Submitted:
10 May 2025
Posted:
12 May 2025
You are already at the latest version
Abstract
Alzheimer’s disease accounts for approximately 50% to 80% of all causes of dementia. Co-existence of AD with other diseases causing dementia poses a diagnostic challenge as we are still far from diagnosing AD accurately and hence to manage it appropriately. Neuroimaging techniques, not only help diagnose AD but also consistently features in diagnostic and research criteria for AD as biomarkers. Molecular biomarkers including Positron emission tomography (PET) and Single Photon emission computed tomography (SPECT) and structural biomarkers including Magnetic Resonance Imaging (MRI) have been used in various therapeutic and prognostic studies in AD. This review highlights the recent advances in the neuroimaging biomarkers including molecular biomarkers (PET and SPECT) and structural biomarkers (MRI) for AD. For the purpose of this review, molecular biomarkers have been further subcategorized into non-specific radiotracers (FDG-PET and SPECT) and specific amyloid and tau related radiotracers. The aim of this review is to discuss the recent advances and evidences on molecular and structural biomarkers of AD.
Keywords:
Alzheimer’s disease
; neuroimaging biomarkers
; molecular biomarkers
; structural biomarkers
Introduction
Alzheimer’s dementia (AD) is the most common cause of dementia accounting for approximately 50- 80% of all causes of dementia (Kanekar and Poot, 2014). AD is characterised by cognitive decline especially memory impairment followed by impairment in other cognitive domains, with histopathological features of amyloid deposition and intra-neuronal tau deposition in senile plaques and neurofibrillary tangles respectively(Humpel, 2011). The incidence of AD increases with age and doubles every 5 years after the age of 60 (Corrada et al., 2010). With increasing life expectancy world-wide prevalence of AD is expected to increase exponentially increasing the urgency of accurate diagnosis in order to initiate management strategies early to help prevent progression of cognitive decline and reduce the morbidity (Rasmussen and Langerman, 2019; Wattamwar and Mathuranath, 2010). AD often coexist with other diseases that cause dementia and despite advancement in diagnostic techniques, we are still far from diagnosing AD accurately and managing appropriately. Neuroimaging not only supports diagnosis of AD as the cause of dementia but also consistently features in the diagnostic criteria for probable AD (Jack et al., 2018).
The currently available therapeutic strategies can alleviate behavioural disturbances in AD but drugs to halt disease progression are still elusive (Bachurin et al., 2017). The complex aetiology and pathology of AD may be responsible for unsuccessful attempts at disease modifying therapy (Mattsson et al., 2015). Imaging biomarkers play an important role not only in visualising the typical abnormalities of AD for diagnosis and monitoring disease progression but also in therapeutics of AD by predicting response to novel AD drugs (Hampel et al., 2017). National Institute on Aging and Alzheimer’s Association (NIA-AA) in 2011, incorporated biomarkers in the diagnostic criteria of AD (McKhann et al., 2011; Wong et al., 2021). Further, the International Working Group (IWG) in 2014 categorised biomarkers for AD into diagnostic and prognostic biomarkers, focussing on MRI and PET biomarkers.(Dubois et al., 2014)
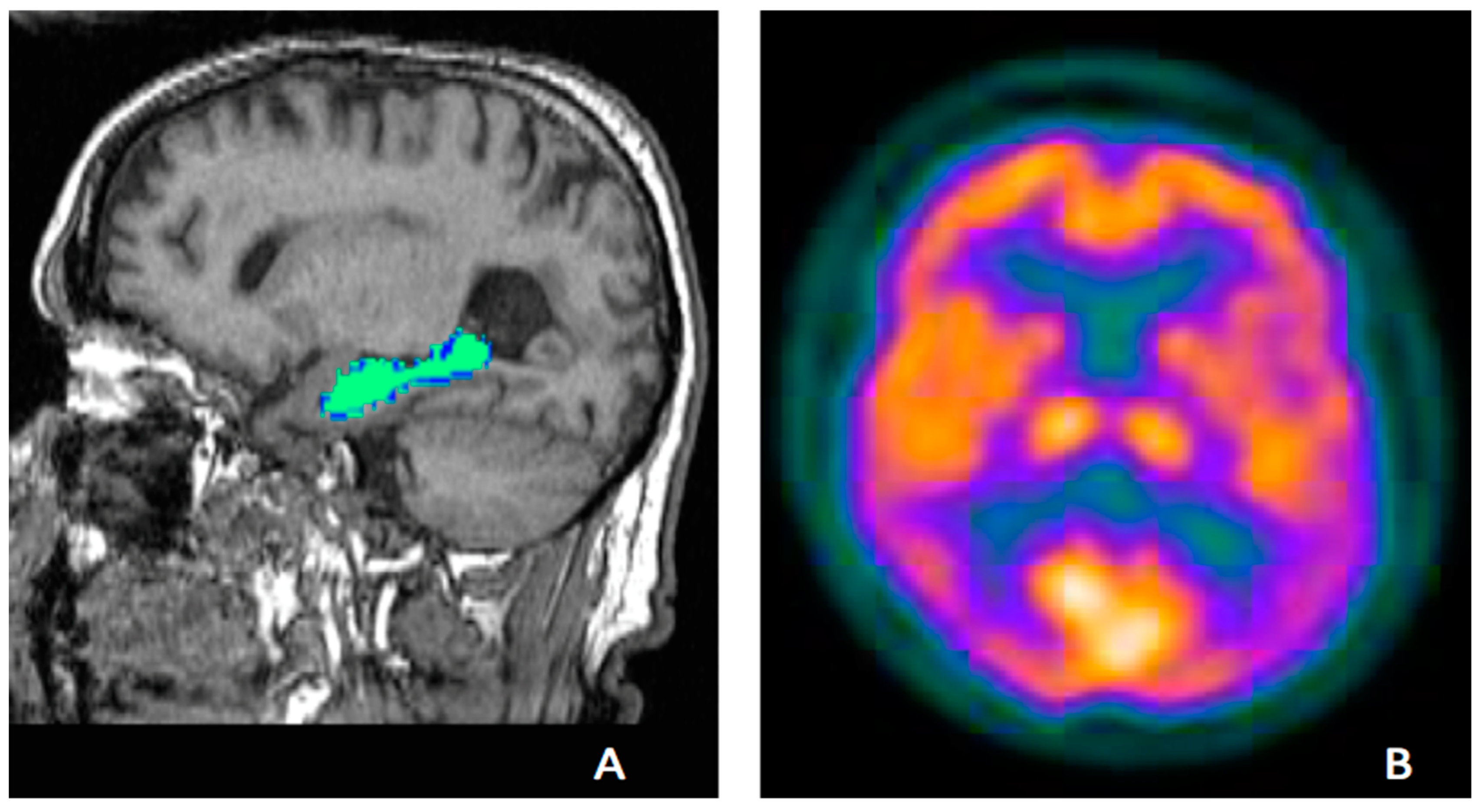
Figure 1.
Showing examples of established biomarkers in AD; Hippocampal volumes on MRI(A) and temporoparietal defects on FDG-PET (B).
Figure 1.
Showing examples of established biomarkers in AD; Hippocampal volumes on MRI(A) and temporoparietal defects on FDG-PET (B).
Recently, NIA-AA, has updated the recommendations for pre-clinical, mild cognitive impairment (MCI) and AD diagnosis and categorised neuroimaging and cerebrospinal fluid (CSF) biomarkers into AT(N) groups. The A denotes Amyloid deposition (A), T denotes pathological fibrillary tau and N signifies neurodegeneration (Jack et al., 2018, 2016).
The recent shift towards different imaging biomarkers in AD research has made it necessary for us to review imaging biomarkers in AD which not only include molecular biomarkers but also MRI biomarkers. This review highlights the recent advances in the imaging biomarkers including molecular biomarkers (PET and SPECT) and structural biomarkers (MRI) for AD. The aim of this review is to discuss the recent advances and evidences for molecular and structural imaging biomarkers of AD.
Molecular Biomarkers
The molecular biomarkers which are commonly used for diagnostic, prognostic or therapeutic purposes in AD can be further subcategorized into non-specific radiotracers, such as FDG-PET , blood flow SPECT and Dopamine Transporter Scan (DaT scan) and specific radiotracers including amyloid and tau radiotracers.
Molecular Biomarkers with Non-Specific Radiotracers
Radioactive tracers such as 18F fluoro-deoxy glucose and 99m Tc-labelled tracer HMPAO (d, 1, hexamethylpropylene amine oxime) are used for brain FDG PET and cerebral blood flow SPECT respectively. To differentiate dementia subtypes in clinical and research settings, patient specific information provided by these techniques is useful. In research settings, these techniques provide details of molecular and pathophysiology of the diseases causing dementia. Details of non-specific radiotracers in AD are provided below.
FDG-PET
FDG-PET has been a well-established and extensively used neuroimaging tool to aid in clinical diagnosis of neurodegenerative conditions including AD as hypo-metabolism in certain brain regions corresponds to neuronal loss and functional impairment (Minoshima et al., 2021; Ou et al., 2019; Sperling et al., 2011). Reduced cerebral blood glucose uptake on FDG-PET in the areas of neurodegeneration, can help distinguishing AD from other causes of dementia (Dave et al., 2020; Mosconi, 2013; Tripathi et al., 2014) and is considered as molecular imaging biomarker for AD(Bouter et al., 2018; Ou et al., 2019). Hypo-metabolism on FDG-PET precedes the detectible atrophy on structural MRI in AD and is a more sensitive technique to detect early neurodegenerative disease (Kljajevic et al., 2014; Matsunari et al., 2007; Salmon et al., 2024). Moreover, characteristic temporo-parietal hypo-metabolism can be seen on FDG-PET even before structural changes in people with AD (Martin-Macintosh et al., 2016; Tripathi and Murray, 2021). With advancement in AD pathology, FDG-PET can detect extension of cortical hypometabolism to the frontal lobes, especially prefrontal association cortex and anterior cingulate gyrus(Brown et al., 2014). Moreover, it has been established that hippocampal, posterior cingulate cortex and precuneus hypo-metabolism is seen in early stage of AD (Bailly et al., 2015; Ishii et al., 1998). Other neocortical areas are involved via brain networks and the disease progresses in stereotypical pattern (Brown et al., 2019).
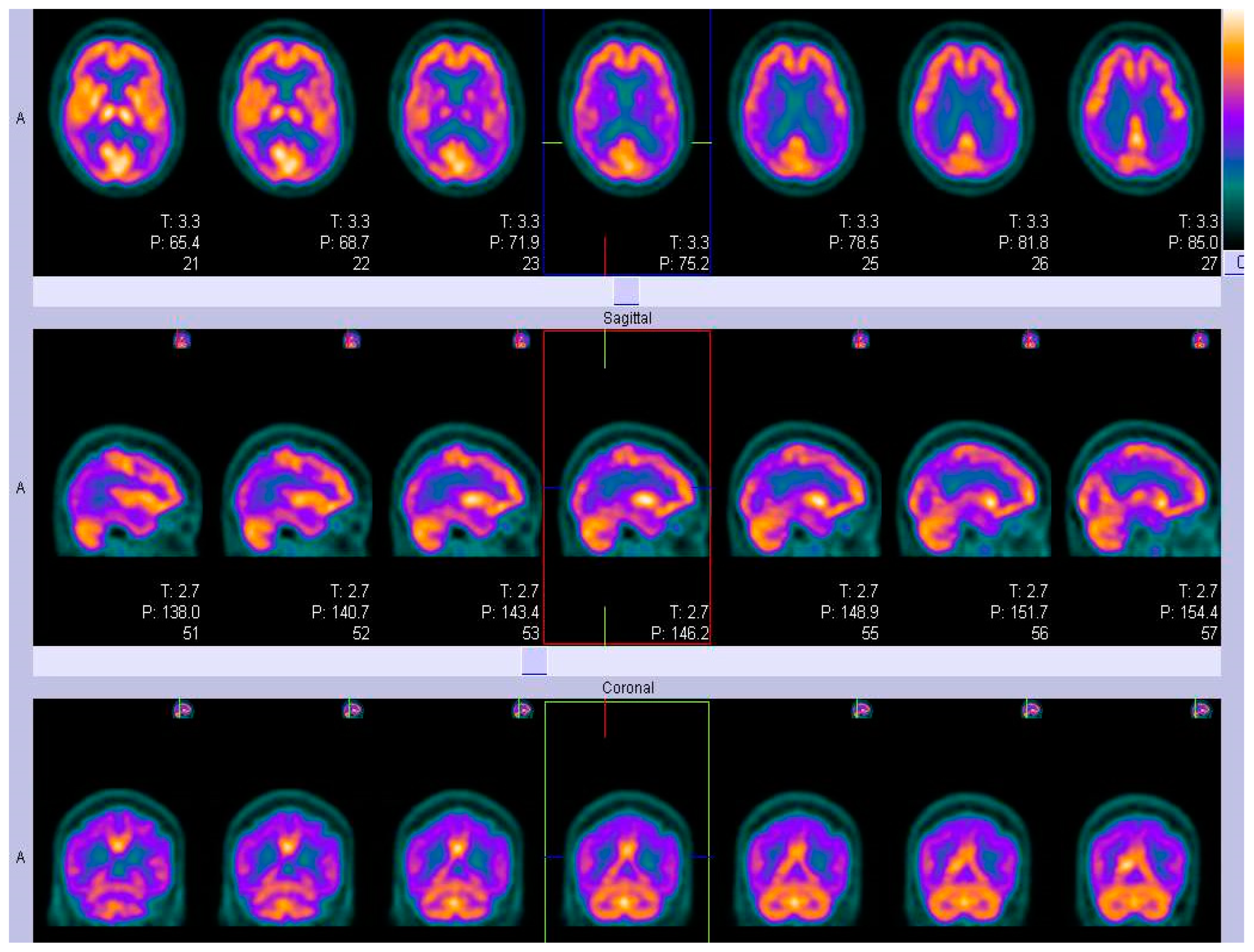
Figure 2.
An example of FDG-PET imaging in typical AD showing temporo-parietal defects in form of diagonal band.
Figure 2.
An example of FDG-PET imaging in typical AD showing temporo-parietal defects in form of diagonal band.
Sensitivity and specificity of 99% and 98% respectively have been reported for FDG-PET to distinguish people with AD from normal subjects. However, the specificity of FDG-PET to distinguish AD from other causes of dementia, including Dementia with Lewy Bodies (DLB) and Frontotemporal dementia (FTD) were reported to be 71% and 65% respectively, while sensitivity remains 99% (Marcus et al., 2014; Mosconi et al., 2008). Recently, FDG-PET has been included as an independent biomarker in the ATN framework for AD diagnosis as hypo-metabolism on FDG-PET predicts greater atrophy, poorer cognitive function, and a higher conversion to AD from mild cognitive impairment (MCI)(Ou et al., 2019). Notably, conversion to AD from MCI can be predicted from a similar glucose uptake pattern as AD on FDG-PET (Ishii K, 2014). Moreover, higher rate of progression and associated cognitive decline can be predicted from severity and progression of hypo-metabolism on FDG-PET in MCI patients. Thus, FDG PET has not only diagnostic value but also prognostic value in people with AD(Dubois et al., 2023; Heyer et al., 2024; Landau et al., 2011; Zhang et al., 2012).
Various clinical trials have used FDG-PET for treatment response evaluation in people with AD (Chen et al., 2010; Høilund-Carlsen et al., 2023) and as an imaging biomarker for measurement of outcome and participant selection in AD and other dementia related therapeutic trials.(Chow et al., 2013; Potkin et al., 2001).
SPECT
SPECT is a molecular imaging modality using gamma-emitting radiotracers, the distribution in the body is detected using a gamma camera(Sharp PF, 2005). SPECT highlights blood flow in different brain regions to evaluate brain and neurological conditions. The radiotracer 133Xe was the first to be used for brain perfusion in 1990 and that has been followed by use of various other radiotracers such as HMPAO (hexamethyl propylene amine oxime), and ECD (ethylcysteinate-dimer), which are static radiotracers in contrast to 133Xe, which is a diffusible radiotracer. However, SPECT should only be used as an aide to the diagnosis of a dementia subtype. The exceptions are Parkinson’s disease dementia and Dementia with Lewy bodies, where Dopamine transporter imaging (DaT) with DaTscanTM (Ioflupane 123-I SPECT), has been found to be useful at confirming an underlying .pre-synaptic dopaminergic deficit(Antonini et al., 1997).
ECD and HMPAO- SPECT
SPECT is being widely used for cerebral blood flow (CBF) studies and help identify functional abnormalities relevant to Alzheimer’s disease(Holman et al., 1992).99mTc-ECD and 99mTc-HMPAO are the two most commonly used static radiotracers (Catafau, 2001), having several technical, economic and logistical advantages over other radiotracers (Devous, 2005). 99mTc-ECD has in vitro chemical stability lasting several hours after reconstitution, faster blood clearance and a high signal to noise ratio making it an efficient technique to elucidate brain functions in various neurological disorders including cerebrovascular disease (Brass et al., 1994) and Alzheimer’s disease (Waldemar et al., 1994). In addition, 99mTc-HMPAO another tracer in which 99mTc is attached with a chelating agent HMPAO and useful for the detection of regional blood flow in the brain and hence used in diagnostic evaluation of dementias. It has greater specificity in comparison to the clinical criteria in differentiating AD from other dementias and can help in differential diagnosis of AD(Dougall et al., 2004; Imokawa et al., 2024; Talbot et al., 1998)
Notably, SPECT radiotracers are relatively less expensive and having a longer half-life than the radiotracers commonly used in PET, enabling more flexibility in tracer provision, administration and imaging time. SPECT has been widely studied, and it may be used for diagnostic work up of people with diseases causing dementia. Earlier, concerns were raised regarding SPECT use due to image quality, artefacts and difficulty in quantifying blood flow, but emerging technology sorted out the shortcomings. Data from the large cross -sectional studies has been used to make inter-subject comparisons using t or z statistics in order to eliminate individual variations in positions, shape and size (Matsuda et al., 2007). The sensitivity and specificity of rCBF SPECT in differentiating AD from VaD are 74.5 and 72.4%, AD from FTD are 79.7 and 79.9%, AD from DLB are 70.2 and 76.2%, and AD from healthy controls are 76.1 and 85.4% respectively (Jang et al., 2013).
Hypoperfusion on SPECT has been well correlated with the onset, the severity, clinical features and prognosis of AD (Valotassiou et al., 2011). Parietal hypoperfusion is most commonly seen in early onset AD (Nitrini et al., 2000) and late onset AD is characterised by medial temporal lobes hypoperfusion (Kemp et al., 2003). Some studies have found hypoperfusion in temporoparietal regions to correlate with mini mental score in people with AD(Rodriguez et al., 1999). Notably, frontal lobe hypoperfusion has been negatively correlated with cognitive functions and positively correlated with rate of progression of the disease.(Nishimura et al., 2007). However, median survival time for people with AD has been negatively correlated with left temporal lobe hypo-perfusion (Claus et al., 1999). Thus, blood flow SPECT can be considered as a biomarker in AD (Gunes et al., 2022; Ito et al., 2017), depicting the disease much earlier than the clinical manifestation (Valotassiou et al., 2018).
Dopamine Transporter SPECT
SPECT investigating the striatal dopamine transporter (DAT) status have been used widely in uncertain parkinsonian syndromes(Scherfler and Nocker, 2009). Despite, no changes in DaT-SCAN in AD on comparison to controls, it is helpful in differentiating AD from DLB. In DLB, there is 40-70% loss of striatal dopamine and dopaminergic cells resulting in loss of dopaminergic transporter(Vaamonde-Gamo et al., 2005). Dopamine transporter SPECT can thus be useful in differentiating neuro-degenerative Parkinsonian syndromes (PS) from non-dopamine deficiency aetiologies including drug induced parkinsonism and essential tremor (AKDEMİR et al., 2021; Plotkin et al., 2005), with sensitivity and specificity of over 90% (Brigo et al., 2014).
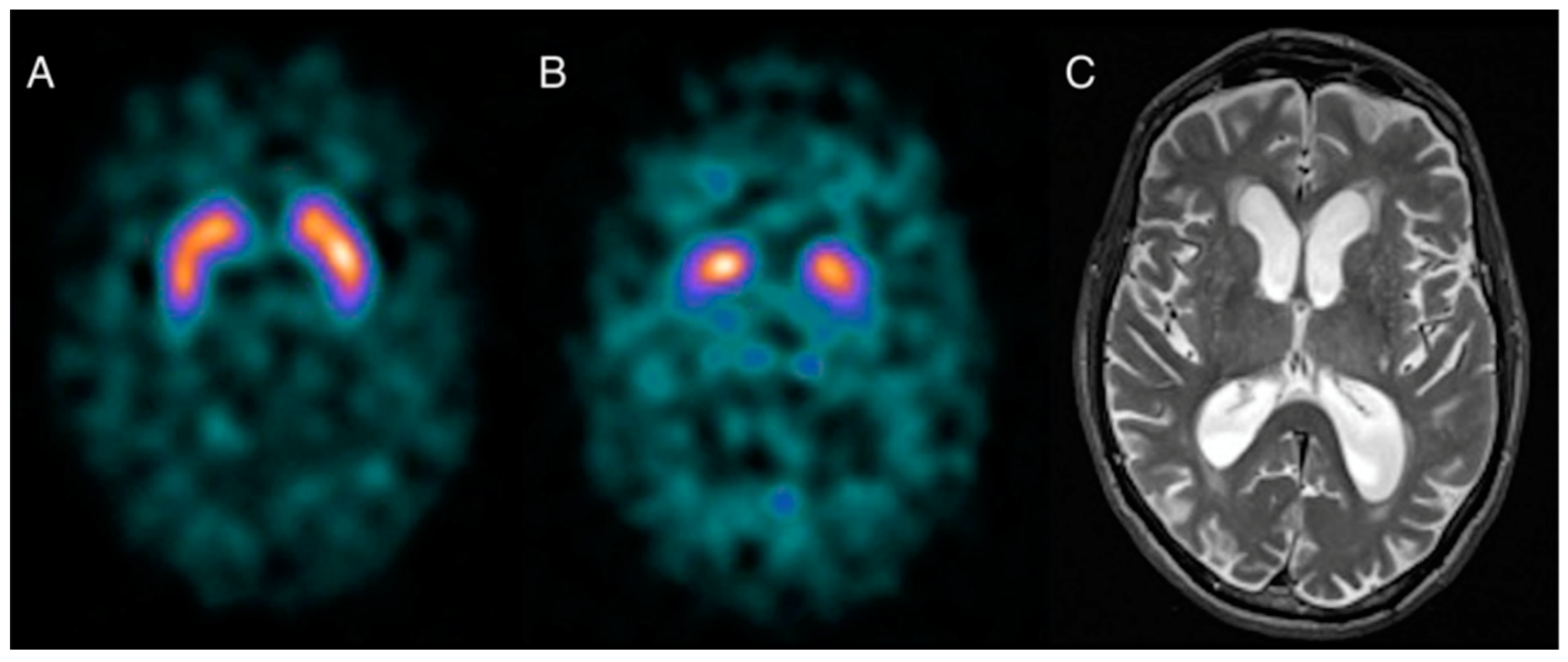
Figure 3.
Normal DAT scan (a)for comparison. DAT scan of a patient with DLB(b)showing lack of tracer uptake in the putamen bilaterally.AxialT2- weighted image (c) of the same patient shows non-specific generalised supratentorial volume loss. Reproduced with Permission (Bhogal et al., 2013).
Figure 3.
Normal DAT scan (a)for comparison. DAT scan of a patient with DLB(b)showing lack of tracer uptake in the putamen bilaterally.AxialT2- weighted image (c) of the same patient shows non-specific generalised supratentorial volume loss. Reproduced with Permission (Bhogal et al., 2013).
Specific Radiotracers
A growing class of radiotracers targeting specific protein aggregates for amyloid-β (Aβ) and tau are providing new avenues for research in AD diagnosis, as these radiotracers directly label the underlying disease pathologies. Amongst the two-specific type of tracers, tau tracers are emerging as preferential for the researchers for therapeutic and prognostic evaluation in AD clinical trials due to failure of agents targeting amyloid pathology. Thus, in this review we provide a brief summary of amyloid PET and greater detail about tau PET.
Amyloid PET
Pittsburg Compound B (PIB) a 11-C labelled PET tracer was first to be used as an amyloid specific radiotracer (Klunk et al., 2004) and demonstrated amyloid deposition precedes clinical manifestation of AD by 15 years. (Jack et al., 2013; Villemagne et al., 2013). However, recently, this has been refuted and proposed that cognitive decline precedes amyloid deposition (Elman et al., 2020), thus, opening a new avenue in research to look beyond our understanding of amyloid in AD. The Amyloid imaging task force (Johnson et al., 2013) has clearly stated that amyloid PET should only be used if there is diagnostic ambiguity and tracers can improve diagnostic accuracy. However, recently it has been reported that initiation and discontinuation of medications in management of AD can be influenced by the use of amyloid PET imaging in clinical practice (Kim et al., 2018).
PiB binds specifically with insoluble fibrillary Aβ and cortical binding of PiB has been seen in more than 90% of people with AD (Rabinovici and Jagust, 2009). Following PIB several other 18F-labelled PET tracers such as [18F]Flutemetamol, [18F]Florbetaben and [18F]Florbetapir have emerged as potential tools to aid in AD diagnosis and are widely used for research purposes ( Filippi et al., 2018). The 18F-labelled PET tracers have half-life of 110 minutes and thus overcoming the disadvantage of PIB, as PIB has a shorter half-life of 20 minutes resulting in practical difficulties for clinical and research use. U.S. FDA has provided its approval for use of [18F]Florbetapir in 2012, for exploring AD or other causes of cognitive impairment and followed by approval of [18F]Flutemetamol and [18F]Florbetaben by U.S. FDA in 2013 and 2014 respectively ( Filippi et al., 2018). Amyloid PET has been found to be more sensitive but less specific than FDG-PET in distinguishing AD from other causes of dementia such as FTD (Rabinovici et al., 2011). Despite the association of amyloid deposition with AD, it has also been consistently found in cognitively healthy people (Jansen et al., 2015), raising the question of whether amyloid deposition is a pathognomonic or necessary feature for the diagnosis of AD.
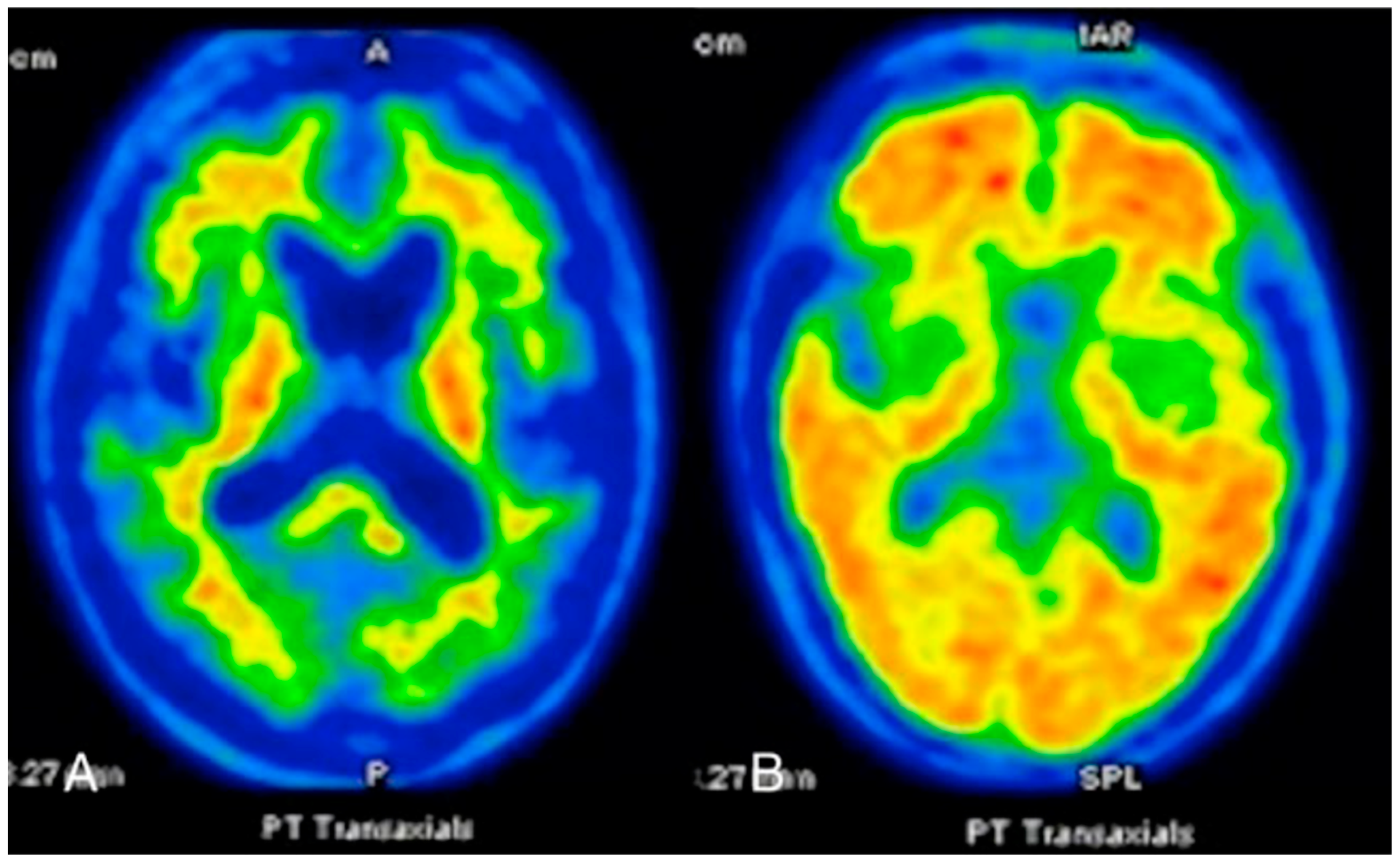
Figure 4.
Axial image of an amyloid PET-CT using 11C-PIB in a patient with Progressive Supranuclear Palsy(A) and Alzheimer’s disease (B). Patient in a shows normal distribution of the tracer, whereas the patient with AD shows a high tracer uptake in the cortices of the frontal, temporal and occipital lobes consistent with a heavy amyloid burden. Reproduced with permission (Bhogal et al., 2013).
Figure 4.
Axial image of an amyloid PET-CT using 11C-PIB in a patient with Progressive Supranuclear Palsy(A) and Alzheimer’s disease (B). Patient in a shows normal distribution of the tracer, whereas the patient with AD shows a high tracer uptake in the cortices of the frontal, temporal and occipital lobes consistent with a heavy amyloid burden. Reproduced with permission (Bhogal et al., 2013).
Although, it is difficult to ascertain timing of amyloid deposition but it is believed to begin at preclinical stage(Jack et al., 2013) but amyloid PET has shown cortical uptake of amyloid tracers in the cingulum, precuneus and frontal, parietal and lateral temporal cortices in people with AD(Wolk and Klunk, 2009). Moreover, amyloid PET has a prognostic value as people with MCI having positive findings on amyloid PET have higher chances of conversion to AD and those who are negative on amyloid PET have higher negative predictive value for conversion to AD from MCI (Echeveste et al., 2025; Nordberg et al., 2013; Okello et al., 2009). It has also been noted that the rate of cognitive decline is directly proportional to amyloid deposition in people with MCI(Huijbers et al., 2015) and amyloid PET may help identifying people at risk of cognitive decline and disease progression(Wahlster et al., 2013).
Amyloid tracers have also been used recently quite frequently to monitor the therapeutic response of the amyloid based drugs. Primary endpoints in these trials are usually measures of cognitive function such as the Alzheimer’s Disease Assessment Scale - Cognitive Subscale (ADAS-cog) (Rosen et al., 1984) or the Clinical Dementia Rating Scale (CDR) (Morris et al., 1997) but due to cognitive reserve and ceiling and floor effects of psychometric tests, the clinical presentations usually differ between people with AD(Podhorna et al., 2016; Stern, 2012). Recently, 18- Florbetapir PET has been used in the PRIME study to evaluate treatment response of human monoclonal antibody on participants with prodromal or mild AD participants, which depicted a dose- and time-dependent Aβ plaques reduction (Sevigny et al., 2016). For the last few decades, most research has slavishly focussed on Aβ as a target for treatment of AD. However, most of the novel therapeutic agents targeting Aβ have failed to improve cognitive function or slow cognitive decline (Oxford et al., 2020; Zhang et al., 2023).
Tau PET
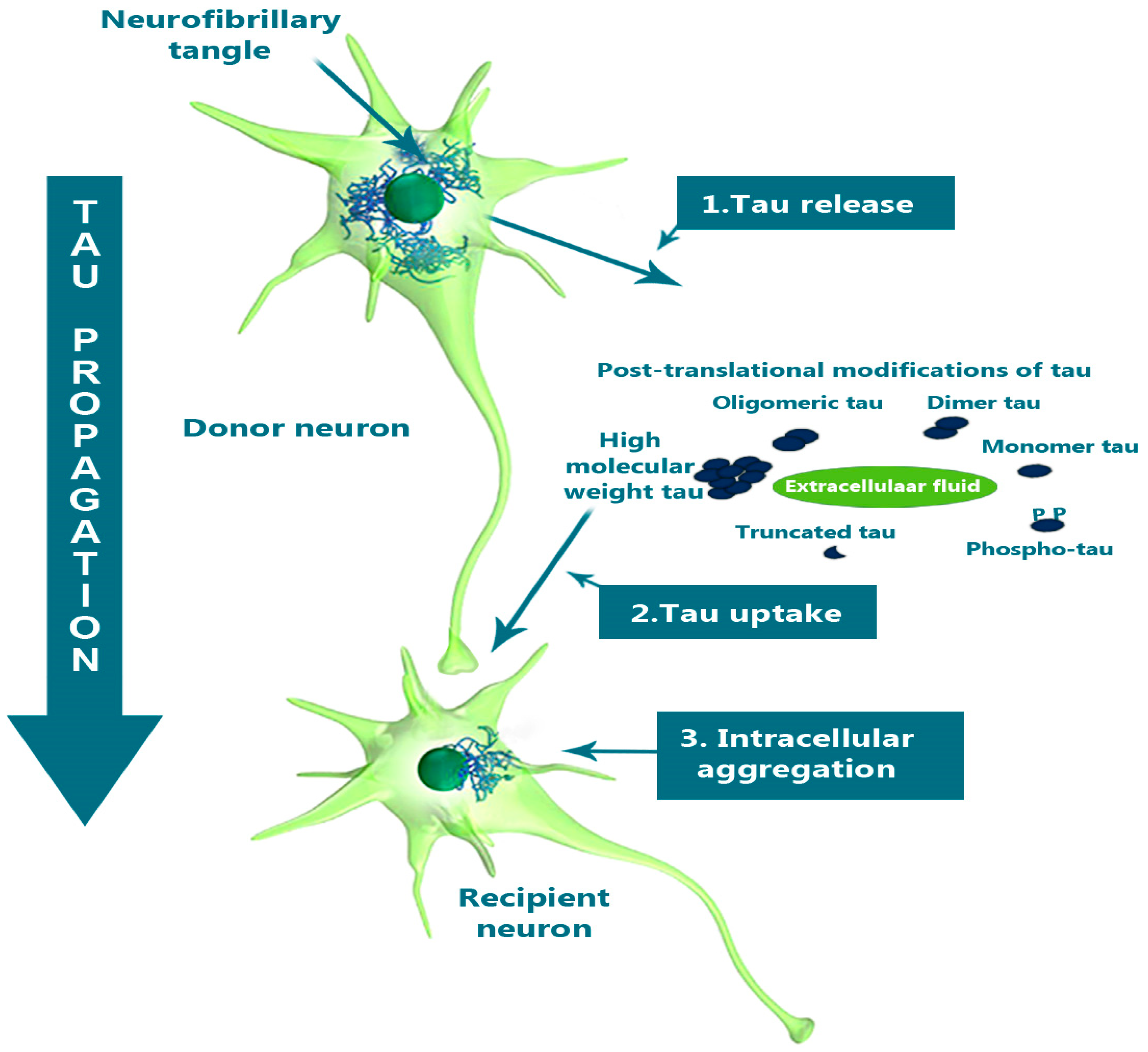
Tau protein helps stabilise the microtubules which are essential for intracellular transport and cytoskeletal support. In its pathological state tau becomes hyper-phosphorylated and accumulates intra-neuronally as Neuro-Fibrillary Tangles (NFTs). The tau propagates intra-neuronally by release of intracellular pathological tau into extracellular space, taken up by recipient neurons and subsequently forms intracellular aggregates in recipient neurons (Takeda, 2019).
Figure 5.
A schematic diagram to illustrate tau propagation hypothesis. Neuron to neuron transmission of tau in AD showing release of pathological tau in extracellular space from donor neuron and further taken up by recipient neuron following post translational modifications and in turn form intracellular aggregates. Adapted with permission from (Takeda, 2019).
Figure 5.
A schematic diagram to illustrate tau propagation hypothesis. Neuron to neuron transmission of tau in AD showing release of pathological tau in extracellular space from donor neuron and further taken up by recipient neuron following post translational modifications and in turn form intracellular aggregates. Adapted with permission from (Takeda, 2019).
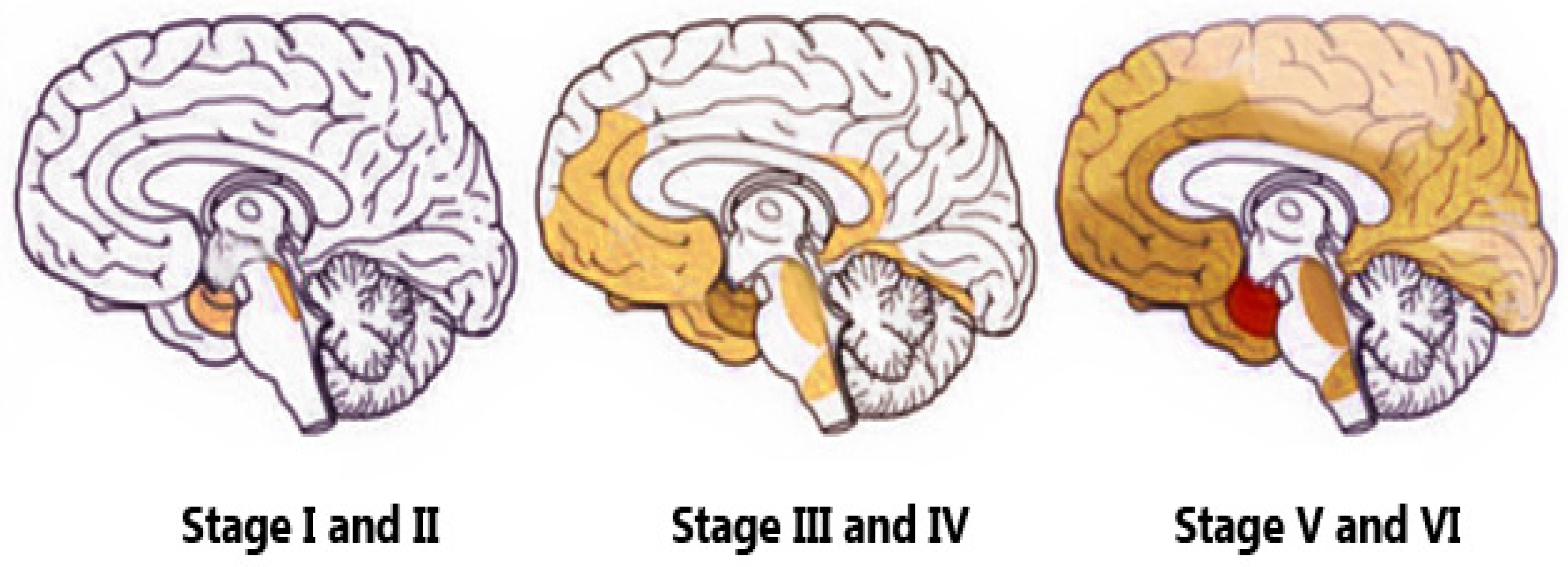
Moreover, clinical severity of dementia is closely associated with tau deposition in comparison to amyloid deposition (Arriagada et al., 1992; Bierer et al., 1995). Notably, Braak’s pathologic staging of AD corresponds with the distribution of NFTs and this is correlated with cognitive impairment (Braak and Braak, 1991). The distribution of NFTs and its correlation with brain atrophy further justify close association of tau protein with neurodegenerative conditions like AD (Whitwell et al., 2008). Furthermore, Clinico-pathological studies reveals close association of tau pathology with loss of neurons and synaptic activity, the correlates of cognition.(Nelson et al., 2012).Recently, tau pathology was reported to be present much earlier than amyloid pathology in younger AD subjects and points towards role of tau in the initial stages of AD and the initiation of the disease process (Yang et al., 2024; Yoshida et al., 2019). After onset of cognitive impairment in AD tau pathology progresses at a faster rate(Braak and Braak, 1991), thus, PET imaging could have an important role in evaluating prognosis of the disease.
Figure 6.
Schematic diagram showing spread of tau pathology starting with entorhinal cortex, then hippocampus, posterior temporal and inferior frontal regions. Image adapted with permission from (Braak and Braak, 1997).
Figure 6.
Schematic diagram showing spread of tau pathology starting with entorhinal cortex, then hippocampus, posterior temporal and inferior frontal regions. Image adapted with permission from (Braak and Braak, 1997).
Following failure of anti-amyloid therapies, a paradigm shift has been observed in the last decade towards tau as therapeutic target and development of several PET tracers to target tau pathology (Yang et al., 2024). A variety of PET ligands have ability to detect tau aggregates formed in AD with a high affinity(Fleisher et al., 2020; Leuzy et al., 2019). The retention pattern of tau PET overlaps with regions brain atrophy(Harrison et al., 2021) and predicts cognitive performance(Ossenkoppele et al., 2019). 2-(1-{6-[(2-[18F]fluoroethyl)(methyl)amino]-2-naphthyl}ethylidene)malononitrile ([18F]FDDNP) was the first PET tau to accomplish imaging in humans and high density of NFTs were observed in the hippocampus(Agdeppa et al., 2001; Shoghi-Jadid et al., 2002). However, FDDNP was reported to bind senile plaques and NFTs equally(Shoghi-Jadid et al., 2002) and there was a quest to search for a selective tau tracer. The tracer which specifically binds to tau should have high affinity towards paired helical filaments (PHF) to produce enough signal to be detected in vivo. Further, the tracer should be more selective towards tau rather Aβ as tau is found to be less frequently distributed in the neocortex in comparison to Aβ.(Villemagne et al., 2012). Furthermore,(18)F-labeled THK-523 or ((18)F-6-(2-fluoroethoxy)-2-(4-aminophenyl)quinoline) was the earliest tau specific tracer to target tau in vivo, but unfortunately, precluded from the use in research or clinical trials due to high retention rate in the white matter(Fodero-Tavoletti et al., 2011; Villemagne et al., 2014). Several other 18F-labeled arylquinoline derivative tau PET radiotracers such as (18)F-THK-5105 and (18)F-THK-5117 were developed(Harada et al., 2015; Okamura et al., 2014) but the more recently developed 18F-THK-5351, has better imaging characteristics and has higher tau binding affinity and lower white matter retention (Harada et al., 2016).
Furthermore, radiotracers 18F-AV-1451 (also known as T807 and 18F-flortaucipir) and18-F -AV-680 (also known as T808) the benzimidazole pyrimidine derivatives were developed (Chien et al., 2013; Zhang et al., 2012) with higher affinity for tau aggregates and lower white matter retention. Recently it has been concluded that 18F-flortaucipir has better sensitivity than amyloid PET and help detect preclinical cognitive changes in people with AD(Ossenkoppele et al., 2019). Further, region based analysis of 18F-flortaucipir, depicted that the spread of tau pathology was consistent with Braak staging.(Cho et al., 2016; Marquié et al., 2017). Recently, FDA has approved first tau PET tracer 18F-AV-1451(18F-flortaucipir) for estimation of NFTs in people who are being evaluated for AD(Barthel, 2020).
Figure 7.
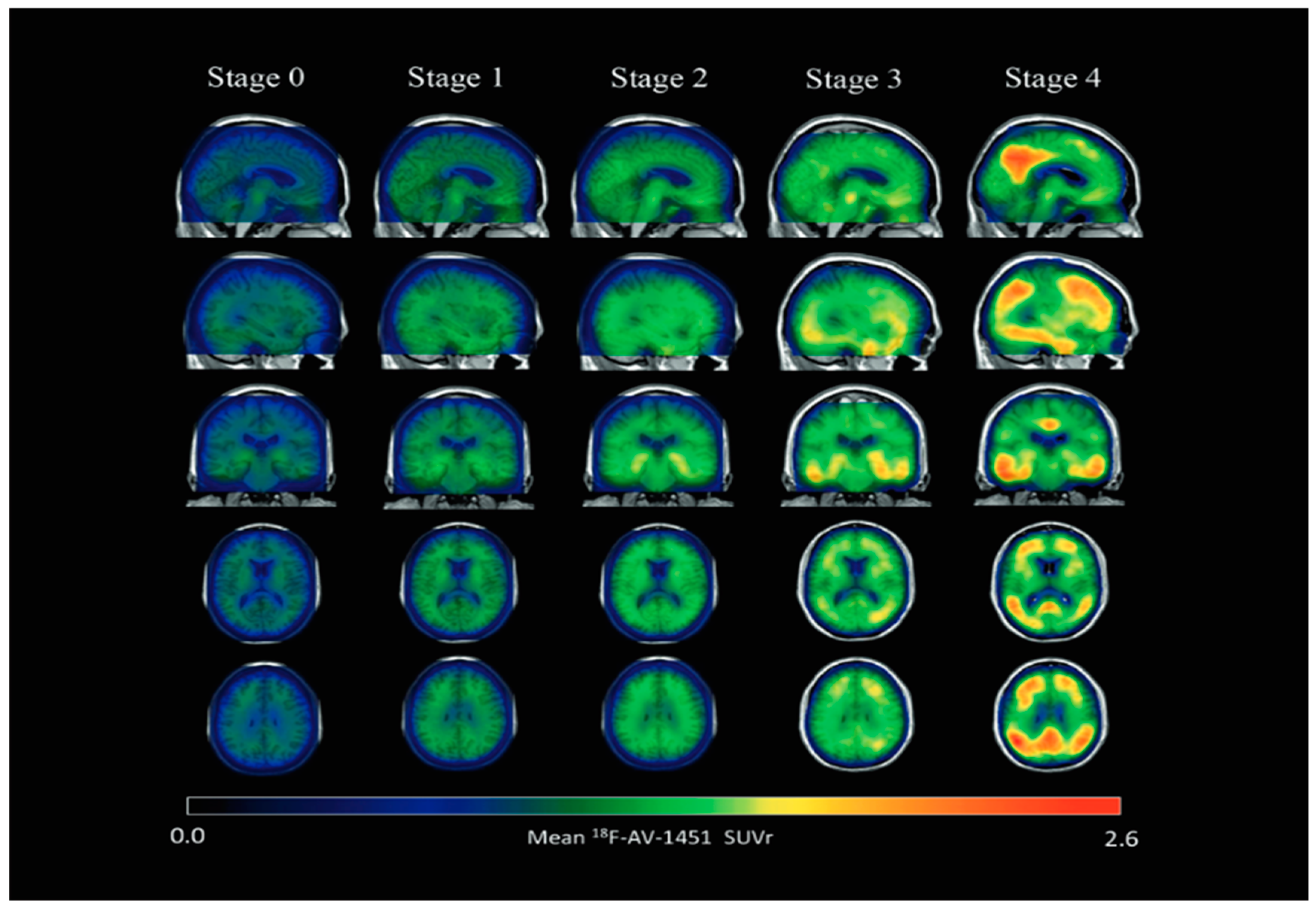
Parametric 18 F-AV-1451 images across stages. In general, 18 F-AV-1451 SUVr increased throughout the cortex and subcortex from stage 0 to stage 4. Participants in stage 0 had tau level corresponding to those of normal young adults. A dominating tau elevation in medial temporal regions (Braak I/II ROIs) was shown in stage 1. While stage 2 presented increased SUVrs in extramedial temporal regions, stage 3 showed greater SUVrs increase in Braak III/IV ROIs including inferior and lateral temporal lobes. Stage 4 had significantly elevated 18F-AV-1451 SUVr extending into the neocortex. ROI region of interest, SUVr standard uptake value ratio. Reproduced with permission(Chen et al., 2021).
Figure 7.
Parametric 18 F-AV-1451 images across stages. In general, 18 F-AV-1451 SUVr increased throughout the cortex and subcortex from stage 0 to stage 4. Participants in stage 0 had tau level corresponding to those of normal young adults. A dominating tau elevation in medial temporal regions (Braak I/II ROIs) was shown in stage 1. While stage 2 presented increased SUVrs in extramedial temporal regions, stage 3 showed greater SUVrs increase in Braak III/IV ROIs including inferior and lateral temporal lobes. Stage 4 had significantly elevated 18F-AV-1451 SUVr extending into the neocortex. ROI region of interest, SUVr standard uptake value ratio. Reproduced with permission(Chen et al., 2021).
In addition, tau PET tracers, such as pyridinyl- butadienyl-benzothiazole derivative 11-C-PBB3 showing higher sensitivity for tau (Maruyama et al., 2013) and MK-6240, a pyrrolo-pyridine-isoquinolone amine has significant tau binding capacity without affinity for normal brain tissue(Hostetler et al., 2016). Notably, 11-C-PBB3 can be quantified using cortical gray matter as reference region for AD and other non-AD taupathies to enhance use in research (Kimura et al., 2016). Further, the newer tau radiotracers such as [18F]RO-948, and [18F]JNJ64349311 (Declercq et al., 2017; Gobbi et al., 2017; Leuzy et al., 2019; Sanabria Bohórquez et al., 2019) have been used to detect tau pathology and it is established that the tau pathology is deposited independently of Aβ deposition and deposition in brain and it is related to age (Lockhart et al., 2017; Pontecorvo et al., 2017; Wuestefeld et al., 2023). Moreover, [18F]RO-948 is also claimed to be promising radiotracer for quantitative imaging in people with AD(Kuwabara et al., 2018).
A recent study suggests that the tau PET is better than amyloid PET and MRI in predicting cognitive change and has a role as a prognostic biomarker in preclinical and prodromal stages of AD(Ossenkoppele et al., 2021).
Structural Biomarkers
Computed tomography (CT) and MRI are two widely used structural imaging technique and CT is less expensive, faster and extensively available than MRI, even in underprivileged nations (Duchesne et al., 2008). However, CT is mostly used to ruling out other reversible causes of dementia such as tumours or subdural haematoma and help elucidate cortical atrophy and ventricular enlargement in AD(Varghese et al., 2013). Cortical atrophy and ventricular enlargement detected on CT scan are very late structural changes in AD and hence limit the use of CT as a biomarker for AD. MRI, another structural imaging technique can readily detect characteristic structural changes of AD such as medial temporal lobe in brain quite early and hence qualify as neuro-imaging biomarker for AD(Dickerson et al., 2011; Georgakas et al., 2023; Johnson et al., 2012).
MRI Biomarkers in AD
It is imperative to discuss the MRI biomarkers amongst the neuroimaging biomarkers as structural MRI is an accessible neuroimaging technique for the evaluation of people with AD and is recommended in various diagnostic guidelines. (National Institute for Health and Care Excellence (UK), 2018). Hippocampus and medial temporal lobe volume measures on MRI are most validated MRI biomarkers for AD but structural and functional connectivity analyses using diffusion tensor imaging and resting state fMRI respectively can depict network disruption in AD. Machine learning techniques offer opportunities to analyse the value of imaging and other biomarkers in AD. (Kehoe et al., 2014).
For more than a decade, a characteristic atrophy pattern on 3DT1weighted and analysis of the location and extent of white matter hyperintensities (WMHs) on T2 weighted MRI have been used to distinguish AD from other causes of dementia (Frisoni et al., 2007). Interestingly, not only visual and voxel-wise analysis of atrophy pattern on MRI images can predict different causes of dementia from AD(Harper et al., 2017) but also location of WMHs in deep and periventricular brain regions are characteristic of cerebral small vessel disease(CSVD), secondary to hypertension, while micro-bleeds in cortical area are characteristic of Aβ pathology(Haller et al., 2018).
With advancement in voxel-based morphometry to extract intracranial volumes including brain volume, hippocampal volume, ventricular volume, cortical thickness and cortical surface area has led to recognition of these as biomarkers in AD. Shape and volume analysis of sub-structural changes in the hippocampus can distinguish AD from other causes of dementia (Kälin et al., 2017). Furthermore, for targeting pre-dementia stages in drug trials, hippocampal volume has been validated as a neuroimaging biomarker.(Hill et al., 2014) The pattern of cortical thinning can detect pre-symptomatic AD subjects, for example in those at genetic risk of AD and can predict severity of symptoms(Dickerson et al., 2009). Furthermore, ventricular volume can also help differentiate AD from healthy controls(Jingnan Wang et al., 2008).
Figure 8.
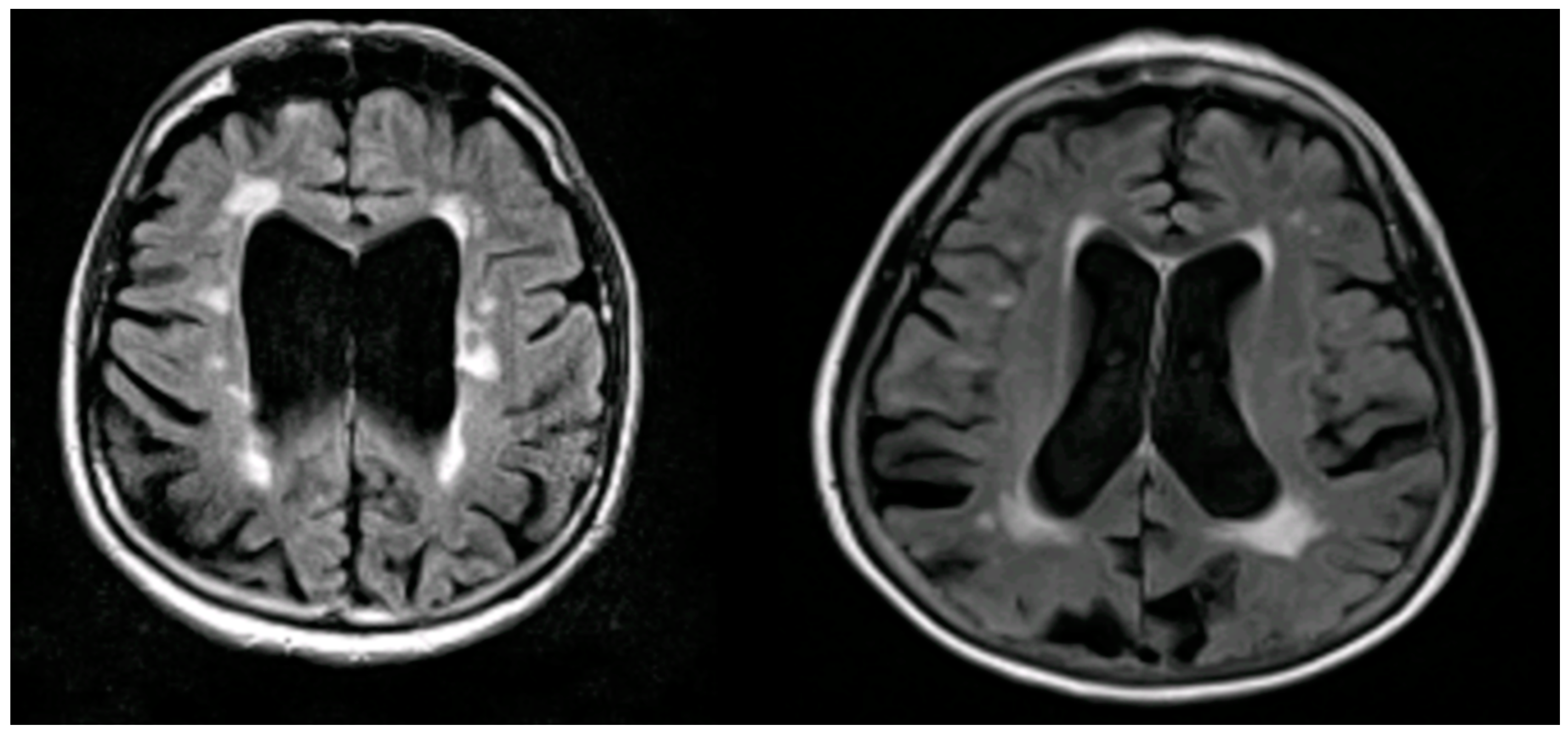
Illustrations of MRI biomarkers in AD showing hippocampal volume(Green and golden colours) and white matter hyperintensities (White and red colours).
Figure 8.
Illustrations of MRI biomarkers in AD showing hippocampal volume(Green and golden colours) and white matter hyperintensities (White and red colours).
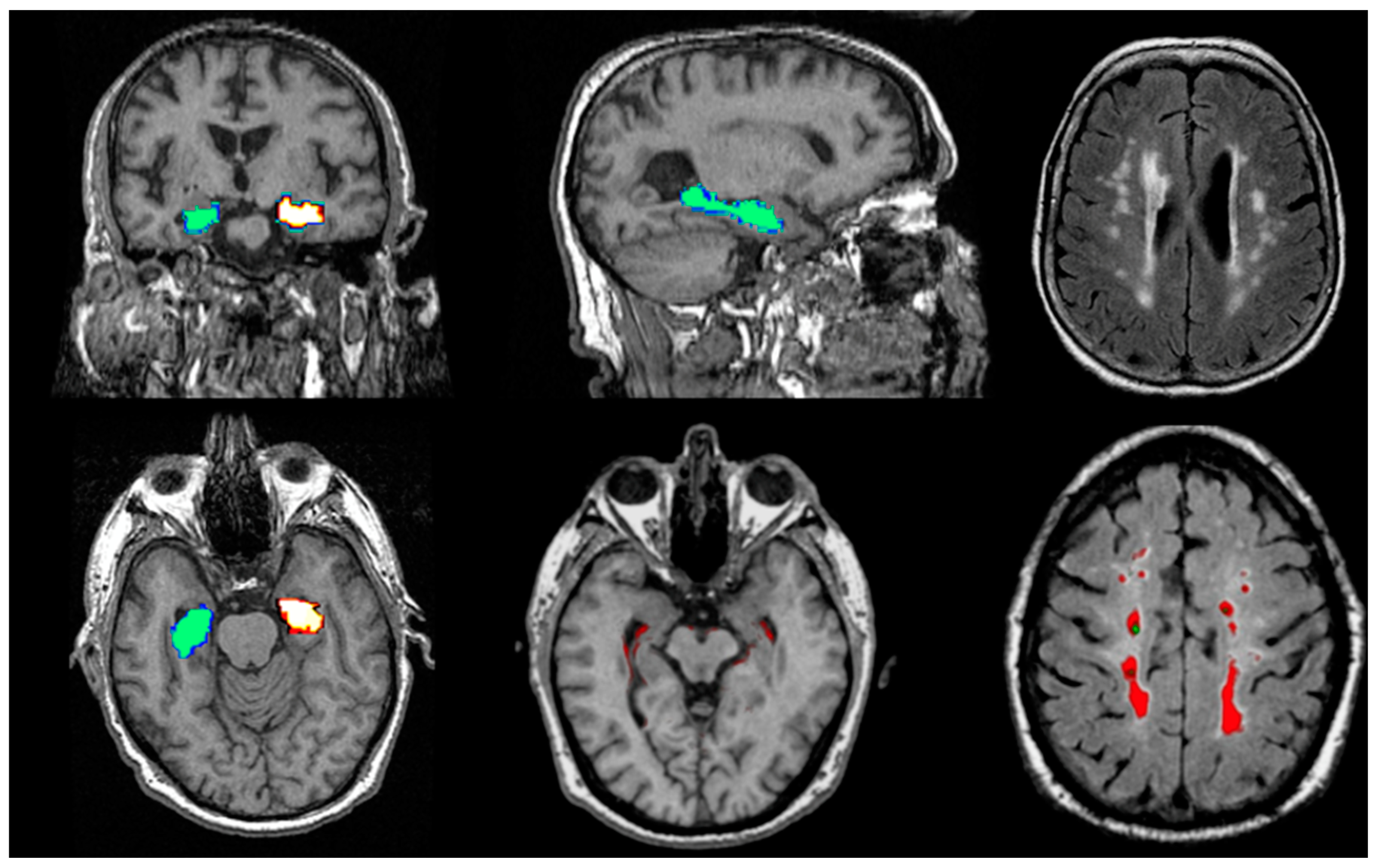
Figure 9.
Illustrations to show WMHs on MRI in people with AD (Courtesy- Jennifer Waymont, University of Aberdeen).
Figure 9.
Illustrations to show WMHs on MRI in people with AD (Courtesy- Jennifer Waymont, University of Aberdeen).
Resting state fMRI has been assessed as a biomarker to distinguish AD from other causes of dementia(Hohenfeld et al., 2018). However, task based fMRI did not show consistent findings (Bakker et al., 2015). Resting state fMRI uses measures based on graph-theory(Khazaee et al., 2015) or functional connectivity(Chen et al., 2011). Resting state fMRI in AD shows changes in the default mode network for interacting brain regions such as hippocampal co-activation (Greicius et al., 2004) and increased activation in medial temporal lobe (Dickerson et al., 2004).
AD has traditionally been considered to be a cortical dementia, but some have demonstrated white matter (WM) abnormalities in AD such as gliosis and demyelination and considered WM damage to be independent of cortical damage (Esrael et al., 2021; Kim et al., 2008). WM damage and axonal deposition of tau may precede the cortical damage (Bendlin et al., 2012; Siger et al., 2009) suggesting not only a link between tau pathology and white matter damage but also the implication of tau in initiation of AD pathogenesis. This WM damage can be quantified using diffusion tensor imaging (DTI), a MRI based neuroimaging technique, which maps the WM microstructure changes in the brain (Croall et al., 2017). Recently, diffuse microstructural changes have been observed in AD on DTI (Esrael et al., 2021).
With regard to the algorithms used for identifying AD from healthy controls, research has been conducted using machine learning, deep learning, or a combination of both approaches and even some studies combine other modalities such as PET and cerebrospinal fluid (CSF) with MRI to differentiate AD from healthy controls and other type of dementias(Xue et al., 2024). Machine learning approaches can classify AD from healthy controls using hippocampal volume, with area under the curve (AUC) of 0.912 (Sørensen et al., 2016). Exploring areas beyond the hippocampus researchers have achieved an AUC of 0.97 using temporal lobe structures including hippocampus, para-hippocampal gyri, entorhinal cortex and peri-rhinal cortex (Chincarini et al., 2011). In order to distinguish AD from other dementias, machine learning approach achieved an AUC of 0.948 and 0.731 with DLB for testing and training dataset, respectively (Lebedev et al., 2013). Moreover, an AUC of 0.93 has been achieved in differentiating AD from FTD by developing frontotemporal dementia index which is a ratio of weighted sum of volumetric indexes of FTD dominant and AD dominant structures on MRI (Yu et al., 2021). Hence, it can be concluded that machine learning seems to be widely used for classification of AD to differentiate it either from healthy controls or other causes of dementia.
Conclusion
Imaging biomarkers are of proven utility in supporting a clinical diagnosis of AD in a person with dementia, in selecting those to participate in clinical trials, monitoring progression and measuring response to treatment. The combination of biomarkers along with other personalised variables and genetic variables in convoluted neural network artificial intelligence algorithms that have been trained and validated using real-world data are likely to be the most valuable in defining who, when, and with what to treat in future.
References
- Agdeppa, E.D., Kepe, V., Liu, J., Flores-Torres, S., Satyamurthy, N., Petric, A., Cole, G.M., Small, G.W., Huang, S.C., Barrio, J.R., 2001. Binding characteristics of radiofluorinated 6-dialkylamino-2-naphthylethylidene derivatives as positron emission tomography imaging probes for beta-amyloid plaques in Alzheimer’s disease. J Neurosci 21, RC189. [CrossRef]
- AKDEMİR, Ü.Ö., BORA TOKÇAER, A., ATAY1, L.Ö., 2021. Dopamine transporter SPECT imaging in Parkinson’s disease and parkinsonian disorders. Turk J Med Sci 51, 400–410. [CrossRef]
- Antonini, A., Leenders, K.L., Vontobel, P., Maguire, R.P., Missimer, J., Psylla, M., Günther, I., 1997. Complementary PET studies of striatal neuronal function in the differential diagnosis between multiple system atrophy and Parkinson’s disease. Brain 120, 2187–2195. [CrossRef]
- Arriagada, P.V., Growdon, J.H., Hedley-Whyte, E.T., Hyman, B.T., 1992. Neurofibrillary tangles but not senile plaques parallel duration and severity of Alzheimer’s disease. Neurology 42, 631–639. [CrossRef]
- Bachurin, S.O., Bovina, E.V., Ustyugov, A.A., 2017. Drugs in Clinical Trials for Alzheimer’s Disease: The Major Trends. Med Res Rev 37, 1186–1225. [CrossRef]
- Bailly, M., Destrieux, C., Hommet, C., Mondon, K., Cottier, J.-P., Beaufils, E., Vierron, E., Vercouillie, J., Ibazizene, M., Voisin, T., Payoux, P., Barré, L., Camus, V., Guilloteau, D., Ribeiro, M.-J., 2015. Precuneus and Cingulate Cortex Atrophy and Hypometabolism in Patients with Alzheimer’s Disease and Mild Cognitive Impairment: MRI and 18F-FDG PET Quantitative Analysis Using FreeSurfer. Biomed Res Int 2015. [CrossRef]
- Bakker, A., Albert, M.S., Krauss, G., Speck, C.L., Gallagher, M., 2015. Response of the medial temporal lobe network in amnestic mild cognitive impairment to therapeutic intervention assessed by fMRI and memory task performance. Neuroimage Clin 7, 688–698. [CrossRef]
- Barthel, H., 2020. First Tau PET Tracer Approved: Toward Accurate In Vivo Diagnosis of Alzheimer Disease. Journal of Nuclear Medicine 61, 1409–1410. [CrossRef]
- Bendlin, B.B., Carlsson, C.M., Johnson, S.C., Zetterberg, H., Blennow, K., Willette, A.A., Okonkwo, O.C., Sodhi, A., Ries, M.L., Birdsill, A.C., Alexander, A.L., Rowley, H.A., Puglielli, L., Asthana, S., Sager, M.A., 2012. CSF T-Tau/Aβ42 predicts white matter microstructure in healthy adults at risk for Alzheimer’s disease. PLoS One 7, e37720. [CrossRef]
- Bhogal, P., Mahoney, C., Graeme-Baker, S., Roy, A., Shah, S., Fraioli, F., Cowley, P., Jäger, H.R., 2013. The common dementias: a pictorial review. Eur Radiol 23, 3405–3417. [CrossRef]
- Bierer, L.M., Hof, P.R., Purohit, D.P., Carlin, L., Schmeidler, J., Davis, K.L., Perl, D.P., 1995. Neocortical Neurofibrillary Tangles Correlate With Dementia Severity in Alzheimer’s Disease. Archives of Neurology 52, 81–88. [CrossRef]
- Bouter, C., Henniges, P., Franke, T.N., Irwin, C., Sahlmann, C.O., Sichler, M.E., Beindorff, N., Bayer, T.A., Bouter, Y., 2018. 18F-FDG-PET Detects Drastic Changes in Brain Metabolism in the Tg4-42 Model of Alzheimer’s Disease. Front Aging Neurosci 10, 425. [CrossRef]
- Braak, H., Braak, E., 1997. Staging of Alzheimer-related cortical destruction. Int Psychogeriatr 9 Suppl 1, 257–261; discussion 269-272.
- Braak, H., Braak, E., 1991. Neuropathological stageing of Alzheimer-related changes. Acta Neuropathol. 82, 239–259. [CrossRef]
- Brass, L.M., Walovitch, R.C., Joseph, J.L., Léveillé, J., Marchand, L., Hellman, R.S., Tikofsky, R.S., Masdeu, J.C., Hall, K.M., Van Heertum, R.L., 1994. The role of single photon emission computed tomography brain imaging with 99mTc-bicisate in the localization and definition of mechanism of ischemic stroke. J Cereb Blood Flow Metab 14 Suppl 1, S91-98.
- Brigo, F., Matinella, A., Erro, R., Tinazzi, M., 2014. [123I]FP-CIT SPECT (DaTSCAN) may be a useful tool to differentiate between Parkinson’s disease and vascular or drug-induced parkinsonisms: a meta-analysis. Eur J Neurol 21, 1369-e90. [CrossRef]
- Brown, J.A., Deng, J., Neuhaus, J., Sible, I.J., Sias, A.C., Lee, S.E., Kornak, J., Marx, G.A., Karydas, A.M., Spina, S., Grinberg, L.T., Coppola, G., Geschwind, D.H., Kramer, J.H., Gorno-Tempini, M.L., Miller, B.L., Rosen, H.J., Seeley, W.W., 2019. Patient-Tailored, Connectivity-Based Forecasts of Spreading Brain Atrophy. Neuron 104, 856-868.e5. [CrossRef]
- Brown, R.K.J., Bohnen, N.I., Wong, K.K., Minoshima, S., Frey, K.A., 2014. Brain PET in Suspected Dementia: Patterns of Altered FDG Metabolism. RadioGraphics 34, 684–701. [CrossRef]
- Catafau, A.M., 2001. Brain SPECT in clinical practice. Part I: perfusion. J Nucl Med 42, 259–271.
- Chen, G., Ward, B.D., Xie, C., Li, W., Wu, Z., Jones, J.L., Franczak, M., Antuono, P., Li, S.-J., 2011. Classification of Alzheimer disease, mild cognitive impairment, and normal cognitive status with large-scale network analysis based on resting-state functional MR imaging. Radiology 259, 213–221. [CrossRef]
- Chen, K., Langbaum, J.B.S., Fleisher, A.S., Ayutyanont, N., Reschke, C., Lee, W., Liu, X., Bandy, D., Alexander, G.E., Thompson, P.M., Foster, N.L., Harvey, D.J., de Leon, M.J., Koeppe, R.A., Jagust, W.J., Weiner, M.W., Reiman, E.M., 2010. Twelve-Month Metabolic Declines in Probable Alzheimer’s Disease and Amnestic Mild Cognitive Impairment Assessed Using an Empirically Pre-Defined Statistical Region-of-Interest: Findings from the Alzheimer’s Disease Neuroimaging Initiative. Neuroimage 51, 654–664. [CrossRef]
- Chen, S.-D., Lu, J.-Y., Li, H.-Q., Yang, Y.-X., Jiang, J.-H., Cui, M., Zuo, C.-T., Tan, L., Dong, Q., Yu, J.-T., for the Alzheimer’s Disease Neuroimaging Initiative, Weiner, M.W., Aisen, P., Petersen, Ronald, Jack, C.R., Jagust, W., Trojanowki, J.Q., Toga, A.W., Beckett, L., Green, R.C., Saykin, A.J., Morris, J.C., Perrin, R.J., Shaw, L.M., Carrillo, M., Potter, W., Barnes, L., Bernard, M., González, H., Ho, C., Hsiao, J.K., Jackson, J., Masliah, E., Masterman, D., Okonkwo, O., Perrin, R., Ryan, L., Silverberg, N., Fleisher, A., Sacrey, D.T., Fockler, J., Conti, C., Veitch, D., Neuhaus, J., Jin, C., Nosheny, R., Ashford, M., Flenniken, D., Kormos, A., Rafii, M., Raman, R., Jimenez, G., Donohue, Michael, Gessert, D., Salazar, J., Zimmerman, C., Cabrera, Y., Walter, S., Miller, G., Coker, G., Clanton, T., Hergesheimer, L., Smith, S., Adegoke, O., Mahboubi, P., Moore, S., Pizzola, J., Shaffer, E., Sloan, B., Harvey, D., Forghanian-Arani, A., Borowski, B., Ward, C., Schwarz, C., Jones, D., Gunter, J., Kantarci, K., Senjem, Matthew, Vemuri, P., Reid, R., Fox, N.C., Malone, I., Thompson, P., Thomopoulos, S.I., Nir, T.M., Jahanshad, N., DeCarli, C., Knaack, A., Fletcher, E., Tosun-Turgut, D., Chen, S.R., Choe, M., Crawford, K., Yushkevich, P.A., Das, S., Koeppe, R.A., Reiman, E.M., Chen, K., Mathis, C., Landau, S., Cairns, N.J., Householder, E., Franklin, E., Bernhardt, H., Taylor-Reinwald, L., Shaw, L.M., Trojanowki, J.Q., Korecka, M., Figurski, M., Crawford, K., Neu, S., Saykin, A.J., Nho, K., Risacher, S.L., Apostolova, L.G., Shen, L., Foroud, T.M., Nudelman, K., Faber, K., Wilmes, K., Thal, L., Khachaturian, Z., Hsiao, J.K., Silbert, L.C., Lind, B., Crissey, R., Kaye, J.A., Carter, R., Dolen, S., Quinn, J., Schneider, L.S., Pawluczyk, S., Becerra, M., Teodoro, L., Dagerman, K., Spann, B.M., Brewer, J., Vanderswag, H., Fleisher, A., Ziolkowski, J., Heidebrink, J.L., Zbizek-Nulph, L., Lord, J.L., Mason, S.S., Albers, C.S., Knopman, D., Johnson, Kris, Villanueva-Meyer, J., Pavlik, V., Pacini, N., Lamb, A., Kass, J.S., Doody, R.S., Shibley, V., Chowdhury, M., Rountree, S., Dang, M., Stern, Y., Honig, L.S., Mintz, A., Ances, B., Winkfield, D., Carroll, M., Stobbs-Cucchi, G., Oliver, A., Creech, M.L., Mintun, M.A., Schneider, S., Geldmacher, D., Love, M.N., Griffith, R., Clark, D., Brockington, J., Marson, D., Grossman, H., Goldstein, M.A., Greenberg, J., Mitsis, E., Shah, R.C., Lamar, M., Samuels, P., Duara, R., Greig-Custo, M.T., Rodriguez, R., Albert, M., Onyike, C., Farrington, L., Rudow, S., Brichko, R., Kielb, S., Smith, A., Raj, B.A., Fargher, K., Sadowski, M., Wisniewski, T., Shulman, M., Faustin, A., Rao, J., Castro, K.M., Ulysse, A., Chen, S., Sheikh, M.O., Singleton-Garvin, J., Doraiswamy, P.M., Petrella, J.R., James, O., Wong, T.Z., Borges-Neto, S., Karlawish, J.H., Wolk, D.A., Vaishnavi, S., Clark, C.M., Arnold, S.E., Smith, C.D., Jicha, G.A., El Khouli, R., Raslau, F.D., Lopez, O.L., Oakley, M., Simpson, D.M., Porsteinsson, A.P., Martin, K., Kowalski, N., Keltz, M., Goldstein, B.S., Makino, K.M., Ismail, M.S., Brand, C., Thai, G., Pierce, A., Yanez, B., Sosa, E., Witbracht, M., Kelley, B., Nguyen, T., Womack, K., Mathews, D., Quiceno, M., Levey, A.I., Lah, J.J., Hajjar, I., Cellar, J.S., Burns, J.M., Swerdlow, R.H., Brooks, W.M., Silverman, D.H.S., Kremen, S., Apostolova, L., Tingus, K., Lu, P.H., Bartzokis, G., Woo, E., Teng, E., Graff-Radford, N.R., Parfitt, F., Poki-Walker, K., Farlow, M.R., Hake, A.M., Matthews, B.R., Brosch, J.R., Herring, S., van Dyck, C.H., Mecca, A.P., Good, S.P., MacAvoy, M.G., Carson, R.E., Varma, P., Chertkow, H., Vaitekunis, S., Hosein, C., Black, S., Stefanovic, B., Heyn, C., Hsiung, G.-Y.R., Kim, E., Mudge, B., Sossi, V., Feldman, H., Assaly, M., Finger, E., Pasternak, S., Rachinsky, I., Kertesz, A., Drost, D., Rogers, J., Grant, I., Muse, B., Rogalski, E., Robson, J., Mesulam, M.-M., Kerwin, D., Wu, C.-K., Johnson, N., Lipowski, K., Weintraub, S., Bonakdarpour, B., Pomara, N., Hernando, R., Sarrael, A., Rosen, H.J., Miller, B.L., Perry, D., Turner, R.S., Johnson, Kathleen, Reynolds, B., MCCann, K., Poe, J., Sperling, R.A., Johnson, K.A., Marshall, G.A., Belden, C.M., Atri, A., Spann, B.M., Clark, K.A., Zamrini, E., Sabbagh, M., Killiany, R., Stern, R., Mez, J., Kowall, N., Budson, A.E., Obisesan, T.O., Ntekim, O.E., Wolday, S., Khan, J.I., Nwulia, E., Nadarajah, S., Lerner, A., Ogrocki, P., Tatsuoka, C., Fatica, P., Fletcher, E., Maillard, P., Olichney, J., DeCarli, C., Carmichael, O., Bates, V., Capote, H., Rainka, M., Borrie, M., Lee, T.-Y., Bartha, R., Johnson, S., Asthana, S., Carlsson, C.M., Perrin, A., Burke, A., Scharre, D.W., Kataki, M., Tarawneh, R., Kelley, B., Hart, D., Zimmerman, E.A., Celmins, D., Miller, D.D., Boles Ponto, L.L., Smith, K.E., Koleva, H., Shim, H., Nam, K.W., Schultz, S.K., Williamson, J.D., Craft, S., Cleveland, J., Yang, M., Sink, K.M., Ott, B.R., Drake, J., Tremont, G., Daiello, L.A., Drake, J.D., Sabbagh, M., Ritter, A., Bernick, C., Munic, D., Mintz, A., O’Connelll, A., Mintzer, J., Wiliams, A., Masdeu, J., Shi, J., Garcia, A., Sabbagh, M., Newhouse, P., Potkin, S., Salloway, S., Malloy, P., Correia, S., Kittur, S., Pearlson, G.D., Blank, K., Anderson, K., Flashman, L.A., Seltzer, M., Hynes, M.L., Santulli, R.B., Relkin, N., Chiang, G., Lin, M., Ravdin, L., Lee, A., Petersen, Ron, Neylan, T., Grafman, J., Montine, T., Petersen, Ronald, Hergesheimer, L., Danowski, S., Nguyen-Barrera, C., Hayes, J., Finley, S., Donohue, Michael, Bernstein, M., Senjem, Matt, Ward, C., Chen, S.R., Koeppe, R.A., Foster, N., Foroud, T.M., Potkin, S., Shen, L., Faber, K., Kim, S., Nho, K., Wilmes, K., Spann, B.M., Vanderswag, H., Fleisher, A., Sood, A., Blanchard, K.S., Fleischman, D., Arfanakis, K., Varon, D., Greig, M.T., Goldstein, B., Martin, K.S., Thai, G., Pierce, A., Reist, C., Yanez, B., Sosa, E., Witbracht, M., Sadowsky, C., Martinez, W., Villena, T., Rosen, H., Marshall, G., Nadarajah, S., Peskind, E.R., Petrie, E.C., Li, G., Yesavage, J., Taylor, J.L., Chao, S., Coleman, J., White, J.D., Lane, B., Rosen, A., Tinklenberg, J., Chiang, G., Mackin, S., Raman, R., Jimenez-Maggiora, G., Gessert, D., Salazar, J., Zimmerman, C., Walter, S., Adegoke, O., Mahboubi, P., Drake, E., Donohue, Mike, Nelson, C., Bickford, D., Butters, M., Zmuda, M., Borowski, B., Gunter, J., Senjem, Matt, Kantarci, K., Ward, C., Reyes, D., Faber, K.M., Nudelman, K.N., Au, Y.H., Scherer, K., Catalinotto, D., Stark, S., Ong, E., Fernandez, D., Zmuda, M., 2021. Staging tau pathology with tau PET in Alzheimer’s disease: a longitudinal study. Transl Psychiatry 11, 483. [CrossRef]
- Chien, D.T., Bahri, S., Szardenings, A.K., Walsh, J.C., Mu, F., Su, M.-Y., Shankle, W.R., Elizarov, A., Kolb, H.C., 2013. Early clinical PET imaging results with the novel PHF-tau radioligand [F-18]-T807. J. Alzheimers Dis. 34, 457–468. [CrossRef]
- Chincarini, A., Bosco, P., Calvini, P., Gemme, G., Esposito, M., Olivieri, C., Rei, L., Squarcia, S., Rodriguez, G., Bellotti, R., Cerello, P., De Mitri, I., Retico, A., Nobili, F., Alzheimer’s Disease Neuroimaging Initiative, 2011. Local MRI analysis approach in the diagnosis of early and prodromal Alzheimer’s disease. Neuroimage 58, 469–480. [CrossRef]
- Cho, H., Choi, J.Y., Hwang, M.S., Lee, J.H., Kim, Y.J., Lee, H.M., Lyoo, C.H., Ryu, Y.H., Lee, M.S., 2016. Tau PET in Alzheimer disease and mild cognitive impairment. Neurology 87, 375–383. [CrossRef]
- Chow, T.W., Fam, D., Graff-Guerrero, A., Verhoeff, N.P.G., Tang-Wai, D.F., Masellis, M., Black, S.E., Wilson, A.A., Houle, S., Pollock, B.G., 2013. Fluorodeoxyglucose positron emission tomography in semantic dementia after 6 months of memantine: an open-label pilot study. Int J Geriatr Psychiatry 28, 319–325. [CrossRef]
- Clark, C.M., Schneider, J.A., Bedell, B.J., Beach, T.G., Bilker, W.B., Mintun, M.A., Pontecorvo, M.J., Hefti, F., Carpenter, A.P., Flitter, M.L., Krautkramer, M.J., Kung, H.F., Coleman, R.E., Doraiswamy, P.M., Fleisher, A.S., Sabbagh, M.N., Sadowsky, C.H., Reiman, E.P., Reiman, P.E.M., Zehntner, S.P., Skovronsky, D.M., AV45-A07 Study Group, 2011. Use of florbetapir-PET for imaging beta-amyloid pathology. JAMA 305, 275–283. [CrossRef]
- Claus, J.J., Walstra, G.J., Hijdra, A., Van Royen, E.A., Verbeeten, B., van Gool, W.A., 1999. Measurement of temporal regional cerebral perfusion with single-photon emission tomography predicts rate of decline in language function and survival in early Alzheimer’s disease. Eur J Nucl Med 26, 265–271. [CrossRef]
- Corrada, M.M., Brookmeyer, R., Paganini-Hill, A., Berlau, D., Kawas, C.H., 2010. Dementia Incidence Continues to Increase with Age in the Oldest Old The 90+ Study. Ann Neurol 67, 114–121. [CrossRef]
- Croall, I.D., Lohner, V., Moynihan, B., Khan, U., Hassan, A., O’Brien, J.T., Morris, R.G., Tozer, D.J., Cambridge, V.C., Harkness, K., Werring, D.J., Blamire, A.M., Ford, G.A., Barrick, T.R., Markus, H.S., 2017. Using DTI to assess white matter microstructure in cerebral small vessel disease (SVD) in multicentre studies. Clin Sci (Lond) 131, 1361–1373. [CrossRef]
- Dave, A., Hansen, N., Downey, R., Johnson, C., 2020. FDG-PET Imaging of Dementia and Neurodegenerative Disease. Semin Ultrasound CT MR 41, 562–571. [CrossRef]
- Declercq, L., Rombouts, F., Koole, M., Fierens, K., Mariën, J., Langlois, X., Andrés, J.I., Schmidt, M., Macdonald, G., Moechars, D., Vanduffel, W., Tousseyn, T., Vandenberghe, R., Van Laere, K., Verbruggen, A., Bormans, G., 2017. Preclinical Evaluation of 18F-JNJ64349311, a Novel PET Tracer for Tau Imaging. J. Nucl. Med. 58, 975–981. [CrossRef]
- Devous, M.D., 2005. Single-photon emission computed tomography in neurotherapeutics. NeuroRx 2, 237–249. [CrossRef]
- Dickerson, B.C., Bakkour, A., Salat, D.H., Feczko, E., Pacheco, J., Greve, D.N., Grodstein, F., Wright, C.I., Blacker, D., Rosas, H.D., Sperling, R.A., Atri, A., Growdon, J.H., Hyman, B.T., Morris, J.C., Fischl, B., Buckner, R.L., 2009. The cortical signature of Alzheimer’s disease: regionally specific cortical thinning relates to symptom severity in very mild to mild AD dementia and is detectable in asymptomatic amyloid-positive individuals. Cereb Cortex 19, 497–510. [CrossRef]
- Dickerson, B.C., Salat, D.H., Bates, J.F., Atiya, M., Killiany, R.J., Greve, D.N., Dale, A.M., Stern, C.E., Blacker, D., Albert, M.S., Sperling, R.A., 2004. Medial temporal lobe function and structure in mild cognitive impairment. Ann Neurol 56, 27–35. [CrossRef]
- Dickerson, B.C., Stoub, T.R., Shah, R.C., Sperling, R.A., Killiany, R.J., Albert, M.S., Hyman, B.T., Blacker, D., Detoledo-Morrell, L., 2011. Alzheimer-signature MRI biomarker predicts AD dementia in cognitively normal adults. Neurology 76, 1395–1402. [CrossRef]
- Dougall, N.J., Bruggink, S., Ebmeier, K.P., 2004. Systematic review of the diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia. Am J Geriatr Psychiatry 12, 554–570. [CrossRef]
- Dubois, B., Feldman, H.H., Jacova, C., Hampel, H., Molinuevo, J.L., Blennow, K., DeKosky, S.T., Gauthier, S., Selkoe, D., Bateman, R., Cappa, S., Crutch, S., Engelborghs, S., Frisoni, G.B., Fox, N.C., Galasko, D., Habert, M.-O., Jicha, G.A., Nordberg, A., Pasquier, F., Rabinovici, G., Robert, P., Rowe, C., Salloway, S., Sarazin, M., Epelbaum, S., de Souza, L.C., Vellas, B., Visser, P.J., Schneider, L., Stern, Y., Scheltens, P., Cummings, J.L., 2014. Advancing research diagnostic criteria for Alzheimer’s disease: the IWG-2 criteria. Lancet Neurol 13, 614–629. [CrossRef]
- Dubois, B., von Arnim, C.A.F., Burnie, N., Bozeat, S., Cummings, J., 2023. Biomarkers in Alzheimer’s disease: role in early and differential diagnosis and recognition of atypical variants. Alzheimers Res Ther 15, 175. [CrossRef]
- Duchesne, S., Caroli, A., Geroldi, C., Barillot, C., Frisoni, G.B., Collins, D.L., 2008. MRI-based automated computer classification of probable AD versus normal controls. IEEE Trans Med Imaging 27, 509–520. [CrossRef]
- Echeveste, B., Prieto, E., Guillén, E.F., Jimenez, A., Montoya, G., Villino, R., Riverol, M., Arbizu, J., 2025. Combination of amyloid and FDG PET for the prediction of short-term conversion from MCI to Alzheimer´s disease in the clinical practice. Eur J Nucl Med Mol Imaging. [CrossRef]
- Elman, J.A., Panizzon, M.S., Gustavson, D.E., Franz, C.E., Sanderson-Cimino, M.E., Lyons, M.J., Kremen, W.S., 2020. Amyloid-β Positivity Predicts Cognitive Decline but Cognition Predicts Progression to Amyloid-β Positivity. Biological Psychiatry 87, 819–828. [CrossRef]
- Esrael, S.M.A.M., Hamed, A.M.M., Khedr, E.M., Soliman, R.K., 2021. Application of diffusion tensor imaging in Alzheimer’s disease: quantification of white matter microstructural changes. Egyptian Journal of Radiology and Nuclear Medicine 52, 89. [CrossRef]
- Filippi, L., Chiaravalloti, A., Bagni, O., Schillaci, O., 2018. 18F-labeled radiopharmaceuticals for the molecular neuroimaging of amyloid plaques in Alzheimer’s disease. Am J Nucl Med Mol Imaging 8, 268–281.
- Fleisher, A.S., Pontecorvo, M.J., Devous, M.D., Lu, M., Arora, A.K., Truocchio, S.P., Aldea, P., Flitter, M., Locascio, T., Devine, M., Siderowf, A., Beach, T.G., Montine, T.J., Serrano, G.E., Curtis, C., Perrin, A., Salloway, S., Daniel, M., Wellman, C., Joshi, A.D., Irwin, D.J., Lowe, V.J., Seeley, W.W., Ikonomovic, M.D., Masdeu, J.C., Kennedy, I., Harris, T., Navitsky, M., Southekal, S., Mintun, M.A., A16 Study Investigators, 2020. Positron Emission Tomography Imaging With [18F]flortaucipir and Postmortem Assessment of Alzheimer Disease Neuropathologic Changes. JAMA Neurol 77, 829–839. [CrossRef]
- Fodero-Tavoletti, M.T., Okamura, N., Furumoto, S., Mulligan, R.S., Connor, A.R., McLean, C.A., Cao, D., Rigopoulos, A., Cartwright, G.A., O’Keefe, G., Gong, S., Adlard, P.A., Barnham, K.J., Rowe, C.C., Masters, C.L., Kudo, Y., Cappai, R., Yanai, K., Villemagne, V.L., 2011. 18F-THK523: a novel in vivo tau imaging ligand for Alzheimer’s disease. Brain 134, 1089–1100. [CrossRef]
- Frisoni, G.B., Pievani, M., Testa, C., Sabattoli, F., Bresciani, L., Bonetti, M., Beltramello, A., Hayashi, K.M., Toga, A.W., Thompson, P.M., 2007. The topography of grey matter involvement in early and late onset Alzheimer’s disease. Brain 130, 720–730. [CrossRef]
- Georgakas, J.E., Howe, M.D., Thompson, L.I., Riera, N.M., Riddle, M.C., 2023. Biomarkers of Alzheimer’s disease: Past, present and future clinical use. Biomarkers in Neuropsychiatry 8, 100063. [CrossRef]
- Gobbi, L.C., Knust, H., Körner, M., Honer, M., Czech, C., Belli, S., Muri, D., Edelmann, M.R., Hartung, T., Erbsmehl, I., Grall-Ulsemer, S., Koblet, A., Rueher, M., Steiner, S., Ravert, H.T., Mathews, W.B., Holt, D.P., Kuwabara, H., Valentine, H., Dannals, R.F., Wong, D.F., Borroni, E., 2017. Identification of Three Novel Radiotracers for Imaging Aggregated Tau in Alzheimer’s Disease with Positron Emission Tomography. J. Med. Chem. 60, 7350–7370. [CrossRef]
- Greicius, M.D., Srivastava, G., Reiss, A.L., Menon, V., 2004. Default-mode network activity distinguishes Alzheimer’s disease from healthy aging: evidence from functional MRI. Proc Natl Acad Sci U S A 101, 4637–4642. [CrossRef]
- Gunes, S., Aizawa, Y., Sugashi, T., Sugimoto, M., Rodrigues, P.P., 2022. Biomarkers for Alzheimer’s Disease in the Current State: A Narrative Review. Int J Mol Sci 23, 4962. [CrossRef]
- Haller, S., Vernooij, M.W., Kuijer, J.P.A., Larsson, E.-M., Jäger, H.R., Barkhof, F., 2018. Cerebral Microbleeds: Imaging and Clinical Significance. Radiology 287, 11–28. [CrossRef]
- Hampel, H., O’Bryant, S.E., Durrleman, S., Younesi, E., Rojkova, K., Escott-Price, V., Corvol, J.-C., Broich, K., Dubois, B., Lista, S., Alzheimer Precision Medicine Initiative, 2017. A Precision Medicine Initiative for Alzheimer’s disease: the road ahead to biomarker-guided integrative disease modeling. Climacteric 20, 107–118. [CrossRef]
- Harada, R., Okamura, N., Furumoto, S., Furukawa, K., Ishiki, A., Tomita, N., Hiraoka, K., Watanuki, S., Shidahara, M., Miyake, M., Ishikawa, Y., Matsuda, R., Inami, A., Yoshikawa, T., Tago, T., Funaki, Y., Iwata, R., Tashiro, M., Yanai, K., Arai, H., Kudo, Y., 2015. [(18)F]THK-5117 PET for assessing neurofibrillary pathology in Alzheimer’s disease. Eur. J. Nucl. Med. Mol. Imaging 42, 1052–1061. [CrossRef]
- Harada, R., Okamura, N., Furumoto, S., Furukawa, K., Ishiki, A., Tomita, N., Tago, T., Hiraoka, K., Watanuki, S., Shidahara, M., Miyake, M., Ishikawa, Y., Matsuda, R., Inami, A., Yoshikawa, T., Funaki, Y., Iwata, R., Tashiro, M., Yanai, K., Arai, H., Kudo, Y., 2016. 18F-THK5351: A Novel PET Radiotracer for Imaging Neurofibrillary Pathology in Alzheimer Disease. J Nucl Med 57, 208–214. [CrossRef]
- Harper, L., Bouwman, F., Burton, E.J., Barkhof, F., Scheltens, P., O’Brien, J.T., Fox, N.C., Ridgway, G.R., Schott, J.M., 2017. Patterns of atrophy in pathologically confirmed dementias: a voxelwise analysis. J. Neurol. Neurosurg. Psychiatry 88, 908–916. [CrossRef]
- Harrison, T.M., Du, R., Klencklen, G., Baker, S.L., Jagust, W.J., 2021. Distinct effects of beta-amyloid and tau on cortical thickness in cognitively healthy older adults. Alzheimers Dement 17, 1085–1096. [CrossRef]
- Heyer, S., Simon, M., Doyen, M., Mortada, A., Roch, V., Jeanbert, E., Thilly, N., Malaplate, C., Kearney-Schwartz, A., Jonveaux, T., Bannay, A., Verger, A., 2024. 18F-FDG PET can effectively rule out conversion to dementia and the presence of CSF biomarker of neurodegeneration: a real-world data analysis. Alzheimers Res Ther 16, 182. [CrossRef]
- Hill, D.L.G., Schwarz, A.J., Isaac, M., Pani, L., Vamvakas, S., Hemmings, R., Carrillo, M.C., Yu, P., Sun, J., Beckett, L., Boccardi, M., Brewer, J., Brumfield, M., Cantillon, M., Cole, P.E., Fox, N., Frisoni, G.B., Jack, C., Kelleher, T., Luo, F., Novak, G., Maguire, P., Meibach, R., Patterson, P., Bain, L., Sampaio, C., Raunig, D., Soares, H., Suhy, J., Wang, H., Wolz, R., Stephenson, D., 2014. Coalition Against Major Diseases/European Medicines Agency biomarker qualification of hippocampal volume for enrichment of clinical trials in predementia stages of Alzheimer’s disease. Alzheimers Dement 10, 421-429.e3. [CrossRef]
- Hohenfeld, C., Werner, C.J., Reetz, K., 2018. Resting-state connectivity in neurodegenerative disorders: Is there potential for an imaging biomarker? Neuroimage Clin 18, 849–870. [CrossRef]
- Høilund-Carlsen, P.F., Revheim, M.-E., Costa, T., Kepp, K.P., Castellani, R.J., Perry, G., Alavi, A., Barrio, J.R., 2023. FDG-PET versus Amyloid-PET Imaging for Diagnosis and Response Evaluation in Alzheimer’s Disease: Benefits and Pitfalls. Diagnostics (Basel) 13, 2254. [CrossRef]
- Holman, B.L., Johnson, K.A., Gerada, B., Carvalho, P.A., Satlin, A., 1992. The scintigraphic appearance of Alzheimer’s disease: a prospective study using technetium-99m-HMPAO SPECT. J Nucl Med 33, 181–185.
- Hostetler, E.D., Walji, A.M., Zeng, Z., Miller, P., Bennacef, I., Salinas, C., Connolly, B., Gantert, L., Haley, H., Holahan, M., Purcell, M., Riffel, K., Lohith, T.G., Coleman, P., Soriano, A., Ogawa, A., Xu, S., Zhang, X., Joshi, E., Della Rocca, J., Hesk, D., Schenk, D.J., Evelhoch, J.L., 2016. Preclinical Characterization of 18F-MK-6240, a Promising PET Tracer for In Vivo Quantification of Human Neurofibrillary Tangles. J. Nucl. Med. 57, 1599–1606. [CrossRef]
- Huijbers, W., Mormino, E.C., Schultz, A.P., Wigman, S., Ward, A.M., Larvie, M., Amariglio, R.E., Marshall, G.A., Rentz, D.M., Johnson, K.A., Sperling, R.A., 2015. Amyloid-β deposition in mild cognitive impairment is associated with increased hippocampal activity, atrophy and clinical progression. Brain 138, 1023–1035. [CrossRef]
- Humpel, C., 2011. Identifying and validating biomarkers for Alzheimer’s disease. Trends Biotechnol 29, 26–32. [CrossRef]
- Imokawa, T., Yokoyama, K., Takahashi, K., Oyama, J., Tsuchiya, J., Sanjo, N., Tateishi, U., 2024. Brain perfusion SPECT in dementia: what radiologists should know. Jpn J Radiol 42, 1215–1230. [CrossRef]
- Ishii, K., Imamura, T., Sasaki, M., Yamaji, S., Sakamoto, S., Kitagaki, H., Hashimoto, M., Hirono, N., Shimomura, T., Mori, E., 1998. Regional cerebral glucose metabolism in dementia with Lewy bodies and Alzheimer’s disease. Neurology 51, 125–130. [CrossRef]
- Ito, K., Inui, Y., Kizawa, T., Kimura, Y., Kato, T., 2017. Current and future prospects of nuclear medicine in dementia. Rinsho Shinkeigaku 57, 479–484. [CrossRef]
- Jack, C.R., Bennett, D.A., Blennow, K., Carrillo, M.C., Dunn, B., Haeberlein, S.B., Holtzman, D.M., Jagust, W., Jessen, F., Karlawish, J., Liu, E., Molinuevo, J.L., Montine, T., Phelps, C., Rankin, K.P., Rowe, C.C., Scheltens, P., Siemers, E., Snyder, H.M., Sperling, R., Contributors, 2018. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimers Dement 14, 535–562. [CrossRef]
- Jack, C.R., Bennett, D.A., Blennow, K., Carrillo, M.C., Feldman, H.H., Frisoni, G.B., Hampel, H., Jagust, W.J., Johnson, K.A., Knopman, D.S., Petersen, R.C., Scheltens, P., Sperling, R.A., Dubois, B., 2016. A/T/N: An unbiased descriptive classification scheme for Alzheimer disease biomarkers. Neurology 87, 539–547. [CrossRef]
- Jack, C.R., Knopman, D.S., Jagust, W.J., Petersen, R.C., Weiner, M.W., Aisen, P.S., Shaw, L.M., Vemuri, P., Wiste, H.J., Weigand, S.D., Lesnick, T.G., Pankratz, V.S., Donohue, M.C., Trojanowski, J.Q., 2013. Tracking pathophysiological processes in Alzheimer’s disease: an updated hypothetical model of dynamic biomarkers. Lancet Neurol 12, 207–216. [CrossRef]
- Jang, J.-W., Kim, S., Na, H.Y., Ahn, S., Lee, S.J., Kwak, K.-H., Lee, M.-A., Hsiung, G.-Y.R., Choi, B.-S., Youn, Y.C., 2013. Effect of white matter hyperintensity on medial temporal lobe atrophy in Alzheimer’s disease. Eur. Neurol. 69, 229–235. [CrossRef]
- Jansen, W.J., Ossenkoppele, R., Knol, D.L., Tijms, B.M., Scheltens, P., Verhey, F.R.J., Visser, P.J., Amyloid Biomarker Study Group, Aalten, P., Aarsland, D., Alcolea, D., Alexander, M., Almdahl, I.S., Arnold, S.E., Baldeiras, I., Barthel, H., van Berckel, B.N.M., Bibeau, K., Blennow, K., Brooks, D.J., van Buchem, M.A., Camus, V., Cavedo, E., Chen, K., Chetelat, G., Cohen, A.D., Drzezga, A., Engelborghs, S., Fagan, A.M., Fladby, T., Fleisher, A.S., van der Flier, W.M., Ford, L., Förster, S., Fortea, J., Foskett, N., Frederiksen, K.S., Freund-Levi, Y., Frisoni, G.B., Froelich, L., Gabryelewicz, T., Gill, K.D., Gkatzima, O., Gómez-Tortosa, E., Gordon, M.F., Grimmer, T., Hampel, H., Hausner, L., Hellwig, S., Herukka, S.-K., Hildebrandt, H., Ishihara, L., Ivanoiu, A., Jagust, W.J., Johannsen, P., Kandimalla, R., Kapaki, E., Klimkowicz-Mrowiec, A., Klunk, W.E., Köhler, S., Koglin, N., Kornhuber, J., Kramberger, M.G., Van Laere, K., Landau, S.M., Lee, D.Y., de Leon, M., Lisetti, V., Lleó, A., Madsen, K., Maier, W., Marcusson, J., Mattsson, N., de Mendonça, A., Meulenbroek, O., Meyer, P.T., Mintun, M.A., Mok, V., Molinuevo, J.L., Møllergård, H.M., Morris, J.C., Mroczko, B., Van der Mussele, S., Na, D.L., Newberg, A., Nordberg, A., Nordlund, A., Novak, G.P., Paraskevas, G.P., Parnetti, L., Perera, G., Peters, O., Popp, J., Prabhakar, S., Rabinovici, G.D., Ramakers, I.H.G.B., Rami, L., Resende de Oliveira, C., Rinne, J.O., Rodrigue, K.M., Rodríguez-Rodríguez, E., Roe, C.M., Rot, U., Rowe, C.C., Rüther, E., Sabri, O., Sanchez-Juan, P., Santana, I., Sarazin, M., Schröder, J., Schütte, C., Seo, S.W., Soetewey, F., Soininen, H., Spiru, L., Struyfs, H., Teunissen, C.E., Tsolaki, M., Vandenberghe, R., Verbeek, M.M., Villemagne, V.L., Vos, S.J.B., van Waalwijk van Doorn, L.J.C., Waldemar, G., Wallin, A., Wallin, Å.K., Wiltfang, J., Wolk, D.A., Zboch, M., Zetterberg, H., 2015. Prevalence of cerebral amyloid pathology in persons without dementia: a meta-analysis. JAMA 313, 1924–1938. [CrossRef]
- Jingnan Wang, Ekin, A., de Haan, G., 2008. Shape analysis of brain ventricles for improved classification of Alzheimer’s patients, in: 2008 15th IEEE International Conference on Image Processing. Presented at the 2008 15th IEEE International Conference on Image Processing, IEEE, San Diego, CA, USA, pp. 2252–2255. [CrossRef]
- Johnson, K.A., Fox, N.C., Sperling, R.A., Klunk, W.E., 2012. Brain imaging in Alzheimer disease. Cold Spring Harb Perspect Med 2, a006213. [CrossRef]
- Johnson, K.A., Minoshima, S., Bohnen, N.I., Donohoe, K.J., Foster, N.L., Herscovitch, P., Karlawish, J.H., Rowe, C.C., Carrillo, M.C., Hartley, D.M., Hedrick, S., Pappas, V., Thies, W.H., Alzheimer’s Association, Society of Nuclear Medicine and Molecular Imaging, Amyloid Imaging Taskforce, 2013. Appropriate use criteria for amyloid PET: a report of the Amyloid Imaging Task Force, the Society of Nuclear Medicine and Molecular Imaging, and the Alzheimer’s Association. Alzheimers Dement 9, e-1-16. [CrossRef]
- Kälin, A.M., Park, M.T.M., Chakravarty, M.M., Lerch, J.P., Michels, L., Schroeder, C., Broicher, S.D., Kollias, S., Nitsch, R.M., Gietl, A.F., Unschuld, P.G., Hock, C., Leh, S.E., 2017. Subcortical Shape Changes, Hippocampal Atrophy and Cortical Thinning in Future Alzheimer’s Disease Patients. Front Aging Neurosci 9, 38. [CrossRef]
- Kanekar, S., Poot, J.D., 2014. Neuroimaging of vascular dementia. Radiol. Clin. North Am. 52, 383–401. [CrossRef]
- Kehoe, E.G., McNulty, J.P., Mullins, P.G., Bokde, A.L.W., 2014. Advances in MRI biomarkers for the diagnosis of Alzheimer’s disease. Biomark Med 8, 1151–1169. [CrossRef]
- Kemp, P.M., Holmes, C., Hoffmann, S.M.A., Bolt, L., Holmes, R., Rowden, J., Fleming, J.S., 2003. Alzheimer’s disease: differences in technetium-99m HMPAO SPECT scan findings between early onset and late onset dementia. J Neurol Neurosurg Psychiatry 74, 715–719. [CrossRef]
- Khazaee, A., Ebrahimzadeh, A., Babajani-Feremi, A., 2015. Identifying patients with Alzheimer’s disease using resting-state fMRI and graph theory. Clin Neurophysiol 126, 2132–2141. [CrossRef]
- Kim, K.W., MacFall, J.R., Payne, M.E., 2008. Classification of white matter lesions on magnetic resonance imaging in elderly persons. Biol Psychiatry 64, 273–280. [CrossRef]
- Kim, Y., Rosenberg, P., Oh, E., 2018. A Review of Diagnostic Impact of Amyloid Positron Emission Tomography Imaging in Clinical Practice. Dement Geriatr Cogn Disord 46, 154–167. [CrossRef]
- Kimura, Y., Endo, H., Ichise, M., Shimada, H., Seki, C., Ikoma, Y., Shinotoh, H., Yamada, M., Higuchi, M., Zhang, M.-R., Suhara, T., 2016. A new method to quantify tau pathologies with (11)C-PBB3 PET using reference tissue voxels extracted from brain cortical gray matter. EJNMMI Res 6, 24. [CrossRef]
- Kljajevic, V., Grothe, M.J., Ewers, M., Teipel, S., Alzheimer’s Disease Neuroimaging Initiative, 2014. Distinct pattern of hypometabolism and atrophy in preclinical and predementia Alzheimer’s disease. Neurobiol Aging 35, 1973–1981. [CrossRef]
- Klunk, W.E., Engler, H., Nordberg, A., Wang, Y., Blomqvist, G., Holt, D.P., Bergström, M., Savitcheva, I., Huang, G., Estrada, S., Ausén, B., Debnath, M.L., Barletta, J., Price, J.C., Sandell, J., Lopresti, B.J., Wall, A., Koivisto, P., Antoni, G., Mathis, C.A., Långström, B., 2004. Imaging brain amyloid in Alzheimer’s disease with Pittsburgh Compound-B. Ann. Neurol. 55, 306–319. [CrossRef]
- Kuwabara, H., Comley, R.A., Borroni, E., Honer, M., Kitmiller, K., Roberts, J., Gapasin, L., Mathur, A., Klein, G., Wong, D.F., 2018. Evaluation of 18F-RO-948 PET for Quantitative Assessment of Tau Accumulation in the Human Brain. J Nucl Med 59, 1877–1884. [CrossRef]
- Landau, S.M., Harvey, D., Madison, C.M., Koeppe, R.A., Reiman, E.M., Foster, N.L., Weiner, M.W., Jagust, W.J., Alzheimer’s Disease Neuroimaging Initiative, 2011. Associations between cognitive, functional, and FDG-PET measures of decline in AD and MCI. Neurobiol. Aging 32, 1207–1218. [CrossRef]
- Lebedev, A.V., Westman, E., Beyer, M.K., Kramberger, M.G., Aguilar, C., Pirtosek, Z., Aarsland, D., 2013. Multivariate classification of patients with Alzheimer’s and dementia with Lewy bodies using high-dimensional cortical thickness measurements: an MRI surface-based morphometric study. J Neurol 260, 1104–1115. [CrossRef]
- Leuzy, A., Chiotis, K., Lemoine, L., Gillberg, P.-G., Almkvist, O., Rodriguez-Vieitez, E., Nordberg, A., 2019. Tau PET imaging in neurodegenerative tauopathies—still a challenge. Mol Psychiatry 24, 1112–1134. [CrossRef]
- Lockhart, S.N., Schöll, M., Baker, S.L., Ayakta, N., Swinnerton, K.N., Bell, R.K., Mellinger, T.J., Shah, V.D., O’Neil, J.P., Janabi, M., Jagust, W.J., 2017. Amyloid and tau PET demonstrate region-specific associations in normal older people. Neuroimage 150, 191–199. [CrossRef]
- Marcus, C., Mena, E., Subramaniam, R.M., 2014. Brain PET in the Diagnosis of Alzheimer’s Disease. Clin Nucl Med 39, e413–e426. [CrossRef]
- Marquié, M., Chong, M.S.T., Antón-Fernández, A., Verwer, E.E., Sáez-Calveras, N., Meltzer, A.C., Ramanan, P., Amaral, A.C., Gonzalez, J., Normandin, M.D., Frosch, M.P., Gómez-Isla, T., 2017. [F-18]-AV-1451 binding correlates with postmortem neurofibrillary tangle Braak staging. Acta Neuropathol 134, 619–628. [CrossRef]
- Martin-Macintosh, E.L., Broski, S.M., Johnson, G.B., Hunt, C.H., Cullen, E.L., Peller, P.J., 2016. Multimodality Imaging of Neurodegenerative Processes: Part 1, The Basics and Common Dementias. AJR Am J Roentgenol 207, 871–882. [CrossRef]
- Maruyama, M., Shimada, H., Suhara, T., Shinotoh, H., Ji, B., Maeda, J., Zhang, M.-R., Trojanowski, J.Q., Lee, V.M.-Y., Ono, M., Masamoto, K., Takano, H., Sahara, N., Iwata, N., Okamura, N., Furumoto, S., Kudo, Y., Chang, Q., Saido, T.C., Takashima, A., Lewis, J., Jang, M.-K., Aoki, I., Ito, H., Higuchi, M., 2013. Imaging of tau pathology in a tauopathy mouse model and in Alzheimer patients compared to normal controls. Neuron 79, 1094–1108. [CrossRef]
- Matsuda, H., Mizumura, S., Nagao, T., Ota, T., Iizuka, T., Nemoto, K., Takemura, N., Arai, H., Homma, A., 2007. Automated discrimination between very early Alzheimer disease and controls using an easy Z-score imaging system for multicenter brain perfusion single-photon emission tomography. AJNR Am J Neuroradiol 28, 731–736.
- Matsunari, I., Samuraki, M., Chen, W.-P., Yanase, D., Takeda, N., Ono, K., Yoshita, M., Matsuda, H., Yamada, M., Kinuya, S., 2007. Comparison of 18F-FDG PET and optimized voxel-based morphometry for detection of Alzheimer’s disease: aging effect on diagnostic performance. J. Nucl. Med. 48, 1961–1970. [CrossRef]
- Mattsson, N., Carrillo, M.C., Dean, R.A., Devous, M.D., Nikolcheva, T., Pesini, P., Salter, H., Potter, W.Z., Sperling, R.S., Bateman, R.J., Bain, L.J., Liu, E., 2015. Revolutionizing Alzheimer’s disease and clinical trials through biomarkers. Alzheimers Dement (Amst) 1, 412–419. [CrossRef]
- McKhann, G.M., Knopman, D.S., Chertkow, H., Hyman, B.T., Jack, C.R., Kawas, C.H., Klunk, W.E., Koroshetz, W.J., Manly, J.J., Mayeux, R., Mohs, R.C., Morris, J.C., Rossor, M.N., Scheltens, P., Carrillo, M.C., Thies, B., Weintraub, S., Phelps, C.H., 2011. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7, 263–269. [CrossRef]
- Minoshima, S., Mosci, K., Cross, D., Thientunyakit, T., 2021. Brain [F-18]FDG PET for Clinical Dementia Workup: Differential Diagnosis of Alzheimer’s Disease and Other Types of Dementing Disorders. Semin Nucl Med 51, 230–240. [CrossRef]
- Morris, J.C., Ernesto, C., Schafer, K., Coats, M., Leon, S., Sano, M., Thal, L.J., Woodbury, P., 1997. Clinical dementia rating training and reliability in multicenter studies: the Alzheimer’s Disease Cooperative Study experience. Neurology 48, 1508–1510. [CrossRef]
- Mosconi, L., 2013. Glucose metabolism in normal aging and Alzheimer’s disease: Methodological and physiological considerations for PET studies. Clin Transl Imaging 1. [CrossRef]
- Mosconi, L., Tsui, W.H., Herholz, K., Pupi, A., Drzezga, A., Lucignani, G., Reiman, E.M., Holthoff, V., Kalbe, E., Sorbi, S., Diehl-Schmid, J., Perneczky, R., Clerici, F., Caselli, R., Beuthien-Baumann, B., Kurz, A., Minoshima, S., de Leon, M.J., 2008. Multicenter standardized 18F-FDG PET diagnosis of mild cognitive impairment, Alzheimer’s disease, and other dementias. J. Nucl. Med. 49, 390–398. [CrossRef]
- National Institute for Health and Care Excellence (UK), 2018. Dementia: Assessment, management and support for people living with dementia and their carers, National Institute for Health and Care Excellence: Clinical Guidelines. National Institute for Health and Care Excellence (UK), London.
- Nelson, P.T., Alafuzoff, I., Bigio, E.H., Bouras, C., Braak, H., Cairns, N.J., Castellani, R.J., Crain, B.J., Davies, P., Del Tredici, K., Duyckaerts, C., Frosch, M.P., Haroutunian, V., Hof, P.R., Hulette, C.M., Hyman, B.T., Iwatsubo, T., Jellinger, K.A., Jicha, G.A., Kövari, E., Kukull, W.A., Leverenz, J.B., Love, S., Mackenzie, I.R., Mann, D.M., Masliah, E., McKee, A.C., Montine, T.J., Morris, J.C., Schneider, J.A., Sonnen, J.A., Thal, D.R., Trojanowski, J.Q., Troncoso, J.C., Wisniewski, T., Woltjer, R.L., Beach, T.G., 2012. Correlation of Alzheimer disease neuropathologic changes with cognitive status: a review of the literature. J Neuropathol Exp Neurol 71, 362–381. [CrossRef]
- Nishimura, T., Hashikawa, K., Fukuyama, H., Kubota, T., Kitamura, S., Matsuda, H., Hanyu, H., Nabatame, H., Oku, N., Tanabe, H., Kuwabara, Y., Jinnouchi, S., Kubol, A., 2007. Decreased cerebral blood flow and prognosis of Alzheimer’s disease: a multicenter HMPAO-SPECT study. Ann Nucl Med 21, 15–23. [CrossRef]
- Nitrini, R., Buchpiguel, C.A., Caramelli, P., Bahia, V.S., Mathias, S.C., Nascimento, C.M., Degenszajn, J., Caixeta, L., 2000. SPECT in Alzheimer’s disease: features associated with bilateral parietotemporal hypoperfusion. Acta Neurol Scand 101, 172–176. [CrossRef]
- Nordberg, A., Carter, S.F., Rinne, J., Drzezga, A., Brooks, D.J., Vandenberghe, R., Perani, D., Forsberg, A., Långström, B., Scheinin, N., Karrasch, M., Någren, K., Grimmer, T., Miederer, I., Edison, P., Okello, A., Van Laere, K., Nelissen, N., Vandenbulcke, M., Garibotto, V., Almkvist, O., Kalbe, E., Hinz, R., Herholz, K., 2013. A European multicentre PET study of fibrillar amyloid in Alzheimer’s disease. Eur. J. Nucl. Med. Mol. Imaging 40, 104–114. [CrossRef]
- Okamura, N., Furumoto, S., Fodero-Tavoletti, M.T., Mulligan, R.S., Harada, R., Yates, P., Pejoska, S., Kudo, Y., Masters, C.L., Yanai, K., Rowe, C.C., Villemagne, V.L., 2014. Non-invasive assessment of Alzheimer’s disease neurofibrillary pathology using 18F-THK5105 PET. Brain 137, 1762–1771. [CrossRef]
- Okello, A., Koivunen, J., Edison, P., Archer, H.A., Turkheimer, F.E., Någren, K., Bullock, R., Walker, Z., Kennedy, A., Fox, N.C., Rossor, M.N., Rinne, J.O., Brooks, D.J., 2009. Conversion of amyloid positive and negative MCI to AD over 3 years. Neurology 73, 754–760. [CrossRef]
- Ossenkoppele, R., Smith, R., Mattsson-Carlgren, N., Groot, C., Leuzy, A., Strandberg, O., Palmqvist, S., Olsson, T., Jögi, J., Stormrud, E., Cho, H., Ryu, Y.H., Choi, J.Y., Boxer, A.L., Gorno-Tempini, M.L., Miller, B.L., Soleimani-Meigooni, D., Iaccarino, L., La Joie, R., Baker, S., Borroni, E., Klein, G., Pontecorvo, M.J., Devous, M.D., Jagust, W.J., Lyoo, C.H., Rabinovici, G.D., Hansson, O., 2021. Accuracy of Tau Positron Emission Tomography as a Prognostic Marker in Preclinical and Prodromal Alzheimer Disease: A Head-to-Head Comparison Against Amyloid Positron Emission Tomography and Magnetic Resonance Imaging. JAMA Neurol 78, 961–971. [CrossRef]
- Ossenkoppele, R., Smith, R., Ohlsson, T., Strandberg, O., Mattsson, N., Insel, P.S., Palmqvist, S., Hansson, O., 2019. Associations between tau, Aβ, and cortical thickness with cognition in Alzheimer disease. Neurology 92, e601–e612. [CrossRef]
- Ou, Y.-N., Xu, W., Li, J.-Q., Guo, Y., Cui, M., Chen, K.-L., Huang, Y.-Y., Dong, Q., Tan, L., Yu, J.-T., on behalf of Alzheimer’s Disease Neuroimaging Initiative, 2019. FDG-PET as an independent biomarker for Alzheimer’s biological diagnosis: a longitudinal study. Alzheimer’s Research & Therapy 11, 57. [CrossRef]
- Oxford, A.E., Stewart, E.S., Rohn, T.T., 2020. Clinical Trials in Alzheimer’s Disease: A Hurdle in the Path of Remedy. Int J Alzheimers Dis 2020, 5380346. [CrossRef]
- Plotkin, M., Amthauer, H., Klaffke, S., Kühn, A., Lüdemann, L., Arnold, G., Wernecke, K.-D., Kupsch, A., Felix, R., Venz, S., 2005. Combined 123I-FP-CIT and 123I-IBZM SPECT for the diagnosis of parkinsonian syndromes: study on 72 patients. J Neural Transm (Vienna) 112, 677–692. [CrossRef]
- Podhorna, J., Krahnke, T., Shear, M., Harrison, J.E., Alzheimer’s Disease Neuroimaging Initiative, 2016. Alzheimer’s Disease Assessment Scale-Cognitive subscale variants in mild cognitive impairment and mild Alzheimer’s disease: change over time and the effect of enrichment strategies. Alzheimers Res Ther 8, 8. [CrossRef]
- Pontecorvo, M.J., Devous, M.D., Navitsky, M., Lu, M., Salloway, S., Schaerf, F.W., Jennings, D., Arora, A.K., McGeehan, A., Lim, N.C., Xiong, H., Joshi, A.D., Siderowf, A., Mintun, M.A., 18F-AV-1451-A05 investigators, 2017. Relationships between flortaucipir PET tau binding and amyloid burden, clinical diagnosis, age and cognition. Brain 140, 748–763. [CrossRef]
- Potkin, S.G., Anand, R., Fleming, K., Alva, G., Keator, D., Carreon, D., Messina, J., Wu, J.C., Hartman, R., Fallon, J.H., 2001. Brain metabolic and clinical effects of rivastigmine in Alzheimer’s disease. Int. J. Neuropsychopharmacol. 4, 223–230. [CrossRef]
- Rabinovici, G.D., Jagust, W.J., 2009. Amyloid imaging in aging and dementia: testing the amyloid hypothesis in vivo. Behav Neurol 21, 117–128. [CrossRef]
- Rabinovici, G.D., Rosen, H.J., Alkalay, A., Kornak, J., Furst, A.J., Agarwal, N., Mormino, E.C., O’Neil, J.P., Janabi, M., Karydas, A., Growdon, M.E., Jang, J.Y., Huang, E.J., Dearmond, S.J., Trojanowski, J.Q., Grinberg, L.T., Gorno-Tempini, M.L., Seeley, W.W., Miller, B.L., Jagust, W.J., 2011. Amyloid vs FDG-PET in the differential diagnosis of AD and FTLD. Neurology 77, 2034–2042. [CrossRef]
- Rasmussen, J., Langerman, H., 2019. Alzheimer’s Disease – Why We Need Early Diagnosis. Degener Neurol Neuromuscul Dis 9, 123–130. [CrossRef]
- Rodriguez, G., Nobili, F., Copello, F., Vitali, P., Gianelli, M.V., Taddei, G., Catsafados, E., Mariani, G., 1999. 99mTc-HMPAO regional cerebral blood flow and quantitative electroencephalography in Alzheimer’s disease: a correlative study. J Nucl Med 40, 522–529.
- Rosen, W.G., Mohs, R.C., Davis, K.L., 1984. A new rating scale for Alzheimer’s disease. Am J Psychiatry 141, 1356–1364. [CrossRef]
- Salmon, E., Collette, F., Bastin, C., 2024. Cerebral glucose metabolism in Alzheimer’s disease. Cortex 179, 50–61. [CrossRef]
- Sanabria Bohórquez, S., Marik, J., Ogasawara, A., Tinianow, J.N., Gill, H.S., Barret, O., Tamagnan, G., Alagille, D., Ayalon, G., Manser, P., Bengtsson, T., Ward, M., Williams, S.-P., Kerchner, G.A., Seibyl, J.P., Marek, K., Weimer, R.M., 2019. [18F]GTP1 (Genentech Tau Probe 1), a radioligand for detecting neurofibrillary tangle tau pathology in Alzheimer’s disease. Eur. J. Nucl. Med. Mol. Imaging 46, 2077–2089. [CrossRef]
- Scherfler, C., Nocker, M., 2009. Dopamine transporter SPECT: how to remove subjectivity? Mov Disord 24 Suppl 2, S721-724. [CrossRef]
- Sevigny, J., Chiao, P., Bussière, T., Weinreb, P.H., Williams, L., Maier, M., Dunstan, R., Salloway, S., Chen, T., Ling, Y., O’Gorman, J., Qian, F., Arastu, M., Li, M., Chollate, S., Brennan, M.S., Quintero-Monzon, O., Scannevin, R.H., Arnold, H.M., Engber, T., Rhodes, K., Ferrero, J., Hang, Y., Mikulskis, A., Grimm, J., Hock, C., Nitsch, R.M., Sandrock, A., 2016. The antibody aducanumab reduces Aβ plaques in Alzheimer’s disease. Nature 537, 50–56. [CrossRef]
- Sharp, P.F., Gemmell, H.G., Murray, A.D. (Eds.), 2005. Practical nuclear medicine, 3rd ed. ed. Springer, London ; New York.
- Shoghi-Jadid, K., Small, G.W., Agdeppa, E.D., Kepe, V., Ercoli, L.M., Siddarth, P., Read, S., Satyamurthy, N., Petric, A., Huang, S.-C., Barrio, J.R., 2002. Localization of neurofibrillary tangles and beta-amyloid plaques in the brains of living patients with Alzheimer disease. Am J Geriatr Psychiatry 10, 24–35.
- Siger, M., Schuff, N., Zhu, X., Miller, B.L., Weiner, M.W., 2009. Regional myo-inositol concentration in mild cognitive impairment Using 1H magnetic resonance spectroscopic imaging. Alzheimer Dis Assoc Disord 23, 57–62. [CrossRef]
- Sørensen, L., Igel, C., Liv Hansen, N., Osler, M., Lauritzen, M., Rostrup, E., Nielsen, M., Alzheimer’s Disease Neuroimaging Initiative and the Australian Imaging Biomarkers and Lifestyle Flagship Study of Ageing, 2016. Early detection of Alzheimer’s disease using MRI hippocampal texture. Hum Brain Mapp 37, 1148–1161. [CrossRef]
- Sperling, R.A., Aisen, P.S., Beckett, L.A., Bennett, D.A., Craft, S., Fagan, A.M., Iwatsubo, T., Jack, C.R., Kaye, J., Montine, T.J., Park, D.C., Reiman, E.M., Rowe, C.C., Siemers, E., Stern, Y., Yaffe, K., Carrillo, M.C., Thies, B., Morrison-Bogorad, M., Wagster, M.V., Phelps, C.H., 2011. Toward defining the preclinical stages of Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7, 280–292. [CrossRef]
- Stern, Y., 2012. Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol 11, 1006–1012. [CrossRef]
- Takeda, S., 2019. Tau Propagation as a Diagnostic and Therapeutic Target for Dementia: Potentials and Unanswered Questions. Front Neurosci 13, 1274. [CrossRef]
- Talbot, P.R., Lloyd, J.J., Snowden, J.S., Neary, D., Testa, H.J., 1998. A clinical role for 99mTc-HMPAO SPECT in the investigation of dementia? J Neurol Neurosurg Psychiatry 64, 306–313. [CrossRef]
- Tripathi, Madhavi, Tripathi, Manjari, Damle, N., Kushwaha, S., Jaimini, A., D’Souza, M.M., Sharma, R., Saw, S., Mondal, A., 2014. Differential Diagnosis of Neurodegenerative Dementias Using Metabolic Phenotypes on F-18 FDG PET/CT. Neuroradiol J 27, 13–21. [CrossRef]
- Tripathi, S.M., Murray, A.D., 2021. Alzheimer’s Dementia: The Emerging Role of Positron Emission Tomography. Neuroscientist 1073858421997035. [CrossRef]
- Vaamonde-Gamo, J., Flores-Barragán, J.M., Ibáñez, R., Gudín, M., Hernández, A., 2005. [DaT-SCAN SPECT in the differential diagnosis of dementia with Lewy bodies and Alzheimer’s disease]. Rev Neurol 41, 276–279.
- Valotassiou, V., Malamitsi, J., Papatriantafyllou, J., Dardiotis, E., Tsougos, I., Psimadas, D., Alexiou, S., Hadjigeorgiou, G., Georgoulias, P., 2018. SPECT and PET imaging in Alzheimer’s disease. Ann Nucl Med 32, 583–593. [CrossRef]
- Valotassiou, V., Sifakis, N., Papatriantafyllou, J., Angelidis, G., Georgoulias, P., 2011. The Clinical Use of SPECT and PET Molecular Imaging in Alzheimer’s Disease, The Clinical Spectrum of Alzheimer’s Disease -The Charge Toward Comprehensive Diagnostic and Therapeutic Strategies. IntechOpen. [CrossRef]
- Varghese, T., Sheelakumari, R., James, J.S., Mathuranath, P., 2013. A review of neuroimaging biomarkers of Alzheimer’s disease. Neurol Asia 18, 239–248.
- Villemagne, V.L., Burnham, S., Bourgeat, P., Brown, B., Ellis, K.A., Salvado, O., Szoeke, C., Macaulay, S.L., Martins, R., Maruff, P., Ames, D., Rowe, C.C., Masters, C.L., Australian Imaging Biomarkers and Lifestyle (AIBL) Research Group, 2013. Amyloid β deposition, neurodegeneration, and cognitive decline in sporadic Alzheimer’s disease: a prospective cohort study. Lancet Neurol 12, 357–367. [CrossRef]
- Villemagne, V.L., Furumoto, S., Fodero-Tavoletti, M., Harada, R., Mulligan, R.S., Kudo, Y., Masters, C.L., Yanai, K., Rowe, C.C., Okamura, N., 2012. The challenges of tau imaging. Future Neurology 7, 409–421. [CrossRef]
- Villemagne, V.L., Furumoto, S., Fodero-Tavoletti, M.T., Mulligan, R.S., Hodges, J., Harada, R., Yates, P., Piguet, O., Pejoska, S., Doré, V., Yanai, K., Masters, C.L., Kudo, Y., Rowe, C.C., Okamura, N., 2014. In vivo evaluation of a novel tau imaging tracer for Alzheimer’s disease. Eur. J. Nucl. Med. Mol. Imaging 41, 816–826. [CrossRef]
- Wahlster, P., Niederländer, C., Kriza, C., Schaller, S., Kolominsky-Rabas, P.L., 2013. Clinical assessment of amyloid imaging in Alzheimer’s disease: a systematic review of the literature. Dement Geriatr Cogn Disord 36, 263–278. [CrossRef]
- Waldemar, G., Walovitch, R.C., Andersen, A.R., Hasselbalch, S.G., Bigelow, R., Joseph, J.L., Paulson, O.B., Lassen, N.A., 1994. 99mTc-bicisate (neurolite) SPECT brain imaging and cognitive impairment in dementia of the Alzheimer type: a blinded read of image sets from a multicenter SPECT trial. J Cereb Blood Flow Metab 14 Suppl 1, S99-105.
- Wattamwar, P.R., Mathuranath, P.S., 2010. An overview of biomarkers in Alzheimer’s disease. Ann Indian Acad Neurol 13, S116-123. [CrossRef]
- Whitwell, J.L., Josephs, K.A., Murray, M.E., Kantarci, K., Przybelski, S.A., Weigand, S.D., Vemuri, P., Senjem, M.L., Parisi, J.E., Knopman, D.S., Boeve, B.F., Petersen, R.C., Dickson, D.W., Jack, C.R., 2008. MRI correlates of neurofibrillary tangle pathology at autopsy: A voxel-based morphometry study. Neurology 71, 743–749. [CrossRef]
- Wolk, D.A., Klunk, W.E., 2009. Update on amyloid imaging: From healthy aging to Alzheimer’s disease. Curr Neurol Neurosci Rep 9, 345–352. [CrossRef]
- Wong, R., Luo, Y., Mok, V.C., Shi, L., 2021. Advances in computerized MRI-based biomarkers in Alzheimer’s disease. Brain Science Advances 7, 26–43. [CrossRef]
- Wuestefeld, A., Pichet Binette, A., Berron, D., Spotorno, N., van Westen, D., Stomrud, E., Mattsson-Carlgren, N., Strandberg, O., Smith, R., Palmqvist, S., Glenn, T., Moes, S., Honer, M., Arfanakis, K., Barnes, L.L., Bennett, D.A., Schneider, J.A., Wisse, L.E.M., Hansson, O., 2023. Age-related and amyloid-beta-independent tau deposition and its downstream effects. Brain 146, 3192–3205. [CrossRef]
- Xue, C., Kowshik, S.S., Lteif, D., Puducheri, S., Jasodanand, V.H., Zhou, O.T., Walia, A.S., Guney, O.B., Zhang, J.D., Poésy, S., Kaliaev, A., Andreu-Arasa, V.C., Dwyer, B.C., Farris, C.W., Hao, H., Kedar, S., Mian, A.Z., Murman, D.L., O’Shea, S.A., Paul, A.B., Rohatgi, S., Saint-Hilaire, M.-H., Sartor, E.A., Setty, B.N., Small, J.E., Swaminathan, A., Taraschenko, O., Yuan, J., Zhou, Y., Zhu, S., Karjadi, C., Alvin Ang, T.F., Bargal, S.A., Plummer, B.A., Poston, K.L., Ahangaran, M., Au, R., Kolachalama, V.B., 2024. AI-based differential diagnosis of dementia etiologies on multimodal data. Nat Med 30, 2977–2989. [CrossRef]
- Yang, J., Zhi, W., Wang, L., 2024. Role of Tau Protein in Neurodegenerative Diseases and Development of Its Targeted Drugs: A Literature Review. Molecules 29, 2812. [CrossRef]
- Yoshida, K., Hata, Y., Ichimata, S., Nishida, N., 2019. Tau and Amyloid-β Pathology in Japanese Forensic Autopsy Series Under 40 Years of Age: Prevalence and Association with APOE Genotype and Suicide Risk. J. Alzheimers Dis. 72, 641–652. [CrossRef]
- Yu, Q., Mai, Y., Ruan, Y., Luo, Y., Zhao, L., Fang, W., Cao, Z., Li, Y., Liao, W., Xiao, S., Mok, V.C.T., Shi, L., Liu, J., National Alzheimer’s Coordinating Center, the Alzheimer’s Disease Neuroimaging Initiative, Frontotemporal Lobar Degeneration Neuroimaging Initiative, 2021. An MRI-based strategy for differentiation of frontotemporal dementia and Alzheimer’s disease. Alzheimers Res Ther 13, 23. [CrossRef]
- Zhang, W., Arteaga, J., Cashion, D.K., Chen, G., Gangadharmath, U., Gomez, L.F., Kasi, D., Lam, C., Liang, Q., Liu, C., Mocharla, V.P., Mu, F., Sinha, A., Szardenings, A.K., Wang, E., Walsh, J.C., Xia, C., Yu, C., Zhao, T., Kolb, H.C., 2012. A highly selective and specific PET tracer for imaging of tau pathologies. J. Alzheimers Dis. 31, 601–612. [CrossRef]
- Zhang, Y., Chen, H., Li, R., Sterling, K., Song, W., 2023. Amyloid β-based therapy for Alzheimer’s disease: challenges, successes and future. Signal Transduct Target Ther 8, 248. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



