
Submitted:
19 June 2025
Posted:
20 June 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: Dentistry is recognized as one of the most stressful healthcare professions, with both physical and psychological demands intensifying after the COVID-19 pandemic period. Irregular work schedules, poor dietary habits, and elevated burnout levels necessitate targeted interventions to support dentists’ well-being and performance. This review explores the effectiveness of educational dietary strategies implemented in workplace settings to reduce health risks and improve professional outcomes. Methods: A systematic review was conducted following PRISMA guidelines. Databases searched included PubMed, Scopus, and the Cochrane Library, covering studies published between 2019 and March 2025. Twenty studies met predefined inclusion criteria, focusing on dietary interventions targeting dentists or healthcare professionals, with relevance to occupational stress, burnout, dietary behavior, or performance. Results: Dentists frequently exhibited poor nutritional behaviors, such as meal skipping, irregular eating, and micronutrient deficiencies. Educational dietary strategies, such as structured meal planning, personalized nutrition education, and provision of antioxidant-rich foods, were linked to improvements in energy, mood, and cognitive focus. Interventions integrating physical activity and stress management yielded additional benefits, including reduced burnout and enhanced psychological resilience. Long-term programs incorporating food literacy and organizational support demonstrated sustained improvements in health and work performance. Conclusions: Educational dietary interventions in dental workplace settings are a promising approach to reduce burnout, enhance resilience, and sustain professional functioning. However, broader implementation requires institutional commitment and integration into occupational health policies.
Keywords:
dentists
; healthcare professionals
; workplace nutrition
; dietary interventions
; burnout
; stress management
; occupational health
; dietary habits
; nutrition education
1. Introduction
Dentistry is widely recognized as one of the most demanding healthcare professions, characterized by high levels of psychological pressure and physical strain [1,2,3,4]. These challenges have intensified in recent years, particularly in the wake of the COVID-19 pandemic, which significantly impacted the health and well-being of dental professionals [1,5,6]. As recovery efforts continue, workplace interventions, especially those targeting dietary habits and mental resilience, are increasingly recognized as essential [7,8]. Extended working hours, heavy clinical loads, and irregular schedules contribute to burnout, poor nutrition, and reduced job performance among dentists [6].
In this sense, workplace dietary interventions have gained attention as practical and sustainable strategies to support both physical and psychological health in healthcare environments [3,7,8]. Numerous studies have highlighted the strong association between stress, poor eating habits, and burnout [9,10]. Τhis is particularly important for dental professionals who experience high cognitive and emotional demands [11]. Recent reviews highlight the importance of nutrition-centered workplace programs in enhancing energy management and enhancing long-term resilience for healthcare professionals including dentists [12,13].
During the pandemic, widespread disruptions in eating patterns were observed among healthcare workers, often triggered by increased stress, altered routines, and limited access to nutritious food [13,14]. Dentists reported elevated levels of emotional eating, irregular meals, and higher consumption of calorie-dense foods [15,16], patterns that frequently coincided with anxiety, depression, and occupational dissatisfaction [17,18].
Emerging research identifies dietary education and resilience-building as key strategies for supporting the recovery and sustained well-being of dental professionals [1,19,20]. Interventions such as nutrition education, structured meal planning, and improved food accessibility at the workplace have shown positive effects on both physiological outcomes and professional performance [21,22]. Educational approaches that incorporate mental health support, behavior change techniques, and personalized feedback appear especially effective in driving sustainable improvements [23,24]. Moreover, interdisciplinary collaboration involving nutritionists, occupational health experts, and dental educators further enhances the adaptability and impact of these interventions [25,26]. This collaborative model allows for personalization based on individual factors such as gender, age, work conditions, and stress levels [1,18,27,28]. Special attention is also needed for shift-working dentists, who are at increased risk for irregular meal patterns, high-calorie snacking, and circadian rhythm disruptions [29,30,31]. Tailored programs that include meal timing guidance and nutrition strategies targeting stress reduction have shown promise in addressing these challenges [6,32,33,34,35,36].
Recent studies emphasize the importance of embedding nutrition education within the professional development of healthcare workers, noting its role in enhancing both clinical competence and personal well-being [37,38,39]. Building on this foundation, this systematic review aims to synthesize current evidence on educational components within workplace dietary interventions for dentists. Its objectives are to identify effective practices, highlight knowledge gaps, and propose future directions to improve nutritional resilience and occupational well-being in dentistry. Specifically, it addresses the research question: “Which educational strategies within dietary interventions are most effective in promoting dentists’ health in the post-pandemic context?”
2. Materials and Methods
For this systematic review, the search period (January 2019 to March 2025) was chosen to capture the most recent developments in workplace dietary interventions, particularly those influenced by the COVID-19 pandemic, which had significant impacts on healthcare working conditions, dietary behaviors, and stress-related outcomes. The post-pandemic period has also seen a marked increase in research focused on occupational health resilience and nutrition-based interventions for healthcare professionals, making this timeframe highly relevant to the objectives of this review. Keywords included combinations of “dentists,” “nutrition,” “burnout,” and “workplace dietary interventions,” using appropriate Boolean operators to refine results.
Studies were eligible for inclusion if they were published in English, between 2019 and 2025, and focused on dentists or healthcare professionals where nutrition was clearly linked to occupational health outcomes. We included cross-sectional studies, case-control studies, interventional studies, and systematic reviews that presented original data [40,41]. Narrative reviews, opinion pieces, editorials, letters, and studies without direct relevance to nutrition or dentistry were excluded.
During the screening process, studies were excluded for the following primary reasons: Reason 1: Irrelevant population: Studies did not focus on dental professionals or comparable healthcare workers (e.g., studies of the general population or unrelated occupational groups). Reason 2: Intervention mismatch: Studies did not include dietary, nutritional, or workplace-based interventions (e.g., focused solely on pharmacological or physical activity interventions without any dietary component). Reason 3: Inadequate outcomes: Studies did not report on relevant outcomes, such as health resilience, professional well-being, performance, or nutritional behavior changes. Reason 4: Study type: Non-original research (e.g., editorials, letters, opinion pieces) or studies lacking full-text availability were excluded. Reason 5 Duplicates: Duplicate records identified across databases were removed.[22].
Study selection followed PRISMA guidelines and used Rayyan QCRI for screening [42,43]. Two reviewers independently selected studies and extracted data on sample size, intervention type, and outcomes related to stress, dietary behavior, and performance [10,18,35]. Quality was assessed using the Newcastle-Ottawa Scale and AMSTAR 2 tools [3,12] Data analysis was descriptive, using SPSS v28.0. Figure 1 presents the PRISMA flowchart outlining the study's search and selection process.
3. Results
The bar chart in Figure 2, illustrates the distribution of scientific publications selected for this systematic review, categorized by year of publication from 2019 to 2024. These 22 studies, identified through a comprehensive search in PubMed, Scopus, and the Cochrane Library, focus on workplace dietary interventions and their role in supporting dentists’ health, performance, and psychological resilience in the post-COVID-19 context. The increased volume of relevant research in recent years, particularly in 2021 and 2024, reflects a growing recognition of the heightened physical and mental stress that dental professionals face, and the urgent need for targeted nutritional strategies within clinical environments. The timeline visualized in the diagram aligns with the pandemic’s impact on occupational well-being, as well as with a global shift toward integrating structured dietary planning, food literacy, and organizational support as part of health promotion in the workplace. This temporal analysis further reinforces the emerging consensus that improving dietary habits among dentists is essential to managing stress, preventing burnout, and maintaining sustainable professional performance.
In Table S1, we present the quality assessment of included studies using Newcastle-Ottawa Scale (NOS) and AMSTAR 2 tools.
Summary of Included Studies
A total of 22 studies were included in this review, comprising systematic reviews, meta-analyses, cross-sectional studies, randomized controlled trials, prospective cohort studies, and educational intervention studies. The selected studies covered a broad range of healthcare professionals with a particular focus on dentists, but also including other healthcare workers such as physicians, nurses, and allied health professionals. The populations studied ranged from university students and early-career healthcare workers to experienced clinical staff across various settings. Interventions included workplace dietary interventions, nutrition education, behavior change programs, and broader multicomponent wellness approaches. Several studies also examined psychosocial factors (e.g., stress, burnout, resilience), emotional eating, and the effects of shift work on dietary habits and occupational well-being. Outcomes most frequently reported included improvements in dietary behaviors (e.g., fruit and vegetable intake, reduction of processed foods), metabolic markers (BMI, cholesterol, blood sugar), mental health (depression, stress, anxiety), and occupational performance. Systematic reviews and meta-analyses highlighted the effectiveness of workplace interventions but also noted heterogeneity across interventions and outcomes. Limitations commonly reported across studies included reliance on self-reported data, small sample sizes, short intervention durations, lack of control groups, and challenges in long-term follow-up. Despite these limitations, the body of evidence supports the role of nutrition-focused interventions in promoting health resilience and professional well-being among dental professionals and healthcare workers.
In Table 2 we present the basic characteristics of the included studies.
Type of Study and Study Design
The dataset presents a diverse array of research designs, reflecting the methodological breadth and scientific rigor of recent investigations into workplace nutrition, mental well-being, and occupational health among healthcare professionals with an emphasis on dentists. The included studies span systematic reviews, meta-analyses, narrative reviews, cross-sectional studies, observational cohort studies, randomized controlled trials (RCTs), and educational intervention studies, conducted across both single-center and multi-country settings. A substantial proportion of the studies consists of systematic reviews and meta-analyses, such as those by Olesinska et al. (2025) [44], Panchbhaya et al. (2022) [49], and Rachmah et al. (2021) [22], which synthesized outcomes across multiple interventions targeting workplace nutrition, burnout, and well-being. These reviews provide higher-level evidence by aggregating outcomes such as BMI reduction, improved diet quality, and mental health indicators. Similarly, Schliemann and Woodside (2019) [21] conducted a review of reviews, offering additional synthesis of evidence across workplace dietary interventions.
By contrast, narrative reviews such as those of Shiri et al. 2023 [33]; Sovold et al. 2021 [50]; Kris-Etherton et al. 2021 [8]) provided broader theoretical perspectives on occupational well-being, nutrition, and mental health, particularly in the post-COVID-19 context. While lacking statistical meta-analysis, these reviews contribute valuable insight into global trends and conceptual frameworks.
Further, cross-sectional studies represented the largest number of primary studies in the dataset, including those by Mangoulia et al. (2025) [18], Hassani et al. (2020) [55], Chen et al. (2023) [35], Peixoto et al. (2021) [53], and Pai et al. (2021) [54], offering detailed snapshots of dietary habits, burnout, stress, sleep quality, emotional eating, and oral health behaviors in healthcare workers and dental professionals. Though limited in establishing causality, these studies highlight prevalent risk factors, behaviors, and correlations in the healthcare sector during and after the pandemic.
A smaller but important segment of studies included randomized controlled trials (RCTs), such as Moro et al. (2022) [48], which applied controlled designs to assess nutrition education interventions, providing robust evidence for their impact on BMI, fasting blood sugar, and nutritional knowledge. Educational intervention studies (e.g., Mancin et al. 2023; Di Prinzio et al. 2025) tested innovative training approaches (such as active learning) to improve nutritional competencies and clinical practice [38,45].
Additionally, observational cohort studies, such as Gilbert et al. (2023) [47] and Tenelanda-Lopez et al. (2020) [56], used longitudinal data to track workplace-related changes in diet, physical activity, and mental health over time, particularly during high-stress periods such as COVID-19 lockdowns.
In summary, the diversity of study types and designs across the included literature contributes to a well-rounded evidence base, capturing emerging themes from dietary behavior change and mental resilience to workplace stress, burnout, and occupational health in dental professionals.
Population and Sample Size
The included studies in this systematic review represent a wide spectrum of target populations, encompassing a variety of professional and demographic groups. A substantial number of these studies focus on healthcare professionals, namely physicians, nurses, and dentists, while others target health science students, industrial laborers, and employees within specific institutional settings. For example, assessed 271 undergraduate and postgraduate nursing and dentistry students in Greece, analyzing psychological dimensions such as stress, resilience, and hope in the aftermath of the COVID-19 pandemic, with an emphasis on academic responsibilities and mental well-being [18]. Similarly, conducted a cross-sectional study of 180 dentists across India, exploring the dynamics of work-life balance and psychological stress using Structural Equation Modeling during the lockdown period [55]. On a much broader scale, carried out a large-scale nationwide survey involving 9,196 in-service physicians across 31 regions in China, providing detailed insights into the dietary behaviors, sleep patterns, and health perceptions of medical professionals [35].
Some studies targeted more specific occupational populations. For instance, a study conducted a randomized controlled field trial involving 104 male petrochemical workers in Iran, evaluating the effects of a priority-oriented nutrition education program based on the Theory of Planned Behavior [46]. Moreover, sample sizes varied considerably depending on study design. Large samples, such as those in Chen et al. (2024)(N=9,196) and Gilbert et al. (2020)(N=1,994), enabled strong multivariate analyses and increased generalizability of the findings [35,47]. In contrast, qualitative studies relied on small, purposive samples (N=22) to explore in-depth narratives through thematic analysis, focusing on healthcare professionals' perceptions of their own dietary behaviors and nutritional self-efficacy [24]. Also, several studies demonstrated methodological strength by performing a priori power calculations. For example, determined their sample size using α = 0.05 and 90% power to detect changes in cholesterol levels, while confirmed that their sample met the statistical threshold based on power analysis [18,46]. These approaches enhanced the internal validity and reliability of their findings. However, some cross-sectional or narrative studies did not report power analyses or justify their sample sizes [55].
In conclusion, the diversity in population types and sample sizes illustrates both the breadth and complexity of the field. From multinational cohorts of physicians to narrowly defined student groups, the effectiveness and reliability of findings are deeply influenced by methodological transparency and statistical strength.
Data Collection Methods
The included studies employed diverse data collection methods, reflecting variations in study design, target populations, and research aims. Quantitative approaches predominated, with structured surveys, validated questionnaires, and biometric assessments frequently used to evaluate dietary habits, mental health, and physical outcomes [18]. For example, Chen et al. 2023 [35] administered a large-scale online survey to over 9,000 physicians in China, while studies like Shiri et al. 2023 [33] and Hassani et al. 2020 [55] utilized Structural Equation Modeling (SEM) to analyze work-life balance and mental health indicators. Furthermore, intervention studies, such as Vivarelli & Fenga [2024] [46], incorporated objective clinical measures (BMI, fasting blood sugar, homocysteine), reducing reliance on self-reported data. Longitudinal designs, as used by Tenelanda-Lopez et al. [56], enhanced causal inference through repeated measures of diet and mental well-being during the COVID-19 pandemic. Also, qualitative studies, such as Hobby et al. (2024) [24], employed semi-structured interviews and thematic analysis, providing strong insights into self-efficacy and contextual factors influencing dietary behaviors. Systematic and narrative reviews (e.g., Olesinska et al. (2025)[44], Schliemann & Woodside (2019)[21]) synthesized data from published literature using systematic search strategies and bias assessments, though without primary data collection. In general, a common limitation across many cross-sectional and observational studies was reliance on self-reported data, prone to recall and social desirability bias [14,18]. Online surveys, while efficient, may further compromise data accuracy [1,4,18]. Ethical approval was typically obtained for primary studies, while reviews relied on secondary, anonymized data. Overall, the dataset reflects a broad range of data collection strategies, both qualitative and quantitative, adapted to the clinical, behavioral, and psychosocial contexts of the research.
Statistical Methodology, Analyses and Recommendations
The statistical methodologies applied across the reviewed studies exhibit a wide range of sophistication, reflecting the design types, research aims, and data availability of each investigation. The choice of statistical tools and the transparency in their application are crucial for assessing the validity, reproducibility, and strength of the reported outcomes. So, quantitative studies predominantly relied on descriptive statistics, inferential tests, and multivariate analyses to assess associations, intervention effects, and predictor-outcome relationships. Basic statistical tools included t-tests, chi-square tests, ANOVA, and correlation coefficients. These were commonly used to compare groups, assess pre-post intervention differences, or identify patterns across categorical and continuous variables.
For example, Hassani et al (2020) applied paired t-tests and ANOVA to determine the impact of a nutrition education program on BMI, fasting blood sugar (FBS), and homocysteine levels, reporting statistically significant improvements across several biomarkers (p < 0.05) [55]. Moro et al. (2022) used Bonferroni-adjusted p-values and regression models to examine the relationships between work status, sleep, and psychosocial health outcomes among Brazilian dentists, thereby enhancing statistical precision [48]. Also, others employed advanced statistical modeling techniques, improving the depth of interpretation by conducting Structural Equation Modeling (SEM) to explore complex relationships between work-life balance, gender, and psychological stress during the COVID-19 lockdown, achieving an explained variance (R²) of 0.627 with statistically significant path coefficients (p < 0.05) [55]. Similarly, multivariate logistic regression analyses were used to explore how changes in physical activity and diet were linked to mental health outcomes such as anxiety, depression, and stress, controlling for demographic variables such as age, income, and occupation [56].
Systematic reviews incorporated meta-analytical techniques, including pooled prevalence estimation, forest plots, and heterogeneity assessment using the I² statistic [22,52]. This statistical transparency is essential for determining the strength of aggregated evidence and identifying potential sources of bias. Further, narrative reviews did not engage in formal statistical testing but synthesized findings from previously conducted studies [8,55]. While valuable for hypothesis generation and policy formulation, their lack of statistical appraisal and heterogeneity analysis limits the ability to draw firm conclusions.
Despite the diversity of methods, a recurring limitation across several studies was the absence of detailed statistical reporting. For example, some cross-sectional studies failed to mention effect sizes, confidence intervals, or specific test statistics. Others did not conduct power analyses or adjust for potential confounders, which could compromise internal validity [14].
Recommendations for future research emphasize the need for a stronger and standardized approach to statistical methodology in health-related workplace studies. First, researchers are encouraged to employ multivariate models consistently in order to control for key confounding variables such as age, gender, socioeconomic status, and lifestyle factors [48,56]. This practice enhances the validity of findings by isolating the true effects of the interventions under investigation. In addition, there should be consistent reporting of confidence intervals and effect sizes alongside p-values. Such metrics provide a clearer understanding of the magnitude and clinical relevance of observed effects, moving beyond mere statistical significance [52,55].
Overall, the reviewed studies applied a broad array of statistical methodologies, with varying degrees of strength and clarity. While many reported statistically significant outcomes, the degree of methodological transparency, confounding adjustment, and data robustness varied substantially. Strengthening these aspects in future research will enhance the credibility and applicability of findings in occupational and public health nutrition contexts.
Limitations Reported In the Reviewed Studies
The reviewed studies presented several limitations affecting the interpretation and generalizability of findings. A key issue was the reliance on self-reported data, which introduces risks of recall bias, social desirability bias, and misclassification, particularly for diet and lifestyle variables [35,55]. Many studies used cross-sectional designs, limiting the ability to infer causality, as associations observed lack temporal or baseline context [14,48]. Additionally, limited geographical scope and narrow participant demographics (e.g., gender-specific or profession-specific samples) further reduced external validity [46,48]. Further, small sample sizes were a common constraint, especially in qualitative studies or those with narrowly defined populations, limiting statistical power and representativeness [24,48]. Short follow-up durations further hindered the assessment of long-term intervention effects. High heterogeneity in intervention design, outcomes, duration, and participant characteristics also complicated data synthesis in systematic reviews, reducing meta-analytical strength [22,44]. Additional limitations included the absence of formal risk of bias assessments, exclusion of non-English studies (introducing potential language and publication bias), inadequate adjustment for confounders, low response rates, and gender imbalances. Some trials also lacked control for clustering effects and failed to include economic evaluations. These issues underline the need for greater methodological strength and more comprehensive reporting in future workplace health research on this theme [33].
Comparative and Cross-Cultural Analysis
A cross-cultural comparison of the selected studies reveals considerable variation in the design, scope, and effectiveness of workplace dietary interventions, shaped by the socio-economic and healthcare contexts of each country. For example, Olesinska et al. [44], in a systematic review of interventions across healthcare staff, highlighted the use of low-cost strategies such as Mediterranean diet promotion and telehealth, which showed positive effects but were limited by small sample sizes and high heterogeneity, common challenges in lower- to middle-income countries with constrained research infrastructure. In contrast, Tenelanda-Lopez et al. [56], in an observational study of nearly 2,000 U.S.-based university and medical center employees, demonstrated how resource-rich environments facilitate the use of repeated measures, multivariate analyses, and large, diverse samples, providing greater insights into the interaction of workplace health behaviors and mental well-being during the COVID-19 pandemic.
Similarly, Chen et al. [35], through a broad multi-center study across 31 Chinese provinces, identified culturally specific dietary habits (e.g., fast eating, irregular meals) as significant risk factors for suboptimal health among physicians, reporting on the importance of culturally tailored interventions. A related qualitative study from Australia by Hobby et al. [24] explored how healthcare professionals’ personal experiences, social norms, and cultural attitudes influence their self-efficacy in delivering nutrition care, reinforcing the need for cultural sensitivity in intervention design. Turkish studies also provided valuable insights: Yaman [14] and Pai et al. [54] documented stress-related changes in emotional eating and burnout among healthcare workers during the pandemic, showing how national healthcare system pressures and societal stressors mediate both psychological and nutritional outcomes. Finally, the review by Rachmah et al. [22] further illustrates how workplace interventions vary internationally, with outcomes influenced by differences in baseline population health, dietary norms, and intervention feasibility across settings. In addition, the Greek study by Mangoulia et al. [18] further illustrated how academic and gender roles influence psychosocial resilience and stress, even within relatively homogeneous student populations. In general, studies involving multiple countries highlighted challenges in synthesizing global evidence due to heterogeneity in intervention types, study designs, and outcome reporting [21,33]. While these systematic reviews reported modest improvements in dietary behavior and well-being, inconsistent reporting standards and cultural barriers limited the strength of conclusions.
Overall, while core strategies such as dietary education, stress reduction, and behavioral counseling appear broadly applicable, their effectiveness is shaped by cultural, economic, and institutional factors. This emphasizes the need for culturally adapted interventions and greater standardization in outcome reporting to enhance international collaboration and evidence synthesis.
Overall Implications
The collective evidence highlights the growing relevance of workplace dietary interventions as a multidimensional strategy to enhance employee well-being, particularly in high-stress healthcare professions such as dentistry and nursing [18,52]. Across diverse cultural and economic contexts, such interventions consistently improved dietary habits, mental health, and biometric outcomes, reinforcing their value as public health tools [44]. Importantly, the psychological and emotional dimensions of these interventions, particularly their impact on stress and emotional eating, emerged as critical factors for success, especially during the COVID-19 pandemic [14,18,24]. Studies from China [35], India [55], and Brazil [48] further underlined how national healthcare structures, workplace culture, and societal norms shape intervention outcomes, highlighting the need for culturally tailored approaches rather than universal models. However, recurring limitations, including reliance on self-reported data, heterogeneity in methods, and limited follow-up, indicate the need for stronger designs [21,47]. Longitudinal, mixed-methods research using standardized outcome measures would strengthen the evidence base and improve cross-study comparability. These findings have clear policy implications. As workplaces increasingly influence health outcomes, integrating nutrition and well-being strategies into organizational policies may contribute to reducing burnout, enhancing resilience, and improving workforce sustainability [33,55]. The positive associations between diet quality and job satisfaction [24,33] support the development of comprehensive, culturally adaptable, and scalable workplace health promotion initiatives. Future research as it is reported in the reviewed studies, should prioritize sustainability, economic evaluation, and cross-sector collaboration to maximize the impact of workplace dietary interventions on public and occupational health.
4. Discussion
This systematic review examined the complex connection between dietary habits, health behaviors, and well-being among healthcare professionals, with particular attention to dentists. The findings demonstrate that work-related factors, such as stress, long working hours, and occupational demands, substantially influence nutritional choices, physical activity levels, and mental health outcomes. Notably, interventions including nutrition education, antioxidant-rich diets, and structured meal planning were frequently linked to improvements in energy, mood, and reductions in burnout symptoms [1,15,57]. Programs that incorporated food literacy, behavioral coaching, and institutional support were among the most effective. However, a consistent barrier across studies was the absence of strong policy-level commitment to integrating these interventions within workplace health promotion frameworks [36,58]. This highlights the need for more comprehensive strategies aimed at cultivating supportive environments that prioritize the holistic well-being of healthcare professionals.
Nutrition Policy, Consumer Practices, and Sustainability in Dietary Choices
On a global scale, several dietary interventions aim to reduce sugar consumption. A notable example is the implementation of the Soft Drinks Industry Levy in the United Kingdom in 2018, which was a targeted fiscal measure to reduce the consumption of high-sugar soft drinks. The policy led to product reformulation and a measurable decline in sugar content and purchases of sugary beverages [59]. Based on these positive public health outcomes, experts have advocated extending such taxation to other high-sugar products, including confectionery and sweetened snacks, to further address obesity and diet-related diseases [60,61]
In parallel, the UK National Health Service (NHS) recommends limiting the intake of free sugars to no more than 30 grams per day, which corresponds to approximately 5% of an adult's daily energy intake [61]. Educational strategies that promote awareness, such as improved nutritional labeling, have also emerged as critical tools in public health nutrition. For instance, front-of-pack labeling (FOPL) systems have been implemented or supported by both governmental and non-governmental organizations across Europe [56]. For example, the Nutri-Score system introduced in France in 2017, following the UK’s traffic light labeling model, and the NutrInform Battery label launched by Italy in 2020, are two prominent examples of FOPL systems aiming to guide consumers toward healthier food choices [62,63]. Studies suggest that color-coded labels, such as Nutri-Score, effectively influence consumer behavior, increasing the likelihood of selecting products with higher nutritional quality [60,64]. Moreover, malnutrition, encompassing undernutrition, overnutrition, and micronutrient deficiencies, collectively referred to as the "triple burden of malnutrition", has profound implications for health, productivity, and overall quality of life [56]. The Food 2030 research and innovation pathway addresses the need for sustainable and culturally diverse healthy diets, highlighting the importance of nutrition across the life course [65].
In addition, the EAT–Lancet Commission advocates for profound global dietary shifts, including doubling the intake of fruits and vegetables and reducing the consumption of added sugars and red meat by at least 50% to support both planetary and human health [66]. The European Food Safety Authority (EFSA) has also raised concern about persistent micronutrient deficiencies, particularly of vitamin D and iodine, due to unhealthy dietary patterns and demographic changes such as population aging. Vulnerable groups include the elderly, individuals with chronic illnesses, low-income populations, and socially isolated individuals, for whom nutritional choices are often limited by accessibility and affordability [67]. These nutritional disparities ultimately affect mental health, well-being, and the ability to work [18].
Overall, the promotion of plant-rich, sustainable, and health-promoting diets must be accompanied by efforts to reduce the carbon footprint of food systems and operate within planetary boundaries [21]. Achieving this objective necessitates a fundamental rethinking and redesign of the entire food system, from production to consumption, through a systemic approach that engages all stakeholders, including producers, processors, distributors, marketers, policymakers, educators, and healthcare professionals [66]. This transformation requires not only structural changes but also a shift in societal attitudes and behaviors toward food [68]. Such diets should emphasize ingredients that are naturally high in dietary fibre, including whole grains, legumes, nuts, seeds, fruits, and vegetables, as well as alternative sources of protein derived from microorganisms, insects, and legumes [67,68].
Achieving these goals will require the alignment and integration of multiple policy frameworks. Key among these are the Common Agricultural Policy (European Commission, n.d.-a), the Common Fisheries Policy (European Commission, n.d.-b), the European Green Deal (European Commission, n.d.-c), the Farm-to-Fork Strategy (European Commission, n.d.-d), the EU White Paper on a Strategy for Europe on Nutrition, Overweight and Obesity-related Issues Europe’s Beating Cancer Plan and the EU Mission on Cancer (European Commission, n.d.-e) [69]. In parallel, synergies with health-related initiatives, such as the EU4 Health program (European Commission, n.d.-f) and the Health Promotion and Disease Prevention Knowledge Gateway, developed by the Joint Research Centre of the European Commission (European Commission, n.d.-g), will be essential to support a comprehensive and coherent approach to public health and sustainable food systems [70].
Health-Promoting and Sustainable Dietary Patterns
Among various dietary patterns, the Mediterranean diet is widely recognized for its health benefits and environmental sustainability. Characterized by a high intake of fruits, vegetables, whole grains, legumes, nuts, and olive oil, alongside moderate consumption of fish and dairy, it is considered a gold standard for nutritionally adequate and culturally acceptable diets [71]. The Mediterranean diet has been associated with reduced risk of cardiovascular disease, type 2 diabetes, certain cancers, and cognitive decline, while also demonstrating a lower environmental footprint compared to Western dietary patterns [72].
In addition to the Mediterranean diet, other regionally adapted, plant-rich dietary models, such as the Nordic diet, which emphasizes root vegetables, berries, whole grains, and rapeseed oil; the traditional Asian diet, which is high in rice, vegetables, soy, and fish; and more modern approaches such as flexitarian or vegetarian diets, have gained attention for their potential to support human and planetary health [73,74,75]. These dietary frameworks not only reduce the environmental burden through lower greenhouse gas emissions, reduced land use, and water conservation, but they also respect regional culinary traditions and cultural acceptability, which are critical for long-term adherence [76]. Incorporating these sustainable diets into national food-based dietary guidelines represents an actionable strategy to align public health promotion with climate goals, while also encouraging diversified food systems that support local economies and biodiversity [77].
Implications for Dentists' Health and Practice
Dentists play a key role in promoting oral and overall health, both in clinical practice and through patient education [78]. However, their own health is often compromised by demanding schedules, irregular work patterns, and poor dietary habits [18,25]. Studies show that inadequate nutrition among healthcare workers, including dentists, contributes to the risk of caries, periodontal disease, and systemic health issues [79,80,81]. Despite their responsibility to model healthy behaviors for patients, dentists frequently prioritize patient care over personal well-being, leading to poor eating patterns characterized by high-sugar, high-fat foods and irregular meals [82]. Such habits not only undermine their physical and oral health but can also impair professional performance and the ability to deliver effective care [1,5,83]. Adequate intake of essential nutrients is critical for immune function, tissue repair, and oral health maintenance [12,82,83,84]. Failure to meet these nutritional needs increases the risk of oral disease and may affect both personal well-being and professional capacity [56,85]. Additionally, high stress levels and irregular working hours further exacerbate poor dietary behaviors among dental professionals, highlighting the need for workplace strategies that support healthy nutrition and stress management in this population [1,4,12].
Psychological Impact of Poor Dietary Habits on Dentists
Studies show that dentists, like other healthcare professionals, often use unhealthy eating patterns, such as high sugar and fat intake or emotional eating, as coping mechanisms for occupational stress [14,24,35]. Such behaviors are linked to increased rates of depression, anxiety, and fatigue, contributing to professional burnout and diminished care quality [1,10,18]. In addition evidence supports the role of dietary interventions, including omega-3 fatty acids, vitamins, and antioxidant-rich foods, in reducing symptoms of depression and anxiety in high-stress healthcare environments [8,12,21]. Furthermore, the dietary behaviors of healthcare professionals have been shown to significantly influence both their mental well-being and their professional confidence in delivering nutritional counseling [86]. For dentists, improving dietary quality may provide dual benefits, enhancing personal mental health while also strengthening their ability to model and promote healthy behaviors to patients [24]. Workplace wellness programs that integrate nutrition education, stress management techniques, and better access to healthy foods can help mitigate psychological risks and improve occupational resilience [33]. Developing such targeted interventions is particularly important given the strong link between nutrition, mental well-being, and clinical performance in dental practice.
Shift Work and Its Impact on Dentists' Eating Habits
Irregular work hours and shift work are known to significantly influence the eating behaviors of healthcare professionals, including dentists [32]. Many dental practitioners, particularly those working in emergency services, extended clinical hours, or academic roles, face irregular schedules that disrupt normal meal patterns. This often results in increased consumption of high-fat snacks, sugary beverages, and calorie-dense convenience foods, which are readily available but nutritionally poor [15,32]. Further, night shift work and long clinical days have been associated with lower intake of fruits and vegetables, irregular meal timing, and higher consumption of processed foods [15,35]. Circadian rhythm disruption further compounds these risks by impairing digestion and altering metabolic processes [32,48]. Research has also highlighted the physiological impacts of shift work on stress levels, dietary habits, and biomarkers. Strong associations have been found between shift work, emotional eating, and adverse health behaviors among healthcare professionals, underscoring the need for targeted interventions to address these risks in shift-based work environments [14,35,47]. Given these findings, it is critical for healthcare institutions, and dental clinics in particular, to implement supportive workplace policies. Providing access to nutritious meals during all working hours, including late shifts, and promoting structured eating patterns could help mitigate the negative dietary impacts of irregular work schedules [10,24,32]. Targeted interventions of this kind may enhance both the physical and oral health of dentists, while also contributing to improved workplace well-being and performance.
Interventions to Improve Dietary Habits in Dentists
Improving the dietary habits of dentists requires targeted interventions that address both structural barriers and behavioral factors influencing nutrition within dental practice settings [23,87]. Facilitating access to nutrient-dense foods, such as fruits, vegetables, whole grains, and lean proteins, within clinics and institutional cafeterias can promote healthier dietary choices [15]. In addition, nutrition education programs tailored to the unique demands of dental professionals can enhance their understanding of the relationship between diet, physical health, mental well-being, and professional performance [23,24].
Comprehensive workplace interventions that combine personalized nutrition counseling, stress management strategies, and promotion of physical activity have been shown to improve dietary behaviors and reduce burnout among healthcare workers including dentists [10,18]. For dentists, creating supportive environments that encourage regular meal breaks, proper hydration, and flexible scheduling can foster sustainable improvements in nutrition and overall well-being [12,32]. For this reason, incorporating nutrition education into the ongoing professional development of dentists can promote healthier eating habits and improve both personal well-being and professional performance [27,88]. Providing training on the role of nutrition in energy balance, immune function, and mental resilience is particularly relevant for dental professionals, who frequently face high workloads, long hours, and stress [24,56]. Educational programs should include evidence-based content on dietary guidelines, the impact of macronutrients and micronutrients, and strategies to manage diet-related fatigue and stress, especially for dentists working irregular schedules or extended clinical shifts [79,80,81]. Beyond education, institutional incentives can further encourage dentists to adopt healthier dietary and lifestyle habits. Strategies may include offering discounts on nutritious meals, providing wellness bonuses or gym memberships, and fostering peer-support groups focused on healthy living [19]. Establishing a culture of health within dental clinics, supported by leadership, workplace policies, and peer engagement, can lead to sustained improvements in dietary behaviors, reduce burnout risk, and enhance job satisfaction and patient care quality [89]. Ultimately, promoting nutrition-focused interventions and education for dentists not only benefits their health and resilience but also enhances the quality and consistency of oral healthcare delivery [1,81].
Strengths and Limitations of the Study
This review synthesizes evidence across diverse healthcare settings and professional groups. It offers valuable insights into how dietary habits influence professional performance and oral health outcomes [26,56]. The inclusion of studies from multiple regions enhances the generalizability of the findings. However, several limitations should be noted. The heavy reliance on self-reported dietary data introduces potential recall and reporting bias [90]. Additionally, the cross-sectional design of many included studies precludes causal inferences [91]. Some studies had small sample sizes, limiting external validity [92], while the influence of socioeconomic status, institutional policies, and workplace environment on dietary behaviors was not consistently controlled [93]. Future research should prioritize longitudinal designs to better assess dietary changes over time and evaluate the effectiveness of workplace nutrition interventions.
Future Research Directions
While existing literature confirms the strong relationship between nutrition, mental well-being, and oral health in healthcare professionals [18,44,45], important gaps remain regarding the long-term impact of dietary habits on overall health and job performance [56]. Future research should prioritize longitudinal studies to clarify causal links between nutrition, burnout reduction, job satisfaction, and physical health outcomes [94]. Randomized controlled trials assessing specific interventions, such as increased intake of omega-3 fatty acids, fruits, and vegetables, are also needed to evaluate their effects on stress, physical health, and oral outcomes [95]. Additionally, the integration of nutrition education into dental and healthcare training programs warrants further investigation [88]. Future studies should also examine how organizational culture, workplace policies, and socioeconomic factors influence dietary habits in diverse healthcare settings including dental offices [26]. Understanding these variables will support the development of tailored interventions that address the specific needs of dental professionals across different clinical and workplace contexts. Ultimately, a deeper understanding of the complex relationship between diet, mental health, and oral health through well-designed longitudinal studies and targeted intervention trials will inform more effective nutrition-based strategies to enhance the well-being and professional performance of dentists.
Conclusions
The findings of this systematic review underscore the pivotal role of educational dietary interventions in supporting the health and professional performance of dentists in the post-COVID era. Evidence-based programs, particularly those integrating behavioral, nutritional, and psychological components, have demonstrated measurable improvements in dietary quality, BMI, stress levels, and burnout reduction among dental professionals. The effectiveness of these strategies is amplified when delivered through flexible digital tools and tailored to the unique occupational demands of dental settings. Going forward, interventions should adopt a multidisciplinary approach, ensure cultural relevance, and utilize continuous evaluation methods to maximize their impact and sustainability.
Author Contributions
Conceptualization, T.K. and M.A.; methodology, M.A.; software, M.A.; validation, T.K. and M.A.; formal analysis, T.K. and M.A.; investigation, T.K. and M.A.; resources, M.A.; data curation, T.K. and M.A.; writing—original draft preparation, T.K. and M.A.; writing—review and editing, T.K. and M.A.; visualization, M.A.; supervision, M.A.; project administration, M.A.; funding acquisition, T.K. and M.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Antoniadou, M. Estimation of Factors Affecting Burnout in Greek Dentists before and during the COVID-19 Pandemic. Dent. J. 2022, 10, 108. [CrossRef]
- Antoniadou, M.; Mangoulia, P.; Myrianthefs, P. Quality of Life and Wellbeing Parameters of Academic Dental and Nursing Personnel vs. Quality of Services. Healthcare 2023, 11, 2792. [CrossRef]
- Melnyk BM, Kelly SA, Stephens J, Dhakal K, McGovern C, Tucker S, et al. Interventions to improve mental health, well-being, physical health, and lifestyle behaviors in physicians and nurses: A systematic review. Am J Health Promot. 2020;34(8):929–41.
- Negucioiu, M.; Buduru, S.; Ghiz, S.; Kui, A.; Șoicu, S.; Buduru, R.; Sava, S. Prevalence and Management of Burnout Among Dental Professionals Before, During, and After the COVID-19 Pandemic: A Systematic Review. Healthcare 2024, 12, 2366. [CrossRef]
- Chakraborty T, Subbiah GK, Damade Y. Psychological distress during COVID-19 lockdown among dental students and practitioners in India: A cross-sectional survey. Eur J Dent. 2020;14(Suppl 1):S70–8.
- Antoniadou, M. Quality of Life and Satisfaction from Career and Work–Life Integration of Greek Dentists before and during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 9865. [CrossRef]
- Wirth MD, Meyer J, Jessup A, Dawson RM. Barriers and facilitators of diet, physical activity levels, and sleep among nursing undergraduates and early-career nurses: A qualitative descriptive study. Am J Health Promot. 2023;37(6):821–9.
- Kris-Etherton PM, Petersen KS, Hibbeln JR, Hurley D, Kolick V, Peoples S, et al. Nutrition and behavioral health disorders: Depression and anxiety. Nutr Rev. 2021;79(3):247–60.
- Canuto R, Garcez A, Spritzer PM, Olinto MTA. Associations of perceived stress and salivary cortisol with the snack and fast-food dietary pattern in women shift workers. Stress. 2021;24(6):763–71.
- Sert E, Kendirkiran G. Effects of emotional eating behaviour and burnout levels of nurses on job performance: A cross-sectional descriptive study. Am J Lifestyle Med. 2024.
- Antoniadou, M.; Manta, G.; Kanellopoulou, A.; Kalogerakou, T.; Satta, A.; Mangoulia, P. Managing Stress and Somatization Symptoms Among Students in Demanding Academic Healthcare Environments. Healthcare 2024, 12, 2522. [CrossRef]
- Kalogerakou T, Antoniadou M. The role of dietary antioxidants, food supplements and functional foods for energy enhancement in healthcare professionals. Antioxidants. 2024;13(12):1508.
- Mentzelou M, Papadopoulou SK, Jacovides C, Dakanalis A, Alexatou O, Vorvolakos T, et al. The COVID-19 pandemic increased the risk of eating disorders and emotional eating symptoms: A review of the current clinical evidence. COVID. 2024;4(11):1704–18.
- Yaman GB, Hocaoğlu Ç. Examination of eating and nutritional habits in health care workers during the COVID-19 pandemic. Nutrition. 2022;105:111839.
- Wolska A, Stasiewicz B, Kaźmierczak-Siedlecka K, Ziętek M, Solek-Pastuszka J, Drozd A, et al. Unhealthy food choices among healthcare shift workers: A cross-sectional study. Nutrients. 2022;14(20):4327.
- Ramachandran S, Shayanfar M, Brondani M. Stressors and mental health impacts of COVID-19 in dental students: A scoping review. J Dent Educ. 2022.
- Maragha T, Donnelly L, Schuetz C, von Bergmann H, Brondani M. Students' resilience and mental health in the dental curriculum. Eur J Dent Educ. 2023;27(1):174–80.
- Mangoulia P, Kanellopoulou A, Manta G, Chrysochoou G, Dimitriou E, Kalogerakou T, et al. Exploring the levels of stress, anxiety, depression, resilience, hope, and spiritual well-being among Greek dentistry and nursing students in response to academic responsibilities two years after the COVID-19 pandemic. Healthcare. 2025;13(1):54.
- Gómez-Polo C, Martín Casado AM, Montero J. Burnout syndrome in dentists: Work-related factors. J Dent. 2022;121:104143.
- Long H, Li Q, Zhong X, Yang L, Liu Y, Pu J, et al. The prevalence of professional burnout among dentists: A systematic review and meta-analysis. J Health Psychol. 2023;28(13):1767–82.
- Schliemann D, Woodside JV. The effectiveness of dietary workplace interventions: A systematic review of systematic reviews. Public Health Nutr. 2019;22(5):942–55.
- Rachmah Q, Martiana T, Mulyono M, Paskarini I, Dwiyanti E, Widajati N, et al. The effectiveness of nutrition and health intervention in workplace setting: A systematic review. J Public Health Res. 2021;11(1):2312.
- Crespo-Escobar P, Vázquez-Polo M, van der Hofstadt M, Nuñez C, Montoro-Huguet MA, Churruca I, et al. Knowledge gaps in gluten-free diet awareness among patients and healthcare professionals: A call for enhanced nutritional education. Nutrients. 2024;16(15):2512.
- Hobby J, Parkinson J, Ball L. Exploring health professionals' perceptions of how their own diet influences their self-efficacy in providing nutrition care. Psychol Health. 2024;39(2):252–67.
- Lieffers JR, Vanzan AGT, de Mello JR. Nutrition care practices of dietitians and oral health professionals for oral health conditions: A scoping review. Nutrients. 2021;13(10):3588.
- Tantimahanon A, Sipiyaruk K, Tantipoj C. Determinants of dietary behaviors among dental professionals: Insights across educational levels. BMC Oral Health. 2024;24:724.
- Riznik P, De Leo L, Dolinsek J, Gyimesi J, Klemenak M, Koletzko B, et al. The knowledge about celiac disease among healthcare professionals and patients in Central Europe. Pediatr Gastroenterol Hepatol Nutr. 2021;72(4):552–7.
- Akbar Z, Shi Z. Unfavorable Mealtime, Meal Skipping, and Shiftwork Are Associated with Circadian Syndrome in Adults Participating in NHANES 2005-2016. Nutrients. 2024 May 23;16(11):1581. [CrossRef]
- Tosoratto J, Tárraga López PJ, López-González ÁA, Vallejos D, Martínez-Almoyna Rifá E, Ramirez-Manent JI. Association of Shift Work, Sociodemographic Variables and Healthy Habits with Obesity Scales. Life (Basel). 2024 Nov 18;14(11):1503. [CrossRef]
- Sejbuk M, Siebieszuk A, Witkowska AM. The role of gut microbiome in sleep quality and health: Dietary strategies for microbiota support. Nutrients. 2024;16(14):2259.
- Mohd Azmi, N.A.S.; Juliana, N.; Mohd Fahmi Teng, N.I.; Azmani, S.; Das, S.; Effendy, N. Consequences of Circadian Disruption in Shift Workers on Chrononutrition and their Psychosocial Well-Being. Int. J. Environ. Res. Public Health 2020, 17, 2043. [CrossRef]
- Bouillon-Minois JB, Thivel D, Croizier C, Ajebo É, Cambier S, Boudet G, et al. The negative impact of night shifts on diet in emergency healthcare workers. Nutrients. 2022;14(4):829.
- Shiri R, Nikunlaakso R, Laitinen J. Effectiveness of workplace interventions to improve health and well-being of health and social service workers: A narrative review of randomised controlled trials. Healthcare. 2023;11(12):1792.
- Etz RS, Solid CA, Gonzalez MM, Reves SR, Britton E, Green LA, et al. Is primary care ready for a potential new public health emergency in the wake of the COVID-19 pandemic, now subsided? Fam Pract. 2024;41(5):732–9.
- Chen M, Xu X, Liu Y, Yao Y, Zhang P, Liu J, et al. Association of eating habits with health perception and diseases among Chinese physicians: A cross-sectional study. Front Nutr. 2023;10:1226672.
- Abouelezz NF, Ahmed WSE, Elhussieny DM, Ahmed GS, Zaky MSME. Dietary habits and perceived barriers of healthy eating among healthcare workers in a tertiary hospital in Egypt: A cross-sectional study. QJM. 2024;117(Suppl 2):hcae175.884.
- Panchbhaya A, Baldwin C, Gibson R. Improving the Dietary Intake of Health Care Workers through Workplace Dietary Interventions: A Systematic Review and Meta-Analysis. Adv Nutr. 2022 Mar;13(2):595-620. Epub 2023 Feb 10. [CrossRef] [PubMed] [PubMed Central]
- Mancin S., Reggiani F., Calatroni M., Morenghi E., Andreoli D., Mazzoleni B.Enhancing clinical nutrition education for healthcare professionals: Engagement through active learning methodologies. Clinical Nutrition Open Science, 2023, 52, 49-57. [CrossRef]
- Breanna Lepre, Helena Trigueiro, Jørgen Torgerstuen Johnsen, Ali Ahsan Khalid, Lauren Ball, Sumantra Ray - Global architecture for the nutrition training of health professionals: a scoping review and blueprint for next steps: BMJ Nutrition, Prevention & Health 2022;5. [CrossRef]
- Prajapati AS, Kulkarni PR, Shah HG, Shah DB, Sodani V, Doshi P. Attitude, practices and experience of dental professionals during COVID-19 pandemic: A cross-sectional survey from Gujarat, India. Adv Hum Biol. 2021;11(3):266–72. [CrossRef]
- Dhillon CN, Ortenzi F. Potential for Impact of Workforce Nutrition Programmes on Nutrition, Health and Business Outcomes: a Review of the Global Evidence and Future Research Agenda. Int J Environ Res Public Health. 2023;20(9):5733. [CrossRef]
- Aggarwal M, Ospina NS, Kazory A, Joseph I, Zaidi Z, Ataya A, et al. The mismatch of nutrition and lifestyle beliefs and actions among physicians: A wake-up call. Am J Lifestyle Med. 2020;14(3):304–15.
- Valizadeh A, Moassefi M, Nakhostin-Ansari A, Hosseini Asl SH, Saghab Torbati M, Aghajani R, Maleki Ghorbani Z, Faghani S. Abstract screening using the automated tool Rayyan: results of effectiveness in three diagnostic test accuracy systematic reviews. BMC Med Res Methodol. 2022 Jun 2;22(1):160. [CrossRef] [PubMed] [PubMed Central]
- Olesińska, W.; Biernatek, M.; Lachowicz-Wiśniewska, S.; Piątek, J. Systematic Review of the Impact of COVID-19 on Healthcare Systems and Society—The Role of Diagnostics and Nutrition in Pandemic Response. J. Clin. Med. 2025, 14, 2482. [CrossRef]
- Di Prinzio RR, Dosi A, Arnesano G, Vacca ME, Melcore G, Maimone M, Vinci MR, Camisa V, Santoro A, De Falco F, De Maio F, Dalmasso G, Di Brino E, Pieri V and Zana S (2025) Eectiveness of a Food Education Program for healthcare workers: a pilot study in a Total Worker Health© approach. Front. Public Health 13:1523131.
- Vivarelli S, Fenga C. Workplace health promotion program: An integrated intervention to promote well-being among healthcare workers. Public Health Toxicol. 2024;4(3):12.
- Gilbert A, Eyler A, Cesarone G, Harris J, Hayibor L, Evanoff B. Exploring university and healthcare workers' physical activity, diet, and well-being during the COVID-19 pandemic. SAGE Open Med. 2023;11:21650799221147814.
- Moro JS, Soares JP, Massignan C, Oliveira LB, Ribeiro DM, Cardoso M, et al. Burnout syndrome among dentists: A systematic review and meta-analysis. J Evid Based Dent Pract. 2022;22(2):101724.
- Panchbhaya A, Baldwin C, Gibson R. Improving the Dietary Intake of Health Care Workers through Workplace Dietary Interventions: A Systematic Review and Meta-Analysis. Adv Nutr. 2022 Mar;13(2):595-620. Epub 2023 Feb 10. [CrossRef]
- Søvold LE, Naslund JA, Kousoulis AA, Saxena S, Qoronfleh MW, Grobler C, et al. Prioritizing the mental health and well-being of healthcare workers: An urgent global public health priority. Front Public Health. 2021;9:679397.
- Mehrotra A, Mehrotra A, Babu AK, Ji P, Mapare SA, Pawar RO. Oral health knowledge, attitude, and practices among healthcare professionals: A questionnaire-based survey. J Pharm Bioall Sci. 2021;13(Suppl 2):S1452–7.
- Özarslan M, Caliskan S. Attitudes and predictive factors of psychological distress and occupational burnout among dentists during COVID-19 pandemic in Turkey. Curr Psychol. 2021;40(7):3113-3124. Epub 2021 Apr 29. [CrossRef]
- Peixoto KO, de Resende CMBM, de Almeida EO, Almeida-Leite CM, Conti PCR, Barbosa GAS, et al. Association of sleep quality and psychological aspects with reports of bruxism and TMD in Brazilian dentists during the COVID-19 pandemic. J Appl Oral Sci. 2021;29:e20201089.
- Pai S, Patil V, Kamath R, Mahendra M, Singhal DK, Bhat V. Work-life balance amongst dental professionals during the COVID-19 pandemic—A structural equation modelling approach. PLoS One. 2021;16(8):e0256663.
- Hassani B, Amani R, Haghighizadeh MH, Araban M. A priority oriented nutrition education program to improve nutritional and cardiometabolic status in the workplace: A randomized field trial. J Occup Med Toxicol. 2020;15(1).
- Tenelanda-López D, Valdivia-Moral P, Castro-Sánchez M. Eating Habits and Their Relationship to Oral Health. Nutrients. 2020 Aug 27;12(9):2619. [CrossRef]
- Potthoff S, Rasul O, Sniehotta FF, Marques M, Beyer F, Thomson R. The relationship between habit and healthcare professional behaviour in clinical practice: A systematic review and meta-analysis. Health Psychol Rev. 2019;13(1):73–90.
- Rosmiati R, Haryana NR, Firmansyah H, Fransiari ME. Workplace nutrition interventions: A systematic review of their effectiveness. Media Publikasi Promosi Kesehatan Indonesia. 2025;8(3):151–66.
- Kuswari M, Rimbawan R, Hardinsyah H, Dewi M, Gifari N. Effect of tele-exercise versus combination of tele-exercise with tele-counselling on obese office employee’s weight loss. Arsip Gizi Pangan. 2021;6(2):131–9.
- Raudenská J, Steinerová V, Javůrková A, Urits I, Kaye AD, Viswanath O, et al. Occupational burnout syndrome and post-traumatic stress among healthcare professionals during the novel coronavirus disease 2019 (COVID-19) pandemic. Best Pract Res Clin Anaesthesiol. 2020;34(3):553–60.
- Hashem K, et al. Outcomes of sugar reduction policies, United Kingdom of Great Britain and Northern Ireland. Bull World Health Organ. 2024;102(6):432–9.
- Topaloglu S. Navigating Nutrition Labeling Choices: Latest News on Nutri-Score and Alternative Systems in Europe. Accessed on 15 June 2025 from https://www.foodchainid.com/resources/navigating-nutrition-labeling-choices-latest-news-on-nutri-score-and-alternative-systems-in-europe/.
- Skretkowicz, Yvette and Perret, Jens Kai, Nutri-Score – A Review of the Literature (February 19, 2024). Available at SSRN: https://ssrn.com/abstract=4731637 or or http://dx.doi.org/10.2139/ssrn.4731637. [CrossRef]
- Song J, Brown MK, Tan M, MacGregor GA, Webster J, Campbell NRC, Trieu K, Ni Mhurchu C, Cobb LK, He FJ. Impact of color-coded and warning nutrition labelling schemes: A systematic review and network meta-analysis. PLoS Med. 2021 Oct 5;18(10):e1003765. [CrossRef]
- Song J, Brown MK, Tan M, et al. Impact of color-coded and warning nutrition labelling schemes: A systematic review and network meta-analysis. PLoS Med. 2021;18:e1003765.
- European Commission. Food 2030 Research and Innovation – Pathways for action 2.0. Brussels: European Commission; 2023.
- Moore Heslin A, McNulty B. Adolescent nutrition and health: characteristics, risk factors and opportunities of an overlooked life stage. Proceedings of the Nutrition Society. 2023;82(2):142-156. [CrossRef]
- EAT–Lancet Commission. Healthy diets from sustainable food systems – Food planet health. Summary report. 2019.
- EU. Questions and Answers on the EU budget: the Common Agricultural Policy and Common Fisheries Policy. Accessed on 15 June 2025 from https://ec.europa.eu/commission/presscorner/detail/en/qanda_20_985.
- EU. EU4Health programme 2021-2027 – a vision for a healthier European Union. Accessed on 15 June 2025 from https://health.ec.europa.eu/funding/eu4health-programme-2021-2027-vision-healthier-european-union_en.
- Guasch-Ferré M., W. C. Willett WC. The Mediterranean diet and health: a comprehensive overview. J internal med. 2021, 290, 549-566. [CrossRef]
- Zupo R, Castellana F, Piscitelli P, Crupi P, Desantis A, Greco E, Severino FP, Pulimeno M, Guazzini A, Kyriakides TC, Vasiliou V, Trichopoulou A, Soldati L, La Vecchia C, De Gaetano G, Donati MB, Colao A, Miani A, Corbo F, Clodoveo ML. Scientific evidence supporting the newly developed one-health labeling tool "Med-Index": an umbrella systematic review on health benefits of mediterranean diet principles and adherence in a planeterranean perspective. J Transl Med. 2023 Oct 26;21(1):755. [CrossRef]
- Krznarić Ž, Karas I, Ljubas Kelečić D, Vranešić Bender D. The Mediterranean and Nordic Diet: A Review of Differences and Similarities of Two Sustainable, Health-Promoting Dietary Patterns. Front Nutr. 2021 Jun 25;8:683678. [CrossRef]
- Christodoulou, C.C.; Pitsillides, M.; Hadjisavvas, A.; Zamba-Papanicolaou, E. Dietary Intake, Mediterranean and Nordic Diet Adherence in Alzheimer’s Disease and Dementia: A Systematic Review. Nutrients 2025, 17, 336. [CrossRef]
- Woodside J, Young IS, McKinley MC. Culturally adapting the Mediterranean Diet pattern - a way of promoting more 'sustainable' dietary change? Br J Nutr. 2022 Aug 28;128(4):693-703. Epub 2022 Jun 23. [CrossRef]
- Ridoutt BG, Hendrie GA, Noakes M. Dietary Strategies to Reduce Environmental Impact: A Critical Review of the Evidence Base. Adv Nutr. 2017 Nov 15;8(6):933-946. [CrossRef]
- van Dooren C, Loken B, Lang T, Meltzer HM, Halevy S, Neven L, Rubens K, Seves-Santman M, Trolle E. The planet on our plates: approaches to incorporate environmental sustainability within food-based dietary guidelines. Front Nutr. 2024 Jul 5;11:1223814. [CrossRef]
- Mills A, Berlin-Broner Y, Levin L. Improving Patient Well-Being as a Broader Perspective in Dentistry. Int Dent J. 2023 Dec;73(6):785-792. Epub 2023 Jun 19. [CrossRef]
- Natarajan, P., Madanian, S. & Marshall, S. Investigating the link between oral health conditions and systemic diseases: A cross-sectional analysis. Sci Rep 15, 10476 (2025). [CrossRef]
- Dimopoulou, M.; Antoniadou, M.; Amargianitakis, M.; Gortzi, O.; Androutsos, O.; Varzakas, T. Nutritional Factors Associated with Dental Caries across the Lifespan: A Review. Appl. Sci. 2023, 13, 13254. [CrossRef]
- Varzakas T, Antoniadou M. A Holistic Approach for Ethics and Sustainability in the Food Chain: The Gateway to Oral and Systemic Health. Foods. 2024 Apr 17;13(8):1224. [CrossRef]
- Tantimahanon, A., Sipiyaruk, K. & Tantipoj, C. Determinants of dietary behaviors among dental professionals: insights across educational levels. BMC Oral Health 24, 724 (2024). [CrossRef]
- Barranca-Enríquez A, Romo-González T. Your health is in your mouth: A comprehensive view to promote general wellness. Front Oral Health. 2022 Sep 14;3:971223. [CrossRef]
- Tohary IA, Jan AS, Alotaibi MA, Alosaimi TB, Alotaibi AEA, Alshayb AA, et al. The impact of diet and nutrition on oral health: A systematic review. Migr Lett. 2022;19(S5):338–46.
- Antoniadou M, Varzakas T. Breaking the vicious circle of diet, malnutrition and oral health for the independent elderly. Crit Rev Food Sci Nutr. 2021;61(19):3233-3255. Epub 2020 Jul 20. [CrossRef]
- Dekker J, Sears SF, Åsenlöf P, Berry K. Psychologically informed health care. Transl Behav Med. 2023 May 13;13(5):289-296. [CrossRef]
- Antoniadou, M.; Varzakas, T. Diet and Oral Health Coaching Methods and Models for the Independent Elderly. Appl. Sci. 2020, 10, 4021. [CrossRef]
- Kataoka M, Adam LA, Ball LE, Crowley J, McLean RM. Nutrition Education and Practice in University Dental and Oral Health Programmes and Curricula: A Scoping Review. Eur J Dent Educ. 2025 Feb;29(1):64-83. Epub 2024 Oct 29. [CrossRef]
- Rentas González L. Wellness Programs: Strategies for Increasing Employees’ Wellness Programs: Strategies for Increasing Employees’ Productivity and Reducing Health Care Costs. Walden University, 2022. Accessed on 15 June 2025 from chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://scholarworks.waldenu.edu/cgi/viewcontent.cgi?article=15723&context=dissertations.
- Ottaviani JI, Sagi-Kiss V, Schroeter H, Kuhnle GGC. Reliance on self-reports and estimated food composition data in nutrition research introduces significant bias that can only be addressed with biomarkers. Elife. 2024 Jun 19;13:RP92941. [CrossRef]
- Savitz DA, Wellenius GA. Can Cross-Sectional Studies Contribute to Causal Inference? It Depends. Am J Epidemiol. 2023 Apr 6;192(4):514-516. [CrossRef]
- Faber J, Fonseca LM. How sample size influences research outcomes. Dental Press J Orthod. 2014 Jul-Aug;19(4):27-9. [CrossRef]
- Thomas TW, Cankurt M. Influence of Food Environments on Dietary Habits: Insights from a Quasi-Experimental Research. Foods. 2024 Jun 26;13(13):2013. [CrossRef]
- Edú-Valsania S, Laguía A, Moriano JA. Burnout: A Review of Theory and Measurement. Int J Environ Res Public Health. 2022 Feb 4;19(3):1780. [CrossRef]
- Dempsey M, Rockwell MS, Wentz LM. The influence of dietary and supplemental omega-3 fatty acids on the omega-3 index: A scoping review. Front Nutr. 2023 Jan 19;10:1072653. [CrossRef]
Figure 1.
Flowchart for the results of the search strategies.
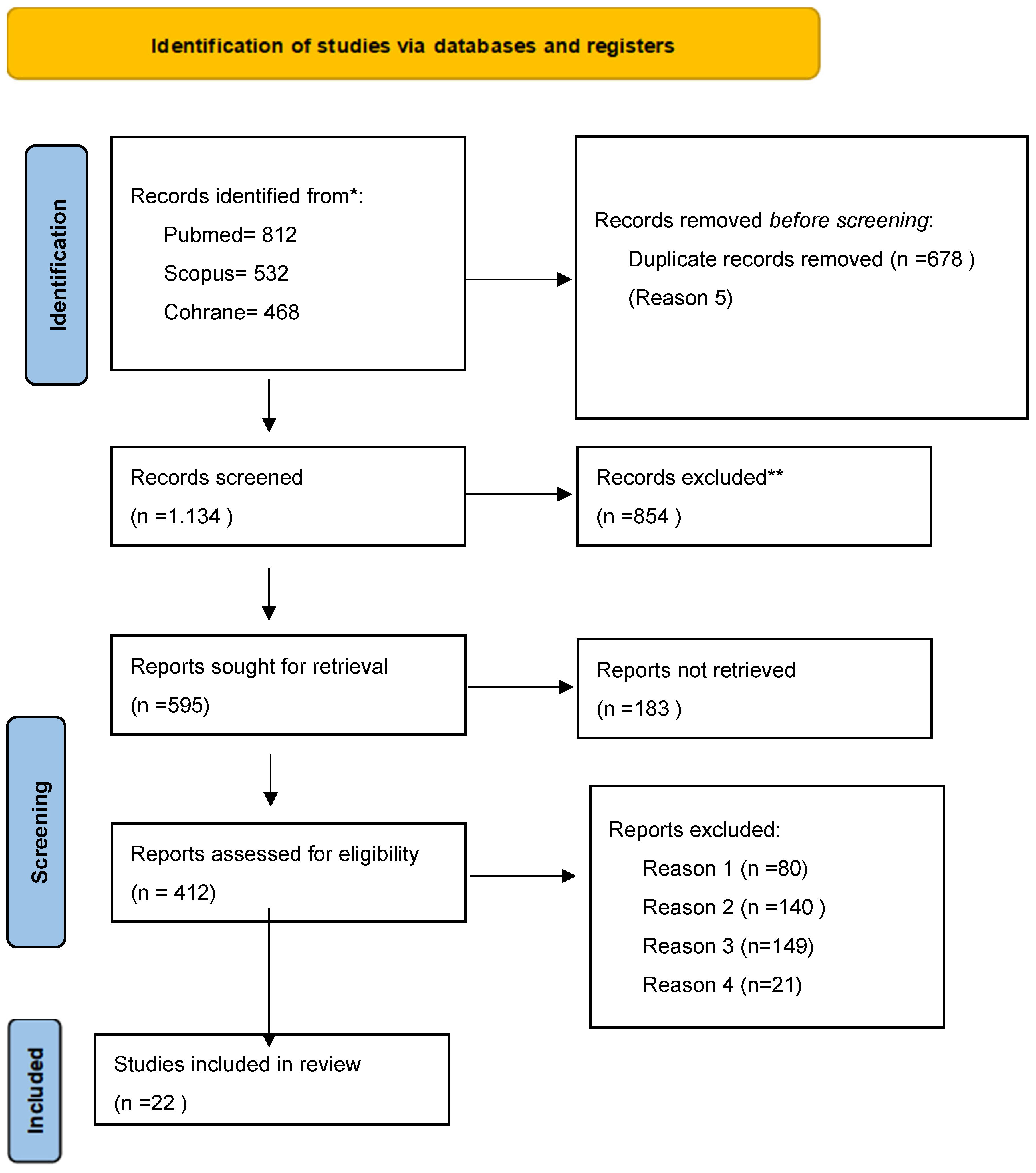
Figure 2.
Distribution of studies included in the systematic review by year of publication.
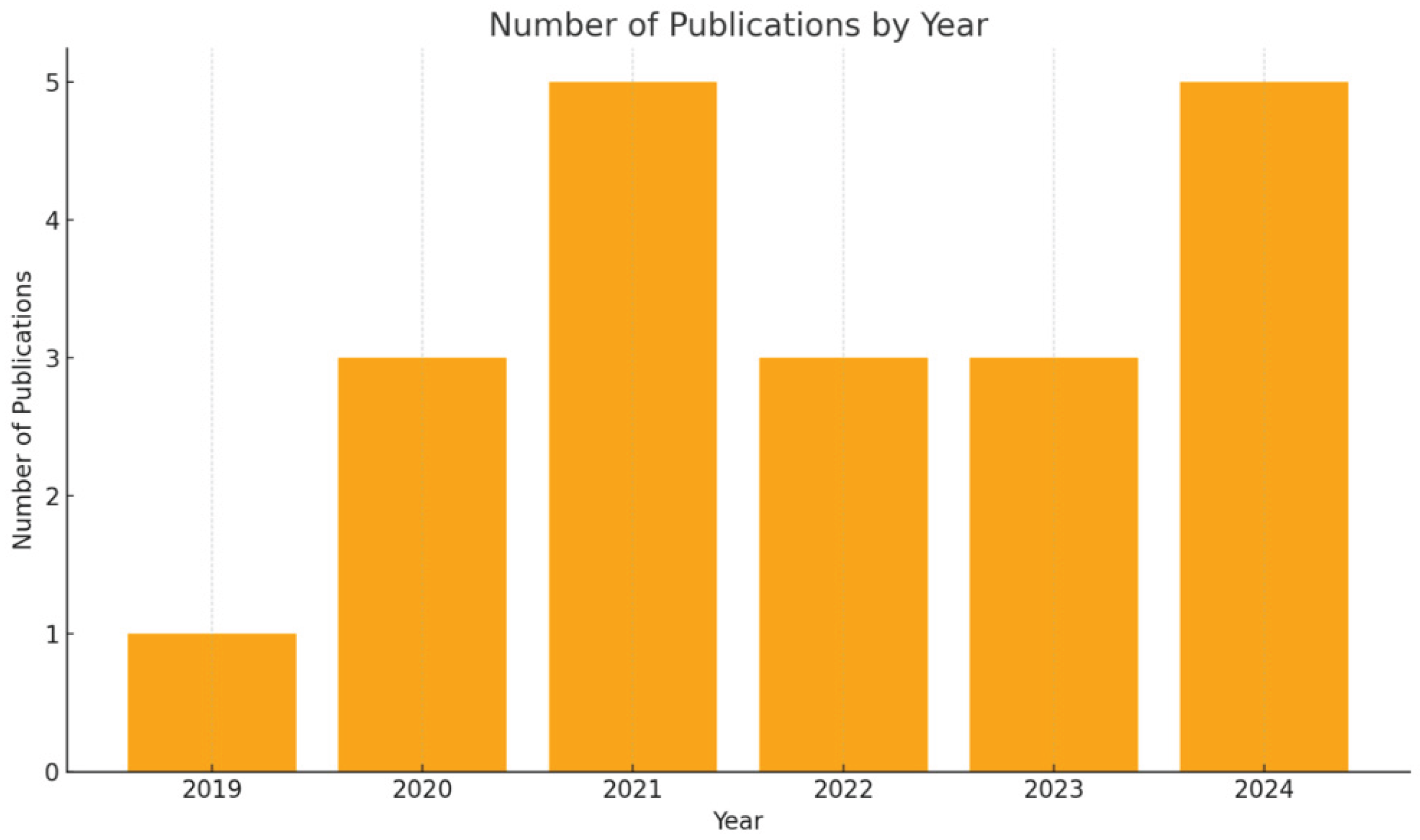

Table 1.
Studies included in this systematic review.
| Authors | Type of study- | Population | Exposure | Comparators | Statistical significance | Limitations | confounders | Outcomes |
|---|---|---|---|---|---|---|---|---|
| 1. Olesinska et al 2025 [44] | Systematic review – Multi-study analysis | healthcare staff from 10 studies | Workplace nutrition interventions (Mediterranean diet, telehealth, education, counseling) | No intervention, usual routine, or standard programs in original studies | Significant improvements in weight, LDL cholesterol, food literacy, and dietary adherence in most studies | Small sample sizes in some studies, high heterogeneity, limited long-term data, few studies with blinding | Variability in design, participant demographics, and adherence levels | Improvements in BMI, diet quality, cardiometabolic markers, food literacy, and quality of life |
| 2. Mangoulia et al 2025 [18] | Cross-sectional – Single-center (National and Kapodistrian University of Athens) | 271 undergraduate and postgraduate dentistry and nursing students in Greece | Psychological well-being: stress, anxiety, depression, resilience, hope, spiritual well-being | Comparisons between nursing and dentistry students, as well as subgroups based on gender, education level, income | Yes – significant differences found across departments and demographic factors; hierarchical regression showed hope as predictor of resilience | Limited generalizability (single institution); predominance of females; different academic levels per department; low response rate; cross-sectional design | Gender, income, educational level, department | High prevalence of stress, anxiety, depression; dentistry students showed higher stress/anxiety; hope strongly predicted resilience; need for targeted interventions identified |
| 3. Di Prinzio et al. 2025 [45] |
Pilot intervention study (pre-post design) | Healthcare workers in an Italian hospital | Food education program based on Total Worker Health© approach | Baseline (pre-intervention) vs. post-intervention comparisons | Yes, significant improvements in dietary behaviors and knowledge (p < 0.05) | Small sample size (pilot), short follow-up, single-center, lack of control group | Gender, age, baseline health status, occupation | Improved dietary knowledge, increased fruit/vegetable intake, reduced intake of sugary snacks and processed foods, positive changes in self-reported eating habits |
| 4.Vivarelli & Fenga 2024 [46] |
Systematic review (multi-country) | 37 studies on dentists | Prevalence of burnout in dentists via MBI subscales | Not applicable (meta-analysis of observational studies) | Pooled prevalence estimates with 95% CI and heterogeneity (I²); Stata 13.0 used | High heterogeneity (I²>90%), variable study quality, no study met all Joanna Briggs criteria | Study design, population differences | Burnout affected 13% of dentists overall, with high emotional exhaustion in 25%, high depersonalization in 18%, and low personal accomplishment in 32%, making emotional exhaustion the most common dimension. |
| 5.Hobby et al 2024 [24] |
Cross-sectional – Single-center (Australia, qualitative study via interviews) | 22 health professionals (including dietitians) with patient contact | Personal dietary behaviors and self-efficacy in providing nutrition care | No direct comparators; thematic contrasts drawn across narratives | Not applicable (qualitative study); thematic saturation reached | Small sample size; self-selection bias; only Australian participants; qualitative limits to generalizability | Life experiences, social interactions, role modeling | Personal diet and lived experiences influence confidence in providing nutrition care; social support and environment impact self-efficacy |
| 6. Gilbert et al 2023 [47] |
Prospective observational – Single-center (University Hospital ‘G. Martino’, Messina, Italy) | Healthcare workers (20–65 years), with or without night shift work | Night shift work (NSW), occupational stress, sleep quality, diet, physiological biomarkers | HCWs without night shifts | Yes – significant associations (e.g., stress, sleep, diet, biomarkers; p<0.05) | Self-report bias, confounding variables (lifestyle), resource-intensive protocol, only one center | Age, sex, smoking, comorbidities, work conditions | Improved well-being, dietary habits, stress, and sleep patterns; physiological biomarkers monitored; 12-month follow-up planned |
| 7.Shiri et al 2023 [33] | Narrative Review of 108 RCTs – Multi-country | Health and social service workers (various roles and countries) | Workplace interventions (mindfulness, ergonomics, coaching, exercise, nutrition, scheduling, resilience) | No intervention or alternative workplace programs | Yes – modest but statistically significant effects across multiple RCTs | Review limited to PubMed; no quality appraisal of studies; short follow-up; clustering effects not always accounted for; small samples in some RCTs | Various (e.g., age, gender, occupation, baseline stress levels) | Modest improvements in burnout, job satisfaction, work ability, well-being; limited effect on occupational injuries; barriers to participation include workload, lack of support, off-hours scheduling |
| 8.Chen et al 2023 [35] | Cross-sectional – Multi-center (Mainland China, 31 regions) | In-service physicians working in Chinese hospitals (N=9,196) | Unhealthy eating habits (e.g., eating too fast, irregular meals, frequent out-of-home meals) | Comparisons made across groups with and without specific eating habits | Significant associations between unhealthy eating habits and suboptimal health/disease (p<0.05) | Self-report bias, gender imbalance (83.3% women), online survey format, possible information bias | Age, sex, working time, sleep quality, exercise, sedentary time, smoking, alcohol consumption | Unhealthy eating habits significantly associated with subhealth and metabolic/micronutrient-related diseases |
| 9.Mancin et al. 2023 [38] |
Educational intervention study (pre-post design, single center) | Healthcare professionals (physicians, nurses, dietitians) in Italy | Active learning–based clinical nutrition education program (interactive workshops, case-based learning) | Baseline (pre-intervention) vs. post-intervention comparisons | Yes — significant improvement in nutrition knowledge scores and self-reported confidence (p < 0.001) | Small sample size, single center, no long-term follow-up, no control group | Baseline knowledge, profession (nurse/doctor/dietitian), prior training | Improved nutrition knowledge, higher confidence in delivering nutrition advice, greater engagement in nutrition-related clinical practice |
| 10. Moro et al 2022 [48] |
Single-center, randomized controlled field trial | 104 male petrochemical workers | Priority-oriented nutrition education program based on Theory of Planned Behavior | Control group received no intervention | Significant improvements in knowledge, FBS, Hcy (all p<0.001), and BMI (p<0.05). | Short intervention duration (3 months), only male participants, possible recall bias via FFQ, no family evaluation | Smoking, alcohol use, medication use excluded; groups balanced on demographics | Improved nutritional knowledge, dietary behavior, BMI, FBS, and homocysteine levels in the intervention group compared to control group; no significant change in hs-CRP |
| 11.Yaman 2022 [14] | Single-center (online nationwide sample via snowball technique) | 405 healthcare workers in Turkey (aged 19–67) | Perceived stress, emotional eating, and changes in nutritional habits during COVID-19 | Participants with vs. without changes in eating habits | Statistical significance found (e.g., P < 0.001 for stress and dietary changes) | Self-report bias, cross-sectional design, no causality, online sampling bias | Psychiatric history, COVID experience, socioeconomic concerns | 58% changed eating habits, 51% gained weight, significant associations with stress and emotional eating |
| 12. Panchbhaya et al, 2022 [49] | Systematic Review & Meta-analysis | Healthcare workers (various professions) from 26 studies | Workplace dietary interventions (education, environment, behavior change) | No intervention or usual care | Yes, significant improvements in fruit & vegetable intake (+0.49 servings/day), small but significant reduction in energy intake and body weight | Heterogeneity in intervention types, duration, and outcomes; publication bias possible; limited long-term follow-up in primary studies | Variability in study design, population characteristics, workplace settings | Increased fruit/vegetable intake, reduced energy intake and body weight, improved overall diet quality |
| 13.Rachmah et al 2021 [22] | Systematic review of 11 intervention studies from multiple countries | Workers aged 19–64 in various settings (industrial, manufacturing, garment, etc, healthcare sector.) | Nutrition and health interventions: education, behavioral change, physical activity, meal/supplement interventions, or combinations | Mostly RCTs or controlled trials; 2 studies without control groups | Most studies reported significant improvements in BMI, blood markers, self-efficacy, knowledge, diet, and behaviors (e.g., more fruit/veg, less alcohol/fat). | Heterogeneity in methods and duration, 2 studies lacked control groups, no risk of bias assessment, English-only studies included | Population/worksite heterogeneity; differences in baseline characteristics and implementation | Improved BMI, biochemical indices (e.g., cholesterol, fasting blood sugar), nutrition knowledge, physical activity, reduced risky behavior, increased fruit/vegetable intake |
| 14.Sovold et al 2021 [50] | Systematic Review – Multi-source, not center-based | General population; focus on public health, diagnostic, and nutrition data | Diagnostic, nutritional deficiencies (Vitamin D, C, E, zinc, selenium), psychosocial impact | Not applicable (multiple studies compared) | Significance varies per included study (some RCTs, some observational); mixed results | Heterogeneity in study designs, inconsistent RCT outcomes, lack of long-term data, many observational designs, regional bias (many Polish studies) | Potential variability across populations and designs included in review | Combined assessment of diagnostics, immune-nutritional status, mental health effects, and pandemic preparedness strategies. |
| 15. Mehrotra et al 2021 [51] | Single-center (Riobamba, Ecuador) | 380 students in healthcare | Eating habits (fruits, vegetables, dairy, snacks, etc.) | Frequency of consumption | Significant association between DMFT and fruit (p=0.049), vegetables (p=0.028) | Single age group, geographic limitation, outdated national data | None adjusted statistically (e.g., brushing habits, socio-economic status) | DMFT index; associations with eating habits |
| 16. Kris-Etherton et al 2021 [8] | Narrative Review – Multi-study based | Global population, all ages | Dietary patterns, specific nutrients (e.g., omega-3s, B-vitamins, zinc, magnesium) | No direct comparator; studies compared various diets/nutrients with behavioral health outcomes | Statistically significant in many included studies; RCTs show benefit of Mediterranean diet | Narrative nature, no meta-analysis; possible residual confounding and reverse causation | Nutritional status, comorbidities, lifestyle factors, socioeconomic status | Improved mood, reduced depression and anxiety with healthy diets; recommendation for dietary guidelines inclusion |
| 17. Özarslan & Caliskan 2021 [52] | Single center | 473 HCWs (doctors, nurses, pharmacists, technicians, interns) | Oral health knowledge, attitude, and practices (questionnaire-based survey) | Differences among HCW groups, gender, education level | Yes (p < 0.05 in multiple comparisons) | Cross-sectional design, limited sample size, self-reporting bias | Gender, profession, education level | Knowledge scores, attitudes (e.g., dental visit frequency), hygiene practices |
| 18. Peixoto et al 2021 [53] | Multicenter, Cross-sectional | 706 dentists in Turkey (FP & FN) | Working in filiation service vs not during COVID-19 | Dentists not involved in filiation (FN group) | Yes (p<0.05 for many variables) | Internet-based survey, self-reported data, single timepoint, possible selection bias | Confounders: age, gender, academic degree; Outcomes: MBI scores, stress, burnout | Habits etc |
| 19. Pai et al 2021 [54] | Single-center, cross-sectional | 641 Brazilian dentists (G1: quarantine, G2: outpatient care, G3: frontline) | COVID-19 pandemic-related psychosocial factors, sleep quality, TMD and bruxism symptoms | Groups based on work status during the pandemic (quarantine, outpatient, frontline) | Yes (p<0.016 for Bonferroni adjusted; p<0.001 for regressions) | Small sample of frontline dentists, self-reported data, cross-sectional design | Working status, pandemic concerns, psychological symptoms | Significant correlation between sleep and depression, stress, anxiety; poor sleep is associated with TMD and bruxism |
| 20. Hassani et al 2020 [55] | Single-center, cross-sectional | 180 dentists across India | COVID-19 lockdown's effect on work-life balance | Gender, relationship status, workplace factors | SEM showed significant associations (e.g., R² = 0.627; p-values < 0.05) | Self-report bias, low response rate (37.5%), limited geographical representation | Non-inclusion of dentists from all states; self-reporting; limited stress scale use | Work-life balance affected by mental/physical health, relationships, workplace; more imbalance in females |
| 21. Tenelanda-Lopez et al 2020 [56] |
Observational – Single-center (Washington University) | 1,994 employees (university & medical center), with ≥2 responses across 3 survey waves | Self-reported physical activity, diet, and mental well-being during COVID-19 | Clinical vs. nonclinical roles; working from home vs. onsite | Yes – maintained/increased PA and diet significantly linked to better well-being outcomes (p<0.05); multivariate regressions used | Self-reported data; limited generalizability; no baseline pre-pandemic data; recall and perception bias | Age, race, gender, income, ethnicity, clinical role | Participants maintaining or improving health behaviors had lower odds of moderate/severe depression, anxiety, and stress; onsite clinical workers reported worse well-being |
| 22. Schliemann & Woodside 2019 [21] | Systematic review of systematic reviews (multi-study, international) | Adult employees across healthcare sectors; general and “at risk” populations in workplace settings | Dietary workplace interventions (education, environmental changes, multicomponent programs) | Usual care, no intervention, or non-diet-focused interventions | Small but positive effects: improved FV intake (+0.2–0.7 portions), reduced fat intake, weight loss (−4.4 to −1.0 kg), HDL increase (+0.06 mmol/L), cholesterol reduction | High heterogeneity, self-reporting bias, lack of long-term data, limited economic outcome reporting, generalizability concerns | Inconsistent population/workplace reporting; unclear effect of dietary component in multicomponent interventions | Improvements in FV and fat intake, BMI, cholesterol; mixed/limited results on productivity, absenteeism, and economic outcomes |
Table 2.
Descriptive Summary of Included Studies by Country and Sector (n = 22).
| Country / Region | Freq. (n) | Percent (%) | Cumulative (%) | Sector | Freq. (n) | Percent (%) |
|---|---|---|---|---|---|---|
| Italy | 3 | 13.6% | 13.6% | Dental / Dentists | 6 | 27.3% |
| Greece | 1 | 4.5% | 18.1% | Physicians | 2 | 9.1% |
| Turkey | 3 | 13.6% | 31.7% | Healthcare workers (mixed) | 7 | 31.8% |
| China | 1 | 4.5% | 36.2% | Nurses | 1 | 4.5% |
| India | 1 | 4.5% | 40.7% | Public health / community health | 1 | 4.5% |
| Ecuador | 1 | 4.5% | 45.2% | Students (healthcare) | 1 | 4.5% |
| Brazil | 1 | 4.5% | 49.7% | Petrochemical workers (industrial) | 1 | 4.5% |
| USA | 1 | 4.5% | 54.2% | Academic medical staff | 1 | 4.5% |
| Australia | 1 | 4.5% | 58.7% | Dietitians & healthcare professionals | 1 | 4.5% |
| Poland | 1 | 4.5% | 63.2% | Public health | 1 | 4.5% |
| UK | 1 | 4.5% | 67.7% | Mixed HCWs | 1 | 4.5% |
| Multi-country (Europe, Global) | 6 | 27.3% | 95% | Multi-sector (systematic reviews) | 6 | 27.3% |
| Finland | 1 | 4.5% | 100% | Multi-professional (health sector) | 1 | 4.5% |
| Total | 22 | 100% | 100% | Total | 22 | 100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



