Submitted:
22 May 2025
Posted:
25 May 2025
You are already at the latest version
Abstract
Background: Chronic pain is a significant global health issue, with conventional treatment strategies often proving insufficient or causing undesirable side effects. Interventional pain management techniques, including neuromodulation, have gained increasing interest as alternative therapeutic options. Cryoablation, a technique leveraging extreme cold to modulate pain pathways, has emerged as a promising tool in chronic pain management. However, its efficacy and role within current clinical practice remain under evaluation. Methods: A narrative review was conducted by searching PubMed, Scopus, Embase, and Web of Science databases for studies published between 2010 and 2024 using the keywords “Cryoneurolysis,” “Cryoanalgesia,” “Cryoablation,” and “Chronic pain.” Only English‐language studies were included. Studies that examined intraoperative cryoablation or lacked statistical analyses (except case reports) were excluded. Results: A total of 55 studies were included: 4 randomized controlled trials (RCTs), 16 retrospective studies, 4 prospective observational studies, and 31 case reports or small case series. The studies displayed significant heterogeneity in patient selection, targeted nerves, procedural protocols, and follow‐up durations. While two RCTs demonstrated a significant pain reduction compared to control groups, other RCTs reported no significant improvement. Observational studies and case reports frequently reported positive outcomes, with some achieving complete pain relief. Cryoablation appears to be most effective in treating neuropathic pain, particularly in patients with peripheral nerve involvement. Conclusions: Cryoablation is a safe and promising technique for chronic pain management, particularly for selected neuropathic pain conditions. However, the current evidence is limited by study heterogeneity and a lack of high‐quality comparative trials. Further well‐designed randomized studies are necessary to define its long‐term efficacy and its potential role relative to other interventional pain therapies, such as radiofrequency ablation.
Keywords:
chronic pain
; neuromodulation
; spinal cord stimulation
; pulsed radiofrequency
; peripheral nerve stimulation
; deep brain stimulation
; pain management
; transcutaneous electrical nerve stimulation
; neuroplasticity
; interventional pain therapy
Introduction
Chronic pain is a global health concern that affects millions of people and imposes a significant burden on healthcare systems worldwide[1,2]. According to the International Association for the Study of Pain (IASP), it is defined as pain that persists or recurs for more than three months, often leading to a host of psychosocial, functional, and economic challenges[1,3]. Despite advancements in conventional medical management—including pharmacological interventions, physical therapy, and psychological support—many patients continue to experience intractable pain or are hindered by the side effects of long-term medication use. These limitations have spurred interest in interventional pain therapies and neuromodulation techniques, which target specific pathways within the nervous system to modulate nociceptive signal transmission. Within the broader field of neuromodulation, a variety of approaches have been investigated for their ability to provide safe and sustained pain relief while minimizing adverse effects. Spinal cord stimulation (SCS), peripheral nerve stimulation (PNS), dorsal root ganglion (DRG) stimulation, deep brain stimulation (DBS), and motor cortex stimulation (MCS) are among the better-known therapies; however, novel modalities continue to emerge[4]. One of the most intriguing recent advances is cryoneurolysis (or cryoanalgesia), which leverages the application of ultra-low temperatures, typically in the range of -70°C, to create a reversible conduction block in targeted peripheral nerves[5,6,7]. Unlike more traditional neurolytic procedures that rely on heat or chemical agents, cryoneurolysis preserves crucial connective tissues (e.g., the perineurium and epineurium), thereby reducing the likelihood of permanent damage while still providing meaningful analgesic effects. Cryoablation involves the use of a highly pressurized cooling gas (nitrous oxide or carbon dioxide) circulating through a sealed probe. As the gas expands, pressure drops decreasing the temperature and creating an ice ball at the tip, due to the Joule-Thomson effect[8]. Several factors influence the degree of analgesia obtainable with cryoneurolysis, specifically:
- the distance between the probe and target nerve;
- the cryoprobe diameter;
- the size of the resulting ice ball;
- the temperature of the immediately surrounding tissue (such as blood, which acts as a heat sink);
- the rate and duration of cold application. The latter two factors are highly dependent upon the gas flow rate and the number of ‘freeze cycles’ applied, usually with 2–3 min of freezing followed by 0.5–2 min of thawing.[9]
Clinical interest in cryoneurolysis has expanded considerably, fueled by its demonstrated efficacy in managing refractory pain conditions, as well as its favorable safety profile. Indeed, evidence suggests that cryoneurolysis can be applied to both sensory and mixed nerves for various chronic pain syndromes, providing meaningful relief without the risks associated with permanent nerve destruction or high-dose analgesics.[5,6] Additionally, advances in imaging guidance (e.g., ultrasound, fluoroscopy and computed tomography) have improved the accuracy of nerve localization, further enhancing procedure success and reducing complications. This narrative review aims to explore the evolving role of neuromodulation therapies, with a particular focus on cryoneurolysis and its potential to revolutionize chronic pain treatment. By examining principles, mechanisms, and clinical outcomes of cryoneurolysis across various chronic pain conditions, we hope to shed light on emerging best practices and inform the development of safer, more effective, and personalized interventions for individuals living with persistent pain.
Materials and Methods
We conducted a systematic search of PubMed, Embase, Web of Science and the Cochrane Library for studies
published between 2010 and 2025 examining the effects of cryoanalgesia on chronic pain.
Search terms included “Cryoneurolysis” “Cryoanalgesia” “Cryoablation” and “Chronic pain” ;. Boolean operators (AND, OR) were used to combine terms. The last search was conducted on 31 March 2025.
We checked clinicaltrial.gov and EUDRACT for trials in course on human.
We included randomized controlled trials, cohort studies and case reports that evaluated the effects Cryoanalgesia on Chronic pain.
Papers describing the application of cryoneurolysis during a surgical procedure (i.e. intraoperative application on the intercostal nerves for post thoracotomy pain) were excluded.
Papers which not reported a statistical analysis (apart from case reports) or simply described a study protocol were excluded from the analysis. Review and all studies not including novel data were excluded.
Only peer-reviewed articles published in English were included.
Papers were searched and screened according to PRISMA guidelines.
Results
We present the number of identified articles, those screened and those that fulfilled inclusion and exclusion criteria in the PRISMA flow chart (Figure 1)
After removing duplicates and excluded non relevant papers, 55 studies were identified within our search parameters.
4 of these studies were RCTs, 16 retrospective and 4 prospective observational studies, 31 were case reports or case series with less than 5 patients studied.
The included studies had very heterogeneous inclusion criteria (not all authors reported having performed a test block before cryoablation, nociceptive and neuropathic pain were not differentiated, different nerves were targeted).
Different devices were used with different protocols of treatment, not all authors reported details of the temperature and number of cycles performed.
Targets were different as studies focused on different anatomical regions and various nerves were treated. (see Figure 2).
The characteristics of included studies are summarized in Table 1.
In order to better define the effectiveness of cryoablation, we narrowed our analysis on studies reporting a 6 months follow-up or longer and including a clear definition of meaningful pain relief (>50% from baseline). We stated the outcome as positive if more than 50% of patients reported more than 50% pain relief from baseline.
Table 2 shows the studies fulfilling these criteria.
Discussion
Our analysis included 4 RCT’s, with different anatomical targets, only 2 of which reported a positive outcome with a better response in the treatment group versus the comparison (sham or steroid injections).
Regarding retrospective and prospective studies the results were overall stated as successful, however, most authors did not use a cutoff to define the success of the procedure, except for six studies who reported >50% pain relief at different follow up (generally less than six months), and one study with a success rate of 8% with a cutoff of only 30% pain relief. [18,21,25,26,27,29,30]
Most authors reported only a mean decrease in NRS scores, ranging from 2 to 4.2 points of reduction.
All case reports and case series reported positive results, often with 100% pain relief.
Given the great heterogeneity of the included studies, it is not possible to draw definite conclusion about the efficacy of cryoablation, however, the published evidence indicates a favorable outcome for this technique, at least in the short term, with an excellent safety profile.
Narrowing the analysis on studies with a follow up of at least 6 months or more we found 16 studies, of which 9 were case reports or case series with less than 5 patients treated (Table 2).
No recommendations can be given regarding the best anatomical targets, since studies are very heterogeneous regarding targeted nerves. The best results were reported by the RCT of Radnovich et al in 2017. The authors applied cryoablation on the saphenous nerve, reporting a successful outcome at 4 months in more than 80% patients. The saphenous nerve has been targeted (in its infrapatellar branch) by McLean who reported more than 50% pain relief in all 23 patients treated, even if only 4 of them reached a 6 months follow-up.[29]
A recent large study targeting the genicular nerves confirmed the positive outcomes associated with cryoablation, even if the percentage of patients with > 50 % pain relief was reported only at three months follow up.[33]
Cryoanalgesia application on the occipital, sciatic and medial branch nerves appears not to be supported by evidence since three RCTs reported no difference versus sham.[11,12,13]
It is worth noticing that despite the poor evidence of efficacy for cryoablation on chronic pain, several studies reported good outcomes for the application of the same technique for acute pain management, particularly for intercostal cryoablation to manage post thoracotomy acute pain.
Multiple reasons for this difference could be hypothesized, a more precise application on target nerves (given the direct visualization of nerves during thoracotomy or thoracoscopy), a more specific relation between the targeted nerves and the pain condition, a different pathophysiology of pain (marked central sensitization as in long lasting chronic pain could reduce the efficacy of peripherally focused neuromodulation techniques).
There are no reported comparisons of cryoablation with other interventional techniques, such as radiofrequency ablation, except for one RCT published in 2024, the authors did not report any improvement with cryoanalgesia compared to RF or placebo[11].
Even if this comparison is outside the scopes of this review, it must be observed that published evidence for radiofrequency ablation indicate generally more favorable outcomes for RF denervation compared to cryoablation.
For example, RF application for chronic knee, sacroiliac or shoulder pain can provide sustained pain relief in more than 50% of patients up to 12 months; such results have not been observed with cryoablation.
Interesting results have been reported with application of cryoablation for neuropathic pain. Yoon et al enrolled 22 patients for cryoneurolysis of refractory peripheral neuropathy on various nerves and showed significant mean reductions in VAS scores for pain over a 12-month period maintaining a 50% pain relief at 6 month follow-up.[16] Another study reported the effects of cryoneurolysis on three patients with recalcitrant neuropathic anterior femoral cutaneous nerve pain. [36] Pain relief of more than 80% was maintained 1 year after the intervention Lastly, a case report involving a refractory sural neuroma, with severe pain refractory to medications and repeated surgeries , reported significant and sustained pain relief after cryoablation[56].
Regarding adverse events, cryoablation can be considered a safe procedure. There are no reports of permanent nerve damage. The only contraindications are Reynaud syndrome, cryoglobulinemia and cold urticaria [8]. The risks of cryoanalgesia are similar to other needle-based percutaneous procedures and include bleeding, bruising and infection. Specific risks include permanent injury to the nerve, injury to the surrounding tissue and discoloration of the skin if the cannula is retracted prior to resolving the ice ball and allowed contact to other areas near the target site[8].
Myonecrosis after cryoablation for knee pain has been reported. It is not clear whether this complication was related to the procedure itself (the accidental transmission of nitrous oxide as a cooling gas into the tissue could increase the risk of infection) or to transmission of skin bacterias into deep tissue during the procedure.[68,69]
Conclusion
Cryoablation is a safe technique. Its efficacy in chronic pain has been demonstrated only in the short term (less than 6 months) follow up for various targets (saphenous nerve, sciatic, intercostal, suprascapular).
Given the paucity and low quality of the studies, it is not possible to give recommendations for the application of cryoablation for chronic pain.
More robust and well conducted studies are needed, to assess the intrinsic efficacy of cryoablation and to compare it to existing technologies, such as radiofrequency ablation.
Author Contributions
Conceptualization, A.T. and G.LB; methodology, A.T, M.M. and G.LB; software A.T, M.M, S.M, C.S. and G.LB, validation, A.T, M.M, S.M, C.S. and G.LB.; formal analysis, A.T, M.M, S.M, C.S. and G.LB; investigation, A.T, M.M, S.M, C.S. and G.LB; data curation, A.T, M.M, S.M, C.S. and G.LB; writing—original draft preparation, A.T, M.M, S.M, C.S. and G.LB.; writing—review and editing, A.T, M.M, S.M, C.S. and G.LB.; visualization, A.T, M.M, S.M, C.S. and G.LB; supervision, A.T AND G.LB. All authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding.
Acknowledgments
None
Conflicts of Interest
The authors declare no conflicts of interest
References
- Werner MU, Kongsgaard UE. I. Defining persistent post-surgical pain: is an update required? Br J Anaesth. 2014;113(1):1-4. [CrossRef]
- Cui A, Li H, Wang D, Zhong J, Chen Y, Lu H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine. 2020;29-30:100587. [CrossRef]
- Baker PN, Van Der Meulen JH, Lewsey J, Gregg PJ. The role of pain and function in determining patient satisfaction after total knee replacement: DATA FROM THE NATIONAL JOINT REGISTRY FOR ENGLAND AND WALES. J Bone Joint Surg Br. 2007;89-B(7):893-900. [CrossRef]
- Wylde V, Beswick A, Bruce J, Blom A, Howells N, Gooberman-Hill R. Chronic pain after total knee arthroplasty. EFORT Open Rev. 2018;3(8):461-470. [CrossRef]
- Panagopoulos A, Tsiplakos P, Katsanos K, Antzoulas P, Lakoumentas J. Cooled radiofrequency ablation versus cryoneurolysis of the genicular nerves for the symptomatic pain management in knee osteoarthritis: a study protocol of a prospective, randomized, single-blinded clinical trial. J Orthop Surg. 2023;18(1):295. [CrossRef]
- Slavin BR, Markowitz MI, Klifto KM, Prologo FJ, Taghioff SM, Dellon AL. Cryoanalgesia: Review with Respect to Peripheral Nerve. J Reconstr Microsurg. 2024;40(04):302-310. [CrossRef]
- Wong J, Bremer N, Weyker PD, Webb CAJ. Ultrasound-Guided Genicular Nerve Thermal Radiofrequency Ablation for Chronic Knee Pain. Case Rep Anesthesiol. 2016;2016:1-3. [CrossRef]
- Ilfeld BM, Finneran JJ. Cryoneurolysis and Percutaneous Peripheral Nerve Stimulation to Treat Acute Pain: A Narrative Review. Anesthesiology. 2020;133(5):1127-1149. [CrossRef]
- Ilfeld BM, Gabriel RA, Trescot AM. Ultrasound-guided percutaneous cryoneurolysis for treatment of acute pain: could cryoanalgesia replace continuous peripheral nerve blocks? Br J Anaesth. 2017;119(4):709-712. [CrossRef]
- Radnovich R, Scott D, Patel AT, et al. Cryoneurolysis to treat the pain and symptoms of knee osteoarthritis: a multicenter, randomized, double-blind, sham-controlled trial. Osteoarthritis Cartilage. 2017;25(8):1247-1256. [CrossRef]
- Truong K, Meier K, Ahrens LC, et al. Cryoneurolysis versus radiofrequency ablation outcome on pain experience in chronic low back pain (COPE): a single-blinded randomised controlled trial. RMD Open. 2024;10(2):e004196. [CrossRef]
- Ilfeld BM, Smith CR, Turan A, et al. Ultrasound-guided Percutaneous Cryoneurolysis to Treat Chronic Postamputation Phantom Limb Pain: A Multicenter Randomized Controlled Trial. Anesthesiology. 2023;138(1):82-97. [CrossRef]
- Kvarstein G, Högström H, Allen SM, Rosland JH. Cryoneurolysis for cervicogenic headache – a double blinded randomized controlled study. Scand J Pain. 2019;20(1):39-50. [CrossRef]
- Grigsby E, Radnovich R, Nalamachu S. Efficacy and Safety of Cryoneurolysis for Treatment of Chronic Head Pain Secondary to Occipital Neuralgia: A Pilot Study. Local Reg Anesth. 2021;Volume 14:125-132. [CrossRef]
- Perry TA, Segal NA. An open-label, single-arm trial of cryoneurolysis for improvements in pain, activities of daily living and quality of life in patients with symptomatic ankle osteoarthritis. Osteoarthr Cartil Open. 2022;4(3):100272. [CrossRef]
- Yoon JHE, Grechushkin V, Chaudhry A, Bhattacharji P, Durkin B, Moore W. Cryoneurolysis in Patients with Refractory Chronic Peripheral Neuropathic Pain. J Vasc Interv Radiol. 2016;27(2):239-243. [CrossRef]
- Zhan C, Yoon J, Baghai Kermani A, Gupta A, Moore W. Abstract No. 587 Safety and efficacy of computed tomography–guided percutaneous cryoneurolysis for chronic intercostal pain syndrome. J Vasc Interv Radiol. 2020;31(3):S256. [CrossRef]
- Das G, Das S, Sahoo R, Shreyas S, Kanthi B, Sharma VS. Efficacy of cryoneurolysis versus intra-articular steroid in sacroiliac joint pain: A retrospective, case-control study. Indian J Anaesth. 2023;67(11):1004-1008. [CrossRef]
- Sidebottom AJ, Carey EC, Madahar AK. Cryoanalgesia in the management of intractable pain in the temporomandibular joint: a five-year retrospective review. Br J Oral Maxillofac Surg. 2011;49(8):653-656. [CrossRef]
- Prologo JD, Gilliland CA, Miller M, et al. Percutaneous Image-Guided Cryoablation for the Treatment of Phantom Limb Pain in Amputees: A Pilot Study. J Vasc Interv Radiol. 2017;28(1):24-34.e4. [CrossRef]
- Department of Radiology, University of Missouri Columbia, One Hospital Drive, Columbia, United States, University of Missouri Columbia School of Medicine, One Hospital Drive, Columbia, United States, Yasin J, et al. CT-guided cryoablation for post-thoracotomy pain syndrome: a retrospective analysis. Diagn Interv Radiol. 2020;26(1):53-57. [CrossRef]
- Moore W, Kolnick D, Tan J, Yu HS. CT Guided Percutaneous Cryoneurolysis for Post Thoracotomy Pain Syndrome. Acad Radiol. 2010;17(5):603-606. [CrossRef]
- Wolter T, Deininger M, Hubbe U, Mohadjer M, Knoeller S. Cryoneurolysis for zygapophyseal joint pain: a retrospective analysis of 117 interventions. Acta Neurochir (Wien). 2011;153(5):1011-1019. [CrossRef]
- Kim CH, Hu W, Gao J, Dragan K, Whealton T, Julian C. Cryoablation for the treatment of occipital neuralgia. Pain Physician. 2015;18(3):E363-368.
- Nemecek Z, Sturm C, Rauen AC, Reisig F, Streitberger K, Harnik MA. Ultrasound-Controlled Cryoneurolysis for Peripheral Mononeuropathies: A Retrospective Cohort Study. Pain Manag. 2023;13(6):363-372. [CrossRef]
- Parekattil S, Gudeloglu A, Ergun O, Galante A, Etafy M, Mendelson R. MP31-10 A COST EFFECTIVE OFFICE BASED TECHNIQUE FOR ULTRASOUND GUIDED PERI-SPERMATIC CORD CRYOABLATION FOR CHRONIC SCROTAL CONTENT PAIN. J Urol. 2021;206(Supplement 3). [CrossRef]
- Tinnirello A. Genicular nerves ablation for chronic knee pain: A single-center retrospective evaluation comparing four ablation modalities. Pain Pract. 2020;20(S1):7-95. [CrossRef]
- Nezami N, Behi A, Manyapu S, et al. Percutaneous CT-Guided Cryoneurolysis of the Intercostobrachial Nerve for Management of Postmastectomy Pain Syndrome. J Vasc Interv Radiol. 2023;34(5):807-813. [CrossRef]
- McLean BC, Nguyen CD, Newman DP. Cryoablation of the Infrapatellar Branch of the Saphenous Nerve Identified by Non-Invasive Peripheral Nerve Stimulator for the Treatment of Non-Surgical Anterior Knee Pain: A Case Series and Review of the Literature. Cureus. Published online June 21, 2020. [CrossRef]
- Calixte N, Kartal IG, Tojuola B, et al. Salvage Ultrasound-guided Targeted Cryoablation of The Perispermatic Cord For Persistent Chronic Scrotal Content Pain After Microsurgical Denervation Of The Spermatic Cord. Urology. 2019;130:181-185. [CrossRef]
- Bellini M, Barbieri M. Percutaneous cryoanalgesia in pain management: a case-series. Anestezjol Intensywna Ter. 2015;47(2):131-133. [CrossRef]
- Prologo J, Mittal A, Knight J, Hsu D, Dolan R, Com D. Percutaneous CT-guided cryoablation for the management of pudendal neuralgia: Long-Term outcomes. J Vasc Interv Radiol. 2018;29(4):S241-2.
- Bianco GL, D’angelo FP, Dos Santos GF, et al. Genicular Nerve Ultrasound-Guided Cryoanalgesia for the Treatment of Chronic Knee Joint Pain: An Observational Retrospective Study. Pain Ther. Published online March 27, 2025. [CrossRef]
- Filipovski I, Gabriel RA, Kestenholz R. Ultrasound-Guided Cryoneurolysis for the Treatment of Painful Diabetic Neuropathy of the Foot: A Case Series. Cureus. Published online March 16, 2024. [CrossRef]
- Stogicza AR, Peng P. Cryoanalgesia for shoulder pain: a motor-sparing approach to rotator cuff disease. Reg Anesth Pain Med. 2022;47(9):576-580. [CrossRef]
- Dalili D, Ahlawat S, Rashidi A, Belzberg AJ, Fritz J. Cryoanalgesia of the anterior femoral cutaneous nerve (AFCN) for the treatment of neuropathy-mediated anterior thigh pain: anatomy and technical description. Skeletal Radiol. 2021;50(6):1227-1236. [CrossRef]
- Moesker AA, Karl HW, Trescot AM. Treatment of Phantom Limb Pain by Cryoneurolysis of the Amputated Nerve. Pain Pract. 2014;14(1):52-56. [CrossRef]
- Sahoo RK, Das G, Pathak L, Dutta D, Roy C, Bhatia A. Cryoneurolysis of Innervation to Sacroiliac Joints: Technical Description and Initial Results—A Case Series. AA Pract. 2021;15(4):e01427. [CrossRef]
- Mendes-Andrade I, Pagan-Rosado R, Ferreira-Silva N, Hurdle MF. A novel approach to refractory coccydynia: ultrasound- fluoroscopy-guided cryoablation of sacrococcygeal nerve. Pain Manag. 2024;14(10-11):541-547. [CrossRef]
- Shaffer JP, Williams VB, Shin SS. Cryoneurolysis for Digital Neuralgia in Professional Baseball Players: A Case Series. Orthop J Sports Med. 2022;10(5):23259671221096095. [CrossRef]
- Gabriel RA, Kestenholz R, Filipovski I. Repeated Ultrasound-Guided Percutaneous Intercostal Cryoneurolysis for the Management of Chronic Postmastectomy Pain Syndrome: A Case Report. AA Pract. 2024;18(3):e01764. [CrossRef]
- Cachemaille M, Geering S, Broome M. Cryoneurolysis of alveolar nerves for chronic dental pain: A new technique and a case series. Pain Pract. 2023;23(7):851-854. [CrossRef]
- Kočan L, Rapčan R, Sudzina R, et al. Radiofrequency denervation and cryoablation of the lumbar zygapophysial joints in the treatment of positive lumbar facet joint syndrome – a report of three cases. Radiol Case Rep. 2022;17(12):4515-4520. [CrossRef]
- Connelly NR, Malik A, Madabushi L, Gibson C. Use of ultrasound-guided cryotherapy for the management of chronic pain states. J Clin Anesth. 2013;25(8):634-636. [CrossRef]
- Matelich B, Berg A, Habeck J, Hutchins J. B32 Ultrasound-guided cryoneurolysis of the supra scapular nerve for chronic shoulder pain: a case series. In: Ultrasound Guided RA (UGRA). BMJ Publishing Group Ltd; 2022:A99.1-A99. [CrossRef]
- Fox S. Pudendal nerve cryoablation for chronic pelvic pain. Dis Colon Rectum. 2019;62(6):e39-e401. [CrossRef]
- Sarridou D, Papadopoulou D, Paraskevopoulos T, Stavropoulou E. Successful treatment of complex regional pain syndrome type 1 of upper limb with cryoneurolysis of the stellate ganglion: A rare case report. Pain Pract. 2022;22(2):285-287. [CrossRef]
- Ramsook R, Spinner D. (468) Cryoablation of a hip disarticulation residual limb neuroma allowing for ambulation and pain relief: a case report. J Pain. 2016;17(4):S91. [CrossRef]
- Joshi DH, Thawait GK, Del Grande F, Fritz J. MRI-guided cryoablation of the posterior femoral cutaneous nerve for the treatment of neuropathy-mediated sitting pain. Skeletal Radiol. 2017;46(7):983-987. [CrossRef]
- Kalava A, Pham K, Okon S. Cryoneurolysis of the Subcostal Nerve: A Technical Description and Case Report. Cureus. Published online April 3, 2024. [CrossRef]
- Sen S, De Haan JB, Mehrafza M, Hernandez N. Ultrasound-Guided Percutaneous Intercostal Cryoneurolysis for Acute-on-Chronic Pain in CLOVES Syndrome. Cureus. Published online January 22, 2023. [CrossRef]
- Jung EY, Lee SS. Treatment of chronic mini-thoracotomy wound pain and lung herniation with intercostal cryoablation and surgical mesh repair: a case report. J Cardiothorac Surg. 2024;19(1):348. [CrossRef]
- MacRae F, Speirs A, Bursuc A, Hashemi M, Winston P. A Case Report of Cryoneurolysis for Dorsal Foot Pain and Toe Clawing in a Patient With Multiple Sclerosis. Arch Rehabil Res Clin Transl. 2023;5(3):100286. [CrossRef]
- Perese J, Oswald J, Gabriel RA. Ultrasound-Guided Percutaneous Cryoneurolysis for Post-Thoracotomy Pain Syndrome: A Case Report. Cureus. Published online December 23, 2022. [CrossRef]
- Koethe Y, Mannes AJ, Wood BJ. Image-guided Nerve Cryoablation for Post-thoracotomy Pain Syndrome. Cardiovasc Intervent Radiol. 2014;37(3):843-846. [CrossRef]
- Rhame EE, DeBonet AF, Simopoulos TT. Ultrasonographic Guidance and Characterization of Cryoanalgesic Lesions in Treating a Case of Refractory Sural Neuroma. Case Rep Anesthesiol. 2011;2011:1-4. [CrossRef]
- MacRae F, Boissonnault E, Hashemi M, Winston P. Bilateral Suprascapular Nerve Cryoneurolysis for Pain Associated With Glenohumeral Osteoarthritis: A Case Report. Arch Rehabil Res Clin Transl. 2023;5(1):100256. [CrossRef]
- Weber G, Saad K, Awad M, Wong TH. Case Report Of Cryoneurolysis For The Treatment Of Refractory Intercostobrachial Neuralgia With Postherpetic Neuralgia. Local Reg Anesth. 2019;Volume 12:103-107. [CrossRef]
- Yarmohammadi H, Nakamoto D, Azar N, Hayek S, Haaga J. Percutaneous computed tomography guided cryoablation of the celiac plexus as an alternative treatment for intractable pain caused by pancreatic cancer. J Cancer Res Ther. 2011;7(4):481. [CrossRef]
- Rupp A, Panchang P, Smith M. A case report of cryoablation for chronic shoulder pain due to osteoarthritis. Interv Pain Med. 2022;1(4):100146. [CrossRef]
- Kalava A, Kassie R, Borick E. Cryoneurolysis of Intercostal Nerves for Postherpetic Neuralgia: A Case Report. Cureus. Published online September 30, 2024. [CrossRef]
- Hampton H, Kalava A. Ischiorectal Approach to Cryoablation of the Pudendal Nerve Using a Handheld Device: A Report of Two Cases. Cureus. Published online August 30, 2023. [CrossRef]
- Fiala M, Azariah A, Woo J, Aal AKA, Levey A. Treating phantom limb pain: cryoablation of the posterior tibial nerve. Radiol Case Rep. 2022;17(9):3168-3171. [CrossRef]
- Gabriel RA, Finneran JJ, Trescot AM, Ilfeld BM. Ultrasound-Guided Percutaneous Cryoneurolysis for Postoperative Analgesia After Limb Amputation: A Case Series. AA Pract. 2019;12(7):231-234. [CrossRef]
- Davis T, Loudermilk E, DePalma M, et al. Twelve-month analgesia and rescue, by cooled radiofrequency ablation treatment of osteoarthritic knee pain: results from a prospective, multicenter, randomized, cross-over trial. Reg Anesth Pain Med. 2019;44(4):499-506. [CrossRef]
- Santi C, Haag T, Cooke C, Schatman M, Tinnirello A. Two-Centre Retrospective Analysis on Selective Sensory Denervation of Shoulder Joint by Means of Cooled Radiofrequency in Chronic Shoulder Pain. J Pain Res. 2024;Volume 17:3139-3150. [CrossRef]
- Klessinger S, Casser HR, Gillner S, et al. Radiofrequency Denervation of the Spine and the Sacroiliac Joint: A Systematic Review based on the Grades of Recommendations, Assesment, Development, and Evaluation Approach Resulting in a German National Guideline. Glob Spine J. 2024;14(7):2124-2154. [CrossRef]
- Cahani D, Chacko J, Hahn B. Myonecrosis: A Rare Complication of Cryoneurolysis. J Emerg Med. 2019;57(3):e73-e76. [CrossRef]
- Fleischmann E, Lenhardt R, Kurz A, et al. Nitrous oxide and risk of surgical wound infection: a randomised trial. The Lancet. 2005;366(9491):1101-1107. [CrossRef]
Figure 1.
Prisma Flowchart.
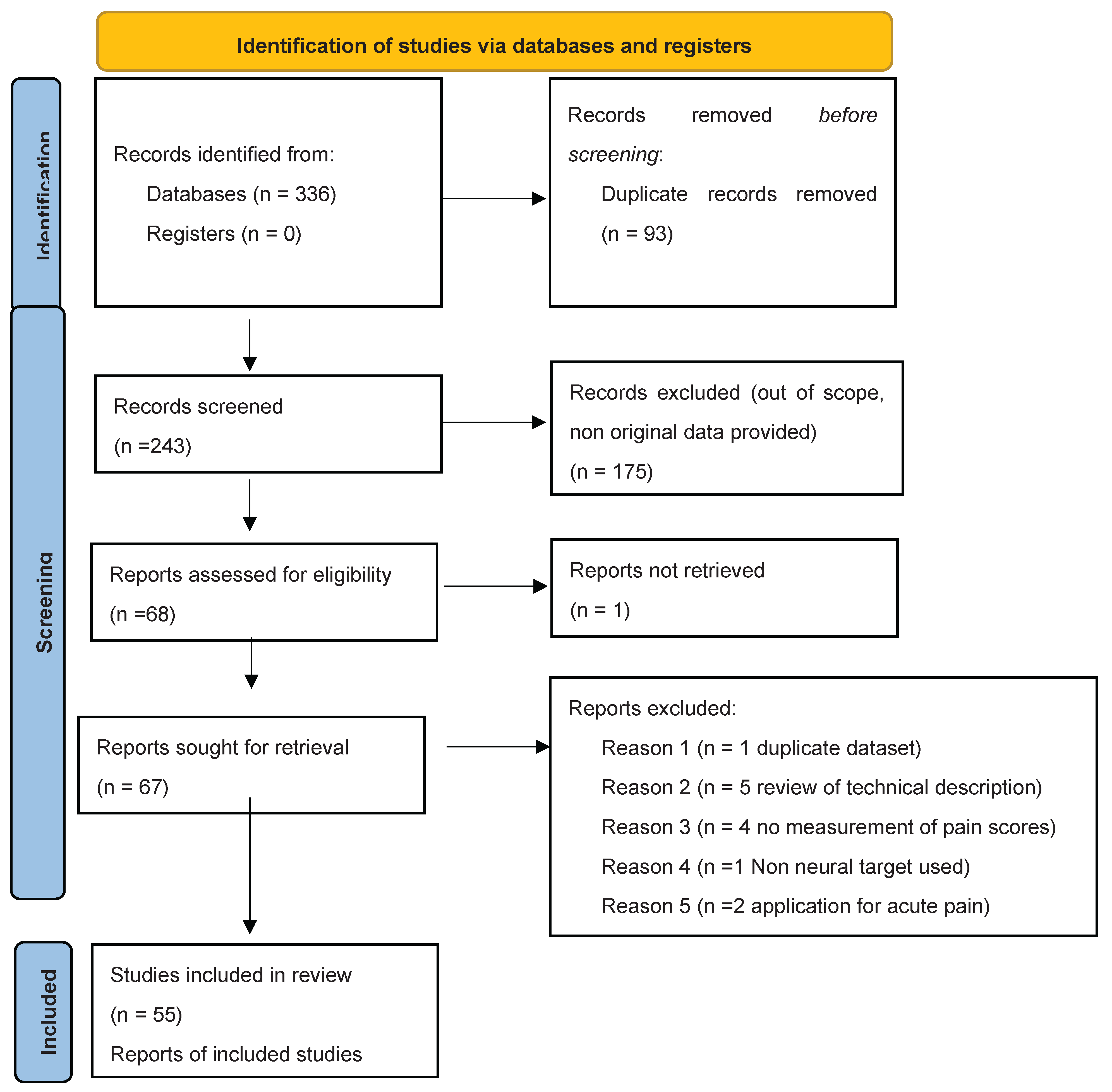
Figure 2.
Number of studies for each anatomical target.
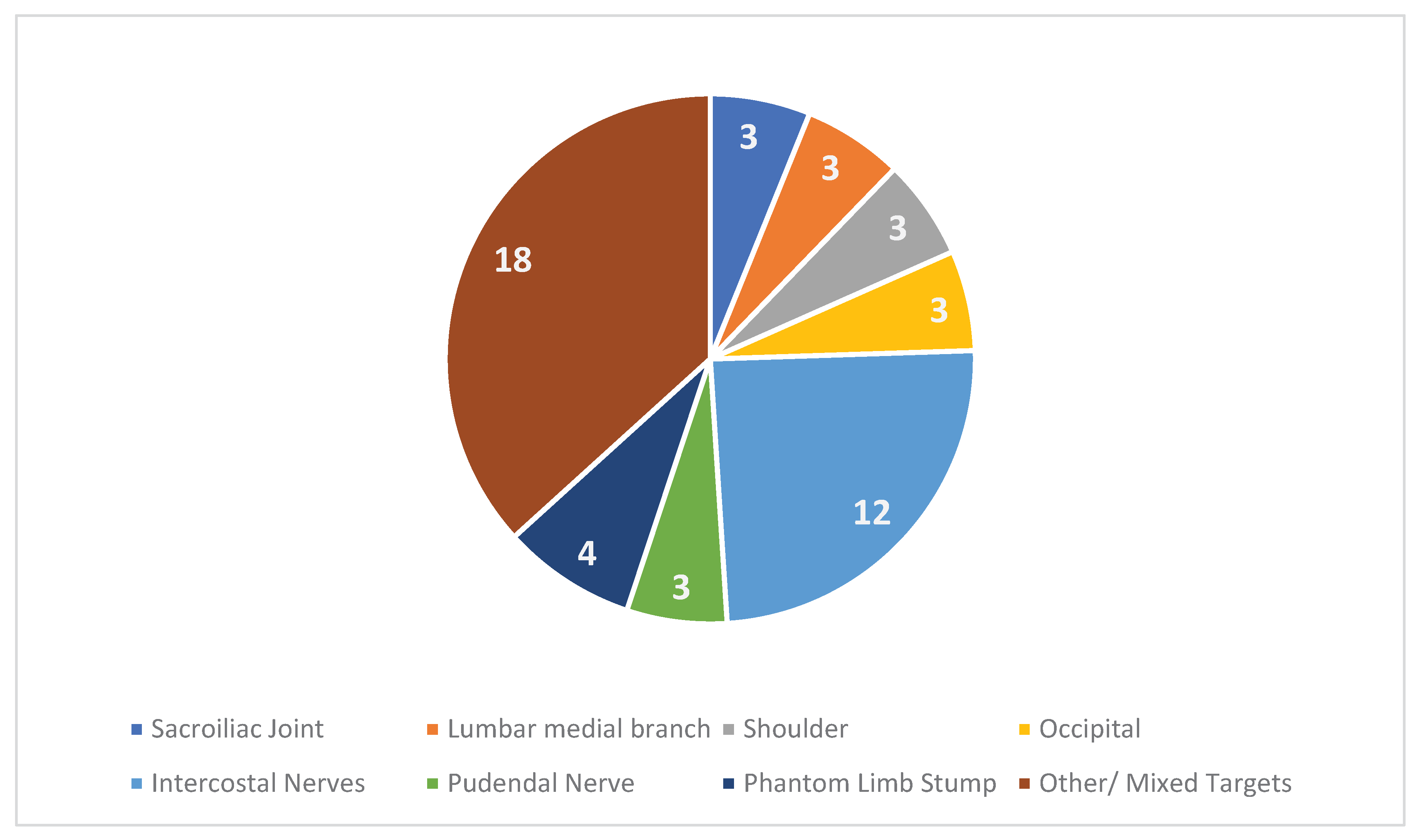

Table 1.
Characteristics of included studies. RCT Randomized Clinical Trial, OR Observational retrospective, OP observational prospective, CS case series, CR case report, US Ultrasound, NS Not Stated, MRI Magnetic Resonance Imaging, VAS Visual Analog Score, NRS Numerical Rating Score, CT Computerized Tomography.
Table 1.
Characteristics of included studies. RCT Randomized Clinical Trial, OR Observational retrospective, OP observational prospective, CS case series, CR case report, US Ultrasound, NS Not Stated, MRI Magnetic Resonance Imaging, VAS Visual Analog Score, NRS Numerical Rating Score, CT Computerized Tomography.
| Author, Year | Design | Patients | Targets | Guidance | Follow Up | Outcomes | Notes |
| Radnovich, 2017[10] |
RCT vs Sham | 180 | Saphenous Nerve | Landmark |
120 days | 87.5% responders at 120 days (VAS reduction > 50%) | 61.2% responders in the sham group at 120 days No adverse events |
| Truong, 2024[11] | RCT vs Sham and RF | 120 | Lumbar medial branch | Fluoroscopic | 6 months | No improvement compared to RF or Placebo | |
| Ilfeld, 2023[12] | RCT vs Sham |
144 | Sciatic (post amputation pain) | US | 4 months | No improvement compared to Placebo | |
| Kvarstein, 2019[13] | RCT Vs Steroid Injection | 52 | Occipital Nerve | US | 18 weeks | Pain relief > 50% in 35 % of patients (no difference) | |
| Grigsby, 2021[14] | OP | 26 | Occipital Nerve | Blind | 56 days | NRS reduction > 2 points in 35% of patients | |
| Perry, 2022[15] | OP | 40 | Sural, Saphenous, Superficial and/or Deep fibular nerves | US | 6 months | Mean NRS reduction 2.8 (< than 50% from baseline) | 22 patients completed follow up |
| Yoon,2016[16] |
OP | 22 | Peripheral neuropathy (mixed 3 plantar neuromas, 3 ileoinguinal, 4 posterior tibial, 7 saphenous, 1 gluteal, 1 sural, 1 genicular, 2 digital nerves) | US |
12 months | 3.2 mean VAS reduction at 12 months. Mean pain relief >50% at 3 months |
|
| Zhan, 2020[17] | OP | 18 | Intercostal | CT | 12 months | 2.3 and 1.3 mean VAS reduction at 6 and 9 months respectively | No significant reduction at 12 months |
| Das, 2023[18] | OR | 83 | Sacroiliac Joint | US | 6 Months | 69% patients with pain reief > 50% after 6 months | |
| Sidebottom, 2011[19] |
OR | 17 | TMJ (auricular nerve and TMJ capsule) | Surgical |
NS | Mean duration of pain relief 7 months, 3/17 patients were pain free at 12 months | 2 temporary numbness |
| Prologo,2017[20] | OR | 21 | Phantom Limb Neuroma | US | 194 ±99 Days | Mean NRS reduction 4.2 | |
| Yasin, 2019[21] | OR | 13 | Intercostal Nerves | CT |
Various, 2-18 months | 61.5% of patients with pain relief > 50% | 1 pneumothorax and 3 pseudohernia |
| Moore, 2010[22] | OR | 18 | Intercostal Nerves | CT | Variable (mean 51 days) | Mean Pain Relief <50% |
|
| Wolter, 2011[23] | OR | 91 | Lumbar Medial Branch | CT | 3 Months | Mean NRS decrease 3.50 points | |
| Kim, 2015[24] | OR | 38 | Occipital Nerve | Landmark | 6 Months | Mean NRS Improvement 3.8 | 2 post op neuritis and 1 haematoma |
| Nemecek, 2023 [25] | OR | 24 | Various (intercostal, saphenous, Peroneal, | US | 6 Months | Pain reduction > 30% in 2/24 Patients | |
| Parekattil, 2021[26] | OR | 35 | Genitofemoral, ilioinguinal and inferior hypogastric nerve |
Blind (surgical) | 1 month | Pain reduction > 50% in 68% of patients | |
| Tinnirello, 2020 [27] | OR | 10 | Genicular Nerves | US | 6 months | Pain relief >50% in 50% of patients at 6 months | |
| Nezami, 2022[28] | OR | 14 | Intercostobrachial nerve | CT | 6 months | Mean NRS decrease 2.9 | |
| McLean,2020[29] | OR | 23 | Saphenous nerve, Infrapatellar branch | Blind | Variable | Pain relief > 50% in all patients | Follow up at 6 months for 4 patients, NS for others. |
| Calixte, 2019[30] | OR | 279 | Genitofemoral, ilioinguinal and inferior hypogastric nerve |
Blind (Surgical) | 5 Years | Pain relief > 50% in 64% of patients | |
| Bellini, 2015[31] | OR | 18 | Facet, Knee, Sacroiliac Joint | 4 months | Mean NRS decrease 4/10 | ||
| Prologo, 2018[32] | OR | 14 | Pudendal Nerve | CT | 18 months | Responder rate 63% | Responder definition not stated |
| Lo Bianco, 2025 [33] | OR | 90 | Genicular nerves | US | 9 Months | Mean NRS 5±1 from 7±2 at Baseline | Pain relief > 50% in 56% of Patients at 3 months (NS at 9 Months) |
| Filipovski, 2024[34] | CS | 3 | Superficial peroneal nerve | US | 5 Years | 2 Patients pain free after 5 years, 1 without results | |
| Stogizka, 2024[35] | CS | 4 | Suprascapular, Axillary, Lateropectoral Nerves | US | 6 Months | 3 Patients with pain relief > 60% | |
| Dalili, 2021[36] |
CS | 3 | Anterior femoral cutaneous nerve | MRI |
12 months | 50% VAS reduction at 12 months in all patients | No adverse events |
| Moesker, 2014[37] |
CS | 5 | Phantom limb | US |
5-30 months | 60% of patients with > 50% pain relief | No adverse events |
| Sahoo, 2021[38] | CS | 5 | Lateral Branches of Sacral Dorsal Nerve Roots | US and Fluoro | 6 months | 100% of patients with > 50% pain relief | |
| Mendes-Andrade, 2024 [39] | CS | 2 | Sacrococcygeal Nerve | Fluoro | >50% pain relief in 100% of patients | ||
| Shaffer, 2022[40] | CS | 3 | Digital Nerves | US | 1 year | Pain Relief 100% | |
| Gabriel, 2024[41] | CR | 1 | Intercostal Nerves | US | |||
| Cachemaille, 2023[42] | CS | 4 | Alveolar Nerves | Blind | 3 months | Pain relief > 50% in 2 patients | |
| Kocân, 2022[43] | CS | 2 | Lumbar medial branches | Fluoroscopic | 6 months | Pain relief 50% at 3 months (<50% at 6 months, better result with RF) | 1 patient treated with RF, 2 with cryo |
| Connelly, 2013[44] | CS | 3 | Intercostal Nerves | US | Variable | Pain relief >50% in 2 patients for 9 months, in 1 patients for 3 months | |
| Matelich, 2022[45] | CS | 3 | Suprascapular Nerve | US | 3-6 months | Duration of pain relief 3-6 months | Pain scores not recorded |
| Fox, 2019[46] | CS | 3 | Pudendal Nerve | CT | NS | 2 Patients with > 50% pain relief | |
| Sarridou, 2022[47] | CR | 1 | Stellate Ganglion | US | 6 Months | Pain relief > 50% for 6 months | |
| Ramsook, 2016[48] | CR | 1 | Hip stump neuroma | US | NS | Pain relief | |
| Joshi, 2017[49] | CR | 1 | Posterior femoral cutaneous nerve | MRI | 5 months | Pain relief 100% at 6 months | |
| Kalava, 2024[50] | CR | 1 | Intercostal Nerves | CT | 3 months | 100% pain relief | |
| Sen, 2023[51] | CR | 1 | Intercostal Nerves | US | 5 days | Pain relief 100% | |
| Jung, 2024[52] | CR | 1 | Intercostal Nerves | Surgical | 8 weeks | Pain relief > 50% | |
| MacRae, 2023[53] | CR | 1 | Superficial Fibular Nerve | US | 5 months | Pain relief (no NRS reported) | |
| Perese, 2022[54] | CR | 1 | Intercostal Nerve | US | 2 months | Pain relief > 50% | |
| Koethe, 2014[55] | CR | 1 | Intercostal Nerves | CT | 8 weeks | Paine relief > 50% | |
| Rhame,2011 [56] |
CR | 1 | Sural Nerve | NS | 3 months | “Excellent pain relief” | |
| MacRae, 2023[57] | CR | 1 | Suprascapular Nerve | US | 7 Months | NRS < 2 | |
| Weber, 2019[58] | CR | 1 | Intercostobrachial Nerve | Blind | 1 Month | Pain relief >50% | |
| Yarmohammadi, 2011[59] | CR | 1 | Celiac Plexus | CT | 6 Months | Pain Relief 70% | |
| Rupp, 2022[60] | CR | 1 | Suprascapular Nerve | US | 3 months | Pain Relief > 50% | |
| Kalavla, 2024[61] | CR | 1 | Intercostal Nerves | US | 2 months | Pain relief > 50% | |
| Hampton, 2023[62] | CR | 2 | Pudendal Nerve | Blind | NS | Pain Relief for 3-4 Months | NRS not measured |
| Fiala, 2022[63] | CR | 1 | Phantom Limb Stump | US | NS | Pain relief < 6 weeks | |
| Gabriel, 2024[41] | CR | 1 | Intercostal Nerves | US | 6 Months | Pain relief >50% |
Table 2.
Studies with a follow up of 6 months or more and a definition of meaningful pain relief.
| Author, Year | Patients | Targets | Guidance | Positive outcome at 6 months |
| Truong, 2024[11] | 120 | Lumbar medial branch | Fluoroscopic | NO |
| Perry, 2022[15] | 40 | sural, saphenous, superficial and/or deep fibular nerves | US | NO |
| Yoon, 2016[16] |
22 | Peripheral neuropathy (mixed 3 plantar neuromas, 3 ileoinguinal, 4 posterior tibial, 7 saphenous, 1 gluteal, 1 sural, 1 genicular, 2 digital nerves) | US |
NO |
| Das, 2023[18] | 83 | Sacroiliac Joint | US | YES |
| Tinnirello, 2020 [27] | 10 | Genicular Nerves | US | YES |
| McLean, 2020[29] | 23 | Saphenous nerve, Infrapatellar branch | Blind | YES |
| Calixte, 2019[30] | 279 | Genitofemoral, ilioinguinal and inferior hypogastric |
Surgical | YES |
| Stogizka, 2024[35] | 4 | Suprascapular,Axillary, Lateropectoral | US | YES |
| Dalili, 2021 [36] |
3 | Anterior femoral cutaneous nerve | MRI |
YES |
| Moesker, 2014[37] |
5 | Phantom limb | US |
YES |
| Sahoo, 2021[38] | 5 | Lateral Branches of Sacral Dorsal Nerve Roots | US and Fluoroscopic | YES |
| Shaffer, 2022[40] | 3 | Digital Nerves | US | YES |
| Kocân, 2022[43] | 2 | Lumbar medial branches | Fluoroscopic | NO |
| Connelly, 2013[44] | 3 | Intercostal | US | YES |
| Sarridou, 2022[47] | 1 | Stellate Ganglion | US | YES |
| Yarmohammadi, 2011[59] | 1 | Celiac Plexus | CT | YES |
Positive outcome is considered pain relief of more than 50% in more than 50% of patients.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



