
Submitted:
30 June 2025
Posted:
02 July 2025
You are already at the latest version
Abstract
Background: Dental professionals face high levels of occupational stress, which intensi-fied during the COVID-19 pandemic, contributing to increased burnout, diminished well-being, and signs of accelerated biological aging. This systematic review explores the role of physical activity as a protective factor for mental and physical health, with a focus on promoting resilience and long-term occupational sustainability in a post-pandemic, volatile, uncertain, complex, and ambiguous (VUCA) environment. Methods: A systematic literature review was conducted following PRISMA 2020 guidelines. Studies published between 2000 and 2024 were identified via PubMed, Scopus, and Cochrane Library using MeSH terms related to dentistry, physical activity, stress management, and occupational health. Inclusion and quality appraisal followed standardized criteria. Results: Out of 850 records screened, 28 studies met the inclusion criteria. The findings consistently indicated that physical activity was associated with reductions in burnout, improved psychological well-being, enhanced postural function, and markers of slowed biological aging among dental professionals. Interventions that combined exercise with ergonomic education, stress reduction techniques, and institutional support showed the greatest impact on professional sustainability. Conclusions: Physical activity, when embedded within broader workplace wellness frameworks, contributes meaningfully to the mental and physical resilience of dentists. Integrating movement, ergonomics, and psychosocial support into dental practice environments may serve as an effective strategy for safeguarding long-term workforce sustainability and public health outcomes.
Keywords:
dentists
; occupational health
; physical activity
; workplace wellness
; stress management
; mental health
; resilience
; sustainability
; ergonomic support
; well-being
1. Introduction
Dentistry is widely recognized as one of the most physically and mentally demanding healthcare professions [1]. Dental practitioners are required to maintain high levels of technical proficiency, precision, and sustained concentration, often while performing repetitive procedures in confined and ergonomically challenging environments [2,3]. These physical demands are compounded by psychological stressors, such as managing patient expectations, minimizing procedural errors, and achieving optimal clinical outcomes, factors that can significantly affect both patient satisfaction and practitioner well-being [4]. Even minor procedural mistakes can have serious implications, thereby intensifying the psychological pressure on practitioners [5,6]. In addition long working hours, continuous education requirements, and the obligation to provide meticulous care under time constraints further augment mental fatigue and emotional exhaustion [7,8,9]. At the same time, the prevalence of musculoskeletal disorders (MSDs) among dentists remains alarmingly high [10]. These conditions have been linked to sustained awkward postures, repetitive hand movements, and prolonged static positioning during clinical procedures [5,10]. Common issues include back and neck pain, shoulder stiffness, and carpal tunnel syndrome which significantly impair quality of life and may even lead to early retirement from clinical practice [4].
In response to these occupational hazards, increasing attention has turned to modifiable protective factors, particularly regular physical activity, as means of promoting resilience and occupational sustainability among healthcare professionals [11,12,13]. Physical activity is associated with numerous health benefits, including reduced stress, enhanced cognitive performance, and improved mood regulation, factors essential for managing the high cognitive and emotional demands of dentistry [6]. In addition, strengthening core muscles and enhancing posture through regular exercise may reduce the ergonomic strain faced by dental professionals [8]. Aerobic activities such as running and swimming are also known to stimulate endorphin release, which contributes to emotional well-being in high-stress professions [14]. Furthermore, regular physical activity contributes to better sleep quality, which is critical for maintaining attention, energy levels, and overall performance during long clinical shifts [6,8,9,15,16]. Beyond general wellness, physical activity has been shown to positively influence biological aging by regulating circadian rhythms and decreasing oxidative stress markers [17].
Dentists are particularly susceptible to accelerated cellular aging due to chronic inflammation and prolonged physical stress [18], but these effects may be controled through exercise, which promotes musculoskeletal health, stabilizes biological rhythms, and supports psychological resilience [19,20]. Although the benefits are well-documented, many dentists struggle to incorporate regular physical activity into their routines due to fatigue, workload, and lack of institutional support [21]. These challenges were further intensified during the COVID-19 pandemic, which forced rapid changes in clinical protocols and heightened mental strain across the profession [22,23]. Post-pandemic findings report on the need for strategies that enhance psychological resilience and reduce burnout, with physical activity identified as a critical component for achieving long-term professional sustainability [6,24,25,26].
Despite this, there remains a significant gap in the literature regarding how physical activity specifically supports the occupational health of dental professionals. Existing reviews often focus on general healthcare workers or rely on pre-pandemic data that may not reflect the current realities of dental practice [27,28,29,30]. Moreover, few interventions have been tailored to address the unique ergonomic and psychological demands faced by dentists in contemporary practice [31].
The present review aims to address this gap by examining how physical activity enhances both physical and mental resilience in dentists, especially in a post-pandemic context. It also seeks to identify evidence-based strategies for integrating exercise into clinical routines, overcoming participation barriers, and informing holistic interventions that promote well-being, career sustainability, and healthy aging within the profession [6,26].
2. Materials and Methods
In this systematic review, we followed guidelines provided by PROSPERO (https://www.crd.york.ac.uk/prospero/) and informed by the systematic review protocol registered under ID CRD42024523797. The methodology involves a thorough search strategy utilizing databases such as PubMed, Scopus, and Cochrane, focusing on quantitative and experimental studies to understand how the pandemic has reshaped the health and work-life conditions of dental professionals. The search was conducted using Boolean operators (e.g., "AND", "OR") and included combinations of keywords such as “dentists”, “physical activity”, “mental health”, “aging”, “circadian rhythm”, “career sustainability”, and “anti-aging”. These keywords were selected to capture studies that explore the multifaceted effects of physical activity on both physical and psychological aspects of dental professionals’ well-being, including its potential role in regulating biological rhythms, supporting longevity, and promoting professional resilience. While terms such as ‘anti-aging,’ ‘circadian rhythm,’ and ‘career sustainability’ were not explicitly used in the database search strategy, they emerged as recurring themes during full-text analysis and synthesis. These terms reflect conceptual lenses through which the findings were interpreted and contextualized. Filters were applied to limit results to human studies, English language, and publication years from 2000 to March 2024.
These databases were selected due to their broad coverage of biomedical, public health, and psychological research, ensuring access to peer-reviewed, high-quality literature relevant to the intersection of physical activity and occupational health [33]. The extended publication window (2000–2024) was intentionally chosen to allow for the inclusion of foundational and pre-pandemic research, enabling the comparison of patterns and trends before and after COVID-19. This helps contextualize post-pandemic findings within a broader historical framework. Although this review focuses on post-pandemic implications, pre-2020 studies were retained when they contributed valuable data on musculoskeletal disorders, stress, and resilience factors among dental professionals, thus enhancing the comprehensiveness of the analysis. A formal comparative analysis (pre vs. post-pandemic) was not conducted due to variability in study designs, outcome measures, and population characteristics, which made direct comparison methodologically inappropriate. This approach aimed to identify a broad range of relevant studies and minimize the exclusion of potentially significant findings [34]. Additionally, quality assessment, data extraction, and statistical analysis have been conducted, following standardized protocols such as the Newcastle-Ottawa scale and SPSS tools [35]. We also conducted our search following the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) (https://www.prisma-statement.org/).
Inclusion and exclusion criteria were applied to select studies for this review. Studies were eligible if published between 2000 and March 2024, and written in English. This timeframe was chosen to capture advancements in research methodologies and data availability over the past two decades, focusing on the impact of physical activity on dentists’ physical, oral, and mental health. We limited studies to those in English to allow accessibility to the review team. To ensure a comprehensive dataset, the review included cross-sectional studies (observational studies that analyze data from a population at a specific point in time), case-control studies (studies comparing subjects with a specific condition to those without), and experimental studies (research involving intervention and control groups). Prospective and cohort studies were excluded to maintain consistency in study design and reduce heterogeneity in the analytical framework. The focus was specifically on observational snapshots and experimental interventions, which allowed for a more uniform comparative analysis across studies [36]. Exclusion criteria were applied to studies that did not focus on dentists or did not consider physical activity as a key factor.
The review process included a thorough assessment of the methodological quality of the selected studies to ensure they met good scientific standards, enhancing the validity of the findings [37]. To evaluate the quality of the included studies, we applied the Newcastle-Ottawa Scale (NOS) (https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp) for observational studies and the JBI Critical Appraisal Tools (https://jbi.global/critical-appraisal-tools) where applicable. These tools assess domains such as sample selection, comparability of groups, and outcome measurement. Two reviewers independently assessed the quality of all included studies and categorized them by study design (e.g., cross-sectional, case-control, experimental). Discrepancies were resolved through discussion, and in case of a negative response from one reviewer, we kept the article when consensus could not be reached. Inter-rater reliability was substantial though, confirming the consistency of the classification process.
A total of 800 records were initially identified through electronic databases, PubMed (n = 410), Scopus (n = 320), and the Cochrane Library (n = 70). An additional 50 records were identified through manual searches, grey literature, and other registers, bringing the total number of identified records to 850. After removing 200 duplicates, 650 records remained for screening at the title and abstract level. Of these, 522 records were excluded for the following reasons: irrelevance to dentistry or occupational health (n = 183), not focusing on physical activity or musculoskeletal disorders (n = 225), and being review articles or protocols without primary data (n = 114). This left 128 records for full-text retrieval. Of these, 19 could not be retrieved. The remaining 109 full-text articles were assessed for eligibility. A total of 84 articles were further excluded for the following reasons: wrong population (non-dental healthcare workers) (n = 25), inadequate outcome measures (n = 20), low-quality studies or insufficient methodology (n = 20), and duplicate or overlapping datasets (n = 16). Ultimately, 28 studies were included in the final review. Figure 1 presents the PRISMA flowchart outlining the study's search and selection process.
3. Results
Twenty-five studies were included in this review, representing a broad range of geographical regions and providing diverse insights into occupational health among dentists. A summary of these studies is presented in Table 1.
A notable trend in literature is the predominant focus on musculoskeletal disorders (MSDs), often prioritized over mental health and job satisfaction among dental professionals. Also, as shown in Figure 2, the number of publications examining the impact of physical activity on dentists’ health has steadily increased from 2000 to 2024. In the early 2000s, annual publication rates were low, with fewer than 10 studies per year. However, from 2010 onward, there was a gradual rise in research output, reflecting growing awareness of the physical demands of dental practice and the potential protective role of physical activity. This trend accelerated significantly after 2017, with a sharp increase in publications post-2020, likely driven by the COVID-19 pandemic’s spotlight on occupational health, burnout, and work-related injuries [47,50]. Many of the studies published during this period, particularly those assessed in this review, emphasize the high prevalence of MSDs and the role of ergonomics, while also drawing attention to the psychological strain dentists face [10,52,53,54,55,56,57,58]. Collectively, this growing body of evidence supports the relevance of physical activity not only for preventing MSDs but also for improving emotional resilience, reducing burnout, and enhancing overall occupational well-being (Figure 1).
The included studies in this review, span a diverse range of countries, each contributing to a broader understanding of occupational health among dental professionals. Three studies were conducted in Turkey, accounting for 10% of the total. All Turkish studies were categorized as “Unspecified,” as they did not clarify whether the research was based in public, private, or mixed-sector settings. Similarly, three studies were carried out in India (10%), none of which reported sector-specific details. Two studies were identified from Italy (6.67%), both lacking information on sector affiliation. China, Pakistan, and Romania each had two studies included (6.67% respectively); only one of the Chinese studies explicitly referred to the public sector [46], while the others were classified as “Unspecified.” Single studies were also conducted in countries such as Finland, Afghanistan, Yemen, Portugal, Lebanon, Bangladesh, Bahrain, Canada, Kuwait, Iran, the United Arab Emirates, South Africa, Germany, Poland, Greece and Croatia, each representing approximately 3.33% of the total. Since across the dataset, the vast majority of studies did not provide sufficient information to determine whether the research was conducted in public or private sector environments we presume that this lack of detail may reflect either a general omission in study reporting or the fact that sectoral context was not a central focus in most investigations.
Population and sample size
The sample sizes varied considerably across the included studies, affecting both the statistical power and the generalizability of their findings. Larger-scale studies, such as the one conducted by Al-Huthaifi et al. (2023) in Yemen involving 310 dental professionals, offer stronger data compared to smaller studies like that of Javed et al. (2023) in Pakistan, which included only 50 participants [37,42]. Similarly, Gandolfi et al. (2021) in Italy surveyed 284 dental professionals, while Berdouses et al. (2020) conducted a nationwide survey in Greece with a substantial sample of 1,500 dentists. [10,48] Both studies provide more reliable estimates regarding the prevalence of musculoskeletal disorders (MSDs) and other occupational health concerns. In contrast, studies with smaller sample sizes, such as some conducted in Turkey and South Africa, limit the extent to which their findings can be generalized to wider populations [40,56].
Data collection methods
Most studies relied on self-administered questionnaires to collect data on occupational health among dental professionals. This approach enables efficient, large-scale data collection and provides both quantitative and qualitative insights. Fourteen of the reviewed studies used questionnaires as their primary tool, highlighting their practicality in assessing musculoskeletal disorders (MSDs), workplace conditions, and health perceptions. Some studies also incorporated interviews for deeper exploration of personal experiences. Also, quantitative data were commonly analyzed using statistical methods such as chi-square tests, ANOVA, t-tests, and multivariate analyses. These techniques allowed researchers to examine associations between variables like ergonomic practices, work hours, and MSD prevalence. Multivariate analysis, in particular, strengthened the findings by accounting for confounding factors such as age, gender, and years of practice. In general, the consistent use of structured data collection and statistical analysis enhanced the reliability of results and supported evidence-based recommendations for improving occupational health in dentistry.
More specifically, the reviewed studies employed a range of statistical methods to examine associations between occupational factors and health outcomes. Descriptive statistics and chi-square tests were frequently used to explore relationships between variables such as gender, working hours, and the prevalence of musculoskeletal disorders (MSDs), as seen in studies by Macrì et al. (2023) in Italy and Peru, and Al-Huthaifi et al. (2023) in Yemen [37,41]. Al-Emara et al. (2024) in Finland applied correlation analysis and age-adjusted models to evaluate the impact of MSDs on work ability [39]. Further, regression analyses, including multivariate models, were used in several studies to control confounders such as age, gender, years of practice, and ergonomic factors. For example, Matur et al. (2023) demonstrated how ergonomic practices and duration of hand use were significant predictors of carpal tunnel syndrome [40]. These multivariate approaches enhanced the interpretability of findings and guided more targeted interventions. Overall, while most studies applied appropriate statistical techniques, limited sample sizes in some cases reduced statistical power. Future research would benefit from larger, more representative samples and longitudinal study designs to assess the long-term effects of occupational exposures and ergonomic interventions. Expanding research to include underrepresented regions and varied dental practice settings will also help refine strategies that address the occupational health needs of the global dental workforce.
Limitations reported
Several limitations were consistently noted across the reviewed studies. A key concern was the heterogeneity in study design, methodology, outcome measures, and sampled populations, which limits comparability and generalizability of the findings. Self-reporting bias was a common issue, with participants potentially under- or overestimating symptoms, a limitation acknowledged in studies such as Al-Emara et al. (2024) in Finland and Azimi et al. (2024) in Afghanistan [4,39]. Small sample sizes further affected the reliability and representativeness of results in studies like Matur et al. (2023) in Turkey, Macrì et al. (2023) in Italy and Peru, and Javed et al. (2023) in Pakistan [40,41,42].
Geographic limitations were also evident. For example, Al-Huthaifi et al. (2023) highlighted the restricted regional scope of their research in Yemen, which may not reflect broader national or international trends [37]. Other studies faced methodological shortcomings, including limited reporting on sampling strategies or the absence of standardized quality assessments, which affect the strength of conclusions. Additionally, as it is already mentioned, many studies did not distinguish between public and private sector settings, reducing the contextual clarity of occupational health risk factors. In general, these limitations report on the need for more methodologically strong research, including larger, more diverse samples, clearly defined variables, and longitudinal designs that better capture the long-term effects of occupational stressors in dentistry.
Cultural diversities
The reviewed studies provide a valuable cross-cultural perspective, offering insights into how workplace practices, economic conditions, and healthcare infrastructure influence occupational health outcomes in dentistry. Research conducted across multiple countries illustrates the varied nature of risks such as musculoskeletal disorders (MSDs), burnout, and work-related stress, and emphasizes the need for tailored preventive approaches. For instance, Macrì et al. (2023) compared dental professionals in Italy and Peru, identifying significant differences in MSD prevalence linked to gender, working hours, and physical activity [41]. Their findings highlight how sociocultural and systemic factors shape occupational risks. Similarly, Al-Huthaifi et al. (2023) in Yemen examined the frequency of MSDs and other occupational hazards among dentists, noting that the lack of ergonomic education and standardized work protocols may contribute to higher rates of work-related injuries in lower-resource settings [37]. In addition, Gandolfi et al. (2021) in Italy found that gender, work hours, and years of experience were significantly associated with MSDs, stressing the importance of ergonomic knowledge and physical activity [10]. In contrast, Al-Emara et al. (2024) in Finland linked MSDs directly to reduced work ability and increased risk of long-term disability, reporting on the need for occupational health interventions even in high-income countries with well-established healthcare systems [39]. Also, from South Asia, Azimi et al. (2024) in Afghanistan reported high levels of fatigue, stress, and back pain, noting that most participants perceived dentistry as a highly stressful profession [4], while Asaduzzaman et al. (2022) in Bangladesh also emphasized the prevalence of ergonomic challenges, particularly among older and more senior practitioners [36]. These findings align with those from India, where long working hours, lack of physical activity, and high levels of occupational stress were repeatedly identified as key contributors to MSDs and obesity in dental professionals [43.]. In addition, in Pakistan, studies by Javed et al. (2023) and Ahmad et al. (2015) highlighted gender disparities in MSD symptoms, low physical activity levels, and inadequate mental health support, especially among female dentists [42,52]. Similarly, Hashim & Al-Ali (2013) in the UAE found a notable prevalence of systemic health problems and unhealthy lifestyle habits, including low rates of regular exercise and high smoking rates, reflecting broader occupational health risks beyond MSDs [54]. Meanwhile, Zhou et al. (2021) in China conducted a comparative study between dentists and office workers in a public hospital, reporting significantly higher rates of neck pain and reduced pain thresholds in dentists [46]. Finally, in Canada, Harris et al. (2020) found a strong correlation between years in practice and the number of MSDs reported, with 83% of dental hygienists experiencing work-related disorders, further reinforcing the cumulative effect of long-term ergonomic strain [51].
These diverse regional findings demonstrate that occupational hazards in dentistry are shaped by a complex interplay of physical, organizational, and cultural factors. They collectively point to the need for localized interventions, ranging from ergonomic training and preventive policies to lifestyle support and mental health resources, designed to address the specific risks faced by dental professionals in different countries. It is then reported that implementing such tailored strategies can significantly enhance occupational well-being and reduce the global burden of work-related health issues in the dental field.
Prevalence and Risk Factors of Musculoskeletal Disorders (MSDs)
The reviewed literature consistently reveals a high prevalence of musculoskeletal disorders (MSDs) among dental professionals, particularly affecting the back, neck, shoulders, and wrists. These disorders are primarily attributed to prolonged static postures, repetitive hand movements, and awkward working angles that are characteristic of dental procedures. Such physical strain not only compromises clinical performance but also significantly reduces quality of life and work longevity, often resulting in absenteeism and financial burden due to disability or decreased productivity [37,39]. Also, ergonomic risk factors were highlighted across numerous studies, with poor posture, insufficient breaks, high patient loads, and lack of ergonomic equipment identified as primary contributors. For example, [48] reported that 54.1% of Greek dentists suffered from MSDs, with distribution patterns influenced by work posture and the use of four-handed dentistry. Similarly, [49] found a 63.05% prevalence of occupational injuries among Croatian dentists, with needle punctures, spinal strain, and eye injuries being the most common. These injuries were linked to factors such as improper posture, noise exposure, and work-related stress.
Moreover, the need for ergonomic awareness and physical activity was emphasized in multiple studies. Sharma & Golchha (2011) demonstrated a significant correlation between regular physical activity and reduced MSD symptoms among Indian dentists [51]. This was echoed by Singh & Purohit (2012), who found that interns and students were generally more physically active and less affected by MSDs than senior faculty, highlighting the role of lifestyle habits and professional hierarchy in occupational health outcomes.[55]. In addition, Harris et al., (2020) conducted a large-scale study of Canadian dental hygienists and found that 83% reported at least one MSD, with carpal tunnel syndrome and tendonitis being especially common [51]. The study also noted that MSD prevalence increased with years of practice, underscoring the cumulative nature of ergonomic strain. Similarly, Kierklo et al., (2011) in Poland found that MSDs were particularly prevalent in the neck and lower back, with significant associations to years of clinical experience and insufficient rest breaks [58]. Other researchers in South Africa reported that 49.32% of dentists experienced vertebral or spinal pain, 18.75% reported wrist pain, and 16.66% experienced shoulder pain, all strongly linked to prolonged static postures and high hand activity [56]. The study also noted that lower limb discomfort, such as leg pain, affected 12.5% of the sample, indicating the widespread physical burden associated with dental work.
Global Patterns and Professional Predictors of MSDs
Musculoskeletal disorders (MSDs) are among the most prevalent occupational health issues in dentistry, driven largely by prolonged static postures, repetitive hand movements, and sustained precision work. Studies across diverse regions confirm the global nature of this problem, linking MSDs to diminished work ability, chronic pain, and reduced professional performance. For example, in Finland, [Al-Emara et al., 2024] found that dentists with MSDs reported significantly lower work ability scores and greater disability, emphasizing the functional impact of these conditions [39]. Similarly, Gandolfi et al., (2021) in Italy identified gender, extended working hours, and years of experience as key predictors, with female practitioners and those with longer clinical exposure showing higher MSD prevalence [10]. Global studies also highlight the role of poor ergonomic conditions, noting that inadequate chair and instrument design contribute significantly to chronic strain [59,60,61,62,63]. These findings suggest the need for targeted, preventive strategies that account for individual risk factors (e.g., gender, workload, years of practice) and workplace ergonomics. Improving design standards and promoting ergonomic education across dental settings can help control the widespread burden of MSDs in the profession.
Physical Activity as a Protective Factor
Physical activity plays a critical role in managing occupational stress and preventing health issues like musculoskeletal disorders (MSDs) among dental professionals. In Afghanistan, Azimi et al. (2024) 3 investigated the impact of physical activity on dentists’ well-being, focusing particularly on reducing fatigue and enhancing mental health [4]. Their findings highlight that physical activity not only alleviates physical strain but also improves mental resilience, making it a valuable tool in managing occupational demands [4]. This aligns with research by Meyerson et al. (2020), which identified the positive effects of coping strategies on burnout, where physical activity emerged as an effective method for managing stress and reducing the risk of burnout in high-stress professions like dentistry [64]. Further supporting the benefits of physical activity, Matur et al. (2023) examined the prevalence of carpal tunnel syndrome (CTS) symptoms among young dentists in Turkey, finding that physical activity played a protective role in controlling the physical strain associated with repetitive hand movements and static postures common in dental work [40]. This protective effect is consistent with other findings, noting that coping strategies involving physical activity and mental resilience significantly reduced burnout and secondary traumatic stress among Israeli dentists [65]. Such strategies provide both physical relief and psychological support, helping dentists maintain a better professional quality of life.
Circadian Rhythms, Sleep, and Stress Resilience in Dentistry
The relationship between physical activity and stress management also extends to the regulation of circadian rhythms and sleep quality, as evidenced by Kurtovic´ et al. (2023) in China, who focused on the theoretical implications of circadian rhythms concerning dental health [9]. Their study emphasizes the importance of sleep and physical activity in maintaining both physical and mental health, which is crucial in preventing burnout and enhancing overall health [9]. This is further supported by Singh et al. (2016), who outline factors contributing to burnout and recommend integrating physical activity as part of a balanced routine for health professionals [66]. Also, the psychological impact of the COVID-19 pandemic has further emphasized the need for physical activity and stress management strategies. In Germany, Mekhemar et al. (2021) found that the pandemic significantly increased levels of anxiety and burnout among dentists, enhancing existing occupational challenges [26]. Incorporating physical activity as a coping mechanism was shown to control some of these psychological impacts, enabling practitioners to better manage stress during the pandemic [26]. This approach is supported by findings from Szalai et al. (2021) on Hungarian dentists, which indicate that physical activity and structured mental health support reduced burnout symptoms and supported resilience in high-stress environments [67]. Finally, this is further supported by the systematic review by White et al. (2024), which synthesized findings from 116 studies and highlighted that physical activity improves mental health not just directly, but also indirectly through enhanced self-efficacy and social support [68]. These mediating and moderating mechanisms are particularly relevant in high-stress professions like dentistry, where cognitive and emotional resilience are critical [69].
Occupational Stress Management and Mental Health Interventions
Studies employing mean-oriented and frequency-oriented ranking methods have highlighted "Long working hours" as the primary stressor in dentistry, with "Tired after work" following closely behind, emphasizing the significant impact of fatigue on mental well-being and career satisfaction [39]. Moreover, financial pressures, high volumes, and the need for excellent patient management skills compound these stressors, as dental professionals often feel the dual pressures of delivering quality care while managing the financial viability of their practice [70]. The high levels of stress and fatigue reported among dentists indicate a pressing need for interventions that address both the mental and physical aspects of their occupational health [59]. To control these stressors, several studies propose a range of comprehensive stress management programs specifically tailored to the unique demands of the dental profession. Cognitive-behavioral therapy (CBT), relaxation training, and mindfulness-based interventions are frequently highlighted as effective measures to alleviate stress and enhance mental resilience [41,71]. Programs incorporating these techniques aim to improve coping strategies among dental professionals by enhancing a greater sense of mental control and awareness, which can reduce stress in high-pressure clinical settings [4]. For instance, mindfulness-based stress reduction (MBSR) has been associated with reduced psychological distress and improved quality of life in healthcare workers, including dentists, by promoting self-regulation and reducing emotional reactivity to daily work stressors [59]. In line with this, Neumann et al. (2022) found that individuals with higher physical fitness levels exhibited significantly greater psychological resilience to daily life stress. The study emphasized the mediating role of general self-efficacy, reinforcing the importance of physical fitness not only for physical health, but also for psychological robustness in demanding professions.[72].
Also, engaging in physical exercise, particularly activities that focus on strengthening the core and postural muscles, helps dental professionals maintain the physical resilience required for their demanding roles [60,70]. Additionally, studies emphasize the importance of including ergonomic interventions, such as stretching routines and posture training, as part of a comprehensive stress management program, which can effectively prevent MSDs and reduce physical discomfort associated with prolonged dental procedures [73]. So, a holistic approach to occupational health in dentistry, which incorporates both physical and mental wellness practices, has been shown to significantly reduce burnout and improve mental health outcomes. Lifestyle adjustments that encourage adequate rest, balanced nutrition, and regular breaks during work hours are critical in sustaining long-term health and job satisfaction [4]. For example, ergonomic adjustments, such as reconfiguring dental workstations and employing adjustable seating, can prevent MSDs and reduce physical strain, while contributing to a more comfortable and supportive work environment [62]. Furthermore, studies underline that addressing root causes of stress through these comprehensive interventions can enhance both job performance and mental well-being, creating a healthier work environment for dental professionals [39,63].
Tailored Interventions and Cultural Approaches to Occupational Health
But while ergonomic interventions are a common focus, there are notable differences across studies in terms of the proposed interventions and their perceived effectiveness. For instance, Mulimani et al. (2018) emphasize physical modifications, such as adjusting dental chairs and workstation layouts, to improve posture and reduce MSDs [73]. In contrast, other research reports the importance of mental health support, including stress management programs and work-life balance adjustments, to address the psychological aspects of occupational stress in dentistry [4]. These variations may derive from differences in study design, sample populations, and cultural contexts, which influence whether physical or psychological interventions are prioritized [71,74].
Additionally, cultural factors appear to play a significant role in shaping how stress management and occupational health are approached in dentistry. In some regions, there is a stronger emphasis on workplace ergonomics, while others prioritize mental health support and work-life balance [41,75]. This divergence suggests that a tailored approach, which considers both physical and psychological needs and adapts to regional practices, maybe the most effective strategy for supporting the occupational health of dental professionals globally [59]. By combining both ergonomic improvements and mental health support, healthcare organizations can create a well-rounded strategy that addresses the comprehensive needs of dental professionals, ultimately leading to enhanced job satisfaction, reduced burnout, and better patient care [75].
The Importance of Education and Continuous Professional Development
Education and training are essential for addressing occupational health issues among dental professionals, as they provide a foundation for reducing physical and mental strain in the workplace [61]. Recent studies underline the importance of targeted ergonomic education in helping dentists maintain proper posture and use ergonomic tools effectively, which is crucial in preventing musculoskeletal disorders (MSDs) caused by prolonged static postures and repetitive movements [37,41]. Incorporating ergonomic awareness into daily practice enables dental professionals to minimize physical strain, leading to better long-term health outcomes [4].
A comprehensive approach to occupational health in dentistry should combine ergonomic training, regular physical activity, and mental health support to address both the physical and psychological demands of the profession [70]. This integrated strategy can support career sustainability by equipping dental professionals with tools to manage stress and prevent burnout [71]. Continuous professional development, through workshops focused on ergonomics, posture, and stress management, has proven to be essential in supporting dental professionals to adopt healthier work habits and maintain long-term well-being [76]. Recent findings emphasize that these workshops not only provide practical strategies for reducing physical strain but also enhance practitioners’ awareness of proper body mechanics and stress management techniques [77]. Further, research by Scheepers et al. (2020) demonstrated a strong link between sedentary behaviors, low physical activity, and increased obesity rates among dental professionals, underlining the pressing need for targeted wellness programs within the field [78]. These programs aim to decrease sedentary habits and cultivate more active lifestyles, contributing to overall health improvements and reduced risks of chronic conditions [79]. Moreover, Al Emara et al. (2024) highlighted that tailored physical activity programs can significantly impact mental and physical health, promoting better occupational outcomes [39]. To add more to this, the World Health Organization (2022) has underlined the importance of integrating workplace wellness initiatives as part of comprehensive occupational health practices, noting their effectiveness in enhancing sustained health and professional productivity [80]. Implementing these programs, which include ergonomic training, structured physical activities, and mental health resources, has been shown to elevate job satisfaction and performance [41,78]. Collective evidence supports a proactive approach that not only addresses physical wellness but also incorporates mental health strategies, creating a well-rounded framework for dental professionals to thrive in their careers [77,78].
Sensitivity Analysis
To assess the review’s conclusions, a sensitivity analysis was performed by sequentially altering key inclusion criteria (Table 2). The findings demonstrated that excluding studies with smaller sample sizes had a low to moderate impact on overall conclusions, with larger-scale research reinforcing previously identified trends. Limiting the analysis to studies employing standardized diagnostic tools showed minimal deviation from the main findings, suggesting strong methodological consistency. However, removing studies from low- and middle-income countries (LMICs) revealed a moderate to high impact, highlighting their role in emphasizing contextual and systemic dimensions of occupational health. Similarly, restricting the dataset to only those studies specifying the healthcare sector led to significant data reduction, resulting in weaker conclusions. Lastly, focusing solely on post-2020 publications caused a thematic shift, with more emphasis on mental health and pandemic-related stressors, while long-standing trends in musculoskeletal disorders were diluted. These results support the stability of core findings while reporting on the importance of inclusive and diverse study populations.
4. Discussion
Previous systematic reviews and meta-analyses in the field have primarily focused on estimating the prevalence of musculoskeletal disorders (MSDs) among dental professionals, offering valuable epidemiological insights into the extent of the problem across regions and professional roles [43]. However, these studies often lack a broader conceptual framework that integrates the physical, psychological, and behavioral dimensions of occupational health. In contrast, the present review adopts a more holistic perspective, examining not only the prevalence of MSDs but also their interplay with psychological stress, burnout, biological aging, and postural strain. It highlights then the role of physical activity as a modifiable protective factor, extending beyond prevalence reporting to explore how structured lifestyle interventions can enhance resilience, reduce long-term occupational risks, and promote professional sustainability in dentistry, particularly within a post-pandemic context characterized by evolving clinical demands and heightened psychosocial pressures.
Integrative Models Beyond Ergonomics
Emerging literature supports the need for holistic approaches in occupational health for dental professionals that go beyond conventional ergonomic interventions3. Although musculoskeletal disorders (MSDs) remain a leading concern, their complex etiology, rooted in both physical and psychological demands, calls for comprehensive strategies that address the full spectrum of workplace challenges [37]. MSDs are not isolated phenomena but are interconnected with mental fatigue, sleep deprivation, and physiological strain induced by static postures and stress accumulation over time [37,39,48]. To respond effectively, a broader health framework must be integrated into clinical and educational settings [37,80,81]. These interventions should not be reactionary but embedded into daily routines, promoting anticipatory self-care rather than symptom-based responses. For instance, micro-movements between patient appointments, personalized ergonomic adjustments, and incorporation of lifestyle practices based on biological rhythms can significantly reduce physical wear and emotional fatigue [37,82].
Preventive Wellness in Education and Clinical Practice
To reduce long-term occupational strain, wellness must be embedded into dental education and clinical environments, not treated solely as an individual responsibility. Institutions should integrate structured wellness practices, including regular movement breaks, circadian-aligned work schedules, and body mechanics training, as part of routine operations [30,83]. Dental schools, in particular, have a critical role in modeling preventive behaviors. Embedding physical activity, stress management, and ergonomic literacy into the curriculum can promote both professional competence and personal well-being [29,84]. Studies show that students with better awareness of sleep hygiene and physical activity demonstrate improved mental resilience and reduced burnout, especially in high-stress academic settings [84]. Post-pandemic evidence further highlights the need for systemic support. Research indicates that COVID-19 has intensified psychological stress and physical health risks among dentists, reinforcing the urgency of building resilience through institutional wellness strategies [85,86,87]. Interventions that normalize self-care within professional culture, rather than treating it as optional, are more likely to be sustained and effective [88]. Additionally, innovative educational tools such as virtual and augmented reality may offer new ways to train healthcare students in ergonomics and wellness in resource-limited contexts [89]. Establishing wellness as a core competency cultivates healthier, more sustainable clinical careers and ultimately benefits the patients and communities these professionals serve.
Technology also plays an increasingly important role in supporting occupational health. Wearable devices and biosensors can monitor stress, posture, and physiological strain in real time, prompting immediate corrective behaviors that reduce the risk of long-term musculoskeletal damage or burnout [10,15,46]. These tools offer personalized feedback loops, helping dental professionals develop awareness of harmful patterns and adopt healthier routines [90]. Moreover, AI-driven platforms are beginning to enhance preventive care by analyzing biometric trends to provide tailored recommendations. Real-time data on fatigue, recovery needs, or stress reactivity can inform individualized schedules, suggest appropriate breaks, or trigger alerts for early intervention. Such technologies not only support proactive self-care but also contribute to broader organizational efforts to sustain a healthier dental workforce.[91].
Institutional and Governmental Responsibility for Health Promotion
Health-promoting behaviors should not be left solely to individual effort; instead, they require structural support from institutions and policymakers [30,83]. Dental clinics, universities, and professional organizations play a critical role in creating environments that facilitate well-being. Offering access to fitness facilities, organizing wellness workshops, and conducting regular ergonomic audits are practical ways to lower barriers to healthy behavior and embed self-care into daily professional routines [29,83,92]. These institutional strategies not only enhance individual health outcomes but also strengthen team cohesion, reduce absenteeism, and improve patient safety through better practitioner focus and reduced burnout risk [30]. Additionally, policies that designate time within working hours for recovery breaks, physical movement, or mental reset activities contribute to a shift in workplace culture, moving it toward sustainability rather than exhaustion [37,83].
Visible leadership support is crucial for embedding these changes. When management and academic leaders endorse and model these practices, a feedback loop of behavioral reinforcement is created, making health-conscious behaviors more socially and institutionally accepted [83,93]. Moreover, as Caron et al. (2023) emphasize, effective health promotion today must align with broader structural policies, bridging health protection, disease prevention, and behavioral interventions in a cohesive strategy [93]. In this context, dental institutions and health authorities must coordinate efforts to create environments where resilience is not an individual luxury but a shared institutional priority.
Cellular Mechanisms and Biological Aging
Emerging research highlights how physical activity directly influences the cellular and molecular pathways of aging, offering protective benefits particularly relevant to high-stress professions like dentistry. Regular exercise has been shown to reduce the accumulation of senescent cells, which are metabolically dysfunctional cells that contribute to tissue degeneration and chronic inflammation [94]. By curbing this accumulation, physical activity promotes healthier cellular turnover and slows down biological aging [95,96]. Also at the mitochondrial level, exercise enhances energy efficiency and biogenesis, reducing oxidative stress and preserving cellular function across multiple organ systems [97]. It also supports telomere maintenance, which is critical for genomic stability and is often compromised by chronic occupational stress [98]. These mechanisms extend healthspan and may contribute to greater professional longevity for dental practitioners, who are regularly exposed to physical and psychological strain.
Beyond structural benefits, physical activity induces favorable biochemical responses, including improved insulin sensitivity, reduced systemic cortisol levels, and more regulated inflammatory cytokines [96,97]. These changes contribute to improved immune regulation, cardiovascular function, and neurological resilience, offering protection against conditions such as cardiovascular disease, metabolic dysfunction, and neurodegeneration, all of which are known to be exacerbated by chronic stress and sedentary lifestyles [99]. Together, these cellular and systemic effects of regular movement demonstrate that physical activity is not only preventive but regenerative [100]. It works at the molecular level to counteract the biological wear and tear imposed by years of clinical practice, making it a powerful tool for supporting long-term well-being and functionality in dental professionals.
Cognitive and Emotional Benefits of Movement
Physical activity has been increasingly recognized as a powerful modulator of brain health, offering substantial cognitive and emotional benefits that extend far beyond traditional physical wellness, particularly vital for dental professionals working in high-pressure environments [101]. Chronic exposure to stressors, precision-based tasks, and psychosocial demands in dentistry can lead to cognitive fatigue, emotional exhaustion, and increased vulnerability to burnout [102]. However, recent neuroscientific evidence underlines the role of structured exercise in promoting neurocognitive resilience and emotional regulation [103]. Mechanistically, aerobic, resistance, and combined training modalities improve neuroplasticity, the brain's capacity to reorganize and form new neural connections in response to experience [104,105,106]. These adaptations are supported by increased levels of brain-derived neurotrophic factor (BDNF), vascular endothelial growth factor (VEGF), and insulin-like growth factor-1 (IGF-1), neuroprotective agents associated with enhanced memory, learning, and stress resilience [107]. In animal and human studies, these neurobiological changes correlate with improved executive function, working memory, attention control, and emotional stability [106].
Importantly, dentistry professionals, who often operate in cognitively demanding environments with limited downtime, stand to benefit significantly from these effects. Structured physical activity acts as a buffer against the detrimental effects of sustained cognitive load and psychosocial stress [108]. For example, even moderate-intensity aerobic training has been shown to reduce cortisol reactivity, normalize autonomic nervous system function, and improve prefrontal cortex regulation, which is essential for decision-making and impulse control under pressure [105]. Further, resistance training contributes to cognitive reserve, the brain’s resilience to neuropathological damage, by stimulating hippocampal volume preservation and reducing neuroinflammatory markers associated with aging and occupational burnout [104]. This is particularly relevant for older practitioners, whose prolonged exposure to occupational stress may accelerate cognitive aging. Taken together, this evidence reinforces that physical activity should not be viewed solely as a tool for musculoskeletal health, but rather as a cornerstone of mental clarity, emotional resilience, and sustainable professional functioning. Embedding movement into daily routines allows dental professionals to optimize cognitive performance, protect emotional well-being, and reduce the long-term impacts of occupational stress[110].
Professional Identity and Role Modeling
Self-care is not merely a personal health strategy, it is a powerful expression of professional identity and leadership within the dental field [111]. When dental professionals visibly prioritize wellness, through regular physical activity, stress management, or ergonomic practices, they embody the values of health, responsibility, and sustainability central to modern healthcare delivery [112]. This visible commitment positions them as role models, influencing not only colleagues and staff but also patients, who may internalize the message that maintaining health is an essential component of professional excellence [113]. According to Koh et al. (2023), role modeling plays a critical function in professional identity formation, particularly in clinical settings where norms and behaviors are learned through observation. In dentistry, this means that a practitioner who integrates wellness habits into daily routines, such as taking movement breaks, practicing good posture, or openly managing workload stress, may directly shape the behaviors and expectations of peers and trainees [114]. These actions can ripple outward, subtly shifting workplace culture toward one that values and supports occupational well-being. Moreover, such wellness-oriented behaviors signal proactive leadership, reinforcing resilience and solidarity within dental teams [5,51,91]. In high-stress clinical environments, professionals who demonstrate health-supportive practices can improve team morale, reduce burnout contagion, and strengthen the psychological safety of the workplace [115]. This aligns with emerging healthcare models that prioritize holistic and preventive care, both for patients and for providers themselves [116]. Ultimately, integrating personal wellness into professional conduct does more than protect individual health, it redefines what it means to lead in the dental profession. Through role modeling, dental practitioners can shape a culture of shared responsibility, where maintaining well-being is viewed not as optional, but as a fundamental aspect of competent and sustainable care delivery.
The Overlooked Role of Sleep and Recovery
While physical activity is widely acknowledged for its protective effects, sleep and recovery remain underrecognized yet critical components of occupational health, particularly in high-demand fields like dentistry [117,118,119]. Poor sleep quality not only diminishes cognitive performance and emotional regulation but also undermines immune function and increases systemic inflammation, effectively neutralizing the gains achieved through exercise or ergonomic interventions [120,121].
Dentists, who often operate under intense time pressures and demanding schedules, are particularly vulnerable to chronic sleep disruption and insufficient recovery. These factors have been strongly linked to burnout, increased risk of musculoskeletal disorders, and diminished clinical performance [122]. Notably, inadequate recovery has been shown to impair neuroplasticity, executive functioning, and metabolic regulation, all of which are essential to sustain professional efficacy and resilience [121]. As it is reported, sleep hygiene practices such as minimizing late-night screen exposure, aligning shift schedules with natural circadian rhythms, and scheduling restorative breaks throughout the workday can substantially improve recovery quality [123]. Evidence also points to the epigenetic benefits of high-quality sleep, including the upregulation of anti-aging genes such as S-Klotho, which supports systemic rejuvenation and protects against age-related decline [95,97]. In light of these findings, recovery should be regarded as a central pillar of occupational health, not merely a supplementary habit. Dental institutions and policymakers must ensure that sleep health is integrated into wellness programs, alongside physical activity and ergonomic strategies, to cultivate a truly sustainable model of professional care and longevity [124].
Contextualizing Interventions by Culture and Resources
Effective occupational health strategies in dentistry must be sensitive to local culture, resource constraints, and institutional norms [125]. Interventions that prove successful in one region may be ineffective, or even counterproductive, elsewhere if they clash with prevailing workplace expectations or sociocultural norms. For example, in some settings, incorporating physical activity during work hours may be perceived as unprofessional or unnecessary, despite strong evidence supporting its role in reducing musculoskeletal disorders and improving mental health [61,76,126]. Furthermore, economic disparities and infrastructure limitations directly influence what preventive measures are feasible [127]. In low-resource environments, access to ergonomic equipment or wellness facilities may be minimal, and time constraints can make structured physical activity difficult to implement [128]. Even when awareness exists, behavioral uptake is shaped by cultural beliefs about health, discipline, and professional identity [61,76,77,78,79,126].
To address these challenges, intervention models must be contextually adaptive rather than prescriptive. Hybrid approaches that combine low-cost ergonomic adjustments, culturally relevant wellness education, peer-led support groups, and scalable digital health tools can offer greater reach and sustainability [129]. As highlighted in recent digital health research, culturally tailored design, both linguistically and socially, enhances adoption and long-term adherence to wellness interventions in professional populations [130]. Future implementation efforts should prioritize co-creation with local stakeholders, flexibility in delivery formats, and respect for cultural practices [131]. Embedding occupational health promotion within regionally aligned frameworks increases the likelihood of program success, enhancing outcomes and fostering institutional shifts toward long-term, health-positive practices [61,62,126].
Long-Term Sustainability of Wellness Practices
As we report already, maintaining wellness behaviors over time requires more than individual motivation. It depends mainly on institutional structures that support continuity, accountability, and engagement [67,79,132]. Simply introducing physical activity or ergonomic strategies is insufficient without ongoing reinforcement mechanisms. Organizations that integrate wellness into performance metrics, provide incentives for health-positive behaviors, or appoint wellness champions are more likely to see lasting adoption across their teams [133].
Evidence from sustainability studies shows that gamification and structured engagement tools, such as leaderboards, recognition systems, and personalized feedback, can significantly increase long-term participation in workplace health programs [134]. Wellness initiatives that incorporate game-based elements and social reinforcement have been shown to maintain participant engagement and lead to sustained health improvements even two years after the intervention [135]. Sustainable health behavior change is most effective when delivered through multi-component systems that integrate environmental cues, organizational norms, and psychological support [136]. In this approach, wellness becomes a cultural shift embedded in daily practice rather than a standalone program [61,62,63,126].
Beyond the institutional level, intersectoral collaboration is essential too. Dental associations, public health agencies, and occupational safety bodies must work together to develop and standardize guidelines that support mental and physical well-being in dental workplaces [78,79]. Aligning wellness programs with broader health policy can help ensure system-wide adoption, enhance workforce retention, and reduce the economic burden of preventable conditions.
Lastly, long-term sustainability depends on the scientific evolution of wellness models [137,138]. Encouraging interdisciplinary research into dental ergonomics, stress physiology, cognitive workload, and behavioral economics can drive the development of more adaptive, evidence-based interventions that mirror the lived experience of dental professionals [78,79,139,140].
5. Conclusions
The dental profession faces escalating physical and psychological demands, particularly in the post-COVID-19 era, increasing the risk of musculoskeletal disorders, burnout, and accelerated biological aging. This review reports on the critical role of physical activity as a modifiable factor that enhances resilience, cognitive function, and cellular health while reducing occupational strain. Complementary strategies, including ergonomic education, sleep optimization, and institutional support, are essential for sustaining long-term well-being. Integrating digital tools, culturally adaptable interventions, and leadership-driven wellness initiatives can lead to healthier, more resilient dental workplaces. A shift toward holistic, preventive care is imperative for ensuring both practitioner health and quality patient outcomes.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Study Appraisal with Reliability Status.
Author Contributions
Conceptualization, M.A. and T.K.; methodology, M.A and T.K.; software, M.A.; validation, M.A and T.K.; formal analysis,M.A and T.K.; investigation, M.A and T.K.; resources, M.A and T.K.; data curation, M.A and T.KM.A and T.K.; writing—review and editing, M.A.; visualization, M.A.; supervision, M.A.; project administration, M.A. and T.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kelly D, Shorthouse F, Roffi V, Tack C. Exercise therapy and work-related musculoskeletal disorders in sedentary workers. Occup Med (Lond). 2018;68(4):262–72. [CrossRef]
- Large, A. Managing patient expectations. BDJ Team. 2020;7(9):31. [CrossRef]
- McDonald JM, Paganelli C. Exploration of Mental Readiness for Enhancing Dentistry in an Inter-Professional Climate. Int J Environ Res Public Health. 2021 Jul 1;18(13):7038. [CrossRef]
- Azimi S, Azimi S, Azami M. Occupational hazards/risks among dental staff in Afghanistan. 2024. [CrossRef]
- Antoniadou, M. Estimation of factors affecting burnout in Greek dentists before and during the COVID-19 pandemic. Dent J (Basel). 2022;10(6):108. [CrossRef]
- Antoniadou M, Mangoulia P, Myrianthefs P. Quality of life and wellbeing parameters of academic dental and nursing personnel vs. quality of services. Healthcare (Basel). 2023;11(20):2792. [CrossRef]
- Miron C, Colosi HA. Work stress, health behaviours and coping strategies of dentists from Cluj-Napoca, Romania. Int Dent J. 2018;68(3):152–61. [CrossRef]
- Arslan SS, Alemdaroğlu İ, Karaduman AA, Yilmaz ÖT. The effects of physical activity on sleep quality, job satisfaction, and quality of life in office workers. Work. 2019;63(1):3–7. [CrossRef]
- Kurtović A, Talapko J, Bekić S, Škrlec I. The relationship between sleep, chronotype, and dental caries: A narrative review. Clocks Sleep. 2023;5(2):295–312. [CrossRef]
- Gandolfi MG, Zamparini F, Spinelli A, Risi A, Prati C. Musculoskeletal disorders among Italian dentists and dental hygienists. Int J Environ Res Public Health. 2021;18(5):2705. [CrossRef]
- Stults-Kolehmainen MA, Sinha R. The effects of stress on physical activity and exercise. Sports Med. 2014;44(1):81–121. [CrossRef]
- Serra MVGB, Camargo PR, Zaia JE, Tonello MGM, Quemelo PRV. Effects of physical exercise on musculoskeletal disorders, stress and quality of life in workers. Int J Occup Saf Ergon. 2018;24(1):62–7. [CrossRef]
- Martín-Rodríguez A, Gostian-Ropotin LA, Beltrán-Velasco AI, Belando-Pedreño N, Simón JA, López-Mora C, et al. Sporting mind: The interplay of physical activity and psychological health. Sports (Basel). 2024;12(1):37. [CrossRef]
- Basso JC, Suzuki WA. The effects of acute exercise on mood, cognition, neurophysiology, and neurochemical pathways: A review. Brain Plast. 2017;2(2):127–52. [CrossRef]
- Al Nawwar MA, Alraddadi MI, Algethmi RA, Salem GA, Salem MA, Alharbi AA. The Effect of Physical Activity on Sleep Quality and Sleep Disorder: A Systematic Review. Cureus. 2023 Aug 16;15(8):e43595. [CrossRef]
- Dhuli K, Naureen Z, Medori MC, Fioretti F, Caruso P, Perrone MA, et al. Physical activity for health. J Prev Med Hyg. 2022;63(2 Suppl 3):E150–9. [CrossRef]
- Militello R, Luti S, Gamberi T, Pellegrino A, Modesti A, Modesti PA. Physical Activity and Oxidative Stress in Aging. Antioxidants (Basel). 2024 ;13(5):557. 1 May. [CrossRef]
- Yang, J.; Luo, J.; Tian, X.; Zhao, Y.; Li, Y.; Wu, X. Progress in Understanding Oxidative Stress, Aging, and Aging-Related Diseases. Antioxidants 2024, 13, 394. [Google Scholar] [CrossRef] [PubMed]
- Burini RC, Anderson E, Durstine JL, Carson JA. Inflammation, physical activity, and chronic disease: An evolutionary perspective. Sports Med Health Sci. 2020 Mar 26;2(1):1-6. [CrossRef]
- Núñez-Cortés, R.; Salazar-Méndez, J.; Nijs, J. Physical Activity as a Central Pillar of Lifestyle Modification in the Management of Chronic Musculoskeletal Pain: A Narrative Review. J. Funct. Morphol. Kinesiol. 2025, 10, 183. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, P. , Seing, I., Ericsson, C. et al. Characteristics of successful changes in health care organizations: an interview study with physicians, registered nurses and assistant nurses. BMC Health Serv Res 20, 147 (2020). [CrossRef]
- Asaduzzaman, M.; Ara, R.; Afrin, S.; Meiring, J.E.; Saif-Ur-Rahman, K.M. Planetary Health Education and Capacity Building for Healthcare Professionals in a Global Context: Current Opportunities, Gaps and Future Directions. Int. J. Environ. Res. Public Health 2022, 19, 11786. [Google Scholar] [CrossRef] [PubMed]
- Dahlgren A, Tucker P, Epstein M, Gustavsson P, Söderström M. Randomised control trial of a proactive intervention supporting recovery in relation to stress and irregular work hours: effects on sleep, burn-out, fatigue and somatic symptoms. Occup Environ Med. 2022 Jul;79(7):460-468. [CrossRef]
- Sakzewski L, Naser-ud-Din S. Work-related musculoskeletal disorders in dentists and orthodontists: A review of the literature. Work. 2014;48(1):37–45. [CrossRef]
- Țâncu AMC, Didilescu AC, Pantea M, Sfeatcu R, Imre M. Aspects regarding sustainability among private dental practitioners from Bucharest, Romania: A pilot study. Healthcare (Basel). 2023;11(9):1326. [CrossRef]
- Mekhemar M, Attia S, Dörfer C, Conrad J. The psychological impact of the COVID-19 pandemic on dentists in Germany. J Clin Med. 2021;10(5):1008. [CrossRef]
- Vered Y, Zaken Y, Ovadia-Gonen H, Mann J, Zini A. Professional burnout: Its relevance and implications for the general dental community. Quintessence Int. 2014;45(1):87–90. [CrossRef]
- Plessas A, Paisi M, Bryce M, Burns L, O'Brien T, Hanoch Y, Witton R. Mental health and wellbeing interventions in the dental sector: A systematic review. Evid Based Dent. 2022:1–8. [CrossRef]
- Almeida MB, Póvoa R, Tavares D, Alves PM, Oliveira R. Prevalence of musculoskeletal disorders among dental students: A systematic review and meta-analysis. Heliyon. 2023 Sep 11;9(10):e19956. [CrossRef]
- Carapeto PV, Aguayo-Mazzucato C. Effects of exercise on cellular and tissue aging. Aging (Albany NY). 2021;13(10):14522–14543. [CrossRef]
- Scott J, Etain B, Miklowitz D, et al. A systematic review and meta-analysis of sleep and circadian rhythms disturbances in individuals at high-risk of developing or with early onset of bipolar disorders. Neurosci Biobehav Rev. 2022;135:104585. [CrossRef]
- McDonald JM, Paganelli C. Exploration of Mental Readiness for Enhancing Dentistry in an Inter-Professional Climate. Int J Environ Res Public Health. 2021 Jul 1;18(13):7038. [CrossRef]
- Siddiqui FM, Jabeen S, Alwazzan A, Vacca S, Dalal L, Al-Haddad B, Jaber A, Ballout FF, Abou Zeid HK, Haydamous J, El Hajj Chehade R, Kalmatov R. Integration of Augmented Reality, Virtual Reality, and Extended Reality in Healthcare and Medical Education: A Glimpse into the Emerging Horizon in LMICs-A Systematic Review. J Med Educ Curric Dev. 2025 ;12:23821205251342315. 29 May. [CrossRef]
- Schiavo, JH. PROSPERO: An international register of systematic review protocols. Med Ref Serv Q. 2019;38(2):171–180. [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY: IBM Corp; 2022. Available from: https://www.ibm.com/products/spss-statistics.
- Asaduzzaman M, Arbia L, Tasdika T, Mondol A, Ray P, Hossain T, Hossain M. Assessing the awareness on occupational health hazards among dentists of different private dental clinics in Dhaka, Bangladesh. J Biol Agric Healthc. 2022;12(18):xx–xx. [CrossRef]
- Al-Huthaifi BH, Al Moaleem MM, Alwadai GS, Abou Nassar J, Sahli AAA, Khawaji AH, et al. High prevalence of musculoskeletal disorders among dental professionals: A study on ergonomics and workload in Yemen. Med Sci Monit. 2023;29:e942294. [CrossRef]
- Eminoğlu DÖ, Kaşali K, Şeran B, Burmaoğlu GE, Aydin T, Bircan HB. An assessment of musculoskeletal disorders and physical activity levels in dentists: A cross-sectional study. Work. 2025 Jan;80(1):396-406. [CrossRef]
- Al-Emara Z, Karaharju-Suvanto T, Furu P, Furu H. Musculoskeletal disorders and work ability among dentists and dental students in Finland. Work. 2024;78(1):73–81. [CrossRef]
- Matur Z, Zengin T, Bolu NE, Oge AE. Prevalence of carpal tunnel syndrome symptoms among young dentists. Cureus. 2023;15(8):e43358. [CrossRef]
- Macrì M, Galindo Flores NV, Stefanelli R, Pegreffi F, Festa F. Interpreting the prevalence of musculoskeletal pain impacting Italian and Peruvian dentists likewise: A cross-sectional study. Front Public Health. 2023;11:1090683. [CrossRef]
- Javed H, Tariq H, Lodhi A, Iftikhar R, Khanzada S, Arshad K, et al. Prevalence of carpel tunnel syndrome among dentists: A cross-sectional study. J Health Rehabil Res. 2023;3:384–388. [CrossRef]
- Chenna D, Pentapati KC, Kumar M, Madi M, Siddiq H. Prevalence of musculoskeletal disorders among dental healthcare providers: A systematic review and meta-analysis. F1000Res. 2022 Sep 16;11:1062. [CrossRef]
- Daou M, Jaoude SA, Khazaka S. Musculoskeletal disorders in dentists: A preprint. Res Square. 2023. [CrossRef]
- AlDhaen, E. Awareness of occupational health hazards and occupational stress among dental care professionals: Evidence from the GCC region. Front Public Health. 2022;10:922748. [CrossRef]
- Zhou Y, Zhou W, Aisaiti A, Wang B, Zhang J, Svensson P, Wang K. Dentists have a high occupational risk of neck disorders with impact on somatosensory function and neck mobility. J Occup Health. 2021;63(1):e12269. [CrossRef]
- Alnaser MZ, Almaqsied AM, Alshatti SA. Risk factors for work-related musculoskeletal disorders of dentists in Kuwait and the impact on health and economic status. Work. 2021;68(1):213–221. [CrossRef]
- Berdouses EB, Sifakaki M, Katsantoni A, et al. Work-related musculoskeletal disorders among Greek dentists: A nationwide survey. Dent Res Oral Health. 2020;4:169–182. [CrossRef]
- Savić Pavičin I, Lovrić Ž, Zymber Çeshko A, Vodanović M. Occupational injuries among dentists in Croatia. Acta Stomatol Croat. 2020;54(1):51–59. [CrossRef]
- Alabdulwahab S, Kachanathu S, Alaulami A. Health-related quality of life among dentists in Middle-East countries: A cross-sectional study. J Indian Assoc Public Health Dent. 2020;18:168. [CrossRef]
- Harris ML, Sentner SM, Doucette HJ, Brillant MGS. Musculoskeletal disorders among dental hygienists in Canada. Can J Dent Hyg. 2020;54(2):61–67.
- Ahmad W, Taggart F, Shafique MS, et al. Diet, exercise and mental-wellbeing of healthcare professionals in Pakistan. PeerJ. 2015;3:e1250. [CrossRef]
- Memarpour M, Badakhsh S, Khosroshahi SS, Vossoughi M. Work-related musculoskeletal disorders among Iranian dentists. Work. 2013;45(4):465–474. [CrossRef]
- Hashim R, Al-Ali K. Health of dentists in United Arab Emirates. Int Dent J. 2013;63(1):26–29. [CrossRef]
- Singh A, Purohit B. Physical activity, sedentary lifestyle, and obesity among Indian dental professionals. J Phys Act Health. 2012;9(4):563–570. [CrossRef]
- Ellapen TJ, Narsigan S, van Herdeen HJ, Pillay K, Rugbeer N. Impact of poor dental ergonomical practice. SADJ. 2011;66(6):272–277.
- Sharma P, Golchha V. Awareness among Indian dentists regarding the role of physical activity in prevention of work-related musculoskeletal disorders. Indian J Dent Res. 2011;22(3):381–384. [CrossRef]
- Kierklo A, Kobus A, Jaworska M, Botuliński B. Work-related musculoskeletal disorders among dentists: A questionnaire survey. Ann Agric Environ Med. 2011;18(1):79–84.
- Lietz J, Kozak A, Nienhaus A. Prevalence and occupational risk factors of musculoskeletal diseases and pain among dental professionals in Western countries: A systematic literature review and meta-analysis. PLoS One. 2018;13(12):e0208628. [CrossRef]
- Alhusain FA, Almohrij M, Althukeir F, et al. Prevalence of carpal tunnel syndrome symptoms among dentists working in Riyadh. Ann Saudi Med. 2019;39(2):104–111. [CrossRef]
- Mehta A, Gupta M, Upadhyaya N. Status of occupational hazards and their prevention among dental professionals in Chandigarh, India: A comprehensive questionnaire survey. Dent Res J (Isfahan). 2013;10(4):446–451.
- Bozkurt S, Demirsoy N, Günendi Z. Risk factors associated with work-related musculoskeletal disorders in dentistry. Clin Investig Med. 2016;39(6):27527.
- Feng B, Liang Q, Wang Y, Andersen LL, Szeto G. Prevalence of work-related musculoskeletal symptoms of the neck and upper extremity among dentists in China. BMJ Open. 2014;4(12):e006451. [CrossRef]
- Meyerson J, Gelkopf M, Eli I, Uziel N. Burnout and professional quality of life among Israeli dentists: The role of sensory processing sensitivity. Int Dent J. 2020;70(1):29–37. [CrossRef]
- Meyerson J, Gelkopf M, Eli I, Uziel N. Stress coping strategies, burnout, secondary traumatic stress, and compassion satisfaction amongst Israeli dentists: A cross-sectional study. Int Dent J. 2022;72(4):476–483. [CrossRef]
- Singh P, Aulak DS, Mangat SS, Aulak MS. Systematic review: Factors contributing to burnout in dentistry. Occup Med (Lond). 2016;66(1):27–31. [CrossRef]
- Szalai E, Hallgató J, Kunovszki P, Tóth Z. Burnout among Hungarian dentists. Orv Hetil. 2021;162(11):419–424. [CrossRef]
- White, R.L. , Vella, S., Biddle, S. et al. Physical activity and mental health: a systematic review and best-evidence synthesis of mediation and moderation studies. Int J Behav Nutr Phys Act 21, 134 (2024). [CrossRef]
- Horowitz AM, Fan X, Bieri G, et al. Blood factors transfer beneficial effects of exercise on neurogenesis and cognition to the aged brain. Science. 2020;369(6500):167–173. [CrossRef]
- Reddy V, Bennadi D. Occupational hazards among dentists: A descriptive study. J Oral Hyg Health. 2015;3. [CrossRef]
- Kızılcı E, Kızılay F, Mahyaddinova T, Muhtaroğlu S, Kolçakoğlu K. Stress levels of a group of dentists while providing dental care under clinical, deep sedation, and general anesthesia. Clin Oral Investig. 2023;27(7):3601–3609. [CrossRef]
- Neumann, R.J. , Ahrens, K.F., Kollmann, B. et al. The impact of physical fitness on resilience to modern life stress and the mediating role of general self-efficacy. Eur Arch Psychiatry Clin Neurosci 272, 679–692 (2022). [CrossRef]
- Mulimani P, Hoe VC, Hayes MJ, et al. Ergonomic interventions for preventing musculoskeletal disorders in dental care practitioners. Cochrane Database Syst Rev. 2018;2018(10):CD011261. [CrossRef]
- Papagerakis S, Zheng L, Schnell S, et al. The circadian clock in oral health and diseases. J Dent Res. 2014;93(1):27–35. [CrossRef]
- Fernandez de Grado G, Denni J, Musset AM, Offner D. Back pain prevalence, intensity and associated factors in French dentists: A national study among 1004 professionals. Eur Spine J. 2019;28(11):2510–2516. [CrossRef]
- Le VNT, Dang MH, Kim JG, et al. Mental health in dentistry: A global perspective. Int Dent J. 2020. [CrossRef]
- Moro JDS, Soares JP, Massignan C, et al. Burnout syndrome among dentists: A systematic review and meta-analysis. J Evid Based Dent Pract. 2022;22(3):101724. [CrossRef]
- Scheepers RA, Emke H, Epstein RM, Lombarts KMJMH. The impact of mindfulness-based interventions on doctors' well-being and performance: A systematic review. Med Educ. 2020;54(2):138–149. [CrossRef]
- Lee CY, Wu JH, Du JK. Work stress and occupational burnout among dental staff in a medical center. J Dent Sci. 2019;14(3):295–301. [CrossRef]
- World Health Organization. Global Oral Health Status Report: Towards Universal Health Coverage for Oral Health by 2030. Geneva: WHO; 2022. Available from: https://www.who.int/publications/i/item/9789240061484.
- Alyousefy MA, Shaiban AS, Alaajam WH, et al. Questionnaire-based study on the prevalence, awareness, and preventive measures of occupational hazards among dental professionals. Med Sci Monit. 2022;28:e938084. [CrossRef]
- Chen XK, Yi ZN, Wong GT, et al. Is exercise a senolytic medicine? A systematic review. Aging Cell. 2021;20(1):e13294. [CrossRef]
- Zábó V, Lehoczki A, Fekete M, Szappanos Á, Varga P, Moizs M, Giovannetti G, Loscalzo Y, Giannini M, Polidori MC, Busse B, Kellermayer M, Ádány R, Purebl G, Ungvari Z. The role of purpose in life in healthy aging: implications for the Semmelweis Study and the Semmelweis-EUniWell Workplace Health Promotion Model Program. Geroscience. 2025 Jun;47(3):2817-2833. [CrossRef]
- Saintila J, Javier-Aliaga D, Del Carmen Gálvez-Díaz N, Barreto-Espinoza LA, Buenaño-Cervera NA, Calizaya-Milla YE. Association of sleep hygiene knowledge and physical activity with sleep quality in nursing and medical students: a cross-sectional study. Front Sports Act Living. 2025 Mar 20;7:1453404. [CrossRef]
- Praditpapha A, Mattheos N, Pisarnturakit PP, Pimkhaokham A, Subbalekha K. Dentists' Stress During the COVID-19 Pandemic: A Repeated Cross-Sectional Study. Int Dent J. 2023 Oct 27;74(2):294–302. [CrossRef]
- Mucharraz y Cano, Yvette, Dávila-Ruiz, Diana, & Cuilty-Esquivel, Karla. (2025). Burnout resilience in the face of the COVID-19 pandemic. Tec Empresarial, 19(1), 36-50. [CrossRef]
- Negucioiu, M.; Buduru, S.; Ghiz, S.; Kui, A.; Șoicu, S.; Buduru, R.; Sava, S. Prevalence and Management of Burnout Among Dental Professionals Before, During, and After the COVID-19 Pandemic: A Systematic Review. Healthcare 2024, 12, 2366. [Google Scholar] [CrossRef] [PubMed]
- Adsett JA, Mudge AM. Interventions to Promote Physical Activity and Reduce Functional Decline in Medical Inpatients: An Umbrella Review. J Am Med Dir Assoc. 2024 Aug;25(8):105052. [CrossRef]
- Gallagher J, Colonio-Salazar F, White S. Supporting dentists' health and wellbeing: A qualitative study of coping strategies in 'normal times'. Br Dent J. 2021. [CrossRef]
- Sezer, B. , Sıddıkoğlu, D. Relationship between work-related musculoskeletal symptoms and burnout symptoms among preclinical and clinical dental students: a cross-sectional study. BMC Musculoskelet Disord 26, 561 (2025). [CrossRef]
- Antoniadou, M. Leadership and Managerial Skills in Dentistry: Characteristics and Challenges Based on a Preliminary Case Study. Dent. J. 2022, 10, 146. [Google Scholar] [CrossRef] [PubMed]
- Karami M, Drouri S, Al Jalil Z, Ettaki S, Jabri M. Musculoskeletal disorders and stress among Moroccan dentists: A cross-sectional study. Integr J Med Sci. 2023. [CrossRef]
- Caron RM, Noel K, Reed RN, Sibel J, Smith HJ. Health Promotion, Health Protection, and Disease Prevention: Challenges and Opportunities in a Dynamic Landscape. AJPM Focus. 2023 Nov 8;3(1):100167. [CrossRef]
- Lu X, Chen Y, Shi Y, Su X, Chen P, Wu D, Shi H. Exercise and exerkines: Mechanisms and roles in anti-aging and disease prevention. Experimental Gerontology 2025, 200, 112685. [CrossRef]
- Zhang X, Englund DA, Aversa Z, Jachim SK, White TA, LeBrasseur NK. Exercise Counters the Age-Related Accumulation of Senescent Cells. Exerc Sport Sci Rev. 2022 Oct 1;50(4):213-221. [CrossRef]
- Guo, J. , Huang, X., Dou, L. et al. Aging and aging-related diseases: from molecular mechanisms to interventions and treatments. Sig Transduct Target Ther 7, 391 (2022). [CrossRef]
- Li, Y. , Tian, X., Luo, J. et al. Molecular mechanisms of aging and anti-aging strategies. Cell Commun Signal 22, 285 (2024). [CrossRef]
- Gao G, Xie Z, Huang H. Mitochondrial function maintenance and mitochondrial training in ageing and related diseases. Journal of Holistic Integrative Pharmacy, 2025, 6, 159–174. [CrossRef]
- Małkowska, P. Positive Effects of Physical Activity on Insulin Signaling. Curr Issues Mol Biol. 2024 ;46(6):5467-5487. 30 May. [CrossRef]
- Almuraikhy S, Sellami M, Al-Amri HS, Domling A, Althani AA, Elrayess MA. Impact of Moderate Physical Activity on Inflammatory Markers and Telomere Length in Sedentary and Moderately Active Individuals with Varied Insulin Sensitivity. J Inflamm Res. 2023 Nov 20;16:5427-5438. [CrossRef]
- Erickson KI, Hillman C, Stillman CM, Ballard RM, Bloodgood B, Conroy DE, Macko R, Marquez DX, Petruzzello SJ, Powell KE; FOR 2018 PHYSICAL ACTIVITY GUIDELINES ADVISORY COMMITTEE*. Physical Activity, Cognition, and Brain Outcomes: A Review of the 2018 Physical Activity Guidelines. Med Sci Sports Exerc. 2019 Jun;51(6):1242-1251. [CrossRef]
- Crielaard L, Nicolaou M, Sawyer A, Quax R, Stronks K. Understanding the impact of exposure to adverse socioeconomic conditions on chronic stress from a complexity science perspective. BMC Med. 2021 Oct 12;19(1):242. [CrossRef]
- Belcher BR, Zink J, Azad A, Campbell CE, Chakravartti SP, Herting MM. The Roles of Physical Activity, Exercise, and Fitness in Promoting Resilience During Adolescence: Effects on Mental Well-Being and Brain Development. Biol Psychiatry Cogn Neurosci Neuroimaging. 2021 Feb;6(2):225-237. [CrossRef]
- Dhahbi, W. , Briki, W., Heissel, A. et al. Physical Activity to Counter Age-Related Cognitive Decline: Benefits of Aerobic, Resistance, and Combined Training—A Narrative Review. Sports Med - Open 11, 56 (2025). [CrossRef]
- Ben Ezzdine L, Dhahbi W, Dergaa I, Ceylan Hİ, Guelmami N, Ben Saad H, Chamari K, Stefanica V, El Omri A. Physical activity and neuroplasticity in neurodegenerative disorders: a comprehensive review of exercise interventions, cognitive training, and AI applications. Front Neurosci. 2025 Feb 28;19:1502417. [CrossRef]
- de Sousa Fernandes MS, Ordônio TF, Santos GCJ, Santos LER, Calazans CT, Gomes DA, Santos TM. Effects of Physical Exercise on Neuroplasticity and Brain Function: A Systematic Review in Human and Animal Studies. Neural Plast. 2020 Dec 14;2020:8856621. [CrossRef]
- Tari A, Norevik C, Scrimgeour, Kobro-Flatmoen A, Storm-Mathisen J, Bergersen L, Wrann CD, Selbæk G, Kivipelto M, MoreiraJBN, Wisløff U. Are the neuroprotective effects of exercise training systemically mediated?Progress in Cardiovascular Diseases 2019, 62, 94–101. [CrossRef]
- Pontes CC, Stanley K, Molayem S. Understanding the Dental Profession's Stress Burden: Prevalence and Implications. Compend Contin Educ Dent. 2024 May;45(5):236-241; quiz 242.
- Gkintoni, E.; Vassilopoulos, S.P.; Nikolaou, G.; Boutsinas, B. Digital and AI-Enhanced Cognitive Behavioral Therapy for Insomnia: Neurocognitive Mechanisms and Clinical Outcomes. J. Clin. Med. 2025, 14, 2265. [Google Scholar] [CrossRef] [PubMed]
- Kim N, Ka S, Park J. Effects of exercise timing and intensity on physiological circadian rhythm and sleep quality: a systematic review. Phys Act Nutr. 2023 Sep;27(3):52-63. [CrossRef]
- Woo D, Shafiee R, Manton JW, Huang J, Fa BA. Self-care and wellness in dentistry—a mini review. J Oral Maxillofac Anesth 2024;3:5.
- Harris M, Eaton K. Exploring dental professionals' perceptions of resilience to dental environment stress: a qualitative study. Br Dent J. 2025 Mar;238(6):395-402. [CrossRef]
- Koh EYH, Koh KK, Renganathan Y, Krishna L. Role modelling in professional identity formation: a systematic scoping review. BMC Med Educ. 2023 Mar 29;23(1):194. [CrossRef]
- McColl E, Paisi M, Plessas A, Ellwood F, Witton R. An individual-level approach to stress management in dentistry. BDJ Team. 2022;9(10):13–6. [CrossRef]
- de Lisser R, Dietrich MS, Spetz J, Ramanujam R, Lauderdale J, Stolldorf DP. Psychological safety is associated with better work environment and lower levels of clinician burnout. Health Aff Sch. 2024 Jul 17;2(7):qxae091. [CrossRef]
- Teisberg E, Wallace S, O'Hara S. Defining and Implementing Value-Based Health Care: A Strategic Framework. Acad Med. 2020 May;95(5):682-685. [CrossRef]
- Hallman DM, Birk Jørgensen M, Holtermann A. On the health paradox of occupational and leisure-time physical activity using objective measurements: Effects on autonomic imbalance. PLoS One. 2017 ;12(5):e0177042. 4 May. [CrossRef]
- Seaton CL, Bottorff JL, Soprovich AL, et al. Men’s Physical Activity and Sleep Following a Workplace Health Intervention: Findings from the POWERPLAY STEP Up challenge. American Journal of Men’s Health. 2021;15(1). [CrossRef]
- Cillekens B, Huysmans MA, Holtermann A, van Mechelen W, Straker L, Krause N, van der Beek AJ, Coenen P. Physical activity at work may not be health enhancing. A systematic review with meta-analysis on the association between occupational physical activity and cardiovascular disease mortality covering 23 studies with 655 892 participants. Scand J Work Environ Health. 2022 Mar 1;48(2):86-98. [CrossRef]
- Sahebi A, Abdi K, Moayedi S, Torres M, Golitaleb M. The prevalence of insomnia among health care workers amid the COVID-19 pandemic: An umbrella review of meta-analyses. J Psychosom Res. 2021 Oct;149:110597. [CrossRef]
- Karihtala T, Puttonen S, Valtonen AM, Kautiainen H, Hopsu L, Heinonen A. Role of physical activity in the relationship between recovery from work and insomnia among early childhood education and care professionals: a cross-sectional study. BMJ Open. 2024 Mar 19;14(3):e079746. [CrossRef]
- Marklund S, Mienna CS, Wahlström J, Englund E, Wiesinger B. Work ability and productivity among dentists: associations with musculoskeletal pain, stress, and sleep. Int Arch Occup Environ Health. 2020 Feb;93(2):271-278. [CrossRef]
- Desai D, Momin A, Hirpara P, Jha H, Thaker R, Patel J. Exploring the Role of Circadian Rhythms in Sleep and Recovery: A Review Article. Cureus. 2024 Jun 3;16(6):e61568. [CrossRef]
- Holtermann A, Mathiassen SE, Straker L. Promoting health and physical capacity during productive work: the Goldilocks Principle. Scand J Work Environ Health. 2019 Jan 1;45(1):90-97. [CrossRef]
- Cipta DA, Andoko D, Theja A, Utama AVE, Hendrik H, William DG, Reina N, Handoko MT, Lumbuun N. Culturally sensitive patient-centered healthcare: a focus on health behavior modification in low and middle-income nations-insights from Indonesia. Front Med (Lausanne). 2024 Apr 12;11:1353037. [CrossRef]
- Garbin AJÍ, Soares GB, Arcieri RM, Garbin CAS, Siqueira CE. Musculoskeletal disorders and perception of working conditions: A survey of Brazilian dentists in São Paulo. Int J Occup Med Environ Health. 2017;30(3):367–377. [CrossRef]
- Manthey, NA. The role of community-led social infrastructure in disadvantaged areas. Cities 2024, 147, 104831. [Google Scholar] [CrossRef]
- Safi A, Cole M, Kelly AL, Zariwala MG, Walker NC. Workplace Physical Activity Barriers and Facilitators: A Qualitative Study Based on Employees Physical Activity Levels. Int J Environ Res Public Health. 2022 Aug 1;19(15):9442. [CrossRef]
- Tang T, Nelson M, Steele Gray C. Adapt to evaluate: Lessons from a multi-site trial of a digitally enabled care transition intervention. Healthc Manage Forum. 2025 Jun 23:8404704251351459. [CrossRef]
- Naderbagi A, Loblay V, Zahed IUM, Ekambareshwar M, Poulsen A, Song YJC, Ospina-Pinillos L, Krausz M, Mamdouh Kamel M, Hickie IB, LaMonica HM. Cultural and Contextual Adaptation of Digital Health Interventions: Narrative Review. J Med Internet Res. 2024 Jul 9;26:e55130. [CrossRef]
- Agnello, D.M. , Anand-Kumar, V., An, Q. et al. Co-creation methods for public health research — characteristics, benefits, and challenges: a Health CASCADE scoping review. BMC Med Res Methodol 25, 60 (2025). [CrossRef]
- Ghosh, T. Occupational health and hazards among health care workers. Int J Occup Saf Health. 2013;3. [CrossRef]
- Wieneke KC, Egginton JS, Jenkins SM, Kruse GC, Lopez-Jimenez F, Mungo MM, Riley BA, Limburg PJ. Well-Being Champion Impact on Employee Engagement, Staff Satisfaction, and Employee Well-Being. Mayo Clin Proc Innov Qual Outcomes. 2019 ;3(2):106-115. 27 May. [CrossRef]
- Elsawah, W. Exploring the effectiveness of gamification in adult education: A learner-centric qualitative case study in a dubai training context. International Journal of Educational Research Open, 2025, 9, 100465. [Google Scholar] [CrossRef]
- Lowensteyn I, Berberian V, Berger C, Da Costa D, Joseph L, Grover SA. The Sustainability of a Workplace Wellness Program That Incorporates Gamification Principles: Participant Engagement and Health Benefits After 2 Years. Am J Health Promot. 2019 Jul;33(6):850-858. [CrossRef]
- Matthews JA, Matthews S, Faries MD, Wolever RQ. Supporting Sustainable Health Behavior Change: The Whole is Greater Than the Sum of Its Parts. Mayo Clin Proc Innov Qual Outcomes. 2024 ;8(3):263-275. 18 May. [CrossRef]
- AlNujaidi HY, Al-Rayes SA, Alumran A. The Evolution of Wellness Models: Implications for Women's Health and Well-Being. Int J Womens Health. 2025 Mar 4;17:597-613. [CrossRef]
- Kallis G, Hickel J, Daniel W O’Neill DW, Jackson T, Victor AP, Raworth K, Schor JB, Steinberger JK, Ürge-Vorsatz D. Post-growth: the science of wellbeing within planetary boundaries. The Lancet Planetary Health 2025, 9, e62–e78. [CrossRef]
- Huttunen M, Kämppi A, Soudunsaari A, et al. The association between dental caries and physical activity, physical fitness, and background factors among Finnish male conscripts. Odontology. 2023;111(1):192–200. [CrossRef]
- Calvo JM, Kwatra J, Yansane A, et al. Burnout and work engagement among US dentists. J Patient Saf. 2021;17(5):398–404. [CrossRef]
Figure 1.
Flowchart for the results of the search strategy.
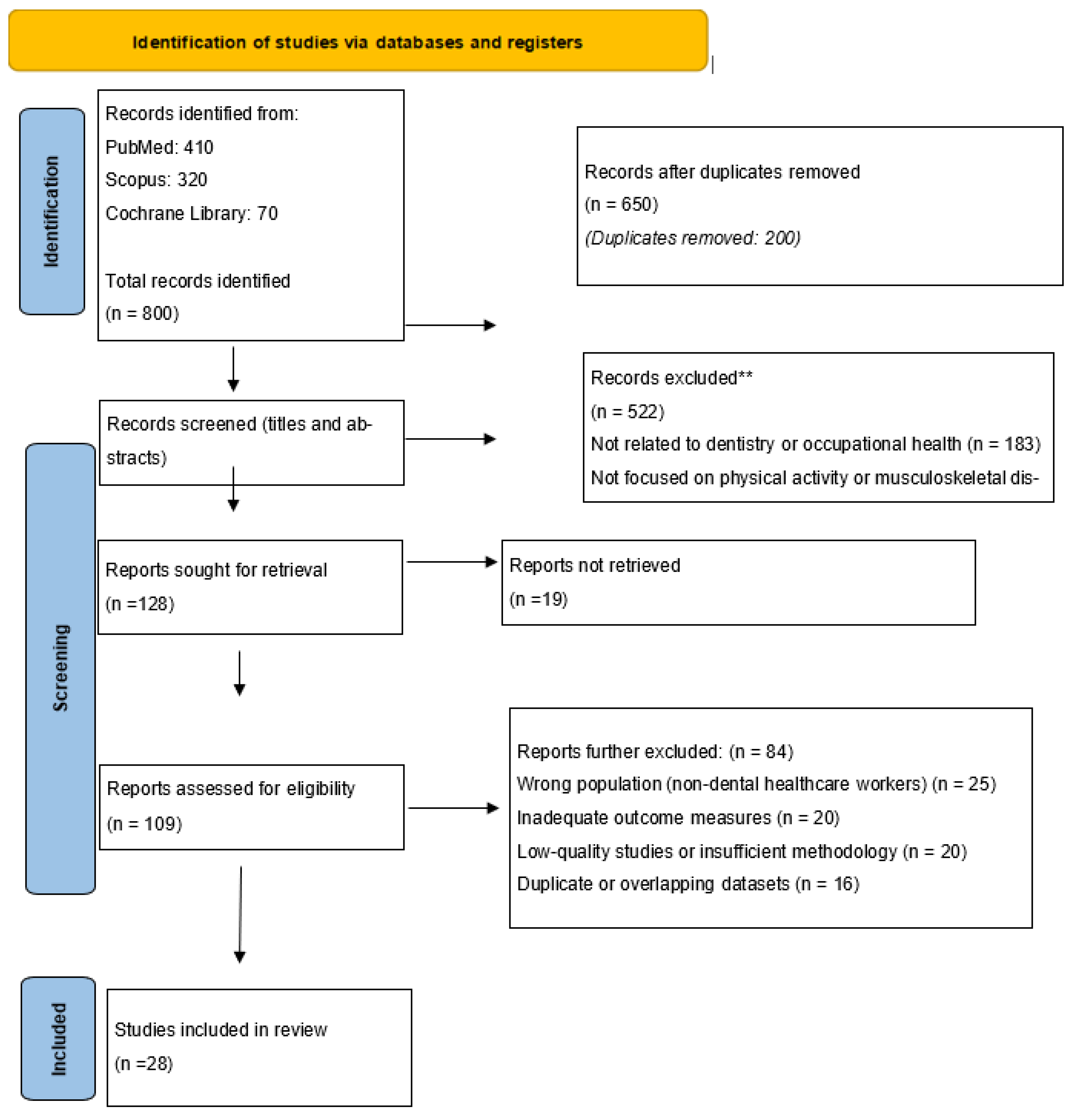
Figure 2.
Trend chart showing the articles published in the database PubMed during the period 2000–2024 with the keyword “physical activity on dentists ” in the title and/or abstract.
Figure 2.
Trend chart showing the articles published in the database PubMed during the period 2000–2024 with the keyword “physical activity on dentists ” in the title and/or abstract.
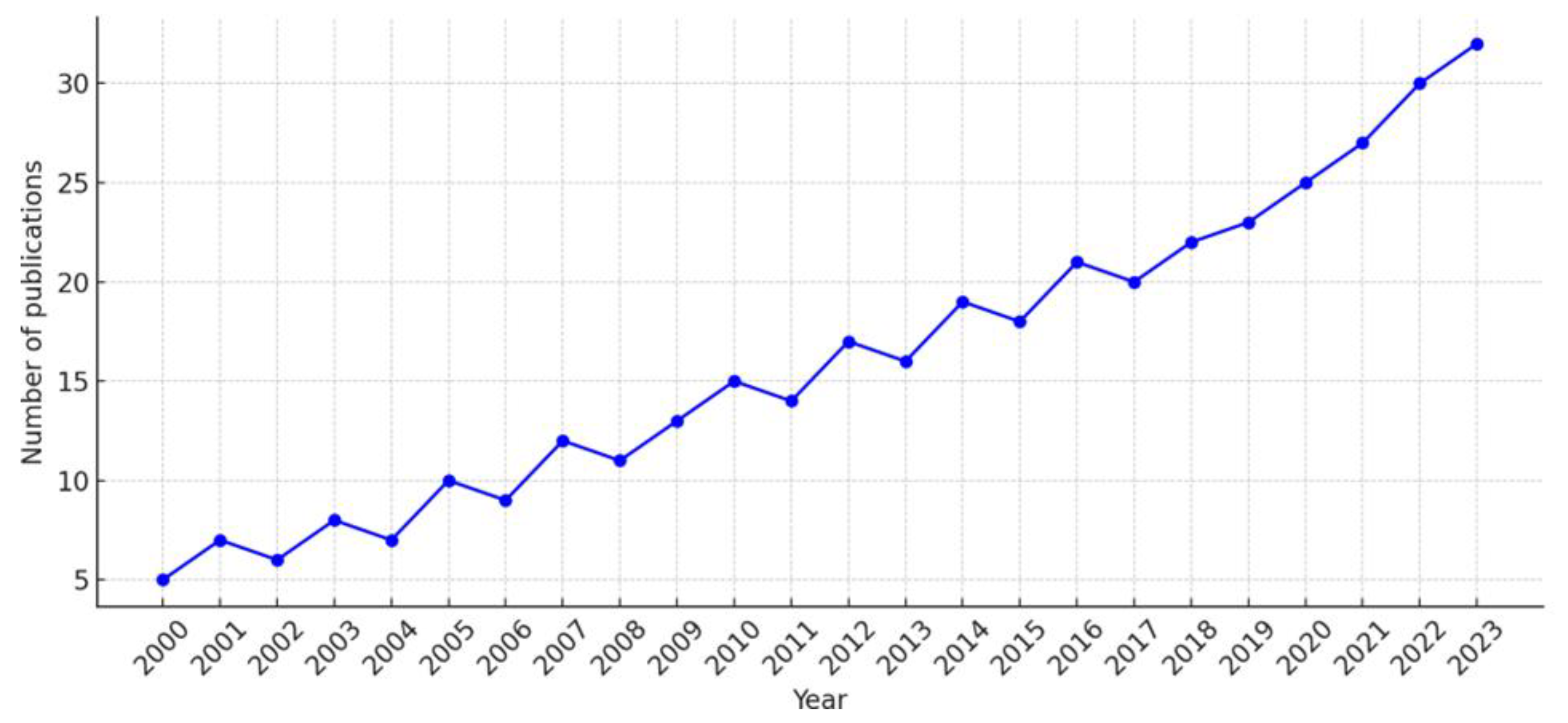

Table 1.
Caption.
| Authors, country, year | Type of study | Sample | Exposure | Comparators | Statistical significance | Limitations | Sample calculation | Confounders | Outcomes |
| 1. Eminoğlu et al, 2025, Turkey [38]. | Cross-sectional study | 234 dentists (both male and female) | Physical activity levels and presence of musculoskeletal disorders (MSDs) | Dentists with different levels of physical activity (e.g., active vs. inactive) | Significant associations found between lower physical activity levels and higher prevalence of MSDs (p < 0.05) | Cross-sectional design limits causal inference; self-reported data may introduce bias | Not reported | Age, gender, years in practice, and BMI were considered | High prevalence of MSDs among dentists; lower physical activity associated with higher MSD occurrence and intensity |
| 2.Sezer, &, Sıddıkoğlu, 2025, Turkey [30]. | Cross-sectional study | 298 dental students (pre-clinical and clinical phases) | Presence of work-related musculoskeletal symptoms (WMSs) | Students with and without WMSs; comparison also made between pre-clinical and clinical students | Significant positive correlation between musculoskeletal symptoms and burnout symptoms (p < 0.01); clinical students showed higher symptom prevalence | Cross-sectional design limits causal interpretation; self-reported data; single-institution sample may limit generalizability | Not reported | Year of study, gender, and academic workload were considered in analyses | High prevalence of WMSs among dental students, particularly in clinical years; strong association with emotional exhaustion and depersonalization domains of burnout |
| 3. Al-Emara et al, 2024, Finland [39] | Cross-sectional questionnaire-based study - Single-centered |
255 dentists | Musculoskeletal disorders (MSDs) and work ability | descriptive study | MSDs were significantly linked to WAS, FWA, and work disability (p < 0.05). | low response rate (21%), possible self-reporting bias, limited to a single country | 1200 questionnaires sent, with a 21% response rate (255 valid responses) | Age, gender, physical exercise, use of dental loupes | Prevalence of musculoskeletal disorders, impact on work ability, sickness absence days |
| 4. Azimi, et al., 2024 Afghanistan [4] |
A cross-sectional study - Single-centered |
206 dentists | physical activity | no | Not highlighted | Not specified | Not specified | Not specified | Backache was the most common MSD. While 55% were vaccinated, 41.6% were not. Most (74%) found dentistry stressful, and 26.7% reported high end-of-day fatigue. |
| 5.Matur et al., 2023 Turkey [40] | Case-control study - Single-centered |
74 dentists under 40 from Istanbul University Faculty of Dentistry and 61 similarly aged and gender-matched administrative personnel as controls. | prevalence of CTS symptoms | Dentists versus control group | Dentists showed higher CTS symptoms and object dropping, with significant links to BCTQ scores and hand usage duration. | Small sample size, lack of EMG examinations for all participants, potential recall bias for object-dropping incidents, and limited specificity of BCTQ as a screening tool. | Not specified. | Age, sex, BMI, hand usage, and family history of CTS. | 55.4% of dentists reported dropping objects, significantly higher than 19.7% in controls (p<0.001). BCTQ scores were significantly higher in dentists, indicating more severe CTS symptoms and functional impairment. |
| 6.Al-Huthaifi et al., 2023 Yemen , [37] | Cross-sectional questionnaire-based study - Multi-centered (conducted in three dental schools) |
310 dental professionals (174 dental students, 50 interns, 72 general practitioners, 14 specialists) | Musculoskeletal disorders and other occupational hazards | descriptive study | Significant differences found in various parameters, including musculoskeletal problems and needlestick injuries (P<0.05) | Included only one city in Yemen, did not compare different levels of dental clinical professions, did not include auxiliary staff, small sample size | Based on G*Power software, 420 questionnaires distributed, 310 valid responses (response rate: 74%) | Gender, age, clinical profession, levels of awareness about occupational hazards | Prevalence of musculoskeletal disorders, awareness of occupational hazards, need for ergonomic education and preventive measures |
| 7.Macrì et al., 2023 Italy and Peru [41] |
Cross-sectional observational study - Multi-centered |
167 dental professionals (86 from Italy and 81 from Peru) | Musculoskeletal pain | descriptive study | Musculoskeletal pain was linked to gender, daily work hours, years of practice, and physical activity. | Small sample size, cross-sectional design, potential cultural differences not fully accounted for, lack of validated questionnaire | 187 questionnaires submitted, 167 valid responses (response rate: ~89%) | Gender, age, occupation, height, working hours, years of work, physical activity, weekly activity, presence of WMSD. | Prevalence of musculoskeletal pain, affected body regions, significant factors associated with pain, need for ergonomic education and intervention |
| 8.Javed, et al., 2023 Pakistan [42] | cross-sectional study - single-centered |
50 dentists, 38% female, aged between 20-50 years. | Neuromuscular Disorders | not specified | Not explicitly stated; however, the study found a higher prevalence of CTS among female dentists. | Small sample size of 50 dentists. | Not specified. | Not detailed | 40% reported mild hand/wrist pain, 10% moderate pain, 30% had daily wrist pain, 40% experienced slight weakness, and 6% moderate weakness. CTS was more prevalent among female dentists. |
| 9.Almeida et al , 2023 Portugal [29]. |
Systematic review and meta-analysis | 29 studies included; total pooled sample size of over 7,000 dental students | Musculoskeletal disorders (MSDs) among dental students | Not applicable (pooled prevalence from included studies) | High pooled prevalence of MSDs among dental students (~74% overall); significant heterogeneity observed among studies (I² > 90%, p < 0.001) | High heterogeneity; variation in methodologies across studies; lack of longitudinal data | Not applicable (systematic review/meta-analysis) | Not analyzed directly due to pooled nature of data; noted variability in assessment tools, gender distribution, and academic stage across studies | High prevalence of MSDs in dental students, particularly in the neck, shoulders, and back; underlines the need for early ergonomic and preventive measures |
| 10.Chenna et al 2022, India [43]. | Systematic review and meta-analysis | 45 studies included (total pooled sample size >12,000 dental healthcare providers) | Occupational risk of musculoskeletal disorders (MSDs) among dental professionals | Not applicable (pooled prevalence estimates from included studies) | Meta-analysis showed a high pooled prevalence of MSDs (overall prevalence ~78%) with significant heterogeneity across studies (I² > 90%, p < 0.001) | High heterogeneity among included studies; variation in MSD definitions and assessment tools; possible publication bias | Not applicable (systematic review/meta-analysis) | Not directly analyzed due to nature of pooled data; most included studies adjusted for age, sex, years of experience where reported | Very high prevalence of MSDs among dental professionals, particularly affecting the neck, back, and shoulders; highlights the need for preventive interventions |
| 11.Daou et al., 2022 Lebanon [44] |
Quantitative research - single-centered |
A total of 314 dentists (184 male and 130 female) | Job satisfaction | tress and satisfaction were linked to leisure, sleep, vacations, relationships, and experience. | Lack of leisure, sleep disorders, fewer vacations, and no outdoor activities were linked to greater psychosocial and patient relationship issues (all P < 0.05). | Not specified | Not specified | Not specified | The study found significant stress and job satisfaction issues among Lebanese dentists, recommending sports, cultural activities, better sleep, and mental health programs. |
| 12.Asaduzzaman et al., (2022). Bangladesh [36] | Multi centered, cross-sectional study | 206 professional dentists | occupational physical health | Comparisons based on gender, age, qualification, and occupation | Male SDPs had higher stress scores (P > 0.05), with significantly higher scores in those aged 50+ and at senior levels (P < 0.05). | Self-reported questionnaire could lead to logical bias Cross-sectional study design made it impossible to detect the connection and identify relevant risk factors |
Not specified | Not specified | Only 3.3% saw saliva as a risk. Most used protection; 73.3% noted aerosol risks, 96.7% sterilized tools, 60% felt treatment pain, 70% cited ergonomic risks, 20% were dissatisfied, and 23.3% unaware of technostress. |
| 13.AlDhae, (2022) Bahrain.[45] |
cross-sectional study - multi centered |
222 dental professionals (44.1% male, 55.9% female), aged 23 to 57, with varying physical activity levels. | physical activity | descriptive study | Ergonomic hazards caused the most job stress (25%), followed by biological hazards; physical had less impact, and chemical showed no effect. | The study’s limitations include its Bahrain-specific sample, which limits generalizability, a low response rate, and potential bias due to participation mainly from hazard-aware employees. | Of 300 healthcare workers with over a year of experience, 239 responded, and 222 questionnaires were analyzed. | Not specifically controlled for. | The study confirmed ergonomic, biological, physical, and chemical hazards, with ergonomic hazards most common and the primary cause of increased job-related stress. |
| 14.Zhou et al., 2021 China [46] |
Comparative cross-sectional study - Single-centered |
100 dentists and 102 control aged 22-60 years. | Physical activity,musculoskeletal disorders | Office workers matched by age and gender. | P-values for various tests included, with significant results highlighted. | Limited to Nanjing area; relatively small sample size; cross-sectional design. | Not specified. | Adjusted for working age and gender. | Dentists reported more neck pain (73% vs. 52%) and lower PPTs, indicating higher pain sensitivity. Women had greater CROM and lower PPTs than men. Mobility decreased with age. |
| 15.Gandolfi et al., (2021) Italy [10] |
Cross-sectional observational study - Multi-centered |
284 dental professionals (dentists and dental hygienists) | Work-related musculoskeletal disorders (WMSD) | descriptive study | WMSDs were significantly linked to gender, daily/weekly working hours, years of experience, and ergonomic knowledge. | Undisclosed mobilization, potential misinterpretation of activities, inability to link WMSD solely to work, and cross-sectional design limiting causality. | 323 questionnaires distributed, 284 valid responses (response rate: 88%) | Gender, age, body fat, height, occupation, work hours, experience, physical activity, mobilization, ergonomic knowledge. | Prevalence of WMSD, most affected body regions, significant factors associated with WMSD, need for ergonomic education |
| 16. Alnaser, et al., (2021) Kuwait [47] |
cross-sectional multicentered |
232 dentists | Work-related musculoskeletal disorders | Descriptive study | Dentists with WMSD were older, had more experience, and worked longer hours. Pain linked to lost workdays; stress was tied to less sleep, lower job satisfaction, and higher male dissatisfaction. | No specific limitations noted | Not specified | Age | Older dentists, those in practice longer, and those working longer hours were more likely to report work-related musculoskeletal disorders (WMSD). There was a significant association between the rating of pain and lost days from work. |
| 17.Berdouses et al., (2020) Greece [48] |
Cross-sectional - Nationwide survey |
1500 Greek dentists (855 males and 645 females) randomly selected and interviewed over the phone. | Work-related musculoskeletal disorders (MSDs) and their correlation with working conditions | MSD variations were linked to posture, four-handed dentistry, and assistant presence. | Higher MSD prevalence was found in those with over 10 years of work, with distribution varying by posture and four-handed dentistry (p < 0.05). | Subjectivity of responses has potential for more accurate responses from recent episodes, and lack of direct comparison to older studies. | The initial sample included 1968 dentists (1007 males, 961 females); 1500 participated (855 males, 645 females). | Gender, years of practice, method of working (seated vs. standing), and use of four-handed dentistry. | 54.1% reported MSDs, mainly back, hand, cervical, shoulder, and leg problems. Four-handed dentistry and seated posture influenced MSD distribution, while exercise correlated with lower MSD prevalence. |
| 18.Pavičin et al., (2020) Croatia [49] |
Quantitative research Single-centered |
406 dentists in Croatia | Occupational injuries among dentists. | Not applicable. | P-values for various tests included, with significant results highlighted | Limited to dentists in Croatia; relatively small sample size; self-reported data. | Not specified | Adjusted for age, gender, specialization, and years of practice | 63.05% of respondents reported injuries from dental practice, mainly needle punctures (57.75%), cuts (20.86%), and eye injuries (13.37%). Key risk factors include improper posture, stress, infection, and noise. |
| 19.AlAbdulwahab et al., 2020 Saudi Arabia [50] |
Quantitative research, multicentered | Sample of 339 dentists (220 females and 119 males) | musculoskeletal disorders | Yes | Statistical significance highlighted | Not mentioned | Not mentioned | Not mentioned | |
| 20.Harris et al., 2020 Canada [51] |
Cross-sectional - multi centered |
647 registered dental hygienists in Canada. | work-related /working hours/physical activity | Not applicable | Positive correlation between years in practice and the number of MSDs reported (r = 0.238; p < 0.001). | Low response rate (2.24%); lacked data on confounders, MSD severity, and work impact. Social media and English-only format skewed responses. | Target sample of 379 ensured 5% margin of error at 95% confidence. | Not specifically controlled for. | 83% reported work-related MSDs, mainly CTS and tendonitis. Incidence rose with years in practice. Half and most schools found prevention training adequate. |
| 21.Miron et al., (2018) Romania. [7] |
Cross-sectional study - Multi-centered |
116 dentists (after excluding inadequately completed questionnaires) from Cluj-Napoca, Romania | Work stress, health behaviors, and coping strategies | descriptive study | Work stress was significantly linked to sociodemographics, health behaviors, and coping strategies. | Low response rate, potential information bias, overrepresentation of young dentists and those who teach at the university, limited generalizability to older age groups | Sample size set at 148; 250 questionnaires distributed to offset low response rate. | Factors included age, workplaces, work hours, job satisfaction, exercise, nutrition, and work-related pain. | Overall work stress scores, predictors of work stress, health behaviors, coping strategies, self-perceived health |
| 22.Ahmad et al., 2015 Pakistan [52]. |
Cross-sectional study - Multi-centered |
1,190 healthcare professionals (doctors, nurses, dentists) | Diet, exercise, mental well-being | No | Found significant (p<0.05) | Non-probability sampling, lack of detailed dietary guidelines for Pakistan, self-reported BMI, and subjective occupational stress assessment. | Followed sample size recommendations by VanVoorhis & Morgan (2007) | Gender, age, income, profession, psychosocial stressors, dietary habits | Low prevalence of regular exercise, high levels of occupational stress, moderate levels of mental well-being, dietary patterns not meeting recommended guidelines |
| 23.Memarpour et al., (2013) Iran, United Arab Emirates [53] |
Cross-sectional study Single centered |
272 dentists (205 generalists and 67 specialists) | Work-related musculoskeletal disorders (MSDs) | No | Found significant (p<0.05) | Not specified | Not specified | Gender, years of work, ergonomic exercise | High prevalence of MSDs, especially in shoulder, neck, and lower back; significant correlation with years of work and ergonomic exercise |
| 24.Hashim & Al-Ali (2013) Dubai, Iran, United Arab Emirates[54]. |
Cross-sectional study Single centered |
733 dentists aged 22-70 years, both male and female, from public and private sectors | Health problems, exercise habits, smoking habits, systemic diseases | No | Found significant (P < 0.05) | Potential inaccuracies in self-reported data | Not specified | Gender, work sector (public vs. private), smoking habits | Low prevalence of regular exercise, significant smoking habits, systemic health problems including cardiovascular diseases |
| 25.Singh & Purohit (2012) India [55] |
Cross-sectional study - single centered |
324 dental health care professionals | Physical activity, sedentary lifestyle, and obesity | No | Found significant (P ≤ .05 for physical activity, P ≤ .001 for obesity) | Not specified | Not specified | Assessment of physical activity, sedentary behavior, and obesity in dental professionals | Physical activity levels (mean MET minutes/week) varied significantly, with students and interns being more active than faculty, who also had the highest obesity rates. These differences were statistically significant. |
| 26.Ellapen et al., (2011) South Africa [56] |
Occupational, epidemiological retrospective study -Single centered |
94 dentists aged 24-75 years old | Poor dental ergonomical practice | No | Found significant (p<0.05) | Lack of radiographs and posture profiles | Not specified | Gender, race, and BMI | Prevalence of musculoskeletal pain and discomfort in different body parts |
| 27.Sharma & Golchha (2011) India [57] |
Questionaire survey single centered |
102 Indian dentists (80 males) from Delhi NCR with recent MSDs; 220 dentists (194 females) from Podlaskie Voivodeship. | Physical activity's role in preventing work-related MSDs. | No | Found significant correlation using Pearson correlation test | Not specified | Not specified | Gender, duration of work, and ergonomic factors | Awareness of physical activity's role in prevention, correlation between physical activity sessions and symptom improvement |
| 28.Kierklo et al., (2011) Poland[58] |
Questionaire survey Single centered |
Work-related musculoskeletal disorders (MSDs) | No | Found significant (p<0.05) | No correlation between work and MSDs, except in specific cases; reliance on self-reported data. | Not specified | Gender, years of practice, work posture, and rest breaks. | High prevalence of MSDs, especially in neck and lower back, correlation between years of practice and MSD occurrence |
Table 2.
Sensitivity Analysis Summary for detailed outcomes.
| Sensitivity Condition | Impact on Findings | Effect Description |
| Exclusion of small sample studies (<100 participants) | Low to moderate | Trends remain consistent, minor statistical shifts |
| Inclusion of studies with standardized MSD diagnostics only | Minimal | Findings confirm reliability across consistent diagnostics |
| Exclusion of studies from LMICs | Moderate to high | Contextual insights reduced, skew toward high-income settings |
| Inclusion of studies specifying sector (public/private) | Significant (data reduction) | Weaker conclusions due to limited data |
| Inclusion of studies published after 2020 only | Shift in thematic focus (less emphasis on MSDs) | More focus on mental health; traditional MSD patterns diluted |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



