Submitted:
29 May 2025
Posted:
29 May 2025
You are already at the latest version
Abstract
The immense role that community health must play in a country’s national development drive cannot be overemphasized regardless of the inequalities in its provision. Non-governmental organizations (NGOs) help to bridge the gap in certain parts of Nigeria. This study explored the community perception of the role of the NGO Access to Basic Medical Care Clinic (ABCC) in basic healthcare provision, with a view to identifying the community perception of the impact, prospects, and challenges of ABCC. Using the convergent mixed methods approach, a self-constructed questionnaire and focus groupsion were used to collect data from 300 conveniently and purposively selected study participants. Descriptive and thematic analyses were done and then triangulated to meet research objectives. The study shows that there is a significant increase in health insurance coverage for all, especially the vulnerable and the uninsured; significant health care provision is in place for hypertensive and diabetic patients; there is a significant reduction in under-five and maternal mortality rates; and hundreds of Nigerians from sudden and untimely death, thereby increasing their life expectancy. Abuse of free services by minorities and the inability of the patients to go for further treatment when being referred or to buy recommended drugs due to lack of financial capacity are major challenges in ABCC. ABCC would serve as a source of motivation for emerging free service clinics, improved standards of health in different localities, a boost in standards of living, and motivation for other entrepreneurs to invest in free service clinics. Inclusion of mental health treatment, adequate provision of funds through partnership with the state government and corporate network with private investors, and collaboration with established hospital and health organizations are recommended for ABCC improvement and sustainability.
Keywords:
Basic-medical-care-clinic
; community perception
; NGO
; public health
; community development
Introduction
Health disparity is one of the major development challenges in developing countries including Nigeria. It has been said that a society is assessed by the way they care for their most vulnerable citizens. Nigeria loses about 2300 under five years olds and 145 women of childbearing age in a day, making it the second largest contributor to the under five and maternal mortality rate in the world (UNICEF 2013). Some of the challenges facing the country in terms of primary health care provision include limited access to health care, poverty and inequalities, lack of skilled health workers, inadequate infrastructure, internal conflict in parts of the country, crime and corruption, low political commitment to implementation of approved health policies.
Consequently, the fundamental essence of the Universal Health Coverage making health care accessible, available and affordable to rural poor is ignored to whatever extent (Atibinye et al. 2015) and health and wellbeing which is the goal three sustainable development goals (SDGs) is very far in view. In an attempt to resolving this menace given the immense role that community health has to play in the country’s national development drive, Access to Basic (medical) Care (ABC) Foundation, a non-governmental organisation initiated in 2012 aim to complement the efforts of the Oyo state government in making quality healthcare available and accessible to all without leaving a deep hole in their pockets. It is developing and sustaining health care for the future. The ABC medical Foundation ensures healthcare for people in the various local government areas of Oyo State.
Methods and Materials
Study Design and Setting
This study uses mixed methods to explores the community perception of the impacts, challenges and prospects of the intervention of Access to Basic medical Care Clinic (ABCC) in boasting primary health care in Oyo state. This study is a part of a larger study evaluating the community perception of the quality of the impacts of ABCC covering all local government in Oyo State.
Study Participants and Sampling
Access to Basic Care Foundation have 10 fully operational clinics that attend to an average of 500 people each, every week. That’s about 5000 patients in a week, an average of 20,000 people in a month. A total of 300 participants were involved in the study. This consisted primarily of a health convenient sample care of patients randomly selected in ABCC primary health care centres. They were selected from three centres based on their availability at the time of visit in Access to Basic (medical) Care Clinic (ABCC) Ibadan Northwest (Eleyele) and Ibadan Southwest (Aleshinloye) They constituted the respondents for the survey questionnaire. In addition, focus group discussion were conducted with some of the patients based on availability at the clinic.
Instrument for Data Collection
A survey questionnaire and focus group guides for patients were used to collect both quantitative (via questionnaire) and qualitative (via focus group) data. The survey is a self constructed-item instrument in three sections: Section A consist of the characteristics, on Socio-demographic and Section B is on the community perception of the impact of healthcare and Section C is on hindrances to the quality of healthcare. The focus group guide contains open ended question to explore their activities, personal experiences of patients, perception of quality in their own view, challenges and prospects of ABC.
Procedure for Data Collection
With the help of research assistant data were collected within three months at the three centres selected. The 300 questionnaires were both self-administered and interviewer administered. All the questionnaires were retrieved on each day of administration; the response rate was 100%. The focus group discussion for group of patients were conducted by the principal investigator at the clinic. Each interview lasted for between 30 to 45 minutes and were all audio-recorded, and field notes were also taken.
Data Analysis
Data cleaning, editing, and coding were firstly carried out. Then, Quantitative data were coded and analysed using SPSS. The qualitative data were transcribed, categorized, coded, thematically analysed, and presented using narratives and verbatim quotes. The two strands of data (quantitative and qualitative) were synergised according to the research objectives: the community perception of the quality of the intervention and the challenges and prospects of the intervention.
Ethical Consideration
No ethical approval was required for this study; however, verbal and written consent from the participants were documented before the study. Institutional approval for the study was obtained. ABCC granted permission from their headquarters and study participants also gave permissions and consents at each centred respectively.
Results
Socio-Demographic Characteristics of Respondents
The age distribution shows that 56% of the respondents are above the age of 60years: they are mostly dependants though many of them still engaged in petty trading, 25.3% are within the range of 41yrs – 60yrs: the respondents are still active physically and economically, 14.3% are below the age of 18yrs: which falls within schooling age, dependent on parents. They are predominantly Muslim (58.7%), petty traders (55.6%), above 60 yrs (56%) and with no formal Education (43%) (Figure 1).
Perception of Impact
This section analyses the perception of the respondents on the impact of ABCC on the community. In the course of this analysis seven (7) factors of comfort are considered, they are Significant increase in health insurance coverage, significant reduction in under five and maternal mortality rate , Quality healthcare is made available and accessible to all, Primary health challenges is tackled , Significant health care provision is in place for hypertensive and diabetic patients, Access to health care for those who are vulnerable and uninsured, Health care services are provided at no cost at all to the patients (Table 1).
Table 2 and table 3 above shows that about 87% of the respondents indicated that Significant increase in health insurance coverage was low before the introduction of ABCC while 96.3% of the respondents indicated Significant increase in health insurance coverage is now high since the introduction of ABCC, 64.7% indicated that significant reduction in under five and maternal mortality rate was low before the introduction of ABCC while 100% indicated that it is now high since the introduction of ABCC (Table 2).
Perception of the Impact of ABCC
Similarly, 98.3% indicated that Significant health care provision is in place for hypertensive and diabetic patients since the introduction of ABCC while 19.3% indicated that it was low before its emergence. Quality healthcare is not made available and accessible to all before the introduction of ABCC. 81% of the respondents indicated that it was low while 98% of the respondents indicated that available and accessibility of Quality healthcare to all is now high since the introduction of ABCC. Also 87% reported that Primary health challenges have not been tackled before and 98.3% reported that it is now being tackle since the introduction of ABCC. Further, Access to health care for those who are vulnerable and uninsured and Health care services are provided at no cost at all to the patients were rated by 90.3% and 89.3% of the respondents respectively as low before the introduction of ABCC while 96.7% and 95% of the respondents respectively indicated that they are high since the emergence of ABCC (Figure 2).
In the focus group section, the respondents for the qualitative data, was also asked what the impact of ABCC since the inception was. Participants expressed an immense gratitude to God for the great impact the clinic has affected in the lives of the community member. These were the words of one of the respondents:
“Many who should have experience sudden death have been saved by God through this clinic. My Blood Pressure was 190 the first time I came to ABCC, and the doctor exclaimed, that I should thank God that He really loves me when he checked it. Now my Blood Pressure has reduced to 120. I have been coming to the clinic for two years now. I pray for sustainability of this clinic. Please report it that change of government should not stop this intervention”- Male/Above 60 years/Muslim/ Secondary Education /Dependant
Another respondent had this to say:
“Many poor people who are uninsured and vulnerable have been given access to primary health care. They don’t collect money for treatment, and they also give us drug for free except the ones they don’t have at that time that they will tell you to go and buy it”- Female/41 – 60 years/Christian/ Secondary Education /Dependant
The above response from the respondents’ shows that ABCC have already started yielding positive result in terms of saving many lives from sudden and untimely death by giving the vulnerable and the uninsured free access to quality health care.
Perception of Hindrances to Quality-of-Service Delivery
This part of the study appraises the perception of the respondents about Hindrances to quality service delivery through factors like Staff shortage. Inadequate supplies, Abuse of the free services, Overwhelming workload, financial challenges and Uncooperative patients (Figure 3). About 57.3% of the respondents indicated that Staff shortage was high while only 42.7% indicated that it was low before the introduction of ABCC while only 6.7% indicated that it is still high since the introduction of ABCC. Inadequate supplies was rate by 29.3% as high and by 70.7% of the respondents rated it as low before ABCC while only 7% indicated that it is still high and 99.3% indicated its low since the introduction of ABCC. Similarly, uncooperative patients were rated by 3% of the respondents as high and 97% as low before the introduction of ABCC while only 25% indicated that it was high and 74.7% indicated that it is now low since the introduction of ABCC. The percentage of respondents that indicated that Abuse of the free services and Overwhelming workload was low before the introduction of ABCC increased from 93% and 35.7% respectively to 99 % after the introduction of ABCC. Finally, financial challenges which was indicated as low by only 9.3% before ABCC is rated as low by 100% since the introduction of ABCC. The above findings align with the qualitative data, while participants are satisfied with overall ABCC clinic services, the study ascertained that they still want more free medicine and services. It would be impossible for free clinics to provide all the services which their patients want. ABCC may need more funds to meet the patient expectations for additional services such as more drugs. The study ascertained that the positive impact of ABCC could be sustained by getting fund from national and international organizations (Figure 3).
Limitations of the Study
This study is limited to only three centres of the ten clinics centre of ABCC in Oyo State, Nigeria. Thus, the findings may not be generalizable to the entire region. However, the mixed methods used for this study and the quality of the participants as well as the content thematic analysis were great strengths for the study.
The Prospect of ABCC
The prospects of ABCC includes it would serve as a source of motivation for emerging free service clinic, improved standard of health in different localities, a boost in standard of living, a moderate control of diseases related to death and motivate other entrepreneur to invest in free service clinic.
Conclusion
The community perception of the impact of ABCC include significant increase in health insurance coverage for all especially the vulnerable and the uninsured, significant health care provision is in place for hypertensive and diabetic patients, significant reduction in under five and maternal mortality rate and have saved hundreds of Nigerians from sudden and untimely death. The challenges of ABCC include abuse of free services by minority and very few uncooperative patients and the inability of the patients to go for further treatment when being referred or to buy recommended drug due to lack of financial capacity. It would be impossible for free clinics to provide all the services which their patients want. ABCC may need more funds to meet the patient expectations for additional services such as more drugs.
Recommendations
The study therefore proposes the following recommendations which are geared towards improving the ABCC in Ibadan metropolis and other NGO clinics in Nigeria generally. Adequate provision of funds through partnership with the state government. Inclusion of mental health treatment considering the 20 to 30 percent of its 200 million population suffering from mental disorders, with rising cases of suicide (WHO, 2014). Affiliation of the clinic with different established hospital and clinic. Collaboration with health organization for provision of regular medicine and medical services. Initiate a corporate network with private investors.
Acknowledgements
The Access to Basic medical Care Foundation for their support and cooperation. Dr. Funke Fayehun for the supervision of this project.
Conflict of Interest
The author declares that there is no Conflict of Interest.
References
- Aigbiremolen, A. et al. (2014), Primary Health Care in Nigeria: From Conceptualization to Implementation. Journal Of Medical and Applied Biosciences, 6 (2), 35 – 43.
- Campbell P, Olufunlayo TF, Onyenwenyi A.O (2010). An assessment of clients satisfaction with services at a model Primary health care in Ogun state, Nigeria. Journal of Hospital Medical, 20(1),13–8. [CrossRef]
- Dotimi, D. A. (2015) Community health practice in Nigeria: prospects and challenges, International Journal of Current Research, 7(1),11989-11992.
- Eneji M. Mai-Lafia D. Song W. (2013). Socio-Economic Impact of Graduate Unemployment on Nigeria and the Vision 20:2020. International Journal of Development Sustainability, 2(1), 1-22.
- Reerink I. Saverborn Y (1996). Quality of primary health care in developing countries. International Journal For Quality in Healthcare, 8(2), 131–139.
- UNICEF (2013), United Nations Children’s Fund. maternal and child health survey. New York.
- Our message remains equality for all.
- www.vanguardngr.com/2016/03/message-remains-equity-mrs-florence-ajimobi/ (accessed 4 April 2017).
- Florence Ajimobi Access to Basic Care Foundation in Ibadan www.ceoafrica.com/viewnews.php?tabnews=245 (accessed 4 April 2017).
- Agburu, J. (2001) Modern Research Methodology, Makurdi: The Solid Printing and Publishing Company.
- Sarantakos, S. (1993) Social Research, London: The Macmillan Press.
- Sanusi, R. Awe, A. (2009) “Perception of National Health Insurance Scheme (NHIS) by Health care consumers in OyoState”.http//www.medwelljournals.com 22/02/2011.
- Reerink I. Saverborn Y (1996). Quality of primary health care in developing countries. International Journal For Quality in Healthcare 8(2), 131–139.
- Stewart, D. ShamdasanI, P. (1990) Focus groups: theory and practice. London: Sage. [CrossRef]
- Punch Newspaper (Nov 13). 30% of Nigerians Suffer Mental Illness – FG, 2018; available at.
- http://saharareporters.com/2018/11/13/30-nigerianssuffer-mental-illness%E2%80%93-fg. Accessed 31.
- March 2020.
- WHO Preventing suicide: A global imperative, 2014 Geneva: WHO.
Figure 1.
Demographic profiles of participants; (a) Religion, (b) Age distribution, (c) Education, (d) Occupation.
Figure 1.
Demographic profiles of participants; (a) Religion, (b) Age distribution, (c) Education, (d) Occupation.
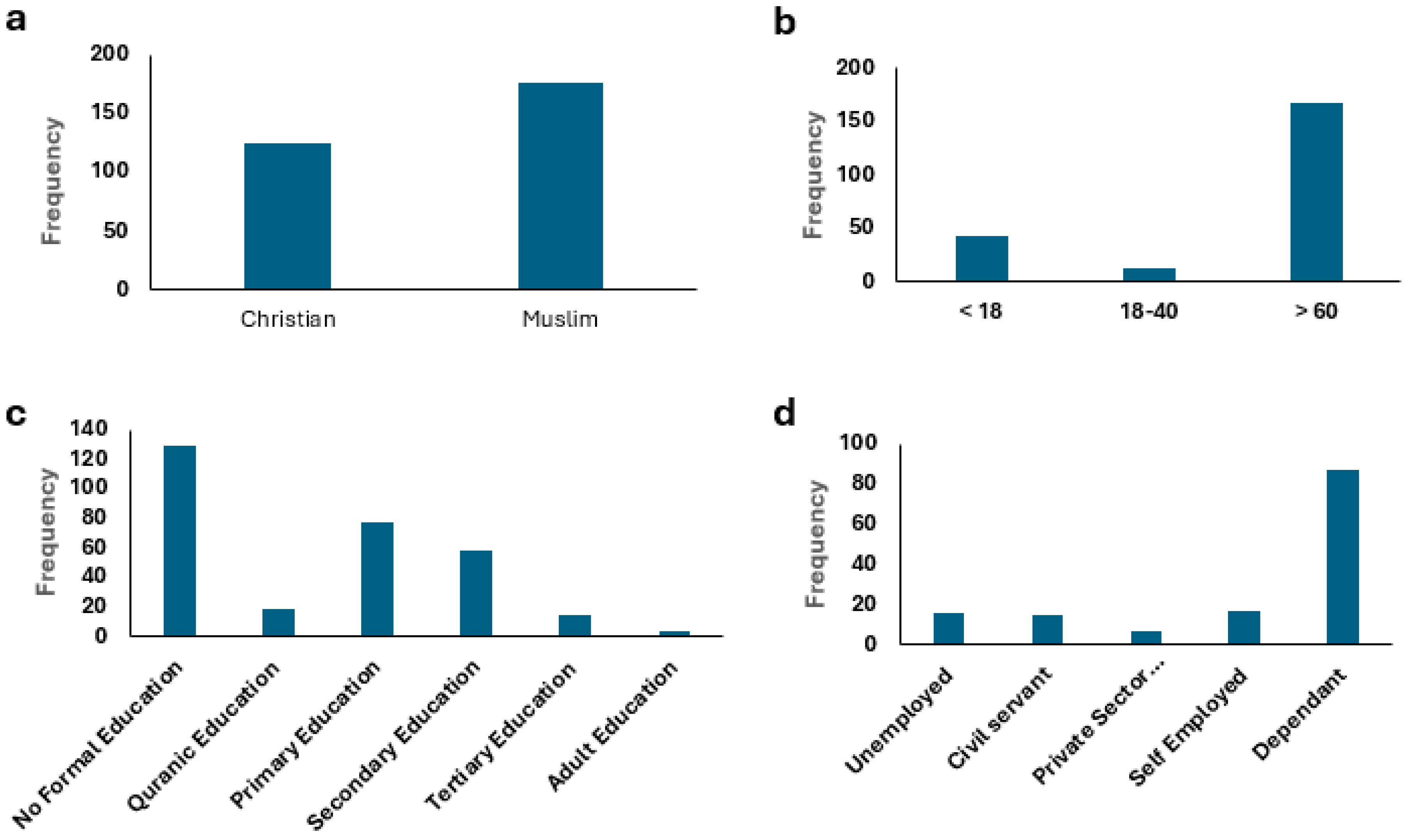
Figure 2.
Respondents’ opinions on the perception of these factors of the impact of ABCC on the community.
Figure 2.
Respondents’ opinions on the perception of these factors of the impact of ABCC on the community.
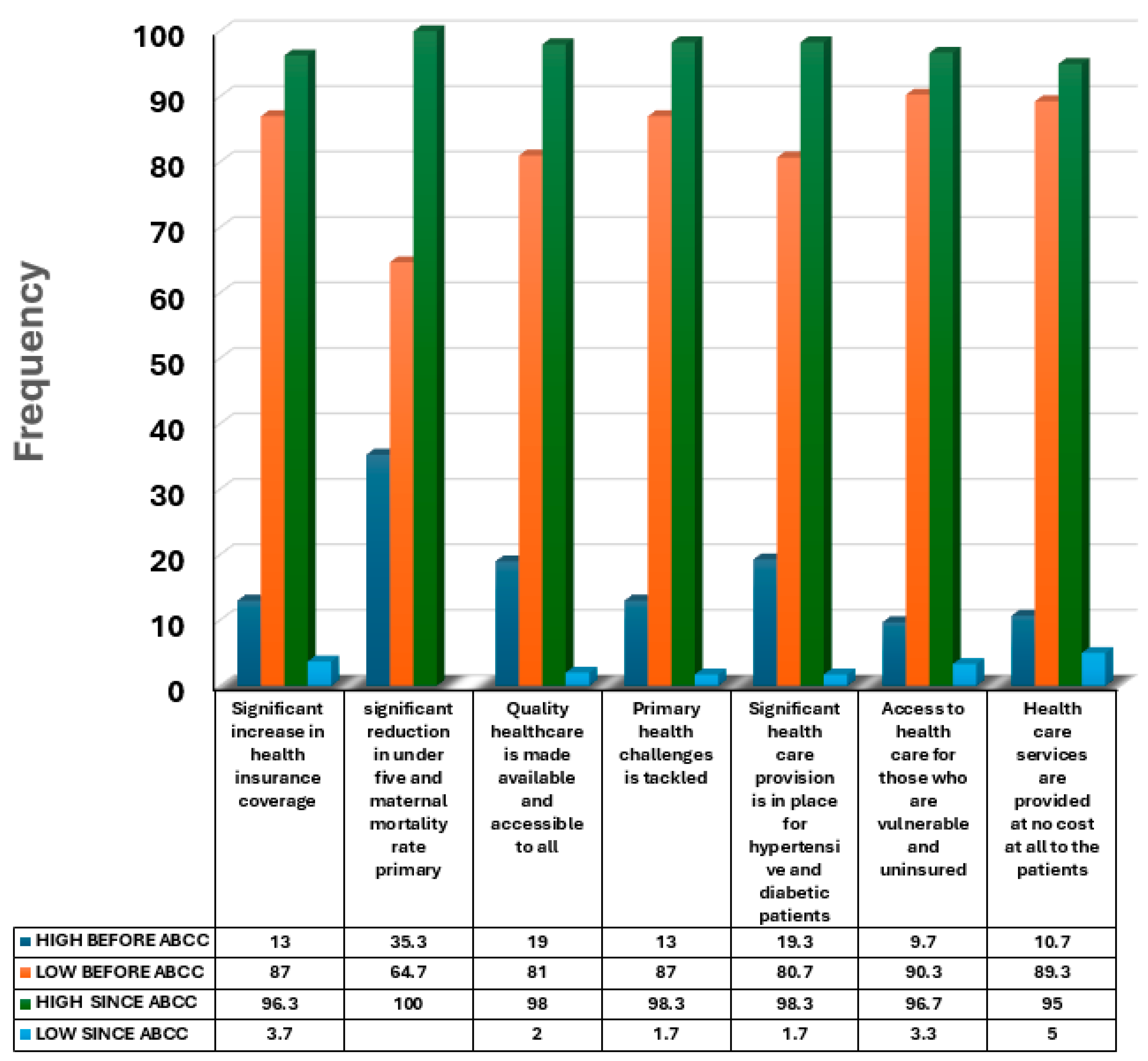
Figure 3.
Perception of Hindrances to Quality-of-Service Delivery, (a) before introduction, (b) since the introduction.
Figure 3.
Perception of Hindrances to Quality-of-Service Delivery, (a) before introduction, (b) since the introduction.
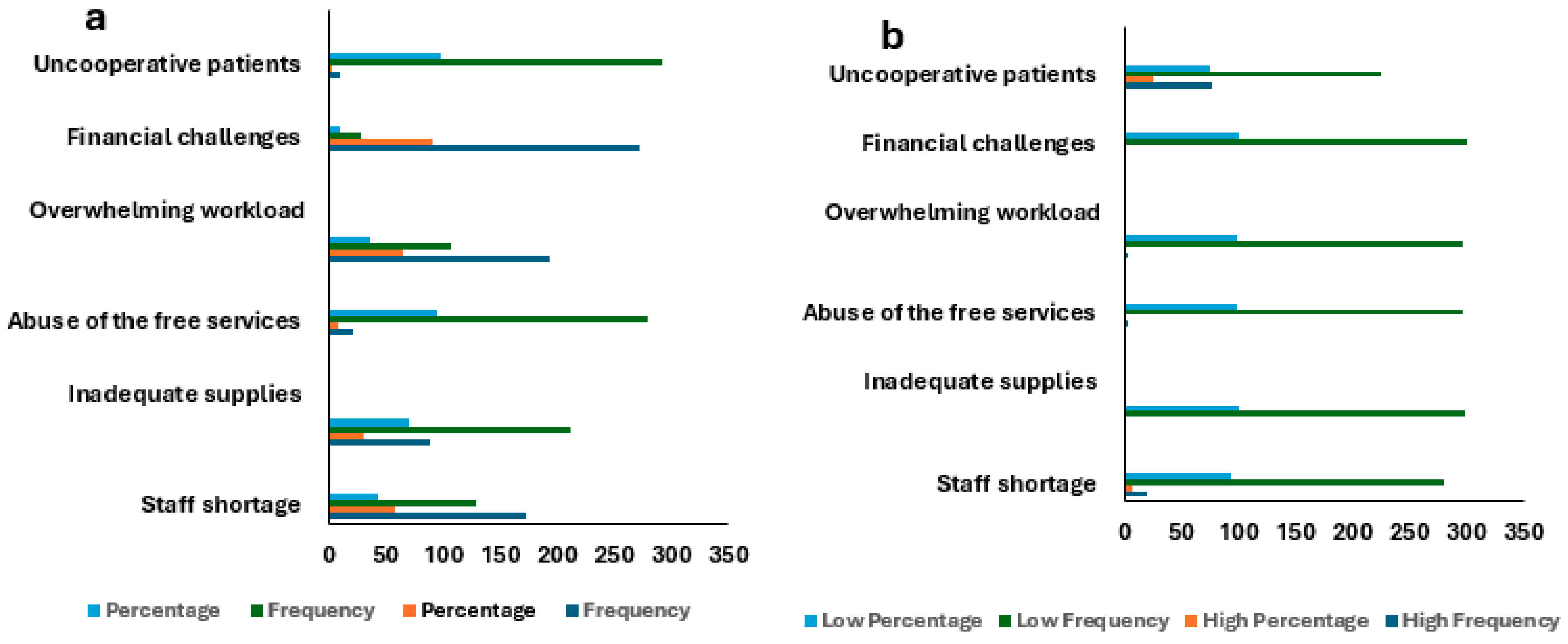

Table 1.
Perception of the Impact Before the Introduction Of ABCC.
| Factors | High | Low | ||
| Frequency | Percentage | Frequency | Percentage | |
| Significant increase in health insurance coverage | 39 | 13.0 | 261 | 87.0 |
| significant reduction in under five and maternal mortality rate | 106 | 35.3 | 194 | 64.7 |
| Quality healthcare is made available and accessible to all | 57 | 19.0 | 243 | 81.0 |
| Primary health challenges is tackled | 39 | 13.0 | 261 | 87.0 |
| Significant health care provision is in place for hypertensive and diabetic patients | 58 | 19.3 | 242 | 80.7 |
| Access to health care for those who are vulnerable and uninsured | 29 | 9.7 | 271 | 90.3 |
| Health care services are provided at no cost at all to the patients | 32 | 10.7 | 268 | 89.3 |
Table 2.
Perception of the Impact Since the Introduction of ABCC.
| Factor | High | Low | ||
| Frequency | Percentage | Frequency | Percentage | |
| Significant increase in health insurance coverage | 289 | 96.3 | 11 | 3.7 |
| significant reduction in under five and material mortality rate primary | 300 | 100.0 | ||
| Quality healthcare is made available and accessible to all | 294 | 98.0 | 6 | 2.0 |
| Primary health challenges is tackled | 295 | 98.3 | 5 | 1.7 |
| Significant health care provision is in place for hypertensive and diabetic patients | 295 | 98.3 | 5 | 1.7 |
| Access to health care for those who are vulnerable and uninsured | 290 | 96.7 | 10 | 3.3 |
| Health care services are provided at no cost at all to the patients | 285 | 95.0 | 15 | 5.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



