Submitted:
15 June 2025
Posted:
17 June 2025
You are already at the latest version
Abstract
Schizophrenia has been associated with increased inflammatory and metabolic disturbances. Perceived family support possibly effectuates changes in inflammatory and metabolic biomarkers. The aim of the present study was to determine the associations between family support, C-reactive protein (CRP) and Body Mass Index (BMI) in a sample of schizophrenic outpatients. In this cross-sectional correlation study 206 schizophrenic outpatients in clinical remission completed the standardized self-report questionnaire that assessed family support (family support scale-FSS). Sociodemographic, clinical and laboratory data were also recorded. 49.5% of the participants had detectable CRP values (≥0.11mg/dl), whereas 14.6% had positive CRP levels (>0.6mg/dl). There was a significant difference in CRP levels across the different BMI groups (normal-weight/ overweight vs. obese). For obese patients, the crude odds ratio (OR) for detectable CRP values was 1.980 with 95% confidence interval (CI) [1.056, 3.713] and for positive CRP values the OR was 27.818 (95% CI [6.300, 122.838]). Significant positive correlations were observed among CRP, BMI and illness duration, while scores on FSS were negatively associated with these variables. Results from the binary logistic regression analysis indicated that both BMI and family support were significant factors in determining the likelihood of having positive CRP levels, with each unit increase in the BMI associated with a 17% (95% CI [0.025, 0.337]) increase in the odds and with each unit increase in family support leading to a 8.6% (95% CI [0.018, 0.15]) decrease. The moderation analysis revealed that the association between family support and the probability of having positive CRP levels depends on BMI values, but the magnitude of the decreased risk for positive CRP associated with the protective effect of family support is significant (b=-0.1972, SE=0.053, OR=0.821, p=0.000, 95% CI [-0.3010, -0.0934]) only for obese patients. The effect of perceived family support on inflammatory responses becomes evident in cases where beyond metabolic complications inflammatory processes have already been established. However, primary interventions are considered necessary for schizophrenic patients in order to maintain BMI within normal limits and avoid the subsequent nosological sequelae.
Keywords:
family support
; C-reactive protein
; Body Mass Index
; schizophrenia
1. Introduction
Contemporary scientific evidence implicates inflammatory processes in the pathogenesis of schizophrenia [1,2,3] with CRP representing one of the most frequently investigated biomarkers for systemic inflammation [4,5]. CRP is a nonspecific acute phase protein that is primarily generated by liver cells, in both acute and chronic inflammation, in response to inflammatory cytokines [6]. A multitude of cross-sectional studies have evidenced increased CRP levels in schizophrenia patients compared to controls [7,8,9] and longitudinal studies have demonstrated that higher CRP levels at baseline may increase the risk of schizophrenia at follow-up [10,11]. However, while observational data show a positive association between CRP and schizophrenia risk, Mendelian Randomization (MR) analyses support that genetically elevated CRP protects against schizophrenia risk [12,13,14]. A deficient immune response hypothesis early in life that could lead to chronic infection and the subsequent increased risk of schizophrenia has been proposed as a plausible explanation to reconcile this controversy [15,16], but no definite conclusion to disentangle this discrepancy has been reached [17].
Multiple studies evidenced that CRP levels in patients with schizophrenia are increased during acute phases [18,19], as well as in cases with more severe psychopathology [20,21], in treatment- resistant [22] and in antipsychotic- free disorder [23] and are associated with positive [24] and negative symptoms [25,26], cognitive deficits [27] and risk of metabolic syndrome [28]. Metabolic disturbances and obesity are highly prevalent among schizophrenic patients [29,30,31], with obesity affecting more than 50% of these patients [29]. BMI is frequently used as an index of obesity and its predictive utility for the occurrence of metabolic syndrome in patients with schizophrenia has been confirmed [32]. According to a research in drug-naïve patients with schizophrenia the levels of BMI and rates of obesity increase in parallel with the duration of the disorder, along its course [33]. Many factors contribute to elevated BMI in patients with schizophrenia, including disorder-specific symptoms, lifestyle elements and socioeconomic issues, such as negative symptoms, social withdrawal, lack of physical activity, insufficient exercise, inadequate sleep, unhealthy diet and psychotropic medications [34,35,36]. The correlation between schizophrenia and BMI has been investigated in genetic and epidemiological studies [37,38,39,40] and a recent research, through an MR framework, has revealed a significant causal association between genetically predicted childhood BMI and the subsequent risk of schizophrenia in adulthood [41].
The positive association between BMI and CRP levels in the general population has been established [42,43] and the raised CRP values observed in individuals with an increased BMI are linked to a condition of low-grade systemic inflammation that affects overweight and obese individuals [44,45]. Research findings support that being overweight significantly raises the likelihood of clinically relevant increases in CRP, particularly pronounced in individuals with obesity [46,47]. MR studies evidence a directional relationship from BMI to CRP levels, whereas the bidirectional association has not been confirmed [43,48]. Among patients with schizophrenia many studies have documented the positive association between BMI and CRP levels; however, the directional relationship between these biomarkers remains elusive due to the cross-sectional nature of most of these studies [28,49]. A recent longitudinal research indicated a bidirectional relationship between BMI and CRP, with the effect of CRP on future BMI being more potent than vice versa [50]. More specifically, research findings support that assuming equal adiposity, patients with schizophrenia may have higher inflammation compared to healthy controls [11]. Thus, inflammation and the metabolic syndrome in schizophrenia have been the focus of scientific interest and individuals with schizophrenia consistently show several metabolic disruptions and have increased systemic inflammation both having effects on the brain and contributing to higher morbidity and premature mortality associated with the disorder [51,52,53,54,55,56].
Research evidence suggests that the inflammatory response may serve as the final common pathway through which environmental risk factors are implicated in the pathophysiology of schizophrenia [57,58,59]. Social support from relationships with family and significant others, possibly through beneficial influences on immune-mediated inflammatory processes, has been identified as a protective factor associated with lower rates of morbidity and mortality [60,61]. Perceived social support which is assumed to be a more representative aspect, appraising the quality of support received, protects against the risks of inflammation [62]. Perceived family support is considered an essential element of social support and refers to how an individual views the assistance provided by the other family members. Most people with schizophrenia live with their family members and even for those who live separately, their families are actively involved in their relative’s life providing care and support [63,64]. Parental support significantly influences the development of coping strategies for individuals with schizophrenia [65]. Existing literature reveals associations between parenting behaviors and child inflammatory markers, suggesting that positive parenting is associated with lower levels of inflammation, while negative parenting is linked to higher levels of inflammation [66]. Also, a higher level of parental support was associated with decreased child inflammation especially when medical conditions were present [67]. Concerning the role of parent – child attachment in obesity, a meta-analytic review demonstrated that BMI was negatively related with secure attachment [68]. Moreover, insecure and disorganized attachment in early infancy has been associated with higher levels of CRP levels in early childhood and predicted later obesity, compared to children with secure attachment [69]. Also, elevated CRP levels and BMI were documented in adults with schizophrenia and positive records for childhood maltreatment [70].
Increased physical morbidity and premature mortality among patients with schizophrenia, mostly due to the higher prevalence of cardiometabolic disorders, have extensively been studied [71,72]. These disorders are associated with increased levels of circulating inflammatory markers, such as CPR [73]. This low-grade inflammation and the metabolic alterations observed among patients with schizophrenia have also been consistently reported [74,75,76] and both inflammatory and metabolic indexes may serve as predictors of clinical outcome [52,77]. Recent research confirmed that the metabolic disturbances recorded in patients with schizophrenia are mainly attributed to schizophrenia - induced obesity [78]. A large-scale multicenter study provided evidence that individuals with both obesity and schizophrenia exhibited more pronounced neurostructural brain alterations than people with only one of these conditions [51]. Research findings have identified a shared genetic liability between binge eating behaviors and schizophrenia, with impaired social cognition as an intermediate phenotype [79]. Also, disordered eating behaviors, such as emotional eating and loss of control eating are prevalent among patients with schizophrenia and are linked with both obesity and inflammation [80,81,82,83]. In search for a favorable factor that would counteract these adverse conditions, family support emerged and several studies evidenced that the active involvement and systematic engagement of family members in the care of schizophrenic patients predicted positive outcomes, by enhancing adaptation resources, improving treatment adherence and ultimately the quality of life of patients with schizophrenia [84]. However, schizophrenia has a tendency to cause cognitive deficits in various domains, including social cognition [85,86], which could affect the ability to perceive family support [87], and possibly undermine its protective influence [88].
The theoretical framework of this study was that the perceived presence of supportive family relationships has the ability to protect individuals with schizophrenia from the adverse inflammatory and metabolic pathophysiological processes, while the perceived absence of such relationships increases disease risks. A literature review did not retrieve any study that explored the association between CRP and perceived family support and further examined whether this association differed along the BMI spectrum in a sample of outpatients with schizophrenia, leaving a knowledge gap we sought to address. Therefore, the purpose of this study was to explore the interrelations between CRP, BMI and perceived family support among individuals with schizophrenia in outpatient treatment. More specifically, elucidating the extent to which the association between CRP and family support is stratified by BMI could improve our understanding about the role of perceived family support and provide opportunities for psychotherapeutic and psychosocial interventions. The abovementioned assumptions give rise to the following hypotheses:
Hypothesis 1.
BMI is positively associated with and predicts CRP.
Hypothesis 2.
Perceived Family Support is negatively related to and predicts CRP.
Hypothesis 3.
BMI interacting with Perceived Family Support serves as a moderator in the association between CRP and Perceived Family Support. The moderator effect of the BMI is assumed to be focused on obese individuals who have higher levels of low-grade inflammation due to their increased BMI.
2. Subjects and Methods
2.1. Research Design
A cross-correlation study was conducted to address the above hypothetical statements. Participants were outpatients with a diagnosis of schizophrenia who received treatment at the Outpatient Psychiatric Department of ‘’Sotiria” General Hospital from October 2022 to March 2024. After the approval from the Clinical Research Ethics Committee of ‘’Sotiria” General Hospital (Approval Number: 26741/21-10-2021), the researchers explained the research objectives to the participants who provided both written and verbal informed consent. This study was performed in accordance with the World Medical Association Declaration of Helsinki (1975, revised 2008), following the ethical principles outlined in the General Data Protection Regulation (GDPR - 2016/679) of the European Union, and the guidelines of the International Committee of Medical Journal Editors. Prior to the performance of any procedures related to this study and according to the ethical considerations, patients were assured that any information obtained would remain confidential, that participation in the survey was completely voluntary and that at any point potential volunteers could opt to withdraw from the study. Once each participant had received comprehensive information on the study procedure and recruited, an appointment was arranged the following morning between 8:00 and 9:00 a.m. to collect the demographic and clinical data, weight and height measurements and then proceed to the laboratory examinations. Before venous blood was drawn, patients were requested to fast for more than eight hours and to maintain a normal diet the night before, avoid alcohol consumption and refrain from strenuous exercise. At the end, each participant was required to complete a semi-structured form created by research staff to gather demographic information and to respond to a self-report questionnaire to evaluate their perception of family support.
2.2. Study Participants
Purposive sampling method was used to perform the study which included 206 outpatients, with a confirmed psychiatric diagnosis of schizophrenia, based on the International Classification of Diseases-10 (ICD-10), who were receiving ongoing treatment at the Psychiatric Outpatients Department. Participants had to fulfill the following inclusion and exclusion criteria: (i) being between 18 and 65 years old, (ii) being in a stable psychiatric condition, in clinical remission, and not having been hospitalized or had changes in psychotropic medication or psychosocial status within 90 days before joining the study, (iii) having been hospitalized for psychiatric issues at least twice before (for diagnostic accuracy), iv) having coherent verbal rapport during the completion of data questionnaire. Participants were excluded if they had untreated visual or hearing impairments, neurological disorders or damage to the central nervous system, developmental disabilities, signs of intellectual disability, severe cognitive and neuropsychological impairment, personality disorders, psychotic disorders associated with clinical medical conditions or substance use, substance addiction and history of substance use in the last six months, and a record of current substance or alcohol abuse. Included participants were prior assessed by a physician to determine the presence of any clinically significant or unstable medical disorder or chronic general medical condition. In this sense, patients with past or present cardiovascular disease, chronic lung disease, liver, kidney disease, arthritis or rheumatoid arthritis, autoimmune, blood diseases, diabetes mellitus and/or HbA1C levels above 5.7%, pregnancy or lactation were excluded. Also, any active infectious illness or primary inflammatory disease; current use of corticosteroids or non-steroidal anti-inflammatory drugs; recent or ongoing use of warfarin or anticoagulant medications; recent or current use of antidepressants; antibiotics or probiotics in the past three months; urine drug screen positive for psychoactive drugs; smoking habits (more than 1 cigarette per day) and drinking habits (more than 1 unit alcohol per week), were excluded from the study. To confirm the above criteria, upon study enrollment, a thorough health assessment and clinical evaluation were performed.
2.3. Minimal Sample Size Calculation
The sample size calculation for the statistical analysis of the binary logistic regression was carried out using G-Power 3.1 software [89]. To compute the required sample size, for the most influential independent variable which is BMI, the significance level was set at 0.05, the statistical power at 0.95, R2 for the other x variables at 0.218 (which is the value calculated by regressing the independent variable of prime interest on all the other independent variables, using multiple linear regression) [90], selecting the normal distribution type for BMI, with 28.8493 as mean value and 4.86474 as the standard deviation, 1.293 as the odds ratio and the probability of y = 1 under H0 as 0.0000689541, which is estimated by using the formula EXP(B)/(1+EXP(B)), with B being the constant intercept estimate B (see results section). The total sample size determined by this calculation was 115, with the actual power of 0.95, thus the sample size in this study was deemed adequate. G-Power software was also used to verify sample adequacy for moderation analysis. To compute the required sample size, in regression with the R square increase, the significance level was set at 0.05, the statistical power at 0.95, with the number of tested predictors at 1, total number of predictors 3 and the effect size determined with the formula: f2 = R2² - R1²/ 1- R2²= 0.08. The total sample size determined by this calculation was 152, with the actual power of 0.95, thus the sample size in this study was also deemed adequate.
2.4. Measurement Tools
Participants in this study provided demographic data and clinical information such as age, gender and illness duration.
2.4.1. BMI
BMI measurements were conducted by trained nurse personnel. Based on a standard formula, each participant’s weight (in kilograms) was divided by their height (in squared meters) to determine their BMI. These measurements were performed with the SECA 769, Electronic scale with height measuring rod (SECA, Hamburg, DE). In this way and according to the World Health Organization criteria, the sample was grouped into underweight with BMI<18.5 kg/m2, normal weight with 18.5≤BMI<25 kg/m2, overweight with 25≤BMI<30 kg/m2 and obese participants with BMI≥30 kg/m2.
2.4.2. CRP
Serum CRP levels were determined using a quantitative turbidimetric test (CRP-turbilatex) with the latex agglutination immuno-turbidimetric method. The lowest detectable limits were 0.11mg/dl and the normal reference values were up to 0.6mg/dl, according to the manufacturer’s instructions (SPINREACT 2021, Spain) and the laboratory reference range. The maximum reference level for CRP was set at 1mg/dl because values above this threshold most likely indicate a suspected infection [91]. The analysis was performed at the clinical biochemistry laboratory of ‘’Sotiria” General Hospital.
2.4.3. Family Support Scale (FSS)
The Greek version of the Family Support Scale is designed to measure the sense of support individuals receive from family members, with whom they reside. The scale is self-administered and includes 13 items on Likert ratings, with 1 denoting 'strongly disagree' to 5 indicating 'strongly agree'. All items revolve around the relationships among cohabiting individuals [92,93,94]. A greater sense of family support is displayed by higher ratings on the scale. People living independently were not required to complete the scale [92]. Cronbach's alpha for this study’s internal reliability was 0.786.
2.5. Statistical Analysis
Initially descriptive analysis was carried out. Means and standard deviations were used to express the continuous variables and percentages were used to report the categorical variables. A Kolmogorov-Smirnov test was used to assess the distribution of data. Skewed variables (illness duration, BMI and scores on FSS) were transformed to normal with the two-step approach [95]. The distribution of CRP was markedly rightly-skewed and was thus treated as a non-normally distributed variable which was assessed with non parametric methods. Using the Kruskal-Wallis test, differences in CRP levels across BMI groups were evaluated. The independent samples t-test was employed to compare illness duration, scores on FSS and BMI differences as to gender. To compare CRP values as to gender we used the Mann–Whitney U test. The correlation of continuous variables was done using the Spearman's correlation test for nonparametric bivariate correlations analyses (including CRP) or using Pearson correlations for normally distributed continuous variables (except CRP). Further, CRP was categorized as a dichotomous variable; with detectable but normal CRP values (≥0.11mg/dl) and positive CRP values (>0.6mg/dl). Unadjusted odds ratios (ORs) and 95% confidence intervals (95% CIs) for detectable and positive CRP values for obese participants were estimated using logistic regression. To assess the risk factors of positive CRP values in patients with schizophrenia a binary logistic regression analysis was performed, adjusted for the effects of possible confounding variables (age, gender, illness duration, BMI and scores on FSS). Moderation by BMI was assessed through the introduction of a BMI*FSS interaction term in the logistic regression analysis. Simple slopes analysis was performed using Hayes' SPSS Process Macro Model 1, to report the moderating effect at different levels of BMI. The data analyses were conducted using SPSS software (Version 24.0). For all statistical analyses, statistical significance was set at p < 0.05 (two-tailed).
3. Results
3.1. General Characteristics of Participants and Scores on Outcome Variables
This study included a total of 206 participants (100 males and 106 females). According to the BMI values, 22.3% of participants were classified as normal weight subjects, 29.1% as overweight and 35% as obese. There were no underweight participants to be included in the study and the sample’s mean weight was within the overweight category. 49.5% of the participants had detectable CRP values, whereas 14.6% had positive CRP levels. Their demographic and clinical characteristics are presented in Table 1.
Regarding gender, no other differences were observed as to the study variables, except from the age, with females being older compared to males (t-test p < 0.05, 44.98 ± 14.37 vs. 41.36± 10.79, Table 1). A Kruskal-Wallis test indicated that there were significant differences in CRP values across the different BMI groups χ2(2) = 12.07, p = 0.002, with a mean rank CRP score of 75.27 for normal weight, 75.36 for overweight and 100.76 for obese participants (Figure 1).
3.2. Correlations Among Continues Variables
Using Pearson correlation significant associations were observed among normally distributed variables. Illness duration positively correlates with BMI values and negatively with scores on FSS. Also, age positively correlates with illness duration and the BMI values (Table 2). Since CRP values were non-normally distributed, the Spearman correlation was employed to determine these relationships. Specifically, CRP had a positive correlation with BMI and a negative association with FSS (Table 3).
3.3. Binary Logistic Regression Analysis Analyses
Simple binary logistic regression analysis was performed to calculate the unadjusted odds ratios (ORs) and 95% confidence intervals (95% CIs) for detectable and positive CRP values for obese participants. Results indicate that obese patients are 1.980 times more likely (OR) to have detectable CRP values with 95% confidence interval (CI) [1.056, 3.713] and 27.818 times more likely (OR) to have positive CRP values with (95% CI [6.300, 122.838]), compared to non-obese participants (Table 4).
A binary logistic regression analysis was conducted to investigate the effects of associated factors (age, gender, illness duration, BMI, scores on FSS) on the likelihood of having positive CRP values (>0.6mg/dl). To assure the reliability and validity of this method necessitates checking that the underlying assumptions are satisfied; independence of observations (absence of autocorrelation or repeated measures and the calculated Durbin –Watson value of 2.140 was within normal range), linearity of the logit which was confirmed with the Box-Tidwell procedure (the relationship between the continuous predictor variables and the log odds of the binary outcome were linear), absence of multicollinearity among the independent variables (checked through the correlation method, the correlation coefficients are <0.70 and the VIF values were within acceptable range), and the absence of significant outliers based on the Cook’s distance (<4/206).
The model was statistically significant (x2(5)=29.379, p<0.001), accounting for 22% (Cox & Snell R Square) and 38.4% (Nagelkerke R Square) of the variance in the presence of positive CRP values and correctly classifying 89.8% of cases. The Hosmer and Lemeshow test suggested a good fit to the data (x2(8)=13.555, p=0.094). In the model BMI was a significant predictor (B=0.158, Wald=5.396, p=0.020, Exp(B)= 1.171, 95% CL [1.025, 1.337]), with each unit increase associated with with 17% increase in the odds of having positive CRP values. At the same time family support was a a significant predictor (B=-0.090, Wald=6.086, p=0.014, Exp(B)= 0.914, 95% CL [0.850, 0.982]), with each unit increase in family support leading to a 8.6% (95% CI [0.018, 0.15]) decrease in the odds of having positive CRP values (Table 5). These results indicate that both BMI and family support are significant risk and protective factors, respectively, which determine the likelihood of the presence of positive CRP values, thus confirming the first and second research hypotheses.
3.4. Moderated Binary Logistic Regression Analysis
Further, a moderated binary logistic regression analysis was conducted utilizing the Model 1 of Hayes PROCESS macro to investigate if the relationship between family support and the likelihood of having positive CRP values was moderated by BMI. The dependent variable was the probability of having positive CRP, the independent variable was family support, the moderator was BMI and included covariates were age, gender and illness duration. The interaction term was significant (B = -0.022, SE = 0.100, p < 0.05), indicating that the effect of family support on the probability of having positive CRP values depended on levels of BMI (Table 6), thus confirming the third hypothesis. Simple slopes analysis revealed that at high levels of BMI (+1 SD), family support was negatively associated with the likelihood of having positive CRP (B = -0.1724, p < 0.01), whereas at low levels of BMI (-1 SD), the association was nonsignificant (B = 0.0519, p = 0.46), (Table 7, Figure 2). The model explained 45% of the variance in positive CRP values (Nagelkerke R² = 0.4521). In Figure 3, to visualize the nature of the BMI by family support interaction as predictors of the probability of having positive CRP and help with the interpretation, we used centered scores of both predictors.
4. Discussion
This study investigates the association between perceived family support, circulating CRP and BMI and the results from the correlation analysis, the binary logistic regression and moderation analysis provide strong evidence confirming the research hypotheses. More specifically, concerning the first hypothesis, the positive correlation between circulating CRP and measured BMI and the role of BMI as a risk factor increasing the likelihood of having positive CRP values is consistent with findings from previous studies conducted with participants from the general population and among patients with schizophrenia [42,43,44,45,46,47,48,49]. Most of these studies suggest that the observed correlation between CRP and BMI is attributed to BMI increase, with CRP being an index of elevated adiposity [45,47,48,96,97,98]. In particular, the pathophysiological process in obesity and metabolic dysregulation implicates systemic inflammation through the activation of macrophages in the adipose tissue, which release inflammatory cytokines causing hyperlipidemia and insulin resistance, further worsening the metabolic status, which in turn promotes the production of cytokines by the adipose tissue, thus contributing to chronic inflammation [99,100,101].
The investigation of the second and third research hypotheses produced the main findings of this study which highlight the protective role of perceived family support among outpatients with schizophrenia, being able to counteract the low-grade inflammation by reducing the likelihood of positive CRP values. Most individuals with schizophrenia, due to the disabilities of the disorder, rely on family members who are their primary caregivers. Clinical evidence suggests that the vast majority of patients with schizophrenia are unable to maintain basic social functions and only a minority retain regular employment [102,103]. In this sense, the existence of a supportive family network is of outmost importance. Supportive family relationships, beyond safeguarding treatment adherence, may motivate healthy behaviors that promote good health and improve overall well-being. Healthy diet and physical exercise are well known anti-inflammatory factors [104,105], frequently encouraged by a protective family environment, whereas pro-inflammatory diets [106], smoking and/or drug abuse are usually deterred.
Evidence from a large general adult population study documented that social/family strain significantly increased the risk of inflammation and most importantly the association of social/family strain with inflammation was stronger than the relationship of social/family support and inflammation [107]. These results are in accordance with our findings and provide a plausible explanation for the steeper slope in the relationship between the odds of having positive CRP values and expressing lower than average perceived family support, while a less steep slope accounts for the relationship between the odds of having positive CRP values and scoring above average on the FSS (Figure 3). Another finding from this study that needs to be clarified is that the protective anti-inflammatory effect of family support is significant only for obese patients. In accordance with other studies with participants from the general population [108,109] and among patients with schizophrenia [28,52,110], obese participants in this study were significantly more likely to have positive CRP values compared to non-obese individuals. In these cases, where beyond metabolic complications inflammatory processes have already been established; family support has the ability to attenuate this low-grade inflammation. Yet, because this study is cross-sectional, precluding the direction of causality, these findings could signify that low perceived family support as experienced by patients in strenuous and adverse family backgrounds may have resulted in increased levels of inflammation.
Studies support that greater social strain is linked to higher levels of inflammation [111,112]. Meanwhile, a meta-analysis suggested that social support and social integration are significantly associated with lower levels of inflammation [113,114]. Research indicates that individuals with schizophrenia have lower perceived social support than those without schizophrenia [88] and frequently early life adversities force them to withdraw and isolate themselves from other family members [115]. However, due to the highly prevalent social cognitive deficits among these patients, their families are the main, if not the only, social network [116]. Their role is to compensate for key social stressors, to protect the emotional health of their vulnerable relatives by combating stigma, enhancing self-esteem and coping strategies, reducing feelings of isolation, increasing social engagement, and promoting a sense of belonging. On the other hand, family strain derived from high levels of expressed emotion, conflictual family relationships, stigma, emotional and financial burdens significantly impact the mental health of individuals with schizophrenia who experience higher levels of distress effectuating increases in pro-inflammatory responses which ultimately lead to poorer treatment outcomes [117,118].
As stated, strain from family relationships may play an important role in inflammatory processes, because relationships with family members are likely to last through significant periods of life and are not a matter of choice, as in other relationships. When family relationships are particularly stressful, the need to maintain them over time may increase the strain experienced by these relationships, making family tension detrimental to health, which is manifested through inflammatory processes. In turn, immune dysregulation may lead to the cluster of chronic metabolic disorders [119]. For instance, research has shown that inflammation can interfere with insulin production and may also cause hypothalamic dysfunction, both of which are involved in weight gain [120,121]. Furthermore, changes in lipid and lipoprotein metabolism linked to inflammation lead to raised triglyceride levels and lowered HDL cholesterol synthesis [122]. From another perspective, the literature suggests that disordered eating behaviours often co-exist with psychotic disorders and social cognitive deficits are particularly prevalent among these patients [79], rendering them less able to appreciate family support. In addition, research studies have already documented cognitive deficits and related neuropsychiatric symptoms associated with obesity, as well as emotional eating behaviors in an attempt to regulate negative emotions [81,123].
More than one third of participants in this study were obese. Findings from other studies among schizophrenic outpatients report comparable or even higher prevalence rates of obesity [29,124,125]. The relationship of schizophrenia and obesity has gained attention due to the high risk of associated comorbidities, such as cardiovascular diseases and metabolic syndrome, increasing all cause morbidity and mortality and reducing life expectancy [126,127]. Several studies have reported associations between obesity and negative symptoms, insomnia and night-eating and a decrease in quality if life among individuals with schizophrenia [128,129,130,131]. An understanding of the clinical factors that predict obesity risk is critical for targeting patients with psychotic disorders who are more prone to weight gain and metabolic syndrome [132]. Patients with schizophrenia are frequently characterized by lack of control over eating behaviors and are more likely to consume unhealthy foods [133]. Several risk factors are implicated in these problematic eating behaviors and include tobacco smoking, type 2 diabetes, sleep disturbances, adverse effects of psychotropics, anxiety and depression [134,135,136,137], and lack of psychosocial rehabilitation [80,138].
The above mentioned findings hold practical implications. The fact that obesity and associated metabolic abnormalities are present even in the early stages of psychotic disorders, suggest the need for early interventions. Standard protocols include effective metabolic monitoring guidelines and preventive measures for patients with schizophrenia, especially for patients on psychiatric medications, upon discharge from psychiatric hospitalization and during follow-up [139,140]. Lifestyle interventions, dietary manipulation and aerobic physical intervention programs effectuate improvements in addressing obesity and preventing weight gain [141,142,143,144]. The most important finding from this study supports family involvement during the treatment of patients with schizophrenia. The National Institute for Health and Care Excellence (NICE) [145] incorporated Family Therapy in clinical guidelines when drafting psychiatric treatment plans, in order to provide psychoeducation, enable families to manage emotions effectively by reducing family strain, improve their communication and problem solving skills [146,147].
This study exhibits certain limitations. Due to the cross-sectional design conclusions about the direction of causality cannot be drawn. Moreover, the generalizability of the overall results is limited because it was a single-center study in a specific geographic area. Another drawback was the lack of control sample to compare the laboratory findings, but the aim of this study was to conduct a correlation and not a comparative analysis. Additionally, data on nutrition and activity measures were not available. Similarly, although we had data on the prescribed antipsychotics and knowing about their differential effects on the immune system, the sample size prevented subgroup analysis by antipsychotic types. Also, there were no underweight participants to be included in the study in order to identify possible differences in results as to other participants. Finally, the results of this study might have been influenced by potential confounding factors, such as incidental psychosocial events, or unknown medications administered to participants during the research period.
4. Conclusion
The results of this study elucidate the relationships between perceived family support, peripheral CRP and BMI and highlight the protective role of family support in moderating inflammatory processes, particularly in outpatients with schizophrenia who are at metabolic risk associated with obesity. The integration of family therapy into psychiatric treatment plans, in addition to standard monitoring of weight and metabolic indices, seems to offer promising results for prevention and intervention purposes.
Author Contributions
Conceptualization, A.P., A.T.; methodology, A.P., A.T., E.K,; software, A.T., I.I., A.P.; validation, A.P., A.T., S.B.; formal analysis, A.P., A.T., S.B.; investigation, A.P., A.T.; resources, A.P., N.S., D.K., C.S.; data curation, A.P., D.K., C.S,; writing—original draft preparation, A.P., I.I.; writing—review and editing, A.P., I.I; supervision, A.P., A.T; project administration, A.P., A.T. All authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Clinical Research Ethics Committee of “Sotiria” General Hospital (Number 26741/21-10-2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Participation in the research was voluntary.
Data Availability Statement
The data and the questionnaires of the study are available upon request from the corresponding author.
Acknowledgments
We would like to thank all participants in our study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Khandaker, G.M.; Cousins, L.; Deakin, J.; Lennox, B.R.; Yolken, R.; Jones, P.B. (2015). Inflammation and immunity in schizophrenia: Implications for pathophysiology and treatment. Lancet Psychiatry 2, 258–270. [CrossRef]
- Müller, N.; Weidinger, E.; Leitner, B.; Schwarz, M.J. (2015) The role of inflammation in schizophrenia. Front. Neurosci. 9:372. [CrossRef]
- Sun, H.-L.; Bai, W.; Li, X.-H.; Huang, H.; Cui, X.-L.; Cheung, T.; Su, Z.-H.; Yuan, Z.; Ng, C.H.; Xiang, Y.-T. (2022). Schizophrenia and Inflammation Research: A Bibliometric Analysis. Front. Immunol. 13:907851. [CrossRef]
- Fond, G.; Lançon, C.; Auquier, P.; Boyer, L. (2018) C-Reactive Protein as a Peripheral Biomarker in Schizophrenia. An Updated Systematic Review. Front. Psychiatry, 9, 392. [CrossRef]
- Ullah, I.; Awan, H.A.; Aamir, A.; Diwan, M.N.; de Filippis, R.; Awan, S.; Irfan, M.; Fornaro, M.; Ventriglio, A.; Vellante, F.; Pettorruso, M.; Martinotti, G.; Di Giannantonio, M.; De Berardis, D. Role and Perspectives of Inflammation and C-Reactive Protein (CRP) in Psychosis: An Economic and Widespread Tool for Assessing the Disease. Int J Mol Sci. 2021 Dec 2;22(23):13032. [CrossRef]
- Moshage, H.J.; Roelofs, H.M.J.; van Pelt, J.F.; Hazenberg, B.P.C.; van Leeuwen, M.A.; Limburg, P.C.; Aarden, L.A.; Yap, S.H. (1988). The effect of interleukin-1, interleukin-6 and its interrelationship on the synthesis of serum amyloid A and C-reactive protein in primary cultures of adult human hepatocytes. Biochem. Biophys. Res. Commun. 155, 112–117. [CrossRef]
- Miller, B.J.; Culpepper, N.; Rapaport, M.H. C-reactive protein levels in schizophrenia: a review and meta-analysis. Clin Schizophr Relat Psychoses. 2014 Jan;7(4):223-30. [CrossRef] [PubMed]
- Fernandes, B.S.; et al. C-reactive protein is increased in schizophrenia but is not altered by antipsychotics: meta-analysis and implications. Mol Psychiatry. [CrossRef]
- Lestra, V.; Romeo, B.; Martelli, C.; Benyamina, A.; Hamdani, N. Could CRP be a differential biomarker of illness stages in schizophrenia? A systematic review and meta-analysis. Schizophr Res. 2022 Aug;246:175-186. [CrossRef] [PubMed]
- Metcalf, S.A.; Jones, P.B.; Nordstrom, T.; Timonen, M.; Mäki, P.; Miettunen, J.; Jääskeläinen, E.; Järvelin, M.R.; Stochl, J.; Murray, G.K.; Veijola, J.; Khandaker, G.M. Serum C-reactive protein in adolescence and risk of schizophrenia in adulthood: A prospective birth cohort study. Brain Behav Immun. 2017 Jan;59:253-259. [CrossRef] [PubMed] [PubMed Central]
- Osimo, E.F.; Baxter, L.; Stochl, J.; et al. Longitudinal association between CRP levels and risk of psychosis: a meta-analysis of population-based cohort studies. npj Schizophr 7, 31 (2021). [CrossRef]
- Hartwig, F.P.; Borges, M.C.; Horta, B.L.; Bowden, J.; Davey Smith, G. Inflammatory biomarkers and risk of schizophrenia: a 2-sample Mendelian randomization study. JAMA Psychiatry 2017;74: 1226–233. [CrossRef]
- Ligthart, S.; Vaez, A.; Vosa, U.; et al. Genome analyses of >200,000 individuals identify 58 loci for chronic inflammation and highlight pathways that link inflammation and complex disorders. Am J Hum Genet 2018;103:691–706. [CrossRef]
- Said, S.; Pazoki, R.; Karhunen, V.; Võsa, U.; Ligthart, S.; Bodinier, B.; Koskeridis, F.; Welsh, P.; Alizadeh, B.Z.; Chasman, D.I.; Sattar, N.; Chadeau-Hyam, M.; Evangelou, E.; Jarvelin, M.-R.; Elliott, P.; Tzoulaki, I.; Dehghan, A. 2022. Genetic analysis of over half a million people characterises C-reactive protein loci. Nat. Commun 13, 2198. [CrossRef]
- Gardner, R.M.; Dalman, C.; Wicks, S.; Lee, B.K.; Karlsson, H. Neonatal levels of acute phase proteins and later risk of non-affective psychosis. Transl. Psychiatry 3, e228. [CrossRef]
- Blomström, Å.; Gardner, R.; Dalman, C.; et al. Influence of maternal infections on neonatal acute phase proteins and their interaction in the development of non-affective psychosis. Transl Psychiatry 5, e502 (2015). [CrossRef]
- Ligthart, S. Commentary: CRP and schizophrenia: cause, consequence or confounding? Int J Epidemiol. 2019 Oct 1;48(5):1514-1515. [CrossRef] [PubMed]
- Jacomb, I.; Stanton, C.; Vasudevan, R.; Powell, H.; O’Donnell, M.; Lenroot, R.; Bruggemann, J.; Balzan, R.; Galletly, C.; Liu, D.; Weickert, C.S.; Weickert, T.W. (2018) C-Reactive Protein: Higher During Acute Psychotic Episodes and Related to Cortical Thickness in Schizophrenia and Healthy Controls. Front. Immunol. 9:2230. [CrossRef]
- Johnsen, E.; Fathian, F.; Korken, R.; Steen, V.; Jorgensen, H.; Gjestad, R.; et al. The serum level of C-reactive protein (CRP) is associated with cognitive performance in acute phase psychosis. BMC Psychiatry (2016) 16:1–11. [CrossRef]
- Fan, X.; Pristach, C.; Liu, E.Y.; Freudenreich, O.; Henderson, D.C.; Goff, D.C. Elevated serum levels of C-reactive protein are associated with more severe psychopathology in a subgroup of patients with schizophrenia. Psychiatry Res. (2007) 149:267–71. [CrossRef]
- Orsolini L, Sarchione F, Vellante F, Fornaro M, Matarazzo I, Martinotti G, Valchera A, Di Nicola M, Carano A, Di Giannantonio M, Perna G, Olivieri L, De Berardis D. Protein-C Reactive as Biomarker Predictor of Schizophrenia Phases of Illness? A Systematic Review. Curr Neuropharmacol. 2018;16(5):583-606. [CrossRef] [PubMed] [PubMed Central]
- Challa, F.; Seifu, D.; Sileshi, M.; Getahun, T.; Geto, Z.; Kassa, D.; Alemayehu, M.; Mesfin, M.; Fekadu, A.; Woldeamanuel, Y. Serum level of high sensitive C-reactive protein and IL - 6 markers in patients with treatment-resistant schizophrenia in Ethiopia: a comparative study. BMC Psychiatry. 2021 Aug 31;21(1):428. [CrossRef] [PubMed] [PubMed Central]
- Fawzi, M.H.; Fawzi, M.M.; Fawzi, M.M.; Said, N.S. C-reactive protein serum level in drug-free male Egyptian patients with schizophrenia. Psychiatry Res 190, 91–97 (2011). [CrossRef]
- Dimitrov, Dimitre H., Shuko Lee, Jesse Yantis, Craig Honaker, Nicole Braida, et Consuelo Walss-Bass. 2016. « Elevated Serum Levels of High-Sensitivity C-Reactive Proteins Are Associated with Severe Delusional Symptoms in a Subgroup of Patients with Schizophrenia ». The Journal of Clinical Psychiatry 77 (1): 131-32. [CrossRef]
- Garcia-Rizo, C.; Fernandez-Egea, E.; Oliveira, C.; Justicia, A.; Bernardo, M.; Kirkpatrick, B. Inflammatory markers in antipsychotic-naïve patients with nonaffective psychosis and deficit vs. nondeficit features. Psychiatry Res. 2012 Jul 30;198(2):212-5. Epub 2012 Mar 8. Erratum in: Psychiatry Res. 2013 Dec 30;210(3):1329. [CrossRef] [PubMed]
- Boozalis, Ted, Antonio L. Teixeira, Raymond Young-Jin Cho, et Olaoluwa Okusaga. 2017. « C-Reactive Protein Correlates with Negative Symptoms in Patients with Schizophrenia ». Frontiers in Public Health 5: 360. [CrossRef]
- Bulzacka, E.; Boyer, L.; Schurhoff, F.; Godin, O.; Berna, F.; Brunel, L.; et al. Chronic peripheral inflammation is associated with cognitive impairment in schizophrenia: results from the multicentric FACE-SZ dataset. Schizophr Bull. (2016) 42:1290–302. [CrossRef]
- Boozalis, Ted, Sridevi Devaraj, Olaoluwa O. Okusaga. 2019. « Correlations between Body Mass Index, Plasma High-Sensitivity C-Reactive Protein and Lipids in Patients with Schizophrenia ». The Psychiatric Quarterly 90 (1): 101-10. [CrossRef]
- Annamalai, A.; Kosir, U.; Tek, C. Prevalence of obesity and diabetes in patients with schizophrenia. World J Diabetes. 2017 Aug 15;8(8):390-396. [CrossRef] [PubMed] [PubMed Central]
- Cordes, J.; Bechdolf, A.; Engelke, C.; Kahl, K.G.; Balijepalli, C.; Lösch, C.; Klosterkötter, J.; Wagner, M.; Maier, W.; Heinz, A.; de Millas, W.; Gaebel, W.; Winterer, G.; Janssen, B.; Schmidt-Kraepelin, C.; Schneider, F.; Lambert, M.; Juckel, G.; Wobrock, T.; Riedel, M.; Moebus, S. Prevalence of metabolic syndrome in female and male patients at risk of psychosis. Schizophr Res. 2017 Mar;181:38-42. [CrossRef]
- Jeong, S.H.; Lee, N.Y.; Kim, S.H.; Chung, I.W.; Youn, T.; Kang, U.G.; et al. Long-term evolution of metabolic status in patients with schizophrenia stably maintained on second-generation antipsychotics. Psychiatry Investig. 2018;15:628–37. [CrossRef]
- Sugawara, N.; Yasui-Furukori, N.; Yamazaki, M.; Shimoda, K.; Mori, T.; Sugai, T.; Matsuda, H.; Suzuki, Y.; Ozeki, Y.; Okamoto, K.; Sagae, T.; Someya, T. Predictive Utility of Body Mass Index for Metabolic Syndrome Among Patients with Schizophrenia in Japan. Neuropsychiatr Dis Treat. 2020 Sep 30;16:2229-2236. [CrossRef]
- Liang, J.; Cai, Y.; Xue, X.; Li, X.; Li, Z.; Xu, C.; Xie, G.; Yu, Y. (2022) Does Schizophrenia Itself Cause Obesity? Front. Psychiatry 13:934384. [CrossRef]
- Chouinard, V.A.; Pingali, S.M.; Chouinard, G.; Henderson, D.C.; Mallya, S.G.; Cypess, A.M.; Cohen, B.M.; Öngür, D. Factors associated with overweight and obesity in schizophrenia, schizoaffective and bipolar disorders. Psychiatry Res. 2016 Mar 30;237:304-10. [CrossRef]
- Limosin, F.; Gasquet, I.; Leguay, D.; Azorin, J.M.; Rouillon, F. (2008). Body mass index and prevalence of obesity in a French cohort of patients with schizophrenia. Acta psychiatrica Scandinavica, 118(1), 19–25. [CrossRef]
- Allison, D.B.; Casey, D.E. Antipsychotic-induced weight gain: a review of the literature. J Clin Psychiatry. 2001;62 Suppl 7:22-31. [PubMed]
- Aoki, R.; Saito, T.; Ninomiya, K.; Shimasaki, A.; Ashizawa, T.; Ito, K.; Ikeda, M.; Iwata, N. Shared genetic components between metabolic syndrome and schizophrenia: Genetic correlation using multipopulation data sets. [CrossRef] [PubMed] [PubMed Central]
- Sørensen, H.J.; Gamborg, M.; Sørensen, T.I.A.; Baker, J.L.; Mortensen, E.L. Childhood body mass index and risk of schizophrenia in relation to childhood age, sex and age of first contact with schizophrenia. Eur Psychiatry. 2016 Apr;34:64-69. [CrossRef]
- Cameron, I.M.; Hamilton, R.J.; Fernie, G.; MacGillivray, S.A. Obesity in individuals with schizophrenia: a case controlled study in Scotland. BJPsych Open. 2017 Oct 17;3(5):254-256. [CrossRef]
- Zeng, M.; Wang, X.; Zhou, J.; Zhang, X.; Zhang, X.; Chi, J.; Lu, C.; Wang, L.; Li, S. Body mass index-specific metabolic profiles in schizophrenia: implications for cognitive dysfunction and psychopathology. J Neural Transm (Vienna). 2025 May 24. [CrossRef]
- Xiao, P.; Li, C.; Mi, J.; Wu, J. Evaluating the distinct effects of body mass index at childhood and adulthood on adult major psychiatric disorders. Sci Adv. 2024 Sep 13;10(37):eadq2452. [CrossRef] [PubMed]
- Choi, J.; Joseph, L.; Pilote, L. Obesity and C-reactive protein in various populations: a systematic review and meta-analysis. Obes Rev. 2013 Mar;14(3):232-44. [CrossRef]
- Timpson, N.J.; Nordestgaard, B.G.; Harbord, R.M.; Zacho, J.; Frayling, T.M.; Tybjærg-Hansen, A.; Smith, G.D. C-reactive protein levels and body mass index: elucidating direction of causation through reciprocal Mendelian randomization. Int J Obes (Lond). 2011 Feb;35(2):300-8. [CrossRef]
- Xu, H.; Barnes, G.T.; Yang, Q.; Tan, G.; Yang, D.; Chou, C.J.; et al. Chronic inflammation in fat plays a crucial role in the development of obesity-related insulin resistance. J Clin Invest (2003) 112(12):1821–30. [CrossRef]
- Kawai, T.; Autieri, M.V.; Scalia, R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am J Physiol Cell Physiol (2021) 320(3):C375–c391. [CrossRef]
- Visser, M.; Bouter, L.M.; McQuillan, G.M.; Wener, M.H.; Harris, T.B. (1999). Elevated C-reactive protein levels in overweight and obese adults. JAMA 282, 2131–2135. [CrossRef]
- Wellen, K.E.; Hotamisligil, G.S. (2003). Obesity-induced inflammatory changes in adipose tissue. J. Clin. Invest. 112, 1785–1788. [CrossRef]
- Welsh, P.; Polisecki, E.; Robertson, M.; Jahn, S.; Buckley, B.M.; de Craen, A.J.; Ford, I.; Jukema, J.W.; Macfarlane, P.W.; Packard, C.J.; Stott, D.J.; Westendorp, R.G.; Shepherd, J.; Hingorani, A.D.; Smith, G.D.; Schaefer, E.; Sattar, N. Unraveling the directional link between adiposity and inflammation: a bidirectional Mendelian randomization approach. J Clin Endocrinol Metab. 2010 Jan;95(1):93-9. [CrossRef]
- Joseph, J.; Depp, C.; Martin, A.S.; Daly, R.E.; Glorioso, D.K.; Palmer, B.W.; Jeste, D.V. Associations of high sensitivity C-reactive protein levels in schizophrenia and comparison groups. Schizophr Res. 2015 Oct;168(1-2):456-60. [CrossRef]
- Van Dyne, A.; Wu, T.C.; Adamowicz, D.H.; Lee, E.E.; Tu, X.M.; Eyler, L.T. Longitudinal relationships between BMI and hs-CRP among people with schizophrenia. Schizophr Res. 2024 Sep;271:337-344. [CrossRef]
- McWhinney, S.R.; Brosch, K.; Calhoun, V.D.; Crespo-Facorro, B.; Crossley, N.A.; Dannlowski, U.; Dickie, E.; Dietze, L.M.F.; Donohoe, G.; Du Plessis, S.; Ehrlich, S.; Emsley, R.; Furstova, P.; Glahn, D.C.; Gonzalez-Valderrama, A.; Grotegerd, D.; Holleran, L.; Kircher, T.T.J.; Knytl, P.; Kolenic, M.; Lencer, R.; Nenadić, I.; Opel, N.; Pfarr, J.K.; Rodrigue, A.L.; Rootes-Murdy, K.; Ross, A.J.; Sim, K.; Škoch, A.; Spaniel, F.; Stein, F.; Švancer, P.; Tordesillas-Gutiérrez, D.; Undurraga, J.; Vázquez-Bourgon, J.; Voineskos, A.; Walton, E.; Weickert, T.W.; Weickert, C.S.; Thompson, P.M.; van Erp, T.G.M.; Turner, J.A.; Hajek, T. Obesity and brain structure in schizophrenia - ENIGMA study in 3021 individuals. Mol Psychiatry. 2022 Sep;27(9):3731-3737. Epub 2022 Jun 14. Erratum in: Mol Psychiatry. 2022 Sep;27(9):3738. doi: 10.1038/s41380-022-01696-3. Erratum in: Mol Psychiatry. 2024 Jan;29(1):56. [CrossRef]
- Nettis, M.A.; Pergola, G.; Kolliakou, A.; O'Connor, J.; Bonaccorso, S.; David, A.; Gaughran, F.; Di Forti, M.; Murray, R.M.; Marques, T.R.; Blasi, G.; Bertolino, A.; Pariante, C.M.; Dazzan, P.; Mondelli, V. Metabolic-inflammatory status as predictor of clinical outcome at 1-year follow-up in patients with first episode psychosis. Psychoneuroendocrinology. 2019 Jan;99:145-153. [CrossRef]
- Crump, C.; Winkleby, M.A.; Sundquist, K.; Sundquist, J. 2013. Comorbidities and mortality in persons with schizophrenia: a Swedish national cohort study. Am. J. Psychiatry 170(3),324–333. [CrossRef]
- Ratliff, J.C.; Palmese, L.B.; Reutenauer, E.L.; Srihari, V.H.; Tek, C. Obese schizophrenia spectrum patients have significantly higher 10-year general cardiovascular risk and vascular ages than obese individuals without severe mental illness. Psychosomatics. 2013 Jan-Feb;54(1):67-73. [CrossRef]
- Tsai, K.Y.; Lee, C.C.; Chou, Y.M.; Su, C.Y.; Chou, F.H. The incidence and relative risk of stroke in patients with schizophrenia: a five-year follow-up study. Schizophr Res. 2012 Jun;138(1):41-7. [CrossRef] [PubMed]
- Laursen, T.M.; Munk-Olsen, T.; Vestergaard, M. 2012. Life expectancy and cardio-vascular mortality in persons with schizophrenia. Curr.Opin.Psychiatry 25(2), 83–88. [CrossRef]
- Radhakrishnan, R.; Kaser, M.; Guloksuz, S. The Link Between the Immune System, Environment, and Psychosis. Schizophr Bull. 2017 Jul 1;43(4):693-697. [CrossRef]
- Mongan, D.; Ramesar, M.; Föcking, M.; Cannon, M.; Cotter, D. Role of inflammation in the pathogenesis of schizophrenia: A review of the evidence, proposed mechanisms and implications for treatment. Early Interv Psychiatry. 2020 Aug;14(4):385-397. [CrossRef]
- Miller, B.J.; Goldsmith, D.R. Evaluating the Hypothesis That Schizophrenia Is an Inflammatory Disorder. Focus (Am Psychiatr Publ). 2020 Oct;18(4):391-401. [CrossRef]
- Uchino, B.N. Social support and health: a review of physiological processes potentially underlying links to disease outcomes. J Behav Med. 2006 Aug;29(4):377-87. [CrossRef]
- McHugh Power, J.; Carney, S.; Hannigan, C.; Brennan, S.; Wolfe, H.; Lynch, M.; Kee, F.; Lawlor, B. Systemic inflammatory markers and sources of social support among older adults in the Memory Research Unit cohort. J Health Psychol. 2019 Mar;24(3):397-406. [CrossRef]
- Kiecolt-Glaser, J.K.; Gouin, J.P.; Hantsoo, L. Close relationships, inflammation, and health. Neurosci Biobehav Rev. 2010 Sep;35(1):33-8. [CrossRef]
- Hsiao, C.Y.; Lee, C.T.; Lu, H.L.; Tsai, Y.F. Living with schizophrenia: Health-related quality of life among primary family caregivers. J Clin Nurs. 2017;26(23–24):5151–9. [CrossRef]
- Chronister, J.; Fitzgerald, S.; Chou, C.C. The meaning of social support for persons with serious mental illness: A family member perspective. Rehabil Psychol. 2021 Feb;66(1):87-101. [CrossRef]
- Mueser, K.T.; Deavers, F.; Penn, D.L.; Cassisi, J.E. Psychosocial treatments for schizophrenia. Annu Rev Clin Psychol. 2013;9:465-97. [CrossRef]
- Verbiest, I.; Michels, N.; Tanghe, A.; Braet, C. Inflammation in obese children and adolescents: Association with psychosocial stress variables and effects of a lifestyle intervention. Brain Behav Immun. 2021 Nov;98:40-47. [CrossRef]
- O'Brien, J.R.; Loi, E.C.; Byrne, M.L.; Zalewski, M.; Casement, M.D. The Link Between Positive and Negative Parenting Behaviors and Child Inflammation: A Systematic Review. Child Psychiatry Hum Dev. 2023 Feb;54(1):51-65. [CrossRef]
- Diener, M.J.; Geenen, R.; Koelen, J.A.; Aarts, F.; Gerdes, V.E.; Brandjes, D.P.; Hinnen, C. (2016). The significance of attachment quality for obesity: A meta-analytic review. Canadian Journal of Behavioural Science, 48(4), 255. [CrossRef]
- Bernard, K.; Hostinar, C.E.; Dozier, M. Longitudinal associations between attachment quality in infancy, C-reactive protein in early childhood, and BMI in middle childhood: preliminary evidence from a CPS-referred sample. Attach Hum Dev. 2019 Feb;21(1):5-22. [CrossRef]
- Aas, M.; Dieset, I.; Hope, S.; Hoseth, E.; Mørch, R.; Reponen, E.; Steen, N.E.; Laskemoen, J.F.; Ueland, T.; Aukrust, P.; Agartz, I.; Andreassen, O.A.; Melle, I. Childhood maltreatment severity is associated with elevated C-reactive protein and body mass index in adults with schizophrenia and bipolar diagnoses. Brain Behav Immun. 2017 Oct;65:342-349. [CrossRef]
- Peritogiannis, V.; Ninou, A.; Samakouri, M. Mortality in Schizophrenia-Spectrum Disorders: Recent Advances in Understanding and Management. Healthcare (Basel). 2022 Nov 25;10(12):2366. [CrossRef]
- Yung, N.C.L.; Wong, C.S.M.; Chan, J.K.N.; Chen, E.Y.H.; Chang, W.C. Excess Mortality and Life-Years Lost in People With Schizophrenia and Other Non-affective Psychoses: An 11-Year Population-Based Cohort Study. Schizophr Bull. 2021 Mar 16;47(2):474-484. [CrossRef]
- Sicras-Mainar, A.; Rejas-Gutiérrez, J.; Navarro-Artieda, R.; Blanca-Tamayo, M. C-reactive protein as a marker of cardiovascular disease in patients with a schizophrenia spectrum disorder treated in routine medical practice. Eur Psychiatry. 2013 Mar;28(3):161-7. [CrossRef]
- Kelly, C.; McEvoy, J.P.; Miller, B.J. Total and differential white blood cell counts, inflammatory markers, adipokines, and incident metabolic syndrome in phase 1 of the clinical antipsychotic trials of intervention effectiveness study, (Schizophr. Res. 209 (2019) 193–197. [CrossRef]
- Mori, N.; McEvoy, J.P.; Miller, B.J. Total and differential white blood cell counts, inflammatory markers, adipokines, and the metabolic syndrome in phase 1 of the clinical antipsychotic trials of intervention effectiveness study, (Schizophr. Res. 169 (2015) 30–76. [CrossRef]
- Boyer, L.; Richieri, R.; Dassa, D.; Boucekine, M.; Fernandez, J.; Vaillant, R.; Padovani, R.; Auquier, P.; Lancon, C. Association of metabolic syndrome and inflammation with neurocognition in patients with schizophrenia, (Psychiatry Res. 210 (2013) 381– 386. [CrossRef]
- Osimo, E.F.; Perry, B.I.; Cardinal, R.N.; Lynall, M.E.; Lewis, J.; Kudchadkar, A.; Murray, G.K.; Perez, J.; Jones, P.B.; Khandaker, G.M. Inflammatory and cardiometabolic markers at presentation with first episode psychosis and long-term clinical outcomes: A longitudinal study using electronic health records. Brain Behav Immun. 2021 Jan;91:117-127. [CrossRef]
- Sarandol, E.; Sarandol, A.; Mercan, S.; Eker, S.S.; Surmen-Gur, E. Antipsychotic-Treated Schizophrenia Patients Develop Inflammatory and Oxidative Responses Independently From Obesity: However, Metabolic Disturbances Arise From Schizophrenia-Related Obesity. Hum Psychopharmacol. 2024 Nov;39(6):e2913. [CrossRef]
- Solmi, F.; Mascarell, M.C.; Zammit, S.; Kirkbride, J.B.; Lewis, G. Polygenic risk for schizophrenia, disordered eating behaviours and body mass index in adolescents. Br J Psychiatry. 2019 Jul;215(1):428-433. [CrossRef]
- Khosravi, M. Biopsychosocial factors associated with disordered eating behaviors in schizophrenia. Ann Gen Psychiatry 19, 67 (2020). [CrossRef]
- Tuncer, G.Z.; Çetinkaya Duman, Z. An examination of emotional eating behavior in individuals with a severe mental disorder. Arch Psychiatr Nurs. 2020 Dec;34(6):531-536. [CrossRef]
- Kouidrat, Y.; Amad, A.; Stubbs, B.; Louhou, R.; Renard, N.; Diouf, M.; Lalau, J.D.; Loas, G. Disordered eating behaviors as a potential obesogenic factor in schizophrenia. Psychiatry Res. 2018 Nov;269:450-454. [CrossRef]
- Tsofliou, F.; Casey, C.; Hughes, C. (2023). Stress and Disordered Eating Patterns. In: Patel, V.B., Preedy, V.R. (eds) Eating Disorders. Springer, Cham. [CrossRef]
- Prabhakaran, S.; Nagarajan, P.; Varadharajan, N.; et al. Relationship Between Quality of Life and Social Support Among Patients with Schizophrenia and Bipolar Disorder: A Cross-Sectional Study. J. Psychosoc. Rehabil. Ment. Health 8, 137–145 (2021). [CrossRef]
- Ospina, L.H.; Beck-Felts, K.; Ifrah, C.; Shagalow, S.; Lister, A.; Russo, S.J.; Gross, J.J.; Kimhy, D. Relationships among inflammation, social cognition, and social functioning in schizophrenia. Schizophr Res. 2022 Oct;248:366-367. [CrossRef]
- Carpentier, A.; Zampetas, D.; Durand, A.; Naassila, M.; Bralet, M.C. Relationships Between Immune-Inflammatory Features and Social Cognitive Impairments in Patients With Schizophrenia Spectrum Disorders: A Systematic Review. Brain Behav. 2025 Apr;15(4):e70384. [CrossRef]
- Lal, C.; Ul Haq, M.S.; Jaleel, F.A.; Jawed, D.N. Correlation Between Social Support, Patient Satisfaction, and Associated Factors in Patients with Schizophrenia. Cureus. 2025 Mar 26;17(3):e81222. [CrossRef]
- Palumbo, C.; Volpe, U.; Matanov, A.; Priebe, S.; Giacco, D. Social networks of patients with psychosis: a systematic review. BMC Res Notes. 2015 Oct 12;8:560. [CrossRef]
- Kang, H. Sample size determination and power analysis using the G*Power software. J Educ Eval Health Prof. 2021;18:17. [CrossRef]
- Yenipınar, A.; Koç, Ş.; Çanga, D.; Kaya, F. (2019). Determining Sample Size in Logistic Regression with G-Power. Black Sea Journal of Engineering and Science, 2(1), 16-22.
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon, R.O., 3rd; Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; Rifai, N.; Smith SCJr Taubert, K.; Tracy, R.P.; Vinicor, F.; Centers for Disease Control and Prevention; American Heart Association. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: A statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation. 2003 Jan 28;107(3):499-511. [CrossRef]
- Tselebis, A.; Anagnostopoulou, T.; Bratis, D.; Moulou, A.; Maria, A.; Sikaras, C.; Ilias, I.; Karkanias, A.; Moussas, G.; Tzanakis, N. The 13 item Family Support Scale: Reliability and validity of the Greek translation in a sample of Greek health care professionals. Asia Pac Fam Med. 2011 Apr 13;10(1):3. [CrossRef]
- Ilias, I.; Tselebis, A.; Theotoka, I.; Hatzimichelakis, E. Association of perceived family support through glycemic control in native Greek patients managing diabetes with diet alone. Ethn Dis. 2004 Winter;14(1):2. [PubMed]
- Tselebis, A.; Bratis, D.; Pachi, A.; Moussas, G.; Karkanias, A.; Harikiopoulou, M.; Theodorakopoulou, E.; Kosmas, E.; Ilias, I.; Siafakas, N.; Vgontzas, A.; Tzanakis, N. [Chronic obstructive pulmonary disease: sense of coherence and family support versus anxiety and depression]. Psychiatriki. 2013 Apr-Jun;24(2):109-16. Greek, Modern. [PubMed]
- Templeton, Gary F. (2011) "A Two-Step Approach for Transforming Continuous Variables to Normal: Implications and Recommendations for IS Research," Communications of the Association for Information Systems: Vol. 28, Article 4. Available online: http://aisel.aisnet.org/cais/vol28/iss1/4.
- Firdous, S. Correlation of CRP, fasting serum triglycerides and obesity as cardiovascular risk factors. J Coll Physicians Surg Pak. 2014 May;24(5):308-13. [PubMed]
- Wensveen, F.M.; Valentić, S.; Šestan, M.; Turk Wensveen, T.; Polić, B. The "Big Bang" in obese fat: Events initiating obesity-induced adipose tissue inflammation. Eur J Immunol. 2015 Sep;45(9):2446-56. [CrossRef]
- Festa, A.; D'Agostino, R., Jr.; Williams, K.; et al. The relation of body fat mass and distribution to markers of chronic inflammation. Int J Obes 25, 1407–1415 (2001). [CrossRef]
- Goldsmith, D.R.; Massa, N.; Miller, B.J.; Miller, A.H.; Duncan, E. The interaction of lipids and inflammatory markers predict negative symptom severity in patients with schizophrenia. NPJ Schizophr. 2021 Oct 20;7(1):50. [CrossRef]
- Park, H.S.; Park, J.Y.; Yu, R. Relationship of obesity and visceral adiposity with serum concentrations of CRP, TNF-alpha and IL-6. Diabetes Res. Clin. Pr. 69, 29–35 (2005). [CrossRef]
- Popa, C.; Netea, M.G.; van Riel, P.L.; van der Meer, J.W.; Stalenhoef, A.F. The role of TNF-alpha in chronic inflammatory conditions, intermediary metabolism, and cardiovascular risk. J. Lipid Res. 48, 751–762 (2007). [CrossRef]
- Correll, C.U.; Stanford, A.D.; Claxton, A.; Du, Y.; Weiden, P.J. (2018). Social and functional outcomes with two doses of aripiprazole lauroxil vs placebo in patients with schizophrenia: A post-hoc analysis of a 12-week phase 3 efficacy study. Psychiatry Research, 2019(274), 176–181. [CrossRef]
- El-Monshed, A.; Amr, M. Association between perceived social support and recovery among patients with schizophrenia, International Journal of Africa Nursing Sciences, Volume 13, 2020, 100236. [CrossRef]
- Cha, H.Y.; Yang, S.J.; Kim, S.W. Higher Dietary Inflammation in Patients with Schizophrenia: A Case-Control Study in Korea. Nutrients. 2021 Jun 13;13(6):2033. [CrossRef]
- Bigseth, T.T.; Engh, J.A.; Andersen, E.; Bang-Kittilsen, G.; Egeland, J.; Falk, R.S.; Holmen, T.L.; Mordal, J.; Nielsen, J.; Ueland, T.; Vang, T.; Fredriksen, M. Alterations in inflammatory markers after a 12-week exercise program in individuals with schizophrenia-a randomized controlled trial. Front Psychiatry. 2023 May 11;14:1175171. [CrossRef]
- Tang, P.Y.; Tee, S.F.; Su, K.P. Editorial: The link between nutrition and schizophrenia. Front Psychiatry. 2022 Nov 21;13:1074120. [CrossRef]
- Yang, Y.C.; Schorpp, K.; Harris, K.M. Social support, social strain and inflammation: evidence from a national longitudinal study of U.S. adults. Soc Sci Med. 2014 Apr;107:124-35. [CrossRef]
- Wee, C.C.; Mukamal, K.J.; Huang, A.; Davis, R.B.; McCarthy, E.P.; Mittleman, M.A. (2008). Obesity and C-reactive protein levels among white, black, and hispanic US adults. Obesity (Silver Spring, Md.), 16(4), 875–880. [CrossRef]
- Lear, S.A.; Chen, M.M.; Birmingham, C.L.; Frohlich, J.J. (2003). The relationship between simple anthropometric indices and C-reactive protein: ethnic and gender differences. Metabolism, 52(12), 1542-1546. [CrossRef]
- Fond, G.; Godin, O.; Llorca, P.M.; Leboyer, M. (2015). Abnormal C-reactive protein (CRP) levels in schizophrenia and schizoaffective disorders. Results from the FACE-SZ dataset. European Psychiatry, 30(S2), S112–S112. [CrossRef]
- Gough, M.; Godde, K. A multifaceted analysis of social stressors and chronic inflammation. SSM Popul Health. 2018 Sep 12;6:136-140. [CrossRef]
- Guevara, J.E.; Murdock, K.W. High social strain and physical health: Examining the roles of anxious arousal, body mass index, and inflammation. Psychoneuroendocrinology. 2019 Aug;106:155-160. [CrossRef]
- Uchino, B.N.; Trettevik, R.; Kent de Grey, R.G.; Cronan, S.; Hogan, J.; Baucom, B.R.W. Social support, social integration, and inflammatory cytokines: A meta-analysis. Health Psychol. 2018 May;37(5):462-471. [CrossRef]
- Lachman, M.E.; Schiloski, K.A. The psychosocial anti-inflammatories: Sense of control, purpose in life, and social support in relation to inflammation, functional health and chronic conditions in adulthood. J Psychosom Res. 2024 Dec;187:111957. [CrossRef]
- Misra, S.; Johnson, K.A.; Parnarouskis, L.M.; Koenen, K.C.; Williams, D.R.; Gelaye, B.; Borba, C.P.C. How Early Life Adversities Influence Later Life Family Interactions for Individuals with Schizophrenia in Outpatient Treatment: A Qualitative Analysis. Community Ment Health J. 2020 Aug;56(6):1188-1200. [CrossRef]
- Hurtado, M.M.; Villena, A.; Quemada, C.; Morales-Asencio, J.M. Personal relationships during and after an initial psychotic episode. First-person experiences. J Ment Health. 2024 Sep 28:1-7. [CrossRef]
- Fagundes, C.P.; Bennett, J.M.; Derry, H.M.; Kiecolt-Glaser, J.K. Relationships and Inflammation across the Lifespan: Social Developmental Pathways to Disease. Soc Personal Psychol Compass. 2011 Nov;5(11):891-903. [CrossRef]
- Aldersey, H.M.; Whitley, R. Family Influence in Recovery from Severe Mental Illness. Community Ment Health J 51, 467–476 (2015). [CrossRef]
- van de Vyver, M. Immunology of chronic low-grade inflammation: relationship with metabolic function. J Endocrinol. 2023 Feb 23;257(1):e220271. [CrossRef]
- Valdearcos, M.; Xu, A.W.; Koliwad, S.K. Hypothalamic inflammation in the control of metabolic function. Annu Rev Physiol. 2015;77:131-60. [CrossRef]
- Cani, P.D.; Amar, J.; Iglesias, M.A.; Poggi, M.; Knauf, C.; Bastelica, D.; Neyrinck, A.M.; Fava, F.; Tuohy, K.M.; Chabo, C.; Waget, A.; Delmée, E.; Cousin, B.; Sulpice, T.; Chamontin, B.; Ferrières, J.; Tanti, J.F.; Gibson, G.R.; Casteilla, L.; Delzenne, N.M.; Alessi, M.C.; Burcelin, R. Metabolic endotoxemia initiates obesity and insulin resistance. Diabetes. 2007 Jul;56(7):1761-72. [CrossRef]
- Khovidhunkit, W.; Kim, M.S.; Memon, R.A.; Shigenaga, J.K.; Moser, A.H.; Feingold, K.R.; Grunfeld, C. Effects of infection and inflammation on lipid and lipoprotein metabolism: mechanisms and consequences to the host. J Lipid Res. 2004 Jul;45(7):1169-96. [CrossRef]
- Huet, L.; Delgado, I.; Dexpert, S.; Sauvant, J.; Aouizerate, B.; Beau, C.; Forestier, D.; Ledaguenel, P.; Magne, E.; Capuron, L. Relationship between body mass index and neuropsychiatric symptoms: Evidence and inflammatory correlates. Brain Behav Immun. 2021 May;94:104-110. [CrossRef]
- Sugai, T.; Suzuki, Y.; Yamazaki, M.; Shimoda, K.; Mori, T.; Ozeki, Y.; Matsuda, H.; Sugawara, N.; Yasui-Furukori, N.; Minami, Y.; Okamoto, K.; Sagae, T.; Someya, T. High Prevalence of Obesity, Hypertension, Hyperlipidemia, and Diabetes Mellitus in Japanese Outpatients with Schizophrenia: A Nationwide Survey. PLoS One. 2016 Nov 17;11(11):e0166429. [CrossRef]
- Catapano, L.; Castle, D. (2004). Obesity in schizophrenia: what can be done about it?. Australasian psychiatry: bulletin of Royal Australian and New Zealand College of Psychiatrists, 12(1), 23–25. [CrossRef]
- Bobes, J. (2007). Schizophrenia and overweight/obesity: Pathophysiology and medical consequences. European Psychiatry, 22(S1), S94–S94. [CrossRef]
- Chen, J.; Perera, G.; Shetty, H.; Broadbent, M.; Xu, Y.; Stewart, R. Body mass index and mortality in patients with schizophrenia spectrum disorders: a cohort study in a South London catchment area: General Psychiatry 2022;35:e100819.
- Arango, C.; Bobes, J.; Kirkpatrick, B.; Garcia-Garcia, M.; Rejas, J. Psychopathology, coronary heart disease and metabolic syndrome in schizophrenia spectrum patients with deficit versus non-deficit schizophrenia: findings from the CLAMORS study. Eur Neuropsychopharmacol. 2011 Dec;21(12):867-75. [CrossRef]
- Palmese, L.B.; DeGeorge, P.C.; Ratliff, J.C.; Srihari, V.H.; Wexler, B.E.; Krystal, A.D.; Tek, C. Insomnia is frequent in schizophrenia and associated with night eating and obesity. Schizophr Res. 2011 Dec;133(1-3):238-43. [CrossRef]
- Kolotkin, R.L.; Corey-Lisle, P.K.; Crosby, R.D.; Swanson, J.M.; Tuomari, A.V.; L'italien, G.J.; Mitchell, J.E. Impact of obesity on health-related quality of life in schizophrenia and bipolar disorder. Obesity (Silver Spring). 2008 Apr;16(4):749-54. [CrossRef]
- Storch Jakobsen, A.; Speyer, H.; Nørgaard, H.C.B.; Hjorthøj, C.; Krogh, J.; Mors, O.; Nordentoft, M. Associations between clinical and psychosocial factors and metabolic and cardiovascular risk factors in overweight patients with schizophrenia spectrum disorders - Baseline and two-years findings from the CHANGE trial. Schizophr Res. 2018 Sep;199:96-102. [CrossRef]
- Yong, N.; Pan, J.; Li, X.; Yu, L.; Hou, X. Influencing factors of obesity in community patients with deficit schizophrenia: a cross-sectional study. Eur J Med Res. 2022 Jun 11;27(1):90. [CrossRef]
- Kim, M.; Yang, S.J.; Kim, H.H.; Jo, A.; Jhon, M.; Lee, J.Y.; Ryu, S.H.; Kim, J.M.; Kweon, Y.R.; Kim, S.W. Effects of Dietary Habits on General and Abdominal Obesity in Community-dwelling Patients with Schizophrenia. Clin Psychopharmacol Neurosci. 2023 Feb 28;21(1):68-76. [CrossRef]
- Lundgren, J.D.; Rempfer, M.V.; Brown, C.E.; Goetz, J.; Hamera, E. The prevalence of night eating syndrome and binge eating disorder among overweight and obese individuals with serious mental illness. Psychiatry Res. 2010 Feb 28;175(3):233-6. [CrossRef]
- Anzengruber, D.; Klump, K.L.; Thornton, L.; Brandt, H.; Crawford, S.; Fichter, M.M.; Halmi, K.A.; Johnson, C.; Kaplan, A.S.; LaVia, M.; Mitchell, J.; Strober, M.; Woodside, D.B.; Rotondo, A.; Berrettini, W.H.; Kaye, W.H.; Bulik, C.M. Smoking in eating disorders. Eat Behav. 2006 Nov;7(4):291-9. [CrossRef]
- García-Mayor, R.V.; García-Soidán, F.J. Eating disoders in type 2 diabetic people: Brief review. Diabetes Metab Syndr. 2017 Jul-Sep;11(3):221-224. [CrossRef]
- Sankaranarayanan, A.; Johnson, K.; Mammen, S.J.; Wilding, H.E.; Vasani, D.; Murali, V.; Mitchison, D.; Castle, D.J.; Hay, P. Disordered Eating among People with Schizophrenia Spectrum Disorders: A Systematic Review. Nutrients. 2021 Oct 27;13(11):3820. [CrossRef]
- Tselebis, A.; Pachi, A. Primary Mental Health Care in a New Era. Healthcare (Basel). 2022 Oct 14;10(10):2025. [CrossRef]
- Cooper SJ, Reynolds GP; With expert co-authors (in alphabetical order):; Barnes T, England E, Haddad PM, Heald A, Holt R, Lingford-Hughes A, Osborn D, McGowan O, Patel MX, Paton C, Reid P, Shiers D, Smith J. BAP guidelines on the management of weight gain, metabolic disturbances and cardiovascular risk associated with psychosis and antipsychotic drug treatment. J Psychopharmacol. 2016 Aug;30(8):717-48. [CrossRef]
- DeJongh, B.M. Clinical pearls for the monitoring and treatment of antipsychotic induced metabolic syndrome. Ment Health Clin. 2021 Nov 8;11(6):311-319. https://doi.org/10.9740/mhc.2021.11.311. [CrossRef]
- Fernández-Abascal, B.; Suárez-Pinilla, P.; Cobo-Corrales, C.; Crespo-Facorro, B.; Suárez-Pinilla, M. (2021). In- and outpatient lifestyle interventions on diet and exercise and their effect on physical and psychological health: a systematic review and meta-analysis of randomised controlled trials in patients with schizophrenia spectrum disorders and first episode of psychosis. Neuroscience and biobehavioral reviews, 125, 535–568. [CrossRef]
- Mucheru, D.; Hanlon, M.C.; McEvoy, M.; Thakkinstian, A.; MacDonald-Wicks, L. (2019). Comparative efficacy of lifestyle intervention strategies targeting weight outcomes in people with psychosis: a systematic review and network meta-analysis. JBI database of systematic reviews and implementation reports, 17(9), 1770–1825. [CrossRef]
- Fernández-Abascal, B.; Suárez-Pinilla, M.; Cobo-Corrales, C.; Crespo-Facorro, B.; Suárez-Pinilla, P. (2023). Lifestyle intervention based on exercise and behavioural counselling and its effect on physical and psychological health in outpatients with schizophrenia spectrum disorders. An exploratory, pragmatic randomized clinical trial. Schizophrenia research, 261, 256–268. [CrossRef]
- Naylor, A.; Flood, A.; Keegan, R. (2024). The effectiveness of physical activity interventions that include both physical activity and psychosocial strategies in people living with a severe mental illness: a systematic review and meta-analysis. International Review of Sport and Exercise Psychology, 1–31. [CrossRef]
- Hahlweg, K.; Baucom, D.H. (2023). Family therapy for persons with schizophrenia: neglected yet important. European archives of psychiatry and clinical neuroscience, 273(4), 819–824. [CrossRef]
- Caqueo-Urízar, A.; Rus-Calafell, M.; Urzúa, A.; Escudero, J.; Gutiérrez-Maldonado, J. The role of family therapy in the management of schizophrenia: challenges and solutions. Neuropsychiatr Dis Treat. 2015 Jan 14;11:145-51. [CrossRef]
- Burbach, F.R. (2018). Family therapy and schizophrenia: a brief theoretical overview and a framework for clinical practice. BJPsych Advances, 24(4), 225–234. [CrossRef]
Figure 1.
CRP values across the different BMI categories.
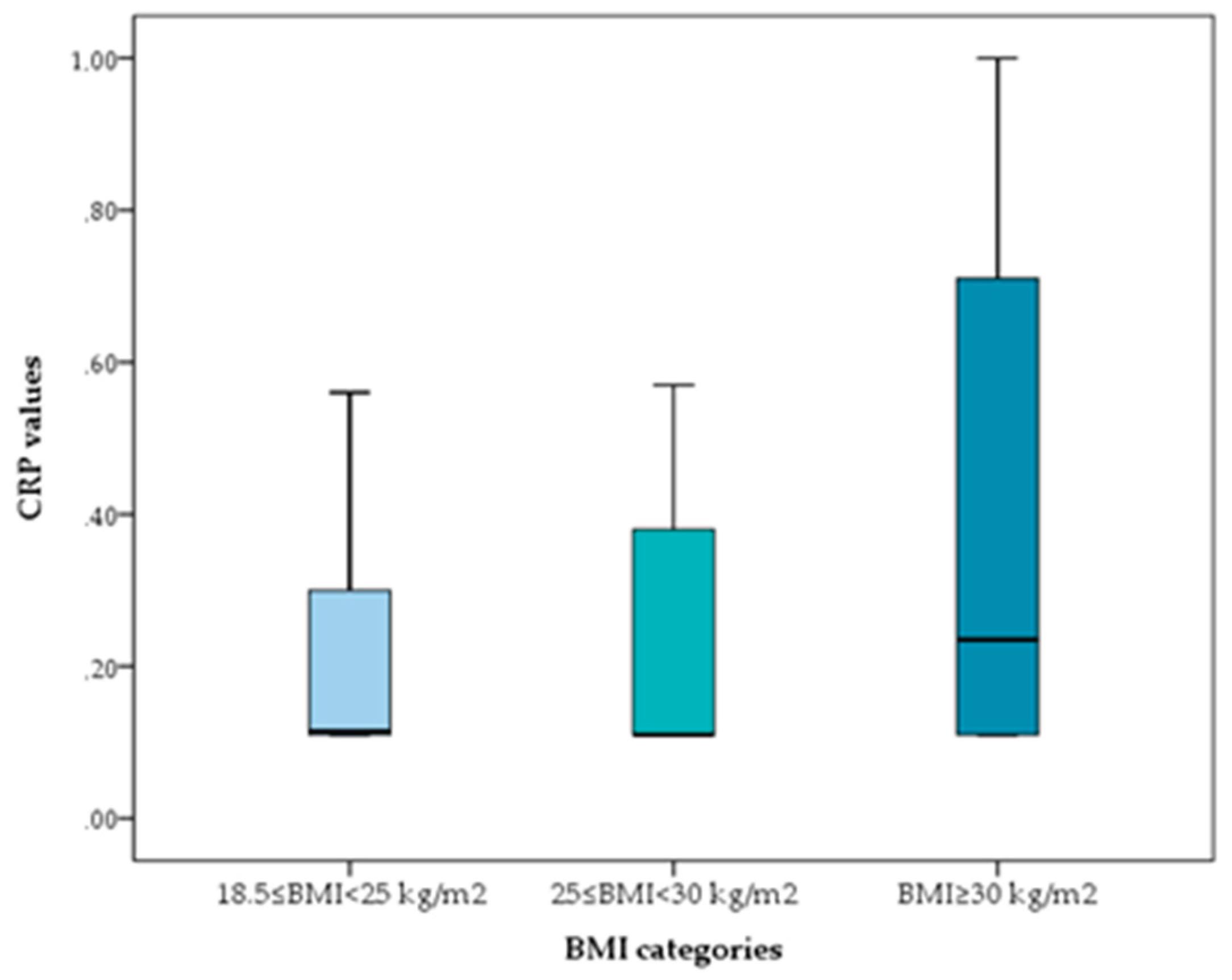
Figure 2.
Simple slopes indicating the interaction of the moderation analysis.
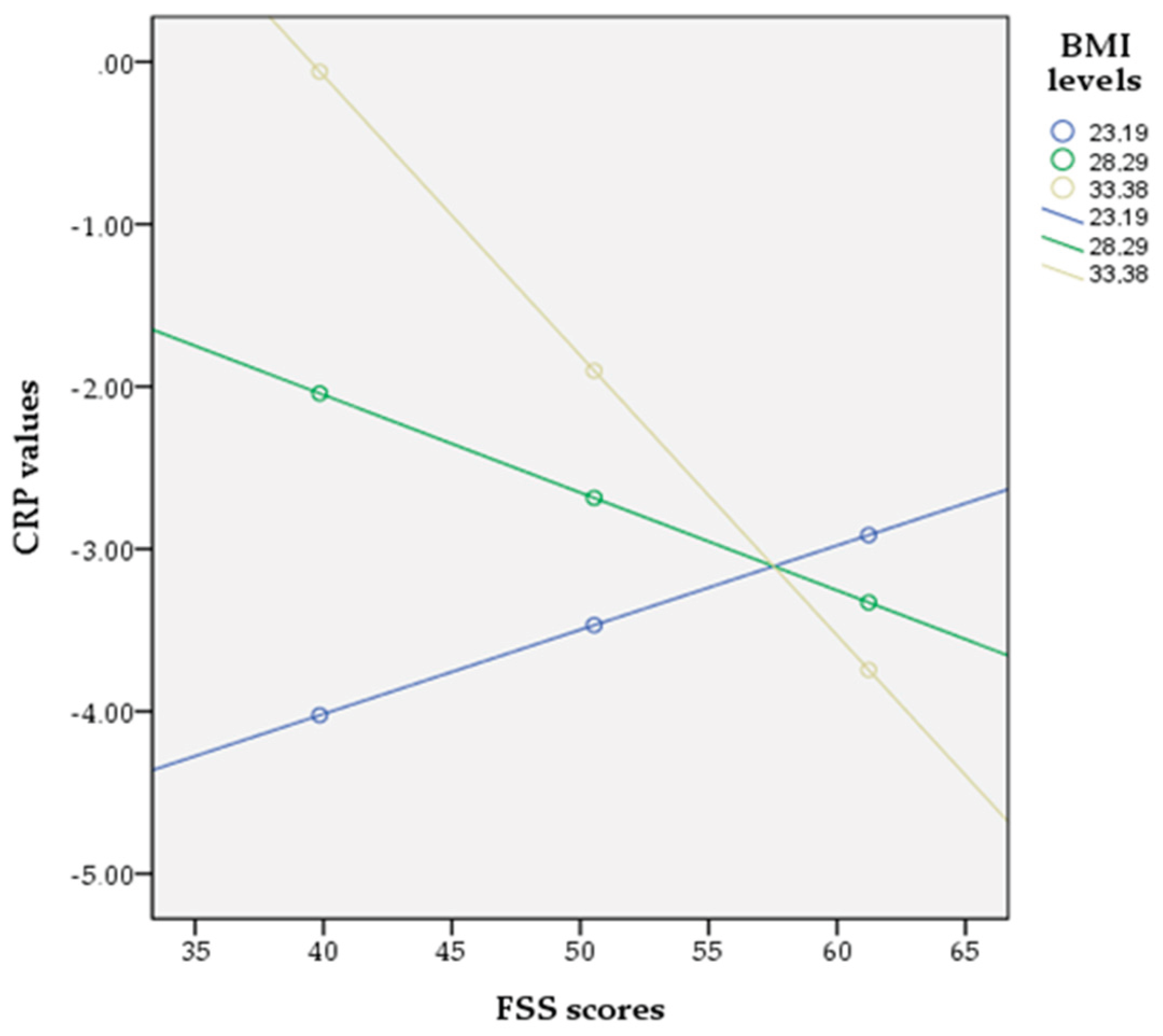
Figure 3.
Line graph of interaction between family support and BMI as predictors of the probability of having positive CRP.
Figure 3.
Line graph of interaction between family support and BMI as predictors of the probability of having positive CRP.
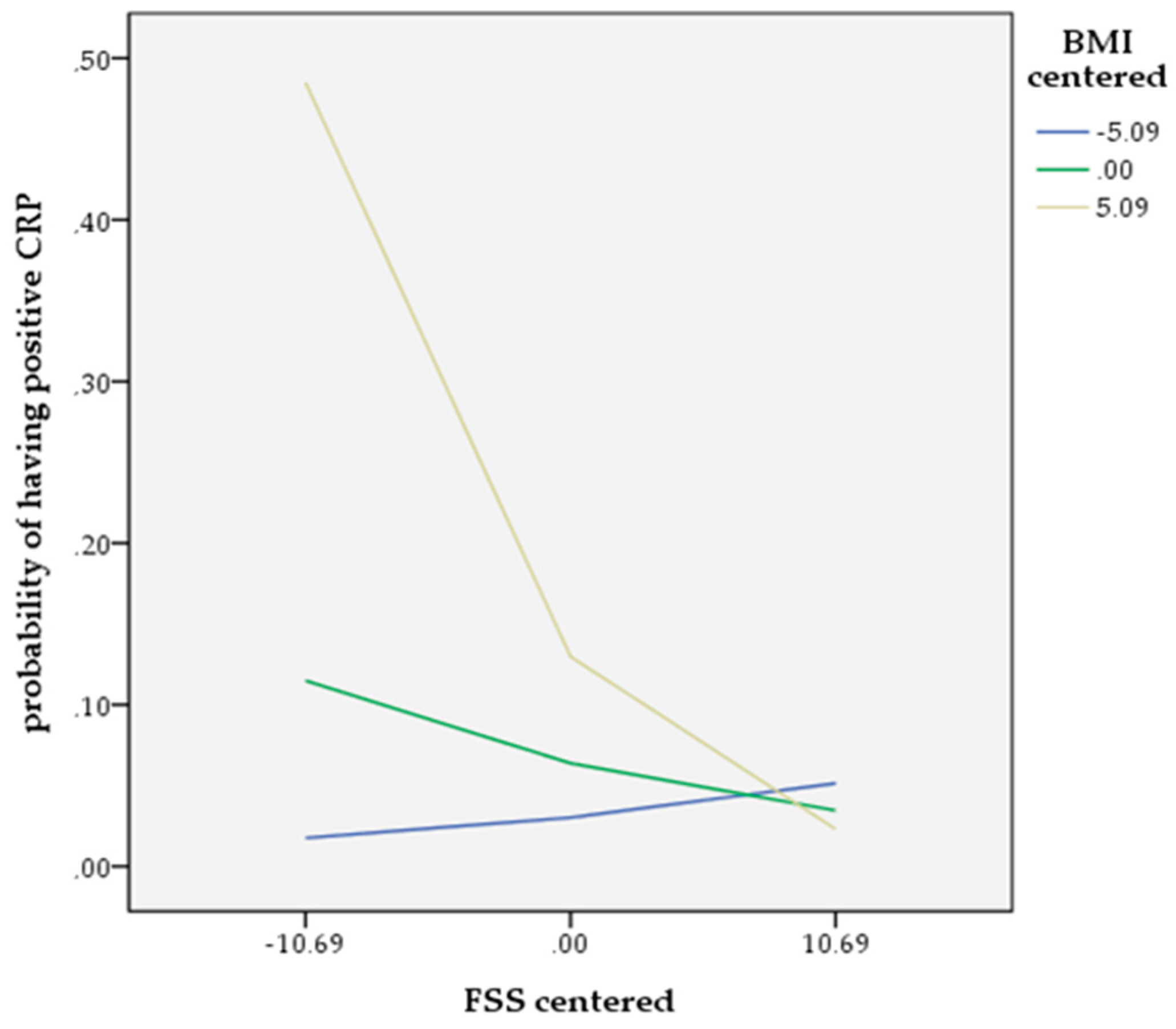

Table 1.
Descriptive statistics of participants.
| Gender | Age | Illnessduration(in years) | BMI(kg/m2) | Family Support Scale (FSS) | CRP(mg/dl) | |||
|---|---|---|---|---|---|---|---|---|
| Male | Mean | 41.36* | 14.44 | 29.24 | 51.03 | Median | 0.17 | |
| N | 100 | 80 | 90 | 82 | N | 94 | ||
| S.D. | 10.79 | 11.01 | 4.22 | 10.62 | IQR | 0.30 | ||
| Female | Mean | 44.98* | 14.90 | 28.44 | 48.83 | Median | 0.19 | |
| N | 106 | 80 | 88 | 88 | N | 88 | ||
| S.D. | 14.37 | 10.01 | 5.44 | 10.23 | IQR | 0.41 | ||
| Total | Mean | 43.22 | 13.98 | 28.85 | 49.89 | Median | 0.17 | |
| N | 206 | 160 | 178 | 170 | N | 182 | ||
| S. D. | 12.85 | 11.97 | 4.86 | 10.45 | IQR | 0.39 | ||
| * t test p<0.05; IQR: interquartile rangeNotes: For illness duration, BMI & FSS the means from the Two-Step transformation are presented | ||||||||
Table 2.
Correlations among Age, Illness duration, BMI, and FSS.
| Pearson CorrelationN: 206 | Age | Illness duration(in years) | BMI(kg/m2) | |
|---|---|---|---|---|
| Illness duration(in years) | r | 0.659** | ||
| p | 0.000 | |||
| BMI(kg/m2) | r | 0.240** | 0.315** | |
| p | 0.001 | 0.000 | ||
| Family Support Scale (FSS) | r | -0.151 | -0.250 | -0.125 |
| p | 0.050 | 0.004 | 0.132 | |
* Pearson Correlations p < 0.05, ** Pearson Correlations p < 0.01.
Table 3.
Correlations among CRP, Age, Illness duration, BMI and FSS.
| Spearman’s rhoN: 206 | Age | Illness duration(in years) | BMI(kg/m2) | Family Support Scale (FSS) | |
|---|---|---|---|---|---|
| CRP | rho | 0.140 | 0.038 | 0.213** | -0.510** |
| p | 0.060 | 0.638 | 0.005 | 0.000 | |
* Spearman’s rho Correlations p < 0.05, ** Spearman’s rho Correlations p < 0.01.
Table 4.
Unadjusted OR values from univariable binary logistic regression analysis.
| Dependent Variables: | Predictor | B | SE | Wald | p | OR (95% CL) |
|---|---|---|---|---|---|---|
| CRP values ≥0.11mg/dl | ObesityBMI≥30 kg/m2 | 0.683 | 0.321 | 4.534 | 0.033* | 1.980 (1.056, 3.713) |
| CRP values >0.6mg/dl | 3.326 | 0.758 | 19.262 | 0.000** | 27.818 (6.300, 122.838) | |
| Notes: B = logistic regression coefficient;Correlations are statistically significant at the *p < 0.05, ** p <0.01 level. | ||||||
Table 5.
Binary logistic regression analysis.
| Dependent Variable: CRP values >0.6mg/dl | B | SE | Wald | p | OR [95% CL] |
|---|---|---|---|---|---|
| Age | -0.047 | 0.049 | 0.923 | 0.337 | 0.954 [0.866, 1.051] |
| Gender | 0.552 | 0.616 | 0.805 | 0.370 | 1.738 [0.520, 5.811] |
| Illness duration | 0.088 | 0.052 | 2.817 | 0.093 | 1.092 [0.985, 1.210] |
| BMI | 0.158 | 0.068 | 5.396 | 0.020* | 1.171 [1.025, 1.337] |
| FSS | -0.090 | 0.037 | 6.086 | 0.014* | 0.914 [0.850, 0.982] |
| Notes: B = logistic regression coefficient;Correlations are statistically significant at the *p < 0.05, ** p <0.01 level. | |||||
Table 6.
Moderated binary logistic regression analysis.
| Dependent Variable: CRP values >0.6mg/dl | B | SE | Wald | p | Exp(B) [LLCL, ULCI] |
|---|---|---|---|---|---|
| Constant | -34.5617 | 15.2349 | 5.1465 | 0.0233 | |
| FSS | 0.5624 | 0.2951 | 3.6332 | 0.0566 | 1.7548 [-0.0159, 1.1408] |
| Moderator (BMI) | 1.2664 | 0.5257 | 5.8028 | 0.0160* | 3.5480 [0.2360, 2.2967] |
| Interaction (FSS*BMI) | -0.0220 | 0.0100 | 4.8079 | 0.0283* | 0.9782 [-0.0417, -0.0023] |
| Covariates | |||||
| Age | -0.0687 | 0.0567 | 1.4648 | 0.2261 | 0.9336 [-0.1799, 0.0425] |
| Gender | 0.4568 | 0.6779 | 0.4541 | 0.5004 | 1.5790 [-0.8719, 1.7856] |
| Illness duration | 0.0897 | 0.0597 | 2.2570 | 0.1330 | 1.0938 [-0.0273, 0.2067] |
| Notes: B = logistic regression coefficient;Correlations are statistically significant at the *p < 0.05, ** p <0.01 level. | |||||
Table 7.
Conditional effects of FSS at different levels of BMI.
| BMI level | Effect of FSS on having positiveCRP values | SE | z | Wald | p | [95% CL] |
|---|---|---|---|---|---|---|
| Low (-1SD): 23.1927 | 0.0519 | 0.0709 | 0.7323 | 0.5362 | 0.4640 | [-0.0870, 0.1908] |
| Mean: 28.2865 | -0.0602 | 0.0390 | -1.5428 | 2.3802 | 0.1229 | [-0.1368, 0.0163] |
| High (+1SD): 33.3803 | -0.1724 | 0.0571 | -3.0197 | 9.1185 | 0.0025* | [-0.2842, -0.0605] |
| Notes: Correlations are statistically significant at the *p < 0.05, ** p <0.01 level. | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



