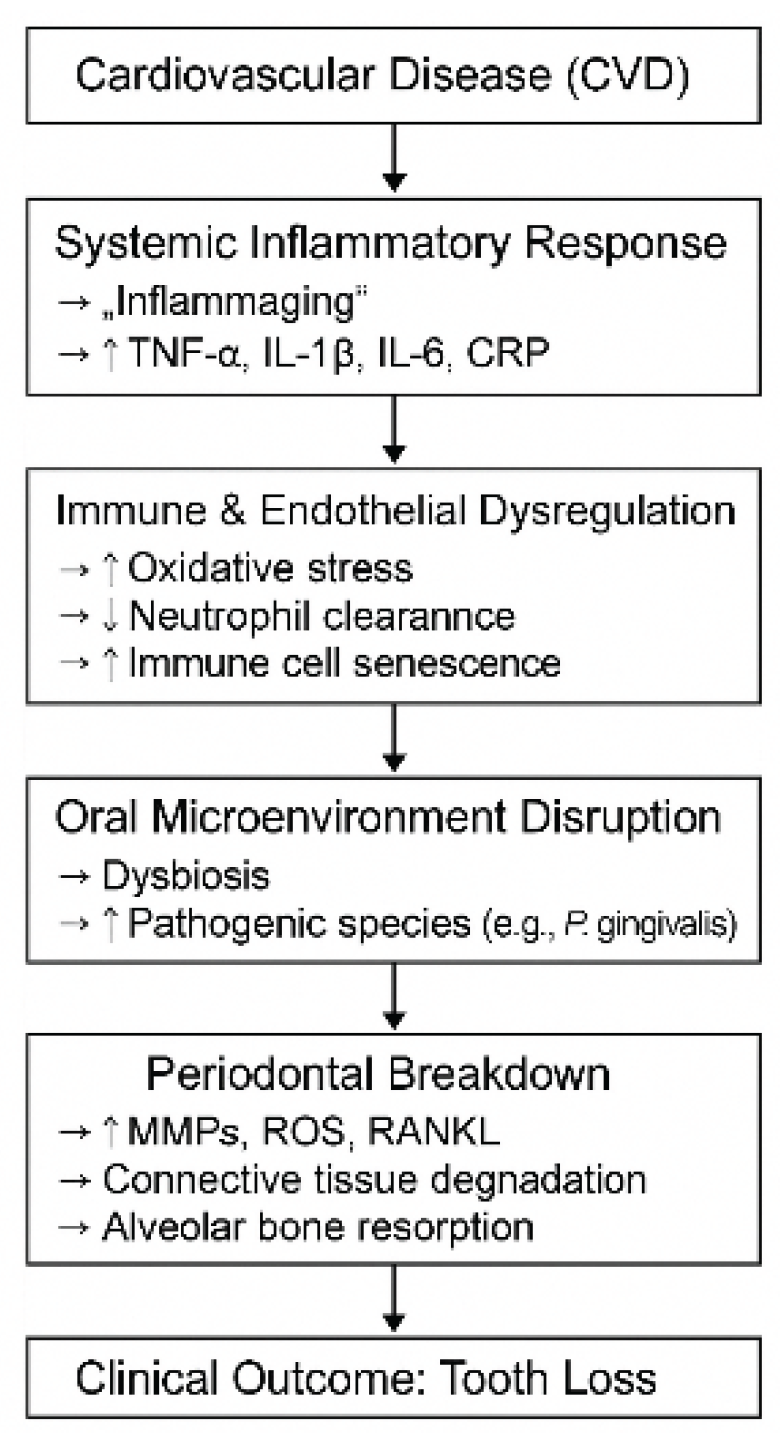
One of the potential mechanisms underlying this association is the presence of chronic low-grade systemic inflammation (termed “inflammaging”, a defining feature shared by both periodontitis and atherosclerosis [44]. Inflammatory mediators such as acute-phase proteins, pro-inflammatory cytokines (e.g., TNF-α, IFN-γ IL-1β, IL-6, IL-2), C-reactive protein (CRP) and elevated leukocyte counts are often elevated in both conditions [44,45,46]. These immune signals contribute not only to vascular dysfunction but also to periodontal tissue breakdown, which highlight inflammation as a common pathway in the pathophysiology of both diseases [44,45,46]. In patients with CVD, these pro-inflammatory mediators are often upregulated due to endothelial dysfunction, lipid oxidation, and immune activation [44,45,46]. Once released into the bloodstream, these cytokines, such as IFN-γ, TNF-α, and interleukins, can disrupt host-microbial homeostasis at distant sites, including the periodontium [44,45,46]. This disruption triggers exaggerated immune responses to oral pathogens, heightening local inflammation in the gingival tissues [44,45,46]. As this inflammatory cascade progresses, it stimulates the release of tissue-destructive enzymes and signaling molecules such as matrix metalloproteinases (MMPs), reactive oxygen species (ROS), and receptor activator of nuclear factor kappa-B ligand (RANKL) [47,48]. These mediators collectively drive the degradation of connective tissue and alveolar bone, weakening the periodontium and increasing vulnerability to attachment loss and eventual tooth loss [47,48].
Moreover, individuals with CVD often show signs of immune dysregulation [49,50]. Neutrophil chemotaxis, phagocytic capacity, and oxidative burst, key components of innate immunity, are often impaired [51,52]. These changes reduce the body’s ability to clear pathogenic biofilms from the gingival sulcus [51,52]. Meanwhile, macrophages tend to shift toward a pro-inflammatory M1 phenotype, sustaining cytokine release without effective resolution of inflammation [53]. T-cell regulation is also disturbed, with a decline in regulatory T-cell activity and a rise in senescent CD8+ T cells, which amplify the inflammatory burden in periodontal tissues [54].
Beyond inflammatory pathways, vascular health plays a key role in oral outcomes [55,56]. CVD is often associated with impaired vascular perfusion and endothelial damage, which can reduce blood flow to the gingiva and periodontal structures [55,57]. This limited circulation restricts oxygen and nutrient delivery, delaying tissue repair and compromising healing [55,57]. As a result, the periodontium becomes more vulnerable to breakdown, setting the stage for tooth loss [55,57].
In contrast, periodontal pathogens are known to trigger platelet aggregation, a critical step in thrombus formation, which can worsen atherosclerotic lesions [58,59,60,61]. This pro-thrombotic potential adds a further risk to systemic health [58,59,60,61]. Additionally, tooth loss itself has been correlated with non-invasive markers of subclinical atherosclerosis, including carotid artery wall thickening, arterial stenosis, and plaque formation [58,59,60,61,62]. These vascular changes reflect the far-reaching consequences of oral disease on systemic health [58,59,60,61,62].
It is worth noting that pharmacologic management of cardiovascular disease (CVD) commonly involves the long-term use of medications such as antihypertensives (e.g., calcium channel blockers, ACE inhibitors), beta-adrenergic blockers, and diuretics [63,64]. While these medications are essential for controlling blood pressure and preventing cardiovascular events, they often induce xerostomia (dry mouth), either through anticholinergic activity or diuretic-induced dehydration [63,64]. Saliva plays a vital role in buffering oral pH, modulating microbial flora, supporting mechanical cleansing [65]. When salivary flow is reduced, especially over time, oral self-cleansing becomes impaired [66]. This enhances bacterial colonization and plaque accumulation along the gingival margins, particularly by pathologic species such as Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans [66]. As a result, these conditions promote periodontal inflammation, enamel demineralization, and clinical attachment loss [67].
Evidence has shown that access to dental care significantly influences oral health outcomes [68,69]. Patients with chronic cardiovascular conditions often face barriers to maintaining regular oral healthcare [68,69]. These may include physical limitations, financial burdens, completing health priorities, or medication burdens [68,69]. In such contexts, oral hygiene routines may decline, which may contribute to the accumulation of dental plaque and the progression of periodontal disease [68,69]. In addition, behavioral risk factors such as smoking, infrequent dental visits, or inadequate hygiene can compound these challenges, accelerating the pathway toward edentulism [70].
Furthermore, emerging evidence supports a strong association between oral infections and systemic diseases, with invasive oral pathogens playing a key role in triggering systemic inflammatory responses through the release of mediators [71]. This connection is particularly relevant for individuals with chronic conditions like cardiovascular disease (CVD), where biological and immunological changes may amplify the risk of oral deterioration, including tooth loss [71].
Collectively, this evidence highlights a multifactorial and synergistic relationship between cardiovascular disease and oral health decline. Shared inflammatory pathways, impaired immune responses, compromised vascular function, medication side effects, and behavioral determinants all interact to increase susceptibility to complete tooth loss in individuals with CVD. Recognizing these overlapping mechanisms emphasizes the need for integrated medical-dental care models, especially for individuals managing chronic systemic diseases.
Figure 1.
Proposed pathway illustrating the inflammatory and immunological mechanisms linking cardiovascular disease to tooth loss.
Figure 1.
Proposed pathway illustrating the inflammatory and immunological mechanisms linking cardiovascular disease to tooth loss.
4.1. Limitation of Research
Despite its strengths, this study has several limitations that should be acknowledged. First, its cross-sectional design precludes any determination of causality between cardiovascular disease and complete edentulism. The directionality of the association stays uncertain, and longitudinal studies are necessary to confirm temporal relationships. Second, although the analysis adjusted for multiple confounders, the possibility of residual confounding cannot be entirely excluded, especially for factors such as smoking history, medication use, or oral hygiene practices, which were not fully accounted for in this dataset. Third, cardiovascular disease status was self-reported, which may introduce recall bias or misclassification. Finally, while NHANES includes clinical dental assessments, it does not capture the specific causes of tooth loss, such as trauma versus periodontal disease, which may influence the interpretation of the observed associations.
This study has several noteworthy strengths. The use of data from the National Health and Nutrition Examination Survey (NHANES) enhances the study’s external validity, as NHANES employs a large, nationally representative sample of U.S. adults and includes both clinical dental assessments and self-reported cardiovascular outcomes. Additionally, the study evaluates multiple subtypes of cardiovascular disease (heart attack, coronary heart disease, congestive heart failure, and stroke), allowing for a more detailed understanding of how various forms of CVD are associated with complete tooth loss. Moreover, the analysis incorporates comprehensive adjustment for demographic, socioeconomic, and health-related confounders.
4.2. Future Perspectives
Future research should aim to build upon these findings by utilizing longitudinal study designs to better determine causal relationships between cardiovascular disease and edentulism. Prospective cohort studies could help determine the temporal sequence and clarify whether tooth loss contributes to cardiovascular risk, or vice versa. In addition, future analyses should incorporate biomarkers of inflammation, detailed oral health histories, and objective cardiovascular assessments to explore the underlying biological mechanisms more precisely. Including variables such as smoking status, oral hygiene behaviors, access to dental care, and medication use would provide a more comprehensive understanding of the multifactorial relationship between oral and systemic health. From a clinical standpoint, interdisciplinary strategies that integrate dental evaluations into cardiovascular risk assessments could enhance early identification of at-risk individuals. Public health policies should also emphasize the importance of maintaining oral health as a preventive measure against systemic diseases, particularly among underserved and aging populations.
5. Conclusion
This study demonstrates a positive association between cardiovascular disease and complete edentulism among U.S. adults. Individuals with congestive heart failure had higher likelihood of complete edentulism. These findings are consistent with the growing body of evidence supporting association between oral and cardiovascular disease through common biologic pathways, such as chronic inflammation, immune dysregulation, and endothelial dysfunction. Recognizing edentulism not only as a dental outcome but also as a potential marker of systemic disease burden may enhance both clinical and public health strategies.
For clinicians, these results emphasize the value of including oral health assessments, particularly edentulism, in comprehensive evaluations of cardiovascular risk. Early referral to dental care providers could aid in prevention and promote holistic care. For policy makers, the findings highlight the urgent need to incorporate oral health into national chronic disease prevention frameworks. Expanding access to dental services for high-risk groups, such as older adults and low-income populations, may reduce the dual burden of tooth loss and cardiovascular disease. While this study focused on CVD as a predictor, the bidirectional interplay between oral and systemic health warrants ongoing investigation. Finally, interdisciplinary collaboration and greater investment in preventive oral care may play a fundamental role in improving overall population health.
Author Contributions
All authors contributed significantly to the research by providing critical feedback, shaping the analysis, and assisting in the development of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
No funding was received for conducting this study. The authors have no relevant financial or non-financial interests to disclose.
Institutional Review Board Statement
Ethical review and approval were exempted for this study as the Institutional Review Board (IRB) determined on the 3 May 2023 that the proposed activity did not involve research on human subjects, as defined by the Department of Health and Human Services (DHHS) and Food and Drug Administration (FDA) regulations.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data used in this article are publicly available and can be found at the Centers for Disease Control and Prevention (CDC) National Center for Health Statistics: National Health and Nutrition Examination Survey (NHANES) Questionnaires, Datasets, and Related Documentation, available at the following website: Accessed December 4, 2023
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Marcenes, W.; Kassebaum, N.J.; Bernabé, E.; Flaxman, A.; Naghavi, M.; Lopez, A.; Murray, C.J.L. Global Burden of Oral Conditions in 1990–2010: A Systematic Analysis. J. Dent. Res.2013, 92, 592–597. [Google Scholar] [CrossRef] [Green Version]. [CrossRef]
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W. Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef]. [CrossRef]
- Abodunrin, O.R.; Olagunju, M.T.; Alade, O.T.; Foláyan, M.O. Relationships between Oral Health and the Sustainable Development Goals: A Scoping Review. BioMed 2023, 3, 460-470. [CrossRef]
- Zhang, S.-Z.; Xie, L.; Shang, Z.-J. Burden of Oral Cancer on the 10 Most Populous Countries from 1990 to 2019: Estimates from the Global Burden of Disease Study 2019. Int. J. Environ. Res. Public Health 2022, 19, 875. [CrossRef]
- Al-Rafee, M. A. (2020). The epidemiology of edentulism and the associated factors: A literature review. Journal of Family Medicine and Primary Care, 9(4), 1841–1843. [CrossRef]. [CrossRef]
- Emami, E., de Souza, R. F., Kabawat, M., & Feine, J. S. (2013). The impact of edentulism on oral and general health. International Journal of Dentistry, 2013, Article 498305. [CrossRef]. [CrossRef]
- McGarry, T. J., Nimmo, A., Skiba, J. F., Ahlstrom, R. H., Smith, C. R., & Koumjian, J. H. (1999). Classification system for complete edentulism. Journal of Prosthodontics, 8(1), 27–39. [CrossRef]. [CrossRef]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global Burden of Severe Tooth Loss: A Systematic Review and Meta-Analysis. J. Dent. Res. 2014, 93, 7. [Google Scholar] [CrossRef] [Green Version]. [CrossRef]
- Holmstrup, P.; Damgaard, C.; Olsen, I.; Björn, K.; Allan, F.; Claus, H.; Nielsen, P.; Riis, H. Comorbidity of Periodontal Disease: Two Sides of the Same Coin? An Introduction for the Clinician. J. Oral Microbiol. 2017, 9, 1332710. [Google Scholar] [CrossRef]. [CrossRef]
- Romandini, M.; Baima, G.; Antonoglou, G.; Bueno, J.; Figuero, E.; Sanz, M. Periodontitis, Edentulism, and Risk of Mortality: A Systematic Review with Meta-Analyses. J. Dent. Res.2021, 100, 37–49. [Google Scholar] [CrossRef] [PubMed]. [CrossRef]
- Singh, A.; Gupta, A.; Peres, M.A.; Watt, R.G.; Tsakos, G.; Mathur, M.R. Association Between Tooth Loss and Hypertension Among a Primarily Rural Middle Aged and Older Indian Adult Population. J. Public Health Dent. 2016, 76, 198–205. [Google Scholar] [CrossRef]. [CrossRef]
- Taboza, Z.A.; Costa, K.L.; Silveira, V.R.; Furlaneto, F.A.; Montenegro, R., Jr.; Russell, S.; Dasanayake, A.; Rego, R.O. Periodontitis, Edentulismo and Glycemic Control in Patients with Type 2 Diabetes: A Cross-Sectional Study. BMJ Open Diabetes Res. Care 2018, 6, 000453. [Google Scholar] [CrossRef] [Green Version].
- Muñoz-Torres, F.J.; Mukamal, K.J.; Pai, J.K.; Willett, W.; Joshipura, K.J. Relationship between Tooth Loss and Peripheral Arterial Disease among Women. J. Clin. Periodontol. 2017, 44, 989–995. [Google Scholar] [CrossRef] [PubMed]. [CrossRef]
- Cheng, F.; Zhang, M.; Wang, Q.; Xu, H.; Dong, X.; Gao, Z.; Chen, J.; Wei, Y.; Qin, F. Tooth Loss and Risk of Cardiovascular Disease and Stroke: A Dose-Response Meta Analysis of Prospective Cohort Studies. PLoS ONE 2018, 13, e0194563. [Google Scholar] [CrossRef] [Green Version]. [CrossRef]
- Lee, H.J.; Choi, E.K.; Park, J.B.; Han, K.D.; Oh, S. Tooth Loss Predicts Myocardial Infarction, Heart Failure, Stroke, and Death. J. Dent. Res. 2019, 98, 164–170. [Google Scholar] [CrossRef] [PubMed]. [CrossRef]
- Goteiner, D.; Craig, R.G.; Ashmen, R.; Janal, M.N.; Eskin, B.; Lehrman, N. Endotoxin Levels are Associated with High-Density Lipoprotein, Triglycerides, and Troponin in Patients with Acute Coronary Syndrome and Angina: Possible Contributions from Periodontal Sources. J. Periodontol. 2008, 79, 2331–2339. [Google Scholar] [CrossRef] [Green Version]. [CrossRef]
- Nascimento, G.G.; Leite, F.R.; Conceição, D.A.; Ferrúa, C.P.; Singh, A.; Demarco, F.F. Is there a Relationship between Obesity and Tooth Loss and Edentulism? A Systematic Review and Meta-Analysis. Obes. Rev. 2016, 17, 587–598. [Google Scholar] [CrossRef] [PubMed]. [CrossRef]
- Choi, H.M.; Han, K.; Park, Y.G.; Park, J.B. Associations between the Number of Natural Teeth and Renal Dysfunction. Medicine 2016, 95, 4681. [Google Scholar] [CrossRef] [PubMed]. [CrossRef]
- Barros, S.P.; Suruki, R.; Loewy, Z.G.; Beck, J.D.; Offenbacher, S. A Cohort Study of the Impact of Tooth Loss and Periodontal Disease on Respiratory Events among COPD Subjects: Modulatory Role of Systemic Biomarkers of Inflammation. PLoS ONE 2013, 8, e68592. [Google Scholar] [CrossRef]. [CrossRef]
- Yoo, J.J.; Yoon, J.H.; Kang, M.J.; Kim, M.; Oh, N. The Effect of Missing Teeth on Dementia in Older People: A Nationwide Population-Based Cohort Study in South Korea. BMC Oral Health2019, 19, 61. [Google Scholar] [CrossRef] [Green Version]. [CrossRef]
- Cademartori, M.G.; Gastal, M.T.; Nascimento, G.G.; Demarco, F.F.; Corrêa, M.B. Is Depression Associated with Oral Health Outcomes in Adults and Elders? A Systematic Review and Meta-Analysis. Clin. Oral Investig. 2018, 22, 2685–2702. [Google Scholar] [CrossRef]. [CrossRef]
- Saito, S.; Ohi, T.; Murakami, T.; Komiyama, T.; Miyoshi, Y.; Endo, K.; Satoh, M.; Asayama, K.; Inoue, R.; Kikuya, M.; et al. Association Between Tooth Loss and Cognitive Impairment in Community-Dwelling Older Japanese Adults: A 4-Year Prospective Cohort Study from the Ohasama Study. BMC Oral Health 2018, 18, 142. [Google Scholar] [CrossRef] [PubMed]. [CrossRef]
- Yang, B.; Petrick, J.L.; Abnet, C.C.; Graubard, B.I.; Murphy, G.; Weinstein, S.J.; Männistö, S.; Albanes, D.; McGlynn, K.A. Tooth Loss and Liver Cancer Incidence in a Finnish Cohort. Cancer Causes Control 2017, 28, 899–904. [Google Scholar] [CrossRef] [PubMed]. [CrossRef]
- Maisonneuve, P.; Amar, S.; Lowenfels, A.B. Periodontal Disease, Edentulism, and Pancreatic Cancer: A Meta-Analysis. Ann. Oncol. 2017, 28, 985–995. [Google Scholar] [CrossRef]. [CrossRef]
- Meyer, M.S.; Joshipura, K.; Giovannucci, E.; Michaud, D.S. A Review of the Relationship between Tooth Loss, Periodontal Disease, and Cancer. Cancer Causes Control 2008, 19, 895–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]. [CrossRef]
- Michaud, D.S.; Fu, Z.; Shi, J.; Chung, M. Periodontal Disease, Tooth Loss, and Cancer Risk. Epidemiol. Rev. 2017, 39, 49–58. [Google Scholar] [CrossRef] [Green Version]. [CrossRef]
- Islas-Granillo, H.; Borges-Yañez, S.A.; Navarrete-Hernández, J.J.; Veras-Hernández, M.A.; Casanova-Rosado, J.F.; Minaya-Sánchez, M.; Casanova-Rosado, A.J.; Fernández-Barrera, M.Á.; Medina-Solís, C.E. Indicators of Oral Health in Older Adults with and Without the Presence of Multimorbidity: A Cross-Sectional Study. Clin. Inter. Aging. 2019, 14, 219–224. [Google Scholar] [CrossRef] [Green Version]. [CrossRef]
- Islas-Granillo, H.; Medina-Solís, C.E.; Márquez-Corona, M.L.; de la Rosa-Santillana, R.; Fernández-Barrera, M.A.; Villalobos-Rodelo, J.J.; Hernández-Martínez, C.T.; Navarrete-Hernández, J.J.; Mendoza-Rodríguez, M. Prevalence of Multimorbidity in Institutionalized Subjects Aged 60 and Over in a Developing Country. Clin. Inter. Aging 2018, 13, 1129–1133. [Google Scholar] [CrossRef] [Green Version]. [CrossRef]
- Kailembo, A.; Preet, R.; Stewart Williams, J. Common Risk Factors and Edentulism in Adults, Aged 50 years and over, in China, Ghana, India and South Africa: Results from the WHO Study on Global AGEing and Adult Health (SAGE). BMC Oral Health 2016, 17, 29. [Google Scholar] [CrossRef] [Green Version]. [CrossRef]
- Hunter E, De Moura Brito L, Piyasena P, et al. Impact of edentulism on community-dwelling adults in low-income, middle-income and high-income countries: a systematic review BMJ Open 2024;14:e085479. [CrossRef]
- American Heart Association. (2017). Cardiovascular disease: A costly burden for America—Projections through 2035. [CrossRef].
- World Health Organization. (2021, June 11). Cardiovascular diseases (CVDs). [CrossRef].
- American Heart Association. (2021). AHA names top heart disease and stroke research advances of 2021. [CrossRef].
- Preisser JS, Moss K, Finlayson TL, Jones JA, Weintraub JA. Prediction Model Development and Validation of 12-Year Incident Edentulism of Older Adults in the United States. JDR Clinical & Translational Research. 2022;8(4):384-393. [CrossRef]
- Antonoglou, G. N., Romandini, M., Meurman, J. H., Surakka, M., Janket, S. J., & Sanz, M. (2023). Periodontitis and edentulism as risk indicators for mortality: Results from a prospective cohort study with 20 years of follow-up. Journal of periodontal research, 58(1), 12–21. [CrossRef]
- Janket, S.-J.; Kunhipurayil, H.H.; Tamimi, F.; Surakka, M.; Li, H.; Van Dyke, T.E.; Meurman, J.H. Edentulism or Poor Oral Hygiene: Which Is the Stronger Predictor for All-Cause Mortality? J. Clin. Med. 2025, 14, 371. [CrossRef]
- Juxiang Peng, Jukun Song, Jing Han, Zhu Chen, Xinhai Yin, Jianguo Zhu, Jinlin Song; The relationship between tooth loss and mortality from all causes, cardiovascular diseases, and coronary heart disease in the general population: systematic review and dose–response meta-analysis of prospective cohort studies. Biosci Rep 31 January 2019; 39 (1): BSR20181773. [CrossRef]
- Carra MC, Rangé H, Caligiuri G, Bouchard P. Periodontitis and atherosclerotic cardiovascular disease: A critical appraisal. Periodontol 2000. 2023; 00:1-34. [CrossRef]
- National Center for Health Statistics. About the National Health and Nutrition Examination Survey. Centers for Disease Control and Prevention. Available online: (accessed on 11 Dec 2024). https://www.cdc.gov/nchs/nhanes/about/.
- American Association of Oral and Maxillofacial Surgeons. Edentulism. MyOMS. Available online: [https://myoms.org/what-we-%20do/dental-implant-surgery/edentulism/ (accessed on 11 Dec 2024).
- Casanova-Rosado, A.J.; Casanova-Rosado, J.F.; Minaya-Sánchez, M.; Robles-Minaya, J.L.; Casanova-Sarmiento, J.A.; Márquez-Corona, M.d.L.; Pontigo-Loyola, A.P.; Isla-Granillo, H.; Mora-Acosta, M.; Márquez-Rodríguez, S.; et al. Association of Edentulism with Various Chronic Diseases in Mexican Elders 60+ Years: Results of a Population-Based Survey. Healthcare 2021, 9, 404. [CrossRef]. [CrossRef]
- Szerszeń, M.; Górski, B.; Kowalski, J. Clinical Condition of the Oral Cavity in the Adult Polish Population below 70 Years of Age after Myocardial Infarction—A Case–Control Study. Int. J. Environ. Res. Public Health2022, 19, 7265. [CrossRef]. [CrossRef]
- D’Orto, B.; Tetè, G.; Nagni, M.; Visconti, R.F.; Polizzi, E.; Gherlone, E.F. Full Arch Implant-Prosthetic Rehabilitation in Patients with Cardiovascular Diseases: A 7-Year Follow-Up Prospective Single Cohort Study. J. Clin. Med. 2024, 13, 924. [CrossRef]. [CrossRef]
- Ebersole, J.L.; Graves, C.L.; Gonzalez, O.A.; Dawson, D., 3rd; Morford, L.A.; Huja, P.E.; Hartsfield, J.K., Jr.; Huja, S.S.; Pandruvada, S.; Wallet, S.M. Aging, Inflammation, Immunity and Periodontal Disease. Periodontology 2000, 2016, 54–75. [Google Scholar] [CrossRef] [PubMed]. [CrossRef]
- D’Aiuto, F.; Graziani, F.; Tetè, S.; Gabriele, M.; Tonetti, M.S. Periodontitis: From Local Infection to Systemic Diseases. Int. J. Immunopathol. Pharmacol. 2005, 18, 1–11. [Google Scholar].
- Fisher, M.A.; Taylor, G.W.; West, B.T.; McCarthy, E.T. Bidirectional Relationship between Chronic Kidney and Periodontal Disease: A Study Using Structural Equation Modeling. Kidney Int. 2011, 79, 347–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]. [CrossRef]
- Gacon, I.; Wieczorek, A. Coexistence of Lack of Clinical Manifestation of Oral Mycosis and Systemic Diseases in Edentulous Patients Using Removable Prosthetic Restorations. Int. J. Environ. Res. Public Health 2020, 17, 6348. [Google Scholar] [CrossRef] [PubMed]. [CrossRef]
- Ebersole, J.L.; Graves, C.L.; Gonzalez, O.A.; Dawson, D., 3rd; Morford, L.A.; Huja, P.E.; Hartsfield, J.K., Jr.; Huja, S.S.; Pandruvada, S.; Wallet, S.M. Aging, Inflammation, Immunity and Periodontal Disease. Periodontology 2000, 2016, 54–75. [Google Scholar] [CrossRef] [PubMed]. [CrossRef]
- D’Aiuto, F.; Graziani, F.; Tetè, S.; Gabriele, M.; Tonetti, M.S. Periodontitis: From Local Infection to Systemic Diseases. Int. J. Immunopathol. Pharmacol. 2005, 18, 1–11. [Google Scholar].
- Fisher, M.A.; Taylor, G.W.; West, B.T.; McCarthy, E.T. Bidirectional Relationship between Chronic Kidney and Periodontal Disease: A Study Using Structural Equation Modeling. Kidney Int. 2011, 79, 347–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]. [CrossRef]
- Tinti, F.; Lai, S.; Noce, A.; Rotondi, S.; Marrone, G.; Mazzaferro, S.; Di Daniele, N.; Mitterhofer, A.P. Chronic Kidney Disease as a Systemic Inflammatory Syndrome: Update on Mechanisms Involved and Potential Treatment. Life 2021, 11, 419. [CrossRef]
- Gacon, I.; Wieczorek, A. Coexistence of Lack of Clinical Manifestation of Oral Mycosis and Systemic Diseases in Edentulous Patients Using Removable Prosthetic Restorations. Int. J. Environ. Res. Public Health 2020, 17, 6348. [Google Scholar] [CrossRef] [PubMed]. [CrossRef]
- Bagatini, M.D.; Cardoso, A.M.; Reschke, C.R.; Carvalho, F.B. Immune System and Chronic Diseases 2018. J. Immunol. Res. 2018, 2018, 8653572. [Google Scholar] [CrossRef] [Green Version]. [CrossRef]
- You, Z.; Cushman, M.; Jenny, N.S.; Howard, G. Regards, Tooth Loss, Systemic Inflammation, and Prevalent Stroke among Participants in the Reasons for Geographic and Racial Difference in Stroke (REGARDS) Study. Atherosclerosis 2009, 203, 615–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]. [CrossRef]
- Sadek, K.M.; El Moshy, S.; Radwan, I.A.; Rady, D.; Abbass, M.M.S.; El-Rashidy, A.A.; Dörfer, C.E.; Fawzy El-Sayed, K.M. Molecular Basis beyond Interrelated Bone Resorption/Regeneration in Periodontal Diseases: A Concise Review. Int. J. Mol. Sci. 2023, 24, 4599. [CrossRef]
- Gutterman, D. D., Chabowski, D. S., Kadlec, A. O., Durand, M. J., Freed, J. K., Ait-Aissa, K., & Beyer, A. M. (2016). The human microcirculation: Regulation of flow and beyond. Circulation Research, 118(1), 157–172. [CrossRef]. [CrossRef]
- Cecoro, G., Annunziata, M., Iuorio, M. T., Nastri, L., & Guida, L. (2020). Periodontitis, Low-Grade Inflammation and Systemic Health: A Scoping Review. Medicina, 56(6), 272. [CrossRef]. [CrossRef]
- Hunter E, De Moura Brito L, Piyasena P, et al. Impact of edentulism on community-dwelling adults in low-income, middle-income and high-income countries: a systematic review BMJ Open 2024;14:e085479. [CrossRef]
- American Heart Association. (2017). Cardiovascular disease: A costly burden for America—Projections through 2035. [CrossRef].
- World Health Organization. (2021, June 11). Cardiovascular diseases (CVDs). [CrossRef].
- American Heart Association. (2021). AHA names top heart disease and stroke research advances of 2021. [CrossRef].
- Hunter E, De Moura Brito L, Piyasena P, et al. Impact of edentulism on community-dwelling adults in low-income, middle-income and high-income countries: a systematic review BMJ Open 2024;14:e085479. [CrossRef]
- Gutterman, D. D., Chabowski, D. S., Kadlec, A. O., Durand, M. J., Freed, J. K., Ait-Aissa, K., & Beyer, A. M. (2016). The human microcirculation: Regulation of flow and beyond. Circulation Research, 118(1), 157–172. [CrossRef]. [CrossRef]
- Celik, D.; Kantarci, A. Vascular Changes and Hypoxia in Periodontal Disease as a Link to Systemic Complications. Pathogens 2021, 10, 1280. [CrossRef]. [CrossRef]
- Theodorakis, N.; Nikolaou, M. From Cardiovascular-Kidney-Metabolic Syndrome to Cardiovascular-Renal-Hepatic-Metabolic Syndrome: Proposing an Expanded Framework. Biomolecules 2025, 15, 213. [CrossRef]
- Tinti, F.; Lai, S.; Noce, A.; Rotondi, S.; Marrone, G.; Mazzaferro, S.; Di Daniele, N.; Mitterhofer, A.P. Chronic Kidney Disease as a Systemic Inflammatory Syndrome: Update on Mechanisms Involved and Potential Treatment. Life 2021, 11, 419. [CrossRef]
- Gacon, I.; Wieczorek, A. Coexistence of Lack of Clinical Manifestation of Oral Mycosis and Systemic Diseases in Edentulous Patients Using Removable Prosthetic Restorations. Int. J. Environ. Res. Public Health 2020, 17, 6348. [Google Scholar] [CrossRef] [PubMed]. [CrossRef]
- Desai, J.P.; Nair, R.U. Oral Health Factors Related to Rapid Oral Health Deterioration among Older Adults: A Narrative Review. J. Clin. Med.2023,12,3202. [CrossRef]
- Marchini, L.; Ettinger, R.L. The Prevention, Diagnosis, and Treatment of Rapid Oral Health Deterioration (ROHD) among Older Adults. J. Clin. Med. 2023, 12, 2559. [CrossRef]
- Pawinska, M.; Kondrat, A.; Jamiolkowski, J.; Paszynska, E. Dental Status and Oral Health Behaviors of Selected 45–74-Year-Old Men from Northeastern Poland. Int. J. Environ. Res. Public Health 2023, 20, 6005. [CrossRef]
- Maria Febbraio, Christopher Bryant Roy, Liran Levin, Is There a Causal Link Between Periodontitis and Cardiovascular Disease? A Concise Review of Recent Findings, International Dental Journal, Volume 72, Issue 1, 2022, Pages 37-51, ISSN 0020-6539, [CrossRef]. [CrossRef]

Table 1.
Descriptive summary of population characteristics.
| Independent variable | With Dentition (n) |
% | Complete Tooth Loss (n) |
% | Total (n) |
||
|---|---|---|---|---|---|---|---|
| Heart Disease* | No heart disease | 8,583 | 84.5 | 1,378 | 6.42 | 9,961 | |
| Have heart disease | 941 | 7.33 | 385 | 1.76 | 1,326 | ||
| Heart Attack (Myocardial Infarction MI) | Yes | 356 | 2.78 | 165 | 0.78 | 521 | |
| No | 9,155 | 89.06 | 1,593 | 7.42 | 10,748 | ||
| Coronary Heart Disease (CHF) | Yes | 349 | 3.08 | 160 | 0.74 | 509 | |
| No | 9,147 | 88.78 | 1,590 | 7.39 | 10,737 | ||
| Congestive Heart Failure (CHF) | Yes | 271 | 1.8 | 144 | 0.58 | 415 | |
| No | 9,229 | 90.02 | 1,616 | 7.61 | 10,845 | ||
| Stroke | Yes | 346 | 2.37 | 136 | 0.64 | 482 | |
| No | 9,167 | 89.46 | 1,624 | 7.52 | 10,791 | ||
| Gender | Male | 6,963 | 42.21 | 2,486 | 6.65 | 9,449 | 0.53 |
| Female | 7,329 | 44.36 | 2,447 | 6.78 | 9,776 | ||
| Race/Ethnicity | Hispanic | 4,065 | 15.14 | 1,351 | 2.72 | 5,416 | |
| White | 4,474 | 52.46 | 1,742 | 7.41 | 6,216 | ||
| Black | 3,221 | 10.22 | 1,023 | 1.67 | 4,244 | ||
| Asian | 1,747 | 4.83 | 463 | 0.75 | 2,210 | ||
| Others | 785 | 3.92 | 354 | 0.87 | 1,139 | ||
| Age in years at screening | Less than 6 | 165 | 0.5 | 2,815 | 6.91 | 2,980 | |
| 11-Jun | 2,234 | 7.52 | 213 | 0.28 | 2,447 | ||
| 18-Dec | 2,111 | 9.29 | 121 | 0.15 | 2,232 | ||
| 19-44 | 4,345 | 32.54 | 455 | 1.38 | 4,800 | ||
| 45-59 | 2,376 | 18.66 | 339 | 1.56 | 2,715 | ||
| Above 60 | 3,061 | 18.07 | 990 | 3.14 | 4,051 | ||
| Education level | 0-11 | 1,931 | 10.8 | 550 | 2.13 | 2,481 | |
| HS/Ged | 2,118 | 21.46 | 443 | 2.48 | 2,561 | ||
| >HS | 5,466 | 59.58 | 762 | 3.55 | 6,228 | ||
| Ratio of family | <100%FPL | 2,889 | 69.58 | 1,263 | 30.42 | 4,152 | |
| 100%-99%FPL | 3,564 | 74.46 | 1,222 | 25.54 | 4,786 | <0.0001 | |
| 200%-399%FPL | 3,382 | 77.18 | 1,000 | 22.82 | 4,382 | ||
| 400%+FPL | 2,886 | 79.68 | 736 | 20.32 | 3,622 | ||
| BMI | Underweight | 1,877 | 7.61 | 1,288 | 4.39 | 3,165 | |
| normal | 4,268 | 26.16 | 453 | 1.97 | 4,721 | ||
| Overweight | 3,648 | 24.58 | 409 | 2.09 | 4,057 | ||
| Obese | 4,355 | 30.68 | 463 | 2.52 | 4,818 | ||
| Diabetes | Yes | 1,365 | 7.38 | 384 | 1.24 | 1,749 | |
| No | 12,647 | 78.54 | 3,737 | 10.99 | 16,384 | ||
| borderline | 273 | 1.67 | 58 | 0.17 | 331 | ||
* Heart Disease includes one or more of the following: CHD, MI, CHF, and stroke.
Table 2.
Multiple logistic regression model for the association between heart disease and tooth loss.
Table 2.
Multiple logistic regression model for the association between heart disease and tooth loss.
| Covariate | Odds Ratio | 95% Confidence Interval | P-value |
|---|---|---|---|
| Heart attack (Myocardial Infarction) | 1.78 | 1.27- 2.49 | 0.001 |
| Sex | 1.04 | 0.86- 1.26 | 0.648 |
| Age (45-59) | 2.23 | 1.61- 3.09 | <0.001 |
| Age (Above 60) | 4.31 | 2.88-6.46 | <0.001 |
| Education (HS/GED) | 0.64 | 0.50-0.82 | 0.001 |
| Education (>HS) | 0.40 | 0.31- 0.50 | <0.001 |
| Poverty (100%-199% FPL) | 0.92 | 0.69- 1.23 | 0.592 |
| Poverty (200%-399% FPL) | 0.54 | 0.37- 0.78 | 0.002 |
| Poverty (400%+ FPL) | 0.38 | 0.25- 0.57 | <0.001 |
| Race (Non-Hispanic White) | 1.54 | 1.05-2.25 | 0.027 |
| Rece (Non-Hispanic Black) | 1.62 | 1.13-2.33 | 0.010 |
| Race (Non-Hispanic Asian) | 1.99 | 1.25- 3.18 | 0.005 |
| Race (Other) | 2.50 | 1.53-4.09 | 0.001 |
| Diabetes (Yes) | 1.13 | 0.85-1.49 | 0.367 |
| Diabetes (Borderline) | 1.12 | 0.68- 1.83 | 0.631 |
| BMI (Normal) | 0.71 | 0.23- 2.18 | 0.545 |
| BMI (Overweight) | 0.84 | 0.26- 2.66 | 0.760 |
| BMI (Obese) | 0.74 | 0.24- 2.25 | 0.596 |
Table 3.
Multiple logistic regression model for the association between heart disease and tooth loss.
Table 3.
Multiple logistic regression model for the association between heart disease and tooth loss.
| Variable | Odds Ratio | 95% Confidence Interval | P-value |
|---|---|---|---|
| Heart Disease* | 1.70 | 1.35- 2.14 | <0.001 |
| Sex | 1.04 | 0.86- 1.25 | 0.664 |
| Age (45-59) | 2.19 | 1.59- 3.02 | <0.001 |
| Age (Above 60) | 4.06 | 2.72- 6.07 | <0.001 |
| Education (HS/GED) | 0.65 | 0.50- 0.83 | 0.001 |
| Education (>HS) | 0.40 | 0.32- 0.50 | <0.001 |
| Poverty (100%-199% FPL) | 0.92 | 0.69- 1.22 | 0.566 |
| Poverty (200%-399% FPL) | 0.54 | 0.37- 0.78 | 0.002 |
| Poverty (400%+ FPL) | 0.38 | 0.26- 0.58 | <0.001 |
| Race (White) | 1.49 | 1.02- 2.19 | 0.039 |
| Race (Black) | 1.57 | 1.09- 2.26 | 0.017 |
| Race (Asian) | 1.99 | 1.24-3.19 | 0.006 |
| Race (Other) | 2.45 | 1.48- 4.06 | 0.001 |
| Diabetes (Yes) | 1.08 | 0.82- 1.42 | 0.558 |
| Diabetes (Borderline) | 1.06 | 0.65- 1.74 | 0.785 |
| BMI (Normal) | 0.71 | 0.23- 2.18 | 0.542 |
| BMI (Overweight) | 0.83 | 0.26- 2.64 | 0.747 |
| BMI (Obese) | 0.73 | 0.24- 2.20 | 0.574 |
* Heart Disease includes one or more of the following: CHD, MI, CHF, and stroke.
Table 4.
Multiple logistic regression model for the association between coronary heart disease and tooth loss.
Table 4.
Multiple logistic regression model for the association between coronary heart disease and tooth loss.
| Variable | Odds Ratio | 95% Confidence Interval | P-value |
|---|---|---|---|
| Coronary heart disease | 1.60 | 1.16- 2.20 | 0.005 |
| Sex | 1.03 | 0.85- 1.24 | 0.721 |
| Age (45-59) | 2.26 | 1.63- 3.12 | <0.001 |
| Age (Above 60) | 4.35 | 2.90- 6.52 | <0.001 |
| Education (HS/GED) | 0.66 | 0.51- 0.85 | 0.003 |
| Education (>HS) | 0.40 | 0.31- 0.51 | <0.001 |
| Poverty (100%-199% FPL) | 0.93 | 0.70- 1.23 | 0.617 |
| Poverty (200%-399% FPL) | 0.53 | 0.37- 0.78 | 0.002 |
| Poverty (400%+ FPL) | 0.37 | 0.25- 0.56 | <0.001 |
| Race (Non-Hispanic White) | 1.52 | 1.03- 2.24 | 0.035 |
| Race (Non-Hispanic Black) | 1.62 | 1.13- 2.34 | 0.010 |
| Race (Non-Hispanic Asian) | 1.99 | 1.25-3.17 | 0.005 |
| Race (Other) | 2.55 | 1.54- 4.21 | 0.001 |
| Diabetes (Yes) | 1.13 | 0.85- 1.52 | 0.365 |
| Diabetes (Borderline) | 1.08 | 0.65- 1.78 | 0.751 |
| BMI (Normal) | 0.71 | 0.23 2.17 | 0.537 |
| BMI (Overweight) | 0.82 | 0.25- 2.61 | 0.731 |
| BMI (Obese) | 0.74 | 0.24 2.25 | 0.593 |
Table 5.
Multiple logistic regression model for the association between congestive heart failure and tooth loss.
Table 5.
Multiple logistic regression model for the association between congestive heart failure and tooth loss.
| Variable | Odds Ratio | 95% Confidence Interval | P-value |
|---|---|---|---|
| Congestive HF | 1.85 | 1.29- 2.67 | 0.002 |
| Sex | 1.01 | 0.84- 1.23 | 0.840 |
| Age (45-59) | 2.26 | 1.64- 3.11 | <0.001 |
| Age (Above 60) | 4.42 | 2.92- 6.68 | <0.001 |
| Education (HS/GED) | 0.64 | 0.50- 0.83 | 0.001 |
| Education (>HS) | 0.39 | 0.31- 0.50 | <0.001 |
| Poverty (100%-199% FPL) | 0.92 | 0.69- 1.22 | 0.556 |
| Poverty (200%-399% FPL) | 0.53 | 0.37- 0.78 | 0.002 |
| Poverty (400%+ FPL) | 0.38 | 0.25- 0.57 | <0.001 |
| Race (Non-Hispanic White) | 1.54 | 1.04- 2.27 | 0.029 |
| Race (Non-Hispanic Black) | 1.59 | 1.10- 2.30 | 0.014 |
| Race (Non-Hispanic Asian) | 1.97 | 1.23- 3.15 | 0.006 |
| Race (Other) | 2.61 | 1.58- 4.32 | <0.001 |
| Diabetes (Yes) | 1.12 | 0.84- 1.50 | 0.404 |
| Diabetes (Borderline) | 1.06 | 0.64- 1.74 | 0.814 |
| BMI (Normal) | 0.71 | 0.23- 2.21 | 0.552 |
| BMI (Overweight) | 0.83 | 0.26- 2.67 | 0.751 |
| BMI (Obese) | 0.74 | 0.24- 2.22 | 0.581 |
Table 6.
Multiple logistic regression model for the association between stroke and tooth loss.
| Variable | Odds Ratio | 95% Confidence Interval | P-value |
|---|---|---|---|
| Stroke | 1.64 | 1.17- 2.29 | 0.005 |
| Sex | 1.01 | 0.84- 1.23 | 0.849 |
| Age (45-59) | 2.26 | 1.64- 3.12 | <0.001 |
| Age (Above 60) | 4.44 | 2.95- 6.69 | <0.001 |
| Education (HS/GED) | 0.64 | 0.50- 0.83 | <0.001 |
| Education (>HS) | 0.40 | 0.31- 0.50 | <0.001 |
| Poverty (100%-199% FPL) | 0.92 | 0.69- 1.23 | 0.601 |
| Poverty (200%-399% FPL) | 0.54 | 0.37- 0.78 | 0.002 |
| Poverty (400%+ FPL) | 0.38 | 0.25- 0.57 | <0.001 |
| Race (Non-Hispanic White) | 1.55 | 1.05- 2.27 | 0.027 |
| Race (Non-Hispanic Black) | 1.60 | 1.11- 2.32 | 0.013 |
| Race (Non-Hispanic Asian) | 2.01 | 1.26- 3.20 | 0.005 |
| Race (Other) | 2.58 | 1.56- 4.29 | 0.001 |
| Diabetes (Yes) | 1.12 | 0.85- 1.49 | 0.390 |
| Diabetes (Borderline) | 1.06 | 0.65- 1.72 | 0.787 |
| BMI (Normal) | 0.68 | 0.22- 2.09 | 0.499 |
| BMI (Overweight) | 0.80 | 0.25- 2.53 | 0.698 |
| BMI (Obese) | 0.72 | 0.24- 2.17 | 0.557 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



