
Submitted:
14 May 2025
Posted:
15 May 2025
You are already at the latest version
Abstract
Obstructive Sleep Apnea is a highly prevalent respiratory disease linked with increased morbidity and mortality, reduced quality of life and increased economic costs if not treated. Oral Appliances are an emerging treatment option for Obstructive Sleep Apnea. This review concludes that many oral appliances marketed as “custom” include modifications and prefabricated items, and therefore do not meet the definition of “custom” oral appliances. This misclassification could hinder accurate characterization and appropriate utilization of oral appliances that do fulfill the definition of custom. To better inform clinical utilization of custom oral appliances, we propose further refining the custom oral appliance classification into semi-custom and precision-custom.
Keywords:
Personalized Medicine
; Obstructive Sleep Apnea
; Oral appliance therapy
; sleep apnea
; respiratory medicine
; sleep disordered breathing
; dental sleep medicine
Introduction
Obstructive Sleep Apnea (“OSA”) is a highly prevalent chronic respiratory disease affecting an estimated 1 billion people globally and 74 million in the United States [1,2]. Unmanaged OSA is linked to increased morbidity and mortality, reduced quality of life, and significant economic costs[3].
Oral appliances (OA), also known as mandibular advancement devices (“MAD”), mandibular repositioning devices (“MRD”), or mandibular advancement splints (“MAS”), are an emerging treatment option for OSA, largely driven by the low compliance rates associated with continuous positive airway pressure (“CPAP”) therapy[4,5]. Clinical practice guidelines (“CPGs”) recommend custom, titratable OAs for patients who refuse or discontinue CPAP therapy or prefer an alternative[6]. Recently, another CPG recommended custom, titratable OAs as frontline therapy for mild and moderate OSA and for severe OSA patients who fail or refuse CPAP trials[7].
This review and follow on analysis evaluates if the definition of 'custom' from the AASM CPG effectively describes, classifies, and differentiates OAs for the treatment of patients with OSA. A more exact classification could facilitate a better understanding of the merits and limitations of this therapy to better inform clinical utilization. The AASM CPG for Oral Appliance Therapy (“OAT”) defines custom OAs as devices, "fabricated using digital or physical impressions and models of an individual patient’s oral structures," and, "Not primarily prefabricated items that are trimmed, bent, relined, or otherwise modified." Prefabricated items are those manufactured without a specific patient in mind. "Records" refer to digital or physical dental casts that are used to create a custom OA5.
Background
OAs have three components. The first is an overlay of the maxillary dental arch. The second is an overlay of the mandibular dental arch. The third is the titration mechanism.
Dental arch overlays are fabricated from the records of each individual patient’s oral structures. Records can be either digital scans or physical molds that are used to create dental casts. Proper fit between the overlays and the dental arches is crucial for mitigating the risk of dental side effects. Repositioning the mandible introduces orthodontic forces that can cause side effects. Overlay fit is essential for absorbing, distributing and mitigating the potentially injurious orthodontic forces. Prior research identifies a dose dependent relationship between the degree of mandibular protrusion and the prevalence of dental side effects[8]. Overlays that poorly fit the dentition, use soft liner materials, or use prefabricated items such as ball clasps to enhance retention may also compromise fit and increase risks of dental side effects.
The third component of an OA is the titration mechanism component. The titration mechanism component articulates and stabilizes the mandibular overlay relative to the maxillary overlay to beneficially reposition the mandible. Prior research reports a dose dependent association between stepwise mandibular repositioning and reductions in airway collapse events[9]. The target therapeutic mandibular location is determined by the healthcare provider. A bite registration is made at the target therapeutic mandibular location and is included in record of oral structures provided to the OA maker.
Overlays can be prefabricated or custom-made. Prefabricated overlays, often called "Boil and Bite" or "Do-it-Yourself" OA’s, are non-custom. Similarly, titration mechanisms can be prefabricated or custom. We identified three categories of titration mechanisms: prefabricated displacement screws, prefabricated interchangeable connectors, and custom interlocking overlays.
There are three categories of titration mechanism components: 1. prefabricated displacement screws, 2. prefabricated interchangeable connectors, and 3. custom, interlocking overlays.
Prefabricated Displacement Screws
These mechanisms are prefabricated items. Displacement screws require overlay modifications to embed the prefabricated fixtures that anchor the displacement screws to the overlays. Examples include anterior pull-OAs and interlocking dorsal-OAs with prefabricated screws, which can be seen in Figure 1 and Figure 2.
Prefabricated Interchangeable Connectors
Connector mechanisms are prefabricated items of various materials and sizes. The maxillary and mandibular overlays must be modified to embed the prefabricated fixtures that anchor the connector items to the overlays. Examples include push-OAs and pull-OAs with prefabricated connectors or Herbst arms. Figure 3, Figure 4 and Figure 5 provide examples of OA’s with prefabricated interchangeable connector and prefabricated fixture items.
Custom Interlocking Overlays
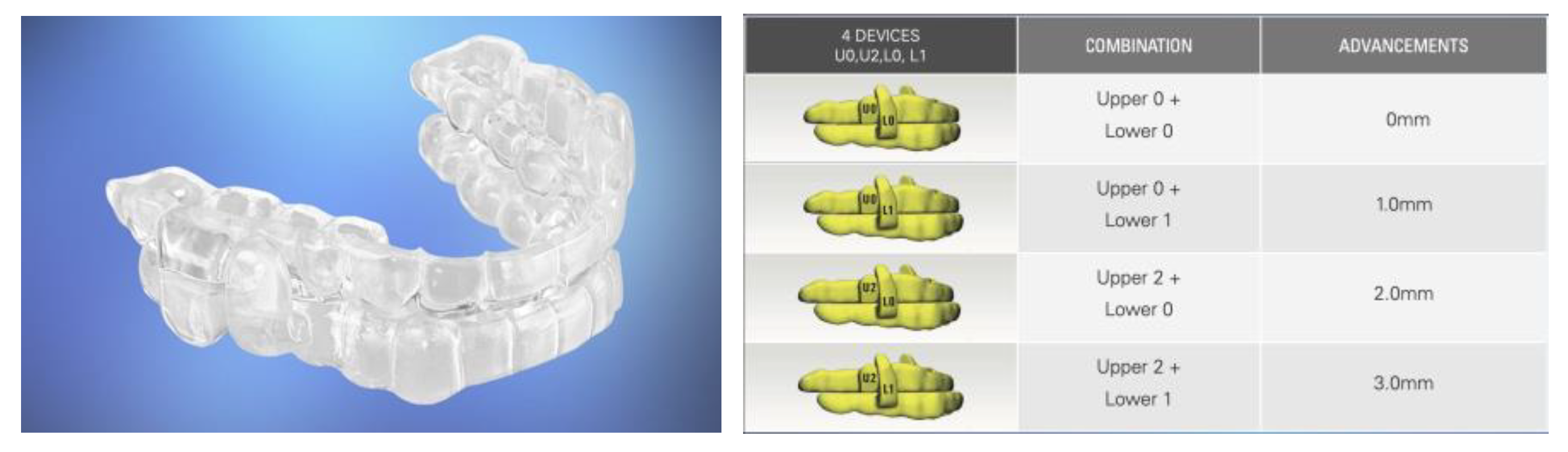
Each overlay has a monolithically embedded interlocking titration post that is directly designed based on the oral structures for each individual patient using computer aided design and forward engineering technologies. There are no prefabricated items. No modifications are required. Each interlocking overlay is purely custom and has a specific mandibular advancement setting defined by the healthcare provider. The combination of different maxillary and mandibular overlays included within a treatment kit enables a range of specific protrusive or retrusive mandibular positions. Figure 5 provides an example of a Dual Post OA with custom interchangeable overlays.
Figure 5.
Dual Post-OA with Interchangeable Overlay Components.
We hypothesize that most OAs labeled as custom do not meet the definition of custom. Most OA’s use prefabricated items and are modified to embed fixtures.
We propose two classifications: Semi-custom and Precision-Custom OAs.
Semi-Custom Oral Appliances
Semi-custom OA’s are made from the records of oral structures for each individual patient. Semi-custom OA’s are either modified, or include prefabricated items, or both.
Precision-Custom Oral Appliances
Precision-custom OA’s are directly and fully designed and manufactured based on the records of an individual patient’s oral records. They are not modified. They do not use prefabricated items. See Table 1 for a summary of our proposed OA classifications.
Further we postulate that semi-custom OA’s, with prefabricated items and modifications, are inherently more complex, which may describe reports of inconsistent performance.
Review
To test our hypotheses and challenge our proposed OA classifications, we evaluated OAT devices from two recent review articles[10,11], including 49 source articles referencing 74 OAT devices. Of these, 51 were described as titratable and custom, with 41 providing enough detail for our evaluation. We assessed each of these devices based on the AASM CPG definition criteria: made from individual patient records and not modified or primarily prefabricated. Figure 6 describes our review approach.
The 2015 AASM CPG’s definition for custom OAT can be distilled into two criteria. These two criteria are as follows:
- Is the OA made from records of an individual patient’s oral structures?
- Is the OA modified (trimmed, bent, relined) or primarily a prefabricated item?
The forty-one OAT devices from our review strategy were evaluated according to these two criteria.
Results
Criterion 1: Made from records of an individual patient’s oral structures?
All 41 OA’s included in our analysis were made from individual patient records, based on descriptions contained in the source articles for each OA.
Criterion 2: Is the OA modified or primarily a prefabricated item?
However 32 of the 41, 78% of the OA’s included in our analysis used prefabricated items. The prefabricated items used were titration mechanisms, anchor fixtures for titration mechanism, or prefabricate retention items like ball clasps. Each included overlay modifications to embed prefabricated fixtures that anchor prefabricated titration mechanisms.
Only nine of forty-one OA’s fully met the two criteria of the AASM CPG definition of a custom OA. These nine did not use prefabricated items. They were not modified.
See Table 2 for an evaluation of each OA according to the definitional criteria.
Discussion
Our review and follow-on analysis confirms our hypothesis that most OAs marketed as custom do not meet the AASM CPG’s criteria for custom OA’s. Although 100% of OA’s in this analysis were made from oral records for an individual patient, 78% included at least one prefabricated component, or were modified, or both.
That 32 of the 41 OA’s use prefabricated titration mechanism items is potentially significant. It reveals that for these 32 OA’s, the titration mechanism, the component that most directly establishes and stabilizes the therapeutic mandibular reposition, is not made based on the oral records for each individual patient. It is prefabricated. It is generic.
Moreover, many of these prefabricated items are repurposed for the treatment of OSA. They were originally designed for other therapies. For example, displacement screws were designed for orthopedic procedures. Herbst arms were designed to correct Class II malocclusions in the field of orthodontics. These prefabricated items were not designed for the treatment of OSA, let alone customized treatment for each individual patient.
Prefabricated titration mechanisms, not made based on individual patient records, limit customization, increase complexity and decrease consistency. Complex product designs, in general, with more parts, modifications and steps, are associated with relatively lower quality and performance than less complex designs[46]. Occam’s razor, the principle of parsimony, applies: all things being equal, a simple product design will be better than a relatively more complex design.
This applies to OA’s. Precision-custom OAs, with fewer parts, fewer steps, and no modifications are inherently less complex and relatively smaller tolerance stacks. Smaller tolerance stacks are associated with less variability and more consistent, predictable performance. Inconsistent performance is often cited as a key barrier to increased OA utilization[47].
Personalized medicine, also known as precision medicine, optimizes therapies by matching treatments with individual patient characteristics[48]. Precision medicine is associated with improved treatment efficacy[49], reduced adverse events[50], enhanced patient engagement[51] and cost-effectiveness[52].
Precision-custom OA’s are a step closer to the promise of personalized medicine than semi-custom OA’s. Unlike semi-custom OA’s, precision custom OA’s are exclusively made from records of each individual patient’s oral records without the modifications and deviations necessary to accommodate prefabricated items. Modifications and prefabricated items make an OA more generic and less personalized.
Implications for Efficacy?
Studies report a dose dependent relationship between mandibular advancement and therapeutic efficacy[9]. These investigations associate 2-millimeter stepwise increases in mandibular repositioning with clinically meaningful reductions in airway collapse events. Semi-custom OAs with larger tolerance stacks may result in clinically meaningful variances in mandibular positions. Studies suggest precision-custom OAs may offer different outcomes than semi-custom oral appliances[10,37,39].
Signs of Different Outcomes Between Semi-Custom and Precision Custom OA’s?
It takes time to interrogate new technologies. For example, the 53 referenced by the 2015 AASM CPG are, on average, over 18 years old[6]. However, are there any recent records, any signs, that associate precision-custom OA’s with different results?
Signs of Different Efficacy
A prospective study prescribed precision-custom OA’s for 288 patients with a 50%, 31% and 19% mix of mild, moderate and severe OSA. The study reported 85% success treating these patients to an AHI < 10, and 73% treating patients to an AHI < 5[45]. A second prospective study prescribed precision-custom OA’s to treat 48 patients with a mix of mild, moderate and severe OSA. The study reported 88% success treating patients to an AHI < 10 and a 50% improvement over baseline[44]. Although not comparative randomized controlled studies, these results represent rates of efficacy that are directionally different than what has been previously reported for semi-custom OA’s[11].
Signs of Different Patient Preferences
One randomized, controlled cross over trial compared patient preference between precision-custom OA’s and semi-custom OA’s[53]. Of the ten patients who completed the study, eight preferred the precision-custom OA. These patients cited comfort, ease of use, and durability as reasons for their preference. The two patients who preferred the semi-custom OA, citing ease of use in combination with their CPAP.
Signs of Different Symptom Alleviation
A prospective, comparative, randomized controlled trial reported 91% success treating snoring with a precision custom OA, in comparison with 58% for combined airway and positional therapy[54]. In a different study, a single arm investigation that included a precision-custom OA for treatment, 85% of patients stated that they achieved their treatment goals, and 97% reported a reduction in snoring[43].
Signs of Different Side Effects
A single-arm, prospective, longitudinal study involving the treatment of OSA patients with a precision-custom OA’s reported no clinically or statistically significant changes in tooth position, overbite, or overjet after a two-year follow-up period[55]. A second, single-arm, comparative, longitudinal study evaluated the side effects associated with treating OSA with precision-custom OA’s. The study also reported no clinically meaningful changes in orthodontic conditions after a two-year follow-up period[56]. A third study using precision-custom OA’s to treat OSA patients more broadly reported on side effects. This study reported no serious adverse events and no adverse events that resulted in the discontinuation of therapy43. Again, these are not randomized controlled trials, but they do indicate results that are different from what is commonly reported for OAT (cite).
There are several limitations to this study. One is that it is based on primary source records that are inconsistent in their controls, their definitions, their mix of OSA severity in their patient populations, and other variables that are relevant to our research topic. A way to remedy this would be to commission a randomized controlled trial comparing precision-custom with semi-custom style OA’s.
Another limitation is dependence on concepts such as design elegance, complexity factors, and tolerance stacking to describe the reported inconsistencies in efficacy. A remedy would be a prospective investigation that directly measures and calculates these values.
Conclusions
Most OA’s that are marketed as custom do not meet the definitional conditions of custom. Most OA’s considered custom include primarily prefabricated items or modifications, or both.
For these OA’s, the primarily prefabricated item is the titration mechanism. The titration mechanism is the critical components of the OA. The titration mechanism dictates the therapeutic relationship of the mandible relative to the maxillary arch, which is the key mechanism of action associated with preventing airway collapse.
Further, product design elegance, complexity factors and tolerance stacks describe how an OA that uses prefabricated items and requires modifications could be associated with less inconsistent performance than an OA that does not.
This analysis reveals that several OA’s do satisfy the definitional conditions for a custom OA. These OA’s are entirely made from records of the oral structures for an individual patient. They do not include prefabricated items. Nor are they modified. As a result, these OA’s represent relatively less complex designs with considerably smaller tolerance stacks.
Several studies provide signs that there are differences in performance between semi-custom and precision-custom OA’s. Although more intensive investigation is warranted, these studies offer initial signs that precision-custom devices may perform differently than semi-custom devices when it comes to efficacy, patient preference, side effects mitigation and symptom alleviation.
In closing, we propose refining the custom OA classification into semi-custom and precision-custom to better inform clinical use.
References
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.-L.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb DJ, Punjabi NM. Diagnosis and Management of Obstructive Sleep Apnea: A Review. JAMA. 2020 Apr 14;323(14):1389-1400. [CrossRef] [PubMed]
- Anandam, A.; Patil, M.; Akinnusi, M.; Jaoude, P.; El-Solh, A.A. Cardiovascular mortality in obstructive sleep apnoea treated with continuous positive airway pressure or oral appliance: An observational study. Respirology 2013, 18, 1184–1190. [Google Scholar] [CrossRef] [PubMed]
- Pépin, J.L.; Woehrle, H.; Liu, D.; Shao, S.; Armitstead, J.P.; Cistulli, P.A.; Benjafield, A.V.; Malhotra, A. Adherence to Positive Airway Therapy After Switching From CPAP to ASV: A Big Data Analysis. J. Clin. Sleep Med. 2018, 15, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.R.; Bakker, J.P.; Stitt, C.J.; Aloia, M.S.; Nouraie, S.M. Age and Sex Disparities in Adherence to CPAP. Chest 2021, 159, 382–389. [Google Scholar] [CrossRef]
- Ramar, K.; Dort, L.C.; Katz, S.G.; Lettieri, C.J.; Harrod, C.G.; Thomas, S.M.; Chervin, R.D. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015. J. Clin. Sleep Med. 2015, 15, 773–827. [Google Scholar] [CrossRef]
- VA/DOD CLINICAL PRACTICE GUIDELINE FOR THE MANAGEMENT OF CHRONIC INSOMNIA DISORDER AND OBSTRUCTIVE SLEEP APNEA 2025. Available online: https://www.healthquality.va.gov/guidelines/CD/insomnia/I-OSA-CPG_2025-Guildeline_final_20250422.pdf (accessed on day month year).
- de Ruiter, M.H.T.; Aarab, G.; de Vries, N.; Lobbezoo, F.; de Lange, J. A Stepwise Titration Protocol for Oral Appliance Therapy in Positional Obstructive Sleep Apnea Patients: Proof of Concept. Sleep Breath. Schlaf Atm. 2020, 24, 1229–1236. [Google Scholar] [CrossRef]
- Kato J, Isono S, Tanaka A, Watanabe T, Araki D, Tanzawa H, Nishino T. Dose-dependent effects of mandibular advancement on pharyngeal mechanics and nocturnal oxygenation in patients with sleep-disordered breathing. Chest. 2000 Apr;117(4):1065-72. [CrossRef] [PubMed]
- Liptak, L.A.; Sall, E.; Kim, S.; Mosca, E.; Charkhandeh, S.; Remmers, J.E. Different Oral Appliance Designs Demonstrate Different Rates of Efficacy for the Treatment of Obstructive Sleep Apnea: A Review Article. Bioengineering 2025, 12, 210. [Google Scholar] [CrossRef]
- Chen Y, Zhang J, Gao X, Almeida FR. Efficacy and adherence of different mandibular advancement devices designs in treatment of obstructive sleep apnea: A systematic review and meta-analysis. Am J Orthod Dentofacial Orthop. 2025 Mar 7:S0889-5406(25)00019-8. [CrossRef] [PubMed]
- Bloch, K.E.; Iseli, A.; Zhang, J.N.; Xie, X.; Kaplan, V.; Stoeckli, P.W.; Russi, E.W. A randomized, controlled crossover trial of two oral appliances for sleep apnea treatment. Am. J. Respir. Crit. Care Med. 2000, 162, 246–251. [Google Scholar] [CrossRef]
- Pépin JL, Raymond N, Lacaze O, Aisenberg N, Forcioli J, Bonte E, Bourdin A, Launois S, Tamisier R, Molinari N. Heat-moulded versus custom-made mandibular advancement devices for obstructive sleep apnoea: a randomised non-inferiority trial. Thorax. 2019 Jul;74(7):667-674. [CrossRef] [PubMed]
- Randerath, W.J.; Heise, M.; Hinz, R.; Ruehle, K.H. An individually adjustable oral appliance vs continuous positive airway pressure in mild-to-moderate obstructive sleep apnea syndrome. Chest. 2002, 122, 569–575. [Google Scholar] [CrossRef]
- Ghazal, A.; Sorichter, S.; Jonas, I.; Rose, E.C. A randomized prospective long-term study of two oral appliances for sleep apnoea treatment. J. Sleep Res. 2009, 18, 321–328. [Google Scholar] [CrossRef]
- Gagnadoux, F.; Fleury, B.; Vielle, B.; Pételle, B.; Meslier, N.; N'Guyen, X.L.; Trzepizur, W.; Racineux, J.L. Titrated mandibular advancement versus positive airway pressure for sleep apnoea. Eur. Respir. J. 2009, 34, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Yanamoto S, Harata S, Miyoshi T, Nakamura N, Sakamoto Y, Murata M, Soutome S, Umeda M. Semi-fixed versus fixed oral appliance therapy for obstructive sleep apnea: A randomized crossover pilot study. J Dent Sci. 2021 Jan;16(1):404-409. PMCID: PMC7770364. [CrossRef] [PubMed]
- Zhou J, Liu YH. A randomised titrated crossover study comparing two oral appliances in the treatment for mild to moderate obstructive sleep apnoea/hypopnoea syndrome. J Oral Rehabil. 2012 Dec;39(12):914-22. [CrossRef] [PubMed]
- Isacsson G, Fodor C, Sturebrand M. Obstructive sleep apnea treated with custom-made bibloc and monobloc oral appliances: a retrospective comparative study. Sleep Breath. 2017 Mar;21(1):93-100. PMCID: PMC5343082. [CrossRef] [PubMed]
- Vecchierini, M.F.; Attali, V.; Collet, J.M.; d'Ortho, M.P.; El Chater, P.; Kerbrat, J.B.; Leger, D.; Monaca, C.; Monteyrol, P.J.; Morin, L.; et al. A custom-made mandibular repositioning device for obstructive sleep apnoea-hypopnoea syndrome: The ORCADES study. Sleep Med. 2016, 19, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Tegelberg, Å.; Nohlert, E.; Bornefalk-Hermansson, A.; Fransson, A.; Isacsson, G. Respiratory outcomes after a 1-year treatment of obstructive sleep apnoea with bibloc versus monobloc oral appliances: A multicentre, randomized equivalence trial. Acta Odontol. Scand. 2020, 78, 401–408. [Google Scholar] [CrossRef]
- Kuna, S.T.; Giarraputo, P.C.; Stanton, D.C.; Levin, L.M.; Frantz, D. Evaluation of an oral mandibular advancement titration appliance. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2006, 101, 593–603. [Google Scholar] [CrossRef]
- Henke, K.G.; Frantz, D.E.; Kuna, S.T. An oral elastic mandibular advancement device for obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 2000, 161, 420–425. [Google Scholar] [CrossRef]
- Vanderveken, O.M.; Van Daele, M.; Verbraecken, J.; Braem, M.J.; Dieltjens, M. Comparative analysis of two custom-made mandibular advancement devices with varied designs for treating moderate to severe obstructive sleep apnea. Sleep Med. 2024, 117, 95–98. [Google Scholar] [CrossRef]
- Schneiderman, E.D.; Schramm, P.J.; Hui, J.; Wilson, P.D.; Marques, P.; German, Z.; McCann, A.L.; Newton, M.N. Randomized Trial of 2 Self-Titrated Oral Appliances for Airway Management. J. Dent. Res. 2020, 100, 155–162. [Google Scholar] [CrossRef]
- Pancer, J.; Al-Faifi, S.; Al-Faifi, M.; Hoffstein, V. Evaluation of variable mandibular advancement appliance for treatment of snoring and sleep apnea. Chest. 1999, 116, 1511–1518. [Google Scholar] [CrossRef]
- Van Haesendonck, G.; Dieltjens, M.; Hamans, E.; Braem, M.J.; Vanderveken, O.M. Treatment efficacy of a titratable oral appliance in obstructive sleep apnea patients: A prospective clinical trial. B-ENT. 2016, 12, 1–8. [Google Scholar]
- Remmers, J.; Charkhandeh, S.; Grosse, J.; Topor, Z.; Brant, R.; Santosham, P.; Bruehlmann, S. Remotely Controlled Mandibular Protrusion during Sleep Predicts Therapeutic Success with Oral Appliances in Patients with Obstructive Sleep Apnea. Sleep 2013, 36, 1517–1525. [Google Scholar] [CrossRef]
- Mehta, A.; Qian, J.; Petocz, P.; Darendeliler, M.A.; Cistulli, P.A. A Randomized, Controlled Study of a Mandibular Advancement Splint for Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med. 2001, 163, 1457–1461. [Google Scholar] [CrossRef] [PubMed]
- Abd-Ellah ME, Mohamed FS, Khamis MM, Abdel Wahab NH. Modified biblock versus monoblock mandibular advancement appliances for treatment of obstructive sleep apnea: A randomized controlled trial. J Prosthet Dent. 2024 Apr;131(4):633-642. [CrossRef] [PubMed]
- Isacsson G, Nohlert E, Fransson AMC, Bornefalk-Hermansson A, Wiman Eriksson E, Ortlieb E, Trepp L, Avdelius A, Sturebrand M, Fodor C, List T, Schumann M, Tegelberg Å. Use of bibloc and monobloc oral appliances in obstructive sleep apnoea: a multicentre, randomized, blinded, parallel-group equivalence trial. Eur J Orthod. 2019 Jan 23;41(1):80-88. PMCID: PMC6343726. [CrossRef] [PubMed]
- Bosschieter PFN, Uniken Venema JAM, Vonk PE, Ravesloot MJL, Hoekema A, Plooij JM, Lobbezoo F, de Vries N. Equal effect of a noncustom vs a custom mandibular advancement device in treatment of obstructive sleep apnea. J Clin Sleep Med. 2022 Sep 1;18(9):2155-2165. PMCID: PMC9435323. [CrossRef] [PubMed]
- Johal A, Haria P, Manek S, Joury E, Riha R. Ready-Made Versus Custom-Made Mandibular Repositioning Devices in Sleep Apnea: A Randomized Clinical Trial. J Clin Sleep Med. 2017 Feb 15;13(2):175-182. PMCID: PMC5263072. [CrossRef] [PubMed]
- Friedman M, Hamilton C, Samuelson CG, Kelley K, Pearson-Chauhan K, Taylor D, Taylor R, Maley A, Hirsch MA. Compliance and efficacy of titratable thermoplastic versus custom mandibular advancement devices. Otolaryngol Head Neck Surg. 2012 Aug;147(2):379-86. [CrossRef] [PubMed]
- Lettieri CJ, Paolino N, Eliasson AH, Shah AA, Holley AB. Comparison of adjustable and fixed oral appliances for the treatment of obstructive sleep apnea. J Clin Sleep Med. 2011 Oct 15;7(5):439-45. PMCID: PMC3190841. [CrossRef] [PubMed]
- Sari E, Menillo S. Comparison of titratable oral appliance and mandibular advancement splint in the treatment of patients with obstructive sleep apnea. ISRN Dent. 2011;2011:581692. PMCID: PMC3169918. [CrossRef] [PubMed]
- Stern, J.; Lee, K.; Kuhns, D.; Martinez-Kratz, J.F. Efficacy and Effectiveness of the ProSomnus® [IA] Sleep Device for the Treatment of Obstructive Sleep Apnea: EFFECTS Study. Cureus 2021, 13, e15391. [Google Scholar] [CrossRef] [PubMed]
- Silva R, Pires L, Belchior I, Moniri A, New generation oral appliances for treatment of obstructive sleep apnea. Sleep Med. 2024, 115 (Suppl. 1).
- Sall, E.; Smith, K.; Desai, A.; Carollo, J.A.; Murphy, M.T.; Kim, S.; Liptak, L.A. Evaluating the Clinical Performance of a Novel, Precision Oral Appliance Therapy Medical Device Made Wholly from a Medical Grade Class VI Material for the Treatment of Obstructive Sleep Apnea. Cureus 2023, 15, e50107. [Google Scholar] [CrossRef]
- Sall, E. 434 Precision Oral Appliance Therapy: The Prime-Time Treatment for OSA. Sleep 2021, 44 (Suppl. 2). [Google Scholar] [CrossRef]
- Remmers, J.E.; Topor, Z.L.; Grosse, J.; Vranjes, N.; Mosca, E.V.; Brant, R.; Bruehlmann, S.; Charkhandeh, S.; Jenabali, A. A Feedback-Controlled Mandibular Positioner Identifies Individuals with Sleep Apnea Who Will Respond to Oral Appliance Therapy. J. Clin. Sleep Med. 2017, 13, 871–880. [Google Scholar] [CrossRef]
- Murphy, M.; Munro, K. Dose Management in DSM; Analysis of Efficacy, Starting Position, Advancement and side effects in consecutive Patient Series Treated with Precision Platform. J. Dent. Sleep Med. 2021, 8, No.3. [Google Scholar]
- Mosca, E.V.; Bruehlmann, S.; Zouboules, S.M.; Chiew, A.E.; Westersund, C.; Hambrook, D.A.; Jahromi, S.A.Z.; Grosse, J.; Topor, Z.L.; Charkhandeh, S.; et al. In-Home Mandibular Repositioning during Sleep Using MATRx plus Predicts Outcome and Efficacious Positioning for Oral Appliance Treatment of Obstructive Sleep Apnea. J. Clin. Sleep Med. 2022, 18, 911–919. [Google Scholar] [CrossRef]
- Kang, R.S.; Knowles, S.; Dekow, M. The Success of Oral Appliance Therapy Based on Symptom-Driven Titration. Mil. Med. 2022, 189, 620–626. [Google Scholar] [CrossRef]
- Knowles, S.; Dekow, M.; Williamson, M.L. Oral Appliances for OSA Treatment: Meeting the Quadruple Aim. Mil. Med. 2021, 188, e718–e724. [Google Scholar] [CrossRef]
- https://doi.org/10.1016/j.cirpj.2019.02.001. [CrossRef]
- https://sleepreviewmag.com/sleep-treatments/therapy-devices/oral-appliances/barriers-sleep-physicians-oat/ (Accessed May 13, 2025).
- Pack, A. Developing a Personalized Approach to Obstructive Sleep Apnea. Sleep Med Clin. 2025 Mar;20(1):127-134. [CrossRef] [PubMed]
- Xu Z, Zhang SY, Huang M, Hu R, Li JL, Cen HJ, Wang ZP, Ou JS, Yin SL, Xu YQ, Wu ZK, Zhang X. Genotype-Guided Warfarin Dosing in Patients With Mechanical Valves: A Randomized Controlled Trial. Ann Thorac Surg. 2018 Dec;106(6):1774-1781. [CrossRef] [PubMed]
- Mancinelli L, Cronin M, Sadée W. Pharmacogenomics: the promise of personalized medicine. AAPS PharmSci. 2000;2(1):E4. PMCID: PMC2750999. [CrossRef] [PubMed]
- Su JH, Zhu YH, Ren TY, Guo L, Yang GY, Jiao LG, Wang JF. Distribution and Antimicrobial Resistance of SalmonellaIsolated from Pigs with Diarrhea in China. Microorganisms. 2018 Nov 26;6(4):117. PMCID: PMC6313467. [CrossRef] [PubMed]
- Yalameha B, Birjandi M, Nouryazdan N, Nasri H, Shahsavari G. Association between the FABP2 Ala54Thr and CRP+1059C/G polymorphisms and small dense LDL level in patients with atherosclerosis: a case-control study. Arch Physiol Biochem. 2023 Feb;129(1):246-252. [CrossRef] [PubMed]
- Ryser AS, Sabol J, Handel S, Walworth P, Dimalanta W, et al. (2024) Soldier Preference in Mandibular Advancement Devices in Patients Who Brux. J Dent Oral Epidemiol 4(2). d. [CrossRef]
- Ioerger P, Afshari A, Hentati F, Strober W, Kallogjeri D, Ju YE, Piccirillo JF. Mandibular Advancement vs Combined Airway and Positional Therapy for Snoring: A Randomized Clinical Trial. JAMA Otolaryngol Head Neck Surg. 2024 Jul 1;150(7):572-579. PMCID: PMC11117146. [CrossRef] [PubMed]
- Vranjes N, Santucci G, Schulze K, Kuhns D, Khai A. Assessment of potential tooth movement and bite changes with a hardacrylic sleep appliance: A 2-year clinical study. J Dent Sleep Med. 2019;6(2). https://www.aadsm.org/docs/jdsm.4.10.19.o2.
- Aziz R, Somaiah S, Kalha AS, Reddy G, Muddaiah S, Shetty B. Comparative assessment of changes in pharyngeal airway space in cases of obstructive sleep apnoea with a customized mandibular repositioning appliance - a clinical study. Sleep Sci. 2021 Jan-Mar;14(Spec 1):16-24. PMCID: PMC8663729. [CrossRef] [PubMed]
Figure 1.
Anterior Pull-OA with Prefabricated Displacement Screws.

Figure 2.
Interlocking Dorsal-OA with Prefabricated Screws.

Figure 3.
Push-OA with Prefabricated Connectors of Different Lengths.

Figure 4.
Pull-OA with Prefabricated Connectors of Different Lengths.

Figure 5.
Push-OA with Prefabricated Herbst Arms of Different Lengths.

Figure 6.
Review Approach.
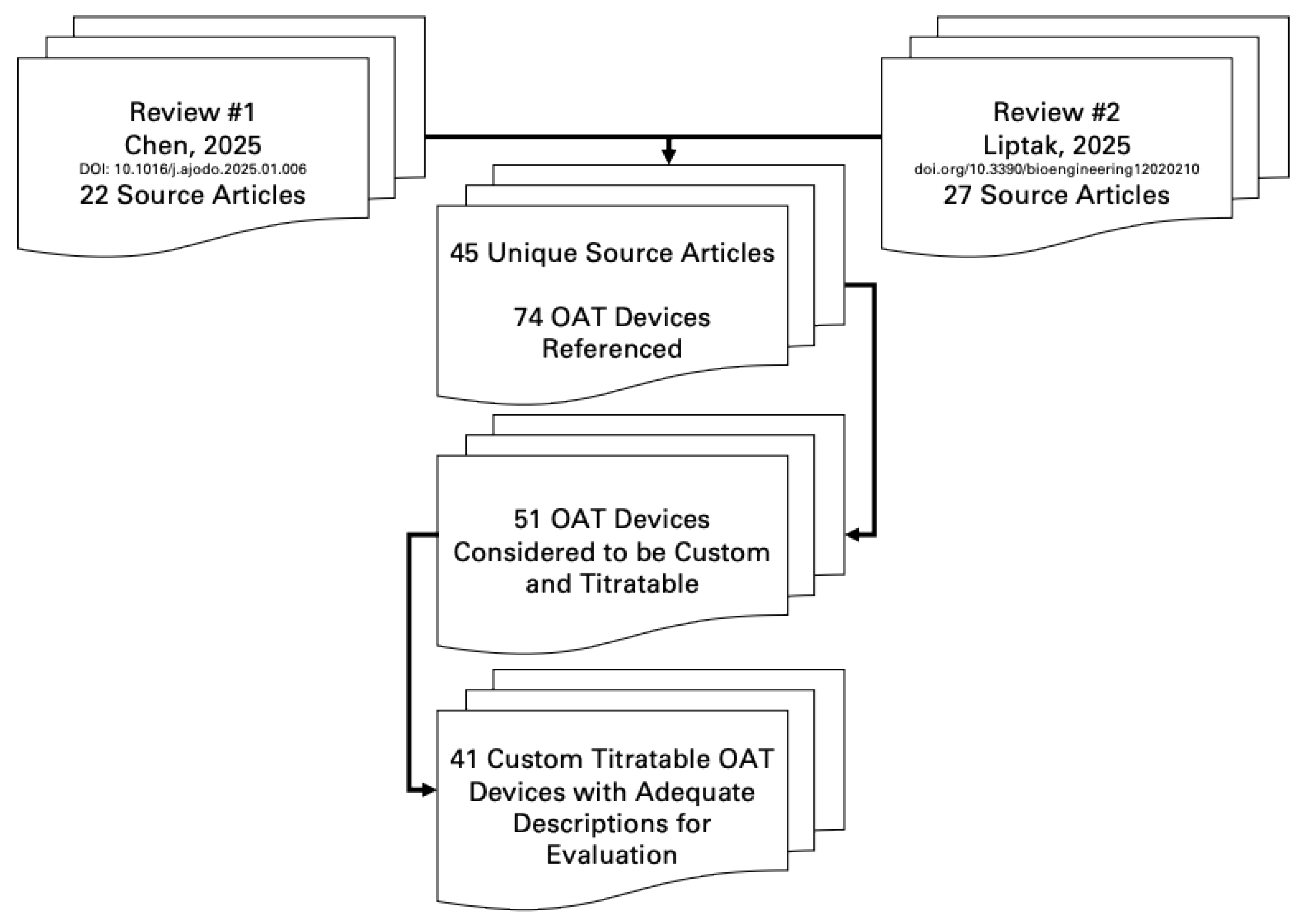

Table 1.
Proposed OA classifications.
| Custom OA Definition Criteria (Summarized) | |||
|---|---|---|---|
| Proposed Classifications | Made from Oral Records of an Individual Patient? | Modified (Trimmed, Bent, Relined)? | Includes Prefabricated Items? |
| Semi-Custom | Yes | Yes | |
| Precision-Custom | Yes | No | |
Table 2.
Evaluation of OA’s.
| Review Article | Author | Reference | Basic Description | 1. Made from Records of Oral Structures? | 2. Is the Device Modified or Primarily Prefabricated? |
|---|---|---|---|---|---|
| Chen 2025 | Bloch 2000 | [12] | Push | Yes | Yes |
| Chen 2025 | Pepin 2019 | [13] | Push | Yes | Yes |
| Chen 2025 | Pepin 2019 | [13] | Push | Yes | Yes |
| Liptak 2025 | Randerath, 2022 | [14] | Push | Yes | Yes |
| Liptak 2025 | Ghazal, 2008 | [15] | Push | Yes | Yes |
| Liptak 2025 | Gagnadoux, 2009 | [16] | Push | Yes | Yes |
| Chen 2025 | Yanamoto 2021 | [17] | Pull | Yes | Yes |
| Chen 2025 | Zhou 2012 | [18] | Pull | Yes | Yes |
| Chen 2025 | Isacsson 2017 | [19] | Pull | Yes | Yes |
| Liptak 2025 | Vecchierini, 2016 | [20] | Pull | Yes | Yes |
| Liptak 2025 | Vecchierini, 2016 | [14] | Pull | Yes | Yes |
| Liptak 2025 | Tegelberg, 2020 | [21] | Pull | Yes | Yes |
| Liptak 2025 | Kuna, 2005 | [22] | Pull | Yes | Yes |
| Liptak 2025 | Henke, 1999 | [23] | Pull | Yes | Yes |
| Liptak 2025 | Vanderveken, 2024 | [24] | Pull | Yes | Yes |
| Liptak 2025 | Schneiderman, 2020 | [25] | Pull | Yes | Yes |
| Liptak 2025 | Pancer, 1999 | [26] | Pull | Yes | Yes |
| Liptak 2025 | Ghazal, 2008 | [12] | Pull | Yes | Yes |
| Chen 2025 | Gagnadoux 2012 | [13] | Interlocking | Yes | Yes |
| Liptak 2025 | Vanderveken, 2024 | [18] | Interlocking | Yes | Yes |
| Liptak 2025 | Van Haesendonck, 2016 | [27] | Interlocking | Yes | Yes |
| Liptak 2025 | Schneiderman, 2020 | [19] | Interlocking | Yes | Yes |
| Liptak 2025 | Remmers, 2013 | [28] | Interlocking | Yes | Yes |
| Liptak 2025 | Mehta, 2001 | [29] | Interlocking | Yes | Yes |
| Liptak 2025 | de Ruiter, 2020 | [7] | Interlocking | Yes | Yes |
| Chen 2025 | Abd-Ellah 2022 | [30] | Bi Block | Yes | Yes |
| Chen 2025 | Isacsson 2019 | [31] | Bi Block | Yes | Yes |
| Chen 2025 | Bosschieter 2022 | [32] | Anterior | Yes | Yes |
| Chen 2025 | Johal 2015 | [33] | Anterior | Yes | Yes |
| Chen 2025 | Friedman 2012 | [34] | Anterior | Yes | Yes |
| Chen 2025 | Lettieri 2011 | [35] | Anterior | Yes | Yes |
| Chen 2025 | Sari 2011 | [36] | Anterior | Yes | Yes |
| Liptak 2025 | Stern, 2021 | [37] | Dual Post | Yes | No |
| Liptak 2025 | Silva, 2023 | [38] | Dual Post | Yes | No |
| Liptak 2025 | Sall, 2023 | [39] | Dual Post | Yes | No |
| Liptak 2025 | Sall, 2021 | [40] | Dual Post | Yes | No |
| Liptak 2025 | Remmers, 2017 | [41] | Dual Post | Yes | No |
| Liptak 2025 | Murphy, 2021 | [42] | Dual Post | Yes | No |
| Liptak 2025 | Mosca, 2022 | [43] | Dual Post | Yes | No |
| Liptak 2025 | Kang, 2024 | [44] | Dual Post | Yes | No |
| Liptak 2025 | Knowles, 2023 | [45] | Dual Post | Yes | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



