Submitted:
03 June 2025
Posted:
04 June 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Introduction: Long COVID syndrome is defined as persistent or new symptoms that appear after an acute SARS-CoV-2 infection and last at least three months without explanation. It is estimated that between 10% and 20% of those infected develop long COVID; however, data is not precise in Latin America. Although high immunization rates have reduced acute symptoms and the pandemic’s impact, there is a lack of evidence of its efficacy in preventing long COVID in the region.
Methods: This scoping review followed PRISMA-ScR guidelines. Studies on vaccinated adults with long COVID from Central and South America and the Caribbean were included (Mexico was also considered). A comprehensive search across multiple databases was conducted. Data included study design, participant characteristics, vaccine type, and efficacy outcomes. Results were presented narratively and in tables.
Results: Out of 3,466 initial records, eight studies met the inclusion criteria after rigorous selection processes. These studies encompassed populations from Brazil, Mexico, Latin America, and Bonaire, with 11,333 participants, 69.3% of whom were female. Vaccination, particularly with three or more doses, substantially reduces the risk and duration of long COVID. Variability was noted in the definitions and outcomes assessed across studies.
Conclusions: This scoping review highlights that SARS-CoV-2 vaccination exhibits potential in reducing the burden of long COVID in the Americas. However, discrepancies in vaccine efficacy were observed depending on the study design, the population studied, and the vaccine regimen employed. Further robust, region-specific investigations are warranted to delineate the effects of vaccination on long COVID outcomes.
Keywords:
post-acute COVID-19 syndrome
; vaccines
; efficacy
; Latin America
1. Introduction
As the COVID-19 pandemic continued its course, it became increasingly clear that a significant percentage of those with the disease were experiencing unexplained symptoms after the resolution of the acute illness[1]. A greater consensus was established about these manifestations, and these symptoms were grouped into a syndrome called long COVID. Definitions of long COVID may still vary and continue to be updated[1].
Most experts agree it is a syndrome characterized by signs, symptoms, and conditions that continue or develop after acute COVID-19 infection[1]. According to the current and most widely adopted definition, these symptoms must be present for at least three months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems.[2]
Studies have shown that around 40% of people infected with SARS-CoV-2 can develop symptoms that can be related to long COVID[3,4]. Although the exact number of people living with this condition is uncertain, it is believed that more than 17 million people across the European Region may have experienced it during the first two years of the pandemic[5].
The statistics become less apparent when evaluating the impact of this syndrome in the Americas. However, in several countries, efforts have been made to clarify the situation in the region[6,7]. Despite most symptoms described by those affected by long COVID are mild and self-limiting, there is a considerable proportion of patients who present with long-lasting and debilitating symptoms that lead to disability and withdrawal from the world of work in otherwise healthy people[8]. Mechanisms recently discovered as possible causes of these disorders have been proposed, such as the persistence of functional viral RNA in various tissues, which can last up to two years[9]. Furthermore, most studies indicate that women are disproportionately affected by this syndrome[8].
Regarding the direct consequences of the virus, the high general rate of immunization with the first vaccine platforms, along with a protective effect due to natural immunity, has significantly limited the acute post-viral effects, understood also as acute post-COVID conditions (PCC) or post-acute sequelae of COVID (PASC)[10]. The COVID-19 vaccines were designed to reduce hospitalization and mortality. Although the use of updated vaccine platforms is based on more updated lineages such as XBB1.5 (which has been prevalent in most of the northern hemisphere), its adoption is still new and in process in Latin America and has even begun to promote the use of mRNA platform for more recent lineages such as JN.1[11].
Information about the effects of vaccination on the long COVID condition is less clear. For instance, the risk of experiencing an adverse cardiovascular event such as stroke, acute myocardial infarction, venous thromboembolism, or type 2 diabetes increases dramatically after the first year of acute COVID infection[12].
Early vaccination has accelerated recovery from post-COVID conditions, demonstrating efficacy in reducing the risk of long COVID[13]. This protective effect was observed in people vaccinated with one or two doses, regardless of vaccination status before or after SARS-CoV-2 infection[13]. The emergence of hypertension and diabetes as post-COVID conditions underscores the importance of vaccination to mitigate the risk of long COVID, particularly among people without a history of vaccination[13].
Regarding the different symptoms presented in long COVID patients, European studies such as COVID Home identified three different phenotypes in convalescent patients: phenotype A, which affects middle-aged patients with few comorbidities and predominantly respiratory symptoms; phenotype B, observed in older women with multimorbidity and characterized by numerous neurological symptoms; and phenotype C, more prevalent in men, similar to phenotype A in the distribution of symptoms but with an average age similar to phenotype B[14].
Other forms of phenotyping, such as those proposed by Hao, further delineate sub-phenotypes based on cardiac-renal, respiratory, musculoskeletal, and digestive manifestations that can also be found in populations in the region and that could be prevented by vaccination[15].
Due to the exploratory nature of our research, we proposed a scoping review against other types of synthesis studies. This scoping review aims to comprehensively respond to the following research question: What was the role of SARS-CoV-2 immunization against the development or severity of long COVID in the Americas region?
2. Materials and Methods
2.1. Protocol and Registration
This study follows the PRISMA-ScR guidelines for reporting scoping reviews[16]. Before the search started, the protocol for this scoping review was uploaded to the Open Science Framework repository[17]. The protocol was elaborated following the Joanna Briggs Institute (JBI) guidelines for reporting Scoping reviews[18,19].
2.2. Eligibility Criteria
This review included observational and experimental studies from Central America, South America, and the Caribbean (Mexico was also considered). The studies involved adults previously vaccinated against SARS-CoV-2 and later developed long COVID, diagnosed clinically by the authors’ criteria. Case reports, case series, opinions, commentaries, systematic reviews, and letters to the editor that did not include original results were excluded. No restrictions on language or year of publication were imposed.
2.3. Information Sources
A comprehensive search was performed in the following bibliographic databases: MEDLINE through PubMed, Scopus, Embase, Web of Science, BIREME-BVS, and SciELO. The most recent search was executed on September 7th, 2024.
2.4. Search
The concepts evaluated were Long COVID and the Effectiveness of vaccination in the prevention of Long COVID. MEsH, DeCS, Emtree, and free terms were used and linked using Boolean operators. We adapted the search strategy for each source of information, which is provided in Supplementary Material Table S1. In addition, the search was supplemented by manual exploration of the bibliographies of all included studies and a search of grey literature through preprint repositories.
2.5. Selection of Sources of Evidence
The authors used the Rayyan Intelligent Systematic Review software[20] to select evidence. In a two-step process, at least two authors (Z-SG, RJ, and F-GL) independently screened and selected all potentially relevant sources of information.
After eliminating the duplicates, the title and abstract were screened to determine whether the study could respond to the review questions. Afterward, a full-text analysis determined whether they met the selection criteria before inclusion. Disagreements on the inclusion were resolved by consensus.
2.6. Data Charting Process
Data extraction was done using the tools suggested by the JBI guidelines for reporting Scoping reviews[18]. Two reviewers (Z-SG, RJ, and F-GL) did the extraction independently and managed disagreements through consensus. Each reviewer validated the data extraction tool before collecting the data.
2.7. Data Items
The variables extracted and assessed were the year and country of publication, study design, participants' characteristics, number of doses and the type of vaccine used in the analysis, the long-COVID definition, and the efficacy measures reported.
2.8. Critical Appraisal of Individual Sources of Evidence
Methodological quality or risk of bias was not assessed as it did not meet the aim of this scoping review.
2.9. Synthesis of Results
A qualitative synthesis was performed, and the results are presented narratively and through figures and tables.
3. Results
3.1. Selection of Evidence Sources
3,466 items were extracted from the sources of information (Figure 1). 1,656 items were eliminated due to duplicates, and 1,810 articles were evaluated by title and abstract. 12 articles were analyzed by full text, discarding seven manuscripts. 5 studies were included from the sources of information, and 3 came from the manual search, with 8 articles included.
3.2. Characteristics and Results of the Sources of Evidence
62.5% (5) of the studies were published in 2023 [6,7,21,22,23] and 37.5% (3) in 2024 [24,25,26]. One article included a population from all of Latin America[6]; four were developed in Brazil [21,22,25,26], two in Mexico [7,24], and one in Bonaire [23]. The most commonly used research design was cohort studies with 50% (4) (3 prospective and one retrospective), 37.5% (3) were cross-sectional studies, and 12.5% (1) were case-control studies (Table 1).
3.3 Population study
The eight articles analyzed included 11,333 participants, 69.3% (7,857) female. Four articles reported the mean and standard deviation of the participants' age in years; three studies described the median and range, with a minimum of 14 years and a maximum of 89 years; and one manuscript did not describe the age of the research subjects (Table 1).
The majority of the sample consisted of participants from Brazil (8,425), followed by Mexico (894), Ecuador (513), and Argentina (480). Panama, Nicaragua, and Costa Rica contributed to the fewest participants (Supplementary Material Figure S1).
3.4. Definitions of Long COVID
The eight articles included define Long COVID, using different characteristics related to the diagnosis of acute COVID-19 infection, the presence of symptoms, and the duration of symptomatology compared with the current definition proposed by Ely et al. (Figure 2, Table 2).
- SARS-CoV-2 infection: All eight articles, as a requirement, include a history of acute COVID-19 infection; 37.5% (3) of the studies describe the need for a positive laboratory test for SARS-CoV-2, and 12.5% (1) include suspicion and confirmation of acute infection.
- Symptoms: The persistence of symptoms from the acute stage was considered by 100% (8) of the studies; remitting and recurrent symptoms and symptom progression were not included in any definition. 62.5% (5) described developing new symptoms after the acute stage of infection.
- Time of presentation: 100% (8) of the studies describe a specific time of permanence of symptomatology following acute infection. 50% (4) consider 12 weeks or more, 12.5% (1) describe 8 weeks or more, and 37.5% (3) use 4 weeks or more as a defining criterion.
3.5. Vaccination Status
Six articles reported the number of doses required to be considered complete vaccination status; 50% (3) used one dose or more of COVID-19 vaccine as a criterion, and the remaining 50% (3) used two doses as a definition.
3.6. Reducing the Incidence of Long COVID
Four studies evaluated the risk of developing Long COVID, using different comparisons concerning the number of doses administered and vaccination status (Figure 3).
Batista et al. evaluated the complete vaccination status, demonstrating that it decreases the risk of Long COVID [25].
3.7. The severity of Symptoms Related to Long COVID
One article studied the change in symptom severity and evaluated 14 symptoms, 13 with neutral results. Describes that vaccination increases the severity of heart palpitations [23].
3.8. Duration of Long COVID Symptoms
Two studies considered symptom persistence as an outcome. Fuller et al. [26] found that vaccination with two or more doses decreases Long COVID symptoms. Del Carpio-Orantes et al. [24] did not identify a significant decrease in vaccinated participants' neurologic, cardiac, pulmonary, gastrointestinal, and musculoskeletal symptoms. One study demonstrated that administering one or more doses before acute COVID-19 infection decreases the time to resolution of long COVID [7].
4. Discussion
This scoping review underscores the complex relationship between SARS-CoV-2 vaccination and long COVID in the Americas. Despite considerable advances in understanding long COVID, including its clinical definitions and phenotypes, the role of immunization in mitigating the syndrome remains unclear.
4.1. What is Already Known About This Topic
The evidence suggests that SARS-CoV-2 immunization, especially with multiple doses, could provide protection against long COVID. For instance, in a systematic review and meta-analysis, Watanabe et al. reported that two vaccine doses were related to a lower risk of developing long COVID compared to no vaccination (OR= 0.64; 95% CI 0.45-0.92) and a significant effect compared to one-dose vaccination (OR= 0.60; 95% CI, 0.43-0.83)[27].
4.2. Main Findings
In Latin America, some studies found no effect with one or two doses of vaccination [21,22], while others found a risk reduction with three or more doses[6,21]. These results contrast with large population-based European studies where COVID-19 vaccination was strongly associated with decreased probability of developing long COVID (HR=0.48; 95% CI 0.34–0.68)[28]. The findings emphasize the necessity for consistency in defining the "complete vaccination" status and its temporal association with SARS-CoV-2 infection.
The protective effect reported with greater vaccine doses is consistent with previously proposed mechanisms, such as reduced virus persistence and immune response regulation [9,11]. However, the neutral effects found in certain studies require additional research into individual and geographical characteristics that may affect vaccine efficacy, such as sex[29], age[13,28], comorbidities[30], time of vaccination (before or after SARS-CoV-2 infection[13,27] or during delta or omicron phases[31]) and type of vaccines[28].
The effect of vaccination on the severity and duration of long COVID is less clear because of the lack of appropriate definitions. Large studies demonstrated that vaccination reduced the incidence of severe thromboembolic and cardiovascular complications of long COVID[32]. Locally, Fuller et al. [26] found that immunization with two or more doses reduced the persistence of symptoms, confirming its possible effect in speeding recovery reported by Peluso et al.[9] On the other hand, Carpio-Orantes et al. 20 reported no significant reduction in specific symptoms among vaccinated individuals. These contradictory results can be related to different long COVID phenotypes and their response to immunization, as previously shown in other cohorts[31].
Additionally, assessing adverse effects was another relevant issue in the selected studies. Berry et al.23 reported an increase in the severity of heart palpitations following immunization in select populations, emphasizing the need to weigh the benefits of vaccination against the potential hazards described in numerous studies[33,34,35].
4.3. Implications for Public Health in the Americas. A call to action
The vast majority of studies evaluating the impact of immunization in long COVID have been developed in regions different than Latin America. Moreover, differences in regional vaccine access and adoption underline critical public health challenges in these countries. With most included studies originating from Brazil and Mexico, the findings may not fully represent the diverse contexts of the region. Expanding research efforts to include underrepresented countries, such as those in Central America, the Caribbean, and the Andean region, is essential for a comprehensive understanding of the impact of vaccination on long COVID.
The emergence of new vaccine platforms designed to cover new lineages offers promising alternatives for reducing long COVID risks. However, their implementation in the Americas has been slow, highlighting the need for robust vaccination campaigns and policies to ensure equitable access.
4.4. Limitations
This review is subject to limitations related to small sample sizes, varied methodologies, and inconsistent definitions of long COVID. Furthermore, the absence of data on specific populations and the restricted scope of observational designs limit the generalizability of findings. Future regional research should prioritize longitudinal and interventional studies to determine the causal association between vaccination and long-term COVID outcomes.
5. Conclusions
In Latin America, vaccination against SARS-CoV-2 appears to reduce the incidence and duration of long COVID, but its effectiveness varies depending on the population and vaccine regimen. These findings highlight the necessity of ongoing research and public health initiatives to improve immunization strategies, especially in areas with varying socioeconomic and healthcare landscapes.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/doi/s1, : Geographic distribution of the participants; : Main concepts and related keywords.
Author Contributions
Zambrano-Sánchez Gabriela: Conceptualization, Investigation, Resources, Validation, Visualization, and Writing-Original Draft preparation. Rivadeneira Josue: Conceptualization, Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing-Original Draft preparation, Writing-Review & Editing. Manterola Carlos: Conceptualization, Methodology, Supervision, Validation, Writing-Review & Editing Otzen Tamara: Conceptualization, Methodology, Supervision, Validation, Writing-Review & Editing Fuenmayor-González Luis: Conceptualization, Investigation, Methodology, Resources, Validation, Visualization, Writing-Original Draft preparation, and Writing-Review & Editing
Funding
This research was funded by ANID + SUBVENCIÓN A INSTALACIÓN EN LA ACADEMIA CONVOCATORIA AÑO 2022 + Folio (85220114).
Institutional Review Board Statement
Due to the nature of this work and the use of secondary data, no ethical approval was needed.
Data Availability Statement
Search results are available under reasonable request.
Acknowledgments
J.R. received a scholarship from ANID–Subdirección de Capital Humano / Doctorado Nacional / 2024–21242396.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- CDC. Long COVID or Post-COVID Conditions 2023. https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html#. (accessed on 11 June 2023).
- Ely EW, Brown LM, Fineberg H V. From the National Academy of Medicine Long Covid Defined Medicine Committee on Examining the Working Definition for Long Covid*. N Engl j Med 2024, 18, 391. [Google Scholar]
- Sk Abd Razak R, Ismail A, Abdul Aziz AF, Suddin LS, Azzeri A, Sha’ari NI. Post-COVID syndrome prevalence: a systematic review and meta-analysis. BMC Public Health 2024, 24, 1–19. [Google Scholar] [CrossRef]
- Woodrow M, Carey C, Ziauddeen N, Thomas R, Akrami A, Lutje V, et al. Systematic Review of the Prevalence of Long COVID 2023. [CrossRef]
- WHO. Post COVID-19 condition (Long COVID) 2022. https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition. (accessed on 11 November 2023).
- Angarita-Fonseca A, Torres-Castro R, Benavides-Cordoba V, Chero S, Morales-Satán M, Hernández-López B, et al. Exploring long COVID condition in Latin America: Its impact on patients’ activities and associated healthcare use. Front Med (Lausanne) 2023, 10, 1168628. [Google Scholar] [CrossRef]
- Núñez I, Gillard J, Fragoso-Saavedra S, Feyaerts D, Islas-Weinstein L, Gallegos-Guzmán AA, et al. Longitudinal clinical phenotyping of post COVID condition in Mexican adults recovering from severe COVID-19: a prospective cohort study. Front Med (Lausanne) 2023, 10, 1236702. [Google Scholar] [CrossRef]
- Alvarez-Moreno CA, Pineda J, Bareño A, Espitia R, Rengifo P. Long COVID-19 in Latin America: Low prevalence, high resilience or low surveillance and difficulties accessing health care? Travel Med Infect Dis 2023, 51, 102492. [Google Scholar] [CrossRef] [PubMed]
- Peluso MJ, Swank ZN, Goldberg SA, Lu S, Dalhuisen T, Borberg E, et al. Plasma-based antigen persistence in the post-acute phase of COVID-19. Lancet Infect Dis 2024, 24, e345–7. [Google Scholar] [CrossRef]
- PAHO/WHO. Summary Situation and COVID-19 Cases and Deaths 2023. https://www.paho.org/en/covid-19-weekly-updates-region-americas. (accessed on 11 November 2023).
- WHO. Statement on the antigen composition of COVID-19 vaccines 2024. https://www.who.int/news/item/26-04-2024-statement-on-the-antigen-composition-of-covid-19-vaccines (accessed ). 30 November.
- Xie Y, Xu E, Bowe B, Al-Aly Z. Long-term cardiovascular outcomes of COVID-19. Nature Medicine 2022, 28, 583–90. [Google Scholar] [CrossRef]
- Gao P, Liu J, Liu M. Effect of COVID-19 Vaccines on Reducing the Risk of Long COVID in the Real World: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health 2022, 19. [Google Scholar] [CrossRef]
- Tami A, van der Gun BTF, Wold KI, Vincenti-González MF, Veloo ACM, Knoester M, et al. The COVID HOME study research protocol: Prospective cohort study of non-hospitalised COVID-19 patients. PLoS One 2022, 17, e0273599. [Google Scholar] [CrossRef]
- Zhang H, Zang C, Xu Z, Zhang Y, Xu J, Bian J, et al. Data-driven identification of post-acute SARS-CoV-2 infection subphenotypes. Nature Medicine 2022, 29, 226–35. [Google Scholar] [CrossRef]
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169, 467–73. [Google Scholar] [CrossRef]
- Zambrano-Sánchez G, Rivadeneira J, Manterola C, Fuenmayor-González L. Immunization as protection against long COVID in the Americas: A scoping review protocol. OSF. [CrossRef]
- Peters MD, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil H. Chapter 11: Scoping Reviews. In: Aromataris E, Munn Z, editors. Joanna Briggs Institute Reviewer’s Manual, 2020.
- Peters MDJ, Godfrey C, McInerney P, Khalil H, Larsen P, Marnie C, et al. Best practice guidance and reporting items for the development of scoping review protocols. JBI Evid Synth 2022, 20, 953–68. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev 2016, 5, 1–10. [Google Scholar] [CrossRef]
- Marra AR, Sampaio VS, Ozahata MC, Lopes R, Brito AF, Bragatte M, et al. Risk factors for long coronavirus disease 2019 (long COVID) among healthcare personnel, Brazil, 2020–2022. Infect Control Hosp Epidemiol 2023, 44, 1972–8. [Google Scholar] [CrossRef]
- Neves Amorim CE, Silveira Cazetta G, Pontello Cristelli M, Requião-Moura LR, Rodrigues da Silva E, Pinheiro Vale L, et al. Long COVID Among Kidney Transplant Recipients Appears to Be Attenuated During the Omicron Predominance. Transplantation 2023, 108, 963–9. [Google Scholar] [CrossRef]
- Berry DSF, Dalhuisen T, Marchena G, Tiemessen I, Geubbels E, Jaspers L. Association between post-infection COVID-19 vaccination and symptom severity of post COVID-19 condition among patients on Bonaire, Caribbean Netherlands: a retrospective cohort study. MedRxiv 2023, 2023-06. [CrossRef]
- Del Carpio-Orantes L, Trelles-Hernández D, García-Méndez S, Sánchez-Díaz JS, Aguilar-Silva A, López-Vargas ER. Clinical-epidemiological characterization of patients with long COVID in Mexico. Gac Med Mex 2024, 160, 144–51. [Google Scholar] [CrossRef]
- Batista KBC, Fernandez MV, Barberia LG, Silva ET da, Pedi VD, Pontes BMLM, et al. Overview of long COVID in Brazil: a preliminary analysis of a survey to think about health policies. Cad Saude Publica 2024, 40, e00094623. [Google Scholar] [CrossRef]
- Fuller T, Flores Mamani R, Ferreira Pinto Santos H, Melo Espíndola O, Guaraldo L, Lopes Melo C, et al. Sex, vaccination status, and comorbidities influence long COVID persistence. J Infect Public Health 2024, 17, 102562. [Google Scholar] [CrossRef]
- Watanabe A, Iwagami M, Yasuhara J, Takagi H, Kuno T. Protective effect of COVID-19 vaccination against long COVID syndrome: A systematic review and meta-analysis. Vaccine 2023, 41, 1783–90. [Google Scholar] [CrossRef]
- Català M, Burn E, Rathod-Mistry T, Kostka K, Yi Man W, Delmestri A, et al. The effectiveness of COVID-19 vaccines to prevent long COVID symptoms: staggered cohort study of data from the UK, Spain, and Estonia 2024. [CrossRef]
- Iba A, Hosozawa M, Hori M, Muto Y, Kihara T, Muraki I, et al. Booster vaccination and post COVID-19 condition during the Omicron variant-dominant wave: A large population-based study. Clinical Microbiology and Infection 2024. [CrossRef]
- Camporesi A, Morello R, Rocca A La, Zampino G, Vezzulli F, Munblit D, et al. Characteristics and predictors of Long Covid in children: a 3-year prospective cohort study. EClinicalMedicine 2024, 76, 102815. [Google Scholar] [CrossRef] [PubMed]
- Wu Q, Zhang B, Tong J, Bailey LC, Bunnell HT, Chen J, et al. Real-world effectiveness and causal mediation study of BNT162b2 on long COVID risks in children and adolescents. EClinicalMedicine 2025, 79, 102962. [Google Scholar] [CrossRef] [PubMed]
- Mercadé-Besora N, Li X, Kolde R, Trinh NT, Sanchez-Santos MT, Man WY, et al. The role of COVID-19 vaccines in preventing post-COVID-19 thromboembolic and cardiovascular complications Cardiac risk factors and prevention. Heart 2024, 110, 635–43. [Google Scholar] [CrossRef]
- Flores-Lastra N, Rivadeneira-Dueñas J, Fuenmayor-González L, Guayasamín-Tipanta G, Jácome-García M, Otzen T, et al. Safety Profile of Homologous and Heterologous Booster COVID-19 Vaccines in Physicians in Quito-Ecuador: A Cross-Sectional Study. Vaccines (Basel) 2023, 11. [CrossRef]
- Faksova K, Walsh D, Jiang Y, Griffin J, Phillips A, Gentile A, et al. COVID-19 vaccines and adverse events of special interest: A multinational Global Vaccine Data Network (GVDN) cohort study of 99 million vaccinated individuals. Vaccine 2024, 42, 2200–11. [Google Scholar] [CrossRef]
- Yaamika H, Muralidas D, Elumalai K. Review of adverse events associated with COVID-19 vaccines, highlighting their frequencies and reported cases. J Taibah Univ Med Sci 2023, 18, 1646–61. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flow diagram for studies selection.
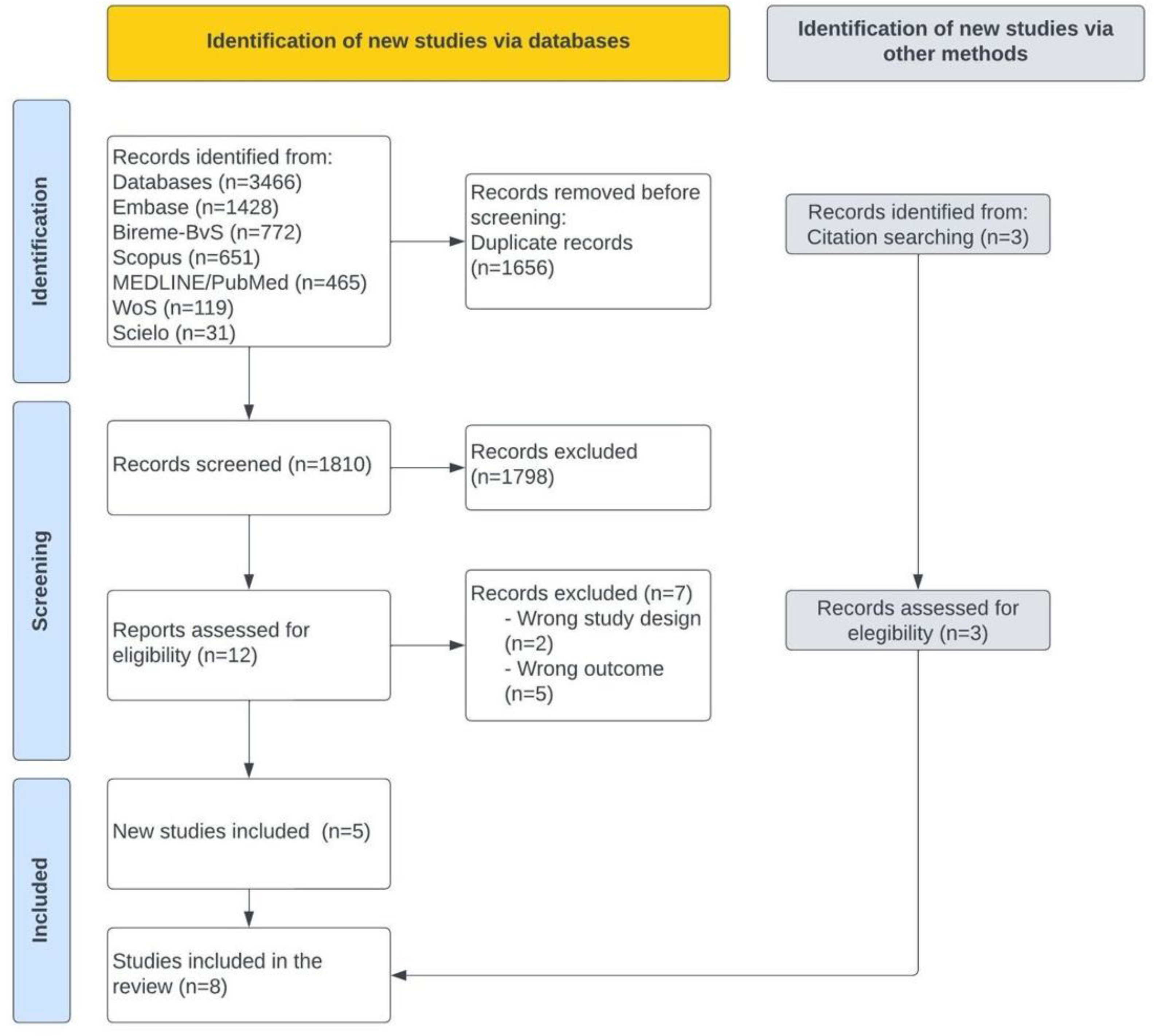
Figure 2.
Variability in Long COVID definitions: Comparison of diagnostic criteria, symptomatology, and duration across primary articles.
Figure 2.
Variability in Long COVID definitions: Comparison of diagnostic criteria, symptomatology, and duration across primary articles.
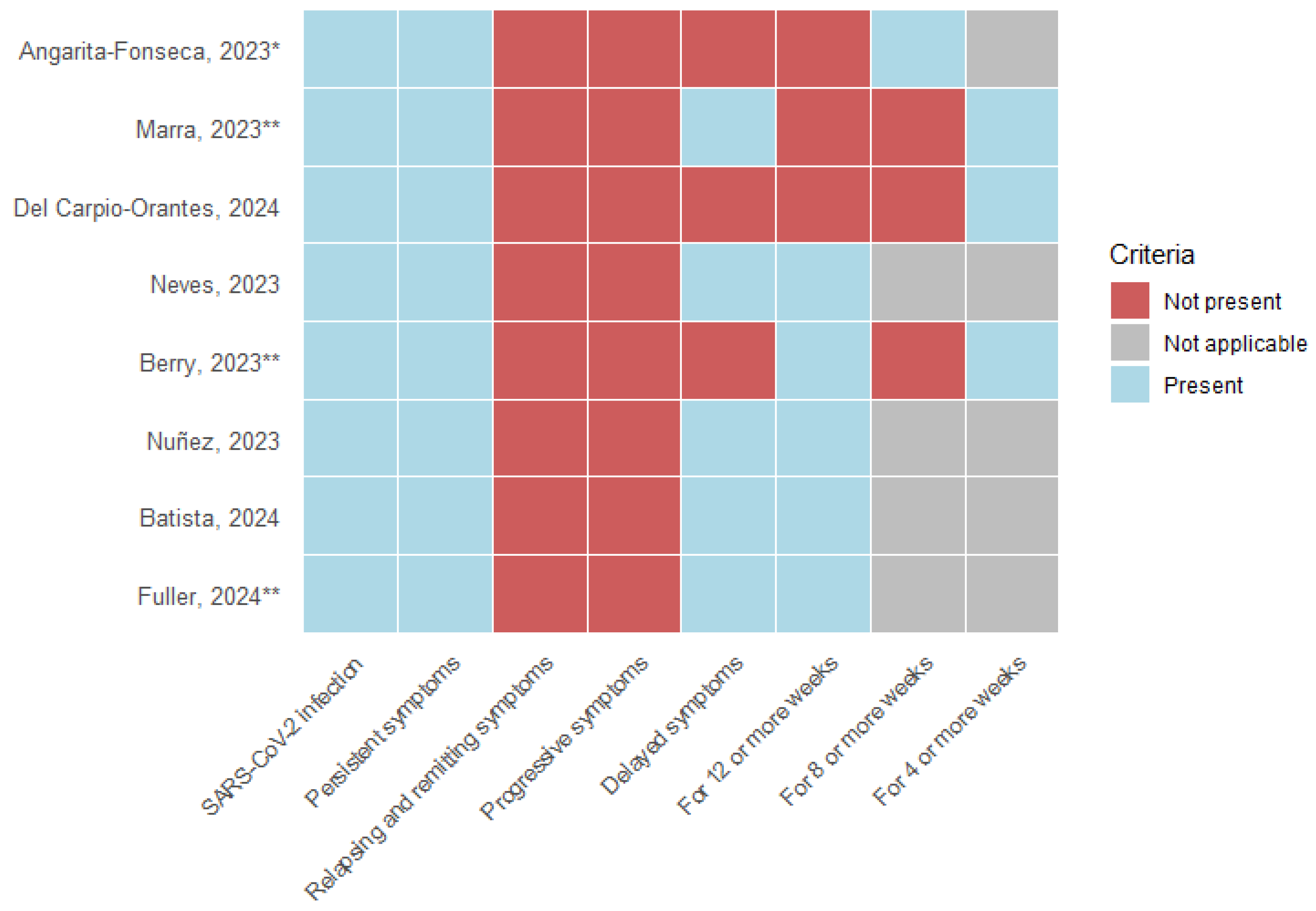
Figure 3.
Impact of vaccination on Long COVID incidence: Dose-dependent risk reduction of primary.
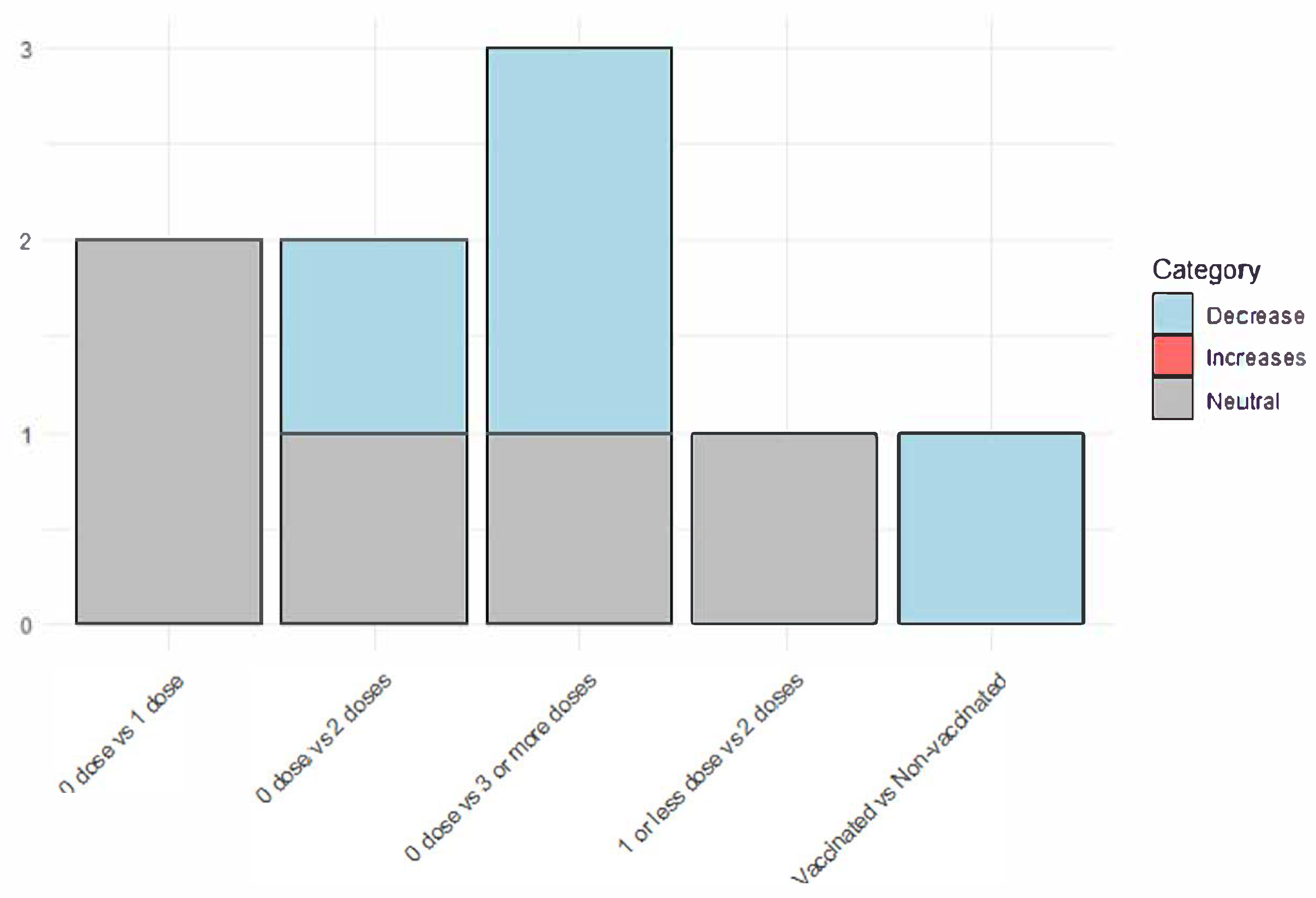

Table 1.
Characteristics of the included studies.
| Author, year | Country | Design | Number of participants | |
|---|---|---|---|---|
| Sex n, (%) | Age, years | |||
| Angarita-Fonseca, 20236 | Latin-America | Cross-sectional study | Men: 840 (34.1); Women:1,626 (65.9) |
Mean (SD): 39.5 (53.3) |
| Berry, 202323 | Bonaire | Retrospective cohort study | Men: 10 (21.2); Women:37 (78.8) |
Median (range): 47 (14 - 89) |
| Marra, 202321 | Brazil | Case-control study | Men: 1,950 (27.6); Women: 5,101 (72.4) |
Mean (SD): General: 37.5 (NR) Cases: 38.1 (8.7); Controls: 37.2 (9.0) |
| Neves, 202322 | Brazil | Prospective cohort study | Men: 338 (56.1); Women: 264 (43.9) |
Mean (SD): 51 (12) |
| Nuñez, 20237 | Mexico | Prospective cohort study | Men: 126 (65.6); Women: 66 (34.4) |
Median (range): 53 (45 - 64) |
| Batista, 202425 | Brazil | Cross-sectional study | Men: 59 (11.9); Women: 437 (88.1) |
NR |
| Del Carpio-Orantes, 202424 | Mexico | Cross-sectional study | Men: 65 (32,0); Women: 138 (68,0%) |
Mean (SD): 41.8 (11.3) |
| Fuller, 202426 | Brazil | Prospective cohort study | Men: 88 (31.8); Women: 188 (68.2) |
Median (range): 45 (18 - 88) |
Table 2.
Efficacy of the immunization against Long COVID.
| Author, year | “Fully vaccinated” status | Vaccine type | Long-COVID definition | Efficacy measures | Conclusions | Limitations |
|---|---|---|---|---|---|---|
| Angarita-Fonseca, 20236 | Two doses | NR | Individuals with a history of probable or confirmed SARS-CoV-2 infection, usually 3 months from the onset of COVID-19 with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis. | Outcome: Risk of development of LCC. Multivariable logistic regression.
|
Fully vaccinated patients were less likely to have LCC compared with unvaccinated or partially vaccinated subjects. | The design of the study allows the occurrence of the different bias. Data collection (electronic survey) and the non-probabilistic sampling, decrease the methodological quality of the study, the effect size, and the potential generalization of results. |
| Berry, 202323 | At least one dose of the Pfizer vaccine at least 8 weeks after SARS-CoV-2 infection | mRNA: 36, Unvaccinated: 11 |
Individuals with a laboratory-confirmed SARS-CoV-2 positive test result, for whom at least one symptom self-attributed to the experienced SARS-CoV-2 infection lasted longer than four weeks. | Outcome: Self-reported change in symptom severity. Multiple covariate adjusted linear regression model. Regression coefficients and 95% CI:
|
Vaccination wassignificantly associated with reduced severity of heart palpitations. | Small sample size; residual confounding may exist due to unmeasured confounding variables; the collection of data outcome data at one point in time, at different intervals since infection (and vaccination, for those applicable limited the comparison of severity scores of Long-COVID symptoms at multiple moments after initial infection at an individual level; Authors reported a linear regression using cathegorical variables to report the effect measures. |
| Marra, 202321 | Analysis were performed whether 1,2,3, or 4 doses were administered. | Inactivated virus= 3,259; Viral vector= 3,255; mRNA=148 |
Signs and symptoms that developed during or following a SARS-CoV-2 RT-PCR confirmed infection, continued for >4 weeks, and could not explained by an alternative diagnosis. | Outcome: Risk of development of long COVID. Logistic Regression multivariable analysis.
|
Four doses of COVID-19 vaccines is associated with a lower probability of develop Long-COVID. | As the study was performed only in Healthcare personnel with positive COVID-19 laboratory results, some infected individuals with no laboratory confirmed results may be lost. Also, information bias could be present. |
| Neves, 202322 | Two doses | Homologous inactivated whole-virion vaccine: 189 (36%); Homologous mRNA vaccine: 24 (5%); Homologous viral-vector vaccine:96 (19%); Heterologous inactivated + mRNA: 86 (17%); Heterologous inactivated + viral vector: 44 (9%); Heterologous mRNA + viral vector: 68 (13%); Other heterologous regimens: 5 (1%) |
Physical complaints newly developed during or after the acute phase, persisting for >12 weeks, and not explained by an alternative diagnosis. | Complete vaccination schedule and the risk of Long COVID. HR: 0.89; 95% CI: 0.57–1.41 |
Complete vaccination schedule was not statistically significant with the risk of develop Long-COVID | A relatively modest participation rate, Also, notable qualitative disparities emerged between survey responders and nonresponders, especially regarding the vaccination rates and the acute-phase symptoms |
| Nuñez, 20237 | At least one dose of any SARS-CoV-2 vaccine at least 14 days before the date on which symptoms of acute infection began | NR | Patients experiencing any symptoms not present before acute COVID-19 onset, and that persisted for longer than 90 days after acute COVID-19 onset. | Outcome: probability to experience a shorter time to PCC resolution. HR: 3.16; 95%CI 1.21-8.26 |
Prior SARS-CoV-2 vaccination and acute COVID-19 symptom were associated with a shorter time to Long-COVID resolution. | Study power/sample size calculations were not performed given the explorative nature of this study and the lack of reliable data on PCC prevalence when it was designed. |
| Batista, 202425 | NR | NR | Symptoms that remain or appear for the first time within three months of SARS-CoV-2 infection. | NR± | The occurrence of prolonged COVID was higher among those who were unvaccinated compared with those who received COVID-19 vaccine. | The sampling method used. The survey was published on social networks, which may have limited its representation of the Brazilian population. Self-selection bias. |
| Del Carpio-Orantes, 202424 | One dose or more | NR | Persistence of COVID-19 symptoms four weeks after the acute episode. |
|
In the present analysis, no risk association was found with the history of vaccination. | The design of the study does not permit to establish proper associations, and the low number of participants. |
| Fuller, 202426 | Two or more doses | NR | Symptoms that began within three months of the positive SARS-CoV-2 test. | Outcome: Persistence of Long COVID in not fully vaccinated people. HR: 1·96, 95 % CI: 1·03–3·7 |
There was a significant association between the persistence of Long-COVID over time with not being fully vaccinated. | The fact that was a single center study with a small sample size. The frequency of comorbidities was high among participants, which may restrict the generalizability of our findings to healthier populations. Furthermore, since the analysis was conducted during the Omicron period, there were no participants who remained uninfected with COVID-19. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



