Submitted:
19 May 2025
Posted:
20 May 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background/Objectives: Long-term residential care facilities for older people were particularly vulnerable to outbreaks during the COVID-19 pandemic due to the unique challenges these facilities face. This scoping review synthetizes international literature on barriers and facilitators to the prevention and management of outbreaks in long-term residential care facilities, identifying priorities for future pandemic preparedness. Methods: A comprehensive search was conducted in PubMed, MEDLINE (Ovid), Web of Science Core Collection, Scopus, and CINAHL databases, and English language articles published since 2019 were retrieved. The records were screened against the eligibility criteria by independent reviewers. A qualitative content analysis was performed. Results: The search identified 3222 records, of which 323 pieces of literature were included. Following the synthesis of the available evidence, the barriers and facilitators for prevention and management of outbreaks in long-term residential care facilities were mapped and presented under the following themes: 1) Infection prevention and control challenges and response to the pandemic, 2) The built environment of nursing homes, 3) Staffing of long-term residential care facilities, 4) Leadership and staff resilience, 5) Support and guidance during the pandemic. Conclusions: The findings from this scoping review highlight the necessity of adopting a comprehensive, integrated, and multidisciplinary approach to ensure preparedness and planning for future pandemics. The prevention and control of infectious disease outbreaks within long-term residential care facilities present unique challenges that require the implementation of integrated health and care systems. It is essential to develop response plans that address all critical elements of long-term residential care.
Keywords:
COVID-19
; nursing homes
; long-term residential care
; older adults
; outbreak management
1. Introduction
The COVID-19 pandemic has posed an unprecedented burden to public health systems internationally [1]. Long-term residential care facilities (LTRCFs) were particularly vulnerable due to the unique challenges these facilities face, and it has been reported that a significant proportion of COVID-19-associated deaths have been among nursing home residents [2,3]. However, there were some disparities between different countries related to the spread of infection in LTRCFs [4]. These disparities may reflect differences in nursing home characteristics and residents’ profiles, as some studies provided evidence of their respective roles in the burden of COVID-19 deaths [5,6]. Furthermore, different responses by LTRCFs to pandemic challenges may have played an even more important role in differences in the scale of outbreaks and their management.
Coronavirus will not be the last pandemic during our lifetime. Scientists warn that the threat posed by zoonoses – infectious diseases that transfer from animals to humans – is on the rise, and the likelihood of a new pandemic occurring is now greater than it has ever been.2 Therefore, we must be ready for the next health crisis. Researchers worldwide are currently sharing their findings on the challenges faced by healthcare systems and their adaptability during the pandemic [7]. This information is still being consolidated, and further research is needed on the experiences of COVID-19 at various levels of healthcare systems, including long-term residential care. Studying the lessons learned from professional, organizational, and local system responses can help inform managerial and policy responses to better prepare for future public health crises [8].
As part of pandemic preparedness, Ireland conducted a national service evaluation and scoping review of international literature to identify the factors associated with COVID-19 outbreaks in LTRCFs to improve the prevention and management of future outbreaks. This paper contributes to the body of evolving knowledge about the factors that contributed to or hindered effective outbreak management in LTRCFs, particularly nursing homes, during the COVID-19 pandemic and presents the findings from a scoping review of international literature to address the following questions:
- What were the barriers and facilitators to effective outbreak management in nursing homes?
- What were the key learnings from practice and experience that improved outbreak management in LTRCFs over the multiple waves?
- What are the priority areas for more effective infection prevention and control and future pandemic preparedness in LTRCFs?
2. Materials and Methods
A scoping review was conducted to identify and synthetize international literature on the barriers, facilitators, key learnings, and priority areas for the future, in relation to prevention and management of COVID-19 outbreaks in LTRCFs.
2.1. Protocol and Registration
A protocol was developed and refined by the research team before the start of the database searches. Due to time constraints, the protocol was not registered.
2.2. Eligibility Criteria
We included all study designs (peer-reviewed primary research, review papers, and editorials) reporting on COVID-19 outbreak management and infection control practices. Policy documents and national or international reports were eligible for inclusion. The setting and population of the eligible publications were LTRCFs for older people, including nursing homes, skilled nursing facilities, retirement homes, assisted-living facilities, residential care homes, or other facilities providing care in a congregated setting for older people. We included full-text available articles and papers that have been written in English since 2019. We excluded articles from settings that are not long-term residential care, such as accommodation services or daycare centres.
2.3. Information Sources
The searches were conducted on PubMed, MEDLINE (Ovid), Web of Science Core Collection (WOS), Scopus, and CINAHL databases. A hand search on GoogleScholar was also performed and the first 200 results were screened against the eligibility criteria.
2.4. Search
A search strategy was developed and piloted before it was fully implemented. The final searches were conducted on 19th April 2023. The final searches were conducted on 19th April 2023. Search terms included “older people”, “residential facilit*”, “Coronavirus*”, “infection prevention and control” and their entry terms. Examples of the search strings are available in Supplementary Appendix 1. The search results were de-duplicated using Endnote and Rayyan online platforms.
2.5. Selection of Sources of Evidence
The title and abstract screening were performed by three researchers independently (BD, DS, SD) using the Rayyan online platform. Each record was screened by at least two researchers before a decision about their inclusion or exclusion was made. Conflicts were resolved by group discussions. Full-text screening was done by the same researchers. Studies were identified as ineligible based on the inclusion and exclusion criteria. A PRISMA flow diagram was used to document the screening process.
2.6. Data Charting Process and Data Items
A data extraction form was developed by the researchers considering the review questions. The form had the following sections: author, year, country, setting, aim, study design, facilitators, barriers, key learnings, future recommendations, and priority areas (if reported). The form was piloted before the data extraction to ensure consistency between the researchers. Two independent researchers completed the data extraction (BD, MS).
2.7. Critical Appraisal of Individual Sources of Evidence
Since this is a scoping review, a critical appraisal of the included records was not performed. Critical appraisal is not a requirement for scoping reviews [9].
2.8. Synthesis of Evidence
A qualitative content analysis was performed, following the three steps: preparation, organising, and reporting [10]. Using a deductive approach, the researchers mapped the data to a pre-defined framework to answer the review questions. The review questions, data extraction form items, and frequency of reports guided the development process of the categories and sub-categories.
3. Results
We identified 3222 records for the title and abstract screening. After screening against the inclusion and exclusion criteria, 323 pieces of literature were included in this scoping review (Supplementary Appendix 1). Further details of the screening process are provided in Figure 1 PRISMA flow diagram.
3.1. Characteristics of Sources of Evidence
Overall, the largest source of the included pieces of literature were non-primary research such as reviews, reports, editorials, commentaries, and others (n=128). 108 articles were reported from the USA, followed by Australia (n=31), Canada (n=26), United Kingdom (n=29), France (n=18), Netherlands and Spain (n=13 each), Italy (n=12), Germany (n=11), Belgium (n=8) China and Ireland (n=7 each), Brazil (n=5), Taiwan (n=5), Singapore (n=5), Israel (n=5) and other countries, from which there were fewer than five articles identified (Hong Kong, Iran, Sweden, Korea, Lithuania, Slovakia, Saudi Arabia, Portugal, Poland, Malaysia, Turkey, Greece, Qatar, Norway, Luxembourg, Romania, Cyprus, New Zealand, South Africa) according to our search and screening criteria.
3.2. Barriers and Facilitators for Prevention and Management of Outbreaks in LTRCFs
3.2.1. Infection Prevention and Control Challenges and Response to the Pandemic
Most articles identified in the scoping review (n=200) reported facilitators or barriers to infection prevention and control (IPC) measures in LTRCFs.
Barriers to implementing testing as a preventive measure for outbreaks included lack of PPE despite the identification of positive cases, limited testing kits, budget shortages, delays in testing, and asymptomatic residents or staff where a symptom-based screening was conducted [11,12,13,14,15,16,17].
Several articles discussed issues with PPE use in LTRCFs, particularly for residents with cognitive impairment, highlighting the importance of PPE use by staff. In our scoping review, while more than half of the articles reporting on PPE focused on PPE use as a protection strategy (n= 44), the remaining articles underlined PPE availability issues (n= 21) [14,17,18,19,20,21]. caused by limited funding or budget allocation primarily to hospitals rather than LTRCFs [18,22].
Hygiene measures such as cleaning and disinfection, waste management, hand washing, and social distancing [23,24,25,26] were implemented, especially in countries with experience controlling infectious disease outbreaks such as Hong Kong and Taiwan [27,28]. However, some challenges in controlling infections included insufficient decontamination, poor hand hygiene, and overflowing bins with used PPE [29,30].
Staff working in multiple LTRCFs increased the risk of COVID-19 outbreaks [31,32,33]. To address this, the Canadian government banned staff mobility,34 and financial support was provided to employ extra staff as reported by Lum et al. [35].
As transferring residents to hospitals can pose a risk of infection spread [36], telemedicine and limiting hospital visits were suggested as alternatives during the pandemic [35,36,37], while some facilities limited hospital visits only to stable residents [36,38].
In terms of facilitating the outbreak prevention and management, international literature suggested various COVID-19 testing strategies, including universal and mass testing, targeted testing with preventive measures, routine testing, symptom-based testing, testing before new admissions to LTRCFs, testing of staff after holidays, and rapid antigen testing. Some studies described the advantages of universal testing of residents and staff in rapidly containing the COVID-19 infection [39,40,41,42]. Studies conducted in Spain and Germany have explored alternative ways to test for COVID-19, e.g., testing the nursing home’s wastewater for the virus [43] and using mouthwash testing after gargling [44] as a cost-effective and fast screening method.
Another significant preventive measure reported in the articles (n=21) was vaccination, especially after the authorisation of the emergency use of the COVID-19 vaccine on December 11, 2020 [14,45,46,47,48,49,50].
Facilities implemented visitor restrictions and new admissions bans to control the virus spread in Hong Kong [35], Belgium, France, Germany, and Italy [51], the USA [26], Turkey [52], and the UK [53]. The IPC measures and visitor screening were also recommended in the USA studies [36,54,55]. Evans [56] suggested screening visitors for international travel, respiratory symptoms, and contact with COVID-19 patients.
Another IPC measure in the LTRCFs was the staff’s daily body temperature screening, however it needed to be complemented with other screening measures [28,51].
The scoping review results indicate that effective IPC measures can be implemented in nursing homes through government support via updated guidance, funding, resource allocation, and addressing staff shortages [22,35,57,58]. Countries that learned lessons from airborne infections like SARS/MERS were better prepared to manage COVID-19. A study conducted in Hong Kong by Lum et al. [35] found that public health interventions and changes in population behaviour were successful in preventing COVID-19 infections in LTRCFs or adult daycare centres.
Overall, after analysing the data from all articles that reported on IPC, it was found that a weakness in one IPC strategy could lead to other weaknesses. Despite the strengths of IPC measures, other challenges mentioned further might have acted as barriers to the prevention and control of COVID-19 outbreaks in LTRCFs.
3.2.2. Social Model of Care and the Built Environment of Nursing Homes
In total, 54 articles were identified that reported building-related factors for IPC implementation. The building characteristics were reported as both a facilitator and a barrier. Most of the barriers were related to facilities’ size and location, availability of communal areas for residents, poor ventilation, inappropriate facilities for isolation, overcrowding, and residents with dementia and wandering behaviour. The factors to overcome these barriers were reported as the important role of nursing home design, including smaller building size, facilities consisting of several buildings, the availability of single ensuite rooms, and better ventilation in preventing and controlling outbreaks.
The size of a nursing home facility played a crucial role in controlling the spread of COVID-19 infection. Larger facilities faced more challenges due to their building design and staff working with both COVID-19-positive and negative residents [30,31,59,60]. In contrast, smaller facilities with single ensuite rooms were more flexible in responding to infection risk and had fewer deaths and COVID-19 cases [61]. The role that the built environment plays in achieving a balance between IPC and the quality of life of nursing home residents was viewed as an important issue. For example, the greenhouse model [62,63,64], which involves creating small, residential-style houses with 10-12 residents and has three core values: being a real home, ensuring a meaningful life, and having empowered staff, was viewed as a significant facilitator.
Communal places like dining rooms and shared spaces were key factors in the spread of airborne infections in LTRCFs [63,65,66,67]; therefore, spending time and eating in individual rooms was suggested.68 Indoor environment characteristics, such as clutter, porous surfaces, and inadequate cleaning of communal areas and residents’ rooms, were also identified as barriers to outbreak management [65]. High-quality air and ventilation were reported as key factors to prevent airborne infections by reducing the concentration of pathogenic viruses in LTRCFs [56,69,70], while poor ventilation was a barrier to managing viral spreading [63,71,72]. An Australian study by Brass et al. [72] found that places with poor ventilation and areas where staff did not use masks, such as lunchrooms, become dangerous sources of airborne infection. CO2 levels in such areas did not return to baseline levels for several hours after these peak periods. As a solution to this risk, refreshing the indoor air in shared areas with effective natural or forced ventilation [72,73] and high-quality air filtration systems and CO2 control [72,74,75] were recommended.
Inappropriate isolation facilities for COVID-19-positive residents were reported as another barrier to IPC in LTRCFs [13,63,76,77]. Goldstein et al. [76] recommended not releasing COVID-19-positive residents from hospitals until proper isolation can be provided at the facility. In addition to poor isolation facilities, residents with dementia who had limited cognitive capacity to comply with isolation principles were a significant risk for infection transmission to themselves and others [78,79,80].
The location of care facilities near densely populated areas poses a challenge in preventing COVID-19 outbreaks due to community-acquired infections [59,81]. Australian studies have shown that community transmission is a strong predictor of outbreaks,65 and nursing homes in metropolitan areas are at higher risk [82].
3.2.3. Nursing Home Staffing
Staffing issues were highlighted in the literature as a significant challenge to coping with the COVID-19 pandemic. There were 123 articles that addressed staff factors in COVID-19 outbreak management. Most of the barriers to outbreak management related to staff issues were staff shortages, lack of paid home isolation periods for staff who tested positive, non-healthcare staff in the facility, temporary staff issues, high turnover rates, lack of policies to support staff, and limited numbers of highly-skilled staff due to financial concerns [12,31,83,84,85,86]. Aïdoud et al. [87] from France argued that geographically isolated nursing homes were challenged with fewer medical and nursing resources. Although self-isolation of staff in their homes (paid isolation leave) was suggested [67,76,88], COVID-19-positive staff in some facilities continued to work [84] due to significant staff shortages.
Facilities were concerned about the intensity of staff movement as it posed a challenge to control the infection spread. To address this issue, some facilities suggested non-essential healthcare workers work remotely.89 Additional staff allocation from a single centre and government financial support to recruit extra staff and deploy staff from different areas of healthcare were found to help address staff shortages [90,92,93].
A small group of studies referred to the support provided to facilities by other healthcare professionals such as staff from Red Cross in Germany [92], military personnel in Canada [85] and Israel [19], charity organisations [19], and non-healthcare staff, however, on some occasions, their IPC knowledge level was concerning. To address this, extensive training was provided to all staff, including non-healthcare staff such as security, cleaning, catering, and others [58,94].
Isolation as an IPC measure during residents’ new admissions or readmissions to the facility from a hospital helped identification of positive cases and prevented outbreaks [66,95,96,97,98,99]. A USA policy recommendation document recommended units having separate entrances/exits or installing temporary walls/doorways for new admissions or re-admissions of COVID-19-positive residents [99]. Although a self-isolation of COVID-19-positive staff in their homes was proposed as an IPC strategy [38,40], this was not always possible for many facilities with staff shortages and there were suggestions that asymptomatic COVID-19-positive staff could work with COVID-19-positive residents [89].
Our scoping review identified that some facilities (especially for-profit) prefer to employ less-skilled or temporary staff to reduce salary costs due to limited budget [30,31,32], while some studies reported that for-profit facilities had more COVID-19 cases [12,82,100]. Recruitment of permanent staff in nursing homes was suggested to address this issue65; however, resource allocation and business models in private nursing homes were the main factors preventing that.
Staff IPC training, including PPE use, was another prominent area reported in the international literature for COVID-19 outbreak prevention and management. Some studies emphasised that staff with inadequate training on PPE use were a risk of spreading the infection [101,102]. In the USA, Cigler [68] found that a significant number of staff were not trained in containment protocols, although, according to Blackman et al. [78], facility-wide mandatory staff training was implemented as part of IPC strategies during the pandemic. As a solution to overcome this challenge, trained IPC nurses (especially registered nurses as infection prevention specialists) were assigned to update staff knowledge on IPC and observe their PPE use [55,91,92,103]. Gosch et al. [55] from Germany recommended designating a person within each LTRCF to lead and coordinate IPC measures.
3.2.4. Leadership and Staff Practices
The COVID-19 pandemic taught many lessons to the world, some of which highlighted the importance of leadership and the power of well-trained staff [13,23,66]. In our scoping review, 51 articles reported on the leadership and resilience of staff during the COVID-19 pandemic. Especially during earlier waves of the pandemic, LTRCF staff faced significant challenges, fear, and anxiety, mostly due to fighting against the unknown while protecting their vulnerable residents.
The COVID-19 pandemic caused negative psychological impact on staff because of the new, highly contagious infection that resulted in high mortality rates in vulnerable population [104], including self-blaming, fear of spreading infection to themselves and their families, concerns about their residents [104,105,106,107], and blaming by the media [31,105,108,109]. Shiftwork for long hours increased the risk of acquiring infection [101,110] and staff burnout [105]. On the other hand, there were discussions on staff commitment and resilience during the pandemic. To reduce the fear of the unknown among staff, it was recommended to create IPC teams consisting of nurses, doctors, caregivers, and LTRCF managers and organise up-to-date training sessions and short daily meetings [106]. In a study by White et al. [105], the importance of teamwork was highlighted to alleviate fears and cope with the emotional impact of illness and death in nursing homes and in the news by sharing their goals of improving the residents’ care and supporting each other in various roles as caregivers, entertainers, spiritual supporters, or family members. Baughman et al. [111] from the USA conducted a 16-week virtual interactive educational IPC series, which enabled nursing home leaders to create a supportive peer-learning community with timely updates on COVID-19 infection control practices as well as emotional support, therefore, similar initiatives may provide valuable mechanisms to support staff resilience and well-being. Furthermore, well-trained and highly skilled staff could take leadership roles in LTRCFs [90,91,112], which is a strong facilitator for effective outbreak prevention and management.
3.2.5. Support and Guidance Received During the Pandemic
In the COVID-19 era, we learned the importance of communication and collaboration in healthcare settings. In this scoping review, 100 articles reported on the help, support, and guidance that enabled cooperation between facilities and healthcare authorities. While the main barriers to outbreak management were lack of government financial support and guidance and LTRCF staff’s knowledge and skills limitations on responding to the rapid deterioration of residents due to COVID-19, examples of facilitators were: staff training, a collaboration between hospitals and LTRCFs, publishing evidence-based best practice guidelines, updating staff about new guidelines on COVID-19 management, and providing mobile or virtual specialist teams to consult residents [65,66,76,87,90,91,92,109,113,114].
Additionally, it was essential to guide staff on how to find and access updated information. For example, in a guideline published by the Australian Government [115], they listed information-sharing channels such as stakeholders, bulk information distribution services, and newsletters.
The literature also reported on assigning IPC champions as designated persons within each LTRCF who were trainers responsible for IPC measures and observation of staff IPC practices [55,65,114,115].
During the pandemic, LTRCFs faced complex COVID-19 cases due to residents’ comorbidities and frailty. To address this challenge, support from multidisciplinary geriatric teams was crucial. The articles reporting on collaboration between acute care facilities (e.g., specialist or geriatric teams) and LTRCFs discussed it as a strategy for timely testing and identifying positive cases, timely access to tests and PPE, and getting expert support for the management of positive cases [118,119,120]. This collaboration and support could be achieved by conducting mobile or virtual team visits [110,119,121].
3.2.6. Learning and Priorities
Most studies in this scoping review highlighted the importance of a comprehensive IPC approach to managing outbreaks in LTRCFs, which includes rigorous IPC measures, early detection and timely isolation, adequate built environment in LTRCFs (e.g., facility design, ventilation, and other engineering measures), and vaccination.
One of the key learnings for future pandemic preparedness made visible by this scoping review was developing and having at disposal an effective and efficient contingency plan at all levels that includes training staff and empowering them in decision-making and embedding IPC into work culture.
Most studies in this scoping review demonstrated that the effectiveness of outbreak prevention and control strongly depends on the preventive attitudes and behaviours among LTRCF staff, such as the thorough implementation of IPC measures and adherence to IPC measures by everyone. Many studies emphasised that training all staff, including non-clinical support staff, was important to ensure everyone followed IPC measures, and often the persons-in-charge were trained to train further the nursing home staff.
National- and facility-level leadership, intersectoral collaboration, and policies that facilitate access to critical resources were all significant enablers of success. Greater integration between hospitals and residential care services, especially regarding staff mobility and readiness to work in different environments was recommended in many studies.
4. Discussion
This scoping review was conducted to explore international literature on factors contributing to outbreak prevention and management in long-term residential care facilities (LTRCFs). It specifically focused on barriers, facilitators, key learnings, and priority areas for the future in relation to COVID-19 outbreaks in LTRCFs to inform policymakers and decision-makers about future pandemic preparedness with support from a synthesis of the international literature.
The COVID-19 pandemic had multiple negative impacts on LTRCFs, especially nursing homes. Our scoping review highlighted numerous ‘fragilities’ in this sector that contributed to poor outcomes, but we also identified multiple facilitators that successfully mitigated some of the adverse impacts. Multiple factors simultaneously contributed to the challenges including infection prevention and control challenges, the built environment of nursing homes, nursing home staffing, leadership and staff practices, and support and guidance received during the pandemic. Findings from this scoping review show many commonalities across organisational, environmental, and individual factors, such as the need for adequate staff levels and training, adequate facilities, and clear communication of guidelines and protocols, that impact the ability to effectively manage the COVID-19 outbreaks in LTRCFs [122] and require multidisciplinary approach and action at all levels [123,124,125]. A scoping review conducted by Giri et al. [122] to describe factors that contributed to the spread and mortality of COVID-19 in nursing homes and provide an overview of responses that were implemented, found that both internal (facility and resident characteristics, staff, and asymptomatic transmission) and external (community infection rates, admissions, and PPE) factors predisposed nursing homes to an increased propensity of spread. Numerous strategies were employed to attempt to mitigate the negative impacts such as widespread testing, isolation and cohorting, staff protection, using technology in care, and physical and mental health support for residents. The review found that changes can be implemented in the physical spaces, practices, and regulations of nursing homes in response to the pandemic. These changes are aimed at preparing for any future pandemics and improving the overall quality of care provided.
This scoping review highlighted the importance of a comprehensive IPC approach to manage outbreaks in LTRCFs. Similar to our results, previous studies found that symptom-based or temperature-based screening and single-point-prevalence testing were found to be ineffective, and repeated universal testing of residents and staff was considered crucial [126,127] as asymptomatic and symptomatic cases may have a similar potential for transmission [128].
To ensure the success of comprehensive outbreak management in future public health crises effective preparedness strategies need to be applied. Likewise, the value of having a detailed formal contingency plan and emergency response protocols in place, which are essential for outbreak prevention and control, was stressed in other studies [125,129]. A key goal of future effective contingency plans is to use complex information to develop integrated models that capture the factors underlying effective outbreak management. A framework was proposed by Behrens and Naylor [125] designed to solicit active engagement from nursing home leaders, government agencies, and other key stakeholders, to facilitate internal and external decision-making and collective action. This framework aims to address public health threats and identifies policy options focused on ensuring a shared understanding of changes in nursing homes’ operations throughout the COVID-19 crisis, improving access to additional essential resources needed to mitigate the impact of the crisis, and promoting shared accountability for consistently achieving accepted standards in core quality domains. Yoon et al. [129] suggested a 6-domain plan to establish a better healthcare system that is prepared to manage a pandemic, which includes medical institutions (including LTCRFs), workforce (supply, training, deployment, well-being), equipment (supply and allocation of resources), COVID-19 surveillance (rapid detection), data and information application (management and sharing), and governance structure. Similarly, at the organisational level, carefully formulating realistic contingency plans, consistent with available resources, is important to improve staff preparedness in the event of a recurrence of the pandemic [129]. Decision-makers play a crucial role in managing outbreaks. They are responsible for staffing, logistics, public health interventions, communication with professionals and the public, planning for future response needs, and setting priorities for funding. To do this, decision-makers must quickly analyse data from various experts across different fields, identify gaps in the data, and use epidemiological analysis to make operational decisions, therefore, a cooperative approach and coordinated efforts can improve decision-making in outbreak response. Thus, a structured approach that will improve the response during outbreaks and reduce the scale of outbreaks needs to be developed [129].
Most studies in this scoping review demonstrated that the effectiveness of outbreak prevention and control strongly depends on the preventive attitudes and behaviours among LTRCF staff, such as adherence to and thorough implementation of IPC measures by everyone. Indeed, given that much behaviour results from decision-making and self-regulation [130], social and behavioural factors are critical to the emergence, spread, and containment of the human disease, and are key determinants of the course, duration, and outcomes of disease outbreaks [131]. Most of the studies included in this scoping review had a common theme running through them - that LTRCF staff showed a great deal of commitment and resilience, despite being faced with the challenge of dealing with an unknown epidemic outbreak. This trait proved to be a strong facilitator and was essential in mitigating the outbreak, even though these nursing homes had limited resources, and their built environments were not conducive for such situations. A Cochrane review [132], showed that a “duty of care” was perceived as an important influence on whether healthcare workers could, or could not, adhere to the guidelines. The review found that when healthcare workers felt they placed a high value on the importance of IPC, they had increased adherence, and incorporated IPC more intuitively into routine practice [133]. Workplaces where all staff adhered to IPC guidelines created a culture whereby healthcare workers had a sense of “pulling together” [134]. Healthcare workers felt they should take professional responsibility for effective control practices [135,136,137]. In addition, peer pressure in the workplace could facilitate adherence, and healthcare workers would remind each other to wear masks/respirators [135,137,138,139]. Lam’s 2018 [138] review that analysed nurses’ readiness for infectious disease outbreaks highlights the importance of leadership, support, training, and education, in addition to individual factors such as knowledge and professional values. Likewise, it was clear in our scoping review that leadership was an important factor in the adoption of preventive attitudes among LTRCF staff and adherence to IPC measures.
To ensure staff are fully and confidently engaged in IPC practices, staff IPC training is an important prerequisite. Nursing homes urgently responded to the COVID-19 pandemic by providing rapid and intensive staff training. Specifically, staff were trained on best practices for preventing the spread of COVID-19 within the nursing home environment and the appropriate protocols to follow in case of an outbreak. Many studies emphasised that training all staff, including non-clinical and support staff, was important to ensure everyone followed IPC measures, and often the persons-in-charge in nursing homes were trained to further train the nursing home staff [141,142].
A systematic review by Nexø et al. [143] suggested that train-the-trainer models can be effective, affordable, and time-saving alternatives to other training programs, considering staff shortages faced by most healthcare systems. Globally, the LTRCF staff training on IPC was one of the identified priorities described in many studies and was instrumental in building capacity through both in-person and virtual training, the latter being most appropriate in the pandemic situation [144].
Lastly, this scoping review showed that the built environment’s role in achieving a balance between infection prevention and control and the quality of life of nursing home residents is a critical issue that needs more attention and reconsideration. The nursing home designs can adversely affect older people, and these problems have been exacerbated by COVID-19 and the associated failures in infection control [63,145,146]. In addition to physical health issues, LTCRFs’ built environment exacerbates psychosocial and mental health challenges brought by COVID-19 due to quarantine, constrained social interaction, restricted visits from family and friends, the cancellation of shared activities, or the wearing of personal protective equipment by staff [147,148].
While most design strategies have been reactive to the context of COVID-19, it is essential to have a proactive approach to improving the quality of life through architectural design. Anderson et al. [63] proposed a multi-scalar model (at macro-, meso-, and micro-levels) that provides convergence between design for infection control and design for improved quality of life that leads to nursing home resilience and, eventually, pandemic readiness.
Designing nursing homes that are adaptable in the face of changing conditions is crucial to prepare for potential vulnerabilities and serious consequences of infectious outbreaks, therefore healthcare leaders need to collaborate with architects and designers to create design solutions for LTRCFs that promote quality of life while also preparing for pandemics and other crises [63].
Future pandemics are inevitable [2]. Still, we can reduce the risk, especially for vulnerable populations such as nursing home residents, by being prepared and incorporating the necessary changes in healthcare infrastructures based on the lessons learned from the COVID-19 pandemic internationally.
5. Limitations
Some limitations should be noted regarding this scoping review. While the authors took many steps to ensure all relevant articles were included in the review, it is possible some studies were missed due to the selection of only English language material. The strength of this review is that we applied a systematic and rigorous search strategy to retrieve relevant articles according to the review questions. Although this research cannot reflect the entire body of research on COVID-19 worldwide, it suggests some evidence for and provides information for the research community, policymakers, and health professionals to revise policies and practices and identify new research areas for future pandemic preparedness.
6. Conclusions and Future Directions
The risk of infectious disease is shared worldwide in an increasingly interconnected world. Findings from this scoping review suggest a comprehensive, integrated, multidisciplinary approach to preparedness planning for future pandemics. The COVID-19 pandemic, including the rapid global circulation of evolved strains, emphasizes the need for a collaborative global strategy for infectious disease research and control. This necessity arises because the prevention and control of infectious disease outbreaks are complex and require integrated health and care systems, alongside response plans that consider all essential aspects of long-term residential care, including an adequate built environment and capable, empowered staff. With the knowledge gained, every LTRCF, particularly nursing homes, can formulate new pandemic preparedness plans that incorporate staff reorganization, PPE procurement, and efficient space allocation strategies. Planning is only one aspect of being future-ready; another is fostering the systems and mindset necessary to manage situations of this scale. For this, employee education, support, and safety are vital. These steps will ensure that the long-term residential care and healthcare systems respond logically and efficiently during these and future challenging times. Undoubtedly, the insights gained from the crisis will guide our actions in the post-COVID-19 world.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, D.S. and E.O.; methodology, D.S., B.D., S.D. and M.S.; writing—original draft preparation: S.D., B.D. and D.S.; writing—review and editing, S.D., B.D., E.O., M.S. and D.S; supervision, S.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Health Services Executive of the Government of Ireland.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments). Where GenAI has been used for purposes such as generating text, data, or graphics, or for study design, data collection, analysis, or interpretation of data, please add “During the preparation of this manuscript/study, the author(s) used [tool name, version information] for the purposes of [description of use]. The authors have reviewed and edited the output and take full responsibility for the content of this publication.”
Conflicts of Interest
The authors declare no conflict of interest.
References
- COVID-19 Excess Mortality Collaborators. Estimating excess mortality due to the COVID-19 pandemic: A systematic analysis of COVID-19-related mortality, 2020–2021. Lancet 2022, 399, 1513–1536. [Google Scholar] [CrossRef] [PubMed]
- Smith, J. Future pandemics are inevitable, but we can reduce the risk. [Internet]. Horizon. The EU Research & Innovation Magazine. 2021 Dec [cited 2024 Aug 24]. Available from: https://projects.research-and-innovation.ec.europa.eu/en/horizon-magazine/qa-future-pandemics-are-inevitable-we-can-reduce-risk.
- Chidambaram, P. Kaiser Family Foundation Issue Brief: state reporting of cases and deaths due to COVID-19 in long-term care facilities. Accessed April 26, 2020. https://www.kff.org/medicaid/issue-brief/state-reporting-of-cases-and-deaths-due-to-covid-19-in-long-term-care-facilities/. 26 April.
- ECDC Public Health Emergency Team; Danis, K.; Fonteneau, L.; Georges, S.; Daniau, C.; Bernard-Stoecklin, S.; Domegan, L.; O’Donnell, J.; Hauge, S.H.; Dequeker, S.; et al. High impact of COVID-19 in long-term care facilities, suggestion for monitoring in the EU/EEA, May 2020. Eurosurveillance 2020, 25, 2000956. [Google Scholar] [PubMed]
- Cazzoletti, L.; Zanolin, M.E.; Tussardi, I.T.; Alemayohu, M.A.; Zanetel, E.; Visentin, D.; Fabbri, L.; Giordani, M.; Ruscitti, G.; Benetollo, P.P.; et al. Risk Factors Associated with Nursing Home COVID-19 Outbreaks: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 8434. [Google Scholar] [CrossRef]
- Brown, K.A.; Jones, A.; Daneman, N.; Chan, A.K.; Schwartz, K.L.; Garber, G.E.; Costa, A.P.; Stall, N.M. Association Between Nursing Home Crowding and COVID-19 Infection and Mortality in Ontario, Canada. JAMA Intern. Med. 2021, 181, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Chemali, S.; Mari-Sáez, A.; El Bcheraoui, C.; Weishaar, H. Health care workers’ experiences during the COVID-19 pandemic: a scoping review. Human resources for health. 2022, 20, 27. [Google Scholar] [CrossRef]
- Turner S, Botero-Tovar N, Herrera MA, et al. Systematic review of experiences and perceptions of key actors and organisations at multiple levels within health systems internationally in responding to COVID-19. Implementation Sci. 2021, 16. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; Hempel, S. PRISMA extension for scoping reviews (PRISMA-ScR), checklist and explanation. Annals of internal medicine. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. Journal of advanced nursing. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Brainard, J.; Rushton, S.; Winters, T.; Hunter, P.R. Introduction to and spread of COVID-19-like illness in care homes in Norfolk, UK. Journal of Public Health. 2021, 43, 228–235. [Google Scholar] [CrossRef]
- Braun, R.T.; Yun, H.; Casalino, L.P.; Myslinski, Z.; Kuwonza, F.M.; Jung, H.Y.; Unruh, M.A. Comparative performance of private equity–owned US nursing homes during the COVID-19 pandemic. JAMA network open. 2020, 3, e2026702. [Google Scholar] [CrossRef]
- Lombardo, F.L.; Bacigalupo, I.; Salvi, E.; Lacorte, E.; Piscopo, P.; Mayer, F.; Ancidoni, A.; Remoli, G.; Bellomo, G.; Losito, G. Italian National Institute of Health Nursing Home Study Group. The Italian national survey on Coronavirus disease 2019 epidemic spread in nursing homes. Int. J. Geriatr. Psychiatry. 2021, 36, 873–882. [Google Scholar] [CrossRef]
- Lynn, J. Playing the cards we are dealt: covid-19 and nursing homes. Journal of the American Geriatrics Society. 2020, 68, 1629. [Google Scholar] [CrossRef] [PubMed]
- McGarry, B.E.; Grabowski, D.C.; Barnett, M.L. Severe staffing and personal protective equipment shortages faced by nursing homes during the COVID-19 pandemic: study examines staffing and personal protective equipment shortages faced by nursing homes during the COVID-19 pandemic. Health affairs. 2020, 39, 1812–1821. [Google Scholar] [CrossRef]
- Meershoek, A.; Broek, L.; Crea-Arsenio, M. Perspectives from the Netherlands: Responses from, Strategies of and Challenges for Long-Term Care Health Personnel. Healthcare Policy. 2022, 17, 14. [Google Scholar] [CrossRef]
- Wachholz, P.A.; Jacinto, A.F. Comment on: Coronavirus Disease 2019 in Geriatrics and Long-Term Care: The ABCDs of COVID-19. Journal of the American Geriatrics Society. 2020, 68, 1168–1169. [Google Scholar] [CrossRef] [PubMed]
- Inzitari, M.; Risco, E.; Cesari, M.; Buurman, B.M.; Kuluski, K.; Davey, V.; Bennett, L.; Varela, J.; Prvu Bettger, J. Nursing homes and long term care after COVID-19: A new ERA? The journal of nutrition health aging. 2020, 24, 1042–1046. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J.; Meschiany, G. Who Helped Long-Term Care Facilities and Who Did Not During COVID-19? A Survey of Administrators in Israel. Journal of Aging Social Policy. 2022, 1–5. [Google Scholar]
- Levitt, A.F.; Ling, S.M. COVID-19 in the long-term care setting: the CMS perspective. Journal of the American Geriatrics Society. 2020, 68, 1366–1369. [Google Scholar] [CrossRef]
- Zhang, J.; Xiao, D.; Perehudof, K.; Younis, M.M.; Zhang, W.H. The Challenges Faced by Nursing Homes During the Early COVID-19 Outbreak. Asia Pacific Journal of Public Health. 2022, 34, 453–455. [Google Scholar] [CrossRef]
- Chan, D.K.; Mclaws, M.L.; Forsyth, D.R. COVID-19 in aged care homes: a comparison of effects initial government policies had in the UK (primarily focussing on England) and Australia during the first wave. International Journal for Quality in Health Care. 2021, 33, mzab033. [Google Scholar] [CrossRef]
- Cowper, B.; Jassat, W.; Pretorius, P.; Geffen, L.; Legodu, C.; Singh, S.; Blumberg, L. COVID-19 in long-term care facilities in South Africa: No time for complacency. SAMJ: South African Medical Journal. 2020, 110. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, A.M. Suspected recurrent SARS-CoV-2 infections among residents of a skilled nursing facility during a second COVID-19 outbreak—Kentucky, July–November 2020. MMWR Morbidity and Mortality Weekly Report. 2021, 70. [Google Scholar] [CrossRef] [PubMed]
- Santana, R.F.; Silva, M.B.; Marcos, D.A.; Rosa, C.D.; Wetzel, W.; Delvalle, R. Nursing recommendations for facing dissemination of COVID-19 in Brazilian Nursing Homes. Revista brasileira de enfermagem. 2020, 73 (Suppl. 2), e20200260. [Google Scholar] [CrossRef] [PubMed]
- Meehan, A.; Uth, R.; Gadbois, E.A.; Baier, R.R.; Gravenstein, S.; Zullo, A.R.; Kabler, H.; Loiacono, M.M.; Bardenheier, B.H. Impact of COVID-19 on influenza and infection control practices in nursing homes. Journal of the American Geriatrics Society. 2023, 71, 661–665. [Google Scholar] [CrossRef]
- Chow, L. Care homes and COVID-19 in Hong Kong: how the lessons from SARS were used to good effect. Age and ageing. 2021, 50, 21–24. [Google Scholar] [CrossRef]
- Huang, C.Y.; Kuo, Y.H.; Chuang, S.T.; Yen, H.R.; Tou, S.I. The experience of executing preventive measures to protect a nursing home in Taiwan from a COVID-19 outbreak. European Geriatric Medicine. 2021, 12, 609–617. [Google Scholar] [CrossRef]
- Biven, S.; Hassell, M.; Viegas, M. Remain Vigilant for the Vulnerable! Kentucky Nurse 2021, 14–15. [Google Scholar]
- Vital COVID lessons ignored. Lamp. 2020;77(5), 12–14. Accessed Aug 27, 2024. https://issuu.com/thelampnswnma/docs/hc_thelamp_octnov20_final.
- Estabrooks, C.A. Staffing for Quality in Canadian Long-Term Care Homes. HealthcarePapers. 2021, 20, 40–50. [Google Scholar] [CrossRef]
- Frazer, K.; Mitchell, L.; Stokes, D.; Lacey, E.; Crowley, E.; Kelleher, C.C. A rapid systematic review of measures to protect older people in long-term care facilities from COVID-19. BMJ open. 2021, 11, e047012. [Google Scholar] [CrossRef]
- Jepsen, D.M.; Barker, R.T. Single-site employment (multiple jobholding) in residential aged care: A response to COVID-19 with wider workforce lessons. Australasian Journal on Ageing. 2022, 41, e298–e304. [Google Scholar] [CrossRef]
- Jones, A.; Watts, A.G.; Khan, S.U.; Forsyth, J.; Brown, K.A.; Costa, A.P.; Bogoch, I.I.; Stall, N.M. Impact of a public policy restricting staff mobility between nursing homes in Ontario, Canada during the COVID-19 pandemic. Journal of the American Medical Directors Association. 2021, 22, 494–497. [Google Scholar] [CrossRef] [PubMed]
- Lum, T.; Shi, C.; Wong, G.; Wong, K. COVID-19 and long-term care policy for older people in Hong Kong. Journal of Aging Social Policy. 2020, 32, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.R.; Huang, H.C.; Huang, H.C.; Chen, W. Preparing for COVID-19: The experiences of a long-term care facility in Taiwan. Geriatrics Gerontology International. 2020, 20, 734. [Google Scholar] [CrossRef]
- Gnasso, R.; Iommazzo, I.; Corbi, G.; Celi, F.; Iannicelli, A.M.; Ferrara, N.; Ruosi, C. Italian long-term care facilities during COVID-19 era: A review. Journal of Gerontology and Geriatrics. 2022, 70, 134–143. [Google Scholar] [CrossRef]
- Bernadou, A.; Bouges, S.; Catroux, M.; Rigaux, J.C.; Laland, C.; Levêque, N.; Noury, U.; Larrieu, S.; Acef, S.; Habold, D.; Cazenave-Roblot, F. High impact of COVID-19 outbreak in a nursing home in the Nouvelle-Aquitaine region, France, March to April 2020. BMC Infectious Diseases. 2021, 21, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Bakaev, I.; Retalic, T.; Chen, H. Universal Testing-Based Response to COVID-19 Outbreak by a Long-Term Care and Post-Acute Care Facility. Journal of the American Geriatrics Society. 2020, 68. [Google Scholar] [CrossRef]
- Escobar, D.J.; Lanzi, M.; Saberi, P.; Love, R.; Linkin, D.R.; Kelly, J.J.; Jhala, D.; Amorosa, V.; Hofmann, M.; Doyon, J.B. Mitigation of a coronavirus disease 2019 outbreak in a nursing home through serial testing of residents and staff. Clinical Infectious Diseases. 2021, 72, e394–e396. [Google Scholar] [CrossRef]
- Montoya, A.; Jenq, G.; Mills, J.P.; Beal, J.; Diviney Chun, E.; Newton, D.; Gibson, K.; Mantey, J.; Hurst, K.; Jones, K.; Mody, L. Partnering with local hospitals and public health to manage COVID-19 outbreaks in nursing homes. Journal of the American Geriatrics Society. 2021, 69, 30–36. [Google Scholar] [CrossRef]
- Zollner-Schwetz, I.; König, E.; Krause, R.; Pux, C.; Laubreiter, L.; Schippinger, W. Analysis of COVID-19 outbreaks in 3 long-term care facilities in Graz, Austria. American Journal of Infection Control. 2021, 49, 1350–1353. [Google Scholar] [CrossRef]
- Davó, L.; Seguí, R.; Botija, P.; Beltrán, M.J.; Albert, E.; Torres, I.; López-Fernández, P.Á.; Ortí, R.; Maestre, J.F.; Sánchez, G.; Navarro, D. Early detection of SARS-CoV-2 infection cases or outbreaks at nursing homes by targeted wastewater tracking. Clinical Microbiology and Infection. 2021, 27, 1061–1063. [Google Scholar] [CrossRef]
- Maricic, T.; Nickel, O.; Aximu-Petri, A.; Essel, E.; Gansauge, M.; Kanis, P.; Macak, D.; Richter, J.; Riesenberg, S.; Bokelmann, L.; Zeberg, H. A direct RT-qPCR approach to test large numbers of individuals for SARS-CoV-2. PLoS One. 2020, 15, e0244824. [Google Scholar] [CrossRef] [PubMed]
- FDA News Release, FDA Approves First COVID-19 Vaccine, Approval Signifies Key Achievement for Public Health (For Immediate Release: August 23, 2021) URL: https://www.fda.gov/news-events/press-announcements/fda-approves-first-COVID-19-vaccine#:~:text=Since%20Dec.,age%20on%20May%2010%2C%202021. Accessed on July 29th, 2024.
- Zhang, J.; Yu, Y.; Petrovic, M.; Pei, X.; Tian, Q.B.; Zhang, L.; Zhang, W.H. Impact of the COVID-19 pandemic and corresponding control measures on long-term care facilities: a systematic review and meta-analysis. Age and Ageing. 2023, 52, afac308. [Google Scholar] [CrossRef]
- Weigl, J.A.; Werlang, T.; Wessendorf, M.; Helbing, H. Vaccine-masked spread of SARS-CoV2 in an elderly care home, and how to prevent a spill-over into the general population. Journal of Public Health. 2021, 1–7. [Google Scholar] [CrossRef]
- Watts, T.; Tucker, M.; Gray, C.; Lee, K.; Modina, K.; Gray, Z. Lessons learned in preventing COVID-19 within a skilled nursing facility during the early pandemic. Geriatric Nursing. 2021, 42, 1388–1396. [Google Scholar] [CrossRef]
- Vilches, T.N.; Nourbakhsh, S.; Zhang, K.; Juden-Kelly, L.; Cipriano, L.E.; Langley, J.M.; Sah, P.; Galvani, A.P.; Moghadas, S.M. Multifaceted strategies for the control of COVID-19 outbreaks in long-term care facilities in Ontario, Canada. Preventive medicine. 2021, 148, 106564. [Google Scholar] [CrossRef] [PubMed]
- Ouslander, J.G.; Saliba, D. Early success of COVID-19 vaccines in nursing homes: Will it stick? Journal of the American Geriatrics Society. 2021, 69, 2060. [Google Scholar] [CrossRef]
- Mbalayen, F.; Dutheillet-de-Lamothe, V.; Letty, A.; Le Bruchec, S.; Pondjikli, M.; Berrut, G.; Benatia, L.; Ndiongue, B.M.; Fourrier, M.A.; Armaingaud, D.; Josseran, L. The COVID-19 pandemic and responses in nursing homes: a cross-sectional study in four European countries. International Journal of Environmental Research and Public Health. 2022, 19, 15290. [Google Scholar] [CrossRef] [PubMed]
- Aykaç, N.; Yüksel Eryiğit, Ö.; Elbek, O. Evaluation Of The Measures Taken In Nursing Homes Of The Istanbul Metropolitan Municipality During The Covid-19 Pandemic. Turkish Journal of Geriatrics/Türk Geriatri Dergisi. 2021, 24. [Google Scholar] [CrossRef]
- Burch, J.; Tort, S. What are the effects of COVID-19 entry regulation measures in long-term care facilities (LTCFs)? Cochrane Clinical Answers. 2021. [Google Scholar] [CrossRef]
- Bergman, C.; Stall, N.M.; Haimowitz, D.; Aronson, L.; Lynn, J.; Steinberg, K.; Wasserman, M. Recommendations for welcoming back nursing home visitors during the COVID-19 pandemic: Results of a Delphi panel. Journal of the American Medical Directors Association. 2020, 21, 1759–1766. [Google Scholar] [CrossRef]
- Gosch, M.; Heppner, H.J.; Singler, K. Recommendations for the management of COVID-19 pandemic in long term care facilities. MMW-Fortschritte der Medizin. 2021, 163, 52–57. [Google Scholar] [CrossRef]
- Evans, G. Coronavirus kills 32 residents in Seattle nursing homes: More testing likely to reveal many milder cases. Hospital Infection Control and Prevention. 2020, 47. [Google Scholar]
- American Geriatrics Society. American Geriatrics Society (AGS) policy brief: COVID-19 and assisted living facilities. Journal of the American Geriatrics Society. 2020, 68, 1131–1135. [Google Scholar] [CrossRef] [PubMed]
- Aitken, G.E.; Holmes, A.L.; Ibrahim, J.E. COVID-19 and residential aged care: priorities for optimising preparation and management of outbreaks. Medical Journal of Australia. 2021, 214. [Google Scholar] [CrossRef] [PubMed]
- Abrams, H.R.; Loomer, L.; Gandhi, A.; Grabowski, D.C. Characteristics of US nursing homes with COVID-19 cases. Journal of the American Geriatrics Society. 2020, 68, 1653–1656. [Google Scholar] [CrossRef]
- Burton, J.K.; McMinn, M.; Vaughan, J.E.; Fleuriot, J.; Guthrie, B. Care-home outbreaks of COVID-19 in Scotland March to May 2020: national linked data cohort analysis. Age and Ageing. 2021, 50, 1482–1492. [Google Scholar] [CrossRef]
- Zimmerman, S.; Dumond-Stryker, C.; Tandan, M.; Preisser, J.S.; Wretman, C.J.; Howell, A.; Ryan, S. Nontraditional small house nursing homes have fewer COVID-19 cases and deaths. Journal of the American Medical Directors Association. 2021, 22, 489–493. [Google Scholar] [CrossRef]
- Grinspun, D.; Matthews, J.H.; Bonner, R.; Moreno-Casbas, T.; Mo, J. COVID-19 pandemic in long-term care: an international perspective for policy considerations. International Journal of Nursing Sciences. 2023, 10, 158–166. [Google Scholar] [CrossRef]
- Anderson, D.C.; Grey, T.; Kennelly, S.; O’Neill, D. Nursing home design and COVID-19: balancing infection control, quality of life, and resilience. Journal of the American Medical Directors Association. 2020, 21, 1519–1524. [Google Scholar] [CrossRef]
- Abbasi, J. COVID-19 crisis advances efforts to reimagine nursing homes. JAMA. 2021, 326, 1568–1570. [Google Scholar] [CrossRef]
- Gilbert, G.L. COVID-19 in a Sydney nursing home: a case study and lessons learnt. The Medical Journal of Australia 2020, 213, 393. [Google Scholar] [CrossRef] [PubMed]
- Barasteh, S.; Azimi, A.V.; Khademi, F.; Goharinezhad, S.; Rassouli, M. Covid-19 and nursing home residents: The potential role of geriatric nurses in a special crisis. Nursing Practice Today. 2020. [Google Scholar] [CrossRef]
- Longmore, M. COVID-19 exposes weaknesses in aged care. Kai Tiaki: Nursing New Zealand 2020, 26, 12–13. [Google Scholar]
- Cigler, B.A. Nursing Homes and COVID-19: One State’s Experience. International Journal of Public Administration. 2021, 44, 963–973. [Google Scholar] [CrossRef]
- Vuylsteke, B.; Cuypers, L.; Baele, G.; Stranger, M.; Paralovo, S.L.; André, E.; Laga, M. The role of airborne transmission in a large single source outbreak of SARS-CoV-2 in a Belgian nursing home in 2020. Epidemics 2022, 40, 100589. [Google Scholar] [CrossRef]
- Wang, Z. Use the environment to prevent and control COVID-19 in senior-living facilities: An analysis of the guidelines used in China. HERD: Health Environments Research Design Journal. 2021, 14, 130–140. [Google Scholar] [CrossRef]
- Brass, A.; Shoubridge, A.P.; Larby, N.; Elms, L.; Sims, S.K.; Flynn, E.; Miller, C.; Crotty, M.; Papanicolas, L.E.; Wesselingh, S.L.; Morawska, L. Targeted reduction of airborne viral transmission risk in long-term residential aged care. Age and ageing. 2022, 51, afac316. [Google Scholar] [CrossRef]
- de Man, P.; Paltansing, S.; Ong, D.S.; Vaessen, N.; van Nielen, G.; Koeleman, J.G. Outbreak of coronavirus disease 2019 (COVID-19) in a nursing home associated with aerosol transmission as a result of inadequate ventilation. Clinical Infectious Diseases. 2021, 73, 170–171. [Google Scholar] [CrossRef]
- Barretto Filho, A.C.; Salotto, D.B.; Schoueri, J.F.; Tsutsui, J.M.; Granato, C.F.; Yamaguchi, M.B.; Carvalho, R.D.; Zacarias, N.; Marcelino, A.S.; Rabelo, R.; Jacob Filho, W. COVID-19 containment management strategies in a nursing home. einstein (São Paulo). 2022, 20, eAO6175. [Google Scholar] [CrossRef]
- Lynch, R.M.; Goring, R. Practical steps to improve air flow in long-term care resident rooms to reduce COVID-19 infection risk. Journal of the American Medical Directors Association. 2020, 21, 893–894. [Google Scholar] [CrossRef]
- Dykgraaf, S.H.; Matenge, S.; Desborough, J.; Sturgiss, E.; Dut, G.; Roberts, L.; McMillan, A.; Kidd, M. Protecting nursing homes and long-term care facilities from COVID-19: a rapid review of international evidence. Journal of the American Medical Directors Association. 2021, 22, 1969–1988. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, A.; Hollmann, P.; Lundebjerg, N.; et al. American Geriatrics Society. American Geriatrics Society policy brief: COVID-19 and nursing homes. Journal of the American Geriatrics Society. 2020, 68, 908–911. [Google Scholar]
- Li, J. Prevention is key to reducing the spread of COVID-19 in long-term care facilities. Infection and Drug Resistance. 2022, 6689–6693. [Google Scholar] [CrossRef] [PubMed]
- Blackman, C.; Farber, S.; Feifer, R.A.; Mor, V.; White, E.M. An illustration of SARS-CoV-2 dissemination within a skilled nursing facility using heat maps. Journal of the American Geriatrics Society. 2020, 68, 2174–2178. [Google Scholar] [CrossRef]
- Aged care: Inconsistent use of, P.P.E. Kai Tiaki Nursing New Zealand. 2020;26(8), 43. Accessed on Aug 25, 2024. https://issuu.com/kaitiaki/docs/kai_tiaki_september_2020.
- Covid-19 News. Australian Journal of Dementia Care. (2021) 10(2), 8. Accessed Aug 25, 2024. https://journalofdementiacare.com/journal-issues/supporting-meaningful-activity-in-hospital/.
- Blain, H.; Rolland, Y.; Schols, J.M.; Cherubini, A.; Miot, S.; O’Neill, D.; Martin, F.C.; Guérin, O.; Gavazzi, G.; Bousquet, J.; Petrovic, M. August 2020 interim EuGMS guidance to prepare European long-term care facilities for COVID-19. European geriatric medicine. 2020, 11, 899–913. [Google Scholar] [CrossRef]
- Ibrahim, J.E.; Li, Y.; McKee, G.; Eren, H.; Brown, C.; Aitken, G.; Pham, T. Characteristics of nursing homes associated with COVID-19 outbreaks and mortality among residents in Victoria, Australia. Australasian Journal on Ageing. 2021, 40, 283–292. [Google Scholar] [CrossRef]
- Jones, K.; Mantey, J.; Washer, L.; Meddings, J.; Patel, P.K.; Montoya, A.; Mody, L. When planning meets reality: COVID-19 interpandemic survey of Michigan Nursing Homes. American Journal of Infection Control 2021, 49, 1343–1349. [Google Scholar] [CrossRef]
- Pillemer, K.; Subramanian, L.; Hupert, N. The importance of long-term care populations in models of COVID-19. Jama. 2020, 324, 25–26. [Google Scholar] [CrossRef] [PubMed]
- Beaulieu, M.; Genesse, J.C.; St-Martin, K. High death rate of older persons from COVID-19 in Quebec (Canada) long-term care facilities: Chronology and analysis. The Journal of Adult Protection 2021, 23, 110–115. [Google Scholar] [CrossRef]
- Gopal, R.; Han, X.; Yaraghi, N. Compress the curve: a cross-sectional study of variations in COVID-19 infections across California nursing homes. BMJ open. 2021, 11, e042804. [Google Scholar] [CrossRef]
- Aïdoud, A.; Poupin, P.; Gana, W.; Nkodo, J.A.; Debacq, C.; Dubnitskiy-Robin, S.; Fougère, B. Helping nursing homes to manage the COVID-19 crisis: an illustrative example from France. Journal of the American Geriatrics Society. 2020, 68, 2475–2477. [Google Scholar] [CrossRef] [PubMed]
- Crotty, F.; Watson, R.; Lim, W.K. Nursing homes: the titanic of cruise ships–will residential aged care facilities survive the COVID-19 pandemic? Internal medicine journal. 2020, 50, 1033. [Google Scholar] [CrossRef]
- Louie, J.K.; Stoltey, J.; Scott, H.M.; DuBois, A.; Golden, L.; Philip, S.; Aragón, T.J. Early COVID-19 successes in skilled nursing facilities in San Francisco.
- Bakerjian, D.; Boltz, M.; Bowers, B.; Gray-Miceli, D.; Harrington, C.; Kolanowski, A.; Mueller, C.A. Expert nurse response to workforce recommendations made by the coronavirus commission for safety and quality in nursing homes. Nursing outlook. 2021, 69, 735–743. [Google Scholar] [CrossRef]
- Baker, N.R.; Dunn, D.; Greenberg, S.A.; Shaughnessy, M. Infection Control in Long-Term Care: An Old Problem and New Priority. Journal of the American Medical Directors Association. 2022, 23, 321. [Google Scholar] [CrossRef] [PubMed]
- Boltz, M. Long-Term Care and the COVID-19 Pandemic: Lessons Learned. Nursing Clinics. 2023, 58, 35–48. [Google Scholar]
- Eichner, L.; Schlegel, C.; Roller, G.; Fischer, H.; Gerdes, R.; Sauerbrey, F.; Schönleber, S.; Weinhart, F.; Eichner, M. COVID-19 case findings and contact tracing in South German nursing homes. BMC Infectious Diseases. 2022, 22, 307. [Google Scholar] [CrossRef]
- Huang, H.; Xie, Y.; Chen, Z.; Xiao, M.; Cao, S.; Mi, J.; Yu, X.; Zhao, Q. Nursing Home in the COVID-19 Outbreak: Challenge, Recovery, and Resiliency. Journal of gerontological social work. 2020, 63, 646–650. [Google Scholar] [CrossRef] [PubMed]
- Heudorf, U.; Müller, M.; Schmehl, C.; Gasteyer, S.; Steul, K. COVID-19 in long-term care facilities in Frankfurt am Main, Germany: incidence, case reports, and lessons learned. GMS hygiene and infection control 2020, 15. [Google Scholar]
- Kimball A, Hatfield KM, Arons M, James A, Taylor J, Spicer K, et al. Asymptomatic and presymptomatic SARS-CoV-2 infections in residents of a long-term care skilled nursing facility — King County, Washington, March 2020. MMWR Morb Mortal Wkly Rep. 2020, 69, 377–381. [Google Scholar] [CrossRef]
- Eye of the Storm. Lamp. 2020;77(3), 14–17. Accessed Aug 27, 2024. https://issuu.com/thelampnswnma/docs/hc_thelamp_junejuly20_fa3.
- Esper, J.J.; Garg, D.; McClafferty, B.R.; Golamari, R.; Jain, R. COVID-19 Isolation and Quarantine Guidelines for Older Adults in Nursing Homes. South Dakota Medicine. 2021, 74. [Google Scholar]
- Lester, P.E.; Holahan, T.; Siskind, D.; Healy, E. Policy recommendations regarding skilled nursing facility management of coronavirus 19 (COVID-19), lessons from New York state. Journal of the American Medical Directors Association. 2020, 21, 888–892. [Google Scholar] [CrossRef] [PubMed]
- Arnedo-Pena, A.; Romeu-Garcia, M.A.; Gascó-Laborda, J.C.; Meseguer-Ferrer, N.; Safont-Adsuara, L.; Prades-Vila, L.; Flores-Medina, M.; Rusen, V.; Tirado-Balaguer, M.D.; Sabater-Vidal, S.; Gil-Fortuño, M. Incidence, mortality, and risk factors of COVID-19 in nursing homes. Epidemiologia. 2022, 3, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Aghili, M.S.; Darvishpoor Kakhki, A.; Gachkar, L.; Davidson, P.M. Predictors of contracting COVID-19 in nursing homes: Implications for clinical practice. Journal of advanced nursing. 2022, 78, 2799–2806. [Google Scholar] [CrossRef] [PubMed]
- Al Hamad, H.; Malkawi, M.M.; Al Ajmi, J.A.; Al-Mutawa, M.N.; Doiphode, S.H.; Sathian, B. Investigation of a COVID-19 outbreak and its successful containment in a long term care facility in Qatar. Frontiers in Public Health. 2021, 9, 779410. [Google Scholar] [CrossRef] [PubMed]
- Dora, A.V. Universal and serial laboratory testing for SARS-CoV-2 at a long-term care skilled nursing facility for veterans—Los Angeles, California, 2020. MMWR Morbidity and mortality weekly report. 2020, 69. [Google Scholar] [CrossRef]
- Gordon, A.L.; Goodman, C.; Achterberg, W.; Barker, R.O.; Burns, E.; Hanratty, B.; Martin, F.C.; Meyer, J.; O’Neill, D.; Schols, J.; Spilsbury, K. Commentary: COVID in care homes—challenges and dilemmas in healthcare delivery. Age and ageing. 2020, 49, 701–705. [Google Scholar] [CrossRef]
- White, E.M.; Wetle, T.F.; Reddy, A.; Baier, R.R. Front-line nursing home staff experiences during the COVID-19 pandemic. Journal of the American Medical Directors Association. 2021, 22, 199–203. [Google Scholar] [CrossRef]
- Yang, X.F.; Li, M.Q.; Liao, L.L.; Feng, H.; Zhao, S.; Wu, S.; Yin, P. A qualitative study of the first batch of medical assistance team’s first-hand experience in supporting the nursing homes in Wuhan against COVID-19. Plos one. 2021, 16, e0249656. [Google Scholar] [CrossRef]
- Palacios, J.; Neckelmann, M.; Dintrans, P.V.; Salas, J.B. Improving long-term care facilities’ crisis response: Lessons from the COVID-19 in Chile. Journal of Long-Term Care 2021. [Google Scholar] [CrossRef]
- Bambury, N.; Barrett, P.M.; Crompton, J.; O’Mahony, M.T.; O’Sullivan, M.B.; Murray, D.E.; Foley Nolan, C.; Sheahan, A. Practicalities and Yield from Mass Swabbing for COVID-19 in Residential Care Facilities in the South of Ireland. Journal of Aging Social Policy. 2022, 1–8. [Google Scholar]
- Powell, T.; Bellin, E.; Ehrlich, A.R. Older adults and Covid-19: The most vulnerable, the hardest hit. Hastings Center Report. 2020, 50, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Peromingo, J.; Serra-Rexach, J.A. Long-Term Care Facilities and the COVID-19 Pandemic: Lessons Learned in Madrid. Journal of the American Geriatrics Society. 2020, 68, 1920. [Google Scholar] [CrossRef] [PubMed]
- Baughman, A.W.; Renton, M.; Wehbi, N.K.; Sheehan, E.J.; Gregorio, T.M.; Yurkofsky, M.; Levine, S.; Jackson, V.; Pu, C.T.; Lipsitz, L.A. Building community and resilience in Massachusetts nursing homes during the COVID-19 pandemic. Journal of the American Geriatrics Society. 2021, 69, 2716–2721. [Google Scholar] [CrossRef]
- Li, Y.; Temkin-Greener, H.; Shan, G.; Cai, X. COVID-19 infections and deaths among Connecticut nursing home residents: facility correlates. Journal of the American Geriatrics Society. 2020, 68, 1899–1906. [Google Scholar] [CrossRef]
- Kolanowski, A.; Cortes, T.A.; Mueller, C.; Bowers, B.; Boltz, M.; Bakerjian, D.; Harrington, C.; Popejoy, L.; Vogelsmeier, A.; Wallhagen, M.; Fick, D. A call to the CMS: Mandate adequate professional nurse staffing in nursing homes. AJN The American Journal of Nursing. 2021, 121, 24–27. [Google Scholar] [CrossRef]
- Lamb, M.J.; La Delfa, A.; Sawhney, M.; Adams, D.; Abdel-Shahied, K.; Belfer, T.; Schembri, J.; Katz, K. Implementation and evaluation of an IPAC SWAT team mobilized to long-term care and retirement homes during the COVID-19 pandemic: A pragmatic health system innovation. Journal of the American Medical Directors Association. 2021, 22, 253–255. [Google Scholar] [CrossRef]
- Australian Government. National COVID-19 Residential Aged Care Emergency Communication Guide. 2021, 10(4), 39. Accessed Aug 28, 2024. www.health.gov.au/sites/default/files/documents/2021/09/national-covid-19-residential-aged-care-emergency-communication-guide.
- 70(8), 273.
- Championing education for COVID-19. (2020) Lamp. 77(6), 31. Accessed Aug 28, 2024. https://search.informit.org/doi/abs/10.3316/informit. 3324.
- Cofais, C.; Veillard, D.; Farges, C.; Baldeyrou, M.; Jarno, P.; Somme, D.; Corvol, A. COVID-19 epidemic: Regional organization centered on nursing homes. Journal of the American Geriatrics Society. 2020, 68, 2191. [Google Scholar] [CrossRef] [PubMed]
- Colas, A.; Baudet, A.; Regad, M.; Conrath, E.; Colombo, M.; Florentin, A. An unprecedented and large-scale support mission to assist residential care facilities during the COVID-19 pandemic. Infection Prevention in Practice. 2022, 4, 100234. [Google Scholar] [CrossRef]
- Liu, M.; Maxwell, C.J.; Armstrong, P.; Schwandt, M.; Moser, A.; McGregor, M.J.; Bronskill, S.E.; Dhalla, I.A. COVID-19 in long-term care homes in Ontario and British Columbia. Cmaj. 2020, 192, E1540–E1546. [Google Scholar] [CrossRef]
- Ni Chroinin, D.; Patil, A. Geriatric outreach to residential aged care: Embracing a dynamic approach in the COVID-19 era. Australas J Ageing. 2020, 39, 310. [Google Scholar] [CrossRef]
- Giri, S.; Chenn, L.M.; Romero-Ortuno, R. Nursing homes during the COVID-19 pandemic: a scoping review of challenges and responses. European Geriatric Medicine. 2021, 12, 1127–1136. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.J.; Monsen, K.A.; Jeppesen, B.; Hanson, C.; Nichols, K.; O’Neill, K.; Lundblad, J. Interprofessional roles and collaborations to address COVID-19 pandemic challenges in nursing homes. Interdisciplinary journal of partnership studies. 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Poupin, P.; N’diaye, D.; Chaumier, F.; Lemaignen, A.; Bernard, L.; Fougère, B. Management of COVID-19 in a French nursing home: experiences from a multidisciplinary mobile team. The Journal of Frailty Aging. 2021, 10, 363–366. [Google Scholar] [CrossRef] [PubMed]
- Behrens, L.L.; Naylor, M.D. “We are alone in this battle”: a framework for a coordinated response to COVID-19 in nursing homes. Journal of aging social policy. 2020, 32, 316–322. [Google Scholar] [CrossRef]
- Arons, M.M.; Hatfield, K.M.; Reddy, S.C.; Kimball, A.; James, A.; Jacobs, J.R.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; Tanwar, S. Presymptomatic SARS-CoV-2 infections and transmission in a skilled nursing facility. New England journal of medicine. 2020, 382, 2081–2090. [Google Scholar] [CrossRef]
- Sanchez, G.V. Initial and repeated point prevalence surveys to inform SARS-CoV-2 infection prevention in 26 skilled nursing facilities—Detroit, Michigan, March–May 2020. MMWR. Morbidity and mortality weekly report. 2020, 69. [Google Scholar] [CrossRef]
- Patel, M.C.; Chaisson, L.H.; Borgetti, S.; Burdsall, D.; Chugh, R.K.; Hoff, C.R.; Murphy, E.B.; Murskyj, E.A.; Wilson, S.; Ramos, J.; Akker, L. Asymptomatic SARS-CoV-2 infection and COVID-19 mortality during an outbreak investigation in a skilled nursing facility. Clinical Infectious Diseases. 2020, 71, 2920–2926. [Google Scholar] [CrossRef]
- Yoon, Y.K.; Lee, J.; Kim, S.I.; Peck, K.R. A systematic narrative review of comprehensive preparedness strategies of healthcare resources for a large resurgence of COVID-19 nationally, with local or regional epidemics: present era and beyond. Journal of Korean Medical Science. 2020, 35. [Google Scholar] [CrossRef]
- Godin, G.; Bélanger-Gravel, A.; Eccles, M.; Grimshaw, J. Healthcare professionals’ intentions and behaviours: a systematic review of studies based on social cognitive theories. Implementation science. 2008, 3, 1–2. [Google Scholar] [CrossRef]
- Bedson, J.; Skrip, L.A.; Pedi, D.; Abramowitz, S.; Carter, S.; Jalloh, M.F.; Funk, S.; Gobat, N.; Giles-Vernick, T.; Chowell, G.; de Almeida, J.R. A review and agenda for integrated disease models including social and behavioural factors. Nature human behaviour. 2021, 5, 834–846. [Google Scholar] [CrossRef]
- Cochrane Effective Practice and Organisation of Care Group; Houghton, C.; Meskell, P.; Delaney, H.; Smalle, M.; Glenton, C.; Booth, A.; Chan, X.H.; Devane, D.; Biesty, L.M. Barriers and facilitators to healthcare workers’ adherence with infection prevention and control (IPC) guidelines for respiratory infectious diseases: a rapid qualitative evidence synthesis. Cochrane database of systematic reviews. 1996, 2020. [Google Scholar]
- Tan, N.C.; Goh, L.G.; Lee, S.S. Family physicians’ experiences, behaviour, and use of personal protection equipment during the SARS outbreak in Singapore: do they fit the Becker Health Belief Model? Asia-Pacific Journal of Public Health / Asia-Pacific Academic Consortium for Public Health 2006, 18, 49–56. [Google Scholar] [CrossRef]
- Corley, A.; Hammond, N.E.; Fraser, J.F. The experiences of health care workers employed in an Australian intensive care unit during the H1N1 influenza pandemic of 2009: a phenomenological study. International Journal of Nursing Studies 2010, 47, 577–585. [Google Scholar] [CrossRef]
- Adeleke, O. Barriers to the implementation of tuberculosis infection control among South African healthcare workers - Emerging Public Health Practitioner Awards. South African Health Review 2012, 2012/2013, 197–203. [Google Scholar]
- Chapman, H.J.; Veras-Estevez, B.A.; Pomeranz, J.L.; Perez-Then, E.N.; Marcelino Bs Lauzardo, M. Perceived barriers to adherence to tuberculosis infection control measures among health care workers in the Dominican Republic. MEDICC Review 2017, 19, 16–22. [Google Scholar] [PubMed]
- Woith, W.; Volchenkov, G.; Larson, J. Barriers and motivators affecting tuberculosis infection control practices of Russian health care workers. International Journal of Tuberculosis and Lung Disease 2012, 16, 1092–1096. [Google Scholar] [CrossRef]
- Zinatsa, F.; Engelbrecht, M.; Van Rensburg, A.J.; Kigozi, G. Voices from the frontline: barriers and strategies to improve tuberculosis infection control in primary health care facilities in South Africa. BMC Health Services Research 2018, 18, 269. [Google Scholar] [CrossRef]
- Moore D, Gamage B, BE, Copes R, Yassi A, BC Interdisciplinary Respiratory Protection Study Group. Protecting health care workers from SARS and other respiratory pathogens: organizational and individual factors that affect adherence to infection control guidelines. American Journal of Infection Control 2005, 33, 88–96. [Google Scholar] [CrossRef]
- Lam, S.K.K.; Kwong, E.W.Y.; Hung, M.S.Y.; Pang, S.M.C.; Chiang, V.C.L. Nurses’ preparedness for infectious disease outbreaks: A literature review and narrative synthesis of qualitative evidence. Journal of Clinical Nursing 2018, 27, e1244–e1255. [Google Scholar] [CrossRef]
- Haigh, K.A.; Liuzzi, F.; Irvine, S.; Thompson, A.; Hepworth, E.; Hoyle, M.C.; Cruise, J.; Hine, P.; Walker, N.F. A ‘train the trainers’ approach to infection prevention and control training in pandemic conditions. Clinical Infection in Practice. 2023, 19, 100228. [Google Scholar] [CrossRef]
- Castro-Sánchez, E.; Alexander, C.M.; Atchison, C.; Patel, D.; Leung, W.; Calamita, M.E.; Garcia, D.M.; Cimpeanu, C.; Mumbwatasai, J.M.; Ramid, D.; Doherty, K. Evaluation of a personal protective equipment support programme for staff during the COVID-19 pandemic in London. Journal of Hospital Infection. 2021, 109, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Nexø, M.A.; Kingod, N.R.; Eshøj, S.H.; Kjærulff, E.M.; Nørgaard, O.; Andersen, T.H. The impact of train-the-trainer programs on the continued professional development of nurses: a systematic review. BMC Medical Education. 2024, 24, 30. [Google Scholar] [CrossRef] [PubMed]
- Penna, A.R.; Hunter, J.C.; Sanchez, G.V.; Mohelsky, R.; Barnes, L.E.; Benowitz, I.; Crist, M.B.; Dozier, T.R.; Elbadawi, L.I.; Glowicz, J.B.; Jones, H. Evaluation of a Virtual Training to Enhance Public Health Capacity for COVID-19 Infection Prevention and Control in Nursing Homes. Journal of Public Health Management and Practice. 2022, 28, 682–692. [Google Scholar] [CrossRef]
- Azuma, K.; Yanagi, U.; Kagi, N.; Kim, H.; Ogata, M.; Hayashi, M. Environmental factors involved in SARS-CoV-2 transmission: effect and role of indoor environmental quality in the strategy for COVID-19 infection control. Environmental health and preventive medicine. 2020, 25, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Lee, H.; Sang, H.; Muller, J.; Yang, H.; Lee, C.; Ory, M. Nursing home design and COVID-19: implications for guidelines and regulation. Journal of the American Medical Directors Association. 2022, 23, 272–279. [Google Scholar] [CrossRef]
- World Health Organization. Mental health and psychosocial considerations during the COVID-19 outbreak. 2020.
- World Health Organization. Infection prevention and control guidance for long-term care facilities in the context of COVID-19: interim guidance, 8 January 2021. World Health Organization; 2021.
Figure 1.
The PRISMA flow diagram summarising the screening process.
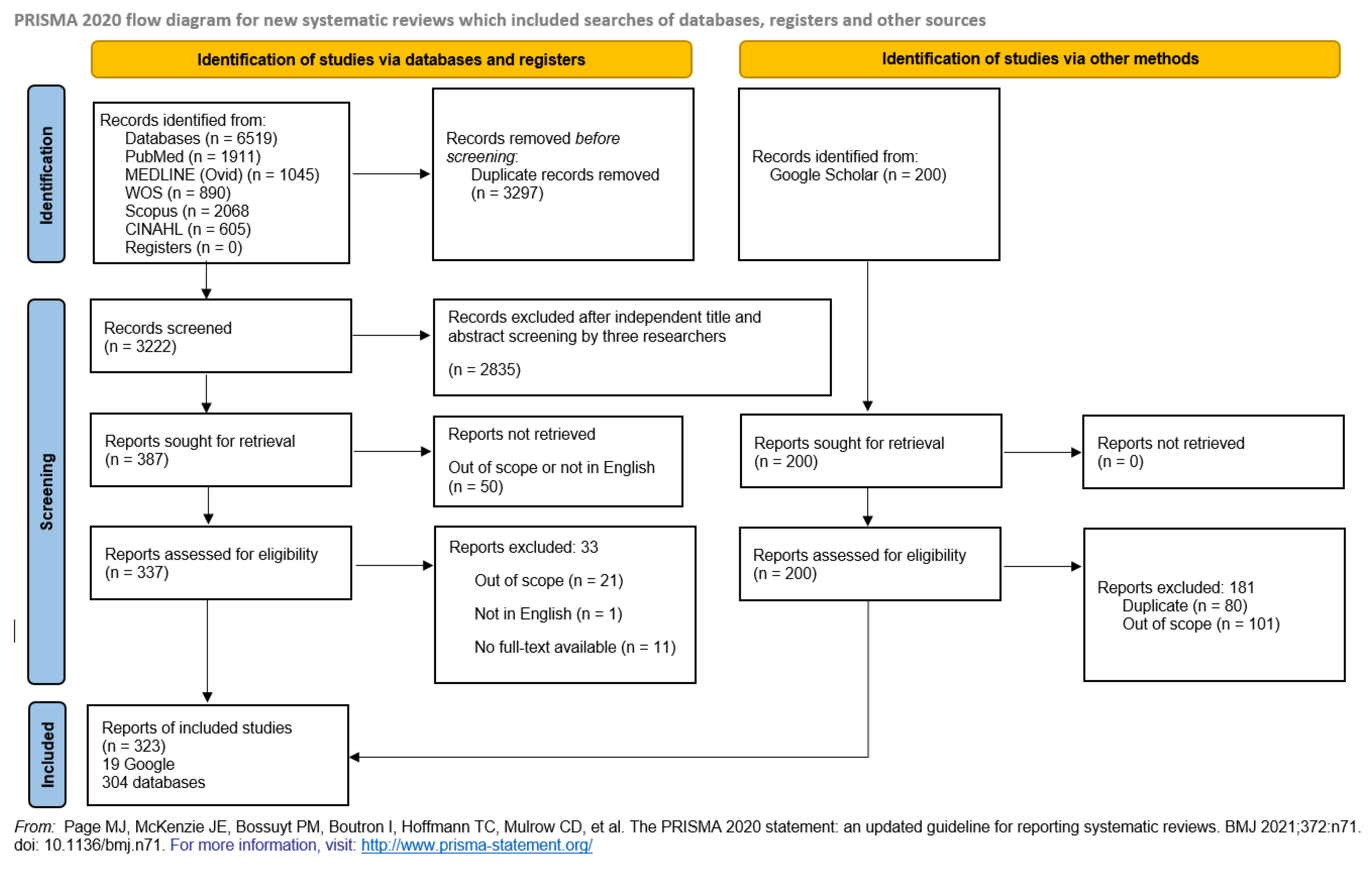
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



