
Submitted:
09 May 2025
Posted:
13 May 2025
You are already at the latest version
Abstract
This review recalls some ISO 15189:2022 requirements for the management of examination results and emerging alternatives for internal quality control (IQC), in relation to Italian Society of Clinical Pathology and Laboratory Medicine (SIPMeL) Recommendations Q19. We have observed phenomena of contrasting “metrological,” or rather “tracealogic,” and “statistical” approaches. SIPMeL Recommendation Q19 picks up IQC with moving average from ISO 15189, which provides for the use of moving average of patient sample results (MA). In the veterinary field the procedure of QC with repeat testing on patient samples (RPT-QC) has met with some success. The “bayesian approach” of IQC making use of the distinction between a priori probability, evidential probability (data) and a posteriori probability (IQC rules). SIPMeL recommendations Q19 strictly adhere to ISO 15189:2022 document. SIPMeL Q19 calls for abandoning the 1-2s rule, using appropriate computer tools, not only control charts, and trying to reduce false positives to very low frequencies. The alternatives to IQC with patient results and Bayesian approach are compatible with ISO 15189 and SIPMeL Q19. In contrast, the alternative with material designed for traceability, with assigned value, is not compatible with ISO standard.

Keywords:
internal quality control
; ISO 15189:2022
; SIPMeL Recommendations Q19
; metrology
; traceability
; statistics
; moving average
; patient samples
; Bayes
1. ISO 15189 and Internal Quality Control on Examination Results (IQC)
This review recalls some ISO 15189:2022 [1] requirements for the management of examination results and emerging alternatives for internal quality control, in relation to SIPMeL Recommendations Q19 [2].
ISO/TC212 WG1 “Quality and competence in the medical laboratory” worked on the revision of ISO 15189 for a long time, from October 2018 to December 2022, which is unusual in ISO tradition. The new ISO 15189 is the result of innovations requested by the ISO ISO committee for conformity assessment (CASCO) leadership and from choices made by WG1 itself [3], elaborated in the intensive preparation work with the outcome also in some compromises [4].
Chapter 7 of ISO 15189:2022 (Processes) includes subchapter 7.3 Examination Processes with clauses 7.3.1 General, 7.3.2 Verification of Examination Methods, 7.3.3 Validation of Examination Methods, 7.3.4 Assessment of Measurement Uncertainty, 7.3.5 Biological Reference Intervals and Clinical Decision Limits, 7.3.6 Documentation of Examination Procedures, and 7.3.7 Ensuring Validity of Examination Results.
Clause 7.3.7 calls for a procedure to monitor the validity of results, detect trends and changes, and apply statistical techniques, monitoring to be planned and reviewed periodically. Laboratories should remember that the same procedure in the new standard takes on a dual use: alongside monitoring of results the estimation of measurement uncertainty (MU), making use of ISO/TS 20914 guidance [5]. The SIPMeL Recommendations Q19 picked up on this and developed the operational consequences [6].
International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) with its Task Force on Global Lab Quality (TF-GLQ) group has also produced Recommendations on Internal Quality Control [7]. Unfortunately, the IFCC Recommendations deviate significantly from ISO 15189 requirements and also contain discrepancies with the scientific literature on the subject [8], eliciting criticism from several Authors [9], so we believe they are not useful for medical laboratories.
2. Alternatives for IQC: Calibration Materials?
We have observed phenomena of contrasting “metrological,” or rather “tracealogic,” and “statistical” approaches. Traceability of examination methods is a cardinal factor for quality assurance of results [10]. It makes use of two fundamental ISO documents: ISO 17511 [11] for the general case and ISO 21151 [12] for the case of methods without reference to the international system of units.
The traceability has been proposed to modify IQC procedures to entrust certified reference materials, i.e., with assigned value, with the functions of Calibration Verification as well as Acceptance/Rejection of analytical runs, collected as “IQC Component I,” leaving to “IQC Component II,” which uses third-party, switchable control materials with concentrations at clinical decision limits, the control of measurement system variability (lot-to-lot variations, measurement drifts, etc.), provision of data for calculation of measurement uncertainty, and satisfaction of allowable performance specifications [13].
This proposal has been countered with very well-founded criticisms: cost of quality control, material designed for trueness not for monitoring, violation of quality control principles, lack of fundamentals for interval of acceptability from uncertainty [14,15].
Traceability by calibration and quality control with measurement uncertainty are two very distinct fields: the former makes use of CLSI EP15 (Verification of Precision and Estimation of Bias) [16], CLSI EP32 (Metrological Traceability) [17], ISO 15189 point 6.5 (Equipment calibration and metrological traceability), ISO 17511 (metrological traceability), ISO 21151 (harmonization traceability). The second, on the other hand, is based on CLSI C24 [18] and addresses control of measurement system variability (lot-to-lot variations, measurement drifts, etc.), uses third-party control materials, with concentrations at clinical decision limits and calculated acceptability interval, provides data for calculation of measurement uncertainty and to meet allowable performance specifications, allows acceptance/rejection decisions of result runs.
3. Alternatives for IQC: Patients' Results
SIPMeL Recommendation Q19 picks up IQC with moving average from ISO 15189, which provides for the use of moving average of patient sample results (MA), explaining that the documented methods refer to MA of patient results, not QC materials, that The main advantage of IQC with MA is that it is continuous and thus offers the possibility of immediately (or at least more quickly) detecting examination problems, especially in the intervals between IQC measurements with materials.
However, MA can be labor-intensive to carefully fine-tune and optimize alarm settings [19,20,21,22]. MA has been well described with real-world experiences [23], also as Exponentially weighted moving average (EWMA) [24,25,26]. Original and interesting, but requiring significant computer resources, is the approach that uses for averaging not patient results but differences between consecutive results [27,28].
4. Alternatives to IQC: Repeated Examinations
The SIPMeL Recommendations Q19 report how in the veterinary field the procedure of QC with repeat testing on patient samples (RPT-QC) has met with some success [29,30,31,32]. Flatland and Freeman's protocol, initially tried on blood counts, involves day-after-day storage of the sample and measurement of the sample from the day before. The control result is the difference between repeated measurements, on which the same statistical QC rules can be applied, starting, for example, from 1-3s.
5. Alternatives for IQC: the “Bayesian” Approach
We have seen the so-called “bayesian approach” of IQC in an early 2015 article on coagulation examinations [33], taken up in a recent experience [34]. The proposal has something in common with the “traceological” scheme described above, but with fewer flaws and more advantages.
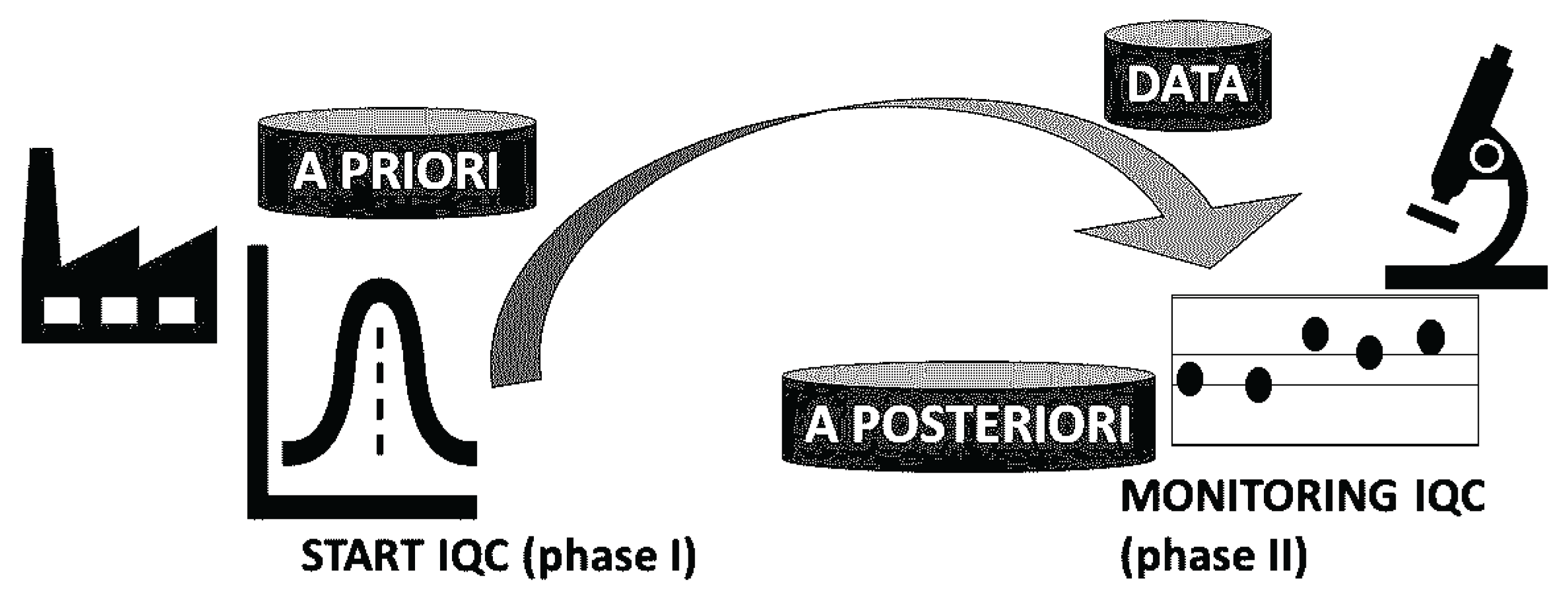
The life of an examination method in the traditional way is through development, validation, verification, initiation of IQC (phase I) and then moving on to IQC monitoring (phase II). It is not a matter of using the algebraic formula of Bayes' theorem, but of making use of the distinction between a priori probability, evidential probability (data) and a posteriori probability (IQC rules).
In practice, the initiation of IQC (phase I) contains the “a priori” probability, the monitoring of (phase II) contains the “a posteriori” probability (Figure 1). Bayesian tools use the manufacturer's available prior information along with the available data stream to derive posterior estimates between series [34].
Figure 1.
Initiation and monitoring of IQC (bayesian approach). “A priori” at the manufacturer, “data or probative” and “a posteriori” at the laboratory. Drawn based on Ref. [34].
Figure 1.
Initiation and monitoring of IQC (bayesian approach). “A priori” at the manufacturer, “data or probative” and “a posteriori” at the laboratory. Drawn based on Ref. [34].
6. SIPMeL Q19 Recommendations for IQC According to ISO 15189: Final Messages
Data on the implementation in laboratories of ISO requirements on IQC are contradictory. For example, the survey conducted by UK NEQAS in 2024 would have given compliance with the requirements for all laboratories, but the responses to the questionnaire were only 127 out of 1200, thus insignificant [38].
SIPMeL recommendations [2] strictly adhere to ISO 15189:2022 document: (7.3.7.2 (a) mandatory IQC procedure for continuous monitoring of results, based on specified criteria, of expected quality relevant to clinical decision making; (7.3.7.2 (b) IQC material selected for stability, matrix and behavior in the method close to patient samples, concentration levels close to clinical decision limits, and over the entire range of the examination method.
(7.3.7.2 c) If necessary, the material is replaced by patient results, e.g., with a moving average or percentage of samples with results below or above thresholds, comparison of patient results with an alternative validated procedure with calibration of the same or higher order (ISO 17511), repetition of retained patient samples. (7.3.7.2 g) IQC must prevent the release of patient results in the case if it does not meet the acceptability criteria, samples must be re-examined after error correction (see 7.5), including those examined since the last successful IQC event.
(7.3.7.2 d) IQC should be performed with a frequency based on the stability and robustness of the examination method and the risk of harm to the patient. (7.3.7.2 (e) Trends and variations should be identified and statistical techniques applied.
(7.3.7.2 f) IQC data should be reviewed at regular intervals. SIPMeL Q19 develops these requirements by adding reference to CLSI C24 for Sigma metrics, highlights the use of IQC for measurement uncertainty, for Point of Care Testing (POCT) services recalls only CLSI POCT07 [39], POCT08 [40], POCT14 [41], warns that materials used in the “pass/fail” mode do not comply with IQC ISO 15189 requirements, which call for monitoring, asks for justifications of alternative procedures, highlights quantitative measurements for qualitative end results and metrics for IQC generated by the process itself (as in the case of Next Generation Sequencing, NGS), proposes monitoring even for nominal qualitative or ordinal numerical results.
At the very least, SIPMeL Q19 calls for abandoning the 1-2s rule, using appropriate computer tools, only control charts, and trying to reduce false positives to very low frequencies, a few events per day, to allow in-depth investigation of the detected phenomena without significantly disrupting the operational flow of diagnostic activity.
The alternatives to IQC with patient results and Bayesian approach are compatible with ISO 15189 and SIPMeL Q19. In contrast, the alternative with material designed for tracking, with assigned value, is not compatible with ISO 15189 and SIPMeL Q19 (Table 1).

Table 1.
Alternatives to IQC, ISO 15189 and SIPMeL Q19 conformity.
| IQC Alternative | ISO 15189 and SIPMeL Q19 conformity. |
|---|---|
| Traceability material (with manufacturer) | No |
| Patient results (moving averages) | Yes |
| Repeated patient examinations | Yes |
| Bayesian approach (with manufacturer) | Yes |
Funding
This research received no external funding.
Institutional Review Board Statement
“Not applicable” for studies not involving humans or animals.
Informed Consent Statement
“Not applicable.” for studies not involving humans.
Data Availability Statement
no new data were created.
Acknowledgments
From the presentation: “The IQC: Metrologists and “Westgardians”, applying the ISO standard”. Updating Course: The Internal Quality Control (IQC): a daily tool for reliability of test results in Laboratory Medicine April 9, 2025, Ancona (Italy), Domus Stella Maris. SIPMeL Q19 Recommendations were produced by SIPMeL National Commission on Quality and Accreditation, SIPMeL Informatics Study Group, SIPMeL Study Group on Health Care Management. The author has reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ISO | International Organization for Standardization |
| SIPMeL | Italian Society of Clinical Pathology and Laboratory Medicine |
| IQC | Internal Quality Control |
| MA | Moving Average |
| RPT-QC | Quality Control with Repeat Testing on Patient Samples |
| CASCO | ISO Committee for Conformity Assessment |
| MU | Measurement Uncertainty |
| IFCC | International Federation of Clinical Chemistry and Laboratory Medicine |
| TF-GLQ | Task Force on Global Lab Quality |
| CLSI | Clinical and Laboratory Standards Institute |
| EWMA | Exponentially Weighted Moving Average |
| POCT | Point of Care Testing |
| NGS | Next Generation Sequencing, |
References
- ISO 15189:2022. Medical laboratories — Requirements for quality and competence.
- Q19 Recommendations for ISO 15189 Accreditation of medical laboratory: examination processes, validity of examination results. 03/04/2024. Document approved by the National Council on 02/27/2024. https://www.sipmel.it/it/lineeguida/approvate/121264 (accessed on 2 May 2025).
- Linko, S. , Boursier, G., Bernabeu-Andreu, F., Dzneladze, N., Vanstapel, F., Brguljan, P., Tosheska-Trajkovska, K., Mehay, H., Panteghini, M., Brugnoni, D., Milinkovic. N., Lohmander, M., Šprongl, L., Çubukçu, H., Thelen. M. EN ISO 15189 revision: EFLM Committee Accreditation and ISO/CEN standards (C: A/ISO) analysis and general remarks on the changes. Clin Chem Lab Med (CCLM). 2025;63, pp. 1084–1098. [CrossRef]
- Pradella, M. New ISO standards for medical biology laboratories, prescriptions and deviations. Ann Biol Clin (Paris). 2022 80, pp 451-453. English, French. [CrossRef]
- ISO/TS 20914:2019. Medical laboratories — Practical guidance for the estimation of measurement uncertainty.
- Pradella, M. Le raccomandazioni SIPMeL per l’accreditamento ISO del monitoraggio di validità dei risultati degli esami CQI per ISO 15189. Riv Ital Med Lab 2024; 20, pp. 209–219. [CrossRef]
- Giannoli, J.M. , Vassault, A, Carobene, A, Liaudet, A.P., Blasutig, I.M., Dabla, P.K., Lin, J., Thomas, A., Tesser Poloni, J.A., Meng, Q.H., Amann. E.P.; International Federation of Clinical Chemistry; Laboratory Medicine Task Force on Global Lab Quality TF-GLQ. Ensuring internal quality control practices in medical Laboratories: IFCC recommendations for practical applications based on ISO 15189:2022. Clin Chim Acta. 2025; 571, pp. 120240. [CrossRef]
- Pradella, M. Divergences between IFCC recommendations for Internal Quality Control and ISO standards. Reference: CCA_120334. 2025. [CrossRef]
- Çubukçu, H.C. , Thelen, M., Plebani, M., Panteghini, M. "IFCC recommendations for internal quality control practice: a missed opportunity" Clinical Chemistry and Laboratory Medicine (CCLM), 2025. [CrossRef]
- Panteghini, M. An improved implementation of metrological traceability concepts is needed to benefit from standardization of laboratory results. Clin Chem Lab Med (CCLM). 2025; 63, pp. 270–278. [CrossRef]
- ISO 17511:2020. In vitro diagnostic medical devices — Requirements for establishing metrological traceability of values assigned to calibrators, trueness control materials and human samples.
- ISO 21151:2020. In vitro diagnostic medical devices — Requirements for international harmonisation protocols establishing metrological traceability of values assigned to calibrators and human samples.
- Braga, F, Pasqualetti, S, Aloisio, E, Panteghini, M. The internal quality control in the traceability era. Clin Chem Lab Med 2021; 59, pp. 291–300. [CrossRef]
- Westgard, J, Bayat, H, Westgard, S. How to evaluate fixed clinical QC limits vs. riskbased SQC strategies. Clin Chem Lab Med (CCLM). 2022; 60, pp. e199–e201. [CrossRef]
- Pradella, M. Controllo di qualità interno: statistica avversaria della metrologia? Riv Ital Med Lab 2021; 17, pp 130-132. [CrossRef]
- CLSI EP15:2014. User Verification of Precision and Estimation of Bias.
- CLSI EP32 ED2:2024 Metrological Traceability in Laboratory Medicine.
- CLSI C24:2016. Statistical Quality Control for Quantitative Measurement Procedures: Principles and Definitions.
- van Andel, E., Henricks, L.M., Giliams, A.P.M., Noordervliet, R.M., Mensink, W.J., Filippo, D., van Rossum, H.H., Cobbaert, C.M., Gillis, J.M.E.P., Schenk, P.W. and den Elzen, W.P.J. Moving average quality control of routine chemistry and hematology parameters – a toolbox for implementation. Clin Chem Lab Med 2022, 60, 1719–1728. [CrossRef]
- van Rossum, H.H. , van den Broek, D. Design and implementation of quality control plans that integrate moving average and internal quality control: incorporating the best of both worlds. Clin Chem Lab Med (CCLM) 2019, 57, 1329–1338. [Google Scholar] [CrossRef] [PubMed]
- van Rossum, H.H. Technical quality assurance and quality control for medical laboratories: a review and proposal of a new concept to obtain integrated and validated QA/QC plans. Crit Rev Clin Lab Sci. 2022, 59, 586–600. [Google Scholar] [CrossRef] [PubMed]
- Cembrowski, G.S. Use of patient data for quality control. Clin Lab Med. 1986, 6, 715–733. [Google Scholar] [CrossRef] [PubMed]
- Çubukçu, H.C. QC Constellation. Clin Chem Lab Med 2024, 62, 2185–2197. [Google Scholar] [CrossRef] [PubMed]
- Carson, P.K. , Yeh, A. B. Exponentially weighted moving average (EWMA) control charts for monitoring an analytical process. Ind Eng Chem Res 2008, 47, 405–411. [Google Scholar] [CrossRef]
- Çubukçu, H.C. The weighting factor of exponentially weighted moving average chart. Turk J Biochem 2020, 45, 639–41. [Google Scholar] [CrossRef]
- Topcu, D.I. , Çubukçu, H.C. Optimization of patient based real-time quality control based on the Youden index. Clin Chim Acta 2022; 534, pp. 50–6. [CrossRef]
- Cembrowski, G.S. Xu, Q., Cervinski, M.A. Average of Patient Deltas: Patient-Based Quality Control Utilizing the Mean Within-Patient Analyte Variation. Clin Chem. 2021, 67, 1019–1029. [Google Scholar] [CrossRef] [PubMed]
- Bietenbeck, A. Cervinski, M.A., Katayev, A., Loh, T.P., van Rossum, H.H., Badrick, T. Understanding Patient-Based Real-Time Quality Control Using Simulation Modeling. Clin Chem. 2020, 66, 1072–1083. [Google Scholar] [CrossRef] [PubMed]
- Flatland, B. , Freeman, K.P. Repeat patient testing quality control (RPT -QC): Background and theory. Vet Clin Pathol. 2024, 53 Suppl 1, 24 -30. [CrossRef]
- Westgard, J.O. Basic QC Practices. Fourth Edition. Training in Statistical Quality Control for Medical Laboratories. 2016. Westgard QC. 7614 Fox Trail. Madison, Wisconsin 53717.
- Daly, S. , Graham, P.A., Freeman, K.P. Repeat patient testing - quality control with canine samples shows promise as an alternative to commercial quality control material for a network of four Sysmex XT -2000iV hematology analyzers. Vet Clin Pathol. 2024, 53 Suppl 1, 39 -47. [CrossRef]
- Westgard, S. , Daly, S., Freeman, K., Flatlan, B.. Repeat Patient QC: A new approach for patient-based control. Webinar Dec 14, 2023.
- Tsiamyrtzis, P. Sobas, F., Négrier, C. Use of prior manufacturer specifications with Bayesian logic eludes preliminary phase issues in quality control: an example in a hemostasis laboratory. Blood Coagul Fibrinolysis 2015, 26, 590–6. [Google Scholar] [CrossRef] [PubMed]
- Jousselme, E. Meijer, P., Sobas, F., Tsiamyrtzis, P.. Complementarity between Bayesian Internal Quality Control results management and External Quality Assessment bivariate z-score analysis: application to a concrete case study. Ann Biol Clin (Paris). 2025, 82, 645–650. [Google Scholar] [CrossRef] [PubMed]
- ISO 15198:2004 Clinical laboratory medicine -- In vitro diagnostic medical devices -- Validation of user quality control procedures by the manufacturer.
- Pradella, M. Produttore di diagnostici e laboratorio medico alleati per il controllo di qualità dei risultati: ritardi e novità. Riv Ital Med Lab 2020, 16, 73–7. [Google Scholar] [CrossRef]
- Pradella, M. Alliance of IVD manufacturer and medical laboratory for quality control of results. Adv Lab Med. 2021, 2, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Reilly-Stitt, C. , Jennings, I. , Kitchen, S., Walker, I.D. Internal Quality Control in Hemostasis Assays. • Semin Thromb Hemost. 2024, 50, 1084–1090. [Google Scholar] [CrossRef] [PubMed]
- CLSI POCT07:2010. Quality Management: Approaches to Reducing Errors at the Point of Care.
- CLSI POCT08.:2010 Quality Practices in Noninstrumented Point-of-Care Testing: An Instructional Manual and Resources for Health Care Workers.
- CLSI POCT14:2020. Point-of-Care Coagulation Testing and Anticoagulation Monitoring.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



