
Submitted:
28 May 2025
Posted:
29 May 2025
You are already at the latest version
Abstract
Background: Drug-resistant epilepsy remains a major therapeutic challenge, especially in preventing the progression of focal seizures to bilateral tonic-clonic seizures (BTCS). Previous studies demonstrated that exogenous rhythmic stimulation at 1.13 Hz syn-chronized with wrist tapping enhances prefrontal cortex activity in epilepsy patients. Methods: We conducted a randomized controlled study involving 60 adult patients with drug-resistant structural focal epilepsy (SFE). Participants were assigned to either an in-tervention group (n = 30), using the EpiTapp™ smartphone application during aura and/or focal onset of BTCS in out-of-hospital settings, or a control group (n = 30) receiving standard care. The study lasted six months. Primary outcomes were BTCS frequency and quality of life measured by the QOLIE-31 scale. Results: Use of EpiTapp™ significantly reduced BTCS frequency by interrupting seizure progression at the focal onset stage. Additionally, 22.6% of patients in the intervention group reported improved quality of life after six months. Conclusions: Exogenous rhythmic stimulation via the EpiTapp™ ap-plication is a promising non-invasive intervention for preventing seizure generalization in patients with drug-resistant structural focal epilepsy. Larger-scale studies are warranted to confirm these findings.
Keywords:
epilepsy
; exogenous rhythmic stimulation
; drug-resistant focal epilepsy
; EpiTapp® application
; quality of life
; non-pharmacological treatment
; wrist tapping
; epileptic seizure prevention
1. Introduction
Epilepsy is a disabling group of central nervous system disorders that are not always fully controllable and often accompany patients throughout their lives. Therefore, improving the quality of life for patients with epilepsy remains a priority. Epileptologists worldwide strive to alleviate the condition of these patients and help them adapt to living with the disease [1,2]. Consequently, the search for new, accessible, and non-invasive treatment methods remains highly relevant and important [3,4,5,6]. It is well established that epileptogenesis involves an imbalance between two systems: epileptic and antiepileptic. The brain’s antiepileptic system has been extensively studied and described in the works of Professor V. A. Karlov [7,8,9]. One key component of this system is the prefrontal cortex. In numerous animal experiments involving the formation of an epileptogenic focus, stimulation of the prefrontal cortex slowed epileptogenesis, whereas its removal accelerated epileptogenesis and increased the risk of death during status epilepticus onset [10]. This brain region also contains the so-called “metronome,” which is responsible for the perception and tracking of internal time [11,12,13,14]. It is known that the individual minute serves as a widely accepted marker of the functional state of the central nervous system [15], reflecting its adaptive mechanisms and responding sensitively to pathological changes, with well-defined normative ranges. In our previous studies of the individual minute in healthy adults and epilepsy patients, we observed that patients with epilepsy exhibit a distortion in the perception of internal time. Specifically, their individual minute is shortened to 49.77 seconds (compared to the normative 55–65 seconds), and their wrist tapping reproduces this internal rhythm at an accelerated rate of 2.54 Hz, compared to the normal 1.13 Hz observed in healthy adults [16,17,18]. It can be hypothesized that these changes result from disruption of the prefrontal cortex “metronome” due to decreased activity in the context of drug-resistant epilepsy. The alterations in internal time perception we observed led to the formulation of a scientific hypothesis: that exogenous rhythmic stimulation can modulate the brain’s bioelectrical activity to interrupt epileptic seizures at the focal onset stage. Coherence analysis of EEG is a well-established neurophysiological method to objectively assess activation in different brain regions. Bowyer S. M. [19] summarized data on using coherence to measure and quantify synchronous brain oscillations in various pathological conditions, including epilepsy, Alzheimer’s disease, schizophrenia, panic attacks, and autism spectrum disorders. An increase in coherence within a brain region reliably indicates increased activity, whereas a decrease suggests reduced activity. Studies have also reported a significant increase in interhemispheric coherence in the prefrontal cortex in patients with drug-induced epilepsy remission. Conversely, decreased coherence in this area has been observed in patients with uncontrolled seizures [20,21,22]. Guided by these findings, we previously investigated the effect of exogenous rhythmic stimulation, delivered via hand tapping at 1.13 Hz (the normal frequency for healthy adults) using the EpiTapp® application, on brain bioelectrical activity through EEG coherence analysis. Our prior study included 111 participants—51 healthy volunteers and 60 epilepsy patients. We observed a statistically significant increase in interhemispheric coherence in the frontal and prefrontal regions in epilepsy patients following exogenous phonostimulation via hand tapping. This suggests activation of these areas and, consequently, a strengthening of the brain’s antiepileptic system [23]. Epileptogenesis is known to involve the formation of a pathological dominant—a sharply increased excitatory focus in the central nervous system that can establish a pathological network [24]. The mechanism underlying the effective impact of exogenous rhythmic stimulation on brain bioelectrical activity can be explained by the replacement of the pathological dominant of the epileptic system with a new, stronger physiological dominant. Similar principles underpin various therapeutic methods such as music therapy, art therapy, aromatherapy, and acupuncture; however, the efficacy of these approaches is often subjective and lacks robust scientific evidence [25,26,27,28,29,30]. We propose that weakening the pathological dominant can be achieved by applying exogenous rhythmic stimulation at the “correct” healthy frequency, reproduced via hand tapping. A literature review revealed a broad range of applications for tempo-rhythm methods in the diagnosis and treatment of diverse diseases [31]. According to Coppola et al., structured auditory stimuli provide non-invasive excitatory cortical stimulation, which can reduce epileptiform activity [32]. Of particular interest are studies investigating the anticonvulsant effects observed in epilepsy patients exposed to the music of W. A. Mozart, specifically Sonata K.448. A portion of this sonata is played at an Andante tempo ranging from 76 to 108 beats per minute, corresponding approximately to 1–2 Hz. Notably, altering the tempo abolishes the therapeutic effect [33,34,35]. A randomized study involving both children and adult epilepsy patients demonstrated that 85% of participants responded positively to Mozart’s music, with an average reduction in epileptiform activity of 31% during listening and 24% post-listening [36,37]. These findings collectively suggest a beneficial influence of tempo and rhythm on the brain’s bioelectrical activity.
The present study focuses on the clinical application of a novel noninvasive approach utilizing exogenous rhythmic stimulation through wrist tapping at the onset of a focal epileptic seizure. The stimulation frequency replicates the average individual rhythm of a healthy adult, recorded in the individual minute mode, and is set at 1.13 Hz. The primary aim of this method is to interrupt bilateral epileptic seizures at the focal onset stage.
2. Materials and Methods
We have developed a novel approach based on the possibility of modulating the structure and frequency of epileptic seizures using the proprietary “Method of Influencing the Individual Rhythm through Exogenous Rhythmic Stimulation” [Russian Federation Patent No. 2015111025, dated October 20, 2017]. This method is implemented via the EpiTapp® application for Android-based mobile devices. From our perspective, the ability of patients to promptly use the application at the earliest signs of an impending epileptic seizure is critically important. This study presents an analysis of the clinical evaluation of exogenous rhythmic stimulation, delivered synchronously through wrist tapping at a frequency of 1.13 Hz using the EpiTapp® application. The total observation period was six months. A total of 60 participants were randomized into two groups: the main group included 30 patients with drug-resistant structural focal epilepsy (SFE). In addition to their regular antiepileptic therapy, patients in this subgroup regularly used the EpiTapp® method as an urgent self-care tool at the onset of seizure prodromes. The median age in this group was 33.5 years [interquartile range: 29.0; 40.0] (Table 1).
Additionally, 30 patients with pharmacoresistant structural focal epilepsy (SFE) comprised the control group. These patients did not use the EpiTapp® application but continued their previously prescribed antiepileptic therapy. The median age in this group was 39.5 years [interquartile range: 31.0; 49.0] (Table 2).
Inclusion criteria for study participants (patients with structural focal epilepsy) were: diagnosis of drug-resistant structural focal epilepsy; age between 21 and 60 years; signed informed consent; both male and female patients. Exclusion criteria included: refusal to participate; presence of acute or chronic neurological, psychiatric, or endocrinological disorders at the time of the study; non-epileptic seizures; seizure frequency fewer than 2 bilateral tonic-clonic seizures (BTCS) per month; seizures occurring exclusively during sleep; subtherapeutic or toxic levels of antiepileptic drugs (AEDs) in the blood; age below 21 or above 60 years; severe cognitive impairment (Frontal Assessment Battery (FAB) score <12; Mini-Mental State Examination (MMSE) score <20); and presence of anxiety or depression at the time of the study (Hospital Anxiety and Depression Scale (HADS) score >11 on the anxiety subscale or >7 on the depression subscale). The groups were comparable in terms of gender (p > 0.05), age (p > 0.05), underlying pathology (p > 0.05), localization of the structural lesion in the dominant (left) hemisphere (p > 0.05), and average monthly frequency of BTCS (p > 0.05).
The study was conducted in two stages (visits), as illustrated in Figure 1.
2.1. Description of the EpiTapp® Application Based on the Principle of Exogenous Rhythmic Stimulation.
During the clinical trial phase at Visit 1, patients with drug-resistant structural focal epilepsy were trained by their treating physicians to use the EpiTapp® application as a first-line emergency self-help tool for seizure precursors (aura) and/or focal epileptic seizures with or without partial impairment of awareness (Figure 2).
The epileptic seizure was interrupted at the focal onset stage by the patient synchronizing wrist taps on the screen of a mobile device in time with an exogenous rhythm set at 1.13 Hz—the average rhythm of a healthy individual—using the EpiTapp® application. Anticipating seizure generalization, the patient initiated the application by tapping its icon on the touchscreen of a smartphone, tablet, or laptop, a feature designed for ease of use, particularly for working patients ( Figure 3). Upon activation, the EpiTapp® application launched automatically.
Statistical Analysis: Descriptive statistics for categorical variables are presented as absolute values, percentages, and their standard errors. The null hypothesis was tested using the chi-square test. Data distribution was assessed by the Shapiro–Wilk test. For comparison of parametric data (normally distributed variables) between groups, Student’s t-test and Fisher’s test were used. Non-parametric paired data are presented as medians with interquartile ranges (Me [Q1; Q3]) and compared using the Wilcoxon signed-rank test. Confidence intervals (95% CI) were calculated to characterize expected variation. Statistical analyses were performed using STATISTICA v.7.0 (StatSoft, USA) and SPSS 22.0 software. All analyses and interpretations were conducted in accordance with current international standards for reporting statistical results in scientific publications.
3. RESULTS
3.1. Analysis of Seizure Diaries to Determine Monthly Frequency of Bilateral Tonic-Clonic Seizures in the Main and Control Groups.
During the 6-month observation period, the main group of patients with structural focal epilepsy (SFE) demonstrated a significant reduction in the monthly number of bilateral tonic-clonic seizures (BTCS). At study inclusion (Visit 1), the total number of BTCS across the group was 82 per month, which decreased to 5 seizures per month after 6 months of using the EpiTapp® application (Visit 2). The median monthly number of BTCS after 6 months was 0 [0; 1], compared to 2 [2; 3] before application use, with this difference reaching statistical significance (p < 0.05). A detailed analysis of seizure diary data at Visits 1 and 2 for the main subgroup is presented in Table 3.
In a comparative analysis of seizure observation diaries from patients in the control subgroup (Table 4), no statistically significant difference was observed in the mean number of bilateral tonic-clonic seizures (BTCS) between Visit 1 and Visit 2, during which patients received only antiepileptic drug therapy. The average number of BTCS was 3.83 ± 2.66 at Visit 1 and 3.93 ± 2.92 at Visit 2 (p > 0.05). The total number of BTCS per month in the control group was 86 at Visit 1 and 88 at Visit 2, also showing no statistically significant change (p > 0.05).
3.2. Quality of Life Outcomes in the Main and Control Groups over a 6-Month Observation Period
Patient-reported outcomes confirmed the safety of the method: individuals with structural focal epilepsy (SFE) who regularly used the EpiTapp® application rated its safety at 100%.
3.2.1. QOLIE-31 Questionnaire Results in the Main Group
According to the QOLIE-31 questionnaire (Figure 4), regular use of the EpiTapp® application over the 6-month observation period resulted in a 22.6% improvement in overall quality of life among patients with epilepsy. The most significant improvements (p < 0.001) were observed in domains related to social and emotional well-being, reduction in anxiety about potential seizure recurrence, and patients’ subjective assessment of quality of life with epilepsy.
Overall, the observed positive dynamics in quality of life among patients with epilepsy, as measured by the QOLIE-31 scale, suggest the potential effectiveness of the EpiTapp® application in patients with drug-resistant structural focal epilepsy (SFE).
3.2.2. QOLIE-31 Questionnaire Results in the Control Group
In contrast, patients in the control group demonstrated negative dynamics on the QOLIE-31 scale over the 6-month observation period (Figure 5), indicating a decline in perceived quality of life in the absence of additional non-pharmacological intervention.
The low quality-of-life scores reported by patients with drug-resistant structural focal epilepsy are, unsurprisingly, primarily linked to persistent anxiety and fear associated with the anticipation of another potentially traumatic seizure, as well as the perceived inability to prevent it. In this context, the use of a non-pharmacological neuromodulatory approach—reproducible exogenous rhythmic stimulation delivered through the EpiTapp® mobile application—emerges as a reliable and accessible tool for urgent self-help in patients with treatment-resistant epilepsy.
4. Discussion
Thus, this study aimed to evaluate the efficacy and safety of a novel approach in epileptology—exogenous rhythmic phonostimulation with rhythm reproduction via wrist tapping—to interrupt epileptic seizures at the stage of focal onset. The stimulation frequency used in our intervention (1.13 Hz) was based on normative values derived from prior research, corresponding to the individual rhythm of healthy adults. The high efficacy in preventing bilateral tonic-clonic seizures, along with the 100% safety profile observed in the study group, suggests a strong potential for broader clinical application. We also consider it a promising area for further research, particularly in optimizing stimulation parameters for different epilepsy subtypes. A key prerequisite for successful use of exogenous rhythmic stimulation is the presence of a focal seizure onset lasting at least 10 seconds, during which the patient’s awareness remains fully preserved. This is essential for timely activation of the application and execution of synchronized wrist tapping. Accordingly, contraindications for this method include generalized seizures without a focal onset, focal seizures with impaired awareness, and phonosensitivity. The method may also be unsuitable for patients with clinically significant anxiety disorders or psychogenic non-epileptic seizures, as these conditions were part of the exclusion criteria in our study. Limitations of the current research include the relatively small sample size and the absence of EEG monitoring during application use. However, future studies are planned to address these limitations.
5. Conclusions
Therefore, we consider the continued investigation of exogenous rhythmic stimulation in other forms of epilepsy, accompanied by simultaneous EEG monitoring, to be a promising and clinically significant research direction.
Author Contributions
Conceptualization, E. Narodova; methods, E. Narodova and S. Prokopenko; software, E. Erakhtin; validation – E. Narodova, V. Narodova, A. Narodov; formal analysis, A. Narodov; investigation, E. Narodova, E. Erakhtin; resources, E. Erakhtin and A. Narodov; data curation, S. Prokopenko; writing — original draft preparation, E. Narodova and V. Narodova; writing — review and editing, S. Prokopenko, E. Narodova, V. Narodova; visualization, E. Erakhtin; supervision, S. Prokopenko; project leaders S. Prokopenko, E. Narodova, V. Narodova. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Professor V.F. Voyno-Yasenetsky, Krasnoyarsk State Medical University (protocol No. 77/2017 dated June 26, 2017).
Informed Consent Statement
Informed consent was obtained from all subjects participating in the study.
Data Availability Statement
Data are available upon request due to ethical and medical confidentiality restrictions.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| SFE | Structural focal epilepsy |
| BTCS | Bilateral tonic-clonic seizures |
| QOLIE-31 | Quality of Life in Epilepsy- 31 |
| AEDs | Antiepileptic Drugs |
| HADS | The Hospital Anxiety and Depression Scale |
| MMSE | The Mini-Mental State Examination |
| FAB | Fullerton Advanced Balance scale |
References
- Christensen, J.; Trabjerg, B.B.; Wagner, R.G.; Newton, C.R.; Kwon, C.S.; Aaberg, K.M.; …; Dreier, J.W. Prevalence of epilepsy: a population-based cohort study in Denmark with comparison to Global Burden of Disease (GBD) prevalence estimates. J. Neurol. Neurosurg. Psychiatry 2025, 96(5), 480–488.
- Massi, D.G.; Feudjio, R.; Eyoum, C.; Paternoster, L.; Magnerou, A.M.; Ferreira, N.T.; …; Mapoure, N.Y. Prevalence of depression in people with epilepsy: A hospital-based study in Cameroon. Epilepsy Behav. 2025, 165, 110326.
- Jiao, D.; Xu, L.; Gu, Z.; Yan, H.; Shen, D.; Gu, X. Pathogenesis, diagnosis, and treatment of epilepsy: electromagnetic stimulation–mediated neuromodulation therapy and new technologies. Neural Regen. Res. 2025, 20(4), 917–935. [CrossRef]
- Tseng, P.T.; Zeng, B.Y.; Hsu, C.W.; Liang, C.S.; Carvalho, A.F.; Brunoni, A.R.; …; Li, C.T. The non-invasive brain or nerve stimulation treatment did not increase seizure frequency in patients with epilepsy: A network meta-analysis. Epilepsy Behav. 2025, 164, 110290. [CrossRef]
- Narodova, E.A.; Shnayder, N.A.; Narodova, V.V.; Dmitrenko, D.V.; Artyukhov, I.P. The role of non-drug treatment methods in the management of epilepsy. Int. J. Biomedicine 2018, 8(1), 9–14. [CrossRef]
- Alipour, M.; Abdolmaleki, M.; Shabanpour, Y.; Zali, A.; Ashrafi, F.; Nohesara, S.; Hajipour-Verdom, B. Advances in magnetic field approaches for non-invasive targeting neuromodulation. Front. Hum. Neurosci. 2025, 19, 1489940. [CrossRef]
- Karlov, V.A. The doctrine of the epileptic system. The merit of the domestic scientific school. Epilepsy Paroxysmal States 2017, 4(9), 76–85.
- Rahimi-Dehkordi, N.; Heidari-Soureshjani, S.; Rostamian, S. A systematic review of the anti-seizure and antiepileptic effects and mechanisms of piperine. CNS Agents Med. Chem. 2025, 25(2), 143–156. [CrossRef]
- Shi, J.; Xie, J.; Li, Z.; He, X.; Wei, P.; Sander, J.W.; Zhao, G. The role of neuroinflammation and network anomalies in drug-resistant epilepsy. Neurosci. Bull. 2025, 1–25. [CrossRef]
- Karlov, V.A. Evolution of L.R. Zenkov. L.R. Zenkov and epilepsy as a model for studying the functional organization of the central nervous system. Epilepsy Paroxysmal Cond. 2018, 10(3), 79–86.
- Baruah, T.; Hegde, S. Impact of Rhythmic Auditory Stimulation on Neurocognition: Proposed Mechanism of Action of Rhythmic Auditory Stimulation on Neurocognitive Abilities. Preprints 2025, 2025041965. [CrossRef]
- Sharma, D.; Jain, V.K. A review of the multidimensional impact of music: psychological, educational and therapeutic perspectives. A Pratibha Spandan’s Journal 2025, 13(1), 1–7.
- Mehta, R.K.; Zhu, Y.; Weston, E.B.; Marras, W.S. Development of a neural efficiency metric to assess human-exoskeleton adaptations. Front. Robot. AI 2025, 12, 1541963. [CrossRef]
- Tsai, C.G.; Li, C.W. The Neural Basis of Groove Sensations: Implications for Music-Based Interventions and Dance Therapy in Parkinson’s Disease., arXiv 2025:2503.02500.
- Halberg, F.; Chibisov, S.M.; Radysh, I.V. Time structures (chronomes) in us and around us. PFUR 2005, 186.
- Narodova, E.A.; Rudnev, V.A.; Shnayder, N.A.; Narodova, V.V.; Erahtin, E.E.; Dmitrenko, D.V.; Shilkina, O.S.; Moskaleva, P.V.; Gazenkampf, K.A. Parameters of the Wrist Tapping using a Modification of the Original Method (Method of exogenous rhythmic stimulation influence on an individual human rhythm). Int. J. Biomedicine 2018, 8(2), 155–158. [CrossRef]
- Narodova, E.A.; Shnayder, N.A.; Narodova, V.V.; Erahtin, E.E.; Shilkina, O.S.; Moskaleva, P.V. Influence of anxiety on wrist tapping parameters and individual perception of one minute in healthy adults and patients with juvenile myoclonic epilepsy. Russ. Open Med. J. 2018, 7(4), 415. [CrossRef]
- Narodova, E.A.; Shnayder, N.A.; Karnauhov, V.E.; Bogomolova, O.D.; Petrov, K.V.; Narodova, V.V. Effect of Wrist Tapping on Interhemispheric Coherence in Patients with Juvenile Myoclonic Epilepsy. Int. J. Biomedicine 2021, 11(1), 73–77. [CrossRef]
- Jamal, W.; Das, S.; Maharatna, K.; et al. Brain connectivity analysis from EEG signals using stable phase-synchronized states during face perception tasks. Physica A 2015, 434, 273–295. [CrossRef]
- Morozova, M.A.; Blagosklonova, N.K. Intrahemispheric EEG coherence depending on clinical manifestations of temporal epilepsy in children. Hum. Physiol. 2007, 33(4), 18–23. [CrossRef]
- Miroshnikov, A. B., Formenov, A. D. Effect of a fidget spinner on the "individual minute" during monotonous work on cardio-training equipment. Therapist 2019, 1, 33–36.
- Feng, X.; Piper, R.J.; Prentice, F.; Clayden, J.D.; Baldeweg, T. Functional brain connectivity in children with focal epilepsy: a systematic review of functional MRI studies. Seizure 2024, 113, 1–10. [CrossRef]
- Marcantoni, I.; Piccolantonio, G.; Ghoushi, M.; Valenti, M.; Reversi, L.; Mariotti, F.; et al. Interhemispheric functional connectivity: an fMRI study in callosotomized patients. Front. Hum. Neurosci. 2024, 18, 1363098. [CrossRef]
- Ukhtomsky, A.A. Dominanta; Piter: St. Petersburg, Russia, 2002; p. 448.
- Trimble, M.R.; Hesdorffer, D.; Hećimović, H.; Osborne, N. Personalised music as a treatment for epilepsy. Epilepsy Behav. 2024, 156, 109829. [CrossRef]
- Gao, S.; Gong, Y.; Xu, C.; Chen, Z. The bidirectional role of music effect in epilepsy: Friend or foe? Epilepsia Open 2024, 9(6), 2112–2127. [CrossRef]
- Guo, X.; Wang, C.; Guo, J. The effect of Mozart’s K. 448 on epilepsy: A systematic literature review and supplementary research on music mechanism. Epilepsy Behav. 2025, 163, 110108.
- Walker, M.C. State-of-the-art gene therapy in epilepsy. Curr. Opin. Neurol. 2025, 38(2), 128–134. [CrossRef]
- Doțen, N. Psychological interventions in the care of people diagnosed with epilepsy. Studia Univ. Mold. Științ. Educ. 2024, 175(5), 212–218.
- Cai, D.C.; Chen, C.Y.; Lo, T.Y. Foot reflexology: recent research trends and prospects. Healthcare 2022, 11(1), 9. [CrossRef]
- Rafiee, M.M.; Istasy, T.A.; Valiante, M. Music in epilepsy: Predicting the effects of the unpredictable. Epilepsy Behav. 2021, 122, 108164. [CrossRef]
- Coppola, G.; Toro, A.; Operto, F.F.; et al. Mozart’s music in children with drug-refractory epileptic encephalopathies. Epilepsy Behav. 2015, 50, 18–22. [CrossRef]
- Marzbani, H.; Marateb, H.R.; Mansourian, M. Neurofeedback: a comprehensive review on system design, methodology and clinical applications. Basic Clin. Neurosci. 2016, 7(2), 143–158. [CrossRef]
- Sesso, G.; Sicca, F. Safe and sound: Meta-analyzing the Mozart effect on epilepsy. Clin. Neurophysiol. 2020, 131(7), 1610–1620. [CrossRef]
- Van Bree, S.; Sohoglu, E.; Davis, M.H.; et al. Sustained neural rhythms reveal endogenous oscillations supporting speech perception. PLoS Biol. 2021, 19(2), e3001142. [CrossRef]
- Niebrzydowska, A.; Grabowski, J.; Niebrzydowska, A. Medication-induced psychotic disorder. A review of selected drugs side effects. Psychiatr. Danub. 2022, 34(1), 11–18. [CrossRef]
- Shnayder, N.A.; Narodova, E.A.; Narodova, V.V.; et al. The role of nondrug treatment methods in the management of epilepsy. In Epilepsy: Advances in Diagnosis and Therapy; Al-Zwaini, I.J., Majeed Albadri, B.A.H., Eds.; IntechOpen: London, UK, 2018. Available online: https://www.intechopen.com/books/epilepsy-advances-in-diagnosis-and-therapy/the-role-of-nondrug-treatment-methods-in-the-management-of-epileps (accessed on 27 May 2025).
Figure 1.
Study design.
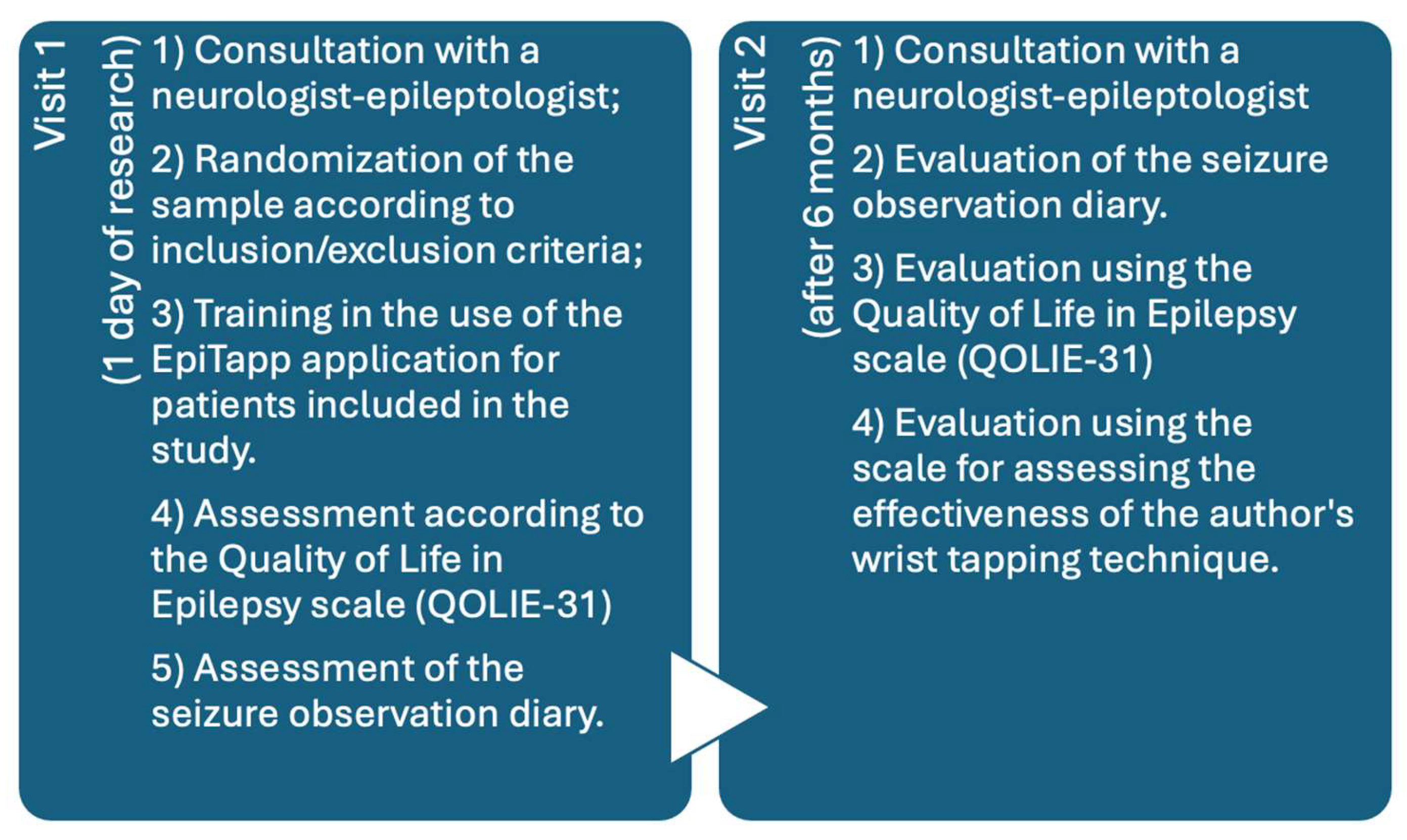
Figure 2.
Outpatient use of the EpiTapp® application. (a) The patient develops a focal onset of a bilateral tonic-clonic seizure. (b, c) In typical cases, bilateral transformation into a generalized tonic-clonic seizure occurs. (d) The patient launches the EpiTapp® application on a mobile device. (e) The patient synchronizes wrist tapping with an exogenous rhythm of 1.13 Hz provided by the application. (f) Seizure generalization is prevented, and the patient returns to normal activity.
Figure 2.
Outpatient use of the EpiTapp® application. (a) The patient develops a focal onset of a bilateral tonic-clonic seizure. (b, c) In typical cases, bilateral transformation into a generalized tonic-clonic seizure occurs. (d) The patient launches the EpiTapp® application on a mobile device. (e) The patient synchronizes wrist tapping with an exogenous rhythm of 1.13 Hz provided by the application. (f) Seizure generalization is prevented, and the patient returns to normal activity.
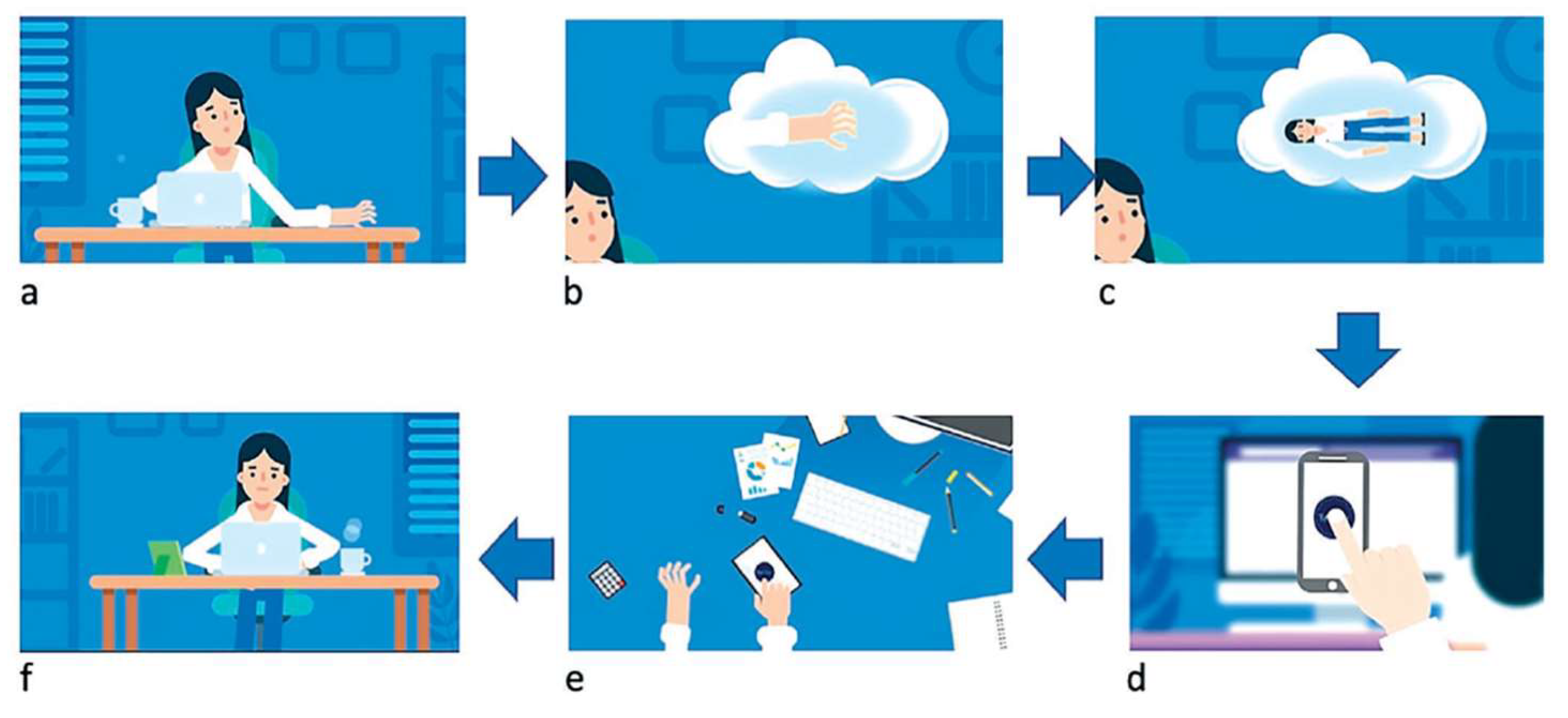
Figure 3.
Demonstration of patient use of the EpiTapp® application.
Figure 4.
Subjective assessment of quality of life in patients of the main group using the QOLIE-31 scale at Visit 1 and Visit 2.
Figure 4.
Subjective assessment of quality of life in patients of the main group using the QOLIE-31 scale at Visit 1 and Visit 2.
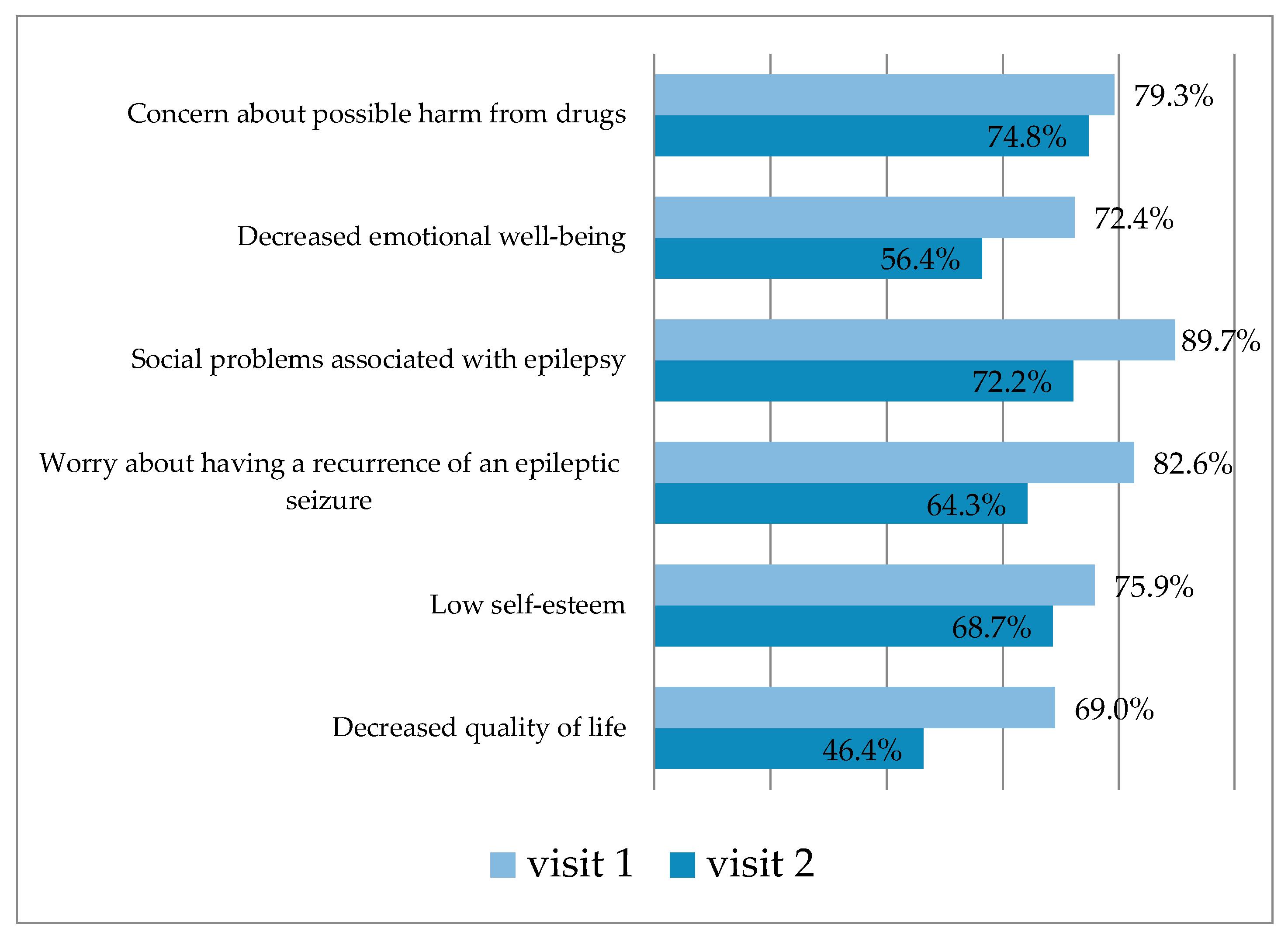
Figure 5.
Subjective assessment of quality of life in patients of the control group using the QOLIE-31 scale at Visit 1 and Visit 2.
Figure 5.
Subjective assessment of quality of life in patients of the control group using the QOLIE-31 scale at Visit 1 and Visit 2.
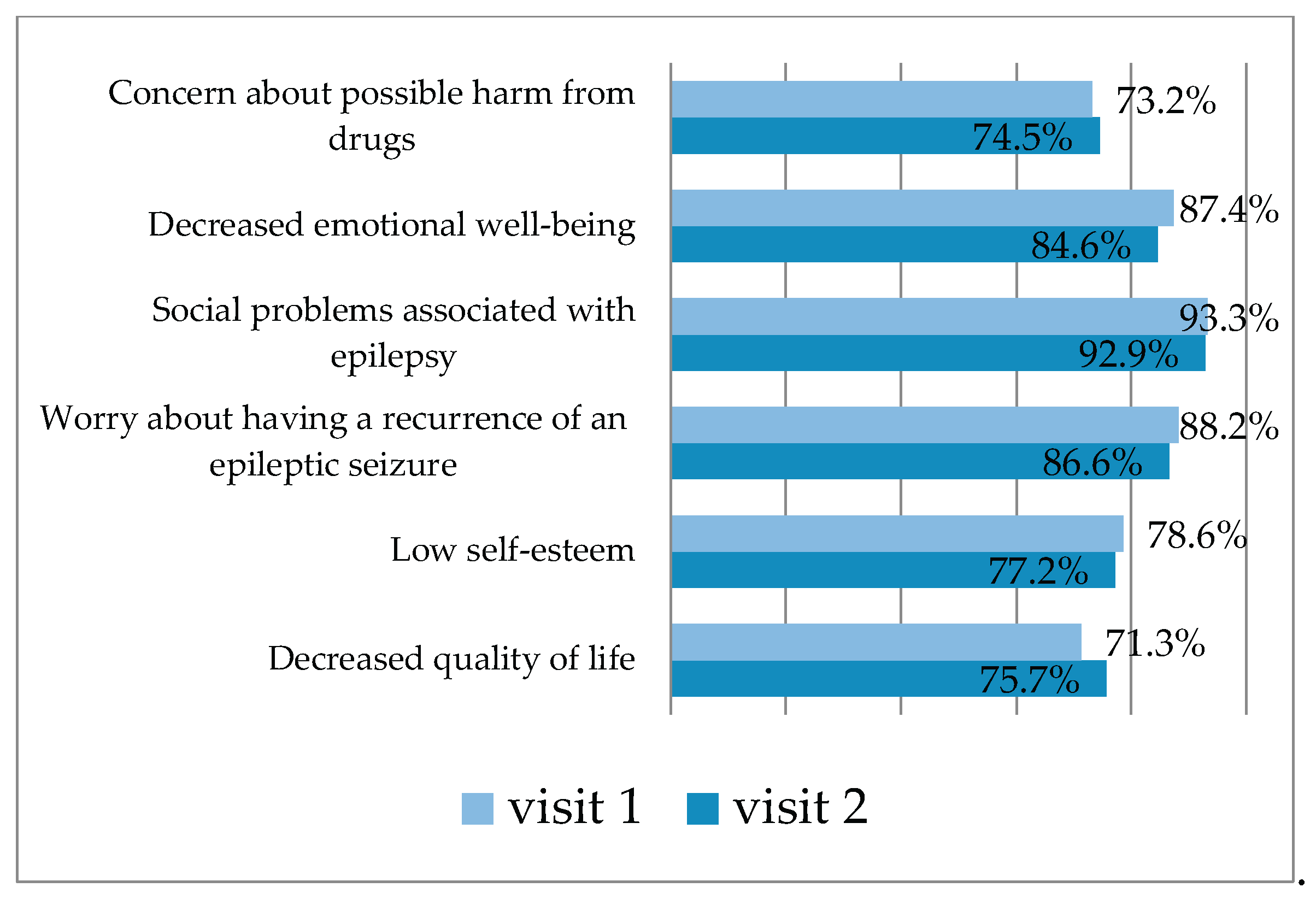

Table 1.
General characteristics of patients in the main group with drug-resistant structural focal epilepsy (n = 30).
Table 1.
General characteristics of patients in the main group with drug-resistant structural focal epilepsy (n = 30).
| Group parameters | Me [P25; P75] |
| Age of patients, years | 33,5 [30,0; 40,0] |
| Duration of epilepsy, years | 7,5 [6,0; 9,0] |
| Average age of epilepsy onset, years | 35 [29,0; 40,0] |
| Number of BTCS*, per month | 3 [2; 4] |
*BTCS - bilateral tonic-clonic seizures.
Table 2.
General characteristics of patients in the control group with drug-resistant structural focal epilepsy (n = 30).
Table 2.
General characteristics of patients in the control group with drug-resistant structural focal epilepsy (n = 30).
| Group parameters | Me [P25; P75] |
| Age of patients, years | 39,5 [31,0; 49,0] |
| Duration of epilepsy, years | 6 [5,0; 8,5] |
| Average age of epilepsy onset, years | 31,5 [27,0; 40,0] |
| Number of BTCS*, per month | 4 [2; 6] |
*BTCS - bilateral tonic-clonic seizures.
Table 3.
Analysis of seizure observation diaries in patients of the main group at Visit 1 and Visit 2.
Table 3.
Analysis of seizure observation diaries in patients of the main group at Visit 1 and Visit 2.
| Type of epileptic seizures | Me [P25; Р75] | *р |
|---|---|---|
| BTCS (visit 1) | 2 [2; 3] | 0,000003 |
| BTCS (visit 2) | 0 [0; 1] |
* – according to the Wilcoxon test.
Table 4.
Analysis of seizure observation diaries in patients of the control group at Visit 1 and Visit 2.
Table 4.
Analysis of seizure observation diaries in patients of the control group at Visit 1 and Visit 2.
| Type of epileptic seizures | Me [P25; Р75] | *р |
|---|---|---|
| BTCS (visit 1) | 3 [2; 6] | 0,62 |
| BTCS (visit 2) | 3 [1; 6] |
* – according to the Wilcoxon test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



