
Submitted:
05 June 2025
Posted:
06 June 2025
You are already at the latest version
Abstract
Mandibular fractures are common in maxillofacial trauma and require precise diagnosis for optimal management. This study evaluates the applicability of the AO CMF classification system in an African setting, aiming to create a structured CT-based profile of mandibular fractures. A retrospective cross-sectional study was conducted over six months at the Central and University Teaching Hospitals of Yaoundé. CT scans of 201 patients were analyzed, and 82 cases of mandibular fractures were identified and classified. Young adult males were predominantly affected, with motorcycle-related accidents being the main cause. Fractures mostly involved the basal bone, particularly in the symphyseal and body regions. The majority were simple fractures, though displaced and fragmented patterns were also observed. The AO CMF classification allowed for detailed mapping of fracture sites, types, and associated dental injuries. This study highlights the importance of standardized diagnostic tools like the AO CMF classification in improving the assessment and management of mandibular trauma in resource-limited settings.
Keywords:
Mandibular fractures
; AO CMF classification
; CT scan
; maxillofacial trauma
; Cameroon
1. Introduction
Maxillofacial trauma refers to any injury compromising the integrity of the face, typically resulting from direct or indirect mechanical forces [1]. Mandibular fractures are a common outcome of such trauma, largely due to the mandible’s prominent position and protective function [2]. Early and thorough evaluation is essential to determine prognosis and guide appropriate treatment [3]. In this regard, the use of advanced imaging modalities is crucial, particularly for mandibular fractures. Given their complex morphology, multidetector computed tomography (MDCT), along with multiplanar reformation (MPR) and 3D reconstruction, is often required for accurate assessment [4]. This approach enables detailed visualization of fracture lines and displacement, while minimizing radiation exposure compared to multiple conventional radiographs [5].
Accurate assessment of maxillofacial fractures also depends on the use of standardized classification systems, which facilitate communication among healthcare professionals and support clinical decision-making [6]. Although several classification systems exist, many suffer from inconsistency and lack of clarity. With the advent of modern radiological tools, classification systems for mandibular trauma—once hindered by inadequate imaging—have evolved to improve clinical accuracy. In this context, the AO CMF (Association for the Study of Internal Fixation – Cranio-Maxillofacial) classification offers a structured and systematic approach to categorizing such injuries, thereby enhancing communication and treatment planning [7].
However, despite its methodological strengths, the real-world applicability of the AO CMF classification remains underexplored, particularly in resource-limited healthcare settings. To date, the integration of modern radiological classifications such as the AO CMF system in Sub-Saharan African clinical practice has rarely been documented, highlighting the need for region-specific evaluations. This study aims to establish a comprehensive CT-based profile of mandibular fractures diagnosed at two major referral hospitals in Yaoundé, Cameroon, while evaluating the practicality and clinical utility of applying the AO CMF classification in an African context.
2. Materials and Methods
This study was conducted as a descriptive, cross-sectional, retrospective analysis at the Central Hospital and University Hospital Center of Yaoundé, located in the political capital of Cameroon. The study aimed to evaluate the applicability of the AO CMF classification in assessing mandibular fractures based on CT scan data.
2.1. Study Design and Population
We included patients aged 18 years and older who underwent cranio-maxillo-facial CT scans for maxillofacial trauma during the study period from November 1st, 2023 to April 30th, 2024. Only those with identifiable mandibular fractures were selected. These patients were admitted to the Radiology and Medical Imaging departments at the two hospitals. The inclusion criteria were based on the availability of CT scans that clearly showed mandibular fractures, and no exclusion criteria were applied.
2.2. Data Collection and Protocol
Data were extracted from patient files and imaging records. The imaging analysis was performed using the MicroDicom DICOM Viewer (32-bit) version 2024. All data were anonymized to protect patient privacy, and no direct patient contact was involved, thus eliminating the need for additional informed consent. Patient data, including sociodemographic information (age, sex), trauma etiology, and the presence of dental injuries, were recorded on individual survey sheets.
2.3. Imaging Analysis
CT scans were analyzed to identify mandibular fractures, classifying them according to the AO CMF classification system. The fractures were categorized by their location on the basal bone, the type of fracture (simple, displaced, comminuted), the involvement of adjacent areas, and any associated dental injuries. Multiplanar reformation (MPR) and 3D reconstruction were used to improve the accuracy of fracture site and displacement assessments.
2.4. Study Variables
The study focused on several key variables:
- Sociodemographic characteristics: age, sex, and fracture etiology.
- Scannographic findings: fracture location (symphyseal, body, angle, etc.), type of fracture, extension to adjacent areas, involvement of the alveolar process, bone loss, atrophy, displacement, and involvement of the condylar process (base, neck, head), as well as deformation or distortion of the condylar process and changes to the vertical ramus height. The classification of dental injuries was done according to the Dental Trauma Guide.
2.5. Statistical Analysis
The data were entered into a database and analyzed using SPSS software (version 25.0). Descriptive statistics were used to summarize quantitative data and qualitative data. Results were presented in tables and graphs for better clarity and understanding.
3. Results
3.1. Sociodemographic and Clinical Characteristics
Between November 1st, 2023 and April 30th, 2024, 201 cranio-maxillo-facial CT scans were performed for maxillofacial trauma. Of these, 82 met the inclusion criteria for our study.
- The mean age of participants was 29.8 years, with a standard deviation of ±7.5 years.
- The age group 18-28 was the most represented (50%), followed by 28-38 (40.24%), (Table 1).
- Males represented 89.02% of the study population, yielding a sex-ratio of 8.1.
3.2. Etiology of Fractures
Road traffic accidents (RTA) were by far the leading cause of fractures, representing 70.7% of cases. The other causes included falls (12.2%), assaults (8.5%), and fights (8.5%), see in Table 2.
3.3. CT Scan Findings of Mandibular Fractures
- Mandibular fractures predominantly affected the basal bone (90.2%), with fewer cases involving the alveolar bone (9.8%).
A significant majority (72%) of fractures were confined to one area, while 28% exhibited extension to adjacent areas as shown in Figure 2.
3.4. Dental and Periodontal Lesions
- 67.1% of mandibular fractures affected the alveolar region, with tooth avulsions and coronoradicular fractures accounting for nearly 60% of all cases (Figure 3).
- Minor (Grade 1) and Major (Grade 2) bone fragmentation occurred in 22% and 7.3% of cases, respectively (Figure 4).
- Bone displacement was a significant finding in approximately one-third (31.7%) of cases.
- We observed a relatively low proportion of cases with bone loss (4.9%).
- Most patients (97.6%) showed no significant bone resorption, maintaining a mandibular bone height of over 20 mm (Table 5).
3.5. Articular Process Fractures
3.6. Articular Process Head Distortion
- A majority of mandibular fractures (93.9%) showed no distortion of the articular process head. 4.9% had in situ distortion, and 1.2% had displaced distortion (Figure 5).
- Mandibular fractures did not alter the vertical ramus height in 91.5% of cases, while 8.5% showed loss of height.
3.7. Classification of Mandibular Fractures: AO CMF Coding Framework
A complete mapping of the observed fractures according to the AO CMF classification is summarized in Table 8.
4. Discussion
4.1. Socio-Demographic Characteristics
In our study, the median age of patients was approximately 30 years, with an interquartile range of ±7.5 years and age extremes ranging from 18 to 54 years. This aligns with findings by Chen et al. in China (2020), who reported a mean age of 30.08 ± 13.47 years [8]. Similarly, Boffano et al. (2015) observed mean ages of 34.8 years in Turin and 32 years in Amsterdam in their comparative European study on mandibular fractures [9].
Regarding age distribution, our findings are consistent with those of Moshy et al. in Tanzania and Adeleke et al. in sub-Saharan Africa (2023), both of whom reported a higher incidence among individuals aged 21–40 years and 18–40 years, respectively [10,11].
We observed a pronounced gender disparity, with 89.0% of cases involving males and 11.0% involving females, yielding a male-to-female ratio of 8:1. This male predominance mirrors the findings of Afrooz et al. in the United States (80.0% male prevalence) [12], Kane et al. in Senegal (115:13 ratio) [13], and Anyanechi et al. in Nigeria, who reported a ratio of 4.4:1 in 2011 [14]. These patterns suggest that sociocultural factors—particularly increased risk-taking behaviors among men—may contribute significantly to the observed disparity.
4.2. Etiology of Fractures
Road traffic accidents (RTAs) were the leading cause of mandibular fractures in our cohort, accounting for more than 70% of cases. Falls, assaults, and interpersonal violence collectively contributed to approximately 29.3%. These results align with those of Sandeep et al. in India (2023), who also identified RTAs as the predominant etiology [15], as well as Bouguila et al. in Tunisia (45% of cases) [16], and Santos et al. in Brazil, where 21.05% of fractures were attributed to motorcycle accidents [17]. Similarly, Anyanechi et al. found that 79.9% of fractures were due to RTAs [14].
In our setting, the majority of these accidents involved two-wheeled vehicles—commonly used as motorcycle taxis in Cameroon. The frequent lack of helmet use significantly increases the risk of mandibular trauma and severe injuries. These local factors—type of transport, absence of stringent traffic regulations, and poor safety practices—likely explain the predominance of RTAs Ngaba Mambo et al. [18].
By contrast, Rocton et al. at La Pitié-Salpêtrière Hospital in Paris, France found that brawls were the main cause (57%), followed by RTAs (12%) [19]. Likewise, Boffano et al. [9] and Afrooz et al. [12] reported assaults as the leading cause of fractures in Europe and the US, respectively.
These differences underscore the influence of geographical, socioeconomic, and cultural contexts on fracture etiology. In areas with limited road infrastructure and weak safety enforcement, RTAs tend to dominate, whereas in more regulated urban settings, interpersonal violence may be a more significant cause.
4.3. CT Scan Features
4.3.1. Fracture Configuration
CT scan analysis revealed that 90.2% of mandibular fractures occurred in the basal bone. Of these, 74.4% were simple fractures, often indicative of lower-energy trauma such as minor accidents or falls. In contrast, 25.6% of fractures were comminuted, suggesting exposure to high-impact forces. Anyanechi et al. previously reported a lower rate of simple fractures (44.3%) [14].
4.3.2. Anatomical Distribution
The most common fracture site was the Symphysis/Parasymphyseal region (42.7%), followed by the Body (23.2%), Articular process (19.5%), and Angle/Ramus region (14.6%). These findings are similar to those reported by Kane et al. (40.3% of fracture sites) [13], Chen et al. (39.29% symphysis/parasymphysis fractures) [8], and Moshy et al. (37.9%) [10].
The Symphysis/Parasymphyseal region appears particularly vulnerable to impacts during frontal collisions. A significant proportion of fractures affect the mandibular body due to its length and exposure to longitudinal impact forces. The Articular process, with its lower incidence of fractures, suggests its involvement is significant due to forces transmitted during lateral impacts.
The results also show that the mandible, considered the bumper of the face, is particularly exposed due to the lack of protection during accidents, particularly those involving frontal collisions. The frequent absence of helmets among motorcycle riders, a widely used mode of transportation in Cameroon, further exposes the mandible to direct trauma.
Furthermore, the results differ from those of Rocton et al., where condylar (32%) and angular (32.0%) fractures were the most common [19]. In Cameroon, Messina Ebogo et al. noted that 33.9% of fractures were localized on the mandibular body, 25% in the parasymphyseal region, and 20% on the mandibular ramus [4]. Similarly, Keubou et al. reported that 35.08% of fractures were located on the horizontal branch and 28.07% on the symphysis/parasymphysis [20].
The discrepancies observed in the fracture locations between the different studies can be explained by several factors. In addition to the demographic and geographic specifics of the populations studied, the trauma mechanism, particularly the direction and intensity of the impact, plays a determining role. Moreover, local habits, such as the limited use of facial protection, increase the vulnerability of the mandible. Finally, the anatomical transition zones defined by the AO CMF, encompassing the interfaces between different anatomical regions, may also influence the types and locations of fractures observed.
These variations highlight the importance of contextualizing study findings according to local specifics and methodologies used, to better understand the causes and trends of mandibular fractures.
4.3.3. Fracture Extension
In 72% of cases, fractures were confined to a single anatomical site. The remaining 28% extended across multiple anatomical regions, as per the AO CMF classification. These complex fractures suggest high-energy trauma and often demand more sophisticated surgical management, increasing the risk of complications such as malunion or delayed healing.
4.3.4. Alveolar Process Involvement
The alveolar process was involved in 67.1% of cases. By comparison, Bicsák et al. (Germany, 2021) reported 40 fractures in the dentoalveolar region out of 541 total fracture sites [21]. The high incidence in our setting may reflect the predominance of frontal trauma. Involvement of this region directly affects dental integrity and often necessitates comprehensive treatment for both bone and dental structures.
4.3.5. Dental Injuries
Dental injuries were absent in 34.1% of patients, indicating that not all fractures result in tooth damage. However, 60.0% of cases presented with avulsions or coronal/root fractures, confirming the frequent association between mandibular trauma and dental injury.
Lieger et al. in Switzerland found that 47.5% of patients with facial fractures had dental involvement—39% in mandibular fractures and 14.5% in maxillary fractures [22]. Agbor Ashu et al. reported an even higher prevalence of dental trauma (83.5%) among victims of motorcycle accidents in Cameroon, with 62.3% experiencing tooth loss and 45.0% suffering coronal or root fractures [23]. These results support our findings and emphasize the need for integrated maxillofacial and dental care in trauma cases.
4.4. Bone Loss and Atrophy
In our study, the vast majority of observed mandibular fractures (95.1%) did not involve bone loss, suggesting these fractures, although present, generally do not result in significant bone destruction. The small proportion of cases with bone loss (4.9%) indicates severe fractures resulting in partial mandibular bone loss, although rare, should not be neglected. Additionally, 97.6% of patients showed no significant bone atrophy, with a vertical height of the mandibular bone exceeding 20 mm. This observation is consistent with our relatively young population, with a mean age of approximately 30 years, and minimal tooth loss. Mild bone atrophy observed in a small number of cases suggests some fractures may lead to minor bone loss, requiring monitoring to prevent atrophy progression.
4.5. Bone Fragmentation
Bone fragmentation was observed in 29.3% of cases. Of these, 70.7% were classified as grade 0 (no fragmentation), while 22% and 7.3% were categorized as minor (grade 1) and major fragmentation (grade 2), respectively. Fragmentation increases treatment complexity and the risk of complications, particularly in major cases that may require bone grafting or reconstructive surgery.
4.6. Displacement
The presence of osseous displacement in nearly one-third (31.7%) of cases indicates many traumas involved sufficient forces to displace bone fragments.
4.7. Fractures in the Anatomical Areas of the Articular Process
According to the distribution of fractures across the anatomical regions of the articular process as defined by the AO CMF, most fractures (80.5%) did not involve this structure. while fractures of the base, neck, and head represented 2.4%, 11%, and 6.1% of cases, respectively. This contrasts with studies by Thapa et al. [24] in China and Marker et al. [25] in the United Kingdom, where fractures of the neck and head were more common.
Additionally, 68.3% of observed fractures showed no bone displacement. Fragmented fractures demonstrated partial, complete, or dislocations of the articular head in 18.3%, 11%, and 2.4% of cases, respectively.
4.8. Angulation
Most mandibular fractures in our series showed no angulation of the condylar head, making surgical management potentially easier. Fractures with moderate (5-45°) and severe (>45°) angulation were rare, representing 8.5% and 1.2% of cases, respectively. These fractures resulted in Decrease in the vertical height of the mandibular ramus in only 8.5% of cases, suggesting most observed mandibular fractures preserved the integrity of this structure.
These findings align with previous literature and suggest the usefulness of CT imaging combined with AO CMF classification for standardized trauma assessment in low-resource settings.
5. Limitations of the Study
This study presents several limitations that should be considered when interpreting the results. First, the relatively small sample size and the single-region focus may limit the generalizability of our findings to broader populations. Second, although CT scan remains the gold standard for mandibular fracture assessment, the analysis was retrospective and did not include intra- or inter-observer variability measurements, which could have enhanced the reproducibility of the classification process. Additionally, the unavailability of the AO COIAC software at the time of this study required manual application of the AO CMF classification, which may have introduced a degree of subjectivity despite the use of validated criteria. Lastly, the absence of long-term clinical follow-up limits the correlation of radiological patterns with therapeutic outcomes.
Despite these limitations, this work provides valuable insight into the radiological profile of mandibular fractures in a resource-limited African setting and constitutes a meaningful first attempt to apply the AO CMF classification in this context.
6. Conclusions
Mandibular fractures remain a significant public health issue in our setting, given their prevalence and the functional, aesthetic, and psychosocial consequences they entail. Effective management requires heightened awareness among healthcare professionals and close interdisciplinary collaboration.
This study contributes to the growing body of data on mandibular fractures in the African context, underlining the importance of integrating standardized diagnostic tools to enhance the management of maxillofacial trauma.
The implementation of the AO CMF classification improves the clarity of fracture descriptions, streamlines communication between clinicians, and supports more structured therapeutic approaches. Expanding its use in routine practice could help standardize diagnosis and optimize treatment decisions—marking a key step toward more consistent clinical practices and improved care quality in mandibular trauma management.
Author Contributions
Conceptualization, M.G.A and J.M.N.V.; Methodology, J.M.N.V. and M.G.A; Software, M.G.A; Validation, M.G.A, A.M.S.E., and J.M.N.V.; Formal analysis, M.G.A; Investigation, M.G.A; Resources, Z.O.F; Data curation, M.G.A; Writing—original draft preparation, M.G.A.; Writing—review and editing, A.M.S.E., J.G.E.B., and J.M.N.V.; Visualization, M.G.A; Supervision, Z.O.F; Project administration, G.A.M.; Funding acquisition, Not applicable. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of the Faculty of Medicine and Biomedical Sciences, University of Yaoundé I (Approval N°0942/2024, March 2024). Administrative authorizations were also obtained from the Central Hospital of Yaoundé (N°184/2024) and the University Hospital Center of Yaoundé (N°058/2024).
Informed Consent Statement
Not applicable. This study was conducted retrospectively using anonymized data from hospital records. No direct patient interaction was involved.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request. Restrictions apply to the availability of these data due to ethical considerations and patient confidentiality.
Acknowledgments
The research team would like to extend sincere gratitude to Dr. Nkomy Vargas Marcello Jaime, Maxillofacial Surgeon, and Mr. Minkeng Simon Landry, Health Anthropologist and Deputy Director of the Mutuelle de Paris, for their support in the development of this work.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Salonen, E.M.; Koivikko, M.P.; Koskinen, S.K. Acute facial trauma in falling accidents: MDCT analysis of 500 patients. Emerg. Radiol. 2008, 15, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Denhez, F.; Giraud, O.; Seigneuric, J.B.; Paranque, A.R. Fractures de la mandibule. EMC Stomatologie 2005, 22-070-A-12. [Google Scholar]
- Sanogo, S. Apport de la tomodensitométrie (TDM) dans les traumatismes du massif facial dans le service d’imagerie médicale de l’hôpital de Sikasso: étude rétro prospective et prospective à propos de 100 cas. Thesis, Université du Mali, Mali, 2022. [Google Scholar]
- Messina, E.; Okala, P.; Ngaba, O.; Edouma, J.; Bombah, F.; Ongolo, P.; et al. Aspects cliniques et scanographiques des traumatismes mandibulaires à l’Hôpital Central de Yaoundé. Health Sci. Dis. 2020, 21, 88–90. [Google Scholar]
- Sanogo, S.; Kouma, A.; Cissé, I.; Guindo, I.; Diarra, O.; Traoré, O.; et al. Profil épidémiologique et tomodensitométrique des fractures maxillo-faciales post-traumatiques à Mopti au Mali. Pan Afr. Med. J. 2022, 41, 309. [Google Scholar] [CrossRef] [PubMed]
- Herve, V. Les traumatismes maxillo-faciaux et leurs implications en pratique odontologique: intérêts d’une approche pluri-disciplinaire. Thesis, Université de France, France, 2018. [Google Scholar]
- Mittermiller, P.A.; Bidwell, S.S.; Thieringer, F.M.; Cornelius, C.P.; Trickey, A.W.; Kontio, R.; et al. The Comprehensive AO CMF Classification System for Mandibular Fractures: A Multicenter Validation Study. Craniomaxillofac. Trauma Reconstr. 2019, 12, 254–265. [Google Scholar] [CrossRef]
- Chen, Y.T.; Chiu, Y.W.; Chang, Y.C.; Lin, C.W. Ten-year retrospective study on mandibular fractures in central Taiwan. J. Int. Med. Res. 2020, 48, 300060520915059. [Google Scholar] [CrossRef]
- Boffano, P.; Kommers, S.C.; Karagozoglu, K.H.; Gallesio, C.; Forouzanfar, T. Mandibular trauma: a two-centre study. Int. J. Oral Maxillofac. Surg. 2015, 44, 998–1004. [Google Scholar] [CrossRef]
- Moshy, J.R.; Msemakweli, B.S.; Owibingire, S.S.; Sohal, K.S. Pattern of mandibular fractures and helmet use among motorcycle crash victims in Tanzania. Afr. Health Sci. 2020, 20, 789–797. [Google Scholar] [CrossRef]
- Adeleke, A.I.; Hlongwa, M.; Makhunga, S.; Ginindza, T.G. Epidemiology of maxillofacial injuries in adults in sub-Saharan Africa: a scoping review. Inj. Epidemiol. 2023, 10, 58. [Google Scholar] [CrossRef]
- Afrooz, P.N.; Bykowski, M.R.; James, I.B.; Daniali, L.N.; Clavijo-Alvarez, J.A. The Epidemiology of Mandibular Fractures in the United States, Part 1: A Review of 13,142 Cases from the US National Trauma Data Bank. J. Oral Maxillofac. Surg. 2015, 73, 2361–2366. [Google Scholar] [CrossRef]
- Kane, M.; Tamba, B.; Gassama, C.B.; Diatta, M.; Ba, A.; Kounta, A.; et al. Clinical and radiological aspects of mandibular fractures: A review of 128 cases. Int. J. Oral Health Dent. 2021, 7, 282–286. [Google Scholar]
- Anyanechi, C.E.; Saheeb, B.D. Mandibular sites prone to fracture: analysis of 174 cases in a Nigerian tertiary hospital. Ghana Med. J. 2011, 45, 111–114. [Google Scholar]
- Sandeep Reddy, B.; Naik, D.; Kenkere, D. Role of multidetector computed tomography in evaluation of maxillofacial trauma. Cureus 2023, 15, e34910. [Google Scholar] [CrossRef] [PubMed]
- Bouguila, J. Epidemiology of maxillo-facial traumatology in Tunis. Rev. Stomatol. Chir. Maxillofac. 2008, 109, 353–357. [Google Scholar] [CrossRef]
- Martins, M.M.; Homsi, N.; Pereira, C.C.; Jardim, E.C.; Garcia, I.R. Jr. Epidemiological evaluation of mandibular fractures in a high-complexity hospital in Rio de Janeiro. J. Craniofac. Surg. 2011, 22, 2026–2030. [Google Scholar] [CrossRef]
- Ngaba Mambo, Y.; Yousse Moungang, D.; Zing, S.; Bengondo Messanga, C. Maxillofacial fractures due to road traffic accidents: epidemiological and clinical aspects in three hospitals in the city of Yaoundé. Int. J. Innov. Sci. Res. Rev. 2021, 3, 1529–1533. [Google Scholar]
- Rocton, S.; Chaine, A.; Ernenwein, D.; Bertolus, C.; Rigolet, A.; Bertrand, J.C.; et al. Fractures de la mandibule: épidémiologie, prise en charge thérapeutique et complications d’une série de 563. Rev. Stomatol. Chir. Maxillofac. 2007, 108, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Keubou, B.L.; Dsongwa, K.A.; Bengondo, M.C. Aspects épidémiologiques et cliniques des fractures mandibulaires traitées par procédé orthopédique à l’hôpital de district de Kumba, Cameroun. Health Sci. Dis. 2017, 18. Available online: http://www.hsdfmsb.org/index.php/hsd/article/view/938 (accessed on 13 April 2025).
- Bicsák, Á.; Abel, D.; Berbuesse, A.; Hassfeld, S.; Bonitz, L. Evaluation of mandibular fractures in a German nationwide trauma center between 2015 and 2017. J. Maxillofac. Oral Surg. 2022, 21, 904–910. [Google Scholar] [CrossRef]
- Lieger, O.; Zix, J.; Kruse, A.; Iizuka, T. Dental injuries associated with facial fractures. J. Oral Maxillofac. Surg. 2009, 67, 1680–1684. [Google Scholar] [CrossRef]
- Agbor, A.M.; Azodo, C.C.; Ebot, E.B.; Naidoo, S. Dentofacial injuries in commercial motorcycle accidents in Cameroon: pattern and cost implication of care. Afr. Health Sci. 2014, 14, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Thapa, S.; Wang, J.; Hu, H.T.; Zhang, F.G.; Ji, P. Epidemiology of surgically managed mandibular condylar fractures at a tertiary referral hospital in urban Southwest China. Open Dent. J. 2017, 11, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Marker, P.; Nielsen, A.; Bastian, H.L. Fractures of the mandibular condyle. Part 1: patterns of distribution of types and causes of fractures in 348 patients. Br. J. Oral Maxillofac. Surg. 2000, 38, 417–421. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Distribution Histogram of Fracture Types According to AO CMF Classification.
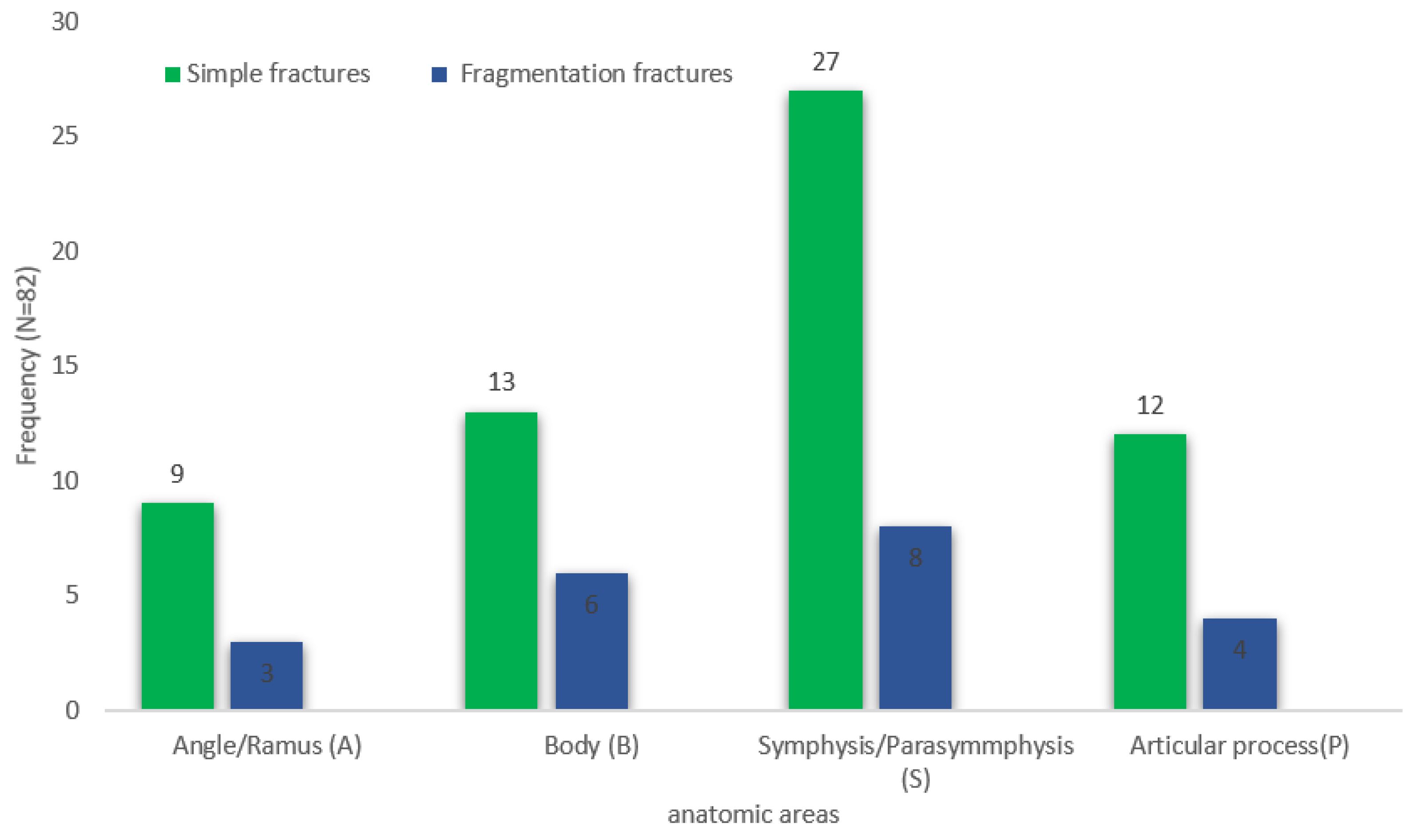
Figure 2.
Distribution Based on the Presence of Fracture Line Extension to Adjacent Areas.
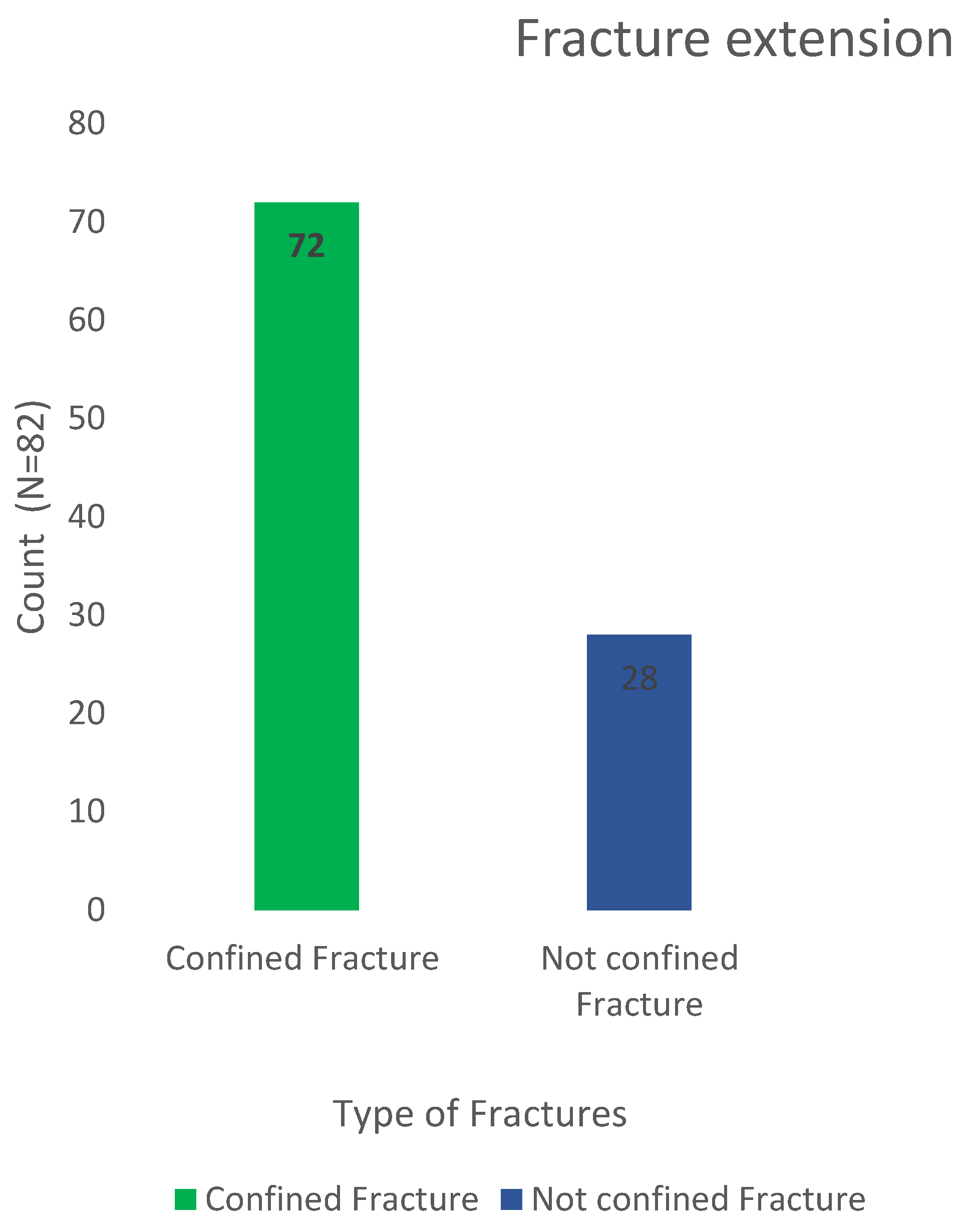
Figure 3.
Distribution of Dental and/or Periodontal Lesions in Mandibular Fractures.
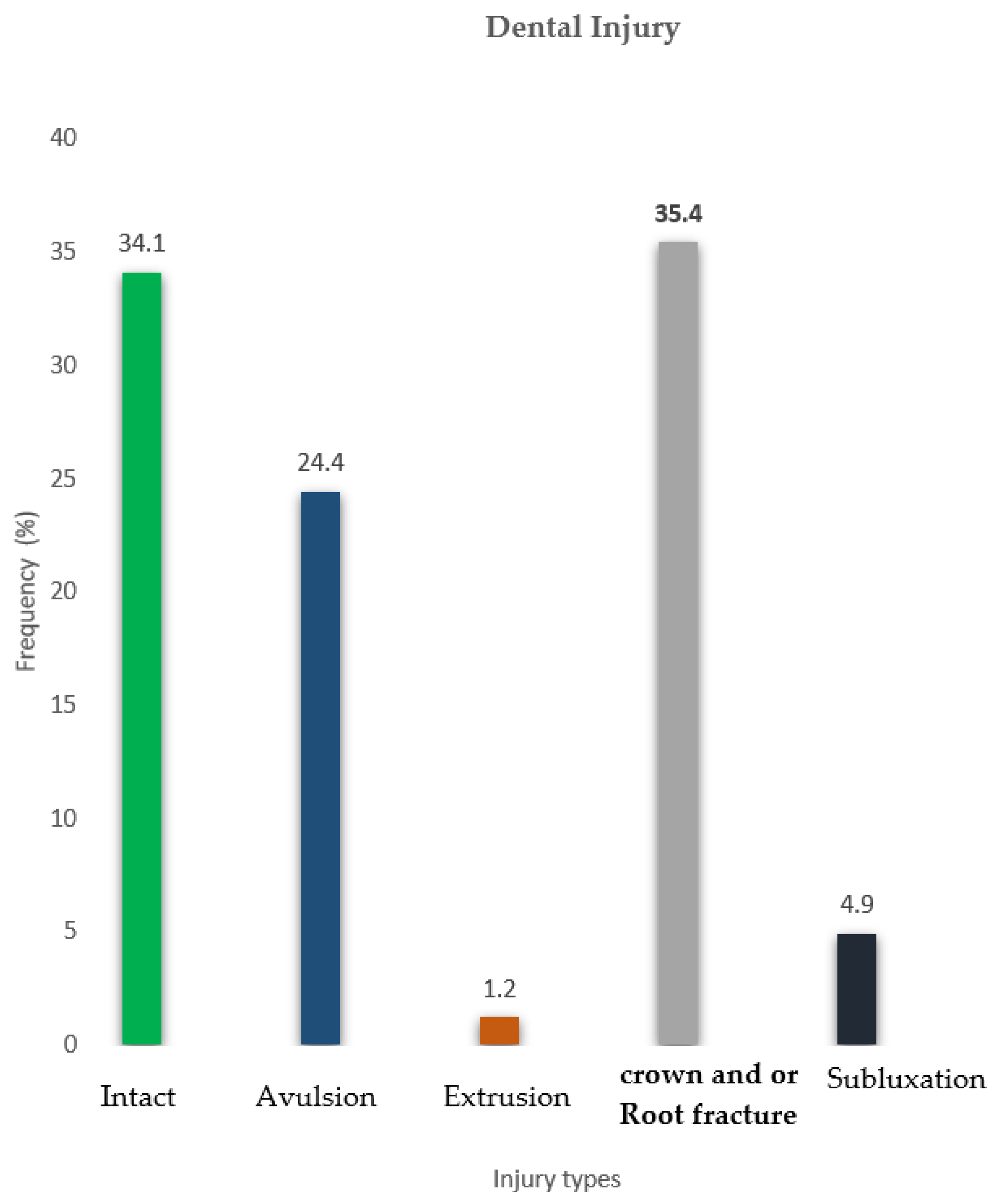
Figure 4.
Distribution of Bone Fragmentation
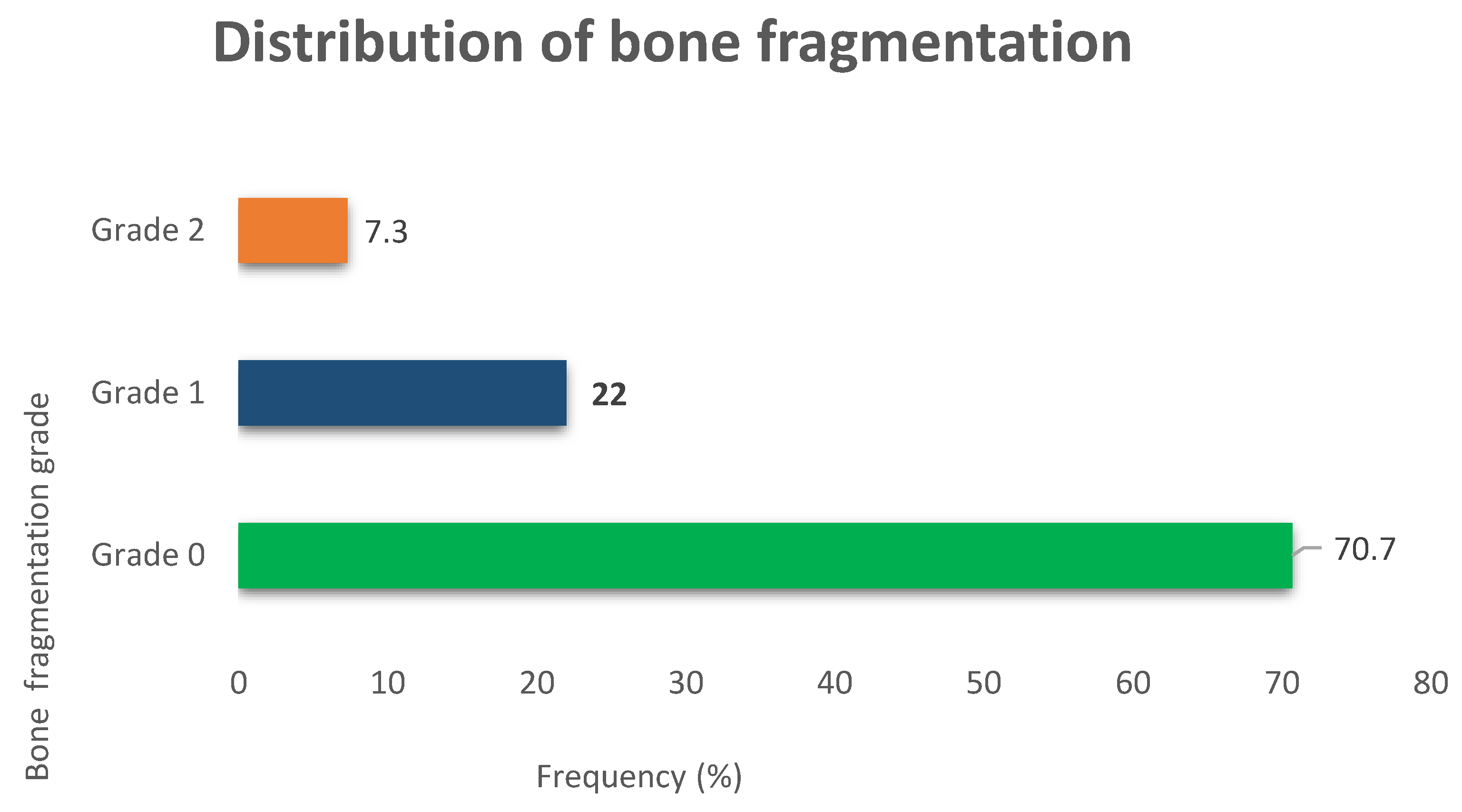
Figure 5.
Distribution of Articular Process Head Distortions in Mandibular Fractures.
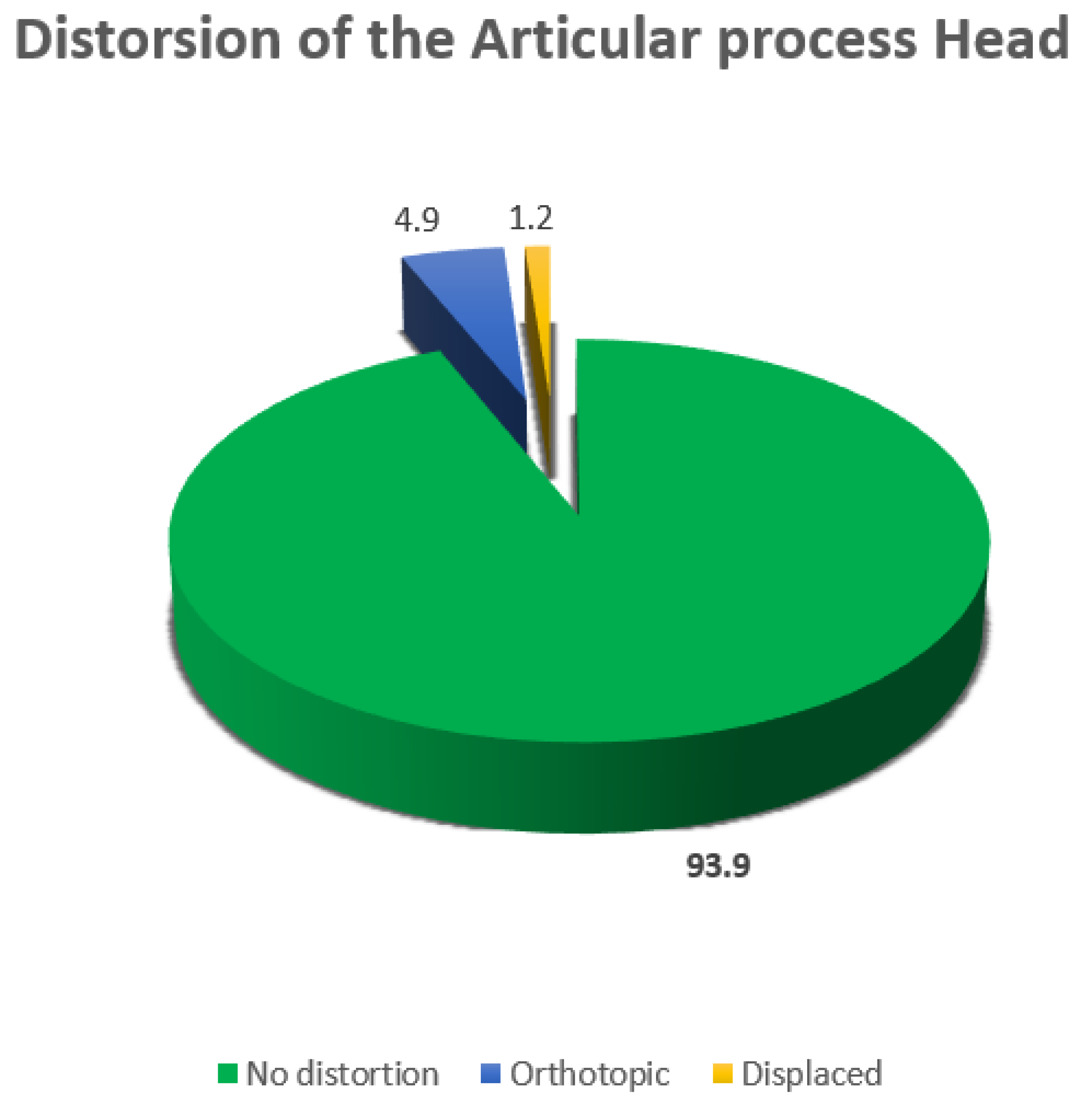
Figure 6.
Breakdown of Articular Head Angulation.
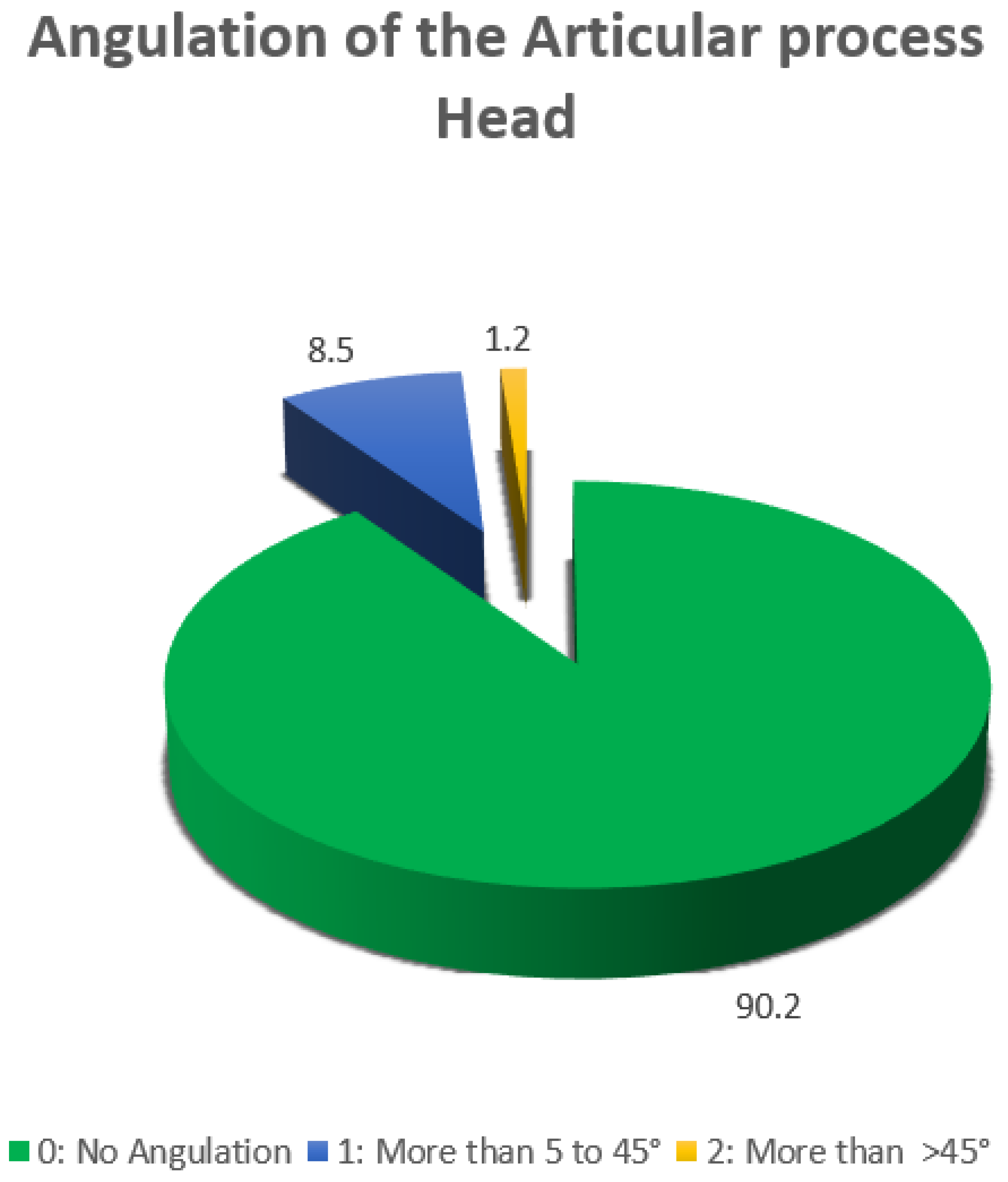
Figure 7.
illustrates a representative case showing a bifocal mandibular fracture with a dystotopic distortion and second-degree angulation of the caudal condylar head fragment, associated with overlapping fragments in a symphyseal/parasymphyseal fracture.
Figure 7.
illustrates a representative case showing a bifocal mandibular fracture with a dystotopic distortion and second-degree angulation of the caudal condylar head fragment, associated with overlapping fragments in a symphyseal/parasymphyseal fracture.
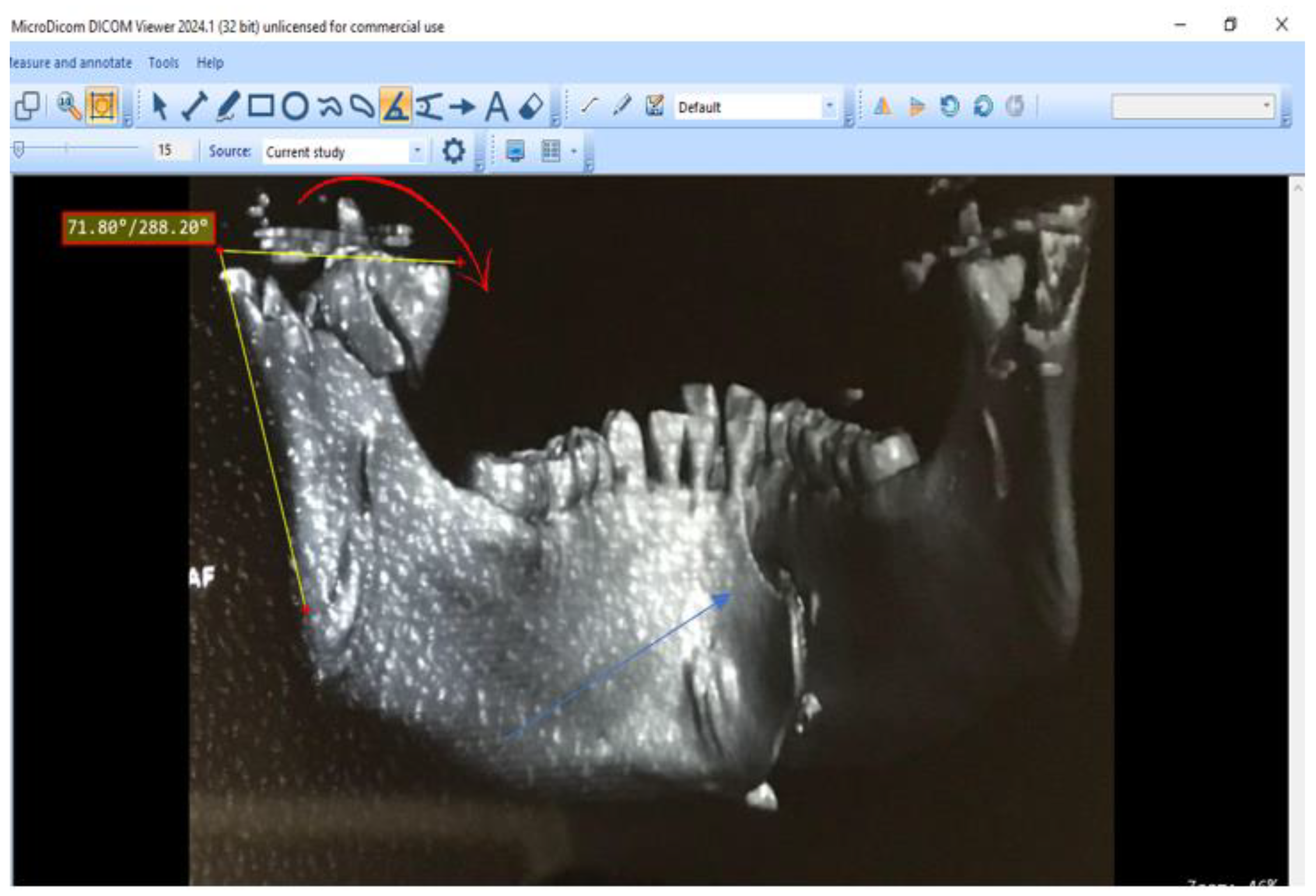

Table 1.
Age and Sex Distribution of the Study Population.
| Age range | Count (N = 82) | Frequency (%) |
|---|---|---|
| 18-28 | 41 | 50 1 |
| 29-38 | 33 | 40.24 |
| 39-48 | 6 | 7.32 |
| 49+ | 2 | 2.44 |
| Total | 82 | 100 |
1 Adeleke et al. 2023.
Table 2.
Etiology of Fractures.
| Etiology | Count (N=82) | Frequency (%) |
|---|---|---|
| RTA (Road Traffic Accidents) | 58 | 70.7 |
| Falls | 10 | 12.2 |
| Assault | 7 | 8.5 |
| Fights | 7 | 8.5 |
Table 3.
Sex-Specific Distribution of Fracture Etiology.
| Etiology | Female (N=9) | Male (N=73) |
|---|---|---|
| RTA (Road Traffic Accidents) | 4 (44.44%) | 54 (73.97%) |
| Falls | 2 (22.22%) | 8 (10.96%) |
| Assault | 0 (0%) | 7 (9.59%) |
| Fights | 3 (33.33%) | 4 (5.48%) |
Table 4.
Fracture Distribution Across AO CMF-Defined Mandibular Transition Areas N=82.
| Location | Simple fracture | Fragmentation fracture |
|---|---|---|
| Symphysis/Parasymphysis | 27 | 8 |
| 32.93% | 9.76% | |
| Body | 13 | 6 |
| 15.85% | 7.32% | |
| Articular process | 12 | 4 |
| 19.67% | 19% | |
| Angle/Ramus | 9 | 3 |
| 15.75% | 14.28% |
Table 5.
Distribution of Bone Loss Associated with Fractures.
| Bone Loss Severity | Count (N=82) | Frequency (%) |
|---|---|---|
| No bone loss, Mandibular vertical height > 20 mm |
80 | 97.6 |
| Minimal bone loss, Mandibular vertical height > 15 to 20 mm |
2 | 2.4 |
Table 6.
Distribution of Fractures According to the Anatomical Regions of the Articular Process.
| Region | Count (N=82) | Frequency (%) |
|---|---|---|
| Base | 2 | 2.4 |
| Neck | 9 | 11 |
| Head | 5 | 6.1 |
| Other locations | 66 | 80.5 |
Table 7.
Distribution of the Displacement Type of the Caudal Fragment of the Articular Process Head.
Table 7.
Distribution of the Displacement Type of the Caudal Fragment of the Articular Process Head.
| Displacement Type | Count (N=82) | Frequency (%) |
|---|---|---|
| Non-displaced | 56 | 68.3 |
| Partial | 15 | 18.3 |
| Complete | 9 | 11 |
| Dislocation | 2 | 2.4 |
Table 8.
AO CMF Classification Codes of Mandibular Fractures in the Study.
| AO CMF Code | Count (N=82) | Fracture Description |
|---|---|---|
| 91A | 3 | Simple and confined fracture of the Angle/Ramus region |
| 91A-CB | 1 | Bifocal simple and confined fracture of the Angle/Ramus region on the right and the base of the condylar process (CP) on the left |
| 91A1a | 1 | Grade 1 fragmentation fracture of the Angle/Ramus region with involvement of the alveolar process |
| 91A2 | 1 | Grade 2 fragmentation fracture of the Angle/Ramus region |
| 91A2-CB | 1 | Grade 2 fragmentation fracture of the Angle/Ramus region on the right and the base of the CP on the left |
| 91Aa | 4 | Simple and confined fracture of the Angle/Ramus region with involvement of the alveolar process |
| 91B | 3 | Simple and confined fracture of the mandibular body (Corpus) |
| 91B1a | 3 | Grade 1 fragmentation fracture of the mandibular body with involvement of the alveolar process |
| 91B-BA | 1 | Bilateral simple fracture confined to the right mandibular body and extending to the left Angle/Ramus region |
| 91B2-B | 1 | Grade 2 fragmentation fracture of the right mandibular body and simple contralateral body fracture |
| 91Ba | 6 | Simple and confined fracture of the mandibular body with involvement of the alveolar process |
| 91Ba-A | 2 | Simple fracture of the mandibular body with involvement of the alveolar process extending to the Angle/Ramus region |
| 91Ba-CN | 1 | Bifocal simple and confined fracture of the mandibular body with involvement of the alveolar process on the right and of the CP head on the left |
| 91Ba-S | 1 | Bifocal simple fracture of the mandibular body with involvement of the alveolar process extending to the Symphysis/Parasymphysis region |
| 91CB | 2 | Simple fracture of the CP base |
| 91CB1 | 1 | Grade 1 fragmentation fracture of the CP base |
| 91CH1p1 | 1 | Grade 1 fragmentation fracture of the CP head with anterior displacement of the caudal fragment and 1st-degree angulation |
| 91CHl | 1 | Grade 1 fragmentation fracture of the CP head |
| 91CHl1 | 1 | Simple fracture of the CP head with medial displacement of the caudal fragment and 1st-degree angulation |
| 91CHm1 | 1 | Simple fracture of the CP head with medial displacement of the caudal fragment and 1st-degree angulation |
| 91CHp | 1 | Simple fracture of the CP head with anterior displacement of the caudal fragment |
| 91CN | 3 | Simple fracture of the CP neck |
| 91CN2-Sa | 1 | Bifocal Grade 2 fragmentation fracture of the CP neck on the right and simple fracture of the Symphysis/Parasymphysis region with involvement of the alveolar process |
| 91CNa | 2 | Simple fracture of the CP neck with ipsilateral alveolar process involvement |
| 91CNm1 | 1 | Simple fracture of the CP neck with medial displacement of the caudal fragment and 1st-degree angulation |
| 91S | 4 | Simple fracture of the Symphysis/Parasymphysis region |
| 91S-CB | 1 | Bifocal simple and confined fracture of the Symphysis/Parasymphysis region on the right and the contralateral CP base |
| 91S-CHl1 | 1 | Bifocal simple fracture of the Symphysis/Parasymphysis region on the right and the CP head on the left with lateral displacement of the caudal fragment and 1st-degree angulation |
| 91S1-CHm | 1 | Bifocal Grade 1 fragmentation fracture of the Symphysis/Parasymphysis region and the CP head on the left with medial displacement of the caudal fragment |
| 91S1a | 3 | Grade 1 fragmentation fracture of the Symphysis/Parasymphysis region with ipsilateral alveolar process involvement |
| 91S1a-B | 2 | Grade 1 fragmentation fracture of the right Symphysis/Parasymphysis region with ipsilateral alveolar process involvement extending to the left body |
| 91S1a-Ba | 1 | Grade 1 fragmentation fracture of the right Symphysis/Parasymphysis region extending to the left body with bilateral alveolar process involvement |
| 91S1a-CN | 2 | Grade 1 fragmentation fracture of the right Symphysis/Parasymphysis region with ipsilateral alveolar process involvement and simple CP neck fracture |
| 91S2a-CHl1 | 1 | Grade 2 fragmentation fracture of the right Symphysis/Parasymphysis region with ipsilateral alveolar process involvement and simple CP head fracture with lateral displacement of the caudal fragment |
| 91Sa | 15 | Simple fracture of the right Symphysis/Parasymphysis region with ipsilateral alveolar process involvement |
| 91Sa-B | 1 | Simple fracture of the right Symphysis/Parasymphysis region with alveolar process involvement extending to the left body |
| 91Sa-Ba | 1 | Simple fracture of the right Symphysis/Parasymphysis region extending to the left body with bilateral alveolar process involvement |
| 91Sa-CHl1 | 1 | Bifocal simple fracture of the right Symphysis/Parasymphysis region with alveolar process involvement and left CP head fracture with lateral displacement and 1st-degree angulation |
| 91B1a-S | 1 | Grade 1 fragmentation fracture of the alveolar process in the body region on the right extending to the Symphysis/Parasymphysis |
| 91S1ad | 1 | Grade 1 fragmentation fracture of the alveolar process in the Symphysis/Parasymphysis region with bone loss |
| 91Sa | 1 | Simple fracture of the alveolar process in the Symphysis/Parasymphysis region |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



