
Submitted:
25 June 2025
Posted:
27 June 2025
You are already at the latest version
Abstract
The complete clinical spectrum of Lyme borreliosis has been known for nearly 50 years. However, this long period has not been sufficient to clarify the diagnosis of the disease. Lyme foundations have emerged, publishing and disseminating guidelines independent of scientific consensus on the internet. These guidelines publish a wide range of symptoms. While many of these are likely to be inaccurate, there is a cluster of symptoms that is usually referred to in scientific publications as post-Lyme or post treatment Lyme disease syndrome (PTLDS) and is called in the popular media as "chronic Lyme disease". Among these symptoms, severe fatigue, brain fog, cognitive decline, memory impairment, joint and muscle pain, limb numbness, headaches, and low-grade fever are the most common. The scientific evidence of this disease is missing. Based on the experience of the leading author of this study, behind the diagnosis of "chronic Lyme disease" or PTLDS there is an underlying focal infection, most commonly chronic tonsillitis and chronic parodontal or periodontal disease. This paper aims to compile the supporting evidence for this hypothesis.
Keywords:
Lyme borreliosis
; chronic Lyme disease
; focal infection
; chronic tonsillitis
; chronic parodontitis
; chronic periodontitis
; post treatment Lyme disease syndrome
1. Introduction
Lyme disease, or as it is known in Europe, Lyme borreliosis (Lb), was discovered by Allen Steere in 1975 while investigating the origin of an arthritis outbreak in Connecticut [1]. In the first years following the discovery, publications began to emerge with titles and contents with the expression "the great imitator," previously used for syphilis (e.g., [2]). The pathogen (Borrelia burgdorferi) does indeed resemble Treponema pallidum, as both belong to the order Spirochaetales. There are also similarities in the clinical presentation, as both diseases exhibit skin lesions, joint and neurological complications, acute and late-stage, chronic clinical forms. This adoption of the concept of "the great imitator" was the "peccatum originale," or the original sin. Since then, it has become widespread that any symptom or complaint for which we cannot find an explanation could be a consequence of Lyme disease, in particular beleived to be part of its chronic manifestation.
The first author of this paper published a pilot study on this topic, titled "Lyme Disease and Chronic Lyme Disease" [3], followed by a preliminary work as an initiative leading to the present study [4]. The title itself is contradictory, as Lyme borreliosis can truly become a chronic illness. The most frequent symptom of Lyme disease, erythema migrans can last for months, Lyme arthritis for years, acrodermatitis chronica atrophicans for up to a decade, or even longer. However, "Chronic Lyme Disease" refers to a set of symptoms that have very little (although some, as will be discussed later) connection to Lb. Numerous studies have found no evidence to support the idea that these patients have an ongoing borrelia infection (e.g., [5]). Although many have attempted to formulate diagnostic criteria for "chronic Lyme disease," there is no consensus. Nevertheless, severe fatigue, brain fog, cognitive decline, memory impairment, joint and muscle pain, limb numbness, headaches, and low-grade fever are commonly mentioned in scientific publications. These are mostly subjective complaints, typically without objective findings. Despite the elusive nature of this symptom complex, we have noticed over 15 years of practice how homogeneous this group of patients is. Most doctors don't look into their patients' mouths; somehow, they don't consider it such an important area for examination...
The aim of this study is to draw attention to the fact that the so-called "chronic Lyme disease" and the symptoms that can develop after successful treatment, despite it, are identical to the symptoms of focal infections.
2. Materials and Methods
2.1. Case Selection Criteria
During the period between October 30, 2024, and May 12, 2025, 50 outpatients diagnosed with clinically confirmed focal infections at the Center for Tick-borne Diseases were asked to indicate in a questionnare which symptoms they considered characteristic of themselves. The questionnaire was compiled from complaints reported by our previous patients.
2.2. Definition of Focal Infection
By our own definition, a focal infection develops due to partially closed abscess(es). These abscesses do not cause local symptoms, spontaneously drain, thus being open, but with distant consequences. This may occur in various parts of the body: gallbladder, prostate, lungs, ovaries, but most commonly in the oral cavity, namely (A) periodontal disease, and (B) chronic tonsillitis.
- (A)
- (B)
- Peaceful, delicate rose (not red) tonsils - a very important criterion. AND
- Pus can be squeezed from the tonsils.
- AND/OR Pus can be seen coming from deep within. Small white pus clumps, sometimes the size of a pinhead or smaller, or even sizable "tonsil stones" may be visible.
- AND/OR The tonsils are pitted, deeply fissured.
- AND/OR The tonsils are spectacularly asymmetrical.
- AND/OR Some parts or the entire tonsils are rounded, swollen, „inflated”.
2.3. Clinical Follow-Up
How can we determine if our patient has been cured of Lyme disease? We have been using comparative immunoblot assays (COMPASS) for nearly 30 years, which is a sensitive procedure and effectively demonstrates microbiological recovery and, if applicable, the survival of Lyme bacteria after antibiotic treatment [6]. The essence of the test is to examine frozen stored older and newer serum samples side by side using the Western blot technique (Figure 10 and Figure 11).
Interestingly, even though we can detect pathogen survival through COMPASS, in most cases, this does not manifest clinically with symptoms or complaints. With this knowledge in mind, we have developed a practice where if someone experiences the symptoms described earlier despite successful treatment, I search for focal inflammation which primarily involves oral examination. This almost always sheds light on the presence or possibility of focal infection.
2.4. Statistical Analyses
Normal distribution of age-related data among patients was checked by Kolmogorov-Smirnov test (https://www.socscistatistics.com/tests/kolmogorov/default.aspx). For comparison, data of 171 patients admitted to the Center of Tick-borne Diseases in Budapest and showing erythema migrans, have been taken into account [7]. Student t-test (in Excel) was used to compare mean age, and Fisher exact test (https://www.langsrud.com/fisher.htm) to compare the ratio of male and female patients according to symptom groups. Differences were regarded significant if P < 0.05.
3. Results
All the symptoms included in the questionnaire filled by the 50 patients having focal infection are listed in Figure 12, which also presents their relative frequencies.
The patients referred to us commonly presented with similar symptoms, primarily fatigue, occasionally severe enough to cause inability to work, joint, bone, connective tissue, and muscle pain, general weakness, fatigue, sweating, non-rotating dizziness, „internal fever” (not indicated by a thermometer), uncertainty, low-grade fever, headaches, limb numbness or other sensory disturbances, muscle weakness, sleep disturbances, blurred vision. Objective symptoms are almost never present, and inflammatory markers in laboratory tests (white blood cell count, CRP, blood sedimentation rate) are also normal (data not shown).
The mean age of theese 50 patients having focal infection was 43.14±12.33 years. This was significantly (P = 0.033) higher than the mean age of 171 patients diagnosed with erythema migrans, i.e., 35.76±23.37 years. However, the ratio of males vs females did not differ significantly between these two goups: it was 76 men vs 95 women among patients showing erythema migrans, whereas 24 men vs 26 women among patients with focal infection (P = 0.75).
Patients having hairloss and diarrhoea had the lowest mean age (34.8 and 38.4 years, respectively), and those with swollen joints had the highest (53 years). The mean age of patients having symptoms of the central nervous system was 42.03±12.17 years, higher but not significantly different from that in the group reported with gastrointestinal signs (36.72±15.68 years) (P = 0.063). However, the mean age of patients with gastrointestinal signs was significantly lower in comparison with the age of patients having musculoskeletal diseases, i.e., 44±12.36 years (P = 0.014). The mean age of patients with chronic tonsillitis (42.53±12.91 years) or dental foci (45.04±11.73 years) was similar (P = 0.46).
Considering the ratio of sexes among patients with focal infection, it was balanced in most symptom groups. However, heat wave was more often characteristic of female (n=7) than of male patients (n=3), while this trend was the opposite in the case of sleeping disorder and muscle pain, in the case of which 1.5 times more men (n=12) developed this condition than women (n=8).
4. Discussion
4.1. Chronic Lyme Disease as a Hot Topic
It is of utmost importance to have an explanation as to what might cause the symptoms of "chronic Lyme disease" to occur despite successful treatment of Lb. However, to the best of our knowledge, no one has yet reported deciphering what causes so many doctors to believe in the existence of "chronic Lyme disease." In our experience, as also shown here, almost every "chronic Lyme patient" has oral foci. Younger individuals tend to have chronic tonsillitis, while older individuals have dental foci, and some experience symptoms due to chronic sinusitis, although in the present study this comparison did not yield a significant difference (probably owing to the limited number of cases). Most doctors do not address these issues, and it is rare for colleagues to thoroughly examine the oral cavity using appropriate tools.
It seems obvious that the foci originated much earlier than the Lb in each case. However, the foci are almost inactive, causing hardly any symptoms, although the presented images show how serious the lesions can be. The role of borrelia infection in activating the foci may be that the influx of numerous Lyme bacteria flooding the body at this time distracts the immune system, which previously controlled bacteria in the focus. Of course, not only Lb can do this, but any other infection as well. Our everyday practice also shows that many of our patients with identical symptoms did not have Lyme disease. Nevertheless, many of them have positive borrelia serology results (despite having symptoms for years, almost all of them have IgM positivity, indicating the quality of the tests). This also contributes to making our Centre for Tick-borne Diseases into a clinic for focal infections. In every article discussing "chronic Lyme disease" or PTLDS, severe fatigue is listed as a leading symptom [8]. Interestingly, this is hardly or not at all mentioned in articles discussing focal infections [9]. The second most common complaint among our patients is severe fatigue, often leading to disability. We believe the main cause of this is chronic inflammation, which occupies the immune system and consumes significant energy. Memory and sleep disturbances, brain fog, are common complaints. Since these patients feel very unwell, they visit doctors for years without receiving help, increasingly focusing on themselves, being sleep-deprived, and consequently experiencing memory impairment and many other subjective complaints. These gradually disappear after successful surgical intervention.
We see these same complaints in post-Lyme syndrome, which has been thoroughly discussed in the scientific medical literature. We consider it an important diagnostic sign because patients literally say the same thing: antibiotic treatment is temporarily effective, but after a few days, weeks, or months, the symptoms return. The success of antibiotic treatment confirms the misdiagnosis of Lyme disease, and so does the relapse, indicating how difficult it is to cure this disease. This prompts the treating physician to prescribe more and more antibiotics, increasingly longer, and more medications in parallel. The failure (and temporary success) of antibiotic treatment is an important diagnostic sign mentioned by many of our patients. One possible explanation is 1. that the metabolism of the focal bacteria is significantly reduced, and since antibiotics exert their effect by targeting metabolic pathways, their efficacy is limited under such conditions, 2. since there is no effective antibiotic against every member of the extremely heterogeneous bacterial population, 3. biofilm formation prevents the penetration of antibiotics, 4. because there is no blood circulation in the wall of the abscess, there is nothing to deliver the active ingredients into the core of the focus. These – particularly when disregarding professional recommendations – can have transient and moderate effects on the extraordinary and high-dose antibiotic combinations.
4.2. Symptoms of "Chronic Lyme Disease" According to Lyme Foundations' Guidelines
The ILADS (International Lyme and Associated Diseases Society) lists 91 symptoms that have been observed in "chronic Lyme disease" [10]. Among these, symptoms such as eyelid swelling, facial flushing, tinnitus, hearing loss, dizziness, torticollis, cogwheel rigidity (a hallmark of Parkinson’s disease), tremors, nocturia, urgency, Alzheimer’s disease, anetoderma, carpal tunnel syndrome, skin tumors, mitral insufficiency, mycosis fungoides, panuveitis, and ulcerative keratitis have never been observed in our cohort of approximately 40,000 Lyme disease patients over the past four decades at the Center for Tick-borne Diseases in Budapest. The authors of the above article evidently accept reports without criticism and do not consider the fundamental rule: the longer Lyme disease persists, the more intense the antibody response will become. Chronic Lyme disease cannot be diagnosed without extremely positive borrelia IgG findings. However, the quoted paper does not mention serology at all. The problem with the plethora of listed symptoms is that Lyme disease is common enough and other symptoms of different origins can easily occur alongside it as a confounding factor. The discovery of newer tick-borne infections has greatly helped Lyme foundations. And thus, instead of the term "seronegative chronic Lyme disease," the term "co-infections," covering surprisingly identical symptoms, emerged.
Anaplasma, babesia, and bartonella are the most commonly mentioned [11]. Based on improperly adjusted or incorrectly interpreted serological findings, a portion of patients is often treated for these pathogens [12]. In another questionnaire by a Lyme foundation in the USA, the symptoms of chronic Lyme disease are listed as follows: fatigue, headaches, joint and muscle pain, twitching, forgetfulness, cognitive impairment, sleep disturbances, heart problems, gastrointestinal issues, digestive disorders, neuropathies (numbness, tingling, altered sensation of hot or cold), depression, mood swings [13]. These symptoms are not truly specific and can sometimes occur in Lyme disease. However, for instance, headaches are almost never present in chronic forms, and gastrointestinal issues, while common, are not typically associated with Lyme disease. There are never any cardiac symptoms in chronic forms. Lyme carditis occurs with a prevalence of per thousand, involves atrioventricular block, always manifests in the first weeks of infection, and then resolves on its own, so there is no chronic variant. Lyme disease does not cause psychiatric disorders [14], although many publications claim the opposite. Numerous reliable studies confirm that the aforementioned symptoms cannot be alleviated by any antibiotic treatment, no matter how prolonged or high-dose [15,16,17].
As shown here, compared to the group with erythema migrans, prolonged manifestation of focal infection is evident from the significantly more advanced age of patients in this study with focal infection (including both chronic tonsillitis and dental foci), as well as musculoskeletal diseases. According to Lohiya et al. [18], periodontitis can be a source of various diseases in the cardiovascular, pulmonary, endocrine, musculoskeletal, central nervous, and reproductive systems. Periodontal disease can serve as a continuous source of infections. Oral health affects overall health. If we ever aim to achieve comprehensive healthcare, dental health should never be considered as a separate, distant, and subordinate component independent of quality of life. Periodontitis increases mortality and the risk of numerous systemic diseases such as diabetes mellitus, premature birth, and several cardiovascular diseases (atherosclerosis, heart attack, and stroke) [19,20,21]. According to a case-control, cross-sectional study, periodontitis doubles the risk of cardiovascular diseases and increases the risk of premature birth sevenfold [22]. It has been proven that there is a causal relationship between periodontitis and heart attack, adverse outcome of pregnancy, diabetes mellitus, and certain respiratory diseases [23]. Periodontal disease causes fibromyalgia, and fibromyalgia causes periodontal disease [24]. Similarly, there is a bidirectional relationship between diabetes and periodontitis, with diabetes often accompanied by pronounced fatigue, although we have not found any publications on the role of periodontal disease in causing fatigue. A Hungarian study indicates how prevalent periodontal disease is: in the capital city and its surroundings, 16% of the population had completely healthy periodontium, while in rural areas, only 5-8% did [25]. Not only periapical abscesses count as focal infections, but also implants, gingivitis, and root-treated teeth. With genetic technology, numerous microbes can be isolated, half of which we cannot culture with currently available tools. Of course, not all detected bacteria have equal importance in maintaining the process, but we know very little about this.
4.3. "Chronic Lyme Disease": Focal Infection with Systemic Consequences?
From the earlier list related to periodontal disease, it is evident that many studies unanimously assert the same thing: focal infections have serious systemic consequences. Yet, many experts do not acknowledge the existence of focal infections, considering the related information merely a passing trend. For about 15 years, we have observed that at least 20 percent of the patients who come to the Center for Tick-borne Diseases, Budapest, present surprisingly similar complaints. These include: severe fatigue, brain fog, cognitive decline, memory impairment, joint and muscle pain, limb numbness, headaches, low-grade fever, sleep disturbances. These symptoms roughly correspond to what Lyme foundations refer to as „chronic Lyme disease”. This has led to the Centre for Tick-borne Diseases, Budapest becoming a gathering center for these patients. What's interesting is that in this patient group, many individuals become symptomatic despite being clinically and serologically confirmed to have been cured of Lyme disease. Their symptoms often develop suddenly and are not supported by laboratory or clinical findings.
Foci can occur elsewhere (e.g., prostate, gallbladder), but oral foci (including sinus cavities) are the most common. This definition is crucial because it explains why there is no fever, local pain, or inflammatory markers in blood tests. A good example of this is infantile otitis media. The infant has a high fever, cries miserably due to pain, and blood test results indicate severe inflammation. The otolaryngologist performs a paracentesis. The crying stops instantly, the fever subsides within hours, and the laboratory parameters normalize over days, even though pus may continue to drain through the perforated eardrum for weeks. (Even if the eardrum closes, pus can still drain through the Eustachian tube, leading to a symptom-poor, chronic process.) In other words, it's an open abscess that now lacks subjective and laboratory signs.
4.4. Chronic Tonsillitis as a Focal Infection
The criteria for chronic tonsillitis are not consistent. Many consider recurrent acute (!) tonsillitis as chronic. There are mostly Russian-language publications suggesting that others have also noticed the focal nature of this condition. However, these publications are inaccessible, and even their abstracts are not available on PubMed or similar databases. Despite the abundant literature on dental focal infections, we could not find any data in the available literature suggesting that others have noticed that chronic tonsillitis causes general symptoms. Yet, we observe the same symptoms behind chronic tonsillitis as those caused by periodontal diseases. However, there is some data supporting the connection between the two focal infections (chronic tonsillitis and dental infection). Genetic analysis of discharge from chronic tonsillitis isolated 42-110 species of bacteria, some of which were identical to those isolated from periodontitis [26]. Russian researchers also raised the connection between chronic tonsillitis and periodontitis [27].
Tonsilolith is the extreme form of chronic tonsillitis. This is essentially calcified pus, which most otolaryngologists consider a harmless phenomenon. On the internet, one can find various tools with which patients can excavate these "stones" from their tonsils themselves (Figure 9.a). However, these stones are formed by a completely different mechanism than kidney or gallstones. In many cases, the body tries to isolate the inflammatory focus by depositing calcium, such as in tuberculosis or toxoplasmosis, and in certain parasitic infections (e.g. cysticercosis) as well. Tonsilolith consists of dead and living bacteria with minimal metabolism: fusobacteria, rods, and cocci are arranged in regular layers. Aerobic bacteria are found on the surface, creating the right environment for anaerobes located deeper [28]. Bacteria (and fungi) in dental foci are similarly structured, forming antibiotic-resistant biofilms [29]. These bacteria are practically uncultivable and resistant to antibiotics. It is a mixed flora so it is an other reason of that it cannot be eradicated with a single or combined antibiotic even with prolonged course. Bacteria detected in throat swabs during culture are never the true pathogens but rather colonized microbes. The antibiotics prescribed against them are ineffective against the microbes residing in tonsil stones. Not only because antibiotics only affect actively metabolizing microbes, and not only because it's a mixed flora, but also because the bacterial colony forms a biofilm, preventing antibiotics from entering the abscess (because that's what a tonsil stone is: a calcified abscess). Tonsil stones are regularly expelled or located deep within the tonsils, so smaller ones can easily be overlooked. The surface of the tonsils is pale pink, with no signs of acute inflammation. Despite being a truly chronic inflammation, blood tests show no signs of inflammation, typically all results are negative. All this misleads doctors and patients. Even though the diagnosis seems straightforward with tonsil compression, we see that otolaryngologists often interpret the picture differently and, the course of action as well.
Conclusions
We hope that the fifty cases and the reasoning presented here are convincing despite the fact that our hypothesis cannot be proven with our previous observations that were not documented in the same way. A multicentric study should be designed in which the diagnostic criteria for Lb, "chronic Lyme disease," focal infections, and PTLDS are clearly defined, and doctors capable of accepting and adhering to these rules should be involved. (It does not seem to be a simple task considering that hardly anyone follows the methodological guideline for Lb.) It seems unfeasible to recruit multiple dentists and otolaryngolgists who accept these criteria and possess the appropriate diagnostic and surgical skills. Patients participating in follow-up examinations are also needed, faithfully and credibly reporting the progression or regression of their subjective complaints, as there is no way to detect objective parameters due to the nature of the issue.
Author Contributions
A.L.: Conceptualization, methodology, study design, and writing of the original and final drafts. Clinical examination of patients. Gy.N: performed the Lyme serological examinations (e.g., the presented COMPASS). Z.V.: examined and treated our dental surgery patients. P.R-K.: examined and performed the ENT surgeries. S.H.: performed statistical analysis of patients data and writing of the final draft. The images in the publication were taken by GyN, P.R-K., Z.V.
Funding
The preparation of this publication received no financial support.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no competing interests. The authors have no financial interests related to the publication.
References
- Steere, A.C.; Malawista, S.E.; Snydman, D.R.; Shope, R.E.; Andiman, W.A.; Ross, M.R.; Steele, F.M. Lyme arthritis: an epidemic of oligoarticular arthritis in children and adults in three connecticut communities. Arthritis Rheum. 1977, 20, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Pachner, A.R. Borrelia burgdorferi in the nervous system: the new "great imitator". Ann N Y Acad Sci. 1988, 539, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Lakos, A. Lyme disease and chronic Lyme disease. Orvostovábbképző Szemle 2017, 24, 47–53. [Google Scholar]
- Lakos, A. Chronic Lyme disease=post-Lyme syndrome=focal infections? Integráló infekciókontroll 2024, 3, 37-50. [in Hungarian].
- Lantos, P.M. Chronic Lyme disease: the controversies and the science. Expert Rev Anti Infect Ther. 2011, 9, 787–97. [Google Scholar] [CrossRef]
- Lakos, A.; Igari, E. Advancement in Borrelia burgdorferi antibody testing: Comparative immunoblot assay (COMPASS). In: Lyme disease, Ed: Karami A. InTech, Rijeka 2012, 55–78. [Google Scholar]
- Hornok, S.; Takács, N.; Nagy, Gy.; Lakos, A. Retrospective molecular analyses of hard ticks (Acari: Ixodidae) from patients admitted to the medical Centre for Tick-Borne Diseases in Central Europe, Hungary (1999-2021) in relation to clinical symptoms. Parasit. Vectors 2025, 8, 229. [Google Scholar] [CrossRef]
- Wester, K.E.; Nwokeabia, B.C.; Hassan, R.; Dunphy, T.; Osondu, M.; Wonders, C.; Khaja, M. What Makes It Tick: Exploring the Mechanisms of Post-treatment Lyme Disease Syndrome. Cureus. 2024, 16, e64987. [Google Scholar] [CrossRef]
- Rogne, A.G.; Müller, E.G.; Udnaes, E.; Sigurdardottir, S.; Raudeberg, R.; Connelly, J.P.; Revheim, M.E.; Hassel, B.; Dahlberg, D. β-Amyloid may accumulate in the human brain after focal bacterial infection: An 18 F-flutemetamol positron emission tomography study. Eur J Neurol. 2021, 28, 877–883. [Google Scholar] [CrossRef]
- Shor, S.; Green, C.; Szantyr, B.; Phillips, S.; Liegner, K.; Burrascano, J.J. Jr.; Bransfield, R.; Maloney, E.L. Chronic Lyme Disease: An Evidence-Based Definition by the ILADS Working Group. Antibiotics (Basel). 2019, 8, 269. [Google Scholar] [CrossRef]
- Boyer, P.H.; Lenormand, C.; Jaulhac, B.; Talagrand-Reboul, E. Human Co-Infections between Borrelia burgdorferi s.l. and Other Ixodes-Borne Microorganisms: A Systematic Review. Pathogens. 2022, 11, 282. [Google Scholar] [CrossRef]
- Lantos P.M.; Wormser, G.P. Chronic coinfections in patients diagnosed with chronic Lyme disease: a systematic review. Am J Med. 2014; 127, 1105-10.
- Lymedisease.org: Lyme disease checklist. [https://www.lymedisease.org/lyme-disease-symptom-checklist/ accessed on March 2, 2024].
- Lantos, P.M.; Rumbaugh, J.; Bockenstedt, L.K.; Falck-Ytter, Y.T.; Aguero-Rosenfeld, M.E.; Auwaerter, P.G.; Baldwin, K.; Bannuru, R.R.; Belani, K.K.; Bowie, W.R.; et al. Clinical practice guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 Guidelines for the prevention, diagnosis and treatment of Lyme Disease. Clin Infect Dis. 2021, 72, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lantos, P.M. Chronic Lyme disease. Infect Dis Clin North Am. 2015, 29, 325–40. [Google Scholar] [CrossRef] [PubMed]
- Berende, A.; Ter Hofstede, H.J.M.; Vos, F.J.; Vogelaar, M.L. erende, A.; Ter Hofstede, H.J.M.; Vos, F.J.; Vogelaar, M.L. Effect of prolonged antibiotic treatment on cognition in patients with Lyme borreliosis Neurology. 2019, 92, e1447-e1455. [CrossRef]
- Klempner, M.S.; Baker, P.J.; Shapiro, E.D.; Marques, A.; Dattwyler, R.J.; Halperin, J.J.; Wormser, G.P. Treatment trials for post-Lyme disease symptoms revisited. Am J Med. 2013, 126, 665–9. [Google Scholar] [CrossRef] [PubMed]
- Lohiya, D.V.; Mehendale, A.M.; Lohiya, D.V.; Lahoti, H.S.; Agrawal, V.N. Effects of periodontitis on major organ systems. Cureus 2023, 15, e46299. [Google Scholar] [CrossRef]
- Fowler, E.B.; Breault, L.G.; Cuenin, M.F. Periodontal disease and its association with systemic disease. Mil Med. 2001, 166, 85–9. [Google Scholar] [CrossRef]
- Sánchez, A.R.; Kupp, L.I.; Sheridan, P.J.; Sánchez, D.R. Maternal chronic infection as a risk factor in preterm low birth weight infants: the link with periodontal infection. J Int Acad Periodontol. 2004, 6, 89–94. [Google Scholar]
- Soskolne, W.A.; Klinger, A. The relationship between periodontal diseases and diabetes: an overview. Ann Periodontol. 2001, 6, 91–8. [Google Scholar] [CrossRef]
- Moutsopoulos, N.M.; Madianos, P.N. Low-grade inflammation in chronic infectious diseases: paradigm of periodontal infections. Ann N Y Acad Sci. 2006, 1088, 251–64. [Google Scholar] [CrossRef]
- Scannapieco, F.A.; Dasanayake, A.P.; Chhun, N. "Does periodontal therapy reduce the risk for systemic diseases? " Dent Clin North Am. 2010, 54, 163–81. [Google Scholar] [CrossRef]
- Sheng-Kai Ma, K.; Lai, J-N. ; Veeravalli, J.J.; Chiu L.T.; Van Dyke T.E.; Wei J.C. Fibromyalgia and periodontitis: Bidirectional associations in population-based 15-year retrospective cohorts. J Periodontol. 2022, 93, 877–87. [Google Scholar] [CrossRef]
- Borbély, J.; Gera, I.; Fejérdy, P.; Soós, B.; Madléna, M.; Hermann, P. Oral health assessment of Hungarian adult population based on epidemiologic examination. (in Hungarian) Fogorvosi Szemle 2011, 104, 3–8. [Google Scholar] [PubMed]
- Jensen, A.; Fagö-Olsen, H.; Sørensen, Ch.; Kilian, M. Molecular mapping to species level of the tonsillar crypt microbiota associated with health and recurrent tonsillitis. PLoS One 2013, 8, e56418. [Google Scholar] [CrossRef] [PubMed]
- Kryukov, A.I.; Krechina, E.K.; A S Tovmasyan, A.S.; Kishinevskiy, A.E.; Danilyuk, L.I.; Filina, E.V. Chronic tonsillitis and periodontal diseases. Vestn Otorinolaringol. 2023, 88, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Stoodley, P.; Debeer, D.; Longwell, M.; Nistico, L.; Hall-Stoodley, L.; Wenig, B.; Krespi, Y.P. Tonsillolith: not just a stone but a living biofilm. Otolaryngol Head Neck Surg. 2009, 141, 316–21. [Google Scholar] [CrossRef]
- Wróblewska, M.; Strużycka, I.; Mierzwińska-Nastalska, E. Significance of biofilms in dentistry. Przegl Epidemiol. 2015, 69, 739–44. [Google Scholar]
Figure 1.
Giant periapical abscess (arrow), the tooth is only held by the bridge. (Photo by Dr. Zoltán Varga).
Figure 1.
Giant periapical abscess (arrow), the tooth is only held by the bridge. (Photo by Dr. Zoltán Varga).

Figure 2.
Giant periodontal pocket (arrow), the tooth is held by connected crowns. (Photo by Dr. Zoltán Varga).
Figure 2.
Giant periodontal pocket (arrow), the tooth is held by connected crowns. (Photo by Dr. Zoltán Varga).
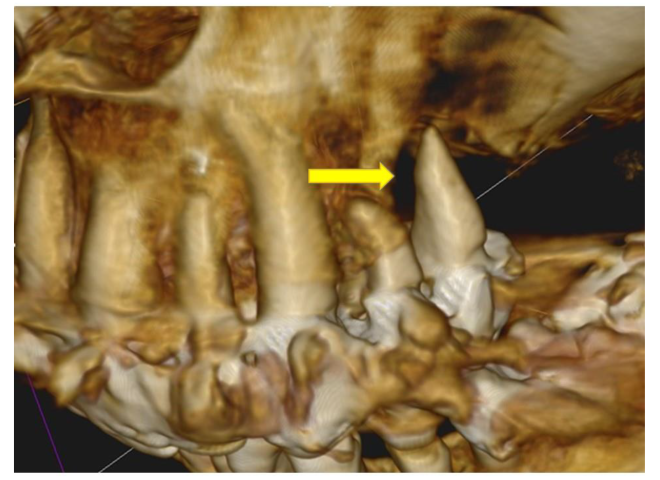
Figure 3.
Periodontitis: giant pocket in a difficult-to-reach area between 2 tooth roots (arrow). Not visible on the panoramic X-ray. (Photo by Dr. Zoltán Varga).
Figure 3.
Periodontitis: giant pocket in a difficult-to-reach area between 2 tooth roots (arrow). Not visible on the panoramic X-ray. (Photo by Dr. Zoltán Varga).
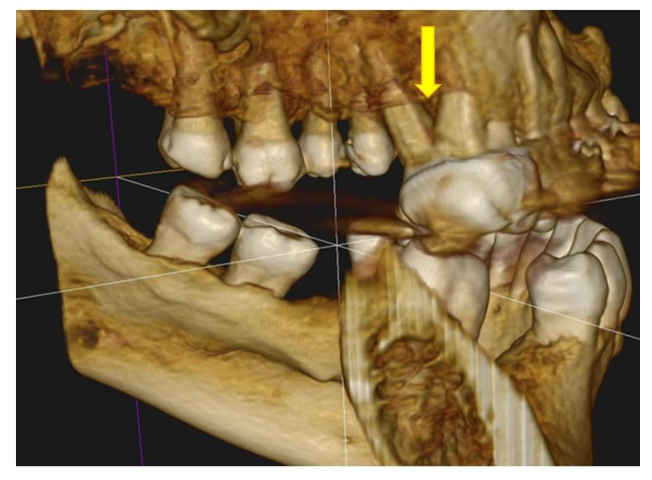
Figure 4.
Enormous periodontal pocket (arrow). (Photo by Dr. Zoltán Varga).

Figure 5.
Periapical abscesses (arrows). This 30 year old male patient has compiled a list of symptoms spanning several years: excessive sweating, occasional chills, insomnia, hot flashes, irritability, gum bleeding, gum disease, fatigue. „I am unable to perform simple tasks.” Frequent upper respiratory infections, frequent low-grade fevers, dizziness, nausea, vomiting, unsteady gait. Numbness in the feet, blurred vision, "floaters," short-term memory impairment, slurred speech, difficulty finding words, weight loss, loss of appetite, diarrhea, frequent changes in bowel movements, weakness, weak limbs, excessive urination, imperative urinate, urination with chills, mood swings, depression, panic, testicular and epididymal inflammation, prostatitis (no pathogen detected). Low back pain, cracking joints, decreased libido, tendon pain, joint pain, muscle cramps, sore throat, neck pain, jaw and tooth pain, ear and nose pain, phlegmy cough, coated tongue, shortness of breath, chest pain. Over 8 years, he received 20 doses of antibiotics. Pus in the tonsils could only be seen when I (L.A.) induced gagging with a spatula (Photo by Dr. Zoltán Varga).
Figure 5.
Periapical abscesses (arrows). This 30 year old male patient has compiled a list of symptoms spanning several years: excessive sweating, occasional chills, insomnia, hot flashes, irritability, gum bleeding, gum disease, fatigue. „I am unable to perform simple tasks.” Frequent upper respiratory infections, frequent low-grade fevers, dizziness, nausea, vomiting, unsteady gait. Numbness in the feet, blurred vision, "floaters," short-term memory impairment, slurred speech, difficulty finding words, weight loss, loss of appetite, diarrhea, frequent changes in bowel movements, weakness, weak limbs, excessive urination, imperative urinate, urination with chills, mood swings, depression, panic, testicular and epididymal inflammation, prostatitis (no pathogen detected). Low back pain, cracking joints, decreased libido, tendon pain, joint pain, muscle cramps, sore throat, neck pain, jaw and tooth pain, ear and nose pain, phlegmy cough, coated tongue, shortness of breath, chest pain. Over 8 years, he received 20 doses of antibiotics. Pus in the tonsils could only be seen when I (L.A.) induced gagging with a spatula (Photo by Dr. Zoltán Varga).

Figure 6.
Pressing on the tonsil causes pus to spread onto the spatula (arrow). A tiny crater can be seen directly beneath the pus (Photo by Dr. Péter Rásonyi-Kovács).
Figure 6.
Pressing on the tonsil causes pus to spread onto the spatula (arrow). A tiny crater can be seen directly beneath the pus (Photo by Dr. Péter Rásonyi-Kovács).

Figure 7.
Surgical image. Pus (arrow) only emerges when the surgeon applies pressure with the Kocher onto the tonsil. (Photo by Dr. Péter Rásonyi-Kovács).
Figure 7.
Surgical image. Pus (arrow) only emerges when the surgeon applies pressure with the Kocher onto the tonsil. (Photo by Dr. Péter Rásonyi-Kovács).

Figure 8.
Nearly touching, scarred, cratered (arrow), almost spherical tonsils. (Photo by Gyöngyi Nagy).
Figure 8.
Nearly touching, scarred, cratered (arrow), almost spherical tonsils. (Photo by Gyöngyi Nagy).

Figure 9.
A. Chronic tonsillitis. The almost completely atrophied tonsil barely emerges from the tonsillar fossae. The red arrow indicates a pus clump about to emerge, while the yellow arrow points to a crater showing recent pus discharge. (Photo by Gyöngyi Nagy).
Figure 9.
A. Chronic tonsillitis. The almost completely atrophied tonsil barely emerges from the tonsillar fossae. The red arrow indicates a pus clump about to emerge, while the yellow arrow points to a crater showing recent pus discharge. (Photo by Gyöngyi Nagy).

Figure 9.
B. Discarding tonsillolith. (internet).

Figure 10.
Immunoblots (IgG) of a patient suffered from acrodermatitis chronica atrophicans. Six years elapsed between the collection of the first (A) and the last (C) samples. It can be observed how intense the immune response develops in true chronic Lyme disease and how long it persists even after recovery. Although the decrease in antibody levels over time is minimal, it is nonetheless detectable — but only through direct comparison of archived and newly collected serum samples. This principle underlies the comparative immunoblot assay (COMPASS). (Arrows indicate the antibody responses where the decrease is most impressive. OspC: surface protein C, 41 kDa: flagellar antigen. Antibodies against the 93 kDa protein appear in infections lasting at least one year.).
Figure 10.
Immunoblots (IgG) of a patient suffered from acrodermatitis chronica atrophicans. Six years elapsed between the collection of the first (A) and the last (C) samples. It can be observed how intense the immune response develops in true chronic Lyme disease and how long it persists even after recovery. Although the decrease in antibody levels over time is minimal, it is nonetheless detectable — but only through direct comparison of archived and newly collected serum samples. This principle underlies the comparative immunoblot assay (COMPASS). (Arrows indicate the antibody responses where the decrease is most impressive. OspC: surface protein C, 41 kDa: flagellar antigen. Antibodies against the 93 kDa protein appear in infections lasting at least one year.).

Figure 11.
Lyme arthritis lasting for a year: this always involves a robust IgG class immune response. Significant seroprogession is evident in the second sample (B), taken 48 days after the first sample (A) following unsuccessful antibiotic treatment (inflammation developed in the other knee joint after treatment). Arrows indicate the most significant changes. The patient recovered after receiving further antibiotic treatment.
Figure 11.
Lyme arthritis lasting for a year: this always involves a robust IgG class immune response. Significant seroprogession is evident in the second sample (B), taken 48 days after the first sample (A) following unsuccessful antibiotic treatment (inflammation developed in the other knee joint after treatment). Arrows indicate the most significant changes. The patient recovered after receiving further antibiotic treatment.

Figure 12.
Summary of clinical symptoms and/or complaints in the most recent 50 patients diagnosed with focal infection (October 30, 2024 – May 12, 2025, Center for Tick-borne Diseases, Budapest).
Figure 12.
Summary of clinical symptoms and/or complaints in the most recent 50 patients diagnosed with focal infection (October 30, 2024 – May 12, 2025, Center for Tick-borne Diseases, Budapest).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



