
Submitted:
12 May 2025
Posted:
14 May 2025
You are already at the latest version
Abstract
Background: Nearly 5 million people in Peru live with visual impairments, many of which are irreversible. Along with eye care services, these individuals could benefit from government services and rehabilitation to improve their quality of life and promote equitable, inclusive social participation. Though numerous government policies address this, little is known about their perception and implementation.
Methods: Semi-structured individual online interviews were conducted with 29 people (7 low vision, 12 blind, 6 educators/rehabilitators, 4 medical doctors) in Peru between July and November 2024. Each participant was asked to respond to the same 16 open-ended questions. Their transcripts were coded into themes in 5 domains: assistive devices, vision rehabilitation services, government assistance programs, accessibility for the visually impaired, and eye care services. The themes were compared among mem-bers of each group.
Results: Themes from educators/rehabilitators aligned well with those with blindness but much less with ophthalmologists and those with low vision. Participants mentioned that assistive devices are not traditionally provided by the government. There was little mention of vision rehabilitation services, particularly from low vision participants. Additionally, participants with visual impairments mentioned a lack of sensitivity from teachers, employers, and transport drivers. Interestingly, none of the participants with visual impairments benefitted from financial assistance.
Conclusions: Many of the barriers are societal, referring to lack of understanding from the public in employment, education, transportation, or the use of assistive devices. People with visual impairments and educators should be included in any policy decisions to promote equality for Peruvians with vision loss.
Keywords:
visual disability
; assistive devices
; vision rehabilitation
; eye care
; accessibility
1. Introduction
Almost 21 million people in Andean Latin America—which includes Venezuela, Colombia, Ecuador, Peru, Bolivia, and Chile—are living with a visual impairment, and more than 870,000 of these individuals are blind [1]. Peru is the second Andean country, after Colombia, with the highest visual impairment (VI) prevalence, with 13.5% of its population affected at all levels, from mild VI to blindness, including near vision problems as reported in 2020 [1-3]. The most common eye diseases prioritized by the Peruvian government include retinopathy of prematurity, refractive errors, cataracts, glaucoma, and diabetic retinopathy [2, 4]. In 2017, VI was the most prevalent functional disability in Peru, affecting 48.3% of individuals with disabilities; a higher rate than any other functional disability [5].
Peru is among 184 out of 193 United Nations (UN) member states to ratify the Convention on the Rights of Persons with Disabilities (CRPD), becoming a State Party in 2008. The CRPD states that independent living must be facilitated by the elimination of accessibility barriers, whether they are found in the physical environment (i.e. schools, workplaces, indoor or outdoor facilities, roads, health infrastructures), in transportation, or in information and communications. In that regard, it emphasizes that these facilitators should include braille and that technologies should be accessible at a minimum cost [6]. By ratifying the CRPD, Peru legally adopts anti-discrimination laws and eliminate accessibility barriers [7]. Furthermore, the adoption of the CRPD’s Optional Protocol, enables individuals to submit direct complaints to the UN Committee on the Rights of Persons with Disabilities [7, 8]
Peru has established a comprehensive legal framework to protect the rights of persons with disabilities with implications for vision rehabilitation services. Indeed, the 1993 Constitution safeguards disabilities rights through Articles 7 and 23 (healthcare, social protection and employment) as well as Article 16 (inclusive education). Peru also emphasizes independent living with community inclusion support (Article 9), personal mobility (Article 20), inclusive and lifelong education (Article 24), and access to essential services, including local rehabilitation programs and comprehensive habilitation services, all of which are particularly relevant for people with visual impairments (PVI) (Article 25 and 26). Article 27 reinforce workplace inclusion by prohibiting discrimination and mandating reasonable accommodations. The legal frameworks emphasize the specific needs such as vision rehabilitation and orientation and mobility (O&M) training as critical to fostering independence and full participation in society [9]. These commitments are further reinforced by national legislation, notably the General Law on Person with Disabilities (Law No. 29973, 2012) [10] and its implementing regulation, Supreme Decree No. 002-2014-MIMP [11].
Vision rehabilitation is a range of services aiming to maintain, improve or restore the quality of life and the independence, prevent accidents and falls and improve or help to maintain the physical and psychological well-being of PVI [12]. Action plan 2014-2019 on eye health included vision rehabilitation as an essential part of a person-centered health care [13]. These services should be accessible to any person with a visual impairment regardless of age and whether the person lives in a rural or in an urban area, given by a sufficient number of trained professionals, ideally provided by a government subsidizing them to ensure equity [14]. As for eye care services, they should meet the same criteria as the vision rehabilitation services. If free services are impossible, they should be affordable or integrated in a universal health coverage plan and be accessible without delay for emergencies, or within a reasonable time frame for a visual assessment [12]. Eye care services are crucial to collect data on the prevalence of VI, to prevent avoidable blindness, to correct refractive errors causing mild to severe VI, to treat curable diseases, or even to monitor degenerative and life-long diseases [12]. Both eye care and vision rehabilitation services should be integrated into general health systems [15].
Unfortunately, the research available on eye care services in Peru is scarce, even when looking in broader research over Latin America, or globally, whereas vision rehabilitation studies are practically inexistent. A Hong et al. (2016) study on universal eye health in Latin America states that Peru has a ratio of 3.13 ophthalmologists per 100,000 inhabitants, which places it below the regional average of 5.2 per 100,000 inhabitants. Moreover, according to the same study, Peru is the antepenultimate most unequal Latin American country relating to the regional repartition of ophthalmologists [16], who tend to settle in the more densely regions and cities because of the better salaries and career opportunities they offer [17, 18]. The biggest and financially most attractive Peruvian cities are found along the coast, while the mountains and the jungle, poorer and less densely populated, have a diminished access to health care in general, and by the very fact to eye care services [19]. Lima alone is home to 38% of the Peruvian population with a VI [5]. In their study about the determinants of eye care service utilization in Peru, Barrenechea-Pulache et al. (2022) [19] found that the population who used the most these services was generally wealthier and more educated than the one who did not. Indeed, people with a lower education level tended to be unaware of possible treatments for their diseases, or even reluctant to them. The authors also noted that if people benefiting from a health insurance (i.e. ESSALUD) were more inclined to use the eye care services than the ones who were unprotected, more than 50% of the ensured did not access to them because of various accessibility difficulties [19].
Little is known about the state of vision rehabilitation in Peru. According to Chiang et al. (2011) Peru has a low vision service coverage between 11% and 50% [14]. Between 50 and 99 primary research studies have been conducted on vision and eye health in Peru between 2000 and 2019, which places the country in the second to the last category [12]. Such a mapping of the state of vision rehabilitation research is not available. On the aspect of vision rehabilitation services, Chiang et al., (2011) states that, as well as for the prevalence of VI and blindness, the difficulties to understand the increasing need are due to insufficient systematic data [12]. Taking into account the person-centered approach supported by the World Health Organization (WHO), vision rehabilitation services should be integrated directly in the eye health services and be more accessible to the people who need it. It is also crucial that PVI receive a service continuum including help for cultural, but also social participation [12]. Scientific literature is generally lacking on the state of eye health for Peru, and particularly vision rehabilitation. The studies that do exist on this last aspect do not allow a precise knowledge on Peru itself, and use a survey administrated to experts, which certainly represents the clinical perspective of the visual impairments but is not person-centered. The present exploratory study wishes to contribute to expose the perspective and the day-to-day reality of the Peruvians with a visual impairment, as recommended by the World Report on Vision [15], as well as to offer the perspective of educational, rehabilitation and medical professionals to be able to compare their insights and perspectives, intended to be as representative as possible. It also addresses the first and the second objective of WHO’s Global Action plan 2014-2019 on eye health. This study aims to generate evidence of the magnitude of eye care services and their effectiveness, exploring in the interview guide the barriers faced in accessing health care, rehabilitation, support and assistance, their environments, education and employment. To address this aim, the study explores the following research questions: a) What are the perceptions of vision rehabilitation services received in Peru by the people with visual impairments? b) What are the perceptions of accessibility for people with a visual impairment regarding barriers associated with education, independent mobility, and activities of daily living? and c) What are the perceptions regarding government assistance programs provided to people with visual impairments?
The overall goal of the study is to develop professional recommendations to improve the social participation and well-being of PVI, based on the input from medical, educational, and rehabilitation professionals, as well as people with a visual impairment in Peru.
2. Materials and Methods
2.1. Recruitment and sampling
All participants were recruited through personal and professional contacts in the area between July and November 2024. In addition, anyone who wished could distribute the invitation to their friends, colleagues, or acquaintances who are eligible, was encouraged to do so. Thus, creating a "snowball effect" that expands the sample and allows for the recruitment of more participants [20]. Purposive sampling was performed to recruit and select a diversity of participants in different areas of the country to collect information from a wider area [21]. Recruitment continued until data saturation was obtained for the group of professionals and PVI.
2.2. Eligibility criteria and ethical considerations
The participants were categorized according to their professional status and personal experience. For PVI, they were required to be at least 18 years old and self-identify as having an irreversible visual impairment that was diagnosed at least one year ago that causes an incapacity in their ability to perform activities of daily living. Participants that were professionals working with PVI (in the areas of medicine, education, or rehabilitation) we required to self-identify as a professional that is currently working, has worked in the field for at least one year, and has contact with PVI at least monthly. Professionals with visual impairments were interviewed based on their professional expertise and not their personal experience during the interviews. The study was conducted in accordance with the declaration of Helsinki. The ethics approval was obtained from the Comité d’Éthique de la Recherche Clinique (CERC) of the Université de Montréal (# 2024-5924).
2.3. Procedure
To better understand the perceptions relating to realities of PVI, a qualitative research study using in-depth semi-structured interviews was conducted. Members of the community living with visual impairments, medical and rehabilitation practitioners, as well as educational staff for students with visual impairments were interviewed by one member of the research team on questions related to each of the following subjects: assistive devices, vision rehabilitation services, government assistance programs, accessibility for the visually impaired, and eye care services (see Appendix for additional information). Participants were requested to respond to each of the questions to the best of their current knowledge. There was no time limit placed on answers to any of the questions. The interview was recorded on the Zoom platform for later analysis.
2.4. Analysis
Interviews were conducted privately by the authors, with each session lasting between 30 to 60 minutes. Upon completion, the recordings were securely stored on a password-protected drive. The interview data were transcribed using Descript, an AI-powered transcription application. The transcripts were then uploaded for further processing and MAXQDA Analytics Pro 24 [22] for data analysis. Data coding was performed by one researcher, with the entire process and findings reviewed collaboratively by all authors to ensure accuracy and consistency.
3. Results
3.1. Sociodemographic characteristics of participants
Twenty-nine participants aged 20 to 70 (19M 10F) were recruited from different areas of Peru. Three eye care professionals were ophthalmologists while one was a specialist in rehabilitation. Educators interviewed were all working in the rehabilitation centers. Seven participants self-identified as having low vision with medical diagnoses and 12 as functionally blind. Additional demographic information can be found in Table 1.
3.2Assistive Devices
The use of assistive devices plays a crucial role in enhancing the independence of PVI. Participants responded to questions related to payment structures, access, and commonly used assistive devices; Table 2 highlights the top 3-4 codes from all groups. The findings reveal that the most frequently used devices among participants are white canes and smartphones, with 82% of PVI in Peru relying on these tools. White canes are typically acquired through donations, while smartphones are purchased by participants using their own resources. Notably, all blind participants reported using smartphones and computers equipped with applications such as JAWS, Envision, Lazarillo, and others. These tools enable effective communication and accessibility, as evidenced by their ability to seamlessly participate in Zoom interviews. Interestingly, only 9% of participants indicated that the government provides assistive devices, primarily tools for educational purposes such as Braille slates, styluses, and abacuses used in schools. Eighty-three percent of rehabilitation & education professionals (R&E) mentioned that assistive devices such as the white cane is through donations. Medical professionals also mention that the white cane is the principal assistive device used by PVI and this device needs to be prescribed to get it from the government health practitioner. Additional information is shown in Table 2 below.
3.3. Vision Rehabilitation Services
Vision rehabilitation services (VRS) are among the most critical benefits that PVI should receive from the government. This right is enshrined in Law N° 29973 [10] and Supreme Decree N° 002-2014-MIMP [11]. Participants responded to questions related to the payment structure, access and professionals in VRS. Our findings reveal that BP and MP identified the presence of the two public VRS such as the Social Health Program (ESSALUD) and the Centers for Basic Special Education (CEBES) as well as the private Rehabilitation Center for the Blind of Lima. LV identified the CEBES while R&E identified only the CEBES and CERCIL. Regarding the access to VRS, both BP and R&E have highlighted the disparities between rural and urban areas due to the centralization of the VRS, the reliance of personal support network and the dependence on referrals to access those services. When we asked about the professionals in the VRS, both BP and R&E identified key components including O&M training, braille education, computer skills instruction, and activities of daily living. However, despite these critical services, 83% of participants with low vision reported a lack of awareness about the availability of VRS.
Interestingly, MP emphasized the prevalence of non-functional rehabilitation services for patients with low vision, with 100% of respondents acknowledging this issue. Additional information is shown in Table 3 below.
3.4. Government Assistance Programs
Government assistance programs have a direct impact on PVI. Indeed, these programs could enhance social inclusion through education and promoting economic independence. Participants responded to questions regarding government assistance for work, education, transportation, and financial needs. The primary themes from these four important topics to improves PVI quality of life is shown in Table 4 below.
3.4.1 Employment
Our findings reveal that BP and R&E highlight the presence of two institutions established to supporting PVI in Peru: 1) The National Council for Disability (CONADIS) and 2) The Municipal Office for the Care of People with Disabilities (OMAPED). However, out of 7 LV respondents, only one was aware of CONADIS. Indeed, the majority of LV participants demonstrated limited knowledge about these institutions. In addition, BP, R&E and MP mentioned that within the government there is a program aimed at assisting people with disabilities in the labour market. Despite this, 41% of respondents (specifically BP and R&E) criticized the inefficiency of the system in delivering effective support to people with disabilities, including PVI. Below are some stories shared by participants:
R&E4: The problem is that no one enforces it, and no one complies with it. Programs aren’t implemented because, I believe, the people in charge of these offices don’t understand the work; they don’t know what it’s like to work with people with disabilities. Their only perspective—most of them, though not all—is that a person with a disability is someone who is there to receive a donation or support.
BP2: What is the approach they take? Very well, here’s the job placement office. "Come, leave your résumé, and we’ll call you," and it never happens. For them, that’s all, right? And no, no, they are not fulfilling the process of readaptation, real relocation, the four R’s, which is part of the International Labour Organization, Convention 159.
BP8: The law says that 5% of the working population in a public institution must be a person with a disability and 3% of workers in a private institution that has more than 50 workers must be people with a disability. But it is not fulfilled either. Here in Ayacucho, no public institution complies, for example, with this mandate that should be mandatory, they do not comply.
LV6: I've heard about CONADIS because my sister worked there for a while, but... more, I don't know. I only know that it's the institution that helps people with disabilities.
3.4.2 Education
Peru has ratified international agreements such as the UN Convention on the Rights of Persons with Disabilities with emphasizes inclusive education. Our study shows that 50% of all participants recognize that inclusive education is being implemented by the government programs, but the transition is challenging. Thus, 50% of all participants reveal that there is a lack of program supporting the education and 27% mention that lack of teacher preparation is the main issue during this transition. Our results also indicate that LV and MP are the groups with lack of knowledge about the government assistance programs aimed to the inclusive education. Notably, our results also show that only R&E know about the program “Support Service and Advice for the attention of Special Educational needs”, that was stablished to support and accompaniment to the PVI in the inclusive schools. Here there are some arguments mentioned by the participants:
BP8: For example, allocating a budget for educational institutions to be accessible to people with disabilities, including people with visual disabilities. When a parent takes a visually impaired child to school to register, they are rejected. Why? Because many times it is not because they are bad, but because of the teacher. They are afraid of assuming that responsibility because they are not prepared.
R&E3: …a specific law for the inclusion of children with disabilities in regular schools. There is a budget, which is budget (106) of the Ministry of Education. This is supposed to provide the supplies such as cane devices, the strips, braille machines, but that is not coming, this is still not being implemented in an organized or coordinated manner.
R&E4: Now [PVI] have participation or are physically included in the schools in their area, but I consider that the development and skills are not being given to them in regular schools because there is no material and there are not yet enough prepared teachers.
3.4.3 Transport
Transport for PVI in Peru is also supported by the law. Indeed, the law 29973 mandates that public transportation systems must be accessible to all individuals, including those with VI [10]. 75% of all participants have knowledge about the benefit of the free public transportation for PVI. Notably, 75% and 55% mentioned that there is non-compliance with the regulations and there is a lack of respect from drivers, respectively. Below are some comments from participants:
BP1: It is said that we have the benefit of, for example, not being charged for the fare when we take public transport. However, there are certain drivers who do not respect this regulation and demand that we pay for it even if we have a card issued by CONADIS.
BP4: Oh? You don’t have fare? Then just get off. There’s a sense of disdain. If you can’t pay, it’s that extreme. It’s not accepted by the transport operators or fare collectors because they lack education. And basically, they don’t have a family member with a disability. Because if you don’t have a family member with a disability, you won’t understand. Why? Because that’s just how the culture is, unfortunately.
LV3: Well, there are many people who, when you show your yellow card to the collectors, the driver gives you a dirty look, they want to get you off, they even hit you. Now, every time I get on public transport, I pay.
R&E1: For example, when you have the yellow card, you are entitled to free passage, but it is not fulfilled. And, for example, the user gets on a bus, and you show them your card, they do not pick you up on the next ride.
R&E2: It's a question of awareness. There are some people who are more aware than others. We cannot generalize, because there are some who do respect the yellow card and there are others who do not, they do not give the opportunity.
3.4.4 Financial needs
Although Peru is still considered a low-income country, the government provides financial assistance to people with disabilities, including those with visual impairments, through the CONTIGO program. Seventy-seven percent of participants revealed that are aware of the financial assistance offered by the CONTIGO program. Among them, 54% identified extreme poverty and severe disability as the primary eligibility criteria for accessing this benefit and 15% mentioned that there is no financial aid for PVI. Interestingly, none of the LV or BP mentioned to receiving financial aid from the government.
3.5 Accessibility for the visually impaired
Accessibility for PVI is undoubtedly a critical component of Peru’s efforts toward greater inclusivity. In this study, we explored the barriers faced by PVI in accessing education and achieving independence both indoors and outdoors. The results reveal that BP identify education as a significant challenge, primarily due to inadequate teacher training (45%). Additionally, social stigmatization (27%) and unequal educational opportunities (27%) are seen as major barriers to accessing education. Similarly, LV and R&E also highlighted the lack of teacher preparation as a key obstacle (67%). In contrast, MP pointed to economic limitations as the primary barrier preventing PVI from accessing education (100%). Orientation and mobility are recognized as essential yet challenging skills for PVI to attain independence. When discussing barriers to indoor and outdoor navigation, the findings demonstrate considerable alignment among all four groups surveyed. Eighty-three percent of BP revealed dependence on others, 75% mentioned presence of street vendors and 58% said that there is absence of inclusive areas. Similarly, 86% of LV respondents also mentioned dependence on others while 42% declare lack of social awareness. MP also revealed that non-empathetic pedestrians and a lack of social awareness are the most prominent barriers that PVI face while they are indoors or outdoors. Here are some quotes mentioned:
BP6: It is the fear of teaching a person with visual impairment, because they do not have the resources or simply because they do not want to do it.
BP11: Teachers should be prepared to care for young people with disabilities. There are many difficulties in this regard, I was even asked: how am I going to evaluate you? So, higher level teachers must be strengthened in this area, so that they are prepared.
LV1: The university does not have a system for her [visually impaired person] and they have verbally asked her to leave, to find another option.
R&E4: Teachers have not assumed this responsibility. This is because the authorities at universities or institutes have not become aware of this responsibility.
BP4: It is believed that visually impaired people are not productive. I mean, why am I going to hire someone? How are they going to get around, how are they going to do it? No, I'd rather hire someone who can see." And that also happens in the family "poor little girl, I have to take care of the poor thing" and they don't let her do anything.
BP12: The issue of bullying is terrible. I have two or three friends who stopped studying because the bullying was terrible.
LV6: They are not empathetic at all. I even stopped having friends.
MP1: Health systems are imposing the use of elevators, ramps. In my opinion it is quite important, yes. But exclusively for a patient with visual impairment… There is none.
BP3: They [transport services] should have staff who are willing to help when they see a person with visual disability.
BP8: For example, in some streets they put the motorcycle in the middle of the sidewalk, or the car has a tire pushed up onto the sidewalk. I don't know why they do that. You go with your white cane, and you crash into that. It's a lack of sensitivity from the part of the population itself.
R&E2: Raising awareness and training drivers in all respects, with more stringent regulations or so that they also feel that it will affect them in some way if they do not comply.
Notably, all groups emphasized the importance of public education as a critical factor in supporting daily living activities and fostering greater independence for PVI.

Table 5.
Accessibility for the visually impaired
| Thematic | Codes | BP | LV | R&E | MP |
| Frequency (%) | |||||
| Education | Inequality of educational opportunities | 3(25) | 2(29) | 1(17) | |
| Social stigmatization | 3(25) | 1(14) | 3(50) | ||
| Economic barriers | 2(17) | 1(17) | 1(25) | ||
| Lack of teacher preparation | 5(42) | 2(29) | 4(67) | ||
| Indoor- | Lack of support staff | 2(33) | |||
| Outdoors | Centralism and marginalization | 1(25) | |||
| Obstacles on the road | 4(33) | 4(67) | |||
| Deteriorated or inadequate sidewalks | 6(50) | 1(14) | 4(67) | ||
| Lack of social awareness | 6(50) | 3(43) | 2(33) | 2(50) | |
| Dependence on others | 10(83) | 6(86) | 3(50) | ||
| Presence of street vendors | 9(75) | 1(14) | 5(83) | ||
| No tactile markings | 4(33) | 1(14) | 2(33) | 2(50) | |
| Non-inclusive areas | 7(58) | 4(67) | 1(25) | ||
| Lack of elevator announcements | 2(17) | 1(14) | 2(33) | 1(25) | |
| Non empathetic pedestrians | 9(75) | 3(43) | 1(17) | 2(50) | |
| Suggestions | Compliance with legislation | 4(33) | 1(14) | 1(17) | |
| Public education (sensitization) | 7(58) | 4(57) | 5(83) | 2(50) | |
| Training of public officials | 3(25) | 2(29) | 4(67) | 2(50) | |
| Structural change | 3(25) | 1(14) | 2(33) | ||
| Inclusive design (Architecture) | 6(50) | 2(29) | 3(50) | 1(25) | |
| Street signage | 3(25) | 2(29) | |||
BP: Blind participants, LV: Low vision participants, R&E: Rehabilitators practitioners/educators, MP: Medical professionals.
Table 6.
Eye Care Services
| Thematic | Codes | BP | LV | R&E | MP |
| Frequency (%) | |||||
| Payment | ESSALUD | 2(17) | 3(43) | 2(33) | 1(25) |
| structure | MINSA (INO, IRO) | 8(67) | 3(43) | 5(83) | 2(50) |
| Personal payment (Private clinics) | 6(50) | 5(71) | 3(50) | 2(50) | |
| Access | By appointment | 5(42) | 5(71) | 3(50) | |
| Geographic gap (centralized) | 3(25) | 1(14) | 1(17) | ||
| Professionals | Low Vision | 2(50) | |||
| Ophthalmologist | 12(100) | 7(100) | 6(100) | 4(100) | |
| Optometrists | 3(25) | 2(29) | 2(33) | ||
BP: Blind participants, LV: Low Vision participants, R&E: Rehabilitators practitioners/educators, MP: medical professionals.
3.6. Eye Care Services
PVI face significant challenges accessing eye care services due to several reasons, such as geographic and economical barriers [23]. All participants revealed that ophthalmologists are the professionals in charge of eye care. LV (29%) and R&E (33%) mentioned the presence of optometrists also as professionals involved in the eye care services. Interestingly, MP (67%) mentioned the presence of low vision professionals who are taking care of non-functional rehabilitation.
Regarding the payment structure and access to eye care services, all participants acknowledged the availability of eye care services across various healthcare providers, including hospitals under the Ministry of Health (such as the National and Regional Institute de Ophthalmology), ESSALUD facilities, and the private clinics. However, access to these services varied in terms of administrative processes and geographic distribution.
Additionally, 42% of BP respondents, 83% of LV respondents, and 50% of R&E respondents noted that scheduling an appointment was necessary to consult an ophthalmologist. Of interest, 25% of BP respondents, 17% of LV respondents, and 17% of R&E respondents highlighted that specialized eye care services were predominantly concentrated in Lima, the country’s capital.
3.7. Differences and similarities between LV and BP perspectives
Since BP and LV are the main user of the VRS and the government assistance programs, we investigated the differences and similarities between both groups. Using the two-cases model from MAXQDA, our results show substantial differences and similarities between BP and LVP. As seen in Figure 1, our results indicate that unlike BP, interviewed LV reported very little knowledge about the VRS and the government assistance programs. Of interest, several perspectives (codes) often overlap; however, for eye care services there are no substantial differences.
4. Discussion
This qualitative research explored different perspectives about how is living with visual impairment in Peru. Interviewing four different groups allowed us to identify differences regarding the challenges faced by the PVI. Interestingly, blind participants and those with low vision have different perspectives about the programs from government and the accessibility of PVI.
Assistive devices
The emergence of new technologies has shown significant potential to improve the quality of life for PVI [24-26]. Our study shows that the white cane is an important tool in orientation and mobility with high prevalence of use among BP; however, LV are reluctant to use it, which is likely due to the stigma leading to embarrassment and concern about being stared at [27]. On the other hand, our findings reveal that 100% of BP reported using smartphones and applications, highlighting their positive impact on activities of daily life. Indeed, smartphones offer the crucial advantages of accessibility and versatility compared to dedicated assistive devices [28]; however, the use of these tools remains largely confined to applications related to reading and orientation. Furthermore, the accessibility of assistive technologies is hindered by their high costs, further limiting widespread adoption [29, 30]. Recently, the Global Education Monitoring Report team from UNESCO mention that in Latin American and the Caribbean, including Peru, the assistive technology is often not available due to lack of resources or lack of training [31], which restricts their ability of PVI to effectively integrate these tools into their daily routines. While assistive devices continue to evolve, offering numerous benefits that could significantly impact the quality of life [29, 32], persistent economic, social, and infrastructural barriers must be addressed to ensure equitable access and utilization.
Vision Rehabilitation Services
Like in other countries, vision rehabilitation services in Peru are aimed at improving the quality of life of PVI and these services include training in the use of devices and technology, training in O&M skills, support in daily life activities, etc. [33]. Those interviewed mentioned that these services are provided mainly by the Social Health Insurance (ESSALUD), CERCIL (Rehabilitation center for Blind) and the Ministry of Education through the Special Basic Education Centers (CREBES). CERCIL is the center that offers the most complete rehabilitation program, yet it is private and only available in Lima. The Ministry of Health and ESSALUD do not offer functional rehabilitation, and this task is achieved by the Ministry of Education; however, there are challenges to reach PVI, particularly in rural and undeserved areas. Our study also indicates that the access to the VRS is through referrals. However, more studies are needed in order to understand how referrals influence services to PVI. Interestingly, similar to studies reported from North America and the United Kingdom, where VRS are more available, our results also indicate that people with low vision reported lack of awareness of VRS and refusal to assist to the VRS due to a perceived lacks of need, social considerations among others [28, 34]
Our participants report that CERCIL have professionals trained to address the diverse needs of PVI. These professionals in the government receive experience-based training but are not certified or specialists. Professionals as well as rehabilitation services are needed to expand across the country to ensure equitable distribution of services. Collaboration between government agencies, educational institutions, and NGOs is essential to strengthen the field of visual rehabilitation in Peru.
Government Assistance programs
The Peruvian government has implemented several assistance program and policies to support PVI, aiming to improve their quality of life, promote inclusive education and ensure access to essential services [10, 35]. These programs are primarily managed by the Ministry of Health (MINSA), Ministry of Education (MINEDU) and the ministry of Development and Social Inclusion (MIDIS). Our results indicate that people with blindness and low vision know about these assistance programs to promote job opportunities; however, they mention these programs are still inefficient. Similar results were obtained regarding available programs for transportation, education and financial assistance. Unfortunately, there are no studies or data showing all the challenges that contribute to their inefficiency. Several likely reasons impeding a good outcome of these programs including limited resources and gaps in implementation (bureaucracy), centralization of the programs, lack of specialized training and professionals, stigma and social exclusion, as well as inadequate monitoring and evaluation. Through a systematic approach in addressing these challenges, the Peruvian government may improve the effectiveness of the programs. Collaborations with NGOs and private organizations could further promote the achievement of these goals.
Accessibility for the visually impaired
Accessibility for PVI is part of the General Law for Persons with Disabilities. This law mandates equal opportunities and accessibility for PVI. In addition, there is a National Accessibility Plan 2018-2025 [36]. Our study shows that lack of teacher preparation is the main barrier to access to an inclusive education according to the BP, LV and R&E. Similar results were reported by the Ministry of Education (2016) [37] the Ombudsman [38] and Valdivieso (2020) [39]. Research to improve inclusive education is almost non-existent in Peru despite that working with the school community to improve school climate for inclusive education had positive effects on the inclusion [39]. Interestingly in 2006, the Ministry of Education created the “Support Service and Advice for the attention of Special Educational needs” (SAANEE) to promote inclusive education for students with disabilities, including those with visual impairments. SAANEE operates within the framework of Peru’s inclusive education policy and provides specialized support to students, teachers and families [40]. Thus, it has been reported that in 2015 about 1940 teachers received virtual training courses on the teaching and learning process for children with visual disabilities [29]. Nevertheless, the implementation of the inclusive education is still challenging [39]. Indeed, our results indicate that the lack of teacher preparation and support programs, social stigmatization and inequalities of educational opportunities for PVI are among the most frequent codes reported by BP, R&E and MP. We speculate that increased funding and greater awareness of its services as well as providing adequate monitoring of the indicators on inclusive education would enhance its adoption [38]. Moreover, we agree with the report by the World Bank about teachers need structural support including better salaries and working conditions especially in rural areas [29].
Indoor and outdoor mobility are very critical for PVI with several impacts including physical, social and mental health [30]. Independent mobility also has a tremendous impact for social interactions and performing daily activities [41, 42]. Our results indicate that BP, LV, and R&E report the necessity or dependence of other to navigate safely both indoors and outdoors. Indeed, several accessibility features should be modified to promote independence of PVI such as additional braille signage, incorporation of tactile markings, improving sidewalks conditions, location of street vendors, and most importantly improving social awareness. In Peru, physical accessibility for PVI, both indoors and outdoors, remains a significant challenge despite legal frameworks and efforts to promote inclusion. Participants in our study suggest that accessibility challenges include compliance with the legislation, inclusive design and structural changes.
Interestingly, when we asked the participants about suggestions to improve the accessibility of PVI, all groups highlight sensitization (education to the society). Indeed, attitudinal barriers have a great influence on personal development and are associated with stigma, discrimination and mistreatment, which are considered more harmful that physical barriers [43, 44]. Previous studies have reported that PVI who has experienced discrimination were more likely to report depression and poor quality of life [45] with negative impact in social interactions [46]. Based on our results and previous studies is imperative to promote strategies to improve awareness and educate the general public to create a more equitable society for all.
Eye care services
Our results indicate that all groups acknowledge the existence of public and private institution providing eye care services. However, PVI face significant challenges in accessing these services, particularly those residing in rural areas, as highlighted by BP, LV and R&E. In fact, it has been reported that the socioeconomic status of many families in the rural areas poses a major barrier, severely limiting their access to that affect the access to the healthcare services [23]. In this context, it has been suggested to create blindness prevention programs targeting people with low socioeconomic status in the Peruvian Amazon [47]. Another point that we would like to highlight is the role of the optometrist in Peru. According to our interviews, unlike developing countries, the optometrists are still facing some challenges such as limited training opportunities and a lack of public awareness about their profession.
Limitations
Though the participants are from different cities across the country, it is likely that most of the responses do not represent the reality in different communities, specifically in rural areas. Over the course of this study, we interviewed persons from different groups, and we encourage a diversity of responses. In this context, the views and opinion expressed do not necessarily reflect those of all individuals in each category.
5. Conclusions
Visual disability is the most frequent disability in Peru and investing in eye health services could have positive benefits in the economic development [48]. Our results reveal that multiple systemic barriers severely hinder the inclusion of PVI into Peruvian society. In fact, many of the barriers highlighted are principally societal, and touch on multiple aspects of everyday life of PVI, including the use of assistive devices, education, employment, and transportation. Though medical professionals are aware of some of the realities of PVI, their knowledge about many of these subjects was more limited than the other groups interviewed. Individuals with lived experience, both those with low vision and blindness, should be consulted, along with rehabilitation professionals and educators to ensure that investments to improve the lives of PVI are well-targeted. A targeted approach to minimizing their impact on the everyday lives of PVI would create more educational and economic opportunities for this vulnerable population. Though this study gives an overview of living with a visual impairment in Peru, further research should be done in each of these areas to examine implementation of services to improve the lives of PVI and promote their full potential.
Author Contributions
J.P.N. and J.L.C.V. conceptualized and planned the study. C.L. and J.L.C.V. participated in data collection (interviews). J.L.C.V. and J.N participated in the data analysis. J.L.C.V., C.L. and J.N wrote the manuscript. J.N. Funding acquisition. All author reviewed and approved the manuscript.
Funding
The present study was supported by a grant from the Fonds de recherche Québec – Santé- Vision Sciences research Network (PP 2324-02#; J.P.N).
Institutional Review Board Statement
The study was conducted in accordance with the declaration of Helsinki. The ethics approval was obtained from the Comité d’Éthique de la Recherche Clinique (CERC) of the Université de Montréal (# 2024-5924).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data generated during and/or analyzed during the current study are not publicly available. These data include participant identifying information that is sensitive and confidential but available upon reasonable request from the corresponding authors.
Acknowledgments
The authors would like to give special thanks to Federacion de Ciegos del Peru for their valuable support.
Conflicts of Interest
The authors declare no competing interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BP | Blind participant |
| CERCIL | Rehabilitation center for Blind |
| CONADIS | National Council for Disability |
| CREBES | Special Basic Education Centers |
| CRPD | Convention on the Rights of Persons with Disabilities |
| ESSALUD | Social Health Insurance |
| LV | Low vision participant |
| MIDIS | Development and Social Inclusion |
| MINEDU | Ministry of Education |
| MINSA | Ministry of Health |
| MP | Medical professional |
| O&M | Orientation & Mobility |
| OMAPED | Municipal Office for the Care of People with Disabilities |
| PVI | Person with visual impairment |
| R&E | Rehabilitation practitioners/Educators |
| SAANEE | Support Service and Advice for the attention of Special Educational needs |
| UN | United Nations |
| VI | Visual impairment |
| WHO | World Health Organization |
Appendix
Demographic questions
Name:
Date of birth:
Gender:
Place of residence:
Professional title:
Place of work:
Years of experience (only for medical, rehab, and educational professional categories of participants):
Visual diagnosis, if known (only for people with visual impairments category of participants):
Age at diagnosis:
Level of education:
Date:
Interview start time:
Interview end time:
Structured interview questions
Assistive devices
Which assistive devices are available to people living with blindness or low vision?
How do people living with blindness or low vision procure these devices?
What is the payment structure for these devices?
Vision rehabilitation services
What professionals are available to offer vision rehabilitation services?
How do people living with visual impairment get access to these professionals?
What is the payment structure for receiving these services?
Government assistance programs
What government programs are available to permit people with visual impairments to respond to their financial needs?
What government programs are available to assist with transportation?
What government programs are available to assist in promoting education or work for people with visual impairments?
Accessibility for the visually impaired
Please describe some accessibility barriers for people with visual impairments when traveling indoors
Please describe accessibility barriers for people with visual impairments when traveling outdoors
What would you suggest to improve accessibility for people living with visual impairments?
What are some barriers that a person with a visual impairment may encounter to access higher education?
Eye care services
What professionals are available to offer eye care services to people with visual impairments?
How do people living with visual impairment get access to these professionals?
What is the payment structure for receiving these services?
References
- IAPB. Country Map & Estimates of Vision Loss. Peru. 2025 [cited 2025 March 3rd]; Available from: https://www.iapb.org/learn/vision-atlas/magnitude-and-projections/countries/peru/.
- Organismo Andino de Salud, Diagnostico situacional de la Salud Ocular por curso de vida en la region andina., O.A.d.S.C.H. Unanue, Editor. 2022: Lima. Peru.
- Bourne, R. , et al., Trends in prevalence of blindness and distance and near vision impairment over 30 years: an analysis for the Global Burden of Disease Study. The Lancet Global Health, 2021, 9, e130–e143. [Google Scholar] [CrossRef] [PubMed]
- Gobierno del Peru. Principales enfermedades de la vista. 2024a [cited 2025 Jan 15]; Available from: https://www.gob.pe/ayc/25514-principales-enfermedades-de-la-vista.
- Bergamino Varillas, J.P. , Discapacidad visual, competencias y empleabilidad en el Perú. Revista De Ciencias De La Gestión, 2018, 3, 84–108. [Google Scholar] [CrossRef]
- OHCHR, Convention on the Rights of Persons with Disabilities. 2024b.
- Parliament of Canada, The United Nations Convention on the Rights of Persons with Disabilities: An Overview, HiIIStudies, Editor. 2021, Parliament of Canada.
- OHCHR. Status of Ratification Interactive Dashboard. 2024a [cited 2024 October 15]; Available from: https://indicators.ohchr.org/.
- Gobierno del Peru, Constitucion Politica del Peru. 2024b.
- Ley N° 29973, Ley General de la Persona con Discapacidad (Law N° 29973, General Law on Person with Disabilities 2012: Lima. Peru.
- Decreto Legislativo N° 002-2014-MIMP, Decreto Supremo N° 002-2014-MIMP. Reglamento de la Ley N° 29973, Ley General de la Persona con Discapacidad" ( Supreme Decree N° 002-2014-MIMP, “Regulations of Law No. 29973, General Law on Persons with Disabilities). 2014.
- Burton, M.J. , et al., The Lancet Global Health Commission on Global Eye Health: vision beyond 2020. The Lancet Global Health, 2021, 9, e489–e551. [Google Scholar] [CrossRef] [PubMed]
- WHO, Universal eye health: a global action plan 2014-2019, W.H. Organization, Editor. 2013.
- Chiang, P.P. , et al., A global survey of low vision service provision. Ophthalmic Epidemiol, 2011, 18, 109–21. [Google Scholar] [CrossRef] [PubMed]
- WHO, World report on vision, WHO, Editor. 2019, WHO.
- Hong, H. , et al., The Challenge of Universal Eye Health in Latin America: distributive inequality of ophthalmologists in 14 countries. BMJ Open, 2016, 6, e012819. [Google Scholar] [CrossRef]
- Toyabe, S.-i. , Trend in geographic distribution of physicians in Japan. International Journal for Equity in Health, 2009, 8, 5. [Google Scholar] [CrossRef] [PubMed]
- Heikkilä, T.J. , et al., How do doctors choose where they want to work? – Motives for choice of current workplace among physicians registered in Finland 1977–2006. Health Policy, 2014, 114, 109–117. [Google Scholar] [CrossRef]
- Barrenechea-Pulache, A. , et al., Determinants of Eye Care Service Utilization among Peruvian Adults: Evidence from a Nationwide Household Survey. Ophthalmic Epidemiology, 2022, 29, 339–348. [Google Scholar] [CrossRef]
- Parker, C., S. Scott, and A. Geddes, Snowball sampling. SAGE research methods foundations, 2019.
- Rai, N. and B. Thapa, A study on purposive sampling method in research. Kathmandu: Kathmandu School of Law, 2015, 5, 8–15. [Google Scholar]
- VERBI Software, MAXQDA 2022 [computer software]. 2021, VERBI Software: Berlin, Germany.
- Barrenechea-Pulache, A. , et al., Determinants of Eye Care Service Utilization among Peruvian Adults: Evidence from a Nationwide Household Survey. Ophthalmic Epidemiol, 2022, 29, 339–348. [Google Scholar] [CrossRef]
- Aminparvin, H. , et al., Follow-up in low vision rehabilitation for users of assistive technology: a scoping review. Disabil Rehabil Assist Technol, 2024: p. 1-12.
- Kathiria, P. , et al., Assistive systems for visually impaired people: A survey on current requirements and advancements. Neurocomputing, 2024, 606, 128284. [Google Scholar] [CrossRef]
- Zhang, X. , et al., Advancements in Smart Wearable Mobility Aids for Visual Impairments: A Bibliometric Narrative Review. Sensors (Basel), 2024. 24(24).
- Hersh, M. , Cane use and late onset visual impairment. Technology and Disability, 2015, 27, 103–116. [Google Scholar] [CrossRef]
- Pundlik, S., P. Shivshanker, and G. Luo, Impact of Apps as Assistive Devices for Visually Impaired Persons. Annual Review of Vision Science, 2023. 9(Volume 9, 2023): p. 111-130.
- Grarcia Mora, M.E. Schwartz, and G. Freire, Disability Inclusion in Latin America and the Caribbean: A Path to Sustainable Development., W.B. Group., Editor. 2021, World Bank: Washington, DC.
- Khan, W. , et al., Outdoor mobility aid for people with visual impairment: Obstacle detection and responsive framework for the scene perception during the outdoor mobility of people with visual impairment. Expert Systems with Applications, 2023, 228, 120464. [Google Scholar] [CrossRef]
- UNESCO, Global Education Monitoring Report 2020–Latin America and the Caribbean–Inclusion and education: All means all. 2020, UNESCO.
- Hoogsteen, K.M.P. and S. Szpiro, A holistic understanding of challenges faced by people with low vision. Res Dev Disabil, 2023, 138, 104517. [Google Scholar] [CrossRef]
- Owsley, C. , et al., Characteristics of low-vision rehabilitation services in the United States. Arch Ophthalmol, 2009, 127, 681–9. [Google Scholar] [CrossRef]
- Lam, N. and S.J. Leat, Barriers to accessing low-vision care: the patient’s perspective. Canadian Journal of Ophthalmology, 2013, 48, 458–462. [Google Scholar] [CrossRef] [PubMed]
- Ley N° 30797, Ley que Promueve la Educacion Inclusiva, modifica el articulo 52 e incorpora los articulos19-A y 62-A en la Ley 28044, Ley General de Educacion. 2018: Lima. Peru.
- CONADIS, Plan Nacional de Accesibilidad 2018-2023. 2018.
- Ministerio de Educacion, Evaluación de diseño e implementación del servicio de apoyo y asesoramiento a las necesidades educativas especiales SAANEE. 2016, Government of Peru.
- Defensoria del Pueblo, El Derecho a la Educacion Inclusiva. Barreras en la implementacion de los servision educativos publicos y privados para estudiantes con disca[acidad y con otras necesidades educativas., I.D. 183, Editor. 2019: Lima-Peru.
- Valdivieso, P. , School Leaders and Inclusive Education in Peru: A Case Study of Principal Leadership in an Effective Inclusive School. International Journal of Innovative Business Strategies, 2020.
- Ministerio de Educacion, Decreto Supremo Nº 002-2005-ED. Aprueban el Reglamento de Educación Básica Especial. 2005., Goverment of Peru.
- Wilson, M. , Who Put That There: The barrier to blind and partially sighted people getting out and about. RNIB: London, UK, 2015.
- Chidiac, S.E., M. A. Reda, and G.E. Marjaba, Accessibility of the Built Environment for People with Sensory Disabilities—Review Quality and Representation of Evidence. Buildings, 2024, 14, 707. [Google Scholar] [CrossRef]
- Calle, A. López, and M. Campillay, Social Inclusion of Persons with Vision Disability: A Qualitative Systematic Review. New Trends in Qualitative Research, 2021; 70. [Google Scholar]
- Calle, A., A. Lopez, and M. Campillary, Social Inclusion of Persons with Vision Disability: A Qualitative Systematic Review. New Trends in Qualitative Research, 2021, 8, 617–629. [Google Scholar]
- Jackson, S.E. , et al., Association of Perceived Discrimination With Emotional Well-being in Older Adults With Visual Impairment. JAMA Ophthalmol, 2019, 137, 825–832. [Google Scholar] [CrossRef]
- Fraser, S. , et al., Stereotyping as a barrier to the social participation of older adults with low vision: a qualitative focus group study. BMJ Open, 2019, 9, e029940. [Google Scholar] [CrossRef]
- Nesemann, J.M. , et al., Association of vision impairment and blindness with socioeconomic status in adults 50 years and older from Alto Amazonas, Peru. Eye (Lond), 2023, 37, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Eckert, K.A. , et al., Update of a Simple Model to Calculate the Annual Global Productivity Loss Due to Blindness and Moderate and Severe Vision Impairment. Ophthalmic Epidemiology, 2023, 30, 142–150. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Two-cases model. Differences between BP and LV coding report from top to bottom. Blue: Assistive devices, Green: VRS, Yellow: Government Assistance programs, Pink: Accessibility and Red: Eye care services.
Figure 1.
Two-cases model. Differences between BP and LV coding report from top to bottom. Blue: Assistive devices, Green: VRS, Yellow: Government Assistance programs, Pink: Accessibility and Red: Eye care services.
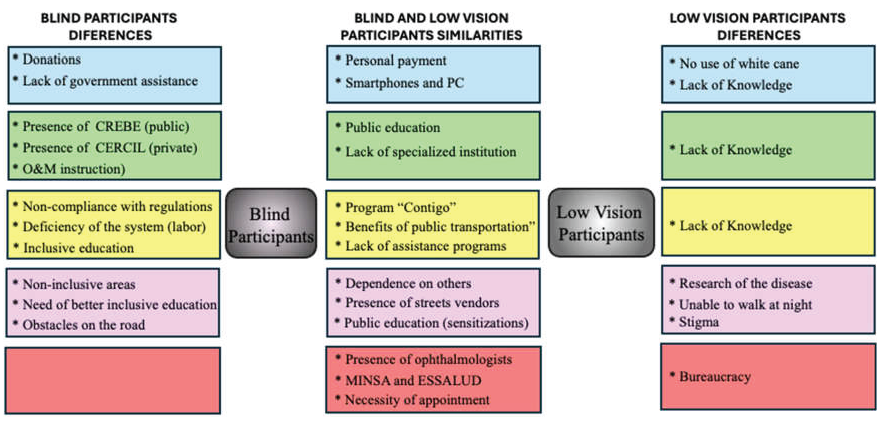
Table 1.
Sociodemographic information of participants.
| Group | ID | Age | Gender | Residence | Occupation | Visual Impairment |
| Blind | BP1 | 20 | F | Trujillo | Undergraduate student | Viral infection |
| participants | BP2 | 49 | M | Lima | Technician and law student | Retinal detachment |
| BP3 | 52 | F | Piura | Technical diploma | Congenital glaucoma | |
| BP4 | 36 | M | Ayacucho | Musician and undergraduate studies | Chronic uveitis and glaucoma | |
| BP5 | 36 | M | Trujillo | Physiotherapist | Congenital cataract, glaucoma | |
| BP6 | 33 | F | Ayacucho | Musician | Retinitis pigmentosa | |
| BP7 | 68 | M | Arequipa | Professor (retired) | Optic atrophy | |
| BP8 | 59 | M | Ayacucho | Non-concluded undergraduated studies | Retinitis pigmentosa | |
| BP9 | 39 | M | Lima | Sociologist and law student | Congenital glaucoma | |
| BP10 | 52 | M | Trujillo | Physiotherapist | ||
| BP11 | 44 | M | Juliaca | Social communicator | Optic nerve damage | |
| BP12 | 47 | M | Chimbote | Technician | Optic nerve damage | |
| Low vision | LV1 | 40 | M | Tingo Maria | Kitchen helper | Retinitis pigmentosa |
| LV2 | 41 | F | Piura | Elementary teacher | Retinitis pigmentosa | |
| LV3 | 60 | M | Piura | Electrician | Retinal detachment (OD) | |
| LV4 | 42 | M | Pucallpa | Soft beverage sales | Retinitis pigmentosa | |
| LV5 | 53 | M | Barranca | Piano teacher | Retinitis pigmentosa | |
| LV6 | 36 | F | Ayacucho | Housewife | Usher’s syndrome | |
| LV7 | 75 | F | Trujillo | Housewife | AMD, cataract | |
| Educator | R&E1 | 57 | M | Arequipa | Special education teacher | NA |
| R&E2 | 47 | F | Trujillo | High school professor | Retinitis pigmentosa | |
| R&E3 | 56 | M | Arequipa | Education and administration | Retinitis pigmentosa | |
| R&E4 | 48 | M | Arequipa | Education | Congenital glaucoma | |
| R&E5 | 57 | F | Ayacucho | Physical education | NA | |
| R&E6 | 59 | F | Chincha | Pedagogical technician | NA | |
| Medical professionals | MP1 MP2 |
55 51 |
M F |
Trujillo Lima |
MD Ophthalmologist MD Rehabilitation |
NA NA |
| MP3 | 54 | M | Lima | MD Ophthalmologist | NA | |
| MP4 | 55 | M | Lima | MD Ophthalmologist | NA |
Table 2.
Use of assistive devices.
| Thematic | Codes | BP | LV | R&E | MP |
| Frequency (%) | |||||
| Payment structure | Free materials (Insurance) | 1(25) | |||
| Free Apps | 6(50) | 3(50) | 1(25) | ||
| Free materials (Government) | 2(17) | ||||
| Personal payment | 12(100) | 1(14) | 5(83) | 2(50) | |
| Access | Prescription | 1(17) | 1(25) | ||
| Importation | 1(17) | 1(25) | |||
| Lack of Knowledge (Access) | 1(14) | ||||
| Social network or friends | 5(42) | 1(14) | 1(17) | 1(25) | |
| Lack of government assistance | 3(25) | 3(50) | 1(33) | ||
| Bureaucracy | 2(17) | 1(14) | 1(17) | ||
| Donations | 7(58) | 5(83) | |||
| Devices | Minimal use of white cane | 5(71) | |||
| Stylus | 6(50) | 3(50) | |||
| Writing slate | 5(42) | 4(67) | |||
| White cane | 12(100) | 1(14) | 6(100) | 4(100) | |
| Computers | 7(58) | 3(43) | 2(33.3) | 1(25) | |
| Smartphones | 12(100) | 3(43) | 6(100) | 2(50) | |
BP: Blind participants, LV: Low vision participants, R&E: Rehabilitators practitioners/educators, MP: Medical professionals.
Table 3.
Vision Rehabilitation Services
| Thematic | Codes | BP | LV | R&E | MP |
| Frequency (%) | |||||
| Payment structure | ESSALUD-CERP-free | 9(75) | 1(25) | ||
| CEBES-Free Education | 4(33) | 1(14) | 4(67) | 1(25) | |
| CERCIL-Private | 1(8) | 3(50) | 1(25) | ||
| Access | Rural-urban divide | 4(33) | 2(33) | ||
| Personal support networks | 3(25) | 3(50) | |||
| Referrals | 7(58) | 1(14) | 4(67) | 2(50) | |
| Professionals | Low vision department -Absence of functional rehabilitation | 1(16.7) | 4(100) | ||
| Lack of Knowledge | 6(86) | ||||
| Lack of specialized institutions | 3(25) | 1(14) | 3(50) | ||
| CREBES practitioners | 4(33) | 2(33) | |||
| Activities of daily living | 2(17) | 5(83) | |||
| O&M | 7(58) | 5(83) | |||
| Computer lessons | 4(33) | 4(67) | |||
| Braille education | 5(42) | 4(67) | |||
BP: Blind participants, LV: Low vision participants, R&E: Rehabilitators practitioners/educators, MP: Medical professionals.
Table 4.
Government Assistance Programs
| Thematic | Codes | BP | LV | R&E | MP |
| Frequency (%) | |||||
| Work | Lack of Knowledge. | 1(14) | 1(17) | 2(50) | |
| CONADIS assists people with disabilities | 2(17) | 1(14) | 3(50) | ||
| Inclusion of people with disabilities in the labor market | 6(50) | 5(83) | 1(25) | ||
| Inefficiency of the system | 7(58) | 2(33) | |||
| OMAPED | 5(42) | 1(17) | |||
| Education | Inequities in education | 1(17) | 1(25) | ||
| SAANEE support and accompaniment | 4(67) | ||||
| Lack of Knowledge | 3(43) | 1(25) | |||
| Inclusive education | 6(50) | 4(67) | 1(25) | ||
| Lack of teacher preparation | 3(25) | 3(50) | |||
| Lack of support programs | 6(50) | 1(14) | 3(50) | 1(25) | |
| Transport | Centralized | 1(8) | 2(29) | 1(17) | |
| Non-compliance with regulations | 9(75) | 6(100) | |||
| Benefit of public transport | 9(75) | 1(14) | 5(83) | ||
| Lack of respect from drivers | 7(58) | 1(14) | 3(50) | ||
| Financial | Little knowledge | 1(8) | 5(71) | 1(25) | |
| needs | Assistance for extreme poverty | 6(50) | 1(14) | 3(50) | 1(25) |
| No financial aid | 2(17) | 1(14) | 1(17) | ||
| Program “CONTIGO” | 9(75) | 3(43) | 4(67) | 1(25) | |
BP: Blind participants, LV: Low vision participants, R&E: Rehabilitators practitioners/educators, MP: Medical professionals.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



