Submitted:
15 May 2025
Posted:
15 May 2025
You are already at the latest version
Abstract
Background: This study explores the association between HSP22/27/60 and the occurrence of STEMI and the prognosis after PCI to compensate for the insufficient risk stratification in the current situation. Methods: This study included 88 patients with STEMI and 90 patients with stable coronary artery disease who were admitted to our hospital. ELISA detected serum levels of HSP22/27/60 to analyze their correlation with STEMI. Dynamic monitoring was conducted on the STEMI group (from before to 4 days after the operation) to evaluate the relationship between the changes in HSP levels and the occurrence of MACE. Results:The serum levels of HSP22/27/60 in STEMI patients were significantly higher than in the control group (P < 0.05). ROC curve analysis showed that these three markers had high diagnostic values for STEMI. The levels of HSP22/HSP27 in STEMI patients peaked on the third day after PCI, while HSP60 peaked at 8 hours after the operation. After 6 months of follow-up, 15 of 88 STEMI patients developed MACE. The predictive value of peak HSP levels for MACE was the highest when HSP22/27/60 were jointly predicted, with an AUC of 0.917 (95% CI: 0.857 - 0.977). Multivariate binary Logistic regression analysis showed that after adjusting for creatinine and N-terminal pro-brain natriuretic peptide, HSP22/27/60 were all independent risk factors for MACE. Conclusions: The serum HSP22/27/60 levels in STEMI patients were significantly increased and had diagnostic value. Its postoperative peak value (especially combined detection) can predict the risk of MACE after PCI and is a potential prognostic marker.
Keywords:
heat shock protein 22
; heat shock protein 27
; heat shock protein 60
; major 35 adverse cardiovascular events
1. Introduction
Cardiovascular diseases (CVD) are the leading cause of death worldwide, it is reported that globally, 17 million people die each year due to ischemic heart disease. Among them, 7.1 million deaths are caused by acute myocardial infarction (AMI) [1]. AMI can be divided into ST-segment elevation myocardial infarction (STEMI) and non-ST-segment elevation myocardial infarction. The primary pathogenesis is the rupture of unstable coronary artery plaques, which triggers a series of pathological processes such as platelet activation, thrombosis, and coronary artery occlusion, eventually leading to the death of myocardial cells due to persistent severe ischemia and hypoxia [2]. To rescue the damaged myocardium, coronary artery blood flow needs to be restored within 20 to 40 minutes after the onset of the disease. Clinically, revascularization can be achieved through coronary artery bypass grafting, open heart surgery, or PCI, among which percutaneous coronary intervention (PCI) is currently the most commonly used interventional method. Although the advancements in cardiovascular treatment techniques in recent years have reduced the early mortality rate of AMI, patients who receive PCI treatment and undergo standardized secondary prevention still face a higher risk of major adverse cardiovascular events (MACE) occurrence [3,4]. Existing studies have shown that ventricular remodeling is a key factor causing poor prognosis in AMI patients, and its core pathological manifestation is myocardial fibrosis. Although endocardial biopsy is the gold standard for diagnosing myocardial fibrosis, its clinical application is limited due to its invasiveness [5]. Therefore, it is of great significance to search for biomarkers with prognostic value.
Heat shock proteins (HSPs) are a family of endogenous proteins that regulate cellular functions and play a key role in maintaining protein homeostasis and cell protection [6]. HSPs were initially named for their role in the heat stress response. Subsequent studies have found that they can be activated under various stress conditions such as hypoxia, oxidative stress, infection, and heavy metal exposure, and they repair damaged proteins and protect cells [7,8,9]. Other studies have shown that HSPs play a role in the heart by regulating multiple molecular mechanisms such as oxidative stress, autophagy, apoptosis, protein subcellular distribution, and proteasome activity. In addition, drugs such as geranyl acetone and cytokines can exert protective effects on the heart by regulating the expression of heat shock proteins [3]. Based on the existing research evidence, HSPs may become a potential therapeutic target for cardiovascular diseases, especially since they have significant value in early diagnosis, condition monitoring, and prognosis evaluation.
The molecular weight of HSPs ranges from 10 to 150 kDa. Their molecular weight can roughly classify them into HSP110, HSP90, HSP70, HSP60, HSP40, and small heat shock proteins (sHSP, including HSP22 and HSP27) [10]. This study mainly explores the relationship between the serum heat shock protein 22 (HSP22), heat shock protein 27 (HSP27), and heat shock protein 60 (HSP60) antibody levels and the occurrence of STEMI. It analyzes the predictive value of HSP22, HSP27, and HSP60 for MACE in STEMI patients at different time points after PCI.
2. Materials and Methods
2.1. Patients
General information: A total of 178 patients who visited the Department of Cardiovascular Medicine of Inner Mongolia Baogang Hospital from June 2024 to November 2024 were selected, among whom 90 were patients with stable coronary heart disease in the control group (56 males and 34 females).Inclusion criteria: Meeting the diagnostic criteria for stable coronary heart disease in he “2019 Edition of the Guidelines for Rational Drug Use in Coronary Heart Disease”. There were 88 STEMI patients in the case group (73 males and 15 females), all of whom visited the hospital for the first time due to chest pain (within 6 hours of onset) and received emergency PCI treatment. The STEMI diagnostic criteria refer to the latest STEMI diagnostic criteria released by the European Society of Cardiology (ESC) and adopt the “1+1” model: 1. Essential conditions: Dynamic changes of myocardial injury markers (such as troponin); 2. Additional conditions (meeting any of the following): ① Symptoms of myocardial ischemia (such as chest pain); ② Newly emerged pathological Q waves; ③ ST-segment changes in an electrocardiogram; ④ Imaging evidence after coronary intervention.
Exclusion criteria: Those meeting any of the following criteria will be excluded: 1. Combined with severe organ failure, including severe cardiac insufficiency (NYHA cardiac function classification grade Ⅲ-Ⅳ), severe renal insufficiency (eGFR <30 mL/min/1.73m²); 2. Have a history of neurological diseases such as stroke or epilepsy in the past; 3. Combined with tumors, rheumatic diseases, or autoimmune system diseases. This research aligns with the principles of the Declaration of Helsinki and has been approved by the Ethics Committee of Inner Mongolia Baogang Hospital (Approval Number: 2024-MER-039). All patients signed the informed consent form.
2.2. Data Extraction and Inflammatory Indexes Analysis
Collect the basic clinical data of the patients, including age, gender, height, and weight, as well as systolic blood pressure, diastolic blood pressure, and heart rate at admission. Meanwhile, record the medical history, smoking history, and drinking history. All patients were required to fast for 10 to 12 hours, and elbow venous blood samples were collected early the next day. Blood samples should be sent for examination immediately after collection. The test indicators include: Blood samples were collected using ethylenediaminetetraacetic acid (EDTA) anticoagulant tubes. The blood routine in the United States was determined using the Beckman Coulter LH750 automatic hematology analyzer. The samples were collected using dry blood collection tubes without anticoagulants. Biochemical indicators (triglycerides, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, alanine aminotransferase, creatinine, uric acid, etc.) were determined using the Roche Cobas 8000 fully automatic biochemical analyzers from Roche Diagnostics, Switzerland. At the same time, record the following indicators measured for the first time after admission: red blood cell count, white blood cell count, platelet count, hemoglobin, monocyte count, alanine aminotransferase, creatinine, uric acid, peak value of troponin I enzyme, left ventricular ejection fraction, etc.
Control group: Peripheral venous blood was collected immediately upon admission. Case group: Peripheral venous blood was collected at the following time points respectively: before the operation/immediately upon admission, 8 hours after the operation, 12 hours after the operation, 24 hours after the operation, 3 days after the operation, and 4 days after the operation. The samples were collected using ethylenediaminetetraacetic acid (EDTA) anticoagulant tubes. After thorough mixing, they were centrifuged (at 3000 r/min, with a centrifugation radius of 10 cm for 20 min), and the supernatant was collected and stored in a refrigerator at -80℃ for testing. ELISA was used for detection. In the control group, HSP22, HSP27, and HSP60 were detected immediately upon admission. In the case group, HSP22 and HSP27 were detected before surgery/immediately upon admission, 24 hours, 3 days, and 4 days, and HSP60 was detected before surgery/immediately upon admission, 8 hours, 12 hours, and 24 hours. The kit is provided by Beijing Jinke Puxi Biotechnology Co., LTD. (both the intra-batch coefficient of variation and the inter-batch coefficient of variation are less than 10%), and the operation should be carried out following the manufacturer’s instructions.
2.3. Statistical Analysis
Statistical analysis was performed using SPSS 23.0 and Graph Pad Prism 8.0. The measurement data were first subjected to the Kolmogorov-Smirnov test for normality. For the measurement data conforming to the normal distribution, the mean ± standard deviation was used for representation, and the independent sample t-test was used to compare groups. The measurement data that did not conform to the normal distribution were expressed as a median and interquartile range [M(Q1, Q3)], and the comparison between groups was performed using the Mann-Whitey U test. Counting data were expressed as rates or percentages, and the chi-square test was used to compare groups. The variables with statistical significance (P < 0.05) in the univariate analysis were included in the multivariate binary Logistic regression model for analysis. The ROC curve evaluated the predictive value of heat shock protein for STEMI, and the predictive efficacy and differences between groups were assessed by AUC and Z tests. All statistical inferences were considered statistically significant when bilateral P < 0.05. A total of STEMI patients undergoing emergency PCI were included in this study, and the occurrence of MACE within the hospital and 6 months was recorded. The patients were divided into high/low heat shock protein groups using the optimal cut-off value determined by ROC. The two groups’ general baseline data and interventional surgery-related data were compared. The independent risk factors of adverse in-hospital events in STEMI patients were analyzed through multivariate binary logistic regression.
3. Results
3.1. Subsection
3.1.1. Comparison of Baseline Data and Serum Levels of HSP22, HSP27, and HSP60 at Admission Between the Stable Coronary Heart Disease Group and the STEMI Group
There were statistically significant differences between the two groups in terms of age, gender, history of hypertension and diabetes, C-reactive protein, systolic blood pressure, diastolic blood pressure, smoking, drinking, white blood cell count, percentage of monocytes, heart rate at admission, troponin, creatinine, NT-Pro BNP (all P < 0.05). There were no statistically significant differences between the two groups in terms of red blood cell count, hemoglobin, platelet count, triglycerides, total cholesterol, LDL-C, HDL-C, D-dimer, alanine aminotransferase, uric acid, urea, and glucose (all P > 0.05), Table 1.
The serum HSP22 level in the STEMI group was 0.586 (0.501, 0.647) ng/mL, which was significantly higher than that in the stable coronary heart disease group (0.365 (0.330, 0.398) ng/mL; U = -10.897, P < 0.001). The serum HSP27 level in the STEMI group was 1.943 (1.685, 2.381) ng/mL, which was also significantly higher than that in the stable coronary heart disease group (1.090 (0.933, 1.185) ng/mL; U = -10.835, P < 0.001). The serum HSP60 level in the STEMI group was 0.371 (0.321, 0.424) ng/mL, which was significantly higher than that in the stable coronary heart disease group (0.209 (0.175, 0.245) ng/mL; U = -10.259, P < 0.001).
ROC curve analysis revealed that all three heat shock proteins had significant predictive value for the occurrence of STEMI, Figure 1. The area under the ROC curve (AUC) for HSP22 in predicting STEMI occurrence was 0.971 (95% CI 0.951 - 0.991, P < 0.001), with a sensitivity of 90.90% and a specificity of 93.30%; the AUC for HSP27 was 0.970 (95% CI 0.950 - 0.990, P < 0.001), with a sensitivity of 86.40% and a specificity of 95.60%; and the AUC for HSP60 was 0.945 (95% CI 0.905 - 0.985, P < 0.001), with a sensitivity of 89.80% and a specificity of 97.80%.
3.1.2. Dynamic Changes of HSP22, HSP27, and HSP60 Expressions in STEMI Patients Before and After Emergency PCI
The expression changes of heat shock proteins during the perioperative period of emergency PCI in STEMI patients are as follows: The baseline level of HSP22 was significantly higher than that of the stable coronary heart disease group (P < 0.001). The expression of HSP22 gradually increased on the 1st day after PCI, peaked on the 3rd day, and decreased on the 4th day, Figure 2. The baseline level of HSP27 was significantly higher than that of the stable coronary heart disease group (P < 0.001). The expression of HSP27 gradually increased on the 1st day after PCI, peaked on the 3rd day, and decreased on the 4th day, Figure 3. The baseline level of HSP60 was significantly higher than that of the stable coronary heart disease group (P < 0.001). The expression of HSP60 significantly increased and peaked 8 hours after PCI, gradually decreasing at 12 hours and 24 hours after PCI, but still higher than before PCI, Figure 4.
3.1.3. The Predictive Value of Peak Levels of HSP22, HSP27, and HSP60 for MACE in STEMI Patients After Emergency PCI
A total of 88 STEMI patients who underwent emergency PCI were included in this study. The follow-up period was 6 months (with no cases lost to follow-up). Among them, 15 cases (17.0%) developed MACE, including 6 cases of cardiogenic shock, 2 cases of recurrent myocardial infarction, and 7 cases of malignant arrhythmia. According to the ROC curve analysis of the predictive efficacy at each time point, the AUC of HSP22 at admission for the case group was 0.646 (95% CI 0.501 - 0.790, P = 0.077), with a sensitivity of 86.7% and a specificity of 49.3%; the AUC of predictive efficacy on the first postoperative day was 0.581 (95% CI 0.424 - 0.738, P = 0.326), with a sensitivity of 60.0% and a specificity of 63.0%; the AUC of predictive efficacy on the third day was 0.805 (95% CI 0.698 - 0.911, P < 0.001), with a sensitivity of 80.0% and a specificity of 68.5%; and the AUC of predictive efficacy on the fourth day was 0.778 (95% CI 0.659 - 0.898, P = 0.001), with a sensitivity of 86.7% and a specificity of 64.4%, Figure 5. The predictive efficacy of HSP27 at admission was 0.506 (95% CI 0.352 - 0.563, P = 0.943), with a sensitivity of 13.3% and a specificity of 71.2%; the predictive efficacy of HSP27 on the first postoperative day was 0.531 (95% CI 0.386 - 0.737, P = 0.710), with a sensitivity of 93.3% and a specificity of 23.3%; the predictive efficacy on the third postoperative day was 0.784 (95% CI 0.681 - 0.887, P < 0.001), with a sensitivity of 86.7% and a specificity of 65.8%; the predictive efficacy on the fourth postoperative day was 0.747 (95% CI 0.609 - 0.884, P = 0.003), with a sensitivity of 66.7% and a specificity of 83.6%, Figure 6. The predictive efficacy of HSP60 at admission was 0.412 (95% CI 0.258 - 0.566, P = 0.284), with a sensitivity of 26.7% and a specificity of 47.9%; the predictive efficacy of HSP60 at 8 hours after surgery was 0.843 (95% CI 0.724 - 0.944, P < 0.001), with a sensitivity of 93.3% and a specificity of 71.2%; the predictive efficacy of HSP60 at 12 hours after surgery was 0.798 (95% CI 0.658 - 0.938, P < 0.001), with a sensitivity of 60.0% and a specificity of 93.2%; the predictive efficacy of HSP60 at 24 hours after surgery was 0.527 (95% CI 0.377 - 0.676, P = 0.743), with a sensitivity of 66.7% and a specificity of 57.5%, Figure 7. The predictive efficacy of peak HSP22 combined with HSP27 after surgery was AUC of 0.830 (95% CI 0.730 - 0.931, P < 0.001), with a sensitivity of 100.0% and a specificity of 53.4%; the predictive efficacy of peak HSP22 combined with HSP60 after surgery was AUC of 0.898 (95% CI 0.833 - 0.962, P < 0.001), with a sensitivity of 100.0% and a specificity of 75.3%; the predictive efficacy of peak HSP27 combined with HSP60 after surgery was AUC of 0.905 (95% CI 0.831 - 0.979, P < 0.001), with a sensitivity of 93.3% and a specificity of 76.7%; the predictive efficacy of the combined peak values of the three was AUC of 0.917 (95% CI 0.857 - 0.977, P < 0.001), with a sensitivity of 100.0% and a specificity of 78.1%, Figure 8.
Based on the ROC curve analysis, the optimal cut-off point was determined by the maximum value of the Youden index (sensitivity + specificity - 1), with the peak values of HSP22 being 2.416 ng/mL, HSP27 being 9.470 ng/mL, and HSP60 being 3.154 ng/mL. These cut-off values divided patients into a high-expression group and a low-expression group (HSP22 Table 2, HSP27 Table 3, HSP60 Table 4). The baseline data of the two groups were comparable (P > 0.05).
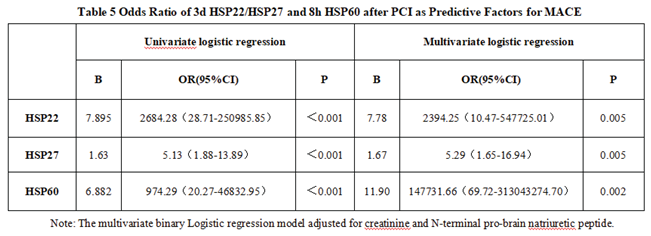
The univariate binary Logistic regression analysis revealed that peak levels of HSP22, HSP27, and HSP60 were all risk factors for MACE occurrence (P < 0.05). The multivariate binary Logistic regression model, after adjusting for creatinine and NT-proBNP, confirmed that HSP22 had an OR of 1.85 (95% CI: 1.32 - 2.59, P = 0.002), HSP27 had an OR of 2.12 (95% CI: 1.45 - 3.10, P < 0.001), and HSP60 had an OR of 2.37 (95% CI: 1.63 - 3.45, P < 0.001). These three factors remained independent risk factors for MACE occurrence in STEMI patients undergoing emergency PCI, Table 5.
4. Discussion
In recent years, significant progress has been made in the research on the pathogenesis of CVD. Multiple studies have demonstrated that endothelial cell damage and inflammatory responses are crucial in atherosclerosis [11,12]. The activation of inflammatory pathways and endothelial cell damage, along with the accumulation of lipid, fibrous components, and calcium, are essential factors contributing to the progression of atherosclerosis and, ultimately, to vascular stenosis [13]. This kind of cell damage can be attributed to various factors, such as oxidative stress, lipid peroxidation, and high cholesterol levels [14,15]. In such an environment of damage and stress, cells activate a series of protective mechanisms, including the expression and release of heat shock proteins [16]. Increasing the expression of such heat shock proteins may serve as a cellular protective mechanism, aiming to alleviate endothelial cells’ stress, injury, and inflammatory responses [17]. Moreover, an increasing amount of evidence indicates that there is a significant correlation between elevated levels of inflammatory factors and biomarkers in patients with coronary artery disease and adverse clinical outcomes [18,19,20].
HSP22 belongs to HSPs and is mainly expressed in the heart, brain, skeletal muscle, and various cancers [21]. Previous studies on human and animal models have shown that HSP22 in the myocardium after acute and chronic ischemia can be significantly induced and released. Specifically, HSP22 increases in hypoxic and hibernating myocardium, indicating an adaptive response to hypoxia. Therefore, HSP22 is a cellular protective protein that prevents irreversible ischemic damage to cardiomyocytes in hypoxic and hibernating states. In vitro studies using isolated cardiomyocytes have shown that overexpression of HSP22 protects cardiomyocytes from stress-induced apoptosis by activating the PI3K/Akt/Smad 1/5/8 survival signaling pathway [22]. The research findings indicate that overexpression of HSP22 can significantly enhance the PI3K activity of cardiomyocytes and the phosphorylation levels of Akt and Smad 1/5/8. Additionally, some studies have revealed the close connection between HSP22 and inducible nitric oxide synthase (iNOS) and demonstrated that the anti-apoptotic effect of HSP22 in cardiomyocytes depends on its induction of iNOS [23,24]. Moreover, overexpression of HSP22 increases the expression and activity of iNOS in cardiomyocytes and cardiac tissues, while the deletion or silencing of HSP22 weakens the expression of iNOS.The key point is that inhibiting iNOS eliminated the cardioprotective effect induced by HSP22. In transgenic (TG) mice with the HSP22 gene, it was found that HSP22 increased a AAA-related protein named valosin-containing protein (VCP). HSP22 co-localizes with AKT and VCP [25],and interacts with these two proteins, mainly existing in the nuclear part of cardiomyocytes. Then, activating transcription factors activates the atomic factor κ- light chain enhancer (NF-kB) of B cells to induce the expression of iNOS in cardiomyocytes. It is worth noting that the down-regulation of HSP22 will increase stress-induced cardiomyocyte death, thereby accelerating the transition from cardiac overload to heart failure during this period [26]. Lack of HSP22 will also disrupt the energy metabolism homeostasis of the heart and increase oxidative damage, thereby leading to cardiac dilation and functional impairment [27]. Therefore, HSP22 may be a new therapeutic target for cardiovascular diseases. HSP27 has a relative molecular mass of approximately 27 kDa and is ubiquitous in various cells and organ tissues. It has functions such as binding and stabilizing the cytoskeleton and can regulate the expression of genes directly related to vascular wall inflammation by activating NF-κB [28]. The possible mechanism of HSP27 in anti-atherosclerosis is: In acute stress states such as ischemia, hypoxia, and high pressure, some proteins in the cells undergo denaturation, causing the level of HSP27 in the body to increase and inducing its phosphorylation [29]. Phosphorylated HSP27 (pHSP27) stabilizes the integrity and viability of the cell membrane by inhibiting Bax, up-regulating glutathione reductase, and reducing reactive oxygen species within the cell [30]. It activates the NF-κB signaling pathway to induce granulocyte-monocyte colony-stimulating factor and binds to ATP-binding transporter A1 and transporter G1, thereby promoting the efflux of total cholesterol [31]. It also inhibits the uptake ability of macrophages for acetylated low-density lipoprotein, suppresses the formation of foam cells, stimulates the secretion of IL-10 through the p38 signaling pathway, reduces the expression of scavenger receptor A, regulates the release of pro-inflammatory factors, and inhibits the progression of inflammatory responses [32,33]. pHSP27 can enhance the re-association of actin, inhibit its degradation, and strengthen the aggregation ability of fibrous actin, ultimately achieving the purpose of inhibiting the progression of atherosclerosis. HSP60 is a highly conserved heat shock protein that plays essential roles and provides protection within cells [34]. HSP60 is mainly located in mitochondria and assists in protein folding, assembly, and transportation [35]. Outside the cell, HSP60 can act as a molecular chaperone, interacting with other proteins and participating in various biological processes [36]. The experiments conducted by Jing Tian et al. provided direct evidence that exogenous HSP60 activates the TLR 4-MyD 88-p38/NF-kB signaling pathway and induces inflammatory responses in cardiomyocytes. Moreover, it was demonstrated that endogenous HSP60 released by ischemic cardiomyocytes promotes the induction of cytokines through the TLR 4-MyD 88-p38/NF-kB pathway [37]. Clinical studies also suggest that HSP60 can induce inflammation, and anti-HSP60 antibodies may promote atherosclerosis [38]. Anti-HSP60 indicates endothelial injury and can serve as a new risk factor for atherosclerosis and a valuable diagnostic marker for patients with mixed connective tissue disease [39]. Furthermore, the polymorphism of the HSP60 gene is associated with the pathological grading and incidence of atherosclerosis to some extent. The study by Wang S et al. demonstrated that HSP60 can bind to MHC Ⅱ on the surface of antigen-presenting cells and be recognized by CD4+ T cells. This indicates that HSP60 can act as an antigen in atherosclerotic plaques, triggering an immune response against HSP60 [40].
This study systematically analyzed HSP22, HSP27, and HSP60 expression characteristics in patients with STEMI. The following significant findings were obtained. Serological tests revealed that the levels of HSP22, HSP27, and HSP60 in STEMI patients at admission were significantly higher than those in patients with stable coronary heart disease (P < 0.05), and it was the first time to confirm that all three can be used as a combined serum biomarker combination for the diagnosis of STEMI. Dynamic monitoring revealed that the peak levels of HSP22, HSP27, and HSP60 have predictive value for MACE events. The combined detection of these three can further enhance the predictive efficacy. Preliminary analysis showed that the sensitivity of the combined detection of HSP22 and HSP27 was as high as 100%, but its specificity was relatively low (53.4%). To verify the reliability of the data, we took the following measures: multiple confirmations of the detection methods of HSP22/27 for inter-batch differences and repeatability, repeated detection of HSP22 and HSP27 on the third day after surgery to determine the accuracy of the data. Considering that the current results may be related to insufficient sample size, we could also introduce inflammatory indicators on the third day after surgery (such as white blood cell count C-reactive protein), combine Logistic regression to construct a new model, and use the Youden index to reselect the critical value to balance sensitivity and specificity. However, the above supplementary experiments could not be completed due to the late detection time of HSP22/27 (patients have been discharged). Unlike previous studies that focused on single indicator research limitations, this study, for the first time, simultaneously confirmed that the serum levels of all three were significantly higher in STEMI patients than in patients with stable coronary heart disease (P < 0.05), providing a new triad of serological biomarker combinations for the early differential diagnosis of STEMI. In addition, the research results also showed differences in the prediction time windows of different HSP - HSP22 and HSP27 on the third day after surgery and HSP60 on the first day after surgery, respectively, which had predictive values for MACE. This temporal specificity provided precise time node guidance for clinical monitoring. The optimization of dynamic monitoring schemes and the design of differentiated HSP monitoring time axes (HSP60 focused on the first day after surgery, HSP22/HSP27 focused on the third day after surgery) provided the evidence-based basis for reducing unnecessary frequent tests in clinical practice. Unlike previous studies that focused on single indicator research limitations, this study, for the first time, simultaneously confirmed that the serum levels of all three were significantly higher in STEMI patients than in patients with stable coronary heart disease (P < 0.05), providing a new triad of serological biomarker combinations for the early differential diagnosis of STEMI. This study has several limitations: Firstly, the relatively small sample size (n=88 in the STEMI group) and low incidence of MACE events (15 cases) may result in insufficient statistical power, necessitating future multicenter, large-scale studies to validate the generalizability of the conclusions further. Secondly, the control group exclusively comprised patients with stable coronary artery disease, excluding healthy individuals, which may underestimate the specificity of HSPs in acute myocardial infarction (AMI). Additionally, the single-center design may limit the results due to regional population characteristics (e.g., the influence of climate and dietary habits on baseline HSP levels), and the applicability of cutoff values has not been validated across different geographical or ethnic groups. Lastly, the short follow-up period (6 months) precluded the assessment of HSPs’ predictive value for long-term prognosis in STEMI patients undergoing emergency PCI. Future research should extend the follow-up duration to clarify the long-term prognostic significance of HSPs, explore combined detection strategies with other biomarkers, and enhance the clinical applicability of the findings by incorporating healthy controls and conducting cross-regional validation.
Author Contributions
Conceptualization,Yaning Hu and Yuansheng Liu; methodology,Yuansheng Liu; validation, Tao Qu.,Chuanjun Chen and Yueping Wang; formal analysis,Fengxu Lin and Yaning Hu; investigation,Yaning Hu and Yuansheng Liu.; resources,Tao Qu.,Chuanjun Chen and Yueping Wang;writing—original draft preparation, Yaning Hu; writing—review and editing,Tao Qu.,Chuanjun Chen.; visualization,Tao Qu.,Chuanjun Chen; supervision,Tao Qu.,Chuanjun Chen; project administration,Tao Qu.,Chuanjun Chen; funding acquisition,Tao Qu.,Chuanjun Chen. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Metallurgical Safety and Health Branch of the Chinese Society for Metals (Grant No.jkws202304).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Inner Mongolia Baogang Hospital (protocol code 2024-MER-039 and May 8th,2024 of approval).” for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Acknowledgments: During the preparation of this manuscript/study, the author(s) used SPSS 23.0 and Graph Pad Prism 8.0 for the purposes of statistical analysis. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| CVD | Cardiovascular diseases |
| STEMI | ST-segment elevation myocardial infarction |
| PCI | Percutaneous coronary intervention |
| MACE | Major adverse cardiovascular events |
| HSPs | Heat shock proteins |
| HSP22 | Heat shock protein 22 |
| HSP27 | Heat shock protein 27 |
| HSP60 | Heat shock protein 60 |
References
- Zhao Y, Cui R, Du R, Song C,et al.Platelet-Derived Microvesicles Mediate Cardiomyocyte Ferroptosis by Transferring ACSL1 During Acute Myocardial Infarction. Mol Biotechnol. 2025 Feb;67(2):790-804. [CrossRef]
- Chen Y, Li M, Wu Y. Heat shock protein 22: A new direction for cardiovascular disease (Review). Mol Med Rep. 2025 Mar;31(3):82. [CrossRef]
- Wang ZY, Lu Y, Zhang WJ, Zhang JX,et al.[Effect of plasma RIPK3 levels on long-term prognosis in patients with acute myocardial infarction undergoing percutaneous coronary intervention]. Zhonghua Xin Xue Guan Bing Za Zhi. 2025 Mar 24;53(3):268-273. Chinese. [CrossRef]
- Sanz-Sánchez J, Teira Calderón A, Neves D, Cortés Villar C, Lukic A, Rumiz González E, Sánchez-Elvira G, Patricio L, Díez-Gil JL, García-García HM, Martínez Dolz L, San Román JA, Amat Santos I. Culprit-Lesion Drug-Coated-Balloon Percutaneous Coronary Intervention in Patients Presenting with ST-Elevation Myocardial Infarction (STEMI). J Clin Med. 2025 Jan 28;14(3):869. [CrossRef]
- O’Gara PT, Kushner FG, Ascheim DD,et al. CF/AHA Task Force. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013 Jan 29;127(4):529-55.
- Chen Y, Li M, Wu Y. Heat shock protein 22: A new direction for cardiovascular disease (Review). Mol Med Rep. 2025 Mar;31(3):82. [CrossRef]
- Benjamin IJ and McMillan DR: Stress (heat shock) proteins:Molecular chaperones in cardiovascular biology and disease.Circ Res 83: 117-132, 1998.
- Deniset JF and Pierce GN: Heat shock proteins: Mediators of atherosclerotic development. Curr Drug Targets 16: 816-826,2015.
- Nayak Rao S: The role of heat shock proteins in kidney disease.J Transl Int Med 4: 114-117, 2016.
- Patnaik S, Nathan S,et al. The Role of Extracellular Heat Shock Proteins in Cardiovascular Diseases. Biomedicines. 2023 May 27;11(6):1557.
- ó Hartaigh B, Bosch JA, Thomas GN,et al. (2012)Which leukocyte subsets predict cardiovascular mortality? From the LUdwigshafen RIsk and Cardiovascular Health (LURIC) Study. Atheroscle -rosis 224(1):161–169.
- Mandal K, Jahangiri M, Xu Q. Autoimmune mechanisms of atherosclerosis. Handb Exp Pharmacol. 2005;170:723–43.
- Núñez J, Núñez E, Bodí V, et al. (2008) Usefulness of the neutrophil to lymphocyte ratio in predicting long-termmortality in ST segment elevationmy-ocardial infarction. Am J Cardiol 101(6):747–752.
- Xu Q. Role of heat shock proteins in atherosclerosis. Arterioscler Thromb Vasc Biol. 2002;22(10):1547–59.
- Savovic Z, Pindovic B, Nikolic M, et al. Prognostic Value of Redox Status Biomarkers in Patients Presenting with STEMI or Non-STEMI: A Prospective Case-Control Clinical Study. J Pers Med. 2023 Jun 26;13(7):1050. [CrossRef]
- Xu Q, Metzler B, Jahangiri M,et al.Molecular chaperones and heat shock proteins in atherosclerosis. Am J Physiol Heart Circ Physiol. 2012;302(3):H506–14. [CrossRef]
- Boteanu RM, Suica VI, Uyy E, Ivan L, Dima SO, Popescu I, Simionescu M, Antohe F. Alarmins in chronic noncommunicable diseases: Atherosclerosis, diabetes and cancer. J Proteomics. 2017;153:21–9.
- Wang S, Zhang G Association Between Systemic Immune-Inflammation Index and Adverse Out-comes inPatientsWithAcuteCoronarySyndrome:A Meta-Analysis. Angiology. 2024 Jun 21:33197241263399.
- de Liyis BG,Ciaves AF, Intizam MH,et al. Hematological biomarkers of troponin, neutrophil-to-lymphocyte ratio, and monocyte-to-lymphocyte ratio serve as effective predictive indicators of high-risk mortality in acute coronary syndrome. Biomedicine (Taipei). 2023 Dec 1;13(4):32-43.
- Antonopoulos AS, Angelopoulos A, Papaniko-laou P, et al. (2022) Biomarkers of Vascular Inflammation for Cardiovascular RiskPrognostica-tion: A Meta-Analysis. JACC Cardiovasc Imaging15(3):460–471. [CrossRef]
- Kappé G, Verschuure P, Philipsen RL, et al. Characterization of two novel human small heat shock proteins: Protein kinase-related HspB8 and testis-specific HspB9. Biochim Biophys Acta 1520: 1-6, 2001. [CrossRef]
- Sui X,Li D, Qiu H,et al.Activation of the bone morphogenetic protein receptor by H11kinase/Hsp22 promotes cardiac cell growth and survival. Circ. Res. 2009, 104, 887–895. [CrossRef]
- Depre C,Wang L, Sui X, et al. H11 kinase prevents myocardial infarction by preemptive preconditioning of the heart. Circ. Res. 2006, 98, 280–288. [CrossRef]
- Chen L, Lizano P,Zhao X, et al.Preemptive conditioning of the swine heart by H11 kinase/Hsp22 provides cardiac protection through inducible nitric oxide synthase. Am. J. Physiol. Heart Circ. Physiol. 2011, 300, H1303–H1310. [CrossRef]
- Lizano P,Rashed E, Kang, H,et al. The valosin-containing protein promotes cardiac survival through the inducible isoform of nitric oxide synthase. Cardiovasc. Res. 2013, 99, 685–693.
- Qiu H, Lizano P, Laure L, et al.H11 kinase/heat shock protein 22 deletion impairs both nuclear and mitochondrial functions of STAT3 and accelerates the transition into heart failure on cardiac overload. Circulation 124: 406-415, 2011. [CrossRef]
- Wu W, Sun X, Shi X, et al.Hsp22 deficiency induces age-dependent cardiac dilation and dysfunction by impairing autophagy, metabolism, and oxidative response. Antioxidants (Basel) 10: 1550, 2021. [CrossRef]
- Adamo L, Rocha-Resende C, Prabhu SD, et al. Reappraising the role of inflammation in heart failure[J]. Nat Rev Cardiol, 2020,17(5):269-285. [CrossRef]
- Wolf D, Ley K. Immunity and inflammation in atherosclerosis[J]. Circ Res,2019,124(2):315-327. [CrossRef]
- Mcdonagh TA, Metra M, Adamo M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure[J]. Eur Heart J,2021,42(36):3599-3726.
- Pulakazhi Venu VK, Adijiang A, Seibert T, et al.O’Brien ER. Heat shock protein 27-derived atheroprotection involves reverse cholesterol transport that is dependent on GM-CSF to maintain ABCA1 and ABCG1 expression in ApoE-/- mice. FASEB J. 2017 Jun;31(6):2364-2379.
- Murphy SP, Kakkar R, McCarthy CP, et al. Inflammation in heart failure: JACC state-of-the-art review[J]. J Am Coll Cardiol,2020,75(11):1324-1340.
- Liu S, Iskandar R, Chen W, et al. Soluble glycoprotein 130 and heat shock protein 27 as novel candidate biomarkers of chronic heart failure with preserved ejection fraction[J]. Heart Lung Circ,2016,25(10):1000-1006. [CrossRef]
- Caruso Bavisotto C, Alberti G, Vitale AM, et al.Hsp60 Post-translational Modifications: Functional and Pathological Consequences. Front Mol Biosci. 2020;7:95.
- Liyanagamage D, Martinus RD. Role of Mitochondrial Stress Pro-tein HSP60 in Diabetes -Induced Neuroinflammation. Mediators Inflamm. 2020;2020:8073516.
- Tian J, Guo X, Liu XM, et al. Extracellular HSP60 induces inflammation through activating and up-regulating TLRs in cardiomyocytes. Cardiovasc Res. 2013 Jun 1;98(3):391-401.
- Knoflach M, Bernhard D, Wick G. Anti-HSP60 immunity is already associated with atherosclerosis early in life. Ann N Y Acad Sci. 2005;1051:323–31.
- Zonnar S, Saeedy SAG, Nemati F,et al.Decrescent role of recombinant HSP60 antibody against atherosclerosis in high-cholesterol diet immunized rabbits. Iran J Basic Med Sci. 2022;25(1):32–8.
- Amirfakhryan H. Vaccination against atherosclerosis: An overview. Hellenic J Cardiol. 2020;61(2):78–91.
- Wang S, Chen Y, Zhou D, et al. Pathogenic Autoimmunity in Atherosclerosis Evolves from HSP60-Reactive CD4 + T Cells. J Cardiovasc Transl Res. 2024 Oct;17(5):1172-1180.
Figure 1.
ROC cuves of HSP22 ,HSP27 and HSP60 for dignosing STEMI(n=178).
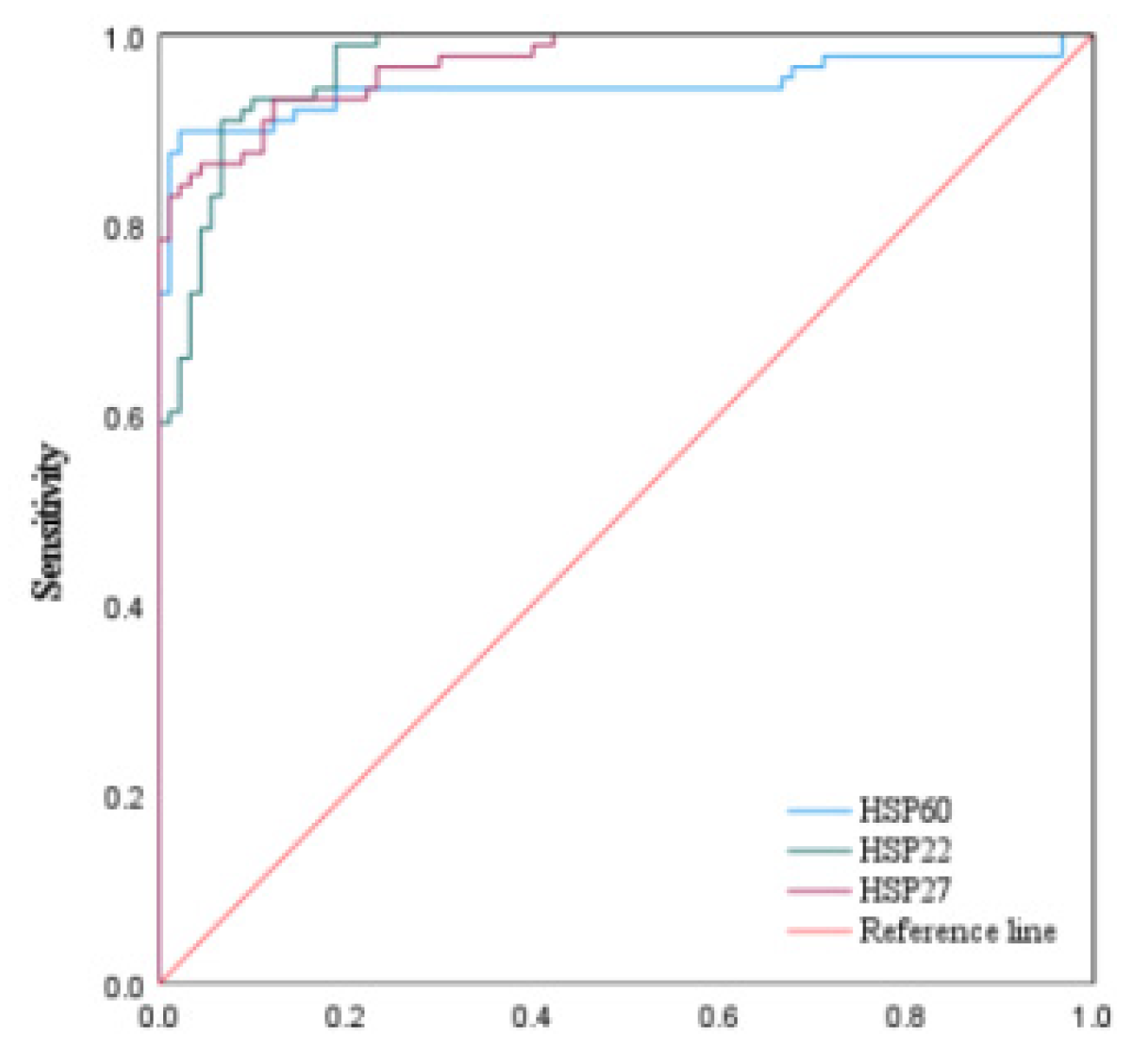
Figure 2.
Alterations in HSP22 Expression Following Emergency PCI in STEMI Patiens.
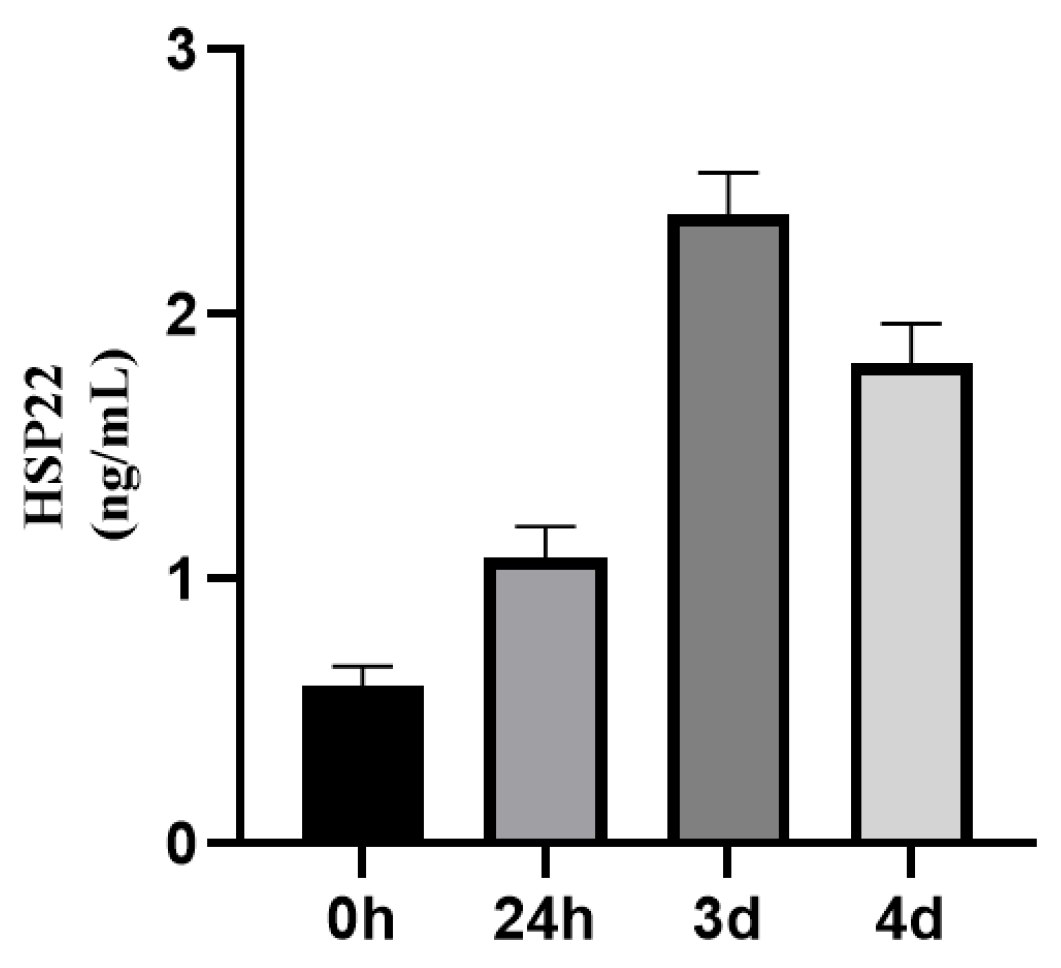
Figure 3.
Alterations in HSP27 Expression Following Emergency PCI in STEMI Patiens.
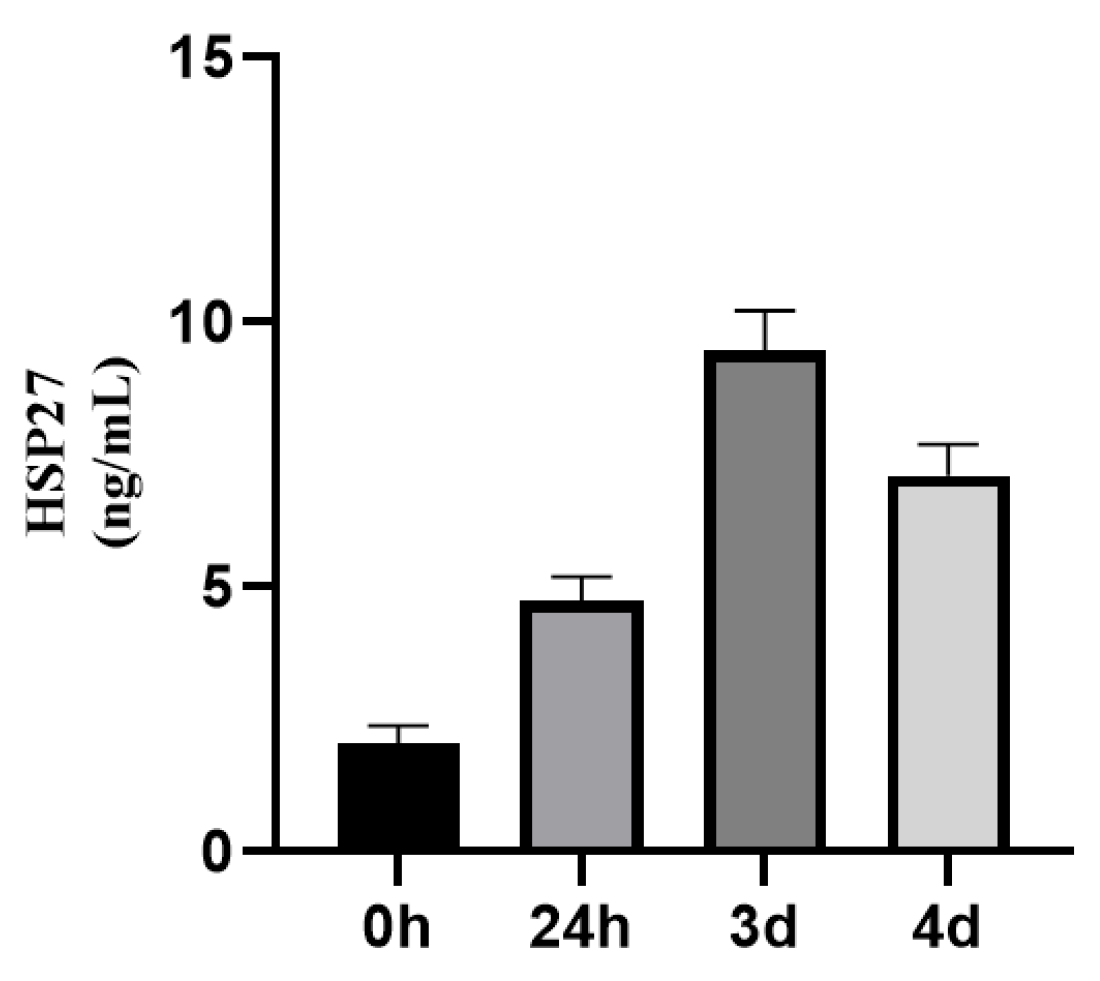
Figure 4.
Alterations in HSP60 Expression Following Emergency PCI in STEMI Patiens.
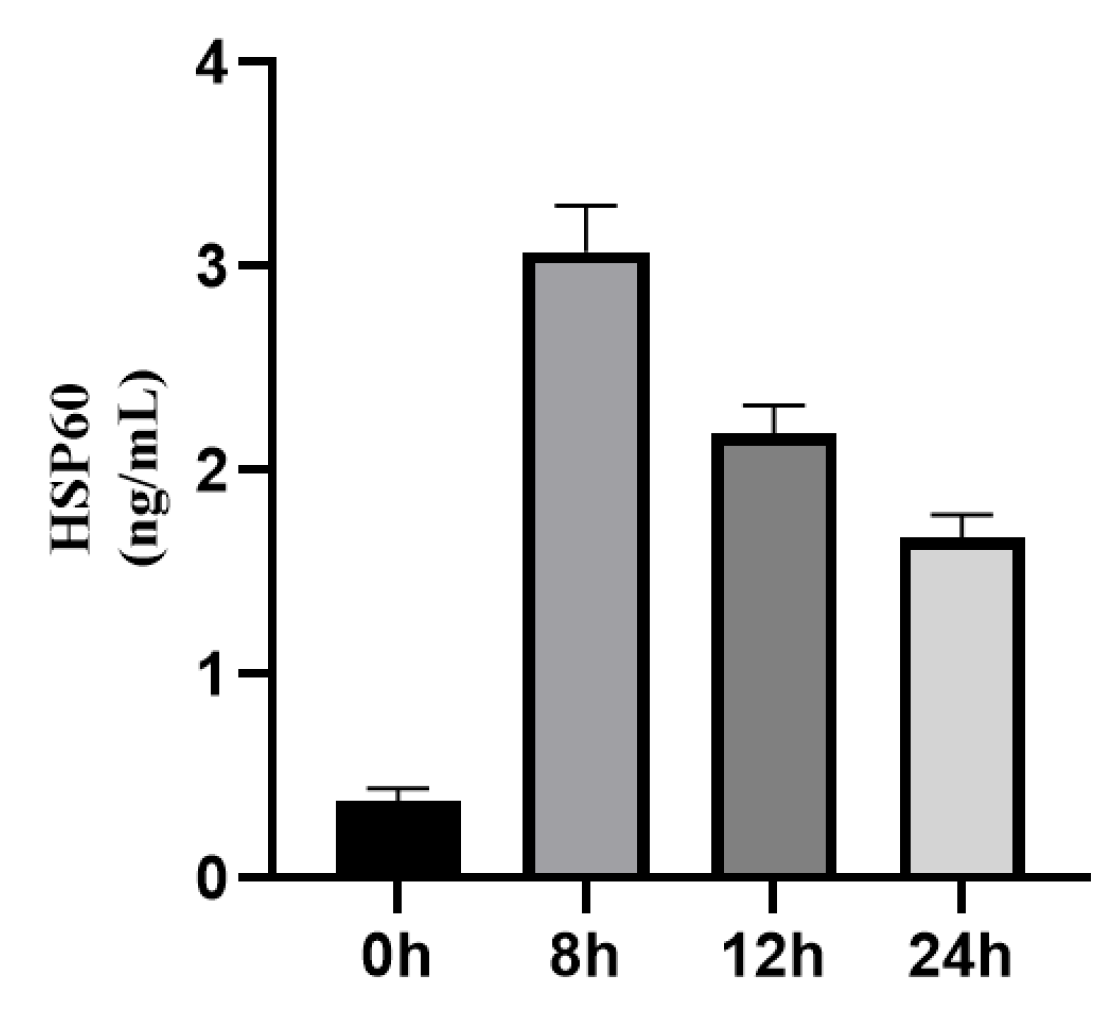
Figure 5.
ROC cuves of Prediction Curves for MACE Occurrence in HSP22 at Different Time Points in STEMI Patients Under aoina Emeraency PCI (N=88).
Figure 5.
ROC cuves of Prediction Curves for MACE Occurrence in HSP22 at Different Time Points in STEMI Patients Under aoina Emeraency PCI (N=88).
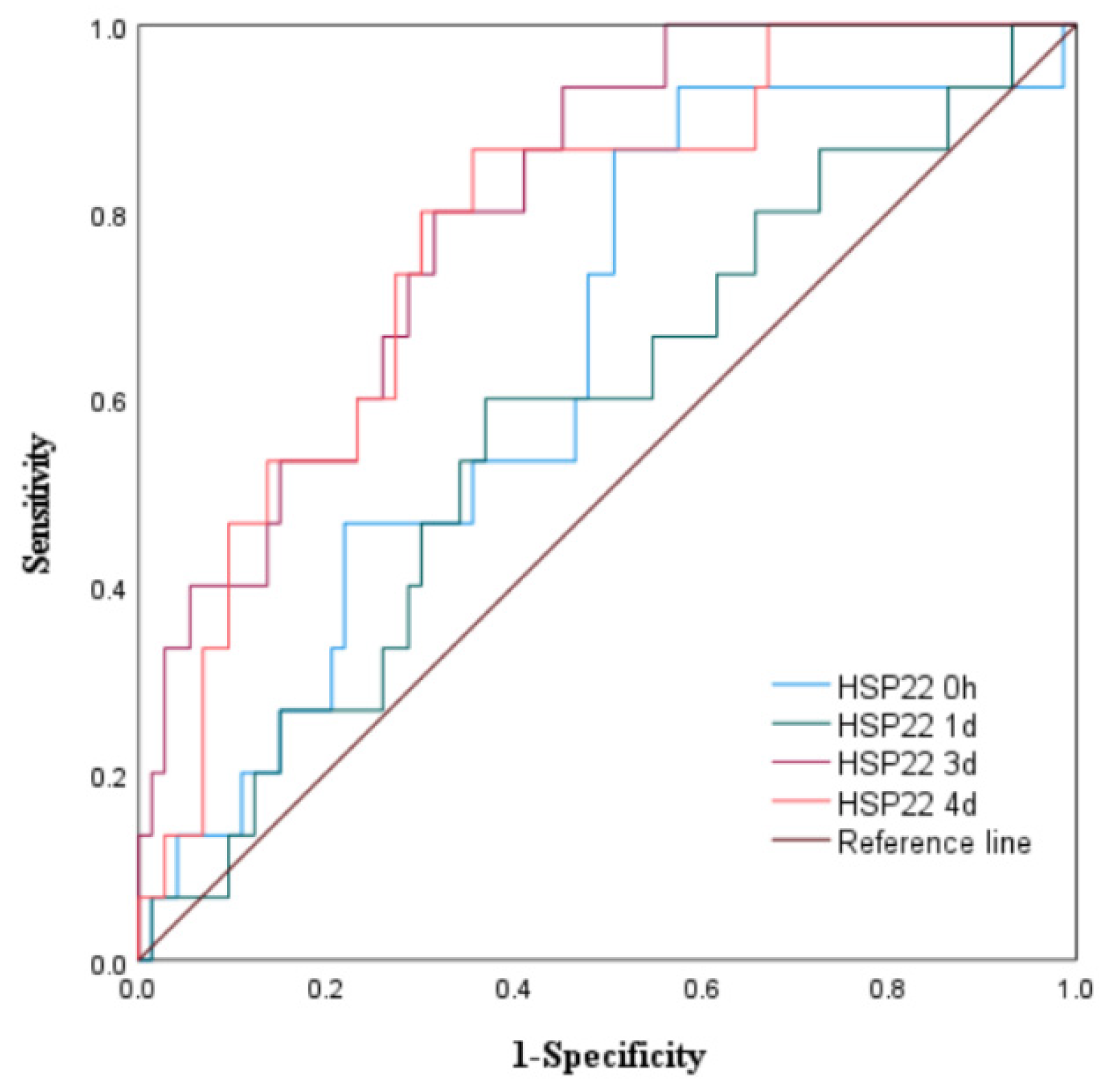
Figure 6.
ROC cuves of Prediction Curves for MACE Occurrence in HSP27 at Different Time Points in STEMI Patients Under aoina Emeraency PCI (N=88).
Figure 6.
ROC cuves of Prediction Curves for MACE Occurrence in HSP27 at Different Time Points in STEMI Patients Under aoina Emeraency PCI (N=88).
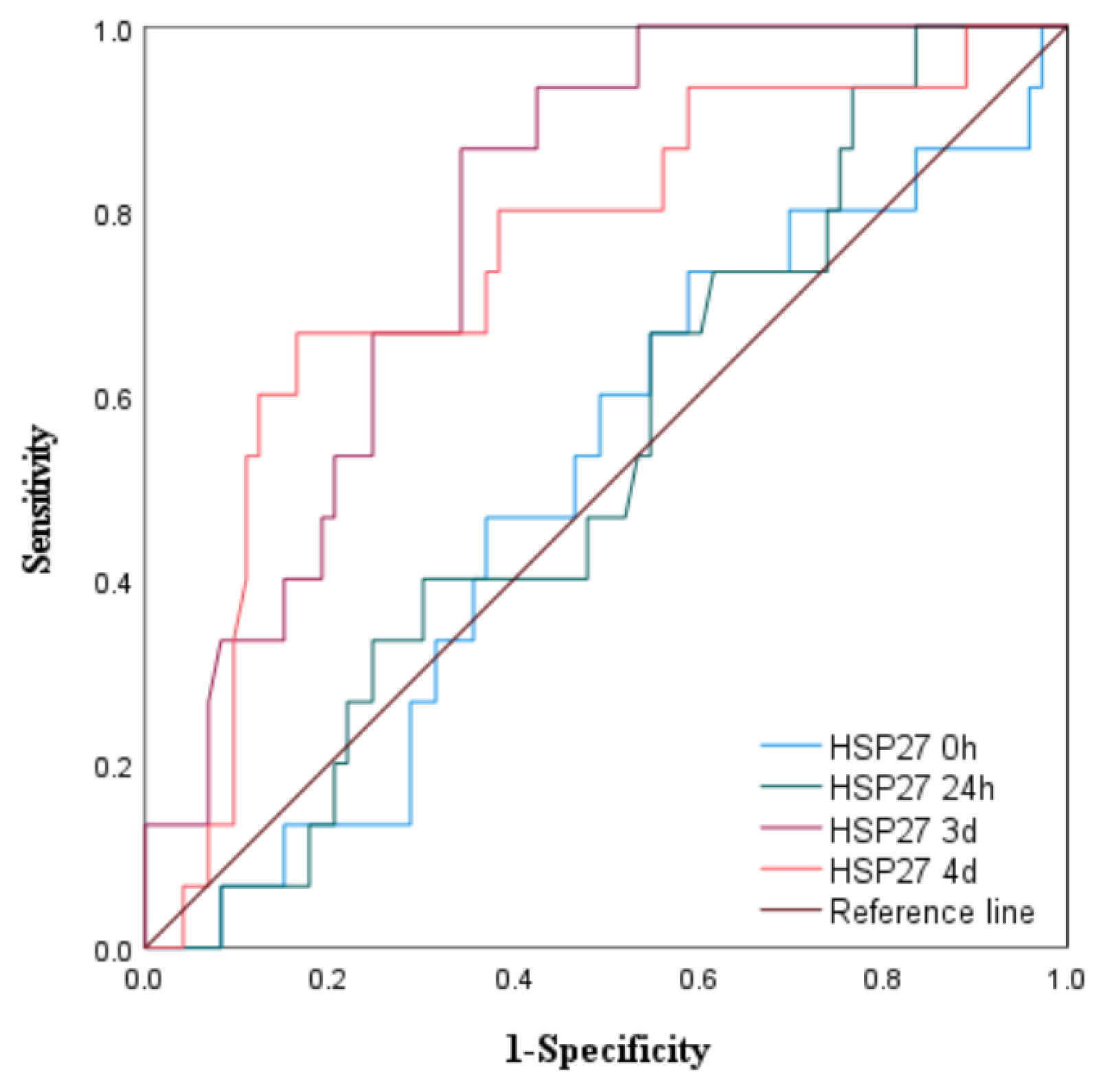
Figure 7.
ROC cuves of Prediction Curves for MACE Occurrence in HSP60 at Different Time Points in STEMI Patients Under aoina Emeraency PCI (N=88).
Figure 7.
ROC cuves of Prediction Curves for MACE Occurrence in HSP60 at Different Time Points in STEMI Patients Under aoina Emeraency PCI (N=88).
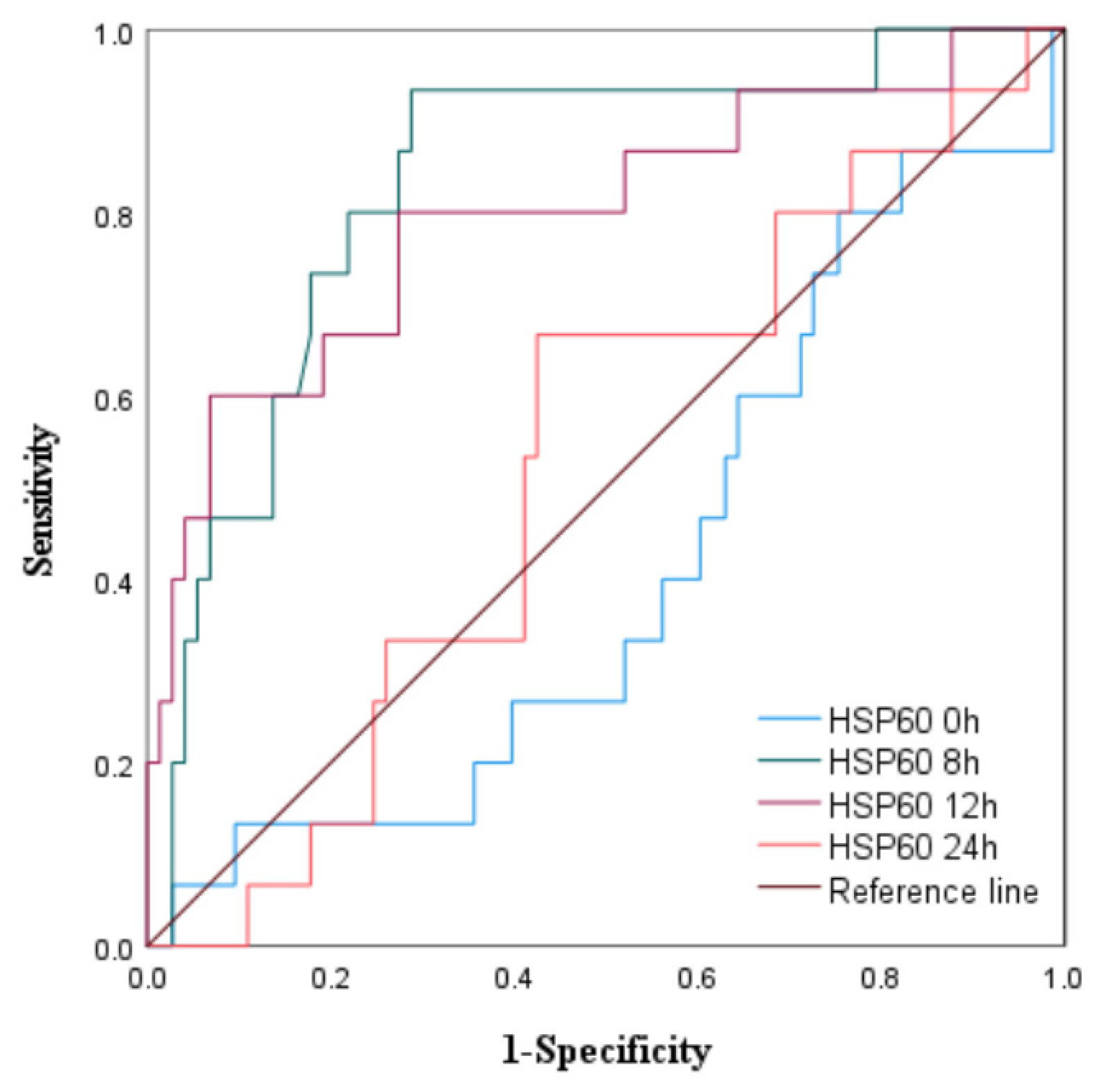
Figure 8.
ROC cuves of postoperative peak levels of HSP22, HSP27 and HSP60 for the occurence of MACE(N=88).
Figure 8.
ROC cuves of postoperative peak levels of HSP22, HSP27 and HSP60 for the occurence of MACE(N=88).
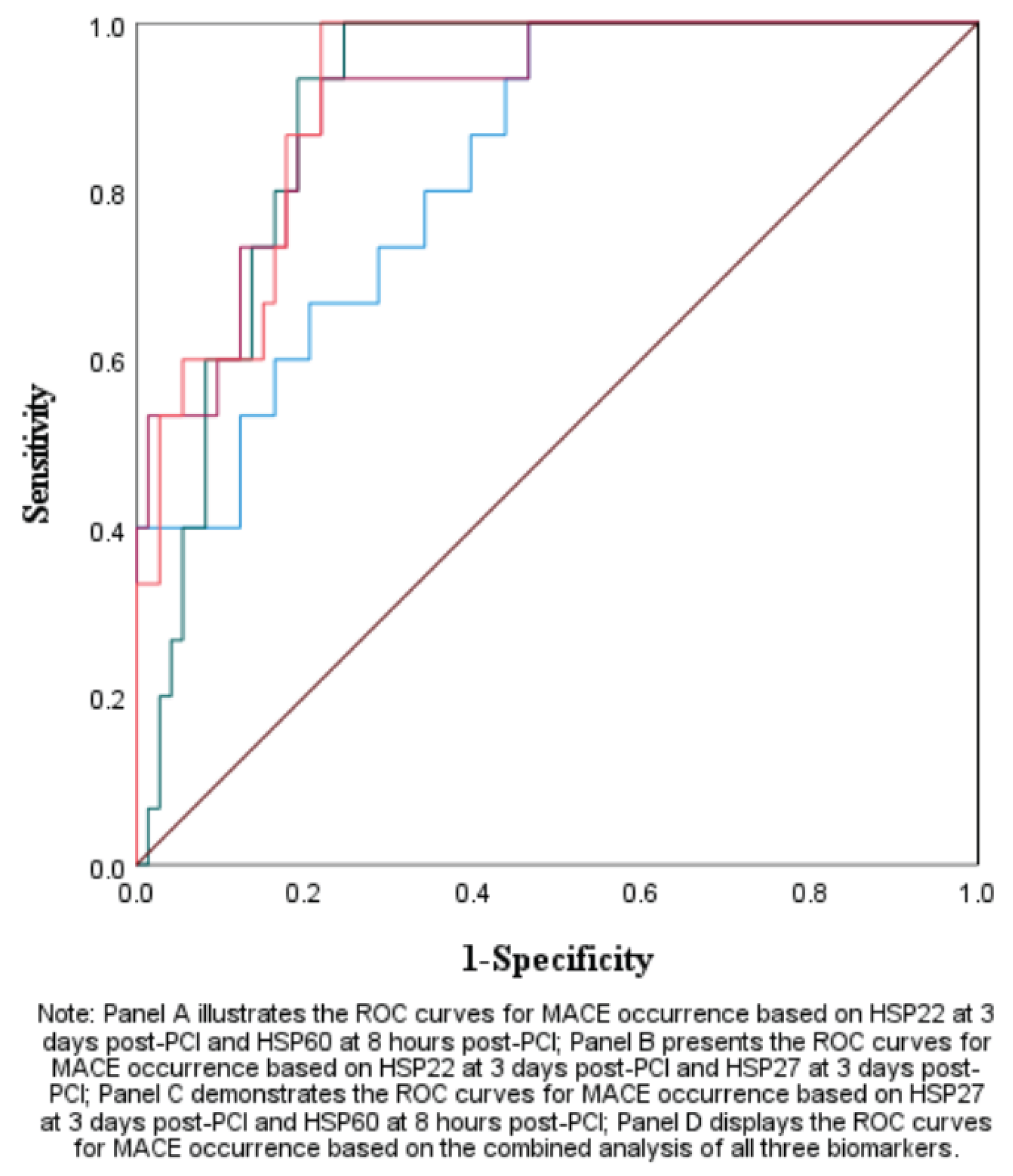

Table 1.
Baseline Data of Patients with Stable Coronary Heart Disease and STEMI.
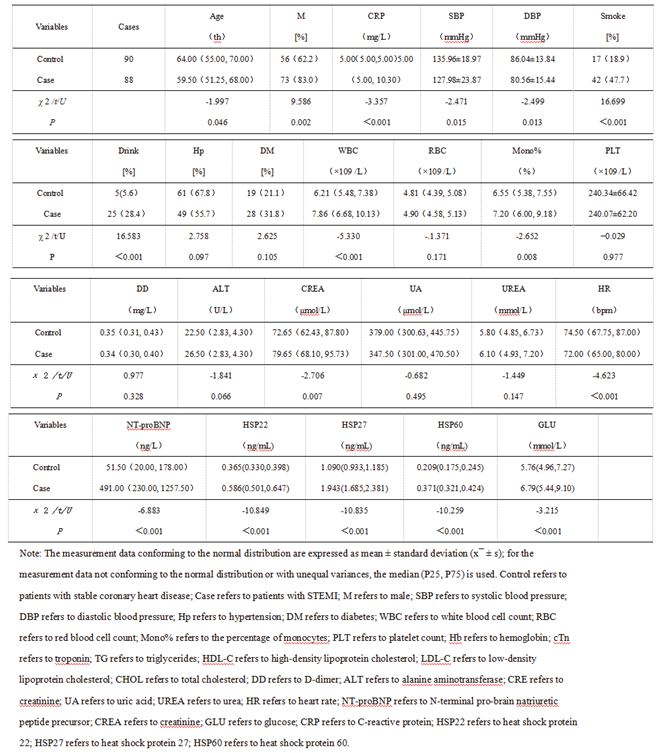 |
Table 2.
Baseline Data of STEMI Patients with High and Low Levels of HSP22 on the 3rd Day after Emergency PCI.
Table 2.
Baseline Data of STEMI Patients with High and Low Levels of HSP22 on the 3rd Day after Emergency PCI.
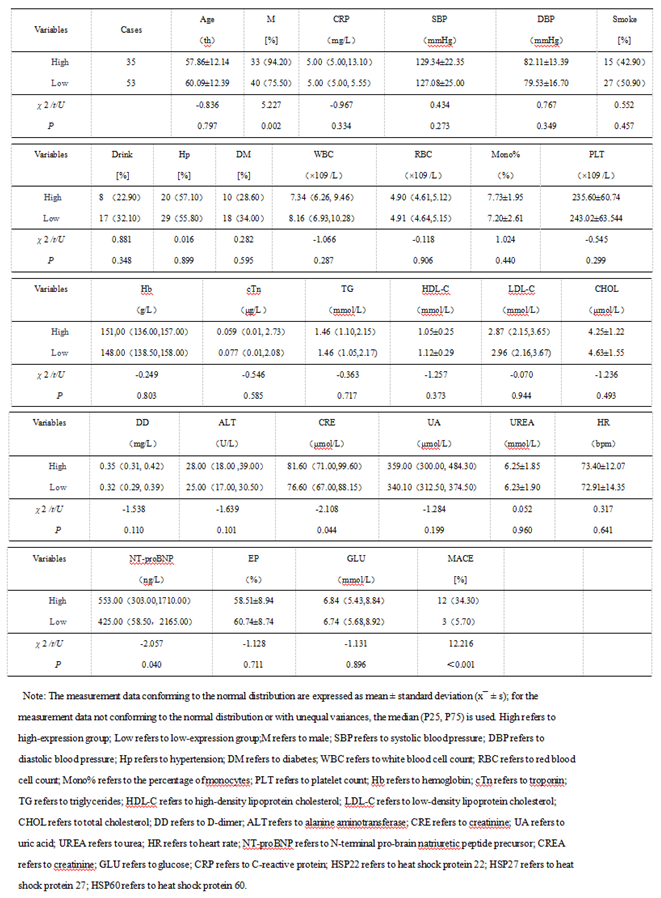 |
Table 3.
Baseline Data of STEMI Patients with High and Low Levels of HSP27 on the 3rd Day after Emergency PCI.
Table 3.
Baseline Data of STEMI Patients with High and Low Levels of HSP27 on the 3rd Day after Emergency PCI.
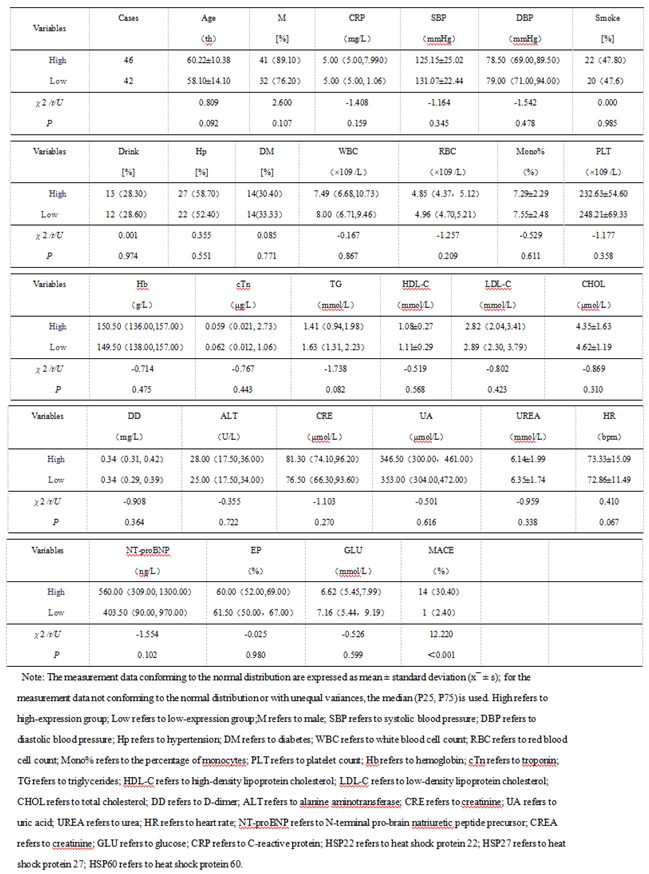 |
Table 4.
Baseline data of STEMI patients with elevated HSP60 levels 8 hours after emergency PCI surgery.
Table 4.
Baseline data of STEMI patients with elevated HSP60 levels 8 hours after emergency PCI surgery.
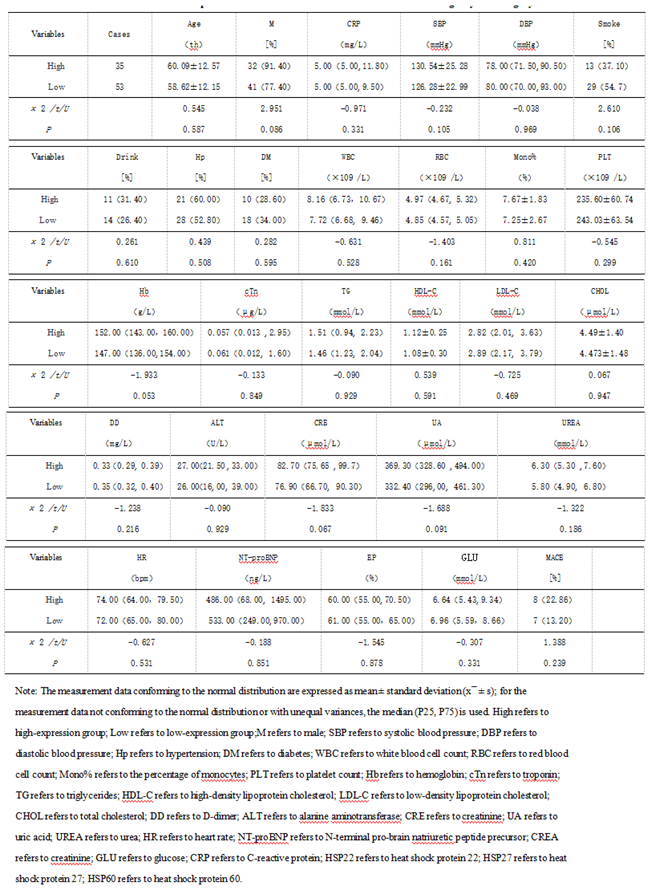 |
Table 5.
Odds Ratio of 3d HSP22/HSP27 and 8h HSP60 after PCI as Predictive Factors for MACE.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



