Submitted:
13 May 2025
Posted:
15 May 2025
You are already at the latest version
Abstract
Background
Cardiac arrest (CA) results in significant mortality worldwide, largely due to the hypoxic-ischaemic brain injury sustained. MicroRNAs (miRNAs/miR), non-coding RNAs that regulate gene expression, have shown diagnostic potential in stroke and other neurological diseases. This work presents the expression and predictive value of blood miRNAs for 6-month neurological outcomes post-CA.
Methods
A comprehensive literature search of PubMed and the Cochrane Library identified clinical studies reporting blood miRNA expression post-CA and its association with 6-month neurological outcomes. MicroRNA expression, patient characteristics, and receiver operator characteristic Area Under Curve (ROC-AUC) values were extracted. MicroRNA expression was examined against neurological outcomes using the Cerebral Performance Score Category (favourable: CPC 1–2; unfavourable: CPC 3–5).
Results
Ten clinical studies (n = 2,414 patients) met inclusion criteria. Eleven miRNAs were differentially expressed within 72 hours of a return of spontaneous circulation (ROSC). ROC-AUC values for blood miRNAs ranged from 0.62–0.89 at various time points. Notably, an up-regulated miR-124-3p at 6hrs post-ROSC could predict unfavourable neurological outcomes with high accuracy (AUC = 0.84), while miR-191-5p was the most accurate predictor of neurological outcomes when taken at 48hrs post-ROSC (AUC = 0.89). Odds ratios and Hazard ratios were collated to establish the clinical value of changes in miRNA expression levels at various time points. 5 studies provided odds ratios and 1 study provided a hazard ratio.
Discussion and Conclusion
miRNAs have distinct and prognostically useful expression changes post-CA and ROSC. MiR-124-3p and miR-191-5p can relatively accurately predict 6-month neurological recovery within 72 hours of ROSC. Although blood miRNAs demonstrate potential as early molecular biomarkers of ischaemic brain damage, further work is required to account for existing pathologies that may also impact circulating miRNA expression. This work additionally emphasises the need for large scale pragmatic trials to establish the role of miRNAs in guiding clinical decision making within this group of patients.
Keywords:
biomarker
; cardiac arrest
; neurological
; microRNA
; ischaemia
; outcome prediction
Introduction
Cardiac arrest (CA) refers to the sudden stop of cardiac output and resulting loss of circulating blood [1]. Annually, 30,000 cardiopulmonary resuscitation (CPR) attempts are made by United Kingdom (UK) Ambulance Service clinicians to restore cardiac function and obtain a return of spontaneous circulation (ROSC) [2]. Despite efforts by clinical teams and recent advancements in resuscitative and emergency medicine, mortality in these patients is still high, with approximately 60% of patients not surviving CA and a further 80% dying of a neurological failure within 12 months [3]. In the recently published and widely distributed PARAMEDIC-3 trial [4], only 2.7% of patients who survived to hospital discharge after an out-of-hospital cardiac arrest (OHCA) had a favourable neurological outcome, representing a clear unmet need to predict and identify unfavourable neurological outcomes in this group of patients.
Hypoxic-ischaemic brain injury (HIBI) and brain death remains the predominant cause of mortality following ROSC [5]. Withdrawal of life-sustaining interventions due to a suspected poor neurological outcome is the most common cause of death following an initially successful resuscitation [6]. Brain injury in resuscitated patients presents in neurocognitive dysfunction, myoclonus, or seizure activity [7]. The brain has a significant metabolic demand, receiving 30% of total cardiac output. This demand has been quantified to approximately 50ml/100g/min of blood [8] and 3.5cc/100g/min of oxygen [9], and irreversible brain damage occurs following 30 minutes of cerebral blood flow levels lower than ~10ml/100g/min [10]. Although global, and not focal ischaemia, the process follows a cascade similar to ischaemic stroke in that brain tissue is metabolically deprived due to under-perfusion. A detailed explanation of ischaemic pathophysiology is outside of the scope for this review but has been covered extensively elsewhere [11,12,13].
The development of blood-based biomarkers could provide an objective measure of HIBI during the period of hypo-perfusion with independence from the effects of anaesthetic or sedative drugs that often confound neurological examinations in the intensive care setting [14]. An ideal biomarker for this context should be easily accessible, have a relatively long half-life, exhibit brain-hypoxia/ischaemia specificity, and demonstrate high sensitivity and specificity for prognostication across various populations and demographics for example age and gender.
MicroRNAs are a family of small non-coding RNA molecules involved in the post-transcriptional regulation of gene expression. These 18-24 nucleotides long, highly conserved RNAs act by base pairing to complementary sequences of target mRNA 3’ untranslated regions (UTR) and result in the inhibition of translation or the degradation of the mRNA [15]. Significant interest has evolved in microRNAs in science and society, with the discovery of miRNAs and their physiological role winning the 2024 Nobel Prize [16]. Further from their role in healthy physiology, a large body of research has investigated the role of miRNAs within cardiovascular [17,18], neurological [19,20], oncological [21,22,23], and immunological diseases [24,25] as potential diagnostic and prognostic biomarkers. MicroRNAs are advantageous in the context of a biomarker as they can be assessed by minimally invasive procedures e.g. venipuncture, quantified by low-cost methods such as quantitative PCR (qPCR), and are relatively stable within the blood and bodily fluids [26,27,28,29].
Less than 1% of patients have no neurological symptoms after a CA [30], and therefore, a molecular biomarker to predict the extent of neurological outcomes following CA would have great clinical utility. This review will investigate the post-CA expression of microRNAs in blood and collate the latest evidence for the prognostic ability of microRNAs when obtained at ROSC for a poor neurological outcome at 6 months, utilising receiver operating characteristic area under the curve (ROC-AUC) values, odds ratios (OR), and hazard ratios (HR).
Methods and Aims
This work involved a comprehensive search of the Cochrane Database and PubMed to extract and identify relevant literature. Literature identified was screened against the inclusion and exclusion criteria of this review, described in Table 1. A reference list of included studies is found in Appendix A. Due to the various methods of quantification, miRNA expression was recorded as either relatively up-regulated or relatively down-regulated, accounting for variation in how microRNA quantification is presented in publications, for example, fold change, objective measures e.g. copies/ml or relative change to an admission value or expression value relative to a spike-in miRNA. This was to standardise the reporting process and to allow meaningful comparisons.
A ‘twice reported’ approach was used to declare significance of reported microRNA findings and to reduce the likelihood of false positive reporting, this matched results for when microRNAs were obtained after ROSC, their expression, the specific microRNA species (ie treating miR-9-5p and miR-9-3p as distinct entities), and the neurological outcome at 6 months. The number of times a result was replicated was then visualised. Statistical work and data visualisation was carried out within Apple Numbers and R studio 4.4.2.
The primary outcome measure for this work was neurological status at 6 months from ROSC. This neurological status was defined using the Cerebral Performance Score Category (CPC), which is a 5-point functional scale. A CPC score of one represents good cerebral performance, 2 represents moderate cerebral disability, 3 represents severe cerebral disability, 4 represents coma or vegetative state, and 5 represents brain death [31].

Table 1.
Table of inclusion and exclusion criteria for studies within this review.
| Inclusion | Exclusion |
| Statistically significant results p <0.05 or FDR adjusted p value of <0.05 | Paediatric cardiac arrest. |
| Published in a peer reviewed journal since 1993*. | Bioinformatic/database driven research or animal models without original patients. |
| Written informed consent from the patient, the patient’s next of kin, or Doctor. | Post-mortem samples/ pathology analysis. |
| Appropriate quantitative methods for microRNA quantification e.g. microarray, polymerase chain reaction, or next generation sequencing. | Case studies. |
| Studies that obtained blood and quantified microRNA expression from patients who had either an in-hospital or out of hospital cardiac arrest within a defined period, either stated directly or deducible from the paper methodology. | Patients in which gene therapy/ gene editing treatments have been administered. |
*MicroRNAs were discovered in 1993 [32] by Lee, Feinbaum, and Ambros and therefore studies published prior to this could not be relevant.
Main Body
Included Studies and Patient Demographics
From 173 potentially eligible titles, 10 clinical studies involving 2414 patients were included. The clinical characteristics of patients involved in the 10 studies are presented in Table 2 and Table 3 and a summary of the methods used in each study is described in Appendix Table A1. The methodology for this study and extraction of relevant data from included studies is presented in a flow chat (Figure 1).
From 2424 patients, 1155 (47.84%) had unfavourable neurological outcomes (CPC 3-5). Of these, 66.15% were men and 33.85% were women, 62.6% had bystander CPR and the time to ROSC was 29.43 mins. In those patients with a favourable neurological outcome (CPC 1-2), 69.19 % were men and 30.81% were female. 74.62% of these patients had bystander CPR and had a reduced time to ROSC of 18.5 mins. With respect to age, those with a good neurological outcome were younger (mean 59.87 years) as compared to those who had a poor neurological outcome (mean 64.45 years). MicroRNAs were obtained from 2hrs to 78hrs from ROSC, with the most frequent sample acquisition point being 48hrs post-ROSC. Patient demographic data, stratified by patient outcome, is shown in Table 2 and Table 3.
Table 2.
Relevant characteristics and clinical data of patients with an unfavourable neurological outcome (CPC 3-5) at 6 months from ROSC. Relevant parameters including age, gender breakdown, bystander cardiopulmonary resuscitation (CPR) and time from CPR onset to return of spontaneous circulation (ROSC). Table generated in Apple Numbers version 13.2.
Table 2.
Relevant characteristics and clinical data of patients with an unfavourable neurological outcome (CPC 3-5) at 6 months from ROSC. Relevant parameters including age, gender breakdown, bystander cardiopulmonary resuscitation (CPR) and time from CPR onset to return of spontaneous circulation (ROSC). Table generated in Apple Numbers version 13.2.
| Patients with an Unfavourable Neurological Outcome after Cardiac Arrest and ROSC (CPC 3-5). | ||||||
| Study Identifier | n | Age (years) | M % | F % | Bystander CPR (y %) | Time to ROSC (min) |
| 1 | 67 | 66 | 87 | 13 | 78 | 26 |
| 2 | 30 | 72 | 53 | 47 | 37 | 25 |
| 3 | 14 | 63 | 9 | 91 | n.a | 30 |
| 4 | 275 | 68 | 77.8 | 22.2 | 66.2 | 30 |
| 5 | 34 | 60 | 73.5 | 26.5 | 52.9 | 34.5 |
| 6 | 118 | 54.08 | 56.8 | 43.2 | n.a | 89.16 |
| 7 | 18 | n.a | n.a | n.a | n.a | n.a |
| 8 | 283 | 68 | 77.4 | 22.6 | 66.1 | 30 |
| 9 | 291 | 68 | 76.92 | 23.08 | 66 | 30 |
| 10 | 25 | 70 | 84 | 16 | 72 | 30 |
| Average | 64.45 | 66.15 | 33.85 | 62.6 | 29.43 | |
| Total | 1155 | |||||
Table 3.
Relevant characteristics and clinical data of patients with a favourable neurological outcome (CPC 1-2) at 6 months from ROSC. Relevant parameters including age, gender breakdown, bystander cardiopulmonary resuscitation (CPR) and time from CPR onset to return of spontaneous circulation (ROSC). Table generated in Apple Numbers version 13.2.
Table 3.
Relevant characteristics and clinical data of patients with a favourable neurological outcome (CPC 1-2) at 6 months from ROSC. Relevant parameters including age, gender breakdown, bystander cardiopulmonary resuscitation (CPR) and time from CPR onset to return of spontaneous circulation (ROSC). Table generated in Apple Numbers version 13.2.
| Patients with a Favourable Neurological Outcome after Cardiac Arrest and ROSC (CPC 1-2). | ||||||
| Study Identifier | n | age (years) | M % | F % | Bystander CPR (y %) | Time to ROSC (min) |
| 1 | 104 | 59 | 88 | 12 | 82 | 19 |
| 2 | 35 | 65 | 74 | 26 | 49 | 16 |
| 3 | 14 | 64 | 9 | 91 | n.a | 20 |
| 4 | 304 | 60 | 82.6 | 17.4 | 79.9 | 20 |
| 5 | 20 | 48 | 60 | 40 | 75 | 13 |
| 6 | 142 | 54.87 | 58.5 | 41.5 | n.a | 57.24 |
| 7 | 9 | n.a | n.a | n.a | n.a | n.a |
| 8 | 307 | 60 | 82.7 | 17.3 | 79.5 | 20 |
| 9 | 299 | 61 | 83.9 | 16.1 | 81 | 20 |
| 10 | 25 | 62 | 84 | 16 | 76 | 20 |
| Average | 59.87 | 69.19 | 30.81 | 74.62 | 18.5 | |
| Total | 1259 | |||||
MicroRNAs and Their Expression Post-ROSC in Patients with an Unfavourable Neurological Outcome
All reported microRNAs, with exception to miR-191-5p and miR-122-5p, were found to be up-regulated across the 2-72hr period following ROSC (Figure 2). Additionally, miR-122-5p expression was subsequently found to be up-regulated at 48hrs, demonstrating a potential temporal specificity to its expression.
Twice reported analysis was carried out within the microRNA data to match results for time obtained, expression, direct microRNA species, and outcome, yielding one miRNA that satisfied these requirements. As seen in Figure 2, microRNA-124-3p expression was up-regulated at 6hrs post-ROSC.
Further to this replication of miR-124-3p at 6hrs, miR-124-3p was also up-regulated at 2 hours, and at 48hrs. miR-124, although not species specific, is reported to be up-regulated at 24hr and 48hrs. Additionally, although not replicated, a similar pattern of sustained expression following CA is seen in miR-9-3p, which was up-regulated at 28, 48, and 72hrs. The remainder of miRNAs and their expression are visualised on Figure 2.
The Accuracy of Acute microRNAs Expression at Predicting Patient Neurological Outcome at 6 Months from ROSC
13 Receiver operator characteristic area under the curve (ROC-AUC) values for several microRNAs across the first 72 hours were obtained and are presented in Figure 3. For accurately predicting neurological outcomes at 6 months, ROC values ranged from 0.62-0.89 when obtained within the first 48hrs. miR-124 and miR-191-5p had the most accurate ROC-AUC value of 0.89 at 48hrs. miR-122-5p was found to have the lowest reported diagnostic accuracy at 0.62 at 48hrs.
Significant Changes in Circulating microRNAs Mostly Predict Unfavourable Neurological Outcomes at 6 Months
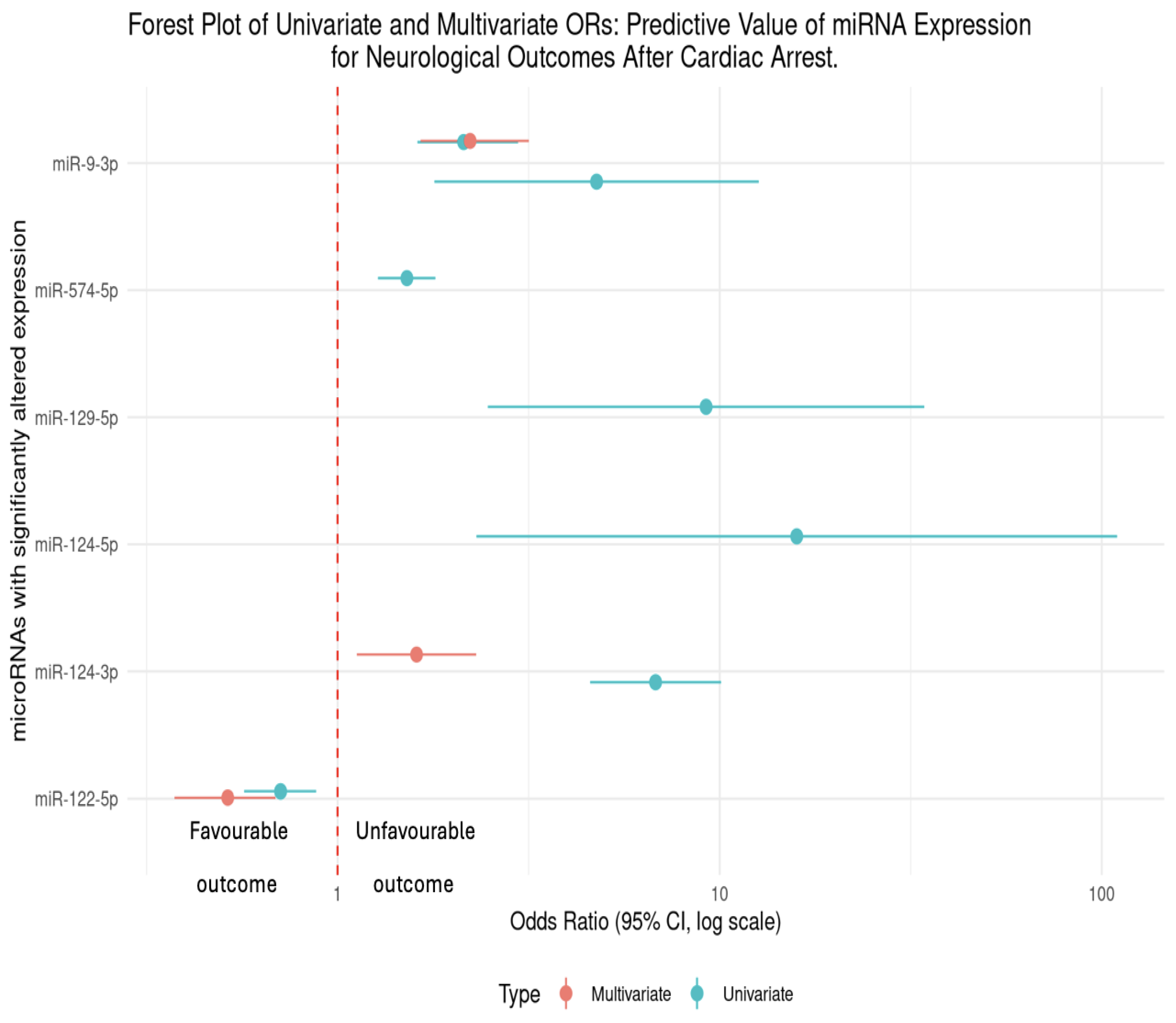
5 studies reported Odds Ratios (OR). Following significant changes in circulating miRNA expression, patients were more likely to have an unfavourable outcome following cardiac arrest and ROSC. This was the exception for miR-122-5p, for which both univariate and multivariate OR was <1 and therefore suggests a neuro-protective effect of having an up-regulated change to miR-122-5p expression. These results are further expanded in Table 3 and visualised in Figure 4.
Hazard Ratio (HR)
Only one eligible study reported a Hazard Ratio (HR). Yu et al 2022 found a down-regulation in miR-191-5p at 48hrs (<0.001) and reported a multivariate-generated hazard ratio (HR) of 0.344 (0.208-0.567) suggesting that patients with a down-regulated miR-191-5p may have a protective association for neurological outcomes (Table 3).
Table 3.
Table of differing associations between microRNAs obtained and neurological outcomes at 6-months, shown by a regression models including univariate and multivariate analysis. Author and year shown in italics. 95% CI = 95% Confidence Interval, OR = Odds Ratio.
Table 3.
Table of differing associations between microRNAs obtained and neurological outcomes at 6-months, shown by a regression models including univariate and multivariate analysis. Author and year shown in italics. 95% CI = 95% Confidence Interval, OR = Odds Ratio.
| Author / Year | Association between microRNAs after ROSC and Neurological Outcomes. |
| Beske et al 2022 | miR-9-3p was up-regulated at 48hrs post-ROSC. Univariate analysis revealed that patients in this study with elevated microRNA levels at 48hrs post-CA were more than twice as likely to have an unfavourable neurological outcome (OR = 2.14, 95%CI [1.62-2.97]), p<0.0001). From multivariate analysis, patients were twice as likely to have a poor neurological outcome with an elevated miR-9-5p (OR = 2.21, 95% CI [1.64-3.15]), p <0.0001). |
| Devaux et al 2016 | miR-124-3p which was up-regulated at 48hrs post-ROSC (p<0.001) found that patients with an elevated miR-124-3p were additionally at risk of an unfavourable outcome, which was quantified to be 6.72 times as likely (univariate OR = 6.72, 95% CI [4.53-9.97]). Following multivariate analysis, this unfavourable outcome was 1.6x as likely in patients with an elevated miR-124-3p (OR = 1.62, 95% CI [1.13-2.32]). |
| Devaux et al 2017 | miR-122-5p at 48hrs was found to be down-regulated (p<0.001) in patients with an unfavourable outcome. In univariate analysis, the odds ratio (OR = 0.71, 95% CI [0.57–0.88]) indicates that for each unit increase in miR-122-5p expression, the odds of a poor neurological outcome decreased by 29%. From multivariate analysis, the OR further decreased to 0.51 (95% CI [0.37–0.68]), suggesting a 49% reduction in the odds of an unfavourable outcome for higher levels of miR-122-5p.This demonstrates that higher miR-122-5p expression may have a neuro-protective effect following cardiac arrest. |
| Boileau et al 2019 | miR-574-5p was up-regulated at 48hrs (p<0.001). From univariate analysis, levels of miR-574-5p was a predictor of neurological outcomes (OR = 1.5, 95% CI [1.26-1.78]). Interestingly, this study reported sex specific differences in men vs women. From multivariate analysis, circulating levels of miR-574-5p predicted neurological outcomes in women (OR = 1.9, 95% CI [1.09-3.45]) but not in men (OR = 1.0, 95% CI [0.74-1.28]). |
| Steffanizzi et al 2020 | Logistic regression of miR-9-3p, miR-124-3p, and miR-129-5p found that these microRNAs were all associated with poorer outcomes, miR-9-3p (OR = 4.81, 95% CI [1.81-12.78]), miR-124-3p (OR = 15.92, 95% CI [2.31-109.74]) and miR-129-5p (OR = 9.2, 95% CI [2.47-34.26]). |
Discussion/Conclusions
This review has collated and presented the most up to date evidence regarding the use of microRNAs as prognostic biomarkers of neurological outcomes following cardiac arrest and return of spontaneous circulation (ROSC), identifying distinct changes in miRNA expression, the individual accuracy of miRNAs, and presenting the association between microRNA expression changes and favourable or unfavourable outcomes in the form of odds ratios (OR). This analysis was unique in that it portrayed them temporally to allow for comparison of expression over time to highlight when, from the literature, is the most optimal time to obtain miRNAs for this type of prognostication and which miRNAs are most clinically useful to predict outcomes.
This work identified that miRNA-124 is a useful biomarker for post-cardiac arrest prognostication of neurological outcomes, with distinct expression and high accuracy for predicting neurological outcomes. The 3 prime species, miRNA-124-3p was found to be up-regulated from 2-48hrs and at 6hrs, a finding replicated twice. Within this context, changes in miR-124-3p could be from heart, vascular, brain, or multi-organ ischaemia with several studies citing miR-124-3p as a biomarker of hypoxia-ischaemia [33,34,35,36]. Further to this, within cell lines exposed to hypoxia and patients presenting with acute myocardial infarction, miR-124-3p expression was significantly increased compared to control patients and control conditions for the cell culture [37]. Interestingly, from further work, hypoxia-induced apoptosis of these cells was eliminated by the inhibition of miR-124-3p, offering a novel therapeutic strategy for diseases of hypoxic-ischaemic nature [38,39].
The use of biomarkers in post-cardiac arrest prognostication is not novel. Established circulating biomarkers such as neuron-specific enolase (NSE), S100B, and neurofilament heavy chain have been explored for this purpose [40,41,42]. Among these, NSE is the only biomarker recommended for prognostication [43]. However, its clinical utility is hindered by variability in standardization, concerns regarding haemolysis-related artefacts [44] and intra-sample variability, with Stern et al 2007 [45] reporting a potential 40% discrepancy in NSE levels from the same patient samples. This raises concerns about its reliability in clinical decision-making. Unlike NSE, miRNAs offer improved stability and specificity due to their role as gene expression regulators in normal physiology. Their expression has been widely explored and shows inter-individual longitudinal stability [46] and their expression remain stable for at least 24hrs at room temperature in whole blood, allowing for complex biomedical testing and analysis [47].
This review identified that miR-122-5p has temporally specific expression following cardiac arrest and ROSC, as miR-122-5p was up-regulated at 6hr then down-regulated at 48hrs. MicroRNA-122-5p is located on chromosome 18q21.31 [48] and involved in modulating several relevant biological pathways in brain health such as inflammation, oxidative stress, angiogenesis, and neuronal survival. Further, miR-122-5p has been found to regulate HIF-1α (Hypoxia-inducible factor 1 alpha), which is essential for cellular responses to low oxygen levels and contributes to neuroprotection and overall cell survival in global (and focal) ischaemia [48,49,50,51]. Interestingly, animal work of myocardial ischaemia reperfusion injury (MI/RI), has shown that upon ischaemia, miR-122-5p expression was up-regulated and that depletion of miR-122-5p alleviated ischaemic injury and suppressed cardiomyocyte apoptosis [52]. A comprehensive understanding of the regulatory and upstream processes involving miR-122-5p expression and its associated gene targets may allow for precision medicine strategies to improve neuroprotective pharmacological therapies in patients with HIBI and myocardial ischaemia.
The volume of pathologies involving miRNAs may negatively impact their clinical translation by confounding their expression. For example, miR-21 is reported within this work to be up-regulated at 48hrs, but miR-21 levels are altered within 29 other disease processes including acute coronary syndrome, hepatitis C, Chron’s disease, multiple sclerosis, pulmonary fibrosis, type 2 diabetes, and several more, indicating a lack of specificity to a particular disease [53]. In a population such the UK, it would be troubling to find a patient without any of these conditions or a family history of such disease, such that, the levels could be assumed to be un-altered by existing pathology or genomic changes to miRNA promoters. Thus, when selecting a miRNA biomarker, the expression of this miRNA in other pathologies should be considered as fully and comprehensively as possible.
A key limitation of this review was the inclusion of several spin-off studies from the large, multi-centre Targeted Temperature Management (TTM) trial [54], which investigated the impact of targeted hypothermia (33°C or 36°C) in unconscious patients following hcardiac arrest. These spin-off studies reported microRNA levels and patient outcomes locally as although the TTM trial was the source and organised the collection of biological samples, it did not publish or collate the biomarker data, leaving individual clinical teams to publish their own analyses from local biobanks of patients involved in the TTM trial. For this review, the spin off studies were treated as separate entities and independent cohorts. Moving forward, larger, independent cohort and case-control studies should validate the microRNAs identified by this review and pragmatic trials should investigate the clinical utility of this data, especially the perception of clinicians in how useful this information is to clinical decision making.
Conclusion
Accurately predicting neurological outcomes and establishing neuroprotective strategies following cardiac arrest remains an unmet need in intensive care medicine. This review has collated and presented miRNA expression at several time points (2hr-72hr) following cardiac arrest and return of spontaneous circulation (ROSC), demonstrated the fluctuation in predictive accuracy of miRNAs for 6-month neurological outcome through ROC-AUC values, and quantitatively assessed associations between expression of miRNAs and outcomes using odds ratios and hazard ratios, using evidence from 10 clinical studies.
From this, I highlight the future of miR-124-3p and miR-122-5p as useful candidate prognostic biomarkers of neurological outcomes after cardiac arrest. Further mechanistic understanding of these miRNA could enhance our confidence in their role of specific biomarkers of global brain ischaemia and long-term damage, and may inspire precision medicine pharmacologic initiatives to mitigate hypoxic-ischaemic brain injury (HIBI) in these patients. New observational and preclinical research will hopefully increase specificity of microRNAs due to their large involvement in normal physiology and pathophysiology across many disease families including cardiovascular, neurological, immunogenic, and oncological, leading to potential confounding of expression values that could be catastrophic for clinical decision making.
Finally, it is vital to stress that prognostication relies on a multi-component approach including clinical examination and expert physician opinion, imaging, neurophysiology, and expertise of the multi-disciplinary team to guide treatment and clinical decision making. This research lays the foundation for future pragmatic trials and the advancement of genomic biomarkers in precision neurocritical post-cardiac arrest care.
Author Contributions
JM conceptualised, researched, and prepared the manuscript.
Funding
Not applicable.
Acknowledgements
Not applicable.
Competing Interests
The author declares no competing interests.
Ethics Approval and Consent to Participate
Not applicable, this work was a review of published clinical studies, all with their own individual ethics approval.
Consent for Publication
Not applicable.
Availability of Data and Materials:
Data was extracted from relevant published studies (see Appendix A) and collated. R studio code for data analysis and collation is available upon reasonable request.
List of Abbreviations
| MicroRNA/miRNA/miR | Micro ribonucleic acid. |
| RNA | Ribonucleic acid. |
| CPR | Cardiopulmonary resuscitation. |
| UK | United Kingdom. |
| OHCA | Out of hospital cardiac arrest. |
| CA | Cardiac arrest. |
| ROSC | Return of spontaneous circulation. |
| HIBI | Hypoxic ischaemic brain injury. |
| mRNA | Messenger ribonucleic acid. |
| UTR | Untranslated region. |
| qPCR | quantitative polymerase chain reaction. |
| ROC-AUC | Receiver operator characteristic area under the curve (value). |
| OR | Odds ratio. |
| HR | Hazard ratio. |
| CPC | Cerebral performance category. |
| FDR | False discovery rate. |
| CI | Confidence interval. |
| NSE | Neuron specific enolase. |
| HIF-1-alpha | Hypoxia inducible factor 1 alpha. |
| MI/RI | Myocardial ischaemia reperfusion injury. |
| TTM | Targeted temperature management. |
Appendix A
References of included studies.
- Beske RP, Bache S, Abild Stengaard Meyer M, Kjærgaard J, Bro-Jeppesen J, Obling L, Olsen MH, Rossing M, Nielsen FC, Møller K, Nielsen N, Hassager C. MicroRNA-9-3p: a novel predictor of neurological outcome after cardiac arrest. Eur Heart J Acute Cardiovasc Care. 2022 Aug 9;11(8):609-616. https://doi.org/10.1093/ehjacc/zuac066
- Gilje P, Gidlöf O, Rundgren M, Cronberg T, Al-Mashat M, Olde B, Friberg H, Erlinge D. The brain-enriched microRNA miR-124 in plasma predicts neurological outcome after cardiac arrest. Crit Care. 2014 Mar 3;18(2):R40. https://doi.org/10.1186/cc13753
- Stammet P, Goretti E, Vausort M, Zhang L, Wagner DR, Devaux Y. Circulating microRNAs after cardiac arrest. Crit Care Med. 2012 Dec;40(12):3209-14. https://doi.org/10.1097/CCM.0b013e31825fdd5e
- Devaux Y, Dankiewicz J, Salgado-Somoza A, Stammet P, Collignon O, Gilje P, Gidlöf O, Zhang L, Vausort M, Hassager C, Wise MP, Kuiper M, Friberg H, Cronberg T, Erlinge D, Nielsen N; for Target Temperature Management After Cardiac Arrest Trial Investigators. Association of Circulating MicroRNA-124-3p Levels With Outcomes After Out-of-Hospital Cardiac Arrest: A Substudy of a Randomized Clinical Trial. JAMA Cardiol. 2016 Jun 1;1(3):305-13. https://doi.org/10.1001/jamacardio.2016.0480
- Oh SH, Kim HS, Park KN, Ji S, Park JY, Choi SP, Lim JY, Kim HJ, On Behalf Of Crown Investigators. The Levels of Circulating MicroRNAs at 6-Hour Cardiac Arrest Can Predict 6-Month Poor Neurological Outcome. Diagnostics (Basel). 2021 Oct 15;11(10):1905. https://doi.org/10.3390/diagnostics11101905
- Yu J, Zhou A, Li Y. Clinical value of miR-191-5p in predicting the neurological outcome after out-of-hospital cardiac arrest. Ir J Med Sci. 2022 Aug;191(4):1607-1612. https://doi.org/10.1007/s11845-021-02745-6
- Shen H, Zaitseva D, Yang Z, Forsythe L, Joergensen S, Zone AI, Shehu J, Maghraoui S, Ghorbani A, Davila A, Issadore D, Abella BS. Brain-derived extracellular vesicles as serologic markers of brain injury following cardiac arrest: A pilot feasibility study. Resuscitation. 2023 Oct;191:109937. https://doi.org/10.1016/j.resuscitation.2023.109937
- Devaux Y, Salgado-Somoza A, Dankiewicz J, Boileau A, Stammet P, Schritz A, Zhang L, Vausort M, Gilje P, Erlinge D, Hassager C, Wise MP, Kuiper M, Friberg H, Nielsen N; TTM-trial investigators. Incremental Value of Circulating MiR-122-5p to Predict Outcome after Out of Hospital Cardiac Arrest. Theranostics. 2017 Jun 25;7(10):2555-2564. https://doi.org/10.7150/thno.19851
- Boileau A, Somoza AS, Dankiewicz J, Stammet P, Gilje P, Erlinge D, Hassager C, Wise MP, Kuiper M, Friberg H, Nielsen N, Devaux Y; TTM-Trial Investigators on behalf of Cardiolinc Network. Circulating Levels of miR-574-5p Are Associated with Neurological Outcome after Cardiac Arrest in Women: A Target Temperature Management (TTM) Trial Substudy. Dis Markers. 2019 Jun 2;2019:1802879. https://doi.org/10.1155/2019/1802879
- Stefanizzi FM, Nielsen N, Zhang L, Dankiewicz J, Stammet P, Gilje P, Erlinge D, Hassager C, Wise MP, Kuiper M, Friberg H, Devaux Y, Salgado-Somoza A. Circulating Levels of Brain-Enriched MicroRNAs Correlate with Neuron Specific Enolase after Cardiac Arrest-A Substudy of the Target Temperature Management Trial. Int J Mol Sci. 2020 Jun 19;21(12):4353. https://doi.org/10.3390/ijms21124353
References
- Lemiale V, Dumas F, Mongardon N, Giovanetti O, Charpentier J, Chiche JD, Carli P, Mira JP, Nolan J, Cariou A. Intensive care unit mortality after cardiac arrest: the relative contribution of shock and brain injury in a large cohort. Intensive Care Med. 2013 Nov;39(11):1972-80. [CrossRef]
- Perkins D.G., Nolan P.J., Soar J, Hawkes C, Wylie J, Skellet S, Lockey A, Hampshire S., Epidemiology of Cardiac Arrest Guidelines. Resuscitation Council UK. May 2020. Available at https://www.resus.org.uk/library/2021-resuscitation-guidelines/epidemiology-cardiac-arrest-guidelines.
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Judd SE, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Mackey RH, Magid DJ, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER 3rd, Moy CS, Mussolino ME, Neumar RW, Nichol G, Pandey DK, Paynter NP, Reeves MJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Wong ND, Woo D, Turner MB; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Executive summary: heart disease and stroke statistics--2014 update: a report from the American Heart Association. Circulation. 2014 Jan 21;129(3):399-410. [CrossRef]
- Couper K, Ji C, Deakin CD, Fothergill RT, Nolan JP, Long JB, Mason JM, Michelet F, Norman C, Nwankwo H, Quinn T, Slowther AM, Smyth MA, Starr KR, Walker A, Wood S, Bell S, Bradley G, Brown M, Brown S, Burrow E, Charlton K, Claxton Dip A, Dra'gon V, Evans C, Falloon J, Foster T, Kearney J, Lang N, Limmer M, Mellett-Smith A, Miller J, Mills C, Osborne R, Rees N, Spaight RES, Squires GL, Tibbetts B, Waddington M, Whitley GA, Wiles JV, Williams J, Wiltshire S, Wright A, Lall R, Perkins GD; PARAMEDIC-3 Collaborators. A Randomized Trial of Drug Route in Out-of-Hospital Cardiac Arrest. N Engl J Med. 2025 Jan 23;392(4):336-348. [CrossRef]
- Sandroni C, Cronberg T, Sekhon M. Brain injury after cardiac arrest: pathophysiology, treatment, and prognosis. Intensive Care Med. 2021 Dec;47(12):1393-1414. [CrossRef]
- Nolan JP, Sandroni C, Böttiger BW, Cariou A, Cronberg T, Friberg H, Genbrugge C, Haywood K, Lilja G, Moulaert VRM, Nikolaou N, Olasveengen TM, Skrifvars MB, Taccone F, Soar J. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: post-resuscitation care. Intensive Care Med. 2021 Apr;47(4):369-421. [CrossRef]
- Chalkias A, Xanthos T. Post-cardiac arrest brain injury: pathophysiology and treatment. J Neurol Sci. 2012 Apr 15;315(1-2):1-8. [CrossRef]
- Lassen NA. Normal average value of cerebral blood flow in younger adults is 50 ml/100 g/min. J Cereb Blood Flow Metab. 1985 Sep;5(3):347-9. [CrossRef]
- Donkor ES. Stroke in the 21st Century: A Snapshot of the Burden, Epidemiology, and Quality of Life. Stroke Res Treat. 2018 Nov 27;2018:3238165. [CrossRef]
- Hossmann KA. Viability thresholds and the penumbra of focal ischemia. Ann Neurol. 1994 Oct;36(4):557-65. [CrossRef]
- Salaudeen MA, Bello N, Danraka RN, Ammani ML. Understanding the Pathophysiology of Ischemic Stroke: The Basis of Current Therapies and Opportunity for New Ones. Biomolecules. 2024 Mar 4;14(3):305. [CrossRef]
- Woodruff TM, Thundyil J, Tang SC, Sobey CG, Taylor SM, Arumugam TV. Pathophysiology, treatment, and animal and cellular models of human ischemic stroke. Mol Neurodegener. 2011 Jan 25;6(1):11. [CrossRef]
- Qin C, Yang S, Chu YH, Zhang H, Pang XW, Chen L, Zhou LQ, Chen M, Tian DS, Wang W. Signalling pathways involved in ischemic stroke: molecular mechanisms and therapeutic interventions. Signal Transduct Target Ther. 2022 Jul 6;7(1):215. Erratum in: Signal Transduct Target Ther. 2022 Aug 12;7(1):278. [CrossRef]
- Sandroni C, D'Arrigo S, Nolan JP. Prognostication after cardiac arrest. Crit Care. 2018 Jun 5;22(1):150. [CrossRef]
- Bhalala OG, Srikanth M, Kessler JA. The emerging roles of microRNAs in CNS injuries. Nat Rev Neurol. 2013 Jun;9(6):328-39. [CrossRef]
- Calin GA, Hubé F, Ladomery MR, Delihas N, Ferracin M, Poliseno L, Agnelli L, Alahari SK, Yu AM, Zhong XB. The 2024 Nobel Prize in Physiology or Medicine: microRNA Takes Center Stage. Noncoding RNA. 2024 Dec 12;10(6):62. [CrossRef]
- Çakmak HA, Demir M. MicroRNA and Cardiovascular Diseases. Balkan Med J. 2020 Feb 28;37(2):60-71. [CrossRef]
- Zhou, Ss., Jin, Jp., Wang, Jq. et al. miRNAS in cardiovascular diseases: potential biomarkers, therapeutic targets and challenges. Acta Pharmacol Sin 39, 1073–1084 (2018). [CrossRef]
- Kapplingattu, S.V., Bhattacharya, S. & Adlakha, Y.K. MiRNAs as major players in brain health and disease: current knowledge and future perspectives. Cell Death Discov. 11, 7 (2025). [CrossRef]
- Gao Y, Han D, Feng J. MicroRNA in multiple sclerosis. Clin Chim Acta. 2021 May;516:92-99. [CrossRef]
- Bassot, A., Dragic, H., Haddad, S.A. et al. Identification of a miRNA multi-targeting therapeutic strategy in glioblastoma. Cell Death Dis 14, 630 (2023). [CrossRef]
- Palizkaran Yazdi, M., Barjasteh, A. & Moghbeli, M. MicroRNAs as the pivotal regulators of Temozolomide resistance in glioblastoma. Mol Brain 17, 42 (2024). [CrossRef]
- Khan, P., Siddiqui, J.A., Kshirsagar, P.G. et al. MicroRNA-1 attenuates the growth and metastasis of small cell lung cancer through CXCR4/FOXM1/RRM2 axis. Mol Cancer 22, 1 (2023). [CrossRef]
- Yao Q, Wang X, He W, Song Z, Wang B, Zhang J, Qin Q. Circulating microRNA-144-3p and miR-762 are novel biomarkers of Graves' disease. Endocrine. 2019 Jul;65(1):102-109. [CrossRef]
- Huang C, Xing X, Xiang X, Fan X, Men R, Ye T, Yang L. MicroRNAs in autoimmune liver diseases: from diagnosis to potential therapeutic targets. Biomed Pharmacother. 2020 Oct;130:110558. [CrossRef]
- Metcalf G.A.D., (2024) Circulating biomarkers for the early detection of imperceptible cancers via biosensor and machine-learning advances, Oncogene. 43, 2135-2142). [CrossRef]
- Gayosso-Gómez, L.V, Ortiz-Quintero, B.,(2021) Circulating MicroRNAs in blood and other body fluids as biomarkers for diagnosis, prognosis, and therapy response in lung cancer, Diagnostics. 11,421. [CrossRef]
- Mitchell P.S, Parkin R.K, Kroh E.M, Fritz B.R, Wyman S.K, Pogosova-Agadjanyan E.L, Peterson A, Noteboom J, O'Briant K.C, Allen A, Lin D.W, Urban N, Drescher C.W, Knudsen B.S, Stirewalt D.L, Gentleman R, Vessella R.L, Nelson P.S, Martin D.B, Tewari M., (2008) Circulating microRNAs as stable blood based biomarkers for cancer detection, Proc. Natl. Acad. Sci USA.105 (30) 10513-10518. [CrossRef]
- Gareev I, Beylerli O, Zhao B., (2024) MiRNAs as potential therapeutic targets and biomarkers for non-traumatic intracerebral hemorrhage, Biomark Res 12,17 (2024). [CrossRef]
- Geocadin, R. G. et al. Standards for Studies of Neurological Prognostication in Comatose Survivors of Cardiac Arrest: A Scientific Statement from the American Heart Association. Circulation 140(9), e517–e542.
- Edgren E, Hedstrand U, Kelsey S, Sutton-Tyrrell K, Safar P. Assessment of neurological prognosis in comatose survivors of cardiac arrest. BRCT I Study Group. Lancet. 1994 Apr 30;343(8905):1055-9. [CrossRef]
- Lee RC, Feinbaum RL, Ambros V. The C. elegans heterochronic gene lin-4 encodes small RNAs with antisense complementarity to lin-14. Cell. 1993 Dec 3;75(5):843-54. [CrossRef]
- Liu X, Feng Z, Du L, Huang Y, Ge J, Deng Y, Mei Z. The Potential Role of MicroRNA-124 in Cerebral Ischemia Injury. Int J Mol Sci. 2019 Dec 23;21(1):120. [CrossRef]
- Huang P, Wei S, Ren J, Tang Z, Guo M, Situ F, Zhang D, Zhu J, Xiao L, Xu J, Liu G. MicroRNA-124-3p alleviates cerebral ischaemia-induced neuroaxonal damage by enhancing Nrep expression. J Stroke Cerebrovasc Dis. 2023 Feb;32(2):106949. [CrossRef]
- Yang, Q., Murata, K., Ikeda, T. et al. miR-124-3p downregulates EGR1 to suppress ischemia-hypoxia reperfusion injury in human iPS cell-derived cardiomyocytes. Sci Rep 14, 14811 (2024). [CrossRef]
- Han F, Chen Q, Su J, Zheng A, Chen K, Sun S, Wu H, Jiang L, Xu X, Yang M, Yang F, Zhu J, Zhang L. MicroRNA-124 regulates cardiomyocyte apoptosis and myocardial infarction through targeting Dhcr24. J Mol Cell Cardiol. 2019 Jul;132:178-188. [CrossRef]
- Liang Y.P, Liu Q, Xu G.H, Zhang J, Chen Y, Hua F.Z, Deng C.Q, Hu Y.H., (2019)The lncRNA ROR/miR-124-3p/TRAF6 axis regulated the ischaemia reperfusion injury-induced inflammatory response in human cardiac myocytes. J Bioenerg Biomembr 51, 381–392. [CrossRef]
- Han F, Chen Q, Su J, Zheng A, Chen K, Sun S, Wu H, Jiang L, Xu X, Yang M, Yang F, Zhu J, Zhang L. MicroRNA-124 regulates cardiomyocyte apoptosis and myocardial infarction through targeting Dhcr24. J Mol Cell Cardiol. 2019 Jul;132:178-188. [CrossRef]
- Hu, G., Ma, L., Dong, F., Hu, X., Liu, S., & Sun, H. (2019). Inhibition of microRNA-124-3p protects against acute myocardial infarction by suppressing the apoptosis of cardiomyocytes. Molecular Medicine Reports, 20, 3379-3387. [CrossRef]
- Hu, J., Ai, M., Xie, S. et al. NSE and S100β as serum alarmins in predicting neurological outcomes after cardiac arrest. Sci Rep 14, 25539 (2024). [CrossRef]
- Rundgren M, Karlsson T, Nielsen N, Cronberg T, Johnsson P, Friberg H. Neuron specific enolase and S-100B as predictors of outcome after cardiac arrest and induced hypothermia. Resuscitation. 2009 Jul;80(7):784-9. [CrossRef]
- Scolletta S, Donadello K, Santonocito C, Franchi F, Taccone FS. Biomarkers as predictors of outcome after cardiac arrest. Expert Rev Clin Pharmacol. 2012 Nov;5(6):687-99. [CrossRef]
- Nolan JP, Sandroni C, Böttiger BW, Cariou A, Cronberg T, Friberg H, Genbrugge C, Haywood K, Lilja G, Moulaert VRM, Nikolaou N, Olasveengen TM, Skrifvars MB, Taccone F, Soar J. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: post-resuscitation care. Intensive Care Med. 2021 Apr;47(4):369-421. [CrossRef]
- Ramont L, Thoannes H, Volondat A, Chastang F, Millet MC, Maquart FX. Effects of hemolysis and storage condition on neuron-specific enolase (NSE) in cerebrospinal fluid and serum: implications in clinical practice. Clin Chem Lab Med. 2005;43(11):1215-7. [CrossRef]
- Stern P, Bartos V, Uhrova J, Bezdickova D, Vanickova Z, Tichy V, Pelinkova K, Prusa R, Zima T. Performance characteristics of seven neuron-specific enolase assays. Tumour Biol. 2007;28(2):84-92. [CrossRef]
- Sandau, U.S., Wiedrick, J.T., McFarland, T.J. et al. Analysis of the longitudinal stability of human plasma miRNAs and implications for disease biomarkers. Sci Rep 14, 2148 (2024). [CrossRef]
- Glinge C, Clauss S, Boddum K, Jabbari R, Jabbari J, Risgaard B, Tomsits P, Hildebrand B, Kääb S, Wakili R, Jespersen T, Tfelt-Hansen J. Stability of Circulating Blood-Based MicroRNAs - Pre-Analytic Methodological Considerations. PLoS One. 2017 Feb 2;12(2):e0167969. [CrossRef]
- Faramin Lashkarian, M., Hashemipour, N., Niaraki, N. et al. MicroRNA-122 in human cancers: from mechanistic to clinical perspectives. Cancer Cell Int 23, 29 (2023). [CrossRef]
- Feng, W., Ying, Z., Ke, F., & Mei-Lin, X. (2021). Apigenin suppresses TGF-β1-induced cardiac fibroblast differentiation and collagen synthesis through the downregulation of HIF-1α expression by miR-122-5p. Phytomedicine, 83, 153481. [CrossRef]
- Bamahel, A.S., Sun, X., Wu, W. et al. Regulatory Roles and Therapeutic Potential of miR-122-5p in Hypoxic-Ischemic Brain Injury: Comprehensive Review. Cell Biochem Biophys (2025). [CrossRef]
- Kong Y, Li S, Cheng X, Ren H, Zhang B, Ma H, Li M, Zhang XA. Brain Ischemia Significantly Alters microRNA Expression in Human Peripheral Blood Natural Killer Cells. Front Immunol. 2020 May 14;11:759. [CrossRef]
- Zhang J, Fu L, Zhang J, Zhou B, Tang Y, Zhang Z, Gu T. Inhibition of MicroRNA-122-5p Relieves Myocardial Ischemia-Reperfusion Injury via SOCS1. Hamostaseologie. 2023 Aug;43(4):271-280. [CrossRef]
- Jenike AE, Halushka MK. miR-21: a non-specific biomarker of all maladies. Biomark Res. 2021 Mar 12;9(1):18. [CrossRef]
- Nielsen N, Wetterslev J, Cronberg T, Erlinge D, Gasche Y, Hassager C, Horn J, Hovdenes J, Kjaergaard J, Kuiper M, Pellis T, Stammet P, Wanscher M, Wise MP, Åneman A, Al-Subaie N, Boesgaard S, Bro-Jeppesen J, Brunetti I, Bugge JF, Hingston CD, Juffermans NP, Koopmans M, Køber L, Langørgen J, Lilja G, Møller JE, Rundgren M, Rylander C, Smid O, Werer C, Winkel P, Friberg H; TTM Trial Investigators. Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. 2013 Dec 5;369(23):2197-206. [CrossRef]
Figure 1.
Flow chart of review methodology and extraction of relevant data from included studies. Common reasons for exclusion also listed.
Figure 1.
Flow chart of review methodology and extraction of relevant data from included studies. Common reasons for exclusion also listed.
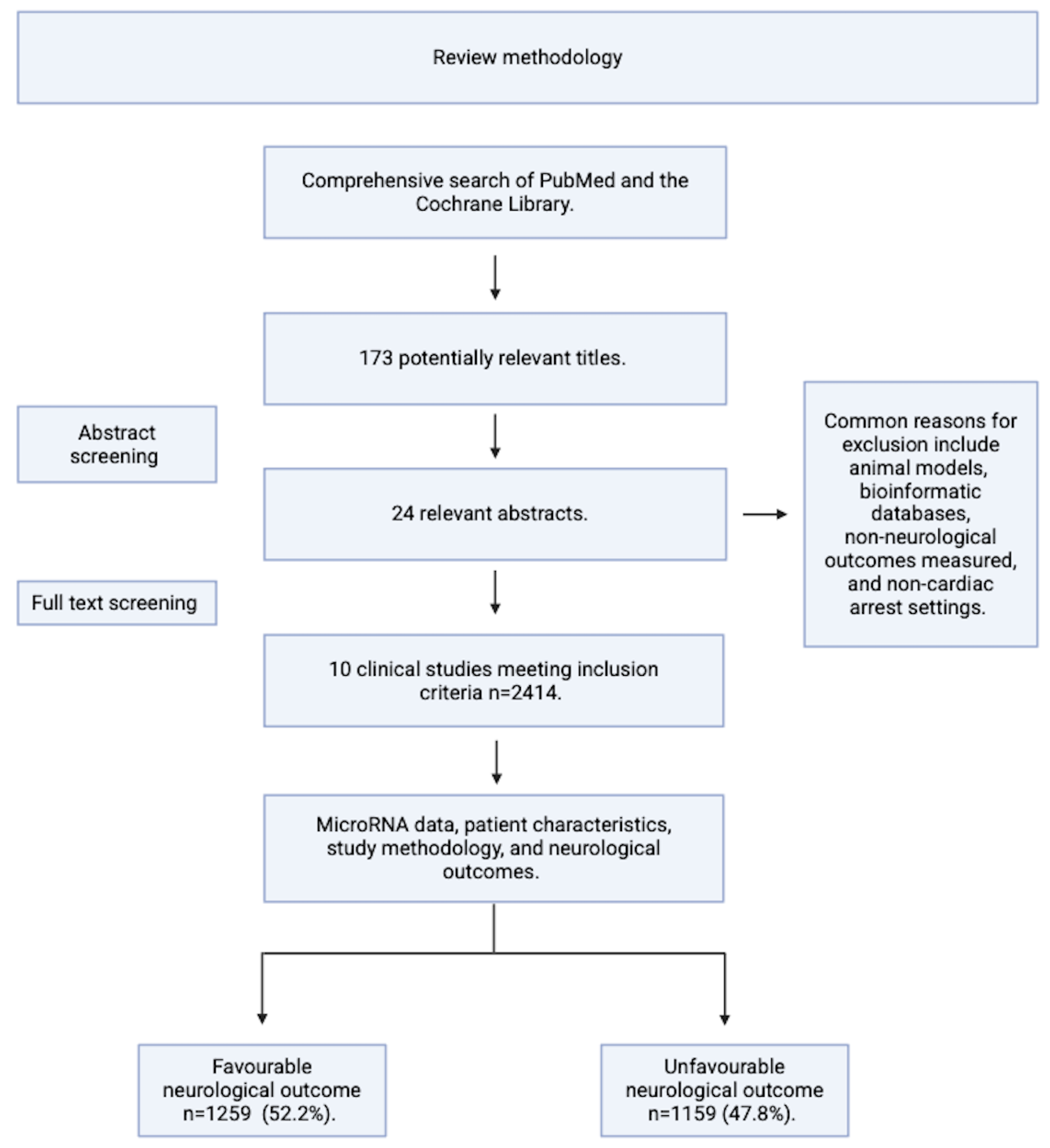
Figure 2.
Distribution of microRNAs within blood of patients with an unfavourable neurological outcome at 6 months across the first 72 hrs following ROSC. MicroRNA expression across the first 72 hours following cardiac arrest and ROSC. Size of dot representing significance of microRNA in terms of how many times this result has been replicated. Expression of microRNA denoted by colour of dot, down-regulated or up-regulated shown by red or blue, respectively. Unfavourable neurological outcome established by either Cerebral Performance Score at 6 months. Figure generated in R-studio.
Figure 2.
Distribution of microRNAs within blood of patients with an unfavourable neurological outcome at 6 months across the first 72 hrs following ROSC. MicroRNA expression across the first 72 hours following cardiac arrest and ROSC. Size of dot representing significance of microRNA in terms of how many times this result has been replicated. Expression of microRNA denoted by colour of dot, down-regulated or up-regulated shown by red or blue, respectively. Unfavourable neurological outcome established by either Cerebral Performance Score at 6 months. Figure generated in R-studio.
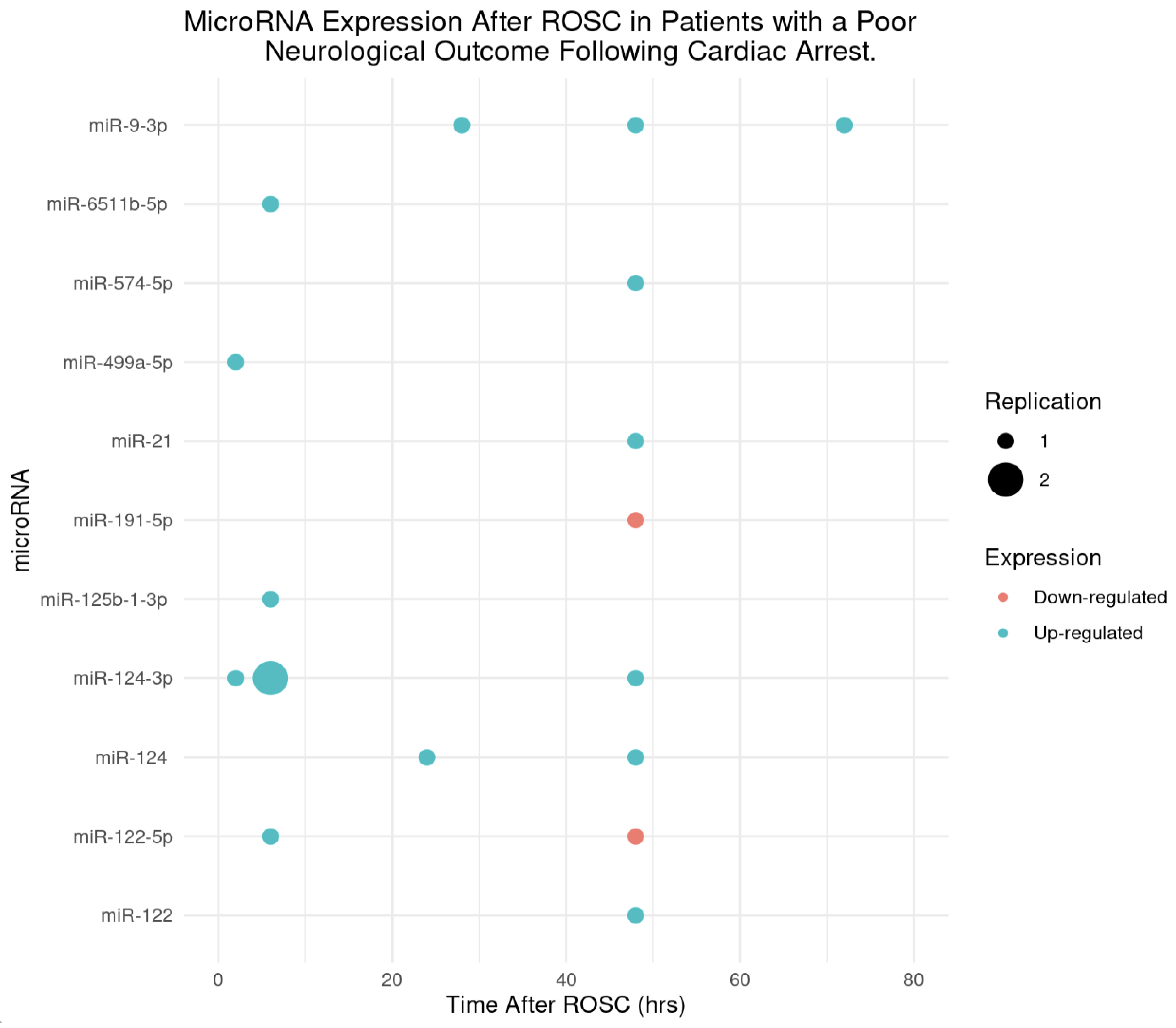
Figure 3.
The accuracy of microRNA levels at different time points following a return of spontaneous circulation to predict neurological outcomes of patients at 6 months. Figure generated using ROC-AUC values and the time in which the blood was obtained for these, to present how the predictive ability of correctly identifying neurological outcomes at 6 months is across the first 60 hours from return of spontaneous circulation. Figure generated in R-studio.
Figure 3.
The accuracy of microRNA levels at different time points following a return of spontaneous circulation to predict neurological outcomes of patients at 6 months. Figure generated using ROC-AUC values and the time in which the blood was obtained for these, to present how the predictive ability of correctly identifying neurological outcomes at 6 months is across the first 60 hours from return of spontaneous circulation. Figure generated in R-studio.
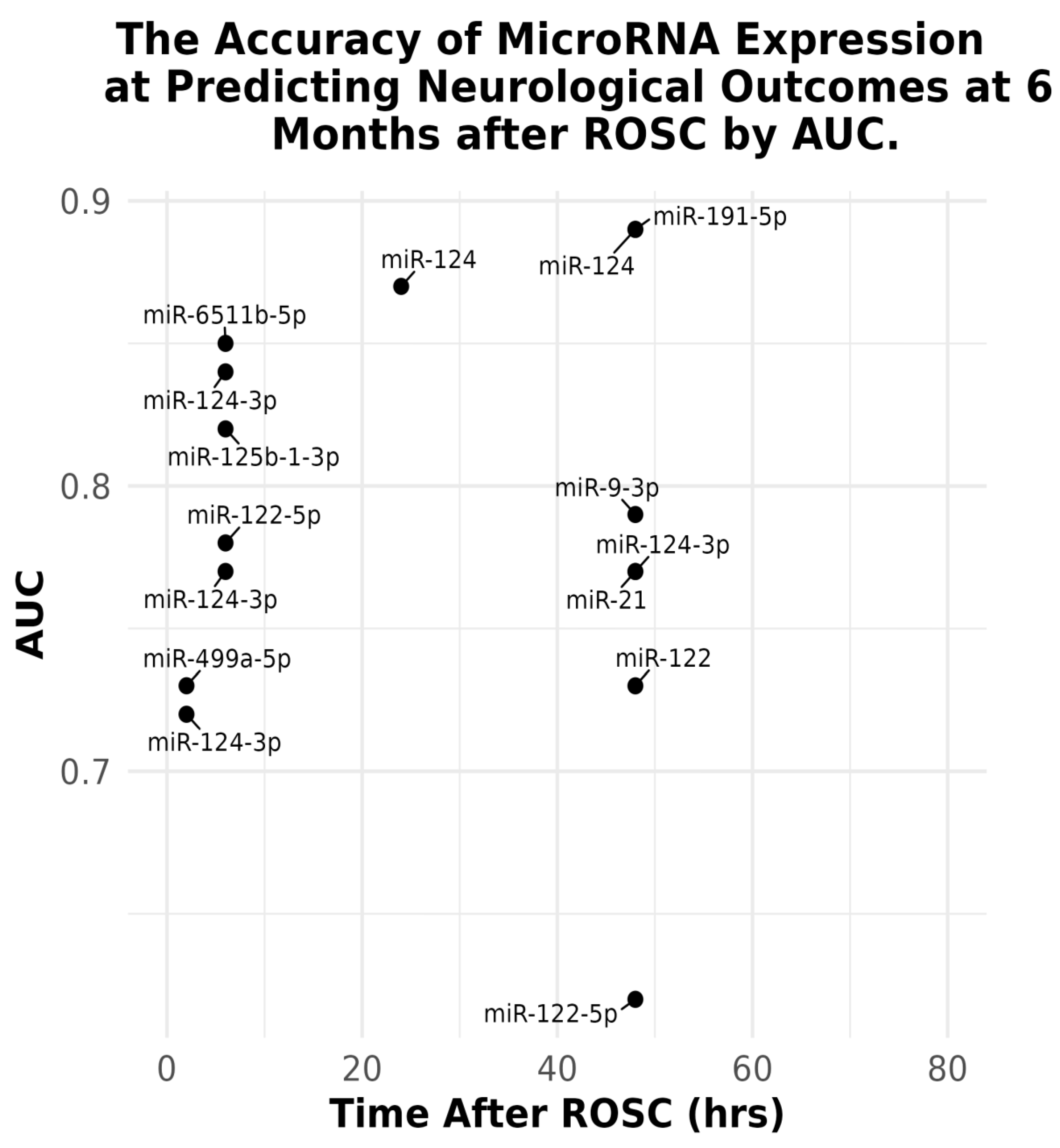
Figure 4.
Collated univariate and multivariate odds ratios (OR) for predicting poor neurological outcomes with differentially expressed microRNAs following cardiac arrest and return of spontaneous circulation (ROSC). Data were extracted in the form of ORs with 95% confidence intervals (CIs) and visualized using R-studio. The direction of change in microRNA expression (upregulated or downregulated) is not depicted but is elaborated on in main text. Blue and red markers represent univariate and multivariate analyses, respectively. The red dashed line represents the null effect (OR = 1), indicating no association with outcome.
Figure 4.
Collated univariate and multivariate odds ratios (OR) for predicting poor neurological outcomes with differentially expressed microRNAs following cardiac arrest and return of spontaneous circulation (ROSC). Data were extracted in the form of ORs with 95% confidence intervals (CIs) and visualized using R-studio. The direction of change in microRNA expression (upregulated or downregulated) is not depicted but is elaborated on in main text. Blue and red markers represent univariate and multivariate analyses, respectively. The red dashed line represents the null effect (OR = 1), indicating no association with outcome.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



