
Submitted:
05 June 2025
Posted:
05 June 2025
You are already at the latest version
Abstract
(1) Background: Knee osteoarthritis (KOA) induces pain, stiffness, and impaired mobility, particularly in aging populations. Despite providing symptom relief, the long-term efficacy of intra-articular hyaluronic acid (HA) injections remains unclear. With its longer intra-articular residence time and potential chondroprotective effects, porcine-derived atelocollagen is an alternative to HA. We aimed to compare the safety and efficacy of collagen versus HA injections in symptomatic KOA. (2) Methods: This retrospective observational study included 40 patients with KOA who received either two cycles of collagen or HA injections at 6-month intervals. Clinical outcomes were assessed, using the Visual Analog Scale (VAS) and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), at baseline and at 6 months after the first and second injections (Cycle 1 and Cycle 2, respectively). Patient satisfaction and adverse events were recorded. Non-inferiority analysis was conducted for VAS and WOMAC score changes. (3) Results: Significant intragroup improvements in VAS and WOMAC scores were noted after each injection cycle (p<0.05), albeit without significant between-group differences, non-inferiority of collagen to HA based on predefined margins, and comparable patient-reported satisfaction (>85% reported improvement after each cycle), with similar incidence of mild adverse events (collagen: 20%, HA: 25%, p=0.705). (4) Conclusion: Intra-articular collagen injections were clinically non-inferior to HA in reducing pain and improving function in patients with KOA across two treatment cycles. Given its favorable safety profile and potential structural benefits, collagen may serve as a viable alternative injectable therapy for the non-surgical management of KOA.
Keywords:
knee osteoarthritis
; intra‐articular injection
; porcine atelocollagen
; hyaluronic acid
; non‐inferiority
1. Introduction
Osteoarthritis (OA) is a degenerative joint disease characterized by progressive degradation of articular cartilage, subchondral bone remodeling, and synovial inflammation [1,2,3,4,5]. The knee is particularly vulnerable to OA owing to its load-bearing function; knee osteoarthritis (KOA) is a significant cause of pain, functional disability, and reduced quality of life in aging populations [6,7]. KOA pathophysiology involves complex biochemical and mechanical interactions that induce cartilage loss, osteophyte formation, and joint-space narrowing, which causes pain, stiffness, and impaired mobility [8].
Treatment for KOA comprises conservative options, such as lifestyle modifications and pharmacotherapy, and invasive surgical interventions including osteotomy and arthroplasty [9]. Intra-articular injections are a minimally invasive alternative treatment for reducing pain, improving joint lubrication, and postponing surgery [9]. Hyaluronic acid (HA) injections are widely used owing to their viscoelastic properties, which enhance synovial fluid viscosity and provide a cushioning effect [10]. Repeated intra-articular HA injections are effective and safe for KOA management, and subsequent treatment cycles consistently maintain and can further enhance pain relief without increasing adverse events [11].
Recently, intra-articular collagen injections have emerged as a promising alternative [12,13,14]. Collagen, a key structural component of articular cartilage, has a longer intra-articular half-life than HA and may exert additional therapeutic effects beyond lubrication, including chondroprotection and structural reinforcement of the cartilage surface [15]. Specifically, type I atelocollagen derived from porcine sources potentially augments the lamina splendens, the superficial zone of cartilage, and thereby enhances joint protection and potentially modulates cartilage metabolism [15,16]. Despite these theoretical advantages, clinical evidence of direct comparisons of the efficacy and safety of collagen and HA injections, across multiple treatment cycles, are limited [14]. Studies on collagen injections for KOA have either been single-arm or short-term investigations that lacked control groups and long-term outcome measures. The clinical relevance of repeated administration—considered essential for chronic conditions, such as OA—remains underexplored [12,13,14].
In this study we aimed to compare the clinical efficacy and safety of collagen and HA after one and two injection cycles of these intra-articular therapies in a clinical context and explore whether collagen injection constitutes a viable alternative or adjunct to HA in routine orthopedic practice. Our results provide a rationale for informed decision making for the non-surgical management of KOA.
2. Materials and Methods
2.1. Study Design and Ethical Approval
This retrospective comparative cohort study adhered to the ethical principles of the Declaration of Helsinki and was approved by the relevant Institutional Review Board. All participants provided written informed consent prior to enrollment.
2.2. Participants and Eligibility Criteria
We enrolled patients (age ≥40 years) who received two cycles of intra-articular injections of either HA or collagen at 6-month intervals, between 2023 and 2024, and were ambulatory after a diagnosis of KOA made at least 3 months prior to screening. Participants had experienced inadequate pain relief from prior treatment with analgesics or non-steroidal anti-inflammatory drug. We screened electronic medical charts of adults and excluded patients with secondary OA or other inflammatory joint disease (e.g., rheumatoid arthritis, psoriatic arthritis, or ankylosing spondylitis); significant joint deformity, instability, or effusion in the affected knee; a history of knee replacement surgery (total or partial) in the index joint; prior intra-articular injections (e.g., corticosteroids or hyaluronic acid) within 3 months before screening; a history of major surgery, arthroscopic intervention in either knee within the past 6 months, uncontrolled comorbidities (including cardiovascular disease or diabetes), active infections, or a history of malignancy within the past 5 years; or current use of systemic corticosteroids, anticoagulants, or immunosuppressive medications.
Among 86 patients identified in the HA group, we excluded 4 patients with secondary OA, 5 with prior knee surgery, 4 with prior intra-articular injections within 3 months, 4 with systemic corticosteroid or anticoagulants, 12 with uncontrolled comorbidities, 8 with a history of malignancy, and 29 who declined to participate, resulting in a final sample included 20 patients. Among 32 patients identified in the collagen group, we excluded 1 patient with prior knee surgery, 3 with uncontrolled comorbidities, 2 with a history of malignancy, and 6 who declined participation, leaving 20 patients in the final analysis.
2.3. Interventions and Injection Protocol
Collagen injections consisted of either CartiZol Active (6% atelocollagen, 1 mL = 60 mg) or CartiZol Ultra (6% atelocollagen, 3 mL = 180 mg), both manufactured by Cellontech (Seoul, Korea). CartiZol Ultra was used once per 6-month cycle, whereas CartiZol Active could be administered up to three times within the same period at the surgeon’s discretion. HA injections employed Synovian, a 3-mL pre-filled syringe of 1,4-butanediol diglycidyl ether-cross-linked HA (LG Life Sciences, Korea) delivered once per cycle. All injections were administered intra-articularly into the knee joint using a standard anterolateral approach, without ultrasound guidance, by experienced orthopedic surgeon under aseptic conditions using a 22-gauge needle, with patients in a supine position. Patients were advised 24-h restriction of high-impact activity and ice application, in case of postprocedural discomfort; no prophylactic antibiotics were used.
2.4. Follow-Up Schedule and Outcome Measures
Data on demographic variables, such as age, sex, body mass index, and radiographic OA grade (based on the Kellgren–Lawrence classification), were collected at baseline [17]. Comorbidities, such as hypertension, diabetes mellitus, thyroid disease, and smoking status, as well as side of injection (right or left knee) and product details were recorded. Each knee was evaluated at baseline (pre-injection) and 6 months after the first and second injections (cycles 1 and 2), wherein a trained orthopedic surgeon documented pain scores using a 10-cm visual analogue scale (VAS), subdivided into pain at rest, pain during walking, and nocturnal pain [18]. Functional status was ascertained with the validated Korean version of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), with subscores for pain, stiffness, and physical function (total score 0–96, with higher scores indicating worse status) [19]. Patient satisfaction was quantified at each follow-up visit using a five-point Likert scale as follows: “marked worsening,” “slight worsening,” “no change,” “slightly improved,” or “very improved.” For statistical analysis, responses were categorized into three levels: no change/worsened, slightly improved, and very improved. Adverse events were monitored through chart review and patient interviews conducted during follow-up visits. Events of interest included post-injection flare pain, joint swelling, local inflammation, or systemic symptoms. All adverse events were reviewed by the clinical team, and their relationship to the injection was determined by the treating physician.
2.5. Statistical Analysis
Descriptive statistics are presented as mean ± standard deviation for continuous measures and as frequency (proportion) for categorical measures. Normality of continuous variables was assessed using the Shapiro–Wilk test. Between-group comparisons for normally distributed continuous variables were performed using independent t-tests, and the Wilcoxon rank-sum test was used when normality was not satisfied. Categorical variables were compared using the chi-square or Fisher’s exact test, depending on sample size and distribution. A two-sided p<0.05 was considered statistically significant for secondary and exploratory analyses. All statistical analyses were performed using SAS (version 9.4; SAS Institute Inc., Cary, NC, USA).
Non-inferiority analysis was conducted using the mean change from baseline in VAS and WOMAC scores. The between-group difference (HA minus collagen) and its 95% confidence interval (CI) were calculated using PROC TTEST in SAS. Non-inferiority (one-sided) was concluded if the lower bound of the 95% CI was above the negative value of the predefined margin. Sample size was determined based on a non-inferiority design to compare the efficacy of intra-articular collagen injections with that of HA in alleviating KOA pain. The null hypothesis assumed the superiority of HA over collagen. The non-inferiority margin was predefined as 1.99 on the VAS, based on prior clinical relevance [20]. The sample size calculation was based on the following parameters: an assumed standard deviation (SD) of 2.34, power (1–β) of 80%, and two-sided significance level (α) of 0.05[21]. Accordingly, the required sample size was estimated at 18 patients per group to adequately demonstrate non-inferiority, defined as the upper bound of the 95% CI for the mean difference remaining below the non-inferiority margin. To enhance the robustness of the findings and to utilize the full extent of the available dataset, the final sample size was set at 20 patients per group. For WOMAC scores, non-inferiority margins were established using previously validated thresholds for minimal clinically important difference (MCID) and substantial clinical benefit (SCB), ensuring that any observed differences would be clinically relevant rather than statistically insignificant. Specifically, the margins applied, for the MCID and SCB, were as follows: for total WOMAC, 16.1 and 25.3; for the WOMAC pain subscale, 4.2 and 6.4; for stiffness, 1.9 and 2.6; and for function, 10.1 and 16.4, respectively [22].
3. Results
3.1. Baseline Characteristics
Baseline clinicodemographic characteristics were well balanced between the two groups. The mean age was 67.3 ± 10.3 and 69.0 ± 9.0 years in the collagen and HA groups, respectively (p=0.737) (Table 1).
3.2. Primary Outcome: Non-Inferiority of VAS and WOMAC Score Changes
The primary outcome involved changes in VAS and WOMAC scores from baseline using non-inferiority testing. Across all VAS domains—resting, walking, and night pain—the collagen group demonstrated non-inferiority to the HA group at both the first and second injection timepoints. All comparisons yielded statistically significant results (p<0.05), and the lower bounds of the 95% CIs were above the predefined non-inferiority margin, and confirmed clinical non-inferiority (Table 2).
Changes in WOMAC total, pain, stiffness, and function scores showed significant improvement in the collagen group, and all 95% CIs remained well within the established non-inferiority margins. These results were consistent across all domains (all p<0.0001) (Table 3).
3.3. Secondary Outcome: VAS and WOMAC Scores
At 6 months after the first and second injections, VAS scores for resting, walking, and night pain significantly improved from the baseline in each treatment group (all p<0.05). There was no significant between-group differences in VAS scores of the HA and collagen groups at any corresponding timepoint (p>0.05) (Figure 1). Similarly, all WOMAC subscores—including pain, stiffness, and physical function—demonstrated significant within-group improvement from baseline at both post-injection assessments (6 months after the first and second injection cycles). Intergroup comparisons revealed no significant differences in WOMAC subscores at any follow-up timepoint (p>0.05 for all) (Figure 2).
3.4. Patient Satisfaction
Patient-reported satisfaction was evaluated at 6 months following both the first and second injections. After the first injection, all patients reported some degree of improvement. In the collagen group, 45% and 55% of patients reported slight and significant improvement, respectively; in the HA group, 50% each reported slight and significant improvement, albeit without significant between-group distributions (p=0.752). At 6 months after the second injection, 85–90% of patients in both groups reported sustained improvement, with comparable satisfaction levels and no significant differences (p=0.889) (Table 4).
3.5. Adverse Events
Adverse events were infrequent and mild in both groups. In the collagen group, four patients (20%) experienced transient symptoms, such as injection-site pain flare or swelling. In the HA group, five patients (25%) reported similar reactions. All adverse effects resolved with conservative management; no serious complications were recorded. No significant between-group difference in adverse event rates was noted (p=0.705).
4. Discussion
This study involved a novel systematic evaluation of the efficacy and safety of repeated collagen injections over a 1-year follow-up period and compared its performance with that of HA. We showed that intra-articular porcine-derived atelocollagen injection generated clinical outcomes that were non-inferior to those of HA over two treatment cycles in symptomatic KOA. Both treatment groups demonstrated significant improvements in pain and joint function (on VAS and WOMAC scores) without significant between-group differences in therapeutic effect. Importantly, the adverse event rate was comparable for the collagen and HA groups, which suggests that collagen, administered in two 6-monthly cycles, is a clinically safe, effective alternative to HA.
HA was selected as the comparator based on clinical relevance and methodological rigor [11] as it is the most extensively used and studied non-operative interventions for KOA and is frequently recommended as a first-line intra-articular therapy in international guidelines [23]. Despite ongoing debate regarding its long-term efficacy, HA remains the benchmark against which novel intra-articular agents are evaluated [11]. We employed a non-inferiority, rather than superiority, framework in our statistical analysis to determine whether collagen could achieve comparable outcomes to HA within an acceptable clinical margin, which reflects our pragmatic clinical question: given that HA is considered safe and modestly effective, a new treatment with similar benefits and an acceptable safety profile—while possibly conferring additional advantages including improved structural integration or prolonged joint surface protection—could be clinically valuable [24].
Across both treatment arms, VAS scores for rest, walking, and nocturnal pain declined significantly from baseline to the end of the second cycle, reflecting a robust reduction in subjective pain burden. All WOMAC subdomains—pain, stiffness, and physical function—improved over time in both groups, and total WOMAC scores nearly halved at follow-up completion. Thus, both collagen and HA effectively address multiple dimensions of symptomatic KOA, including nociceptive pain and joint mobility and function [11,14]. Our findings are consistent with previous reports of beneficial effects of both HA and collagen in KOA [11,14]. Multiple randomized controlled trials and meta-analyses have shown that HA provides modest pain relief and functional improvement, despite variable magnitude and effect duration [11]. Collagen-based intra-articular injections, although less studied, have gained attention in recent years [14]. In a multicenter retrospective study, Volpi et al. [25] confirmed the safety and tolerability of three intra-articular injections of low-molecular-weight (<3 kDa) bovine-derived hydrolyzed collagen. Their findings, based on a large patient cohort, provided stronger evidence than the earlier study by De Luca et al. [40], without significant adverse effects [26]. In a double-blind, randomized, active-controlled trial by Martin et al. [27] intra-articular type I hydrolyzed porcine collagen was compared to HA in patients with KOA. At both 3- and 6-month follow-ups, collagen injections demonstrated comparable efficacy and safety to HA, suggesting that collagen may serve as a viable alternative treatment for KOA [27]. A multicenter, randomized, double-blind study by Lee et al. [28] to evaluate intra-articular type I atelocollagen in KOA and other cartilage defects showed no significant difference in VAS scores between the collagen and placebo groups at 4 and 12 weeks, but found a significant improvement in the collagen group at 24 weeks. This is one of the first studies to directly compare two full cycles of collagen and HA injections in a real-world setting to generate novel data regarding long-term use and repeat-dose tolerability.
More than 90% of our participants in both groups reported either “slight improvement” or “marked improvement” following each injection cycle. Although a small number of patients reported no change after the second injection, none indicated worsening of symptoms, and satisfaction ratings remained stable across cycles. The similarity in satisfaction trends between groups underscores that collagen therapy was perceived as at least as beneficial as HA by the patients themselves, which further supports its clinical acceptability. Lee et al. [28] demonstrated higher patient and physician satisfaction rates in the collagen group, suggesting that intra-articular atelocollagen may effectively alleviate KOA pain and related cartilage disorders. HA products have a long-established safety profile and are routinely administered at multiple intervals without serious cumulative toxicity [11]. To address concerns regarding repeat-dose safety, we specifically designed our study to include two consecutive cycles of treatment and compared collagen against HA in this context. Our findings revealed no significant intergroup difference in the frequency or severity of adverse events, with only minor, self-limiting complaints such as transient joint discomfort and swelling. These results support the tolerability of collagen over a repeated dosing schedule and position it as a feasible long-term injectable strategy for KOA [14].
The mechanisms underlying the observed clinical improvements differ between HA and collagen, which may have implications for personalized treatment selection. HA acts primarily by restoring the viscoelastic properties of synovial fluid, thereby improving joint lubrication and absorbing mechanical shocks during movement [29,30]. HA exhibits anti-inflammatory and analgesic properties through modulation of nociceptive signaling, reduction of cytokine activity (e.g., interleukin-1β, tumor necrosis factor-α), and inhibition of metalloproteinase-mediated cartilage degradation [29,30]. However, intra-articular half-life of HA is relatively short, and repeated administrations are frequently needed to maintain its clinical effects [11]. Collagen, a key structural protein comprising up to 75% of the dry weight of connective tissues like cartilage, plays a crucial role in supporting tissue architecture and cellular function [15]. In vitro studies showed that collagen preparations can enhance chondrocyte proliferation, stimulate extracellular matrix and HA production, and suppress inflammatory mediators [31,32]. Animal studies, including those using purified porcine atelocollagen and collagen tripeptides, demonstrated reduced inflammation, promotion of tissue repair, and delayed cartilage degeneration, suggesting a potential therapeutic role of collagen in cartilage regeneration and OA management [15,33]. Although HA primarily addresses the mechanical symptoms of OA, collagen may exert a dual function—providing symptomatic relief and potentially mitigating cartilage degradation. This hypothesis aligns with our observation that collagen-treated patients exhibited sustained improvements after two injection cycles with a low incidence of side effects.
Despite its strengths, including rigorous outcome assessment, standardized dosing intervals, and direct comparison with a gold-standard therapy, our study has some limitations. First, the majority of patients enrolled were women, which may limit the generalizability of the findings to male populations. However, this reflects the epidemiological characteristics of KOA in Asian populations, where the disease shows a markedly higher prevalence among women [34-38]. Second, the retrospective observational study design incurs an inherent risk of selection bias and residual confounding. Despite comparable between-group baseline characteristics, unmeasured factors such as activity level, adherence to rehabilitation, or prior injection response could have influenced outcomes. Third, the sample size was relatively small (n=40), limiting the statistical power to detect subtle between-group differences. Larger studies are needed to validate our findings and explore subgroup effects based on disease severity, comorbidities, or imaging characteristics. Fourth, while we assessed efficacy over two injection cycles (approximately 12 months), the long-term durability of these benefits beyond 1 year remains unknown. Structural outcomes such as radiographic progression, cartilage volume, or biomarkers of cartilage turnover were not evaluated. Fifth, the study was not blinded, which may have introduced expectation bias, particularly in the subjective satisfaction assessments. However, this reflects real-world conditions, where blinding is frequently unfeasible. Lastly, while we employed validated tools such as VAS and WOMAC [18,19], we did not include imaging or biochemical markers to assess potential disease-modifying effects of collagen, which could be an important direction for future research.
5. Conclusions
This study provides preliminary evidence that intra-articular collagen injection is a safe, effective treatment for KOA that ensured pain relief and functional gains comparable to those of HA over a two-cycle regimen. Collagen represents a viable alternative injectable therapy for non-surgical intervention in KOA, especially for those with refractory KOA or intolerance of HA.
Author Contributions
Dr Kim had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: Kim.; Acquisition, analysis, or interpretation of data: In,Choi; Drafting of the manuscript: Kim, In; Critical revision of the manuscript for important intellectual content: All authors; Administrative, technical, or material support: Choi; Supervision: Kim.
Funding
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (RS-2023-00215891) and Research Fund of Seoul St. Mary’s Hospital , The Catholic University of Korea. (ZC25CISI0102)
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Seoul St. Mary’s Hospital (KC24QISI0639).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data published in this research are available on request from the corresponding author (MSK).
Conflicts of Interest
The authors declare no conflict of interest.
List of Abbreviations
CI confidence interval
KOA knee osteoarthritis
MCID minimal clinically important difference
OA osteoarthritis
SCB substantial clinical benefit
SD standard deviation
VAS visual analogue scale
WOMAC the Western Ontario and McMaster Universities Osteoarthritis Index
References
- Choi, B.S.; Ro, D.H.; Lee, M.C.; Han, H.S. Isolated Polyethylene Insert Exchange for Instability after Total Knee Arthroplasty: Comparable Survival Rates and Range of Motion and Improved Clinical Scores Regardless of Hyperextension. Clin Orthop Surg 2024, 16, 550-558. [CrossRef]
- Hsu, C.E.; Tsai, M.H.; Wu, H.T.; Huang, J.T.; Huang, K.C. Phenotype-considered kinematically aligned total knee arthroplasty for windswept-deformity-associated osteoarthritis: surgical strategy and clinical outcomes. Knee Surg Relat Res 2024, 36, 16. [CrossRef]
- Kim, C.H.; Park, Y.B.; Baek, S.H. Clinical and Radiological Outcomes of Computer-Assisted Navigation in Primary Total Knee Arthroplasty for Patients with Extra-articular Deformity: Systematic Review and Meta-Analysis. Clin Orthop Surg 2024, 16, 430-440. [CrossRef]
- Kim, J.I.; Kim, J.K.; Kang, M.W.; Han, H.S. Do the Clinical and Radiological Features of Knees with Mucoid Degeneration of the Anterior Cruciate Ligament Differ According to Knee Osteoarthritis Status? Clin Orthop Surg 2024, 16, 405-412. [CrossRef]
- Kim, S.E.; Choi, B.S.; Ro, D.H.; Lee, M.C.; Han, H.S. Fixed-Bearing and Higher Postoperative Knee Flexion Angle as Predictors of Satisfaction in Asian Patients Undergoing Posterior-Stabilized Total Knee Arthroplasty. Clin Orthop Surg 2024, 16, 733-740. [CrossRef]
- Glyn-Jones, S.; Palmer, A.J.; Agricola, R.; Price, A.J.; Vincent, T.L.; Weinans, H.; Carr, A.J. Osteoarthritis. Lancet 2015, 386, 376-387. [CrossRef]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745-1759. [CrossRef]
- Loeser, R.F.; Goldring, S.R.; Scanzello, C.R.; Goldring, M.B. Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum 2012, 64, 1697-1707. [CrossRef]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage 2019, 27, 1578-1589. [CrossRef]
- Katz, J.N.; Arant, K.R.; Loeser, R.F. Diagnosis and Treatment of Hip and Knee Osteoarthritis: A Review. Jama 2021, 325, 568-578. [CrossRef]
- Altman, R.; Hackel, J.; Niazi, F.; Shaw, P.; Nicholls, M. Efficacy and safety of repeated courses of hyaluronic acid injections for knee osteoarthritis: A systematic review. Semin Arthritis Rheum 2018, 48, 168-175. [CrossRef]
- Czarnocki, Ł.; Dębiński, M.; Sasinowski, T.; Runo, E.; Deszczyński, J. Collagen injections as an alternative therapy for musculoskeletal disorders. Chir Narzadow Ruchu Ortop Pol 2017, 82, 221-224.
- Milani, L. A new and refined injectable treatment for musculoskeletal disorders. Bioscaffold properties of collagen and its clinical use. Physiological Regulating Medicine 2010, 1, 3-15.
- Tarantino, D.; Mottola, R.; Palermi, S.; Sirico, F.; Corrado, B.; Gnasso, R. Intra-Articular Collagen Injections for Osteoarthritis: A Narrative Review. Int J Environ Res Public Health 2023, 20. [CrossRef]
- Suh, D.S.; Yoo, J.C.; Woo, S.H.; Kwak, A.S. Intra-Articular Atelocollagen Injection for the Treatment of Articular Cartilage Defects in Rabbit Model. Tissue Eng Regen Med 2021, 18, 663-670. [CrossRef]
- Borja-Flores, A.; Macías-Hernández, S.I.; Hernández-Molina, G.; Perez-Ortiz, A.; Reyes-Martínez, E.; Belzazar-Castillo de la Torre, J.; Ávila-Jiménez, L.; Vázquez-Bello, M.C.; León-Mazón, M.A.; Furuzawa-Carballeda, J.; et al. Long-Term Effectiveness of Polymerized-Type I Collagen Intra-Articular Injections in Patients with Symptomatic Knee Osteoarthritis: Clinical and Radiographic Evaluation in a Cohort Study. Adv Orthop 2020, 2020, 9398274. [CrossRef]
- Misir, A.; Yildiz, K.I.; Kizkapan, T.B.; Incesoy, M.A. Kellgren-Lawrence grade of osteoarthritis is associated with change in certain morphological parameters. Knee 2020, 27, 633-641. [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res (Hoboken) 2011, 63 Suppl 11, S240-252. [CrossRef]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol 1988, 15, 1833-1840.
- Tubach, F.; Ravaud, P.; Baron, G.; Falissard, B.; Logeart, I.; Bellamy, N.; Bombardier, C.; Felson, D.; Hochberg, M.; van der Heijde, D.; Dougados, M. Evaluation of clinically relevant changes in patient reported outcomes in knee and hip osteoarthritis: the minimal clinically important improvement. Ann Rheum Dis 2005, 64, 29-33. [CrossRef]
- Waddell, D.D.; Cefalu, C.A.; Bricker, D.C. A second course of hylan G-F 20 for the treatment of osteoarthritic knee pain: 12-month patient follow-up. J Knee Surg 2005, 18, 7-15. [CrossRef]
- Kim, M.S.; Koh, I.J.; Choi, K.Y.; Sung, Y.G.; Park, D.C.; Lee, H.J.; In, Y. The Minimal Clinically Important Difference (MCID) for the WOMAC and Factors Related to Achievement of the MCID After Medial Opening Wedge High Tibial Osteotomy for Knee Osteoarthritis. Am J Sports Med 2021, 49, 2406-2415. [CrossRef]
- Phillips, M.; Bhandari, M.; Grant, J.; Bedi, A.; Trojian, T.; Johnson, A.; Schemitsch, E. A Systematic Review of Current Clinical Practice Guidelines on Intra-articular Hyaluronic Acid, Corticosteroid, and Platelet-Rich Plasma Injection for Knee Osteoarthritis: An International Perspective. Orthop J Sports Med 2021, 9, 23259671211030272. [CrossRef]
- Tweed, C.D.; Quartagno, M.; Clements, M.N.; Turner, R.M.; Nunn, A.J.; Dunn, D.T.; White, I.R.; Copas, A.J. Exploring different objectives in non-inferiority trials. Bmj 2024, 385, e078000. [CrossRef]
- Volpi, P.; Zini, R.; Erschbaumer, F.; Beggio, M.; Busilacchi, A.; Carimati, G. Effectiveness of a novel hydrolyzed collagen formulation in treating patients with symptomatic knee osteoarthritis: a multicentric retrospective clinical study. Int Orthop 2021, 45, 375-380. [CrossRef]
- De Luca, P.; Colombini, A.; Carimati, G.; Beggio, M.; de Girolamo, L.; Volpi, P. Intra-Articular Injection of Hydrolyzed Collagen to Treat Symptoms of Knee Osteoarthritis. A Functional In Vitro Investigation and a Pilot Retrospective Clinical Study. J Clin Med 2019, 8. [CrossRef]
- Martin Martin, L.S.; Massafra, U.; Bizzi, E.; Migliore, A. A double blind randomized active-controlled clinical trial on the intra-articular use of Md-Knee versus sodium hyaluronate in patients with knee osteoarthritis ("Joint"). BMC Musculoskelet Disord 2016, 17, 94. [CrossRef]
- Lee, H.S.; Oh, K.J.; Moon, Y.W.; In, Y.; Lee, H.J.; Kwon, S.Y. Intra-articular Injection of Type I Atelocollagen to Alleviate Knee Pain: A Double-Blind, Randomized Controlled Trial. Cartilage 2021, 13, 342s-350s. [CrossRef]
- Altman, R.D.; Bedi, A.; Karlsson, J.; Sancheti, P.; Schemitsch, E. Product Differences in Intra-articular Hyaluronic Acids for Osteoarthritis of the Knee. Am J Sports Med 2016, 44, 2158-2165. [CrossRef]
- Migliore, A.; Procopio, S. Effectiveness and utility of hyaluronic acid in osteoarthritis. Clin Cases Miner Bone Metab 2015, 12, 31-33. [CrossRef]
- Furuzawa-Carballeda, J.; Muñoz-Chablé, O.A.; Macías-Hernández, S.I.; Agualimpia-Janning, A. Effect of polymerized-type I collagen in knee osteoarthritis. II. In vivo study. Eur J Clin Invest 2009, 39, 598-606. [CrossRef]
- Ohara, H.; Iida, H.; Ito, K.; Takeuchi, Y.; Nomura, Y. Effects of Pro-Hyp, a collagen hydrolysate-derived peptide, on hyaluronic acid synthesis using in vitro cultured synovium cells and oral ingestion of collagen hydrolysates in a guinea pig model of osteoarthritis. Biosci Biotechnol Biochem 2010, 74, 2096-2099. [CrossRef]
- Naraoka, T.; Ishibashi, Y.; Tsuda, E.; Yamamoto, Y.; Kusumi, T.; Toh, S. Periodic knee injections of collagen tripeptide delay cartilage degeneration in rabbit experimental osteoarthritis. Arthritis Res Ther 2013, 15, R32. [CrossRef]
- Lee, D.W.; Song, D.S.; Han, H.S.; Ro, D.H. Accurate, automated classification of radiographic knee osteoarthritis severity using a novel method of deep learning: Plug-in modules. Knee Surg Relat Res 2024, 36, 24. [CrossRef]
- Migliorini, F.; Maffulli, N.; Schäfer, L.; Simeone, F.; Bell, A.; Hofmann, U.K. Minimal clinically important difference (MCID), substantial clinical benefit (SCB), and patient-acceptable symptom state (PASS) in patients who have undergone total knee arthroplasty: a systematic review. Knee Surg Relat Res 2024, 36, 3. [CrossRef]
- Park, J.; Chaar, O.; Narayanakurup, J.; Abdelhamead, A.S.A.; Ro, D.H.; Kim, S.E. Do knee alignment patterns differ between Middle Eastern and East Asian populations? A propensity-matched analysis using artificial intelligence. Knee Surg Relat Res 2025, 37, 11. [CrossRef]
- Yang, H.Y.; Yoon, T.W.; Kim, J.Y.; Seon, J.K. Radiologic Assessment of Knee Phenotypes Based on the Coronal Plane Alignment of the Knee Classification in a Korean Population. Clin Orthop Surg 2024, 16, 422-429. [CrossRef]
- Yoon, J.Y.; Moon, S.W. Impacts of asymmetric hip rotation angle on gait biomechanics in patients with knee osteoarthritis. Knee Surg Relat Res 2024, 36, 23. [CrossRef]
Figure 1.
Changes in the visual analogue scale (VAS) scores for resting pain (A), walking pain (B), and night pain (C) at baseline, 6 months after the first injection, and 6 months after the second injection in the hyaluronic acid (HA) and collagen groups.
Figure 1.
Changes in the visual analogue scale (VAS) scores for resting pain (A), walking pain (B), and night pain (C) at baseline, 6 months after the first injection, and 6 months after the second injection in the hyaluronic acid (HA) and collagen groups.
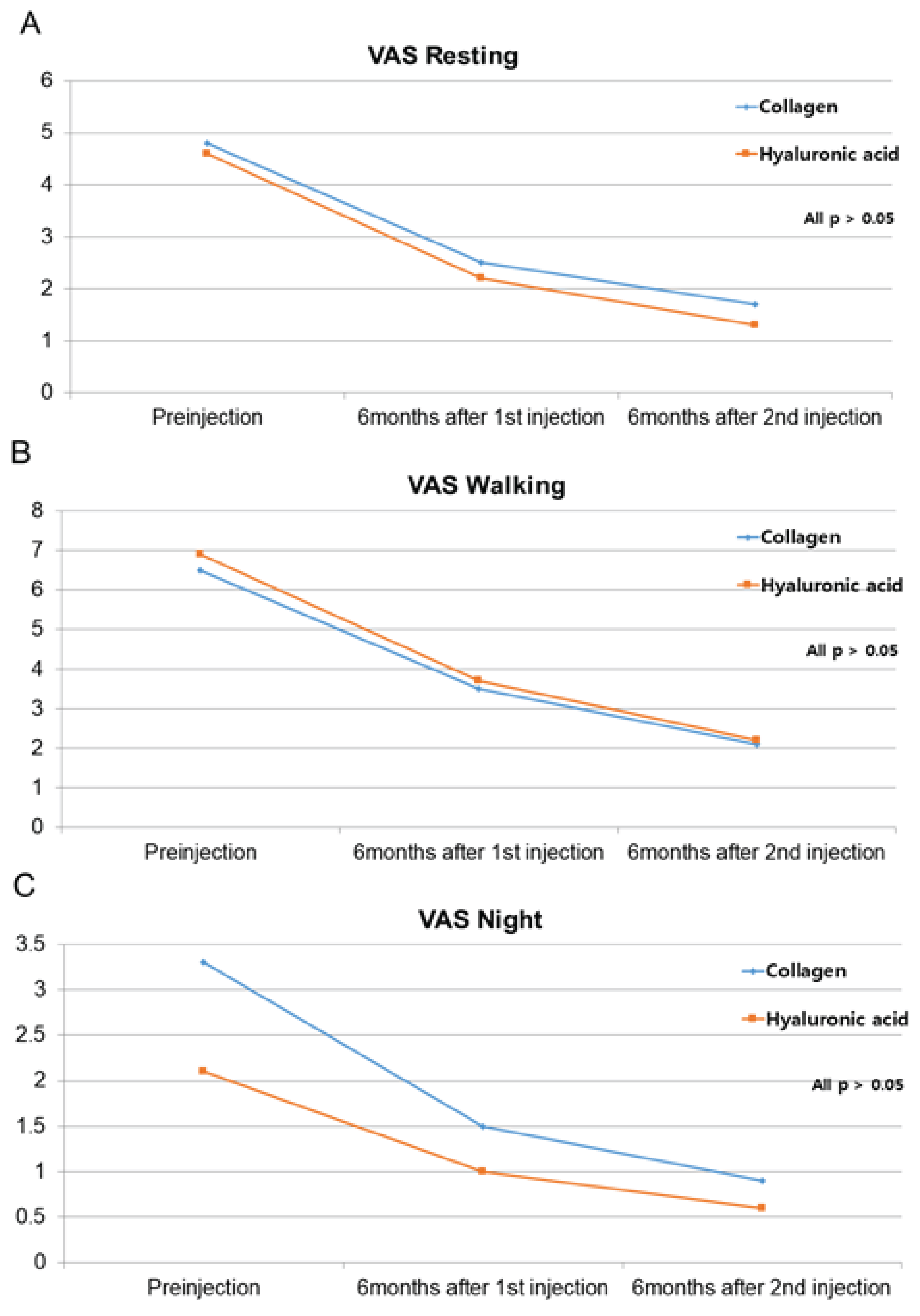
Figure 2.
Changes in the WOMAC subscores (pain, stiffness, and physical function) at baseline, 6 months after the first injection, and 6 months after the second injection in the HA and collagen group.
Figure 2.
Changes in the WOMAC subscores (pain, stiffness, and physical function) at baseline, 6 months after the first injection, and 6 months after the second injection in the HA and collagen group.
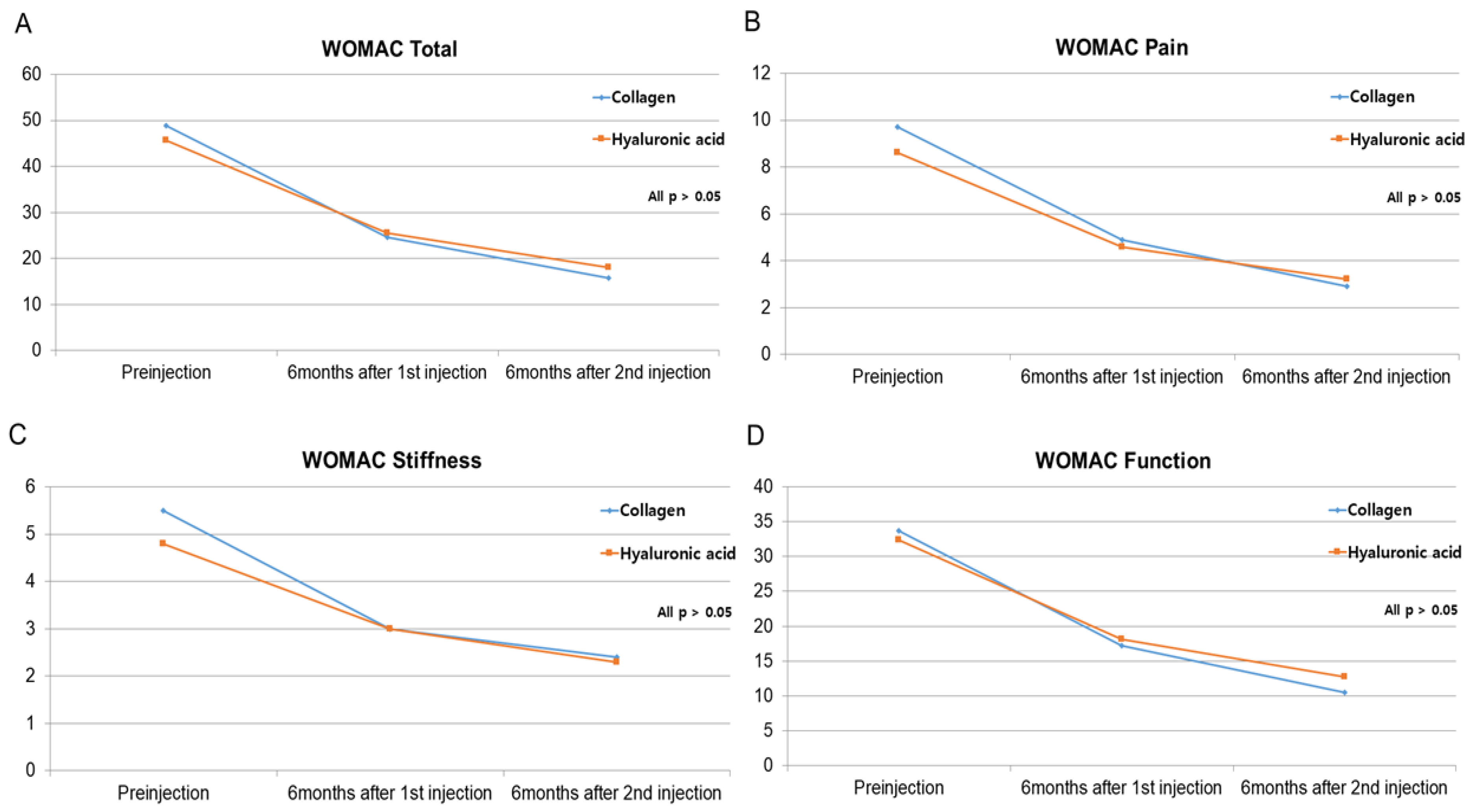

Table 1.
Baseline clinicodemographic characteristics of the study participants.
| Collagen | Hyaluronic acid | p-value | |
|---|---|---|---|
| Age, years | 67.3±10.3 | 69.0±9.0 | 0.737 |
| Sex, female/male, n | 15/5 | 16/4 | 1 |
| BMI | 23.5±3.8 | 24.8±3.2 | 0.257 |
| Kellgren–Lawrence OA grade | 2.8±1.0 | 2.35±0.99 | 0.151 |
| II | 7(35%) | 10(50%) | 0.337 |
| III | 13(65%) | 10(50%) | |
| Injection site (Rt, %) | 14(70%) | 18(90%) | 0.235 |
| Underlying disease | |||
| Hypertension | 11(55%) | 10(50%) | 0.751 |
| Diabetes | 4(20%) | 5(25%) | 1 |
| Thyroid disease | 4(20%) | 0(0%) | 0.106 |
| Smoking (n, %) | 6(30%) | 6(30%) | 1 |
| Pre-injection | |||
| VAS resting | 4.8±2.5 | 4.6±3.0 | 0.776 |
| VAS walking | 6.5±2.1 | 6.9±2.0 | 0.538 |
| VAS night | 3.3±3.3 | 2.1±2.5 | 0.299 |
| Total WOMAC | 48.9±14.9 | 45.7±20.6 | 0.583 |
| Pain WOMAC | 9.7±4.0 | 8.6±4.4 | 0.438 |
| Stiffness WOMAC | 5.5±2.1 | 4.8±2.2 | 0.281 |
| Function WOMAC | 33.7±10.3 | 32.4±15.3 | 0.745 |
Numerical variables are presented as the mean ± SD, and categorical variables as the frequency (proportion). BMI, body mass index; OA, osteoarthritis; VAS, visual analogue scale; WOMAC, the Western Ontario and McMaster Universities Osteoarthritis Index.
Table 2.
Evaluation of non-inferiority using the visual analogue scale scores in the collagen and hyaluronic acid groups.
Table 2.
Evaluation of non-inferiority using the visual analogue scale scores in the collagen and hyaluronic acid groups.
| Collagen | Hyaluronic acid | Non-inferiority test (margin: VAS = 1.99) | ||
|---|---|---|---|---|
| p-value | 95% CI | |||
| Pre-injection - 1st injection | ||||
| VAS resting | 2.3±2.0 | 2.4±2.2 | 0.004 | (-1.218, ∞) |
| VAS walking | 3.0±2.5 | 3.2±2.1 | 0.010 | (-1.433, ∞) |
| VAS night | 1.8±2.3 | 1.1±1.4 | <0.0001 | (-0.312, ∞) |
| Pre-injection - 2nd injection | ||||
| VAS resting | 3.1±2.1 | 3.3±2.6 | 0.011 | (-1.459, ∞) |
| VAS walking | 4.4±2.4 | 4.7±2.5 | 0.019 | (-1.635, ∞) |
| VAS night | 2.4±2.6 | 1.6±2.0 | 0.0003 | (-0.440, ∞) |
Numerical variables are presented as mean ± SD. VAS, visual analogue scale; WOMAC, the Western Ontario and McMaster Universities Osteoarthritis Index.
Table 3.
Evaluation of non-inferiority using the WOMAC scores of the collagen and hyaluronic acid groups.
Table 3.
Evaluation of non-inferiority using the WOMAC scores of the collagen and hyaluronic acid groups.
| Collagen | Hyaluronic acid | Non-inferiority test (margin: WOMAC = MCID) | Non-inferiority test (margin : WOMAC = SCB) | |||
|---|---|---|---|---|---|---|
| p-value | 95% CI | p-value | 95% CI | |||
| Pre-injection - 1st injection | ||||||
| Total WOMAC | 24.3±11.0 | 20.1±10.4 | <0.0001 | (-1.502, ∞) | <0.0001 | (-1.502, ∞) |
| Pain WOMAC | 4.8±2.6 | 4.0±2.6 | <0.0001 | (-0.634, ∞) | <0.0001 | (-0.634, ∞) |
| Stiffness WOMAC | 2.5±1.7 | 1.8±1.3 | <0.0001 | (-0.043, ∞) | <0.0001 | (-0.043, ∞) |
| Function WOMAC | 16.5±7.8 | 14.2±7.3 | <0.0001 | (--1.724, ∞) | <0.0001 | (--1.724, ∞) |
| Pre-injection - 2nd injection | ||||||
| Total WOMAC | 33.2±12.8 | 27.6±14.9 | <0.0001 | (-1.858, ∞) | <0.0001 | (-1.858, ∞) |
| Pain WOMAC | 6.8±3.1 | 5.4±3.4 | <0.0001 | (-0.384, ∞) | <0.0001 | (-0.384, ∞) |
| Stiffness WOMAC | 3.1±1.9 | 2.5±1.9 | <0.0001 | (-0.372, ∞) | <0.0001 | (-0.372, ∞) |
| Function WOMAC | 23.2±8.9 | 19.7±10.5 | <0.0001 | (-1.651, ∞) | <0.0001 | (-1.651, ∞) |
Numerical variables are presented as mean ± SD. VAS, visual analogue scale; WOMAC, the Western Ontario and McMaster Universities Osteoarthritis Index.
Table 4.
Patient satisfaction levels stratified by group and timepoint.
| Collagen | Hyaluronic acid | p-value | |
|---|---|---|---|
| Six months after the 1st injection | 0.752 | ||
| No change (n, %) | 0(0%) | 0(0%) | |
| Slightly improved (n, %) | 9(45%) | 10(50%) | |
| Very improved (n, %) | 11(55%) | 10(50%) | |
| Six months after the 2nd injection | 0.889 | ||
| No change (n, %) | 2(10%) | 3(15%) | |
| Slightly improved (n, %) | 15(75%) | 14(70%) | |
| Very improved (n, %) | 3(15%) | 3(15%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



