
Submitted:
05 June 2025
Posted:
11 June 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The selection of resin-based restorative materials is a complex clinical decision influenced by practitioner characteristics, purchasing behaviors, and external factors. This pilot study aimed to investigate how professional background, procurement practices, and the COVID-19 pandemic have shaped dentists’ preferences in material selection. A structured questionnaire was distributed digitally to clinicians at the Department of Dentistry, National and Kapodistrian University of Athens, collecting data on selection criteria, purchasing patterns, and responsiveness to regulatory, environmental, and pandemic-related influences. The results showed that clinical performance factors, such as handling properties, durability, and biocompatibility, were consistently prioritized over economic or marketing aspects. Age and educational background significantly influenced preferences: older and more experienced practitioners placed greater emphasis on brand reputation and regulatory compliance, while younger or internationally trained dentists gave more weight to cost and availability. The pandemic modestly influenced preferences toward materials that support streamlined workflows and prompted greater interest in new products, especially among experienced clinicians. Environmental considerations were secondary but more prominent among female respondents. These findings emphasize the multifactorial nature of restorative material selection and suggest that product development and educational strategies should be tailored to the evolving needs of diverse dental practitioners.
Keywords:
resin-based restorative materials
; dental material selection
; purchasing behavior
; clinical decision-making
; COVID-19 pandemic
; environmental sustainability
; dentist preferences
; dental education
; material performance
; dental practice trends
1. Introduction
Resin-based restorative materials are essential in modern dentistry, widely used for both restorative and esthetic treatments due to their superior mechanical properties, biocompatibility, and ability to blend with natural tooth structures [1,2,3]. These materials have increasingly replaced traditional options such as dental amalgam, offering advantages like enhanced esthetics, reduced invasiveness, and improved patient satisfaction [2,3,4]. The development of new technologies, including bulk-fill composites, flowable resins, and nanocomposites, has expanded the range of clinical indications and improved handling, wear resistance, and polymerization properties [5,6,7,8,9]. As a result, these materials support faster procedures and greater long-term success, making them a cornerstone of contemporary restorative practice [7,8,9,10,11,12].
Despite their benefits, the ever-expanding array of resin-based materials can present a challenge for practitioners [1,7]. Dentists must carefully select materials based on a combination of factors, including ease of handling, polymerization behavior, esthetics, and physical performance, often balancing these with the clinical situation, such as cavity type, location, and expected longevity of the restoration [1,7,13,14,15]. Additionally, clinicians increasingly consider how materials comply with international quality standards, such as ISO 4049:2019, which define essential performance characteristics, including flexural strength and water sorption [11,16,17].
As has already been mentioned, dental material selection is not purely technical; individual practitioner characteristics also play a significant role [18,19,20]. Research has shown that factors such as age, years of clinical experience, and educational background influence the preferences and confidence levels of dentists when choosing restorative materials [21]. Experienced clinicians may prioritize brand reputation and regulatory compliance, while younger or internationally trained professionals may emphasize affordability or ease of access [22]. Moreover, external influences, such as advertising, brand perception, and economic constraints, can shape product selection [23]. Marketing strategies that build strong brand identities can influence perceived quality and trust, while financial considerations often require a balance between cost-effectiveness and expected material longevity [14,24,25,26]. A well-known brand may instill confidence and simplify the decision-making process, especially when practitioners lack the time or resources to assess new materials thoroughly [27,28,29]. Also, environmental sustainability is another factor that is becoming increasingly relevant in dentistry [30,31,32,33]. There is growing interest in green procurement, recyclable packaging, and sustainable product development, driven by both regulatory trends and heightened ecological awareness among practitioners and patients alike [34,35,36]. Studies indicate that these concerns are particularly influential among female and younger dentists, suggesting a generational shift in ethical and professional priorities [33,35,37,38,39]. The COVID-19 pandemic further complicated clinical decision-making [40]. The disruption of supply chains, increased emphasis on infection control, and financial pressures forced many dental professionals to reconsider their material choices, often favoring products that support streamlined workflows, require fewer appointments, or are more readily available [41]. These changes are likely to leave a lasting impact on how restorative materials are selected and valued [42].
Despite the substantial research into dental materials, there remains a noticeable gap in the literature concerning how clinicians specifically make decisions about resin-based restorative materials in real-world contexts. Understanding this process is vital, as the dentist’s material choice can directly impact treatment outcomes, patient satisfaction, and long-term restoration success. Addressing this gap requires a holistic view of the material selection process, one that considers not just the clinical and mechanical factors, but also the human, environmental, and contextual dimensions [33]. To this end, the present pilot study aims to explore the key factors influencing dentists’ selection of resin-based restorative materials. To guide this investigation, the study focuses on understanding several key dimensions of clinical decision-making related to resin-based restorative materials. Specifically, it explores which clinical and material-specific criteria dentists prioritize during material selection, such as handling properties, durability, and esthetics. It also examines how practitioner characteristics, including age, years of experience, and educational background, influence material preferences and decision-making behavior. Furthermore, the study investigates the extent to which external factors, such as cost, brand perception, marketing, and adherence to regulatory standards, shape the selection process. Particular attention is then given to how the COVID-19 pandemic has impacted dentists’ purchasing behaviors and material preferences, especially in response to workflow disruptions and economic pressures. Lastly, the study assesses the role of environmental and sustainability considerations in restorative material choice, reflecting the profession’s growing attention to eco-conscious clinical practice.
2. Materials and Methods
2.1. Study Design and Sample
This cross-sectional study employed a questionnaire-based research design, a widely accepted method in healthcare research for collecting large volumes of data efficiently and systematically [33,43]. The structured questionnaire used in this study was carefully designed to gather both quantitative and qualitative data, allowing for a comprehensive assessment of the impact of external factors, such as the COVID-19 pandemic, on purchasing behaviors and material preferences; it also aimed to examine broader trends in product selection, environmental concerns, and the factors influencing dentists' final decisions [14,31,34,44,45]. The study adheres to the principles of ethical conduct in research involving human subjects and is conducted following the guidelines outlined in the Declaration of Helsinki, and was approved by the Ethics and Research Committee of the Department of Dentistry (16.05.2024/44982). The study sample consisted of dental clinicians currently enrolled in the Department of Dentistry at the National and Kapodistrian University of Athens, Greece. The study was conducted between October 2023 and January 2025. Exclusion criteria included dental students, individuals from non-dental disciplines, and those who did not fulfill informed consent.
2.2. Questionnaire Design
A structured questionnaire was used as the primary data collection tool for this study [33,46]. It was developed based on relevant literature, expert input from restorative dentistry faculty, and pilot testing to ensure clarity and relevance [47]. The questionnaire included five main sections: (1) demographic data (e.g., age, gender); (2) professional characteristics (e.g., clinical experience, postgraduate training, employment setting); (3) knowledge of resin-based materials [12,43,48,49,50,51,52,53,54,55,56]; (4) material selection preferences for anterior and posterior restorations [57,58]; and (5) influencing factors, including clinical, economic, environmental, and COVID-19-related considerations [14,23,24,28,29,35,37,38,39,44,45,59]. A preliminary pilot test was conducted with a small group of dentists (excluded from the final sample) to evaluate the clarity, language, and structure of the questionnaire [33,60]. Based on their feedback, revisions were made to improve wording, eliminate ambiguities, and refine response formats. The finalized questionnaire included closed-ended, multiple-choice, and Likert-scale items, organized into four sections: demographics, professional characteristics, knowledge of resin materials, and selection preferences for anterior and posterior restorations. Content validity was confirmed by a panel of three restorative dentistry experts from the National and Kapodistrian University of Athens, ensuring alignment with clinical practice and academic standards. Internal consistency was assessed using Cronbach’s alpha, with values above 0.70 considered acceptable [61,62].
The questionnaire included 23 closed-ended and 5 open-ended questions, focusing on the decision-making process for selecting resin-based restorative materials based on individual preferences and clinical scenarios. It was organized into five sections: Part A (Q1–Q5) covered demographics; Part B (Q6–Q12) addressed personal experience with restorative materials; Part C (Q13–Q18) examined material specifications and selection criteria for anterior and posterior teeth; Part D (Q19–Q23) explored procurement-related influencing factors; and Part E (Q24–Q28) consisted of open-ended questions for qualitative insights.
To minimize bias, several measures were implemented during the study design and data collection phases as suggested elsewhere [63]. A diverse sample of dentists from the Athens Dental School was included to reduce selection bias [63]. Anonymity and confidentiality were ensured to limit response bias [64], while neutral wording in the questionnaire helped prevent measurement bias [64]. Participation was voluntary, and respondents were assured there were no right or wrong answers to reduce social desirability bias [27,65]. Data was cleaned for inconsistencies and missing values, and non-parametric analyses were used when normality assumptions were unmet [66,67]. These strategies aimed to strengthen the reliability and validity of our findings [68].
2.3. Data Collection and Processing
Data was collected via both printed and electronic questionnaires. Statistical analyses were conducted using IBM SPSS v29. After data cleaning and checks for normality and missing values, descriptive statistics (means, SDs, frequencies, percentages) were used to summarize responses. Spearman correlations assessed associations between professional characteristics and selection factors, while Mann-Whitney tests compared subgroups (e.g., gender, employment setting). Categorical variables were dummy-coded, and significance was set at p < .05, with stronger associations at p < .01.
3. Results
The sample included a balanced group of dentists, with females representing 55.2% and 65.5% being under 45 years old, indicating a relatively young workforce. Most participants (82.8%) had graduated from domestic dental schools. About half (50.6%) had less than five years of clinical experience, and 33.3% had pursued further specialization. In terms of employment, 55.2% worked in private clinics and 21.8% in public settings. Procurement practices varied: 31.0% purchased materials more than twice annually, while another 31.0% were not involved in purchasing. Additionally, 63.9% reported performing fewer than 20 composite resin restorations per week.
3.1. Material Choice for Posterior Restorations
Figure 1 presents mean scores and confidence intervals for factors influencing resin material selection in conservative restorations. Product quality (M = 4.29), ease of handling (M = 4.18), and patient safety (M = 4.18) were rated highest, highlighting the emphasis on durability, usability, and biocompatibility. Material properties like durability and biocompatibility also scored highly (M = 4.07), while compliance with standards was moderately important (M = 3.68). In contrast, the cost (M = 3.10) and market availability (M = 3.30) were less influential. Brand reputation (M = 3.56) had a moderate impact, and environmental concerns (M = 3.39) were considered but ranked lower than clinical factors.
Related findings from correlation analysis (data not shown) indicate that frequent purchasers are more likely to prefer packable composites, and foreign-trained dentists show a modest preference for both packable and bulk-fill resins. No significant associations were found for amalgam use, reinforcing its limited role in current clinical practice.
3.2. Selection of Restorative Materials Based on Clinical Properties
Table 1 presents dentists' preferences regarding resin materials with specific physical properties. For esthetic restorations, compliance with ISO specifications (48.3%) was the top priority, followed by ease of handling (26.4%), while brand name (18.4%) and storage potential (10.3%) were less influential. Notably, 26.4% did not specify a preference, suggesting uncertainty or limited emphasis on water absorption. Regarding flexural strength, 59.8% would not use low-strength materials in posterior teeth, and 54.0% rejected materials with inferior mechanical properties. Few were willing to compromise strength for color stability (16.1%), faster polymerization (9.2%), or higher radiopacity (2.3%). Only 2.3% did not consider flexural strength important, highlighting its critical role in material selection. A small portion (5.7%) did not respond.
3.3. Impact of Professional Characteristics on Selection Priorities
Figure 2 compares selection priorities between dentists aged ≤45 and those >45. Older dentists consistently rated all three key factors, material properties, ease of handling, and brand reputation, higher than their younger peers. The largest gap was in brand reputation, suggesting older clinicians place more trust in established manufacturers. While both groups prioritized material performance and handling, older dentists emphasized these more strongly, reflecting greater clinical experience and familiarity with long-term outcomes.
3.4. Influence of Educational Background on Selection Preferences
Figure 3 compares the impact of educational background on the importance placed on price, availability, and compliance with specifications. Dentists trained abroad rated all three factors higher than those trained domestically, with the greatest emphasis on regulatory compliance. This suggests foreign-trained dentists prioritize adherence to standards, cost, and accessibility more heavily, while domestic graduates show greater flexibility in these areas.
3.5. Gender-Based Differences in Material Selection Behavior
Table 2 highlights gender-based differences in decision-making for aesthetic resin restorations. While both genders prioritized material longevity (M = 4.22, SD = 0.97), female dentists placed greater importance on clinical history (M = 3.75 vs. 3.28), scientific evidence (M = 3.00 vs. 2.69), and peer discussions (M = 3.27 vs. 3.03) than males. Women were also more influenced by printed and digital advertisements and rated environmental impact (carbon footprint) significantly higher (M = 2.54 vs. 1.82). Correlation analysis supported these trends, showing positive associations between female gender and preference for clinically proven materials (r = 0.291), sustainability (r = 0.306), and scientific sources (r = 0.218), indicating a more evidence-based and eco-conscious approach among female practitioners.
3.6. Influence of Professional Characteristics on Regulatory and Material Property Priorities
Table 3 presents correlations between professional traits and preferences in resin material selection. Female dentists showed greater concern for long-term storage (r = .230, p < .05), while older practitioners placed more trust in established brands (r = .217, p < .05). Frequent purchasers prioritized ISO compliance (r = .197, p < .05), whereas those not involved in procurement were less likely to consider it important (r = –.201). Older dentists were more likely to overlook flexural strength (r = .211, p < .05), as were frequent buyers (r = .247, p < .05), suggesting a preference for clinical convenience. Conversely, those performing over 20 restorations weekly strongly rejected low-strength materials (r = .306, p < .05), giving emphasis on durability and clinical performance.
3.7. Influence of Packaging, Usability, and Patient Factors on Material Selection
Table 4 shows gender-based differences in the perceived importance of packaging and clinical factors in material selection. Female dentists placed more emphasis on environmental concerns, including carbon footprint (M = 2.46 vs. 1.74) and packaging waste (M = 2.33 vs. 1.79). They were also more influenced by advertising (M = 1.96 vs. 1.46), though marketing had a low overall impact. Clinically, adhesive compatibility (M = 3.87) and material versatility (M = 3.77) were top priorities for both genders. Women valued simple packaging design and dosing ease slightly more than men, while ease of application was highly rated across the board (M = 3.70). Regarding patient-related factors, medical history (M = 3.03) and financial situation (M = 2.71) were moderately important, with men showing slightly greater concern for cost.
3.8. Impact of COVID-19 on Material Purchasing Behavior
Table 5 summarizes changes in purchasing behavior due to COVID-19, stratified by experience level. Only 11.5% of dentists reported increased orders, mainly among those with over five years of experience (16.3% vs. 6.8%). Interest in materials with faster workflows rose for 19.5% of respondents, more notably among experienced dentists (30.2%). Similarly, interest in trying new materials was higher in this group (34.9% vs. 15.9%). While 41.4% reported no change in preferences, uncertainty was more common among less experienced practitioners (36.4% vs. 4.7%). Correlation analysis supported these trends, linking greater experience with increased preference for efficient materials (r = 0.267) and openness to innovation (r = 0.218), while other practitioner traits showed no significant association.
4. Discussion
This study aimed to investigate the factors influencing dentists’ selection of resin-based restorative materials, with a focus on clinical performance, practitioner characteristics, and external influences such as the COVID-19 pandemic and environmental considerations. The findings highlight the complexity of the decision-making process, revealing that material choice is not solely determined by physical properties but is also shaped by individual experience, educational background, procurement roles, and broader contextual factors.
4.1. Material Choice for Posterior Restorations
The results of this study confirm that dentists prioritize clinical performance, ease of handling, and patient safety when selecting resin-based restorative materials for posterior restorations. Among these, mechanical durability, particularly in load-bearing areas, was consistently identified as the most critical factor, aligning with current evidence-based guidelines and recommendations [4,7,13]. Flexural strength, wear resistance, and reduced polymerization shrinkage are essential properties for posterior restorations, where occlusal forces are highest [8,9]. This focus on structural integrity supports prior research emphasizing that the long-term success of posterior composites is more dependent on mechanical performance than on esthetics or novelty [19]. Handling ease was also a prominent factor, reinforcing the value of materials that simplify placement and reduce technique sensitivity, especially in complex posterior restorations where moisture control and access are challenging [4,13]. This preference may be linked to the growing adoption of bulk-fill materials and user-friendly delivery systems that reduce chairside time without compromising clinical outcomes [5,6].
Further, although cost, brand reputation, and marketing exposure were considered, they ranked consistently lower in importance. These findings are in line with prior studies indicating that while economic and brand factors can influence initial product awareness, they rarely outweigh performance-based considerations in clinical selection [14,23,29]. This suggests that dentists in our sample rely primarily on clinical evidence and material reliability when making restorative decisions, particularly in posterior applications where mechanical failure carries greater risk.
4.2. Selection of Restorative Materials Based on Clinical Properties
The findings show that dentists place substantial emphasis on regulatory compliance, particularly ISO specifications, when selecting materials for esthetic restorations prone to water absorption. Nearly half of the respondents (48.3%) identified compliance with standards such as ISO 4049:2019 as the most important selection criterion, indicating that practitioners view regulatory benchmarks as essential for ensuring clinical reliability and safety [17,49,54]. This aligns with existing literature demonstrating that ISO standards play a central role in guiding clinicians toward materials with validated mechanical and physical properties, including acceptable levels of water sorption, solubility, and flexural strength [10,11,52,55]. In addition to compliance, handling versatility, material adaptability, and adhesive compatibility were consistently valued. These preferences reflect the increasing demand for materials that not only meet technical standards but also integrate smoothly into various restorative workflows. Studies have shown that modern resin composites with enhanced handling characteristics contribute to improved procedural efficiency and reduced technique sensitivity, particularly in esthetic cases [4,6,13,53]. Such emphasis on clinical and functional properties over marketing-driven factors like brand name or cost supports earlier observations that dentists prioritize evidence-based, performance-oriented features in material selection [14,29,58]. Moreover, compatibility with adhesive systems and the ability to adapt to different cavity configurations are crucial, especially in anterior teeth where esthetic and structural integrity must be carefully balanced [7,13,57]. Collectively, these results reinforce the notion that material selection is governed less by price or reputation and more by compliance with technical specifications and functional performance, a trend that reflects the profession's increasing alignment with standardized, quality-driven practice models [16,59].
4.3. Impact of Professional Characteristics on Selection Priorities
This study identified professional experience and procurement involvement as key drivers in restorative material selection. More experienced clinicians demonstrated a stronger inclination toward innovative, efficiency-focused materials, likely a reflection of their exposure to evolving technologies and familiarity with product performance over time [22]. Similarly, dentists directly involved in procurement decisions gave greater weight to regulatory compliance and long-term durability, whereas those less involved tended to prioritize ease of handling and esthetic qualities. These findings are consistent with research suggesting that procurement responsibilities enhance awareness of technical specifications and material standards [59].
Educational background also played a role. Foreign-trained dentists placed higher importance on cost, availability, and compliance, suggesting that variations in global training and regulatory environments may influence purchasing criteria [20,21]. This may be tied to differences in curriculum emphasis or healthcare system structure, particularly in regions where cost-effectiveness and regulatory scrutiny are more prominent [22].
Gender-based distinctions were evident as well. Male dentists showed a greater focus on cost-efficiency and practical use, while female practitioners adopted a more evidence-informed and environmentally conscious approach. This was reflected in their stronger reliance on peer-reviewed research, greater sensitivity to environmental impacts such as packaging waste, and higher interest in clinically established products [37,38,65]. These results support previous studies indicating that female clinicians often adopt more research-driven and sustainability-aware decision frameworks [37,38,39].
Age also influences preferences. Older dentists demonstrated greater brand loyalty, placing more trust in established manufacturers, whereas younger practitioners were more open to adopting newer materials. This trend aligns with literature highlighting the influence of brand recognition in clinical confidence and material selection, particularly among experienced practitioners [28,29].
Furthermore, this study explored how professional characteristics correlate with preferences for specific physical and mechanical properties. Female dentists, for instance, showed a stronger preference for materials with higher water absorption, possibly valuing extended storage stability [10]. Brand trust was more pronounced among older practitioners, further reinforcing the connection between clinical longevity and product confidence [28]. Additionally, clinicians engaged in purchasing showed higher regard for ISO compliance and material specifications, mirroring findings that link procurement roles with enhanced understanding of regulatory and quality standards [59]. In general, our findings support the case that material selection is a multifactorial process, shaped not only by product features but also by the clinician’s training, experience, role, and values.
4.4. Product Selection Influences and Environmental Considerations
External influences such as peer recommendations and clinical success rates emerged as key drivers in resin material selection, reinforcing the role of professional networks and evidence-based outcomes in shaping clinical decisions [20,21,42]. While advertising and marketing had limited overall impact, they were slightly more influential among female practitioners, a trend also observed in recent literature on gendered responses to promotional strategies in healthcare and dental marketing [26,45]. Nonetheless, both printed and digital advertising were generally rated as less important compared to functional and clinical attributes [24,29]. Environmental considerations, including sustainability and packaging recyclability, were more frequently emphasized by female dentists, consistent with broader findings on gender-based sensitivity to eco-conscious practices [35,37,38]. These results align with studies indicating that female professionals are more likely to integrate environmental values into product selection and procurement behavior [30,33,39].
Although product performance, ease of handling, and durability remain the most critical factors in material selection, this study demonstrates that personal values and external pressures, such as environmental sustainability, social norms, and peer influence, also contribute to decision-making. These secondary yet meaningful factors suggest that restorative material selection is increasingly guided by a combination of clinical evidence and ethical or societal considerations, particularly in the context of a growing awareness of green dentistry and responsible procurement [34,36].
4.5. Effects of COVID-19 on Purchasing Preferences
Following the onset of the COVID-19 pandemic, many dental professionals experienced disruptions in service provision, with reduced working hours and a shift toward emergency-only treatments [40]. Simultaneously, the cost of dental materials increased, placing further strain on procurement and practice management [40,41]. These challenges prompted a reevaluation of material selection criteria, particularly among more experienced clinicians. Further, the study's findings indicate that the pandemic influenced purchasing behavior most notably among practitioners with over five years of experience. This group demonstrated an increased preference for innovative and efficiency-oriented materials, suggesting a shift toward products that facilitate faster procedures and streamlined workflows. Such preferences are consistent with broader observations that crises tend to accelerate the adoption of tools and techniques that improve productivity and clinical reliability [41,42]. Despite these shifts, a substantial portion of respondents reported no significant change in purchasing behavior. This suggests that for many clinicians, factors such as material availability, cost constraints, or specific patient care protocols may have outweighed pandemic-related pressures. Additionally, less experienced dentists exhibited greater uncertainty in adjusting their material choices, likely reflecting a more cautious approach or limited exposure to alternative products during training and early practice. Notably, our results highlight how external pressures, such as global health emergencies, can act as catalysts for change, especially among clinicians already attuned to innovation and adaptability. At the same time, the persistence of pre-pandemic purchasing patterns among other segments of the dental workforce underlines the complex connection of clinical, economic, and personal factors in restorative material selection.
4.6. Study Limitations and Strengths
While this pilot study offers valuable insights into factors influencing resin-based material selection, several limitations can be acknowledged. The sample was limited to dentists affiliated with the National and Kapodistrian University of Athens, which may affect the generalizability of results due to institutional and contextual biases [69,70]. As a pilot investigation, the primary aim was exploratory, to test the feasibility of the instrument and identify relevant variables for future research [71,72]. Consequently, findings should be interpreted as preliminary and hypothesis-generating rather than conclusive [73]. Also, the modest sample size and single-institution design limit external validity. Broader, multicenter studies with more diverse populations would strengthen generalizability and support cross-context comparisons [74]. Additionally, the self-reported nature of the questionnaire introduces potential biases, including social desirability and recall error, despite measures taken to ensure anonymity and clarity [65]. Nonetheless, the study addresses a clear gap by exploring how professional characteristics shape material selection, including sustainability considerations. It also contributes validated survey tools and original data from a typically underrepresented population, laying the groundwork for future, large-scale research.
5. Conclusions
This study highlights the multifactorial nature of resin-based material selection, driven primarily by clinical performance, handling properties, and regulatory compliance. However, professional characteristics, such as gender, age, experience, and procurement involvement, also play a significant role. Female dentists emphasized longevity and environmental impact, while older and more experienced clinicians showed stronger brand loyalty. Those involved in procurement prioritized compliance, suggesting that technical engagement supports more informed choices. These findings underline the need to tailor education and marketing to diverse practitioner profiles and support further research to guide evidence-based, context-sensitive material selection.
Author Contributions
Conceptualization, M.A. and A.K.Z.; methodology, M.A.; software, M.A.; validation, M.A. and A.K.Z.; formal analysis, M.A.; investigation, M.A. and A.K.Z.; resources, M.A and A.K.Z.; data curation, M.A.; writing—original draft preparation, M.A. and A.K.Z.; writing—review and editing, M.A. and A.K.Z.; visualization, M.A. and A.K.Z.; supervision, M.A.; project administration, M.A.; funding acquisition, M.A. and A.K.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics and Research Committee of the Department of Dentistry (16.05.2024/44982).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed at the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Yadav R, Lee HH. Ranking and selection of dental restorative composite materials using FAHP-FTOPSIS technique: An application of multi criteria decision making technique. Journal of the Mechanical Behavior of Biomedical Materials. 2022, 132:105298. [CrossRef]
- Aminoroaya A, Neisiany RE, Khorasani SN, Panahi P, Das O, Madry H, et al. A review of dental composites: Challenges, chemistry aspects, filler influences, and future insights. Composites Part B: Engineering. 2021, 216:108852. [CrossRef]
- Cho K, Rajan G, Farrar P, Prusty G. Dental resin composites: A review on materials to product realizations. Composites Part B: Engineering. 2021, 230:109495. [CrossRef]
- Ferracane JL, Hilton TJ, Stansbury JW, Watts DC, Silikas N, Ilie N, et al. Academy of Dental Materials guidance-Resin composites: Part II-Technique sensitivity (handling, polymerization, dimensional changes). Dent Mater. 2017, 33(11):1171–91.
- Chesterman J, Jowett A, Gallacher A, Nixon P. Bulk-fill resin-based composite restorative materials: A review. BDJ. 2017, 222:337–44. [CrossRef]
- Matos JD, Nakano LJ, Scalzer G, Bottino M, Vasconcelos J, Jesus R, et al. Characterization of Bulk-Fill Resin Composites in Terms of Physical, Chemical, Mechanical and Optical Properties and Clinical Behavior. Inter J Odontostomatol. 2021, 15:226–33.
- Pratap B, Gupta RK, Bhardwaj B, Nag M. Resin based restorative dental materials: characteristics and future perspectives. Jpn Dent Sci Rev. 2019, 55(1):126–38. [CrossRef]
- Sengupta A, Naka O, Mehta SB, Banerji S. The clinical performance of bulk-fill versus the incremental layered application of direct resin composite restorations: a systematic review. Evidence-based dentistry. 2023, 24(3):143. [CrossRef]
- Soni N, Bairwa S, Sumita S, Goyal N, Choudhary S, Gupta M, et al. Mechanical Properties of Dental Resin Composites: A Review. International Journal of Research Publication and Reviews. 2024, 5:7675–83. [CrossRef]
- Huang W, Ren L, Cheng Y, Xu M, Luo W, Zhan D, et al. Evaluation of the Color Stability, Water Sorption, and Solubility of Current Resin Composites. Materials. 2022, 15(19):6710. [CrossRef]
- Yap AU, Eweis AH, Yahya NA. Dynamic and Static Flexural Appraisal of Resin-based Composites: Comparison of the ISO and Mini-flexural Tests. Oper Dent. 2018, 43(5):E223–e31.
- Zhang N, Xie C. Polymerization shrinkage, shrinkage stress, and mechanical evaluation of novel prototype dental composite resin. Dental materials journal. 2020, 39(6):1064–71.
- Pizzolotto L, Moraes RR. Resin Composites in Posterior Teeth: Clinical Performance and Direct Restorative Techniques. Dentistry journal. 2022;10(12).
- Zaware PDN. Exploration of market potential towards dental material brands: An assessment with preferences of dentists in India. Available at SSRN 3819251. 2020.
- Lorenz J, Wilhelm C, Urich J, Weigl P, Sader R. Different Esthetic Assessment of Anterior Restorations by Patient and Expert: A Prospective Clinical Study. Journal of esthetic and restorative dentistry : official publication of the American Academy of Esthetic Dentistry [et al]. 2024.
- Scopes -ISO/TC 106 Dentistry Subcommittees 1 and 2. [Internet]. Available from: iso.org/files/live/sites/tc106/files/TC%20106%20and%20SC%20Scopes 2018-11-09.pdf.
- International Organization for Standardization G, Switzerland. ISO 4049:2019. Dentistry-Polymer-based restorative materials. 2019:29.
- Bhaskar AS, Khan A. Comparative analysis of hybrid MCDM methods in material selection for dental applications. Expert Syst Appl. 2022, 209(C):8.
- Demarco FF, Cenci MS, Montagner AF, de Lima VP, Correa MB, Moraes RR, et al. Longevity of composite restorations is definitely not only about materials. Dent Mater. 2023, 39(1):1–12.
- Barnes E, Bullock AD, Bailey SE, Cowpe JG, Karaharju-Suvanto T. A review of continuing professional development for dentists in Europe(*). European journal of dental education. 2013, 17 Suppl 1:5–17.
- Ghoneim A, Yu B, Lawrence H, Glogauer M, Shankardass K, Quiñonez C. What influences the clinical decision-making of dentists? A cross-sectional study. PloS one. 2020 15(6):e0233652.
- Nascimento GG, Correa MB, Opdam N, Demarco FF. Do clinical experience time and postgraduate training influence the choice of materials for posterior restorations? Results of a survey with Brazilian general dentists. Brazilian dental journal. 2013, 24(6):642–6.
- Mallinson DJ, Hatemi PK. The effects of information and social conformity on opinion change. PloS one. 2018;13(5):e0196600.
- Prudnikov Y, Nazarenko A. The role of content marketing in the promotion of medical goods and services. 2021.
- Al-Sbei R, Ataya J, Jamous I, Dashash M. The Impact of a Web-Based Restorative Dentistry Course on the Learning Outcomes of Dental Graduates: Pre-Experimental Study. JMIR formative research. 2024, 8:e51141.
- Anshasi RJ, Alsubahi N, Alhusein AA, Lutfi Khassawneh AA, Alrawad M, Alsyouf A. Evolving perspectives in dental marketing: A study of Jordanian dentists' attitudes towards advertising and practice promotion. Heliyon. 2025, 11(1):e41143.
- Bispo Júnior JP. Social desirability bias in qualitative health research. Revista de saude publica. 2022, 56:101.
- Burke FJ. The evidence base for 'own label' resin-based dental restoratives. Dent Update. 2013;40(1):5–6.
- Shaw K, Martins R, Hadis MA, Burke T, Palin W. 'Own-Label' Versus Branded Commercial Dental Resin Composite Materials: Mechanical And Physical Property Comparisons. Eur J Prosthodont Restor Dent. 2016, 24(3):122–9.
- Barakat B, Milhem M, Naji GM, Alzoraiki M, Muda HB, Ateeq A, et al. Assessing the Impact of Green Training on Sustainable Business Advantage: Exploring the Mediating Role of Green Supply Chain Practices. Sustainability [Internet]. 2023, 15(19).
- Ririn Y, Rahmat STY, Rina A. How packaging, product quality and promotion affect the purchase intention? Russian Journal of Agricultural and Socio-Economic Sciences. 2019;92(8):46–55.
- Rundh B. Linking packaging to marketing: how packaging is influencing the marketing strategy. British Food Journal. 2013, 115(11):1547–63.
- Antoniadou M, Chrysochoou G, Tzanetopoulos R, Riza E. Green Dental Environmentalism among Students and Dentists in Greece. Sustainability [Internet]. 2023, 15(12).
- Duane B, Ramasubbu D, Harford S, Steinbach I, Stancliffe R, Croasdale K, et al. Environmental sustainability and procurement: purchasing products for the dental setting. British dental journal. 2019, 226(6):453–8.
- Mulimani P. Green dentistry: the art and science of sustainable practice. British dental journal. 2017, 222(12):954–61.
- Beske-Janssen P, Johnsen T, Constant F, Wieland A. New competences enhancing Procurement’s contribution to innovation and sustainability. Journal of Purchasing and Supply Management. 2023, 29(3):100847.
- Mittal R, Maheshwari R, Tripathi S, Pandey S. Eco-friendly dentistry: Preventing pollution to promoting sustainability. Indian Journal of Dental Sciences. 2020, 12:251.
- Ogiemwonyi O, Alam M, Alshareef R, Alsolamy M, Azizan N, Mat N. Environmental factors affecting green purchase behaviors of the consumers: Mediating role of environmental attitude. Cleaner Environmental Systems. 2023, 100130.
- Țâncu AMC, Imre M, Iosif L, Pițuru SM, Pantea M, Sfeatcu R, et al. Is Sustainability Part of the Drill? Examining Knowledge and Awareness Among Dental Students in Bucharest, Romania. Dentistry journal. 2025, 13(3).
- Farrokhi F, Farrokhi F, Mohebbi SZ, Khami MR. A scoping review of the impact of COVID-19 on dentistry: financial aspects. BMC Oral Health. 2024, 24(1):945.
- Rey-Martínez MS, Rey-Martínez MH, Martínez-Rodríguez N, Meniz-García C, Suárez-Quintanilla JM. Influence of the Sanitary, Economic, and Social Crisis of COVID-19 on the Emotional State of Dentistry in Galicia (Spain). Int J Environ Res Public Health. 2023, 20(4).
- Al-Asmar AA, Al-Hiyasat AS, Abu-Awwad M, Mousa HN, Salim NA, Almadani W, et al. Reframing Perceptions in Restorative Dentistry: Evidence-Based Dentistry and Clinical Decision-Making. International journal of dentistry. 2021, 2021:4871385.
- Maier C, Thatcher J, Grover V, Dwivedi Y. Cross-sectional research: A critical perspective, use cases, and recommendations for IS research. International Journal of Information Management. 2023;70:102625.
- Klaiman K, Ortega D, Garnache C. Consumer preferences and demand for packaging material and recyclability. Resources, Conservation and Recycling. 2016;115.
- Veleva S, Tsvetanova A. Characteristics of the digital marketing advantages and disadvantages. IOP Conference Series: Materials Science and Engineering. 2020, 940:012065.
- Ranganathan P, Caduff C. Designing and validating a research questionnaire - Part 1. Perspectives in clinical research. 2023, 14(3):152–5.
- Khanal B, Chhetri D. A Pilot Study Approach to Assessing the Reliability and Validity of Relevancy and Efficacy Survey Scale. Janabhawana Research Journal. 2024, 3:35–49.
- Brewster J, Roberts HW. 12-Month flexural mechanical properties of conventional and self-adhesive flowable resin composite materials. Dental materials journal. 2023, 42(4):598–609.
- Calabrese L, Fabiano F, Bonaccorsi LM, Fabiano V, Borsellino C. Evaluation of the Clinical Impact of ISO 4049 in Comparison with Miniflexural Test on Mechanical Performances of Resin Based Composite. International journal of biomaterials. 2015, 2015:149798.
- Erickson RL, Barkmeier WW. Comparisons of ISO depth of cure for a resin composite in stainless-steel and natural-tooth molds. European journal of oral sciences. 2019, 127(6):556–63.
- Fan PL, Schumacher RM, Azzolin K, Geary R, Eichmiller FC. Curing-light intensity and depth of cure of resin-based composites tested according to international standards. Journal of the American Dental Association (1939). 2002;133(4):429–34; quiz 91–3.
- Flury S, Hayoz S, Peutzfeldt A, Hüsler J, Lussi A. Depth of cure of resin composites: is the ISO 4049 method suitable for bulk fill materials? Dent Mater. 2012, 28(5):521–8.
- Heintze S, Zimmerli B. Relevance of in-vitro tests of adhesive and composite dental materials. A review in 3 parts. Part 2: non-standardized tests of composite materials. Schweizer Monatsschrift für Zahnmedizin = Revue mensuelle suisse d'odonto-stomatologie = Rivista mensile svizzera di odontologia e stomatologia / SSO. 2011, 121:916–30.
- Heintze SD, Zimmerli B. Relevance of in vitro tests of adhesive and composite dental materials, a review in 3 parts. Part 1: Approval requirements and standardized testing of composite materials according to ISO specifications. Schweiz Monatsschr Zahnmed. 2011, 121(9):804–16.
- Ilie N. ISO 4049 versus NIST 4877: Influence of stress configuration on the outcome of a three-point bending test in resin-based dental materials and interrelation between standards. Journal of dentistry. 2021;110:103682.
- Moore BK, Platt JA, Borges G, Chu TM, Katsilieri I. Depth of cure of dental resin composites: ISO 4049 depth and microhardness of types of materials and shades. Oper Dent. 2008, 33(4):408–12.
- Arandi NZ. Current trends in placing posterior composite restorations: Perspectives from Palestinian general dentists: A questionnair study. Journal of International Society of Preventive & Community Dentistry. 2024, 14(2):112–20.
- Ilie N, Hilton TJ, Heintze SD, Hickel R, Watts DC, Silikas N, et al. Academy of Dental Materials guidance-Resin composites: Part I-Mechanical properties. Dent Mater. 2017, 33(8):880–94.
- Megremis SJ. Assuring the Safety of Dental Materials: The Usefulness and Application of Standards. Dental clinics of North America. 2022, 66(4):673–89.
- Bujang MA, Omar E, Foo D, Hon YK. Sample size determination for conducting a pilot study to assess reliability of a questionnaire. Restorative Dentistry & Endodontics. 2024, 49.
- Hussey I, Alsalti T, Bosco F, Elson M, Arslan R. An Aberrant Abundance of Cronbach’s Alpha Values at .70. Advances in Methods and Practices in Psychological Science. 2025, 8(1):25152459241287123.
- Tavakol M, Dennick R. Making Sense of Cronbach's Alpha. Inter J Med Educ. 2011, 2:53–5.
- Agrawal AA, Prakash N, Almagbol M, Alobaid M, Alqarni A, Altamni H. Synoptic review on existing and potential sources for bias in dental research methodology with methods on their prevention and remedies. World J Methodology. 2023, 13(5):426–38.
- Vaidyanathan AK. Controlling bias in research. Journal of Indian Prosthodontic Society. 2022, 22(4):311–3.
- Latkin CA, Edwards C, Davey-Rothwell MA, Tobin KE. The relationship between social desirability bias and self-reports of health, substance use, and social network factors among urban substance users in Baltimore, Maryland. Addictive behaviors. 2017, 73:133–6.
- Guo M, Wang Y, Yang Q, Li R, Zhao Y, Li C, et al. Normal Workflow and Key Strategies for Data Cleaning Toward Real-World Data: Viewpoint. Interactive journal of medical research. 2023, 12:e44310.
- Ranganathan P, Hunsberger S. Handling missing data in research. Perspectives in clinical research. 2024, 15(2):99–101.
- Ahmed I, Ishtiaq S. Reliability and validity: Importance in Medical Research. JPMA The Journal of the Pakistan Medical Association. 2021, 71(10):2401–6.
- Patino CM, Ferreira JC. Inclusion and exclusion criteria in research studies: definitions and why they matter. Jornal brasileiro de pneumologia : publicacao oficial da Sociedade Brasileira de Pneumologia e Tisilogia. 2018, 44(2):84.
- Torgerson DJ, Torgerson CJ. Pilot Randomised Controlled Trials. In: Torgerson DJ, Torgerson CJ, editors. Designing Randomised Trials in Health, Education and the Social Sciences: An Introduction. London: Palgrave Macmillan UK; 2008. p. 119–26.
- Leon AC, Davis LL, Kraemer HC. The role and interpretation of pilot studies in clinical research. J Psychiatric Res. 2011, 45(5):626–9.
- Thabane L, Ma J, Chu R, Cheng J, Ismaila A, Rios LP, et al. A tutorial on pilot studies: the what, why and how. BMC Medical Res Methodol. 2010, 10(1):1.
- Hallingberg B, Turley R, Segrott J, Wight D, Craig P, Moore L, et al. Exploratory studies to decide whether and how to proceed with full-scale evaluations of public health interventions: a systematic review of guidance. Pilot and Feasibility Studies. 2018, 4(1):104. [CrossRef]
- Bornstein M, Al-Nawas B, Kuchler U, Tahmaseb A. Consensus Statements and Recommended Clinical Procedures Regarding Contemporary Surgical and Radiographic Techniques in Implant Dentistry. Inter J oral Maxillofacial Implants. 2014, 29:78–82. [CrossRef]
Figure 1.
Mean scores and confidence intervals for factors influencing the selection of resin restorative materials for conservative restorations.
Figure 1.
Mean scores and confidence intervals for factors influencing the selection of resin restorative materials for conservative restorations.
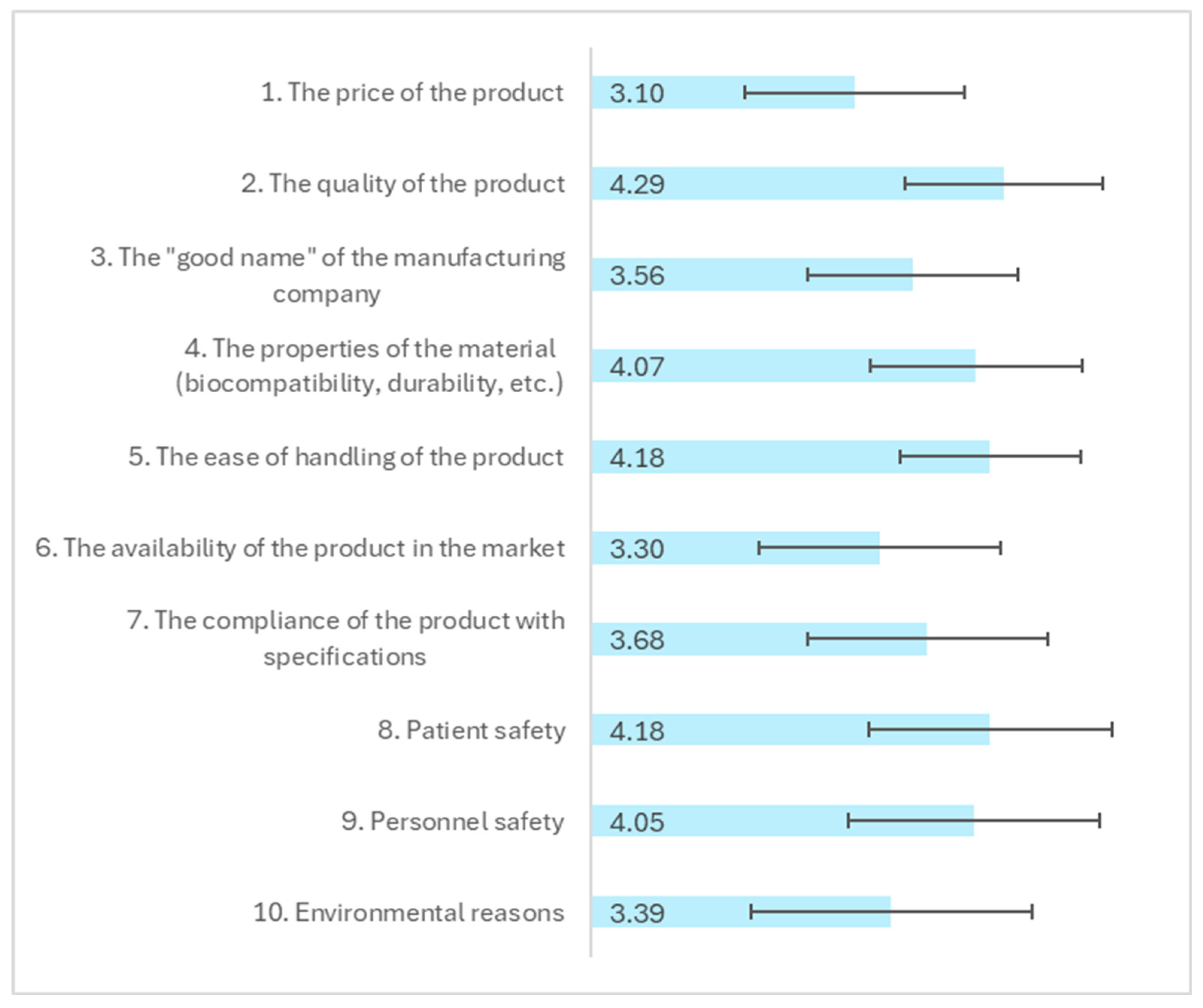
Figure 2.
Mean scores and 95% confidence intervals (CIs) by age group, for three key factors influencing the selection of resin restorative materials, the "good name" of the manufacturing company, the properties of the material and the ease of handling of the product.
Figure 2.
Mean scores and 95% confidence intervals (CIs) by age group, for three key factors influencing the selection of resin restorative materials, the "good name" of the manufacturing company, the properties of the material and the ease of handling of the product.
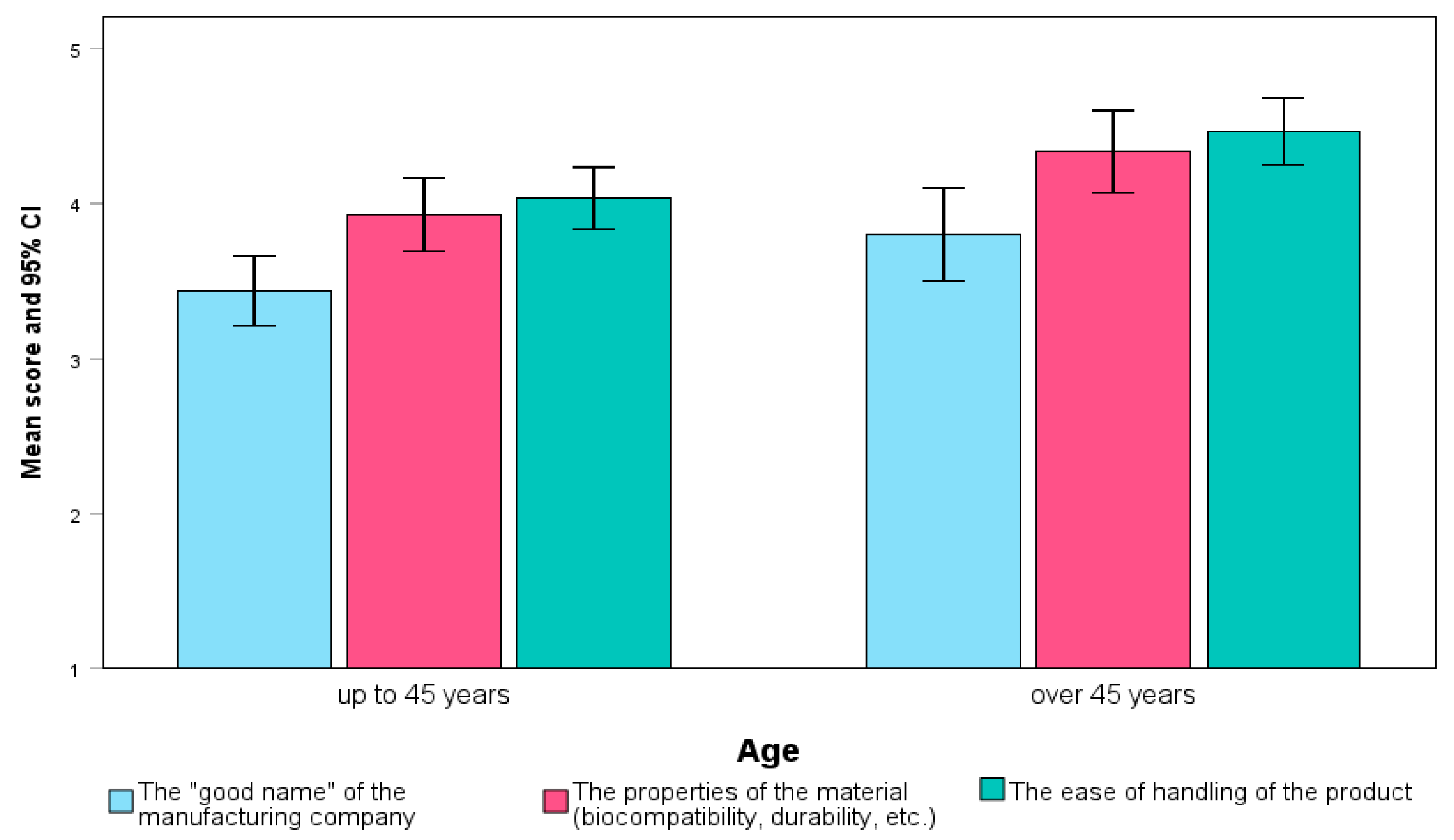
Figure 3.
Mean scores and 95% confidence intervals (CIs) for factors influencing the selection of resin restorative materials, by dental school: the price of the product, the availability of the product in the market, and the compliance of the product with specifications.
Figure 3.
Mean scores and 95% confidence intervals (CIs) for factors influencing the selection of resin restorative materials, by dental school: the price of the product, the availability of the product in the market, and the compliance of the product with specifications.
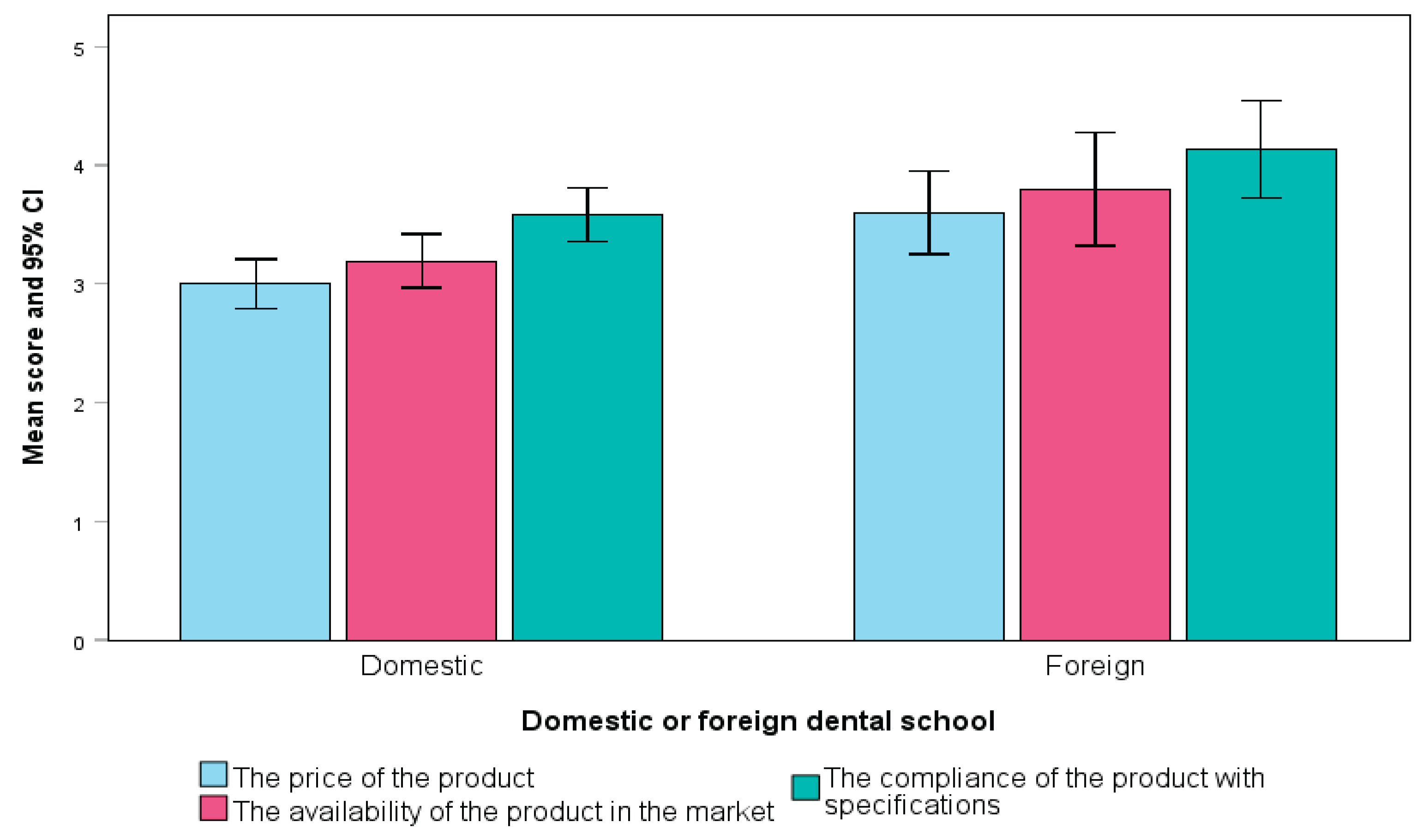

Table 1.
Preferences for Resin Restorative Materials with Specific Properties.
| N | % | |
|---|---|---|
| Would you choose a product with increased water absorption for aesthetic restorations because it is: | ||
| Lower cost | 3 | 3.4% |
| Trusted brand name | 16 | 18.4% |
| With greater ease of handling | 23 | 26.4% |
| With long-term storage of the material | 9 | 10.3% |
| The most important thing for me is that the material complies with ISO specifications | 42 | 48.3% |
| I don't know/don't answer | 23 | 26.4% |
| Would you choose a resin material that has lower flexural strength (i.e., has a lower ability to resist deformation under applied forces) but: | ||
| Has greater color stability | 14 | 16.1% |
| Requires shorter polymerization time and therefore less working time | 8 | 9.2% |
| Has greater radiopacity than dentin and is easier to see on X-rays | 2 | 2.3% |
| I do not consider flexural strength important | 2 | 2.3% |
| I would not choose a material that is inferior in this property for posterior teeth | 52 | 59.8% |
| I would not choose a material that is inferior in physical and mechanical properties | 47 | 54.0% |
| I do not know/do not answer | 5 | 5.7% |
Table 2.
Preferences and Information-Seeking Behavior When Selecting Resin Restorative Materials.
| Total$$(M, SD) | Male$$(M, SD) | Female$$(M, SD) | Mann-Whitney p-value | ||||
|---|---|---|---|---|---|---|---|
| For conservative aesthetic restorations with composite resin: | |||||||
| 1. I like to try new materials frequently to see which one works best. | 3.06 | 1.03 | 3.10 | .97 | 3.02 | 1.08 | 0.827 |
| 2. I look for published studies on efficacy and longevity before trying a new material. | 2.86 | 1.15 | 2.69 | 1.26 | 3.00 | 1.05 | 0.254 |
| 3. I look for material to have a long history of clinical success before adopting it into my practice. | 3.54 | 1.03 | 3.28 | 1.00 | 3.75 | 1.02 | 0.027 |
| 4. I rarely try new aesthetic materials. | 2.47 | 1.05 | 2.23 | .90 | 2.67 | 1.14 | 0.089 |
| 5. I am interested in trying new generations of materials I already trust. | 3.59 | .96 | 3.54 | .91 | 3.63 | 1.00 | 0.631 |
| 6. I rarely change the aesthetic resin materials I use unless they are no longer available on the market. | 2.72 | 1.18 | 2.72 | 1.02 | 2.73 | 1.30 | 0.888 |
| 7. I trust the resin materials I learned to use in school during my studies. | 2.08 | 1.11 | 2.00 | .95 | 2.15 | 1.24 | 0.826 |
| 8. I generally trust the one that provides the longest working time. | 2.49 | 1.07 | 2.41 | 1.02 | 2.56 | 1.11 | 0.550 |
| 9. I trust the resin materials that I often hear colleagues speak positively about. | 3.16 | 1.10 | 3.03 | 1.04 | 3.27 | 1.14 | 0.235 |
| 10. I trust the material whose printed advertising has convinced me. | 1.93 | .95 | 1.67 | .70 | 2.15 | 1.07 | 0.038 |
| 11. I trust the material whose advertising in digital media has convinced me. | 1.93 | .94 | 1.67 | .74 | 2.15 | 1.03 | 0.027 |
| 12. I have not observed any conscious behavior on my part when choosing aesthetic materials for immediate restorations. | 2.33 | 1.12 | 2.21 | .98 | 2.44 | 1.22 | 0.487 |
| Seeking information before purchasing resin restorative material | |||||||
| 1. The ISO specifications that it must include. | 3.02 | 1.07 | 3.05 | 1.19 | 3.00 | .97 | .712 |
| 2. The opinion of a trusted partner/colleague regarding the product. | 3.25 | .88 | 3.18 | .88 | 3.31 | .88 | .476 |
| 3. Any discount offer that my supplier may have. | 2.74 | .98 | 2.64 | .93 | 2.81 | 1.02 | .610 |
| 4. The lifespan of the material. | 3.22 | .97 | 3.08 | .90 | 3.33 | 1.02 | .269 |
| 5. The carbon footprint it leaves in the environment. | 2.22 | 1.03 | 1.82 | .97 | 2.54 | .97 | <.001 |
| 6. The longevity of clinical restorations with this material. | 4.22 | .97 | 4.10 | .97 | 4.31 | .97 | .194 |
Table 3.
Correlations Between Professional Characteristics and Selection of Resin Restorative Materials with Specific Properties.
Table 3.
Correlations Between Professional Characteristics and Selection of Resin Restorative Materials with Specific Properties.
| Gender (Female vs Male) | Age (over 45 years) | Dental school (foreign vs domestic) | Post-grad studies in dentistry | Clinical experience (over 5 years) | Employment (private clinic vs other) | Purchasing resin restorations over 2 times/year | Not responsible for supply of resin restorations | Performing over 20 restorations/ week | |
|---|---|---|---|---|---|---|---|---|---|
| Would you choose a product with increased water absorption for aesthetic restorations because it is: | |||||||||
| Lower cost | 0.044 | 0.128 | -0.086 | 0.112 | 0.065 | -0.083 | 0.009 | 0.146 | -0.011 |
| Trusted brand name | -0.049 | .217* | 0.019 | 0.179 | 0.124 | -0.049 | 0.066 | 0.066 | -0.138 |
| With greater ease of handling | -0.141 | -0.106 | 0.209 | 0.015 | -0.071 | -0.036 | 0.049 | -0.008 | 0.060 |
| With long-term storage of the material | .230* | 0.071 | -0.055 | 0.123 | -0.034 | 0.003 | -0.065 | -0.065 | 0.094 |
| The most important thing for me is that the material complies with ISO specifications | 0.085 | -0.072 | -0.076 | 0.145 | 0.011 | -0.100 | 0.197 | -0.201 | -0.009 |
| Would you choose a resin material that has lower flexural strength (i.e., has a lower ability to resist deformation under applied forces) but: | |||||||||
| Has greater color stability | -0.171 | -0.120 | -0.117 | 0.109 | -0.058 | -0.046 | -0.091 | .247* | -0.117 |
| Requires shorter polymerization time and therefore less working time | -0.033 | -0.063 | 0.171 | -0.003 | 0.083 | -0.033 | -0.127 | -0.042 | 0.094 |
| It has greater radiopacity than dentin and is easier to see on X-rays | -0.016 | -0.111 | -0.070 | 0.038 | 0.002 | -0.016 | -0.103 | -0.103 | 0.045 |
| I do not consider flexural strength important | 0.138 | .211* | -0.070 | 0.038 | 0.155 | 0.138 | 0.063 | -0.103 | 0.045 |
| I would not choose a material that is inferior to this property for posterior teeth | 0.109 | -0.046 | 0.126 | 0.013 | -0.080 | 0.015 | -0.007 | -0.007 | -0.004 |
| I would not choose a material that is inferior in physical and mechanical properties | 0.050 | -0.010 | 0.055 | -0.039 | 0.036 | 0.050 | 0.120 | -0.029 | .306** |
Table 4.
Influence of Packaging and Selection Factors in Resin Restorative Material Choice.
| Total$$(M, SD) | Male$$(M, SD) | Female$$(M, SD) | Mann-Whitney p-value | ||||
|---|---|---|---|---|---|---|---|
| For conservative aesthetic restorations with composite resin: | |||||||
| 1. The appearance of the product packaging. | 1.38 | .74 | 1.26 | .59 | 1.48 | .82 | 0.203 |
| 2. The environmental footprint of the packaging. | 2.14 | 1.00 | 1.74 | .97 | 2.46 | .92 | <.001 |
| 3. The increased advertising and promotional activities that have been carried out. | 1.74 | .87 | 1.46 | .64 | 1.96 | .97 | 0.005 |
| 4. Its ease of supply. | 2.69 | 1.04 | 2.64 | 1.06 | 2.73 | 1.03 | 0.446 |
| 5. The volume of packaging materials (waste). | 2.09 | 1.01 | 1.79 | .98 | 2.33 | .97 | 0.006 |
| 6. Its compliance with specifications. | 3.70 | 1.16 | 3.69 | 1.13 | 3.71 | 1.20 | 0.869 |
| Factors influencing resin restorative material selection | |||||||
| 1. The visual appeal of the packaging | 1.75 | .87 | 1.46 | .72 | 1.98 | .91 | 0.003 |
| 2. The practical and easy way of dosing | 2.90 | .99 | 2.82 | .91 | 2.96 | 1.05 | 0.577 |
| 3. The simple design of the packaging | 2.53 | 1.08 | 2.33 | 1.08 | 2.69 | 1.06 | 0.155 |
| 4. Detailed instructions for use | 3.29 | 1.00 | 3.38 | 1.04 | 3.21 | .97 | 0.446 |
| 5. The reduced time to learn the application technique | 3.44 | 1.00 | 3.38 | .99 | 3.48 | 1.01 | 0.545 |
| 6. The reduced time to apply it clinically | 3.49 | .95 | 3.54 | .91 | 3.46 | .99 | 0.837 |
| 7. The simple application technique | 3.70 | .90 | 3.74 | .82 | 3.67 | .97 | 0.885 |
| 8. The wide range of applications of the material | 3.77 | .92 | 3.72 | .89 | 3.81 | .96 | 0.464 |
| 9. The long shelf life of the packaging | 3.43 | 1.04 | 3.41 | 1.09 | 3.44 | 1.01 | 0.862 |
| 10. Its storage in non-specific conditions | 3.18 | 1.08 | 3.13 | 1.10 | 3.23 | 1.08 | 0.546 |
| 11. Its compatibility with different adhesive systems or techniques | 3.87 | .90 | 4.03 | .81 | 3.75 | .96 | 0.189 |
| 12. Its price | 3.55 | .94 | 3.49 | .97 | 3.60 | .92 | 0.655 |
| 13. The patient's preferences | 2.37 | 1.13 | 2.33 | 1.08 | 2.40 | 1.18 | 0.849 |
| 14. The patient's medical history | 3.03 | 1.14 | 3.08 | 1.13 | 3.00 | 1.15 | 0.808 |
| 15. The patient's age | 2.86 | 1.17 | 2.82 | 1.12 | 2.90 | 1.22 | 0.694 |
| 16. The patient's financial situation | 2.71 | 1.19 | 2.85 | 1.18 | 2.60 | 1.20 | 0.330 |
Table 5.
Effects of the COVID-19 Pandemic on the Approach to Resin Restorative Materials.
| Effects of the COVID-19 pandemic on the approach to resin restorative materials | Total sample (N = 87) |
Clinical experience (in years) | ||||
|---|---|---|---|---|---|---|
| up to 5 years (N = 44) |
over 5 years (N = 43) |
|||||
| Ν | % | Ν | % | Ν | % | |
| My orders for resin restorative materials have increased | 10 | 11.5% | 3 | 6.8% | 7 | 16.3% |
| My orders for restorative resin materials have decreased | 4 | 4.6% | 2 | 4.5% | 2 | 4.7% |
| My interest in purchasing materials with an easy and fast workflow has increased | 17 | 19.5% | 4 | 9.1% | 13 | 30.2% |
| My interest in trying new materials has increased | 22 | 25.3% | 7 | 15.9% | 15 | 34.9% |
| My interest in trying new materials has decreased | 3 | 3.4% | 0 | 0.0% | 3 | 7.0% |
| There has been no significant change in my preferences | 36 | 41.4% | 17 | 38.6% | 19 | 44.2% |
| I don't know / no answer | 18 | 20.7% | 16 | 36.4% | 2 | 4.7% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



