
Submitted:
30 June 2025
Posted:
01 July 2025
You are already at the latest version
Abstract
Background/Objectives: Commonly characterized by limited metastatic sites, low tumor burden has been associated with favorable patient outcomes in various malignancies. However, its prognostic relevance in avelumab maintenance therapy for advanced urothelial carcinoma (UC) remains incompletely defined. Methods: We retrospectively analyzed 26 patients with advanced UC who received avelumab maintenance therapy following disease control with first-line platinum-based chemotherapy between March 2021 and May 2025. Patients were categorized by their metastatic pattern at chemotherapy initiation: lymph node-only (as a surrogate for low tumor burden), non-visceral (excluding visceral organ involvement, but including bone), or visceral disease. Survival outcomes were assessed using the Kaplan–Meier method. Results: Among the cohort, 46.2% had lymph node-only metastasis and 57.7% had non-visceral disease. The median progression-free survival (PFS) and overall survival (OS) from the start of avelumab were 5.6 months and 21.7 months, respectively. OS from the initiation of platinum-based chemotherapy was 28.7 months. Patients with lymph node-only metastasis demonstrated significantly longer OS from chemotherapy initiation compared with those with other metastatic patterns (41.1 vs. 22.9 months, P = 0.044). However, the PFS and OS from avelumab initiation did not significantly differ. No survival benefit was observed for patients with non-visceral disease compared with those with visceral metastases. Conclusions: Lymph node-only metastasis, representing low tumor burden, was associated with significantly improved long-term survival in advanced UC patients undergoing avelumab maintenance following chemotherapy. These findings support the clinical utility of baseline tumor burden and metastatic pattern in risk stratification and shared decision-making for maintenance therapy in advanced UC.
Keywords:
urothelial carcinoma
; avelumab
; maintenance therapy
; low tumor burden
; lymph node metastasis
; visceral metastasis
; platinum-based chemotherapy
; prognostic factor
Introduction
The treatment landscape for advanced urothelial carcinoma (UC), including both locally advanced and metastatic disease, has evolved substantially in recent years, with multiple therapeutic options now available. According to the National Comprehensive Cancer Network guidelines, several combination regimens are currently recommended as category 1 options for systemic therapy in advanced UC cases [1]. Enfortumab vedotin (EV) in combination with pembrolizumab is listed as the preferred first-line regimen [2]. Additionally, the triplet regimen of gemcitabine, cisplatin, and nivolumab followed by nivolumab maintenance is recommended as an alternative [3]. Furthermore, the previous approach, gemcitabine and cisplatin followed by avelumab maintenance, continues to be endorsed as a category 1 regimen [4]. All three regimens are supported by the highest level of clinical evidence. Although all three regimens are supported by the highest level of clinical evidence, the optimal selection of patients for each treatment strategy remains unclear. These regimens differ in both efficacy and safety profiles, necessitating individualized treatment decisions based on various clinical factors such as performance status, renal function, comorbidities, and patient preferences. Accordingly, determining the most appropriate regimen in real-world clinical practice remains a significant challenge [5].
While these developments have expanded the treatment choices for UC, the clinical significance of metastatic distribution at the time of treatment initiation, such as lymph node-only or non-visceral disease, remains incompletely defined. In particular, avelumab has been established as a switch maintenance option for patients without disease progression after platinum-based chemotherapy, yet its efficacy in distinct metastatic patient subgroups has not been fully characterized in real-world practice.
In this study, we retrospectively examined the outcomes of avelumab maintenance therapy in patients with advanced UC, with a particular focus on the prognostic implications of metastatic distribution at baseline. To support more individualized treatment strategies under shared decision-making, we aimed to clarify whether the presence of lymph node-only or non-visceral metastases could influence survival outcomes in these patients.
Patients and Methods
Patient Population
We retrospectively identified 26 consecutive patients with advanced UC (either locally advanced or metastatic) who received avelumab as maintenance therapy following first-line platinum-based chemotherapy without evidence of disease progression between March 2021 and May 2025 at Kyushu Cancer Center, Japan.
Avelumab was administered intravenously at a dosage of 10 mg/kg every two weeks, which was continued until radiologic or clinical disease progression or the development of unacceptable toxicity, in accordance with previously established protocols [4,6]. No study-specific procedures or additional clinical assessments were mandated. Patients were monitored as per routine clinical practice, with follow-up schedules determined at the discretion of the treating physician [7]. The best response to platinum-based chemotherapy and avelumab treatment was evaluated by assessing the tumor response according to the Response Evaluation Criteria in Solid Tumors, version 1.1 [8]. Clinical data were extracted from each patient’s electronic medical records.
In this study, lymph node-only metastasis was defined as the involvement of lymph nodes, irrespective of the presence or absence of residual primary tumors in the urinary tract. Non-visceral metastasis was defined as the absence of metastases to visceral organs, not considering bone metastasis. This definition was applied because the cohort excluding patients with lymph node-only metastasis overlapped entirely with the group categorized as having visceral metastases when bone lesions were considered part of visceral spread.
This study was conducted with approval from the Institutional Review Board of the National Hospital Organization Kyushu Cancer Center (approval number: 2014-99) and complied with the principles outlined in the Declaration of Helsinki. Because of the retrospective design of this study, informed consent was obtained through an opt-out approach.
Statistical Analysis
All statistical analyses were performed using EZR version 1.40 (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria) [9]. Progression-free survival (PFS) was defined as the interval from treatment initiation to the date of investigator-assessed clinical and/or radiographic disease progression. Overall survival (OS) was defined as the interval from treatment initiation to the date of death from any cause. Survival outcomes were estimated using the Kaplan–Meier method. Patients who had not experienced an event were censored at the date of last follow-up. A two-sided P-value < 0.05 was considered statistically significant.Results
Patient Characteristics
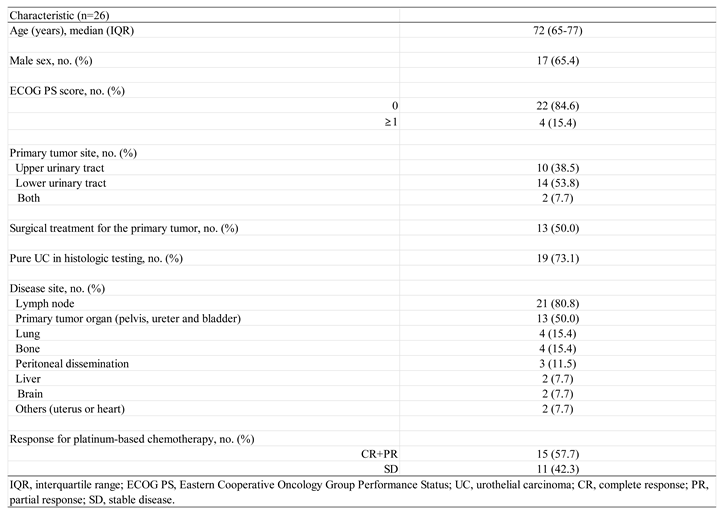
The baseline characteristics of the patients at the initiation of first-line platinum-based chemotherapy are summarized in Table 1. All 26 patients with advanced UC who demonstrated no disease progression after platinum-based chemotherapy proceeded to receive avelumab maintenance therapy.
The median age was 72 years (interquartile range (IQR), 65–77), with 17 male patients (65.4%). The Eastern Cooperative Oncology Group (ECOG) performance status was 0 in 22 patients (84.6%). Histopathological examination revealed pure UC in 19 patients (73.1%). Primary tumor resection had been performed in 13 patients (50.0%). The most common metastatic site was the lymph nodes, followed by the lungs, bones, peritoneum, liver, and brain. Residual primary tumors were present in half of the cohort.
Using the study-specific definitions, 12 patients (46.2%) had lymph node-only metastasis and 15 patients (57.7%) were categorized as having non-visceral metastasis.
Efficacy in the Overall Cohort
The median follow-up duration from the initiation of platinum-based chemotherapy was 16.2 months (IQR, 7.4–24.9). At the time of analysis, five patients (19.2%) remained on avelumab maintenance therapy, while 14 patients (53.8%) had died during follow-up.
The median PFS and OS from the start of avelumab maintenance were 5.6 months (95% confidence interval [CI], 2.2–6.8) and 21.7 months (95% CI, 13.3–35.1), respectively (Figure 1 and Figure 2). Additionally, the median OS measured from the initiation of first-line platinum-based chemotherapy was 28.7 months (95% CI, 16.6–41.1) (Figure 3).
Efficacy in Patients with Lymph Node-Only Metastasis and Non-Visceral Metastasis
The log-rank test revealed no statistically significant difference in PFS from the initiation of avelumab maintenance therapy between patients with lymph node-only metastasis and those with other metastatic sites (6.5 vs. 2.6 months, P = 0.118) (Figure 4). Similarly, OS from the start of avelumab therapy did not significantly differ between the two groups (35.1 vs. 17.0 months, P = 0.062) (Figure 5). However, when OS was calculated from the initiation of first-line platinum-based chemotherapy, the patients with lymph node-only metastasis had significantly longer survival than those with other metastatic patterns (41.1 vs. 22.9 months, P = 0.044) (Figure 6).
The log-rank test also showed no significant difference in PFS from the initiation of avelumab maintenance between patients with non-visceral and visceral metastases (6.2 vs. 2.6 months, P = 0.158) (Figure 7). Likewise, OS from the start of avelumab therapy was not significantly different between these groups (23.4 vs. 14.4 months, P = 0.165) (Figure 8). When OS was measured from the initiation of first-line platinum-based chemotherapy, no significant difference was observed between patients with non-visceral and visceral metastases (29.0 vs. 28.7 months, P = 0.113) (Figure 9).
Discussion
This retrospective study evaluated the efficacy of avelumab maintenance therapy in patients with advanced UC, focusing on those with lymph node-only or non-visceral metastases at the initiation of platinum-based chemotherapy. This subgroup was selected because avelumab is used as switch maintenance therapy in patients without disease progression after first-line treatment, and both patients and physicians often consider metastatic status when choosing a treatment strategy before initiating systemic therapy [10]. Our results demonstrated that patients with lymph node-only metastasis, regardless of the presence of residual primary tumors, had significantly longer OS when measured from the initiation of platinum-based chemotherapy compared with those with other metastatic patterns. However, PFS and OS from the start of avelumab maintenance did not significantly differ between the groups. Additionally, patients with non-visceral metastases, including bone involvement, did not show a clear survival advantage over those with visceral disease. These findings were consistent across all endpoints evaluated: PFS and OS from the start of avelumab and OS from the start of first-line chemotherapy.
The era of shared decision-making has become increasingly feasible, even for patients with advanced UC, as the expansion of therapeutic options now empowers patients to actively participate in treatment selection. Under this model, clinical decisions should incorporate not only efficacy and safety data, but also an individualized assessment of the patient’s circumstances, such as lifestyle, occupational responsibilities, treatment schedule preferences, financial burden, and personal goals of care [11]. Importantly, the ultimate therapeutic goal is to achieve meaningful clinical benefit while minimizing treatment-related toxicity. In certain cases, it may be preferable to choose a regimen with a more favorable safety profile, even if it does not demonstrate the highest objective response rate reported in trials. If comparable survival outcomes can be achieved with fewer adverse events, such strategies may benefit both patients and physicians responsible for managing treatment toxicity. This patient-centered perspective emphasizes the importance of balancing efficacy and quality of life, particularly in the long-term management of advanced malignancies.
The concept of low tumor burden is increasingly recognized as a clinically relevant prognostic and predictive factor across urologic malignancies. However, its definition and significance vary depending on the tumor type, biological behavior, and treatment context, even within the urologic oncology field [4,12,13]. In advanced UC, low tumor burden is most commonly defined qualitatively, including with lymph node-only metastasis, non-visceral metastasis, or a limited number of metastatic sites. These features are generally considered surrogate markers of a less aggressive disease phenotype and are associated with improved outcomes [4,12,15,16,17].
In the evolving treatment landscape of advanced UC, two pivotal trials, JAVELIN Bladder 100 and EV-302, have demonstrated the efficacy of novel regimens in distinct clinical settings. In the JAVELIN Bladder 100 trial, avelumab maintenance following first-line platinum-based chemotherapy achieved a median OS of 23.8 months [18]. Notably, the outcomes were even more favorable in patients with lymph node-only metastasis, with a median OS of 31.9 months and median PFS of 8.7 months [19]. The regimen was well tolerated, with grade ≥ 3 treatment-related adverse events (TRAEs) observed in 47.4% and treatment discontinuation in only 11.9% of patients [4]. In contrast, the EV-302 trial evaluated EV plus pembrolizumab as first-line therapy, reporting a median OS of 33.8 months in the overall cohort. The outcomes were particularly favorable among patients with lymph node-only metastasis, with a median PFS of 22.1 months and median OS not reached at the data cutoff (median follow-up: 29.1 months) [20]. However, toxicity was more pronounced in this trial, with grade ≥ 3 TRAEs in 67.5% and treatment discontinuation in 35.1% of patients [2].
Our retrospective analysis supports these findings. Among the patients treated with avelumab maintenance, those with lymph node-only metastasis achieved a median OS of 41.1 months from the start of platinum-based chemotherapy. While PFS and OS from the initiation of avelumab were not significantly different compared with those with other metastases, the extended OS in the lymph node-only group suggests durable disease control with a less intensive regimen. Taken together, these results reinforce lymph node-only metastasis as a favorable-risk characteristic, associated with excellent long-term outcomes. While EV plus pembrolizumab offers substantial clinical benefit, the higher toxicity profile may limit its use in certain populations. For appropriately selected patients, such as those with low tumor burden, good performance status, and lymph node-only disease, avelumab maintenance remains a compelling and less toxic alternative, especially within the framework of shared decision-making.
The definition of “visceral” remains ambiguous in clinical oncology. According to the National Cancer Institute’s Dictionary of Cancer Terms, “visceral” refers to the viscera, the soft internal organs of the body, including the lungs, heart, and organs of the digestive, excretory, reproductive, and circulatory systems [21]. However, in the context of metastatic UC, the classification of metastatic sites as “visceral” is not standardized across clinical trials or retrospective studies. This inconsistency complicates the interpretation of subgroup analyses and application of clinical trial data to real-world settings. In the JAVELIN Bladder 100 trial, the patients were stratified by metastatic site at the initiation of first-line platinum-based chemotherapy, distinguishing between visceral and non-visceral disease. In that trial, non-visceral disease included locally advanced tumors, lymph node-only metastases, and bone metastases [19]. In contrast, the EV-302 trial, which evaluated EV plus pembrolizumab in previously untreated advanced UC cases, classified bone metastases as visceral involvement [2]. These differing definitions have important implications for how efficacy outcomes are interpreted across studies, as well as how treatment strategies are formulated in clinical practice. In our study, we adopted a definition consistent with that used in the JAVELIN Bladder 100 trial, classifying bone metastases as non-visceral. This approach was chosen because when the patients with lymph node-only metastasis were excluded, this group completely overlapped with those categorized as having visceral metastases when bone lesions were considered visceral, which would have confounded subgroup distinction. This approach allowed for a more direct comparison with prior avelumab-based data and enabled a clearer analysis of the prognostic relevance of lymph node-only disease. However, the variation in definitions across studies underscores the urgent need for a consensus in classifying UC metastatic patterns, especially as treatment paradigms continue to evolve.
Visceral metastasis has long been recognized as an indicator of poor prognosis in multiple malignancies. However, the term “visceral” is inconsistently applied, sometimes restricted to parenchymal organs, such as the liver or lung, and at other times broadened to encompass bone because of its uniformly adverse prognostic impact. Indeed, bone metastases are consistently associated with inferior survival in a range of solid tumors, including breast, lung, and prostate cancers, as well as renal cell carcinoma and UC [22,23,24,25]. In UC specifically, bone involvement has been shown to be an independent predictor of shorter OS when compared with other metastatic sites [25,26,27]. Accordingly, when visceral disease is employed as a surrogate for high-risk biology, it is reasonable, particularly in UC, to classify bone metastasis as visceral on the basis of its established prognostic significance. Alternatively, a simpler and clinically intuitive approach, dichotomizing patients into “lymph-node-only” and “all other metastases” (encompassing both bone and visceral sites) groups, may yield sharper prognostic discrimination and thereby better guide therapeutic decision-making.
This study has several limitations that should be acknowledged. First, its retrospective design and single-center setting inherently introduce potential biases in patient selection, clinical management, and data interpretation. Second, the small sample size limits the statistical power to detect subtle differences between subgroups, particularly in analyses comparing non-visceral and visceral metastases. Third, our classification of metastatic sites, particularly the designation of bone metastases as non-visceral, was based on definitions used in prior studies, such as the JAVELIN Bladder 100 trial. However, the lack of a universally accepted definition of “visceral metastasis” complicates comparisons across studies and may limit the generalizability of our findings. Despite these limitations, our results offer meaningful real-world insights into the prognostic relevance of metastatic distribution, especially the favorable outcomes associated with lymph node-only disease, in UC patients receiving avelumab maintenance therapy.
Conclusions
This study suggests that UC patients with lymph node-only metastasis have a more favorable prognosis when treated with avelumab maintenance following platinum-based chemotherapy. While PFS and OS during avelumab therapy did not significantly differ, OS from first-line treatment was notably longer in the lymph node-only metastasis subgroup. These findings support the value of metastatic distribution, especially lymph node-only disease, as a prognostic factor in guiding maintenance treatment strategies for UC.
Author Contributions
Study concept and design: N.F., M.N. and T.N.; acquisition of data: N.F., J.T., A.T., S.N., M.N., and N.T.; statistical analysis: N.F. and T.N.; analysis and interpretation of data: all authors; drafting of the original manuscript: N.F., M.N., and T.N.; critical revision of the manuscript for important intellectual content: all authors; supervision: M.N. and T.N. All authors have read and approved the final version of the manuscript.
Funding
No funding was received.
Institutional Review Board Statement
The present study was approved by the Institutional Review Board of National Hospital Organization Kyushu Cancer Center (approval number: 2014-99).
Informed Consent Statement
The need to obtain informed consent was waived because of the retrospective design. However, the ability to opt-out was provided through the websites of all participating institutions.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We thank J. Iacona, Ph.D., from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Conflicts of Interest
The authors declare that they have no conflict of interest for this study.
References
- National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology: Bladder Cancer; Version 1.2025. Available online: https://www.nccn.org/professionals/physician_gls/pdf/bladder.pdf (accessed on 1 June 2025).
- Powles, T.; Valderrama, B.P.; Gupta, S.; Bedke, J.; Kikuchi, E.; Hoffman-Censits, J.; Iyer, G.; Vulsteke, C.; Park, S.H.; Shin, S.J.; et al. Enfortumab vedotin and pembrolizumab in untreated advanced urothelial cancer. N. Engl. J. Med. 2024, 390, 875–888. [Google Scholar] [CrossRef] [PubMed]
- van der Heijden, M.S.; Sonpavde, G.; Powles, T.; Necchi, A.; Burotto, M.; Schenker, M.; Sade, J.P.; Bamias, A.; Beuzeboc, P.; Bedke, J.; et al. Nivolumab plus gemcitabine–cisplatin in advanced urothelial carcinoma. N. Engl. J. Med. 2023, 389, 1778–1789. [Google Scholar] [CrossRef]
- Powles, T.; Park, S.H.; Voog, E.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Kalofonos, H.; Radulović, S.; Demey, W.; Ullén, A.; et al. Avelumab maintenance therapy for advanced or metastatic urothelial carcinoma. N. Engl. J. Med. 2020, 383, 1218–1230. [Google Scholar] [CrossRef]
- Grande, E.; Hussain, S.A.; Barthélémy, P.; Kanesvaran, R.; Giannatempo, P.; Benjamin, D.J.; Hoffman, J.; Birtle, A. Individualizing first-line treatment for advanced urothelial carcinoma: A favorable dilemma for patients and physicians. Cancer Treat Rev. 2025, 134, 102900. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Park, S.H.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Ullén, A.; Loriot, Y.; Sridhar, S.S.; Sternberg, C.N.; Bellmunt, J.; et al. Avelumab first-line maintenance for advanced urothelial carcinoma: Results from the JAVELIN Bladder 100 trial after ≥2 years of follow-up. J. Clin. Oncol. 2023, 41, 3486–3492. [Google Scholar] [CrossRef]
- Furubayashi, N.; Minato, A.; Tomoda, T.; Hori, Y.; Kiyoshima, K.; Negishi, T.; Haraguchi, Y.; Koga, T.; Kuroiwa, K.; Fujimoto, N.; et al. Organ-specific tumor response to avelumab maintenance therapy for advanced urothelial carcinoma: A multicenter retrospective study. Anticancer Res. 2023, 43, 5689–5698. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur J Cancer. 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Grivas, P.; Huber, C.; Pawar, V.; Roach, M.; May, S.G.; Desai, I.; Chang, J.; Bharmal, M. Management of Patients With Advanced Urothelial Carcinoma in an Evolving Treatment Landscape: A Qualitative Study of Provider Perspectives of First-Line Therapies. Clin Genitourin Cancer. 2022, 20, 114–122. [Google Scholar] [CrossRef]
- Elwyn, G.; Frosch, D.; Thomson, R.; Joseph-Williams, N.; Lloyd, A.; Kinnersley, P.; Cording, E.; Tomson, D.; Dodd, C.; Rollnick, S.; et al. Shared decision making: A model for clinical practice. J. Gen. Intern. Med. 2012, 27, 1361–1367. [Google Scholar] [CrossRef]
- Shiota, M.; Terada, N.; Saito, T.; Yokomizo, A.; Kohei, N.; Goto, T.; Kawamura, S.; Hashimoto, Y.; Takahashi, A.; Kimura, T.; et al. Differential prognostic factors in low- and high-burden de novo metastatic hormone-sensitive prostate cancer patients. Cancer Sci. 2021, 112, 1524–1533. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Arén Frontera, O.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthélémy, P.; Porta, C.; George, S.; et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N Engl J Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef]
- Sweeney, C.J.; Chen, Y.-H.; Carducci, M.; Liu, G.; Jarrard, D.F.; Eisenberger, M.; Wong, Y.-N.; Hahn, N.; Kohli, M.; Cooney, M.M.; et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N Engl J Med. 2015, 373, 737–746. [Google Scholar] [CrossRef]
- Barthélémy, P.; Loriot, Y.; Thibault, C.; Fléchon, A.; Voog, E.; Eymard, J.C.; Simon, C.; Gross-Goupil, M.; et al. AVENANCE real-world study of avelumab first-line maintenance treatment for advanced urothelial carcinoma: Analyses in low tumor burden subgroups. J Clin Oncol. [CrossRef]
- Bellmunt, J.; Théodore, C.; Demkov, T.; Komyakov, B.; Sengelov, L.; Daugaard, G.; Caty, A.; Carles, J.; Jagiello-Gruszfeld, A.; Karyakin, O.; et al. Phase III trial of vinflunine plus best supportive care compared with best supportive care alone after a platinum-containing regimen in patients with advanced transitional cell carcinoma of the urothelial tract. J Clin Oncol. 2009, 27, 4454–4461. [Google Scholar] [CrossRef] [PubMed]
- Thorsteinsson, K.; Brandt, S.B.; Jensen, J.B. Patients with metastatic or locally advanced bladder cancer not undergoing systemic oncological treatment—Characteristics and long-term outcome in a single-center Danish cohort. Cancers (Basel). 2025, 17, 1105. [Google Scholar] [CrossRef] [PubMed]
- Grivas, P.; Grande, E.; Davis, I.D.; Moon, H.H.; Grimm, M.-O.; Gupta, S.; Barthélémy, P.; Thibault, C.; Guenther, S.; Hanson, S.; et al. Avelumab first-line maintenance treatment for advanced urothelial carcinoma: Review of evidence to guide clinical practice. ESMO Open. 2023, 8, 102050. [Google Scholar] [CrossRef]
- Bellmunt, J.; Powles, T.; Park, S.H.; Voog, E.; Valderrama, B.P.; Gurney, H.; Ullén, A.; Loriot, Y.; Sridhar, S.S.; Tsuchiya, N.; et al. Avelumab first-line maintenance for advanced urothelial carcinoma: Long-term outcomes from the JAVELIN Bladder 100 trial in patients with nonvisceral or lymph node-only disease. Eur Urol. 0302. [Google Scholar] [CrossRef]
- Available online: https://ascopubs.org/doi/10.1200/JCO.2025.43.5_suppl.664 (accessed on 1 June 2025).
- Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/visceral (accessed on 1 June 2025).
- Zhang, J.; Cai, D.; Hong, S. Prevalence and prognosis of bone metastases in common solid cancers at initial diagnosis: A population-based study. BMJ Open. 2023, 13, e069908. [Google Scholar] [CrossRef]
- Makrakis, D.; Talukder, R.; Lin, G.I.; Diamantopoulos, L.N.; Dawsey, S.; Gupta, S.; Carril-Ajuria, L.; Castellano, D.; de Kouchkovsky, I.; Koshkin, V.S.; et al. Association Between Sites of Metastasis and Outcomes With Immune Checkpoint Inhibitors in Advanced Urothelial Carcinoma. Clin. Genitourin. Cancer. 2022, 20, e440–e452. [Google Scholar] [CrossRef]
- Ruatta, F.; Derosa, L.; Escudier, B.; Colomba, E.; Guida, A.; Baciarello, G.; Loriot, Y.; Fizazi, K.; Albiges, L. Prognosis of renal cell carcinoma with bone metastases: Experience from a large cancer centre. Eur. J. Cancer. 2019, 107, 79–85. [Google Scholar] [CrossRef]
- Stellato, M.; Santini, D.; Cursano, M.C.; Foderaro, S.; Tonini, G.; Procopio, G. Bone metastases from urothelial carcinoma: The dark side of the moon. J Bone Oncol. 2021, 31, 100405. [Google Scholar] [CrossRef]
- Huang, Y.; Xie, C.; Li, Q.; Huang, X.; Huang, W.; Yin, D. Prognostic factors and nomogram for the overall survival of bladder cancer bone metastasis: A SEER-based study. Medicine (Baltimore). 2023, 102, e33275. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Gu, H.; Zhang, D.; Wen, M.; Yan, Z.; Song, B.; Xie, C. Establishment and validation of a nomogram for predicting overall survival of upper-tract urothelial carcinoma with bone metastasis: A population-based study. BMC Urol. 2024, 24, 100. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Progression-free survival from the start of avelumab maintenance therapy in the overall study population of advanced urothelial carcinoma patients.
Figure 1.
Progression-free survival from the start of avelumab maintenance therapy in the overall study population of advanced urothelial carcinoma patients.
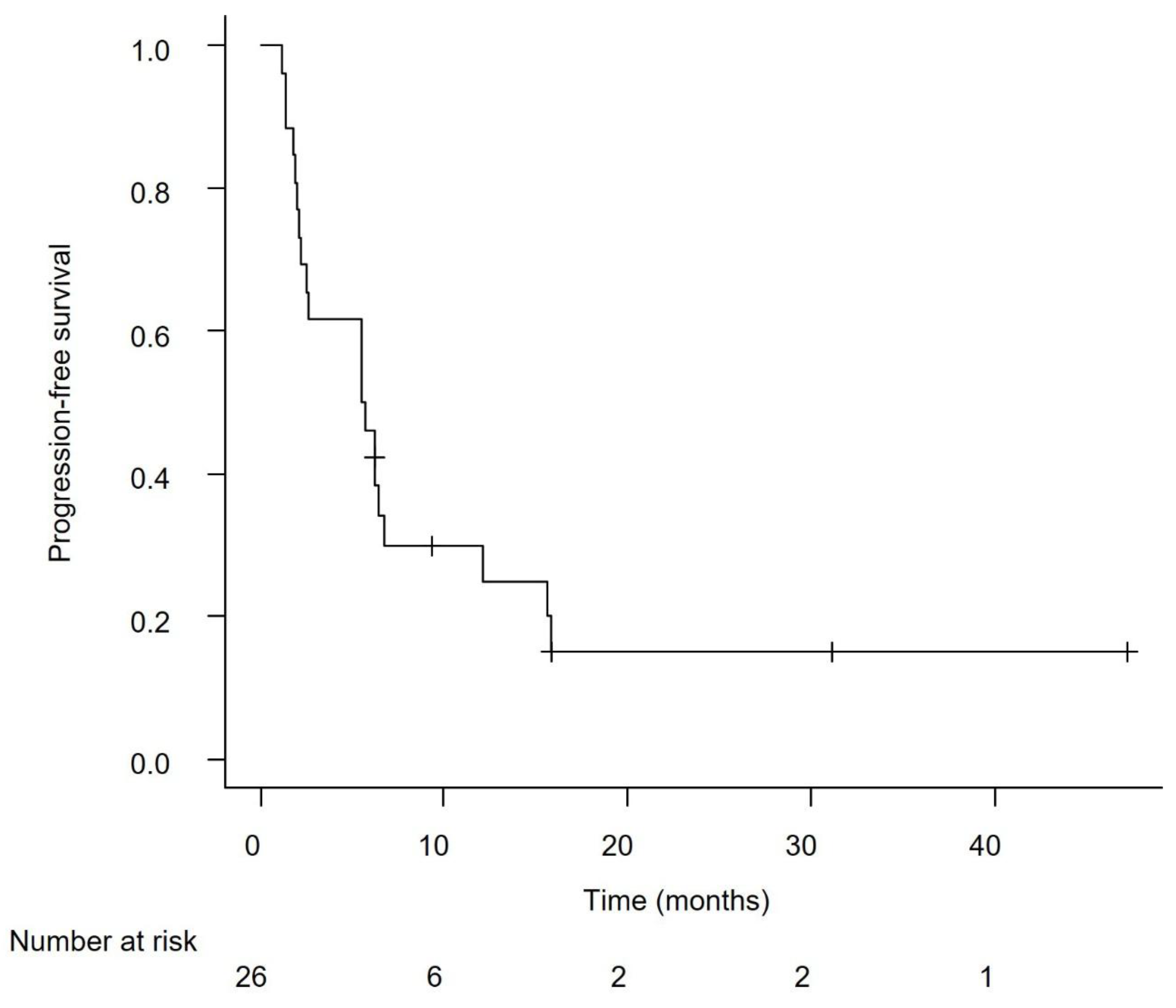
Figure 2.
Overall survival from the start of avelumab maintenance therapy in the overall study population of advanced urothelial carcinoma patients.
Figure 2.
Overall survival from the start of avelumab maintenance therapy in the overall study population of advanced urothelial carcinoma patients.
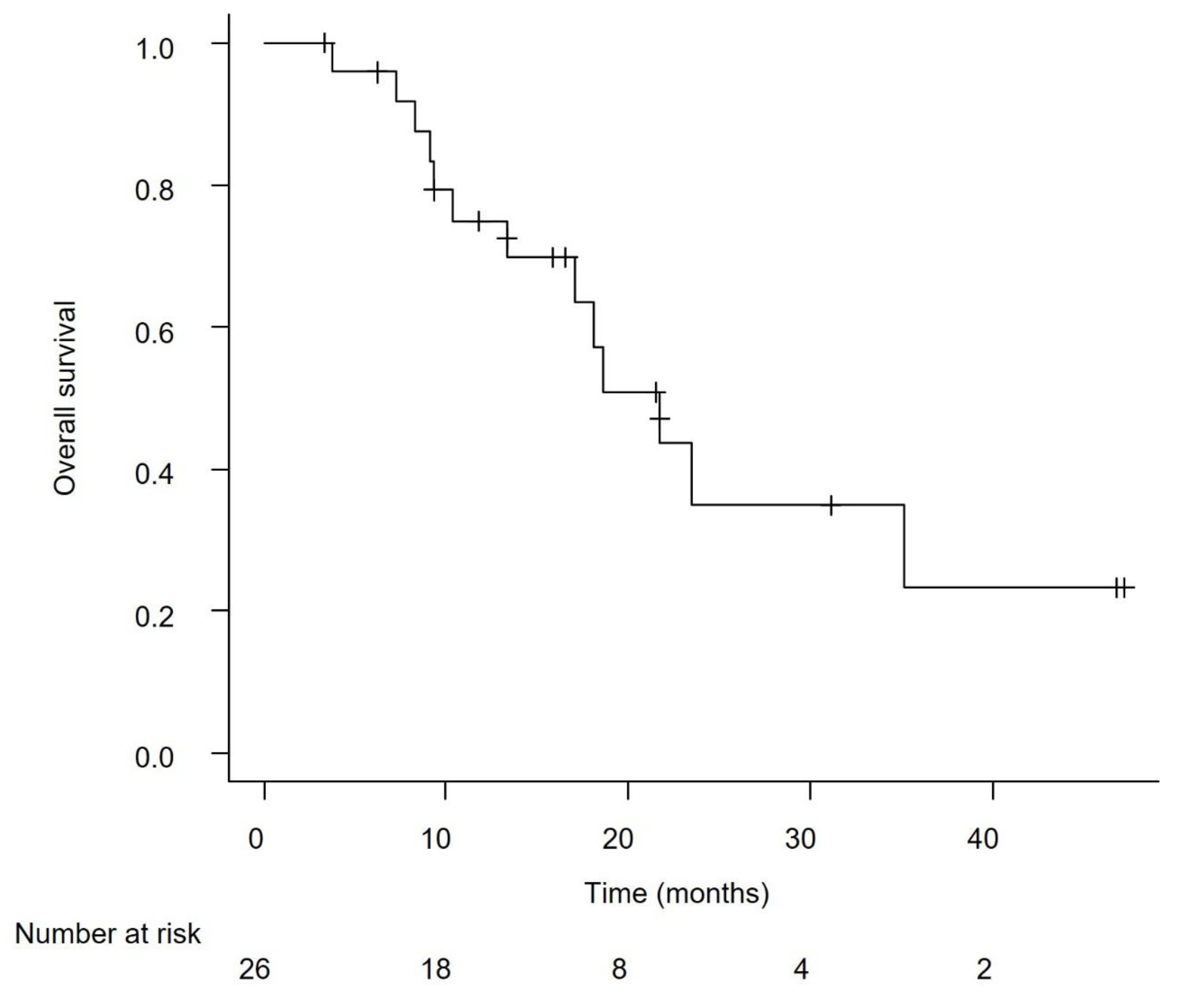
Figure 3.
Overall survival from the initiation of first-line platinum-based chemotherapy in the overall study population of advanced urothelial carcinoma patients.
Figure 3.
Overall survival from the initiation of first-line platinum-based chemotherapy in the overall study population of advanced urothelial carcinoma patients.
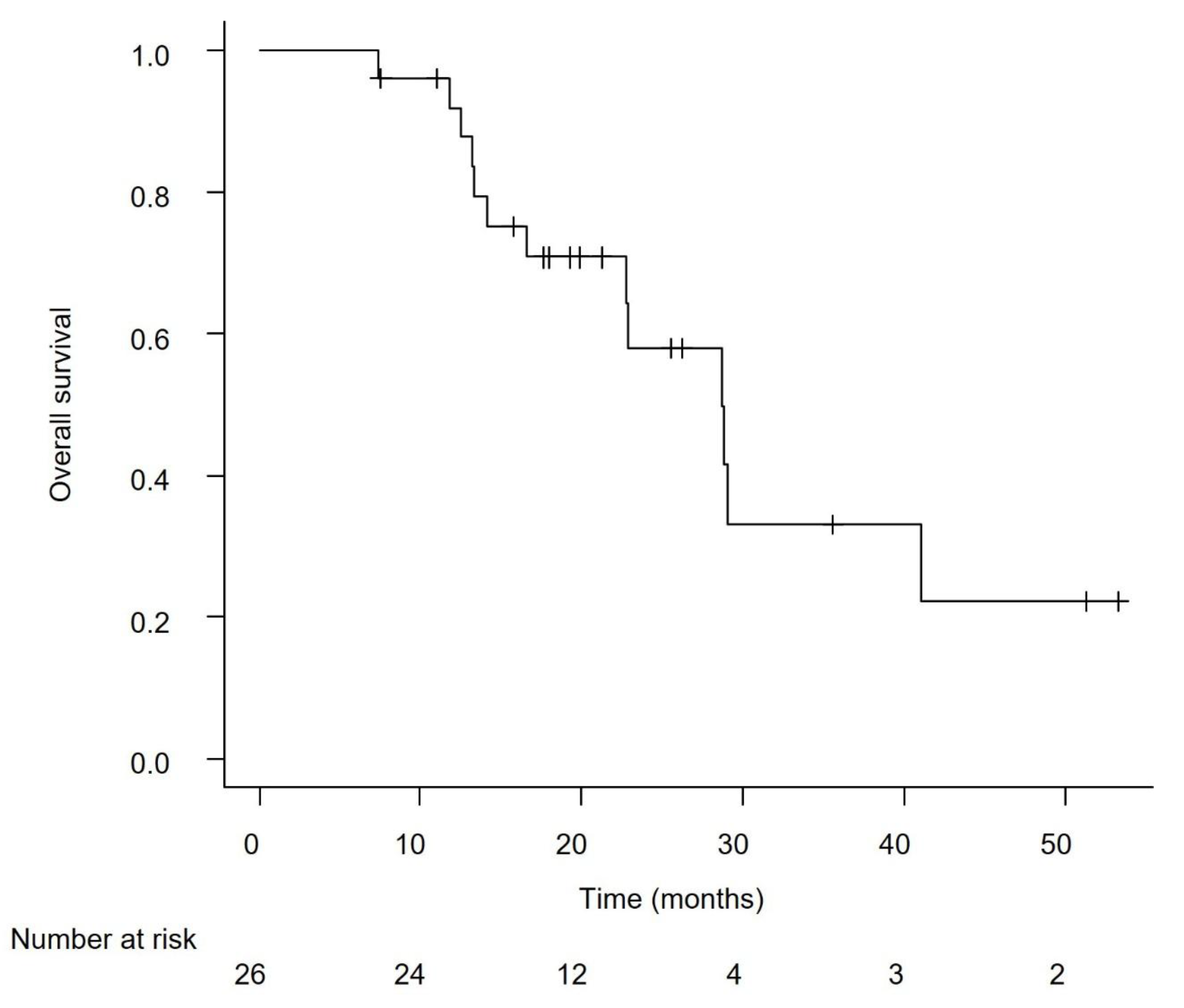
Figure 4.
Progression-free survival (PFS) from the start of avelumab in advanced urothelial carcinoma patients with lymph node-only metastasis versus other metastatic patterns. No statistically significant difference in PFS was observed between the groups (P = 0.118).
Figure 4.
Progression-free survival (PFS) from the start of avelumab in advanced urothelial carcinoma patients with lymph node-only metastasis versus other metastatic patterns. No statistically significant difference in PFS was observed between the groups (P = 0.118).
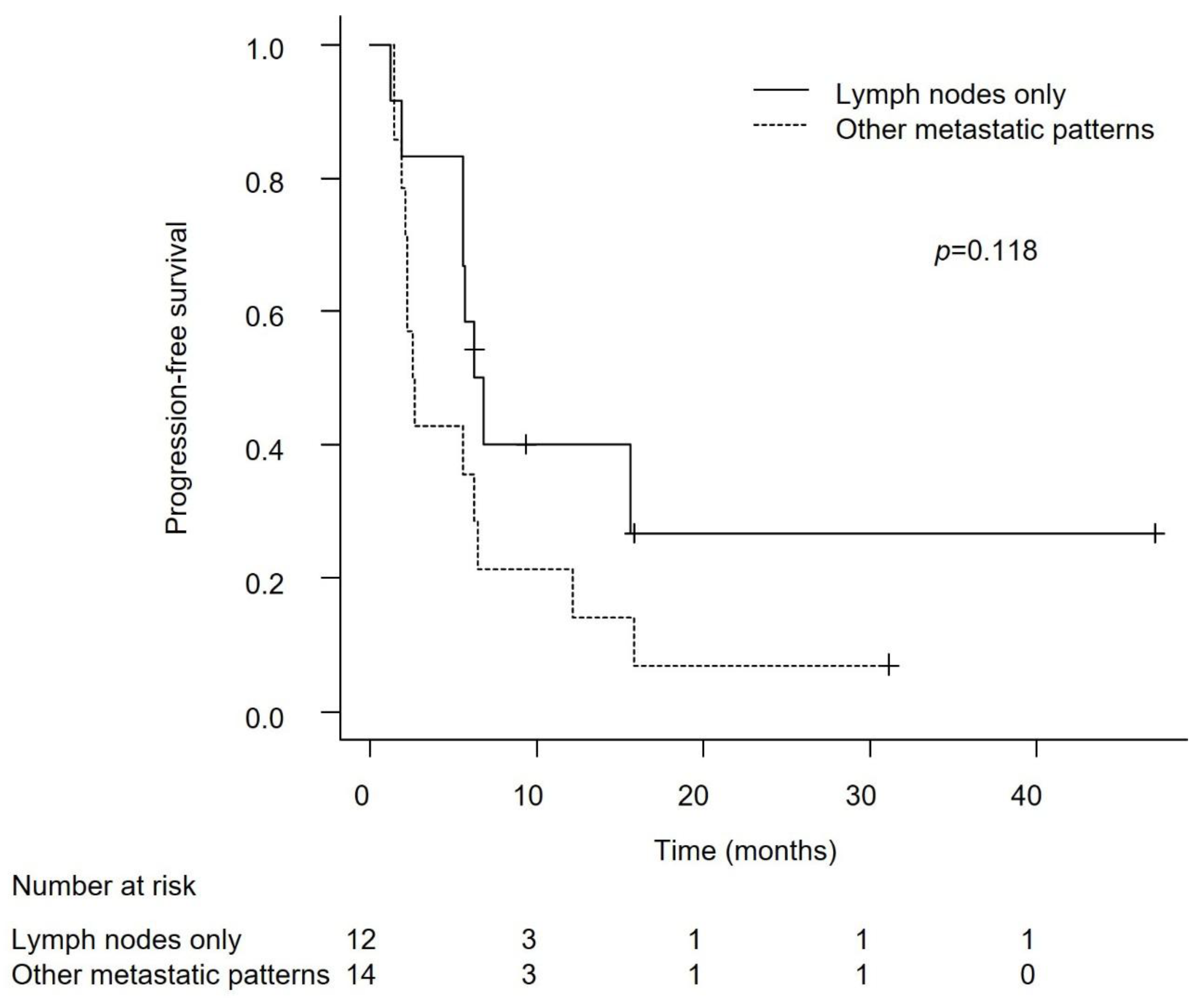
Figure 5.
Overall survival (OS) from the start of avelumab in advanced urothelial carcinoma patients with lymph node-only metastasis versus other metastatic patterns. The difference in OS between the groups was not statistically significant (P = 0.062).
Figure 5.
Overall survival (OS) from the start of avelumab in advanced urothelial carcinoma patients with lymph node-only metastasis versus other metastatic patterns. The difference in OS between the groups was not statistically significant (P = 0.062).
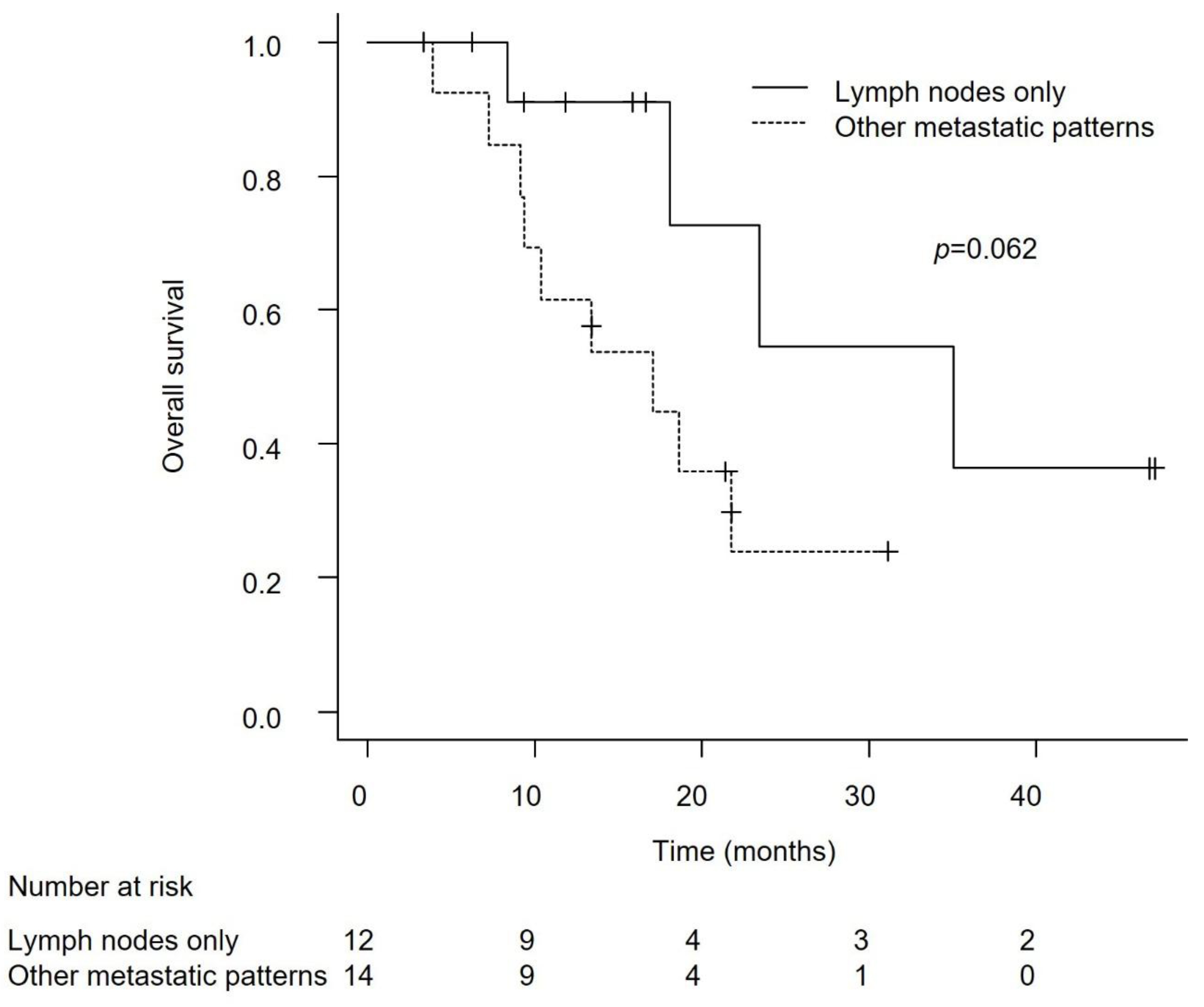
Figure 6.
Overall survival (OS) from the initiation of platinum-based chemotherapy in advanced urothelial carcinoma patients with lymph node-only metastasis versus other metastatic patterns. The lymph node-only group displayed statistically significantly longer OS (P = 0.044).
Figure 6.
Overall survival (OS) from the initiation of platinum-based chemotherapy in advanced urothelial carcinoma patients with lymph node-only metastasis versus other metastatic patterns. The lymph node-only group displayed statistically significantly longer OS (P = 0.044).
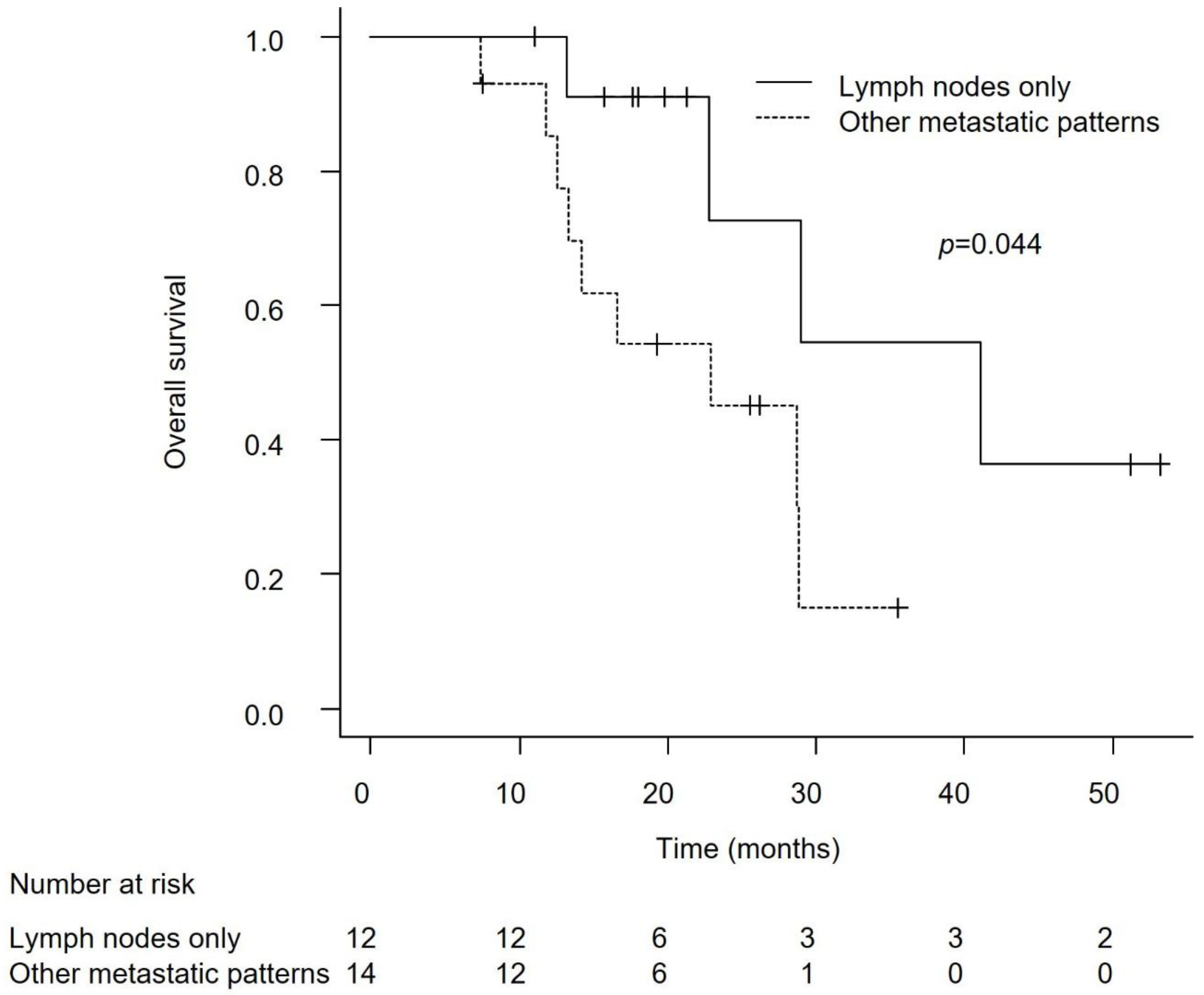
Figure 7.
Progression-free survival (PFS) from the start of avelumab in advanced urothelial carcinoma patients with non-visceral versus visceral metastasis. No significant difference in PFS was observed between the groups (P = 0.158).
Figure 7.
Progression-free survival (PFS) from the start of avelumab in advanced urothelial carcinoma patients with non-visceral versus visceral metastasis. No significant difference in PFS was observed between the groups (P = 0.158).
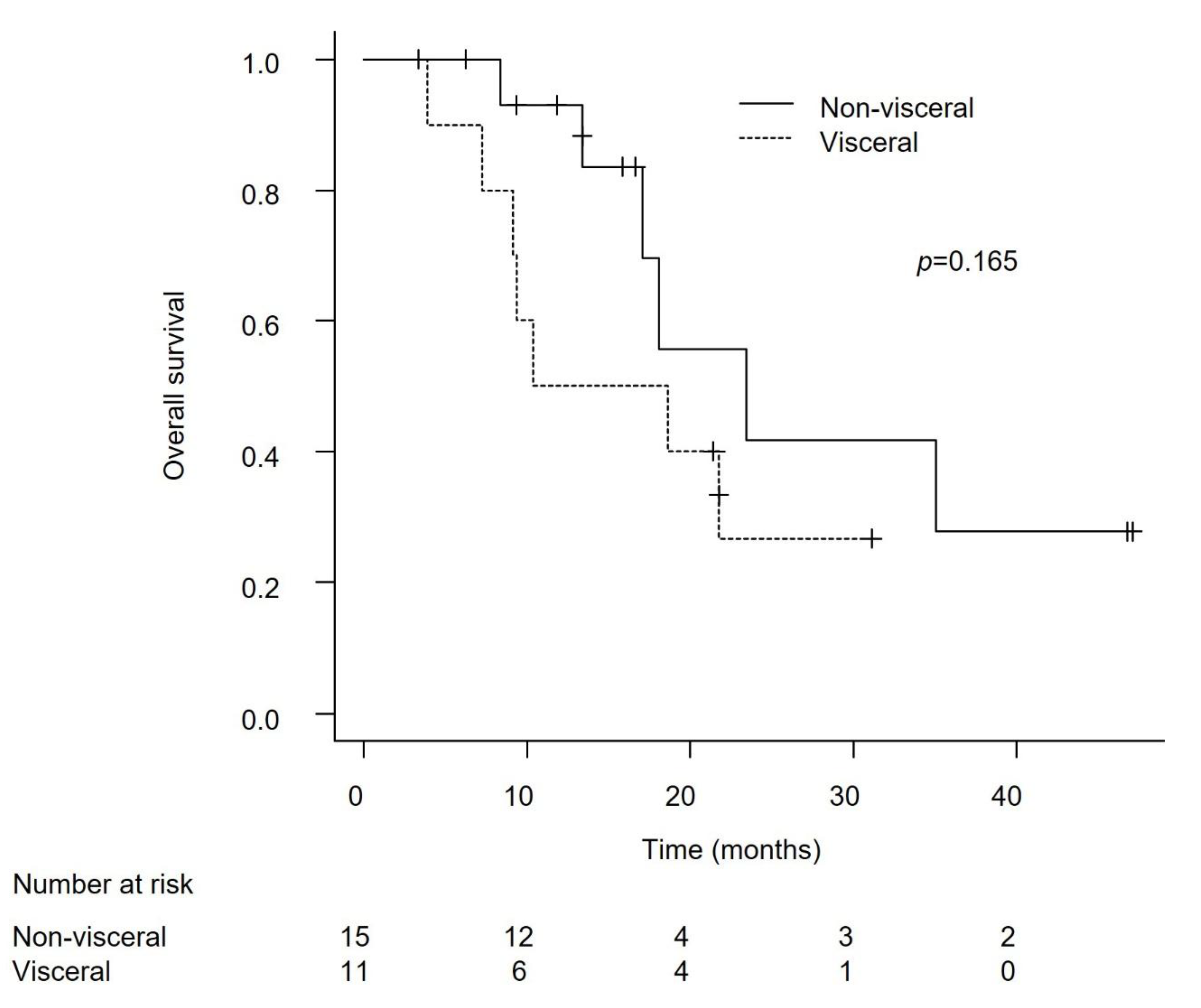
Figure 8.
Overall survival (OS) from the start of avelumab in advanced urothelial carcinoma patients with non-visceral versus visceral metastasis. The difference in OS between the groups was not statistically significant (P = 0.165).
Figure 8.
Overall survival (OS) from the start of avelumab in advanced urothelial carcinoma patients with non-visceral versus visceral metastasis. The difference in OS between the groups was not statistically significant (P = 0.165).
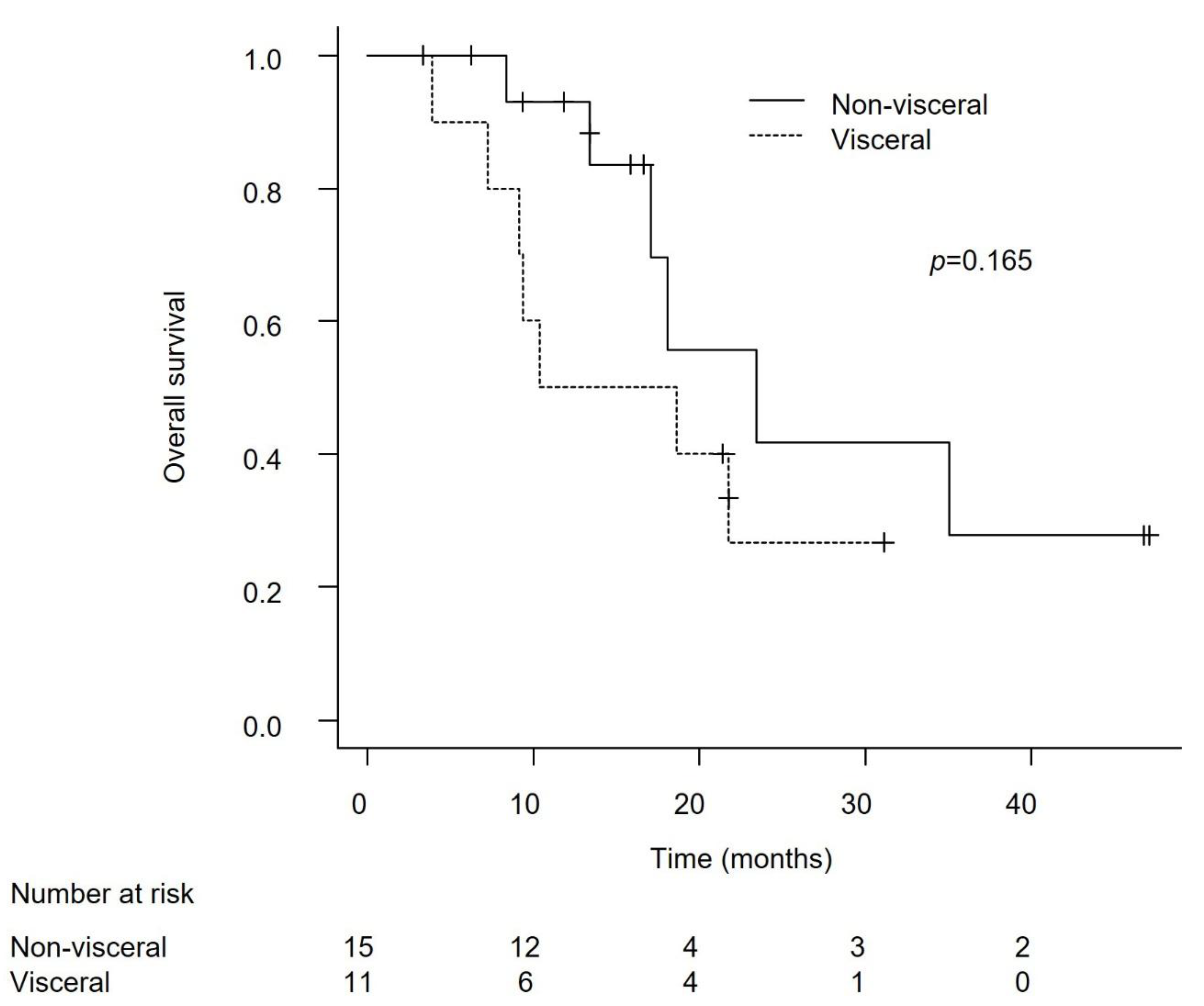
Figure 9.
Overall survival (OS) from the initiation of first-line platinum-based chemotherapy in advanced urothelial carcinoma patients with non-visceral versus visceral metastases. No statistically significant difference in OS was observed between the groups (P = 0.113).
Figure 9.
Overall survival (OS) from the initiation of first-line platinum-based chemotherapy in advanced urothelial carcinoma patients with non-visceral versus visceral metastases. No statistically significant difference in OS was observed between the groups (P = 0.113).
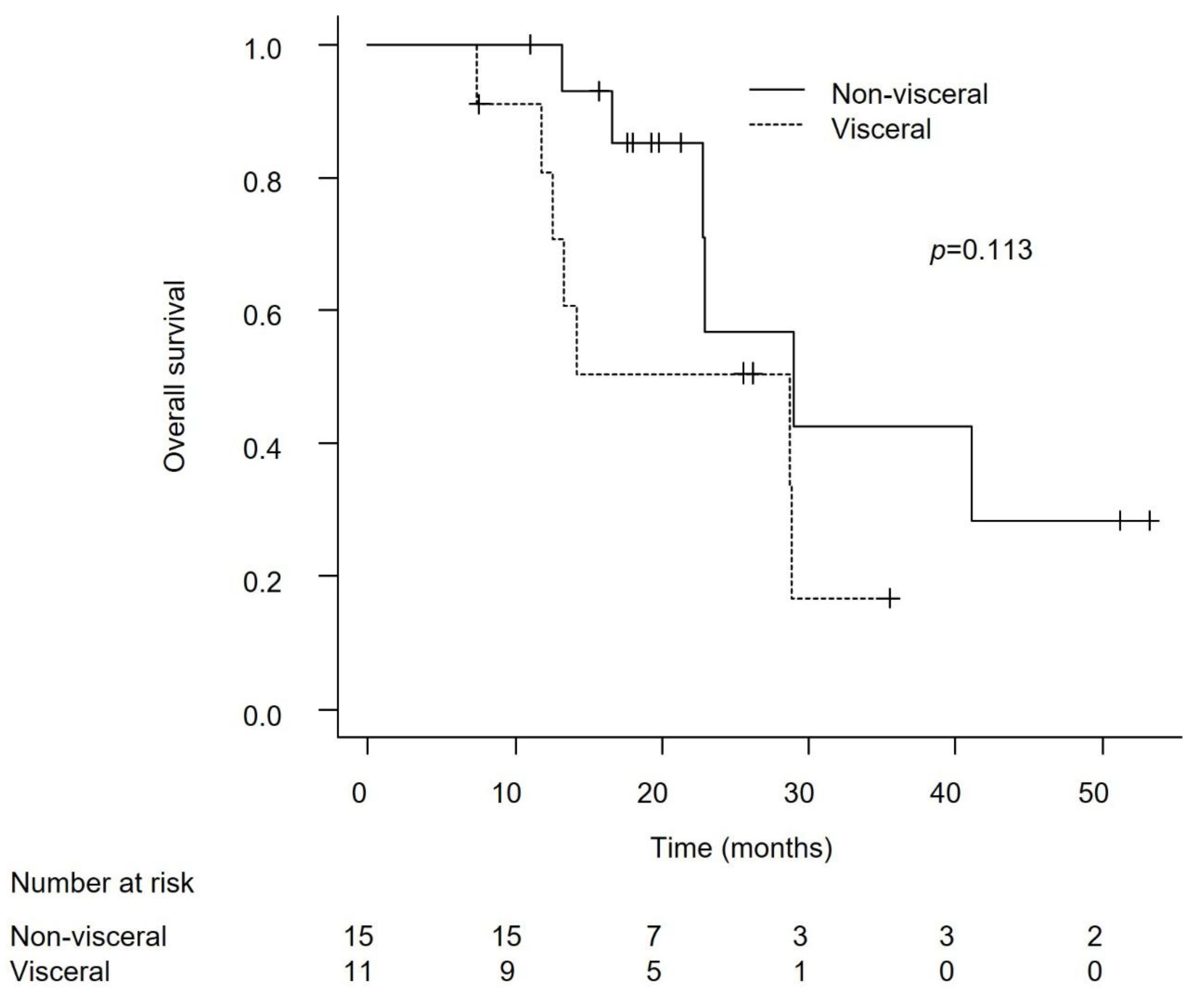

Table 1.
Advanced urothelial carcinoma patient characteristics at the start of platinum-based chemotherapy.
Table 1.
Advanced urothelial carcinoma patient characteristics at the start of platinum-based chemotherapy.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



