Submitted:
30 June 2025
Posted:
02 July 2025
You are already at the latest version
Abstract
Background/Objectives: Antibiotics are the recommended first-line therapy for acute uncomplicated lower urinary tract infections (cystitis), but antibiotic resistance and tolerability concerns require antibiotic-sparing strategies. This study evaluated D-mannose as a stand-alone alternative. Methods: This multicenter, randomized, controlled, double-blind study, compared D-mannose to fosfomycin in women aged 18–70 with cystitis. Clinical cure (CC) was assessed using the Acute Cystitis Symptom Score (ACSS) up to day 8, with non-inferiority tested at the 15% margin. Post hoc analytical approaches accounted for potential bias due to low sample sizes and missing values. Results: The study randomized 118 patients. At baseline, severe symptoms (ACSS ≥12) were more frequent in the D-mannose group compared to fosfomycin (32.8% vs. 22.8%). Efficacy analyses were performed on the per-protocol set (D-mannose: N = 57; fosfomycin: N = 54). Median time to CC was 5.0 days (D-mannose) and 3.0 days (fosfomycin) overall, and 4.0 days vs. 3.0 days in the subgroup of moderate disease severity. The point estimate for the CC rate difference on day 8 (−10.1%) favored fosfomycin but was within the non-inferiority margin. Due to wide confidence intervals, non-inferiority was not statistically demonstrated. The post hoc analysis yielded smaller confidence intervals with estimated CC rates of 84.2% (D-mannose) vs. 83.5% (fosfomycin) on day 8 and statistically confirmed non-inferiority. Recurrence rates were similar (13.2% vs. 13.3%) and there was no statistically significant difference for additional antibiotic use (19.3% vs. 11.1%). Investigators and patients favored D-mannose over fosfomycin for tolerability, and gastrointestinal adverse events were less frequent (9.8% vs. 24.6%). Conclusions: D-mannose treatment was non-inferior to fosfomycin in uncomplicated cystitis according to post hoc analyses and may be an alternative to antibiotic first-line therapy, not least because of the favorable risk-benefit ratio.
Keywords:
urinary tract infection (UTI)
; cystitis
; D-mannose
; antibiotics
; acute cystitis symptom score
; non-inferiority
1. Introduction
Acute uncomplicated infections of the lower urinary tract are common in the outpatient setting. Risk factors include female sex, sexual intercourse, and vaginal infection [1]. The lifetime prevalence of urinary tract infections (UTI) among women is approximately 40% and recurrent episodes of UTI occur in one in five women [2].
Most cases of acute uncomplicated UTIs (hereafter referred to as cystitis unless otherwise noted) are caused by bacterial pathogens, primarily uropathogenic Escherichia coli (E. coli), which accounts for 75% of all cases [3]. Diagnosis of acute cystitis does not require microbiological confirmation and, in the absence of vaginal discharge, can be made on the basis of clinical symptoms alone, i.e., dysuria, frequency, and urgency [4]. Dipstick urinalysis for blood, leukocytes, and nitrite can increase diagnostic accuracy, especially in equivocal cases [4]. The Acute Cystitis Symptom Score (ACSS), a validated questionnaire with high sensitivity and specificity, enables the symptom-based diagnosis and subsequent monitoring of the infection [5].
The European Association of Urology (EAU) guidelines on urological infections recommend oral antibiotics, namely fosfomycin trometamol, pivmecillinam, or nitrofurantoin, as first-line treatment for cystitis [4]. The German guideline in addition recommends nitroxoline and trimethoprim [5]. Fosfomycin, a broad-spectrum antibiotic that disrupts cell wall synthesis [6], achieves a clinical cure (CC) rate of 78.7% in cystitis with a single dose according to a post hoc calculation [7]. Although generally well tolerated, gastrointestinal side effects such as diarrhea and nausea are common [8], likely due to imbalances in the gut microbiome [9]. The global burden of antibiotic resistance also affects the treatment of cystitis [10]. According to the current guidelines, non-antibiotic options such as ibuprofen and certain phytotherapies can be considered in non-geriatric patients or patients with mild to moderate symptoms as primary therapy as part of a symptomatic approach following participatory decision-making [4,5].
An example of an effective and causal non-antibiotic strategy is the disruption of bacterial adhesion to the urinary tract epithelium, a key step in infection [11]. Glycoproteins serve as adhesive structures for uropathogenic bacteria with so-called type 1 fimbriae [12]. D-mannose, a natural glucose epimer, saturates these bacterial adhesive structures, namely FimH, and prevents bacterial attachment to bladder cells [13]. Thanks to this mechanism, D-mannose is classified and marketed for the prevention and treatment of cystitis under medical device regulations [14].
Several studies have demonstrated the efficacy of D-mannose, alone or in combination, for the prevention of recurrent UTI and provided preliminary support for its use in acute treatment [15,16,17,18,19,20]. A non-interventional study (NIS) in acute cystitis was performed with D-mannose as monotherapy [21] and a post hoc analysis of this NIS compared D-mannose with antibiotics, showing promising potential as an alternative treatment [22]. However, direct, high-level, comparative evidence against antibiotics was still limited. Therefore, the present randomized controlled clinical trial was designed to confirm the safety and efficacy of D-mannose as a stand-alone treatment for acute cystitis as compared to antibiotic first-line therapy.
2. Results
2.1. Study Population
The clinical study (EudraCT 2021-003466-12) was conducted from May 2022 to August 2023 in 22 medical practices and clinical trial units in Germany. The trial ended as planned. By July 2023, a total of 134 adult female outpatients with symptoms of acute cystitis had been screened and 118 patients randomized. The full analysis set (FAS) and the safety evaluation population (SEP) consisted of 61 patients randomized to the D-mannose group and 57 patients randomized to the fosfomycin group. Of these, 25 patients discontinued the study prematurely, mainly due to the need for additional antibiotic therapy for cystitis (Supplementary Figure S1). The per-protocol set (PPS) included 57 patients in the D-mannose group and 54 patients in the fosfomycin group. Reasons for exclusion from the FAS were: missing visits (five patients), violation of a key exclusion criterion (one patient), and prohibited concomitant medication (one patient).
2.2. Patient Characteristics
Patient demographic and clinical characteristics were well balanced, with no significant differences between the two treatment groups (Table 1). Similar values were obtained for the PPS (Supplementary Table S1).
2.3. Clinical Cure (CC)
According to the per-protocol analysis, on day 8 the CC rate according to the main definition (ACSS Typical Domain Score ≤4 including all items) was lower in the D-mannose group (82.5%; 47/57 patients) than in the fosfomycin group (92.6%; 50/54 patients) (Figure 1A). Results were similar for the CC definition variation 1 (ACSS Typical Domain Score ≤4 excluding the item ‘incomplete voiding’) and the CC definition variation 2 (ACSS Typical Domain Score ≤3 excluding the items ‘incomplete voiding’ and ‘suprapubic pain’). Namely, the proportion of patients with CC was lower in the D-mannose group compared to the fosfomycin group in variation 1 (82.5% vs. 94.4%) and variation 2 (84.2% vs. 94.4%). The difference in CC rates (point estimate −10.1%, main definition) on day 8 did not exceed the non-inferiority threshold of −15.0%. However, non-inferiority could not be demonstrated at this point due to wide confidence intervals. The proportion of patients with CC (main definition) increased in both treatment groups until day 29. The difference in CC rates (−4.0%) on day 29 between the D-mannose group and the fosfomycin group (89.8%; 44/49 patients vs. 93.8%; 45/48 patients) as well as the lower limit of the 95% CI (−14.9, 6.9) did not exceed the −15% margin and therefore the criterion for non-inferiority was met.
Per-protocol time-to-event analyses showed that patients in the D-mannose group achieved CC two days later than patients in the fosfomycin group (median time to CC 5.0 days vs. 3.0 days). In patients with moderate disease severity at baseline (ACSS Typical Domain Score 6–12), the difference between the groups was reduced to one day (median time to CC 4.0 days vs. 3.0 days). Patients with severe disease at baseline (ACSS Typical Domain Score ≥12) reached CC after a median of 6.0 days (D-mannose) and 3.0 days (fosfomycin). Of note, rapid improvement in symptoms indicating considerable healing progress was observed days before the definition of CC was reached (see section ‘Time course of ACSS Typical Domain Score’). This early onset of symptom improvement possibly weighs more in patients’ perception than achieving formal CC (see section ‘Global assessment of efficacy’). The proportion of patients who achieved CC within the first eight days according to the time-to-event analyses in the total population (86.0% vs. 94.4%) was consistent with the analysis of CC rates as described above. The minor differences between the approaches can be attributed to the respective evaluation schedules. The rate-based approach considered only the CC rates on day 8 specifically, whereas the time-to-event approach analyzed the first occurrence of CC at any time up to day 8.
Post hoc analyses corrected for potential bias due to missing values and the persistence rule (i.e., per-protocol CC persisted until recurrence of UTI or the last day of the study). To reduce this bias, a multiple imputation procedure was applied to the data, and the persistence rule was disregarded. This approach resulted in estimated CC rates of 84.2% for D-mannose and 83.5% for fosfomycin on day 8. Estimates over time showed strong improvement from day 1 to day 8 in both groups, with an approximately linear course from day 1 to day 8 in the D-mannose group. In the fosfomycin group, the increase in CC rates was initially greater up to day 3 and less thereafter. From day 6 on, the curves converged considerably, indicating a reduced difference between the groups (Figure 1).
Post hoc analyses of time-to-event evaluations were based on the CC data of the per-protocol analysis and the time of first occurrence of CC without (Figure 2A) and after (Figure 2B) multiple imputation of the ACSS Typical Domain Scores. Furthermore, the time-to-event estimators for single time points were based on post hoc models as proposed by Möllenhoff et al. [23], applying the standard Kaplan-Meier (KM) technique (Figure S2A) and a parametric structure (Figure S2B). This statistical technique enabled use of a difference scale even for time-to-event models. Consequently, the same non-inferiority margin (15%) could be used for both CC endpoints (CC rate and time to CC).
The results were consistent with the per-protocol analyses with regard to median time-to-event (D-mannose: 5 days; fosfomycin: 3 days). Multiple imputation in the rate-based approach (basic model) slightly altered the non-inferiority assessments of the treatment differences in CC from day 1 to day 8 (Figure 2A,B). The precision of the conclusion increased, as indicated by the steady decrease of confidence interval lengths from the basic model (Figure 2B) to the nonparametric Möllenhoff model (Figure 2C) and parametric Möllenhoff model (Figure 2D). Therefore, the parametric model was considered to be a more adequate description of the time trends reported.
All four approaches indicated a treatment difference in favor of fosfomycin from day 3 to day 5 only. But thereafter this difference clearly narrowed, and the point estimators were above the defined non-inferiority margin of −15.0% (Figure 2A–D). On day 8, non-inferiority of D-mannose to fosfomycin was statistically demonstrated given the lower boundary of the confidence interval was within the limits of the predefined non-inferiority margin in all the post hoc analytical approaches (Figure 2B–D).
Based on the meaningful results of the post hoc imputation and modelling approaches, post hoc simulations were performed to estimate the sample size required to demonstrate non-inferiority in future trials (Figure 3). The simulations applied both Möllenhoff approaches with CC on day 8 as an efficacy parameter due to its clinical relevance (main definition as defined per protocol without the persistence rule). Accordingly, non-inferiority estimates (M1) <0.15, i.e., the difference between test and comparator treatment including 95% CI did not exceed 15% in favor of the comparator, might be achieved with high probability even with sample sizes of n = 50 per group in the nonparametric Möllenhoff KM model and with sample sizes of at least n = 80 per group applying the parametric Möllenhoff model. To sum up, the parametric Möllenhoff model is anticipated to generate more precise estimates due to its relative complexity, especially with small sample sizes.
2.4. Time Course of ACSS Typical Domain Score
The proportion of patients with more severe symptoms at baseline was greater in the D-mannose group as compared to the fosfomycin group in the PPS (31.6% vs. 24.1%, Supplementary Table S1). Despite this disbalance, both treatments showed a strong and rapid improvement of symptoms according to the per-protocol analysis of the ACSS Typical Domain Score (Supplementary Figure S3). The post hoc analysis with multiple imputation of missing values is consistent with the per-protocol analysis. Accordingly, in both groups, symptom severity was reduced by at least 80% from day 1 to day 8. The reduction in the fosfomycin group was stronger over the first few days, but the courses converged towards day 8, indicating comparable symptom relief in both groups overall (Figure 4). No further differences between the groups were observed in the follow-up phase from day 9 (data not shown).
2.5. UTI Recurrence and Antibiotic Treatment
During the follow-up phase, the incidence of UTI recurrence (defined as an ACSS Typical Domain Score ≥6 in patients who were previously in CC) was 12.3% (7/57 patients) in the D-mannose group and 13.0% (7/54 patients) in the fosfomycin group. However, unequal overall dropout rates (14.0%, 8/57 patients vs. 5.6%, 3/54 patients) necessitated a post hoc analysis to adjust for the number of dropouts. This analysis estimated a mean recurrence rate of 13.2% in the D-mannose group and 13.3% in the fosfomycin group, supporting similar recurrence rates in both groups. Additional antibiotic treatment was required at various times up to day 29 in 11 patients (19.3%) in the D-mannose group compared to 6 patients (11.1%) in the fosfomycin group. The rate was not significantly different for the two groups (rate difference: 8%; 95% CI −6, 21).
2.6. Microbiological Status
The proportion of patients with a negative urine culture on day 8 was lower in the D-mannose group than in the fosfomycin group (57.4%, 31/54 evaluable patients vs. 66.7%, 34/51 evaluable patients), but the difference did not reach statistical significance (p = 0.311; normal approximation of the difference applying an arcsine transformation). Among patients with a positive urine culture at baseline (D-mannose: N = 34, fosfomycin: N = 33; PPS), 39.4% (13/33 evaluable patients) in the D-mannose group vs. 59.4% (19/32 evaluable patients) in the fosfomycin group had a negative urine culture on day 8. The difference in microbiological success rate was −20.0% (95% CI: −43.8, 3.8).
2.7. Global Assessment of Efficacy
Efficacy of treatment was rated either ‘very good’ or ‘good’ by the majority of investigators (66.7%, 38/57 patients vs. 75.9%, 41/54 patients) and patients (70.2%, 40/57 patients vs. 79.6%, 43/54 patients) in the D-mannose and the fosfomycin group, respectively. Overall, this suggests high treatment satisfaction with only minor differences between the groups despite the delay in achieving CC (Supplementary Figure S4).
2.8. Safety Results
Treatment-emergent adverse events (AEs) occurred in 32.8% of patients in the D-mannose group and 45.6% of patients in the fosfomycin group. All AEs were mild to moderate in intensity, with one exception. A total of 2.5% of patients discontinued treatment and withdrew from the study due to AEs. The incidence of drug-related AEs was distinctly higher in the fosfomycin group (22.8%) compared to the D-mannose group (9.8%). The most affected System Organ Class was gastrointestinal disorders with an AE incidence of 9.8% in the D-mannose group compared to 24.6% in the fosfomycin group, with diarrhea occurring in 1.6 % and 21.1% of the SEP, respectively. Group comparisons revealed a statistically significant difference in the occurrence of gastrointestinal disorders in favor of D-mannose. A small p-value (p <0.08) in the group comparison of AEs related to the study drug indicated a trend towards better tolerability of D-mannose compared to fosfomycin overall (Table 2).
On day 8, tolerability was rated ‘very good’ or ‘good’ by 91.8% of investigators (56/61 patients) for D-mannose and 82.5% (47/57 patients) for fosfomycin, with a statistically significant advantage for D-mannose (p = 0.0456) (Figure 5). Patients’ tolerability ratings were similar (90.2%, 55/61 patients vs. 82.5%, 47/57 patients; p = 0.0075). ‘Very good’ tolerability was reported more frequently for D-mannose than for fosfomycin (investigator ratings 73.8%, 45/61 patients vs. 56.1%, 32/57 patients; patient ratings 75.4%, 46/61 patients vs. 50.9%, 29/57 patients). The proportion of patients with ‘poor’ or ‘very poor’ tolerability was similar in both treatment groups on day 8. Day 29 assessments showed similar results (data not presented).
3. Discussion
The present proof-of-concept study showed comparable efficacy of D-mannose monotherapy in females with cystitis compared to antibiotic first-line therapy with fosfomycin, using a non-inferiority design. Both treatments achieved high CC rates on day 8 with a difference in median time to CC of two days only (5.0 vs. 3.0 days). In patients with typical symptom severity at baseline, the difference until CC was reduced even further to one day (4.0 vs. 3.0 days). Due to the small sample size, which led to wide confidence intervals, non-inferiority with a margin of 15% could not be demonstrated in the per-protocol analysis, but a trend was apparent. A post hoc analysis that accounted for the small sample size showed CC rates of 84% on day 8 for both groups and statistically confirmed non-inferiority. Furthermore, although the proportion of patients with severe symptoms at baseline was higher in the D-mannose group (32.8% vs. 22.8%), the time course of symptoms demonstrated strong and rapid improvement under both treatments, emphasizing the comparable efficacy of both. The recurrence rates during the follow-up phase were low and almost identical in both arms (13.2% vs. 13.3%). Moreover, no statistically significant difference in the need for additional antibiotic treatment was observed (19.3% vs. 11.1%) throughout the study, which showed antibiotic-sparing potential of at least 80% for D-mannose. Despite the two- or one-day difference in time to cure, only 10% of patients were less satisfied with efficacy of D-mannose compared to fosfomycin, according to the global assessment. The global assessment of tolerability by investigators and patients favored D-mannose over fosfomycin and the incidence of gastrointestinal adverse events was substantially reduced with D-mannose treatment (9.8% vs. 24.6%), in particular the frequency of diarrhea (1.6% vs. 21.1%).
This non-inferiority study was designed with a significantly higher degree of standardization than previously published studies on D-mannose in this indication. The present study is therefore well suited to provide valid evidence for the efficacy of D-mannose and fosfomycin in the treatment of cystitis. The high level of standardization is reflected in the treatment allocation per randomization, the choice of comparator, the statistical approach, the choice of endpoints, and the precise definition of the study population. The key selection criteria focused on the severity and limited duration of clinical signs before study entry, without restriction to patients with a positive urine culture. Therefore, the study population represents standard clinical cystitis cases very well.
The concept of D-mannose as an appropriate treatment for cystitis was based on preliminary evidence from several trials which not only showed that D-mannose monotherapy could effectively protect against UTI recurrence [15,16,17,19], but also suggested symptom improvement in acute therapy [15]. A non-interventional study then provided evidence for the effectiveness of D-mannose monotherapy in cystitis with 78.6% patients free of cystitis symptoms up to day 7 [21]. In comparison, the spontaneous healing rate has been reported to be up to 50% after one week [5]. Of note, the time and definition of CC assessment varies between clinical trials in this indication but mostly lies within a range of ±1 day in comparison to the present study, which used day 8 for assessment of CC.
Fosfomycin was selected precisely because it is highly efficacious, recommended for first-line treatment, and has the highest possible compliance rate due to its single dose use [4], all of which makes it the most appropriate antibiotic comparator. Cure rates of 78% for CC and 79% to 84% for microbiological cure have been estimated for fosfomycin from two meta-analyses [22], and while the estimates showed no significant differences from other antibiotics, another recent meta-analysis concluded that fosfomycin might be more efficacious than other first-line antibiotics [24]. The fosfomycin results from the present study are consistent with previously reported estimates. The CC rates achieved with D-mannose are also in line with previously reported data [21,22], and the ACSS Typical Domain Score showed a similar time course, with a decline starting from the first day of treatment and a reduction of approximately 80% in median symptom scores by the end of the observation period [22].
Another non-antibiotic treatment investigated in a similar randomized clinical non-inferiority trial is the phytotherapeutic Canephron® (BNO 1045), which was likewise shown to provide antibiotic-sparing potential. It was found that 83.5% of patients treated with Canephron® and 89.8% of patients treated with fosfomycin did not require additional antibiotic therapy. Although the treatment effect estimate met the non-inferiority criterion [25], the claim was based on antibiotic sparing as a surrogate endpoint for clinical efficacy instead of a hard CC endpoint. It is worth noting that the Canephron® study included approximately 300 patients per group, which exceeds the size of the present study. It also exceeds the current simulation results for D-mannose, which indicate a sample size of at least 80 per group to demonstrate non-inferiority of D-mannose to fosfomycin in future studies applying a direct efficacy endpoint. The microbiological success rate of fosfomycin treatment was lower in the Canephron® study (36.7%) than in the present study (59.4%). Given the similar CC rates in both studies, the inconsistent microbiological results call into question the accuracy and clinical relevance of the microbiological endpoints and therefore their suitability for non-inferiority assessment. This also applies to the combined endpoint of clinical and microbiological cure as recommended by the European Medicines Agency (EMA) guideline on clinical trials in UTI [26]. Clinical trials routinely apply cut-off levels at baseline of 103 CFU/ml or higher for patients with a positive urine culture despite the presence of clinical symptoms [25,27], leaving up to 40% of patients unevaluable for (combined) microbiological endpoints. Finally, in clinical routine, microbiological assessments are interpreted in the context of clinical symptoms. They are impacted by – and therefore dependent on – clinical symptoms, which calls into question endpoints that combine clinical and microbiological cure. These aspects further underline the lack of suitability of both the microbiological endpoint and combined clinical and microbiological endpoint for assessments of efficacy. Consequently, a purely clinical assessment of cure based on a validated symptom score, i.e., the ACSS Typical Domain Score, is unambiguous and no less suitable than the combination of symptom burden and microbiological examination [28].
The present study uses the ACSS Typical Domain Score as a patient-reported outcome measure (PROM) for diagnosis at enrolment, assessment of clinical course, and definition of CC. This is appropriate because the ACSS assesses the typical symptoms of acute cystitis and has been shown to be an effective diagnostic and monitoring tool [7,28,29]. It is compatible with the diagnostic criteria set out in the current guidelines of the US Food and Drug Administration (FDA) and the EMA guidelines [22,28]. The suitability of the ACSS for clinical trials has been previously evaluated [7,28,29] and it is mentioned in the current disease management guidelines [4,5]. Furthermore, the consistency of CC rates and recurrence rates from the present study in comparison to other studies suggest that a purely symptom-based approach is accurate. The efficacy endpoints based on the ACSS Typical Domain Score therefore enable valid conclusions on the suitability of D-mannose monotherapy for uncomplicated cystitis.
The benefits of antibiotic use are indisputable, but the increasing prevalence of antibiotic resistance calls for restrictions on their use. Although the resistance rates of E. coli to fosfomycin and nitrofurantoin are reported to be low, resistance of uropathogens to other typical antibiotics is observed in more than 20% of cases. For trimethoprim the rate is even higher [30]. It follows that antibiotic resistance is also an issue in the treatment of UTI and the use of antibiotics should wherever possible be avoided. Furthermore, fosfomycin has attracted particular attention as an effective treatment against multidrug-resistant pathogens. Resistance to fosfomycin could threaten its role in this context should resistance spread [6]. Which is why the EMA has issued recommendations to restrict its use [31]. Although these restrictions do not directly affect the oral use of fosfomycin for cystitis in women, they do highlight the need for a cautious approach to antibiotic therapy and for alternative treatment options. In addition, tolerability issues affect the use of antibiotics in the treatment of cystitis, with gastrointestinal side effects such as diarrhea or nausea frequently reported [8] and attributable to antibiotic-induced imbalances in the gut microbiome [9]. These disruptions may contribute to increased rates of infection, immune dysregulation, and metabolic disorders. Furthermore, the gut microbiome has been discussed as a possible factor in the development of antibiotic resistance [9].
According to the German guideline, non-antibiotic therapies should be considered as an alternative to antibiotic therapy in non-geriatric patients following participatory decision-making [5]. However, the guideline emphasizes that the primary non-antibiotic treatments mentioned may be associated with a higher symptom burden and higher complication rates in pyelonephritis than observed with antibiotics. For these non-steroidal, anti-inflammatory substances (ibuprofen, diclofenac) and phytotherapeutics (uva-ursi, BNO 1045), the guideline shows an average saving of 63% on antibiotics in acute therapy. According to the present study, D-mannose has the potential for avoiding antibiotics in acute therapy in at least 80% of patients. The study also showed that although this substantial antibiotic-sparing effect of D-mannose was associated with a longer time to CC, no complications and fewer AE were observed with D-mannose, and the overall therapeutic outcome including symptom relief was comparable to that of fosfomycin.
Despite meeting stringent study design criteria as outlined above, the results of the present study are subject to certain limitations. The relatively small sample size, due to slow recruitment, reduced the statistical power of the study. As a sample size of 50 per group was estimated to be sufficient for the proof-of-concept status of the study, the confidence intervals were rather wide and testing in the per-protocol analysis could, therefore, not confirm non-inferiority statistically, despite clear trends. A post hoc analysis reduced the width of the confidence intervals and generated a valid estimate of the efficacy of D-mannose. The state-of-the-art statistical methods used in this analysis to account for the small sample size are robust and appropriate. Accordingly, the post hoc analysis demonstrated non-inferiority in the key endpoint of CC rate and congruent progress in symptom relief based on the ACSS Typical Domain Score. Taken together, the overall trend observed and the post hoc demonstration of non-inferiority are sufficient to classify D-mannose therapy as a medically relevant alternative to antibiotic treatment. Furthermore, the simulations showed that future pivotal studies would be successful with a sample size of at least 80 patients per group.
In conclusion, the present study indicates that D-mannose is an effective and well tolerated treatment for cystitis. D-mannose was shown to be comparable to antibiotics in terms of CC rates and symptom relief, while demonstrating a superior risk profile, particularly in terms of adverse effects such as diarrhea. As a result, it offers a favorable risk-benefit ratio, making it a viable alternative to first-line antibiotic therapy, particularly in self-medication and in patients who are reluctant to undergo antibiotic therapy.
4. Materials and Methods
4.1. Study Design and Conduct
MCMK0220 was a phase IV, multicenter, randomized, double-blind, double-dummy, active-controlled, two-arm, parallel-group study. It was designed as a proof-of-concept study to compare the efficacy, safety, and tolerability of oral treatment with D-mannose versus oral treatment with fosfomycin trometamol in female patients with cystitis. The study duration was eight days (acute phase) with a follow-up to day 29.
The study was conducted in accordance with the guidelines of the International Council for Harmonization for Good Clinical Practice and the principles of the Declaration of Helsinki. It was approved by an independent ethics committee, and written informed consent was obtained from all participants. Data were collected in medical practices and clinical trial units in Germany.
4.2. Participants and Treatments
Female outpatients aged 18-70 years were eligible if they had clinical signs and symptoms of cystitis with onset not earlier than 72 hours prior to enrollment, an ACSS Typical Domain Score of ≥6 at baseline, and leukocyturia at baseline. Key exclusion criteria were episodes of acute cystitis in the four weeks before enrollment or meeting the definition of chronic recurrent cystitis (³3 episodes in six months), the presence of or predisposition to complicated urinary tract infections, evidence of pyelonephritis, or vulvovaginitis. Details of the inclusion and exclusion criteria, including prior antibiotic use, are provided in the supplement.
Patients were randomized in a 1:1 ratio to receive the investigational treatment of D-mannose or the comparator treatment of fosfomycin. The randomization schedule was generated with SAS 9.4 TS1M7 prior to the start of the investigation by an external service provider. A block randomization scheme with four patients per block (with an allocation ratio of treatment groups 1:1) was applied. A double-dummy technique and identical appearance of all treatment packages (investigational treatment, comparator, placebos) ensured the blinding of the study. Treatment packages were prepared by an external service provider and dispatched to the study sites. Packages were numbered sequentially. Patients, investigators, and on-site study personnel remained blinded throughout the study. Sealed emergency codes made it possible to match randomization numbers and treatment packages only in an emergency.
Patients in the D-mannose group received 2 g of D-mannose for five days (three times daily on days 1–3 and twice daily on days 4–5), plus a single dose of fosfomycin-matching placebo. Patients randomized to the fosfomycin group received a single dose of 3 g fosfomycin trometamol on day 1, plus D-mannose-matching placebo for five days.
4.3. Endpoints and Assessments
No primary endpoint was defined for this proof-of-concept study. Efficacy endpoints included change in ACSS Typical Domain Score up to day 8, proportion of patients with CC (three definitions) on day 8 and day 29, time to CC within the first eight days, proportion of patients with UTI recurrence, proportion of patients requiring additional antibiotic treatment for UTI, and proportion of patients with a microbiologically negative urine culture on day 8. Safety endpoints included adverse events as well as investigator and patient global assessments of tolerability on day 8 and day 29. Details of the endpoints are provided in the supplement.
The ACSS Typical Domain Score includes six patient-reported items: urinary frequency, urgency, dysuria, suprapubic pain, incomplete voiding, and visible blood in the urine. Symptom intensity is rated on a four-point Likert scale (0 = none, 1 = mild, 2 = moderate, 3 = severe). A summary Typical Domain Score of ≥6 indicates a clinical diagnosis of cystitis [28,32]. The ACSS questionnaire was completed daily in the evening until day 8 and in the follow-up phase if indicated.
4.4. Statistical Methods
4.4.1. Sample Size Estimation
Initially, it was planned to randomize 436 patients. The sample size was adjusted due to slow recruitment, and a statistical power approach for a proof-of-concept study was incorporated by protocol amendment. The approach assumed that approximately 50 patients per treatment group would provide approximately 70% power to detect one-sided p-values ≤0.10. Assuming a dropout rate of 15%, 120 patients would be randomized.
4.4.2. Analyses According to Protocol
Efficacy assessments were performed on the PPS, which included all patients in the FAS, i.e., all randomized patients with at least one documented dose of study drug and post-baseline efficacy data who had no relevant protocol deviations and were considered clinically evaluable. The PPS was considered a more conservative analysis population in a non-inferiority setting. Key efficacy endpoints were analyzed using a non-inferiority testing procedure with a non-inferiority margin of 15% for rate differences at the lower limit of the confidence intervals (95% two-sided Wald confidence intervals). The non-inferiority margin was determined based on the treatment effect on CC rates of antibiotics compared to placebo, with appropriate adjustment according to the relevant FDA guideline [33].
Safety assessments were generally performed on the SEP, which included all randomized patients with at least one documented dose of study drug and a post treatment safety assessment. For tolerability assessments, differences between treatment groups were evaluated using the Wilcoxon rank test adjusted for center and additionally for baseline ACSS severity status, respectively (van Elteren test). A one-sided significance level of 2.5% was used. For numerical data with metric scale, the number of valid observations, arithmetic mean, standard deviation, median, minimum, and maximum values were presented. For categorical data, the absolute numbers (n) and percentages (%) (based on valid cases) were presented.
All per-protocol analyses were performed using SAS version 9.4.
4.4.3. Post Hoc Analyses
Post hoc analyses were performed to quantify and compare the daily changes in cure between treatment groups and to account for the limited sample size as well as possible data bias due to both (the per-protocol replacement of) missing values and the CC persistence rule defined in the protocol. To achieve this, missing ACSS data were replaced using a multiple imputation procedure and the persistence rule was not applied in the post hoc analyses. In addition, the model approach recently published by Möllenhoff and Tresch [23] was applied in the post hoc analyses of the time-to-event endpoints. The results hereof were influenced by the censoring times, which are important in time-to-event analyses. Therefore, the time-to-event endpoints did not need multiple imputation. The proposed time-to-event models considered two cases: a) a nonparametric approach using KM estimators and b) a parametric approach with assumed lognormal distributed data to maximize precision as proposed by the Akaike information criterion (AIC) values. With the Möllenhoff model, it was possible to calculate a rate difference for the time-to-event data in addition to the CC rates from the rate-based approach. This enabled comparison of the time pattern including estimation of p-values and confidence intervals (even for subsets of days) as well as comparison of treatment effects on the same scale, at all time points, and in each model. The four analyses used models of differing complexity to generate results on comparable scales. It was expected that the refined statistical methods of the Möllenhoff models (especially parametric modelling with bootstrap estimates of variance estimators) would increase the precision of the results.
Furthermore, the variances of the parametric model were estimated by bootstrap to enhance the statistical quality of the results. Bootstrap methods allow a more robust inference when theoretical derivations are complex or inapplicable (here: variance estimators and related confidence intervals) [23,34]. For both models, so-called ‘confidence bands’ were constructed for the treatment differences in the time interval considered (days 1 to 8). These bands could be used to test for non-inferiority of D-mannose versus fosfomycin at each time point and for groupings of time points.
In addition, the ACSS Typical Domain Score after multiple imputations was descriptively investigated for treatment differences. Estimates of UTI recurrence were also investigated for potential bias due to unequal dropout rates and compared by group.
Based on the study data, simulation analyses were performed using both Möllenhoff models to assess whether non-inferiority could have been achieved with higher sample sizes. All post hoc analyses were performed applying the R software (www.r-project.org/, version 3.6.3) and related software packages.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, In- and exclusion criteria, Endpoints, Clinical Cure (CC) Definition, Definition of recurrence of UTI, Table S1: Descriptive presentation of patient demographic and clinical characteristics, Figure S1: Patient disposition flowchart (all enrolled subjects), Figure S2: Treatment differences in CC, Figure S3: Per-protocol analysis of ACSS Typical Domain Score from baseline (V1) to day 8, Figure S4: Global assessment of efficacy on day 8.
Author Contributions
Conceptualization, F.W., P.G., O.E., A.B. and H.L.; methodology, F.W., P.G., O.E., A.B.; formal analysis, H.L.; investigation, H.T.; writing—review and editing, F.W., H.T., P.G., O.E., A.B., N.I. and H.L. All authors have read and agreed to the published version of the manuscript.
Funding
The study was sponsored by MCM Klosterfrau Vertriebsgesellschaft mbH. Post hoc data analysis, manuscript writing and editorial assistance were funded by MCM Klosterfrau Vertriebsgesellschaft mbH.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Medical Association in Sachsen (Ethikkommission der Sächsischen Landesärztekammer) (EK-AMG-MCF-11/21-1, and EK-MPG-MCF-1/21-1) on March 15, 2022. The study was registered in the EU Clinical Trials Register (2021-003466-12) on December 16, 2021.
Informed Consent Statement
Informed consent for participation was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
Medical writing assistance was provided by Karin Eichele (mediwiz, Schwabach, Germany). Language and editorial support was provided by Rupert Maitland (Poupas, France). Figures were designed by Franziska Keenan (justbefrank, Fuerth, Germany). We also thank PHARMALOG – Institut für klinische Forschung GmbH for their clinical trial support.
Conflicts of Interest
F.W. is a consultant of MCM Klosterfrau Vertriebsgesellschaft mbH. He is a speaker of the DFG (German Research Foundation) funded research group BARICADE (FOR5427/1-466687329) and a member of the DZIF (German Center for Infection Research; site: Giessen-Marburg-Langen). H.T. was the coordinating investigator of the clinical trial. H.L. is a consultant at MCM Klosterfrau Vertriebsgesellschaft mbH. P.G., O.E., N.I., and A.B. are employees of MCM Klosterfrau Vertriebsgesellschaft mbH. The funder was involved in the research design, collection, analysis, and interpretation of the data, the decision to publish the results, and in writing the manuscript.
References
- Foxman, B. Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect. Dis. Clin. North Am. 2014, 28, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.C.; Hawking, M.K.D.; Quigley, A.; McNulty, C.A.M. Incidence, severity, help seeking, and management of uncomplicated urinary tract infection: a population-based survey. Br. J. Gen. Pract. 2015, 65, e702–e707. [Google Scholar] [CrossRef] [PubMed]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nature Reviews Microbiology 2015, 13, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Bonkat G., Bartoletti R., Bruyère F., Cai T., Geerlings S.E., Köves B., Kranz J., Schubert S., Pilatz A., Veeratterapillay R., Wagenlehner F. EAU Guidelines on Urological Infections. In: EAU Guidelines, edition presented at the annual EAU Congress Paris 2024. ISBN 978-94-92671-23-3.
- Deutsche Gesellschaft für Urologie e., V. S3 Leitlinie: Epidemiologie, Diagnostik, Therapie, Prävention und Management unkomplizierter, bakterieller, ambulant erworbener Harnwegsinfektionen bei Erwachsenen – Aktualisierung 2024. Langversion, 3.0, AWMF Registernummer: 043/044. Available online: https://register.awmf.org/de/leitlinien/detail/043-044 (accessed on 25 October 2024).
- Castañeda-García, A.; Blázquez, J.; Rodríguez-Rojas, A. Molecular Mechanisms and Clinical Impact of Acquired and Intrinsic Fosfomycin Resistance. Antibiotics 2013, 2, 217–236. [Google Scholar] [CrossRef]
- Alidjanov, J.F.; Overesch, A.; Abramov-Sommariva, D.; Hoeller, M.; Steindl, H.; Wagenlehner, F.M.; Naber, K.G. Acute Cystitis Symptom Score questionnaire for measuring patient-reported outcomes in women with acute uncomplicated cystitis: Clinical validation as part of a phase III trial comparing antibiotic and nonantibiotic therapy. Investig Clin Urol 2020, 61, 498–507. [Google Scholar] [CrossRef]
- Keating, G.M. Fosfomycin trometamol: a review of its use as a single-dose oral treatment for patients with acute lower urinary tract infections and pregnant women with asymptomatic bacteriuria. Drugs 2013, 73, 1951–1966. [Google Scholar] [CrossRef]
- Hiergeist, A.; Gessner, A. The human intestinal microbiome and why you have to think twice before prescribing antibiotics! MMW Fortschr. Med. 2018, 160, 58–62. [Google Scholar] [CrossRef]
- von Vietinghoff, S.; Shevchuk, O.; Dobrindt, U.; Engel, D.R.; Jorch, S.K.; Kurts, C.; Miethke, T.; Wagenlehner, F. The global burden of antimicrobial resistance - urinary tract infections. Nephrol. Dial. Transplant 2024, 39, 581–588. [Google Scholar] [CrossRef]
- Sarshar, M.; Behzadi, P.; Ambrosi, C.; Zagaglia, C.; Palamara, A.T.; Scribano, D. FimH and Anti-Adhesive Therapeutics: A Disarming Strategy Against Uropathogens. Antibiotics 2020, 9. [Google Scholar] [CrossRef]
- Terlizzi, M.E.; Gribaudo, G.; Maffei, M.E. UroPathogenic Escherichia coli (UPEC) Infections: Virulence Factors, Bladder Responses, Antibiotic, and Non-antibiotic Antimicrobial Strategies. Frontiers in Microbiology 2017, 8. [Google Scholar] [CrossRef]
- Spaulding, C.N.; Hultgren, S.J. Adhesive Pili in UTI Pathogenesis and Drug Development. Pathogens 2016, 5. [Google Scholar] [CrossRef] [PubMed]
- Scaglione, F.; Musazzi, U.M.; Minghetti, P. Considerations on D-mannose Mechanism of Action and Consequent Classification of Marketed Healthcare Products. Front. Pharmacol. 2021, 12, 636377. [Google Scholar] [CrossRef] [PubMed]
- Domenici, L.; Monti, M.; Bracchi, C.; Giorgini, M.; Colagiovanni, V.; Muzii, L.; Benedetti Panici, P. D-mannose: a promising support for acute urinary tract infections in women. A pilot study. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 2920–2925. [Google Scholar]
- Porru, D.; Parmigiani, A.; Tinelli, C.; Barletta, D.; Choussos, D.; Di Franco, C.; Bobbi, V.; Bassi, S.; Miller, O.; Gardella, B.; et al. Oral D-mannose in recurrent urinary tract infections in women: a pilot study. Journal of Clinical Urology 2014, 7, 208–213. [Google Scholar] [CrossRef]
- Kranjčec, B.; Papeš, D.; Altarac, S. d-mannose powder for prophylaxis of recurrent urinary tract infections in women: a randomized clinical trial. World Journal of Urology 2014, 32, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Phé, V.; Pakzad, M.; Haslam, C.; Gonzales, G.; Curtis, C.; Porter, B.; Chataway, J.; Panicker, J.N. Open label feasibility study evaluating D-mannose combined with home-based monitoring of suspected urinary tract infections in patients with multiple sclerosis. Neurourology and Urodynamics 2017, 36, 1770–1775. [Google Scholar] [CrossRef]
- Lenger, S.M.; Bradley, M.S.; Thomas, D.A.; Bertolet, M.H.; Lowder, J.L.; Sutcliffe, S. D-mannose vs other agents for recurrent urinary tract infection prevention in adult women: a systematic review and meta-analysis. American Journal of Obstetrics & Gynecology 2020, 223, 265.e1–265.e13. [Google Scholar]
- Parazzini, F.; Ricci, E.; Fedele, F.; Chiaffarino, F.; Esposito, G.; Cipriani, S. Systematic review of the effect of D-mannose with or without other drugs in the treatment of symptoms of urinary tract infections/cystitis (Review). Biomed. Rep. 2022, 17, 69. [Google Scholar] [CrossRef]
- Wagenlehner, F.; Baumgartner, L.N.; Schopf, B.; Milde, J. Non-interventional study with Femannose® N to investigate tolerance, quality of life and course of symptoms in acute uncomplicated urinary tract infection. Journal Pharmakol u Ther 2020, 29. [Google Scholar]
- Wagenlehner, F.; Lorenz, H.; Ewald, O.; Gerke, P. Why d-Mannose May Be as Efficient as Antibiotics in the Treatment of Acute Uncomplicated Lower Urinary Tract Infections—Preliminary Considerations and Conclusions from a Non-Interventional Study. Antibiotics 2022, 11. [Google Scholar] [CrossRef]
- Möllenhoff, K.; Tresch, A. Investigating non-inferiority or equivalence in time-to-event data under non-proportional hazards. Lifetime Data Anal. 2023, 29, 483–507. [Google Scholar] [CrossRef] [PubMed]
- Hadidi, M.F.; Alhamami, N.; Alhakami, M.; Abdulhamid, A.S.; Alsharif, A.; Alomari, M.S.; Alghamdi, Y.A.; Alshehri, S.; Ghaddaf, A.A.; Alsenani, F.M.; et al. Antibiotics efficacy in clinical and microbiological cure of uncomplicated urinary tract infection: a systematic review and network meta-analysis. World Journal of Urology 2024, 42, 221. [Google Scholar] [CrossRef] [PubMed]
- Wagenlehner, F.M.; Abramov-Sommariva, D.; Höller, M.; Steindl, H.; Naber, K.G. Non-Antibiotic Herbal Therapy (BNO 1045) versus Antibiotic Therapy (Fosfomycin Trometamol) for the Treatment of Acute Lower Uncomplicated Urinary Tract Infections in Women: A Double-Blind, Parallel-Group, Randomized, Multicentre, Non-Inferiority Phase III Trial. Urol. Int. 2018, 101, 327–336. [Google Scholar]
- EMA / Committee for Medicinal Products for Human Use (CHMP). Guideline on the evaluation of medicinal products indicated for treatment of bacterial infections. 19 May 2022. CPMP/EWP/558/95 Rev 3. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-evaluation-medicinal-products-indicated-treatment-bacterial-infections-revision-3_en.pdf (accessed on 31 October 2024).
- Jansåker, F.; Thønnings, S.; Hertz, F.B.; Kallemose, T.; Værnet, J.; Bjerrum, L.; Benfield, T.; Frimodt-Møller, N.; Knudsen, J.D. Three versus five days of pivmecillinam for community-acquired uncomplicated lower urinary tract infection: A randomised, double-blind, placebo-controlled superiority trial. eClinicalMedicine 2019, 12, 62–69. [Google Scholar] [CrossRef]
- Alidjanov, J.F.; Naber, K.G.; Pilatz, A.; Radzhabov, A.; Zamuddinov, M.; Magyar, A.; Tenke, P.; Wagenlehner, F.M. Evaluation of the draft guidelines proposed by EMA and FDA for the clinical diagnosis of acute uncomplicated cystitis in women. World Journal of Urology 2020, 38, 63–72. [Google Scholar] [CrossRef]
- Alidjanov, J.F.; Naber, K.G.; Pilatz, A.; Radzhabov, A.; Zamuddinov, M.; Magyar, A.; Tenke, P.; Wagenlehner, F.M. Additional assessment of Acute Cystitis Symptom Score questionnaire for patient-reported outcome measure in female patients with acute uncomplicated cystitis: part II. World Journal of Urology 2020, 38, 1977–1988. [Google Scholar] [CrossRef]
- Schmiemann, G.; Gágyor, I.; Hummers-Pradier, E.; Bleidorn, J. Resistance profiles of urinary tract infections in general practice--an observational study. BMC Urol. 2012, 12, 33. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Recommendations to restrict use of fosfomycin antibiotics. Available online: https://www.ema.europa.eu/en/documents/referral/fosfomycin-article-31-referral-recommendations-restrict-use-fosfomycin-antibiotics_en.pdf (accessed on 31 October 2024).
- Alidjanov, J.F.; Pilatz, A.; Abdufattaev, U.A.; Wiltink, J.; Weidner, W.; Naber, K.G.; Wagenlehner, F. German validation of the Acute Cystitis Symptom Score. Urologe A 2015, 54, 1269–1276. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services - Food and Drug Administration. Non-Inferiority Clinical Trials to Establish Effectiveness - Guidance for Industry (FDA-2010-D-0075). Available online: https://www.fda.gov/media/78504/download (accessed on 25 December 2024).
- Bootstrap Methods and their Application; Davison, A.C., Hinkley, D.V., Eds.; Cambridge University Press: Cambridge, 1997; ISBN 9780521574716. [Google Scholar]
Figure 1.
Time course of clinical cure (CC) rates (main definition, i.e., ACSS Typical Domain Score ≤4 including all items) up to day 8 according to the per-protocol analysis (A) and the post hoc analysis after applying multiple imputation procedures (B). Markers indicate CC rate estimates, error bars indicate 95% CIs. Analyses were performed on the per-protocol set (PPS).
Figure 1.
Time course of clinical cure (CC) rates (main definition, i.e., ACSS Typical Domain Score ≤4 including all items) up to day 8 according to the per-protocol analysis (A) and the post hoc analysis after applying multiple imputation procedures (B). Markers indicate CC rate estimates, error bars indicate 95% CIs. Analyses were performed on the per-protocol set (PPS).
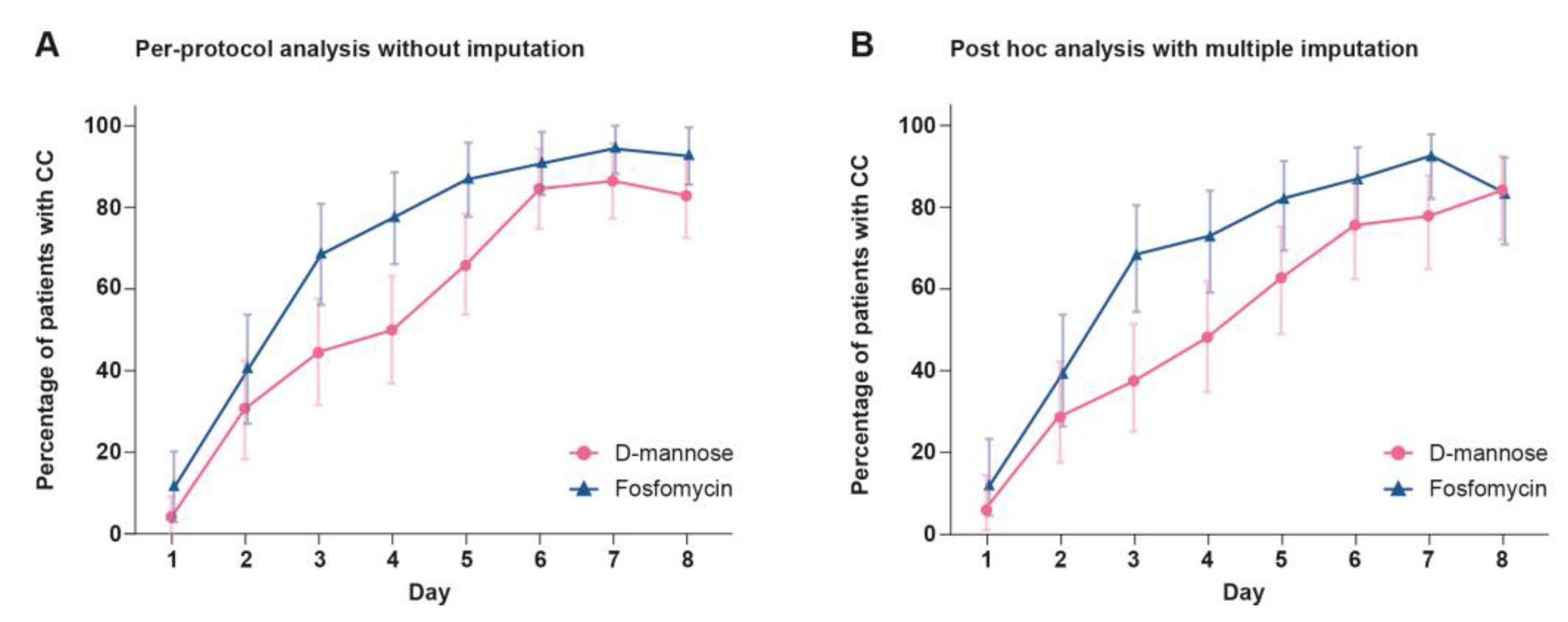
Figure 2.
Non-inferiority assessments for treatment differences in clinical cure (CC) from day 1 to day 8 in the per-protocol set (PPS) based on the per-protocol analysis of CC rates (A), based on the post hoc analyses of CC rates after multiple imputation (B), or based on the post hoc analyses of time to CC applying either Kaplan-Meier (KM) estimates (nonparametric Möllenhoff model) (C) or parametric estimators (parametric Möllenhoff model) (D). Red markers indicate point estimates of treatment differences, bars indicate 95% CI. The dashed line indicates the non-inferiority margin.
Figure 2.
Non-inferiority assessments for treatment differences in clinical cure (CC) from day 1 to day 8 in the per-protocol set (PPS) based on the per-protocol analysis of CC rates (A), based on the post hoc analyses of CC rates after multiple imputation (B), or based on the post hoc analyses of time to CC applying either Kaplan-Meier (KM) estimates (nonparametric Möllenhoff model) (C) or parametric estimators (parametric Möllenhoff model) (D). Red markers indicate point estimates of treatment differences, bars indicate 95% CI. The dashed line indicates the non-inferiority margin.
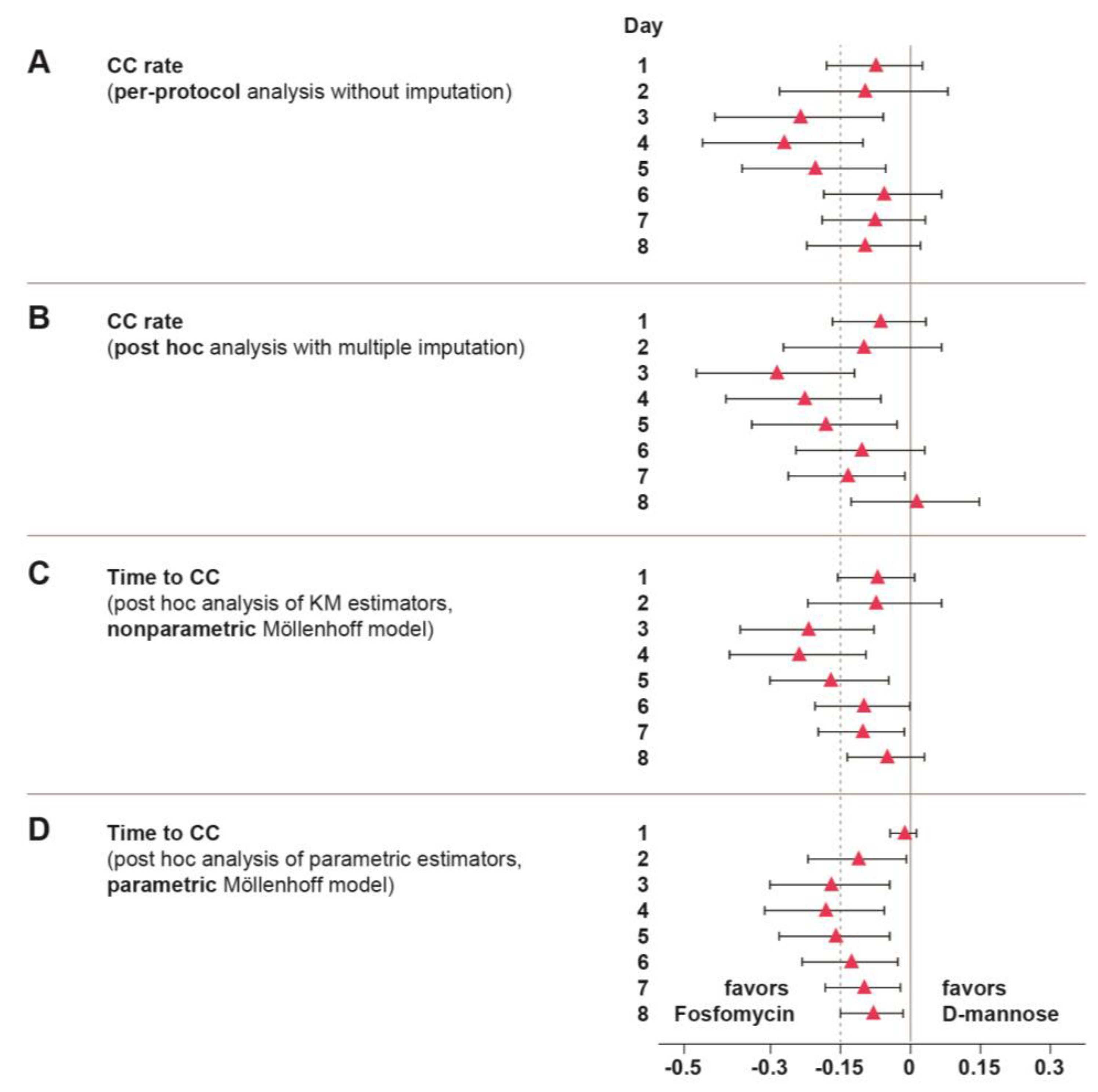
Figure 3.
Simulation of the sample sizes required to demonstrate non-inferiority for different treatments with regard to CC (main definition, i.e., ACSS Typical Domain Score ≤4 including all items). Non-inferiority estimates (M1) are presented by group sample sizes for day 8 based on the nonparametric Möllenhoff model and the parametric Möllenhoff model using study data from the per-protocol set (PPS). Markers indicate the M1 estimates. The dashed line (M1 predefined) indicates the pre-specified non-inferiority margin of 0.15.
Figure 3.
Simulation of the sample sizes required to demonstrate non-inferiority for different treatments with regard to CC (main definition, i.e., ACSS Typical Domain Score ≤4 including all items). Non-inferiority estimates (M1) are presented by group sample sizes for day 8 based on the nonparametric Möllenhoff model and the parametric Möllenhoff model using study data from the per-protocol set (PPS). Markers indicate the M1 estimates. The dashed line (M1 predefined) indicates the pre-specified non-inferiority margin of 0.15.
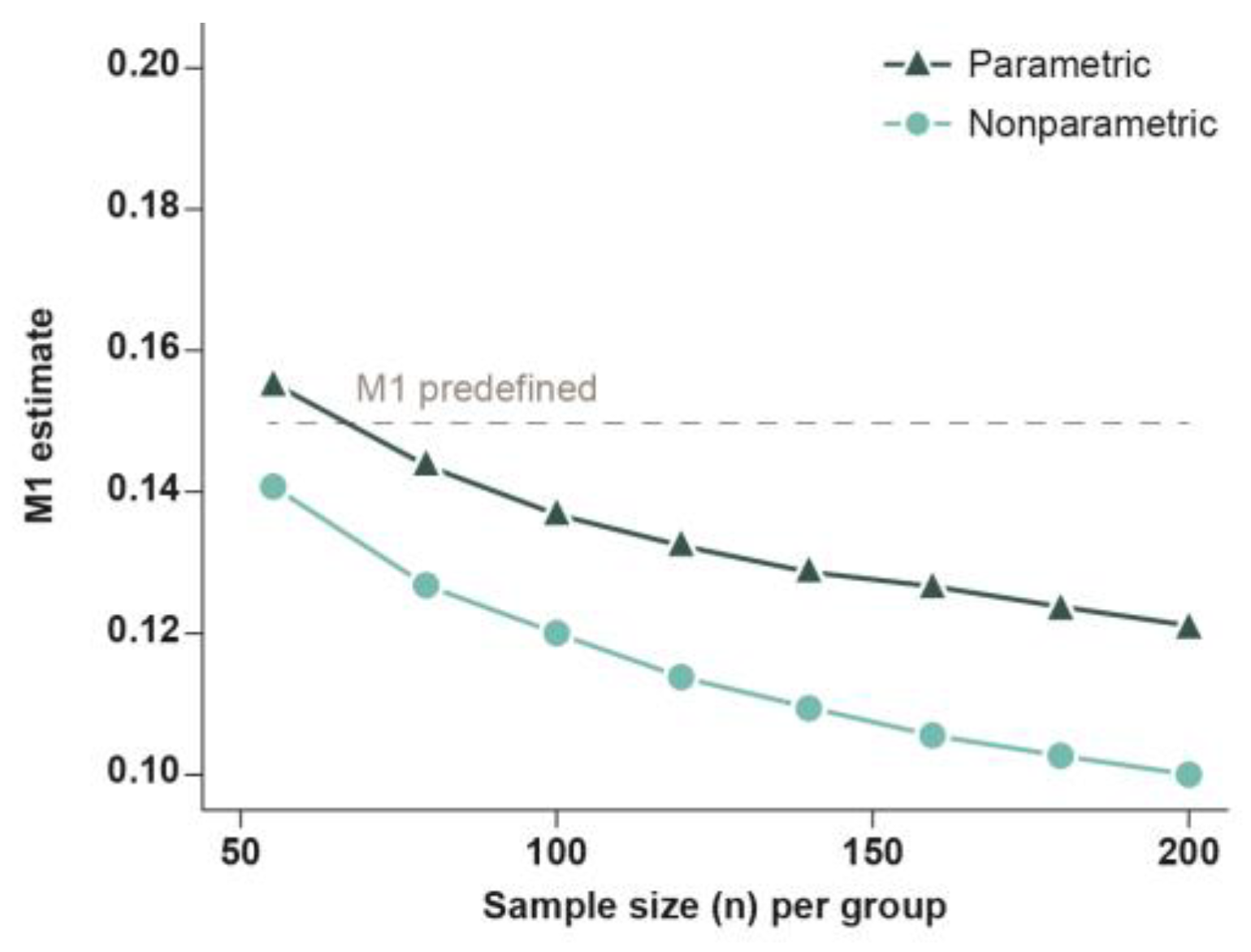
Figure 4.
Post hoc analysis of ACSS Typical Domain Score over time after multiple imputation in the per-protocol set (PPS). Boxes indicate 25% to 75% quartiles; lines indicate the medians. Whiskers are maximum 1.5 times the interquartile range (IQR) in length. Outliers (>1.5 × IQR) are indicated by colored circles.
Figure 4.
Post hoc analysis of ACSS Typical Domain Score over time after multiple imputation in the per-protocol set (PPS). Boxes indicate 25% to 75% quartiles; lines indicate the medians. Whiskers are maximum 1.5 times the interquartile range (IQR) in length. Outliers (>1.5 × IQR) are indicated by colored circles.
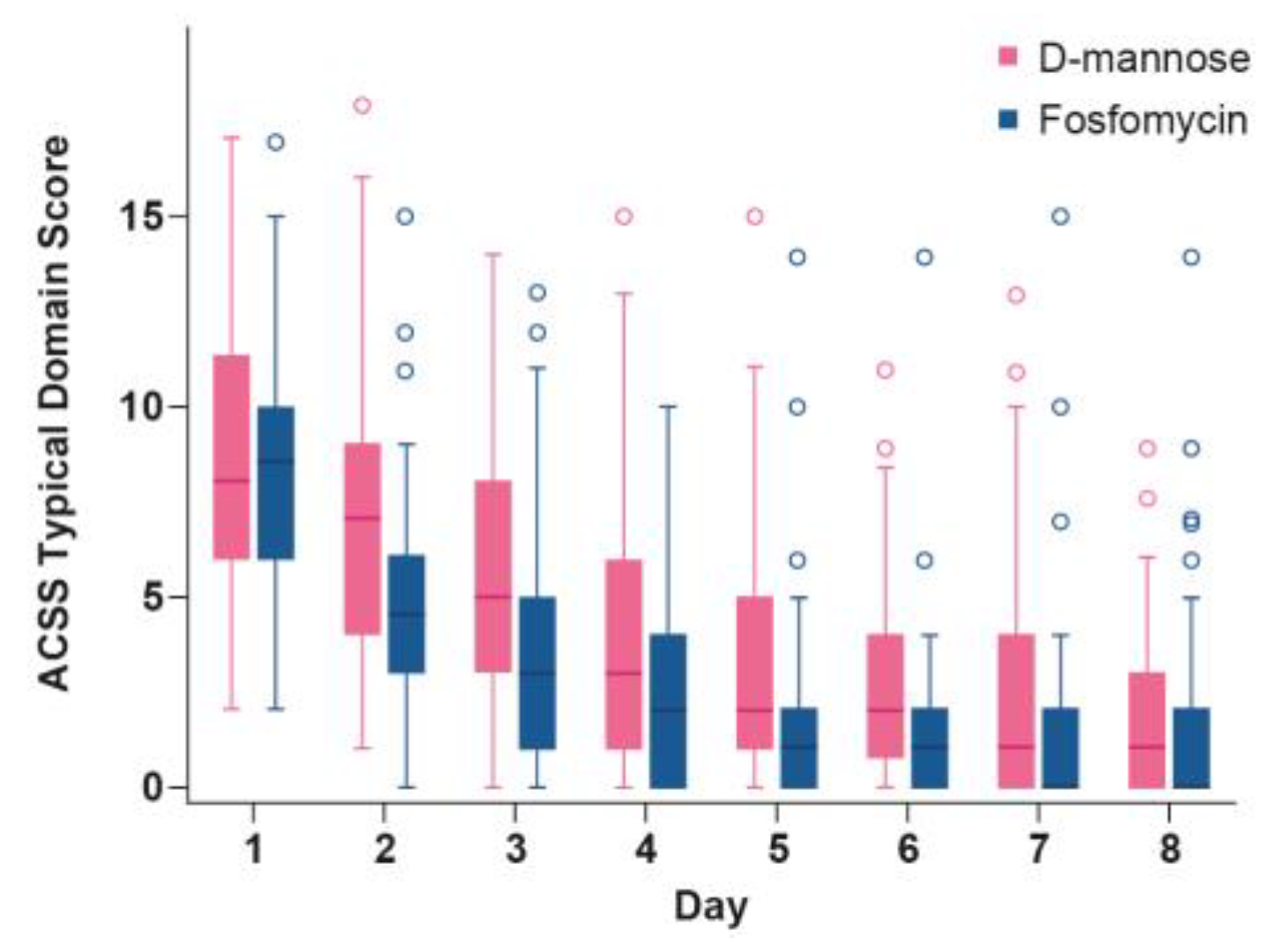
Figure 5.
Global assessment of tolerability on day 8 in the safety evaluation population (SEP). Missing data at visit 2 was imputed with the worst category ‘very poor’ in case of discontinuation due to intolerable AEs. All other missing data are summarized under the category ‘missing’.
Figure 5.
Global assessment of tolerability on day 8 in the safety evaluation population (SEP). Missing data at visit 2 was imputed with the worst category ‘very poor’ in case of discontinuation due to intolerable AEs. All other missing data are summarized under the category ‘missing’.
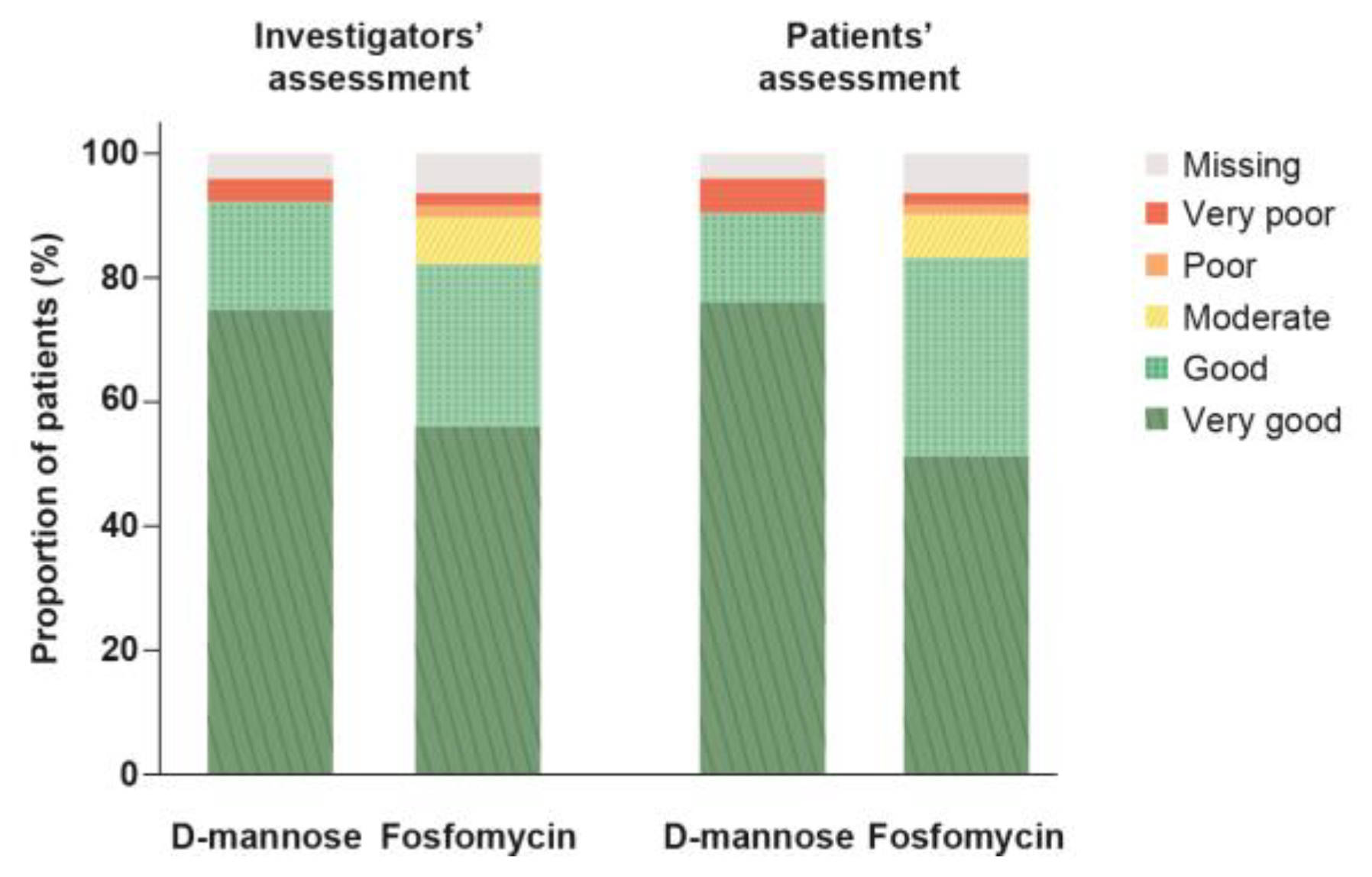

Table 1.
Descriptive presentation of patient demographic and clinical characteristics at baseline in the safety evaluation population (SEP) by treatment group.
Table 1.
Descriptive presentation of patient demographic and clinical characteristics at baseline in the safety evaluation population (SEP) by treatment group.
| D-mannose | Fosfomycin | Statistics | |
|---|---|---|---|
| N = 61 | N = 57 | p-value | |
| Age, years | |||
| Mean (SD) | 40.8 (13.9) | 41.5 (14.9) | p = 0.793b |
| Median | 40.0 | 41.0 | |
| Min–Max | 21–69 | 18–70 | |
| Ethnic origin | |||
| Caucasian, n (%) | 58 (95.1) | 57 (100.0) | p = 0.245c |
| Asian, n (%) | 3 (4.9) | 0 (0.0) | |
| BMI | |||
| Mean (SD) | 24.94 (4.66) | 25.56 (5.74) | p = 0.523b |
| Median | 23.46 | 23.44 | |
| Min–Max | 18.3–38.1 | 17.6–41.6 | |
| Positive urine culture for bacteria, n (%) | 36 (59.0) | 35 (61.4) | p = 0.852c |
| E. coli infection, n (%) | 28 (45.9) | 29 (50.9) | p = 0.713c |
| ACSS Typical Domain Scorea | |||
| Mean (SD) | 10.8 (3.0) | 10.2 (2.8) | p = 0.263b |
| Median | 11.0 | 10.0 | |
| Min–Max | 6–17 | 6–16 | |
|
Disease severity by category (ACSS Typical Domain Score)a |
|||
| Moderate (6–12), n (%) | 41 (67.2) | 44 (77.2) | p = 0.305c |
| Severe (>12), n (%) | 20 (32.8) | 13 (22.8) | p = 0.113d |
aThe ACSS Typical Domain Score can range from 0 to 18, bt-test, cFisher’s exact test, d(one-sided) test after arcsin(sqrt(x))-trafo for scores = ‘severe’. p-values <0.05 indicate statistically significant differences (none found).
Table 2.
Patients with treatment-emergent adverse events during the study in the safety evaluation population (SEP).
Table 2.
Patients with treatment-emergent adverse events during the study in the safety evaluation population (SEP).
| D-mannose | Fosfomycin | Statistics | |
|---|---|---|---|
| N = 61 | N = 57 | OR [95% CI]a; p-value | |
| Overview of patients with treatment-emergent AEs, n (%) | |||
| Any AEs during the study | 20 (32.8) | 26 (45.6) | 0.58 [0.26, 1.31]; p = 0.187 |
| AEs during the acute phase | 9 (14.8) | 16 (28.1) | 0.45 [0.16, 1.20]; p = 0.114 |
| SAEs | 0 (0.0) | 1 (1.8) | n.e. |
| Severe AEs | 0 (0.0) | 1 (1.8) | n.e. |
| AEs leading to treatment discontinuation | 2 (3.3) | 1 (1.8) | n.e. |
| AEs leading to study withdrawal | 2 (3.3) | 1 (1.8) | n.e. |
| AEs related to study device/drug | 6 (9.8) | 13 (22.8) | 0.37 [0.11, 1.15]; p = 0.079 |
| Patients with AEs by System Organ Class, n (%) | |||
| Gastrointestinal disorders | 6 (9.8) | 14 (24.6) | 0.34 [0.10, 1.03]; p = 0.048 |
| General disorders and administration site conditions | 2 (3.3) | 0 (0.0) | n.e. |
| Infections and infestations | 8 (13.1) | 7 (12.3) | 1.08 [0.32, 3.77]; p = 1.0 |
| Metabolism and nutrition disorders | 0 (0.0) | 1 (1.8) | n.e. |
| Musculoskeletal and connective tissue disorders | 2 (3.3) | 0 (0.0) | n.e. |
| Nervous system disorders | 6 (9.8) | 8 (14.0) | 0.67 [0.18, 2.38]; p = 0.574 |
| Reproductive system and breast disorders | 1 (1.6) | 1 (1.8) | n.e. |
| Respiratory, thoracic, and mediastinal disorders | 0 (0.0) | 2 (3.5) | n.e. |
aexact Fisher-test (OR = odds ratio estimate and 95% CI; p). n.e. (not evaluable) denotes data with totals less than or equal to 3. p-values < 0.05 indicate statistical significance (highlighted in bold).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



