Submitted:
06 June 2025
Posted:
08 June 2025
You are already at the latest version
Abstract
Healthcare supply chain management operates under complex uncertainty, high risk, and the imperative of sustainable resource optimization. This study investigates the underlying mechanisms through which digital intelligence drives strategic decision optimization in healthcare supply chains. Drawing on the Resource Based View (RBV) and Dynamic Capabilities Theory (DCT), we develop a chain mediated model in which innovation capability and supply chain resilience (absorptive, response, and restorative capabilities), serve as sequential mediators. Using structural equation modeling (SEM) on data collected from healthcare supply chain organizations in China, we find that digital intelligence indirectly enhances decision optimization by fostering innovation and resilience in tandem. Specifically, digital intelligence strengthens innovation capability, which in turn activates all three dimensions of resilience, and together these capabilities produce a synergistic effect that sustains decision improvement. Our findings offer practical theoretical guidance for healthcare institutions seeking to deploy digital intelligence technologies, reinforce dynamic process management, and achieve continuous optimization of supply chain decision making.
Keywords:
digital intelligence
; innovation capability
; supply chain resilience
; decision optimization
; healthcare supply chain
1. Introduction
Healthcare supply chain systems have been facing unprecedented transformations and challenges. On one hand, the global demand for pharmaceuticals and medical services continues to grow rapidly, placing increasing pressure on resource allocation and supply efficiency [1]. According to the IQVIA Institute (2024), global medicine usage rose by 14% over the past five years and is projected to grow another 12% by 2028, with China leading in both consumption volume and expenditure [2]. On the other hand, population aging and the rising prevalence of chronic diseases have driven a long term and diversified demand for healthcare services. By 2040, individuals aged 60 and above are expected to account for 28% of China’s population [3], with a sharp increase in patients requiring long term treatment for diabetes, cardiovascular conditions, and other chronic illnesses. These developments have accelerated the integration of digital healthcare services such as telemedicine, e-prescriptions, and online pharmaceutical distribution into existing healthcare systems [4].
Meanwhile, emerging models such as Personalized medicine, smart healthcare, remote services, and precision medicine are reshaping patient centered service delivery. Healthcare supply chains are evolving beyond traditional drug logistics and inventory systems into collaborative networks that integrate hospitals, pharmaceutical manufacturers, digital platforms, and end users [5]. Digital technologies including artificial intelligence, predictive analytics, smart inventory control, and multi-stakeholder collaboration platforms, are playing a pivotal role in enhancing responsiveness, operational efficiency, and patient satisfaction [6,7].
Moreover, the outbreak of COVID-19 revealed the structural vulnerabilities of traditional supply chains and underscored the critical importance of resilience in healthcare systems. The ability to sense disruptions, respond rapidly, and recover systematically has become a fundamental requirement for the sustainable performance of healthcare supply chains [8,9].
In recent years, a growing body of literature has systematically reviewed how digital technologies can enhance system resilience and operational efficiency within the healthcare supply chain. These studies consistently highlight that technologies such as artificial intelligence (AI), blockchain, and big data analytics can improve data driven decision making, agile responsiveness, and resource allocation efficiency particularly in domains such as hospital operations, pharmaceutical distribution, and emergency medical supply management [5,8]. In parallel, other research streams have focused on the development of supply chain resilience capabilities, proposing full cycle frameworks encompassing sensing, response, recovery, and adaptation, while emphasizing the critical role of Industry 4.0 technologies in enhancing these dynamic processes [10,11,12].
Although these studies have expanded the understanding of digital transformation in healthcare supply chains, the majority remain qualitative or case based, and there is a lack of integrative investigation into the system-level architecture of healthcare supply chains. More specifically, limited attention has been paid to the mechanisms through which digital intelligence resources are transformed into strategic decision making advantages via organizational capabilities [13,14].
To address these gaps, this study develops a theoretical framework by integrating the Resource Based View (RBV) and the Dynamic Capabilities Theory (DCT). RBV emphasizes the strategic value of firm specific resources in achieving competitive advantage, with digital intelligence (DI) conceptualized as a high-potential strategic resource. DCT explains how firms absorb, reconfigure, and dynamically deploy such resources under environmental uncertainty to develop adaptive organizational capabilities, innovation capability (IC) and supply chain resilience (SCR). Building on this perspective, this study proposes that DI influences decision optimization (DO) in the healthcare supply chain indirectly and profoundly through the capability building pathways of IC and SCR.
In summary, to address the current lack of system level integration and the unclear mechanism pathways in the digital transformation of healthcare supply chains, this study aims to develop a theory driven analytical framework that systematically explores how digital intelligence enhances decision optimization through the mediating roles of innovation capability and supply chain resilience.
This research adopts an integrated perspective of the Resource Based View (RBV) and Dynamic Capabilities Theory (DCT) to uncover the mediating pathways through which digital resources are converted into strategic decision outcomes, thereby extending the theoretical foundation of digital transformation research in the context of healthcare supply chain management. On the other hand, the study provides empirical evidence and practical guidance for healthcare organizations to strengthen resilient operations and improve decision making efficiency under conditions of high uncertainty.
Unlike previous studies that primarily emphasized IT systems or digital tools, this study focuses on the technical characteristics of digital intelligence as a central feature of digital transformation. In light of the high demand volatility and complex service challenges in the healthcare industry, the research framework is constructed by integrating the Resource Based View (RBV) and Dynamic Capabilities Theory (DCT) to reflect the realities of highly dynamic environments. This study explores a parallel and sequential mediation mechanism composed of innovation capability and the three dimensions of supply chain resilience: absorptive, response, and restorative capabilities. It aims to reveal how digital technology resources can be transformed into decision optimization advantages through the collaborative functioning of organizational capabilities. By investigating how digital intelligence enhances organizational learning, innovation, and dynamic responsiveness, this study provides a new perspective on the deep level impact of digital transformation on healthcare supply chain management.
This study aims to explore the key drivers influencing decision optimization in the healthcare supply chain, with the goal of providing both theoretical support and practical guidance for the sustainable development of the healthcare industry. The structure of the study is as follows. Section 2 provides a comprehensive review of the relevant literature on digital intelligence, innovation capability, and supply chain resilience including absorptive, response, and restorative capabilities, as well as decision optimization, and identifies the theoretical foundation and knowledge gaps addressed in this study. Section 3 presents the conceptual model and research hypotheses, along with a detailed explanation of the research methodology, variable development, and measurement approach. Section 4 reports the empirical findings based on structural equation modeling (SEM) and interprets the statistical significance of the results. Section 5 discusses the research outcomes, highlights the theoretical and practical implications, outlines the study’s limitations, and proposes directions for future research.
2. Literature Review
2.1. Digital Intelligence
With the continuous penetration of advanced digital technologies such as artificial intelligence, big data analytics, and the Internet of Things, digital transformation has become a critical force in reshaping core organizational capabilities and promoting high quality development [15]. In the context of healthcare supply chains, digital transformation is regarded as a systemic innovation process driven by data, aiming to optimize resource allocation, enhance service effectiveness, and ensure medical quality [16]. In this transformation, organizations urgently need to build intelligent systems capable of sensing, analyzing, learning, and forecasting to cope with highly uncertain external environments.
Among the various technological attributes encompassed by digital transformation, digital intelligence (DI) has increasingly drawn scholarly attention due to its deep impact on supply chain responsiveness and decision making capabilities [17]. DI primarily relies on advanced technologies such as AI, machine learning, and big data analytics to restructure supply chain processes through intelligent sensing, intelligent analysis, and intelligent decision making. Empirical studies have shown that intelligent algorithms can significantly improve the efficiency of key supply chain functions, such as route optimization, demand forecasting, and inventory scheduling in healthcare systems [18,19]. In practice, the integration of AI with Vendor Managed Inventory (VMI) systems has enhanced information flow between hospitals and pharmaceutical firms, enabling automated replenishment and data visualization [20], while AI-based platforms have improved order responsiveness and production planning accuracy in pharmaceutical enterprises [21].
However, existing research largely treats digital intelligence as a technical tool, lacking structured modeling and theoretical interpretation of its role as an independent variable. In particular, studies exploring how DI influences strategic decision making through organizational capability pathways in the healthcare supply chain context remain scarce. To address this gap, this study conceptualizes DI as a key driving force that reflects a digital system’s capacity for autonomous cognition, intelligent analysis, and data driven decision making.
2.2. Innovation Capability
Innovation capability in healthcare supply chain management is widely recognized as a critical driver for organizations to gain competitive advantage in dynamic environments. It encompasses not only the adoption of emerging technologies, but also process optimization, service model restructuring, and rapid responsiveness to external changes [22]. From various theoretical perspectives, innovation capability can be further specified as follows: From the perspective of technological resource integration, it reflects an organization’s ability to identify, absorb, and deploy advanced digital technologies such as artificial intelligence, blockchain, and IoT to support efficient coordination and service execution [23]. From the perspective of process redesign, it involves continuous improvement of operational mechanisms, reduction of redundancies, and enhancement of system flexibility [24]. From the service model restructuring lens, innovation capability enables the transformation of traditional linear supply models into patient centered, multi-point coordinated intelligent networks [25].
Additionally, the synergistic accumulation of organizational learning, data driven capabilities, and cross functional integration is considered a core component of innovation capability [26], while dynamic responsiveness to environmental disruptions also entails the reconfiguration of processes and strategic plans [27]. Overall, innovation capability is not only essential for the deep application of digital technologies, but also serves as a driving force for platform based coordination, smart operations, and decision optimization in healthcare supply chains [28].
However, existing research has not yet sufficiently examined how innovation capability functions as a dynamic organizational capability that mediates the relationship between digital intelligence and decision optimization via supply chain resilience. To address this gap, the present study incorporates innovation capability as a core mediating variable to explore its role in converting digital intelligence into strategic value, thereby extending theoretical insights into capability building and performance enhancement in healthcare supply chain management.
2.3. Supply Chain Resilience
In contemporary supply chain research, resilience is widely defined as an organization’s ability to maintain core functions and rapidly recover in the face of external disruptions [29]. Zhao et al. (2023) further conceptualize resilience as a dynamic process encompassing absorptive, response, and restorative capabilities, highlighting the full cycle of sensing, reacting, and rebuilding in turbulent environments [30]. Building on this, Senna et al. (2023) propose a systemic framework in which resilience in healthcare supply chains is not merely reactive, but represents a structured, multi-layered, and dynamic set of capabilities embedded within a cyclical mechanism linking antecedents, mediators, and outcomes [10].
In the healthcare context, the ongoing disruptions caused by pandemics, large scale disasters, and population aging necessitate supply chains that are capable of rapid adaptation, diversified responses, and effective recovery [31]. In response, recent studies have begun integrating Dynamic Capabilities Theory (DCT) into resilience research, emphasizing the relevance of sensing, seizing, and reconfiguring mechanisms in uncertain environments [32].
Although some studies acknowledge the multi-stage nature of resilience, there remains a lack of in depth integration between resilience and DCT. To address this gap, the present study adopts a DCT informed approach and constructs a three dimensional structure of absorptive, response, and restorative capabilities as mediating variables, aiming to systematically assess how resilience bridges the relationship between digital intelligence and decision optimization in complex healthcare supply chains.
2.3.1. Absorptive Capability
Absorptive capability is commonly defined as an organization’s ability to sense, identify, and integrate external information, early warning signals, and potential disruptions in the pre-disruption phase [33]. Zhao et al. (2023) identify absorptive capability as a critical starting point for resilient operations, enabling supply chains to detect disturbance sources and proactively consolidate relevant information resources at an early stage [30]. In an empirical study of emerging economies, Tortorella et al. (2023) emphasize that, in the context of healthcare, absorptive capability also reflects the system’s sensitivity to heterogeneous and multi-source data, such as pandemic forecasts, fluctuations in patient demand, and policy shifts, which indicates its predictive and preemptive capacity [34].
Wright et al. (2024) argue that establishing preemptive mechanisms for information perception and integration enhances the healthcare supply chain’s ability to anticipate crises and avoid delayed responses [35]. In addition, Kumar et al. (2023) highlight that absorptive capability relies heavily on the support of AI, big data, and other digital technologies, which accelerate information sensing and improve data processing quality, thereby creating an intelligent link between information and decision making [36].
Although its preemptive role in resilience management has been widely recognized, the conceptual boundaries, operational mechanisms, and quantitative measurement of absorptive capability in healthcare supply chains remain underdeveloped. Therefore, this study defines absorptive capability as the ability of an organization to integrate, recognize, and internalize heterogeneous information from multiple sources prior to disruptions. It emphasizes its core role in forecasting, early warning, and risk prevention, and conceptualizes it as the first stage dimension of supply chain resilience.
2.3.2. Absorptive Capability
Unlike absorptive capability, which emphasizes the identification and anticipation of risks before disruptions occur, response capability focuses on an organization’s ability to rapidly mobilize critical resources and make effective decisions during the occurrence of disruptions [37]. This capability is reflected in how quickly identified risk signals are translated into concrete actions such as activating alternative routes, adjusting inventory strategies, and reallocating resources in a timely and efficient manner [38].
In healthcare systems, the response window to disruptions is extremely narrow. In time sensitive areas such as vaccine distribution, emergency drug delivery, and surgical supply provision, response efficiency is directly linked to patient safety and continuity of care [10]. Developing such capability requires not only refined internal process management but also support from digital technologies such as artificial intelligence and machine learning, which enable real time feedback, rapid scenario modeling, and intelligent path optimization [36]. Tortorella et al. (2023), in their study of emerging economies, found that healthcare institutions with standardized, platform based, and modularized response systems are better equipped to translate disruption signals into swift operational actions [34].
However, most existing studies treat resilience as a single aggregated construct, overlooking the phase specific nature and structured mechanisms of response capability within supply chain disruption scenarios. Therefore, this study conceptualizes response capability as the operational competence of healthcare organizations to respond immediately, mobilize resources, and implement strategic actions at the point of disruption. It is positioned as the second stage dimension of the supply chain resilience mechanism and is empirically examined in the proposed research model.
2.3.3. Restorative Capability
Restorative capability refers to an organization’s ability to effectively reorganize resources, rebuild disrupted processes, restructure operational systems, and even regenerate capabilities following a supply chain disruption, thereby enabling the system to return to its original or an even more optimal state [39]. It represents the final and most decisive stage of supply chain resilience, determining whether the system can fully recover or even achieve post disruption performance improvement [40].
From the perspective of dynamic capabilities, restorative capability is essentially the strategic integration and reconstruction of prior absorptive and response efforts. It reflects not only operational recovery but also the organization’s transformative capacity for structural renewal and capability realignment [41]. Healthcare organizations with strong restorative capability can resume essential services, optimize critical nodes, and maximize operational efficiency even under resource constraints [42]. In complex, multi-stakeholder healthcare supply chains operating in dynamic environments, restoration also requires cross system coordination of economic, environmental, and social resources to ensure a stable and efficient restart, which is vital for the long term sustainability of pharmaceutical and medical operations [43].
However, in the context of healthcare supply chain management, how digital technologies can enhance organizational coordination and resource reconfiguration during the recovery stage remains an underexplored area. Therefore, this study further investigates restorative capability as a critical component of resilience and empirically examines its mediating role in the digital transformation decision optimization pathway.
2.4. Decision Optimization
Decision optimization in the healthcare supply chain has increasingly emerged as a central focus for ensuring operational efficiency, service safety, and long term sustainability [44]. As a multidimensional process, decision optimization involves comprehensive coordination across various supply chain stages, including resource procurement, inventory allocation, and patient end service delivery [45,46].
With the accelerated integration of artificial intelligence into healthcare systems, decision optimization is evolving beyond static, rule based models. It now entails the dynamic configuration of decision paths and resource structures, based on multi-source data and advanced analytics. Emerging technologies, particularly large language models (LLMs), support semantic interpretation, trend forecasting, and complex judgment, thus improving the quality and agility of strategic decisions [47,48].
To explore the underlying mechanisms of decision optimization in healthcare supply chains, this study adopts the Resource Based View (RBV) as its theoretical foundation. RBV emphasizes that organizations gain sustainable advantage by developing and leveraging rare, inimitable, and embedded internal resources [49]. In this context, digital capabilities, organizational agility, and process reconfiguration serve as essential enablers of intelligent decision systems.
However, existing research remains primarily focused on static reasoning, with limited exploration of how decision making structures operate in dynamic environments shaped by artificial intelligence, edge computing, and platform governance. Therefore, this study defines decision optimization as a context adaptive mechanism that combines technological intelligence, dynamic organizational capabilities, and resource reconfiguration to support strategic decision making. This conceptualization is further tested through empirical investigation.
3. Hypotheses Development
3.1. Research Hypothesis
3.1.1. Digital Intelligence and Decision Optimization
DIn the highly uncertain environment of healthcare, organizations are required to make high quality decisions that balance real time responsiveness, efficient resource allocation, and patient satisfaction [16,50]. As a key technological attribute of digital transformation, Digital Intelligence refers to the organization’s ability to leverage AI, big data analytics, and machine learning to enable predictive analysis, route optimization, and intelligent decision making [51]. Particularly in the context of healthcare supply chains, organizations must navigate complex trade offs among compliance, safety, and timely delivery necessitating a highly structured decision system that relies on advanced information processing and cross functional coordination [52]. The integration of intelligent technologies allows healthcare organizations to identify risk signals, simulate intervention strategies, and rapidly generate optimal decision paths, especially in areas such as inventory allocation, demand forecasting, and service flow management [53]. From the perspective of the Resource Based View (RBV), Digital Intelligence represents a distinctive and inimitable strategic resource that enhances the agility, precision, and sustainability of decision making systems [49,54]. Therefore, this study proposes the following hypothesis:
H1:
Digital Intelligence has a positive effect on Decision Optimization.
3.1.2. Digital Intelligence and Innovation Capability
The intelligent attributes of digital technologies and organizational innovation capabilities are increasingly becoming key drivers of transformation in the healthcare supply chain. Through digital intelligence, healthcare organizations are able to collect, share, and integrate data more effectively, which in turn facilitates knowledge creation, accelerates cross departmental integration, and supports new product development, process optimization, organizational restructuring, as well as the development of novel services and business models suited to complex medical environments [55,56,57]. In particular, the embedded application of artificial intelligence (AI) within healthcare networks demonstrates strong cross organizational innovation potential, especially in terms of knowledge integration, process coordination, and service automation [58,59]. Empirical findings by Belhadi et al. (2024) further indicate that under highly dynamic supply chain conditions, AI driven innovation mechanisms significantly enhance organizational innovation performance [41]. Therefore, this study proposes the following hypothesis:
H2:
Digital Intelligence has a positive effect on Innovation Capability.
3.1.3. Digital Intelligence and Supply Chain Resilience
Resilience capability, defined as a process based capacity comprising absorptive, response, and restorative functions, requires the integrated support of digital technologies, organizational resources, and structural mechanisms [60]. Among various digital transformation features, digital intelligence provides healthcare organizations with enriched information flows, more efficient resource allocation methods, and accelerated task execution mechanisms, thereby enabling dynamic adaptability [30,34]. Digital intelligence enhances absorptive capability by enabling proactive and predictive mechanisms. Through artificial intelligence and big data analytics, healthcare organizations can detect abnormal patterns in large scale datasets, helping decision makers identify potential sources of disruption and forecast future risks or demand fluctuations. This allows a shift from passive information reception to proactive early warning systems [61]. Regarding response capability, digital intelligent systems facilitate rapid scenario analysis, identify resource bottlenecks and task priorities, and enable route optimization, resource reallocation, and automatic task initiation via intelligent algorithms, significantly improving real time responsiveness [18,62]. Finally, digital intelligence empowers restorative capability by enabling organizations to self repair and reconfigure operations. AI based systems can predict recovery bottlenecks based on failure points and dynamically optimize recovery paths, thereby enhancing the efficiency of system reconstruction and the quality of service resumption [51]. Therefore, this study proposes the following hypothesis:
H3-1.
Digital Intelligence has a positive effect on Absorptive Capability.
H3-2.
Digital Intelligence has a positive effect on Response Capability.
H3-3.
Digital Intelligence has a positive effect on Restorative Capability.
3.1.4. Innovation Capability and Decision Optimization
Innovation capability is considered a critical enabler for strategic and intelligent decision making. Organizations with strong innovation capabilities are better positioned to leverage advanced digital technologies, optimize operational structures, and develop adaptive decision frameworks [63]. Innovation capability fosters the integration of new technologies into decision processes, enabling real time data utilization, predictive modeling, and scenario planning [54]. Moreover, innovation serves as a mediating mechanism that translates digital and big data competencies into enhanced strategic decisions and sustainable outcomes [64]. Kumar & Raj (2025) further emphasize that innovation capability strengthens supply chain performance by bridging data capabilities and decision optimization, particularly through enhanced supply chain integration and resilience [65]. Therefore, this study proposes the following hypothesis:
H4.
Innovation Capability has a positive effect on Decision Optimization.
3.1.5. Innovation Capability and Supply Chain Resilience
Although supply chain resilience can enhance an organization’s ability to adapt and recover, without sufficient support from innovation capability, its role may be limited to passive defense rather than proactive optimization [66]. Innovation capability enables the transformative application of digital technologies within healthcare supply chains, allowing organizations to more effectively absorb external information, respond to disruptions, and reconfigure service processes thus facilitating a shift from risk response to system evolution [8].
First, innovation capability enhances absorptive capability by fostering agile learning mechanisms and cross boundary information integration. Tetteh et al. (2025) noted that innovation oriented healthcare organizations can leverage data analytics and knowledge recombination to increase sensitivity to potential risks and improve the efficiency of information absorption [67]. Second, innovation capability strengthens the structural flexibility of response capability by supporting process modularization, platform based collaboration, and algorithmic optimization. Fernando et al. (2023) emphasized that technological innovation capability is a critical enabler for rapid adjustment and efficient resource allocation, especially in multi-organizational responses to sudden disruptions [68]. Finally, innovation facilitates restorative capability by enabling organizations to implement structural optimization and system reconfiguration following a crisis allowing not only a return to the previous state but also the achievement of superior performance [52]. Therefore, this study proposes the following hypothesis:
H5-1.
Innovation Capability has a positive effect on Absorptive Capability.
H5-2.
Innovation Capability has a positive effect on Response Capability.
H5-3.
Innovation Capability has a positive effect on Restorative Capability.
3.1.6. Supply Chain Resilience and Decision Optimization
Resilience capability in the healthcare supply chain refers to an integrative process capability constructed through embedded workflows, sensing systems, and feedback mechanisms, which collectively support timely, precise, and coordinated decision making [69]. First, absorptive capability acts as a precondition for decision optimization by enabling risk perception, data assimilation, and early warning, which help organizations form accurate cognitive assessments in the face of uncertainty or volatility [70]. Second, response capability determines the feasibility of organizational decisions. From the perspective of decentralized decision making, strong responsiveness allows for rapid command deployment and real time resource reallocation [71]. In the healthcare context, explainable AI enhances decision transparency and controllability, improves inventory turnover, and prevents resource mismatch [72]. Finally, restorative capability reflects the organization’s ability to recover from disruptions, serving as a foundation for decision system stability and continuity [73]. As shown by Vega et al. (2023), recovery capability influences how swiftly an organization can learn from interruptions, repair processes, and optimize its decision structure [74]. Therefore, this study proposes the following hypothesis:
H6-1.
Absorptive Capability has a positive effect on Decision Optimization.
H6-2.
Response Capability has a positive effect on Decision Optimization.
H6-3.
Restorative Capability has a positive effect on Decision Optimization.
3.1.7. The Mediated Effects of Innovation Capability and Supply Chain Resilience
In the highly dynamic context of healthcare supply chains, digital intelligence (DI), enabled by technologies such as artificial intelligence and big data analytics, empowers organizations to develop systematic capabilities for data sensing, analysis, and intelligent judgment. This forms a critical foundation for the development of innovation mechanisms and the activation of supply chain resilience [55,58]. Innovation capability (IC) plays a pivotal role in amplifying the positive effects of resilience mechanisms, enabling organizations to engage in process redesign, system reconfiguration, and service innovation in response to external disruptions or resource adjustments. These innovation driven actions contribute to more rational, efficient, and sustainable decision making processes [13,75].
First, DI driven innovation capability strengthens the value realization of absorptive capability. Innovation mechanisms improve the efficiency of information filtering, knowledge transformation, and solution generation, allowing resilience systems to more effectively convert external inputs into strategic decisions. As Belhadi et al. (2024) observed, in AI assisted environments, highly innovative organizations are more capable of transforming data insights into forward looking strategies, thereby improving predictive accuracy and decision quality in pharmaceutical supply chains [41]. Second, innovation capability enhances the operational flexibility of response capability. When resilience mechanisms trigger emergency responses, innovation facilitates the development of modular processes and platform based coordination mechanisms. These innovations support algorithmic modeling and task synchronization based on digital intelligence systems, improving the feasibility and effectiveness of crisis esponse decision making. Finally, the real time feedback and simulation functions provided by digital intelligence technologies require innovation capability to enable process restart, recovery, and structural optimization. Through innovation, organizations can reconfigure operations in a way that not only restores but also improves upon pre crisis performance [66].
Therefore, digital intelligence activates innovation capability, which in turn enhances the three sequential stages of resilience, absorptive, response, and restorative capabilities to jointly form an intelligence driven pathway for organizational adaptation and decision optimization. Therefore, this study proposes the following hypothesis:
H7.
Innovation Capability mediates the relationship between Digital Intelligence and Decision Optimization.
H8-1.
Absorptive Capability mediates the relationship between Digital Intelligence and Decision Optimization.
H8-2.
Response Capability mediates the relationship between Digital Intelligence and Decision Optimization.
H8-3.
Restorative Capability mediates the relationship between Digital Intelligence and Decision Optimization.
H9-1.
Innovation Capability and Absorptive Capability sequentially mediate the relationship between Digital Intelligence and Decision Optimization.
H9-2.
Innovation Capability and Response Capability sequentially mediate the relationship between Digital Intelligence and Decision Optimization.
H9-3.
Innovation Capability and Restorative Capability sequentially mediate the relationship between Digital Intelligence and Decision Optimization.
3.2. Research Model
This study develops a conceptual model and research hypotheses based on the Resource Based View (RBV) and Dynamic Capabilities Theory (DCT). The RBV provides a foundational theoretical lens for understanding how firms formulate strategic decisions to achieve sustainable competitive advantage (Ferreira et al., 2025). In particular, for healthcare supply chain systems undergoing digital transformation, it is essential to leverage internal digital technology resources in conjunction with the dynamic capabilities framework to enhance organizational processes [76]. By enabling supply chain innovation through digital technologies, organizations can enhance their supply chain resilience to effectively respond to external changes [32]. This process ultimately supports optimal decision making, strengthens organizational competitiveness, and contributes to sustainable performance in healthcare supply chains [77,78]. Therefore, this study proposes a research model in which intelligence, derived from digital transformation, serves as the independent variable. Its impact on decision optimization, the dependent variable, is examined through the mediating roles of supply chain innovation capability and supply chain resilience. The latter is conceptualized as consisting of absorptive capability, response capability, and restorative capability. The full model is presented in Figure 1.
3.3. Measurement
Based on the theoretical model and hypotheses proposed in this study, a structured questionnaire was designed. All measurement items were adapted from well established and validated scales in prior literature. Five items were used to measure each of the core constructs digital intelligence, innovation capability, and decision optimization while three items were assigned to each of the mediating variables: absorptive capability, response capability, and restorative capability. The full list of measurement items is presented in <Table 1>. 5 Likert scale was adopted for all items [79], capturing participants’ level of agreement with each statement, ranging from 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, to 5 = strongly agree.
3.4. Demographics
This study targeted managerial level respondents within organizations that constitute the healthcare supply chain in China. Data were collected through an online survey using the platform wjx.cn, employing a random sampling method. The survey was conducted over a five month period, from October 7, 2024, to March 7, 2025. A total of 381 questionnaires were collected. After removing 21 invalid responses due to missing or illogical information, 360 valid responses were retained, resulting in an effective response rate of 94.48%. General demographic characteristics of the respondents are presented in <Table 2>. Among the respondents, 69.2% were aged under 35, and 29.4% were aged between 35 and 50, indicating that most participants were young or mid-level managers within healthcare supply chain organizations. This age group is typically characterized by being energetic and open to adopting new technologies and ideas, although their managerial experience may be relatively limited. In terms of education, 62.2% held a bachelor’s degree. Regarding work experience, 54.4% of respondents had less than 5 years of experience, 37.8% had 5 to 15 years. As for the annual revenue of the respondents’ organizations, 54.7% were from small enterprises (less than CNY 40 million), 31.4% from medium sized enterprises (CNY 40 million to 400 million), and 13.9% from large enterprises (over CNY 400 million). In terms of ownership type, 61.9% of the enterprises were domestic, 31.1% were Sino foreign joint ventures, and 6.9% were wholly foreign owned enterprises.
4. Data Analysis and Results
4.1. Exploratory Factor Analysis
Exploratory factor analysis (EFA) was conducted using SPSS 26.0, and the results are presented in <Table 3>. To assess the suitability of the data for factor analysis, the Kaiser-Meyer-Olkin (KMO) measure and Bartlett’s test of sphericity were performed. The KMO value for this study was 0.914. According to Kaiser and Rice (1974), a KMO value close to 1 indicates strong correlations among variables and a high degree of factorability; values above 0.9 suggest that the data are “marvelous” for factor analysis [80]. Bartlett’s test yielded a Chi-square value of 6574.182 with 276 degrees of freedom, and the result was statistically significant (p < 0.001), indicating the presence of common factors among the items and supporting the appropriateness of conducting factor analysis [81]. Using the principal component analysis method, the cumulative variance explained by the extracted factors was 76.565%, exceeding the commonly accepted threshold of 50% [82], indicating a high level of explanatory power. The Varimax rotation was applied, and the rotated component matrix showed that all factor loadings had absolute values above 0.60, indicating good convergent validity between the items and their corresponding factors [83]. Additionally, the Cronbach’s alpha coefficients for each construct exceeded 0.80, meeting the criteria for excellent to good internal consistency [84], demonstrating that the measurement scales have high reliability.
4.2. Confirmatory Factor Analysis
Confirmatory factor analysis (CFA) was conducted using AMOS 24.0 to evaluate the consistency between the latent constructs and their corresponding measurement items, and to verify the validity of the measurement scales. The results are presented in <Table 4>. All constructs demonstrated Composite Reliability (C.R.) values greater than 0.80 and Average Variance Extracted (AVE) values above 0.50. According to conventional criteria (C.R. > 0.70; AVE > 0.50), these findings indicate good convergent validity [85]. Additionally, all standardized factor loadings exceeded 0.70, suggesting strong associations between each latent construct and its observed indicators. Model fit indices were also satisfactory, with Chi-square/df = 1.737 (< 3), GFI = 0.916, AGFI = 0.893, NFI = 0.939, RFI = 0.929, IFI = 0.973, TLI = 0.969, and CFI = 0.973. Most indices were close to or exceeded the recommended threshold of 0.90, indicating a good overall model fit and a well structured measurement model.
4.3. Correlation Analysis
Pearson correlation analysis was conducted using SPSS 26.0, and the results are presented in <Table 5>. According to the classification proposed by Schober et al. (2018), the absolute magnitude of the observed correlation coefficients can be interpreted as follows: 0.90~1.00 = very strong, 0.70~0.89 = strong, 0.40~0.69 = moderate, 0.10~0.39 = weak, and 0.00~0.10 = negligible correlation [86]. The results of this study indicated that the correlation coefficients among variables ranged from 0.307 to 0.613 and were all statistically significant at the 0.01 level (p < 0.01), suggesting significant positive correlations among the key constructs. In addition, the results of the discriminant validity test showed that the square roots of the AVEs for all constructs were greater than the absolute values of the inter construct correlations, indicating that the measurement model possesses satisfactory discriminant validity.
4.4. Path Analysis
Path analysis was conducted using AMOS 24.0, and the results are presented in <Table 6> [87]. The effect of DI on DO was not statistically significant (β = 0.132, p > 0.05), thus Hypothesis H1 was rejected. DI had a significant positive effect on IC (β = 0.308, p < 0.001), supporting Hypothesis H2. In addition, DI had significant positive effects on all three resilience capabilities: AC (β = 0.482, p < 0.001), supporting H3-1; RPC (β = 0.538, p < 0.001), supporting H3-2; and RTC (β = 0.518, p < 0.001), supporting H3-3. However, IC had a significant negative effect on DO (β = -0.420, p < 0.001), thus H4 was rejected. IC positively influenced AC (β = 0.314, p < 0.001), supporting H5-1; RPC (β = 0.362, p < 0.001), supporting H5-2; and RTC (β = 0.417, p < 0.001), supporting H5-3. All three resilience capabilities showed significant positive effects on DO (β = 0.351, p < 0.001), supporting H6-1; RPC (β = 0.341, p < 0.001), supporting H6-2; and RTC (β = 0.666, p < 0.001), supporting H6-3.
4.5. Test of Mediating Effect
Mediation analysis was conducted using AMOS 24.0 with 5,000 bootstrap samples, and the results are presented in <Table 7>. The total effect of DI on DO was found to be significantly positive (p < 0.001), while the direct effect was not statistically significant (p > 0.05). In contrast, the indirect effect was significantly positive (p < 0.001), indicating that IC and SCR function as full mediators in the relationship between DI and DO. Specifically, the indirect effect of DI-->IC-->DO was significantly negative (p < 0.001), thus Hypothesis H7 was rejected. Meanwhile, the indirect effects of DI-->AC-->DO, DI-->RPC-->DO, and DI-->RTC-->DO were all significant (p < 0.001), supporting Hypotheses H8-1, H8-2, and H8-3, respectively. Furthermore, the results of the serial mediation analysis revealed that the three paths DI-->IC-->AC-->DO, DI-->IC-->RPC-->DO, DI-->IC-->RTC-->DO were also statistically significant (p < 0.001), thereby supporting Hypotheses H9-1, H9-2, and H9-3 [88].
5. Discussion
5.1. Conclusions
To deepen the understanding of how strategic decision optimization can be achieved in the context of digital intelligence driven transformation of healthcare supply chains, this study empirically tested the causal relationships among digital intelligence, innovation capability, supply chain resilience (absorptive, response, and restorative capabilities), and decision optimization using structural equation modeling.
First, the path analysis results indicate that digital intelligence does not exert a statistically significant direct effect on decision optimization in healthcare supply chains. This finding contrasts with those of Senapati et al. (2024) and Ivanov et al. (2019) [49]. One plausible explanation is that digital technologies, when implemented as isolated tools without deep integration into management processes, may fail to directly enhance decision performance. As Tiwari et al. (2024) argue, digital infrastructure must be effectively aligned with network operations and process management to foster system autonomy and generate strategic advantages such as resilience, coordination, and efficiency [89]. The results of the mediation analysis in this study further support this view. Digital intelligence was found to have a significant direct positive effect on both innovation capability and supply chain resilience, consistent with findings by Apell & Eriksson (2023) and Abourokbah et al. (2023) [55,56]. However, in contrast to Al-Surmi et al. (2022), this study reveals that innovation capability has a significant negative effect on decision optimization [54]. A potential explanation lies in the fact that innovation in intelligent systems often entails high initial investment and operational complexity, which may hinder internal collaboration and decision efficiency in the short term [52]. In addition, the study confirms that innovation capability positively influences all three dimensions of resilience absorptive, response, and restorative capabilities, which aligns with the findings of Mehmood et al. (2025) and Adana et al. (2024) [66,71]. Moreover, each of the three resilience dimensions was shown to significantly enhance decision optimization.
Second, the mediation analysis demonstrates that, in line with Junaid et al. (2023), supply chain resilience (absorptive, response, and restorative capabilities) fully mediates the relationship between digital intelligence and decision optimization. Furthermore, innovation capability and resilience capability, as two distinct but complementary organizational competencies, were found to jointly contribute to the sustainable improvement of decision making [75]. Notably, however, innovation capability exhibits a significant negative full mediation effect between digital intelligence and decision optimization, which contradicts the findings of Jum’a et al. (2024) [64]. This raises the possibility that a non-linear mechanism, such as a U shaped mediation or moderation effect, may exist in this relationship [90]. In the early stages, low levels of innovation capability, characterized by underdeveloped platform integration and insufficient information sharing may disrupt supply chain coordination and diminish decision efficiency. However, as innovation capability matures and collaborative mechanisms improve, it may strengthen the adaptive responsiveness of the resilience system and enhance intelligent decision making support, ultimately leading to substantial improvements in decision performance [91].
5.2. Theoretical Contribution
This study establishes a theoretical foundation for future research on digital intelligent transformation in healthcare supply chains, grounded in an integrated perspective of the Resource Based View (RBV) and Dynamic Capabilities Theory (DCT). It deepens the theoretical understanding of how digital intelligence influences supply chain decision optimization, contributing significantly to theoretical development within this domain.
Firstly, this research systematically integrates RBV and DCT within the context of digital intelligent transformation in healthcare supply chain management. Previous studies predominantly emphasized the technological dimension, lacking theoretical and empirical exploration of how resources translate into capabilities, and how capabilities support strategic decision making. Due to inherent complexities, demand uncertainty, and high risk characteristics, healthcare supply chains require a dual theoretical perspective involving strategic resource identification and dynamic capability construction. By integrating RBV and DCT, this study theoretically clarifies how healthcare organizations leverage digital intelligence as a strategic resource, transforming it through dynamic pathways involving innovation capability and supply chain resilience into strategic advantages for decision optimization.
Secondly, this research develops a novel structured path analysis framework by conducting a refined three dimensional structural decomposition (absorptive, response, and restorative capabilities) of healthcare supply chain resilience. Furthermore, it proposes a chain mediated mechanism between innovation capability and supply chain resilience. This mechanism specifies that digital technological resources, when encountering environmental disruptions and resource constraints, do not operate in isolation. Instead, they require the activation of internal organizational innovation mechanisms and dynamic responsiveness via resilience mechanisms to systematically enhance resource allocation efficiency, risk management, and strategic decision making capability. Consequently, this study provides a fresh theoretical perspective and solid foundation for future fine grained theoretical construction and multi-level research in supply chain management.
5.3. Practical Implications
This study provides forward looking and practical managerial implications for achieving the sustainable and healthy development of healthcare supply chains in the context of digital intelligence transformation.
Firstly, based on the specific results of the path analysis, healthcare supply chain organizations can proactively adopt Real Time Inventory Management systems, Robotic Process Automation (RPA), and intelligent scheduling systems to enhance decision making timeliness. These technological solutions are particularly suitable for managing critical scenarios such as emergency logistics, vaccine distribution, and high turnover inventory items [92,93]. In terms of improving system intelligence, healthcare organizations can integrate AI based predictive algorithms, machine learning driven decision support systems, pharmaceutical demand forecasting models, and intelligent replenishment models. These technologies are crucial for chronic medication management, personalized prescription services, and telemedicine drug delivery processes [94].
Secondly, the identified mediation mechanisms also provide valuable managerial insights. Healthcare organizations should further enhance their process mechanisms by establishing multi-party collaborative platforms for early warning and response, facilitating real time data sharing and integration among hospitals, pharmaceutical companies, and logistics providers. For example, integrating hospital information systems (HIS), pharmaceutical enterprise resource planning (ERP) systems, and logistics transportation management systems (TMS) through standardized application programming interfaces (APIs) can enable real time data collection and dynamic analysis [95,96]. Meanwhile, healthcare organizations should establish contingency plans for redundant pharmaceutical resources, proactively engage alternative suppliers, third party logistics providers, and emergency inventory storage facilities, and create effective resource sharing and mobilization mechanisms [97]. These measures can significantly enhance the continuity and efficiency of healthcare supply chain decision making and service provision.
5.4. Limitations and Future Research
Despite offering valuable theoretical and practical insights into the digital transformation and continuous optimization of healthcare supply chains, this study is subject to several limitations that warrant further exploration.
First, the empirical analysis is based on cross sectional data. Given the progressive and phased nature of digital transformation, future research could benefit from longitudinal or panel data to more systematically examine how the development of digital capabilities influences the long term stability and sustainability of decision making performance.
Second, the data collected in this study are primarily drawn from healthcare supply chain organizations in mainland China. While representative to a certain extent, the findings may be limited by region specific institutional settings, healthcare system structures, and technological adoption environments. Thus, future studies should extend the research scope to other countries or regions, particularly those with different regulatory frameworks or levels of digital infrastructure in order to enable cross country comparisons and enhance the external validity and global relevance of the results.
Lastly, as emerging technologies such as generative artificial intelligence, the Internet of Things, and biometric systems become increasingly integrated into the healthcare sector, the scope of digital transformation continues to expand. Future research could incorporate these developments to re-examine their impact on supply chain resilience, organizational innovation behavior, and complex decision making processes, thereby providing more forward looking theoretical frameworks and strategic recommendations.
Author Contributions
Writing—original draft preparation and writing—review and editing, J.-Y.M.; Conceptualization and data analysis, T.-W.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets of this study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have influenced the work reported in this paper. There are no conflict of interest.
References
- Nguyen, A.; Lamouri, S.; Pellerin, R.; Tamayo, S.; Lekens, B. Data analytics in pharmaceutical supply chains: state of the art, opportunities, and challenges. International Journal of Production Research. 2022, 60, 6888–6907. [Google Scholar] [CrossRef]
- The IQVIA Institute. The Global Use of Medicines 2024: Outlook to 2028. 2024.
- Sun, X.; Li, X. Aging and chronic disease: public health challenge and education reform. Frontiers in public health. 2023, 11, 1175898. [Google Scholar] [CrossRef]
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas, 2022, 139, 6–11. [Google Scholar] [CrossRef]
- Avinash, B.; Joseph, G. Reimagining healthcare supply chains: a systematic review on digital transformation with specific focus on efficiency, transparency and responsiveness. Journal of Health Organization and Management. 2024, 38, 1255–1279. [Google Scholar] [CrossRef]
- Ali, O.; Abdelbaki, W.; Shrestha, A.; Elbasi, E.; Alryalat, M. A. A.; Dwivedi, Y. K. A systematic literature review of artificial intelligence in the healthcare sector: Benefits, challenges, methodologies, and functionalities. Journal of Innovation & Knowledge. 2023, 8, 100333. [Google Scholar]
- Mehedy, M. T. J.; Jalil, M. S.; Saeed, M.; Snigdha, E. Z.; Khan, N.; Hasan, M. M. Big Data and Machine Learning in Healthcare: A Business Intelligence Approach for Cost Optimization and Service Improvement. The American Journal of Medical Sciences and Pharmaceutical Research. 2025, 7, 115–135. [Google Scholar] [CrossRef]
- Arji, G.; Ahmadi, H.; Avazpoor, P.; Hemmat, M. Identifying resilience strategies for disruption management in the healthcare supply chain during COVID-19 by digital innovations: A systematic literature review. Informatics in Medicine Unlocked. 2023, 38, 101199. [Google Scholar] [CrossRef]
- Gera, N.; Singh, R. Identifying key drivers of supply chain resilience in Indian pharmaceutical industry for enhanced export performance. International Journal of Pharmaceutical and Healthcare Marketing. 2025. [CrossRef]
- Senna, P.; Reis, A.; Dias, A.; Coelho, O.; Guimarães, J.; Eliana, S. Healthcare supply chain resilience framework: antecedents, mediators, consequents. Production Planning & Control. 2023, 34, 295–309. [Google Scholar]
- Rehman, O. U.; Ali, Y. Enhancing healthcare supply chain resilience: decision-making in a fuzzy environment. The International Journal of Logistics Management. 2022, 33, 520–546. [Google Scholar] [CrossRef]
- Zamani, E. D.; Smyth, C.; Gupta, S.; Dennehy, D. Artificial intelligence and big data analytics for supply chain resilience: a systematic literature review. Annals of Operations Research. 2023, 327, 605–632. [Google Scholar] [CrossRef] [PubMed]
- Bag, S.; Dhamija, P.; Singh, R. K.; Rahman, M. S.; Sreedharan, V. R. Big data analytics and artificial intelligence technologies based collaborative platform empowering absorptive capacity in health care supply chain: An empirical study. Journal of Business Research. 2023, 154, 113315. [Google Scholar] [CrossRef]
- Khan, F. S.; Masum, A. A.; Adam, J.; Karim, M. R.; Afrin, S. AI in Healthcare Supply Chain Management: Enhancing Efficiency and Reducing Costs with Predictive Analytics. Journal of Computer Science and Technology Studies. 2024, 6, 85–93. [Google Scholar] [CrossRef]
- Uzhakova, N.; Fischer, S. Data-driven enterprise architecture for pharmaceutical R&D. Digital. 2024, 4, 333–371. [Google Scholar]
- Yadav, P. Digital transformation in the health product supply chain: a framework for analysis. Health Systems & Reform. 2024, 10, 2386041. [Google Scholar]
- Dadhich, A.; Dadhich, P. Artificial Intelligence from Vaccine Development to Pharmaceutical Supply Chain Management in Post-COVID-19 Period. In Blockchain, IoT, and AI Technologies for Supply Chain Management.2023, 143-161.
- Long, P.; Lu, L.; Chen, Q.; Chen, Y.; Li, C.; Luo, X. Intelligent selection of healthcare supply chain mode–an applied research based on artificial intelligence. Frontiers in Public Health. 2023, 11, 1310016. [Google Scholar] [CrossRef]
- Abdollahi, A.; Ebrahimpour, M.; Ramazanian, M.; Moradi, M. Intelligent distributed supply chain management in the pharmaceutical industry. Journal of Strategic Management Studies. 2024, 14, 141–167. [Google Scholar]
- Shen, J.; Bu, F.; Ye, Z.; Zhang, M.; Ma, Q.; Yan, J.; Huang, T. Management of drug supply chain information based on “artificial intelligence+ vendor managed inventory” in China: perspective based on a case study. Frontiers in Pharmacology. 2024, 15, 1373642. [Google Scholar] [CrossRef]
- Al-Shboul, M. D. A. Do artificial intelligence system adoptions foster production management supply chain performance in pharmaceutical manufacturing firms? An empirical exploring study from the MENA region. Business Process Management Journal. 2024, 30, 2427–2455. [Google Scholar] [CrossRef]
- Tian, S.; Wu, L.; Ciano, M. P.; Ardolino, M.; Pawar, K. S. Enhancing innovativeness and performance of the manufacturing supply chain through datafication: The role of resilience. Computers & Industrial Engineering. 2024, 188, 109841. [Google Scholar]
- Moderno, O. B. D. S.; Braz, A. C.; Nascimento, P. T. D. S. Robotic process automation and artificial intelligence capabilities driving digital strategy: a resource-based view. Business Process Management Journal. 2024, 30, 105–134. [Google Scholar] [CrossRef]
- Wang, D.; Liu, W.; Liang, Y.; Wei, S. Decision optimization in service supply chain: the impact of demand and supply-driven data value and altruistic behavior. Annals of Operations Research. 2023, 1–22. [Google Scholar] [CrossRef]
- Martínez-Peláez, R.; Ochoa-Brust, A.; Rivera, S.; Félix, V. G.; Ostos, R.; Brito, H.; Mena, L. J. Role of digital transformation for achieving sustainability: mediated role of stakeholders, key capabilities, and technology. Sustainability. 2023, 15, 11221. [Google Scholar] [CrossRef]
- Adama, H. E.; Popoola, O. A.; Okeke, C. D.; Akinoso, A. E. Economic theory and practical impacts of digital transformation in supply chain optimization. International Journal of Advanced Economics. 2024, 6, 95–107. [Google Scholar] [CrossRef]
- Bahrami, M.; Shokouhyar, S.; Seifian, A. Big data analytics capability and supply chain performance: the mediating roles of supply chain resilience and innovation. Modern Supply Chain Research and Applications. 2022, 4, 62–84. [Google Scholar] [CrossRef]
- Liu, Z.; Shi, Y.; Yang, B. Open innovation in times of crisis: An overview of the healthcare sector in response to the COVID-19 Pandemic. Journal of Open Innovation: Technology, Market, and Complexity. 2022, 8, 21. [Google Scholar] [CrossRef]
- Hendry, L. C.; Stevenson, M.; MacBryde, J.; Ball, P.; Sayed, M.; Liu, L. Local food supply chain resilience to constitutional change: the Brexit effect. International Journal of Operations & Production Management. 2019, 39, 429–453. [Google Scholar]
- Zhao, N.; Hong, J.; Lau, K. H. Impact of supply chain digitalization on supply chain resilience and performance: A multi-mediation model. International Journal of Production Economics. 2023, 259, 108817. [Google Scholar] [CrossRef]
- Anozie, U. C.; Adewumi, G.; Obafunsho, O. E.; Toromade, A. S.; Olaluwoye, O. S. Leveraging advanced technologies in Supply Chain Risk Management (SCRM) to mitigate healthcare disruptions: A comprehensive review. World Journal of Advanced Research and Reviews. 2024, 23, 1039–1045. [Google Scholar]
- Stadtfeld, G. M.; Gruchmann, T. Dynamic capabilities for supply chain resilience: a meta-review. The International Journal of Logistics Management. 2024, 35, 623–648. [Google Scholar] [CrossRef]
- Singh, R. K.; Modgil, S. Adapting to disruption: the impact of agility, absorptive capacity and ambidexterity on supply chain resilience. International Journal of Productivity and Performance Management. 2025, 74, 637–658. [Google Scholar] [CrossRef]
- Tortorella, G.; Prashar, A.; Samson, D.; Kurnia, S.; Fogliatto, F. S.; Capurro, D.; Antony, J. Resilience development and digitalization of the healthcare supply chain: an exploratory study in emerging economies. The International Journal of Logistics Management. 2023, 34, 130–163. [Google Scholar] [CrossRef]
- Wright, A. M.; Snowdon, A.; Saunders, M.; Trampas, D. The necessity of healthcare supply chain resilience for crisis preparedness. In Healthcare Management Forum. 2024, 37, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Naz, F.; Luthra, S.; Vashistha, R.; Kumar, V.; Garza-Reyes, J. A.; Chhabra, D. Digging DEEP: Futuristic building blocks of omni-channel healthcare supply chains resiliency using machine learning approach. Journal of Business Research. 2023, 162, 113903. [Google Scholar] [CrossRef]
- Saarinen, L.; Oddsdottir, H.; Rehman, O. Resilience through appropriate response: a simulation study of disruptions and response strategies–case COVID-19 and the grocery supply chain. Operations Management Research. 2024, 17, 1078–1099. [Google Scholar] [CrossRef]
- Maheshwari, P.; Kamble, S. S.; Belhadi, A.; Gupta, S.; Mangla, S. K. Resilient healthcare network for simultaneous product allocations during supply chain disruptions. In Supply Chain Forum: An International Journal. 2024, 25, 407–427. [Google Scholar] [CrossRef]
- Tetteh, F. K.; Nyamekye, B.; Williams, E.; Attah, J.; Degbe, F. D. Effect of Supply Chain Analytics on Healthcare Supply Chain Performance: The Relevance of Building Responsive, Resilience, Restoration (3rs) and Desorptive Capabilities. Resilience, Restoration (3rs) and Desorptive Capabilities.
- Vanany, I.; Ali, M. H.; Tan, K. H.; Kumar, A.; Siswanto, N. A supply chain resilience capability framework and process for mitigating the COVID-19 pandemic disruption. IEEE Transactions on Engineering Management. 2021. [CrossRef]
- Belhadi, A. , Mani, V., Kamble, S. S., Khan, S. A. R., & Verma, S. Artificial intelligence-driven innovation for enhancing supply chain resilience and performance under the effect of supply chain dynamism: an empirical investigation. Annals of Operations Research. 2024, 333, 627–652. [Google Scholar]
- Tortorella, G. L.; Prashar, A.; Antony, J.; Fogliatto, F. S.; Gonzalez, V.; Godinho Filho, M. Industry 4.0 adoption for healthcare supply chain performance during COVID-19 pandemic in Brazil and India: the mediating role of resilience abilities development. Operations Management Research. 2024, 17, 389–405. [Google Scholar] [CrossRef]
- Silva, A. C.; Marques, C. M.; de Sousa, J. P. A simulation approach for the design of more sustainable and resilient supply chains in the pharmaceutical industry. Sustainability. 2023, 15, 7254. [Google Scholar] [CrossRef]
- Badejo, O.; Ierapetritou, M. Optimization of pharmaceutical supply chains: Navigating disruptions and operational uncertainty utilizing risk measures. AIChE Journal. 2025, e18770. [Google Scholar] [CrossRef]
- Mahdavimanshadi, M.; Anaraki, M. G.; Mowlai, M.; Ahmadirad, Z. A multistage stochastic optimization model for resilient pharmaceutical supply chain in COVID-19 pandemic based on patient group priority. In 2024 Systems and Information Engineering Design Symposium (SIEDS). 2024, 382–387. [Google Scholar]
- Li, Q.; Zhang, H.; Liu, K.; Zhang, Z. J.; Jasimuddin, S. M. Linkage between digital supply chain, supply chain innovation and supply chain dynamic capabilities: An empirical study. The International Journal of Logistics Management. 2024, 35, 1200–1223. [Google Scholar] [CrossRef]
- Aghaei, R.; Kiaei, A. A.; Boush, M.; Vahidi, J.; Barzegar, Z.; Rofoosheh, M. The Potential of Large Language Models in Supply Chain Management: Advancing Decision-Making, Efficiency, and Innovation. arXiv preprint. 2025, 2501.15411. [Google Scholar]
- Wang, Y.; Wang, J.; Zhang, H.; Song, J. Bridging Prediction and Decision: Advances and Challenges in Data-Driven Optimization. Nexus. 2025. [CrossRef]
- Ivanov, D.; Dolgui, A.; Das, A.; Sokolov, B. Digital supply chain twins: Managing the ripple effect, resilience, and disruption risks by data-driven optimization, simulation, and visibility. Handbook of ripple effects in the supply chain. 2019, 309–332. [Google Scholar]
- Kasparis, E.; Huang, Y.; Lin, W.; Vasilakis, C. Improving timeliness in the neglected tropical diseases preventive chemotherapy donation supply chain through information sharing: a retrospective empirical analysis. PLoS Neglected Tropical Diseases. 2021, 15, e0009523. [Google Scholar] [CrossRef]
- Shah, A.; Che Mat, C. R.; Ibrahim, A.; Zhang, Y.; Muzammil, S. Digital supply chain reshaping industrial ecology: a study from the Pharma Industry. In Industrial ecology: a fusion of material and energy in green supply chain context. 2024, 107-123.
- Adhikari, A.; Joshi, R.; Basu, S. Collaboration and coordination strategies for a multi-level AI-enabled healthcare supply chain under disaster. International Journal of Production Research. 2025, 63, 497–523. [Google Scholar] [CrossRef]
- Lee, K. L.; Wong, S. Y.; Alzoubi, H. M.; Al Kurdi, B.; Alshurideh, M. T.; El Khatib, M. Adopting smart supply chain and smart technologies to improve operational performance in manufacturing industry. International Journal of Engineering Business Management. 2023, 15, 18479790231200614. [Google Scholar] [CrossRef]
- Al-Surmi, A.; Bashiri, M.; Koliousis, I. AI based decision making: combining strategies to improve operational performance. International Journal of Production Research. 2022, 60, 4464–4486. [Google Scholar] [CrossRef]
- Abourokbah, S. H.; Mashat, R. M.; Salam, M. A. Role of absorptive capacity, digital capability, agility, and resilience in supply chain innovation performance. Sustainability. 2023, 15, 3636. [Google Scholar] [CrossRef]
- Apell, P.; Eriksson, H. Artificial intelligence (AI) healthcare technology innovations: the current state and challenges from a life science industry perspective. Technology Analysis & Strategic Management. 2023, 35, 179–193. [Google Scholar]
- Papalexi, M.; Bamford, D.; Breen, L. Key sources of operational inefficiency in the pharmaceutical supply chain. Supply Chain Management: An International Journal. 2020, 25, 617–635. [Google Scholar] [CrossRef]
- Gama, F.; Magistretti, S. Artificial intelligence in innovation management: A review of innovation capabilities and a taxonomy of AI applications. Journal of Product Innovation Management. 2025, 42, 76–111. [Google Scholar] [CrossRef]
- Cannavale, C.; Esempio Tammaro, A.; Leone, D.; Schiavone, F. Innovation adoption in inter-organizational healthcare networks–the role of artificial intelligence. European Journal of Innovation Management. 2022, 25, 758–774. [Google Scholar] [CrossRef]
- Furstenau, L. B.; Zani, C.; Terra, S. X.; Sott, M. K.; Choo, K. K. R.; Saurin, T. A. Resilience capabilities of healthcare supply chain and supportive digital technologies. Technology in Society. 2022, 71, 102095. [Google Scholar] [CrossRef]
- Saha, R. Empowering Absorptive Capacity in Healthcare Supply Chains Through Big Data Analytics and AI-Driven Collaborative Platforms: A Prisma-Based Systematic Review. Innovatech Engineering Journal. 2024, 1, 10–70937. [Google Scholar] [CrossRef]
- Kazancoglu, I.; Ozbiltekin-Pala, M.; Mangla, S. K.; Kazancoglu, Y.; Jabeen, F. Role of flexibility, agility and responsiveness for sustainable supply chain resilience during COVID-19. Journal of cleaner production. 2022, 362, 132431. [Google Scholar] [CrossRef]
- Makarevic, M.; Tas, P. G. Strategic decision-making in process optimization of healthcare technology manufacturing. Journal of Supply Chain Management Science. 2024, 5(3-4), 117-142.
- Jum'a, L.; Zimon, D.; Madzik, P. Impact of big data technological and personal capabilities on sustainable performance on Jordanian manufacturing companies: the mediating role of innovation. Journal of Enterprise Information Management. 2024, 37, 329–354. [Google Scholar] [CrossRef]
- Kumar, R. R.; Raj, A. Big data adoption and performance: mediating mechanisms of innovation, supply chain integration and resilience. Supply Chain Management: An International Journal. 2025, 30, 67–85. [Google Scholar] [CrossRef]
- Mehmood, S.; Nazir, S.; Fan, J.; Nazir, Z. Achieving supply chain sustainability: enhancing supply chain resilience, organizational performance, innovation and information sharing: empirical evidence from Chinese SMEs. Modern Supply Chain Research and Applications. 2025, 7, 2–29. [Google Scholar] [CrossRef]
- Tetteh, F. K.; Amoako, D. K.; Kyeremeh, A.; Atiki, G.; Degbe, F. D.; Nyame, P. E. D. Unraveling the interplay between supply chain analytics and healthcare supply chain performance: establishing an underlying mechanism and a boundary condition. International Journal of Quality & Reliability Management. 2025, 42, 752–783. [Google Scholar]
- Fernando, Y.; Tseng, M. L.; Nur, G. M.; Ikhsan, R. B.; Lim, M. K. Practising circular economy performance in Malaysia: managing supply chain disruption and technological innovation capability under industry 4.0. International Journal of Logistics Research and Applications. 2023, 26, 1704–1727. [Google Scholar] [CrossRef]
- Revilla, E.; Acero, B.; Sáenz, M. J. Resilience in the Supply Chain. In The Palgrave Handbook of Supply Chain Management. 2024, 601–625. [Google Scholar]
- Javan-Molaei, B.; Tavakkoli-Moghaddam, R.; Ghanavati-Nejad, M.; Asghari-Asl, A. A data-driven robust decision-making model for configuring a resilient and responsive relief supply chain under mixed uncertainty. Annals of Operations Research. 2024, 1–38. [Google Scholar] [CrossRef]
- Adana, S.; Manuj, I.; Herburger, M.; Cevikparmak, S.; Celik, H.; Uvet, H. Linking decentralization in decision-making to resilience outcomes: a supply chain orientation perspective. The International Journal of Logistics Management. 2024, 35, 256–280. [Google Scholar] [CrossRef]
- Sadeghi, K.; Ojha, D.; Kaur, P.; Mahto, R. V.; Dhir, A. Explainable artificial intelligence and agile decision-making in supply chain cyber resilience. Decision Support Systems. 2024, 180, 114194. [Google Scholar] [CrossRef]
- Xiang, Y.; Li, X.; Liu, W.; Luo, F.; Wang, M. Enhancing chromium supply chain security through resilience strategies: decision support based on system dynamics simulations. Journal of Cleaner Production. 2025, 144981. [Google Scholar] [CrossRef]
- Vega, D.; Arvidsson, A.; Saiah, F. Resilient supply management systems in times of crisis. International Journal of Operations & Production Management. 2023, 43, 70–98. [Google Scholar]
- Junaid, M.; Zhang, Q.; Cao, M.; Luqman, A. Nexus between technology enabled supply chain dynamic capabilities, integration, resilience, and sustainable performance: An empirical examination of healthcare organizations. Technological Forecasting and Social Change. 2023, 196, 122828. [Google Scholar] [CrossRef]
- Tyagi, S. Analytics in healthcare supply chain management in the new normal era: a review and future research agenda. Benchmarking: An International Journal. 2024, 31, 2151–2175. [Google Scholar] [CrossRef]
- Hussain, M.; Ajmal, M.; Subramanian, G.; Khan, M.; Anas, S. Challenges of big data analytics for sustainable supply chains in healthcare–a resource-based view. Benchmarking: An International Journal. 2024, 31, 2897–2918. [Google Scholar] [CrossRef]
- Li, Q.; Zhang, H.; Liu, K.; Zhang, Z. J.; Jasimuddin, S. M. Linkage between digital supply chain, supply chain innovation and supply chain dynamic capabilities: An empirical study. The International Journal of Logistics Management. 2024, 35, 1200–1223. [Google Scholar] [CrossRef]
- Joshi, A.; Kale, S.; Chandel, S.; Pal, D. K. Likert scale: Explored and explained. British journal of applied science & technology. 2015, 7, 396. [Google Scholar]
- Kaiser, Henry F. ; Rice, John. "Little Jiffy, Mark Iv". Educational and Psychological Measurement. 1974, 34, 111–117. [Google Scholar] [CrossRef]
- Arsham, H.; Lovric, M. Bartlett's Test. International encyclopedia of statistical science. 2011, 2, 20–23. [Google Scholar]
- Suhr, D. D. Principal component analysis vs. exploratory factor analysis. SUGI 30 proceedings. 2005, 203, 1–11. [Google Scholar]
- Fabrigar, L. R.; Wegener, D. T.; MacCallum, R. C.; Strahan, E. J. Evaluating the use of exploratory factor analysis in psychological research. Psychological methods. 1999, 4, 272. [Google Scholar] [CrossRef]
- Babbie, E.; Wagner-Huang, W. E.; Zaino, J. Adventures in social research: Data analysis using IBM SPSS statistics. Sage Publications. 2022.
- Fornell, C.; Larcker, D.F. Structural equation models with unobservable variables and measurement error: Algebra and statistics. J. Mark. Res. 1981, 18, 382–388. [Google Scholar] [CrossRef]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation coefficients: Appropriate use and interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- Alwin, D. F.; Hauser, R. M. The decomposition of effects in path analysis. American sociological review. 1975, 37–47. [Google Scholar] [CrossRef]
- Wen, Z.; Ye, B. Analyses of mediating effects: the development of methods and models. Advances in psychological Science. 2014, 22, 731. [Google Scholar] [CrossRef]
- Tiwari, M. K.; Bidanda, B.; Geunes, J.; Fernandes, K.; Dolgui, A. Supply chain digitisation and management. International Journal of Production Research. 2024, 62, 2918–2926. [Google Scholar] [CrossRef]
- Kalnins, A. Should moderated regressions include or exclude quadratic terms? Present both! Then apply our linear algebraic analysis to identify the preferable specification. Organizational Research Methods. 2024, 27, 29–63. [Google Scholar] [CrossRef]
- Xiao, J. , & Bao, Y. Partners' knowledge utilization and exploratory innovation: the moderating effect of competitive and collaborative relationships. International Journal of Operations & Production Management. 2022, 42, 1356–1383. [Google Scholar]
- Roosevelt, S. C.; Veemaraj, E.; Kirubakaran, S. Real Time Stock Inventory Management System. In 2024 8th International Conference on Inventive Systems and Control (ICISC). 2024, 156–162. [Google Scholar]
- Tayab, A.; Li, Y. The contribution of the RPA technology in enhancing better business performance in Warehouse management. IEEE Access. 2024, 12, 142419–142426. [Google Scholar] [CrossRef]
- Mousa, B. A.; Al-Khateeb, B. Predicting medicine demand using deep learning techniques: A review. Journal of intelligent systems. 2023, 32, 20220297. [Google Scholar] [CrossRef]
- Naz, A.; Ali, M.; Cheema, S. M.; Pires, I. M. Cloud-Based Framework for Data Exchange to Enhance Global Healthcare. Procedia Computer Science. 2024, 241, 570–575. [Google Scholar] [CrossRef]
- Torab-Miandoab, A.; Samad-Soltani, T.; Jodati, A.; Akbarzadeh, F.; Rezaei-Hachesu, P. A unified component-based data-driven framework to support interoperability in the healthcare systems. Heliyon. 2024, 10. [Google Scholar] [CrossRef]
- Contreras, N. A.; Guerrero, W.; Besiou, M. Pharmaceutical Inventory Management Using Industry 4.0 Technologies Based on Collaborative Demand: A System Dynamics Approach. 7th European Conference on Industrial Engineering and Operations Management. 2024, 957-973.
Figure 1.
Research Model.
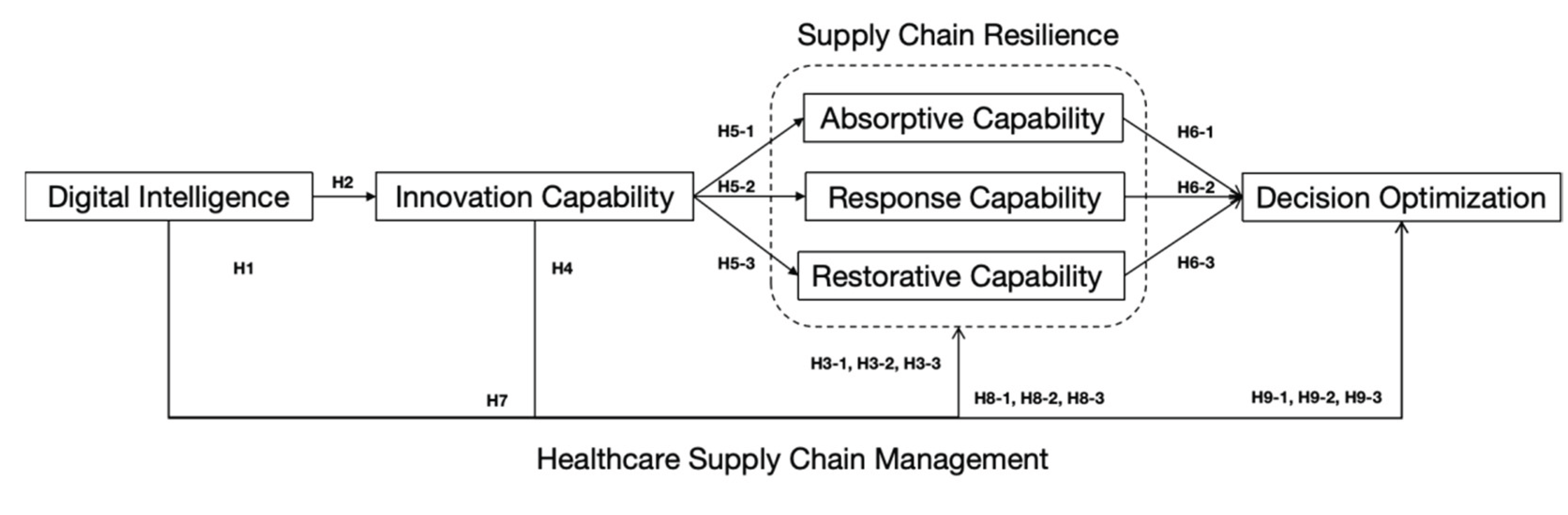

Table 1.
Variable Measurement.
| Variables | Items | Sources | |
|---|---|---|---|
| Digital Intelligence | DI1 | We use smart technologies to control and optimize production processes. | Lee et al., (2023) [53] |
| DI2 | We use smart technologies to analyze data and support decision making. | ||
| DI3 | We use smart technologies to plan and allocate resources effectively. | ||
| DI4 | We use smart technologies to monitor and control inventory levels. | ||
| DI5 | We use smart technologies to estimate and control costs more accurately. | ||
| Innovation Capability | IC1 | We continuously innovate in our supply chain collaborations and partnerships. | Jum'a et al., (2024) [64] |
| IC2 | We continuously upgrade our digital technology systems to support innovation. | ||
| IC3 | We are committed to delivering innovative supply services. | ||
| IC4 | We pursue innovation in our supply chain process management. | ||
| IC5 | We continuously develop supply market resources for innovative capability. | ||
| Absorptive Capability | AC1 | We are able to prepare backup resources in advance to respond to potential supply chain disruptions. | Zhao et al., (2023)[30] Abourokbah et al., (2023) [55] |
| AC2 | We are able to anticipate potential risks before supply chain disruptions occur. | ||
| AC3 | We are able to sense market changes before supply chain disruptions happen. | ||
| Response Capability | RPC1 | We are able to make the right risk management decisions at the time of supply chain disruptions. | Zhao et al., (2023)[30] Kazancoglu et al., (2022) [62] |
| RPC2 | We are able to maintain supply chain connectivity and collaboration at the time of disruptions. | ||
| RPC3 | We are able to adapt our response strategies during supply chain disruptions. | ||
| Restorative Capability | RTC1 | We are able to extract useful knowledge from disruptions and achieve better supply chain operations. | Zhao et al., (2023) [30] |
| RTC2 | We are able to speedily and efficiently return to normal operations after being disrupted. | ||
| RTC3 | We are able to restructure resources and develop new continuity plans after being disrupted. | ||
| Decision Optimization | DO1 | We make managerial decisions more efficiently and accurately with the support of digital technologies. | Al-Surmi et al., (2022) [54] |
| DO2 | We identify and respond to risks more effectively by leveraging digital technologies. | ||
| DO3 | We improve our strategic planning through the use of digital tools and data analytics. | ||
| DO4 | We optimize our operational decision-making with the aid of digital technologies. | ||
| DO5 | We make product development decisions that are increasingly driven by data and digital intelligence. | ||
Table 2.
Demographic Characteristics of the Respondents.
| Variables | Category | Frequency | Ratio (%) |
|---|---|---|---|
| Gender | Male | 160 | 44.4 |
| Female | 200 | 55.6 | |
| Age | < 35 | 249 | 69.2 |
| 35 ~ 50 | 106 | 29.4 | |
| > 50 | 5 | 1.4 | |
| Education Background | Associate Degree | 53 | 14.7 |
| Bachelor | 224 | 62.2 | |
| Master | 54 | 15.0 | |
| Doctor | 29 | 8.1 | |
| Professional Experience | < 5 | 196 | 54.4 |
| 5 ~ 15 | 136 | 37.8 | |
| > 5 | 28 | 7.8 | |
| Annual Revenue of the Respondent’s Organization (CNY) | < 40 million | 197 | 54.7 |
| 40 ~ 400 million | 113 | 31.4 | |
| > 400 million | 50 | 13.9 | |
| Ownership Type of the Organization | Domestic Enterprise | 223 | 61.9 |
| Sino-Foreign Joint Venture | 112 | 31.3 | |
| Wholly Foreign-Owned Enterprise | 25 | 6.9 |
Table 3.
Exploratory Factor Analysis Results.
| Variables | Codes | Factor Loading | Cronbach’s α | |||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | |||
| Digital Intelligence | DI1 | 0.050 | 0.054 | 0.772 | 0.155 | 0.061 | 0.170 | 0.874 |
| DI2 | 0.197 | 0.052 | 0.709 | 0.117 | 0.150 | 0.119 | ||
| DI3 | 0.252 | 0.101 | 0.811 | 0.104 | 0.089 | 0.096 | ||
| DI4 | 0.231 | 0.170 | 0.745 | 0.122 | 0.121 | 0.158 | ||
| DI5 | 0.194 | 0.165 | 0.764 | 0.055 | 0.153 | 0.095 | ||
| Innovation Capability | IC1 | 0.020 | 0.779 | 0.116 | 0.091 | 0.117 | 0.150 | 0.880 |
| IC2 | 0.086 | 0.790 | 0.093 | 0.079 | 0.072 | 0.108 | ||
| IC3 | 0.023 | 0.765 | 0.131 | 0.069 | 0.115 | 0.125 | ||
| IC4 | 0.066 | 0.802 | 0.101 | 0.110 | 0.146 | 0.055 | ||
| IC5 | 0.075 | 0.853 | 0.033 | 0.096 | 0.029 | 0.127 | ||
| Absorptive Capability | AC1 | 0.252 | 0.140 | 0.179 | 0.893 | 0.114 | 0.067 | 0.963 |
| AC2 | 0.247 | 0.174 | 0.146 | 0.891 | 0.072 | 0.075 | ||
| AC3 | 0.250 | 0.143 | 0.175 | 0.902 | 0.078 | 0.093 | ||
| Response Capability | RPC1 | 0.251 | 0.151 | 0.189 | 0.079 | 0.839 | 0.124 | 0.898 |
| RPC2 | 0.263 | 0.189 | 0.135 | 0.131 | 0.800 | 0.137 | ||
| RPC3 | 0.237 | 0.147 | 0.180 | 0.056 | 0.850 | 0.115 | ||
| Restorative Capability | RTC1 | 0.327 | 0.248 | 0.187 | 0.155 | 0.118 | 0.736 | 0.842 |
| RTC2 | 0.251 | 0.212 | 0.249 | 0.090 | 0.137 | 0.777 | ||
| RTC3 | 0.287 | 0.263 | 0.269 | 0.024 | 0.200 | 0.692 | ||
| Decision Optimization | DO1 | 0.790 | 0.163 | 0.217 | 0.179 | 0.178 | 0.217 | 0.931 |
| DO2 | 0.833 | 0.004 | 0.191 | 0.215 | 0.194 | 0.170 | ||
| DO3 | 0.680 | 0.120 | 0.276 | 0.179 | 0.207 | 0.138 | ||
| DO4 | 0.840 | 0.044 | 0.195 | 0.175 | 0.185 | 0.163 | ||
| DO5 | 0.771 | 0.007 | 0.218 | 0.255 | 0.232 | 0.245 | ||
| Eigen Value(Rotated) | 3.921 | 3.629 | 3.531 | 2.776 | 2.490 | 2.028 | - | |
| Explained Variance(%) | 16.339 | 15.122 | 14.711 | 11.568 | 10.376 | 8.449 | ||
| Cumulative Variance(%) | 16.339 | 31.461 | 46.172 | 57.740 | 68.117 | 76.565 | ||
| KMO=0.914, Bartlett=6574.182, Sig=0.000, df=276 | ||||||||
Table 4.
Confirmatory Factor Analysis Results.
| Variables | Codes | Unstd. | S.E. | T-Value | p | Std. | C.R. | AVE |
|---|---|---|---|---|---|---|---|---|
| Digital Intelligence | DI1 | 1 | 0.703 | 0.876 | 0.587 | |||
| DI2 | 1.069 | 0.087 | 12.249 | *** | 0.698 | |||
| DI3 | 1.217 | 0.084 | 14.501 | *** | 0.840 | |||
| DI4 | 1.319 | 0.094 | 14.032 | *** | 0.809 | |||
| DI5 | 1.189 | 0.089 | 13.414 | *** | 0.769 | |||
| Innovation Capability | IC1 | 1 | 0.764 | 0.883 | 0.602 | |||
| IC2 | 1.001 | 0.069 | 14.416 | *** | 0.756 | |||
| IC3 | 1.001 | 0.072 | 13.970 | *** | 0.735 | |||
| IC4 | 1.127 | 0.075 | 15.079 | *** | 0.787 | |||
| IC5 | 0.967 | 0.060 | 16.019 | *** | 0.833 | |||
| Absorptive Capability | AC1 | 1 | 0.947 | 0.963 | 0.896 | |||
| AC2 | 0.987 | 0.029 | 34.594 | *** | 0.926 | |||
| AC3 | 1.030 | 0.025 | 40.989 | *** | 0.966 | |||
| Response Capability | RPC1 | 1 | 0.887 | 0.899 | 0.748 | |||
| RPC2 | 0.919 | 0.046 | 19.876 | *** | 0.827 | |||
| RPC3 | 0.995 | 0.046 | 21.738 | *** | 0.880 | |||
| Restorative Capability | RTC1 | 1 | 0.817 | 0.851 | 0.656 | |||
| RTC2 | 1.000 | 0.060 | 16.550 | *** | 0.815 | |||
| RTC3 | 1.251 | 0.077 | 16.172 | *** | 0.798 | |||
| Decision Optimization | DO1 | 1 | 0.849 | 0.932 | 0.734 | |||
| DO2 | 1.110 | 0.047 | 23.376 | *** | 0.908 | |||
| DO3 | 0.812 | 0.050 | 16.360 | *** | 0.732 | |||
| DO4 | 1.091 | 0.048 | 22.778 | *** | 0.895 | |||
| DO5 | 1.079 | 0.048 | 22.413 | *** | 0.887 | |||
| CMIN=411.783, DF=237, CMIN/DF=1.737, GFI=0.916, AGFI=0.893, NFI=0.939, RFI=0.929, IFI=0.973, TLI=0.969, CFI=0.973, RMSEA=0.045, SRMR=0.036 | ||||||||
1 Note: ***p﹤0.000.
Table 5.
Descriptive Statistics and Bivariate Correlations Results.
| Variables | M | SD | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|---|---|
| Digital Intelligence | 3.343 | 0.754 | 0.766 | |||||
| Innovation Capability | 3.114 | 0.603 | .307** | 0.776 | ||||
| Absorptive Capability | 3.900 | 0.830 | .392** | .311** | 0.947 | |||
| Response Capability | 3.131 | 0.823 | .423** | .348** | .314** | 0.865 | ||
| Restorative Capability | 3.223 | 0.742 | .532** | .464** | .351** | .473** | 0.810 | |
| Decision Optimization | 3.940 | 0.932 | .536** | .240** | .531** | .557** | .613** | 0.857 |
1 Note: **p﹤0.01.
Table 6.
Path Analysis Results.
| Hypothesis | Path | Estimate | SE | CR | p | Results |
|---|---|---|---|---|---|---|
| H1 | DI-->DO | 0.132 | 0.084 | 1.571 | 0.116 | Rejected |
| H2 | DI-->IC | 0.308 | 0.057 | 5.419 | *** | Supported |
| H3-1 | DI-->AC | 0.482 | 0.078 | 6.168 | *** | Supported |
| H3-2 | DI-->RPC | 0.538 | 0.081 | 6.660 | *** | Supported |
| H3-3 | DI-->RTC | 0.518 | 0.063 | 8.272 | *** | Supported |
| H4 | IC-->DO | -0.420 | 0.082 | -5.126 | *** | Rejected |
| H5-1 | IC-->AC | 0.314 | 0.081 | 3.855 | *** | Supported |
| H5-2 | IC-->RPC | 0.362 | 0.083 | 4.393 | *** | Supported |
| H5-3 | IC-->RTC | 0.417 | 0.063 | 6.627 | *** | Supported |
| H6-1 | AC-->DO | 0.351 | 0.048 | 7.371 | *** | Supported |
| H6-2 | RPC-->DO | 0.341 | 0.054 | 6.354 | *** | Supported |
| H6-3 | RTC-->DO | 0.666 | 0.095 | 6.997 | *** | Supported |
| CMIN=431.904, DF=240, CMIN/DF=1.80, GFI=0.912, AGFI=0.890, NFI=0.936, RFI=0.926, IFI=0.970, TLI=0.966, CFI=0.970, RMSEA=0.047, SRMR=0.045 | ||||||
1 Note: *p﹤0.05, **p﹤0.01 and ***p﹤0.001(two-tailed).
Table 7.
Mediating Effect Test Results.
| Hypothesis | Path | Estimation | S.E. | Bias-Corrected 95% CI | Results | ||
|---|---|---|---|---|---|---|---|
| Lover | Upper | p | |||||
| Total effect | |||||||
| DI-->DO | 0.858 | 0.101 | 0.668 | 1.065 | *** | - | |
| Direct effect | |||||||
| DI-->DO | 0.132 | 0.099 | -0.054 | 0.333 | 0.172 | - | |
| Indirect effect | |||||||
| DI-->DO | 0.726 | 0.102 | 0.547 | 0.941 | *** | - | |
| H7 | DI-->IC-->DO | -0.130 | 0.040 | -0.223 | -0.067 | *** | Rejected |
| H8-1 | DI-->AC-->DO | 0.169 | 0.041 | 0.100 | 0.261 | *** | Supported |
| H8-2 | DI-->RPC-->DO | 0.183 | 0.041 | 0.115 | 0.278 | *** | Supported |
| H8-3 | DI-->RTC-->DO | 0.345 | 0.070 | 0.230 | 0.505 | *** | Supported |
| H9-1 | DI-->IC-->AC-->DO | 0.034 | 0.011 | 0.018 | 0.063 | *** | Supported |
| H9-2 | DI-->IC-->RPC-->DO | 0.038 | 0.015 | 0.017 | 0.077 | *** | Supported |
| H9-3 | DI-->IC-->RTC-->DO | 0.086 | 0.025 | 0.048 | 0.155 | *** | Supported |
1 Note: 5000 bootstrap samples. 2 Note: *p﹤0.05, **p﹤0.01 and ***p﹤0.001(two-tailed).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



