Submitted:
13 June 2025
Posted:
16 June 2025
You are already at the latest version
Abstract
Background/Objectives: Post-stroke cognitive impairment significantly impacts long-term functional outcomes, particularly in instrumental activities of daily living (IADLs). Working memory training (WMT) has emerged as a potential cognitive rehabilitation strategy; however, its transfer to real-world functionality remains unclear. This study evaluated whether adaptive computerized WMT enhances IADL performance compared to a non-adaptive control condition in chronic stroke survivors. Methods: A single-blind, randomized controlled trial was conducted with 50 adults aged 50–79 years, ≥12 months post-ischemic stroke, diagnosed with mild neurocognitive disorder. Participants were randomized to adaptive WMT or non-adaptive cognitive training, each completing 25 home-based sessions over 12 weeks via a standardized online platform. Primary outcomes included the Lawton and Brody IADL Scale and the Working Memory Questionnaire (WMQ); secondary outcomes included the Working Memory Index (WMI) from the WAIS-IV. Analyses included frequentist and Bayesian methods. Results: Both groups showed significant pre–post improvements in IADL independence and WMI (p < .05; BF₁₀ > 10), with no significant between-group differences on overall IADL outcomes. The adaptive WMT group demonstrated specific gains in WMQ-Storing (p = 0.033; BF₁₀ = 3.83), while the control group improved in WMQ-Attention and IADL-Assistance Required (p = 0.004–0.035; BF₁₀ > 6). Bayesian ANOVA indicated that these effects were primarily driven by the interventions, with minimal influence from depressive symptoms or global cognition. Conclusions: Adaptive WMT yielded domain-specific cognitive benefits but did not enhance IADL performance beyond non-adaptive training. These findings highlight the limited far-transfer of WMT and the importance of designing ecologically valid, multimodal rehabilitation strategies post-stroke.
Keywords:
Stroke
; Functional Independence
; Working memory training
; Randomized Controlled Trial
; Neuroplasticity.
1. Introduction
As of 2021, an estimated 93.8 million individuals worldwide live with the consequences of stroke, corresponding to a crude prevalence rate of 1189 per 100,000 people, with nearly equal distribution between men and women and 65% of survivors being under the age of 70 [1,2]. Cognitive impairment affects approximately two-thirds to three-quarters of stroke survivors, compromising not only basic activities of daily living (ADLs) but also instrumental activities of daily living (IADLs) such as managing finances, shopping, preparing meals, and handling household tasks. A systematic review and meta-analysis reported a medium association (r = 0.37) between cognitive deficits and limitations in daily functioning, underscoring that impairments in attention, memory, language, and executive functions contribute significantly to long-term disability [3,4].
IADLs serve as critical indicators of functional independence, quality of life, and social participation [5]. Persistent difficulties in IADL performance—documented from three months up to 11 years post-stroke—highlight the need for routine cognitive assessments to enable early detection and personalized rehabilitation strategies [6,7,8,9]. In this context, working memory has emerged as a pivotal cognitive function [10]. A recent study demonstrated that lower working memory capacity, measured by Forward Digit Span (FDS) and Backward Digit Span (BDS), is significantly correlated with greater IADLs dependency (p = 0.005 for FDS; p = 0.010 for BDS). Moreover, survivors without cognitive impairment exhibited markedly lower IADLs scores (0.38 ± 1.071) compared to those with impairment (5.41 ± 5.06, p = 0.001) [11]. Complementing these findings, another study underscored that working memory is essential for maintaining and manipulating information—a process fundamental to functional recovery [12]. Thus, early cognitive screening and targeted interventions aimed at enhancing working memory are imperative for improving IADLs performance, promoting independence, and optimizing long-term rehabilitation outcomes.
Research on working memory training (WMT) in stroke rehabilitation has produced mixed findings, with some studies reporting cognitive improvements but limited evidence supporting gains in IADLs. A systematic review examined cognitive rehabilitation for post-stroke attention deficits and found that while divided attention showed moderate short-term improvements (SMD = 0.67, p < 0.0001), no significant long-term effects were observed on global cognitive function (SMD = 0.16, p = 0.41; n = 99) or functional independence [13,14]. Similarly, a pilot study demonstrated statistically significant improvements in working memory scores after computerized WMT, but these gains did not translate into broader cognitive or functional benefits [15].
Despite evidence supporting near-transfer effects, the far-transfer of cognitive gains to real-world IADLs performance remains unsubstantiated. A systematic review by van de Ven et al. (2016) found that while WMT improved tasks similar to training, there was no evidence of functional gains in everyday activities [16]. Importantly, when active control groups were used, no significant differences emerged in IADLs outcomes. Additionally, a Cochrane review by Das Nair et al. (2016) found small, short-term improvements in self-reported memory function (SMD = 0.36, p = 0.01) but no long-term effects on IADLs, mood, or quality of life, suggesting that observed benefits may be temporary or task-specific [17].
Several methodological limitations undermine the generalizability of these findings. Many studies had small sample sizes (e.g., Westerberg et al., n = 20), lacked active control conditions, and failed to conduct long-term follow-ups. Additionally, most studies relied on laboratory-based cognitive assessments rather than ecologically valid IADL measures, limiting their clinical applicability [16]. These limitations highlight the critical need for robust randomized controlled trials (RCTs) with extended follow-ups, larger samples, and validated functional outcome measures to determine whether WMT can contribute meaningfully to post-stroke rehabilitation.
The theoretical foundation for WMT in stroke rehabilitation is anchored in neuroplasticity, cognitive training models, and the challenge of transfer effects. Neuroplasticity, the capacity of the brain to reorganize itself by forming new neural connections, underlies cognitive training interventions [18]. Empirical evidence demonstrates that WMT can induce task-specific changes in functional connectivity, particularly within frontoparietal networks implicated in executive function [19]. However, while localized neural adaptations occur, the extent to which these modifications translate to functional independence in daily life remains debated [20]. IADLs such as medication management, financial decision-making, and meal preparation, demand the coordinated integration of multiple cognitive and motor domains [21]. While working memory is crucial for maintaining and manipulating information during complex tasks, IADLs performance also requires intact problem-solving, motor sequencing, and adaptive decision-making [22]. Evidence suggests that improving isolated cognitive functions does not necessarily lead to gains in real-world functional outcomes, as IADLs depend on domain-general cognitive integration rather than single-domain improvements.
A fundamental limitation in WMT research is the challenge of achieving far-transfer effects, in which cognitive improvements extend beyond the trained task to real-world activities. The ecological validity of traditional WMT paradigms is often limited, as training exercises are decontextualized from everyday challenges [23]. Furthermore, stroke survivors exhibit substantial interindividual variability in baseline cognitive reserve, lesion location, and rehabilitation engagement, affecting training efficacy and transfer potential [24]. Given these constraints, emerging mechanistic models advocate for hybrid interventions combining WMT with real-world functional training to enhance IADLs performance [25]. Studies should focus on designing ecologically valid, multimodal rehabilitation strategies that leverage both cognitive and motor learning principles to optimize post-stroke functional recovery.
The efficacy of WMT in improving functional independence after stroke remains an unresolved question in cognitive rehabilitation research. While prior studies have demonstrated near-transfer effects—where cognitive gains are confined to tasks closely resembling training—the evidence for far-transfer to IADLs is inconsistent and methodologically limited. Given that IADLs require the integration of multiple cognitive and motor domains, the assumption that isolated working memory improvements will generalize to complex real-world tasks remains empirically unverified. Moreover, many existing studies suffer from small sample sizes, inadequate control conditions, and a reliance on laboratory-based cognitive measures with limited ecological validity. Addressing these limitations is imperative to refine rehabilitation strategies and optimize post-stroke functional recovery.
This study employs a rigorously designed randomized controlled trial (RCT) with an active control group, ensuring that observed effects are attributable to WMT rather than nonspecific training factors. Standardized, ecologically valid IADLs assessments will be used to evaluate real-world functional outcomes, with a longitudinal follow-up to assess the persistence of potential benefits.
We hypothesize that, while WMT may enhance task-specific cognitive performance, it will not produce significant improvements in IADL functioning compared to standard rehabilitation. This study will provide critical empirical evidence to determine the translational value of WMT and inform the development of targeted interventions that effectively promote functional independence in stroke survivors.
2. Materials and Methods
Study Design
This study employed a single-blind, RCT design comprising two parallel arms: an experimental group receiving working memory training and an active control group. Randomization was performed using a computer-generated sequence by an independent statistician prior to participant enrollment. Allocation was concealed until completion of the baseline assessments to mitigate selection and performance biases. Outcome evaluators were blinded to group assignment and pre-intervention data to ensure objectivity in data collection.
Participants
Participants were recruited from the Instituto Neurológico de Colombia between October 2021 and November 2023. A total of 1,343 stroke survivors were referred by treating clinicians. After applying the inclusion and exclusion criteria, 50 participants were randomized into the trial (see Figure 1 for the CONSORT flow diagram). All participants provided written informed consent, and the study received ethical approval from the institutional review board (Approval Code: 449011-19.02-013).
Inclusion criteria were as follows: (1) age between 50 and 79 years old; (2) history of a first-ever ischemic stroke confirmed via computed tomography (CT) or functional magnetic resonance imaging (fMRI); (3) stroke onset ≥12 months prior to enrollment; (4) minimum completion of primary education; and (5) fulfillment of DSM-5 criteria for mild neurocognitive disorder, operationalized using the Montreal Cognitive Assessment (MoCA), with cutoffs adjusted for educational attainment (scores of 21–22 for 5–10 years of education, and 23–24 for ≥11 years).
Additional eligibility requirements included access to a computer with a stable internet connection, availability of a primary caregiver during online sessions, and no concurrent participation in formal cognitive or physical rehabilitation programs. Exclusion criteria included: (1) significant motor impairment of the dominant upper limb preventing use of digital interfaces; (2) clinically significant depressive symptoms (Yesavage Geriatric Depression Scale score ≥10); (3) history of major psychiatric disorders; (4) aphasia or communication disorders interfering with assessment; (5) diagnosis of major neurocognitive disorder; and (6) inability to provide informed consent. Due to substantial heterogeneity and incomplete neuroimaging reports, data on lesion location and volume were not included in this analysis.
Assessment Procedures
All assessments were conducted via secure video conferencing using the Google Meet platform. Evaluations were supervised in real time by a licensed neuropsychologist. The assessment protocol was divided into two sessions to minimize fatigue and maximize adherence. In the first session, the following instruments were administered: a standardized sociodemographic interview, the Instrumental Activities of Daily Living scale (Neuronorma adaptation), and the Working Memory Questionnaire. The participant, caregiver, and neuropsychologist joined a secure online session, during which the caregiver was instructed to support only technical logistics (e.g., screen sharing) and to refrain from providing cognitive assistance unless explicitly instructed.The second session focused on neuropsychological assessment and included the administration of the Working Memory Index. Standardized instructions and demonstration trials were provided before task initiation. The neuropsychologist observed the participant’s screen during task completion to ensure protocol compliance and recorded performance in real time. The caregiver was again present to assist with screen sharing but was asked to remain passive during task execution. All assessments were conducted in a controlled digital environment, with consistent protocols across participants to ensure standardization and reduce measurement variability.
Intervention
Participants assigned to the intervention group received a fully automated, adaptive computerized working memory training program, while those in the control group completed a non-adaptive version of the same program. Both versions were accessed through a secure online platform (https://braining.me) and developed by the research team using identical user interfaces, visual design, and task structures to control for engagement, expectancy, and usability.
Each training protocol comprised six computerized tasks specifically targeting working memory processes, including updating, maintenance, and manipulation. Tasks provided both trial-by-trial feedback and cumulative performance summaries. The key distinction between conditions was the adaptivity of the training protocol: the adaptive version employed a real-time difficulty adjustment algorithm that dynamically increased task complexity based on individual performance (ranging from 1 to 15 stimuli), thereby maintaining an optimal challenge level. In contrast, the non-adaptive control condition used a fixed low-difficulty threshold (1 to 5 stimuli), which did not change throughout the training period, thus minimizing cognitive load and limiting potential for skill acquisition.
Participants were instructed to complete daily training sessions of approximately 50 minutes each, targeting a total of 25 sessions over a 12-week period. Each session resumed from the final difficulty level attained on the previous day to ensure continuity in training progression. Training was conducted remotely, with participants using personal computers in their home environment.
To monitor adherence and identify potential barriers, participants received weekly follow-up calls from a trained research assistant. During these structured interviews, participants reported perceived cognitive, emotional, and social changes, as well as technical challenges encountered. Technical support was provided as needed to ensure consistent access and minimize dropout.
Outcome Measures
All outcome measures were collected at two time points: baseline (pre-intervention) and post-intervention (within 12 weeks of completing the training program). Assessments were administered in one or two sessions, depending on participant availability and fatigue levels, and were supervised remotely by a licensed neuropsychologist.
Primary Outcome Measures
The primary outcome was instrumental activities of daily living (IADLs), assessed using two validated instruments:
Lawton and Brody Instrumental Activities of Daily Living Scale: This scale evaluates functional competence across domains such as medication management, financial handling, transportation, and housekeeping. Both total scores and item-level responses were analyzed to capture granular changes in specific IADL components [26].
Working Memory Questionnaire: A self-report measure designed to capture everyday difficulties related to working memory in daily contexts [27].
All raw scores were adjusted for age and education based on available normative data. Importantly, neither the Lawton IADL scale nor the Working Memory Questionnaire was included in the training protocol, ensuring that outcome data reflected transfer effects rather than task-specific improvements.
Secondary Outcome Measures
Secondary outcomes focused on working memory capacity, assessed using the following performance-based neuropsychological tasks:
Working Memory Index: Derived from standardized subtests of the Wechsler Adult Intelligence Scale-IV (WAIS-IV), assessing verbal working memory span and manipulation [28].
See Table 1 for an overview of all cognitive tasks, scoring procedures, and associated outcome variables.
Background Measures
To ensure that all participants met the inclusion criteria regarding cognitive and affective status, two standardized screening instruments were administered prior to randomization:
Montreal Cognitive Assessment (MoCA): This brief cognitive screening tool was used to exclude participants with probable major neurocognitive disorder or dementia [29]. The MoCA has demonstrated adequate internal consistency in older adult populations (Cronbach’s α = 0.75) and provides a global index of cognitive functioning, including attention, memory, executive function, and visuospatial abilities.
Geriatric Depression Scale – Short Form (GDS-15): To exclude clinically significant depressive symptoms, the GDS-15 was administered [30]. This self-report measure is widely used in geriatric populations and has demonstrated acceptable internal reliability (Cronbach’s α = 0.72). A cutoff score of ≥10 was used as the exclusion criterion in accordance with validated thresholds for moderate to severe depression.
These background measures ensured that cognitive impairment was consistent with a diagnosis of mild neurocognitive disorder and not confounded by unrecognized dementia or depression.
Sample Size Determination
A priori power analysis was conducted using G*Power 3.1 software [31] to determine the required sample size for a repeated-measures analysis with two groups (adaptive vs. non-adaptive training) and two time points (pre- and post-intervention). The analysis assumed an alpha level of 0.05, a power of 0.90, and an effect size consistent with prior cognitive training studies in post-stroke populations. The results indicated that a minimum of 30 participants was required to detect a statistically significant group × time interaction. To allow for potential attrition and increase statistical power, a total of 50 participants were randomized (25 per group).
Randomization and Blinding
Participants were randomized to either the intervention group (adaptive working memory training) or the active control group (non-adaptive training) using a computer-generated sequence produced by Research Randomizer software. Randomization occurred immediately following telephone screening and prior to accessing participants’ medical records to minimize allocation bias. In cases where subsequent medical review revealed non-eligibility based on inclusion/exclusion criteria, the participant was informed of their exclusion and replaced with a new recruit maintaining the integrity of the randomization process.
Group assignment was stratified to minimize imbalances across critical baseline characteristics, including age, sex, years of education, level of computer experience, and MoCA scores. Importantly, participants were not informed of the adaptive nature of the intervention group; instead, they were told that the study was comparing two types of computerized cognitive training programs.
To reduce bias, outcome assessors were blinded to group assignment. Allocation was concealed using participant ID codes managed by the research coordinator, and assessors were not involved in the training sessions. At the conclusion of randomization, 25 participants had been assigned to each group.
Statistical Analysis
Before and after treatment, the patients’ performance was evaluated by comparing the mean scores obtained in the Lawton Instrumental Activities of daily living, Working Memory Questionnaire and the Working Memory Index. Data were analyzed using RStudio v. 1.4.1106 and the level of significance was set at p < .05 for all tests. The normality of the data was checked using the Shapiro–Wilks test. Descriptive statistics were calculated as a mean or median (with standard deviation, interquartile range), while categorical variables were presented as percentage frequencies. Student’s t-test and Mann–Whitney U test were used to test the significant differences in gains between the two groups. The effect size (Cohen’s d) was calculated to determine the group difference for each outcome measure. Cohen suggested that d = 0.2 be considered a 'small' effect size, 0.5 represents a 'medium' effect size and 0.8 a 'large' effect size (Gignac & Szodorai, 2016).
Bayesian Analyisis
In addition to traditional null hypothesis significance testing (NHST), Bayesian analyses were conducted to quantify the strength of evidence for group differences and the probability of the null hypothesis given the data. Bayesian independent samples t-tests were computed using the BayesFactor package in R. Bayes factors (BF₁₀) were interpreted using the guidelines where values between 1 and 3 indicate anecdotal evidence, 3–10 moderate evidence, and values >10 strong evidence for the alternative hypothesis [32].
3. Results
The flow of participants through the study can be seen in the CONSORT-SPI 2018 diagram (Figure 1).
Baseline Characteristics
Out of 1343 potential participants who were screened, 50 passed all in- and exclusion criteria. However, there were 18 dropouts. Finally, 32 patients were included in the final analyses (see Figure 1 for participant flowchart including drop-out reasons). Prior to training, the two groups did not differ in age, educational level, sex or baseline cognitive functioning (see Table 2 for scores and statistics). The Active Control Group included 16 participants, consisting of 10 men (62.5%) and 6 women (37.5%), ranging in age from 52 to 67 years (M = 59.4, SD = 4.9). Years of formal education varied between 5 and 17 years (M = 11.4, SD = 3.2). Time since ischemic stroke ranged from 11 to 112 months (M = 41.8, SD = 25.7). Vascular risk factors included hypertension in 7 participants (43.7%) and diabetes in 1 participant (6.25%).
The Experimental Group consisted of 16 participants as well, comprising 7 men (43.7%) and 9 women (56.2%) aged between 50 and 70 years (M = 62.1, SD = 6.2). Years of education ranged from 5 to 17 (M = 11.3, SD = 4.6). Time since the cerebrovascular event ranged from 24 to 127 months (M = 70.2, SD = 36.1). Hypertension was reported in 7 participants (43.7%) and diabetes in 4 (25%).
Mood and Cognitive Screening
Mood status was assessed using the Geriatric Depression Scale. In both groups, at least 75% of participants scored within the non-depressed range, while the remaining 25% showed scores consistent with mild depressive symptoms. In the Active Control Group, scores ranged from 0 to 8 (M = 3.1, SD = 3.0). In the Experimental Group, scores ranged from 0 to 5 (M = 1.8, SD = 1.4), suggesting overall lower depressive symptomatology. Global cognitive functioning was evaluated using the Montreal Cognitive Assessment (MoCA), adjusted for years of education. Both groups met criteria for mild neurocognitive disorder, with comparable performance: the Control Group scored M = 24.1 (SD = 1.6) and the Experimental Group M = 23.6 (SD = 0.8). These results indicate a relatively preserved cognitive profile consistent with the inclusion criteria.
The following section presents comparisons of the study variables using non-parametric tests, supported by Bayes factor analysis. The first set of comparisons pertains to baseline measurements, with descriptive and inferential statistics summarized in Table 2. The table reports descriptive values (mean, standard deviation, standard error, and coefficient of variation) for each variable at the initial assessment, along with the results of the Mann–Whitney U test, statistical significance (S.S), and the Bayes factor (BF₁₀).
Baseline comparisons revealed no statistically significant differences between the experimental and control groups across any of the measured variables (p > 0.05; see Table 2). All Bayes factor values (BF₁₀ < 1) consistently favored the null hypothesis, indicating stronger evidence for the absence of group differences prior to the intervention. Descriptive statistics further demonstrated comparable means and coefficients of variation between groups, suggesting a homogenous distribution of scores across cohorts. These findings support baseline equivalence and provide a robust foundation for evaluating post-intervention outcomes.
Similarly, a comparison of the variables between the control group and the experimental group was conducted for the second administration of the scales. The results are presented in Table 3.
As shown in Table 3, no statistically significant differences were observed between the control and experimental groups on the majority of variables following the intervention (p > 0.05). The corresponding Bayes Factors (BF₁₀), which were either close to or below 1, further support the null hypothesis, indicating an absence of group-level differences. An exception was observed for the WMI variable, which yielded a statistically significant effect (p = 0.015) and a BF₁₀ of 2.412, suggesting moderate evidence in favor of the alternative hypothesis. The mean score in the experimental group (103.94) exceeded that of the control group (93.69), reflecting a marked improvement in this domain attributable to the intervention.
Following between-group comparisons, within-group analyses were conducted to evaluate pre- to post-intervention changes for each group independently. Table 4 presents the results of these paired comparisons, including the Wilcoxon signed-rank test statistic (W), z-values, corresponding p-values, and Bayes Factors (BF₁₀) for each outcome measure.
As shown in Table 4, the variable IADL-I increased from 9.688 to 12.563 (W = 9.500, z = –2.699, p = 0.007), with a Bayes Factor (BF₁₀) of 34.076, indicating strong evidence in favor of the alternative hypothesis. In contrast, the variable WMQ(Storing) showed a decrease from 15.375 to 12.438 (W = 98.000, z = 2.158, p = 0.033), with a BF₁₀ of 3.827, which reflects moderate evidence supporting a significant change. Additionally, the variable WMI exhibited a notable increase from 92.625 to 103.938 (W = 3.000, z = –3.361, p < 0.05), accompanied by a markedly high BF₁₀, indicating very strong evidence for a substantial effect.
Conversely, the remaining variables IADL-AR, IADL-D, WMQ(Attention), WMQ(executive), WMQ (Full Scale), did not reach statistical significance (p > 0.05), and their BF₁₀ values remained below the conventional threshold of 3, suggesting insufficient evidence to reject the null hypothesis in these cases.
When conducting the same comparison for the control group, the results are presented in Table 5
The results presented in Table 5 reveal statistically significant changes in several of the analyzed variables. Specifically, the IADL-I subscale showed an increase in the mean score from 10.188 (SD = 3.619) to 12.563 (SD = 2.476). The associated test statistics (W = 0.000, z = –3.059, p = 0.002, BF₁₀ = 134.676) provide very strong evidence in favor of a significant time-related effect on this variable. Similarly, the IADL-AR subscale showed a reduction from 2.688 (SD = 2.938) to 0.900 (SD = 1.197) (W = 21.000, z = 2.201, p = 0.035, BF₁₀ = 6.687), indicating a statistically meaningful decrease. The WMQ (Attention) score also decreased from 13.063 (SD = 6.005) to 9.250 (SD = 6.191) (W = 111.500, z = 2.925, p = 0.004, BF₁₀ = 77.418), suggesting a notable post-intervention effect. In the case of WMQ (Full Scale), the score dropped from 36.313 (SD = 14.988) to 29.813 (SD = 15.510) (W = 102.000, z = 2.385, p = 0.018, BF₁₀ = 3.357). Additionally, the WMI dimension showed an increase from 89.938 (SD = 7.380) to 93.688 (SD = 7.040) (W = 6.500, z = –2.550, p = 0.012, BF₁₀ = 21.669), indicating a statistically significant improvement.
In contrast, no significant pre- to post-intervention changes were observed in the IADL-D, WMQ (Storing), WMQ (Executive) subscales, as their p-values exceeded the conventional alpha threshold (p > 0.05), and their BF₁₀ values remained below the cutoff typically used to indicate substantial evidence for an effect (i.e., BF₁₀ < 3).
A comparative analysis between the experimental and active control groups revealed that both showed statistically significant improvements in the IADL-I and WMI subscales, suggesting that both cognitive training modalities may positively influence these domains. However, distinctive patterns emerged across groups: the experimental group exhibited a significant reduction in WMQ (storing) (p = 0.033, BF₁₀ = 3.827), whereas the active control group demonstrated significant improvements in IADL-AR (p = 0.035, BF₁₀ = 6.687) and WMQ (Attention) (p = 0.004, BF₁₀ = 77.418)—effects that were not significant in the experimental condition. Additionally, the WMQ (Full Scale) score decreased significantly in the control group (p = 0.018, BF₁₀ = 3.357), whereas the same outcome showed only a trend toward significance in the experimental group (p = 0.062, BF₁₀ = 2.279).
These findings suggest a differential pattern of change across groups: although both interventions were associated with significant improvements in specific cognitive domains, each appears to exert its effect on distinct functional dimensions. This highlights the importance of considering the nature and specificity of cognitive training strategies when evaluating their impact on post-stroke cognitive recovery.
To determine whether the differences observed between pretest and posttest scores in the assessed variables can be attributed solely to the intervention, or whether they may also be explained by the influence of covariates such as depressive symptoms (Depression Yesavage Test) or global cognitive performance (MOCA Test), a Bayesian repeated measures analysis of variance (ANOVA) was conducted. This methodological approach allowed for the quantitative evaluation of multiple explanatory models, enabling direct comparisons between models that include or exclude the aforementioned covariates.
As an initial step, we examined whether the pretest–posttest difference in the IADL-I variable, for both the experimental and control groups, was influenced by depressive symptoms as a covariate, or whether the observed change could be attributed exclusively to the intervention. The results of this analysis are presented in Table 6.
Bayesian analysis results indicate that, within the experimental group, the model including only the effect of time was the most probable (P(M|data) = 0.506), with very strong evidence (BF = 17.237) and minimal contribution from depressive symptoms (Depression Yesavage Test, BF = 0.860). In contrast, in the control group, although a strong effect of time was also observed (BF = 14.531), the most probable model included depression as a covariate (P(M|data) = 0.656; BF = 2.314), suggesting that other factors may partially account for the observed differences.
Additionally, the Bayesian analyses conducted to evaluate the effect of cognitive performance (MOCA Test) on the dependent variable WMI showed that, in both the experimental and control groups, the model including both time and MOCA Test was the most probable. However, the specific contribution of MOCA Test was substantially greater in the control group (BF = 5.559, moderate to strong evidence) compared to the experimental group (BF = 1.149, weak or anecdotal evidence). These findings suggest that, although the intervention was a key determinant in the improvement of WMI, cognitive differences measured by the MOCA Test played a more relevant role in explaining the observed changes within the active control group. These results are summarized in Table 7.
In the control group, the Bayesian repeated measures analysis conducted to evaluate the effect of time and the depression covariate (Depression Yesavage Test) on the attention variable WMQ (Attention) indicated that the most probable model included both factors (P(M|data) = 0.503). The effect of time was extremely robust (BF = 21.567), reflecting a significant difference between the pretest (M = 13.06, SD = 6.01) and posttest (M = 9.25, SD = 6.19) scores, which was primarily attributable to the effect of time or the intervention itself, although a specific contribution of depression was also identified (BF = 1.113). The model exhibited a high explanatory capacity, with a mean R² of 72.7% (95% CI: 54.2%–84.3%).
Regarding the IADL-AR variable in the control group, the Bayesian analysis revealed that the most probable model was the one including only the depression covariate, with a posterior probability of 0.399. The contribution of this covariate yielded anecdotal evidence (BF = 1.100), while the effect of time was negligible (BF = 0.368), consistent with the stability observed in the pretest and posttest means (both M = 1.75). This model also showed a high explanatory capacity, with a mean R² of 76.1% (95% CI: 47.9%–90.8%), suggesting that depressive symptoms may be weakly related to individual variation in IADL-AR scores, although not to changes over time or in response to the intervention.
Moreover, the Bayesian analysis for the same variable IADL-AR indicated that the most probable model was the null model, with a posterior probability of 0.391. Neither the cognitive covariate (MOCA TOT) (BF = 0.786) nor the effect of time (BF = 0.427) provided sufficient evidence to explain significant variance in this variable. This finding aligns with the observed identical means in the pretest and posttest (both M = 1.75). The overall explanatory capacity of the model remained high (mean R² = 78.9%, 95% CI: 56.1%–91.7%), which may indicate that unmeasured individual factors contributed substantially to the observed variance.
For the remaining variables included in the study, neither the depression covariate nor the cognitive measure (MOCA) demonstrated a significant contribution to explaining the changes observed between pretest and posttest assessments, either within the control or experimental groups. In all these cases, the most probable models were those including only the effect of time, supported by strong Bayes Factors (BF), whereas the effects of the covariates showed weak or anecdotal evidence. These findings suggest that the observed differences in the assessed variables are primarily attributable to the intervention itself or the passage of time, rather than to individual factors such as depression or cognitive performance.
4. Discussion
The present study revealed that both adaptive working memory training (WMT) and an active control (non-adaptive) training produced significant gains in objective working memory capacity (WMI) and instrumental activities of daily living (IADL) independence. Specifically, participants in both groups showed robust pre–post improvements in WMI and the IADL–Independent (IADL–I) subscale (WMI increased from ~90 to ~94; IADL–I from 10.2 to 12.6) with very strong statistical (p<.05) and Bayesian evidence (BF₁₀≫10) (Table 5). These parallel improvements suggest that any structured cognitive training can enhance test-based working memory performance and basic IADL independence in post-stroke patients, consistent with prior findings that engaging cognitive exercises can bolster capacity under practice conditions [33].
However, the pattern of change diverged between groups in ways that hint at differential mechanisms. The adaptive WMT group (experimental condition) showed a significant reduction in self-reported Working Memory Questionnaire (WMQ) Storing subscale (p=0.033, BF₁₀≈3.8), whereas the control group improved on the IADL–Assistance Required (IADL–AR) subscale and the WMQ Attention subscale (both p≈0.035–0.004, BF₁₀>6). In other words, only the adaptive training was associated with gains in the “Storing” aspect of working memory (perhaps reflecting enhanced updating of information), while the non-adaptive training primarily improved participants’ attention-related memory complaints and reduced their need for assistance in daily tasks. Notably, the WMQ Full Scale score (overall subjective WM complaints) declined significantly in the control group (p=0.018, BF₁₀≈3.36) but only showed a trend in the experimental group. Thus, although both groups objectively improved on WMI, their subjective reports differed: the control group reported broad improvements in WM problems, whereas the adaptive group reported improvements specifically in storage/updating.
This dissociation between objective and subjective memory measures is striking. It suggests that objective test gains did not translate uniformly into perceived real-world memory function. The adaptive group’s enhanced WMI (↑93.7 vs 89.9) occurred alongside relatively modest changes in the WMQ total and subscales. Conversely, the control group’s subjective WM complaints improved more than the adaptive group’s, despite similar WMI gains. Such a mismatch echoes the well-known finding that cognitive training often yields limited far transfer to everyday cognition: meta-analytic reviews conclude that working memory training produces reliable near-transfer (on similar tasks) but no convincing broad “real-world” cognitive benefits [34,35]. In our sample, patients’ insight may also play a role – some stroke patients (especially with right-hemisphere lesions) exhibit anosognosia or reduced awareness of deficits [36]. This could partly explain why subjective WMQ scores did not parallel objective gains, or why the control group (perhaps due to expectancy or task differences) felt greater improvement.
Importantly, pre–post gains in IADL and WMI were largely driven by the interventions themselves, not baseline mood or cognition. Bayesian repeated-measures ANOVAs (with covariates) indicated that in the adaptive group, improvements in IADL–I were best explained by time (training) alone (BF₁₀≈17.2 for time; BF₁₀≈0.86 for depression). In the control group, time also had a strong effect (BF₁₀≈14.5), but the most probable model included depressive symptoms (Yesavage Test) as a covariate (BF₁₀≈2.31). Similarly, while WMI gains were driven by training in both groups, baseline global cognition (MoCA) played a much larger role in the control group (BF₁₀≈5.56, moderate evidence) than in the adaptive group (BF₁₀≈1.15, anecdotal). In practical terms, this implies that the adaptive training’s effects on memory were relatively independent of patients’ mood or cognitive status, whereas in the non-adaptive group, participants who were already higher-functioning (or less depressed) benefited more. Thus, covariates were generally weak contributors, except that baseline depression and cognition modestly modulated outcomes in the control group.
These findings fit within broader theories of neuroplasticity and cognitive training. According to a recent study, effective rehabilitation depends on experience-dependent plasticity: improvements arise from specific, intense, salient, and repetitive practice [37]. In our study, both training regimens involved repetition and some level of difficulty adjustment, but only the adaptive WMT continuously scaled task challenge to participant performance. This adaptive “optimal challenge” may have preferentially engaged the neural circuits underpinning working memory updating. In this sense, the adaptive group’s specific gain in WMQ (Storing) may reflect a strengthening of dynamic memory-updating mechanisms, consistent with the specificity principle of training-induced plasticity [33]. By contrast, the control regimen (with fixed or less-challenging tasks) perhaps served more as a general mental exercise, yielding broader subjective improvements (e.g. in attention complaints) but fewer gains in complex updating. Notably, the authors found that adaptive versus non-adaptive training made little difference: exposure to variable task difficulty alone was sufficient to boost working memory performance, with no additional far transfer [38]. Our results partially concur: both groups improved objective WMI equally, suggesting that adaptivity per se was not required for baseline gains. However, the pattern of transfer differed, implying that adaptivity may shape which cognitive processes benefit.
The transfer of cognitive training to everyday function remains controversial. Some recent trials in stroke report that computerized cognitive training improves neuropsychological scores but yields minimal functional gains [39]. For example, this study found significant improvements in processing speed and language tasks after adaptive training, yet no change in basic or instrumental ADLs [39]. In contrast, our results showed a sizeable IADL–I improvement in both groups (mean ∆ ≈ +2.4 points) and a large reduction in the need for assistance (IADL–AR ↓1.8). This discrepancy could arise from differences in patient chronicity, intensity of spontaneous recovery, or the specific IADL measure used. It may also reflect our finding that even non-adaptive cognitive exercises can bolster everyday independence in the short term. Nevertheless, our improvements in IADL coexist with the broader literature cautioning that gains on ‘brain training’ tasks often do not translate into far transfer [34,35]. In particular, recents findings emphasize that most training benefits remain task-specific, with little evidence for enhancements in general cognition or daily-life performance [34]. Our data mirror this: aside from IADL–I, other daily-life measures (e.g. IADL–Dependent) did not change, and only certain IADL subscales improved (differently by group). Thus, even where we see promising IADL results, they should be interpreted cautiously in light of transfer limitations.
From a clinical standpoint, these findings highlight both potential and challenge for cognitive rehabilitation after stroke. On one hand, the adaptive WMT appeared to tap into updating-related plasticity, consistent with the idea that training difficulty and task relevance can guide recovery of specific cognitive mechanisms [37]. On the other hand, improvements did not generalize uniformly, underscoring that cognitive gains do not automatically resolve functional deficits. Stroke recovery is complex and highly individual: lesion location/extent predicts which cognitive and ADL abilities are affected [39], and personal factors (motivation, insight, mood) also modulate outcomes. A “one-size-fits-all” program is unlikely to fully address this heterogeneity [39]. In line with this, recent reviews advocate for multimodal, ecologically valid interventions: for example, combining cognitive exercises with goal-oriented ADL tasks or aerobic exercise to maximize plasticity (e.g. enriching the training environment) [37,38,39]. Our data suggest that future programs should incorporate such principles – for instance, adapting tasks based on patient progress, varying stimuli to promote generalization, and explicitly linking training to daily activities. Notably, despite some gains here, key WMQ subscales (e.g. Executive) and the IADL–Dependent score showed no change, hinting that either the training dose was insufficient or the measures lacked sensitivity.
5. Conclusions
Several caveats temper our conclusions. Sample size was modest and attrition nontrivial, which reduces statistical power and raises the risk of Type I/II errors. The training duration and intensity (number of sessions) were limited; a longer or more intensive regimen might produce larger or more durable effects. Our IADL instrument may have ceiling or floor effects (e.g. low baseline IADL–AR scores in many patients), possibly obscuring subtler changes. Likewise, the WMQ is a subjective questionnaire; responses can be biased by patient insight or demand characteristics. Finally, although we included covariates (depression, MoCA), other factors (e.g. lesion site, fatigue) were not controlled and could influence outcomes. Future work should employ larger, more diverse samples, include active control tasks closely matched in engagement, and assess long-term follow-up to confirm persistence of gains.
In sum, both adaptive WMT and non-adaptive cognitive practice yielded improvements in working memory performance and IADL independence post-stroke, but adaptive training led to changes suggestive of enhanced memory-updating processes. The dissociation between objective and subjective outcomes underscores the need to bridge lab-based gains with real-world function. Designing more ecologically valid training programs — for example, by integrating cognitive tasks with daily living activities, providing strategy instruction, or combining mental with physical exercises — may promote transfer and engage neuroplasticity more fully. Such hybrid interventions, guided by principles of intensity, variety, and relevance, hold promise for improving functional recovery. Ultimately, our findings highlight that while cognitive training can harness brain plasticity after stroke, its effectiveness depends critically on training specificity and the match between tasks and patients’ everyday needs.
Author Contributions
Conceptualization, Daniel Landínez and Andrés Grisales; Methodology, Daniel Landínez; Software, Andrés Grisales; Validation, Daniel Landinez and Andrés Grisales; Formal Analysis, Andres Grisales; Investigation, Daniel Landinez; Resources, Daniel Landínez; Data Curation, Andres Grisales; Writing – Original Draft Preparation, Daniel Landinez; Writing – Review and Editing, Daniel Landinez and Andrés Grisales; Visualization, Daniel Landinez; Supervision, Daniel Landinez; Project Administration, Daniel Landínez. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Instituto Neurologico de Colombia, Colombia (protocol code 449011-19.0.013 issued September 15 2021.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The dataset used in this research is owned by Instituto Neurológico de Colombia (Colombia), and as such, its accessibility is subject to the institution’s policies and regulations. For this reason, the data is available upon request, as any data sharing must be approved by the university.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Feigin VL, Brainin M, Norrving B, Martins SO, Pandian J, Lindsay P, et al. World Stroke Organization: Global Stroke Fact Sheet 2025. International Journal of Stroke [Internet]. 2025 Feb 3;20(2):132–44. Available online: https://journals.sagepub.com/doi/10.1177/17474930241308142.
- Martin SS, Aday AW, Allen NB, Almarzooq ZI, Anderson CAM, Arora P, et al. 2025 Heart Disease and Stroke Statistics: A Report of US and Global Data From the American Heart Association. Circulation [Internet]. 2025 Feb 25;151(8). Available online: https://www.ahajournals.org/doi/10.1161/CIR.0000000000001303.
- El Husseini N, Katzan IL, Rost NS, Blake ML, Byun E, Pendlebury ST, et al. Cognitive Impairment After Ischemic and Hemorrhagic Stroke: A Scientific Statement From the American Heart Association/American Stroke Association. Stroke [Internet]. 2023 Jun 1;54(6):E272–91. Available online: https://www.ahajournals.org/doi/10.1161/STR.0000000000000430.
- Elendu C, Amaechi DC, Elendu TC, Ibhiedu JO, Egbunu EO, Ndam AR, et al. Stroke and cognitive impairment: understanding the connection and managing symptoms. Annals of Medicine & Surgery [Internet]. 2023 Dec;85(12):6057–66. Available online: https://journals.lww.com/10.1097/MS9.0000000000001441.
- Blomgren C, Samuelsson H, Blomstrand C, Jern C, Jood K, Claesson L. Long-term performance of instrumental activities of daily living in young and middle-aged stroke survivors—Impact of cognitive dysfunction, emotional problems and fatigue. Abete P, editor. PLoS One [Internet]. 2019 May 16;14(5):e0216822. Available online: https://dx.plos.org/10.1371/journal.pone.0216822.
- Stolwyk RJ, Mihaljcic T, Wong DK, Chapman JE, Rogers JM. Poststroke Cognitive Impairment Negatively Impacts Activity and Participation Outcomes. Stroke [Internet]. 2021 Feb 1;52(2):748–60. Available online: https://www.ahajournals.org/doi/10.1161/STROKEAHA.120.032215.
- de Menezes KKP, Scianni AA, Avelino PR, Faria-Fortini I, Bastos VS, Faria CDC de M. Contextual and clinical factors as explainers of stroke severity, residual motor impairments, and functional independence during hospitalization. Journal of Stroke and Cerebrovascular Diseases [Internet]. 2025 Jan 1;34(1):108154. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1052305724005974.
- Heldner MR, Chalfine C, Houot M, Umarova RM, Rosner J, Lippert J, et al. Cognitive Status Predicts Return to Functional Independence After Minor Stroke: A Decision Tree Analysis. Front Neurol [Internet]. 2022 Feb 17;13. Available online: https://www.frontiersin.org/articles/10.3389/fneur.2022.833020/full.
- MANCUSO M, IOSA M, ABBRUZZESE L, MATANO A, COCCIA M, BAUDO S, et al. The impact of cognitive function deficits and their recovery on functional outcome in subjects affected by ischemic subacute stroke: results from the Italian multicenter longitudinal study CogniReMo. Eur J Phys Rehabil Med [Internet]. 2023 Jun 1;59(3):284–93. Available online: https://www.minervamedica.it/index2.php?show=R33Y2023N03A0284.
- Lugtmeijer S, Lammers NA, de Haan EHF, de Leeuw FE, Kessels RPC. Post-Stroke Working Memory Dysfunction: A Meta-Analysis and Systematic Review. Neuropsychol Rev [Internet]. 2021 Mar 24;31(1):202–19. Available online: http://link.springer.com/10.1007/s11065-020-09462-4.
- Irfani Fitri F, Fithrie A, Rambe AS. Association between working memory impairment and activities of daily living in post-stroke patients. Med Glas [Internet]. 2020 Jul 12;17(2):433–8. Available online: https://medicinskiglasnik.ba/article/246.
- Malouin F, Belleville S, Richards CL, Desrosiers J, Doyon J. Working memory and mental practice outcomes after stroke. Arch Phys Med Rehabil [Internet]. 2004 Feb;85(2):177–83. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0003999303007718.
- Loetscher T, Potter KJ, Wong D, das Nair R. Cognitive rehabilitation for attention deficits following stroke. Cochrane Database of Systematic Reviews [Internet]. 2019 Nov 10;2019(11). Available online: https://doi.wiley.com/10.1002/14651858.CD002842.pub3.
- Loetscher T, Lincoln NB. Cognitive rehabilitation for attention deficits following stroke. Cochrane Database of Systematic Reviews [Internet]. 2013 May 31;2013(5). Available online: https://doi.wiley.com/10.1002/14651858.CD002842.pub2.
- Westerberg H, Jacobaeus H, Hirvikoski T, Clevberger P, Östensson ML, Bartfai A, et al. Computerized working memory training after stroke–A pilot study. Brain Inj [Internet]. 2007 Jan 3;21(1):21–9. Available online: http://www.tandfonline.com/doi/full/10.1080/02699050601148726.
- van de Ven RM, Murre JMJ, Veltman DJ, Schmand BA. Computer-Based Cognitive Training for Executive Functions after Stroke: A Systematic Review. Front Hum Neurosci [Internet]. 2016 Apr 20;10(APR2016):1–27. Available online: http://journal.frontiersin.org/Article/10.3389/fnhum.2016.00150/abstract.
- das Nair R, Cogger H, Worthington E, Lincoln NB. Cognitive rehabilitation for memory deficits after stroke. Cochrane Database of Systematic Reviews [Internet]. 2016 Sep 1;2016(9). Available online: http://doi.wiley.com/10.1002/14651858.CD002293.pub3.
- Kleim JA, Jones TA. Principles of Experience-Dependent Neural Plasticity: Implications for Rehabilitation After Brain Damage. Journal of Speech, Language, and Hearing Research [Internet]. 2008 Feb;51(1). Available online: http://pubs.asha.org/doi/10.1044/1092-4388%282008/018%29.
- Karbach J, Verhaeghen P. Making Working Memory Work: A Meta-Analysis of Executive-Control and Working Memory Training in Older Adults. Psychol Sci [Internet]. 2014 Nov 8;25(11):2027–37. Available online: https://journals.sagepub.com/doi/10.1177/0956797614548725.
- von Bastian CC, Eschen A. Does working memory training have to be adaptive? Psychol Res [Internet]. 2016 Mar 26;80(2):181–94. Available online: http://link.springer.com/10.1007/s00426-015-0655-z.
- Cahn-Weiner DA, Boyle PA, Malloy PF. Tests of Executive Function Predict Instrumental Activities of Daily Living in Community-Dwelling Older Individuals. Appl Neuropsychol [Internet]. 2002 Sep;9(3):187–91. Available online: http://www.tandfonline.com/doi/abs/10.1207/S15324826AN0903_8.
- M. Tucker A, Stern Y. Cognitive Reserve in Aging. Curr Alzheimer Res [Internet]. 2011 Jun 1;8(4):354–60. Available online: http://www.eurekaselect.com/openurl/content.php?genre=article&issn=1567-2050&volume=8&issue=4&spage=354.
- Simons DJ, Boot WR, Charness N, Gathercole SE, Chabris CF, Hambrick DZ, et al. Do “Brain-Training” Programs Work? Psychological Science in the Public Interest [Internet]. 2016 Oct 2;17(3):103–86. Available online: https://journals.sagepub.com/doi/10.1177/1529100616661983.
- Lövdén M, Bäckman L, Lindenberger U, Schaefer S, Schmiedek F. A theoretical framework for the study of adult cognitive plasticity. Psychol Bull [Internet]. 2010 Jul;136(4):659–76. Available online: https://doi.apa.org/doi/10.1037/a0020080.
- Robertson IH, Murre JMJ. Rehabilitation of brain damage: Brain plasticity and principles of guided recovery. Psychol Bull [Internet]. 1999;125(5):544–75. Available online: https://doi.apa.org/doi/10.1037/0033-2909.125.5.544.
- Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9(3 Pt 1):179–186. [CrossRef]
- Vallat-Azouvi C, Pradat-Diehl P, Azouvi P. The Working Memory Questionnaire: a scale to assess everyday life problems related to deficits of working memory in brain injured patients. Neuropsychol Rehabil. 2012;22(4):634–649. [CrossRef]
- Wechsler D. Wechsler Adult Intelligence Scale–Fourth Edition (WAIS–IV) manual. San Antonio (TX): Pearson Assessment; 2008.
- Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. [CrossRef]
- Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982;17(1):37–49. [CrossRef]
- Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. [CrossRef]
- Jeffreys H. Theory of probability. 3rd ed. Oxford: Oxford University Press; 1961.
- Maier M, Ballester BR, Verschure PFMJ. Principles of neurorehabilitation after stroke based on motor learning and brain plasticity mechanisms. Front Syst Neurosci. 2019;13:74. [CrossRef]
- Simons DJ, Boot WR, Charness N, Gathercole SE, Chabris CF, Hambrick DZ, et al. Do “brain-training” programs work? Psychol Sci Public Interest. 2016;17(3):103–186. [CrossRef]
- Melby-Lervåg M, Redick TS, Hulme C. Working memory training does not improve performance on measures of intelligence or other measures of “far transfer”: Evidence from a meta-analytic review. Perspect Psychol Sci. 2016;11(4):512–534. [CrossRef]
- Mulhern M. Cognitive rehabilitation interventions for post-stroke populations. Delaware J Public Health. 2023;9(3):70–74. [CrossRef]
- Kleim JA, Jones TA. Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. J Speech Lang Hear Res. 2008;51(1 Suppl):S225–S239. [CrossRef]
- von Bastian CC, Eschen A. Does working memory training have to be adaptive? Psychol Res. 2016;80(2):181–194. [CrossRef]
- Soni AK, Kumar M, Kothari S. Efficacy of home-based computerized adaptive cognitive training in patients with post-stroke cognitive impairment: a randomized controlled trial. Sci Rep. 2025;15:1072. [CrossRef]
Figure 1.
CONSORT-SPI 2018 diagram showing flow of patients through the study.
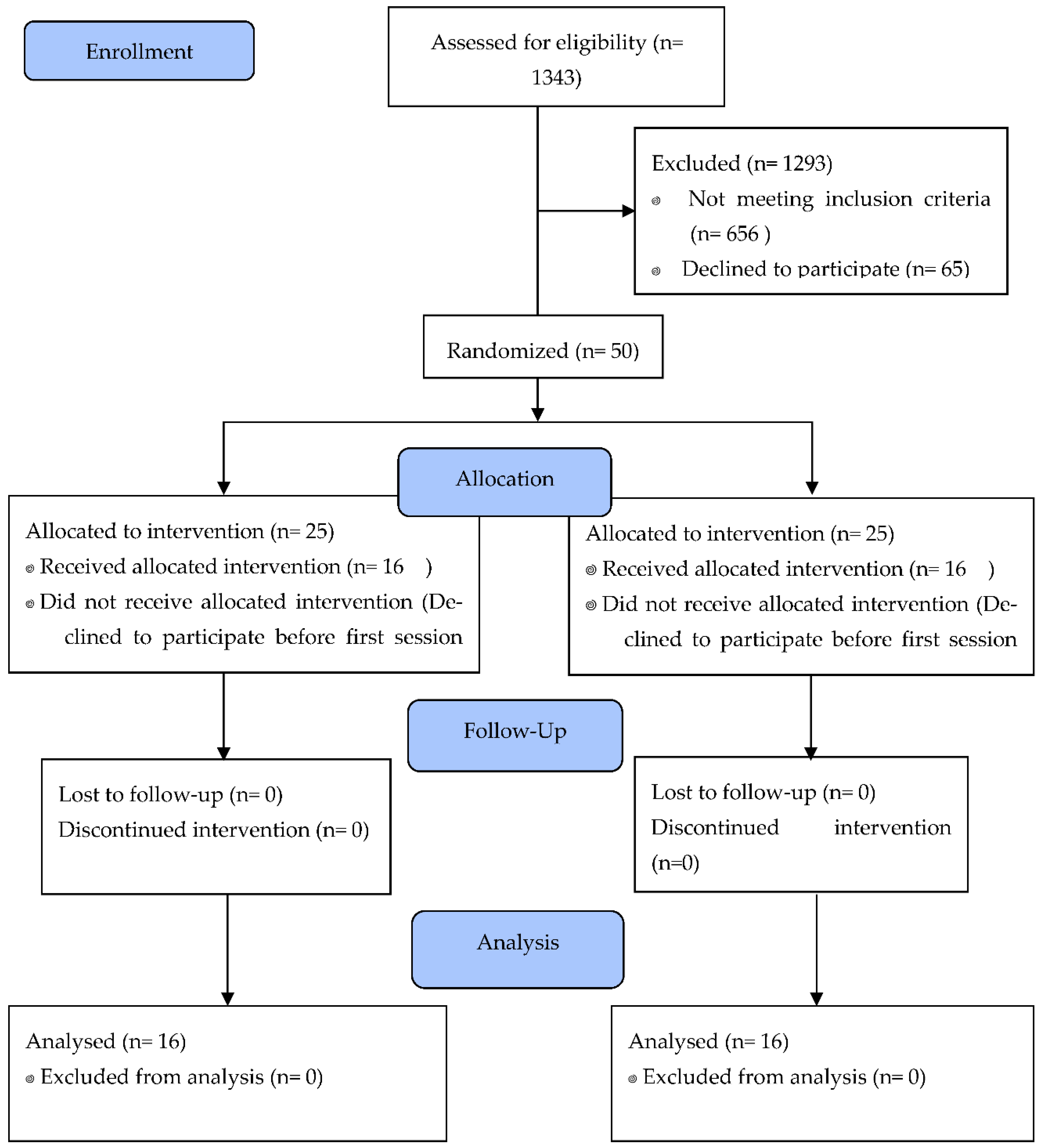

Table 1.
Tasks used for every domain.
| Domain | Task | Outcome measure |
|---|---|---|
| Primary outcome measure | ||
| IADL | Lawton Instrumental activities of daily living: (Cronbach’s α = 0.94). | Number of activities performed:
|
| e.g. Using the telephone |
|
|
| Working memory Questionnaire: (Cronbach’s α = 0.89). e.g. When you shop, do you often spend more than the budget you set for yourself? |
30 questions Each question was rated on a five-point Likert-type scale, ranging from 0 (“no problem at all”) to 4 (“very severe problem in everyday life”). Three sub- scores were computed, for each of the three domains (maximal score 40 for each), as well as a total score (out of 120). Higher scores corresponded to more difficulties/complaints. |
|
| Secondary outcome measure | ||
| Working memory | Working memory Index: Arithmetic task, forward, backward and sequencing digit span. (Cronbach’s α = 0.94). e.g. There are 25 gum tablets in each package. How many tablets are there in 8 packages? |
Age-corrected z-scores of total number of correct items |
Table 2.
Descriptive and comparative statistics of baseline variables.
| Variables | Group | Mean | SD | SE | C.V | U | S.S | BF₁₀ | ||
|---|---|---|---|---|---|---|---|---|---|---|
| IADL- I | Control | 10.188 | 3.619 | 0.905 | 0.355 | 144.500 | 0.543 | 0.370 | ||
| Experimental | 9.688 | 3.516 | 0.879 | 0.363 | ||||||
| IADL-AR | Control | 2.688 | 2.938 | 0.734 | 1.093 | 123.500 | 0.878 | 0.358 | ||
| Experimental | 3.000 | 3.651 | 0.913 | 1.217 | ||||||
| IADL-D | Control | 1.125 | 1.893 | 0.473 | 1.683 | 111.000 | 0.504 | 0.408 | ||
| Experimental | 1.313 | 1.537 | 0.384 | 1.171 | ||||||
| WMQ (Storing) | Control | 14.188 | 5.764 | 1.441 | 0.406 | 114.000 | 0.610 | 0.371 | ||
| Experimental | 15.375 | 7.464 | 1.866 | 0.485 | ||||||
| WMQ (Attention) | Control | 13.063 | 6.005 | 1.501 | 0.460 | 132.500 | 0.880 | 0.345 | ||
| Experimental | 13.188 | 6.493 | 1.623 | 0.492 | ||||||
| WMQ (Executive) | Control | 9.063 | 5.709 | 1.427 | 0.630 | 120.500 | 0.791 | 0.362 | ||
| Experimental | 10.188 | 6.969 | 1.742 | 0.684 | ||||||
| WMQ (Full Scale) | Control | 36.313 | 14.988 | 3.747 | 0.413 | 123.500 | 0.880 | 0.337 | ||
| Experimental | 38.750 | 18.746 | 4.686 | 0.484 | ||||||
| WMI | Control | 89.938 | 7.380 | 1.845 | 0.082 | 91.000 | 0.165 | 0.601 | ||
| Experimental | 92.625 | 8.539 | 2.135 | 0.092 |
Note. IADL-I= Instrumental activities of daily living-Independent; IADL-AR= Instrumental activities of daily living- Assistance Required; IADL-D= Dependent; WMQ= Working memory questionnaire; WMI= working memory index.
Table 3.
Descriptive and comparative statistics at posttest.
| Variables | Group | Mean | SD | SE | C.V | U | S.S | BF₁₀ |
|---|---|---|---|---|---|---|---|---|
| IADL- I | Control | 12.563 | 2.476 | 0.619 | 0.197 | 141.500 | 0.598 | 0.375 |
| Experimental | 12.563 | 1.931 | 0.483 | 0.154 | ||||
| IADL-AR | Control | 0.900 | 1.197 | 0.379 | 1.330 | 24.500 | 0.088 | 0.992 |
| Experimental | 1.889 | 1.453 | 0.484 | 0.769 | ||||
| IADL-D | Control | 1.750 | 2.315 | 0.818 | 1.323 | 19.000 | 0.939 | 0.483 |
| Experimental | 1.200 | 1.095 | 0.490 | 0.913 | ||||
| WMQ (Storing) | Control | 12.438 | 6.470 | 1618 | 0.520 | 128.000 | 0.999 | 0.337 |
| Experimental | 12.438 | 7.711 | 1928 | 0.620 | ||||
| WMQ (Attention) | Control | 9.250 | 6.191 | 1548 | 0.669 | 109.000 | 0.485 | 0.412 |
| Experimental | 11.125 | 6.292 | 1573 | 0.566 | ||||
| WMQ (Executive) | Control | 8.125 | 5.353 | 1338 | 0.659 | 137.500 | 0.734 | 0.353 |
| Experimental | 7.938 | 5.285 | 1321 | 0.666 | ||||
| WMQ (Full Scale) | Control | 29.813 | 15.510 | 3878 | 0.520 | 126.500 | 0.970 | 0.341 |
| Experimental | 31.500 | 18.221 | 4555 | 0.578 | ||||
| WMI | Control | 93.688 | 7.040 | 1760 | 0.075 | 63.500 | 0.015 | 2.412 |
| Experimental | 103.938 | 11.509 | 2877 | 0.111 |
Note. IADL-I= Instrumental activities of daily living-Independent; IADL-AR= Instrumental activities of daily living- Assistance Required; IADL-D= Dependent; WMQ= Working memory questionnaire; WMI= working memory index.
Table 4.
Comparative tests of related samples (pretest–posttest) in the experimental group.
| Variables | Mean | S.D | C.V. | W | z | p | BF10 |
|---|---|---|---|---|---|---|---|
| IADL-I-PRE | 9.688 | 3.516 | 0.363 | 9.500 | -2.699 | 0.007 | 34.076 |
| IADL-I-POS | 12.563 | 1.931 | 0.154 | ||||
| IADL-AR-PRE | 3.000 | 3.651 | 1.217 | 17.000 | -0.140 | 0.943 | 0.326 |
| IADL-AR-POS | 1.889 | 1.453 | 0.769 | ||||
| IADL-D-PRE | 1.313 | 1.537 | 1.171 | 6.000 | 1.604 | 0.174 | 1.439 |
| IADL-D-POS | 1.200 | 1.095 | 0.913 | ||||
| WMQ (Storing)PRE | 15.375 | 7.464 | 0.485 | 98.000 | 2.158 | 0.033 | 3.827 |
| WMQ (Storing)POS | 12.438 | 7.711 | 0.620 | ||||
| WMQ (Attention) PRE | 13.188 | 6.493 | 0.492 | 85.000 | 1.420 | 0.163 | 0.856 |
| WMQ (Attention)POS | 11.125 | 6.292 | 0.566 | ||||
| WMQ (Executive)PRE | 10.188 | 6.969 | 0.684 | 88.500 | 1.619 | 0.109 | 1.291 |
| WMQ (Executive)POS | 7.938 | 5.285 | 0.666 | ||||
| WMQ (Full Scale) PRE | 38.750 | 18.746 | 0.484 | 104.500 | 1.887 | 0.062 | 2.279 |
| WMQ (Full Scale)POS | 31.500 | 18.221 | 0.578 | ||||
| WMI-PRE | 92.625 | 8.539 | 0.092 | 3.000 | -3.361 | <0.001 | 180.797 |
| WMI- POS | 103.938 | 11.509 | 0.111 |
Note. IADL-I= Instrumental activities of daily living-Independent; IADL-AR= Instrumental activities of daily living- Assistance Required; IADL-D= Dependent; WMQ= Working memory questionnaire; WMI= working memory index.
Table 5.
Comparative tests of related samples (pretest–posttest) in the active control group.
| Variables | Mean | S.D | C.V. | W | z | p | BF10 |
|---|---|---|---|---|---|---|---|
| IADL-I-PRE | 10.188 | 3.619 | 0.355 | 0.000 | -3.059 | 0.002 | 134.676 |
| IADL-I-POS | 12.563 | 2.476 | 0.197 | ||||
| IADL-AR-PRE | 2.688 | 2.938 | 1.093 | 21.000 | 2.201 | 0.035 | 6.687 |
| IADL-AR-POS | 0.900 | 1.197 | 1.330 | ||||
| IADL-D-PRE | 1.125 | 1.893 | 1.683 | 6.000 | 0.365 | 0.854 | 0.398 |
| IADL-D-POS | 1.750 | 2.315 | 1.323 | ||||
| WMQ (Storing)PRE | 14.188 | 5.764 | 0.406 | 78.000 | 1.601 | 0.116 | 1.147 |
| WMQ (Storing)POS | 12.438 | 6.470 | 0.520 | ||||
| WMQ (Attention) PRE | 13.063 | 6.005 | 0.460 | 111.500 | 2.925 | 0.004 | 77.418 |
| WMQ (Attention)POS | 9.250 | 6.191 | 0.669 | ||||
| WMQ (Executive)PRE | 9.063 | 5.709 | 0.630 | 88.000 | 1.034 | 0.312 | 0.383 |
| WMQ (Executive)POS | 8.125 | 5.353 | 0.659 | ||||
| WMQ (Full Scale) PRE | 36.313 | 14.988 | 0.413 | 102.000 | 2.385 | 0.018 | 3.357 |
| WMQ (Full Scale)POS | 29.813 | 15.510 | 0.520 | ||||
| WMI-PRE | 89.938 | 7.380 | 0.082 | 6.500 | -2.550 | 0.012 | 21.669 |
| WMI- POS | 93.688 | 7.040 | 0.075 |
Note. IADL-I= Instrumental activities of daily living-Independent; IADL-AR= Instrumental activities of daily living- Assistance Required; IADL-D= Dependent; WMQ= Working memory questionnaire; WMI= working memory index.
Table 6.
Bayesian repeated measures ANOVA for analyzing the effect of the depression variable.
| Group | Likely Model | P(M|data) | Time Effect (BF_incl) | DYT Effect (BF_incl) | Mean R² (95% CI) |
|---|---|---|---|---|---|
| Experimental | Time | 0.506 | 17.237 (Very Strong) | 0.860 (Weak) | 0.406 [0.197–0.578] |
| Control | Time + DYT | 0.656 | 14.531 (Very Strong) | 2.314 (Moderate) | 0.580 [0.319–0.754] |
Note. DYT= Depression Yesavage Test.
Table 7.
Bayesian repeated measures ANOVA for analyzing the effect of performance in MoCA Test.
| Grupo | Likely Model | P(M|data) | Time Effect (BF_incl) | MOCA TOT Effect (BF_incl) | Mean R² (95% CI) |
|---|---|---|---|---|---|
| Experimental | Time + MOCA TOT | 0.534 | 628.129 (very strong) | 1.149 (Anecdotical) | 0.692 [0.518–0.812] |
| Control | Time + MOCA TOT | 0.779 | 11.688 (strong) | 5.559 (Moderate to strong) | 0.717 [0.433–0.857] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



