
Submitted:
23 May 2025
Posted:
23 May 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and long COVID are two post-viral diseases, which share many common symptoms and pathophysiological alterations. Yet a mechanistic explanation of disease induction and maintenance is lacking. This hinders the discovery and implementation of biomarkers and treatment options, and ultimately the establishment of effective clinical resolution. Here, we propose that acute viral infection results in (in)direct endothelial dysfunction and senescence, which at the blood-brain barrier, cerebral arteries, gastrointestinal tract, and skeletal muscle can explain symptoms. The endothelial senescence-associated secretory phenotype (SASP) is proinflammatory, pro-oxidative, procoagulant, primed for vasoconstriction, and characterized by impaired regulation of tissue repair, but also leads to dysregulated inflammatory processes. Immune abnormalities in ME/CFS and long COVID can account for the persistence of endothelial senescence long past the acute infection by preventing their clearance, thereby providing a mechanism for the chronic nature of ME/CFS and long COVID. The systemic and tissue-specific effects of endothelial senescence can thus explain the multisystem involvement in and subtypes of ME/CFS and long COVID, including dysregulated blood flow and perfusion deficits. This can occur in all tissues, but especially the brain as evidenced by findings of reduced cerebral blood flow and impaired perfusion of various brain regions, post-exertional malaise (PEM), gastrointestinal disturbances, and fatigue. Paramount to this theory is the affected endothelium, and the bidirectional sustainment of immune abnormalities and endothelial senescence. The recognition of endothelial cell dysfunction and senescence as a core element in the aetiology of both ME/CFS and Long COVID should aid in the establishment of effective biomarkers and treatment regimens.
Keywords:
virus-Induced endothelial senescence
; Long COVID
; ME/CSF
1. Introduction
Post-viral disease is an umbrella term used to describe a range of conditions that occur after viral infection, with long COVID and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) being the most studied. These diseases are characterized by a variety of symptoms that most commonly include unresolved fatigue, post-exertional malaise (PEM), cognitive dysfunction and brain fog, orthostatic intolerance, autonomic dysfunction, gastrointestinal disturbances, myalgia, neuralgia, sensory sensitivities, and others [1,2]. Importantly, these symptoms persist long after acute infection.
The incidence of ME/CFS has increased over recent years [3] as a result of the COVID-19 pandemic, specifically due to the fact that a subset of patients who contract SARS-CoV-2 develop long-lasting symptoms, referred to as long COVID, that meet the diagnostic criteria for ME/CFS [4,5,6], and as such, SARS-CoV-2 viral infection is a trigger for ME/CFS [7,8]. A meta-analysis suggested that 51% of patients with long COVID meet the diagnostic criteria for ME/CFS [9]. Adding to the growing challenge of post-viral diseases is the fact that there are neither official mechanistic explanations for long COVID and ME/CFS, nor established diagnostic biomarkers and effective treatments. Elucidating the pathophysiological complexities associated with long COVID, ME/CFS, and other post-viral diseases is of paramount importance for clinical advancement in the field. From this, it is likely that effective diagnostic techniques and therapeutic strategies will result.
There are a number of proposed hypotheses to explain the induction and maintenance of ME/CFS and long COVID, some involving the central nervous system [10,11,12], the vasculature [13,14,15,16,17,18,19], viral persistence [20,21,22,23], immune dysregulation [24], autoantibody generation [16,25], and the (neuro)endocrine system [26,27]. Anomalous clotting processes, characterized by the formation of heterogeneous (amyloid) deposits referred to as fibrinaloid complexes (microclots) and platelet dysregulation [28,29], are features of both long COVID and ME/CFS [19,30,31,32,33,34,35]. It has, however, proven difficult to decipher cause and effect in this regard. In particular, the vascular component of long COVID and ME/CFS pathology has received much attention in recent years, especially due to the haematological and vascular consequences of SARS-CoV-2 infection, as well as the virus’ predilection for endothelial cells [36]. There is extensive evidence pointing to endothelial dysfunction in both long COVID [37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52] and ME/CFS [18,40,53,54,55,56,57,58,59,60]. Consequentially, many hypotheses regarding the pathogenesis of ME/CFS and long COVID are centred around endothelial cell dysfunction, often along with downstream consequences of other systems [14,15,16,46,61,62,63,64,65]. Blood flow dynamics are perturbed in both long COVID and ME/CFS cohorts, with major findings revolving around reduced cerebral blood flow [66,67,68] and reduced perfusion of certain brain regions and organs [69,70,71,72,73].
Here, we present further evidence of the endothelium being a primary site of disease induction and maintenance, through a process of endothelial senescence. With this, we discuss a novel hypothesis that can explain the multisystem and chronic nature of ME/CFS and long COVID. We review the evidence of endothelial senescence as the functional culprit of ME/CFS and long COVID. Furthermore, we provide a link between acute infection and the induction of ME/CFS and long COVID, and between vasculature-related disease mechanisms and immune dysfunction that are typically observed in long COVID and ME/CFS.
Senescence and Associated Mechanisms
Cellular senescence is one of the hallmark of aging, and describes a state of stable cell cycle arrest combined with other molecular, morphological, and metabolic changes. The response of cells to enter a senescence programme occurs following persistent and unresolved stress leading to cellular damage and dysregulation [74]. This can be due to replicative exhaustion, called replicative senescence, in which continuous shortening of the telomeres towards a critically short length signals for chronic activation of the DNA damage response and activation of cell cycle arrest pathways [75,76]. Other senescence triggers, such as hyperactivation of oncogenes (e.g. Ras), drive oncogene-induced senescence [77]; such programmes have likely evolved as a cell-intrinsic mechanism to suppress cell proliferation and tumour formation [78]. Radiation, radiomimetic drugs, genotoxins, or reactive oxygen species (ROS) can all lead to excessive DNA damage, driving DNA damage-induced senescence [79]. Induction of senescence through viral infection is a more recent phenomenon which clearly plays a role in the pathology of several viral diseases.
Although there is no single unique biomarker of senescence, senescent cells can be detected by their presentation of a panel of senescence-associated features. Exit from the cell cycle is identified by the high expression of cyclin kinase inhibitors, CDKN1A and CDKN2A, encoding p21 and p16 respectively, which establish and maintain cell cycle arrest [80]. Senescent cells exhibit profound nuclear alterations including persistent DNA damage which are distinct from acute DNA lesions, termed DNA-SCARS (DNA Segments with Chromatin Alterations Reinforcing Senescence [81]), chromatin changes (termed senescence-associated heterochromatin foci, SAHFs [82]), and loss of nuclear membrane integrity underpinned by decreased lamin B1 expression, leading to cytoplasmic chromatin fragments (CCFs) [83]. Senescent cells exhibit strong upregulation of anti-apoptotic pathways [84], which explains their resistance towards programmed cell death despite their high levels of internal cellular damage.
Organelle dysfunction is also highly apparent in senescent cells, and includes disrupted mitochondrial ATP production [85] and lysosomal hypertrophy [86]. Mitochondrial dysfunction of senescent cells has been demonstrated to be essential for their hypersecretory phenotype, known collectively as the senescence-associated secretory phenotype (SASP) [87,88]. The high lysosomal load of senescent cells leads to high levels of the lysosomal enzyme, β-galactosidase, even at suboptimal pH 6.0 [89,90].
The SASP encapsulates a pro-inflammatory and tissue-remodelling secretome [88], though its exact components depends on the cell type, mode of senescence induction (e.g. replicative, DNA damage, oncogene-induced), and stage of senescence (e.g. early, middle, or late) [91]. This phenotype is highly immunogenic (containing, for example, interleukin (IL)-6, IL-8, and tumour necrosis factor (TNF)-α)); thus, senescent cells attract immune cells, such as CD8+ T cells, natural killer cells, and neutrophils, to coordinate their removal [92,93,94]. Hence, senescence is a physiological state that evolved to aid tumour cell removal and tissue remodelling [78]. Additionally, the SASP drives paracrine senescence of local cells, which may provide another tumour-suppressive mechanism that restricts cancerous transformation [95].
Senescence and virus infection are bidirectional and hence self-reinforcing processes, whereby viral infection can drive senescence, and senescence predisposes to further viral infection. Vascular endothelial senescence is apparent in lung autopsy samples from patients with severe COVID-19 [96] and is likely involved in the pathophysiology of COVID-19. For example, replicative senescent endothelial cells are especially susceptible to SARS-CoV-2 infection compared to non-senescent cells [97]. Importantly, SARS-CoV-2 viral proteins degrade host cell components of the DNA damage response, ablating the cell’s DNA repair capacity and driving cell senescence [98]. Cultured media from virus-induced senescent fibroblasts can induce senescence in human endothelial cells, highlighting an important role of bystander or paracrine senescence after virus infection through the SASP [99]. Viruses therefore likely evolved to exploit the senescence programme to exacerbate their propagation across tissues. For example, the SASP of irradiation-induced senescent endothelial cells increases expression of viral entry proteins, ACE2 and TMPRSS2, in SARS-CoV-2-permissive human lung epithelial cells, an effect which can be blocked with a neutralising anti-IL1α antibody [100]. Moreover, treatment with senolytic drugs that remove senescent cells by targeting their anti-apoptotic pathways improved mouse survival from coronavirus infections, thus underscoring the importance of senescent cells in driving acute disease pathology [99,100,101].
Endothelial Senescence as an Explanation for the Induction and Maintenance ME/CFS and Long COVID
Recently, we discussed the role of a dysregulated endothelium and vasculature in explaining ME/CFS symptoms, and how herpesvirus infection can drive vascular dysfunction [63]. Latent endothelial cell infection might be sufficient to induce symptoms associated with ME/CFS, and particularly its organ-specificity is an important factor for symptom manifestation.
While there is currently no causative proof of this hypothesis, here we present an expanded role of viral infections in promoting chronic endothelial dysfunction and senescence. We propose that viral infection results in direct and indirect endothelial modulation resulting in long-term endothelial senescence. These senescent endothelial cells can persist for months to years after the acute infection, sustained by a dysfunctional immune system (discussed later; Figure 1).
The burden and organ-location of endothelial senescence seems crucial; for example, senescent endothelial cells within specific arteries (e.g. carotid and vertebral arteries) can explain reduced cerebral blood flow (and other perfusion deficits) observed in patients due to their impaired regulation of the vasculature in response to perfusion requirements, which can subsequently cause neurological symptoms as a result of impaired oxygenation, glucose supply, and waste clearance; senescent endothelial cells of the blood-brain barrier (BBB) can also inform the neurological symptoms associated with ME/CFS and long COVID; senescent endothelial cells that reside by skeletal muscle and the consequences of impaired perfusion might be able to explain bioenergetic disturbances in myocytes, observed myopathies, exercise-intolerance, and PEM; a senescent endothelium in the gastrointestinal tract will lead to impaired barrier function, gut dysbiosis, and potentially microbial translocation into circulation and other tissues [62,102]. Indeed, senescent endothelial cells and other vascular cells, in particular, have the potential to cause systemic physiological dysfunction [103]. This pathology has the potential to explain the persistence of pathological mechanisms (Figure 1), such as vascular dysregulation and perturbed blood flow, immune recruitment and dysregulation, persistent clotting pathology, platelet dysregulation, increased intestinal permeability, and impaired blood-brain barrier function, as well as the persistence of symptoms and the multisystem nature of ME/CFS and long COVID.
It is necessary to ascertain whether the viruses implicated in ME/CFS and long COVID, including SARS-CoV-2, EBV, HHV-6, influenza A virus, enteroviruses, parvovirus B19, and potentially others, are capable of infecting endothelial cells and causing endothelial dysfunction. Indeed, these viruses do have the ability to infect endothelial cells (Table 1). Importantly, SARS-CoV-2 and influenza A virus can induce endothelial senescence [51,96,99,104,105,106]. The other viruses can induce senescence in other cell types [107,108,109]. These results indicate that the aforementioned viruses can indeed infect endothelial cells, although more studies are required to assess the potential of these viruses, in addition to SARS-CoV-2 and influenza A, in inducing endothelial senescence, specifically.
With regards to SARS-CoV-2, increased levels of chitotriosidase and stathmin 1 were found in plasma samples from hospitalised COVID-19 patients 3 months after infection [110], which are suggestive of the induction of cellular senescence [111]. Indications of T-cell senescence have also been observed in long COVID patients [112] and COVID-19 survivors [113]. There is a clinical trial recruiting patients for the investigation of senescent cells (cell type not specified) and their secretome in long COVID patients (NCT ID: NCT04903132).
Direct viral infection of endothelial cells is not a prerequisite for senescence induction, as inflammatory cues and oxidative stress, as well as some specific molecules, such as endothelin-1 (ET-1), SARS-CoV-2 spike protein, leukocyte microparticles, angiotensin II, homocysteine, cytokines, and others [105,122,170,171,172,173,174], have the potential to induce endothelial senescence. Hence, induction of post-viral diseases might be independent of endothelial cell viral infection.
Sfera et al (2021) published hypotheses involving gastrointestinal-associated endothelial senescence as an important pathological component of ME/CFS and long COVID pathology [62,175]. These studies focussed on the intestinal barrier, where endothelial senescence enables the subsequent translocation of microorganisms and inflammagens (such as LPS) into circulation and tissues, including skeletal muscle and central nervous system, which can then give rise to pathology. Although the present hypothesis encompasses the systemic endothelium, as well as tissue-specific sites such as arteries, neurovasculature, and skeletal muscle, and not only the gastrointestinal tract, Sfera et al offered mechanistic reasoning for the induction of endothelial senescence via SAR-CoV-2-induced upregulation of angiotensin II [175].
Endothelial Senescence-Associated Secretory Phenotype (SASP) in ME/CFS and Long COVID
The consequences of endothelial senescence [176] in a micro- and macrovascular context have been reviewed [177], with a specific focus on their proinflammatory, pro-oxidant, procoagulant, and vasoconstrictor effects [178]. Endothelial senescence is characterized by a specific profile of expressed and secreted molecules, the endothelial SASP (Figure 2). This is characterized by: an increase in proinflammatory cytokines including IL-1β, IL-6 [179], and tumour necrosis factor-α (TNF-α); an increase in procoagulant factors including tissue factor (TF) [180], plasminogen-activator inhibitor-1 (PAI-1) [181,182], and von Willebrand factor (vWF) [183]; a dysregulation of vasomodulators including reduced nitric oxide (NO) and increased endothelins [184,185,186]; an increase in adhesion molecules including intercellular adhesion molecule-1 (ICAM-1) [186], vascular cell adhesion molecule-1 (VCAM-1), and fibronectin [182]; an increase in chemokines including monocyte-chemoattractant protein-1 (MCP-1)/C-C motif ligand 2 (CCL2), MCP-2, IL-8/chemokine (C-X-C motif) ligand 8 (CXCL8) [179]; an increase in growth factors including vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF), platelet-derived growth factor (PDGF), transforming growth factor-β (TGF-β); and an increase in ROS production [176,187,188,189,190,191].
Specific endothelial markers that can be indicative of their senescence have been shown to be increased in ME/CFS and long COVID cohorts, including ET-1 [40,42,45,58,59,192,193], VEGF-A [194], VCAM-1 [59,192], ICAM-1 [45,195], PAI-1 [59], IL-8 [45], MCP-1 [45], and FGF-2 [194]. Elevated levels of ET-1 in long COVID, but also during acute COVID-19 [196,197,198], are known to induce endothelial senescence [170,176]. A variety of other molecules or processes (e.g. inflammation, oxidative stress, signalling molecules, intracellular cues, etc.) can also induce endothelial senescence independent of ET-1 [190,191,199]. In conclusion, there is experimental evidence suggestive of endothelial senescence in long COVID and ME/CFS, and that many of these upregulated molecules, such as ET-1, are in turn capable of inducing endothelial senescence. Further investigation into burden of senescence endothelial cells and the SASP in long COVID and ME/CFS is thus warranted.
Senescent Endothelial Cells and Vascular Dysfunction
Hypotheses and inferences regarding perfusion deficits and vascular abnormalities in ME/CFS and long COVID are based upon the evidence of predominant manifestation of vasoconstriction, enhanced sympathetic activity, and perturbed blood flow and perfusion [14,15,66,67,68,69,200,201,202]. We suggest that endothelial senescence (and potentially the dysfunction and senescence of other vascular cells, including smooth muscle cells) contributes to these mechanisms and symptoms.
The SASP associated with senescent endothelial cells is a profile, in the context of vascular regulation, that favours the effects of vasoconstriction [176,177,203]. Indeed, perfusion deficits and vascular abnormalities in ME/CFS and long COVID are often related to vasoconstriction and enhanced sympathetic activity [14,15,66,67,68,69,200,201,202]. An increase in ET-1 and a concurrent decrease in NO, particularly due to a reduced eNOS activity, is associated with the SASP [185]. These phenomena have consequences for the regulation of blood flow and hence provides a mechanistic link between endothelial senescence and the reduced cerebral blood flow underlying orthostatic intolerance in long COVID [68,201] and ME/CFS [66,67,72] (Figure 1).
Senescent endothelial cells exhibit phenotypic changes and increased adhesive properties to the basement membrane which impact haemodynamics [204], and also display increased permeability caused by compromised barrier integrity [205,206,207]. The endothelial SASP is associated with age-related arterial dysfunction and stiffness [177,208], and hence can explain blood flow perturbations and perfusion deficits observed in blood vessels of patients, e.g. the carotid and vertebral arteries [209]. There are also signs of cardiac abnormalities and inefficiencies in ME/CFS and long COVID [210,211,212], which can be explained, in part, by endothelial senescence [176].
Since endothelial senescence affects both systemic and microcirculation [176,177], it raises the question of whether impaired blood flow regulation and subsequent perfusion deficits can contribute to the multisystem involvement observed in ME/CFS and long COVID, as well as the manifestation of non-specific symptoms. Vascular abnormalities, including blood flow disturbances and perfusion deficits, may help explain symptoms across various physiological systems, accounting for both specific and non-specific symptoms [14,15]. For instance, this systemic dysregulation of blood flow, along with other pathological effects of endothelial senescence, could contribute to the persistent, unresolved fatigue (and exercise intolerance) experienced by patients. Relevantly, there is an association between endothelial dysfunction and (cognitive) fatigue [213].
Proinflammatory Component of the Endothelial SASP and Immune Dysfunction, Exhaustion, & Senescence – A Possible Explanation for the Maintenance of Endothelial Senescence in ME/CFS and Long COVID
The SASP of senescent endothelial cells recruits and activates immune cells via the expression of cytokines, chemokines, and adhesion molecules [214,215]. These processes, along with impaired barrier function and increased permeability [207,216], may lead to immune dysregulation and tissue infiltration of immune cells [217]. Senescent endothelial cells promote immune exhaustion and senescence [218], which is also implicated in patients with ME/CFS and long COVID [28,219,220]. However, senescence of leukocytes likely also occurs independently of senescent endothelial cells during SARS-CoV-2 infection [221].
In acute COVID-19, there are various studies reporting indications of immune exhaustion and immunosenescence in patients [222,223,224,225], as well as in long COVID [112,226]. While it is unknown whether immunosenescence occurs in patients with ME/CFS [227], there are indications of immune exhaustion [28,227]. The idea that senescent immune cells can give rise to the myriad symptoms associated with ME/CFS and long COVID is unconvincing, but that is not to say that immune deficits are negligible in ME/CFS and long COVID pathology – it is plausible that such immune deficits sustain the primary pathology of ME/CFS and long COVID. In the context of the present hypothesis, these immune deficits might sustain endothelial senescence.
Natural killer (NK) cells are involved in clearing senescent cells [228,229], but their cytotoxicity is reduced in patients with ME/CFS [230,231]. Neutrophil extracellular traps (NETs) implicated in long COVID [232,233], which are released from activated neutrophils in response to senescent endothelial cells, can aid in endothelial remodelling [234] and are also structurally associated with heterogeneous fibrinaloid microclots [235]. Along with NK cells and neutrophils, macrophages and T-cells can also eliminate senescent cells [229]. Macrophages and CD8+ T-cells also exhibit functional deficits in ME/CFS and long COVID and correlate with symptoms [28,236,237,238,239]. Furthermore, the complement system aids in removal of senescent cells [240], and complement dysfunction is implicated in the pathophysiology of ME/CFS [18,241,242] and long COVID [243]. Lastly, dysfunctional immune cells are also capable of inducing endothelial senescence [244], and endothelial cells can function to clear defective and senescent leukocytes [245]. The evidence of immune exhaustion in ME/CFS and long COVID and immune senescence in long COVID, together with endothelial senescence, can explain the myriad symptoms and chronicity of ME/CFS and long COVID.
Considering the role of natural killer cells, neutrophils, T-cells, macrophages, and the complement system in clearing senescent endothelial cells, the impaired function of these immune cells and systems in ME/CFS [239,246] and long COVID [247,248] offer an explanation for the maintenance of endothelial senescence, linking it bidirectionally with immune dysfunction, i.e. endothelial senescence induces immune dysfunction, and dysfunctional immune cells enable the sustainment of endothelial senescence long past the acute infection. Additionally, senescent fibroblasts evade immune responses by expressing the major histocompatibility complex molecule HLA-E, which normally inhibits NK cell and CD8+ T-cell responses via engagement of the immune inhibitory natural killer group 2A (NKG2A) receptor, thereby preventing leukocyte cytotoxicity and hindering the removal of senescent cells [94]. Indeed, it has been shown that irradiation-induced senescent endothelial cells also express HLA-E, which enables their evasion of NK cell cytotoxicity [249]. Hence, this provides another mechanism by which senescent endothelial cells may persist and can direct future experiments investigating this hypothesis (Figure 3).
Senescence of Brain Microvascular Endothelial Cells and Neurological Symptoms
Brain microvascular endothelial cells (BMECs) form the essential and highly selective blood-brain barrier (BBB), which plays a crucial role in maintaining homeostasis of the central nervous system. However, senescent BMECs may contribute to age-related dysfunction and the breakdown of the BBB [250,251], potentially leading to neurovascular issues and thus cognitive impairment, as well as an increased risk of neurological disorders [252]. Senescent BMECs show signs of loss of barrier integrity and increased permeability [205,206], as well as perturbed mitochondrial function and overall cellular bioenergetics [253]. They also impair the regulation of microglia and can result in dysregulated inflammatory sequelae in the central nervous system [254].
Using SARS-CoV-2 as an example again, this virus has the ability to directly infect BMECs [255,256,257] and hence supports the current hypothesis and notion of BMEC senescence as a result of acute viral infection. Additionally, there is evidence of herpesvirus infection of BMECs [128] and infection of the central nervous system in ME/CFS [130], as well as evidence of BMEC infection by enterovirus [151,154,258] and influenza A virus [259,260]. Senescence of BMECs and the local and systemic ramifications that ensue can explain cognitive impairment and other neurological issues associated with ME/CFS and long COVID – indeed, many recent studies have shown that endothelial senescence can bring about cognitive dysfunction [203,233,261,262]. To add, peripheral endothelial senescence has been shown to have an impact on BBB integrity and cognition [263] and hence neurological symptoms might also occur due to peripheral endothelial senescence. Interestingly, ET-1 – released by senescent endothelial cells and has been found to be upregulated in ME/CFS and long COVID (as discussed earlier) – is associated with cognitive dysfunction [264]. Hence, the effects of endothelial senescence impact not just blood flow regulation and tissue perfusion in the periphery, but also the central nervous system.
Importantly, disruption of BBB integrity and function has been demonstrated in long COVID cohorts [114,265,266] and have been included in several hypotheses for ME/CFS [11,60,200,267]. The proinflammatory profile of BMECs SASP [268] is one that supports various neuro-centred hypotheses of ME/CFS and long COVID [11,71,200,269], which encompass neuroinflammation, BBB disruption, and impaired perfusion, and seek to link such mechanisms to (neurological) symptoms. Hence, the neurovascular and neuroinflammatory mechanisms of ME/CFS and long COVID can be a result of endothelial senescence, thereby giving rise to cognitive deficits and other neurological symptoms.
The findings of herpesvirus RNA and protein in the central nervous system of ME/CFS patients [130] can be a reflection of both impaired immune function and impaired BBB integrity, with the latter brought about by senescence of BMECs. Mechanism-focused reviews on BMEC senescence and the consequences thereof for both neurological and peripheral function are published [203,233,251,261,263]. Of course, in light of reduced cerebral blood flow, senescence of BMECs might be secondary in the contribution to neurological symptoms in ME/CFS and long COVID. Perfusion deficits in various brain regions in ME/CFS and long COVID [70,72,270] might be a result of a local burden of senescent BMECs.
Endothelial Senescence and Gastrointestinal Symptoms
ME/CFS and long COVID cohorts demonstrate a variety of gastrointestinal disturbances and symptoms [271,272]. There is evidence of gut dysbiosis in ME/CFS [273,274,275] and long COVID [276,277], coupled to increased intestinal permeability and microbial translocation in both diseases [274,278,279]. Relevantly, several hypotheses of disease induction and maintenance are centred around gut integrity and microbiota [280,281,282,283].
Sfera et al have published on the role of endothelial senescence in a gastrointestinal context, and the subsequent ramifications for intestinal barrier integrity and of microbial (and LPS) translocation into circulation [62]; hence, the gastrointestinal aspect of this theory is not elaborated further here. U[284,285ltimately, endothelial senescence at the intestinal border can lead to loss of barrier integrity and increased gut permeability, subsequently enabling microbial translocation which can promote inflammation and tissue damage in the systemic vasculature and organs (Figure 1).
To add, there is evidence that gut dysbiosis and some microbial metabolites, such as trimethylamine-N-oxide and phenylacetic acid, can induce endothelial senescence and contribute to systemic vascular pathology in this context [284,285]; hence, the bidirectional consequences of endothelial senescence and gut dysbiosis are of interest in the context of the present hypothesis.
Senescence of Endothelial Cells and Post-Exertional Malaise
One of the more deliberating symptoms of patients with ME/CFS and long COVID is PEM, which is the worsening of symptoms or development of new symptoms in response to physical or psychological exertion. Unlike fatigue, this is typically a delayed reaction, but one that can last for hours or days. We argue here that the impact of physical exertion on a dysfunctional, maladaptive, and a specifically senescent endothelium is enough to induce a significant systemic response that gives rise to PEM.
The transition from rest to exercise demands a rapid and tightly coordinated increase in oxygen delivery in order to accommodate the increased metabolic demand of the working skeletal muscle tissue [286]. These increases in oxygen and nutrient delivery are accomplished by sympathetic signalling, increasing the cardiac output, breathing frequency, but also microvascular regulation, all promoting additional oxygen extraction from the blood [287]. Invasive cardio-pulmonary exercise testing in both ME/CFS and long COVID patients, however, has indicated a peripheral problem of impaired oxygen extraction during exercise, as cardiac and pulmonary function were less affected [288,289]. Malfunctioning endothelial cells may predispose to perturbations in efficient oxygen and nutrient exchange, especially upon exertion, affecting oxygen perfusion and diffusion and local tissue oxygenation. Also, by-products build up in skeletal muscle tissues causing cell acidification occurs following exertion. The insufficiency of a senescent endothelium to efficiently dispose of these exertion-induced waste products worsens exertion and local muscle pain. This skeletal muscle pathology is likely further exacerbated by the SASP-induced dysregulation of immune cells and inflammatory responses.
These dynamic perfusive responses are governed partly by the endothelium, which rapidly adjusts vascular tone through both mechanical and chemical cues. However, endothelial senescence may severely impair vasodilation, as the SASP is marked by a predominance of vasoconstrictors over vasodilators. The SASP is associated with an increased expression of ET-1, and reduced eNOS and NO expression. ET-1 is indeed significantly higher in ME/CFS [40,58,59,192] and long COVID [40,42,45,59,192,193] patients, along with some initial evidence of decreased NO expression and eNOS function in ME/CFS [56,286,290]. This vasomotor imbalance is especially harmful during exercise, as increased blood flow and the resulting shear stress should induce vasodilation to ensure proper tissue perfusion. This is further supported by the important role of ET-1 in regulating blood flow dynamics during exercise [291,292,293], as it is associated with lower oxygen consumption during exercise [294].
ET-1 also exerts direct effects on skeletal muscle cells and tissue. Beyond its previously addressed role as vasoconstrictor, ET-1 can also bind to the endothelin B receptor on myoblasts and hinder skeletal muscle myogenesis [295]. The same study also noted that ET-1 reduces the expression of MyoD, MyoG, and MyHC on cultured myoblasts and of MyHC in differentiated myotubes. Proinflammatory sequelae, including the expression of IL-6 and TNF-α, also ensue in myoblasts exposed to ET-1 [296]. Glucose uptake is impaired in skeletal muscle cells exposed to ET-1, via the inhibition of Akt [297]. In addition to ET-1 causing endothelial senescence, ET-1 can induce fibrosis (exemplified via the expression of fibronectin) in cultured myoblasts via ROS production and activation of the PI3K-AKT-GSK pathway [298]. Indeed, increased levels of fibronectin in ME/CFS and long COVID have been reported [299] as well as thickening of the capillary basement membranes in long COVID [300,301], with the latter emphasizing possible substance exchange issues. Together, these can help with explaining the pathophysiology of muscle-specific alterations in ME/CFS and long COVID.
PAI-1, another component of the endothelial SASP, can exert deleterious effects on skeletal muscle cells and tissue [302]. Most notably, it inhibits skeletal myogenesis and promotes fibrosis [302], ultimately compromising skeletal muscle regenerative capacity. Indeed, senescent endothelial cells are associated with myopathy in dystrophic skeletal muscle in mice [303]. Moreover, senescent markers (although not identified to be from endothelial cells) are upregulated in skeletal muscle tissue from patients with Duchenne muscular dystrophy [304].
Senescent endothelial cells exhibit an impaired healing ability which implicates vascular and surrounding tissues [176,268,305]. Although some components of the SASP, such as PDGF-AA, have been shown to be beneficial in tissue repair [187], this is in the context of injury and the subsequent acute response, and not from the perspective of virus-induced senescence and the persistence of senescent endothelial cells. Endothelial cells form part of the microenvironment from which satellite cells and myocytes receive constant signalling and hence regulation, and secrete growth factors, angiopoietin-1, and microRNAs that can activate or inhibit satellite cells [306,307,308]. How these cells communicate with each other, and how exercise worsens this inter-cellular communication, is currently unknown.
In conclusion, a senescent endothelium will impair nutrient delivery to and waste removal from skeletal muscle tissue. Senescent endothelial cells and their consequences on local blood flow, perfusion, and immune function are not conducive to effective tissue supply and waste removal, and tissue remodelling and repair [17]; hence these factors can lead to pathological insult upon exertion and impaired muscle regeneration (Figure 4). These effects can result in an delayed recovery response upon exercise and an exaggerated intolerance to a second exercise insult if conducted in close succession to the first, i.e. the second exercise intervention will result in impairments greater than those observed in the first exercise intervention – this is reflected in consecutive exercise regimens involving cardiopulmonary exercise tests in ME/CFS [309,310].
Procoagulant Factors of Senescent Endothelial Cells and Prolonged Coagulation Abnormalities
Abnormal clotting, including heterogeneous fibrinaloid microclots and dysregulated platelets, are major features of long COVID and ME/CFS. Heterogeneous fibrinaloid microclots can be induced by minuscule amounts of suitable trigger molecules [311,312,313,314]. We have previously noted increased levels of heterogeneous microclots, dysregulated platelets, abnormal clotting kinetics [19,35], along with dysregulated coagulation and endothelial markers [18]. Other groups have also found dysregulated platelets in ME/CFS cohorts [32,315,316]. Furthermore, with the evidence of a dysfunctional endothelium in ME/CFS and long COVID, an impairment in the regulation of coagulation is expected.
Senescent endothelial cells and their proinflammatory SASP prompt thrombotic processes [317] by cytokine- and chemokine-mediated recruitment of platelets which can lead to dysregulated clot formation and platelet levels [318,319,320,321], and by releasing procoagulant factors such as TF [180,321] and vWF [183]. Silva et al (2017) inferred that the release of TF was dependent on NAPH-oxidase- and cyclooxygenase 2-induced oxidative stress, and also demonstrated that such procoagulant activity in senescent endothelial cells was blunted with NAPDH oxidase and cyclooxygenase 2 inhibitors [321]. Furthermore, PAI-1 – expressed as part of the endothelial SASP [181,322] – can help to explain the persistence of heterogeneous fibrinaloid microclots and other clotting abnormalities in patients, as elevations in PAI-1 leads to a reduction in activated plasmin and therefore a reduction in fibrinolysis.
It has also been shown that atherosclerotic plaque-derived microparticles induce endothelial senescence in cultured endothelial cells, and promote the expression of tissue factor and procoagulant microparticles, as well as a reduced expression of NO via the downregulation of eNOS [323]. In ME/CFS, plasma from ME/CFS patients downregulates NO expression in healthy endothelial cells [290], highlighting the role of plasma-derived substances and extracellular vesicles in altering vascular function and offering a target for therapy. The link between endothelial senescence and thrombosis has been discussed [324,325].
It is unknown if dysfunctional and/or senescent endothelial cells (and possibly the extracellular vesicles that they secrete [326,327]) are the primary inducers of heterogeneous fibrinaloid microclots. Microclots are heterogeneous aggregations in blood that stain positive with thioflavin T, an amyloid dye, and are composed of fibrin(ogen) and other plasma and intracellular proteins [202,328]. It is hypothesized that extracellular vesicles, apoptotic bodies, and cellular debris can also induce microclot formation [329,330]; if this is true, the increased load of heterogeneous microclots in long COVID might be explained by immune deficits which hinder clearance of cell debris and related particles in circulation. Additionally, these immune deficits can also explain the persistence of heterogeneous microclots, as leukocytes (as well as proteolytic mechanisms) are to be responsible for microclot clearance (Figure 5). Senescent cells have been associated with amyloid pathology [331], and amyloid aggregates are capable of inducing cellular senescence [332,333]. While it has been shown that microclot induction can occur in the presence of bacterial inflammagens and SARS-CoV-2 spike protein [311,312,313,314,334], other in vivo mechanisms – such as (senescent) endothelial-derived vesicle induction of platelet aggregation and subsequent anomalous clotting processes [335], activation of neutrophils and NETosis, accumulation of cellular debris and extracellular vesicles due to impaired immune function, and other potential mechanisms which will not be discussed here – need to be further investigated to explain the induction and persistence of these heterogeneous microclots. Since the endothelium plays a pivotal role in regulating coagulation, these links can guide future experiments investigating the induction of and the various phenotypes representative of the total population of heterogeneous microclots.
Senescent Endothelial Cells and the Relation to Herpesviruses
There is a substantial amount of evidence implicating the herpesviridae EBV and HHV-6 in ME/CFS [20,129,130] and long COVID [336,337]. Previously, we proposed that herpesviruses, specifically EBV and HHV-6, can infect and cause dysfunction in endothelial cells, causing symptoms associated with ME/CFS and long COVID [63].
Here, induction of senescence as a result of herpesvirus infection can occur in non-immune cells [338] and is specifically proposed to occur in endothelial cells (and also via indirect mechanisms). This would then lead to subsequent viral latency and cellular dysfunction that can contribute to pathophysiological mechanisms and symptoms, especially when clearance of these cells is implicated by a dysfunctional immune system and immune evasion strategies of viruses. We also recognize the importance of host susceptibility to such a pathological cycle induced by acute viral infection, but this is normally not known.
Herpesviridae are well known to be able to lie latent or dormant for many decades [339]. Thus, as well as direct infection, immune alterations and endothelial senescence induced by the acute infection that initiated PVD may lead to herpesvirus reactivation. This may also be true for other infections and overall immunity.
Future Considerations
Confirming the details of the mechanisms proposed here (Figure 6) in vivo will require the detection and quantification of cell-specific senescence (e.g. endothelial senescence) in patients, and these are still being developed [340,341]. The measurement of senescence-associated biomarkers in biological samples (e.g. urine, plasma, etc.) is likely insufficient to corroborate – specifically – endothelial senescence as a cause and driving factor of ME/CFS and long COVID, although, as discussed, many plasma markers in patients are suggestive of a senescent endothelium.
What might offer valuable information are biopsies of both small and large vessels and subsequent immunohistochemistry and imaging processing of tissues [342]. A study by Veroutis et al (2024) performed temporal artery biopsies and subsequently identified and quantified endothelial cell senescence in vascular tissue, establishing a senescence specific signature that can be used to study endothelial senescence in a neurological context [343]. A similar approach can be implemented to investigate the hypothesis of endothelial senescence as a cause and driving factor for neurological pathology and symptom manifestation. Advancements in senescence-imaging of musculoskeletal tissue can inform the investigation of endothelial senescence in muscle tissue and its relation to fatigue, exercise intolerance, and PEM. Other system-specific investigations can be carried out in this manner, e.g. the gastrointestinal vasculature.
Senotherapeutics are a new class of drugs and natural products that consist of two members: senomorphics and senolytics [344]. Senolytics selectively clear senescent cells [345,346], while senomorphics are compounds that modulate their behaviour. If, as we argue here, endothelial senescence is central to ME/CFS and Long COVID, then it is reasonable that senotherapeutics and related treatments [341] might offer therapeutic benefit to ME/CFS and long COVID patients. Indeed, some have been shown to aid in COVID-19 disease severity and ameliorate neuropathology associated with SARS-CoV-2 infection [100,101,347]. Given the more general value of carefully chosen combinations of natural products in these diseases, it seems that a trawl among relevant natural products acting as senolytics or senomorphics might be worthwhile. In a similar vein, further studies are required to assess the burden of cellular senescence in ME/CFS and long COVID, and specifically the senescent burden of the endothelium and vasculature.
Conclusions
ME/CFS and long COVID are the two most studied post-viral diseases, yet an official mechanistic explanation of disease induction and maintenance is lacking. Here, we offer a detailed mechanistic explanation involving the endothelium, immune system, and senescence. We propose that acute viral infection can result in direct and indirect modulation of endothelial cells that can lead to endothelial dysfunction and, in particular, that this dysfunction is represented by senescence. Supporting this theory is the known ability of SARS-CoV-2 to cause endothelial senescence. Immune deficits are prominent characteristics of ME/CFS and long COVID pathology, with notable deficits in leukocyte and complement function; furthermore, endothelial senescence can itself give rise to immune deficits, leading to amplification. We propose that these deficits sustain endothelial senescence by ineffectively clearing senescent endothelial cells. This, along with the expression of HLA-E by senescent endothelial cells and the consequential evasion of the immune system, can explain the chronicity of ME/CFS and long COVID pathology.
We suggest that this systems analysis can effectively link immune dysfunction with the continuing symptoms associated with ME/CFS and long COVID, and can explain the multisystemic nature of these conditions. Importantly, the hypothesis presented here might be extended to include the senescence of other vascular cells, such as smooth muscle cells, endothelial progenitor cells, and leukocytes. However, endothelial cells are here proposed to be the most significant cell type implicated due to their important physiological roles and capability to cause local and systemic pathology that can result in symptom manifestation (Figure 6). On this basis, senotherapeutics would be seen to have the potential to provide a novel and valuable treatment strategy. Additionally, the idea of endothelial senescence as the primary point of pathology in ME/CFS and long COVID can account for why previous clinical trials without the implementation of senotherapeutics and related drugs failed to bring about significant amelioration.
Author Contributions
J.M.N.: Wrote and conceptualized the paper. E.P.: Edited the paper, funding, co-corresponding author; study leader; R.C.I.W., A.S., D.B.K., L.K.: contributed to paper writing and editing, and B.F.: edited the paper. All authors have read and agreed to the published this version of the manuscript.
Funding
J.M.N. thanks Kanro Foundation, E.P. thanks PolyBio Research Foundation, Balvi Foundation and Kanro Foundation for funding, D.B.K. thanks the Balvi Foundation (grant 18) and the Novo Nordisk Foundation for funding (grant NNF20CC0035580). The content and findings reported and illustrated are the sole deduction, view and responsibility of the researchers and do not reflect the official position and sentiments of the funders. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgements
J.M.N. thanks Kanro Foundation, E.P. thanks PolyBio Research Foundation, Balvi Foundation and Kanro Foundation for funding, D.B.K. thanks the Balvi Foundation (grant 18) and the Novo Nordisk Foundation for funding (grant NNF20CC0035580). The content and findings reported and illustrated are the sole deduction, view and responsibility of the researchers and do not reflect the official position and sentiments of the funders. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Komaroff, A.L. and W.I. Lipkin, ME/CFS and Long COVID share similar symptoms and biological abnormalities: road map to the literature. Frontiers in Medicine, 2023. 10.
- Al-Aly, Z. and E. Topol, Solving the puzzle of Long Covid. Science, 2024. 383(6685): p. 830-832.
- Mirin, A.A., M. E. Dimmock, and L.A. Jason, Updated ME/CFS prevalence estimates reflecting post-COVID increases and associated economic costs and funding implications. Fatigue: Biomedicine, Health & Behavior, 2022. 10(2): p. 83-93.
- Reuken, P.A. , et al., Longterm course of neuropsychological symptoms and ME/CFS after SARS-CoV-2-infection: a prospective registry study. European Archives of Psychiatry and Clinical Neuroscience, 2024. 274(8): p. 1903-1910.
- Morita, S. , et al., Phase-dependent trends in the prevalence of myalgic encephalomyelitis / chronic fatigue syndrome (ME/CFS) related to long COVID: A criteria-based retrospective study in Japan. PLOS ONE, 2024. 19(12): p. e0315385.
- Ryabkova, V.A. , et al., Similar Patterns of Dysautonomia in Myalgic Encephalomyelitis/Chronic Fatigue and Post-COVID-19 Syndromes. Pathophysiology, 2024. 31(1): p. 1-17.
- Jamal, A. , et al., Post-SARS-CoV-2 Onset Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Symptoms in Two Cohort Studies of COVID-19 Recovery. medRxiv, 2024: p. 2024.11.08.24316976.
- Bonilla, H. , et al., Myalgic Encephalomyelitis/Chronic Fatigue Syndrome is common in post-acute sequelae of SARS-CoV-2 infection (PASC): Results from a post-COVID-19 multidisciplinary clinic. Frontiers in Neurology, 2023. 14.
- Dehlia, A. and M.A. Guthridge, The persistence of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) after SARS-CoV-2 infection: A systematic review and meta-analysis. Journal of Infection, 2024. 89(6): p. 106297.
- Saury, J.-M. , The role of the hippocampus in the pathogenesis of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Medical Hypotheses, 2016. 86: p. 30-38.
- Tate, W. , et al., Molecular Mechanisms of Neuroinflammation in ME/CFS and Long COVID to Sustain Disease and Promote Relapses. Frontiers in Neurology, 2022. 13.
- Hayden, M.R. , Hypothesis: neuroglia activation due to increased peripheral and CNS proinflammatory cytokines/chemokines with neuroinflammation may result in long COVID. Neuroglia, 2021. 2(1): p. 7-35.
- Ahamed, J. and J. Laurence, Long COVID endotheliopathy: hypothesized mechanisms and potential therapeutic approaches. The Journal of clinical investigation, 2022. 132(15).
- Wirth, K.J. and M. Löhn, Microvascular Capillary and Precapillary Cardiovascular Disturbances Strongly Interact to Severely Affect Tissue Perfusion and Mitochondrial Function in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Evolving from the Post COVID-19 Syndrome. Medicina, 2024. 60(2): p. 194.
- Wirth, K.J. and M. Löhn, Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and Comorbidities: Linked by Vascular Pathomechanisms and Vasoactive Mediators? Medicina, 2023. 59(5): p. 978.
- Wirth, K. and C. Scheibenbogen, A Unifying Hypothesis of the Pathophysiology of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS): Recognitions from the finding of autoantibodies against ß2-adrenergic receptors. Autoimmunity Reviews, 2020. 19(6): p. 102527.
- Kell, D.B. and E. Pretorius, The potential role of ischaemia–reperfusion injury in chronic, relapsing diseases such as rheumatoid arthritis, Long COVID, and ME/CFS: evidence, mechanisms, and therapeutic implications. Biochemical Journal, 2022. 479(16): p. 1653-1708.
- Nunes, M. , et al., Data-independent LC-MS/MS analysis of ME/CFS plasma reveals a dysregulated coagulation system, endothelial dysfunction, downregulation of complement machinery. Cardiovascular Diabetology, 2024. 23(1): p. 254.
- Nunes, J.M. , et al., The Occurrence of Hyperactivated Platelets and Fibrinaloid Microclots in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Pharmaceuticals, 2022. 15(8): p. 931.
- Apostolou, E. and A. Rosén, Epigenetic reprograming in myalgic encephalomyelitis/chronic fatigue syndrome: A narrative of latent viruses. Journal of Internal Medicine, 2024. 296(1): p. 93-115.
- Buonsenso, D. et al. Long COVID: A proposed hypothesis-driven model of viral persistence for the pathophysiology of the syndrome. in Allergy and Asthma Proceedings. 2022. OceanSide Publications.
- Proal, A.D. and M.B. VanElzakker, Long COVID or Post-acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms. Front Microbiol, 2021. 12: p. 698169.
- Proal, A.D. , et al., SARS-CoV-2 reservoir in post-acute sequelae of COVID-19 (PASC). Nature Immunology, 2023. 24(10): p. 1616-1627.
- Bansal, A.S. , et al., What causes ME/CFS: the role of the dysfunctional immune system and viral infections. Journal of Immunology and Allergy, 2022. 3(2): p. 1-15.
- Kell, D.B. and E. Pretorius, Are fibrinaloid microclots a cause of autoimmunity in Long Covid and other post-infection diseases? Biochem J, 2023. 480(15): p. 1217-1240.
- Stanculescu, D., L. Larsson, and J. Bergquist, Hypothesis: Mechanisms That Prevent Recovery in Prolonged ICU Patients Also Underlie Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Frontiers in Medicine, 2021. 8.
- Morris, G., G. Anderson, and M. Maes, Hypothalamic-Pituitary-Adrenal Hypofunction in Myalgic Encephalomyelitis (ME)/Chronic Fatigue Syndrome (CFS) as a Consequence of Activated Immune-Inflammatory and Oxidative and Nitrosative Pathways. Molecular Neurobiology, 2017. 54(9): p. 6806-6819.
- Eaton-Fitch, N. , et al., Immune exhaustion in ME/CFS and long COVID. JCI Insight, 2024. 9(20).
- Saito, S. , et al., Diverse immunological dysregulation, chronic inflammation, and impaired erythropoiesis in long COVID patients with chronic fatigue syndrome. Journal of Autoimmunity, 2024. 147: p. 103267.
- Pretorius, E. , et al., Prevalence of symptoms, comorbidities, fibrin amyloid microclots and platelet pathology in individuals with Long COVID/Post-Acute Sequelae of COVID-19 (PASC). Cardiovascular Diabetology, 2022. 21(1): p. 148.
- Dalton, C.F. , et al., Increased fibrinaloid microclot counts in platelet-poor plasma are associated with Long COVID. medRxiv, 2024: p. 2024.04.04.24305318.
- Vu, L.T. , et al., Single-cell transcriptomics of the immune system in ME/CFS at baseline and following symptom provocation. Cell Reports Medicine, 2024. 5(1).
- Giloteaux, L. , et al., Dysregulation of extracellular vesicle protein cargo in female myalgic encephalomyelitis/chronic fatigue syndrome cases and sedentary controls in response to maximal exercise. Journal of Extracellular Vesicles, 2024. 13(1): p. 12403.
- Aggarwal, A. , et al., Dysregulated platelet function in patients with postacute sequelae of COVID-19. Vascular Medicine, 2024. 29(2): p. 125-134.
- Pretorius, E., M. Nunes, and D. Kell, Flow Clotometry: Measuring Amyloid Microclots in ME/CFS, Long COVID, and Healthy Samples with Imaging Flow Cytometry. 2024.
- Liu, J. , et al., SARS-CoV-2 cell tropism and multiorgan infection. Cell Discovery, 2021. 7(1): p. 17.
- Ambrosino, P. , et al., Persistent Endothelial Dysfunction in Post-Acute COVID-19 Syndrome: A Case-Control Study. Biomedicines, 2021. 9(8): p. 957.
- Lambadiari, V. , et al., Association of COVID-19 with impaired endothelial glycocalyx, vascular function and myocardial deformation 4 months after infection. European Journal of Heart Failure, 2021. 23(11): p. 1916-1926.
- Fogarty, H. , et al., Persistent endotheliopathy in the pathogenesis of long COVID syndrome. Journal of Thrombosis and Haemostasis, 2021. 19(10): p. 2546-2553.
- Haffke, M. , et al., Endothelial dysfunction and altered endothelial biomarkers in patients with post-COVID-19 syndrome and chronic fatigue syndrome (ME/CFS). Journal of Translational Medicine, 2022. 20(1): p. 138.
- Oikonomou, E. , et al., Endothelial dysfunction in acute and long standing COVID−19: A prospective cohort study. Vascular Pharmacology, 2022. 144: p. 106975.
- Willems, L.H. , et al., Sustained inflammation, coagulation activation and elevated endothelin-1 levels without macrovascular dysfunction at 3 months after COVID-19. Thrombosis Research, 2022. 209: p. 106-114.
- Kuchler, T. , et al., Persistent endothelial dysfunction in post-COVID-19 syndrome and its associations with symptom severity and chronic inflammation. Angiogenesis, 2023. 26(4): p. 547-563.
- Vassiliou, A.G. , et al., Endotheliopathy in Acute COVID-19 and Long COVID. International Journal of Molecular Sciences, 2023. 24(9): p. 8237.
- Alfaro, E. , et al., Endothelial dysfunction and persistent inflammation in severe post-COVID-19 patients: implications for gas exchange. BMC Medicine, 2024. 22(1): p. 242.
- Wu, X. , et al., Damage to endothelial barriers and its contribution to long COVID. Angiogenesis, 2024. 27(1): p. 5-22.
- Ståhlberg, M. , et al., Post-Acute COVID-19 Syndrome: Prevalence of Peripheral Microvascular Endothelial Dysfunction and Associations with NT-ProBNP Dynamics. The American Journal of Medicine, 2024.
- Muys, M. , et al., Exploring Hypercoagulability in Post-COVID Syndrome (PCS): An Attempt at Unraveling the Endothelial Dysfunction. Journal of Clinical Medicine, 2025. 14(3): p. 789.
- Smadja, D.M. , et al., Circulating endothelial cells: a key biomarker of persistent fatigue after hospitalization for COVID-19. Angiogenesis, 2024. 28(1): p. 8.
- Thomas, D. , et al., CCL2-mediated endothelial injury drives cardiac dysfunction in long COVID. Nature Cardiovascular Research, 2024. 3(10): p. 1249-1265.
- Xu, S.-w., I. Ilyas, and J.-p. Weng, Endothelial dysfunction in COVID-19: an overview of evidence, biomarkers, mechanisms and potential therapies. Acta Pharmacologica Sinica, 2023. 44(4): p. 695-709.
- Perico, L., A. Benigni, and G. Remuzzi, SARS-CoV-2 and the spike protein in endotheliopathy. Trends Microbiol, 2024. 32(1): p. 53-67.
- Scherbakov, N. , et al., Peripheral endothelial dysfunction in myalgic encephalomyelitis/chronic fatigue syndrome. ESC Heart Failure, 2020. 7(3): p. 1064-1071.
- Sørland, K. , et al., Reduced Endothelial Function in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome-Results From Open-Label Cyclophosphamide Intervention Study. Front Med (Lausanne), 2021. 8: p. 642710.
- Blauensteiner, J. , et al., Altered endothelial dysfunction-related miRs in plasma from ME/CFS patients. Scientific Reports, 2021. 11(1): p. 10604.
- Sandvik, M.K. , et al., Endothelial dysfunction in ME/CFS patients. PLOS ONE, 2023. 18(2): p. e0280942.
- McLaughlin, M. , et al., People with Long COVID and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Exhibit Similarly Impaired Vascular Function. The American Journal of Medicine, 2023.
- Cambras, T. , et al., Skin Temperature Circadian Rhythms and Dysautonomia in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: The Role of Endothelin-1 in the Vascular Tone Dysregulation. International Journal of Molecular Sciences, 2023. 24(5): p. 4835.
- Domingo, J.C. , et al., Association of circulating biomarkers with illness severity measures differentiates myalgic encephalomyelitis/chronic fatigue syndrome and post-COVID-19 condition: a prospective pilot cohort study. Journal of Translational Medicine, 2024. 22(1): p. 343.
- Renz-Polster, H. , et al., The Pathobiology of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: The Case for Neuroglial Failure. Frontiers in Cellular Neuroscience, 2022. 16.
- Lubell, J. , Letter: Could endothelial dysfunction and vascular damage contribute to pain, inflammation and post-exertional malaise in individuals with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS)? Journal of Translational Medicine, 2022. 20(1): p. 40.
- Sfera, A. , et al., Endothelial Senescence and Chronic Fatigue Syndrome, a COVID-19 Based Hypothesis. Frontiers in Cellular Neuroscience, 2021. 15.
- Nunes, J.M., D. B. Kell, and E. Pretorius, Herpesvirus Infection of Endothelial Cells as a Systemic Pathological Axis in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Viruses, 2024. 16(4): p. 572.
- de Rooij, L.P.M.H., L. M. Becker, and P. Carmeliet, A Role for the Vascular Endothelium in Post–Acute COVID-19? Circulation, 2022. 145(20): p. 1503-1505.
- Kruger, A. , et al., Vascular Pathogenesis in Acute and Long COVID: Current Insights and Therapeutic Outlook. Semin Thromb Hemost, 2024(EFirst).
- van Campen, C.M.C. , et al., The Cardiac Output–Cerebral Blood Flow Relationship Is Abnormal in Most Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Patients with a Normal Heart Rate and Blood Pressure Response During a Tilt Test. Healthcare, 2024. 12(24): p. 2566.
- van Campen, C.M.C. , et al., Cerebral blood flow is reduced in ME/CFS during head-up tilt testing even in the absence of hypotension or tachycardia: A quantitative, controlled study using Doppler echography. Clinical Neurophysiology Practice, 2020. 5: p. 50-58.
- van Campen, C.M.C., P. C. Rowe, and F.C. Visser, Orthostatic Symptoms and Reductions in Cerebral Blood Flow in Long-Haul COVID-19 Patients: Similarities with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Medicina, 2022. 58(1): p. 28.
- Thapaliya, K. , et al., Brainstem volume changes in myalgic encephalomyelitis/chronic fatigue syndrome and long COVID patients. Frontiers in Neuroscience, 2023. 17.
- Chien, C. , et al., Altered brain perfusion and oxygen levels relate to sleepiness and attention in post-COVID syndrome. Annals of Clinical and Translational Neurology, 2024. 11(8): p. 2016-2029.
- Lee, J.-S., W. Sato, and C.-G. Son, Brain-regional characteristics and neuroinflammation in ME/CFS patients from neuroimaging: A systematic review and meta-analysis. Autoimmunity Reviews, 2024. 23(2): p. 103484.
- Li, X., P. Julin, and T.-Q. Li, Limbic Perfusion Is Reduced in Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Tomography, 2021. 7(4): p. 675-687.
- Pizzuto, D.A. , et al., Lung perfusion assessment in children with long-COVID: A pilot study. Pediatric Pulmonology, 2023. 58(7): p. 2059-2067.
- van Deursen, J.M. , The role of senescent cells in ageing. Nature, 2014. 509(7501): p. 439-446.
- Harley, C.B., A. B. Futcher, and C.W. Greider, Telomeres shorten during ageing of human fibroblasts. Nature, 1990. 345(6274): p. 458-460.
- von Zglinicki, T. , Role of oxidative stress in telomere length regulation and replicative senescence. Ann N Y Acad Sci, 2000. 908: p. 99-110.
- Narita, M. , et al., Spatial coupling of mTOR and autophagy augments secretory phenotypes. Science, 2011. 332(6032): p. 966-70.
- Campisi, J. , Senescent cells, tumor suppression, and organismal aging: good citizens, bad neighbors. Cell, 2005. 120(4): p. 513-22.
- Passos, J.F. , et al., Feedback between p21 and reactive oxygen production is necessary for cell senescence. Mol Syst Biol, 2010. 6: p. 347.
- Stein, G.H. , et al., Differential roles for cyclin-dependent kinase inhibitors p21 and p16 in the mechanisms of senescence and differentiation in human fibroblasts. Mol Cell Biol, 1999. 19(3): p. 2109-17.
- Rodier, F. , et al., DNA-SCARS: distinct nuclear structures that sustain damage-induced senescence growth arrest and inflammatory cytokine secretion. Journal of Cell Science, 2011. 124(1): p. 68-81.
- Narita, M. , et al., Rb-mediated heterochromatin formation and silencing of E2F target genes during cellular senescence. Cell, 2003. 113(6): p. 703-16.
- Ivanov, A. , et al., Lysosome-mediated processing of chromatin in senescence. J Cell Biol, 2013. 202(1): p. 129-43.
- Kirkland, J.L. and T. Tchkonia, Senolytic drugs: from discovery to translation. J Intern Med, 2020. 288(5): p. 518-536.
- Miwa, S. , et al., Mitochondrial dysfunction in cell senescence and aging. J Clin Invest, 2022. 132(13).
- Robbins, E., E. M. Levine, and H. Eagle, Morphologic changes accompanying senescence of cultured human diploid cells. J Exp Med, 1970. 131(6): p. 1211-22.
- Correia-Melo, C. , et al., Mitochondria are required for pro-ageing features of the senescent phenotype. Embo j, 2016. 35(7): p. 724-42.
- Coppé, J.P. , et al., Senescence-associated secretory phenotypes reveal cell-nonautonomous functions of oncogenic RAS and the p53 tumor suppressor. PLoS Biol, 2008. 6(12): p. 2853-68.
- Dimri, G.P. , et al., A biomarker that identifies senescent human cells in culture and in aging skin in vivo. Proc Natl Acad Sci U S A, 1995. 92(20): p. 9363-7.
- Kurz, D.J. , et al., Senescence-associated (beta)-galactosidase reflects an increase in lysosomal mass during replicative ageing of human endothelial cells. J Cell Sci, 2000. 113 ( Pt 20): p. 3613-22.
- Oguma, Y. , et al., Meta-analysis of senescent cell secretomes to identify common and specific features of the different senescent phenotypes: a tool for developing new senotherapeutics. Cell Communication and Signaling, 2023. 21(1): p. 262.
- Lagnado, A. , et al., Neutrophils induce paracrine telomere dysfunction and senescence in ROS-dependent manner. Embo j, 2021. 40(9): p. e106048.
- Ovadya, Y. , et al., Impaired immune surveillance accelerates accumulation of senescent cells and aging. Nat Commun, 2018. 9(1): p. 5435.
- Pereira, B.I. , et al., Senescent cells evade immune clearance via HLA-E-mediated NK and CD8+ T cell inhibition. Nature Communications, 2019. 10(1): p. 2387.
- Nelson, G. , et al., A senescent cell bystander effect: senescence-induced senescence. Aging Cell, 2012. 11(2): p. 345-9.
- D’Agnillo, F. , et al., Lung epithelial and endothelial damage, loss of tissue repair, inhibition of fibrinolysis, and cellular senescence in fatal COVID-19. Science Translational Medicine, 2021. 13(620): p. eabj7790.
- Urata, R. , et al., Senescent endothelial cells are predisposed to SARS-CoV-2 infection and subsequent endothelial dysfunction. Scientific Reports, 2022. 12(1): p. 11855.
- Gioia, U. , et al., SARS-CoV-2 infection induces DNA damage, through CHK1 degradation and impaired 53BP1 recruitment, and cellular senescence. Nat Cell Biol, 2023. 25(4): p. 550-564.
- Lee, S. , et al., Virus-induced senescence is a driver and therapeutic target in COVID-19. Nature, 2021. 599(7884): p. 283-289.
- Camell, C.D. , et al., Senolytics reduce coronavirus-related mortality in old mice. Science, 2021. 373(6552).
- Pastor-Fernández, A. , et al., Treatment with the senolytics dasatinib/quercetin reduces SARS-CoV-2-related mortality in mice. Aging Cell, 2023. 22(3): p. e13771.
- Potgieter, M. , et al., The dormant blood microbiome in chronic, inflammatory diseases. FEMS Microbiol Rev, 2015. 39(4): p. 567-91.
- Wang, X. and B. He, Endothelial dysfunction: molecular mechanisms and clinical implications. MedComm, 2024. 5(8): p. e651.
- Bordoni, V. , et al., SARS-CoV-2 infection of airway epithelium triggers pulmonary endothelial cell activation and senescence associated with type I IFN production. Cells, 2022. 11(18): p. 2912.
- Meyer, K. , et al., SARS-CoV-2 Spike Protein Induces Paracrine Senescence and Leukocyte Adhesion in Endothelial Cells. Journal of Virology, 2021. 95(17): p. 10.1128/jvi.00794-21.
- Lipskaia, L. , et al., Evidence that SARS-CoV-2 induces lung cell senescence: potential impact on COVID-19 lung disease. American journal of respiratory cell and molecular biology, 2022. 66(1): p. 107-111.
- Schulz, L. , et al., Influenza Virus-Induced Paracrine Cellular Senescence of the Lung Contributes to Enhanced Viral Load. Aging Dis, 2023. 14(4): p. 1331-1348.
- Yan, Y. , et al., NS1 of H7N9 Influenza A Virus Induces NO-Mediated Cellular Senescence in Neuro2a Cells. Cellular Physiology and Biochemistry, 2017. 43(4): p. 1369-1380.
- Arvia, R. , et al., Parvovirus B19 induces cellular senescence in human dermal fibroblasts: putative role in systemic sclerosis–associated fibrosis. Rheumatology, 2021. 61(9): p. 3864-3874.
- Lekva, T. , et al., Markers of cellular senescence is associated with persistent pulmonary pathology after COVID-19 infection. Infect Dis (Lond), 2022. 54(12): p. 918-923.
- Lynch, S.M. , et al., Role of Senescence and Aging in SARS-CoV-2 Infection and COVID-19 Disease. Cells, 2021. 10(12): p. 3367.
- Berentschot, J.C. , et al., Immunological profiling in long COVID: overall low grade inflammation and T-lymphocyte senescence and increased monocyte activation correlating with increasing fatigue severity. Frontiers in Immunology, 2023. 14.
- Lord, J.M. , et al., Accelerated immune ageing is associated with COVID-19 disease severity. Immunity & Ageing, 2024. 21(1): p. 6.
- Kempuraj, D. , et al., COVID-19 and Long COVID: Disruption of the Neurovascular Unit, Blood-Brain Barrier, and Tight Junctions. The Neuroscientist, 2024. 30(4): p. 421-439.
- Otifi, H.M. and B.K. Adiga, Endothelial dysfunction in Covid-19 infection. The American journal of the medical sciences, 2022. 363(4): p. 281-287.
- Mroueh, A. , et al., COVID-19 promotes endothelial dysfunction and thrombogenicity: role of proinflammatory cytokines/SGLT2 prooxidant pathway. Journal of Thrombosis and Haemostasis, 2024. 22(1): p. 286-299.
- Liu, F. , et al., SARS-CoV-2 infects endothelial cells in vivo and in vitro. Frontiers in cellular and infection microbiology, 2021. 11: p. 701278.
- Yang, R.-C. , et al., SARS-CoV-2 productively infects human brain microvascular endothelial cells. Journal of neuroinflammation, 2022. 19(1): p. 149.
- Caccuri, F. , et al., SARS-CoV-2 Infection Remodels the Phenotype and Promotes Angiogenesis of Primary Human Lung Endothelial Cells. Microorganisms, 2021. 9(7): p. 1438.
- Yamada, S. , et al., SARS-CoV-2 causes dysfunction in human iPSC-derived brain microvascular endothelial cells potentially by modulating the Wnt signaling pathway. Fluids and Barriers of the CNS, 2024. 21(1): p. 32.
- Hatch, C.J. , et al., SARS-CoV-2 infection of endothelial cells, dependent on flow-induced ACE2 expression, drives hypercytokinemia in a vascularized microphysiological system. Frontiers in Cardiovascular Medicine, 2024. 11.
- Meyer, K. , et al., SARS-CoV-2 spike protein expressing epithelial cells promotes senescence associated secretory phenotype in endothelial cells and increased inflammatory response. bioRxiv, 2021: p. 2021.04.16.440215.
- Kedor, C. , et al., Chronic COVID-19 Syndrome and Chronic Fatigue Syndrome (ME/CFS) following the first pandemic wave in Germany – a first analysis of a prospective observational study. medRxiv, 2021: p. 2021.02.06.21249256.
- Vernon, S.D. , et al., Incidence and Prevalence of Post-COVID-19 Myalgic Encephalomyelitis: A Report from the Observational RECOVER-Adult Study. Journal of General Internal Medicine, 2025.
- Farina, A. , et al., Innate Immune Modulation Induced by EBV Lytic Infection Promotes Endothelial Cell Inflammation and Vascular Injury in Scleroderma. Front Immunol, 2021. 12: p. 651013.
- Indari, O. , et al., Early biomolecular changes in brain microvascular endothelial cells under Epstein–Barr virus influence: a Raman microspectroscopic investigation. Integrative Biology, 2022. 14(4): p. 89-97.
- Jones, K. , et al., Infection of human endothelial cells with Epstein-Barr virus. J Exp Med, 1995. 182(5): p. 1213-21.
- Casiraghi, C., K. Dorovini-Zis, and M.S. Horwitz, Epstein-Barr virus infection of human brain microvessel endothelial cells: A novel role in multiple sclerosis. Journal of Neuroimmunology, 2011. 230(1): p. 173-177.
- Pricoco, R. , et al., One-year follow-up of young people with ME/CFS following infectious mononucleosis by Epstein-Barr virus. Frontiers in Pediatrics, 2024. 11.
- Kasimir, F. , et al., Tissue specific signature of HHV-6 infection in ME/CFS. Frontiers in Molecular Biosciences, 2022. 9: p. 1044964.
- Ruiz-Pablos, M. , et al., Epstein-Barr virus and the origin of myalgic encephalomyelitis or chronic fatigue syndrome. Frontiers in immunology, 2021. 12: p. 656797.
- Shikova, E. , et al., Cytomegalovirus, Epstein-Barr virus, and human herpesvirus-6 infections in patients with myalgic еncephalomyelitis/chronic fatigue syndrome. Journal of medical virology, 2020. 92(12): p. 3682-3688.
- Takatsuka, H. , et al., Endothelial damage caused by cytomegalovirus and human herpesvirus-6. Bone marrow transplantation, 2003. 31(6): p. 475-479.
- Caruso, A. , et al., HHV-6 infects human aortic and heart microvascular endothelial cells, increasing their ability to secrete proinflammatory chemokines. J Med Virol, 2002. 67(4): p. 528-33.
- Caruso, A. , et al., Human herpesvirus-6 modulates RANTES production in primary human endothelial cell cultures. J Med Virol, 2003. 70(3): p. 451-8.
- Wu, C.A. and J.D. Shanley, Chronic infection of human umbilical vein endothelial cells by human herpesvirus-6. J Gen Virol, 1998. 79 ( Pt 5): p. 1247-56.
- Rotola, A. , et al., Human herpesvirus 6 infects and replicates in aortic endothelium. J Clin Microbiol, 2000. 38(8): p. 3135-6.
- Mozhgani, S.-H. , et al., Human Herpesvirus 6 Infection and Risk of Chronic Fatigue Syndrome: A Systematic Review and Meta-Analysis. Intervirology, 2021. 65(1): p. 49-57.
- Zeng, H. , et al., A(H7N9) virus results in early induction of proinflammatory cytokine responses in both human lung epithelial and endothelial cells and shows increased human adaptation compared with avian H5N1 virus. J Virol, 2015. 89(8): p. 4655-67.
- Bauer, L. , et al., The pro-inflammatory response to influenza A virus infection is fueled by endothelial cells. Life Science Alliance, 2023. 6(7): p. e202201837.
- Marchenko, V. , et al., Influenza A Virus Causes Histopathological Changes and Impairment in Functional Activity of Blood Vessels in Different Vascular Beds. Viruses, 2022. 14(2): p. 396.
- Marchesi, S. , et al., Acute inflammatory state during influenza infection and endothelial function. Atherosclerosis, 2005. 178(2): p. 345-350.
- Marchenko, V.A. and I.N. Zhilinskaya, Endothelial activation and dysfunction caused by influenza A virus (Alphainfluenzavirus influenzae). Problems of Virology, 2024. 69(6): p. 465-478.
- Hiyoshi, M. , et al., Influenza A virus infection of vascular endothelial cells induces GSK-3β-mediated β-catenin degradation in adherens junctions, with a resultant increase in membrane permeability. Archives of Virology, 2015. 160(1): p. 225-234.
- Armstrong, S.M. , et al., Influenza infects lung microvascular endothelium leading to microvascular leak: role of apoptosis and claudin-5. PLoS One, 2012. 7(10): p. e47323.
- Suo, J. , et al., Influenza virus aggravates the ox-LDL-induced apoptosis of human endothelial cells via promoting p53 signaling. Journal of Medical Virology, 2015. 87(7): p. 1113-1123.
- Xia, B. , et al., FBXL19 in endothelial cells protects the heart from influenza A infection by enhancing antiviral immunity and reducing cellular senescence programs. American Journal of Physiology-Heart and Circulatory Physiology, 2024. 327(4): p. H937-H946.
- Magnus, P. , et al., Chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME) is associated with pandemic influenza infection, but not with an adjuvanted pandemic influenza vaccine. Vaccine, 2015. 33(46): p. 6173-6177.
- Chang, H. , et al., Increased risk of chronic fatigue syndrome following infection: a 17-year population-based cohort study. Journal of Translational Medicine, 2023. 21(1): p. 804.
- Liang, C.-C. , et al., Human endothelial cell activation and apoptosis induced by enterovirus 71 infection. Journal of Medical Virology, 2004. 74(4): p. 597-603.
- Luo, W. , et al., Proteomic Analysis of Human Brain Microvascular Endothelial Cells Reveals Differential Protein Expression in Response to Enterovirus 71 Infection. BioMed Research International, 2015. 2015(1): p. 864169.
- Ji, W. , et al., The Disruption of the Endothelial Barrier Contributes to Acute Lung Injury Induced by Coxsackievirus A2 Infection in Mice. International Journal of Molecular Sciences, 2021. 22(18): p. 9895.
- Han, S. , et al., Emerging concerns of blood-brain barrier dysfunction caused by neurotropic enteroviral infections. Virology, 2024. 591: p. 109989.
- Zhu, Y. , et al., Enterovirus 71 enters human brain microvascular endothelial cells through an ARF6-mediated endocytic pathway. Journal of Medical Virology, 2023. 95(7): p. e28915.
- Saijets, S. , et al., Enterovirus infection and activation of human umbilical vein endothelial cells. Journal of medical virology, 2003. 70(3): p. 430-439.
- Schmidt-Lucke, C. , et al., Interferon Beta Modulates Endothelial Damage in Patients with Cardiac Persistence of Human Parvovirus B19 Infection. The Journal of Infectious Diseases, 2010. 201(6): p. 936-945.
- Wen, J. and C. Huang, Coxsackieviruses B3 infection of myocardial microvascular endothelial cells activates fractalkine via the ERK1/2 signaling pathway. Mol Med Rep, 2017. 16(5): p. 7548-7552.
- O'Neal, A.J. and M.R. Hanson, The Enterovirus Theory of Disease Etiology in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Critical Review. Front Med (Lausanne), 2021. 8: p. 688486.
- Chia, J.K.S. and A.Y. Chia, Chronic fatigue syndrome is associated with chronic enterovirus infection of the stomach. Journal of Clinical Pathology, 2008. 61(1): p. 43-48.
- Chia, J. , et al., Acute enterovirus infection followed by myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and viral persistence. J Clin Pathol, 2010. 63(2): p. 165-8.
- Tschöpe, C. , et al., High Prevalence of Cardiac Parvovirus B19 Infection in Patients With Isolated Left Ventricular Diastolic Dysfunction. Circulation, 2005. 111(7): p. 879-886.
- Bachelier, K. , et al., Parvovirus B19-induced vascular damage in the heart is associated with elevated circulating endothelial microparticles. PLoS One, 2017. 12(5): p. e0176311.
- Rinkūnaitė, I. , et al., The Effect of a Unique Region of Parvovirus B19 Capsid Protein VP1 on Endothelial Cells. Biomolecules, 2021. 11(4): p. 606.
- von Kietzell, K. , et al., Antibody-mediated enhancement of parvovirus B19 uptake into endothelial cells mediated by a receptor for complement factor C1q. Journal of virology, 2014. 88(14): p. 8102-8115.
- Pasquinelli, G. , et al., Placental endothelial cells can be productively infected by Parvovirus B19. Journal of Clinical Virology, 2009. 44(1): p. 33-38.
- Seishima, M. , et al., Chronic fatigue syndrome after human parvovirus B19 infection without persistent viremia. Dermatology, 2008. 216(4): p. 341-6.
- Kerr, J.R. and D.L. Mattey, Preexisting psychological stress predicts acute and chronic fatigue and arthritis following symptomatic parvovirus B19 infection. Clin Infect Dis, 2008. 46(9): p. e83-7.
- Rasa-Dzelzkaleja, S. , et al., The persistent viral infections in the development and severity of myalgic encephalomyelitis/chronic fatigue syndrome. Journal of Translational Medicine, 2023. 21(1): p. 33.
- Rasa-Dzelzkalēja, S. , et al., Association of Human Parvovirus B19 Infection with Development and Clinical Course of Myalgic Encephalomyelitis / Chronic Fatigue Syndrome. Proceedings of the Latvian Academy of Sciences. Section B. Natural, Exact, and Applied Sciences., 2019. 73(5): p. 411-418.
- Abdul, Y. , et al., Endothelin A receptors contribute to senescence of brain microvascular endothelial cells. Can J Physiol Pharmacol, 2022. 100(12): p. 1087-1096.
- El Habhab, A. , et al., Significance of neutrophil microparticles in ischaemia-reperfusion: Pro-inflammatory effectors of endothelial senescence and vascular dysfunction. Journal of Cellular and Molecular Medicine, 2020. 24(13): p. 7266-7281.
- Park, S.-H. , et al., Angiotensin II-induced upregulation of SGLT1 and 2 contributes to human microparticle-stimulated endothelial senescence and dysfunction: protective effect of gliflozins. Cardiovascular diabetology, 2021. 20: p. 1-17.
- Zhang, D. , et al., Homocysteine accelerates senescence of endothelial cells via DNA hypomethylation of human telomerase reverse transcriptase. Arterioscler Thromb Vasc Biol, 2015. 35(1): p. 71-8.
- Shang, D., H. Liu, and Z. Tu, Pro-inflammatory cytokines mediating senescence of vascular endothelial cells in atherosclerosis. Fundamental & Clinical Pharmacology, 2023. 37(5): p. 928-936.
- Sfera, A. , et al., Intoxication With Endogenous Angiotensin II: A COVID-19 Hypothesis. Front Immunol, 2020. 11: p. 1472.
- Bloom, S.I. , et al., Mechanisms and consequences of endothelial cell senescence. Nat Rev Cardiol, 2023. 20(1): p. 38-51.
- Wang, P. , et al., Endothelial Senescence: From Macro- to Micro-Vasculature and Its Implications on Cardiovascular Health. International Journal of Molecular Sciences, 2024. 25(4): p. 1978.
- Sabbatinelli, J. , et al., Where Metabolism Meets Senescence: Focus on Endothelial Cells. Frontiers in Physiology, 2019. 10.
- Giuliani, A. , et al., Senescent Endothelial Cells Sustain Their Senescence-Associated Secretory Phenotype (SASP) through Enhanced Fatty Acid Oxidation. Antioxidants, 2023. 12(11): p. 1956.
- Hasan, H. , et al., Thrombin Induces Angiotensin II-Mediated Senescence in Atrial Endothelial Cells: Impact on Pro-Remodeling Patterns. Journal of Clinical Medicine, 2019. 8(10): p. 1570.
- Cohen, C. , et al., Glomerular endothelial cell senescence drives age-related kidney disease through PAI-1. EMBO Molecular Medicine, 2021. 13(11): p. e14146.
- Grillari, J. , et al., Subtractive hybridization of mRNA from early passage and senescent endothelial cells. Exp Gerontol, 2000. 35(2): p. 187-97.
- Alavi, P. , et al., Aging Is Associated With Organ-Specific Alterations in the Level and Expression Pattern of von Willebrand Factor. Arteriosclerosis, Thrombosis, and Vascular Biology, 2023. 43(11): p. 2183-2196.
- Han, Y. and S.Y. Kim, Endothelial senescence in vascular diseases: current understanding and future opportunities in senotherapeutics. Experimental & Molecular Medicine, 2023. 55(1): p. 1-12.
- Matsushita, H. , et al., eNOS Activity Is Reduced in Senescent Human Endothelial Cells. Circulation Research, 2001. 89(9): p. 793-798.
- Minamino, T. , et al., Endothelial cell senescence in human atherosclerosis: role of telomere in endothelial dysfunction. Circulation, 2002. 105(13): p. 1541-4.
- Demaria, M. , et al., An essential role for senescent cells in optimal wound healing through secretion of PDGF-AA. Dev Cell, 2014. 31(6): p. 722-33.
- Prattichizzo, F. , et al., Anti-TNF-α treatment modulates SASP and SASP-related microRNAs in endothelial cells and in circulating angiogenic cells. Oncotarget, 2016. 7(11): p. 11945-58.
- Khavinson, V. , et al., Senescence-Associated Secretory Phenotype of Cardiovascular System Cells and Inflammaging: Perspectives of Peptide Regulation. Cells, 2023. 12(1): p. 106.
- Liao, Y.-L. , et al., Senescent endothelial cells: a potential target for diabetic retinopathy. Angiogenesis, 2024. 27(4): p. 663-679.
- Shosha, E. , et al., Mechanisms of Diabetes-Induced Endothelial Cell Senescence: Role of Arginase 1. Int J Mol Sci, 2018. 19(4).
- Zerón-Rugerio, M.F. , et al., Sleep and circadian rhythm alterations in myalgic encephalomyelitis/chronic fatigue syndrome and post-COVID fatigue syndrome and its association with cardiovascular risk factors: A prospective cohort study. Chronobiology International, 2024. 41(8): p. 1104-1115.
- Svitailo, V.S. and M.D. Chemych, Indicators of blood coagulation function, concentration of endothelin-1 and Long-COVID. 2024.
- Philippe, A. , et al., VEGF-A plasma levels are associated with impaired DLCO and radiological sequelae in long COVID patients. Angiogenesis, 2024. 27(1): p. 51-66.
- Kavyani, B. , et al., Dysregulation of the Kynurenine Pathway, Cytokine Expression Pattern, and Proteomics Profile Link to Symptomology in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Molecular Neurobiology, 2024. 61(7): p. 3771-3787.
- Abraham, G.R. , et al., Endothelin-1 is increased in the plasma of patients hospitalised with Covid-19. Journal of Molecular and Cellular Cardiology, 2022. 167: p. 92-96.
- Turgunova, L. , et al., The Association of Endothelin-1 with Early and Long-Term Mortality in COVID-19. Journal of Personalized Medicine, 2023. 13(11): p. 1558.
- Farhangrazi, Z.S. and S.M. Moghimi, Elevated circulating endothelin-1 as a potential biomarker for high-risk COVID-19 severity. Precis Nanomed, 2020. 3: p. 622-628.
- Yokoi, T. , et al., Apoptosis signal-regulating kinase 1 mediates cellular senescence induced by high glucose in endothelial cells. Diabetes, 2006. 55(6): p. 1660-5.
- Wirth, K.J., C. Scheibenbogen, and F. Paul, An attempt to explain the neurological symptoms of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Journal of Translational Medicine, 2021. 19(1): p. 471.
- Wang, Y. , et al., Cerebral blood flow alterations and host genetic association in individuals with long COVID: A transcriptomic-neuroimaging study. Journal of Cerebral Blood Flow & Metabolism, 2025. 45(3): p. 431-442.
- Kell, D.B., G. J. Laubscher, and E. Pretorius, A central role for amyloid fibrin microclots in long COVID/PASC: origins and therapeutic implications. Biochem J, 2022. 479(4): p. 537-559.
- Kim, S.Y. and J. Cheon, Senescence-associated microvascular endothelial dysfunction: A focus on the blood-brain and blood-retinal barriers. Ageing Research Reviews, 2024. 100: p. 102446.
- Chala, N. , et al., Mechanical Fingerprint of Senescence in Endothelial Cells. Nano Lett, 2021. 21(12): p. 4911-4920.
- Stamatovic, S.M. , et al., Decline in Sirtuin-1 expression and activity plays a critical role in blood-brain barrier permeability in aging. Neurobiol Dis, 2019. 126: p. 105-116.
- Yamazaki, Y. , et al., Vascular Cell Senescence Contributes to Blood–Brain Barrier Breakdown. Stroke, 2016. 47(4): p. 1068-1077.
- Najari Beidokhti, M. , et al., Lung endothelial cell senescence impairs barrier function and promotes neutrophil adhesion and migration. GeroScience, 2025.
- Donato, A.J. , et al., Cellular and molecular biology of aging endothelial cells. J Mol Cell Cardiol, 2015. 89(Pt B): p. 122-35.
- van Campen, C.M.C., P. C. Rowe, and F.C. Visser, Cerebral Blood Flow Is Reduced in Severe Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Patients During Mild Orthostatic Stress Testing: An Exploratory Study at 20 Degrees of Head-Up Tilt Testing. Healthcare, 2020. 8(2): p. 169.
- Nunes, J.M., D. B. Kell, and E. Pretorius, Cardiovascular and haematological pathology in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): A role for viruses. Blood Rev, 2023. 60: p. 101075.
- McMaster, M.W. , et al., The Impact of Long COVID-19 on the Cardiovascular System. Cardiology in Review, 2024.
- Hira, R. , et al., Attenuated cardiac autonomic function in patients with long-COVID with impaired orthostatic hemodynamics. Clinical Autonomic Research, 2025.
- Ohno, Y. , et al., The diagnostic value of endothelial function as a potential sensor of fatigue in health. Vascular Health and Risk Management, 2010. 6(null): p. 135-144.
- Honda, S. , et al., Cellular senescence promotes endothelial activation through epigenetic alteration, and consequently accelerates atherosclerosis. Scientific Reports, 2021. 11(1): p. 14608.
- Li, Z. , et al., Neutrophil extracellular traps potentiate effector T cells via endothelial senescence in uveitis. JCI Insight, 2025. 10(2).
- Rolas, L. , et al., Senescent endothelial cells promote pathogenic neutrophil trafficking in inflamed tissues. EMBO reports, 2024. 25(9): p. 3842-3869.
- Appelman, B. , et al., Muscle abnormalities worsen after post-exertional malaise in long COVID. Nature Communications, 2024. 15(1): p. 17.
- Pantsulaia, I., W. M. Ciszewski, and J. Niewiarowska, Senescent endothelial cells: Potential modulators of immunosenescence and ageing. Ageing Research Reviews, 2016. 29: p. 13-25.
- Müller, L. and S. Di Benedetto, Inflammaging, immunosenescence, and cardiovascular aging: insights into long COVID implications. Frontiers in Cardiovascular Medicine, 2024. 11.
- Francavilla, F. , et al., Inflammaging and Immunosenescence in the Post-COVID Era: Small Molecules, Big Challenges. ChemMedChem. n/a(n/a): p. e202400672.
- Schmitt, C.A. , et al., COVID-19 and cellular senescence. Nature Reviews Immunology, 2023. 23(4): p. 251-263.
- Pedroso, R.B. , et al., Rapid progression of CD8 and CD4 T cells to cellular exhaustion and senescence during SARS-CoV2 infection. Journal of Leukocyte Biology, 2024. 116(6): p. 1385-1397.
- De Biasi, S. , et al., Marked T cell activation, senescence, exhaustion and skewing towards TH17 in patients with COVID-19 pneumonia. Nat Commun, 2020. 11(1): p. 3434.
- Zhang, J. , et al., Elevated CD4(+) T Cell Senescence Associates with Impaired Immune Responsiveness in Severe COVID-19. Aging Dis, 2024. 16(1): p. 498-511.
- Srivastava, R. , et al., High Frequencies of Phenotypically and Functionally Senescent and Exhausted CD56(+)CD57(+)PD-1(+) Natural Killer Cells, SARS-CoV-2-Specific Memory CD4(+) and CD8(+) T cells Associated with Severe Disease in Unvaccinated COVID-19 Patients. bioRxiv, 2022.
- Wiech, M. , et al., Remodeling of T Cell Dynamics During Long COVID Is Dependent on Severity of SARS-CoV-2 Infection. Frontiers in Immunology, 2022. 13.
- Van Campenhout, J. , et al., Unravelling the Connection Between Energy Metabolism and Immune Senescence/Exhaustion in Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Biomolecules, 2025. 15(3): p. 357.
- Arora, S. , et al., Invariant natural killer and T-cells coordinate removal of senescent cells. Med, 2021. 2(8): p. 938-950.e8.
- Kale, A. , et al., Role of immune cells in the removal of deleterious senescent cells. Immunity & Ageing, 2020. 17(1): p. 16.
- Eaton-Fitch, N. , et al., A systematic review of natural killer cells profile and cytotoxic function in myalgic encephalomyelitis/chronic fatigue syndrome. Systematic Reviews, 2019. 8(1): p. 279.
- Baraniuk, J.N., N. Eaton-Fitch, and S. Marshall-Gradisnik, Meta-analysis of natural killer cell cytotoxicity in myalgic encephalomyelitis/chronic fatigue syndrome. Frontiers in Immunology, 2024. 15.
- Thierry, A.R. , NETosis creates a link between diabetes and Long COVID. Physiological Reviews, 2024. 104(2): p. 651-654.
- Shafqat, A. , et al., Cellular senescence in brain aging and cognitive decline. Frontiers in Aging Neuroscience, 2023. 15.
- Binet, F. , et al., Neutrophil extracellular traps target senescent vasculature for tissue remodeling in retinopathy. Science, 2020. 369(6506): p. eaay5356.
- Pretorius, E. , et al., Circulating microclots are structurally associated with Neutrophil Extracellular Traps and their amounts are strongly elevated in long COVID patients. 2024.
- Gil, A. , et al., Identification of CD8 T-cell dysfunction associated with symptoms in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and Long COVID and treatment with a nebulized antioxidant/anti-pathogen agent in a retrospective case series. Brain Behav Immun Health, 2024. 36: p. 100720.
- Curriu, M. , et al., Screening NK-, B- and T-cell phenotype and function in patients suffering from Chronic Fatigue Syndrome. J Transl Med, 2013. 11: p. 68.
- Mandarano, A.H. , et al., Myalgic encephalomyelitis/chronic fatigue syndrome patients exhibit altered T cell metabolism and cytokine associations. J Clin Invest, 2020. 130(3): p. 1491-1505.
- Maya, J. , Surveying the Metabolic and Dysfunctional Profiles of T Cells and NK Cells in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. International Journal of Molecular Sciences, 2023. 24(15): p. 11937.
- Arese, P., F. Turrini, and E. Schwarzer, Band 3/Complement-mediated Recognition and Removal of Normally Senescent and Pathological Human Erythrocytes. Cellular Physiology and Biochemistry, 2005. 16(4-6): p. 133-146.
- Lutz, L. , et al., Evaluation of Immune Dysregulation in an Austrian Patient Cohort Suffering from Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Biomolecules, 2021. 11(9): p. 1359.
- Rohrhofer, J. , et al., Immunological Patient Stratification in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Journal of Clinical Medicine, 2024. 13(1): p. 275.
- Baillie, K. , et al., Complement dysregulation is a prevalent and therapeutically amenable feature of long COVID. Med, 2024. 5(3): p. 239-253.e5.
- Yu, S. , et al., M1 macrophages accelerate renal glomerular endothelial cell senescence through reactive oxygen species accumulation in streptozotocin-induced diabetic mice. International Immunopharmacology, 2020. 81: p. 106294.
- Gao, C. , et al., Endothelial cell phagocytosis of senescent neutrophils decreases procoagulant activity. Thromb Haemost, 2013. 109(06): p. 1079-1090.
- Sun, Y. , et al., Immunometabolic changes and potential biomarkers in CFS peripheral immune cells revealed by single-cell RNA sequencing. Journal of Translational Medicine, 2024. 22(1): p. 925.
- Almulla, A.F. , et al., Immune activation and immune-associated neurotoxicity in Long-COVID: A systematic review and meta-analysis of 103 studies comprising 58 cytokines/chemokines/growth factors. Brain, Behavior, and Immunity, 2024.
- Altmann, D.M. , et al., The immunology of long COVID. Nature Reviews Immunology, 2023. 23(10): p. 618-634.
- Riederer, I. , et al., Irradiation-induced up-regulation of HLA-E on macrovascular endothelial cells confers protection against killing by activated natural killer cells. PLoS one, 2010. 5(12): p. e15339.
- Kiss, T. , et al., Single-cell RNA sequencing identifies senescent cerebromicrovascular endothelial cells in the aged mouse brain. Geroscience, 2020. 42(2): p. 429-444.
- Knopp, R.C. , et al., Cellular senescence and the blood-brain barrier: Implications for aging and age-related diseases. Exp Biol Med (Maywood), 2023. 248(5): p. 399-411.
- Graves, S.I. and D.J. Baker, Implicating endothelial cell senescence to dysfunction in the ageing and diseased brain. Basic & Clinical Pharmacology & Toxicology, 2020. 127(2): p. 102-110.
- Sakamuri, S.S.V.P. , et al., Glycolytic and Oxidative Phosphorylation Defects Precede the Development of Senescence in Primary Human Brain Microvascular Endothelial Cells. GeroScience, 2022. 44(4): p. 1975-1994.
- Phoenix, A., R. Chandran, and A. Ergul, Cerebral microvascular senescence and inflammation in diabetes. Frontiers in Physiology, 2022. 13: p. 864758.
- Cantuti-Castelvetri, L. , et al., Neuropilin-1 facilitates SARS-CoV-2 cell entry and infectivity. Science, 2020. 370(6518): p. 856-860.
- Lukiw, W.J., A. Pogue, and J.M. Hill, SARS-CoV-2 Infectivity and Neurological Targets in the Brain. Cellular and Molecular Neurobiology, 2022. 42(1): p. 217-224.
- Stein, S.R. , et al., SARS-CoV-2 infection and persistence in the human body and brain at autopsy. Nature, 2022. 612(7941): p. 758-763.
- Volle, R. , et al., Differential permissivity of human cerebrovascular endothelial cells to enterovirus infection and specificities of serotype EV-A71 in crossing an in vitro model of the human blood–brain barrier. Journal of General Virology, 2015. 96(7): p. 1682-1695.
- Higazy, D. , et al., Altered gene expression in human brain microvascular endothelial cells in response to the infection of influenza H1N1 virus. Animal Diseases, 2022. 2(1): p. 25.
- Lei, Y. , et al., Influenza H7N9 virus disrupts the monolayer human brain microvascular endothelial cells barrier in vitro. Virology Journal, 2023. 20(1): p. 219.
- Real, M.G.C. , et al., Endothelial Cell Senescence Effect on the Blood-Brain Barrier in Stroke and Cognitive Impairment. Neurology, 2024. 103(11): p. e210063.
- Ahire, C. , et al., Accelerated cerebromicrovascular senescence contributes to cognitive decline in a mouse model of paclitaxel (Taxol)-induced chemobrain. Aging Cell, 2023. 22(7): p. e13832.
- Budamagunta, V. , et al., Effect of peripheral cellular senescence on brain aging and cognitive decline. Aging Cell, 2023. 22(5): p. e13817.
- Pushpam, M. , et al., Recurrent endothelin-1 mediated vascular insult leads to cognitive impairment protected by trophic factor pleiotrophin. Experimental Neurology, 2024. 381: p. 114938.
- Greene, C. , et al., Blood–brain barrier disruption and sustained systemic inflammation in individuals with long COVID-associated cognitive impairment. Nature Neuroscience, 2024. 27(3): p. 421-432.
- Chaganti, J. , et al., Blood brain barrier disruption and glutamatergic excitotoxicity in post-acute sequelae of SARS COV-2 infection cognitive impairment: potential biomarkers and a window into pathogenesis. Frontiers in Neurology, 2024. 15.
- Williams PhD, M.V. , et al., Epstein-Barr Virus dUTPase Induces Neuroinflammatory Mediators: Implications for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Clinical Therapeutics, 2019. 41(5): p. 848-863.
- Ungvari, Z. , et al., Ionizing radiation promotes the acquisition of a senescence-associated secretory phenotype and impairs angiogenic capacity in cerebromicrovascular endothelial cells: role of increased DNA damage and decreased DNA repair capacity in microvascular radiosensitivity. Journals of Gerontology Series A: Biomedical Sciences and Medical Sciences, 2013. 68(12): p. 1443-1457.
- VanElzakker, M.B. , et al., Neuroinflammation in post-acute sequelae of COVID-19 (PASC) as assessed by [11C]PBR28 PET correlates with vascular disease measures. Brain, Behavior, and Immunity, 2024. 119: p. 713-723.
- Shan, Z.Y. , et al., Neuroimaging characteristics of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): a systematic review. Journal of Translational Medicine, 2020. 18(1): p. 335.
- Ashktorab, H. , et al., Gastrointestinal Manifestations and Their Association with Neurologic and Sleep Problems in Long COVID-19 Minority Patients: A Prospective Follow-Up Study. Digestive Diseases and Sciences, 2024. 69(2): p. 562-569.
- Steinsvik, E.K. , et al., Gastric dysmotility and gastrointestinal symptoms in myalgic encephalomyelitis/chronic fatigue syndrome. Scandinavian Journal of Gastroenterology, 2023. 58(7): p. 718-725.
- Guo, C. , et al., Deficient butyrate-producing capacity in the gut microbiome is associated with bacterial network disturbances and fatigue symptoms in ME/CFS. Cell Host & Microbe, 2023. 31(2): p. 288-304.e8.
- Shukla, S.K. , et al., Changes in Gut and Plasma Microbiome following Exercise Challenge in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). PLOS ONE, 2015. 10(12): p. e0145453.
- Giloteaux, L. , et al., Reduced diversity and altered composition of the gut microbiome in individuals with myalgic encephalomyelitis/chronic fatigue syndrome. Microbiome, 2016. 4(1): p. 30.
- Liu, Q. , et al., Gut microbiota dynamics in a prospective cohort of patients with post-acute COVID-19 syndrome. Gut, 2022. 71(3): p. 544-552.
- Su, Q. , et al., The gut microbiome associates with phenotypic manifestations of post-acute COVID-19 syndrome. Cell Host & Microbe, 2024. 32(5): p. 651-660.e4.
- Martín, F. , et al., Increased gut permeability and bacterial translocation are associated with fibromyalgia and myalgic encephalomyelitis/chronic fatigue syndrome: implications for disease-related biomarker discovery. Frontiers in Immunology, 2023. 14.
- Mouchati, C. , et al., Increase in gut permeability and oxidized ldl is associated with post-acute sequelae of SARS-CoV-2. Frontiers in Immunology, 2023. 14.
- Stallmach, A. , et al., The gastrointestinal microbiota in the development of ME/CFS: a critical view and potential perspectives. Frontiers in Immunology, 2024. 15.
- Wang, J.-H. , et al., Clinical evidence of the link between gut microbiome and myalgic encephalomyelitis/chronic fatigue syndrome: a retrospective review. European Journal of Medical Research, 2024. 29(1): p. 148.
- Zollner, A. , et al., The Intestine in Acute and Long COVID: Pathophysiological Insights and Key Lessons. Yale J Biol Med, 2024. 97(4): p. 447-462.
- Liu, S., A. S. Devason, and M. Levy, From intestinal metabolites to the brain: Investigating the mysteries of Long COVID. Clin Transl Med, 2024. 14(3): p. e1608.
- Ke, Y. , et al., Gut flora-dependent metabolite Trimethylamine-N-oxide accelerates endothelial cell senescence and vascular aging through oxidative stress. Free Radical Biology and Medicine, 2018. 116: p. 88-100.
- Saeedi Saravi, S.S. , et al., Gut microbiota-dependent increase in phenylacetic acid induces endothelial cell senescence during aging. BioRxiv, 2023: p. 2023.11. 17.567594.
- Poole, D.C., B. J. Behnke, and T.I. Musch, The role of vascular function on exercise capacity in health and disease. The Journal of Physiology, 2021. 599(3): p. 889-910.
- Korthuis, R.J. , Exercise hyperemia and regulation of tissue oxygenation during muscular activity. Skeletal Muscle Circulation, 2011.
- Joseph, P. , et al., Insights From Invasive Cardiopulmonary Exercise Testing of Patients With Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. CHEST, 2021. 160(2): p. 642-651.
- Singh, I. , et al., Persistent Exertional Intolerance After COVID-19: Insights From Invasive Cardiopulmonary Exercise Testing. Chest, 2022. 161(1): p. 54-63.
- Bertinat, R. , et al., Decreased NO production in endothelial cells exposed to plasma from ME/CFS patients. Vascular Pharmacology, 2022. 143: p. 106953.
- Barrett-O'Keefe, Z. , et al., Taming the "sleeping giant": the role of endothelin-1 in the regulation of skeletal muscle blood flow and arterial blood pressure during exercise. Am J Physiol Heart Circ Physiol, 2013. 304(1): p. H162-9.
- Rapoport, R.M. and D. Merkus, Endothelin-1 Regulation of Exercise-Induced Changes in Flow: Dynamic Regulation of Vascular Tone. Frontiers in Pharmacology, 2017. 8.
- Wray, D.W. , et al., Endothelin-1-mediated vasoconstriction at rest and during dynamic exercise in healthy humans. American Journal of Physiology-Heart and Circulatory Physiology, 2007. 293(4): p. H2550-H2556.
- Bevan, G.H. , et al., Endothelin-1 and peak oxygen consumption in patients with heart failure with preserved ejection fraction. Heart & Lung, 2021. 50(3): p. 442-446.
- Liu, S.-Y. , et al., Endothelin-1 impairs skeletal muscle myogenesis and development via ETB receptors and p38 MAPK signaling pathway. Clinical Science, 2024. 138(12): p. 711-723.
- Tsai, C.H. , et al., Endothelin-1-mediated miR-let-7g-5p triggers interlukin-6 and TNF-α to cause myopathy and chronic adipose inflammation in elderly patients with diabetes mellitus. Aging (Albany NY), 2022. 14(8): p. 3633-3651.
- Horinouchi, T. , et al., Endothelin-1 suppresses insulin-stimulated Akt phosphorylation and glucose uptake via GPCR kinase 2 in skeletal muscle cells. British Journal of Pharmacology, 2016. 173(6): p. 1018-1032.
- Alcalde-Estévez, E. , et al., Endothelin-1 induces cellular senescence and fibrosis in cultured myoblasts. A potential mechanism of aging-related sarcopenia. Aging (Albany NY), 2020. 12(12): p. 11200-11223.
- Liu, Z. , et al., Increased circulating fibronectin, depletion of natural IgM and heightened EBV, HSV-1 reactivation in ME/CFS and long COVID. medRxiv, 2023.
- Aschman, T. , et al., Post-COVID exercise intolerance is associated with capillary alterations and immune dysregulations in skeletal muscles. Acta Neuropathol Commun, 2023. 11(1): p. 193.
- Hejbøl, E.K. , et al., Myopathy as a cause of fatigue in long-term post-COVID-19 symptoms: Evidence of skeletal muscle histopathology. Eur J Neurol, 2022. 29(9): p. 2832-2841.
- Rahman, F.A. and M.P. Krause, PAI-1, the Plasminogen System, and Skeletal Muscle. International Journal of Molecular Sciences, 2020. 21(19): p. 7066.
- Young, L.V. , et al., Loss of dystrophin expression in skeletal muscle is associated with senescence of macrophages and endothelial cells. American Journal of Physiology-Cell Physiology, 2021. 321(1): p. C94-C103.
- Sugihara, H. , et al., Cellular senescence-mediated exacerbation of Duchenne muscular dystrophy. Sci Rep, 2020. 10(1): p. 16385.
- Berenjabad, N.J., V. Nejati, and J. Rezaie, Angiogenic ability of human endothelial cells was decreased following senescence induction with hydrogen peroxide: possible role of vegfr-2/akt-1 signaling pathway. BMC Mol Cell Biol, 2022. 23(1): p. 31.
- Dinulovic, I., R. Furrer, and C. Handschin, Plasticity of the Muscle Stem Cell Microenvironment. Adv Exp Med Biol, 2017. 1041: p. 141-169.
- Christov, C. , et al., Muscle Satellite Cells and Endothelial Cells: Close Neighbors and Privileged Partners. Molecular Biology of the Cell, 2007. 18(4): p. 1397-1409.
- Mierzejewski, B. , et al., miRNA-126a plays important role in myoblast and endothelial cell interaction. Scientific Reports, 2023. 13(1): p. 15046.
- Keller, B. , et al., Cardiopulmonary and metabolic responses during a 2-day CPET in myalgic encephalomyelitis/chronic fatigue syndrome: translating reduced oxygen consumption to impairment status to treatment considerations. Journal of Translational Medicine, 2024. 22(1): p. 627.
- van Campen, C.M.C. and F.C. Visser, Comparing Idiopathic Chronic Fatigue and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) in Males: Response to Two-Day Cardiopulmonary Exercise Testing Protocol. Healthcare, 2021. 9(6): p. 683.
- Pretorius, E. , et al., Acute induction of anomalous and amyloidogenic blood clotting by molecular amplification of highly substoichiometric levels of bacterial lipopolysaccharide. J R Soc Interface, 2016. 13(122).
- Pretorius, E. , et al., Both lipopolysaccharide and lipoteichoic acids potently induce anomalous fibrin amyloid formation: assessment with novel Amytracker™ stains†. Journal of The Royal Society Interface, 2018. 15(139): p. 20170941.
- Kell, D.B. and E. Pretorius, Proteins behaving badly. Substoichiometric molecular control and amplification of the initiation and nature of amyloid fibril formation: lessons from and for blood clotting. Prog Biophys Mol Biol, 2017. 123: p. 16-41.
- Ryu, J.K. , et al., SARS-CoV-2 spike protein induces abnormal inflammatory blood clots neutralized by fibrin immunotherapy. biorxiv, 2021: p. 2021.10. 12.464152.
- Bonilla, H. , et al., Comparative analysis of extracellular vesicles in patients with severe and mild myalgic encephalomyelitis/chronic fatigue syndrome. Frontiers in Immunology, 2022. 13: p. 841910.
- Jahanbani, F. , et al., Phenotypic characteristics of peripheral immune cells of Myalgic encephalomyelitis/chronic fatigue syndrome via transmission electron microscopy: A pilot study. PloS One, 2022. 17(8): p. e0272703.
- Bochenek, M.L. , et al., The endothelial tumor suppressor p53 is essential for venous thrombus formation in aged mice. Blood Advances, 2018. 2(11): p. 1300-1314.
- Valenzuela, C.A. , et al., SASP-Dependent Interactions between Senescent Cells and Platelets Modulate Migration and Invasion of Cancer Cells. Int J Mol Sci, 2019. 20(21).
- Venturini, W. , et al., Platelet Activation Is Triggered by Factors Secreted by Senescent Endothelial HMEC-1 Cells In Vitro. Int J Mol Sci, 2020. 21(9).
- Ma, S. , et al., Vascular Aging and Atherosclerosis: A Perspective on Aging. Aging Dis, 2024. 16(1): p. 33-48.
- Silva, G.C. , et al., Replicative senescence promotes prothrombotic responses in endothelial cells: Role of NADPH oxidase- and cyclooxygenase-derived oxidative stress. Experimental Gerontology, 2017. 93: p. 7-15.
- Khan, S.Y. , et al., Premature senescence of endothelial cells upon chronic exposure to TNFα can be prevented by N-acetyl cysteine and plumericin. Sci Rep, 2017. 7: p. 39501.
- Abbas, M. , et al., Endothelial Microparticles From Acute Coronary Syndrome Patients Induce Premature Coronary Artery Endothelial Cell Aging and Thrombogenicity. Circulation, 2017. 135(3): p. 280-296.
- Bochenek, M.L., E. Schütz, and K. Schäfer, Endothelial cell senescence and thrombosis: Ageing clots. Thrombosis Research, 2016. 147: p. 36-45.
- Sepúlveda, C., I. Palomo, and E. Fuentes, Mechanisms of endothelial dysfunction during aging: Predisposition to thrombosis. Mechanisms of Ageing and Development, 2017. 164: p. 91-99.
- Mas-Bargues, C., C. Borrás, and M. Alique, The contribution of extracellular vesicles from senescent endothelial and vascular smooth muscle cells to vascular calcification. Frontiers in Cardiovascular Medicine, 2022. 9: p. 854726.
- Mørk, M. , et al., Elevated blood plasma levels of tissue factor-bearing extracellular vesicles in patients with atrial fibrillation. Thrombosis Research, 2019. 173: p. 141-150.
- Kruger, A. , et al., Proteomics of fibrin amyloid microclots in long COVID/post-acute sequelae of COVID-19 (PASC) shows many entrapped pro-inflammatory molecules that may also contribute to a failed fibrinolytic system. Cardiovascular Diabetology, 2022. 21(1): p. 190.
- Rubin, O. , et al., Microparticles in stored red blood cells: submicron clotting bombs? Blood Transfus, 2010. 8 Suppl 3(Suppl 3): p. s31-8.
- Schuermans, S., C. Kestens, and P.E. Marques, Systemic mechanisms of necrotic cell debris clearance. Cell Death & Disease, 2024. 15(8): p. 557.
- Walton, C.C. , et al., Senescence as an Amyloid Cascade: The Amyloid Senescence Hypothesis. Front Cell Neurosci, 2020. 14: p. 129.
- Li, R. , et al., Alzheimer’s Amyloid-β Accelerates Cell Senescence and Suppresses SIRT1 in Human Neural Stem Cells. Biomolecules, 2024. 14(2): p. 189.
- Flanary, B.E. , et al., Evidence That Aging And Amyloid Promote Microglial Cell Senescence. Rejuvenation Research, 2007. 10(1): p. 61-74.
- Grobbelaar, Lize M., et al., SARS-CoV-2 spike protein S1 induces fibrin(ogen) resistant to fibrinolysis: implications for microclot formation in COVID-19. Bioscience Reports, 2021. 41(8).
- Lopez-Vilchez, I. , et al., Tissue factor-enriched vesicles are taken up by platelets and induce platelet aggregation in the presence of factor VIIa. Thromb Haemost, 2007. 97(2): p. 202-11.
- Tabachnikova, A. , et al., The Role of Epstein-Barr Virus in Long COVID. The Journal of Immunology, 2024. 212(1_Supplement): p. 1121_6087-1121_6087.
- Vojdani, A. , et al., Reactivation of herpesvirus type 6 and IgA/IgM-mediated responses to activin-A underpin long COVID, including affective symptoms and chronic fatigue syndrome. Acta Neuropsychiatrica, 2024. 36(3): p. 172-184.
- Chen, Y.-L. , et al., The Epstein-Barr virus replication and transcription activator, Rta/BRLF1, induces cellular senescence in epithelial cells. Cell Cycle, 2009. 8(1): p. 58-65.
- Huang, W., L. Bai, and H. Tang, Epstein-Barr virus infection: the micro and macro worlds. Virology Journal, 2023. 20(1): p. 220.
- Ou, H.-L. , et al., Cellular senescence in cancer: from mechanisms to detection. Molecular Oncology, 2021. 15(10): p. 2634-2671.
- García-Fleitas, J. , et al., Chemical Strategies for the Detection and Elimination of Senescent Cells. Accounts of Chemical Research, 2024. 57(9): p. 1238-1253.
- Neri, F. , et al., A Fully-Automated Senescence Test (FAST) for the high-throughput quantification of senescence-associated markers. GeroScience, 2024. 46(5): p. 4185-4202.
- Veroutis, D. , et al., Senescent cells in giant cell arteritis display an inflammatory phenotype participating in tissue injury via IL-6-dependent pathways. Annals of the Rheumatic Diseases, 2024. 83(3): p. 342-350.
- Lagoumtzi, S.M. and N. Chondrogianni, Senolytics and senomorphics: Natural and synthetic therapeutics in the treatment of aging and chronic diseases. Free Radical Biology and Medicine, 2021. 171: p. 169-190.
- Chaib, S., T. Tchkonia, and J.L. Kirkland, Cellular senescence and senolytics: the path to the clinic. Nature medicine, 2022. 28(8): p. 1556-1568.
- Zhang, L. , et al., Targeting cellular senescence with senotherapeutics: senolytics and senomorphics. The FEBS journal, 2023. 290(5): p. 1362-1383.
- Aguado, J. , et al., Senolytic therapy alleviates physiological human brain aging and COVID-19 neuropathology. Nature Aging, 2023. 3(12): p. 1561-1575.
Figure 1.
Overview of the present hypothesis. Acute viral infections induce endothelial senescence via direct and indirect mechanisms, which is then sustained by immune dysfunction and impaired clearance of senescent endothelial cells. (EC – endothelial cell).
Figure 1.
Overview of the present hypothesis. Acute viral infections induce endothelial senescence via direct and indirect mechanisms, which is then sustained by immune dysfunction and impaired clearance of senescent endothelial cells. (EC – endothelial cell).
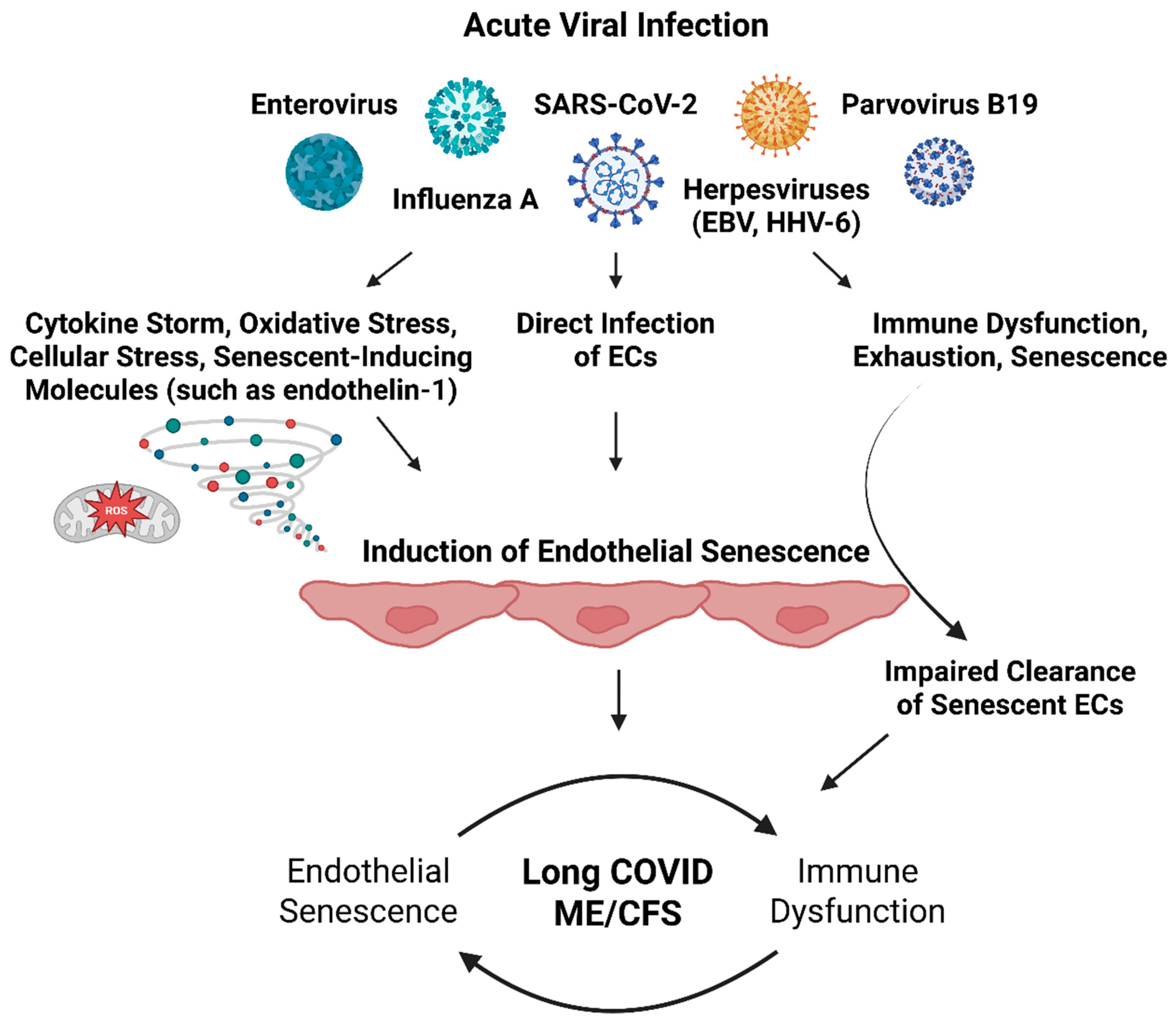
Figure 2.
The Senescence-Associated Secretory Phenotype (SASP) of Senescent Endothelial Cells. Senescent endothelial cells and their associated SASP is one that is proinflammatory, procoagulant, and prooxidative, and upregulates the expression of adhesion molecules, chemokines, and growth factors. Furthermore, and important to the findings of perturbed blood flow and perfusion deficits in long COVID and ME/CFS, the expression of vasomodulators is dysregulated in senescent endothelial cells, which predominantly manifests as a vasoconstriction effects and subsequent blood flow and perfusion deficits (uncoupling between ET-1 and NO).
Figure 2.
The Senescence-Associated Secretory Phenotype (SASP) of Senescent Endothelial Cells. Senescent endothelial cells and their associated SASP is one that is proinflammatory, procoagulant, and prooxidative, and upregulates the expression of adhesion molecules, chemokines, and growth factors. Furthermore, and important to the findings of perturbed blood flow and perfusion deficits in long COVID and ME/CFS, the expression of vasomodulators is dysregulated in senescent endothelial cells, which predominantly manifests as a vasoconstriction effects and subsequent blood flow and perfusion deficits (uncoupling between ET-1 and NO).
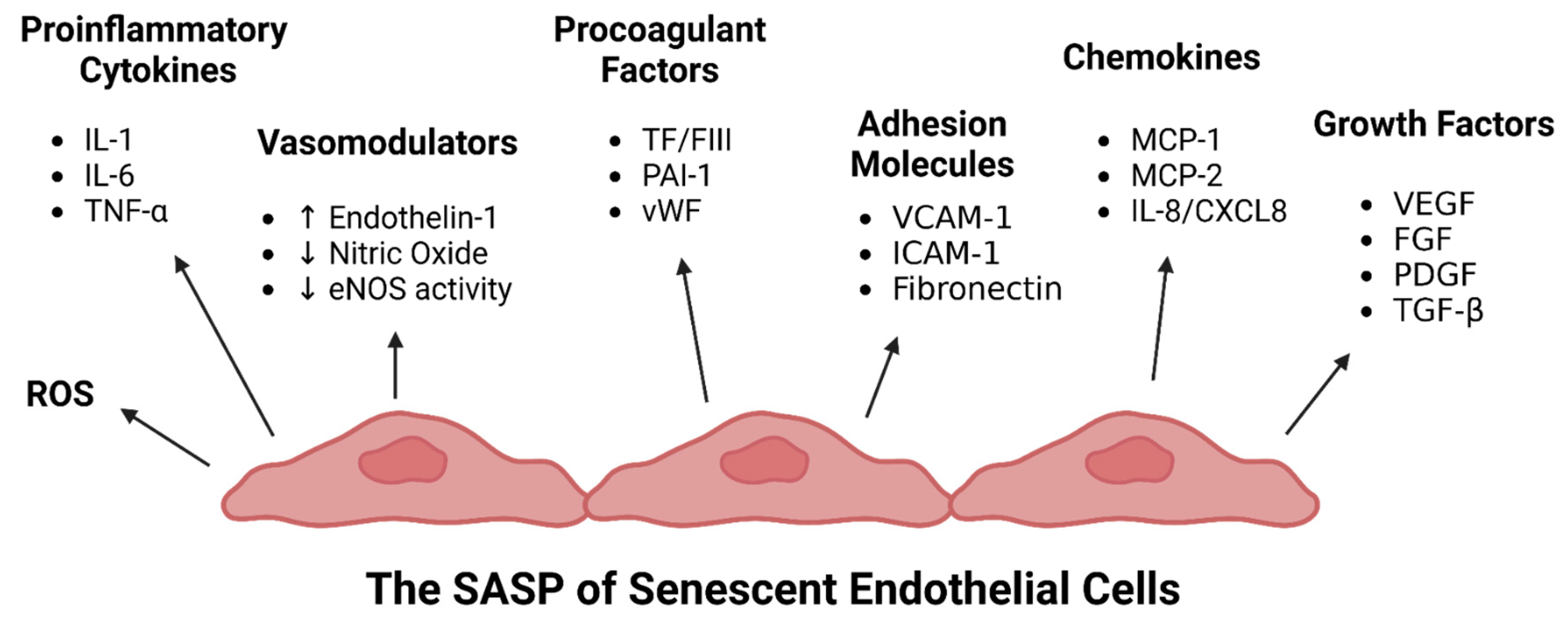
Figure 3.
Maintenance of Endothelial Senescence by Impaired Immune Function and Expression of HLA-E. Immune dysfunction including reduced NK cell cytotoxicity, impaired macrophage phagocytosis, dysregulated NETosis, and shortcomings in complement function – which, incidentally, are common features of ME/CFS and Long COVID – lead to ineffective clearance of senescent cells, enabling their persistence and expression of the SASP over long periods of time. In turn, the endothelial SASP exerts immunomodulatory effects that induce immune activation and recruitment, tissue infiltration, and leukocyte dysfunction and exhaustion, along with vasoconstriction effects, immunothrombosis, and impaired tissue healing and repair. Furthermore, senescent endothelial cells express HLA-E, which evades NK and CD8+ T-cell responses.
Figure 3.
Maintenance of Endothelial Senescence by Impaired Immune Function and Expression of HLA-E. Immune dysfunction including reduced NK cell cytotoxicity, impaired macrophage phagocytosis, dysregulated NETosis, and shortcomings in complement function – which, incidentally, are common features of ME/CFS and Long COVID – lead to ineffective clearance of senescent cells, enabling their persistence and expression of the SASP over long periods of time. In turn, the endothelial SASP exerts immunomodulatory effects that induce immune activation and recruitment, tissue infiltration, and leukocyte dysfunction and exhaustion, along with vasoconstriction effects, immunothrombosis, and impaired tissue healing and repair. Furthermore, senescent endothelial cells express HLA-E, which evades NK and CD8+ T-cell responses.
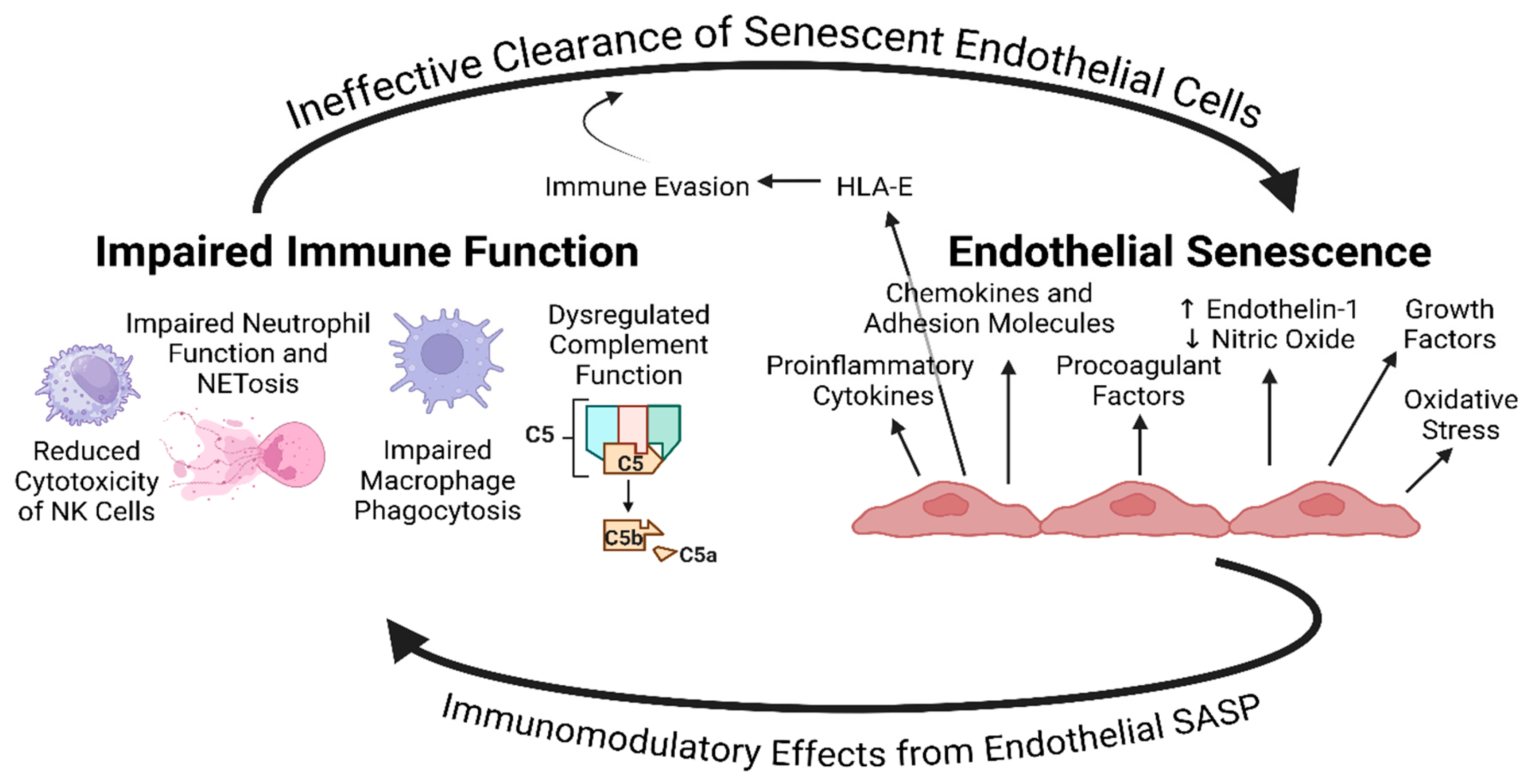
Figure 4.
Effects of Endothelial Senescence on Skeletal Muscle Tissue. Uncoupling between perfusion requirements and blood flow, as well as basement membrane thickening impeding the diffusion barrier, are primary to molecular and cellular dysregulation at tissues. In theory, the resulting oxygenation deficit could lead to local hypoxia, as well as the accumulation of waste products upon exercise. Combined with immune impairments, this may result in further disruptions of the structural and functional integrity of skeletal muscle tissue. The senescent immune environment may additionally inhibit skeletal muscle regeneration upon injury, via elevated levels of ET-1 and PAI-1, impairing various steps of myogenesis.
Figure 4.
Effects of Endothelial Senescence on Skeletal Muscle Tissue. Uncoupling between perfusion requirements and blood flow, as well as basement membrane thickening impeding the diffusion barrier, are primary to molecular and cellular dysregulation at tissues. In theory, the resulting oxygenation deficit could lead to local hypoxia, as well as the accumulation of waste products upon exercise. Combined with immune impairments, this may result in further disruptions of the structural and functional integrity of skeletal muscle tissue. The senescent immune environment may additionally inhibit skeletal muscle regeneration upon injury, via elevated levels of ET-1 and PAI-1, impairing various steps of myogenesis.
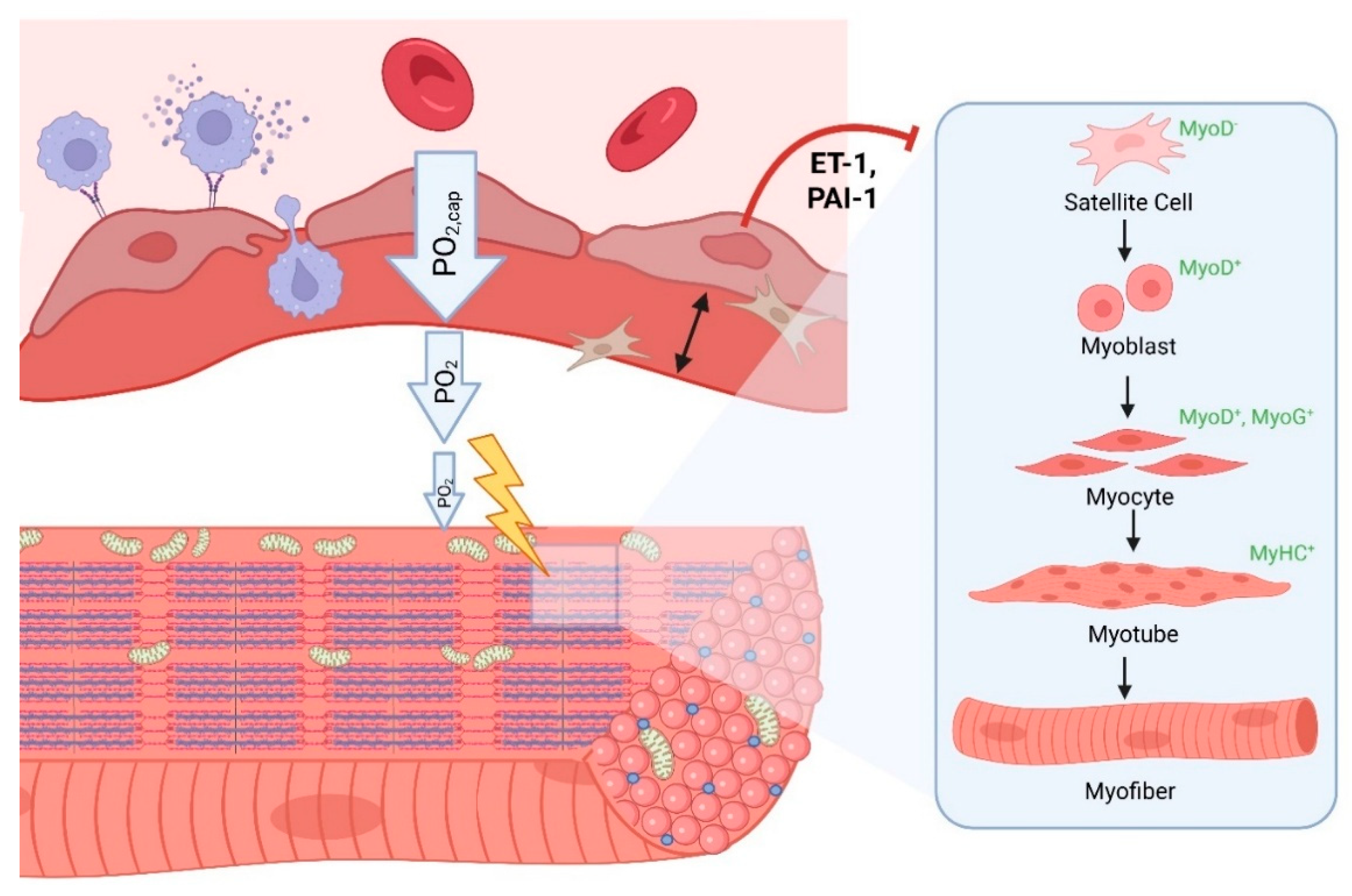
Figure 5.
Procoagulant Effects of the Endothelial SASP. Senescent endothelial cells adopt a procoagulant and proinflammatory phenotype, leading to platelet dysregulation, immunothrombosis, and heterogeneous fibrinaloid microclot formation. The inability of dysfunctional immune cells to efficiently clear accumulating cellular debris and fibrin in circulation provides ample scaffold upon which coagulation can occur leading to microclot formation and persistence. This persistence is further exacerbated by elevations in PAI-1 which hinders fibrinolysis.
Figure 5.
Procoagulant Effects of the Endothelial SASP. Senescent endothelial cells adopt a procoagulant and proinflammatory phenotype, leading to platelet dysregulation, immunothrombosis, and heterogeneous fibrinaloid microclot formation. The inability of dysfunctional immune cells to efficiently clear accumulating cellular debris and fibrin in circulation provides ample scaffold upon which coagulation can occur leading to microclot formation and persistence. This persistence is further exacerbated by elevations in PAI-1 which hinders fibrinolysis.
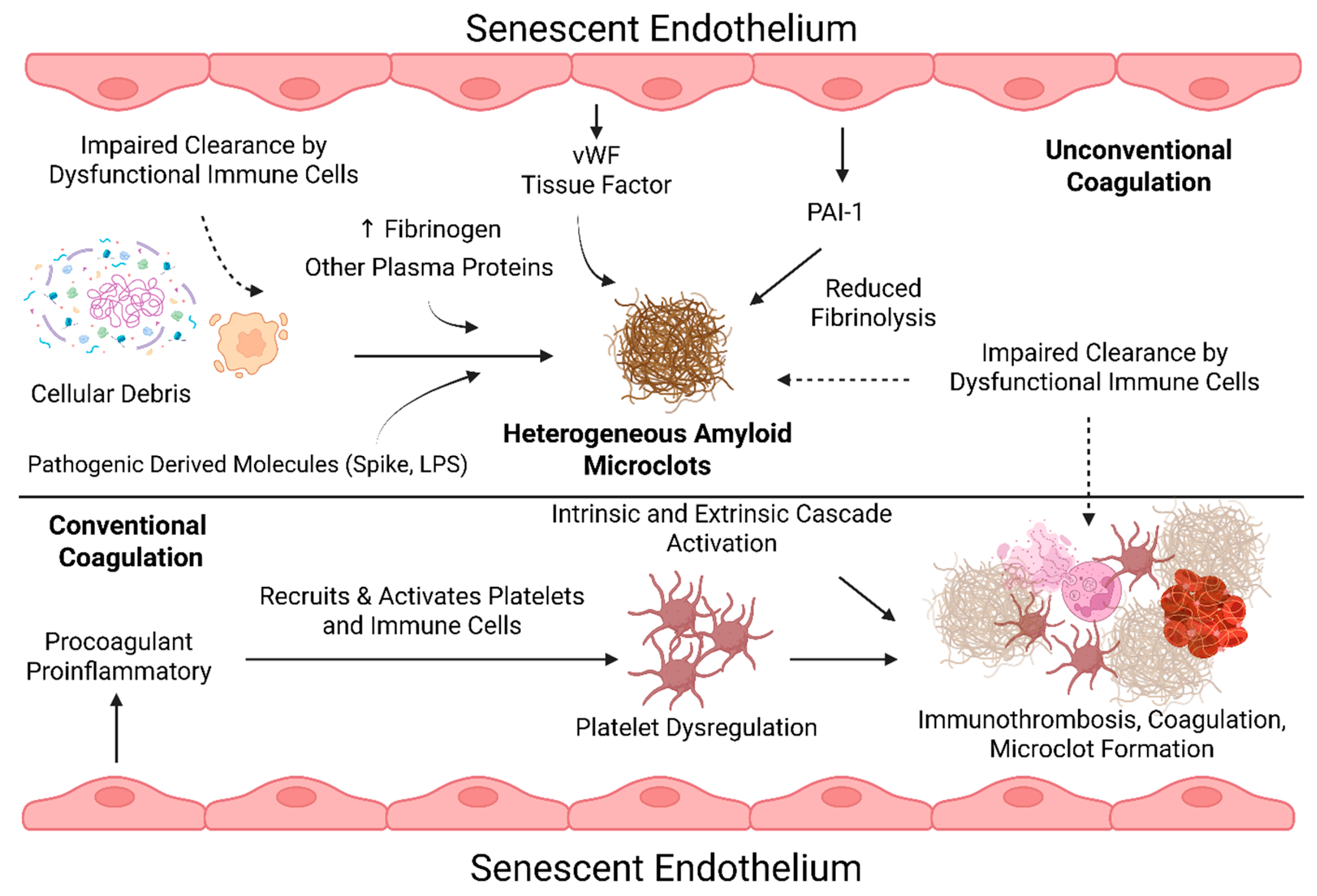
Figure 6.
Summary of disease induction and maintenance with a focus on endothelial senescence, as well as its relation to symptom manifestation in long COVID and ME/CFS.
Figure 6.
Summary of disease induction and maintenance with a focus on endothelial senescence, as well as its relation to symptom manifestation in long COVID and ME/CFS.
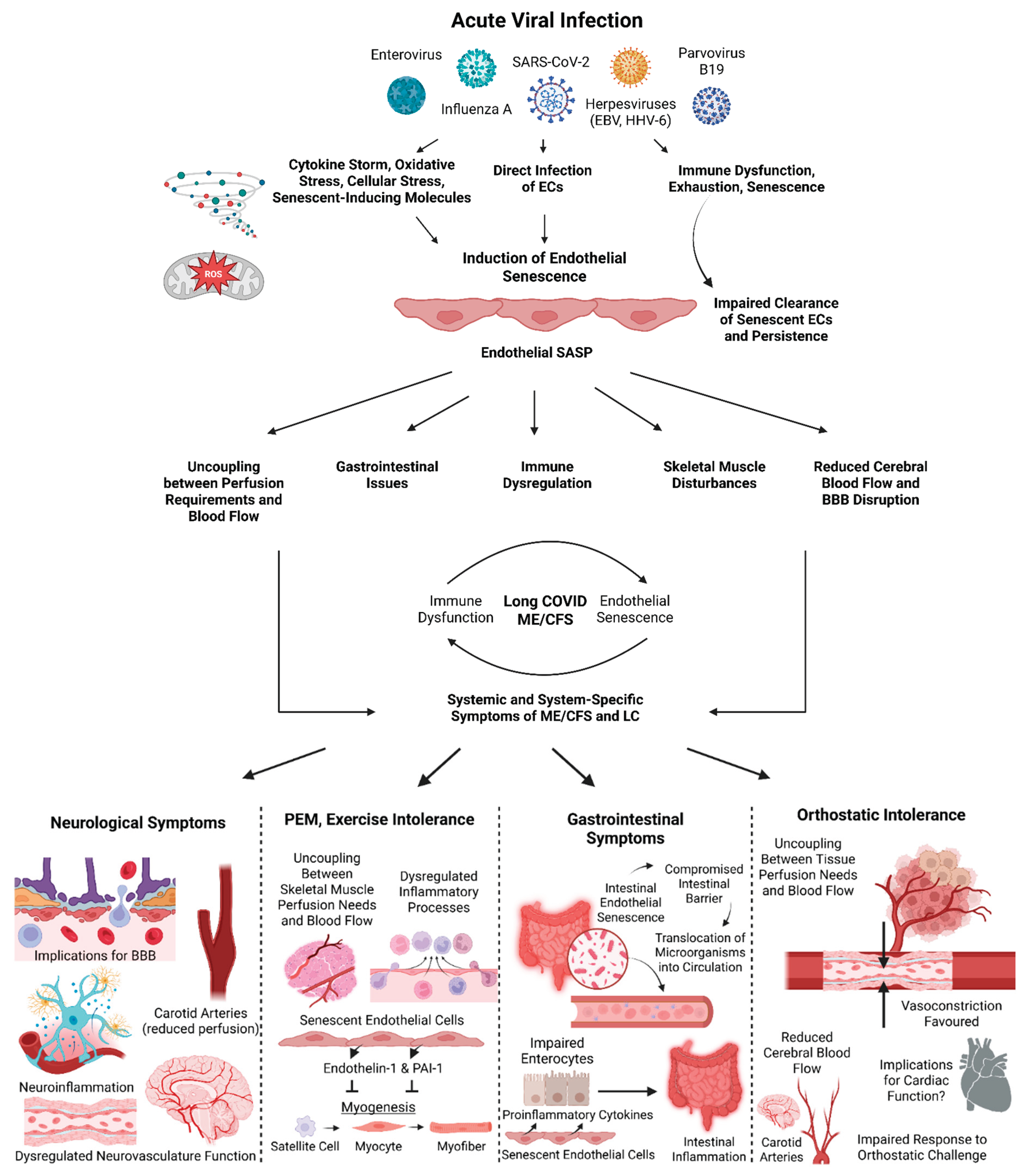

Table 1.
Evidence of SARS-CoV-2 and other viruses implicated in ME/CFS in causing endothelial dysfunction, direct infection, and induction of specifically endothelial senescence. References are included as a directory to the studies that demonstrate such evidence. While we are focusing solely on endothelial cells, it deserves mentioning that there is evidence, albeit not cited here, of senescence induction in non-endothelial cells for these viruses.
Table 1.
Evidence of SARS-CoV-2 and other viruses implicated in ME/CFS in causing endothelial dysfunction, direct infection, and induction of specifically endothelial senescence. References are included as a directory to the studies that demonstrate such evidence. While we are focusing solely on endothelial cells, it deserves mentioning that there is evidence, albeit not cited here, of senescence induction in non-endothelial cells for these viruses.
| Virus | Endothelial Dysfunction | Direct Endothelial Infection | Induction of Endothelial Senescence | Implicated in ME/CFS |
|---|---|---|---|---|
| SARS-CoV-2 | [38,51,104,114,115,116] | [117,118,119,120,121] | [104,105,106,122] | [4,7,8,9,123,124] |
| EBV | [63,125,126] | [125,127,128] | Unknown | [129,130,131,132] |
| HHV-6 | [63,133,134,135] | [134,135,136,137] | Unknown | [130,138] |
| Influenza A | [139,140,141,142,143] | [144,145,146] | [139,147] | [148,149] |
| Enteroviruses | [150,151,152,153] | [150,151,154,155,156,157] | Unknown | [158,159,160] |
| Parvovirus B19 | [156,161,162,163] | [164,165] | Unknown | [166,167,168,169] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



