Submitted:
16 February 2026
Posted:
26 February 2026
You are already at the latest version
Abstract
Japan has achieved universal health coverage and among the highest life expectancies worldwide; however, rapid population aging, workforce decline, fiscal pressures, and marked regional disparities threaten system sustainability. Despite a relatively low physician-to-population ratio, Japan maintains one of the highest hospital bed densities among OECD countries, reflecting a hospital-centered care model associated with prolonged stays and high inpatient expenditures.This study is a narrative review incorporating secondary ecological analyses using aggregated prefecture-level data. The quantitative analyses are explicitly hypothesis-generating and exploratory rather than causal. Publicly available national datasets from 2021–2022 were used to examine international differences in hospital bed and physician densities and to assess associations between hospital bed supply, per capita medical expenditure, life expectancy, and healthy life expectancy across Japan’s 47 prefectures. Descriptive statistics and Pearson correlation analyses were performed, with outcomes stratified by sex.Higher hospital bed density was consistently associated with increased inpatient expenditure but showed no positive relationship with life expectancy or healthy life expectancy. Among men, both indicators were negatively correlated with bed density, whereas no significant associations were observed among women.A case study of Yubari City, Hokkaido, suggests that large-scale bed reduction did not worsen mortality indicators and was accompanied by reduced medical expenditures and greater reliance on community-based and long-term care. Overall, these ecological, hypothesis-generating findings highlight potential inefficiencies of excess inpatient capacity and underscore the need for regionally tailored bed planning and strengthened primary and generalist care in Japan’s super-aged society.
Keywords:
population aging
; healthcare reform
; health outcomes
; primary care physicians
; generalists
; fee-for-service
; community-based care
Introduction
Japan’s healthcare system has achieved universal health coverage, low infant mortality, and one of the highest life expectancies worldwide, reflecting long-standing efforts by healthcare professionals and policymakers. Its accessibility and quality are often cited as a global benchmark.
However, rapid population aging, workforce decline, fiscal constraints, and persistent regional disparities now threaten system sustainability. Since the COVID-19 pandemic, excess mortality has increased and life expectancy has stagnated, potentially accelerating population decline and raising concerns about economic vitality and international competitiveness [1,2,3]. These trends underscore the need to reassess the organization and delivery of healthcare services.
The Japan Hospital Association has acknowledged that reductions in hospitals and inpatient beds are unavoidable, advocating regional reorganization of care delivery and clearer institutional roles. Given projected demographic and workforce changes, maintaining the current hospital-centered model is increasingly difficult, necessitating strategic downsizing and stronger inter-institutional collaboration [4,5].
Japan relies heavily on hospitals. According to the OECD, it has the highest per capita numbers of total and acute care beds among member countries, combined with relatively long hospital stays and limited long-term care capacity. This structure encourages prolonged hospitalization of patients who could be managed in community or long-term care settings, contributing to inefficiencies and rising inpatient expenditures, particularly in regions with surplus beds [6].
Population aging further strains public finances, with concerns about equity for socioeconomically disadvantaged populations. Nevertheless, evidence suggests that residential socioeconomic status does not substantially affect access to certain surgical services, indicating a degree of resilience within Japan’s universal healthcare system [7].
Despite a relatively low physician-to-population ratio, Japan maintains exceptionally high hospital bed density, especially in rural areas, leading to mismatches between infrastructure, medical need, and utilization. Structural reform is therefore required to optimize resource allocation and control costs.
This narrative review compares Japan’s hospital bed and physician densities with international benchmarks and examines prefecture-level associations between bed density and key health indicators, including per capita healthcare expenditure, life expectancy, and healthy life expectancy. The case of Yubari City, Hokkaido, where health outcomes remained stable and costs declined following hospital closure after municipal bankruptcy, illustrates the potential role of primary care physicians and hospital generalists in sustaining population health amid infrastructure contraction [8].
Finally, this study proposes policy recommendations to enhance the sustainability, equity, and quality of Japan’s healthcare system under ongoing demographic and economic pressures.
Methods
Study Design
This study is a narrative review incorporating secondary ecological analyses using aggregated prefecture-level data. Quantitative analyses were exploratory and hypothesis-generating, not intended to establish causality.
Data Sources
Publicly available national and prefectural datasets were used. Hospital bed data were obtained from official prefectural statistics compiled by the Ministry of Health, Labour and Welfare (MHLW) [9]. Per capita medical expenditure data were sourced from MHLW national health insurance expenditure reports [10]. Life expectancy and healthy life expectancy data were derived from national statistics and governmental reports [11,12].
Variables
Primary variables included hospital beds per 100,000 population, per capita medical expenditure (JPY), life expectancy at birth, and healthy life expectancy. Life expectancy outcomes were stratified by sex to account for known gender differences.
Statistical Analysis
Descriptive statistics summarized national and international patterns. Prefecture-level associations between hospital bed density and medical expenditure, life expectancy, and healthy life expectancy were examined using Pearson’s correlation coefficients, with scatter plots for visualization.
No multivariable adjustments were performed, and potential confounders such as socioeconomic factors, health behaviors, and healthcare workforce distribution were not controlled for. All analyses were conducted at the ecological level.
Japan’s Healthcare Context in International Perspective
According to 2021 OECD data, Japan has about 12.62 hospital beds per 1,000 population—the second highest among OECD countries after Korea—nearly double that of Germany (7.76) and France (5.65) (Figure 1A). In contrast, physician density is relatively low at 2.65 per 1,000, compared with Germany (4.55) and Italy (4.24) (Figure 1B). This combination of high bed availability and low physician density is unusual among developed countries and reflects Japan’s distinctive historical and institutional context.
Unlike many OECD countries with centralized healthcare planning, Japan has historically allowed relatively free market entry for medical facilities. Licensed physicians can establish hospitals or clinics if minimum regulations are met, and private hospitals independently secure funding. Until the 1980s, hospital bed supply was largely unregulated to expand nationwide access postwar, which improved geographic coverage but complicated resource coordination and expenditure control.
High patient choice under universal health insurance further challenges coordinated, continuous care across the spectrum from primary care to specialized treatment, home recovery, and long-term care. Recent regional planning efforts focus on strengthening family physician roles, clarifying the function of small- and medium-sized hospitals, and developing integrated community care networks through multidisciplinary collaboration. Understanding this historical balance between market-driven entry and limited regulation is key to interpreting current inefficiencies and guiding reforms for sustainability and regional equity.
Structural Factors Influencing Hospital Bed Supply and Utilization
Japan’s healthcare infrastructure has been shaped by its historical development. After World War II, rapid expansion of medical access prioritized a free-entry system, with over 80% of hospitals privately owned, often by individual physicians or small family-run organizations. Under a “free-labeling” framework, private hospitals secure their own funding, and licensed physicians can establish hospitals or clinics by meeting minimal regulations [15]. This decentralized structure contributed to widespread hospital proliferation, especially in regions with stable or growing demand.
Hospital behavior is further influenced by Japan’s fee-for-service national health insurance system, which incentivizes admissions, prolonged stays, and high occupancy. For example, neonatal intensive care units generate higher reimbursements, illustrating supply-induced demand [16]. Payment reforms, such as the Diagnostic Procedure Combination/Per-Diem Payment System (DPC/PDPS), have reduced resource use, but without measurable improvements in care quality [17].
Insufficient functional differentiation among hospitals adds to inefficiency. Acute care bed demand is estimated at only 40% of supply, leading to supply-sensitive utilization where hospitalization reflects bed availability as much as medical need [18]. Evidence from cardiology shows that centralizing specialists while decentralizing acute care hospitals regionally can improve quality, emphasizing the need for both concentration of expertise and appropriate distribution [19].
Unlike systems that employ global budgeting, capitation, or bundled payments to contain volume-driven care, Japan lacks strict mechanisms to cap hospital bed supply or overall reimbursed services. Consequently, hospital operators may perceive maintaining large bed capacity as a business imperative rather than a purely clinical necessity. Understanding the interplay of historical context, financial incentives, and insufficient functional differentiation is essential for addressing inefficiencies and guiding future healthcare policy reforms in Japan.
Regional Variations and Economic Influences
An analysis of 1992 national health insurance data found that Fukuoka Prefecture had 43% higher per capita inpatient expenditure than the national average, largely due to prolonged hospitalizations for stroke. Inpatient costs were more closely associated with bed supply than actual medical need, highlighting structural drivers of regional variation [20].
Data across Japan’s 47 prefectures (2022) reveal substantial differences in hospital bed density and medical expenditure (Figure 2). Several rural western prefectures, including Kochi, Kagoshima, Nagasaki, and Kumamoto, exhibit the highest bed densities and per capita expenditures, despite not having worse health outcomes or markedly older populations. These differences cannot be explained by age composition alone.
Economic factors play a key role. Lower land and labor costs in rural areas make hospital operation and expansion more feasible, supporting many small-scale hospitals run by local physicians where alternative care options are limited. Rural areas also have less developed home care, visiting nursing, and community-based services. Staff turnover, limited collaboration frameworks, and a shortage of highly functional home-visit nursing providers often make hospitalization the default for chronic disease management or rehabilitation, even when less intensive care could suffice [21,22].
Historical factors further contribute. Western Japan hosts numerous older medical schools founded before World War II, whose alumni networks and departmental affiliations maintain extensive hospital systems. While these institutions support continuity in education and care, they may hinder adaptation of infrastructure to evolving healthcare needs.
Impact on Health Outcomes and System Efficiency
A high number of hospital beds does not necessarily lead to better health outcomes. For example, Nagano Prefecture has low bed density and moderate healthcare spending but consistently ranks high in life expectancy and public health indicators. While bed density correlates with inpatient costs, its link to health outcomes is unclear, suggesting that abundant inpatient infrastructure is not essential for good population health.
Figure 3 presents scatter plots by prefecture, stratified by sex, showing the relationships between number of hospital beds and both life expectancy and healthy life expectancy. Among women, no significant correlation was observed between medical expenditures and either outcome. (Figure 3C,D) Surprisingly, among men, both life expectancy and healthy life expectancy were negatively correlated with the number of hospital beds. (Figure 3A,B)
One speculative explanation for the observed association in men—but not in women—is that women generally have longer life expectancy and healthier lifestyles, potentially making them less sensitive to healthcare system effects. In contrast, men may delay seeking care until disease is more advanced, which could contribute to higher healthcare costs despite shorter life expectancy.
Consistent with these findings, large-scale analyses of U.S. Medicare beneficiaries have demonstrated substantial interregional variation in hospital bed capacity and overall healthcare supply, with differences of up to two- to fourfold. Regions with greater bed availability exhibited hospitalization rates up to 30% higher; however, no significant association with mortality risk was observed, a pattern that was consistent across racial and income groups [23]. Moreover, regional differences in healthcare supply had minimal impact on major health outcomes, including mortality and hospitalization rates [24].
While these indicators—life expectancy and healthy life expectancy—do not capture the full spectrum of health outcomes, the data suggest that a greater number of hospital beds does not necessarily translate into longer or healthier lives. Conversely, regions with high bed densities often report longer hospital stays, higher rates of admissions that might be avoidable, and greater patient exposure to hospital-acquired conditions. These observations imply that surplus inpatient capacity may contribute to inefficiencies and could potentially compromise care quality.
The Role of Primary Care Physicians and Hospital Generalists in Addressing Bed Oversupply
Primary care physicians and hospital generalists, who manage a broad spectrum of inpatient cases, are well positioned to address challenges from Japan’s oversupply of hospital beds. Unlike narrowly focused specialists, hospital generalists provide comprehensive, patient-centered care, particularly suited to multimorbid and aging populations common in high bed-density hospitals.
Japanese hospitalists and generalists prioritize inpatient management, geriatric care, and diagnostic, therapeutic, and safety oversight, enabling them to care effectively for older patients and those with multiple comorbidities [25]. In many rural and suburban hospitals, they oversee daily inpatient care—including admissions for ambulatory care-sensitive conditions, rehabilitation, or extended observation—allowing them to identify avoidable or unnecessarily prolonged hospitalizations and promote community-based alternatives.
Hospital generalists also serve as clinical leaders in small- and medium-sized hospitals, influencing governance, quality improvement, and staff education. They can advocate for programs such as hospital-at-home care, post-discharge follow-up, and strengthened collaboration with home care providers, thereby reducing reliance on inpatient beds. Evidence supports their impact on efficiency: patients with aspiration pneumonia managed by hospitalists show shorter stays, lower costs, and optimized care practices, including reduced unnecessary testing [26].
Increasingly, Japan is evaluating generalist and hospitalist roles by hospital size and regional characteristics, institutionalizing their contributions to healthcare reform and resource redistribution [27]. Their perspectives are critical for informed decisions on bed consolidation, ensuring that reductions do not compromise care for vulnerable populations.
However, several limitations exist. Nationwide optimization of hospital bed use through generalist involvement is uncertain due to variability in hospital size, regional context, patient populations, physician availability, and financial structures. Definitions, training, and role allocation for hospitalists and generalists remain inconsistent, and most evidence comes from single-disease or individual-facility studies, limiting generalizability.
Case Study: Yubari City’s Hospital Closure and Its Impact on Health Outcomes and Expenditures
Yubari City in Hokkaido, once a prosperous coal-mining town from the early to mid-20th century, experienced a dramatic population decline following the closure of its mines and eventually declared municipal bankruptcy in 2007. As a result, the city’s only advanced medical facility—a 171-bed municipal general hospital—was downsized to a 19-bed inpatient clinic and a 40-bed long-term care facility, effectively reducing inpatient hospital beds in the city to near zero.
Remarkably, despite a rapidly aging population, there was no substantial change in the city’s total mortality before and after the hospital closure (Figure 4A). In fact, the number of emergency transports significantly declined post-closure (Figure 4B).
Sex-specific standardized mortality ratios (SMRs) for all-cause mortality, cancer, and heart disease remained stable or slightly decreased (Figure 5A,B).
Although cerebrovascular mortality increased slightly for both sexes, pneumonia-related mortality showed a notable decline. This may be attributed to residents’ proactive efforts to receive pneumococcal vaccinations and to enhance oral care for aspiration pneumonia prevention, driven by local dentists and community health initiatives [28]. These preventive activities appear to have intensified after the hospital’s closure.
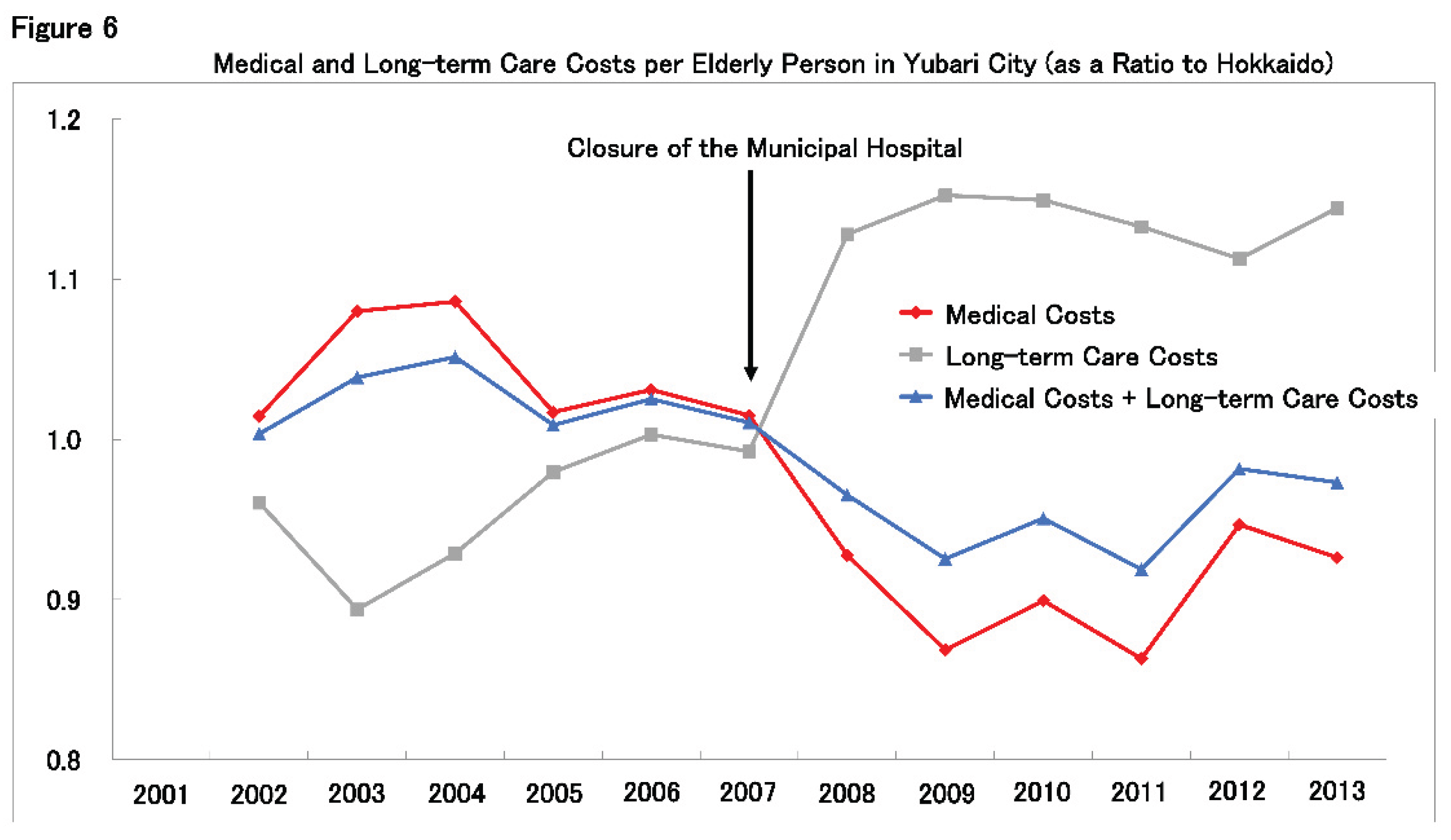
Figure 6 illustrates the trend in per-capita medical and long-term care expenditures for older adults in Yubari, expressed as a ratio to the overall averages in Hokkaido. Following the hospital closure, medical expenditures dropped sharply, while long-term care costs increased significantly, suggesting a shift from medical services to community-based care. Overall, the combined per-capita cost of medical and long-term care decreased relative to the Hokkaido average.
In summary, despite the closure of Yubari’s general hospital in 2007 and the near-elimination of inpatient beds, SMRs for all-cause, cancer, cardiovascular, and pneumonia mortality remained unchanged or decreased. Concurrently, healthcare expenditures and emergency transports declined, indicating a reduced societal burden of healthcare.
Several factors likely contributed to Yubari’s ability to sustain health outcomes: the development of an integrated 24-hour medical and long-term care system; strengthened social networks within the community; and increased health awareness and preventive behavior among residents. This shift from hospital-centered acute care to community-based, supportive care was facilitated by the active involvement of primary care and generalist physicians, who played a central role in maintaining local healthcare.
A potential counterargument is that improvements in Yubari’s health indicators and cost reductions may simply reflect the out-migration of high-dependency patients to other municipalities. To examine this possibility, the number of dialysis patients—who typically require high-cost, intensive care—was analyzed. Using two indicators (the number of certified physically disabled residents with renal impairment from 2006 to 2012, and new dialysis initiations from 1999 to 2009), little change was found before and after the municipal bankruptcy. Although dialysis patient numbers remained stable, further research is warranted to assess whether patients with other high-dependency conditions may have relocated to access care elsewhere, these findings suggest that no large-scale outflow of severely diseased patients occurred.
It is important to note that Yubari is a relatively small municipality, with a tightly knit community structure that may have facilitated public engagement and collective action. Additionally, the city’s proximity to Sapporo may have allowed some access to tertiary care facilities when necessary. Therefore, Yubari’s experience may not be entirely generalizable to all municipalities.
While health indicators appeared stable following the hospital closure, it is essential to note that mortality rates alone may not fully capture the broader health impact, particularly regarding chronic disease progression, quality of life, or unmet healthcare needs. Nevertheless, the series of events surrounding Yubari’s hospital closure offer important insights for the future of healthcare in Japan, particularly as discussions intensify around hospital downsizing and strategic withdrawal. Yubari may serve as a valuable model for reimagining healthcare delivery in a super-aged society.
Policy Considerations for Sustainable and Equitable Care
Ensuring the sustainability and equity of Japan’s healthcare system in the face of demographic and economic challenges requires a multifaceted policy approach.
- ▪
- Evidence-Based Regional Bed Planning
The adoption of analytical tools and planning frameworks to determine appropriate hospital bed numbers based on regional population demographics, disease burden, and service utilization patterns is essential to better align supply with actual need. Several international examples provide useful models. In France, each region develops a Schéma régional de santé (SRS), a regional health plan that organizes healthcare delivery according to local needs, including authorization, bed allocation, and functional differentiation. The SRS represents a prototypical mechanism for implementing regional bed planning and service reorganization [29]. In Germany, substantial reforms are underway that restructure hospital planning through functional designation, coupled with financial support for maintenance costs and diagnosis-related groups [30]. In Canada, provincial governments are investing in and evaluating initiatives aimed at strengthening home- and community-based care while reducing reliance on hospital-based inpatient services [31].
- ▪
- Promoting Hospital Consolidation and Service Diversification
Financial and administrative incentives can encourage small hospitals—particularly in rural areas—to merge or transition toward outpatient, rehabilitation, or long-term care functions. Such restructuring has the potential to optimize resource utilization while preserving access to essential healthcare services.
- ▪
- Strengthening Community-Based and Outpatient Care
Reducing dependence on inpatient services requires sustained investment in home care providers, public health nursing, primary care clinics, and integrated care platforms. The training and deployment of community health workers can further support chronic disease management and health promotion. In recent years, technology-enabled inpatient-level care delivered at home has been rapidly implemented. A systematic review encompassing 69 studies demonstrated that technology-enabled home care models do not increase the risk of hospital readmission compared with conventional hospital-based inpatient care [32]. In addition, systematic reviews of Hospital-at-Home (HaH) programs have reported that, relative to standard inpatient treatment, HaH may achieve comparable or even superior clinical outcomes [33].
- ▪
- Reforming Payment Systems
A gradual transition from volume-based fee-for-service reimbursement toward value-based or bundled payment models can better incentivize quality, efficiency, and patient-centered outcomes, while mitigating the tendency toward unnecessary service volume.
- ▪
- Collaborative Stakeholder Engagement
Successful healthcare reform depends on the active involvement of medical associations, hospital leadership, policymakers, and local communities. Transparent data sharing, consensus-building, and shared decision-making processes are essential to ensure that reforms are contextually appropriate, feasible, and broadly supported.
Functional Differentiation as a Pathway to Sustainable Regional Healthcare
A constructive way forward is not complex but rather rests on a clear functional differentiation within regional healthcare systems. Highly time-sensitive and resource-intensive conditions—such as acute ischemic stroke, major trauma, and advanced cardiovascular emergencies—should be centralized in large, well-equipped regional hub hospitals operating 24 hours a day with full specialist coverage. Attempting to provide comprehensive emergency services in numerous small- or medium-sized hospitals with 100–200 beds is neither clinically realistic nor efficient. When supported by coordinated emergency transport systems, including physician-staffed helicopters, centralization can improve survival even when geographic distances increase.
In contrast, the majority of healthcare needs in aging societies—management of chronic diseases, minor acute illnesses, rehabilitation, and end-of-life care—are better addressed outside hospitals. These services should be delivered through community-based primary care, home care, and integrated long-term care systems, as exemplified by practical experiences in rural areas such as Yubari. Strengthening primary care and supporting everyday living environments allows healthcare systems to maintain quality of care while reducing unnecessary hospitalizations and prolonged inpatient stays.
Public discourse in Japan frequently emphasizes “physician shortages” or “maldistribution of physicians” without adequately addressing the underlying structural issue of excessive hospital bed capacity. Such framing risks obscuring the core problem: the persistence of a hospital-centered model sustained by historical arrangements and entrenched interests rather than by current population needs. Without confronting bed oversupply and clarifying functional roles across care settings, discussions focused solely on workforce numbers are unlikely to produce meaningful or sustainable reform.
Limitations
This study has several limitations. First, the quantitative analyses use aggregated prefecture-level data, preventing individual-level inference and raising the risk of ecological fallacy. Second, associations between hospital bed density, healthcare expenditure, and health outcomes should not be interpreted as causal; reverse causation is possible, as regions with higher medical demand may maintain greater inpatient capacity. Third, analyses were not adjusted for potential confounders, including socioeconomic factors, health behaviors, disease prevalence, healthcare workforce distribution, and regional policies. Observed sex-specific associations may reflect differences in healthcare-seeking behavior or social determinants rather than supply effects. Fourth, the cross-sectional data limit evaluation of temporal relationships and causal pathways.
The case of Yubari City is an extreme, context-specific example of hospital downsizing following municipal bankruptcy and should be viewed as an illustrative policy experiment rather than a generalizable model. Yubari’s small population, strong community cohesion, and proximity to tertiary care may explain the stability of mortality indicators. The study lacks a formal comparison group, making it unclear whether observed changes result from hospital closures or other factors such as national trends, demographic shifts, or selective migration. Yubari’s highly specific context further limits generalizability. Finally, assessment of selection bias based solely on dialysis patients is insufficient, and broader evaluations using diverse populations and outcomes are needed.
Conclusions
This narrative review suggests that an oversupply of hospital beds, particularly in regions with limited physician availability, may lead to inefficiencies without clear health benefits. The experience of Yubari City illustrates that well-coordinated, community-based care supported by hospital generalists can sustain population health even after substantial hospital downsizing, although its unique context warrants cautious interpretation.
In Japan, policy initiatives such as the Regional Healthcare Vision provide a framework for rural bed planning through functional differentiation of hospitals. Our findings indicate that regionally tailored strategies, combined with strengthened primary and generalist care, may help maintain health outcomes while reducing reliance on excess inpatient capacity. Future studies using more robust designs and quantitative data on generalist physicians are needed to clarify system-level effects.
Importantly, healthcare policy should move beyond a narrow focus on cost containment and infrastructure preservation toward approaches that emphasize access, quality, and population needs. Refining data-driven, region-specific strategies in collaboration with frontline professionals may enhance sustainability in Japan and offer lessons for other aging societies.
Author Contributions
H.K. performed the study, statistical analysis, and wrote the manuscript; H.M. provided critical comments, and approved the final version. All the authors have read and approved the final version of this manuscript.
Funding
This research received no external funding.
Ethics approval and consent to participate
This study used publicly available data; therefore, ethics approval and informed consent were not required.
Consent for publication
All authors consent to the publication of this article in the Journal of Rural Medicine.
Data availability statement
Data supporting the findings of this study are available from the corresponding author upon request.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Kusunoki H. Unraveling Rising Mortality: Statistical Insights from Japan and International Comparisons. Healthcare (Basel). 2025; 13: 1305. [CrossRef]
- Devanathan G, Chua PLC, Nomura S, et al. Excess mortality during and after the COVID-19 emergency in Japan: a two-stage interrupted time-series design. BMJ Public Health. 2025; 3: e002357. [CrossRef]
- Ministry of Health, Labour and Welfare: Life Expectancy in 2025 Reaches 81.09 Years for Men and 87.13 Years for Women — Women Maintain the World’s No. 1 Position for the 40th Consecutive Year. Available at: https://www.satsuki-jutaku.mlit.go.jp/journal/article/p=2818 (accessed December 15, 2025).
- At the 74th Annual Meeting of the Japan Hospital Association, President Takao Aizawa emphasized the need for a fundamental review of Japan’s secondary medical care zones, asserting that the decline in hospitals and hospital beds is a natural trend, and that hospitals should pursue coexistence rather than competition (Source: Medical Reform, m3.com; Hospital Newspaper) Available at: https://www.m3.com/news/iryoishin/1288335 (accessed December 15, 2025).
- Lecture by Takao Aizawa, President of the Japan Hospital Association, presented at the 74th Annual Meeting of the Japan Hospital Association (Source: Byoin Shimbun.com) Available at: https://www.byoinshinbun.com/nitibyo_news.php?id=421 (accessed December 15, 2025).
- Available at: https://www.oecd.org/content/dam/oecd/en/publications/reports/2019/04/oecd-economic-surveys-japan-2019_ccac75f4/fd63f374-en.pdf (accessed December 15, 2025).
- Tomioka S, Fujino Y, Nakaya T, et al. Equality of Treatment for Hip Fracture Irrespective of Regional Differences in Socioeconomic Status: Analysis of Nationwide Hospital Claims Data in Japan. Tohoku J Exp Med. 2019; 247: 161-171. [CrossRef]
- Morita H. Analysis of Factors Contributing to the Reduction in Per Capita Medical Expenditure for Elderly Residents in Yubari City. Social Insurance Journal. 2014; 2584: 12–29. https://cir.nii.ac.jp/crid/1522262180335660288.
- Available at: https://www.mhlw.go.jp/toukei/saikin/hw/iryosd/22/dl/11gaikyou04.pdf (accessed December 15, 2025).
- Available at: https://www.mhlw.go.jp/content/iryohi_r04.pdf (accessed December 15, 2025).
- Available at: https://www.mhlw.go.jp/toukei/saikin/hw/life/tdfk20/dl/tdfk20-10.pdf (accessed December 15, 2025).
- Available at: https://www.mhlw.go.jp/content/10904750/001363069.pdf (accessed December 15, 2025).
- OECD Hospital beds Hospital beds is a measure of the number of beds maintained, staffed, and immediately available for use in hospitals for delivering inpatient care. Available at: https://www.oecd.org/en/data/indicators/hospital-beds.html (accessed December 15, 2025).
- OECD Doctors Doctors are defined as “practising” physicians who provide direct care to patients. Available at: https://www.oecd.org/en/data/indicators/doctors.html (accessed December 15, 2025).
- Katori T. Japan’s healthcare delivery system: From its historical evolution to the challenges of a super-aged society. Glob Health Med. 2024; 6: 6-12. [CrossRef]
- Shigeoka H, Fushimi K. Supplier-induced demand for newborn treatment: evidence from Japan. J Health Econ. 2014; 35: 162-78. [CrossRef]
- Hamada H, Sekimoto M, Imanaka Y. Effects of the per diem prospective payment system with DRG-like grouping system (DPC/PDPS) on resource usage and healthcare quality in Japan. Health Policy. 2012; 107: 194-201. [CrossRef]
- Fushimi K, Matsuda S. Health resource reallocation by casemix data in Japan. BMC Health Services Research 2009, 9(Suppl 1): A10. [CrossRef]
- Park S, Lee J, Ikai H, et al. Decentralization and centralization of healthcare resources: investigating the associations of hospital competition and number of cardiologists per hospital with mortality and resource utilization in Japan. Health Policy. 2013;113(1-2):100-9. [CrossRef]
- Une H. Medical expenditure for the elderly and factors related to its geographical variations within Fukuoka Prefecture. Nihon Koshu Eisei Zasshi. 1996; 43: 28-36.
- Ohta R, Ryu Y, Katsube T, et al. Rural Homecare Nurses’ Challenges in Providing Seamless Patient Care in Rural Japan. Int J Environ Res Public Health. 2020; 17: 9330. [CrossRef]
- Fukui S, Yamamoto-Mitani N, Fujita J. Five types of home-visit nursing agencies in Japan based on characteristics of service delivery: cluster analysis of three nationwide surveys. BMC Health Serv Res. 2014; 14: 644. [CrossRef]
- Fisher ES, Wennberg JE, Stukel TA, Skinner JS, Sharp SM, Freeman JL, Gittelsohn AM. Associations among hospital capacity, utilization, and mortality of US Medicare beneficiaries, controlling for sociodemographic factors. Health Serv Res. 2000; 34:1351-62.
- Krakauer H, Jacoby I, Millman M, Lukomnik JE. Physician impact on hospital admission and on mortality rates in the Medicare population. Health Serv Res. 1996; 31:191-211.
- Miyagami T, Shimizu T, Kosugi S, et al. Roles considered important for hospitalist and non-hospitalist generalist practice in Japan: a survey study. BMC Prim Care. 2023; 24: 139. [CrossRef]
- Tsutsumi T, Shin JH, Tsunemitsu A, et al. The Evaluation of Hospitalist Care for Patients with Aspiration Pneumonia Using Risk-adjusted Performance Indicators Developed from a Nationwide Inpatient Database. Intern Med. 2025; 64: 1031-1039. [CrossRef]
- Tago M, Hirata R, Shikino K, et al. A Classification Method for General Medicine Physicians to Advance Field Research in Japan. Int J Gen Med. 2025; 18: 5033-5038. [CrossRef]
- Hatta M, Ichiki T, Morita H, et al. A combination of oral care and 23-valent-pneumococcal vaccination is able to reduce pneumonia incidence in nursing homes. The Dental Journal of Health Sciences University of Hokkaido. 2015; 34: 45-53. https://hsuh.repo.nii.ac.jp/record/10457/files/45-53.pdf.
- Available at: https://prs.sante-iledefrance.fr/srs/index.html (accessed December 15, 2025).
- Available at: https://www.bundesgesundheitsministerium.de/presse/pressemitteilungen/krankenhausreform-passiert-den-bundesrat.html (accessed December 15, 2025).
- Available at: https://www.cihi.ca/en/topics/home-care/reports-and-releases (accessed December 15, 2025).
- Shi C, Dumville J, Rubinstein F, et al. Inpatient-level care at home delivered by virtual wards and hospital at home: a systematic review and meta-analysis of complex interventions and their components. BMC Med. 2024; 22: 145. [CrossRef]
- Leong MQ, Lim CW, Lai YF. Comparison of Hospital-at-Home models: a systematic review of reviews. BMJ Open. 2021; 11: e043285. [CrossRef]
Figure 1.
A: Number of hospital beds per 1,000 inhabitants in G7 countries and Korea, 2021. Data sourced from Reference [13]. B: Number of physicians per 1,000 inhabitants in G7 countries and Korea, 2022. Data sourced from Reference [14].
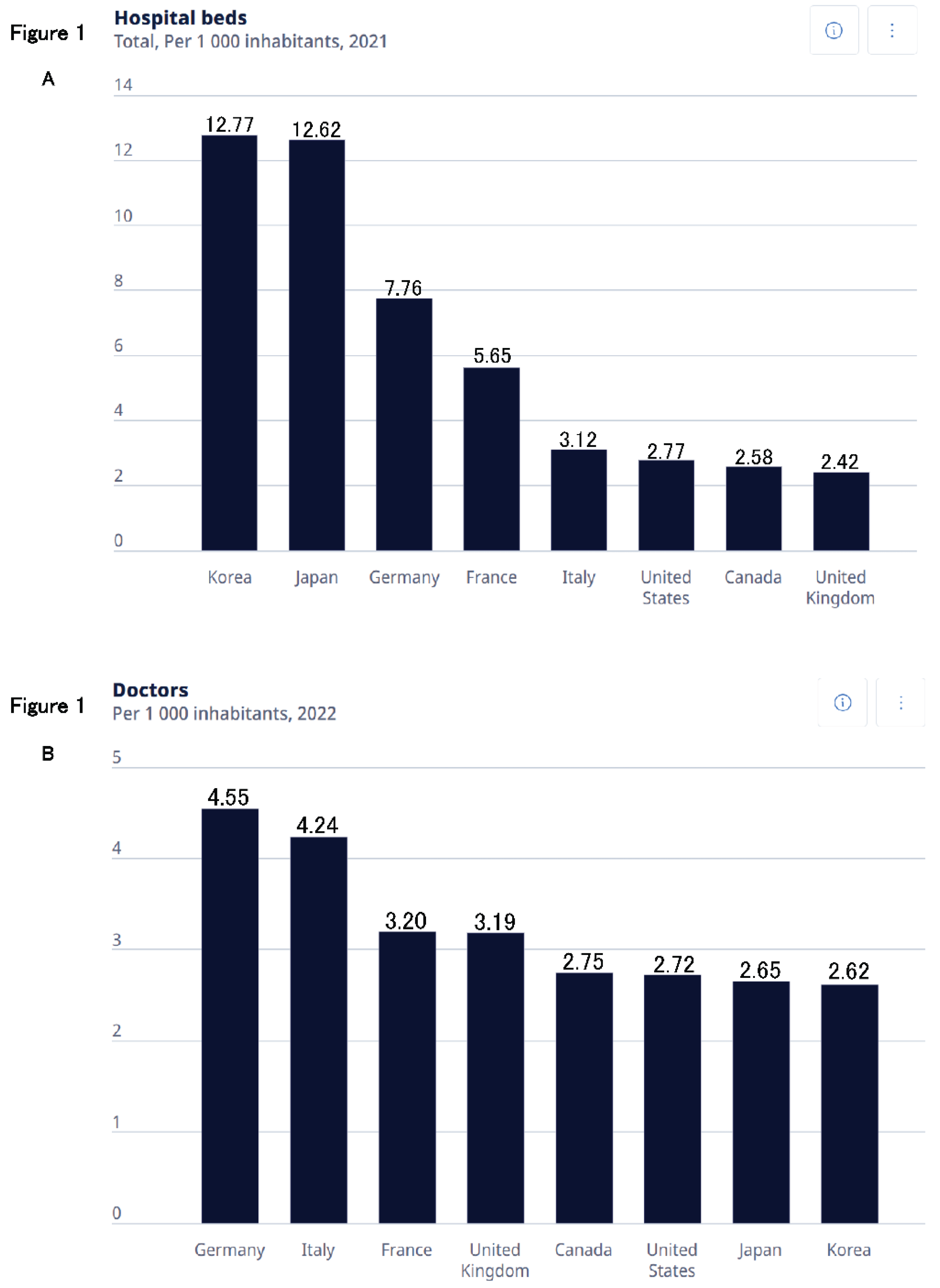
Figure 2.
Association Between the Number of Hospital Beds per 100,000 People and Medical Expenditure per Capita.
Figure 2.
Association Between the Number of Hospital Beds per 100,000 People and Medical Expenditure per Capita.
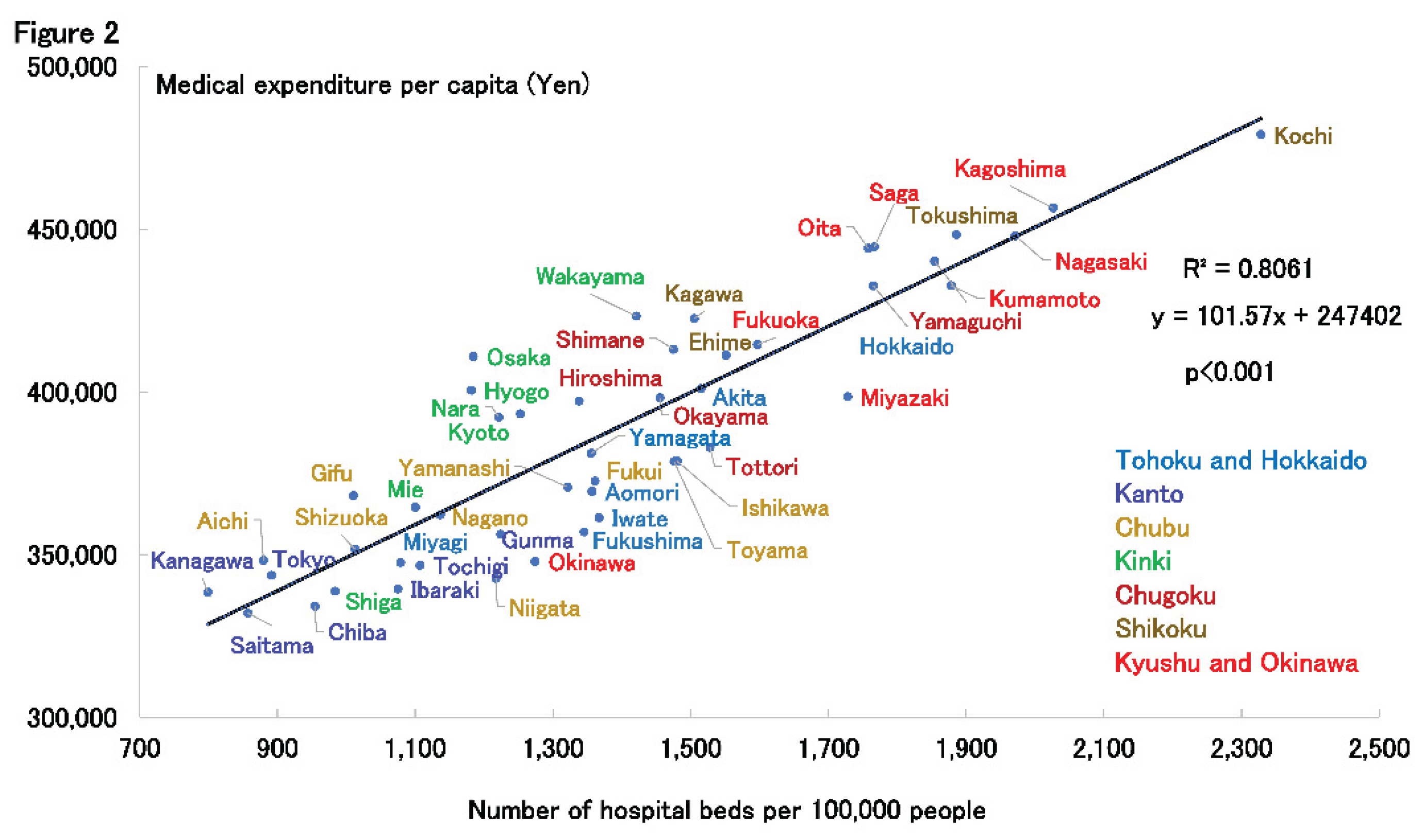
Figure 3.
A: Association Between the Number of Hospital Beds per 100,000 People and Life Expectancy in Men. B: Association Between the Number of Hospital Beds per 100,000 People and Healthy Life Expectancy in Men. C: Association Between the Number of Hospital Beds per 100,000 People and Life Expectancy in Women. D: Association Between the Number of Hospital Beds per 100,000 People and Healthy Life Expectancy in Women.
Figure 3.
A: Association Between the Number of Hospital Beds per 100,000 People and Life Expectancy in Men. B: Association Between the Number of Hospital Beds per 100,000 People and Healthy Life Expectancy in Men. C: Association Between the Number of Hospital Beds per 100,000 People and Life Expectancy in Women. D: Association Between the Number of Hospital Beds per 100,000 People and Healthy Life Expectancy in Women.
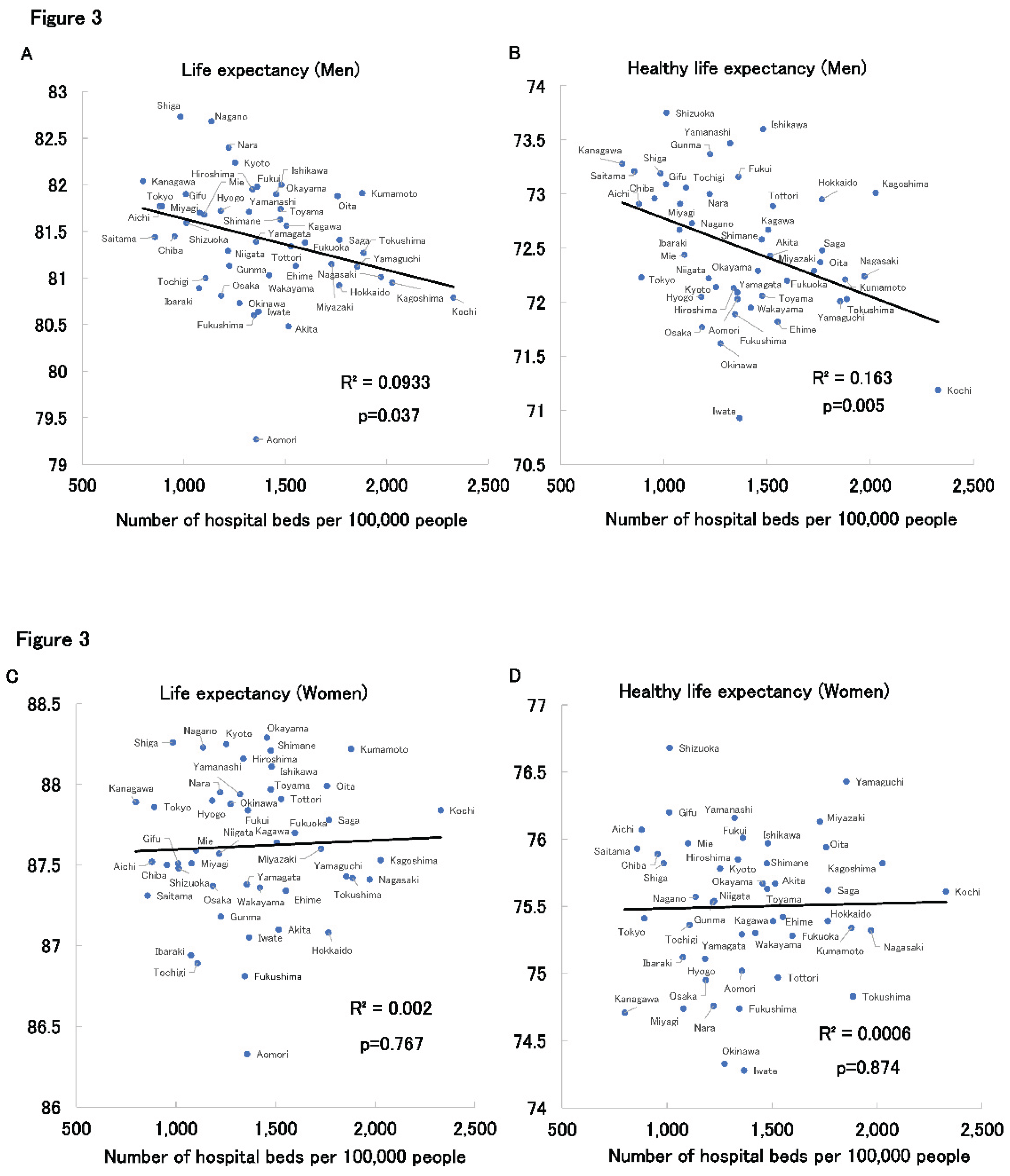
Figure 4.
Cited from Reference [8]. A: Trends in the Total Number of Deaths Before and After the Closure of the Municipal Hospital. B: Trends in the Number of Emergency Dispatches Before and After the Closure of the Municipal Hospital.
Figure 4.
Cited from Reference [8]. A: Trends in the Total Number of Deaths Before and After the Closure of the Municipal Hospital. B: Trends in the Number of Emergency Dispatches Before and After the Closure of the Municipal Hospital.
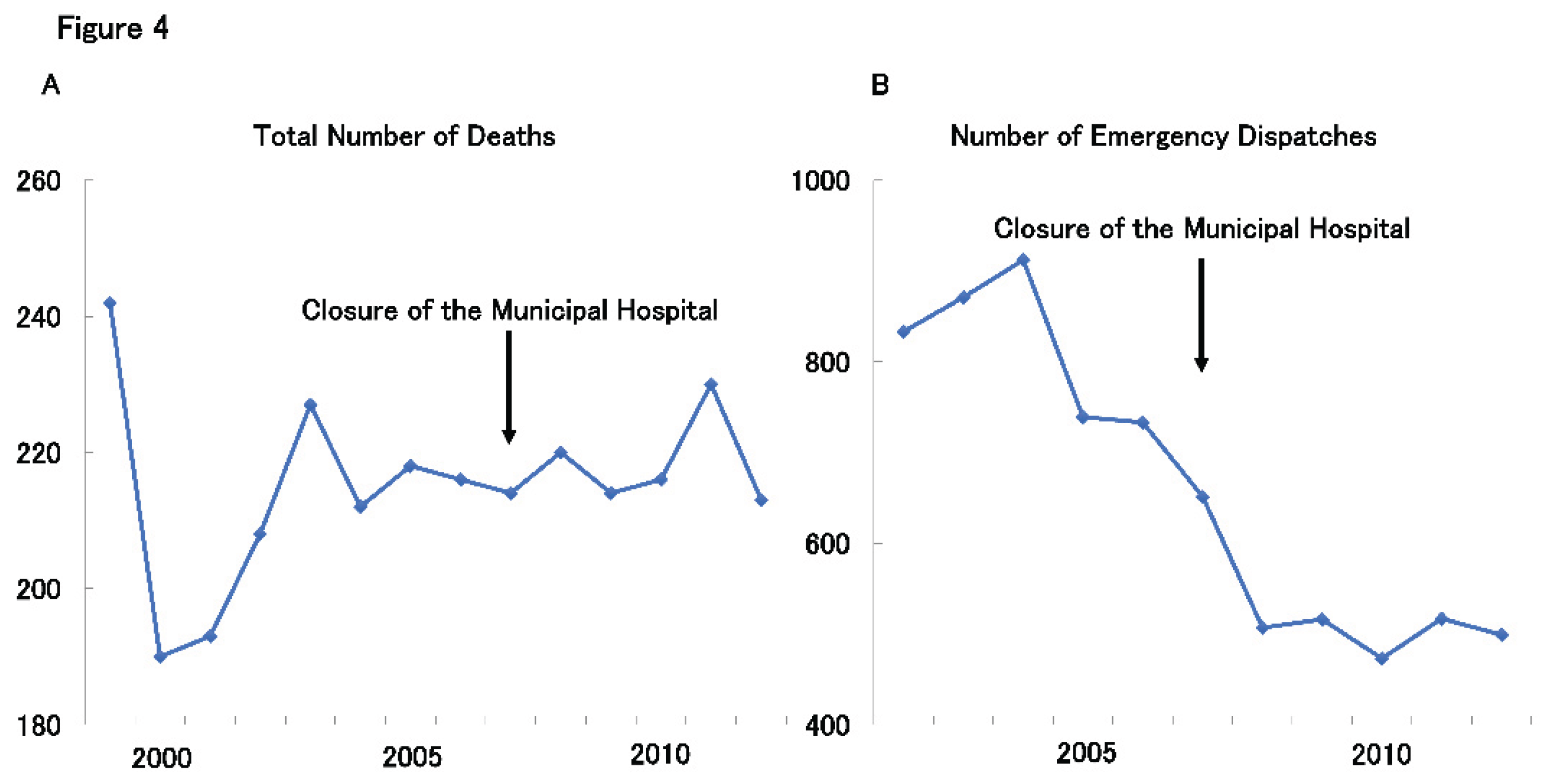
Figure 5.
Cited from Reference [8]. A: Standardized Mortality Ratios (SMRs) for All-Cause Mortality, Cancer, Heart Disease, Cerebrovascular Disease, and Pneumonia Before and After the Closure of the Municipal Hospital in Men. B: Standardized Mortality Ratios (SMRs) for All-Cause Mortality, Cancer, Heart Disease, Cerebrovascular Disease, and Pneumonia Before and After the Closure of the Municipal Hospital in Women.
Figure 5.
Cited from Reference [8]. A: Standardized Mortality Ratios (SMRs) for All-Cause Mortality, Cancer, Heart Disease, Cerebrovascular Disease, and Pneumonia Before and After the Closure of the Municipal Hospital in Men. B: Standardized Mortality Ratios (SMRs) for All-Cause Mortality, Cancer, Heart Disease, Cerebrovascular Disease, and Pneumonia Before and After the Closure of the Municipal Hospital in Women.
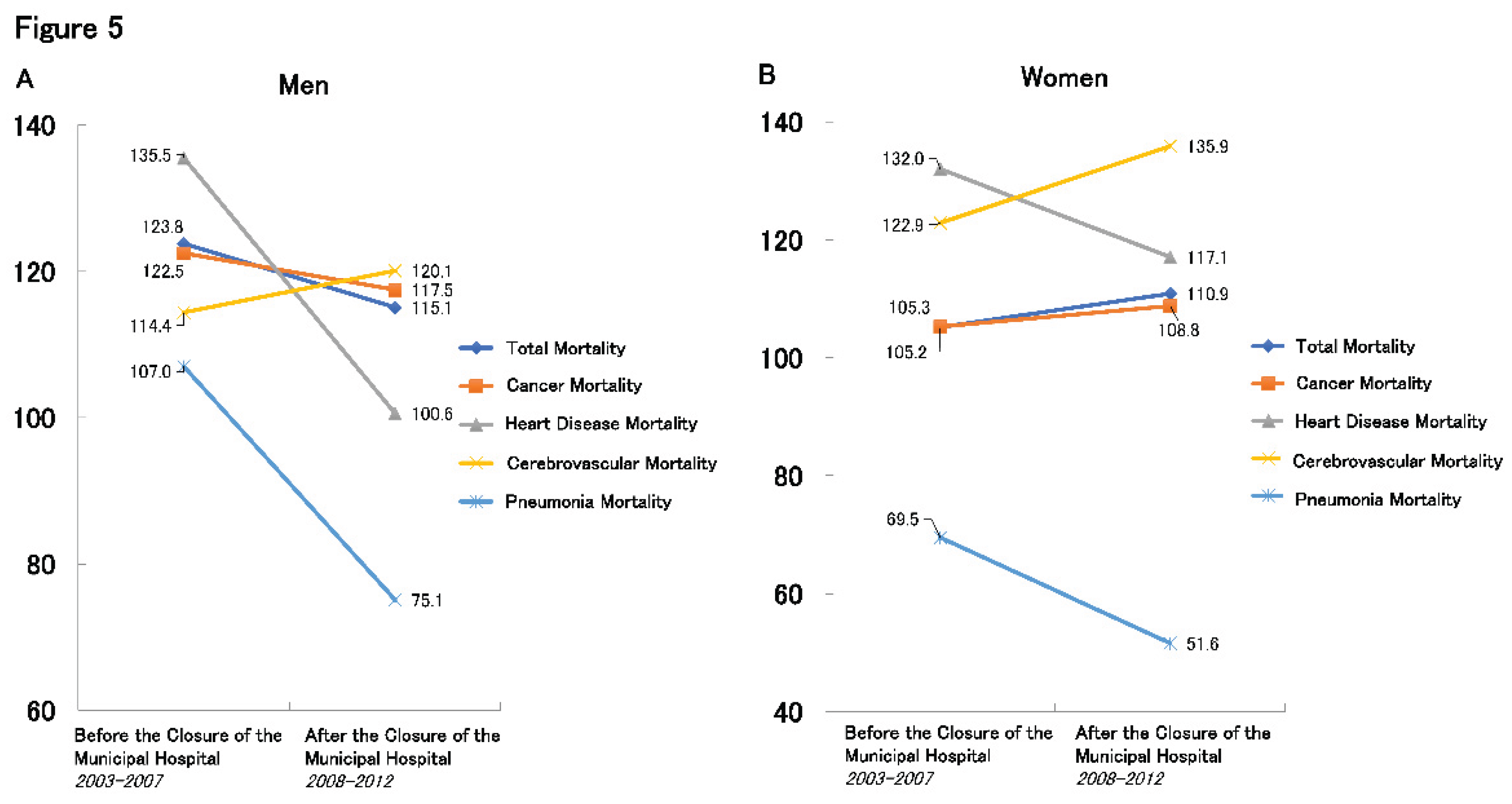
Figure 6.
Cited from Reference [8]. Trends in the Medical and Long-term Care Costs per Elderly Person in Yubari City (as a Ratio to Hokkaido).
Figure 6.
Cited from Reference [8]. Trends in the Medical and Long-term Care Costs per Elderly Person in Yubari City (as a Ratio to Hokkaido).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



