
Submitted:
12 June 2025
Posted:
18 June 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: The COVID-19 pandemic progressed unevenly across the 417 municipalities of Bahia, Brazil. Pinpointing where and when risk peaked is vital for guiding interventions and preparing for future emergencies. Methods: We performed an ecological spatiotemporal study using confirmed cases recorded in e-SUS Notifica and Sivep-Gripe from January 2020 to December 2022. A discrete Poisson space-time scan in SaTScan (spatial window ≤ 50 % of the population; temporal window ≤ 6 months) identified clusters. For each cluster we calculated relative risk (RR) and log-likelihood ratio, considering p < 0.05 significant. Results: Thirty-three clusters were detected, 25 statistically significant. The largest cluster (164 municipalities; May 2020–June 2021) comprised 702 720 observed versus 338 822 expected cases (RR = 2.8). Two overlapping large clusters (185 and 136 municipalities) during January–February 2022—coinciding with Omicron circulation—showed RR ≈ 2.2. Localised clusters reached RR = 3.37. Spatially, risk concentrated in the south, southwest and east of the state, with isolated contryside outbreaks. Conclusions: The heterogeneous spatiotemporal dynamics of COVID-19 in Bahia underscore the value of real-time cluster detection for targeted surveillance and resource allocation. Tailored strategies, supported by genomic surveillance and socioeconomic indicators, are essential to mitigate future respiratory events.
Keywords:
COVID-19
; SARS-CoV-2
; Spatiotemporal analysis
1. Introduction
The COVID-19 pandemic has emerged as the most impactful public health event in recent decades, exposing significant challenges in containing the spread of its etiological agent, SARS-CoV-2, and in managing healthcare systems [1]. From the first recorded cases in China in December 2019 to its rapid dissemination across continents, this viral disease has exhibited complex and heterogeneous transmission patterns determined by biological, social, economic, and environmental factors [2].
By the first half of 2020, Brazil quickly became one of the epicenters of this health emergency, consistently ranking among the countries with the highest number of accumulated cases and deaths [3]. Due to its continental dimensions and deep socioeconomic inequalities, the course of the pandemic in Brazil varied significantly across regions, states, and municipalities [4]. This scenario was exacerbated by the absence of a nationally coordinated strategy for containment and mitigation [5,6].
In Bahia, COVID-19 presented unique epidemiological characteristics due to the heterogeneity of its territory, which includes densely populated urban zones and remote rural areas. During the first two years of the pandemic, epidemic peaks of varying intensity occurred, with the highest incidence recorded in the early weeks of 2022. Compared to other Brazilian states, Bahia maintained relatively lower incidence and mortality rates [7,8].
The emergence and dissemination of SARS-CoV-2 variants posed new challenges in pandemic control due to their distinct transmissibility and severity characteristics, resulting in different incidence and mortality patterns [9]. Brazil played a central role in this scenario, as evidenced by the identification of the Gamma variant (P.1) in Manaus, which rapidly spread nationally and internationally. The high viral load in the country, exacerbated by regional inequalities and delays in mass vaccination efforts, intensified the circulation of variants of concern [10]. In Bahia, different subtypes shaped the behavior of epidemic waves, with peaks frequently associated with the predominance of highly transmissible variants [11].
Although the pandemic has been overcome, it remains essential to investigate the transmission dynamics of SARS-CoV-2, especially as it was marked by the emergence of variants with varying degrees of transmissibility and immune escape [12]. Retrospective analyses of spatiotemporal patterns and the factors influencing virus dissemination can provide relevant information for countries to prevent and prepare for future public health emergencies, especially those involving emerging respiratory viruses [13]. This study aims to characterize the spatiotemporal patterns of COVID-19 in the state of Bahia, Brazil, from 2020 to 2022.
2. Materials and Methods
Study Design and Period
This is an ecological spatiotemporal study of confirmed COVID-19 cases in the state of Bahia, Brazil, conducted with the municipality of residence as the spatial unit of analysis and the month of occurrence as the temporal unit, covering the period from 2020 to 2022.
Study Area and Population
Bahia is in the Northeast region of Brazil and comprises 417 municipalities, which are organized into 28 Administrative Regions and 9 Health Macroregions. It is the fourth most populous state in Brazil and the fifth largest in territorial extension, covering 6.6% of the country’s geographic area and 36.3% of the region [14,15].
Data Sources
Data on COVID-19 cases, categorized by municipality of residence and month of occurrence, were obtained from the Bahia State Health Department’s website, through the Flu Notification System (e-SUS Notifica) [16] and the Acute Respiratory Distress Syndrome Epidemiological Surveillance System (Sivep-Gripe) [17].
Population data and geographic coordinates (latitude and longitude) necessary for calculating the centroid of each municipality were obtained from the Brazilian Institute of Geography and Statistics (IBGE) [14].
Analytical Procedures
To analyze the spatiotemporal distribution of COVID-19 and identify high-risk clusters for disease incidence in Bahia from January 2020 to December 2022, data were aggregated by month of occurrence and municipality of residence. Spatiotemporal cluster analysis was conducted using the discrete Poisson statistical model, which is appropriate for count data with heterogeneous populations. This model assumes that the number of cases in each spatial unit follows a Poisson distribution proportional to the local population [18].
For each municipality in Bahia (n = 417), geographic coordinates (latitude and longitude), monthly average population, and the number of COVID-19 cases were provided. The implemented spatiotemporal scan procedure creates virtual cylinders over the map, where the circular base represents the geographic area and the height corresponds to the time interval. The base radius and temporal duration of the cylinders vary to identify potential clusters with high incidence rates [19].
The analysis considered clusters of different spatial sizes and temporal intervals, with a maximum search radius of 50% of the population at risk and a maximum temporal window of six months. The statistical criterion adopted was the Log Likelihood Ratio (LLR), and the statistical significance of the clusters was assessed using Monte Carlo tests with random simulations. The identified clusters were classified in terms of relative risk (RR), reflecting the ratio between observed and expected cases within the analyzed area and period. Only statistically significant clusters (p < 0.05) were considered for result interpretation.
Spatiotemporal analysis was performed using SaTScan software version 10.2.1. Graphs were generated using the ggplot2 package, in R software version 4.3.1.
3. Results
The spatiotemporal analysis identified a total of 33 COVID-19 clusters in Bahia between January 2020 and December 2022, of which 25 clusters were statistically significant (p < 0.05; Table 1). The most prominent cluster (Cluster 1) encompassed 164 municipalities within a geographic range of 586.3 km and was observed from May 1, 2020, to June 30, 2021. This extensive cluster, with a risk population of approximately 265.6 million (aggregated across the entire analysis window), recorded 702,720 cases compared to the 338,822 expected cases, yielding an observed-to-expected ratio of 2.07, an adjusted relative risk (RRa) of 2.8, and a Log-Likelihood Ratio (LLR) of 200,435.8 (p < 0.0001) (Table 1).
The municipalities comprising Cluster 1 span 20 regions and 6 macro-regions of the state, with more than half (61.7%) located in the South and Southwest macro-regions of Bahia. Municipalities from the East (22.8%), where the state capital and metropolitan region are situated, and the Extreme-South (11.4%) also stand out. In this cluster, the highest accumulated incidence rates per 100,000 inhabitants were recorded in the municipalities of Maracás (19,109.5), Itabuna (17,080.7), Ibirataia (16,254.5), Conceição do Almeida (18,543.6), and Itororó (16,024.1), with the first three located in the South macro-region. In the same period, the accumulated incidence of COVID-19 in the state of Bahia was 7,563.97/100,000 inhabitants (Table 1)..
Clusters identified during the early months of 2022 also revealed high risks. Cluster 2, detected from January 1 to February 28 of that year, involved 185 municipalities with a risk population of 265.9 million, presenting 102,534 observed cases versus 46,983 expected cases, resulting in an observed/expected ratio of 2.18, an RRa of 2.26, and an LLR of 25,385.5 (p < 0.0001). This cluster involved municipalities from 18 regions and 5 health macro-regions, with the majority (70.8%) located in the South and Southwest macro-regions. Municipalities with the highest accumulated incidence rates per 100,000 inhabitants in this cluster were: Maetinga (7,879.3), Aratuípe (6,340.4), Ibiassucê (5,356.5), Ibirapuã (4,645.3), and Paramirim (3,692.0), three of them belonging to the Southwest macro-region. The accumulated incidence of COVID-19 in Bahia during this same period was 1,281.25/100,000 inhabitants (Table 1).
Cluster 3, also spanning from January 1 to February 28, 2022, involved 136 municipalities from 10 regions and 5 health macro-regions, with a predominance of the Central-East and Northeast macro-regions, which together accounted for 58.1% of the total municipalities. This cluster had a risk population of 183.1 million, with 66,092 observed cases compared to 32,340 expected cases (observed/expected ratio of 2.04, RRa of 2.08, LLR = 13,821.2, p < 0.0001) (Table 1).
Other statistically significant clusters were more spatially localized and temporally brief. For example, Cluster 5, which comprised a single municipality during the period from September 1 to October 31, 2022, demonstrated the highest relative risk among isolated clusters. This cluster, with a risk population of 1,933,320, reported 1,139 cases compared to 353.1 expected cases, yielding an observed-to-expected ratio of 3.23, an annual incidence of 352.8 cases per 100,000 inhabitants, and an LLR of 548.1 (p < 0.0001). Additional statistically significant clusters (Clusters 6 to 25) exhibited relative risks ranging from 1.42 to 3.37 and LLR values between 61.9 and 1,949.1, highlighting epidemic peaks in small spatial aggregates during distinct periods. Conversely, Clusters 26 to 33 did not reach statistical significance (p-values ranging from 0.092 to 0.99) and were not further considered in the risk characterization (Table 1).
Figure 1 illustrates high-risk COVID-19 clusters in Bahia, Brazil, from 2020 to 2022, categorized by magnitude of relative risk, highlighting the centroids of 33 clusters identified during different phases of the pandemic.
Figure 2 overlays these clusters on a satellite map, providing geographic context for the affected areas. The distribution reveals concentrations of clusters in the north, northeast, and south of the state, as well as additional clusters in coastal and inland areas.
4. Discussion
The spatiotemporal analysis of the COVID-19 spread in Bahia between 2020 and 2022 revealed significant variations in the transmission of SARS-CoV-2, presenting patterns that reflect the interaction between epidemiological, sociodemographic, and healthcare infrastructure factors. The results of this study highlight the presence of 25 clusters that demonstrated important aspects in terms of geographic extent, duration, and relative risk. These findings support the hypothesis that the pandemic did not behave uniformly across the state of Bahia, as it presented as localized outbreaks or epidemic peaks, distinct both spatially and temporally, associated with different epidemic waves and the emergence of viral variants.
Cluster 1, the largest and longest lasting, encompassed 164 municipalities and remained active for fourteen months, from May 2020 to June 2021. This period corresponds to the initial phase of the pandemic, marked by the introduction and rapid spread of the virus, ineffective and inconsistent responses across federal, state, and municipal governments [20,21], and the slow implementation of the vaccination campaign during the first half of 2021 [22]. The elevated relative risk (RR = 2.8) and high observed/expected ratio (2.07) reflect the rapid and prolonged spread of the virus, possibly driven by high population density and intercity mobility. In this context, the health macroregions of Southern and Southwestern Bahia were important centers of viral transmission.
In 2020, following the occurrence of the first imported cases of COVID-19 due to air travel, the expansion of the disease in Bahia began to be influenced by population movement associated with cultural and political events throughout the year [23]. Although official June festivals, traditionally characterized by intense internal migrations, were suspended by state decree, the excessive flow of people during this period contributed to the virus's spread to smaller municipalities [24]. In the second half of the year, municipal elections also mobilized large gatherings, from electoral campaigns to the voting day, favoring new transmission waves. By the end of the year, Christmas and New Year celebrations intensified movements, family gatherings, and clandestine parties, resulting in a significant increase in cases in the first weeks of 2021. These events highlight the impact of social dynamics and mobility on the spread of COVID-19 in the state [25,26,27].
The distribution of cases in certain regions of the state may also be related to key municipalities, with higher economic activity, especially in agribusiness, which determines intense circulation of people and vehicles in surrounding areas. The existence of important federal highways connecting municipalities in the interior of Bahia to the Southeast region of the country, where COVID-19 had high incidence, is also noteworthy. These routes likely facilitated the spread of SARS-CoV-2 in these areas [28,29].
Larger urban centers were epicenters of the COVID-19 pandemic in Bahia, acting as vectors for the virus's spread to smaller municipalities. This dynamic is associated with intrinsic characteristics of these metropolitan areas, such as high population density, which plays a key role in disease transmission, especially during the community transmission phase. Evidence of this relationship has been documented in studies conducted in various geographical contexts, such as China, the United States, India, and countries in Africa, all of which emphasize the influence of human crowding on accelerating viral transmission [30,31,32,33,34].
Although this study did not directly analyze variables related to socioeconomic factors, it must be considered that SARS-CoV-2 transmission tends to be higher in areas of greater social vulnerability. In this regard, many municipalities in the interior that formed part of the epidemiologically relevant clusters in this study have high social vulnerability index (SVI) and low human development index (HDI). Even in large urban centers, there are areas marked by poverty, which increases the risk of virus spread [35,36,37].
The clusters identified in early 2022 (Clusters 2 and 3) highlight the impact of variants of concern, such as Omicron, which are characterized by greater transmissibility and partial immune escape [38]. The high observed/expected ratios and significant relative risks indicate that, even with advancements in vaccination, the circulation of new variants continued to generate localized outbreaks. These findings emphasize the importance of genomic surveillance and the adaptation of control strategies in response to viral evolution, particularly after the initiation of the COVID-19 vaccination campaign [39].
The identification of localized and temporally brief clusters, such as Cluster 5, which showed the highest relative risk (RR = 3.37), suggests the influence of specific contextual factors, such as social gatherings, inequalities in healthcare access, or the introduction of the virus into previously less affected areas, underscoring the need for differentiated approaches to pandemic control, considering the particularities of each region [40].
The geographic distribution of the clusters, with concentrations in the east, south, and southwest of the state, as well as in coastal and inland areas, reflects the heterogeneity of the Bahian territory. Densely populated urban areas, such as Salvador, Feira de Santana, Ilhéus, and Itabuna, also acted as epicenters of dissemination, while rural and hard-to-reach regions displayed distinct patterns, possibly related to lower mobility and greater underreporting. The overlap of the clusters on the satellite map provides valuable insights into the relationship between transmission dynamics and geographic features, such as proximity to highways and population density [28,29].
The methodology used, based on the Poisson model and spatiotemporal scanning analysis, proved robust for identifying patterns of transmission and risk areas. However, it is important to recognize the inherent limitations of secondary data analysis, which may be subject to underreporting and delays in data inclusion, as well as variability in data quality depending on the healthcare infrastructure of each region. Additionally, the analysis did not explicitly consider socioeconomic and behavioral factors that may have influenced transmission dynamics. Also, cluster detection with the discrete Poisson model assumes that every individual in the study area is exposed to the same baseline risk, so the expected number of cases in each geographic unit is simply proportional to its population size, and when the true risk varies systematically across units with markedly different demographic compositions, this equal-risk assumption can be violated, potentially producing biased cluster estimates [41].
The findings of this study carry implications for epidemiological surveillance and public-policy planning. First, our results show that cluster analysis can bolster the health system’s capacity to respond to emerging diseases and serve as a practical tool for managing future public-health events. Accordingly, we recommend embedding statistical techniques for detecting high-risk clusters into routine surveillance of respiratory viruses. Doing so will facilitate early detection and the rapid deployment of control measures, such as targeted vaccination drives, large-scale testing, and focused prevention and health-education initiatives.
Second, this retrospective assessment of the COVID-19 pandemic in Bahia pinpointed the areas most vulnerable to SARS-CoV-2 transmission, providing a basis for interventions that tackle the factors underlying these disparities. Finally, future investigations should integrate socioeconomic and behavioral data to yield a more comprehensive account of the forces shaping SARS-CoV-2 spread.
Author Contributions
Conceptualization, R.d.C.S., M.Y.T.I. and M.G.T.; methodology R.C.S.; software, R.C.S; validation, R.d.C.S., M.C.N.C. M.Y.T.I. and M.G.T.; formal analysis, R.d.C.S. and R.C.S.; investigation, R.d.C.S. and R.C.S.; resources, R.d.C.S.; data curation, R.d.C.S.; writing—original draft preparation, R.d.C.S. and R.C.S.; writing—review and editing, R.d.C.S., R.C.S., M.C.N.C. M.Y.T.I. and M.G.T; supervision, M.C.N.C. M.Y.T.I. and M.G.T; project administration, M.G.T. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding
Institutional Review Board Statement
This study utilized publicly available, non-identifiable data, which exempts it from the requirement of submission to an ethics committee, in accordance with the resolution of the National Health Council (Resolution No. 510, of April 7, 2016).
Informed Consent Statement
Patient consent was waived due to the use of anonymized data with unrestricted public access.
Data Availability Statement
The COVID-19 data used for this research are available for download on the website of the Bahia State Health Department, at https://dados.ba.gov.br/dataset/dados_covid and population and geographic data can be obtained at https://www.ibge.gov.br/
Conflicts of Interest
The authors declare no conflicts of interest
Abbreviations
The following abbreviations are used in this manuscript:
SVI - Social vulnerability index
HDI - Human development index
e-SUS Notifica - Flu Notification System
Sivep - Acute Respiratory Distress Syndrome Epidemiological Surveillance System
IBGE - Brazilian Institute of Geography and Statistics
LLR - Log Likelihood Ratio
RR - Relative risk
Appendix A

Scheme 1. Municipalities comprising each spatiotemporal high-risk clusters for COVID-19 identified using scan statistics with a Poisson model. Bahia, Brazil, 2020-2022.
Scheme 1. Municipalities comprising each spatiotemporal high-risk clusters for COVID-19 identified using scan statistics with a Poisson model. Bahia, Brazil, 2020-2022.
| Cluster ID | Municipalities included |
|---|---|
| 01 | Una, São José da Vitória, Santa Luzia, Buerarema, Arataca, Jussari, Itabuna, Camacan, Itapé, Canavieiras, Ilhéus, Mascote, Barro Preto, Ibicaraí, Itaju do Colônia, Pau Brasil, Itajuípe, Floresta Azul, Uruçuca, Almadina, Belmonte, Santa Cruz da Vitória, Coaraci, Potiraguá, Firmino Alves, Itororó, Itapebi, Itacaré, Itapitanga, Itapetinga, Ibicuí, Aurelino Leal, Ubaitaba, Itarantim, Santa Cruz Cabrália, Gongogi, Itagimirim, Nova Canaã, Iguaí, Maraú, Dário Meira, Eunápolis, Itagibá, Maiquinique, Ubatã, Ibirapitanga, Caatiba, Barra do Rocha, Camamu, Macarani, Itambé, Ipiaú, Ibirataia, Aiquara, Igrapiúna, Boa Nova, Itagi, Planalto, Poções, Porto Seguro, Barra do Choça, Piraí do Norte, Jitaúna, Nova Ibiá, Ribeirão do Largo, Gandu, Ituberá, Itabela, Apuarema, Guaratinga, Itamari, Nilo Peçanha, Bom Jesus da Serra, Taperoá, Jequié, Wenceslau Guimarães, Teolândia, Vitória da Conquista, Cairu, Manoel Vitorino, Presidente Tancredo Neves, Encruzilhada, Anagé, Jaguaquara, Jucuruçu, Valença, Mirante, Itamaraju, Cravolândia, Itaquara, Prado, Lafaiete Coutinho, Mutuípe, Jiquiriçá, Caetanos, Itiruçu, Belo Campo, Ubaíra, Cândido Sales, Santa Inês, Laje, Lajedo do Tabocal, Jaguaripe, Vereda, Aratuípe, Caraíbas, Irajuba, São Miguel das Matas, Maracás, Santo Antônio de Jesus, Muniz Ferreira, Amargosa, Itanhém, Tremedal, Brejões, Tanhaçu, Vera Cruz, Alcobaça, Nazaré, Varzedo, Teixeira de Freitas, Dom Macedo Costa, Aracatu, Elísio Medrado, Planaltino, Contendas do Sincorá, Nova Itarana, Maetinga, Conceição do Almeida, Salinas da Margarida, São Felipe, Itaparica, Milagres, Medeiros Neto, Maragogipe, Salvador, Iramaia, Barra da Estiva, Saubara, Piripá, Lauro de Freitas, Caravelas, Sapeaçu, Castro Alves, Santa Teresinha, Madre de Deus, Cruz das Almas, Presidente Jânio Quadros, São Félix, Marcionílio Souza, Simões Filho, Itatim, Ituaçu , Iaçu, Cachoeira, Lajedão, Muritiba, São Francisco do Conde, Candeias, Governador Mangabeira, Cabaceiras do Paraguaçu, Ibirapuã, Cordeiros, Brumado. |
| 02 | Caravelas, Nova Viçosa, Teixeira de Freitas, Ibirapuã , Alcobaça, Mucuri, Vereda, Lajedão , Prado, Medeiros Neto, Itamaraju, Itanhém, Jucuruçu, Itabela, Porto Seguro, Guaratinga, Eunápolis, Santa Cruz Cabrália, Itagimirim, Itapebi, Belmonte, Potiraguá , Itarantim, Mascote, Maiquinique , Canavieiras, Pau Brasil, Camacan, Macarani, Santa Luzia, Itapetinga, Ribeirão do Largo, Encruzilhada, Arataca, Una, Itaju do Colônia, Jussari , São José da Vitória, Itambé, Itororó, Buerarema, Itapé, Firmino Alves, Caatiba , Cândido Sales, Santa Cruz da Vitória, Ibicaraí, Floresta Azul, Itabuna, Nova Canaã, Barra do Choça, Vitória da Conquista, Barro Preto, Ilhéus, Almadina , Itajuípe, Ibicuí, Coaraci, Belo Campo, Planalto, Iguaí, Tremedal, Uruçuca, Itapitanga , Poções, Dário Meira, Piripá , Anagé, Aurelino Leal, Itacaré, Boa Nova, Cordeiros, Bom Jesus da Serra, Gongogi, Caraíbas, Ubaitaba, Itagibá, Maetinga, Itagi, Maraú, Presidente Jânio Quadros, Caetanos, Condeúba, Barra do Rocha, Ubatã, Aiquara , Ipiaú, Ibirapitanga, Mirante, Aracatu, Camamu, Ibirataia, Mortugaba , Manoel Vitorino, Jitaúna, Tanhaçu, Guajeru , Jequié, Igrapiúna, Jacaraci , Nova Ibiá, Apuarema, Piraí do Norte, Gandu, Itamari , Malhada de Pedras, Ituberá, Brumado, Nilo Peçanha, Wenceslau Guimarães, Caculé, Contendas do Sincorá, Lafaiete Coutinho, Rio do Antônio, Licínio de Almeida, Urandi, Teolândia, Taperoá, Jaguaquara, Ituaçu , Itiruçu, Ibiassucê, Cairu, Itaquara, Presidente Tancredo Neves, Barra da Estiva, Cravolândia, Lajedo do Tabocal, Maracás, Dom Basílio, Pindaí, Jiquiriçá , Valença, Mutuípe, Iramaia, Lagoa Real, Santa Inês, Ubaíra, Candiba, Livramento de Nossa Senhora, Irajuba, Laje, Planaltino, Sebastião Laranjeiras, Rio de Contas, Jussiape, Ibicoara, Caetité, Guanambi, Brejões, Jaguaripe, São Miguel das Matas, Aratuípe, Marcionílio Souza, Amargosa, Nova Itarana, Santo Antônio de Jesus, Muniz Ferreira, Varzedo, Elísio Medrado, Vera Cruz, Itaetê, Nazaré, Milagres, Dom Macedo Costa, Igaporã, Abaíra, Paramirim, Conceição do Almeida, Érico Cardoso, São Felipe, Salinas da Margarida, Iaçu, Palmas de Monte Alto, Itaparica, Iuiu , Maragogipe, Mucugê, Salvador, Santa Teresinha, Matina, Tanque Novo, Castro Alves, Itatim, Sapeaçu. |
| 03 | Santa Brígida, Paulo Afonso, Pedro Alexandre, Jeremoabo, Coronel João Sá, Sítio do Quinto, Glória, Antas, Novo Triunfo, Rodelas, Cícero Dantas, Adustina , Fátima, Canudos, Macururé, Paripiranga, Banzaê , Heliópolis, Euclides da Cunha, Ribeira do Pombal, Chorrochó, Ribeira do Amparo, Uauá, Quijingue, Cipó, Monte Santo, Tucano, Itapicuru, Abaré, Curaçá, Nova Soure, Cansanção, Olindina, Nordestina, Araci, Crisópolis, Andorinha, Rio Real, Sátiro Dias, Teofilândia, Jaguarari, Acajutiba, Itiúba, Jandaíra , Biritinga , Santaluz, Aporá, Barrocas, Queimadas, Valente, Senhor do Bonfim, Inhambupe, Conceição do Coité, Serrinha, Juazeiro, Conde, Água Fria, Retirolândia, Lamarão, Filadélfia, Esplanada, São Domingos, Ichu , Ponto Novo, Cardeal da Silva, Ouriçangas, Entre Rios, Aramari , Santanópolis , Santa Bárbara, Antônio Gonçalves, Candeal, Gavião, Pindobaçu, Nova Fátima, Irará, Alagoinhas, Capim Grosso, Tanquinho, Riachão do Jacuípe, Caldeirão Grande, São José do Jacuípe, Araçás, Pedrão, Saúde, Caém , Capela do Alto Alegre, Quixabeira, Coração de Maria, Pé de Serra, Teodoro Sampaio, Itanagra , Campo Formoso, Feira de Santana, Catu, Pojuca, Serra Preta, Várzea da Roça, Anguera , Conceição do Jacuípe, Serrolândia, Terra Nova, Sobradinho, Mirangaba, Pintadas, Amélia Rodrigues, Mata de São João, Jacobina, São Gonçalo dos Campos, Várzea do Poço, São Sebastião do Passé, Ipecaetá, Antônio Cardoso, Mairi, Dias d'Ávila, Santo Amaro, Conceição da Feira, Camaçari, Santo Estêvão, Ipirá, São Francisco do Conde, Miguel Calmon, Candeias, Baixa Grande, Governador Mangabeira, Cachoeira, Cabaceiras do Paraguaçu, Muritiba, Simões Filho, Madre de Deus, São Félix, Rafael Jambeiro, Cruz das Almas, Saubara, Piritiba, Lauro de Freitas. |
| 04 | Pilão Arcado, Campo Alegre de Lourdes, Buritirama , Remanso, Xique-Xique, Barra, Itaguaçu da Bahia, Sento Sé, Mansidão, Gentio do Ouro, Central, Jussara, Uibaí , Presidente Dutra, Santa Rita de Cássia, Morpará, São Gabriel, Irecê, Ibipeba, Casa Nova, Umburanas, Ipupiara, João Dourado, Wanderley, Ibititá , Lapão, Ibotirama, Cotegipe, América Dourada, Ourolândia, Brotas de Macaúbas, Barra do Mendes, Sobradinho, Barro Alto, Canarana, Muquém de São Francisco, Oliveira dos Brejinhos, Várzea Nova, Cafarnaum, Campo Formoso, Souto Soares, Morro do Chapéu, Cristópolis , Mirangaba, Angical, Mulungu do Morro, Brejolândia , Riachão das Neves, Bonito, Tabocas do Brejo Velho, Paratinga, Ibitiara, Seabra, Iraquara, Jacobina, Catolândia, Boquira, Antônio Gonçalves, Formosa do Rio Preto, Pindobaçu, Miguel Calmon, Juazeiro, Saúde, Utinga, Sítio do Mato, Serra Dourada, Wagner, Ibipitanga, Tapiramutá, Baianópolis, Palmeiras, Lençóis, Piritiba, Senhor do Bonfim, Novo Horizonte, Caém , Jaguarari, Filadélfia, Caldeirão Grande, Boninal , Ponto Novo, Barreiras, Macaúbas, Serrolândia, Várzea do Poço, Santana, Mundo Novo, Lajedinho, Andorinha, Quixabeira, Rio do Pires, Canápolis , Piatã, Bom Jesus da Lapa, Itiúba, Andaraí, Ruy Barbosa, Caturama, Capim Grosso, Mairi, Botuporã, Várzea da Roça, Ibiquera , Nova Redenção, Santa Maria da Vitória, Mucugê, São José do Jacuípe, Queimadas, Curaçá, Baixa Grande, Macajuba, Serra do Ramalho, Érico Cardoso, Abaíra, Tanque Novo, Luís Eduardo Magalhães, Uauá, Paramirim, Monte Santo, Gavião, Riacho de Santana, Capela do Alto Alegre, São Desidério, Cansanção, São Félix do Coribe, Boa Vista do Tupim, Pintadas, Itaetê, Nordestina, Itaberaba, São Domingos, Santaluz, Nova Fátima, Ibicoara, Jussiape, Rio de Contas, Matina, Valente, Igaporã, Pé de Serra, Abaré, Retirolândia, Marcionílio Souza, Chorrochó, Ipirá, Livramento de Nossa Senhora, Caetité, Coribe, Riachão do Jacuípe, Canudos, Iaçu, Quijingue, Iramaia, Carinhanha, Dom Basílio, Conceição do Coité, Correntina, Lagoa Real, Barra da Estiva, Euclides da Cunha, Araci, Palmas de Monte Alto, Ituaçu , Guanambi, Planaltino, Serra Preta, Macururé, Barrocas, Malhada, Ichu , Rafael Jambeiro, Feira da Mata, Itatim, Candeal, Nova Itarana, Maracás, Contendas do Sincorá, Teofilândia, Milagres, Tucano, Ibiassucê, Ipecaetá, Serrinha, Brumado, Tanquinho, Irajuba, Candiba, Santa Teresinha, Rio do Antônio, Anguera , Lajedo do Tabocal, Banzaê , Brejões, Rodelas, Iuiu , Pindaí, Santa Bárbara, Lamarão, Santo Estêvão, Malhada de Pedras, Itiruçu, Biritinga , Tanhaçu, Jeremoabo, Caculé, Antônio Cardoso, Feira de Santana, Ribeira do Pombal, Lafaiete Coutinho, Sebastião Laranjeiras, Amargosa, Elísio Medrado, Castro Alves, Santa Inês, Novo Triunfo, Cícero Dantas, Santanópolis , Cabaceiras do Paraguaçu, Licínio de Almeida, Jaborandi, Cipó, Itaquara, Nova Soure, Glória, Guajeru , Aracatu, Água Fria, Ubaíra, Varzedo, Sapeaçu, Jaguaquara, Sátiro Dias, Cravolândia, Governador Mangabeira, São Miguel das Matas, Muritiba, Irará, Cruz das Almas, Conceição do Almeida, Conceição da Feira, Urandi, São Gonçalo dos Campos, Mirante, Ribeira do Amparo, Manoel Vitorino, Antas, Paulo Afonso, Heliópolis, Coração de Maria, Jiquiriçá , Caetanos, Ouriçangas, Dom Macedo Costa, São Félix, Mutuípe, Jequié, Jacaraci , Santo Antônio de Jesus, São Felipe, Laje, Fátima, Pedrão, Santa Brígida, Presidente Jânio Quadros, Conceição do Jacuípe, Olindina, Sítio do Quinto, Maetinga, Cachoeira, Cocos |
| 05 | Caetité |
| 06 | Sobradinho |
| 07 | Pojuca |
| 08 | Pé de Serra, Riachão do Jacuípe, Nova Fátima |
| 09 | Lagoa Real, Ibiassucê, Caetité |
| 10 | Santa Cruz Cabrália |
| 11 | São Francisco do Conde, Madre de Deus, Candeias |
| 12 | Madre de Deus, São Francisco do Conde |
| 13 | Maiquinique |
| 14 | Santa Bárbara |
| 15 | Itapetinga, Itororó |
| 16 | Porto Seguro |
| 17 | Ibipitanga |
| 18 | Remanso |
| 19 | Bonito |
| 20 | Iuiu |
| 21 | Vereda |
| 22 | Cotegipe |
| 23 | Itanagra |
| 24 | Ituberá, Nilo Peçanha |
| 25 | Esplanada, Cardeal da Silva |
| 26 | Macajuba |
| 27 | Várzea da Roça |
| 28 | Presidente Dutra |
| 29 | Catolândia |
| 30 | Catu |
| 31 | Baixa Grande |
| 32 | Quixabeira |
| 33 | São Domingos |
References
- Morgan OW, Aguilera X, Ammon A, Amuasi J, Fall IS, Frieden T, et al. Disease surveillance for the COVID-19 era: time for bold changes. Lancet. (2021); 397(10292):2317-2319. [CrossRef]
- Li CX, Noreen S, Zhang LX, Saeed M, Wu PF, Li JH, et al. A critical analysis of SARS-CoV-2 (COVID-19) complexities, emerging variants, and therapeutic interventions and vaccination strategies. Biomedicine & Pharmacotherapy; (2022); 146, 112550. [CrossRef]
- Raymundo CE, Oliveira MC, Eleuterio TdA, André SR, da Silva MG, Queiroz ERdS, et al. Spatial analysis of COVID-19 incidence and the sociodemographic context in Brazil. PLoS ONE; (2021). 16(3): e0247794. [CrossRef]
- Sott MK, Bender MS, da Silva Baum K. Covid-19 Outbreak in Brazil: Health, Social, Political, and Economic Implications. International Journal of Health Services. (2022); 52(4):442-454. [CrossRef]
- Martins JP, Siqueira BA, Sansone NMS & Marson FAL. COVID-19 in Brazil: a three-year update. Diagnostic Microbiology and Infectious Disease, 116074 (2023). [CrossRef]
- Castro MC, Kim S, Barberia L, Ribeiro AF, Gurzenda S, Ribeiro KB, Abbott E, Blossom J, Rache B, Singer BH. Spatiotemporal pattern of COVID-19 spread in Brazil. 2021, Science 372:821–826. [CrossRef]
- Oliveira JF, Jorge DCP, Veiga RV, et al. Mathematical modeling of COVID-19 in 14.8 million individuals in Bahia, Brazil. Nat Commun 12, 333 (2021). [CrossRef]
- Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde e Ambiente. Boletim Epidemiológico Especial. Doença pelo Coronavírus COVID-19 N.º 147, de 28/01/2022. https://www.gov.br/saude/pt-br/media/pdf/2022/boletim_epidemiologico_covid_61 1.pdf.
- Campbell F, Archer B, Laurenson-Schafer H, et al. (2021). Increased transmissibility and global spread of SARS-CoV-2 variants of concern as at June 2021. Eurosurveillance, 26(24), 2100509. [CrossRef]
- Faria NR, Mellan TA, Whittaker C, et al. (2021). Genomics and epidemiology of the P.1 SARS-CoV-2 lineage in Manaus, Brazil. Science, 372(6544), 815–821. [CrossRef]
- Bahia. Boletim Epidemiológico Covid-19 N.º 976 - 31/12/2022. Secretaria de Saúde. Bahia, 31 dezembro 2022. Disponível em: https://www.saude.ba.gov.br/wp-content/uploads/2022/12/Boletim-Infografico-31-12-2022.pdf.
- Martin A, Markhvida M, Hallegatte S et al. Socio-Economic Impacts of COVID-19 on Household Consumption and Poverty. EconDisCliCha 4, 453–479 (2020). [CrossRef]
- Kan Z, Kwan MP, Wong MS, Huang J, Liu D. Identifying the space-time patterns of COVID-19 risk and their associations with different built environment features in Hong Kong. Sci. Total Environ. (2021), 772, 145379.
- IBGE. Instituto Brasileiro de Geografia e Estatística. Censo Demográfico 2022. Rio de Janeiro: IBGE; 2022. Disponível em: https://censo2022.ibge.gov.br/sobre/conhecendo-o-brasil.html.
- LEAL, MB; et al. A experiência do observatório baiano de regionalização: uma ferramenta para avaliação e qualificação da gestão regionalizada do SUS na Bahia. RECIIS - Revista Eletrônica de Comunicação, Informação e Inovação em Saúde, Rio de Janeiro, v. 6, n. 2, p. 1-7, ago. 2012. [CrossRef]
- Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Análise Epidemiológica e Vigilância de Doenças Não Transmissíveis. e-SUS Notifica: Manual de Instruções. Brasília/DF, 2022. http://bvsms.saude.gov.br/bvs/publicacoes/esus_notifica_manual_instrucoes.pdf.
- Bahia. Secretaria Estadual de Saúde da Bahia. Diretoria de Vigilância Epidemiológica. Guia Rápido Sivep-Gripe. Maio, 2021. https://www.saude.ba.gov.br/wp-content/uploads/2021/05/GUIA-RAPIDO-SIVEP-GRIPE-atualizado-em-maio_2021.pdf.
- Cruz OG & Freitas, LP. Estudos Ecológicos (2021). Cluster Espaço-Temporal https://ogcruz.github.io/Curso_eco_2021/an%C3%A1lise-espa%C3%A7o-temporal.html#cluster-espa%C3%A7o-temporal.
- Kulldorff, M. (1997). A spatial scan statistic. Communications in Statistics - Theory and Methods, 26(6), 1481–1496. [CrossRef]
- Romão GA & Brito IS (2022). Falhas das funções de governança na resposta à covid-19: o caso do isolamento social no Brasil. Multitemas, 27(66), 95–121. [CrossRef]
- Rocha MM, Almeida PEG, Tenório GG, Artuzo RM & Mendes HDM. (2022). As respostas dos governos municipais à Covid-19 no Brasil: a política de distanciamento social nas cidades médias nos primeiros meses da pandemia. Teoria e Cultura, 17(1). [CrossRef]
- Maciel E, Fernandez M, Calife K, Garrett D, Domingues C, Kerr L, et al. A campanha de vacinação contra o SARS-CoV-2 no Brasil e a invisibilidade das evidências científicas. Ciênc saúde coletiva. 2022 - Mar; 27(3): 951–6. [CrossRef]
- GeoCombate COVID-19 Bahia. Nota Técnica 05 - Análise da Interiorização da COVID-19 na Bahia [Internet]. Salvador: Secretaria da Saúde do Estado da Bahia; 2020. Acessado em 08/02/2025. Disponível em: https://covid19.estudoscolaborativos.sei.ba.gov.br/wp-content/uploads/2021/03/Interiorizacao-da-COVID-19-na-Bahia.pdf.
- Bahia. Diário Oficial do Estado da Bahia. Decreto nº 19.722 de 22 de maio de 2020. Estabelece medidas complementares de prevenção ao contágio e de enfrentamento da propagação do novo coronavírus, causador da COVID-19, na forma que indica. 23 de maio de 2020. Ano CIV. Edição n° 22.908, página 5.
- Fortuna DBS & Fortuna, JL. (2020). Perfil epidemiológico dos casos de COVID-19 no município de Teixeira de Freitas-BA no período de julho a setembro de 2020. Brazilian Journal of Health Review, 3(6), 16278-16294. Acesso em: 09/02/2025. Disponível em: https://ojs.brazilianjournals.com.br/ojs/index.php/BJHR/article/view/19888.
- Aguiar, S. (2020). COVID-19: A doença dos espaços de fluxos. Geographia, 22(48), p. 51-74. [CrossRef]
- Bahia. Superintendência de Estudos Econômicos e Sociais da Bahia. Panorama da COVID-19 na Bahia em 2020. Salvador: Disponível em: https://www.sei.ba.gov.br/index.php?option=com_content&view=article&id=1234.
- Souza SS, Costa EL, Calazans MIP, Antônio MMP, Dias CRC, Cardoso JP. Análise espacial dos casos de COVID-19 notificados no estado da Bahia, Brasil. Cad Saúde Colet, 2022; 30(4) 572-583. [CrossRef]
- Silva RJ, Silva K, Mattos J. Análise espacial sobre a dispersão da covid-19 no Estado da Bahia. SciELO Prepr. 2020. [CrossRef]
- Zhou C, Su F, Pei T, Zhang U, Du Y, Luo B, et al. COVID-19: challenges to GIS with Big Data. Geogr Sustainability. 2020;1(1):77-87. [CrossRef]
- Sun F, Matthews S, Yang C, Hu MH. A spatial analysis of the COVID-19 period prevalence in U.S. counties through June 28, 2020: where geography matters? Ann Epidemiol. 2020;52:54-59.e1. [CrossRef]
- Murugesan B, Karuppannan S, Mengistie AT, Ranganathan M, Gopalakrishnan G. Distribution and trend analysis of COVID-19 in India: geospatial approach. J Geog Stud. 2020;4(1):1-9. [CrossRef]
- Monié, FA. África subsaariana diante da pandemia de Coronavírus/COVID-19: difusão espacial, impactos e desafios. Espaço e Economia. 2020;18. [CrossRef]
- Sodoré AA, Monié F, Pouya LP. Distribuição geográfica e difusão espacial do coronavírus/Covid-19 no Burquina Fasso (África Ocidental). Rev Tamoios. 2020;16(1):167-87. [CrossRef]
- Castro RR, Santos RSC, Sousa GJB, et al. Spatial dynamics of the COVID-19 pandemic in Brazil. Epidemiology and Infection. 2021;149:e60. [CrossRef]
- The Lancet. Redefining vulnerability in the era of COVID-19. Lancet. 2020 Apr 4;395(10230):1089. [CrossRef]
- Maciel JAC, Castro-Silva II, Farias MR de. Análise inicial da correlação espacial entre a incidência de COVID-19 e o desenvolvimento humano nos municípios do estado do Ceará no Brasil. Rev bras epidemiol [Internet]. 2020;23:e200057. [CrossRef]
- Dhama K, Nainu F, Frediansyah A, Yatoo MI, Mohapatra RK, Chakraborty S, Zhou H, Islam MR, Mamada SS, Kusuma HI et al. Global emerging Omicron variant of SARS-CoV-2: Impacts, challenges and strategies. J. Infect. Public Health 2022, 16, 4–14. [CrossRef]
- Ling-Hu, T.; Rios-Guzman, E.; Lorenzo-Redondo, R.; Ozer, E.A.; Hultquist, J.F. Challenges and Opportunities for Global Genomic Surveillance Strategies in the COVID-19 Era. Viruses 2022, 14, 2532. [Google Scholar] [CrossRef] [PubMed]
- Andrade LA, da Paz WS, Lima AGCF, Araújo DC, Duque AM, Peixoto MVS, Góes MAO, Souza CDF, Ribeiro CJN, Lima SVMA, Santos MB, Santos AD. Spatiotemporal Pattern of COVID-19-Related Mortality during the First Year of the Pandemic in Brazil: A Population-based Study in a Region of High Social Vulnerability. Am J Trop Med Hyg. 2021 Nov 10;106(1):132-141. [CrossRef]
- Xu F, Beard K. A comparison of prospective space-time scan statistics and spatiotemporal event sequence based clustering for COVID-19 surveillance. PLoS One. 2021 Jun 10;16(6):e0252990. [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Centroids of spatiotemporal high-risk clusters for COVID-19 identified using scan statistics with a Poisson model, according to the magnitude of relative risk. Bahia, Brazil, 2020-2022.
Figure 1.
Centroids of spatiotemporal high-risk clusters for COVID-19 identified using scan statistics with a Poisson model, according to the magnitude of relative risk. Bahia, Brazil, 2020-2022.
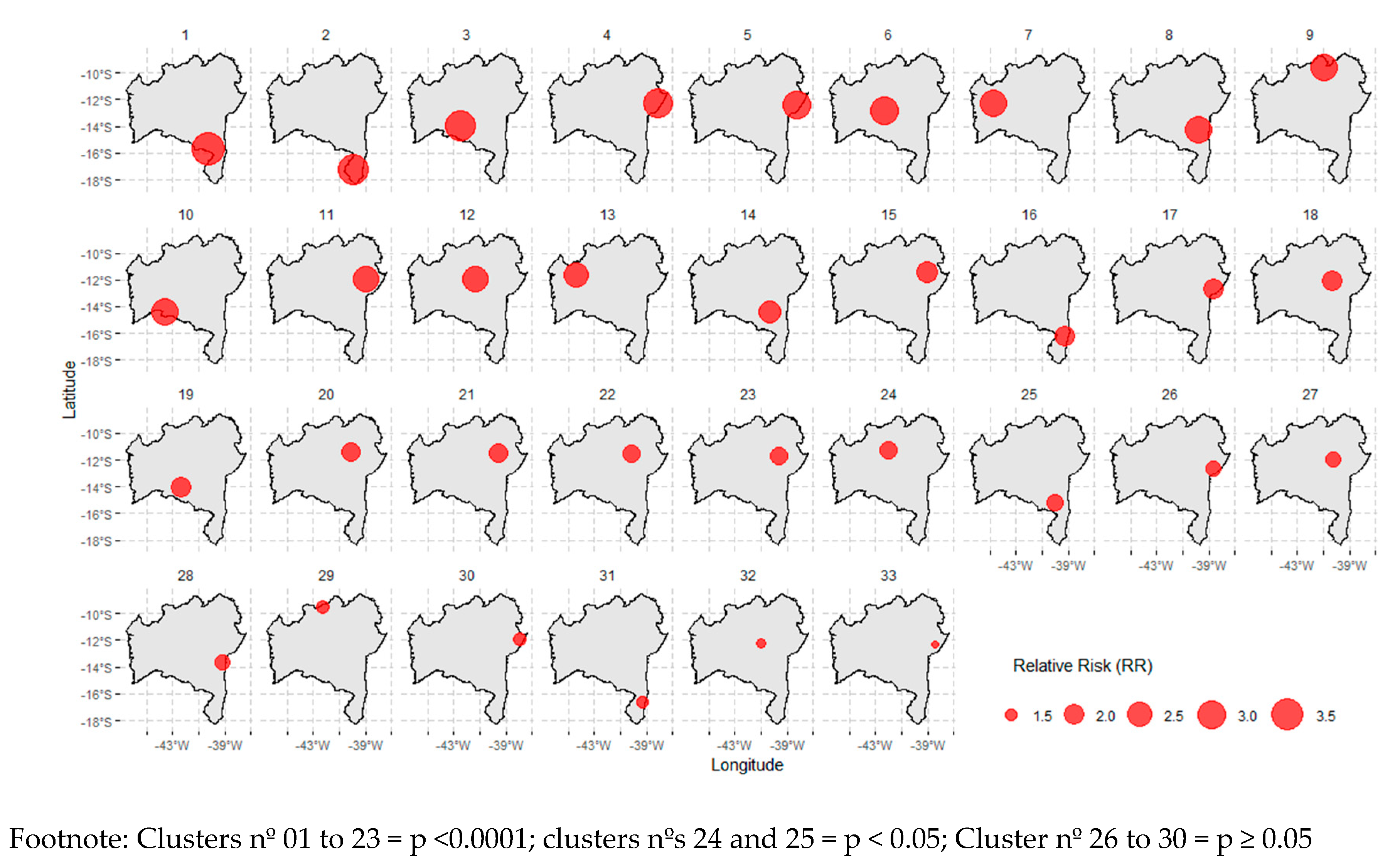
Figure 2.
Overlap of the spatiotemporal high-risk clusters for COVID-19, identified using scan statistics with a Poisson model. Bahia, Brazil, 2020-2022.
Figure 2.
Overlap of the spatiotemporal high-risk clusters for COVID-19, identified using scan statistics with a Poisson model. Bahia, Brazil, 2020-2022.
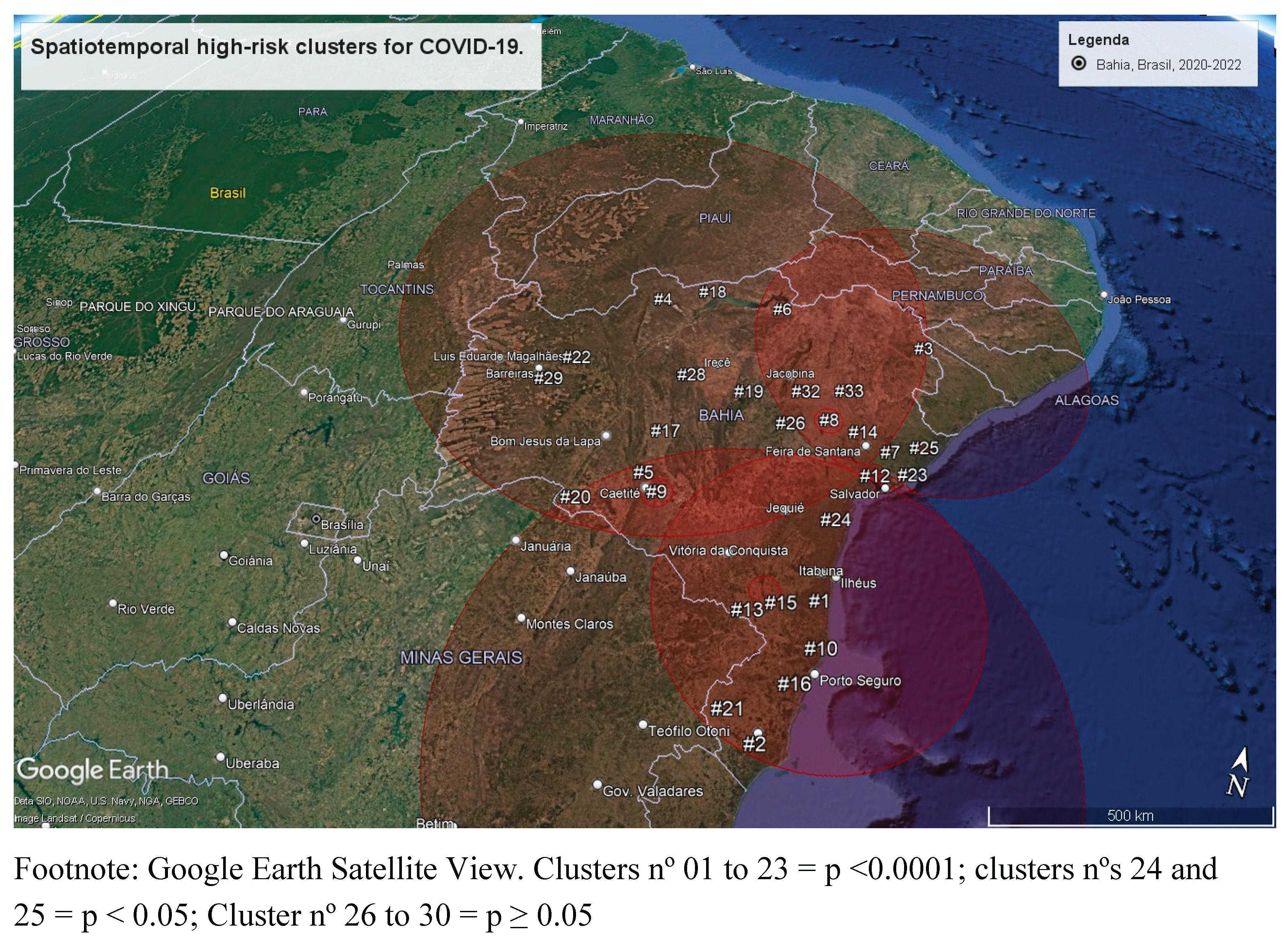
Table 1.
Spatiotemporal high-risk clusters for COVID-19 identified using scan statistics with a Poisson model. Bahia, Brazil, 2020-2022.
Table 1.
Spatiotemporal high-risk clusters for COVID-19 identified using scan statistics with a Poisson model. Bahia, Brazil, 2020-2022.
| Cluster ID | Number of cities involved | Span (km) | Time frame | Population at risk | Number of cases | Expected cases | Annual cases per 100000 | RRa | LLRb | p |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 164 | 586.3 | 2020/5/1 - 2021/6/30 | 265617828 | 702720 | 338821.52 | 226.8 | 2.8 | 200435.8 | <0.0001 |
| 2 | 185 | 596.8 | 2022/1/1 - 2022/2/28 | 265939620 | 102534 | 46982.8 | 238.7 | 2.26 | 25385.5 | <0.0001 |
| 3 | 136 | 460.7 | 2022/1/1 - 2022/2/28 | 183056436 | 66092 | 32340.1 | 223.5 | 2.08 | 13821.2 | <0.0001 |
| 4 | 270 | 940.7 | 2022/7/1 - 2022/7/31 | 260730168 | 34459 | 24202.3 | 155.7 | 1.43 | 1949.1 | <0.0001 |
| 5 | 1 | - | 2022/9/1 - 2022/10/31 | 1933320 | 1139 | 353.1 | 352.8 | 3.23 | 548.1 | <0.0001 |
| 6 | 1 | - | 2021/10/1 - 2021/11/30 | 935196 | 477 | 170.8 | 305.4 | 2.79 | 183.7 | <0.0001 |
| 7 | 1 | - | 2021/8/1 - 2021/8/31 | 1228764 | 340 | 114.1 | 326 | 2.98 | 145.4 | <0.0001 |
| 8 | 3 | 30.5 | 2021/8/1 - 2021/9/30 | 2045316 | 687 | 373.6 | 201.1 | 1.84 | 105.1 | <0.0001 |
| 9 | 3 | 42.4 | 2021/8/1 - 2021/8/31 | 2851284 | 523 | 264.7 | 216.1 | 1.98 | 97.9 | <0.0001 |
| 10 | 1 | - | 2021/10/1 - 2021/11/30 | 1079256 | 399 | 197.1 | 221.4 | 2.02 | 79.5 | <0.0001 |
| 11 | 3 | 18.8 | 2022/11/1 - 2022/11/30 | 4898124 | 729 | 440 | 181.2 | 1.66 | 79.1 | <0.0001 |
| 12 | 2 | 10.2 | 2022/7/1 - 2022/7/31 | 2115732 | 392 | 196.4 | 218.3 | 2.00 | 75.3 | <0.0001 |
| 13 | 1 | - | 2021/11/1 - 2021/11/30 | 327204 | 111 | 29.39 | 413.0 | 3.78 | 65.9 | <0.0001 |
| 14 | 1 | - | 2021/11/1 - 2021/11/30 | 770568 | 181 | 69.22 | 286.0 | 2.61 | 62.2 | <0.0001 |
| 15 | 2 | 28.36 | 2021/11/1 - 2021/11/30 | 3134412 | 488 | 281.57 | 189.6 | 1.73 | 61.9 | <0.0001 |
| 16 | 1 | - | 2021/11/1 - 2021/11/30 | 6109620 | 828 | 548.83 | 165.0 | 1.51 | 61.3 | <0.0001 |
| 17 | 1 | - | 2021/8/1 - 2021/8/31 | 519600 | 142 | 48.23 | 322.0 | 2.94 | 59.6 | <0.0001 |
| 18 | 1 | - | 2021/9/1 - 2021/11/30 | 1518444 | 642 | 413.76 | 169.7 | 1.55 | 53.8 | <0.0001 |
| 19 | 1 | - | 2021/9/1 - 2021/9/30 | 583620 | 135 | 52.43 | 281.6 | 2.58 | 45.1 | <0.0001 |
| 20 | 1 | - | 2021/8/1 - 2021/8/31 | 409716 | 103 | 38.03 | 296.2 | 2.71 | 37.7 | <0.0001 |
| 21 | 1 | - | 2021/8/1 - 2021/8/31 | 226656 | 71 | 21.04 | 369.1 | 3.37 | 36.4 | <0.0001 |
| 22 | 1 | - | 2022/4/1 - 2022/4/30 | 490020 | 110 | 44.02 | 273.3 | 2.50 | 34.8 | <0.0001 |
| 23 | 1 | - | 2022/7/1 - 2022/7/31 | 222168 | 66 | 20.62 | 350.0 | 3.20 | 31.4 | <0.0001 |
| 24 | 2 | 10.16 | 2022/11/1 - 2022/11/30 | 1297692 | 193 | 116.57 | 181.1 | 1.66 | 20.9 | <0.001 |
| 25 | 2 | 13.70 | 2022/7/1 - 2022/7/31 | 1547040 | 221 | 143.60 | 168.3 | 1.54 | 17.9 | 0.003 |
| 26 | 1 | - | 2021/11/1 - 2021/11/30 | 396072 | 71 | 35.58 | 218.2 | 2.00 | 13.6 | 0.092 |
| 27 | 1 | - | 2022/11/1 - 2022/11/30 | 512616 | 85 | 46.05 | 201.9 | 1.85 | 13.2 | 0.132 |
| 28 | 1 | - | 2021/8/1 - 2021/8/31 | 560880 | 93 | 52.06 | 195.4 | 1.79 | 13.1 | 0.146 |
| 29 | 1 | - | 2022/11/1 - 2022/11/30 | 126840 | 32 | 11.39 | 307.2 | 2.81 | 12.4 | 0.233 |
| 30 | 1 | - | 2022/7/1 - 2022/7/31 | 1832664 | 239 | 170.12 | 153.7 | 1.40 | 12.4 | 0.243 |
| 31 | 1 | - | 2021/9/1 - 2021/9/30 | 692388 | 103 | 62.20 | 181.1 | 1.66 | 11.2 | 0.536 |
| 32 | 1 | - | 2022/11/1 - 2022/11/30 | 349368 | 61 | 31.38 | 212.6 | 1.94 | 10.9 | 0.613 |
| 33 | 1 | - | 2021/11/1 - 2021/11/30 | 316968 | 54 | 28.47 | 207.4 | 1.90 | 9.1 | 0.99 |
a Relative Risk; b Log Likelihood Ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



