Submitted:
09 May 2025
Posted:
12 May 2025
You are already at the latest version
Abstract
Acute megakaryoblastic leukemia (AMKL) is a heterogeneous form of acute myeloid leukemia (AML) and is significantly more common in children than in adults. In non-Down syndrome children with AMKL, inv(16)(p13q24)/CBFA2T3::GLIS2 is the most frequent genetic aberration. Pediatric CBFA2T3::GLIS2-positive AMKL is strongly associated with a poor prognosis and a high cumulative incidence of relapse. One of the key laboratory signs of CBFA2T3::GLIS2-positive AMKL is the RAM immunophenotype, which includes dim to negative CD45 and CD38 expression, extremely bright CD56 and a lack of HLA-DR on leukemic cells. This immunophenotype looks very similar to that of solid tumor bone marrow (BM) infiltration. For this reason, in cases of isolated extramedullary involvement of CBFA2T3::GLIS2-positive AMKL, excluding solid tumors may be challenging. The differential diagnosis between extramedullary AMKL relapse and secondary tumors is especially difficult. We report a case of a 3.5-year-old girl with isolated extramedullary CBFA2T3::GLIS2-positive AMKL relapse, which was misdiagnosed as secondary Ewing sarcoma. The morphological differential diagnosis between Ewing sarcoma and AMKL presents significant challenges owing to their overlapping histological features (small round blue cell morphology and similar growth patterns). The tumor cells immunophenotype was completely mirrored that at the initial diagnosis of AMKL. Additional cytogenetic and molecular studies confirmed the presence of the CBFA2T3::GLIS2 fusion, but no Ewing sarcoma-specific EWSR1 fusion transcripts were found. Thus, extramedullary CBFA2T3::GLIS2-positive AMKL relapse was confirmed. The patient’s clinical condition gradually worsened, and the patient died 5 months after diagnosis. The presented case demonstrates difficulties in the differential diagnosis between AMKL relapse and the development of a secondary tumor.
Keywords:
Acute megakaryoblastic leukemia
; inv(16)(p13q24)/CBFA2T3::GLIS2
; extramedullary relapse
1. Introduction
Acute megakaryoblastic leukemia (AMKL) is a rare molecularly heterogeneous subtype of acute myeloid leukemia (AML) that is usually described as the M7 type of AML according to the FAB classification [1,2,3]. The incidence of AMKL ranges from 4 to 15% among pediatric AML cases, and AMKL accounts for approximately 1% of adult AML cases. AMKL can be divided into Down syndrome AMKL (DS-AMKL) and non-DS-AMKL, which is associated with a worse survival prognosis [4,5,6,7,8]. CBFA2T3::GLIS2, resulting from cryptic inversion of chromosome 16, is the most frequent chimeric oncogene in non-Down syndrome AMKL [1,9,10,11,12]. The presence of this fusion gene has been described predominantly in infants and young children, and it is associated with an extremely poor prognosis (5-year overall survival rate of less than 34.3%) and a high cumulative incidence of relapse [9,10,13,14]. One of the key laboratory signs of CBFA2T3::GLIS2-positive AMKL is the so-called RAM immunophenotype [15,16,17], which is characterized by dim to negative CD45 and CD38 expression, extremely bright CD56 and a lack of HLA-DR on leukemic cells [16,18]. This antigen expression profile looks very similar to that of solid tumor bone marrow (BM) infiltration [16,19,20], whereas in CBFA2T3::GLIS2-positive AMKL, the expression of typical myeloid and progenitor markers (CD33, CD117, and CD34) is usually visible [16,17,20,21]. Moreover, the expression of platelet markers (CD61, CD41a, and CD42b) is always indicative of AMKL [22,23].
Pediatric AML often manifests with extramedullary lesions, including myeloid sarcoma (MS), also known as chloroma [24,25,26,27], which is a solid lesion of extramedullary accumulation of malignant myeloid cells or their precursors [28]. Establishing the diagnosis of AMKL in cases of isolated extensive extramedullary involvement may be challenging. In addition to the difficulties that arise in the differential diagnosis using radiation methods, pathological diagnostics can also produce a contradictory picture when identifying and classifying atypical myeloid cells [29,30].
Herein, we present a case of isolated extramedullary relapse of CBFA2T3::GLIS2-positive AMKL after a second allo-HSCT in a 3.5-year-old girl who was misdiagnosed with secondary Ewing sarcoma.
2. Case Presentation
A 1.7-year-old girl was referred to a local hospital because of fever, pallor and cytopenia. Laboratory tests revealed bicytopenia (Hb 74 g/L, total WBC count 5.4×109/L, neutrophils 2.7×109/L, and platelet count 580×109/L) and an increased LDH level (754 units/L). An abdominal ultrasound revealed mild hepatosplenomegaly. Morphological evaluation of the bone marrow aspirate revealed 96% blasts with megakaryocytic morphology (Figure 1A). Bone marrow immunophenotyping revealed 95% CD45-negative blasts with bright expression of CD33, CD117 and CD56 and characteristic features of AMKL, including CD11a negativity and the expression of the platelet antigens CD61 and CD41a (Figure 2A). Conventional cytogenetic evaluation of the bone marrow aspirate revealed isolated trisomy 3, and inv(16)(p13q24)/CBFA2T3::GLIS2 was found in 90% of the nuclei by FISH (Figure 1C). RNA-seq of the BM aspirate revealed CBFA2T3::GLIS2 fusion transcript expression with an exon 9–exon 3 junction. No accompanying mutations in AML-related genes were detected by NGS. No leukemic cells were detected in the cerebrospinal fluid.
Thus, the diagnosis of AMKL with inv(16)(p13q24)/CBFA2T3::GLIS2 was established, and the patient received AML-MRD-2018 protocol induction therapy, consisting of cytarabine, etoposide and idarubicin [31,32]. According to the protocol stratification system [31], the patient was allocated to the high-risk (HR) group. Although complete remission (CR) was achieved after induction, a high MFC-MRD level (1.541%) was detected (Figure 2B). In addition, RT‒PCR negativity was not reached, with only a 2-log reduction in relative CBFA2T3::GLIS2 expression. The treatment continued with high-dose cytarabine in conjunction with fludarabine and idarubicin (FLAI course), while the patient remained highly MFC-MRD refractory (1.172%), and after the third cycle of chemotherapy with HDaraC and fludarabine (FLA), the MFC-MRD level even increased to 2.122% (Figure 2B). Thus, a decision to proceed to hematopoietic stem cell transplantation (HSCT) without further attempts to achieve MRD-negative remission was made. After myeloablative conditioning with treosulfan 42 g/m2, fludarabine and thiotepa 10 mg/kg b.w., the patient received HSCT from her HLA-identical sibling. One month after HSCT, MFC-MRD (0.013%) was still detectable in the BM, as well as CBFA2T3::GLIS2 expression was positive. To prevent overt leukemia relapse, the patient was treated with venetoclax and decitabine. Eight months after the initial diagnosis and 3 months after HSCT, the MFC-MRD level increased to 2.685%. Low-dose cytarabine in combination with 6-mercaptopurine was administered, and donor lymphocyte infusions were given, with no influence on MRD, whose level remained high at 1.184%. Owing to inevitable AMKL relapse, a second haploidentical HSCT was performed 10 months after diagnosis (5 months after HSCT #1). On day +31 after the second HSCT, MFC-MRD-negative and RT‒PCR-negative remission was documented for the first time.
On day +143 after the second HSCT, MFC-MRD reappeared (0.028%; Figure 2B). The patient was treated with azacitidine and bortezomib, with subsequent MFC-MRD elimination on day +165. Three months later, the patient was admitted with pain in the right hip area. A CT scan and MRI revealed a periosteal reaction of the femur, an extraosseous soft tissue mass and focal liver lesions (Figure 3). The MFC-MRD results were negative in the BM. On the basis of the MFC-MRD results and imaging data, a secondary bone tumor was suspected, rather than leukemia relapse. A core biopsy of the right femur was performed, but the material obtained was insufficient for reliably verifying the diagnosis. On the basis of the first histological examination result, the diagnosis of Ewing sarcoma was suspected.
3. Laboratory Studies at the Time of Relapse Diagnosis
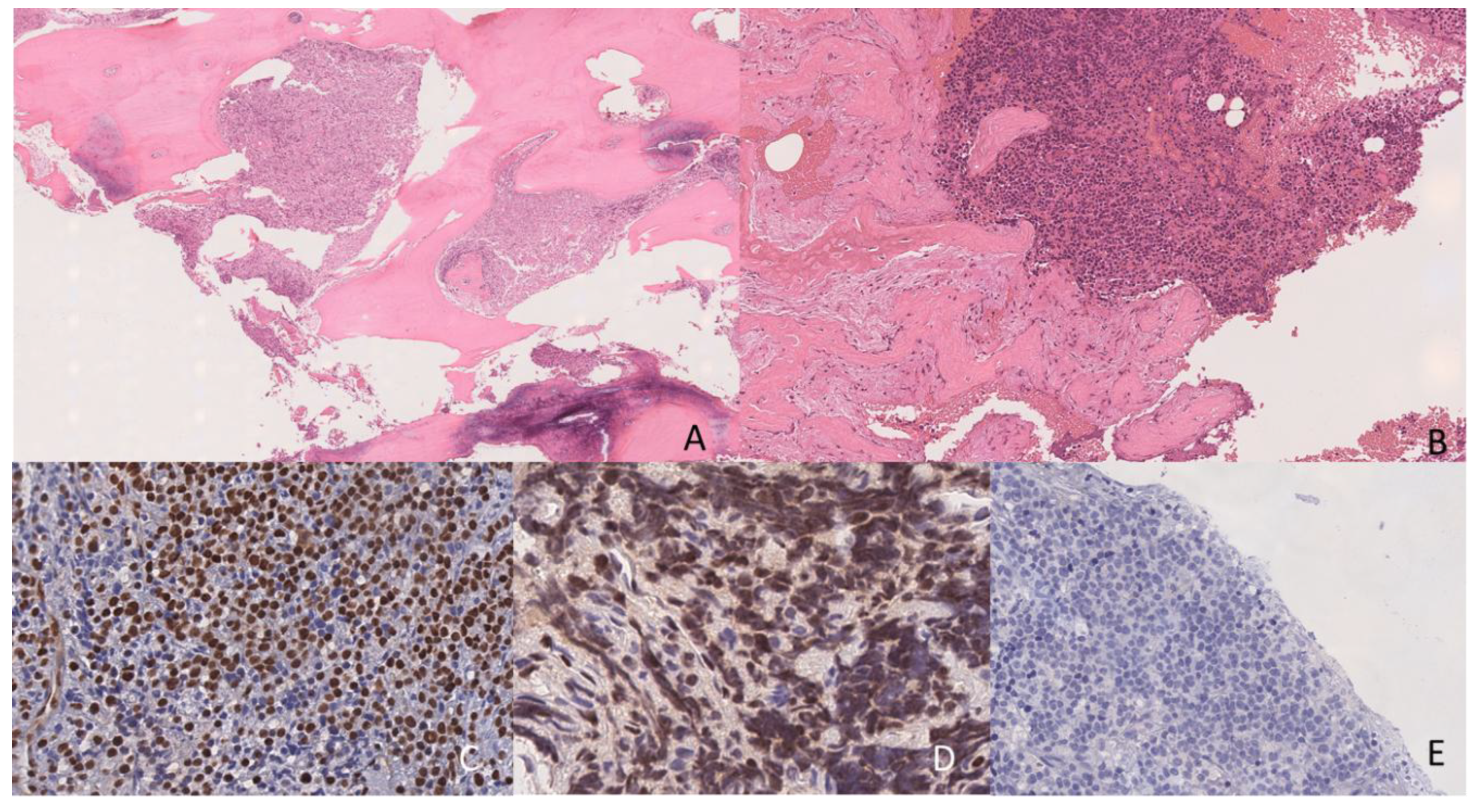
The patient was admitted to Dmitry Rogachev National Medical Research Center of Pediatric Hematology; Oncology and Immunology to repeat biopsy and verify the diagnosis. An open biopsy of the right femur and extraosseous soft tissue component was performed. The tumor demonstrated a distinctive morphological pattern characterized by sheets and nests of monomorphic small round cells infiltrating the intertrabecular spaces. The neoplastic cells presented high nuclear-to-cytoplasmic ratios; with round to oval nuclei containing finely dispersed chromatin and inconspicuous nucleoli. Cellular proliferation was intersected by prominent fibrous trabeculae; creating a compartmentalized architecture. Focal areas of geographic necrosis and hemorrhage were present throughout the lesion. The tumor cells displayed brisk mitotic activity with numerous atypical mitotic figures. The overall histological appearance bore a striking resemblance to Ewing sarcoma; necessitating careful immunohistochemical evaluation for definitive diagnosis (Figure 4). The expression of Fli1; ERG; and LMO2 and negative reactions for MPO; CD99; and CD61 were detected. However; the quality of the extracted nucleic acids from the obtained biopsy material was insufficient for performing molecular confirmation of the diagnosis. Considering the patient's initial diagnosis of AMKL; controversial cell morphology; similarity of the immunophenotypes of Ewing sarcoma and CBFA2T3::GLIS2-positive AML; and the lack of molecular diagnostics; comprehensive additional immunophenotypic and molecular studies were performed to confirm the diagnosis of a secondary tumor rather than extramedullary recurrence of AML.
BM microscopy revealed the absence of any signs of tumor lesions in three of the four puncture sites; although in one specimen, a conglomerate of suspicious cells was found, confirming the tumor nature of these cells was impossible (Figure 1B). MFC-MRD was detected in 0.028% of residual leukemic cells, which were CD45 negative, CD33 positive, CD117 positive, CD11a negative, and HLA-DR negative and also highly expressed CD56 and were heterogeneously positive for CD34. This immunophenotype completely mirrored that at the initial diagnosis of AMKL. The cells were isolated by flow cell sorting, and FISH confirmed the presence of the CBFA2T3::GLIS2 gene fusion (Figure 1D). RT‒PCR-based investigation of the whole BM sample revealed the presence of the respective fusion transcript (a 1-log reduction in CBFA2T3::GLIS2 expression from the time of diagnosis). Considering that AMKL cells reappeared in the BM, a new biopsy of the tumor mass in the femur was performed. An MFC study of the tumor mass revealed cells with an immunophenotype that completely resembled that of the initially diagnosed AMKL, which was confirmed by the positivity for the thrombocytic antigens CD61 and CD41a (Figure 2C). A FISH study of intraosseous tumor dabs revealed CBFA2T3::GLIS2 fusion formation and the absence of EWSR1 rearrangement (Figure 1E, F). A pure tumor cell suspension was isolated from the homogenized biopsy material by flow cell sorting for additional molecular studies. FISH of the sorted cells confirmed the presence of the CBFA2T3::GLIS2 fusion (data not shown). RNA-seq analysis of the tumor biopsy material confirmed the expression of the CBFA2T3::GLIS2 fusion transcript, with its sequence fully matching that obtained by the initial RNA-seq results (Figure 1G). No Ewing sarcoma-specific EWSR1 fusion transcripts were found.
Finally, the diagnosis was changed from secondary Ewing sarcoma to extramedullary relapse of AMKL with inv(16)(p13q24)/CBFA2T3::GLIS2. Palliative chemotherapy with low-dose cytarabine in conjunction with 6-mercaptopurine was administered. The patient’s clinical condition gradually worsened, and the patient died 5 months after biopsy.
4. Discussion
AMKL is a very heterogeneous form of AML [22,33] and is defined by the presence of leukemic megakaryoblastic cells expressing platelet-specific surface glycoproteins [23,34]. AMKL is significantly more common in children than in adults, accounting for 4–15% of pediatric AML cases, as reported by large collaborative studies [10,11,12]. Except for the expression of CD61, CD41 and isoforms of CD42, the antigen expression profiles of AMKL cells vary greatly [23], in accordance with the genetic subgroups of this AML type. In non-Down syndrome children with AMKL, CBFA2T3::GLIS2 is the most frequent chimeric oncogene identified to date [1,10,35]. The most common chimeric CBFA2T3::GLIS2 transcript is formed between exon 11 of CBFA2T3 and exon 3 of GLIS2 [10,13,36], but other rare fusion transcripts, such as CBFA2T3-ex10/GLIS2-ex3, CBFA2T3-ex12/GLIS2-ex1 [10], and CBFA2T3-ex10/GLIS2-ex2 [13], have also been reported. AMKL with CBFA2T3::GLIS2 has a very specific immunophenotype, which is usually referred to as the RAM phenotype [15,16,17]. Although the majority of AMKL cases are CD45 positive [23,33], the RAM phenotype belongs to the CD45-negative AMKL subgroup. Moreover, these patients are characterized by extremely bright CD56 and the absence of HLA-DR and CD38 [16,18]. Furthermore, CD56+CD45- cells are always suggestive of BM metastases of various solid tumors [16,19,20,37], and even BM differentiation between leukemia and nonhematopoietic tumors is one of the main questions in the CBFA2T3::GLIS2-positive AMKL diagnosis [16,20]. Pediatric AMKL with the CBFA2T3::GLIS2 fusion is strongly associated with a poor prognosis because of the high frequency of primary induction failure and a high cumulative incidence of relapse [1,13]. Considering the very poor treatment response and initial BM relapse after the first HSCT in the present case, the second relapse was absolutely expectable. Moreover, extramedullary involvement both at diagnosis and in relapse is relatively frequent in CBFA2T3::GLIS2-positive leukemia patients compared with AML patients without this genetic aberration [38,39,40].
Ewing sarcoma is diagnosed very rarely as a secondary malignant neoplasm [41,42,43,44], accounting for less than 1.5% of all secondary tumors after the treatment of all childhood cancers [41,45]. In our case, CT and MRI revealed a characteristic localization of the tumor in the proximal metadiaphysis of the femur, with cortical destruction and a spiculated periosteal reaction, which could indeed be interpreted as Ewing sarcoma [46]. However, the obtained ADC values of the extramedullary mass, ranging from 0.240×10−3 to 0.426×10−3 mm2/s, were slightly lower than the values obtained in the MS research (minimum value was 0.36×10−3 mm2/s) [29].
The differential diagnosis between leukemia relapse and secondary tumors is crucial in the case of secondary leukemia development. It is typically necessary to prove the diagnosis of secondary tumors rather than a lineage switch at relapse for the types of leukemia that demonstrate increased lineage plasticity [47,48,49], such as AL with KMT2A, ZNF384 or DUX4 gene rearrangements or early T-cell acute lymphoblastic leukemia (ETP-ALL) [50,51]. For such cases, the main tumor site is the BM, and the differences in the morphology and/or immunophenotype between initially diagnosed leukemia and secondary leukemia make it necessary to confirm the relapse or a secondary tumor by molecular studies [51]. In our patient, we observed no differences in the immunophenotypes between initial AMKL and BM leukemic cells at the MFC-MRD level or extramedullary relapse. Nevertheless, the specific location of the small round cell tumor without BM involvement, even at the MFC-MRD level, led to the misinterpretation of relapse development as secondary Ewing sarcoma. Typically, distinguishing between solid tumors and acute leukemia by antigen expression profile analysis is not difficult [19], as the vast majority of AL patients express hematopoietic markers, including the panleukocytic antigen CD45 and markers of either lymphoid or myeloid lineages [52], whereas the immunophenotypes of nonhematopoietic tumors are significantly different, and CD45 negativity is the obligatory feature of nonhematopoietic cells [19]. However, in the presented case, these differences were not as obvious. As mentioned above, excluding solid tumors is always one of the main questions in the diagnosis of AMKL with the RAM phenotype [16,18]. Although it is relatively easy to perform in the BM [16], differential diagnosis of isolated extramedullary tumors seems much more difficult. The morphological differential diagnosis between Ewing sarcoma and megakaryoblastic sarcoma presents significant challenges owing to their overlapping histological features, including small round blue cell morphology and similar growth patterns. Immunohistochemically, both tumors can express CD99, which is traditionally considered a marker for Ewing sarcoma; however, megakaryoblastic sarcoma may also show variable expression of this marker, making the interpretation more complex [53]. The definitive diagnosis often requires a comprehensive panel of immunohistochemical markers, including specific megakaryocytic markers (such as CD41, CD61, and Factor VIII), CD99, FLI1, and NKX2.2, along with molecular testing for EWSR1 rearrangement, as no single marker is exclusively specific for either entity, and the interpretation must be performed in the context of the complete clinical and pathological picture [54]. In such complicated cases, only MFC, with its wide range of applicable antigens, and comprehensive genetic studies, are always capable of confirming the development of MS or nonhematopoietic tumors.
In summary, the presented case demonstrates the difficulties of differential diagnosis between leukemia relapse and the development of a secondary tumor. Not only significant changes in the presenting features but also atypical locations can lead to misdiagnosis and incorrect treatment. While making a diagnosis solely based on one method could be insufficient, in-depth laboratory and radiation studies, together with accurate and precise anamnesis investigations, can be effective enough for the correct tumor type definition with subsequent selection of a treatment strategy.
5. Methods
Immunophenotyping
Analysis of the immunophenotype of tumor cells was performed by using 10-color combinations of monoclonal antibodies according to the diagnostic standards of the Moscow–Berlin group, as described previously [52]. All the samples were processed according to the manufacturer's recommendations. At least 30,000 nucleated cells were collected from each diagnostic sample by using a Navios (Beckman Coulter [BC], Indianapolis, IN, USA) flow cytometer. The EuroFlow guidelines for machine performance monitoring were used [55]. Flow-Check Pro Fluorospheres (BC) were used for daily cytometer optimization. The results were analyzed with Kaluza Analysis 2.1 (BC). Leukemic cells were gated on the basis of CD45 and lineage-associated antigen expression and side-scatter light characteristics [52]. Residual normal cells preserved in a sample were used as an internal control. Minimal residual disease (MRD) was evaluated by MFC according to the FlowCluster group approach [56], with an adaptation for the RAM phenotype [16,57].
Leukemic blasts were isolated for cytogenetic and molecular studies from BM samples and soft tissue biopsy samples via a FACS Aria III sorter (Becton Dickinson [BD], San Jose, CA, USA) as described previously [58]. Sample preparation depended on the downstream molecular study. For FISH, an erythrocyte lysis buffer with a fixative (FACS Lyse; BD) was used, and the presorted samples were diluted with RPMI-1640 medium (PanEco, Russia). For PCR and sequencing, a nonfixative lysis agent (PharmLyse; BD) was used, and the cells were diluted with phosphate-buffered saline (Cell Wash; BD). The cells were sorted in purity mode and collected into Eppendorf tubes containing the relevant buffer. From 10,000 to 15,000 cells were sorted in duplicate for FISH, and 3 to 5 million cells were sorted in duplicate for molecular studies.
Cytogenetic and Molecular Studies
Conventional GTG-banded karyotyping was performed on bone marrow aspirates, which were cultured according to a previously described method [59]. The results were interpreted following the International System for Human Cytogenomic Nomenclature-2024 [60].
Fluorescence in situ hybridization (FISH) was conducted with a Cytocell CBFA2T3::GLIS2 dual-color dual-fusion probe (Cytocell, Cambridge, UK) and the Kreatech EWSR1 dual-color break-apart probe (Leica Biosystems, Nussloch, Germany). Reverse transcription‒polymerase chain reaction (RT‒PCR) for the CBFA2T3::GLIS2 fusion transcript was performed with the following primers and probe: CBFA2T3-F, ACGCCGAGGACACAAAGAAGGG; GLIS2-R, ACACCATCCAAATAGCGCAG; and GLIS2-P, FAM-CGAGGCACTGGGCACTGGAGGC-BHQ1. Whole-transcriptome sequencing (RNA-seq) was carried out by using the NEBNext Ultra II Directional RNA library preparation Kit (NEB, Ipswich, MA, USA) for bone marrow aspirates and the VAHTS Universal V8 RNA-seq Kit (Vazyme, Nanjing, PRC) for a biopsy sample of the extramedullary mass. The samples were sequenced on an Illumina NextSeq platform (Illumina, San Diego, CA, USA) and analyzed using the Arriba fusion detection algorithm [61]. Additionally, mutations in genes relevant to myeloid neoplasm development were examined using the Qiagen human Myeloid Neoplasms panel (Qiagen, Hilden, Germany). Sequencing was performed on an Illumina MiSeq platform (Illumina, San Diego, CA, USA), and data analysis was conducted using the Qiagen built-in pipeline.
Author Contributions
Conceptualization: S.L., E.M., E.Z. and A.P.; methodology, validation, and investigation, E.M., S.B., D.A., S.K., A.D., A.S., M.G., I.S., G.T., Y.O., E.Z. and A.P.; data curation, S.L., E.M., S.B., D.A., O.L., E.Z. and A.P. ; original draft preparation, S.L., S.B., D.A., E.Z. and A.P.; visualization: E.M., S.B., D.A., E.Z. and A.P. supervision, G.T., Y.O., G.N., A.M., E.Z. and A.P.; project administration: G.N., A.M., E.Z. and A.P.. All authors have read and agreed to the published version of the manuscript.
Funding
The authors thank “Science for Children” foundation for the support of diagnostic studies (immunophenotyping, cytogenetics and molecular genetics) for the pediatric AML.
Patient Consent Statement
Informed consent for the collection and investigation of samples was obtained from patients’ parents.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interests
Authors declare no relevant conflicts of interests.
References
- de Rooij, J.D.; Branstetter, C.; Ma, J.; Li, Y.; Walsh, M.P.; Cheng, J.; Obulkasim, A.; Dang, J.; Easton, J.; Verboon, L.J.; et al. Pediatric non-Down syndrome acute megakaryoblastic leukemia is characterized by distinct genomic subsets with varying outcomes. Nat Genet 2017, 49, 451-456. [CrossRef]
- Bennett, J.M.; Catovsky, D.; Daniel, M.T.; Flandrin, G.; Galton, D.A.; Gralnick, H.R.; Sultan, C. Criteria for the diagnosis of acute leukemia of megakaryocyte lineage (M7). A report of the French-American-British Cooperative Group. Ann Intern Med 1985, 103, 460-462. [CrossRef]
- Bloomfield, C.D.; Brunning, R.D. FAB M7: acute megakaryoblastic leukemia--beyond morphology. Ann Intern Med 1985, 103, 450-452. [CrossRef]
- Athale, U.H.; Razzouk, B.I.; Raimondi, S.C.; Long, X.; Behm, F.G.; Head, D.R.; Srivastava, D.K.; Rubnitz, J.E.; Bowman, L.; Pui, C.H.; et al. Biology and outcome of childhood acute megakaryoblastic leukemia: a single institution's experience. Blood 2001, 97, 3727-3732. [CrossRef]
- Barnard, D.R.; Alonzo, T.A.; Gerbing, R.B.; Lange, B.; Woods, W.G. Comparison of childhood myelodysplastic syndrome, AML FAB M6 or M7, CCG 2891: Report from the Children's Oncology Group. Pediatric Blood and Cancer 2007, 49, 17-22. [CrossRef]
- Pagano, L.; Pulsoni, A.; Vignetti, M.; Mele, L.; Fianchi, L.; Petti, M.C.; Mirto, S.; Falcucci, P.; Fazi, P.; Broccia, G.; et al. Acute megakaryoblastic leukemia: experience of GIMEMA trials. Leukemia 2002 16:9 2002, 16, 1622-1626. [CrossRef]
- Ribeiro, R.C.; Oliveira, M.S.P.; Fairclough, D.; Hurwitz, C.; Mirro, J.; Behm, F.G.; Head, D.; Silva, M.L.M.; Raimondi, S.C.; Crist, W.M.; et al. Acute Megakaryoblastic Leukemia in Children and Adolescents: A Retrospective Analysis of 24 Cases. Leukemia & Lymphoma 1993, 10, 299-306. [CrossRef]
- Tallman, M.S.; Neuberg, D.; Bennett, J.M.; Francois, C.J.; Paietta, E.; Wiernik, P.H.; Dewald, G.; Cassileth, P.A.; Oken, M.M.; Rowe, J.M. Acute megakaryocytic leukemia: the Eastern Cooperative Oncology Group experience. Blood 2000, 96, 2405-2411.
- Du, Y.; Yang, L.; Qi, S.; Chen, Z.; Sun, M.; Wu, M.; Wu, B.; Tao, F.; Xiong, H. Clinical Analysis of Pediatric Acute Megakaryocytic Leukemia With CBFA2T3-GLIS2 Fusion Gene. J Pediatr Hematol Oncol 2024, 46, 96-103. [CrossRef]
- Gruber, T.A.; Larson Gedman, A.; Zhang, J.; Koss, C.S.; Marada, S.; Ta, H.Q.; Chen, S.C.; Su, X.; Ogden, S.K.; Dang, J.; et al. An inv(16)(p13.3q24.3)-encoded CBFA2T3-GLIS2 fusion protein defines an aggressive subtype of pediatric acute megakaryoblastic leukemia. Cancer cell 2012, 22, 683-683. [CrossRef]
- Rørvik, S.D.; Torkildsen, S.; Bruserud, Ø.; Tvedt, T.H.A. Acute myeloid leukemia with rare recurring translocations—an overview of the entities included in the international consensus classification. Annals of Hematology 2024, 103, 1103-1119. [CrossRef]
- Wu, K.; Liu, H.; Xie, Y.; LiuCui, Y.; Cai, J.; Wang, R.; Wang, Y.; Wang, X.; Chen, X.; Zhao, S.; et al. Genomic Landscape of Pediatric Non-Down's Syndrome Acute Megakaryoblastic Leukemia in China. In Proceedings of the 65th ASH Annual Meeting, San Diego, California, 29 November 2023, 2023; p. 4331.
- Masetti, R.; Pigazzi, M.; Togni, M.; Astolfi, A.; Indio, V.; Manara, E.; Casadio, R.; Pession, A.; Basso, G.; Locatelli, F. CBFA2T3-GLIS2 fusion transcript is a novel common feature in pediatric, cytogenetically normal AML, not restricted to FAB M7 subtype. Blood 2013, 121, 3469-3472. [CrossRef]
- Smith, J.L.; Ries, R.E.; Hylkema, T.; Alonzo, T.A.; Gerbing, R.B.; Santaguida, M.T.; Brodersen, L.E.; Pardo, L.; Cummings, C.L.; Loeb, K.R.; et al. Comprehensive Transcriptome Profiling of Cryptic CBFA2T3-GLIS2 Fusion-positive AML Defines Novel Therapeutic Options – A COG and TARGET Pediatric AML Study. Clinical cancer research : an official journal of the American Association for Cancer Research 2020, 26, 726-726. [CrossRef]
- Eidenschink Brodersen, L.; Alonzo, T.A.; Menssen, A.J.; Gerbing, R.B.; Pardo, L.; Voigt, A.P.; Kahwash, S.B.; Hirsch, B.; Raimondi, S.; Gamis, A.S.; et al. A recurrent immunophenotype at diagnosis independently identifies high-risk pediatric acute myeloid leukemia: a report from Children's Oncology Group. Leukemia 2016, 30, 2077-2080. [CrossRef]
- Zangrando, A.; Cavagnero, F.; Scarparo, P.; Varotto, E.; Francescato, S.; Tregnago, C.; Cuccurullo, R.; Fagioli, F.; Nigro, L.L.; Masetti, R.; et al. CD56, HLA-DR, and CD45 recognize a subtype of childhood AML harboring CBFA2T3-GLIS2 fusion transcript. Cytometry A 2021, 99, 844-850. [CrossRef]
- Liu, H.; Wu, K.; Hu, W.; Chen, X.; Tang, Y.; Ma, Y.; Chen, C.; Xie, Y.; Yu, L.; Huang, J.; et al. Immunophenotypic clustering in paediatric acute myeloid leukaemia. Br J Haematol 2024, 204, 2275-2286. [CrossRef]
- Pardo, L.M.; Voigt, A.P.; Alonzo, T.A.; Wilson, E.R.; Gerbing, R.B.; Paine, D.J.; Dai, F.; Menssen, A.J.; Raimondi, S.C.; Hirsch, B.A.; et al. Deciphering the Significance of CD56 Expression in Pediatric Acute Myeloid Leukemia: A Report from the Children's Oncology Group. Cytometry B Clin Cytom 2020, 98, 52-56. [CrossRef]
- Ferreira-Facio, C.S.; Botafogo, V.; Ferrao, P.M.; Canellas, M.C.; Milito, C.B.; Romano, S.; Lopes, D.V.; Teixeira, L.C.; Oliveira, E.; Bruno-Riscarolli, E.; et al. Flow Cytometry Immunophenotyping for Diagnostic Orientation and Classification of Pediatric Cancer Based on the EuroFlow Solid Tumor Orientation Tube (STOT). Cancers (Basel) 2021, 13. [CrossRef]
- Gajendra, S.; Anupurba, S.; Gupta, R.; Mallick, S.; Panda, D.; Thakral, D.; Gupta, S.K.; Bakhshi, S.; Seth, R.; Rai, S.; et al. Acute myeloid leukemia with RAM immunophenotype: A new underdiagnosed entity. Int J Lab Hematol 2023, 45, 541-552. [CrossRef]
- Panda, D.; Chatterjee, G.; Sardana, R.; Khanka, T.; Ghogale, S.; Deshpande, N.; Badrinath, Y.; Shetty, D.; Narula, G.; Banavali, S.; et al. Utility of CD36 as a novel addition to the immunophenotypic signature of RAM-phenotype acute myeloid leukemia and study of its clinicopathological characteristics. Cytometry B Clin Cytom 2021, 100, 206-217. [CrossRef]
- Chisholm, K.M.; Smith, J.; Heerema-McKenney, A.E.; Choi, J.K.; Ries, R.E.; Hirsch, B.A.; Raimondi, S.C.; Wang, Y.C.; Dang, A.; Alonzo, T.A.; et al. Pathologic, cytogenetic, and molecular features of acute myeloid leukemia with megakaryocytic differentiation: A report from the Children's Oncology Group. Pediatr Blood Cancer 2023, 70, e30251. [CrossRef]
- Brouwer, N.; Matarraz, S.; Nierkens, S.; Hofmans, M.; Novakova, M.; da Costa, E.S.; Fernandez, P.; Bras, A.E.; de Mello, F.V.; Mejstrikova, E.; et al. Immunophenotypic Analysis of Acute Megakaryoblastic Leukemia: A EuroFlow Study. Cancers (Basel) 2022, 14. [CrossRef]
- Bisschop, M.M.; Revesz, T.; Bierings, M.; van Weerden, J.F.; van Wering, E.R.; Hahlen, K.; van der Does-van den Berg, A. Extramedullary infiltrates at diagnosis have no prognostic significance in children with acute myeloid leukaemia. Leukemia 2001, 15, 46-49. [CrossRef]
- Dinikina, Y.V.; Maschan, A.A. Extramedullary involvement in pediatric myeloid leukemia: challenges of diagnosis and treatment. Clinical cases and a literature review (In Russ.). Pediatric Hematology/Oncology and Immunopathology 2023, 22, 123-141. [CrossRef]
- Samborska, M.; Derwich, K.; Skalska-Sadowska, J.; Kurzawa, P.; Wachowiak, J. Myeloid sarcoma in children – diagnostic and therapeutic difficulties. Contemporary Oncology 2016, 20, 444-444. [CrossRef]
- Støve, H.K.; Sandahl, J.D.; Abrahamsson, J.; Asdahl, P.H.; Forestier, E.; Ha, S.Y.; Jahnukainen, K.; Jónsson, Ó.G.; Lausen, B.; Palle, J.; et al. Extramedullary leukemia in children with acute myeloid leukemia: A population-based cohort study from the Nordic Society of Pediatric Hematology and Oncology (NOPHO). Pediatric blood & cancer 2017, 64. [CrossRef]
- Khoury, J.D.; Solary, E.; Abla, O.; Akkari, Y.; Alaggio, R.; Apperley, J.F.; Bejar, R.; Berti, E.; Busque, L.; Chan, J.K.C.; et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia 2022, 36, 1703-1719. [CrossRef]
- Meyer, H.J.; Beimler, M.; Borte, G.; Pönisch, W.; Surov, A. Radiological and Clinical Patterns of Myeloid Sarcoma. Radiology and Oncology 2019, 53, 213-213. [CrossRef]
- Roberts, A.S.; Shetty, A.S.; Mellnick, V.M.; Pickhardt, P.J.; Bhalla, S.; Menias, C.O. Extramedullary haematopoiesis: radiological imaging features. Clin Radiol 2016, 71, 807-814. [CrossRef]
- Vasilyeva, M.S.; Kalinina, I.I.; Venyov, D.A.; Lebedeva, S.A.; Bankole, V.A.; Abashidze, Z.A.; Aleinikova, O.V.; Zerkalenkova, E.A.; Gaskova, M.V.; Itov, A.B.; et al. Preliminary results of treatment of intermediate-risk patients according to the AML-MRD-2018 protocol. Pediatric Hematology/Oncology and Immunopathology 2025, 24, 14-25.
- Lebedeva, S.A.; Kalinina, I.I.; Kazakova, A.N.; Bankole, V.A.; Vasileva, M.S.; Venyov, D.A.; Baydildina, D.D.; Aleinikova, O.V.; Popa, A.V.; Maschan, A.A.; et al. The prognostic significance of partner genes and breakpoint locations in children with KMT2A-rearranged acute myeloid leukemia. Pediatric Hematology/Oncology and Immunopathology 2025, 24, 58-65.
- Alexenko, M.; Illarionova, O.; Verzhbitskaya, T.; Zerkalenkova, E.; Novikova, I.; Panferova, A.; Fechina, L.; Tsaur, G.; Olshanskaya, J.; Popov, A. Immunophenotypic characterization of acute megakaryoblastic leukaemia in children. Pediatric Hematology/Oncology and Immunopathology 2019, 18, 35-40. [CrossRef]
- Schweitzer, J.; Zimmermann, M.; Rasche, M.; von Neuhoff, C.; Creutzig, U.; Dworzak, M.; Reinhardt, D.; Klusmann, J.H. Improved outcome of pediatric patients with acute megakaryoblastic leukemia in the AML-BFM 04 trial. Ann Hematol 2015, 94, 1327-1336. [CrossRef]
- Hara, Y.; Shiba, N.; Ohki, K.; Tabuchi, K.; Yamato, G.; Park, M.J.; Tomizawa, D.; Kinoshita, A.; Shimada, A.; Arakawa, H.; et al. Prognostic impact of specific molecular profiles in pediatric acute megakaryoblastic leukemia in non-Down syndrome. Genes Chromosomes Cancer 2017, 56, 394-404. [CrossRef]
- Thiollier, C.; Lopez, C.K.; Gerby, B.; Ignacimouttou, C.; Poglio, S.; Duffourd, Y.; Guegan, J.; Rivera-Munoz, P.; Bluteau, O.; Mabialah, V.; et al. Characterization of novel genomic alterations and therapeutic approaches using acute megakaryoblastic leukemia xenograft models. J Exp Med 2012, 209, 2017-2031. [CrossRef]
- Theodorakos, I.; Paterakis, G.; Papadakis, V.; Vicha, A.; Topakas, G.; Jencova, P.; Karchilaki, E.; Taparkou, A.; Tsagarakis, N.J.; Polychronopoulou, S. Interference of bone marrow CD56(+) mesenchymal stromal cells in minimal residual disease investigation of neuroblastoma and other CD45(-)/CD56(+) pediatric malignancies using flow cytometry. Pediatr Blood Cancer 2019, 66, e27799. [CrossRef]
- Masetti, R.; Bertuccio, S.N.; Pession, A.; Locatelli, F. CBFA2T3-GLIS2-positive acute myeloid leukaemia. A peculiar paediatric entity. Br J Haematol 2019, 184, 337-347. [CrossRef]
- Pession, A.; Masetti, R.; Rizzari, C.; Putti, M.C.; Casale, F.; Fagioli, F.; Luciani, M.; Lo Nigro, L.; Menna, G.; Micalizzi, C.; et al. Results of the AIEOP AML 2002/01 multicenter prospective trial for the treatment of children with acute myeloid leukemia. Blood 2013, 122, 170-178. [CrossRef]
- Masetti, R.; Pigazzi, M.; Togni, M.; Astolfi, A.; Indio, V.; Manara, E.; Casadio, R.; Pession, A.; Basso, G.; Locatelli, F. CBFA2T3-GLIS2 fusion transcript is a novel common feature in pediatric, cytogenetically normal AML, not restricted to FAB M7 subtype. Blood 2013, 121, 3469-3472. [CrossRef]
- Zollner, S.K.; Kauertz, K.L.; Kaiser, I.; Kerkhoff, M.; Schaefer, C.; Tassius, M.; Jabar, S.; Jurgens, H.; Ladenstein, R.; Kuhne, T.; et al. Ewing Sarcoma as Secondary Malignant Neoplasm-Epidemiological and Clinical Analysis of an International Trial Registry. Cancers (Basel) 2022, 14. [CrossRef]
- Loning, L.; Zimmermann, M.; Reiter, A.; Kaatsch, P.; Henze, G.; Riehm, H.; Schrappe, M. Secondary neoplasms subsequent to Berlin-Frankfurt-Munster therapy of acute lymphoblastic leukemia in childhood: significantly lower risk without cranial radiotherapy. Blood 2000, 95, 2770-2775.
- Applebaum, M.A.; Goldsby, R.; Neuhaus, J.; DuBois, S.G. Clinical features and outcomes in patients with secondary Ewing sarcoma. Pediatr Blood Cancer 2013, 60, 611-615. [CrossRef]
- Kim, G.E.; Beach, B.; Gastier-Foster, J.M.; Murata-Collins, J.L.; Rowland, J.M.; O'Donnell, R.J.; Goldsby, R.E. Ewing sarcoma as a second malignant neoplasm after acute lymphoblastic leukemia. Pediatr Blood Cancer 2005, 45, 57-59. [CrossRef]
- Zhu, N.; Ni, H.; Guo, S.; Shen, Y.Q.; Chen, Q. Bone complications of cancer treatment. Cancer Treat Rev 2024, 130, 102828. [CrossRef]
- Almond, L.M.; Charalampakis, M.; Ford, S.J.; Gourevitch, D.; Desai, A. Myeloid Sarcoma: Presentation, Diagnosis, and Treatment. Clin Lymphoma Myeloma Leuk 2017, 17, 263-267. [CrossRef]
- Semchenkova, A.; Mikhailova, E.; Komkov, A.; Gaskova, M.; Abasov, R.; Matveev, E.; Kazanov, M.; Mamedov, I.; Shmitko, A.; Belova, V.; et al. Lineage Conversion in Pediatric B-Cell Precursor Acute Leukemia under Blinatumomab Therapy. Int J Mol Sci 2022, 23. [CrossRef]
- Dorantes-Acosta, E.; Pelayo, R. Lineage switching in acute leukemias: a consequence of stem cell plasticity? Bone Marrow Res 2012, 2012, 406796. [CrossRef]
- Silbert, S.K.; Rankin, A.W.; Hoang, C.N.; Semchenkova, A.; Myers, R.M.; Zerkalenkova PhD, E.; Wang, H.-W.; Kovach, A.E.; Yuan, C.M.; Delgado Colon, D.; et al. Project EVOLVE: An international analysis of postimmunotherapy lineage switch, an emergent form of relapse in leukemia. Blood 2025, blood.2024026655-blood.2024026655. [CrossRef]
- Permikin, Z.; Popov, A.; Verzhbitskaya, T.; Riger, T.; Plekhanova, O.; Makarova, O.; Fronkova, E.; Trka, J.; Meyer, C.; Marschalek, R.; et al. Lineage switch to acute myeloid leukemia during induction chemotherapy for early T-cell precursor acute lymphoblastic leukemia with the translocation t(6;11)(q27;q23)/KMT2A-AFDN: A case report. Leuk Res 2022, 112, 106758. [CrossRef]
- Demina, I.; Dagestani, A.; Borkovskaia, A.; Semchenkova, A.; Soldatkina, O.; Kashpor, S.; Olshanskaya, Y.; Roumiantseva, J.; Karachunskiy, A.; Novichkova, G.; et al. Immunophenotypic but Not Genetic Changes Reclassify the Majority of Relapsed/Refractory Pediatric Cases of Early T-Cell Precursor Acute Lymphoblastic Leukemia. International journal of molecular sciences 2024, 25. [CrossRef]
- Popov A.; Verzhbitskaya T.; Movchan L.; Demina I.; Mikhailova E.; Semchenkova A.; Permikin Zh.; Shman T.; Karachunskiy A.; G., N. Flow cytometry in acute leukemia diagnostics. Guidelines of Russian-Belarusian multicenter group for pediatric leukemia studies. Pediatric Hematology/Oncology and Immunopathology 2023, 22, 165-177.
- Novello, M.; Coli, A.; Della Pepa, G.M.; Martini, M.; Doglietto, F.; De Stefano, V.; Bellesi, S.; Pescarmona, E.; Lauriola, L. Myeloid sarcoma with megakaryoblastic differentiation mimicking a sellar tumor. Neuropathology : official journal of the Japanese Society of Neuropathology 2014, 34, 179-184. [CrossRef]
- Cannatella, J.; Ganapathi, K.; Horvai, A. Hematolymphoid Neoplasms Rarely Mimic Undifferentiated Pleomorphic Sarcoma of Soft Tissue. Archives of pathology & laboratory medicine 2020, 144, 1547-1552. [CrossRef]
- Kalina, T.; Flores-Montero, J.; Lecrevisse, Q.; Pedreira, C.E.; van der Velden, V.H.; Novakova, M.; Mejstrikova, E.; Hrusak, O.; Bottcher, S.; Karsch, D.; et al. Quality assessment program for EuroFlow protocols: summary results of four-year (2010-2013) quality assurance rounds. Cytometry A 2015, 87, 145-156. [CrossRef]
- Buldini, B.; Maurer-Granofszky, M.; Varotto, E.; Dworzak, M.N. Flow-Cytometric Monitoring of Minimal Residual Disease in Pediatric Patients With Acute Myeloid Leukemia: Recent Advances and Future Strategies. Front Pediatr 2019, 7, 412. [CrossRef]
- Boztug, H.; Schumich, A.; Potschger, U.; Muhlegger, N.; Kolenova, A.; Reinhardt, K.; Dworzak, M. Blast cell deficiency of CD11a as a marker of acute megakaryoblastic leukemia and transient myeloproliferative disease in children with and without Down syndrome. Cytometry B Clin Cytom 2013, 84, 370-378. [CrossRef]
- Semchenkova, A.; Zerkalenkova, E.; Demina, I.; Kashpor, S.; Volchkov, E.; Zakharova, E.; Larin, S.; Olshanskaya, Y.; Novichkova, G.; Maschan, A.; et al. Recognizing Minor Leukemic Populations with Monocytic Features in Mixed-Phenotype Acute Leukemia by Flow Cell Sorting Followed by Cytogenetic and Molecular Studies: Report of Five Exemplary Cases. Int J Mol Sci 2023, 24. [CrossRef]
- den Nijs, J.I.; Gonggrijp, H.S.; Augustinus, E.; Leeksma, C.H. Hot bands: a simple G-banding method for leukemic metaphases. Cancer Genet Cytogenet 1985, 15, 373-374. [CrossRef]
- ISCN 2020: An International System for Human Cytogenomic Nomenclature (2020). ISCN 2020 2020. [CrossRef]
- Uhrig, S.; Ellermann, J.; Walther, T.; Burkhardt, P.; Frohlich, M.; Hutter, B.; Toprak, U.H.; Neumann, O.; Stenzinger, A.; Scholl, C.; et al. Accurate and efficient detection of gene fusions from RNA sequencing data. Genome Res 2021, 31, 448-460. [CrossRef]
Figure 1.
Morphological, cytogenetic and molecular examination of primary CBFA2T3::GLIS2-positive AMKL and isolated extramedullary relapse samples. A – Morphology of the BM in primary AMKL; B – morphology of a BM cell conglomerate in a relapse sample; C – FISH with the Cytocell CBFA2T3::GLIS2 dual-color dual-fusion probe (Cytocell, Cambridge, UK) in the BM in primary AMKL; D – FISH with the CBFA2T3::GLIS2 probe in the flow-sorted BM population from a second relapse sample; E – FISH with the CBFA2T3::GLIS2 probe in the intraosseous tumor dab from relapse; F – FISH with the Kreatech EWSR1 dual-color break-apart probe (Leica Biosystems, Nussloch, Germany) in the intraosseous tumor dab from relapse; G – the CBFA2T3::GLIS2 fusion transcript detected by RNA-seq in a relapse sample.
Figure 2.
Flow cytometric studies in the presented case. A – Immunophenotype of BM blasts in primary AMKL; B – illustrative dot plots for the key points of MFC-MRD monitoring in the BM; C – immunophenotype of leukemic blasts in the extramedullary mass biopsy at the second relapse. Leukemic blasts are red, whereas the remaining nucleated cells are gray.
Figure 2.
Flow cytometric studies in the presented case. A – Immunophenotype of BM blasts in primary AMKL; B – illustrative dot plots for the key points of MFC-MRD monitoring in the BM; C – immunophenotype of leukemic blasts in the extramedullary mass biopsy at the second relapse. Leukemic blasts are red, whereas the remaining nucleated cells are gray.
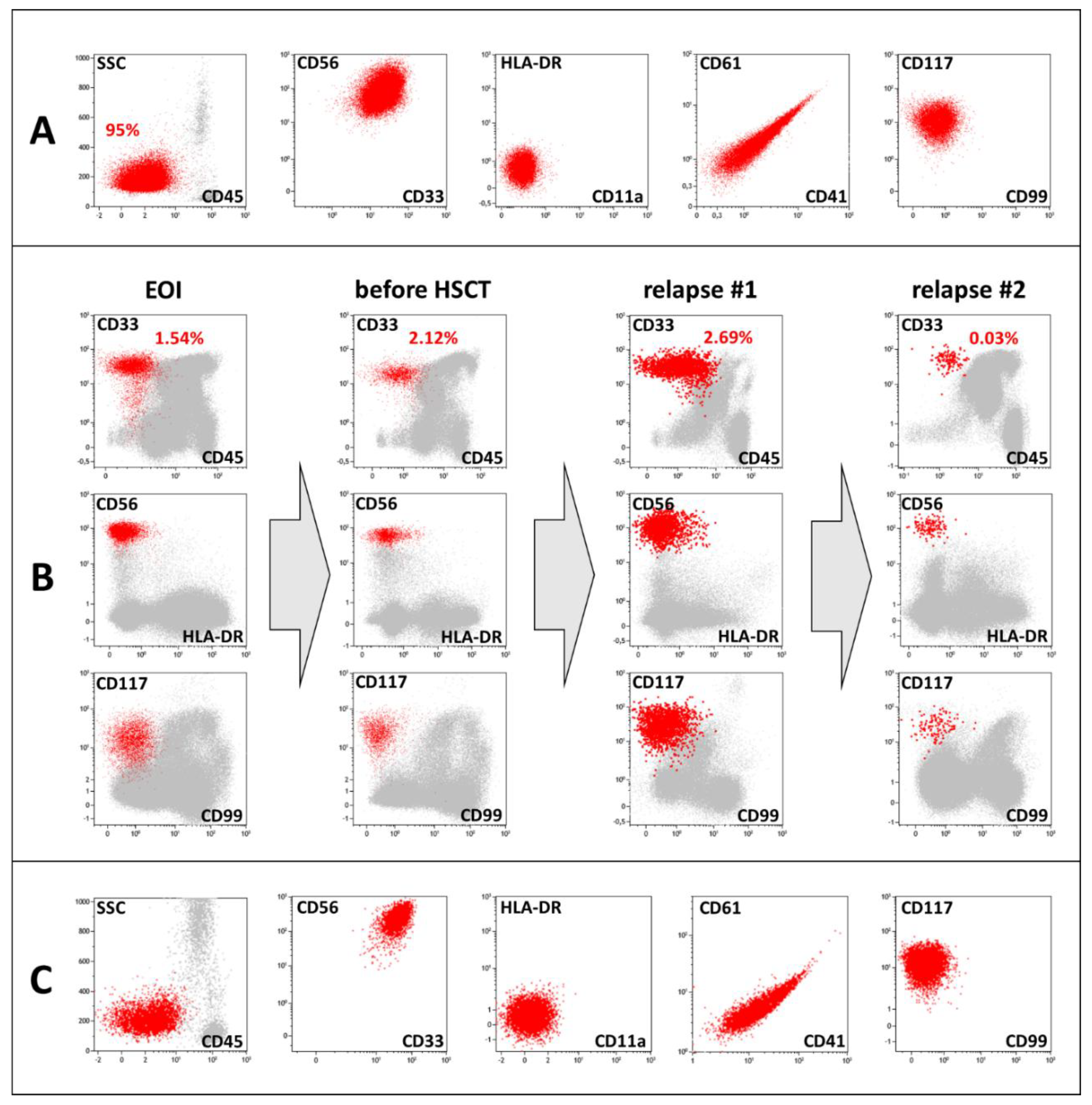
Figure 3.
MR and CT images from the second relapse. Axial MR and CT images (A): T1-weighted (a), contrast-enhanced fat-suppressed T1-weighted (b), T2-weighted (c), STIR (d), DWI (e) and ADC map with an area with restricted diffusion (0.295×10−3 mm2/s) (f) sequences. Pre- (g) and postcontrast (h) CT scans demonstrating the subperiosteal extramedullary lesion (arrowheads), peripheral soft tissue edema (white arrows) and spiculated periosteal reaction with cortical destruction (empty arrowheads) at the proximal right femur. Sagittal MR images (B): STIR (a), T2-weighted (b) and contrast-enhanced T1-weighted (c) sequences revealed subperiosteal extramedullary relapse of AMKL (arrowheads) and intramedullary bone marrow edema (stars) extending to the middle of the diaphysis with peripheral soft tissue edema (white arrow).
Figure 3.
MR and CT images from the second relapse. Axial MR and CT images (A): T1-weighted (a), contrast-enhanced fat-suppressed T1-weighted (b), T2-weighted (c), STIR (d), DWI (e) and ADC map with an area with restricted diffusion (0.295×10−3 mm2/s) (f) sequences. Pre- (g) and postcontrast (h) CT scans demonstrating the subperiosteal extramedullary lesion (arrowheads), peripheral soft tissue edema (white arrows) and spiculated periosteal reaction with cortical destruction (empty arrowheads) at the proximal right femur. Sagittal MR images (B): STIR (a), T2-weighted (b) and contrast-enhanced T1-weighted (c) sequences revealed subperiosteal extramedullary relapse of AMKL (arrowheads) and intramedullary bone marrow edema (stars) extending to the middle of the diaphysis with peripheral soft tissue edema (white arrow).
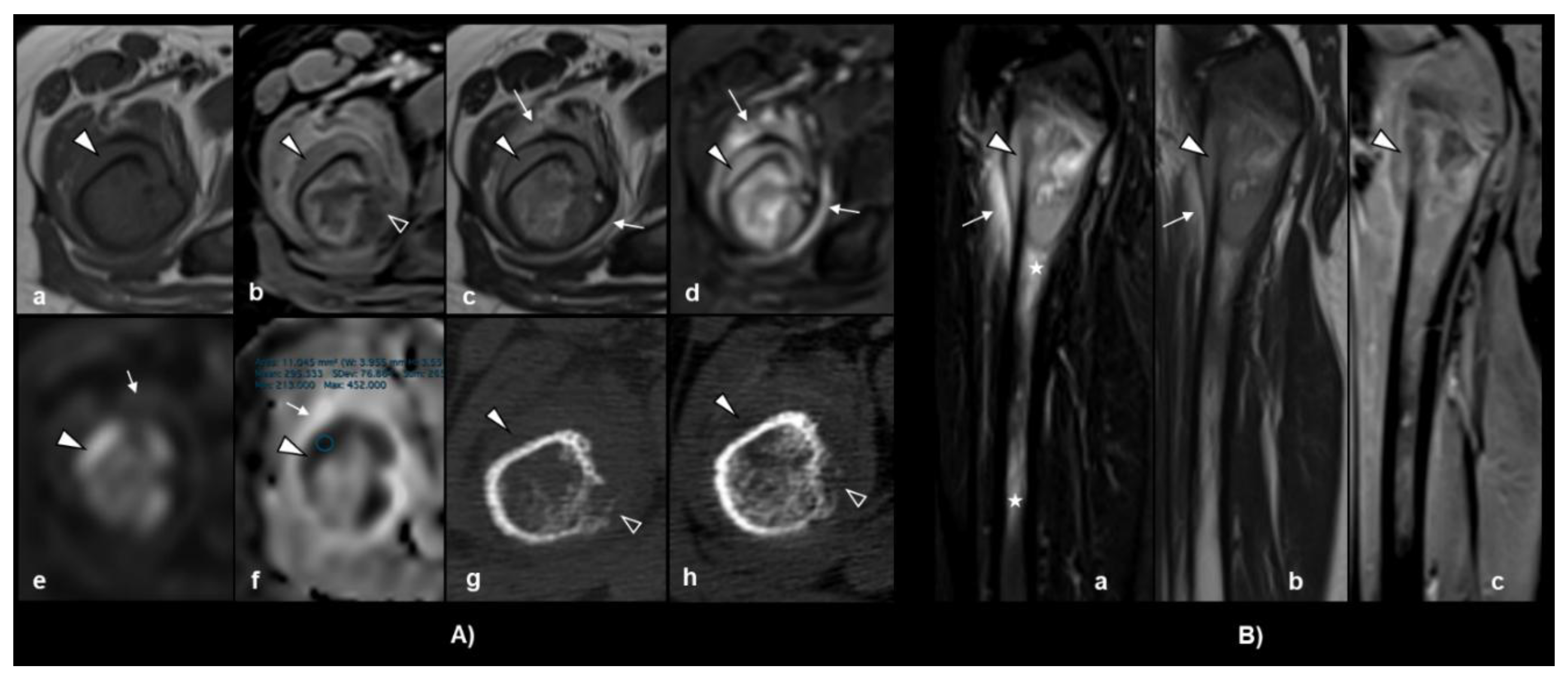
Figure 4.
Histopathological and immunohistochemical findings. (A, B) H&E staining revealed a malignant small round cell tumor with characteristic morphological features (×200 and ×400, respectively). Immunohistochemical staining revealed strong nuclear positivity for (C) FLI-1 and (D) ERG and negativity for (E) CD61. Most other specific markers were nonreactive. Given the tumor location and morphology, Ewing sarcoma was initially considered in the differential diagnosis, but further workup confirmed AMKL with extramedullary involvement.
Figure 4.
Histopathological and immunohistochemical findings. (A, B) H&E staining revealed a malignant small round cell tumor with characteristic morphological features (×200 and ×400, respectively). Immunohistochemical staining revealed strong nuclear positivity for (C) FLI-1 and (D) ERG and negativity for (E) CD61. Most other specific markers were nonreactive. Given the tumor location and morphology, Ewing sarcoma was initially considered in the differential diagnosis, but further workup confirmed AMKL with extramedullary involvement.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



