
Submitted:
25 June 2025
Posted:
25 June 2025
You are already at the latest version
Abstract
Background and Objectives: The objective is to recognise that anaemia can induce both psychological problems and physical ailments. This research sought to assess alexithymia, mental symptoms, and quality of life in female patients suffering from iron deficiency anaemia. Methods: The study comprised 150 healthy controls and 151 women diagnosed with iron-deficient anaemia. Alongside laboratory analyses, the Sociodemographic and Clinical Data Form, Beck Depression Scale (BDS), State-Trait Anxiety Inventory (STAI Form TX-1, TX-2), World Health Organisation Quality of Life Scale Short Form Turkish Version (WHOQOL-BREF-TR), and Toronto Alexithymia Scale (TAS-20) were administered to all participants. The Iron-deficiency Anaemia Group exhibited lower scores on the WHOQOL-BREF and STAI-1 while demonstrating a higher score on the Toronto Alexithymia Scale compared to the control group. The prevalence of iron-deficiency anaemia, Beck Depression Scale scores, and STAI Form TX-2 scores was elevated in the likely alexithymia group compared to the non-alexithymia group, whereas the WHOQOL-BREF-TR scores were diminished in the former group. The Toronto Alexithymia Scale score had a positive correlation with total iron binding capacity, the Beck Depression Scale, and the STAI Form TX-2 score, while demonstrating a negative correlation with haemoglobin, iron (Fe), and the WHOQOL-BREF-TR score. Multivariate analysis indicated that elevated total iron binding capacity (OR: 1.003, 95% CI: 1.000-1.006; p=0.044), increased STAI-2 score (OR: 1.098, 95% CI: 1.050-1.147; p< 0.001), and diminished WHOQOL-BREF score (OR: 0.966, 95% CI: 0.950-0.982; p< 0.001) were independently correlated with probable alexithymia or alexithymia. In conclusion, women with iron-deficient anaemia exhibit higher levels of alexithymia, alongside diminished state-trait anxiety and quality of life. The alexithymia levels in these patients correlate with elevated iron-binding capability, heightened anxiety, and diminished quality of life.
Keywords:
i̇ron deficiency
; anaemia
; alexithymia
; anxiety
; depression
; quality of life
1. Introduction
Iron deficiency anaemia constitutes a significant public health issue, predominantly affecting women aged 15 to 49, particularly in poorer nations [1,2]. This condition is characterised by somatic symptoms as well as central nervous system manifestations, including dizziness, distraction, and delays in motor and cognitive development [3,4]. Iron influences the function of iron-dependent enzymes essential for dopamine, serotonin, and noradrenaline in the brain, whereas iron shortage can impact neurophysiological processes, cognitive function, and social behaviours [5]. Alterations associated with iron shortage, particularly in the hippocampus, corpus striatum, and monoamine concentrations, have been demonstrated to induce anxiety, sadness, sleep disturbances, and psychotic illnesses in individuals with iron deficiency anaemia [6]. Reduced brain myelination and compromised monoamine oxidase metabolism in anaemia influence neurobiological pathways and may lead to emotional and psychological issues that predispose individuals to mental diseases. Treatment for anaemia has been proposed to enhance cognitive functioning in brain regions and diminish the likelihood of depression [7,8]. Furthermore, a study on patients with anaemia has demonstrated that this condition diminishes their quality of life [9].
Likewise, Strauss et al. indicated that the quality of life for patients with iron-deficient anaemia improved following treatment[10]. Alexithymia refers to the challenge of identifying and articulating emotions and is more prevalent among men [11,12]. The reduction in emotional awareness associated with alexithymia is evident in numerous mental and neurological diseases [13]. Patients diagnosed with restless legs syndrome attributed to iron insufficiency had greater levels of alexithymia compared to the healthy control group [14]. While insufficient vitamin levels may contribute to the pathogenesis of alexithymia [15], the correlation between iron deficiency and alexithymia has, to our knowledge, not been investigated. This study sought to examine alexithymia, psychiatric symptoms, quality of life, and iron deficiency diagnoses in patients with iron deficiency anaemia, prevalent among women aged 18-49, in relation to laboratory values, and to compare our findings with those of a healthy control group.
2. Materials and Methods
Approval from the local ethics committee was secured on 25 September 2023, under the reference number E-50716828-100-375697. This study adhered to the ethical criteria outlined in the 2013 edition of the Declaration of Helsinki. The cohort comprised 160 women diagnosed with iron deficiency anaemia, who were hospitalised at the internal medicine clinic at Elazig Fethi Sekin City Hospital between September 2023 and February 2024, fulfilled the study requirements, and received no therapy. The healthy control group, comparable to the patient group for sociodemographic factors, comprised 155 healthy women who attended Elazig Fethi Sekin City Hospital for annual check-ups and exhibited no medical issues. The internal medicine specialist assessed the participants. A psychiatrist subsequently conducted structured interviews based on the DSM-5, lasting approximately 30 minutes. Serum ferritin levels of 15 ng/mL or lower and haemoglobin levels below 12 g/dL, regarded as the most effective non-invasive indicators for diagnosing iron deficiency, were established as criteria [16]. The study's inclusion criteria were female participants aged 18-49, absence of known psychiatric disorders or intellectual disabilities, no organic or neurological conditions that could impair cognitive function, a diagnosis limited to iron deficiency anaemia within the patient group, and exclusion of anaemia caused by factors other than iron deficiency. The participants underwent evaluation by the same psychiatrist using the Structured Clinical Interview for DSM-5, and those having mental diagnoses were eliminated from the study. Nine individuals from the patient cohort declined to participate in the study, while five persons from the control group were excluded from the evaluation due to incomplete responses on the study scales. Consequently, 151 female patients constituted the iron deficiency anaemia group, while 150 healthy female people comprised the control group. Upon acquiring the written consent of all participants, their sociodemographic data and laboratory values were documented. The Beck Depression Inventory, State-Trait Anxiety Inventory, World Health Organisation Quality of Life Scale Short Form Turkish Version, and Toronto Alexithymia Scale-20 were administered.
2.1. Statistical Examination
The Statistical Package for the Social Sciences [SPSS] version 21.0 was employed for the statistical analysis. The categorical variables are displayed as frequencies and percentages. The continuous variables were evaluated using the Kolmogorov-Smirnov test and histograms to determine the normality of their distributions. The normally distributed numerical parameters were compared using Student's t-test, while non-normally distributed data were analysed with the Mann-Whitney U test. Categorical variables were compared using Chi-square tests or Fisher's exact tests where applicable. The correlation between the two variables was assessed using Spearman's or Pearson's correlation coefficient. A statistical difference was deemed significant when the p-value was less than 0.05. Univariate and multivariate logistic regression analyses employing a stepwise methodology were conducted. Variables that maintained significance [p < 0.05] in the multivariate model were deemed independent predictors of alexithymia. Hosmer-Lemeshow goodness-of-fit statistics were conducted, and odds ratios [ORs] together with 95% confidence intervals [CIs] were computed for each predictor.
3. Results
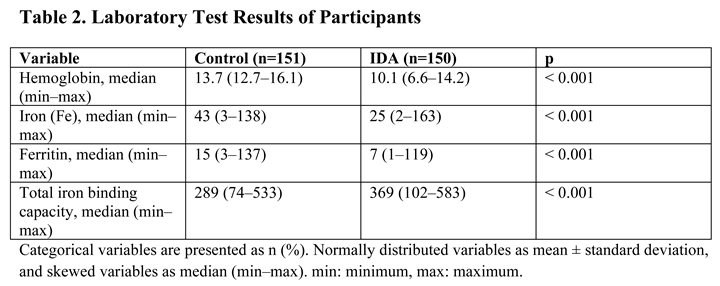
The study comprised 301 female volunteers, with 150 assigned to the iron-deficiency anaemia group and 151 to the control group. No substantial variations were observed in marital status, educational attainment, home location, or intake of alcohol and cigarettes. The Iron-deficiency Anaemia Group was marginally older [36 [16–68] vs 31 [18–64]] and exhibited a higher household income level than the control group. Table 1 delineates the baseline features of the patients. Regarding laboratory test outcomes and various scales employed; haemoglobin, iron, and ferritin levels, along with WHOQOL-BREF-TR and STAİ Form TX-1 scores, were diminished, whereas total iron binding capacity and Toronto Alexithymia Scale scores were elevated in the Iron-deficiency.
When patients were categorised into two groups [without alexithymia vs. with likely alexithymia or alexithymia], 126 [42%] patients were identified as having probable alexithymia or alexithymia. No significant variations in age or demographic data were observed between the groups, with the exception of place of residence.
The prevalence of iron-deficiency anaemia, Beck Depression Scale scores, and STAİ Form TX-2 scores was elevated in the likely alexithymia group compared to the non-alexithymia group, whereas WHOQOL-BREF-TR scores were diminished in the former group [Table 4].
Table 5 presents the correlations between Toronto Alexithymia Scale scores and various numerical parameters. The alexithymia scores were positively correlated with total iron binding capacity, the Beck Depression Scale, and the STAI Form TX-2 scores. Conversely, significant negative correlations were observed with haemoglobin levels, iron [Fe], and WHOQOL-BREF-TR scores.
A binary logistic regression analysis was subsequently performed to determine the independent predictors of probable alexithymia or alexithymia. Multivariate analysis revealed that elevated total iron binding capacity [OR: 1.003; 95% CI: 1.000–1.006; p = 0.044], higher STAI Form TX-2 scores [OR: 1.098; 95% CI: 1.050–1.147; p < 0.001], and lower WHOQOL-BREF-TR scores [OR: 0.966; 95% CI: 0.950–0.982; p < 0.001] were independently associated with probable alexithymia or alexithymia.
Table 6 provides a summary of the logistic regression results. The following instruments were employed in the present study: the Beck Depression Scale, WHOQOL-BREF-TR, STAI Forms TX-1 and TX-2, and the Toronto Alexithymia Scale.
A sociodemographic and clinical data form, developed by the researchers, was utilised in alignment with information derived from clinical experience and vetted sources, tailored to the study's objectives. The Beck Depression Scale [BDS] was created to assess the risk of depression, the intensity of depressive symptoms, and variations in severity among individuals. A validity and reliability assessment of the scale in Turkey was done [17,18]. The Cronbach's alpha reliability coefficient for the overall scale in this investigation was determined to be 0.78.
The Toronto Alexithymia Scale [TAS-20] is a self-assessment tool including 20 items designed to evaluate the degree of alexithymia. A validity and reliability evaluation of the scale in Turkish was done [19,20]. This study established the cut-off values for alexithymia: a score of 51 or less indicated non-alexithymia, a score between 52 and 60 suggested potential alexithymia, and a score of 61 or above confirmed alexithymia. The Cronbach's alpha reliability coefficient for the entire scale was determined to be 0.80. The State-Trait Anxiety Inventory [STAI Form TX-1, TX-2] was created by Spielberger. Validity-reliability research was undertaken in Turkey. The inventory comprises two sections and contains 40 products. STAI-1 evaluates state anxiety through items 1-20, while STAI-2 analyses trait anxiety via things 21-40. The average score on the scale ranges from 36 to 41 [21,22]. This study evaluated the Cronbach's alpha reliability coefficient of the scale as 0.80 for STAI 1 and 0.82 for STAI 2. The Turkish version of the World Health Organisation Quality of Life Scale Short Form [WHOQOL-BREF-TR] was established by the WHO, and a study on its validity and reliability in Turkish was done [23,24].
4. Discussion
This study revealed that women with iron deficiency anaemia exhibited elevated levels of alexithymia, moderate anxiety, and diminished quality of life in comparison to healthy controls. The prevalence of iron deficiency anaemia, depressive symptoms, and trait anxiety levels escalated in individuals who struggled to articulate their emotions, resulting in a diminished quality of life. The alexithymia levels in female patients with iron-deficient anaemia were correlated with elevated iron-binding capacity, heightened anxiety levels, and diminished quality of life. Emotional behaviours are influenced by iron levels in the brain, especially in cases of iron shortage. The correlation between hunger and depression has been proposed in women of reproductive age. Lee et al. demonstrated that patients with iron-deficient anaemia exhibited elevated anxiety levels and a high prevalence of depression [26]. A separate investigation indicated that the treatment of iron deficiency alleviated feelings of anxiety and sadness in patients [27]. Furthermore, diminished haemoglobin and plasma ferritin levels have been correlated with depression [28,29]. Our investigation revealed no disparity in depressive symptoms between women with iron deficiency and healthy women; however, those with anaemia exhibited moderate levels of state anxiety. In this context, our research diverges from existing literature. Anaemia diminishes patients' quality of life, which deteriorates more as haemoglobin levels decline [30]. Iron supplementation enhances the quality of life for those with anaemia [31]. Prior research on individuals with anaemia indicates that their quality of life diminishes across nearly all domains, encompassing emotional well-being and overall health perception, with the most significant decline observed in aspects connected to physical activity. Furthermore, a decline in haemoglobin levels correlates with a deterioration in quality of life [32,33]. Our study indicated that the quality of life for women with iron-deficient anaemia was diminished. In this regard, our research aligns with other studies. Our study's most significant conclusion is that alexithymia scores elevated in patients with iron-deficient anaemia. Alexithymia, characterised by the inability to identify and articulate emotions, arises from the influence of dopaminergic and glutamatergic systems in the brain [34]. Alexithymia is known to be prevalent, particularly in neurological diseases characterised by dopaminergic dysfunction [35]. The alexithymia levels in patients with restless legs syndrome attributed to iron insufficiency were similarly shown to be elevated [14]. The iron element, integral to the production and operation of neurotransmitters, may induce alexithymia symptoms via the potential dopaminergic system. Moreover, individuals with alexithymia may exhibit symptoms of malnutrition and eating disorders, such as food intake restriction, binge eating, and/or vomiting [36]. This indicates that this circumstance may induce iron shortage in individuals with alexithymia, whereas those with iron deficiency anaemia may exhibit alexithymia, so corroborating our findings. Alexithymia escalates with a reduction in ferritin levels [37]. Our study revealed a significant prevalence of iron deficiency anaemia among individuals with elevated alexithymia scores. A positive link was identified between alexithymia and iron binding capacity, whereas a negative correlation was detected with haemoglobin and iron levels. It was also established that an increase in alexithymia correlated with heightened depressive symptoms and trait anxiety levels, while quality of life diminished. In this context, our data align with existing literature for comparable parameters assessed in other disorders [38,39]. Consequently, individuals with alexithymia are perceived to have heightened anxiety and depression, perhaps leading to a diminished quality of life. Moreover, it may be asserted that elevated iron binding capacity, diminished quality of life, and heightened trait anxiety are independently linked components contributing to the onset of alexithymia.
The cross-sectional design of our study constitutes one of our shortcomings. One of our strengths is that the sample group comprised females, and there is a lack of prior studies assessing the link between anxiety, depression, quality of life, and alexithymia in patients with iron deficiency anaemia.
5. Conclusions
Alexithymia may serve as a clinical marker for the early detection of iron-deficiency anaemia, even prior to the availability of laboratory data. Future studies with larger sample sizes are warranted to further investigate the relationship between iron-deficiency anaemia and alexithymia, ideally incorporating analyses of underlying neurobiological mechanisms, particularly those involving neurotransmitters. A clearer understanding of this association could facilitate non-invasive diagnostic approaches to anaemia. Moreover, the evaluation and management of emotional symptoms such as sadness and anxiety during treatment and follow-up may contribute to improved quality of life in affected patients.
Author Contributions
Conceptualization, B.A.K.; methodology, B.A.K., T.T.Y.; software, B.A.K., T.T.Y.; validation, B.A.K., T.T.Y., S.Y.; formal analysis, B.A.K.; investigation, B.A.K., S.Y.; resources, B.A.K.; data curation, B.A.K., T.T.Y.; writing—original draft preparation, B.A.K.; writing—review and editing, T.T.Y., S.Y.; visualization, B.A.K.; supervision B.A.K.; project administration, B.A.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The work received ethical approval from the Firat University Non-Interventional Research Ethics Committee on September 25, 2023, under the reference number E-50716828-100-375697.
Informed Consent Statement
Before the study commenced, the participants executed the Informed Consent Form.
Data Availability Statement
The authors affirm that the data underpinning the findings of this investigation are accessible within the article and additional materials.
Conflicts of Interest Statement
The writers own no interest-based affiliations.
References
- WHO. Anaemia. An Overview (WHO, 2021).
- Alem, A. Z. , Efendi, F., McKenna, L., Felipe-Dimog, E. B., Chilot, D., Tonapa, S. I.,..., Zainuri, A. Prevalence and factors associated with anemia in women of reproductive age across low-and middle-income countries based on national data. Scientific Reports 2023, 13, 20335. [Google Scholar] [CrossRef] [PubMed]
- East P, Doom JR, Blanco E, Burrows R, Lozoff B, Gahagan S. Iron deficiency in infancy and neurocognitive and educational outcomes in young adulthood. Dev Psychol. 2021, 57, 962–975. [Google Scholar] [CrossRef] [PubMed]
- Demirci, K. , BAŞ, F. Y., Arslan, B., Salman, Z., Akpinar, A.,, DEMİRDAŞ, A. Demir Eksikliği Anemisi Olan Kadın Hastalarda Erişkin Dikkat Eksikliği Hiperaktivite Belirtilerinin ve Tanısının Araştırılması. Arch Neuropsychiatry 2017, 54, 72–77. [Google Scholar] [CrossRef]
- Ferreira A, Neves P, Gozzelino R. Multilevel Impacts of Iron in the Brain: The Cross Talk between Neurophysiological Mechanisms, Cognition, and Social Behavior. Pharmaceuticals 2019, 12, 126. [Google Scholar] [CrossRef]
- Shah, H. E. , Bhawnani, N., Ethirajulu, A., Alkasabera, A., Onyali, C. B., Anim-Koranteng, C.,, Mostafa, J. A. (.
- Kim, J.; Wessling-Resnick, M. Wessling-Resnick M. Iron and mechanisms of emotional behavior. Journal of Nutritional Biochemistry 2014, 25, 1101–1107. [Google Scholar] [CrossRef]
- Ahmed T, Lamoureux-Lamarche C, Berbiche D, Vasiliadis HM. The association between anemia and depression in older adults and the role of treating anemia. Brain Behav. 2023, 13, e2973. [Google Scholar] [CrossRef]
- Kim, Y. J. , Han, K. D., Cho, K. H., Kim, Y. H.,, Park, Y. G. Anemia and health-related quality of life in South Korea: data from the Korean national health and nutrition examination survey 2008–2016. BMC public health 2019, 19, 1–8. [Google Scholar] [CrossRef]
- Strauss WE, Auerbach M. Health-related quality of life in patients with iron deficiency anemia: impact of treatment with intravenous iron. Patient Relat Outcome Meas. 2018, 9, 285–298. [Google Scholar] [CrossRef]
- Hogeveen J, Grafman J. Alexithymia. Handb Clin Neurol. 2021, 183, 47–62. [Google Scholar] [CrossRef]
- Levant, R. F. , Hall, R. J., Williams, C. M.,, Hasan, N. T. Gender differences in alexithymia. Psychology of men, masculinity 2009, 10, 190. [Google Scholar]
- Ricciardi, L. , Demartini, B., Fotopoulou, A.,, Edwards, M. J. Alexithymia in neurological disease: a review. The Journal of neuropsychiatry and clinical neurosciences 2015, 27, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz O, Şengül Y, Şengül HS, Parlakkaya FB, Öztürk A. Investigation of alexithymia and levels of anxiety and depression among patients with restless legs syndrome. Neuropsychiatr Dis Treat. 2018, 14, 2207–2214. [Google Scholar] [CrossRef]
- Terock, J. , Hannemann, A., Weihs, A., Janowitz, D.,, Grabe, H. J. Alexithymia is associated with reduced vitamin D levels, but not polymorphisms of the vitamin D binding-protein gene. Psychiatric Genetics 2021, 31, 126–134. [Google Scholar] [CrossRef]
- Çoban E, Timurağaoğlu A. Yaşlı hastalarda demir eksikliği anemisine yaklaşım. T Klin J Med Sci 2004, 24, 267–270. [Google Scholar]
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961, 4, 561–571. [Google Scholar] [CrossRef]
- Hisli, N. Beck Depresyon Ölçeğinin bir Türk örnekleminde geçerlilik ve güvenilirliği [Reliability and validity of Beck Depression Scale in a Turkish sample] Psikoloji Dergisi. 1988, 6, 118–122. 6.
- Bagby RM, Parker JD, Taylor GJ. The twenty-item Toronto Alexithymia Scale – I. Item selection and cross-validation of the factor structure. J Psychosom Res. 1994, 38, 23–32. [Google Scholar] [CrossRef]
- Güleç H, Köse S, Güleç MY. Reliability and factorial validity of the Turkish version of the 20-item Toronto alexithymia scale (TAS-20) Klinik Psikofarmakol Bülteni. 2009, 19, 214–220.
- Öner N, Le Compte A. Süreksiz durumluk /sürekli kaygı envanteri el kitabı. 1. Baskı. İstanbul: Boğaziçi Üniversitesi Yayını, 1983; 1-26.
- Spielberger CD, Gorsuch RL, Lushene RE. Test manual for the State Trait Anxiety Inventory. 1st ed. California: Consulting Psychologists Press, 1970.
- The WHOQOL Group: The world health organization quality of life assessment (WHOQOL): Development and general psychometric properties. Social Science and Medicine 1998, 46, 1569–1585. [CrossRef]
- Eser SY, Fidaner H, Fidaner C, Elbi H, Eser E: Yaşam kalitesinin ölçülmesi, WHOQOL-100 ve WHOQOL-BREF. 3P Dergisi 1999 ;(7): 5-13 (Ek 2).
- gholamreza Noorazar, S. , Ranjbar, F., Nemati, N., Yasamineh, N.,, Kalejahi, P. Relationship between severity of depression symptoms and iron deficiency anemia in women with major depressive disorder. Journal of Research in Clinical Medicine 2015, 3, 219–224. [Google Scholar]
- Lee, H. S. , Chao, H. H., Huang, W. T., Chen, S. C. C.,, Yang, H. Y. Psychiatric disorders risk in patients with iron deficiency anemia and association with iron supplementation medications: a nationwide database analysis. BMC psychiatry 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Arshad, H. , Arshad, A., Hafiz, M. Y., Muhammad, G., Khatri, S.,, Arain, F. Psychiatric Manifestations of Iron Deficiency Anemia-A Literature Review. European Psychiatry 2023, 66, S243–S244. [Google Scholar] [CrossRef]
- Corwin EJ, Murray-Kolb LE, Beard JL. Low hemoglobin level is a risk factor for postpartum depression. J. Nutr. 2003, 133, 4139–4142. [Google Scholar] [CrossRef]
- Albacar G, Sans T, Martin-Santos R et al. An association between plasma ferritin concentrations measured 48 h after delivery and postpartum depression. J. Affect. Disord. 2011, 131, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Wouters HJCM, van der Klauw MM, de Witte T, Stauder R, Swinkels DW, Wolffenbuttel BHR, Huls G. Association of anemia with health-related quality of life and survival: a large population-based cohort study. Haematologica. 2019, 104, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Jain, A. K. , Vare, S., Sircar, S., Joshi, A. D.,, Jain, D. Impact of iron deficiency anemia on quality of life in patients with ulcerative colitis. Advances in Digestive Medicine 2023, 10, 15–20. [Google Scholar] [CrossRef]
- AlexanderMKewalramaniRAgodoaIGlobeDAssociation of anemia correction with health related quality of life in patients not on dialysisCurr Med Res Opin200723122997300817958944.
- Strauss, W. E. ,, Auerbach, M. Health-related quality of life in patients with iron deficiency anemia: impact of treatment with intravenous iron. Patient related outcome measures.
- Schore, AN. Relational trauma, brain development and dissociation. In: Ford JD, Courtois CA, editors. Treating Complex Traumatic Stress Disorders in Children and Adolescents: Scientific Foundations and Therapeutic Models. New York: The Guilford Press;
- Ricciardi, L. , Demartini, B., Fotopoulou, A.,, Edwards, M. J. Alexithymia in neurological disease: a review. The Journal of neuropsychiatry and clinical neurosciences 2015, 27, 179–187. [Google Scholar] [CrossRef]
- Nowakowski, M. E. , McFarlane, T.,, Cassin, S. Alexithymia and eating disorders: a critical review of the literature. Journal of eating disorders 2013, 1, 1–14. [Google Scholar] [CrossRef]
- Sheikh, A. D. , Babienko, V.,, Kobolev, E. Influence of latent iron deficiency on cognitive abilities in students. Journal of Education, Health and Sport 2022, 12, 117–124. [Google Scholar] [CrossRef]
- Namdar, N. D. ,, ARIKAN, İ. The relationship between alexithymia, anxiety, depression, and severity of the disease in psoriasis patients. Journal of Surgery and Medicine 2020, 4, 226–229. [Google Scholar]
- Tesio V, Di Tella M, Ghiggia A, Romeo A, Colonna F, Fusaro E, Geminiani GC, Castelli L. Alexithymia and Depression Affect Quality of Life in Patients With Chronic Pain: A Study on 205 Patients With Fibromyalgia. Front Psychol. 2018, 9, 442. [Google Scholar] [CrossRef]

Table 1.
Baseline Characteristics of Participants.
| Characteristic | Control (n=151) | IDA Group (n=150) | p-value |
|---|---|---|---|
| Gender | Female: 151 (100%) | Female: 150 (100%) | |
| Marital Status | Single/Widowed: 62 (41.1%) Married: 89 (58.9%) |
Single/Widowed: 49 (32.7%) Married: 101 (67.3%) |
0.131 |
| Age, median (min–max) | 31 (18–64) | 36 (16–68) | 0.048 |
| Level of Education | Illiterate: 1 (0.7%) Primary: 15 (9.9%) High school: 33 (21.9%) University: 102 (67.5%) |
Illiterate: 1 (0.7%) Primary: 15 (10%) High school: 40 (26.7%) University: 94 (62.7%) |
0.803 |
| Place of Residence | Rural: 6 (4%) Urban: 145 (96%) |
Rural: 7 (4.7%) Urban: 143 (95.3%) |
0.767 |
| Household Income Level | Low: 28 (18.5%) Medium: 111 (73.5%) High: 12 (8%) |
Low: 14 (9.3%) Medium: 129 (86%) High: 7 (4.7%) |
0.026* |
| Alcohol Consumption | No: 144 (95.4%) Yes: 7 (4.6%) |
No: 145 (96.7%) Yes: 5 (3.3%) |
0.564 |
| Smoking | No: 126 (83.4%) Yes: 25 (16.6%) |
No: 114 (76%) Yes: 36 (24%) |
0.108 |
| Psychiatric Illness History | No: 148 (98%) Yes: 3 (2%) |
No: 145 (96.7%) Yes: 5 (3.3%) |
0.501 |
| Family Psychiatric History | No: 148 (98%) Yes: 3 (2%) |
No: 145 (96.7%) Yes: 5 (3.3%) |
0.501 |
| Suicide Attempt | No: 150 (99.3%) Yes: 1 (0.7%) |
No: 149 (99.3%) Yes: 1 (0.7%) |
0.996 |
| IDA Treatment History | No: 68 (45%) Yes: 83 (55%) |
No: 47 (31.3%) Yes: 103 (68.7%) |
0.014* |
* p-values indicate significant differences between groups. Categorical variables are presented as n (%); normally distributed variables as mean ± standard deviation; skewed variables as median (min–max). min: minimum, max: maximum.
 |
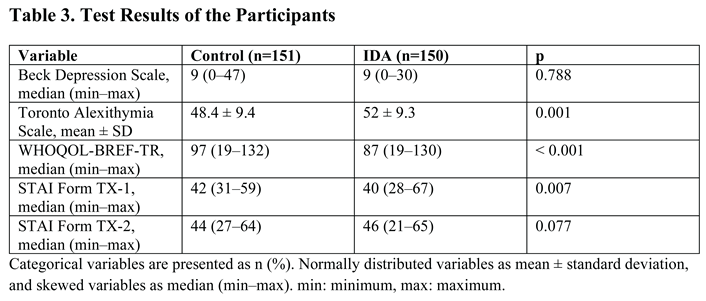 |
Table 4.
Characteristics of Participants Between No Alexithymia and Probable Alexithymia or Alexithymia.
Table 4.
Characteristics of Participants Between No Alexithymia and Probable Alexithymia or Alexithymia.
| Variable | No Alexithymia (n=175) | Probable Alexithymia or Alexithymia (n=126) | p |
|---|---|---|---|
| Age, median (min–max) | 34 (16–64) | 35 (18–68) | 0.333 |
| Marital Status | Single or widowed: 67 (38.3) Married: 108 (61.7) |
Single or widowed: 44 (34.9) Married: 82 (65.1) |
0.551 |
| Level of Education | Illiterate: 14 (8) Primary school: 47 (26.9) High school: 112 (64) University: 2 (1.1) |
Illiterate: 16 (12.7) Primary school: 26 (20.6) High school: 84 (66.7) University: 0 (0) |
0.230 |
| Place of residence | Rural: 4 (2.3) Urban: 171 (97.7) |
Rural: 9 (7.1) Urban: 117 (92.9) |
0.041 |
| Household income level | Low: 31 (17.7) Medium: 133 (76) High: 11 (6.3) |
Low: 11 (8.7) Medium: 107 (84.9) High: 8 (6.3) |
0.083 |
| Alcohol consumption | No: 168 (96) Yes: 7 (4) |
No: 121 (96) Yes: 5 (4) |
0.989 |
| Smoking | No: 139 (79.4) Yes: 36 (20.6) |
No: 101 (80.2) Yes: 25 (19.8) |
0.876 |
| Iron-deficiency Anemia | No: 101 (57.7) Yes: 74 (42.3) |
No: 50 (39.7) Yes: 76 (60.3) |
0.002 |
| Hemoglobin, median (min–max) | 13 (6.6–16) | 11.4 (7–16.1) | 0.017 |
| Iron (Fe), median (min–max) | 34 (2–133) | 29 (2–163) | 0.062 |
| Ferritin, median (min–max) | 11 (2–137) | 9 (1–135) | 0.288 |
| Total iron binding capacity, median (min–max) | 302 (74–583) | 334 (130–571) | 0.084 |
| Beck Depression Scale, median (min–max) | 7 (0–34) | 10 (0–47) | < 0.001 |
| WHOQOL-BREF-TR, median (min–max) | 98 (19–132) | 86 (49–115) | < 0.001 |
| STAI Form TX-1, median (min–max) | 42 (31–59) | 41 (28–67) | 0.443 |
| STAI Form TX-2, median (min–max) | 44 (21–65) | 46 (31–64) | < 0.001 |
Categorical variables are presented as n (%). Normally distributed variables as mean ± standard deviation, and skewed variables as median (min–max). min: minimum, max: maximum.
Table 5.
Correlation Between Toronto Alexithymia Scale and Other Numerical Parameters.
| Parameter | r | p-value |
|---|---|---|
| WHOQOL-BREF-TR | -0.431 | < 0.001* |
| Beck Depression Scale | 0.302 | < 0.001* |
| STAI Form TX-2 | 0.169 | 0.003* |
| Hemoglobin (Hb) | -0.175 | 0.002* |
| Iron (Fe) | -0.164 | 0.004* |
| Total iron binding capacity | 0.117 | 0.042* |
| STAI Form TX-1 | -0.095 | 0.102 |
| Ferritin | -0.069 | 0.235 |
| Age | 0.009 | 0.873 |
* p < 0.05; Pearson correlation was used.
Table 6.
Independent Predictors for Probable Alexithymia or Alexithymia.
| Risk Factors | Adjusted OR (95% CI) | p-value |
|---|---|---|
| Total iron binding capacity | 1.003 (1.000–1.006) | 0.044* |
| Beck Depression Scale | 1.032 (0.998–1.068) | 0.068 |
| WHOQOL-BREF-TR | 0.966 (0.950–0.982) | < 0.001* |
| STAI Form TX-2 | 1.098 (1.050–1.147) | < 0.001* |
OR: odds ratio; 95% CI: 95% confidence interval. The p-value of the Hosmer–Lemeshow test was 0.059.The following variables were included in the multivariate logistic regression: Level of Education, Household Income, Place of Residence, Iron-deficiency Anemia, Beck Depression Scale, WHOQOL-BREF, STAI-2, Iron (Fe), Total Iron Binding Capacity. * p < 0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



