
Submitted:
21 May 2025
Posted:
23 May 2025
You are already at the latest version
Abstract
Candida species, particularly Candida albicans constitute a major cause of vulvovaginal candidiasis (VVC) in women of reproductive age. Over the years, the epidemiologic patterns of VVC have been shifting towards non-albicans (NAC) species and the antifungal resistance rates have been gradually increasing. We performed a retrospective study to determine the epidemiological pattern of VVC and the antifungal susceptibility rates in Greece between 2020 and 2024 in a Maternity / Gynaecological Clinic. Species identification and ssusceptibility testing was performed using Vitek 2 and assessed according to EUCAST. In total, 526 vaginal swab samples were collected, including C.albicans (57.9%) and NAC sp (42.1%). Median women age was 36.3(10-92), and was comparable between groups. Among NAC, C. glabrata (26.4%), was identified as the predominant species, followed by C. krusei (7.6%), C. parapsilosis (5.1%) and C. tropicalis (3.0%). For C. albicans isolates, fluconazole and itraconazole resistance rates increased from 9,3% in 2020 to 22.3% and 20.9% in 2024 respectively. No resistance to voriconazole was detected until 2023 and 2024, that rates reached 3.2 and 15.2 respectively. For NAC, except for C. glabrata and C. krusei that exhibit intrinsic resistance to fluconazole, C parapsilosis and C. tropicalis showed decreased susceptibility to fluconazole at 3.5 and 12.5% respectively. Echinocandin resistance rates remained low throughout the study period with an exception for C. glabrata which exhibited a resistance rate of 13,8% to caspofungin. In a number of cases, insufficient evidence pertaining to clinical breakpoints for fungi did not allow in vitro susceptibility assessment. The escalation of antifungal resistance and the shifting epidemiologic patterns of VVC constitutes a significant concern and highlights the need for nationwide surveillance programs, more focused diagnostic methods, proper antifungal stewardship policies as well as the development of novel antifungal treatments.
Keywords:
Candida albicans
; non-albicans Candida
; Vaginosis
; Vulvovaginal Candidosis
; vaginal infections
; candida resistance
; antifungal resistance
1. Introduction
Vulvovaginal candidosis (VVC) is a common condition responsible for one third of all vulvovaginitis cases in women of reproductive age. It is estimated that the infection affects 70-75% of women at least once in their lifetime, while 5-8% of women will experience recurrent infection, defined as four or more episodes every year [1] Current data suggest that, the prevalence of recurrent VVC will significantly rise by 2030, with nearly 158 million new cases annually [2].
Data on the frequency of VVC are limited, as the condition is not a reportable disease and is often self-diagnosed without clinical or laboratory confirmation. Among symptomatic women who have received microbiologic confirmation, the prevalence of VVC varies depending on the country and population studied. Reported prevalence rates range from 5.3- 60%, with higher rates observed in countries such as Tunisia, Nigeria, Australia and Brazil [3-7]. The most recently reported prevalence of VVC in Greece was 11.9%, in agreement with a previous Greek epidemiological survey comprising 4743 patients (12.1%) [7,8].
Candida albicans, which is a common genito-urinary tract commensal, has been the predominant species isolated from clinical samples of women diagnosed with VVC. However, non-albicans Candida (NAC) species have recently gained scientific and epidemiological interests as their prevalence increasing globally, accounting for approximately 10% to 45% of cases of VVC in some studies [9]. This shift may be attributed to the introduction of over-the-counter antifungals and short-course treatments, which effectively suppress C. albicans but may allow overgrowth of other species [9,10]. Interestingly, Dan et al. found a higher rate of non-albicans species in asymptomatic women (44.5%) compared to those with sporadic (19.4%) or chronic (21%) vaginitis [11].
The diagnosis of VVC remains challenging, often relying on clinical suspicion which can result in inappropriate treatment. Traditional methods including wet-mount microscopy and microbiological cultures, which constitute the gold-standard, are time consuming and may be neglected in routine clinical practice due to limited physician training [12,13]. Current diagnostic techniques in clinical settings are often inadequate, with even trained physicians frequently failing to make correct diagnoses [14]. In the United States, over 60% of VVC cases lack diagnostic testing, potentially leading to misdiagnosis and inappropriate treatment [15], underlining the pressing need for rapid and accurate diagnostic tests [16].
Treatment approaches also differ significantly among healthcare providers. While fluconazole is commonly prescribed for VVC [15,17], prescription patterns vary based on physicians' training backgrounds [17]. The availability of over-the-counter (OTC) antifungal medications since 1991 has further influenced prescribing trends [18], but studies suggest women may use them inappropriately. Only a minority of women can correctly diagnose VVC from symptoms, potentially leading to misuse of OTC treatments for other gynecological conditions [19]. While physician-diagnosed cases achieve better symptom relief, conse-quently many women self-diagnose and treat with OTC medications [20]. Indicatively, in Sweden, 93% of antifungal drug sales for VVC were OTC products [21].
As a result, the emergence of antifungal resistance poses an additional challenge to the management of fungal infections. A substantial number of studies indicate a rise in fluconazole-resistant C. albicans strains [22,23] In addition, the inherent azole resistance, as well as, the acquired resistance mechanisms of NAC species have become a growing issue, as these species are increasingly being identified in cases of VVC and treatment options remain limited [24].Data in Greece remains scarce as to the epidemiology and antifungal susceptibility of Candida sp in VVC, the latest report coming from Maraki et al, exploring trends between 2012 and 2017 [7].
We aimed to investigate the epidemiology of VVC caused by C. albicans and NAC species, analysing their prevalence and distribution patterns over a five-year period (2020-2024). Additionally, we evaluated the antifungal susceptibility profiles of Candida species for five different antifungal agents, including fluconazole, itraconazole, amphotericin B, caspofungin and anidulafungin providing a summary of antifungal resistance rates over a five-year period.
2. Materials and Methods
2.1. Study Design & Patient enrolment
We performed a retrospective descriptive analysis of data derived from the laboratory records of females tested positive and diagnosed with VVC caused by Candida albicans or NAC species at Leto General, Maternity and Gynecology Clinic S.A. located in Athens, between 2020-2024. Participants consisted of consecutive women presenting with symptoms of VVC, including individuals with recurrent manifestations. Study was conducted according to Declaration of Helsinki and Good Clinical Research Practice principles and approved by respective ethics committee and local institutional review board (364B/31.10.2023). Due to retrospective study nature, informed consent was waived as long as GDPR was implemented
2.2. Sample Collection and Microbiology Methods
Vaginal swabs were collected from women using sterile technique in order to avoid contamination. Specimens were collected from both the vaginal fornix and the vaginal wall and immediately got transported to the microbiology laboratory under controlled conditions to maintain sample integrity. Swab samples were streaked on selective media, including Sabouraud’s Dextrose Agar with Chloramphenicol. Cultures were incubated at 35-37 oC for 24-48 hours under aerobic conditions and positive growth was identified through macroscopic and microscopic evaluations. Antifungal susceptibility testing was performed using the bioMérieux VITEK® 2 automated system. Results were assessed according to the latest EUCAST breakpoints for each antifungal agent.
2.3. Statistical Methodology
Statistical analysis was performed using SPSS software, version 29.0.2.0 (20). To analyse data, we employed descriptive statistical methods. The results were presented as frequencies and percentages for each fungal species to determine the annual epidemiological trends, as well as the distribution of pathogens across different age groups. Inferential statistics, such as Chi-square tests were used to determine statistical significance. Also, the annual resistance rates for each antifungal agent were expressed as percentages per year. Furthermore, we graphically displayed the antifungal resistance trends observed from 2020 to 2024 using line graph to illustrate the period’s progression.
3. Results
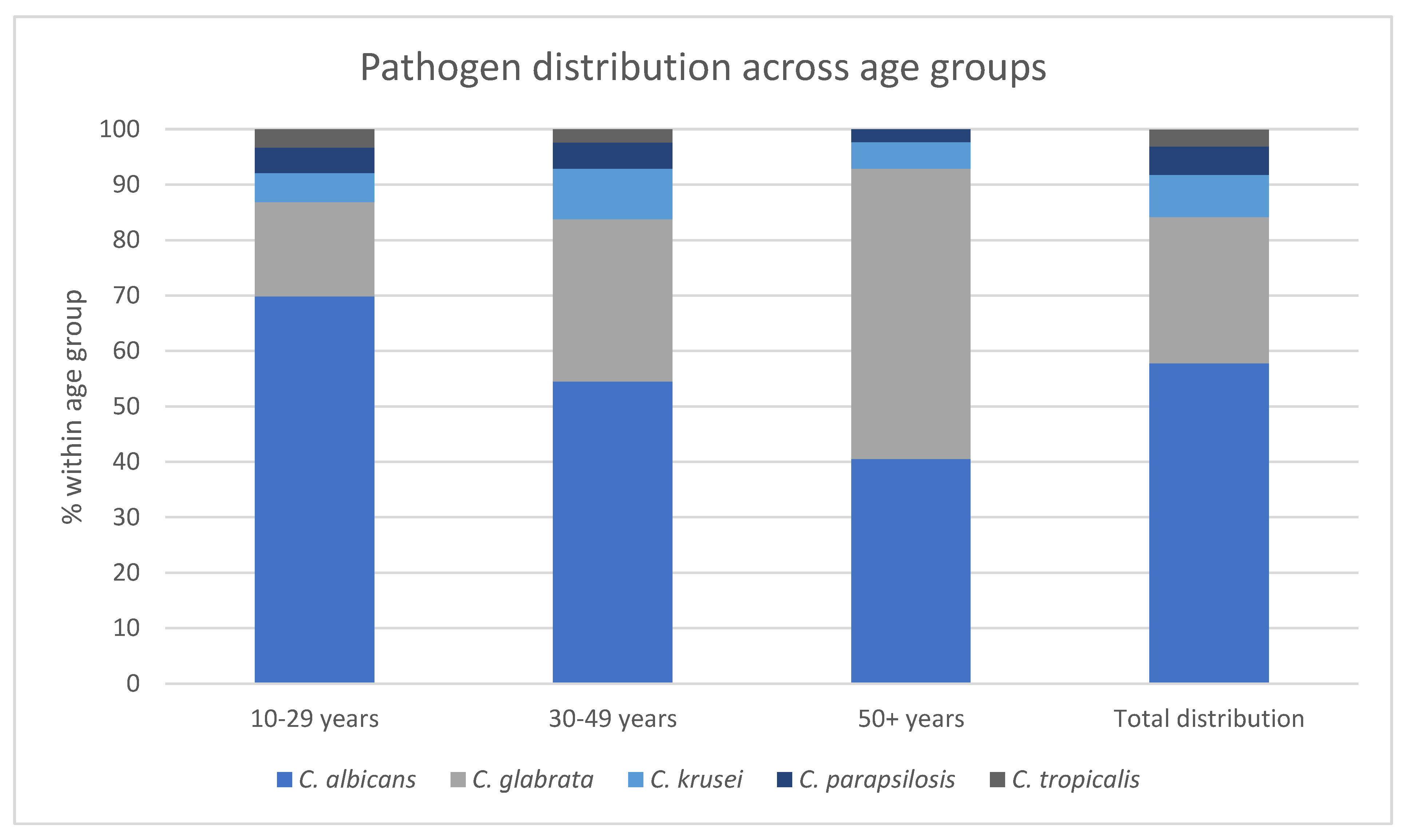
In the present study a total of 526 cases of VVC were identified from January 2020 to June 2024. The mean age of the participants was 36.28 years ranging from 10 to 92 years. C. albicans was the most prevalent species (57.8%) followed by C. glabrata (26.4%), C. krusei (7.6%), C. parapsilosis (5.1%) and C. tropicalis (3.0%). Error! Reference source not found. shows the distribution of Candida isolates during the study period. Pathogen distribution varied significantly across different age groups (p <0.001) (Error! Reference source not found.). Within the group of women aged 50 and above NAC species were identified in 59,6% of cases while C. albicans vaginitis was observed in 40,5%. In contrast, C. albicans vaginitis was more common in younger women occurring in 69,9% of women aged 10-29 years old and 54,5% in those aged 30-49 years, while NAC species were detected in 30,1% and 45,5% of women in these age groups respectively. Error! Reference source not found. illustrates pathogen distribution within different age groups.

Table 1.
Candida spp. distribution during study period.
| Candida spp. | 2020 n (%) |
2021 n (%) |
2022 n (%) |
2023 n (%) |
2024 n (%) |
2020-2024 n (%) |
|---|---|---|---|---|---|---|
| C. albicans | 54 (45,8) | 26 (27,4) | 42 (51,9) | 61 (79,2) | 121 (78,1) | 304 (57,8) |
| C. glabrata | 46 (39,0) | 41 (43,2) | 23 (28,4) | 4 (5,2) | 25 (16,1) | 139 (26,4) |
| C. krusei | 12 (10,2) | 13 (13,7) | 8 (9,9) | 3 (3,9) | 4 (2,6) | 40 (7,6) |
| C. parapsilosis | 6 (5,1) | 9 (9,5) | 4 (4,9) | 4 (5,2) | 4 (2,6) | 27 (5,1) |
| C. tropicalis | 0 | 6 (6,3) | 4 (4,9) | 5 (6,5) | 1 (0,6) | 16 (3,0) |
| Total cases/year | 118 | 95 | 81 | 77 | 155 | 526 |
Table 2.
Pathogen distribution across age groups.
| Age group |
C. albicans n (% within age group) |
C. glabrata n (% within age group) |
C. krusei n (% within age group) |
C. parapsilosis n (% within age group) |
C. tropicalis n (% within age group) |
|---|---|---|---|---|---|
| 10-29 years | 113 (69,9) | 27 (17,0) | 9 (5,2) | 9 (4,6) | 7 (3,3) |
| 30-49 years | 168 (54,5) | 88 (29,3) | 28 (9,1) | 16 (4,7) | 9 (2,4) |
| 50+ years |
23 (40,5) | 24 (52,4) | 3 (4,8) | 2 (2,3) | 0 (0,0) |
| Total distribution | 304 (57,8) | 139 (26,4) | 40 (7,6) | 27 (5,1) | 16 (3,0) |
Figure 1.
Pathogen distribution across ages groups.
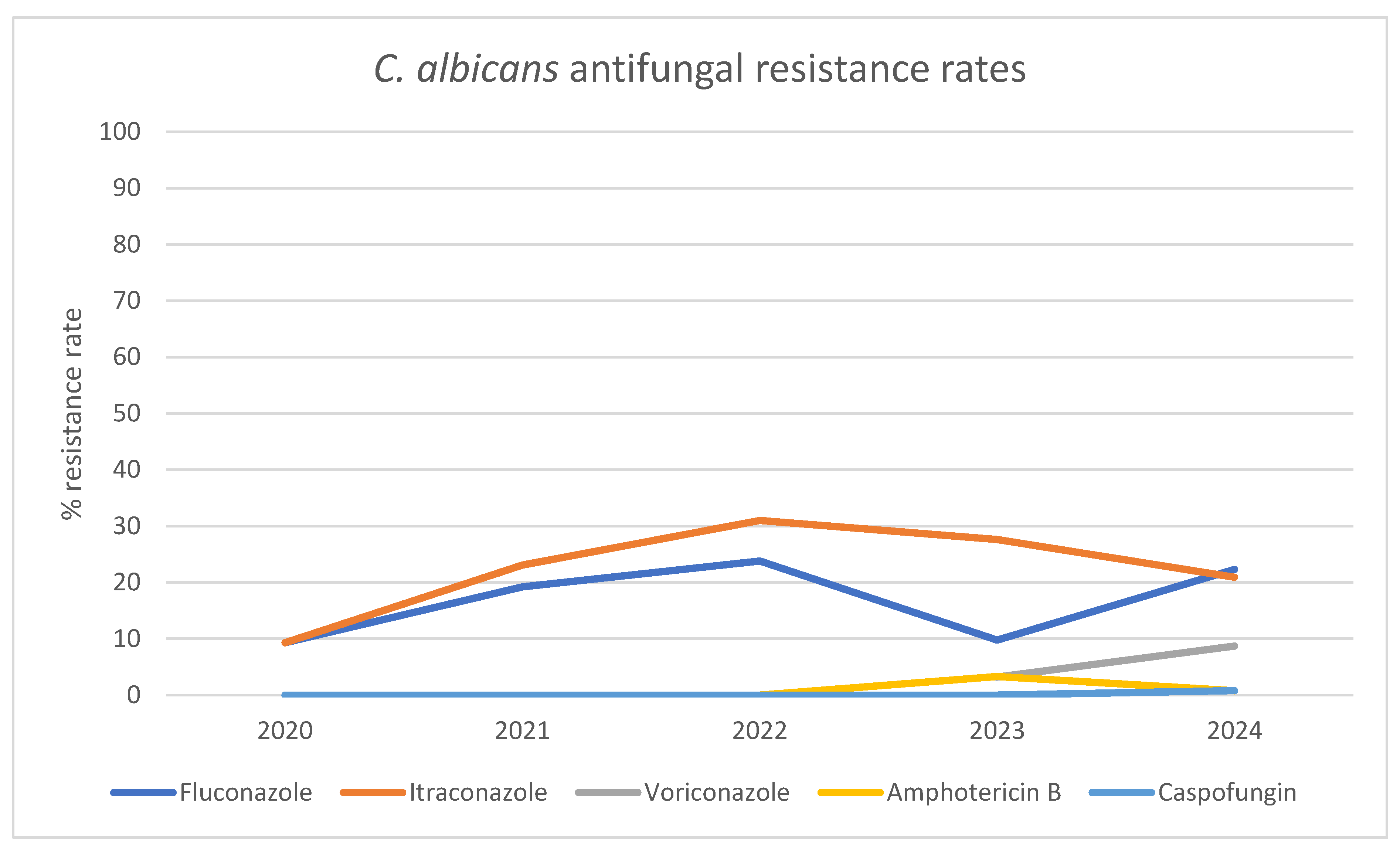
Susceptibility testing for C. albicans isolates revealed increasing azole resistance rates (Error! Reference source not found., Error! Reference source not found.). Fluconazole and itraconazole resistance rates raised from 9,3% in 2020 to 22.3% and 20.9% in 2024 respectively. The highest resistance rates were observed in 2022, with resistance reaching as high as 23.8% for fluconazole and 31,0% for itraconazole. Respective rates for voriconazole increased from 3,2% in 2023 to 8,7% in 2024. No resistance to amphotericin b and caspofungin was detected until 2023, with rates remaining low at approximately 0,8% in 2024.
Table 3.
Candida albicans resistance rates for tested antifungal agents.
| Antifungal Agent | 2020 n (% Resistance Rate) |
2021 n (% Resistance Rate) |
2022 n (% Resistance Rate) |
2023 n (% Resistance Rate) |
2024 n (% Resistance Rate) |
|---|---|---|---|---|---|
| Fluconazole | 5 (9,3) |
5 (19,2) | 10 (23,8) | 6 (9,8) | 27 (22,3) |
| Itraconazole | 5 (9,3) |
6 (23,1) | 13 (31,0) | 8 (27,6) | 23 (20,9) |
| Voriconazole | ND |
ND | ND | 1 (3,2) | 8 (8,7) |
| Amphotericin B | 0 (0,0) |
0 (0,0) | 0 (0,0) | 2 (3,3) | 1 (0,8) |
| Caspofungin | 0 (0,0) | 0 (0,0) | 0 (0,0) | 0 (0,0) | 1 (0,8) |
Figure 2.
C. albicans antifungal resistance rates.
The resistance rates of NAC species are summarized in Error! Reference source not found.. For NAC species, C. glabrata and C. krusei exhibit intrinsic azole resistance while C. tropicalis and C. parapsilosis exhibited decreased susceptibility to fluconazole with overall resistance rates of 12,5% and 3,7% during the study period. Amphotericin B resistance rates for C. glabrata and C. krusei were 13,7% and 13,2% respectively. The overall amphotericin B resistance among NAC species increased from 10,9% in 2020 reaching a peak of 17,9% in 2022 and subsequently decreased to 5,9% in 2024. Echinocandin resistance rates remained low throughout the study period, however, C. glabrata exhibited a resistance rate of 13,8% to caspofungin.
Table 4.
NAC species antifungal resistance rates.
| NAC Species | Fluconazole n (% Resistance Rate) |
Itraconazole n (% Resistance Rate) |
Amphotericin B n (% Resistance Rate) |
Micafungin n (% Resistance Rate) |
Caspofungin n (% Resistance Rate) |
Anidulafungin n (% Resistance Rate) |
|---|---|---|---|---|---|---|
| C. glabrata | 139 (100) |
139 (100) | 19 (13,7) | 0 (0,0) | 19 (13,8) | 0 (0,0) |
| C. krusei | 40 (100) | 40 (100) | 5 (13,2) | ND | ND | ND |
| C. parapsilosis | 1 (3,7) | 0 (0,0) | 0 (0,0) | 0 (0,0) | 0 (0,0) | 0 (0,0) |
| C. tropicalis | 2 (12,5) | 1 (10,0) | 0 (0,0) | ND | 0 (0,0) | 0 (0,0) |
4. Discussion
VVC is a common fungal infection that is often associated with high morbidity and a substantial impact on women’s quality of life. This study investigated the epidemiology and antifungal susceptibility trends of VVC in Greece during a five-year period (2020-2024). In our study, C. albicans (57.8%) was the predominant species followed by NAC species (42,2%), however, non-albicans sp prevailed as age progressed. We recorded increasing resistance of C.albicans and NAC sp along various regimens through the years.
Our findings support the growing trend of shifting epidemiological patterns towards NAC species in VVC and align with the results of other studies such as this conducted in Ethiopia and which reported similar recovery rates [25] Higher occurrence of NAC vaginitis was found in studies conducted in India and Lebanon [26,27], while lower incidence was observed in China, Kuwait and Brazil [28-30].
C.glabrata was responsible for more than half of NAC VVC cases, in line with previous authors [7]. Most studies identify C. glabrata as the predominant NAC species, accounting for approximately 50% to 66% of NAC-related vaginitis. However, the distribution of NAC species in women with VVC varies by geographic region and population. The second most prevalent NAC species differ across studies, with C. tropicalis, C. parapsilosis, and C. krusei being reported in varying frequencies [9,11,28]. Notably, pathogen distribution varied significantly across age groups in our study, with NAC species being more frequently isolated in women aged 50 and above. These results were consistent with previous studies, which reported higher prevalence of NAC species in older women with VVC [7,31,32].Prior exposure to antifungal agents and the use of hormone replacement treatment may be associated with this observation [9].
For C. albicans the resistance rates for fluconazole and itraconazole increased from 9,3% in 2020 to 22,3% and 19,0% in 2024 respectively. Voriconazole resistance raised from 3,2% to 8,7% during 2023 and 2024. The observed resistance rates are significantly higher than those reported by previous studies conducted in Greece, in which a 6,6% overall resistance to fluconazole was reported [7]. Similarly, lower resistance rates have been reported in other regions including China, United Kingdom, Vietnam, and Iran [33-36]. The findings concerning azole resistance raise significant concerns, especially due to indiscriminate and unnecessary fluconazole exposure evoking a number of resistance mechanisms [37]. Overexpression of efflux pump genes (CDR1, CDR2, and MDR1) contributes to azole resistance in some isolates [38], however, ERG11 gene mutations and overexpression are more prevalent in fluconazole-resistant strains [39]. Clonal spread of specific genotypes, particularly CC69 and DST79, is associated with fluconazole non-susceptibility in VVC patients [39]. Resistance mechanisms are not limited to C. albicans; similar patterns have been observed in C. glabrata. For NAC species except for C. glabrata and C. krusei which exhibit intrinsic azole resistance, C. parapsilosis and C. tropicalis showed decreased susceptibility to fluconazole with an overall resistance rate of 3,7% and 12,5% respectively. Besides efflux pumps, Candida species can develop resistance to various antifungal classes through alterations in drug targets and biosynthetic pathways [40].
Regarding echinocandin resistance, C. albicans as well as NAC species presented high susceptibility rates within the study period and our results were consistent with data reported in previous years in our country [7,8]. However, echinocandin resistance in Candida species, particularly C. glabrata, has emerged as a growing concern in treating VVC and invasive candidiasis [41,42]. In the present study C. glabrata exhibited a resistance rate of 13,8% to caspofungin. Resistance mechanisms involve mutations in FKS genes encoding glucan synthase, the target enzyme of echinocandins [42], thus reducing drug sensitivity and increase minimum inhibitory concentrations [42]. Echinocandin resistance typically develops after 3-4 weeks of treatment and is associated with poor outcomes [43]. Standardized susceptibility testing methods can detect resistant strains, but variability exists among clinical laboratories [44].
Currently, the use of new echinocandins including caspofungin, anidulafungin and micafungin, is evaluated for their efficacy in treating resistant infections. Caspofungin has demonstrated promising results in treating mucosal and invasive candidiasis that is unresponsive to other therapies, with response rates ranging from 82% to 100% [45]. In the context of VVC, all tested strains showed high in vitro sensitivity to caspofungin [46], suggesting that, caspofungin holds potential as a first-line treatment for Candida vaginitis. Data is limited on micafungin or anidulafungin efficacy on VVC, except for isolated reports as rescue therapy [47], necessitating more clinical trial before their use in this setting.
The overall resistance rate to amphotericin B for NAC species increased reaching a peak of 17,9% in 2022, before decreasing to 5,9% in 2024. A recent meta-analysis of 63 studies found a varying picture of amphotericin B resistance rates for C. parapsilosis ranging from 0% to 46.9%, however with an overall pooled rate of 1,3% [48].For cases involving azole-resistant Candida species, vaginal suppositories containing amphotericin B have been used successfully. In a previous study, 99.8% of C. albicans isolates and all NAC isolates (100%) were found to be susceptible to amphotericin [7].
Our study has some limitations, including those of an observational retrospective study. Even though a large number of samples were identified our data lacked clinical information such as prior exposure to antifungal or antibiotic treatments, use of hormone replacement therapy, potential pregnancy and comorbidities. Although all cases included were symptomatic patients, our analysis could not distinguish between recurrent cases. The biofilm-forming capacity of Candida isolates from recurrent VVC patients is heterogeneous and associated with altered antifungal sensitivity, particularly to fluconazole [49] Interestingly, C. albicans can switch phenotypes during successive episodes of recurrent VVC, potentially contributing to treatment challenges [50]. Moreover, in a number of cases insufficient evidence pertaining to clinical breakpoints for certain fungal species did not allow in vitro susceptibility assessment. Of note, we have to keep in mind that where minimum inhibitory concentration has been assessed, fluconazole resistance identified through in vitro susceptibility testing does not always correlate with clinical (phenotypic) resistance. The phenomenon of trailing growth exhibited by Candida—a result of its diverse resistance mechanisms and ability to form biofilms—can obscure the true relationship between in vitro susceptibility and in vivo treatment efficacy [51,52]. Additionally, negative culture results do not necessarily rule out active infection; they may instead reflect recent antifungal treatment, poor-quality swab collection, the presence of inhibitory substances, or sampling errors that miss the site of infection. Various types of rapid molecular diagnostic tests for VVC have become broadly available with promising performance characteristics, however their use complicate antifungal susceptibility testing [16,53]
To conclude, VVC caused by NAC species is rising, particularly among older women, as this is supported by an increasing number of reports including the present study. The relatively high resistance rates observed for C. albicans, as well as the inherently resistant nature of NAC species highlight the need for routine susceptibility testing to guide appropriate treatment. With the increasing availability of advanced diagnostic tools and susceptibility testing, therapeutic decisions should be driven by evidence-based approaches, taking antifungal stewardship principles into consideration. Emerging therapies, including novel antifungal agents such as oteseconazole and ibrexafungerp, offer promising solutions to current treatment challenges and broaden the range of options available to clinicians and patients [24]. Moreover, adjunctive treatments including probiotics [54], as well as, the ongoing development of a vaccine—currently in clinical trials—offers the potential to revolutionize the prevention of VVC [24]. However, the long-term success of these innovations will rely heavily on their judicious use, guided by informed clinical decision-making and robust antifungal stewardship to ensure sustainable and effective outcomes [24,55,56].
Author Contributions
AT: KA conceived idea; AT, CV attended patients; AT, DP, VP, ED collected data; PDZ,IR,ED,VP, performed microbiological identifications; KA,DP analyzed data; DP,KA wrote manuscript and drew figures and tables; AT,KA oversaw study.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available upon request from the corresponding author.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| VVC | Vulvovaginal candidiasis |
| NAC | Non-albicans Candida |
| OTC | Over the counter |
| EUCAST | European Committee on Antimicrobial Susceptibility Testing |
References
- Sobel, J.D. Vulvovaginal candidosis. Lancet (London, England) 2007, 369, 1961–1971. [Google Scholar] [CrossRef]
- Denning, D.W.; Kneale, M.; Sobel, J.D.; Rautemaa-Richardson, R. Global burden of recurrent vulvovaginal candidiasis: a systematic review. The Lancet. Infectious diseases 2018, 18, e339–e347. [Google Scholar] [CrossRef] [PubMed]
- Andrioli, J.L.; Oliveira, G.S.; Barreto, C.S.; Sousa, Z.L.; Oliveira, M.C.; Cazorla, I.M.; Fontana, R. [Frequency of yeasts in vaginal fluid of women with and without clinical suspicion of vulvovaginal candidiasis]. Rev Bras Ginecol Obstet 2009, 31, 300–304. [Google Scholar] [CrossRef]
- Jacob, L.; John, M.; Kalder, M.; Kostev, K. Prevalence of vulvovaginal candidiasis in gynecological practices in Germany: A retrospective study of 954,186 patients. Curr Med Mycol 2018, 4, 6–11. [Google Scholar] [CrossRef]
- Amouri, I.; Sellami, H.; Borji, N.; Abbes, S.; Sellami, A.; Cheikhrouhou, F.; Maazoun, L.; Khaled, S.; Khrouf, S.; Boujelben, Y.; et al. Epidemiological survey of vulvovaginal candidosis in Sfax, Tunisia. Mycoses 2011, 54, e499–505. [Google Scholar] [CrossRef]
- Bradshaw, C.S.; Morton, A.N.; Garland, S.M.; Morris, M.B.; Moss, L.M.; Fairley, C.K. Higher-risk behavioral practices associated with bacterial vaginosis compared with vaginal candidiasis. Obstet Gynecol 2005, 106, 105–114. [Google Scholar] [CrossRef]
- Maraki, S.; Mavromanolaki, V.E.; Stafylaki, D.; Nioti, E.; Hamilos, G.; Kasimati, A. Epidemiology and antifungal susceptibility patterns of Candida isolates from Greek women with vulvovaginal candidiasis. Mycoses 2019, 62, 692–697. [Google Scholar] [CrossRef]
- Grigoriou, O.; Baka, S.; Makrakis, E.; Hassiakos, D.; Kapparos, G.; Kouskouni, E. Prevalence of clinical vaginal candidiasis in a university hospital and possible risk factors. Eur J Obstet Gynecol Reprod Biol 2006, 126, 121–125. [Google Scholar] [CrossRef]
- Makanjuola, O.; Bongomin, F.; Fayemiwo, S.A. An Update on the Roles of Non-albicans Candida Species in Vulvovaginitis. J Fungi (Basel) 2018, 4. [Google Scholar] [CrossRef]
- Martens, M.G.; Hoffman, P.; El-Zaatari, M. Fungal species changes in the female genital tract. J Low Genit Tract Dis 2004, 8, 21–24. [Google Scholar] [CrossRef]
- Dan, M.; Poch, F.; Levin, D. High rate of vaginal infections caused by non-C. albicans Candida species among asymptomatic women. Med Mycol 2002, 40, 383–386. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.G.; Marconi, C.; Bellen, G.; Donders, F.; Michiels, T. Effect of short training on vaginal fluid microscopy (wet mount) learning. J Low Genit Tract Dis 2015, 19, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.G.; Bellen, G. Anything wrong with conventional wet mount microscopy? J Low Genit Tract Dis 2014, 18, E26–27. [Google Scholar] [CrossRef] [PubMed]
- Sobel, J.D.; Hay, P. Diagnostic techniques for bacterial vaginosis and vulvovaginal candidiasis - requirement for a simple differential test. Expert Opin Med Diagn 2010, 4, 333–341. [Google Scholar] [CrossRef]
- Benedict, K.; Lyman, M.; Jackson, B.R. Possible misdiagnosis, inappropriate empiric treatment, and opportunities for increased diagnostic testing for patients with vulvovaginal candidiasis-United States, 2018. PLoS One 2022, 17, e0267866. [Google Scholar] [CrossRef]
- Akinosoglou, K.; Schinas, G.; Papageorgiou, D.; Polyzou, E.; Massie, Z.; Ozcelik, S.; Donders, F.; Donders, G. Rapid Molecular Diagnostics in Vulvovaginal Candidosis. Diagnostics 2024, 14, 2313–2313. [Google Scholar] [CrossRef]
- Adib, S.M.; Bared, E.E.; Fanous, R.; Kyriacos, S. Practices of Lebanese gynecologists regarding treatment of recurrent vulvovaginal candidiasis. N Am J Med Sci 2011, 3, 406–410. [Google Scholar] [CrossRef]
- McCaig, L.F.; McNeil, M.M. Trends in prescribing for vulvovaginal candidiasis in the United States. Pharmacoepidemiol Drug Saf 2005, 14, 113–120. [Google Scholar] [CrossRef]
- Ferris, D.G.; Dekle, C.; Litaker, M.S. Women's use of over-the-counter antifungal medications for gynecologic symptoms. J Fam Pract 1996, 42, 595–600. [Google Scholar]
- Yano, J.; Sobel, J.D.; Nyirjesy, P.; Sobel, R.; Williams, V.L.; Yu, Q.; Noverr, M.C.; Fidel, P.L., Jr. Current patient perspectives of vulvovaginal candidiasis: incidence, symptoms, management and post-treatment outcomes. BMC Womens Health 2019, 19, 48. [Google Scholar] [CrossRef]
- Mardh, P.A.; Wagstrom, J.; Landgren, M.; Holmen, J. Usage of antifungal drugs for therapy of genital Candida infections, purchased as over-the-counter products or by prescription: 2. Factors that may have influenced the marked changes in sales volumes during the 1990s. Infect Dis Obstet Gynecol 2004, 12, 99–108. [Google Scholar] [CrossRef] [PubMed]
- File, B.; Sobel, R.; Becker, M.; Nyirjesy, P. Fluconazole-Resistant Candida albicans Vaginal Infections at a Referral Center and Treated With Boric Acid. Journal of lower genital tract disease 2023, 27, 262–265. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Ahmed, J.; Gul, A.; Ikram, A.; Lalani, F.K. Antifungal susceptibility testing of vulvovaginal Candida species among women attending antenatal clinic in tertiary care hospitals of Peshawar. Infection and Drug Resistance 2018, 11, 447–447. [Google Scholar] [CrossRef]
- Akinosoglou, K.; Livieratos, A.; Asimos, K.; Donders, F.; Donders, G.G.G. Fluconazole-Resistant Vulvovaginal Candidosis: An Update on Current Management. Pharmaceutics 2024, Vol. 16, Page 1555 2024, 16, 1555–1555. [Google Scholar] [CrossRef]
- Bitew, A.; Abebaw, Y. Vulvovaginal candidiasis: Species distribution of Candida and their antifungal susceptibility pattern. BMC Women's Health 2018, 18, 1–10. [Google Scholar] [CrossRef]
- Ghaddar, N.; Anastasiadis, E.; Halimeh, R.; Ghaddar, A.; Dhar, R.; Alfouzan, W.; Yusef, H.; El Chaar, M. Prevalence and antifungal susceptibility of Candida albicans causing vaginal discharge among pregnant women in Lebanon. BMC Infectious Diseases 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Kumari, V.; Banerjee, T.; Kumar, P.; Pandey, S.; Tilak, R. Emergence of non-albicans Candida among candidal vulvovaginitis cases and study of their potential virulence factors, from a tertiary care center, North India. Indian J Pathol Microbiol 2013, 56, 144–147. [Google Scholar] [CrossRef]
- Alfouzan, W.; Dhar, R.; Ashkanani, H.; Gupta, M.; Rachel, C.; Khan, Z.U. Species spectrum and antifungal susceptibility profile of vaginal isolates of Candida in Kuwait. Journal de mycologie medicale 2015, 25, 23–28. [Google Scholar] [CrossRef]
- Brandolt, T.M.; Klafke, G.B.; Gonçalves, C.V.; Bitencourt, L.R.; Martinez, A.M.B.d.; Mendes, J.F.; Meireles, M.C.A.; Xavier, M.O. Prevalence of Candida spp. in cervical-vaginal samples and the in vitro susceptibility of isolates. Brazilian journal of microbiology : [publication of the Brazilian Society for Microbiology] 2017, 48, 145–150. [Google Scholar] [CrossRef]
- Zhai, Y.; Liu, J.; Zhou, L.; Ji, T.; Meng, L.; Gao, Y.; Liu, R.; Wang, X.; Li, L.; Lu, B.; et al. Detection of Candida species in pregnant Chinese women with a molecular beacon method. Journal of medical microbiology 2018, 67, 783–789. [Google Scholar] [CrossRef]
- Intra, J.; Sala, M.R.; Brambilla, P.; Carcione, D.; Leoni, V. Prevalence and species distribution of microorganisms isolated among non-pregnant women affected by vulvovaginal candidiasis: A retrospective study over a 20 year-period. Journal of Medical Mycology 2022, 32, 101278–101278. [Google Scholar] [CrossRef] [PubMed]
- Song, N.; Kan, S.; Pang, Q.; Mei, H.; Zheng, H.; Li, D.; Cui, F.; Lv, G.; An, R.; Li, P.; et al. A prospective study on vulvovaginal candidiasis: multicentre molecular epidemiology of pathogenic yeasts in China. Journal of the European Academy of Dermatology and Venereology : JEADV 2022, 36, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Anh, D.N.; Hung, D.N.; Tien, T.V.; Dinh, V.N.; Son, V.T.; Luong, N.V.; Van, N.T.; Quynh, N.T.N.; Van Tuan, N.; Tuan, L.Q.; et al. Prevalence, species distribution and antifungal susceptibility of Candida albicans causing vaginal discharge among symptomatic non-pregnant women of reproductive age at a tertiary care hospital, Vietnam. BMC infectious diseases 2021, 21. [Google Scholar] [CrossRef]
- Ratner, J.C.; Wilson, J.; Roberts, K.; Armitage, C.; Barton, R.C. Increasing rate of non-Candida albicans yeasts and fluconazole resistance in yeast isolates from women with recurrent vulvovaginal candidiasis in Leeds, United Kingdom. Sexually Transmitted Infections 2025, 101, 21–26. [Google Scholar] [CrossRef]
- Rezaei-Matehkolaei, A.; Shafiei, S.; Zarei-Mahmoudabadi, A. Isolation, molecular identification, and antifungal susceptibility profiles of vaginal isolates of Candida species. Iranian Journal of Microbiology 2016, 8, 410–410. [Google Scholar]
- Wang, X.; Chen, L.; Ruan, H.; Xiong, Z.; Wang, W.; Qiu, J.; Song, W.; Zhang, C.; Xue, F.; Qin, T.; et al. Oteseconazole versus fluconazole for the treatment of severe vulvovaginal candidiasis: a multicenter, randomized, double-blinded, phase 3 trial. Antimicrobial Agents and Chemotherapy 2023, 68, e00778–00723. [Google Scholar] [CrossRef]
- Sobel, J.D.; Sobel, R. Current treatment options for vulvovaginal candidiasis caused by azole-resistant Candida species. Expert Opin Pharmacother 2018, 19, 971–977. [Google Scholar] [CrossRef]
- Bhattacharya, S.; Sobel, J.D.; White, T.C. A Combination Fluorescence Assay Demonstrates Increased Efflux Pump Activity as a Resistance Mechanism in Azole-Resistant Vaginal Candida albicans Isolates. Antimicrob Agents Chemother 2016, 60, 5858–5866. [Google Scholar] [CrossRef]
- Wu, Y.; Li, C.; Wang, Z.; Gao, J.; Tang, Z.; Chen, H.; Ying, C. Clonal spread and azole-resistant mechanisms of non-susceptible Candida albicans isolates from vulvovaginal candidiasis patients in three Shanghai maternity hospitals. Med Mycol 2018, 56, 687–694. [Google Scholar] [CrossRef]
- Bhattacharya, S.; Sae-Tia, S.; Fries, B.C. Candidiasis and Mechanisms of Antifungal Resistance. Antibiotics (Basel) 2020, 9. [Google Scholar] [CrossRef]
- Lotfali, E.; Erami, M.; Fattahi, M.; Nemati, H.; Ghasemi, Z.; Mahdavi, E. Analysis of molecular resistance to azole and echinocandin in Candida species in patients with vulvovaginal candidiasis. Curr Med Mycol 2022, 8, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Perlin, D.S. Echinocandin Resistance in Candida. Clin Infect Dis 2015, 61 Suppl 6, S612–617. [Google Scholar] [CrossRef]
- Arendrup, M.C.; Perlin, D.S. Echinocandin resistance: an emerging clinical problem? Curr Opin Infect Dis 2014, 27, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Perlin, D.S. Echinocandin resistance, susceptibility testing and prophylaxis: implications for patient management. Drugs 2014, 74, 1573–1585. [Google Scholar] [CrossRef]
- Kartsonis, N.A.; Saah, A.; Lipka, C.J.; Taylor, A.; Sable, C.A. Second-line therapy with caspofungin for mucosal or invasive candidiasis: results from the caspofungin compassionate-use study. J Antimicrob Chemother 2004, 53, 878–881. [Google Scholar] [CrossRef]
- Cornely, O.A.; Lasso, M.; Betts, R.; Klimko, N.; Vazquez, J.; Dobb, G.; Velez, J.; Williams-Diaz, A.; Lipka, J.; Taylor, A.; et al. Caspofungin for the treatment of less common forms of invasive candidiasis. J Antimicrob Chemother 2007, 60, 363–369. [Google Scholar] [CrossRef]
- Akdag, D.; Pullukcu, H.; Yamazhan, T.; Metin, D.Y.; Sipahi, O.R.; Ener, B.; Isikgoz Tasbakan, M. Anidulafungin treatment for fluconazole-resistant Candida albicans vaginitis with cross-resistance to azoles: a case report. J Obstet Gynaecol 2021, 41, 665–666. [Google Scholar] [CrossRef]
- Yamin, D.; Akanmu, M.H.; Al Mutair, A.; Alhumaid, S.; Rabaan, A.A.; Hajissa, K. Global Prevalence of Antifungal-Resistant Candida parapsilosis: A Systematic Review and Meta-Analysis. Tropical Medicine and Infectious Disease 2022, 7, 188–188. [Google Scholar] [CrossRef]
- Sherry, L.; Kean, R.; McKloud, E.; O'Donnell, L.E.; Metcalfe, R.; Jones, B.L.; Ramage, G. Biofilms Formed by Isolates from Recurrent Vulvovaginal Candidiasis Patients Are Heterogeneous and Insensitive to Fluconazole. Antimicrob Agents Chemother 2017, 61. [Google Scholar] [CrossRef]
- Soll, D.R.; Galask, R.; Isley, S.; Rao, T.V.; Stone, D.; Hicks, J.; Schmid, J.; Mac, K.; Hanna, C. Switching of Candida albicans during successive episodes of recurrent vaginitis. J Clin Microbiol 1989, 27, 681–690. [Google Scholar] [CrossRef]
- MacCallum, D.M.; Coste, A.; Ischer, F.; Jacobsen, M.D.; Odds, F.C.; Sanglard, D. Genetic dissection of azole resistance mechanisms in Candida albicans and their validation in a mouse model of disseminated infection. Antimicrob Agents Chemother 2010, 54, 1476–1483. [Google Scholar] [CrossRef] [PubMed]
- Rex, J.H.; Nelson, P.W.; Paetznick, V.L.; Lozano-Chiu, M.; Espinel-Ingroff, A.; Anaissie, E.J. Optimizing the correlation between results of testing in vitro and therapeutic outcome in vivo for fluconazole by testing critical isolates in a murine model of invasive candidiasis. Antimicrob Agents Chemother 1998, 42, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Nyirjesy, P.; Brookhart, C.; Lazenby, G.; Schwebke, J.; Sobel, J.D. Vulvovaginal Candidiasis: A Review of the Evidence for the 2021 Centers for Disease Control and Prevention of Sexually Transmitted Infections Treatment Guidelines. Clinical Infectious Diseases 2022, 74, S162–S168. [Google Scholar] [CrossRef]
- Akinosoglou, K.; Schinas, G.; Polyzou, E.; Tsiakalos, A.; Donders, G.G.G. Probiotics in the Management of Vulvovaginal Candidosis. J Clin Med 2024, 13. [Google Scholar] [CrossRef]
- Donders, G.G.G.; Viera Baptista, P. The ReCiDiF method to treat recurrent vulvovaginal candidosis: A friend with benefits. Aust N Z J Obstet Gynaecol 2018, 58, E5. [Google Scholar] [CrossRef]
- Donders, G.G.; Bellen, G.; Mendling, W. Management of recurrent vulvo-vaginal candidosis as a chronic illness. Gynecol Obstet Invest 2010, 70, 306–321. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



