Submitted:
14 May 2025
Posted:
15 May 2025
You are already at the latest version
Abstract
Optical Coherence Tomography (OCT) is a relatively new medical imaging device that provides high-resolution and real-time visualization of biological tissues. Initially designed for ophthalmology, OCT is starting to be applied in other types of pathologies, like cancer diagnosis. This review highlights its impact on disease diagnosis, biopsy guidance, and treatment monitoring. Despite its advantages, OCT has limitations, particularly in tissue penetration and differentiating between malignant and benign lesions. To overcome these challenges, the integration of nanoparticles has emerged as a transformative approach, which significantly enhances contrast and tumor vascularization at the molecular level. Gold and superparamagnetic iron oxide nanoparticles, for instance, have demonstrated great potential in increasing OCT’s diagnostic accuracy through enhanced optical scattering and targeted biomarker detection. Beyond these innovations, integrating OCT with multimodal imaging methods, including magnetic resonance imaging (MRI), positron emission tomography (PET), and ultrasound, offers a more comprehensive approach to disease assessment, particularly in oncology. Additionally, advances in Artificial Intelligence (AI) and biosensors have further expanded OCT’s capabilities, enabling real-time tumor characterization and optimizing surgical precision. However, despite these advancements, clinical adoption still faces several hurdles. Issues related to nanoparticle biocompatibility, regulatory approvals, and standardization need to be addressed. Moving forward, research should focus on refining nanoparticle technology, improving AI-driven image analysis, and ensuring broader accessibility to OCT-guided diagnostics. By tackling these challenges, OCT could become an essential tool in precision medicine, facilitating early disease detection, real-time monitoring, and personalized treatment for improved patient outcomes.
Keywords:
optical coherence tomography (OCT)
; nanoparticles
; artificial intelligence (AI)
; targeted imaging and precision medicine
1. Introduction and Background
Optical Coherence Tomography (OCT), first developed in 1991 by Huang et al., marked a revolutionary milestone in medical imaging technology [1]. Originally applied in ophthalmology, OCT provided high-sensitivity micrometer resolution, cross-sectional retinal imaging in vivo [2,3], significantly improving early detection and quantitative monitoring of a variety of retinal disorders [4]. Over the last decades, OCT has expanded beyond ophthalmology, becoming a useful diagnostic tool in dermatology, oncology, and other medical fields. OCT is a non-invasive, non-contact imaging technique based on low-coherence interferometry to create 3D volumetric images of biological tissues [5,6,7]. The underlying principle is a Michelson-type interferometer employing a low-coherence light source: the light beam is splitted into two paths, one directed toward the sample and the other to a reference mirror; the recombination of the reflected beams generates an interference pattern only when the two optical path lengths match within the short coherence length of the source, which is on the order of micrometers, thus enabling depth-resolved imaging. OCT technology has continually improved [8]. In early OCT devices, called time-domain OCT (TD-OCT), the depth profile of the sample was retrieved by varying the path of the reference mirror. More efficient implementation allowing fast acquisition was the second generation of OCT devices, the spectral-domain OCT (SD-OCT) [9], in which the depth information is extracted in one shot, from the interference spectrum. Image quality, high speed, and high sensitivity of SD-OCT, which became the standard, opened the way to volumetric imaging in vivo [10]. Advancements in laser technology led to the swept-source OCT [SS-OCT], a spectral-domain configuration in which a wavelength-swept laser is used for rapidly tuning the emitted wavelength over a broad range [11,12]. The axial resolution of OCT, determined by the coherence length of the light source, is typically on the order of 10 μm. This micrometer-scale precision is critical for resolving thin structures like retinal layers or dermal microstructures [13,14]. OCT’s imaging depth generally spans a few millimeters, which is sufficient for examining semi-transparent tissues such as the retina, although deeper penetration remains challenging for denser tissues [15]. By acquiring depth profiles [A-scans] in raster scanning, the OCT systems generate cross-sectional images (B-scans) and en-face visualizations (C-scans), enabling comprehensive 3D imaging [16]. Lateral resolution, determined by the spot size of the probing beam, is limited by the optics.
A defining characteristic of OCT is its reliance on low-coherence light, which allows for precise measurement of optical path length differences based on interferometric detection of back-scattered light from tissue layers. This enables the high axial resolution that sets OCT apart from imaging modalities like ultrasound or MRI [17,18]. However, the coherent nature of the light source inherently introduces challenges, such as speckle noise, which degrades image quality and makes fine structural details difficult to resolve. Recent advancements, including photonic lanterns, have addressed this issue by reducing speckle contrast and enhancing image quality [17,19]. Compared to other imaging techniques, OCT provides unique advantages. Ultrasound, which operates using sound waves, typically offers a resolution of around 200 μm, while MRI delivers excellent soft tissue contrast but with lower spatial resolution. Moreover, OCT does not require ionizing radiation, making it safer for repeated use [20,21]. The performance of OCT depends on the properties of the light source. The spectral bandwidth of the OCT light source is indirectly proportional to the depth resolution. Superluminescent diodes (SLDs) are widely used for their broad spectral bandwidth and high output power, providing the micrometer-scale resolution required for clinical diagnostics [22]. Supercontinuum light sources, emerging as alternatives, offer ultra-broad spectral outputs for exceptional resolution and deeper tissue imaging, but their complexity and cost have limited widespread adoption [23]. Additionally, tunable lasers, often employed in frequency-domain OCT, enhance spectral data acquisition, enabling precise imaging of specific tissue types [24]. Performance parameters that are coupled are axial resolution and imaging depth. Shorter wavelengths provide higher resolution imaging but are limited by scattering in tissue, while longer wavelengths penetrate deeper into tissues but sacrifice resolution [25]. To overcome these trade-offs, innovations such as line-field confocal OCT and dual-channel systems have been developed [12], enhancing both imaging depth and resolution for broader clinical applications [26].
After recalling the background on the OCT technique, this review focuses on OCT’s transformative role in pathology, emphasizing its ability to visualize microstructures for diagnostics across ophthalmology, dermatology, oncology, and other medical applications. OCT’s non-invasive, real-time imaging capabilities have the potential for early detection and surgical guidance, offering significant advantages in patient care [27,28]. Recent advancements, including the integration of nanoparticles as contrast agents and multimodal imaging with MRI, demonstrate the growing potential of OCT in complex diagnostic workflows.
By bridging current clinical applications with emerging innovations, this review provides a comprehensive perspective on OCT’s evolution and its expanding role in modern medicine. The discussion of its technical foundations, limitations, and future possibilities aims to deepen understanding and highlight pathways for continued advancements in medical diagnostics.
2. Basics of OCT Imaging in Pathology
2.1. OCT’s Role in Pathological Diagnosis
As mentioned, OCT has emerged as a valuable high-resolution imaging tool in pathology, offering real-time cross-sectional visualization of biological tissues. Its non-invasive nature and ability to assess tissue microstructure make it a promising adjunct to conventional histopathological methods in diagnosing various diseases, including oncological, ophthalmological, neurological, and vascular disorders [1,29]. This section explores the role of OCT in detecting pathological changes, highlights the key histopathological features identifiable with OCT, and discusses its advantages and limitations.
OCT enables the detection of early structural abnormalities, which may relate to changes in tissue composition, extracellular matrix organization, and cellular density (Figure 1) [4,30]. Clearly, being an interferometry technique, OCT provides information on the structure of the sample, without any information on the material reflectance properties, like microscopy intensity-based imaging techniques.
While histopathology remains the gold standard for diagnosing cellular-level abnormalities, OCT offers several advantages in real-time tissue assessment, non-invasive imaging, immediate diagnosis [7], dynamic imaging capabilities [16], and repeated monitoring (Figure 2) [29].
However, OCT also has several limitations compared to histological examination: Limited Tissue Penetration; OCT typically penetrates only a few millimeters, making it less effective for deep tissue imaging [33], Lower Cellular Resolution; While OCT provides high-resolution images at micrometer scale, it does not match the subcellular detail seen in histology [34], Lack of Molecular Analysis; Histopathology allows for immunohistochemical staining and genetic profiling, whereas OCT primarily provides structural imaging [29].
2.2. OCT for Tissue Characterization and Guiding Biopsies
OCT has demonstrated its potential as a powerful tool for tissue characterization and biopsy guidance, significantly enhancing diagnostic accuracy and procedural efficiency across various medical fields. OCT enables precise biopsy targeting, reducing sampling errors and improving disease detection rates [28,35]. Traditional biopsy techniques often rely on blind sampling, where tissue is extracted based on preoperative imaging or physician estimation, which can result in false negatives or inadequate samples. In contrast, OCT-guided biopsy enables real-time visualization of tissue architecture, allowing clinicians to identify regions of interest (ROIs) and select optimal sampling sites, thereby improving diagnostic capability. Through improved accuracy of tumor identification and reduced likelihood of non-diagnostic samples, OCT represents a critical advancement in the field of diagnostic medicine [33,36].
One of the primary advantages of OCT in biopsy guidance is that it analyzes tissue layer disruptions, increased backscattering, and irregular tissue morphology. OCT provides a detailed map of suspicious regions, allowing for precise, targeted biopsy sampling [35,37]. This capability is particularly valuable in colorectal and esophageal cancer screening, where submucosal abnormalities can be detected with higher sensitivity than traditional white-light endoscopy [36].
Furthermore, OCT provides real-time intraoperative imaging, enabling surgeons and pathologists to assess tissue margins and tumor boundaries without needing frozen section analysis or extended pathology wait times [21,34]. This feature is particularly beneficial in breast-conserving surgery, where ensuring clear surgical margins is crucial in reducing recurrence rates [38]. OCT has also demonstrated success in urological surgeries, where cross-polarization OCT (CP-OCT) has been utilized for bladder cancer resection, providing feedback in real-time on tissue characteristics and minimizing unnecessary excess tissue removal [39].
As research continues to advance, OCT-guided biopsy is expected to integrate with artificial intelligence (AI) and multimodal imaging to further refine tissue classification and automate suspicious region detection [40]. Thus, OCT-guided biopsy represents a significant advancement in precision diagnostics, improving sampling accuracy, reducing procedural errors, and ultimately enhancing patient outcomes [29].
2.3. Clinical Applications of OCT
In ophthalmology, OCT is primarily utilized for the detection and monitoring of macular diseases, including diabetic retinopathy, age-related macular degeneration (AMD), and retinal vein occlusion. Studies have shown that SS-OCT can effectively screen for macular pathologies in cataract surgery patients, with sensitivity and specificity rates ranging from 63%–83% and 72%–89%, respectively [41,42]. As previously highlighted, OCT plays a critical role in evaluating retinal integrity, assisting in the diagnosis of conditions such as macular edema and retinal vein occlusion [40,43].
In dermatology, OCT provides detailed imaging of vascular networks and tissue morphology, enhancing the diagnostic accuracy of non-melanoma skin cancers [15,16]. Additionally, dynamic OCT has been used to visualize microvascular changes in conditions such as psoriasis, port-wine stains, and chronic venous ulcers, aiding in disease monitoring and treatment evaluation [44,45].
In vascular imaging, intravascular OCT (IVOCT) has enabled the detailed visualization of atherosclerotic plaques, vascular occlusions, and neovascularization, making it an essential tool in cardiology and ophthalmology [21,46]. Its ability to provide quantitative measurements of vessel morphology has been particularly beneficial in assessing diabetic retinopathy and cardiovascular disease and guiding endovascular interventions [25].
3. OCT in Oncology: Tumor Markers, Personalized Medicine, and Real-Time Treatment
3.1. The Role of OCT in Tumor Detection and Tumor Microenvironment Analysis
OCT has been extensively studied across various cancers, with significant applications in the diagnosis and assessment of malignancies in the skin, ocular tissues, breast, lungs, cervix, endometrium, colorectal region, brain, bladder, prostate, ovary, and the gastrointestinal tract [47]. OCT enables the differentiation between benign and malignant ocular tumors by visualizing key features such as hyperreflective epithelial thickening and abrupt transition zones (Fig2) [48,49]. In breast cancer, OCT demonstrates over 90% sensitivity in detecting residual cancerous tissue, aids lesion characterization, and, through polarization-sensitive OCT (PS-OCT), effectively differentiates breast cancer subtypes by analyzing the additional information of collagen birefringence, which provides critical insights into tumor invasiveness and treatment response [50,51,52].
Furthermore, in lung cancer, studies have demonstrated that OCT can effectively identify malignant pulmonary nodules, with some research indicating that it can achieve diagnostic accuracies comparable to histopathological assessments [53,54]. In the detection and evaluation of cervical cancer, particularly for identifying cervical intraepithelial neoplasia (CIN) and other precancerous lesions studies have revealed that OCT can achieve sensitivities ranging from 85% to 98% in detecting cervical lesions, although specificity can vary widely, often reported between 39% and 81% due to high false-positive rates [55,56,57]. Also, OCT has shown significant potential in the detection and evaluation of endometrial cancer; it is capable of differentiating normal, hyperplastic, and malignant tissues. Advanced OCT technologies, such as real-time rotational OCT, have been shown to effectively delineate endometrial layers with strong histological correlation [58]. Additionally, OCT's ability to assess endometrial vascularization and neovascularization offers critical insights into physiological and pathological changes, supporting its application in infertility assessment and cancer detection [58,59].
Moreover, in colorectal cancer, OCT has been validated as an effective tool for detecting dysplasia in submucosal layers, a critical step in early diagnosis and intervention [36]. The use of full-field OCT (FF-OCT) in neurosurgery is currently being explored for its potential to enhance real-time visualization of brain tissues, aiding in the precise removal of tumors and improving post-surgical outcomes [60]. In bladder cancer, CP-OCT has shown 94% sensitivity and 84% specificity in detecting high-grade urothelial dysplasia and carcinoma, making it an important tool for guiding biopsies and tumor resections [39].
While the diagnostic value of OCT in prostate cancer detection remains debated, recent advancements in needle-based OCT systems have demonstrated its potential for in vivo imaging and real-time identification of malignant tissues, which could revolutionize instant diagnosis and treatment planning, ultimately improving patient outcomes [61,62]. Over and above that, OCT has shown great potential in detecting and characterizing ovarian cancer based on microstructural changes, including collagen alterations [63,64]. The integration of OCT with AI techniques, such as convolutional neural networks (CNNs) for image processing, has demonstrated promising results in automating cancer detection, improving diagnostic accuracy, and reducing pathologists' workload [65]. Additionally, FF-OCT and intraoperative OCT applications, including their use in laparoscopic procedures, have enhanced real-time tumor margin assessment and metastasis detection [64]. Last but not least, in the oral cavity, OCT could identify dysplastic lesions and oral squamous cell carcinoma [66]. Also, in the esophagus, OCT is instrumental in detecting early neoplastic changes associated with conditions such as Barrett's esophagus, which can lead to esophageal adenocarcinoma. OCT’s ability to enable high-resolution imaging of the esophageal mucosa assists in identifying dysplastic areas that may not be visible through conventional endoscopy [36].
3.2. OCT-Guided Personalized Cancer Treatment
OCT enables real-time imaging during surgical procedures, allowing for immediate visualization of tumor characteristics and surrounding tissues. This capability is particularly crucial in complex surgeries where accurate tumor delineation directly impacts surgical success and long-term patient outcomes. Intraoperative OCT has been extensively studied for its role in guiding tumor resection by providing instant feedback on margin status.
Researchers demonstrated the utility of OCT in monitoring microstructural changes in pancreatic tumor organoids treated with radiation [67]. By capturing these changes in real time, clinicians can make immediate adjustments to treatment protocols, enhancing the precision of cancer therapies [68]. Additionally, a study explored the integration of OCT with confocal microscopy, effectively creating a “virtual biopsy” that combines high-resolution imaging with deep tissue penetration [69]. This approach enables immediate evaluation of skin lesions and supports real-time treatment decisions during dermatological procedures [29].
The application of OCT in breast-conserving surgery is particularly promising. A multicenter study demonstrated that intraoperative OCT could be used to assess tumor margins, ensuring complete excision and reducing the likelihood of reoperation [70,71]. By allowing surgeons to scan excised tissue in real time, OCT significantly lowers the incidence of positive margins. Furthermore, OCT has been investigated for its role in lymph node assessment during oncologic surgeries [72]. Studies suggest that OCT can detect micrometastases that might be missed by conventional histopathology, thereby enhancing real-time staging and treatment planning. These applications reinforce the value of OCT in improving surgical precision and reducing recurrence rates [28,73].
3.3. Key Limitations of OCT in Oncology
Despite its advantages, several limitations must be addressed to maximize its clinical utility. One of the most significant limitations of OCT in oncology is its limited imaging depth, which typically ranges between 1 mm to 2 mm in biological tissues. This limitation arises due to the high scattering of near-infrared light in biological tissues, which limits the penetration of OCT signals beyond superficial layers. As a result, deeper tumors or infiltrative malignancies may not be adequately visualized, limiting the comprehensive assessment of tumor margins and depth of invasion [68]. Another challenge in OCT imaging for oncology is its limited specificity in differentiating between tissues. While OCT excels in identifying tissue microarchitecture, it may not always reliably distinguish dysplastic lesions from invasive cancers, leading to potential false positives or false negatives [29]. In a study by Sunny et al. [66] OCT exhibited high sensitivity in detecting dysplastic lesions, but its specificity varied significantly depending on tissue type and imaging parameters. Also, differences in tumor regions, such as highly proliferative vs. necrotic areas, can result in OCT capturing inconsistent tissue characteristics, making standardized assessment difficult [74].
Recent advancements in nanotechnology-based contrast agents have shown promise in overcoming many of OCT’s limitations in oncology. Consequently, there is an increasing need for contrast-enhanced imaging approaches to improve OCT’s specificity in oncological applications. Nanoparticle-enhanced OCT imaging integrates tumor-specific nanoparticles, allowing for targeted imaging of cancerous tissues with improved sensitivity and contrast. This approach leverages nanoparticles conjugated with biomolecular markers, enabling OCT to highlight malignant regions with greater specificity [73].
4. Nanoparticles in OCT Imaging: Enhancing Diagnostic and Therapeutic Capabilities
4.1. The Role of Nanoparticles in OCT Contrast Enhancement
Hence, as it has been mentioned in the previous section, nanoparticles have emerged as pivotal agents for enhancing the contrast, sensitivity, and optical scattering in OCT through several mechanisms rooted in their unique optical properties. The integration of nanoparticles into OCT technology has shown substantial promise in overcoming the inherent limitations of standard OCT, particularly concerning tissue optical contrast. One of the primary ways nanoparticles improve OCT is through their peculiar scattering properties. The effective manipulation of the scattering cross-section of nanoparticles has been well-documented [27,75]. For instance, it has been shown that the size and shape of gold nanoparticles (GNPs, also referred to as AuNPs) can be tuned to optimize their scattering characteristics, thus improving the quality and contrast of OCT images in challenging environments like highly scattering biological tissues [75,76,77]. Another noteworthy enhancement comes from the development of nanoparticles that serve as photothermal agents, which leverage the thermal response of the nanoparticles under laser excitation to alter the phase and the intensity of the OCT signal [78,79]. This adjustment helps to augment the imaging contrast further by increasing backscattering from the regions containing nanoparticles. Additionally, this method allows for deeper tissue imaging, which is particularly beneficial in complex structures such as tumors, where traditional imaging might falter due to scattering effects [78,80]. Enhanced imaging sensitivity has been demonstrated in vivo, where nanoparticles have markedly improved the visibility of microcirculatory dynamics in tumor environments and facilitated the identification of distinct pathological changes [78,81]. Furthermore, advancements in the design of nanoparticle contrast agents, including the use of Janus microspheres and multifunctional nanoparticles, have broadened the scope of OCT applications. These innovative materials are capable of enhancing both absorption and scattering concurrently, thus producing a synergistic effect that significantly boosts imaging resolution and depth penetration in various tissues, including in vivo scenarios [78,82].
Also, particularly when it comes to metallic nanoparticles such as gold and silver. A fundamental mechanism by which nanoparticles increase optical scattering is through plasmon resonance. Metallic nanoparticles can support localized surface plasmon resonances (LSPRs), which occur when the conduction electrons in the nanoparticles oscillate at specific frequencies in response to incident light. This phenomenon significantly amplifies the scattering cross-section of the nanoparticles, leading to enhanced backscattering of light in the OCT system. For instance, specific studies have reported that GNPs exhibit highly efficient scattering processes, where the scattering cross-section can reach up to 0.7 × 10^-10 cm² per nanoparticle [27]. Such strong scattering capabilities are particularly effective in the near-infrared region, commonly used in OCT imaging of biological tissues. Additionally, the control over the size and shape of nanoparticles allows for tuning their optical properties, resulting in varied scattering efficiencies [83]. The architecture of nanoparticle assemblies can also lead to synergistic increases in scattering, further enhancing overall imaging contrast [76]. Another important mechanism involves the enhancement of scattering due to interactions between nanoparticles and the surrounding medium. The relative refractive index contrast between nanoparticles and their environment plays a critical role in the backscattering of light. In biological media, nanoparticles can effectively increase the backscattering coefficient, allowing for clearer differentiation between tissue and lesions, and facilitating enhanced imaging capabilities [27,84]. Moreover, employing engineered nanoparticles with magnetic and plasmonic properties presents a new frontier in OCT image enhancement. These hybrid nanoparticles can increase scattering and dynamically adjust their properties in response to external magnetic fields, improving contrast and signal clarity during imaging procedures [85].
4.2. Types of Nanoparticles for OCT Applications
Multiple types of nanoparticles are under investigation as contrast agents in OCT due to their unique optical properties, which expand the capability of OCT for enhanced imaging in biomedical applications. Notably, AuNPs and silver nanoparticles (AgNPs) stand out prominently, with silicon nanoparticles (SiNPs) and various hybrid nanoparticle systems also showing potential. AuNPs are extensively studied for OCT due to their strong light-scattering ability resulting from surface plasmon resonance (SPR). Gold nano bipyramids are extensively studied for OCT due to their strong light-scattering ability resulting from surface plasmon resonance and tunable absorption properties that can be optimized for specific imaging applications, especially in vivo settings [78,86]. Research indicates that these structures improve the delineation of vascular structures and help visualize intricate biological processes, broadening their applicability in areas like melanoma research [76,78]. AgNPs’ localized SPR provides strong scattering signals, which can significantly enhance contrast during imaging. Recent studies have demonstrated the application of AgNPs in SS-OCT, showing favorable results in improving the imagery of animal tissues and outperforming more conventional contrast agents such as titanium dioxide (TiO₂) nanoparticles. The manipulation of AgNPs’ size and shape further enhances capabilities, allowing for tailored imaging based on specific biological contexts [87].
SiNPs are gaining interest for their high refractive index and favorable scattering characteristics, making them suitable candidates for contrast enhancement in OCT [77,88]. Emerging materials, such as plasmonic copper sulfide nanoparticles, are being explored as innovative contrast agents that operate differently from traditional scattering agents. Rather than scattering light, copper sulfide nanoparticles absorb probing light, enabling improved contrast in OCT images by creating dark contrast properties at specific optical transparency windows [80]. Recent discoveries indicate that integrating magnetic and plasmonic materials can yield innovative contrast agents capable of optimizing OCT while assisting in molecular recognition tasks, thereby enhancing diagnostic capabilities in clinical practice [89,90]. This novel approach can significantly enhance visualization in applications requiring differential imaging techniques.
AuNPs enhance OCT due to their unique scattering properties, influenced by their size, shape, surface chemistry, and strong light-scattering capabilities [78,91]. Various forms of AuNPs, including nanoshells, nanorods, and nanoprisms, can be engineered to manipulate their scattering properties, tailoring them for specific OCT applications [83]. Furthermore, the ease of conjugation of gold nanoparticles with antibodies or peptides enhances their ability to target specific tissues or cells, significantly increasing the contrast and specificity of OCT imaging in pathological situations such as cancer [76]. Iron oxide nanoparticles, particularly superparamagnetic forms, exhibit strong light-scattering and magnetic properties that enhance their utility in imaging technologies, including OCT. These nanoparticles can alter the local magnetic field and induce localized susceptibility, resulting in increased contrast in OCT images. Their size allows for enhanced scattering efficiency, and they can be utilized in magnetomotive OCT applications to track cellular uptake and migration effectively [92]. This function is particularly valuable in characterizing inflammatory processes and studying cardiovascular diseases through the imaging of macrophage activity at vasculature sites [85]. Quantum dot nanoparticles (QDs) enhance OCT imaging through their unique optical properties, including size-tunable fluorescence and high quantum yield [93]. Quantum dots are particularly valuable because they can be engineered to emit at specific wavelengths that align with the imaging capabilities of OCT systems, thus providing improved contrast and imaging depth [94]. The tunability of their emission spectra allows for simultaneous imaging of multiple targets, facilitating comprehensive assessments of biological processes in real-time [93].
Despite promising preclinical results, the use of biocompatible nanoparticles in OCT still faces challenges related to synthesis consistency, cytotoxicity risks [95,96], and clinical translation [97], including stability and integration into clinical workflows [98]. Table 1 summarizes all the benefits and difficulties around nanoparticle applications in OCT (Table 1).
4.3. Tumor-Targeting Nanoparticles in OCT Imaging for Personalized Medicine
OCT can be employed to monitor changes in the optical properties of tissues after administering nanoparticles, providing insights into their biodistribution and localization [99,100]. A recent study investigated the use of OCT in conjunction with microneedle-based transdermal drug delivery systems. This research highlighted how OCT's chronological assessment capabilities can evaluate the penetration depth and distribution of nanoparticles administered via microneedles. Specifically, OCT allowed for the visualization of microchannels created by microneedling and the resulting drug delivery efficiency, thus demonstrating a dual role of monitoring both the device's performance and the biodynamics of nanoparticle transport in vivo [101]. Moreover, certain studies have demonstrated that OCT can effectively monitor the deployment of nanoparticles in ocular applications [102,103,104]. Evidence shows the effectiveness of intraoperative OCT (iOCT) in evaluating drug deposition within the subretinal space during surgeries utilizing nanoparticle formulations [105]. This provides critical feedback regarding the placement and integrity of therapeutics within sensitive ocular environments. Additionally, OCT has been shown to visualize the interactions between nanoparticles and biological barriers, allowing researchers to study how morphology influences biodistribution data. Another promising avenue is the pursuit of OCT-enhanced imaging of AuNPs, which have distinct optical properties facilitating their detection via OCT techniques. Such applications suggest that OCT is applicable for real-time monitoring of theranostic nanoparticles and could serve as an in vivo diagnostic tool by enhancing contrast imaging capabilities when nanoparticles are utilized [99]. One study demonstrated the potential to observe physiological changes in the skin during the transdermal delivery of AuNPs, allowing for quantitative assessments of therapeutic penetration and localization [106]. Table 2 outlines the key benefits (e.g., enhanced imaging contrast, theranostic applications) and challenges (e.g., toxicity, regulatory hurdles) of using nanoparticles in OCT (Table 2).
5. Future Directions in OCT Imaging for Pathology and Oncology
5.1. Overcoming OCT Limitations with Nanotechnology
Nanoparticles have significant potential to enhance the differentiation of tumor subtypes by serving as versatile platforms for delivering diagnostic and therapeutic agents that can recognize unique molecular features in various cancers. Each tumor subtype exhibits a distinct set of biomarkers, often characterized by specific protein expressions or genetic profiles. A study discussing prognostic implications in small cell lung cancer (SCLC) illustrates that specific molecular subtypes correlate with distinct immune characteristics and treatment responses, underscoring the potential for nanoparticle-mediated identification based on varying biomarker expressions [107]. Furthermore, research in ovarian cancer indicates that different tumor-associated markers are enriched in subtype classifications, suggesting that nanoparticle systems can be tailored to isolate and visualize these specific markers effectively [108].
Moreover, engineered nanoparticles can serve as powerful tools in the characterization and differentiation of breast cancer subtypes. The investigation of high-forming binding protein 17 (FBP17) has shown its expression to be linked to differentiation among ductal carcinomas, suggesting a role for FBP17 in subtype classification [109]. By combining these differentiation markers with nanoparticles that can bind selectively to them, researchers may enhance the resolution of subtype differentiation in diagnostic settings. Next-generation nanoparticles, particularly those engineered for enhanced contrast in imaging technologies, including OCT, are expected to transform tumor imaging paradigms. Recent advances in material science have led to multifunctional nanoparticles that incorporate imaging contrast agents, allowing them to highlight tumor tissues in real-time [110]. These advancements may include the use of nanoscale agents that are sensitive to specific optical frequencies and provide enhanced contrast by exploiting the optical scatter of tumor microenvironment characteristics. In OCT, nanoparticles can be designed to reflect OCT light more efficiently in the presence of tumor markers, creating a stronger contrast between healthy and malignant tissues. By encoding optical properties into the nanoparticles in correspondence with specific biochemical markers or cellular structures, researchers can achieve high-resolution imaging that reveals details about tumor subtype heterogeneity [111]. Engineered nanoparticles can also be modified to respond uniquely to tumor microenvironment cues, such as pH or enzyme activity, enhancing their specificity in imaging applications. This can lead to improved visualization of not only tumor size and shape but also subcellular characteristics relevant to subtype classification. By conjugating nanoparticles with ligands that selectively bind to proteins overexpressed in specific tumor types—such as HER2 in breast cancers or CD44 in certain bladder cancers—researchers can utilize the enhanced imaging capabilities of these systems to delineate subtype features with improved clarity [112].
5.2. Multimodal Imaging: Integrating OCT with MRI, PET, and Ultrasound
Combining OCT with other imaging modalities like ultrasound, MRI, and PET significantly enhances diagnostic accuracy by utilizing the unique advantages of each technology [113,114]. This integration allows for a more comprehensive assessment, leading to improved identification of diseases and better patient management.
The combination of OCT and MRI is particularly effective in diagnosing neurodegenerative diseases such as Multiple Sclerosis (MS) and Alzheimer’s disease. OCT provides high-resolution images of the retina, allowing for the assessment of retinal nerve fiber layer (RNFL) thickness, which has been identified as a potential biomarker associated with brain atrophy detected by MRI [115]. Research shows that changes in retinal structure observable through OCT correlate with cognitive decline and brain volume in Alzheimer's patients, indicating that OCT can provide valuable information about underlying neurological conditions [115,116]. The integration of these technologies not only enhances the specificity of diagnoses but also aids in monitoring disease progression more accurately. In oncology, the combination of OCT and MRI can elucidate the characteristics of tumors, particularly in organs such as the breast or prostate. MRI provides detailed soft-tissue morphology, while OCT can delineate the microstructural features of tumors in real time, which is crucial for surgical planning and treatment strategies [117].
Merging OCT with Positron Emission Tomography (PET) enhances diagnostic capabilities, particularly in cancer detection and monitoring. PET provides insights into the metabolic activity of tissues, while OCT excels in structural imaging [118]. The simultaneous use of these modalities allows for the identification of malignant lesions that may not be evident via PET alone. Integrative approaches using OCT alongside functional imaging from PET have shown improvements in diagnostic accuracy when investigating various malignancies. PET can identify hypermetabolic areas indicative of malignancy, while OCT clarifies lesion boundaries and provides additional histological information, yielding a superior overall diagnostic profile [119].
Ultrasound imaging combined with OCT offers distinct advantages, particularly in assessing superficial lesions. While ultrasound provides excellent spatial resolution and can evaluate depth, it is limited in providing detailed microstructural information about soft tissues. Conversely, OCT delivers high-resolution images of retinal and other tissues, allowing for the assessment of structural anomalies that ultrasound cannot effectively capture. In dermatological applications, the integration of OCT with ultrasound can enhance the evaluation of skin lesions, providing a comprehensive approach to diagnose conditions such as skin cancers [117].
Recent studies indicate that multimodal imaging approaches, such as the combination of OCT with MRI and PET, can lead to significant improvements in diagnostic accuracy across various patient populations [120]. In patients with uncertain diagnoses, the incorporation of additional imaging modalities often results in more definitive diagnostics—up to 31% improvement in diagnoses has been noted, showcasing the power of combined data [121]. Moreover, in instances of complex conditions such as multiple sclerosis, integrating OCT with MRI has demonstrated a greater capacity to predict disability outcomes than using MRI alone [122,123]. Furthermore, in conditions like glaucoma, OCT’s ability to measure retinal thickness and nerve fiber layer integrity complements ultrasound’s ability to assess optic disc morphology, leading to enhanced diagnostic reliability for glaucoma detection [124]. This combination can help ensure that patients receive prompt and appropriate interventions, ultimately improving prognoses.
While such integrated approaches have the potential to enhance diagnostic accuracy and provide more comprehensive clinical information, several obstacles inhibit their widespread implementation in clinical practice. One of the primary challenges in multimodal imaging with OCT arises from technical limitations associated with each imaging modality. For instance, OCT is highly sensitive to motion artifacts due to its reliance on coherent light, and any patient movement can lead to suboptimal images [125]. Secondly, combining data from multiple imaging modalities increases the volume of information that clinicians must manage. The integration process is often cumbersome, necessitating advanced software solutions and skilled personnel capable of interpreting the resulting multimodal data [120].
5.3. Personalized Medicine: Combination of AI and OCT-Guided Precision Oncology
The combination of smart probes, biosensors, and AI significantly enhances OCT-guided diagnostics, specifically in the realm of personalized medicine [126,127]. This integration provides a multifaceted approach that enables more accurate diagnostic assessments, tailored treatment strategies, and improved patient outcomes [118]. Firstly, by using targeted biosensors, clinicians can detect subtle biochemical changes related to various diseases. This is particularly valuable in oncological applications where early detection is crucial. Combining AI with data from these smart probes allows for sophisticated analysis and pattern recognition; this increases the probability of identifying cancerous tissues with greater accuracy compared to standard OCT imaging alone [128]. Secondly, coupled with AI, these probes can analyze data instantaneously, providing immediate feedback regarding the cancer microenvironment, metabolic changes, or inflammatory responses in tissues. For instance, AI algorithms can process OCT data to monitor tumor responses to treatment, allowing clinicians to make swift adjustments to personalized therapy based on live data [129]. This capability is particularly beneficial in managing chronic diseases where adjustments to treatment protocols are frequently needed.
Additionally, the substantial amount of data generated by OCT systems integrated with biosensors can be efficiently managed by AI algorithms. Traditional methods of data interpretation can be time-consuming and prone to human error. AI technology automates the diagnostic process by analyzing patterns in OCT scans combined with biosensor outputs, reducing variability and improving diagnostic reliability [130]. Recent studies have demonstrated that AI can analyze OCT images of oral lesions with a sensitivity and specificity of over 98%, assisting clinicians in making informed decisions [131]. Such automated systems fulfill a crucial role in personalized medicine by providing consistent monitoring across patient populations. Next, the integration of smart probes and AI facilitates the development of personalized treatment plans tailored to the patient’s unique biological profile. For example, biosensors that detect specific biomarkers allow clinicians to evaluate a patient’s response to therapy in real time. With continuous data acquisition, AI can correlate biomarkers with treatment outcomes, optimizing personalized therapeutic approaches for individual patients [132]. This precision medicine approach significantly enhances treatment effectiveness while minimizing potential side effects by allowing for timely adjustments based on real-time data.
Moreover, smart probes and biosensors can be miniaturized and designed for point-of-care use, making advanced diagnostics accessible outside traditional clinical settings. This portability enables earlier interventions and monitoring in rural or underserved areas, contributing to timely personalized medicine strategies [133]. For instance, in oral oncology, portable biosensors paired with AI-driven OCT diagnostics allow for non-invasive assessments in outpatient settings, facilitating earlier diagnoses and interventions for at-risk populations [134].
6. Conclusion
OCT has proved to be a transformative imaging technology, providing high-resolution, real-time visualization of tissue microstructures in various pathological conditions. In oncology, OCT facilitates early tumor detection, intraoperative margin assessment, and real-time monitoring of treatment response, offering a non-invasive and precise alternative to conventional imaging modalities. However, despite its advantages, OCT faces limitations, particularly in imaging depth and specificity, which restrict its ability to assess deep-seated tumors and differentiate between malignant and benign lesions with high accuracy. The integration of nanoparticles into OCT imaging has been proposed as a promising solution to enhance contrast, improve tumor delineation, and enable targeted imaging of specific biomarkers.
Nanoparticles, particularly gold and superparamagnetic iron oxide nanoparticles, have demonstrated significant potential in overcoming OCT’s limitations by improving scattering properties, increasing imaging contrast, and enabling functional imaging at a molecular level. Their ability to serve as contrast agents and therapeutic carriers underscores their role in advancing OCT-based precision oncology. Furthermore, the combination of OCT with multimodal imaging techniques such as MRI, PET, and ultrasound has shown promise in enhancing diagnostic accuracy by leveraging complementary imaging strengths.
Beyond oncology, OCT's integration with artificial intelligence (AI) and biosensors has further strengthened its role in personalized medicine. AI-driven image analysis facilitates real-time tumor characterization, aiding in the optimization of treatment strategies and minimizing unnecessary tissue removal during surgery. The incorporation of smart and stimuli-responsive imaging agents enables OCT to provide dynamic insights into tumor microenvironment changes, opening new possibilities for targeted therapy and theranostics.
Despite these advancements, challenges remain in translating nanoparticle-enhanced OCT and multimodal imaging into routine clinical practice. Issues related to biocompatibility, regulatory approval, and scalability must be addressed to ensure safe and effective implementation. Future research should focus on refining nanoparticle formulations, enhancing targeting specificity, and integrating AI-driven image processing to optimize OCT’s clinical utility. By addressing these challenges, OCT has the potential to become an indispensable tool in precision oncology, facilitating early diagnosis, real-time treatment monitoring, and personalized therapeutic interventions, ultimately improving patient outcomes.
Funding
This work was supported by the European Union’s Horizon Europe research and innovation programme under the project PROCT, Grant Agreement No. 101069279.
Conflicts of Interest
The authors declare no conflict of interest.
References
- D. Huang et al., “Optical Coherence Tomography,” Science (1979), vol. 254, no. 5035, pp. 1178–1181, Nov. 1991. [CrossRef]
- E. A. Swanson et al., “In vivo retinal imaging by optical coherence tomography,” Opt Lett, vol. 18, no. 21, p. 1864, Nov. 1993. [CrossRef]
- A.F. Fercher, C. K. Hitzenberger, W. Drexler, G. Kamp, and H. Sattmann, “In Vivo Optical Coherence Tomography,” Am J Ophthalmol, vol. 116, no. 1, pp. 113–114, Jul. 1993. [CrossRef]
- L. M. Sakata, J. DeLeon-Ortega, V. Sakata, and C. A. Girkin, “Optical coherence tomography of the retina and optic nerve – a review,” Clin Exp Ophthalmol, vol. 37, no. 1, pp. 90–99, Jan. 2009. [CrossRef]
- A. Mokhtari, B. M. Maris, and P. Fiorini, “A Survey on Optical Coherence Tomography—Technology and Application,” Bioengineering, vol. 12, no. 1, p. 65, Jan. 2025. [CrossRef]
- A. Pizurica et al., “Multiresolution Denoising for Optical Coherence Tomography: A Review and Evaluation,” Curr Med Imaging Rev, vol. 4, no. 4, pp. 270–284, Nov. 2008. [CrossRef]
- W. Drexler, M. Liu, A. Kumar, T. Kamali, A. Unterhuber, and R. A. Leitgeb, “Optical coherence tomography today: speed, contrast, and multimodality,” J Biomed Opt, vol. 19, no. 7, p. 071412, Jul. 2014. [CrossRef]
- J. Fujimoto and E. Swanson, “The Development, Commercialization, and Impact of Optical Coherence Tomography,” Investigative Opthalmology & Visual Science, vol. 57, no. 9, p. OCT1, Jul. 2016. [CrossRef]
- A.F. Fercher, C. K. Hitzenberger, G. Kamp, and S. Y. El-Zaiat, “Measurement of intraocular distances by backscattering spectral interferometry,” Opt Commun, vol. 117, no. 1–2, pp. 43–48, May 1995. [CrossRef]
- M. Wojtkowski, R. Leitgeb, A. Kowalczyk, T. Bajraszewski, and A. F. Fercher, “In vivo human retinal imaging by Fourier domain optical coherence tomography,” J Biomed Opt, vol. 7, no. 3, p. 457, 2002. [CrossRef]
- M. Choma, M. Sarunic, C. Yang, and J. Izatt, “Sensitivity advantage of swept source and Fourier domain optical coherence tomography,” Opt Express, vol. 11, no. 18, p. 2183, Sep. 2003. [CrossRef]
- A. Dubois et al., “Line-field confocal optical coherence tomography for high-resolution noninvasive imaging of skin tumors,” J Biomed Opt, vol. 23, no. 10, p. 1, Oct. 2018. [CrossRef]
- R. K. Manapuram, V. G. R. Manne, and K. V. Larin, “Development of phase-stabilized swept-source OCT for the ultrasensitive quantification of microbubbles,” Laser Phys, vol. 18, no. 9, pp. 1080–1086, Sep. 2008. [CrossRef]
- S. Caujolle et al., “Speckle variance OCT for depth resolved assessment of the viability of bovine embryos,” Biomed Opt Express, vol. 8, no. 11, p. 5139, Nov. 2017. [CrossRef]
- B. Wan et al., “Applications and future directions for optical coherence tomography in dermatology*,” British Journal of Dermatology, vol. 184, no. 6, pp. 1014–1022, Jun. 2021. [CrossRef]
- S. Schuh et al., “Imaging Blood Vessel Morphology in Skin: Dynamic Optical Coherence Tomography as a Novel Potential Diagnostic Tool in Dermatology,” Dermatol Ther (Heidelb), vol. 7, no. 2, pp. 187–202, Jun. 2017. [CrossRef]
- R. Maltais-Tariant, R. Itzamna Becerra-Deana, S. Brais-Brunet, M. Dehaes, and C. Boudoux, “Speckle contrast reduction through the use of a modally-specific photonic lantern for optical coherence tomography,” Biomed Opt Express, vol. 14, no. 12, p. 6250, Dec. 2023. [CrossRef]
- Y. Li, Y. Ling, J. Mao, and Y. Su, “Robust and automated dispersion compensation for FD-OCT using fractional Fourier transform,” in Optical Coherence Tomography and Coherence Domain Optical Methods in Biomedicine XXVIII, J. A. Izatt and J. G. Fujimoto, Eds., SPIE, Mar. 2024, p. 85. [CrossRef]
- M. R. N. Avanaki, M. J. Marques, A. Bradu, A. Hojjatoleslami, and A. G. Podoleanu, “A new algorithm for speckle reduction of optical coherence tomography images,” J. A. Izatt, J. G. Fujimoto, and V. V. Tuchin, Eds., Mar. 2014, p. 893437. [CrossRef]
- S. Lotz et al., “Large area robotically assisted optical coherence tomography (LARA-OCT),” Biomed Opt Express, vol. 15, no. 6, p. 3993, Jun. 2024. [CrossRef]
- T. Peñate Medina et al., “Imaging Inflammation – From Whole Body Imaging to Cellular Resolution,” Front Immunol, vol. 12, Jun. 2021. [CrossRef]
- P. M. McNamara, H. M. Subhash, and M. J. Leahy, “In vivo full-field en face correlation mapping optical coherence tomography,” J Biomed Opt, vol. 18, no. 12, p. 1, Dec. 2013. [CrossRef]
- W. J. Brown, S. Kim, and A. Wax, “Noise characterization of supercontinuum sources for low-coherence interferometry applications,” Journal of the Optical Society of America A, vol. 31, no. 12, p. 2703, Dec. 2014. [CrossRef]
- D. Angmo, M. Nongpiur, R. Sharma, T. Sidhu, R. Sihota, and T. Dada, “Clinical utility of anterior segment swept-source optical coherence tomography in glaucoma,” Oman J Ophthalmol, vol. 9, no. 1, p. 3, 2016. [CrossRef]
- V. J. Srinivasan et al., “Ultrahigh-Speed Optical Coherence Tomography for Three-Dimensional and En Face Imaging of the Retina and Optic Nerve Head,” Investigative Opthalmology & Visual Science, vol. 49, no. 11, p. 5103, Nov. 2008. [CrossRef]
- S. del Río-Sancho, C. Gallay, S. Ventéjou, and S. Christen-Zaech, “In vivo evaluation of skin of children with LC-OCT : An objective assessment,” Journal of the European Academy of Dermatology and Venereology, vol. 37, no. 9, pp. 1897–1905, Sep. 2023. [CrossRef]
- J. Hu et al., “Dynamic single gold nanoparticle visualization by clinical intracoronary optical coherence tomography,” J Biophotonics, vol. 10, no. 5, pp. 674–682, May 2017. [CrossRef]
- R. John, S. G. Adie, E. J. Chaney, M. Marjanovic, K. V. Tangella, and S. A. Boppart, “Three-dimensional Optical Coherence Tomography for Optical Biopsy of Lymph Nodes and Assessment of Metastatic Disease,” Ann Surg Oncol, vol. 20, no. 11, pp. 3685–3693, Oct. 2013. [CrossRef]
- J. Wang, Y. Xu, and S. A. Boppart, “Review of optical coherence tomography in oncology,” J Biomed Opt, vol. 22, no. 12, p. 1, Dec. 2017. [CrossRef]
- A. Jabbar, R. Khalid, H. Cabrera, N. Mahmood, and M. Q. Mehmood, “Revolutionizing endoscopy: non-invasive high-resolution imaging with time-domain optical coherence tomography,” in Unconventional Optical Imaging IV, M. P. Georges, N. Verrier, and I. Georgakoudi, Eds., SPIE, Jun. 2024, p. 77. [CrossRef]
- K. B. E. Holm et al., “Optical coherence tomography for presurgical delineation of basal cell carcinomas on the face—A comparison with histopathology,” J Cutan Pathol, vol. 50, no. 5, pp. 441–449, May 2023. [CrossRef]
- K. Schuetzenberger et al., “Comparison of optical coherence tomography and high frequency ultrasound imaging in mice for the assessment of skin morphology and intradermal volumes,” Sci Rep, vol. 9, no. 1, p. 13643, Sep. 2019. [CrossRef]
- H. Demirci and DanielW. Steen, “Limitations in imaging common conjunctival and corneal pathologies with Fourier-domain optical coherence tomography,” Middle East Afr J Ophthalmol, vol. 21, no. 3, p. 220, 2014. [CrossRef]
- J. A. Linehan et al., “Feasibility of optical coherence tomography imaging to characterize renal neoplasms: limitations in resolution and depth of penetration,” BJU Int, vol. 108, no. 11, pp. 1820–1824, Dec. 2011. [CrossRef]
- H.-W. Wang and Y. Chen, “Clinical applications of optical coherence tomography in urology,” Intravital, vol. 3, no. 1, p. e28770, Jan. 2014. [CrossRef]
- T.-H. Tsai, C. L. Leggett, and A. J. Trindade, “Optical coherence tomography in gastroenterology: a review and future outlook,” J Biomed Opt, vol. 22, no. 12, p. 1, Dec. 2017. [CrossRef]
- Q. Zhu et al., “Novel image features of optical coherence tomography for pathological classification of lung cancer: Results from a prospective clinical trial,” Front Oncol, vol. 12, Oct. 2022. [CrossRef]
- J. G. SUN, S. G. ADIE, E. J. CHANEY, and S. A. BOPPART, “SEGMENTATION AND CORRELATION OF OPTICAL COHERENCE TOMOGRAPHY AND X-RAY IMAGES FOR BREAST CANCER DIAGNOSTICS,” J Innov Opt Health Sci, vol. 06, no. 02, p. 1350015, Apr. 2013. [CrossRef]
- N. Gladkova et al., “Cross-polarization optical coherence tomography for early bladder-cancer detection: statistical study,” J Biophotonics, vol. 4, no. 7–8, pp. 519–532, Aug. 2011. [CrossRef]
- T. Schlegl et al., “Fully Automated Detection and Quantification of Macular Fluid in OCT Using Deep Learning,” Ophthalmology, vol. 125, no. 4, pp. 549–558, Apr. 2018. [CrossRef]
- E. Yeu, J. P. Berdahl, P. K. Gupta, and M. Patterson, “Sensitivity and specificity of SS-OCT for detecting macular pathologies vs SD-OCT,” J Cataract Refract Surg, vol. 50, no. 5, pp. 481–485, May 2024. [CrossRef]
- Y. Qin, S. Ye, L. Liu, and M. Wu, “Impact of lens opacity and axial length on concomitant screening of maculopathy by swept-source optical coherence tomography-based optical biometer,” Ann Transl Med, vol. 10, no. 15, pp. 815–815, Aug. 2022. [CrossRef]
- F. Scarinci, L. M. Jampol, R. A. Linsenmeier, and A. A. Fawzi, “Association of Diabetic Macular Nonperfusion With Outer Retinal Disruption on Optical Coherence Tomography,” JAMA Ophthalmol, vol. 133, no. 9, p. 1036, Sep. 2015. [CrossRef]
- M. Ulrich et al., “Dynamic Optical Coherence Tomography in Dermatology,” Dermatology, vol. 232, no. 3, pp. 298–311, 2016. [CrossRef]
- J. J. Vélez González et al., “Dynamic optical coherence tomography of chronic venous ulcers,” Journal of the European Academy of Dermatology and Venereology, vol. 38, no. 1, pp. 223–231, Jan. 2024. [CrossRef]
- A.H. Kashani et al., “Optical coherence tomography angiography: A comprehensive review of current methods and clinical applications,” Prog Retin Eye Res, vol. 60, pp. 66–100, Sep. 2017. [CrossRef]
- L. Yang et al., “Research progress on the application of optical coherence tomography in the field of oncology,” Front Oncol, vol. 12, Jul. 2022. [CrossRef]
- C. Başkan and A. Kılıcarslan, “How Can We Diagnose Ocular Surface Squamous Neoplasia With Optical Coherence Tomography?,” Cureus, Mar. 2023. [CrossRef]
- R. J. Aboumourad, A. Galor, and C. L. Karp, “Case Series: High-resolution Optical Coherence Tomography as an Optical Biopsy in Ocular Surface Squamous Neoplasia,” Optometry and Vision Science, vol. 98, no. 5, pp. 450–455, May 2021. [CrossRef]
- F.A. South, E. J. Chaney, M. Marjanovic, S. G. Adie, and S. A. Boppart, “Differentiation of ex vivo human breast tissue using polarization-sensitive optical coherence tomography,” Biomed Opt Express, vol. 5, no. 10, p. 3417, Oct. 2014. [CrossRef]
- J. Wang et al., “Complementary use of polarization-sensitive and standard OCT metrics for enhanced intraoperative differentiation of breast cancer,” Biomed Opt Express, vol. 9, no. 12, p. 6519, Dec. 2018. [CrossRef]
- E. V. Gubarkova et al., “Diagnostic Accuracy of Cross-Polarization OCT and OCT-Elastography for Differentiation of Breast Cancer Subtypes: Comparative Study,” Diagnostics, vol. 10, no. 12, p. 994, Nov. 2020. [CrossRef]
- L. P. Hariri, M. Mino-Kenudson, M. Lanuti, A. J. Miller, E. J. Mark, and M. J. Suter, “Diagnosing Lung Carcinomas with Optical Coherence Tomography,” Ann Am Thorac Soc, vol. 12, no. 2, pp. 193–201, Feb. 2015. [CrossRef]
- L. van Manen et al., “The clinical usefulness of optical coherence tomography during cancer interventions,” J Cancer Res Clin Oncol, vol. 144, no. 10, pp. 1967–1990, Oct. 2018. [CrossRef]
- J. Gallwas et al., “Validation of an ex vivo human cervical tissue model for optical imaging studies,” Lasers Surg Med, vol. 44, no. 3, pp. 245–248, Mar. 2012. [CrossRef]
- C. Ren et al., “Multi-center clinical study using optical coherence tomography for evaluation of cervical lesions in-vivo,” Sci Rep, vol. 11, no. 1, p. 7507, Apr. 2021. [CrossRef]
- J. Gallwas et al., “Detection of cervical intraepithelial neoplasia by using optical coherence tomography in combination with microscopy,” J Biomed Opt, vol. 22, no. 1, p. 016013, Jan. 2017. [CrossRef]
- T. S. M. Law et al., “Endometrial Vascularization Characterized by Optical Coherence Tomography and Immunohistochemistry in Women Undergoing In Vitro Fertilization-Embryo Transfer Treatment,” Medicina (B Aires), vol. 55, no. 4, p. 81, Mar. 2019. [CrossRef]
- A.A. Plekhanov et al., “Quantitative Assessment of Polarization and Elastic Properties of Endometrial Tissue for Precancer/Cancer Diagnostics Using Multimodal Optical Coherence Tomography,” Diagnostics, vol. 14, no. 19, p. 2131, Sep. 2024. [CrossRef]
- O. Assayag et al., “Imaging of non-tumorous and tumorous human brain tissues with full-field optical coherence tomography,” Neuroimage Clin, vol. 2, pp. 549–557, 2013. [CrossRef]
- B.G. Muller et al., “Customized Tool for the Validation of Optical Coherence Tomography in Differentiation of Prostate Cancer,” Technol Cancer Res Treat, vol. 16, no. 1, pp. 57–65, Feb. 2017. [CrossRef]
- J. E. Freund et al., “Optical Coherence Tomography in Urologic Oncology: a Comprehensive Review,” SN Compr Clin Med, vol. 1, no. 2, pp. 67–84, Feb. 2019. [CrossRef]
- S. Takae, K. Tsukada, Y. Sato, N. Okamoto, T. Kawahara, and N. Suzuki, “Accuracy and safety verification of ovarian reserve assessment technique for ovarian tissue transplantation using optical coherence tomography in mice ovary,” Sci Rep, vol. 7, no. 1, p. 43550, Mar. 2017. [CrossRef]
- I.T. A. Peters et al., “Noninvasive Detection of Metastases and Follicle Density in Ovarian Tissue Using Full-Field Optical Coherence Tomography,” Clinical Cancer Research, vol. 22, no. 22, pp. 5506–5513, Nov. 2016. [CrossRef]
- D. Schwartz, T. W. Sawyer, N. Thurston, J. Barton, and G. Ditzler, “Ovarian cancer detection using optical coherence tomography and convolutional neural networks,” Neural Comput Appl, vol. 34, no. 11, pp. 8977–8987, Jun. 2022. [CrossRef]
- S. P. Sunny et al., “Intra-operative point-of-procedure delineation of oral cancer margins using optical coherence tomography,” Oral Oncol, vol. 92, pp. 12–19, May 2019. [CrossRef]
- S. Roy et al., “SOX2 and OCT4 mediate radiation and drug resistance in pancreatic tumor organoids,” Cell Death Discov, vol. 10, no. 1, p. 106, Mar. 2024. [CrossRef]
- M. K. E. Perwein, J. Welzel, N. De Carvalho, G. Pellacani, and S. Schuh, “Dynamic Optical Coherence Tomography: A Non-Invasive Imaging Tool for the Distinction of Nevi and Melanomas,” Cancers (Basel), vol. 15, no. 1, p. 20, Dec. 2022. [CrossRef]
- S. Cappilli et al., “Line-Field Confocal Optical Coherence Tomography: A New Skin Imaging Technique Reproducing a ‘Virtual Biopsy’ with Evolving Clinical Applications in Dermatology,” Diagnostics, vol. 14, no. 16, p. 1821, Aug. 2024. [CrossRef]
- V. Yarovaya, K. Sioufi, and C. L. Shields, “Parafoveolar retinoblastoma regression with foveal preservation following intra-arterial chemotherapy documented on hand-held optical coherence tomography in a newborn,” Int J Retina Vitreous, vol. 3, no. 1, p. 43, Dec. 2017. [CrossRef]
- A.M. Zysk et al., “Intraoperative Assessment of Final Margins with a Handheld Optical Imaging Probe During Breast-Conserving Surgery May Reduce the Reoperation Rate: Results of a Multicenter Study,” Ann Surg Oncol, vol. 22, no. 10, pp. 3356–3362, Oct. 2015. [CrossRef]
- T..-T. P. Nguyen et al., “Advantages of Widefield Optical Coherence Tomography in the Diagnosis of Retinopathy of Prematurity,” Front Pediatr, vol. 9, Jan. 2022. [CrossRef]
- E. A. T. Say, S. U. Shah, S. Ferenczy, and C. L. Shields, “Optical Coherence Tomography of Retinal and Choroidal Tumors,” J Ophthalmol, vol. 2011, pp. 1–12, 2011. [CrossRef]
- A. Karl et al., “Optical coherence tomography for bladder cancer - ready as a surrogate for optical biopsy? - results of a prospective mono-centre study,” Eur J Med Res, vol. 15, no. 3, p. 131, 2010. [CrossRef]
- C. Zhou et al., “Photothermal optical coherence tomography in ex vivo human breast tissues using gold nanoshells,” Opt Lett, vol. 35, no. 5, p. 700, Mar. 2010. [CrossRef]
- V. P. Nguyen et al., “Chain-like gold nanoparticle clusters for multimodal photoacoustic microscopy and optical coherence tomography enhanced molecular imaging,” Nat Commun, vol. 12, no. 1, p. 34, Jan. 2021. [CrossRef]
- M. Y. Kirillin et al., “Laser-ablated silicon nanoparticles: optical properties and perspectives in optical coherence tomography,” Laser Phys, vol. 25, no. 7, p. 075604, Jul. 2015. [CrossRef]
- P. Si et al., “Gold Nanoprisms as Optical Coherence Tomography Contrast Agents in the Second Near-Infrared Window for Enhanced Angiography in Live Animals,” ACS Nano, vol. 12, no. 12, pp. 11986–11994, Dec. 2018. [CrossRef]
- J.M. Tucker-Schwartz, K. R. Beavers, W. W. Sit, A. T. Shah, C. L. Duvall, and M. C. Skala, “In vivo imaging of nanoparticle delivery and tumor microvasculature with multimodal optical coherence tomography,” Biomed Opt Express, vol. 5, no. 6, p. 1731, Jun. 2014. [CrossRef]
- R. Marin et al., “Plasmonic Copper Sulfide Nanoparticles Enable Dark Contrast in Optical Coherence Tomography,” Adv Healthc Mater, vol. 9, no. 5, Mar. 2020. [CrossRef]
- P. Tang et al., “Plasmonic Nanoprobe of (Gold Triangular Nanoprism Core)/(Polyaniline Shell) for Real-Time Three-Dimensional pH Imaging of Anterior Chamber,” Anal Chem, vol. 89, no. 18, pp. 9758–9766, Sep. 2017. [CrossRef]
- J. Zhang, J. Liu, L. Wang, Z. Li, and Z. Yuan, “Retroreflective-type Janus microspheres as a novel contrast agent for enhanced optical coherence tomography,” J Biophotonics, vol. 10, no. 6–7, pp. 878–886, Jun. 2017. [CrossRef]
- O. Liba, E. D. SoRelle, D. Sen, and A. de la Zerda, “Contrast-enhanced optical coherence tomography with picomolar sensitivity for functional in vivo imaging,” Sci Rep, vol. 6, no. 1, p. 23337, Mar. 2016. [CrossRef]
- M. Lapierre-Landry, A. Y. Gordon, J. S. Penn, and M. C. Skala, “In vivo photothermal optical coherence tomography of endogenous and exogenous contrast agents in the eye,” Sci Rep, vol. 7, no. 1, p. 9228, Aug. 2017. [CrossRef]
- J. Hu et al., “Magnetic Nanoplatelets for High Contrast Cardiovascular Imaging by Magnetically Modulated Optical Coherence Tomography,” ChemPhotoChem, vol. 3, no. 7, pp. 529–539, Jul. 2019. [CrossRef]
- Q. Xu et al., “Monitoring the topical delivery of ultrasmall gold nanoparticles using optical coherence tomography,” Skin Research and Technology, vol. 26, no. 2, pp. 263–268, Mar. 2020. [CrossRef]
- I. Mondal, S. Raj, P. Roy, and R. Poddar, “Silver nanoparticles (AgNPs) as a contrast agent for imaging of animal tissue using swept-source optical coherence tomography (SSOCT),” Laser Phys, vol. 28, no. 1, p. 015601, Jan. 2018. [CrossRef]
- S. V. Zabotnov et al., “Structural and optical properties of nanoparticles formed by laser ablation of porous silicon in liquids: Perspectives in biophotonics,” Quantum Elec (Woodbury), vol. 50, no. 1, pp. 69–75, Jan. 2020. [CrossRef]
- A. Ariza de Schellenberger, W. C. Poller, V. Stangl, U. Landmesser, and E. Schellenberger, “Macrophage uptake switches on OCT contrast of superparamagnetic nanoparticles for imaging of atherosclerotic plaques,” Int J Nanomedicine, vol. Volume 13, pp. 7905–7913, Nov. 2018. [CrossRef]
- A.L. Oldenburg, R. L. Blackmon, and J. M. Sierchio, “Magnetic and Plasmonic Contrast Agents in Optical Coherence Tomography,” IEEE Journal of Selected Topics in Quantum Electronics, vol. 22, no. 4, pp. 133–145, Jul. 2016. [CrossRef]
- C. Zhou et al., “Ex vivo imaging of human thyroid pathology using integrated optical coherence tomography and optical coherence microscopy,” J Biomed Opt, vol. 15, no. 01, p. 1, Jan. 2010. [CrossRef]
- R. John, E. J. Chaney, and S. A. Boppart, “Dynamics of Magnetic Nanoparticle-Based Contrast Agents in Tissues Tracked Using Magnetomotive Optical Coherence Tomography,” IEEE Journal of Selected Topics in Quantum Electronics, vol. 16, no. 3, pp. 691–697, 2010. [CrossRef]
- J. Hu et al., “Quantum Dots Emitting in the Third Biological Window as Bimodal Contrast Agents for Cardiovascular Imaging,” Adv Funct Mater, vol. 27, no. 41, Nov. 2017. [CrossRef]
- A. Papagiannaros, J. Upponi, W. Hartner, D. Mongayt, T. Levchenko, and V. Torchilin, “Quantum dot loaded immunomicelles for tumor imaging,” BMC Med Imaging, vol. 10, no. 1, p. 22, Dec. 2010. [CrossRef]
- A. Gul et al., “Biofabrication of silver nanoparticles using Spirulina platensis : In vitro anti-coagulant, thrombolytic and catalytic dye degradation activity,” Microsc Res Tech, vol. 86, no. 7, pp. 823–833, Jul. 2023. [CrossRef]
- C. Sun et al., “PEG-Mediated Synthesis of Highly Dispersive Multifunctional Superparamagnetic Nanoparticles: Their Physicochemical Properties and Function In Vivo,” ACS Nano, vol. 4, no. 4, pp. 2402–2410, Apr. 2010. [CrossRef]
- Y. Xue et al., “Enhanced Physiological Stability and Long-Term Toxicity/Biodegradation In Vitro/In Vivo of Monodispersed Glycerolphosphate-Functionalized Bioactive Glass Nanoparticles,” Particle & Particle Systems Characterization, vol. 36, no. 4, Apr. 2019. [CrossRef]
- Y. Li et al., “Combined surface functionalization of MSC membrane and PDA inhibits neurotoxicity induced by Fe3O4 in mice based on apoptosis and autophagy through the ASK1/JNK signaling pathway,” Aging, vol. 15, no. 14, pp. 6933–6949, Jul. 2023. [CrossRef]
- Q. Xu et al., “Monitoring the topical delivery of ultrasmall gold nanoparticles using optical coherence tomography,” Skin Research and Technology, vol. 26, no. 2, pp. 263–268, Mar. 2020. [CrossRef]
- A. Sastry et al., “Microscope-Integrated OCT-Guided Volumetric Measurements of Subretinal Blebs Created by a Suprachoroidal Approach,” Transl Vis Sci Technol, vol. 10, no. 7, p. 24, Jun. 2021. [CrossRef]
- J. Zhao et al., “In vivo monitoring of microneedle-based transdermal drug delivery of insulin,” J Innov Opt Health Sci, vol. 11, no. 05, Sep. 2018. [CrossRef]
- A. Kavalaraki, E. Spyratou, M. A. Kouri, and E. P. Efstathopoulos, “Gold Nanoparticles as Contrast Agents in Ophthalmic Imaging,” Optics, vol. 4, no. 1, pp. 74–99, Jan. 2023. [CrossRef]
- V. P. Nguyen, J. Hu, J. Zhe, S. Ramasamy, U. Ahmed, and Y. M. Paulus, “Advanced nanomaterials for imaging of eye diseases,” ADMET DMPK, Feb. 2024. [CrossRef]
- C. Yang et al., “Nanoparticles in ocular applications and their potential toxicity,” Front Mol Biosci, vol. 9, Jul. 2022. [CrossRef]
- A. Narawane et al., “Optical clearing with tartrazine enables deep transscleral imaging with optical coherence tomography,” J Biomed Opt, vol. 29, no. 12, Dec. 2024. [CrossRef]
- M. Moothanchery, R. Z. Seeni, C. Xu, and M. Pramanik, “Photoacoustic microscopy imaging for microneedle drug delivery,” in Photons Plus Ultrasound: Imaging and Sensing 2018, A. A. Oraevsky and L. V. Wang, Eds., SPIE, Feb. 2018, p. 199. [CrossRef]
- J. Qi, J. Zhang, N. Liu, L. Zhao, and B. Xu, “Prognostic Implications of Molecular Subtypes in Primary Small Cell Lung Cancer and Their Correlation With Cancer Immunity,” Front Oncol, vol. 12, Mar. 2022. [CrossRef]
- B.S. Harrington et al., “UGDH promotes tumor-initiating cells and a fibroinflammatory tumor microenvironment in ovarian cancer,” Journal of Experimental & Clinical Cancer Research, vol. 42, no. 1, p. 270, Oct. 2023. [CrossRef]
- P. Suman, S. Mishra, and H. Chander, “High formin binding protein 17 (FBP17) expression indicates poor differentiation and invasiveness of ductal carcinomas,” Sci Rep, vol. 10, no. 1, p. 11543, Jul. 2020. [CrossRef]
- C. Bernardo, P. Eriksson, N. Marzouka, F. Liedberg, G. Sjödahl, and M. Höglund, “Molecular pathology of the luminal class of urothelial tumors,” J Pathol, vol. 249, no. 3, pp. 308–318, Nov. 2019. [CrossRef]
- J. I. Warrick et al., “FOXA1, GATA3 and PPARɣ Cooperate to Drive Luminal Subtype in Bladder Cancer: A Molecular Analysis of Established Human Cell Lines,” Sci Rep, vol. 6, no. 1, p. 38531, Dec. 2016. [CrossRef]
- L. Geistlinger et al., “Multi-omic analysis of subtype evolution and heterogeneity in high-grade serous ovarian carcinoma,” Feb. 19, 2019. [CrossRef]
- P. Milani, F. Scotti, and F. Bergamini, “Comment on: Diagnostic algorithm utilising multimodal imaging including optical coherence tomography angiography for the detection of myopic choroidal neovascularization,” Eye, vol. 35, no. 1, pp. 349–350, Jan. 2021. [CrossRef]
- M. Usman, K. Iqbal, M. H. Ali, and K. Nafees, “Features and Diagnostic Accuracy of Optical Coherence Tomography Angiography in Neovascular Age-related Macular Degeneration,” Cureus, Dec. 2019. [CrossRef]
- X. Hao et al., “Correlation between retinal structure and brain multimodal magnetic resonance imaging in patients with Alzheimer’s disease,” Front Aging Neurosci, vol. 15, Feb. 2023. [CrossRef]
- N. Aslam et al., “Multiple Sclerosis Diagnosis Using Machine Learning and Deep Learning: Challenges and Opportunities,” Sensors, vol. 22, no. 20, p. 7856, Oct. 2022. [CrossRef]
- P. Koulen, J. Schliesser, G. Gallimore, N. Kunjukunju, N. Sabates, and F. Sabates, “Clinical application of optical coherence tomography in combination with functional diagnostics: advantages and limitations for diagnosis and assessment of therapy outcome in central serous chorioretinopathy,” Clinical Ophthalmology, p. 2337, Nov. 2014. [CrossRef]
- W. Jerjes, H. Stevenson, D. Ramsay, and Z. Hamdoon, “Enhancing Oral Cancer Detection: A Systematic Review of the Diagnostic Accuracy and Future Integration of Optical Coherence Tomography with Artificial Intelligence,” J Clin Med, vol. 13, no. 19, p. 5822, Sep. 2024. [CrossRef]
- N. Seth et al., “18 F-FDG PET and PET/CT as a diagnostic method for Ewing sarcoma: A systematic review and meta-analysis,” Pediatr Blood Cancer, vol. 69, no. 3, Mar. 2022. [CrossRef]
- R.A. Leitgeb and B. Baumann, “Multimodal Optical Medical Imaging Concepts Based on Optical Coherence Tomography,” Front Phys, vol. 6, Oct. 2018. [CrossRef]
- G. Perini, E. Rodriguez-Vieitez, A. Kadir, A. Sala, I. Savitcheva, and A. Nordberg, “Clinical impact of 18F-FDG-PET among memory clinic patients with uncertain diagnosis,” Eur J Nucl Med Mol Imaging, vol. 48, no. 2, pp. 612–622, Feb. 2021. [CrossRef]
- N. Cerdá-Fuertes et al., “Optical coherence tomography versus other biomarkers: Associations with physical and cognitive disability in multiple sclerosis,” Multiple Sclerosis Journal, vol. 29, no. 13, pp. 1540–1550, Nov. 2023. [CrossRef]
- E. Caverzasi et al., “Imaging correlates of visual function in multiple sclerosis,” PLoS One, vol. 15, no. 8, p. e0235615, Aug. 2020. [CrossRef]
- G.M. Richter et al., “Regression Analysis of Optical Coherence Tomography Disc Variables for Glaucoma Diagnosis,” J Glaucoma, vol. 25, no. 8, pp. 634–642, Aug. 2016. [CrossRef]
- S. Mrejen, S. Khan, R. Gallego-Pinazo, L. M. Jampol, and L. A. Yannuzzi, “Acute Zonal Occult Outer Retinopathy,” JAMA Ophthalmol, vol. 132, no. 9, p. 1089, Sep. 2014. [CrossRef]
- T. Wasilewski, W. Kamysz, and J. Gębicki, “AI-Assisted Detection of Biomarkers by Sensors and Biosensors for Early Diagnosis and Monitoring,” Biosensors (Basel), vol. 14, no. 7, p. 356, Jul. 2024. [CrossRef]
- G. Yammouri and A. Ait Lahcen, “AI-Reinforced Wearable Sensors and Intelligent Point-of-Care Tests,” J Pers Med, vol. 14, no. 11, p. 1088, Nov. 2024. [CrossRef]
- A. Sahu et al., “Evaluation of a Combined Reflectance Confocal Microscopy–Optical Coherence Tomography Device for Detection and Depth Assessment of Basal Cell Carcinoma,” JAMA Dermatol, vol. 154, no. 10, p. 1175, Oct. 2018. [CrossRef]
- H. Niioka et al., “Automated diagnosis of optical coherence tomography imaging on plaque vulnerability and its relation to clinical outcomes in coronary artery disease,” Sci Rep, vol. 12, no. 1, p. 14067, Aug. 2022. [CrossRef]
- D.H. Kim, S. W. Kim, and S. H. Hwang, “Efficacy of optical coherence tomography in the diagnosing of oral cancerous lesion: systematic review and meta-analysis,” Head Neck, vol. 45, no. 2, pp. 473–481, Feb. 2023. [CrossRef]
- M. A. Sorkhabi, I. O. Potapenko, T. Ilginis, M. Alberti, and J. Cabrerizo, “Assessment of Anterior Uveitis Through Anterior-Segment Optical Coherence Tomography and Artificial Intelligence-Based Image Analyses,” Transl Vis Sci Technol, vol. 11, no. 4, p. 7, Apr. 2022. [CrossRef]
- A. Kh. M. Khalifa et al., “Impact of Optical Coherence Tomography Imaging on Decision-Making During Percutaneous Coronary Intervention in Patients Presented With Acute Coronary Syndromes,” Circulation Journal, vol. 85, no. 10, p. CJ-20-0942, Sep. 2021. [CrossRef]
- G.J. Ughi et al., “A neurovascular high-frequency optical coherence tomography system enables in situ cerebrovascular volumetric microscopy,” Nat Commun, vol. 11, no. 1, p. 3851, Jul. 2020. [CrossRef]
- V. Panzarella et al., “Application of Targeted Optical Coherence Tomography in Oral Cancer: A Cross-Sectional Preliminary Study,” Diagnostics, vol. 14, no. 19, p. 2247, Oct. 2024. [CrossRef]
Figure 1.
Imaging of morpheaform basal cell carcinoma (BCC) on the forehead above the eyebrow (Case 2), using dynamic and structural OCT alongside dermoscopy and histopathology. (A1) D-OCT of adjacent normal skin shows evenly distributed linear, dotted, and branching vessels. (A2) D-OCT of the central tumor region reveals increased vessel density and diameter, with serpiginous and branching patterns. (B) Dermoscopy image showing the clinical appearance of the lesion. (C1) Structural OCT of normal skin displays an intact dermoepidermal junction (DEJ) and hair follicles with shadowing. (C2, C3) OCT images near tumor borders (proximal and distal) show disrupted layering and partial DEJ loss, indicating tumor extension. (D1, D2) Histopathology at distal (D3) and proximal (P3) scan sites reveals no visible tumor, in contrast to OCT-detected abnormalities. (D3) Histology from the tumor center confirms BCC with infiltrative basaloid strands [31].
Figure 1.
Imaging of morpheaform basal cell carcinoma (BCC) on the forehead above the eyebrow (Case 2), using dynamic and structural OCT alongside dermoscopy and histopathology. (A1) D-OCT of adjacent normal skin shows evenly distributed linear, dotted, and branching vessels. (A2) D-OCT of the central tumor region reveals increased vessel density and diameter, with serpiginous and branching patterns. (B) Dermoscopy image showing the clinical appearance of the lesion. (C1) Structural OCT of normal skin displays an intact dermoepidermal junction (DEJ) and hair follicles with shadowing. (C2, C3) OCT images near tumor borders (proximal and distal) show disrupted layering and partial DEJ loss, indicating tumor extension. (D1, D2) Histopathology at distal (D3) and proximal (P3) scan sites reveals no visible tumor, in contrast to OCT-detected abnormalities. (D3) Histology from the tumor center confirms BCC with infiltrative basaloid strands [31].
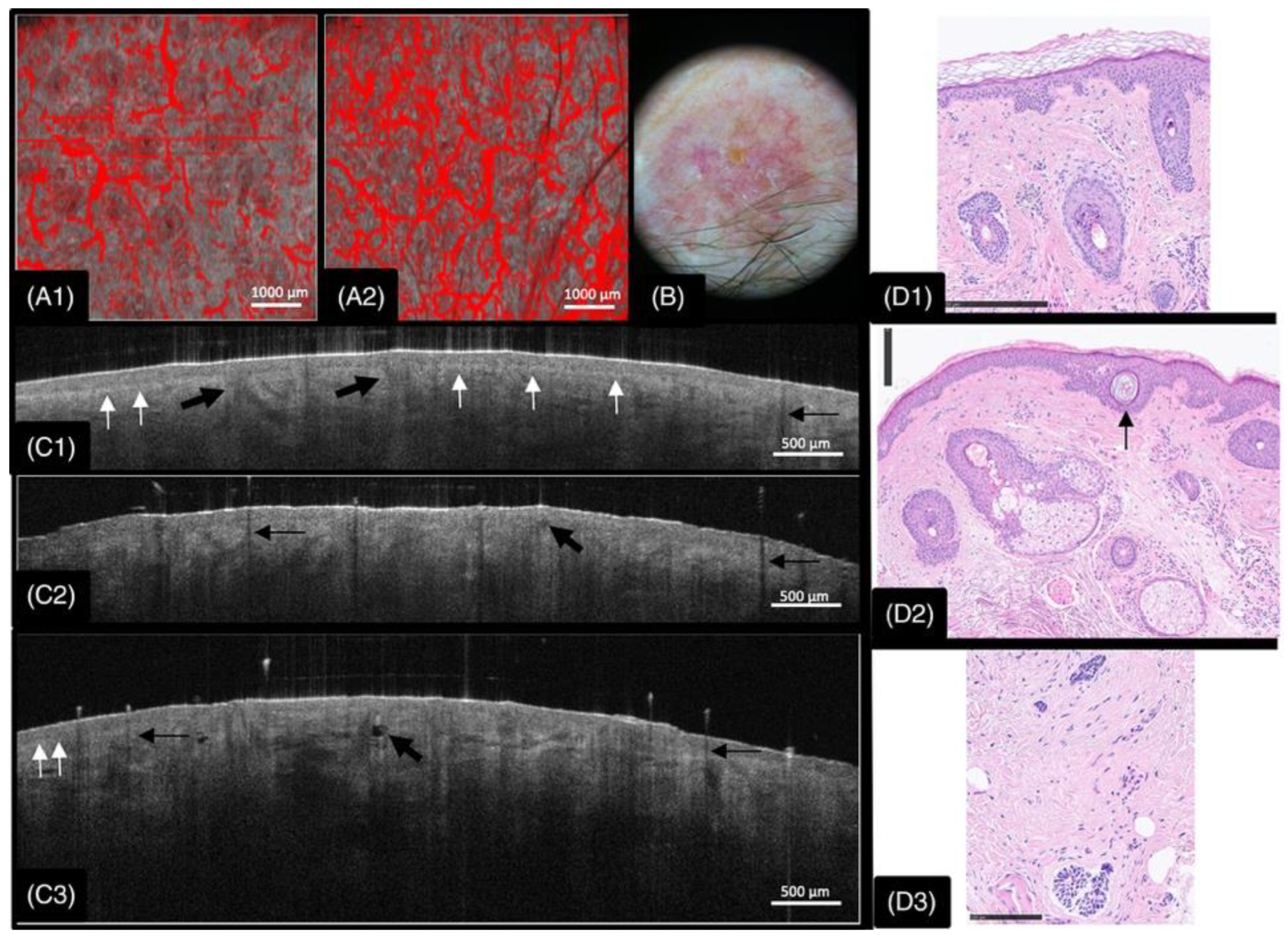
Figure 2.
Exemplary cross-sectional images of murine skin were obtained by (b) OCT and (c) HFUS and corresponding (a) histology (H&E staining). Enlarged cross-sections, as indicated by the orange rectangles, are depicted in (d,e). Dashed orange lines in images (a,d,e) indicate the skin layers corresponding to (a) epidermis, (b) papillary dermis, (c) reticular dermis, (d) subcutis, (e) sebaceous glands and hair follicles, and (f) muscle. Skin layers with letters labeled with an asterisk are not distinguishable [32].
Figure 2.
Exemplary cross-sectional images of murine skin were obtained by (b) OCT and (c) HFUS and corresponding (a) histology (H&E staining). Enlarged cross-sections, as indicated by the orange rectangles, are depicted in (d,e). Dashed orange lines in images (a,d,e) indicate the skin layers corresponding to (a) epidermis, (b) papillary dermis, (c) reticular dermis, (d) subcutis, (e) sebaceous glands and hair follicles, and (f) muscle. Skin layers with letters labeled with an asterisk are not distinguishable [32].
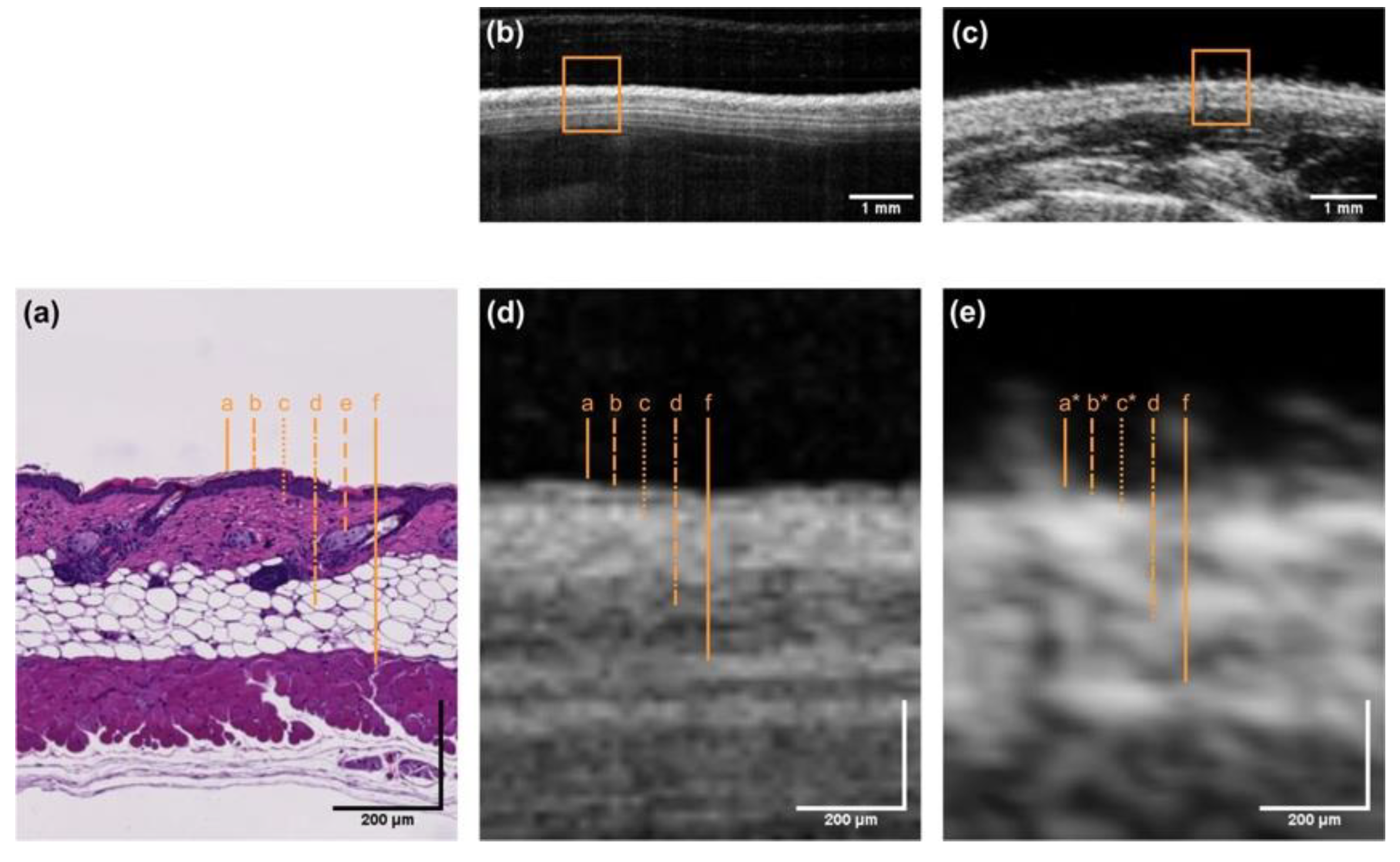

Table 1.
Comparison of Nanoparticle Types for OCT Imaging (Summarizing properties, advantages, and challenges).
Table 1.
Comparison of Nanoparticle Types for OCT Imaging (Summarizing properties, advantages, and challenges).
| Nanoparticle Type | Optical Property | Application in OCT | Advantages | Challenges |
| AuNPs | SPR | Contrast Enhancement | High Biocompatibility | Cost, Aggregation Issues |
| AgNPs | Strong Scattering | Image Enhancement | High Stability | Toxicity Concerns |
| SiNPs | High Reflective Index | Deep Tissue Imaging | Biodegradable | Limited Studies |
| QDs | Fluorescence | Multiplex Imaging | Tunable Emission | Potential Cytotoxicity |
Table 2.
Advantages and Challenges of Nanoparticles in OCT-Based Personalized Medicine.
| Advantage | Description | Example Nanoparticles |
| High Contrast Imaging | Improves visualization of microstructures | AuNPs, AgNPs and QDs |
| Theranostic Capabilities | Enables simultaneous diagnosis and treatment | Magnetic, Hybrid Nanoparticles |
| Real-Time Monitoring | Facilitates intraoperative tracking | Plasmonic Nanoparticles |
| Biodegradability | Minimizes long-term toxicity | PLGA, Chitosan |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



