Submitted:
08 May 2025
Posted:
12 May 2025
You are already at the latest version
Abstract
Background/Objectives: Artificial intelligence (AI) is transforming drug discovery and development by enhancing the speed and precision of identifying drug candidates and optimizing their efficacy. This review evaluates the application of AI in various stages of drug discovery, from hit identification to lead optimization, and its impact on clinical outcomes. The objective is to provide insights into the role of AI across therapeutic areas and assess its contributions to improving clinical trial efficiency and pharmaceutical outcomes. Methods: A systematic review followed PRISMA guidelines to analyze studies published between 2015 and 2025, focusing on AI in drug discovery and development. A comprehensive search was performed across multiple databases to identify studies employing AI techniques. Studies were categorized based on AI methods, clinical phase, and therapeutic area. Percentages of AI methods used, clinical phase stages, and the therapeutic regions were analyzed to identify trends. Results: AI methods included machine learning (ML) at 40.9%, molecular modeling and simulation (MMS) at 20.7%, and deep learning (DL) at 10.3%. Oncology accounted for the majority of studies (72.8%), followed by dermatology (5.8%) and neurology (5.2%). In clinical phases, 39.3% of studies were in the preclinical stage, 23.1% in Clinical Phase I, and 11.0% in the transitional phase. Clinical outcome reporting was observed in 45% of studies, with 97% reporting industry partnerships. Conclusions: AI significantly enhances drug discovery and development, improving drug efficacy and clinical trial outcomes. Future work should focus on expanding AI applications into underrepresented therapeutic areas and refining models to handle complex biological systems.
Keywords:
artificial intelligence
; clinical outcomes
; clinical trials
; drug discovery
; hit identification
; lead optimization
; pharmaceutical industry
1. Introduction
The traditional drug discovery and development process is an arduous and resource-intensive endeavor. Historically, it takes approximately 10 to 15 years to develop a new therapeutic agent from initial discovery to regulatory approval, with costs often exceeding $1 to $2 billion [1,2,3]. Moreover, the likelihood of a new compound successfully navigating all phases of clinical trials and reaching the market remains dismally low, and estimates suggest that fewer than 1 in 10 drug candidates entering Phase I clinical trials are ultimately approved [4,5]. Key bottlenecks include the inefficient identification of druggable targets, the costly and time-consuming high-throughput screening (HTS) of large chemical libraries, suboptimal lead optimization, and poorly designed clinical trials that fail to stratify patient populations adequately [6]. Artificial Intelligence (AI) has emerged as a disruptive and transformative technology in the pharmaceutical and biomedical industries in recent years. By leveraging massive datasets, advanced algorithms, and high-performance computing, AI tools can uncover patterns and insights that would be nearly impossible for human researchers to detect unaided. These tools have been applied to almost any stage of the drug discovery pipeline, from target identification and validation, hit-to-lead optimization, absorption, distribution, metabolism, excretion, and toxicity (ADMET) profiling, to clinical trial simulation and recruitment strategies [7,8]. Unlike traditional, largely sequential workflows, AI models can parallel process and integrate multi-omics data streams (genomic, proteomic, phenotypic, chemical), potentially compressing the preclinical phase from several years to a few months [9,10].
Several AI-native and AI-integrated biotech firms have already demonstrated tangible progress in reducing timelines and increasing efficiency. Insilico Medicine, a leading AI drug discovery company, announced in 2021 that it successfully identified a novel target for idiopathic pulmonary fibrosis and advanced a drug candidate into preclinical trials in just 18 months (a process that typically takes 4 – 6 years) at a cost of only $150,000, excluding wet lab validation [11]. Similarly, Exscientia, in partnership with Sumitomo Dainippon Pharma, developed a novel small-molecule drug candidate (DSP-1181) for obsessive-compulsive disorder (OCD) in less than 12 months, making it the first AI-designed molecule to enter human clinical trials [12]. Another prominent example, Recursion Pharmaceuticals, uses automated high-throughput imaging combined with deep learning models to identify phenotypic changes in cells, allowing for rapid repurposing of existing molecules and discovering novel therapeutics [13]. Meanwhile, Schrödinger, renowned for its physics-based molecular simulations, integrates AI to predict molecular interactions with high accuracy. This hybrid approach of physics-informed AI is revolutionizing virtual screening by significantly improving hit rates and reducing reliance on exhaustive laboratory testing [14,15]. These pioneering firms are not just proof-of-concept models; they represent a paradigm shift in how drugs are discovered, optimized, and brought to market. Increasing investment from big pharmaceutical companies (e.g., Roche, Bayer, Novartis) into AI collaborations further underscores the seriousness with which the industry views these innovations. Despite these remarkable advances, the extent of AI's measurable impact on key drug development metrics, such as preclinical cycle times, clinical success rates, and regulatory approval efficiencies, remains poorly characterized in the literature. While individual case studies and company press releases highlight success stories, there is a pressing need for a systematic, evidence-based review that consolidates current findings and evaluates the robustness of AI's contributions across different stages of the drug development lifecycle. Furthermore, understanding these AI platforms' scalability, reproducibility, and generalizability is critical for stakeholders, including regulators, investors, and clinical researchers, who are cautiously optimistic but demand empirical validation before widespread adoption.
This systematic review aimed to address the existing knowledge gap by comprehensively analyzing published literature on the application of AI in drug discovery and development. The primary objective was to evaluate how AI influenced the acceleration of drug development timelines, particularly from target identification through preclinical optimization and into clinical trials. The review quantified the impact of AI tools on critical performance metrics such as the reduction of development cycle times, improvements in hit identification and lead optimization, and the readiness for Investigational New Drug (IND) applications. Secondary objectives included assessing the enhancement of pipeline productivity, time-to-IND milestones, and real-world clinical outcomes of drug candidates developed or optimized using AI. Furthermore, the review examined broader industry trends, including licensing agreements, venture capital investments, strategic partnerships, and major pharmaceutical companies' incorporation of AI frameworks. By synthesizing these findings, the review provided meaningful insights into AI’s practical impact on the pharmaceutical industry and offered evidence to guide future research directions, regulatory considerations, and commercial strategies.
2. Results
2.1. Systematic Literature Search and Study Selection Workflow
A systematic literature search was conducted across four major scientific databases to capture a comprehensive set of studies involving AI in drug discovery and development. The initial search phase retrieved a total of 19,465 records. Among these, the highest number of records originated from PubMed (n = 10,055, representing 51.6% of all records), followed by Web of Science (n = 7,217, or 37.1%), SCOPUS (n = 2,129, or 10.9%), and a smaller number from the Cochrane Library (n = 64, or 0.3%) (Figure 1). In addition, six additional records were identified through manual searches and gray literature sources, including four from Google search and two from ClinicalTrials.gov, which together contributed only 0.03% to the total count. After removing duplicates across these sources, 10,348 unique records were retained for further screening, indicating that 46.9% of the initially identified articles were duplicates. These 10,348 records then underwent a title screening phase to evaluate fundamental relevance to the topic. At this stage, 9,060 records (equivalent to 87.6% of the screened titles) were excluded due to being unrelated to AI applications in drug development or lacking relevance to pharmaceutical sciences. The remaining 1,288 records (12.4% of those screened by title) proceeded to the next stage: abstract screening.
A more refined selection process was carried out during the abstract screening phase. Each abstract was reviewed for the use of AI techniques in the context of drug discovery or development and the presence of meaningful scientific or therapeutic contributions. As a result, 975 records (75.7% of abstracts reviewed) were excluded because they did not meet these criteria. The remaining 313 articles (24.3% of abstracts screened; 1.6% of the original dataset) were retained for full-text review. The full-text review phase involved a detailed assessment of the study’s methodology, focus, and outcomes. From these 313 full-text articles, 140 articles (44.7%) were excluded. The reasons for exclusion were systematically categorized as follows: 94 articles (30.0% of full-texts assessed; 67.1% of exclusions) did not utilize adaptive AI methods, such as reinforcement learning, generative adversarial networks, or other self-improving algorithms, which were key inclusion criteria. Twenty-eight articles (8.9% of full-texts; 20.0% of exclusions) were unrelated to drug discovery or development applications. These included AI use in other domains such as medical diagnostics or image analysis, without clear links to pharmaceutical pipelines. Eighteen articles (5.8% of full-texts; 12.9% of exclusions) lacked measurable drug development outcomes, such as predictive performance, lead optimization, or translational results, rendering them insufficiently aligned with the review objectives. Following this rigorous filtering process, 173 studies were deemed eligible and subsequently included in the final scoping review. This constitutes 55.3% of the full-text articles assessed, and only 1.8% of the total records identified at the outset. Despite the relatively small final inclusion rate, this subset of studies provides a focused and high-quality evidence base for analyzing how adaptive AI methods are currently integrated within the pharmaceutical research and development landscape. These selected studies form the basis of the subsequent analysis on methodological trends, therapeutic targets, and measurable impacts of AI in modern drug discovery.
2.2. Distribution of AI Applications Across Drug Development Stages, Geographic Trends, Industry Collaboration, and AI Technology Adoption
A comprehensive analysis of the 173 included studies reveals valuable insights into how AI is applied throughout various stages of drug development, its geographic distribution, the degree of industry partnership, translational impact, and the spectrum of AI methodologies employed. Figure 2A provides a comprehensive overview of the distribution of AI applications across various stages of drug development, with an intense concentration in the early phases of the drug discovery pipeline. The preclinical stage remains the most active, with 68 out of 173 studies (39.3%) focused at this level. This highlights AI's integral role in the foundational aspects of drug research, including target identification, virtual screening, de novo molecule generation, molecular docking, quantitative structure–activity relationship (QSAR) modeling, and ADMET prediction. The dominance of preclinical AI applications underscores its transformative potential in accelerating early-stage discovery and optimizing lead compounds before entering human trials. Next, 19 studies (11.0%) were positioned in the transitional phase between preclinical and Clinical Phase I, often associated with IND (Investigational New Drug) enabling activities. At this stage, AI is applied in predictive toxicology, in silico dose selection, early biomarker discovery, and simulation of pharmacokinetic parameters, contributing to safer and more informed transitions into human testing.
The Clinical Phase I stage showed a significant increase in AI integration, with 40 studies (23.1%), indicating growing confidence in AI tools for safety profiling, pharmacokinetics modeling, and real-time monitoring during early human exposure. These tools assist in optimizing dosage regimens and reducing early-phase attrition by predicting adverse events and guiding early clinical decisions. Five studies (2.9%) were conducted at the Clinical Phase I/Ib level and 17 studies (9.8%) at the Phase I/II level in the hybrid early clinical stages. These phases typically involve dose expansion and initial efficacy assessments, where AI supports patient stratification, digital biomarker identification, and adaptive trial designs. Moving into Clinical Phase Ib/II and Phase IIa, the number of AI-based studies declines, with 2 (1.2%) and 16 (9.2%) studies, respectively. These phases often focus on proof-of-concept evaluation, and AI is leveraged here to analyze multidimensional patient data, integrate omics datasets, and assist in go/no-go decisions. Despite the complexity of these phases, the use of AI remains underutilized. The later stages of development show the lowest AI engagement: Clinical Phase IIb with five studies (2.9%) and Clinical Phase II/III with just two studies (0.6%). These phases are centered on dose optimization, large-scale efficacy, and comparative effectiveness trials, where high regulatory standards, data integrity demands, and the need for explainability and validation of AI models limit the application of AI.
Figure 2B illustrates the global geographic distribution of AI-based drug discovery studies, revealing a highly skewed landscape dominated by a few technologically advanced nations. The United States stands at the forefront, contributing 129 out of 179 studies (72.1%), underscoring its leading role in the convergence of AI and pharmaceutical innovation. This dominance is attributed to multiple factors, including robust federal and private sector investment in biotechnology, an extensive network of academic and industry collaborations, high-performance computing infrastructure, and an entrepreneurial ecosystem that fosters the rapid development and deployment of AI platforms in drug discovery. In a distant second, China contributed 16 studies (8.9%), reflecting its rapidly expanding capabilities in AI and pharmaceutical research and development (R&D). China's significant government support for AI innovation, coupled with its growing pharmaceutical market and increasing academic output in computational biology, signals strong momentum in this space. The United Kingdom accounted for nine studies (5.0%), indicative of its established strength in biomedical research, AI innovation hubs in Cambridge, London, and Oxford, and a regulatory environment that supports digital health technologies. Other contributors include South Korea (6 studies; 3.4%), Denmark (6 studies; 3.4%), and Japan (6 studies; 3.4%). These countries possess strong healthcare systems, government-sponsored AI initiatives, and active collaborations between academic and pharmaceutical sectors. Their participation reflects growing regional investment in AI-assisted drug development, albeit at a more modest scale compared to the US. More minor but notable contributions were seen from Singapore (3 studies; 1.7%), Spain (2 studies; 1.1%), Canada (1 study; 0.6%), and Australia (1 study; 0.6%). These nations are increasingly integrating AI into biomedical research but may face challenges related to scale, funding, or data accessibility that limit broader adoption. Notably, regions such as Africa, South America, and large parts of Southeast Asia were absent from the dataset, highlighting a significant global disparity in adopting and implementing AI technologies in drug discovery. This absence underscores the need for capacity-building initiatives, enhanced international collaborations, and knowledge-sharing frameworks that can democratize access to AI resources and training.
Figure 2C provides a comprehensive assessment of the translational maturity of AI-driven drug discovery studies, focusing on three critical indicators: timeline impact, clinical outcome reporting, and industry partnership. Remarkably, all 173 studies (100%) demonstrated some form of timeline impact, signifying that AI integration consistently contributes to accelerating various stages of the drug development pipeline. This universal influence highlights AI’s role in enhancing research efficiency, expediting compound selection, and shortening time-to-decision in early-stage drug discovery. A prominent example is Insilico Medicine's AI-designed drug candidate INS018_055, a small molecule targeting idiopathic pulmonary fibrosis (IPF) [16]. Developed using their proprietary AI platform, this compound progressed from target identification to a preclinical candidate in under 18 months, a process that traditionally takes several years. As of recent updates, INS018_055 has entered Phase II clinical trials, underscoring how AI can dramatically compress timelines and bridge computational discovery with clinical translation. However, when examining clinical outcome reporting, the data reveals a significant drop-off in translational depth. Only 77 studies (45%) reported measurable clinical outcomes, such as pharmacokinetic parameters, safety profiles, or preliminary efficacy indicators. The majority of 96 studies (55%) did not report any clinical outcomes, suggesting that many AI applications remain confined to preclinical or in silico stages, where direct clinical relevance is either unexplored or not yet achieved. This imbalance highlights a key bottleneck in validating AI-derived insights within real-world clinical contexts. Furthermore, formal industry partnerships were surprisingly high, with 168 studies (97%) reporting collaboration with industry stakeholders. This finding contrasts with prior expectations and suggests that AI in drug discovery is increasingly seen as a strategic asset by pharmaceutical and biotech companies. These partnerships likely facilitate access to proprietary datasets, advanced computational tools, and regulatory expertise, which can enhance AI solutions' real-world applicability and scalability.
Industry-wide, licensing agreements and strategic collaborations have become primary conduits for integrating AI into mainstream pipelines. For instance, Sanofi entered into a $1.2 billion partnership with Exscientia to use AI to discover novel oncology and immunology therapies [17]. Similarly, AstraZeneca has formed long-term collaborations with BenevolentAI, embedding AI platforms directly into its discovery engine [18]. These high-value deals validate the commercial potential of AI-driven discovery and position pharmaceutical companies to leverage AI across multiple therapeutic areas. From a funding perspective, the sector is also witnessing substantial venture capital investment. In 2023 alone, AI-driven biotech startups raised over $4.5 billion globally, with major recipients including Recursion Pharmaceuticals, XtalPi, and Insilico Medicine. Recursion, in particular, has established an expansive AI-first infrastructure integrating single-cell analysis, phenotypic imaging, and multi-modal data fusion, attracting public market interest (IPO in 2021) and private capital from major players such as SoftBank [19]. Big Pharma continues to gain momentum in the incorporation of AI frameworks. Pfizer, Merck, Roche, and Novartis have each developed or partnered on bespoke AI initiatives. Pfizer, for example, uses IBM Watson and other internal models for clinical trial optimization and target prediction [20]. Roche acquired Flatiron Health and Foundation Medicine to strengthen its data analytics and real-world evidence platforms, reinforcing AI's role in personalized oncology [21]. Meanwhile, Novartis has embedded AI into its Novartis AI Innovation Lab, leveraging partnerships with Microsoft to create scalable machine learning frameworks for drug discovery and development [22].
Figure 2D provides an in-depth overview of the diverse AI techniques employed across drug discovery studies, revealing a dynamic and evolving technological landscape. Machine Learning (ML) remains the most dominant technique, featured in 170 studies (40.9%), representing a significant proportion of the total. Its prevalence reflects ML’s broad utility in tasks such as predictive modeling, compound prioritization, toxicity forecasting, and high-dimensional data interpretation. ML’s adaptability and scalability make it a cornerstone of AI-enabled drug discovery platforms [23]. Molecular Modeling and Simulation (MMS) was the second most frequently applied method in 86 studies (20.7%). MMS techniques, such as molecular docking, molecular dynamics simulations, and free energy perturbation, are fundamental to structure-based drug design and offer mechanistic insights that complement data-driven approaches [24,25,26]. Deep Learning (DL), used in 43 studies (10.3%), underscores the growing reliance on complex neural networks for handling unstructured data such as molecular images, protein structures, and compound libraries. DL techniques are particularly advantageous in modeling nonlinear relationships and developing end-to-end learning frameworks, including convolutional and graph neural networks that power many modern cheminformatics and bioinformatics pipelines [27,28]. Omics Integration (OM) was observed in 27 studies, reflecting the increasing emphasis on multi-omics data (genomics, proteomics, metabolomics) for systems-level understanding of disease mechanisms and drug response. Generative Models (GM) appeared in 25 studies, illustrating the rising interest in de novo molecular generation. These models, which include variational autoencoders (VAEs), generative adversarial networks (GANs), and transformer-based frameworks, are instrumental in creating novel chemical entities with optimized pharmacokinetic and pharmacodynamic profiles [29,30]. Their use highlights the shift toward AI systems capable not only of prediction but also of creativity.
Structure-Based Drug Design (SBDD) techniques were used in 21 studies, emphasizing their role in rational drug design informed by high-resolution structural data. SBDD often integrates docking, pharmacophore modeling, and homology modeling, which, combined with AI tools, accelerate the discovery of structure-activity relationships [31,32]. Physics-Based Modeling (PBM) was utilized in 17 studies, combining AI with traditional biophysical simulations to capture atomic-level interactions and predict binding affinities with higher precision. Reinforcement Learning (RL) was employed in 12 studies, gradually adopting this powerful paradigm for optimizing compound synthesis paths, multi-objective design, and adaptive trial strategies. RL’s ability to learn optimal policies from sequential decisions makes it especially suitable for iterative drug design workflows [33,34]. Computer Vision (CV) techniques, found in six studies, were mainly applied in analyzing histopathological images, high-throughput screening outputs, and chemical structure recognition [35]. Despite being a relatively underutilized method, CV has strong potential in visual data processing across drug discovery and diagnostics. Knowledge Graphs (KG) were used in 5 studies, facilitating the integration of heterogeneous biomedical data into relational frameworks. KGs enable AI systems to infer novel relationships, such as drug-disease or gene-compound links, supporting hypothesis generation and drug repurposing [36,37]. Natural Language Processing (NLP) appeared in 4 studies, primarily focused on mining scientific literature, clinical trial records, and patents for actionable insights [38,39]. NLP tools are pivotal in automating knowledge extraction and transforming unstructured text into structured datasets for AI models.
Figure 3 highlights the diversity and technological sophistication of leading AI drug discovery platforms by illustrating the number and types of AI techniques integrated into each. Each bar represents a prominent platform developed by a pharmaceutical or AI-driven biotech company, and the colored segments within each bar denote the variety of AI approaches implemented. This comparative analysis offers a bird’s-eye view of innovation trends and technological focus areas within the AI-biopharma ecosystem. Chemistry42, developed by Insilico Medicine, is unique in its integration of generative AI, deep learning, and reinforcement learning, three core AI methods that enable the platform to autonomously design novel chemical structures and optimize them for drug-like properties. This configuration supports an end-to-end generative chemistry pipeline, where molecules are created and refined iteratively through reinforcement learning. Despite lacking support from big data analytics or structural biology integration, Chemistry42 focuses squarely on de novo molecular generation, making it a powerful tool for early-stage drug discovery [40]. Unigen™, from Compugen, stands out for its singular focus on predictive machine learning. Though it does not yet integrate other AI techniques, this focus enables it to excel in structure prediction, synthesis planning, and molecular property forecasting. Such a streamlined approach highlights how a targeted use of AI can still deliver substantial value in drug discovery, especially when paired with quantum physics principles. RADR® AI, the platform developed by Lantern Pharma, represents a different approach. It uses ensemble machine learning and big data analytics, reflecting its strong orientation toward biomarker discovery, drug repurposing, and precision oncology [41]. RADR® doesn’t create new molecules but leverages existing compounds and vast multi-omics datasets to identify high-probability therapeutic matches, showing how AI can facilitate drug repositioning and personalized therapy development. Meanwhile, Schrödinger’s platform integrates predictive ML and physics-based modeling, reinforcing its role as a leader in structure-guided drug design. By simulating molecular interactions at the atomic level and predicting binding affinities, Schrödinger achieves high accuracy in lead optimization and virtual screening campaigns. Incorporating physics-based modeling is especially valuable in ensuring that AI predictions are grounded in physical and chemical reality, giving researchers more confidence in silico results.
Dynamo™, by Relay Therapeutics, combines predictive machine learning, motion simulation, and structural biology, supporting a synthesis-aware drug design environment. By predicting synthetic accessibility and integrating structural data, Dynamo™ helps chemists prioritize compounds that are biologically relevant and synthetically feasible. Platforms like HiFiBiO’s DIS™ and Flex-NK™ showcase the specialized application of AI in immunotherapy and cell-based therapies. HiFiBiO focuses on single-cell analysis and predictive ML, enabling the discovery of immune targets at a granular resolution, which is ideal for antibody and T-cell engineering. Flex-NK™, on the other hand, leverages deep learning, predictive ML, and single-cell analysis to optimize NK-cell-based cancer therapies, highlighting the growing role of AI in cellular and gene therapy design. Recursion OS leads the field regarding AI technique integration, employing six out of ten tracked AI approaches: generative AI, deep learning, predictive ML, big data analytics, structural biology, and single-cell analysis. This diversity reflects Recursion’s commitment to large-scale phenotypic screening and multi-modal data fusion. The platform analyzes vast amounts of image-based cellular data and integrates it with molecular insights to drive target discovery and drug repurposing. TITAN-X, developed by NIMML Institute, and SmartCube®, from PsychoGenics, each implement three primary AI techniques with different orientations. TITAN-X emphasizes protein engineering, using predictive ML, big data analytics, and structural biology to evolve novel proteins for therapeutic or industrial use. SmartCube®, in contrast, incorporates motion simulation, predictive ML, and big data analytics to study behavioral phenotypes, particularly in neuropsychiatric disorders, a niche application of AI that blends behavioral science with drug discovery [42]. Lastly, PIONEER™ by Evaxion Biotech showcases a compact but impactful setup with generative AI and deep learning, aligning with Evaxion Biotech’s mission to build human-centric drug development platforms [43]. It uses digital twin technology and AI to enhance translational research, especially in areas where patient variability significantly affects outcomes.
2.3. Landscape of AI Applications in Pharmaceutical R&D: Trends and Case Studies
Over the past decade (2015–2025), the pharmaceutical industry has witnessed a transformative integration of AI across drug discovery and development pipelines. Table 1 provides a comprehensive overview of AI-enabled innovations deployed across various therapeutic domains, ranging from oncology and gastroenterology to infectious diseases and immunology. Oncology emerges as the most prominent therapeutic area leveraging AI tools. Multiple case studies from biotech firms like A2A Pharmaceuticals, Accutar Biotechnology, Black Diamond Therapeutics, Compugen, and Evaxion Biotech highlight the versatile use of AI in structure-based drug design, epitope prediction, predictive modeling, and virtual screening. For instance, a study utilizes structure-based drug design combined with virtual screening and ADMET predictions to target triple-negative breast cancer (TNBC), high-grade serous ovarian cancer (HGSOC), and endometrial cancer with TP53 mutations [44]. Similarly, another study employed AI platforms such as ChemiRise and Chemi-Net to optimize the pharmacokinetics/pharmacodynamics (PK/PD) of potential drugs for ER+/HER2- breast cancer [45]. The consistent clinical advancement into Phase I and II trials underscores AI’s clinical promise in oncologic settings. Beyond target identification, AI is also used for combination therapy modeling and antibody design. Platforms like Unigen™, NovareAI, and Flex-NK™ integrate machine learning with omics data and spatial transcriptomics to identify novel therapeutic strategies. Exscientia and Evotec, for instance, utilize generative design models and simulation-guided clinical trial planning, marking a shift from empirical to computationally guided therapeutic development.
While oncology dominates, AI’s impact extends to a broad spectrum of other therapeutic areas. In gastroenterology, Celsius Therapeutics and Landos Biopharma use platforms like SCOPE and TITAN-X for single-cell RNA-seq analysis, predictive analytics, and disease stratification in conditions like ulcerative colitis and Crohn’s disease. In infectious diseases, Generate Biomedicines applied iterative ML-based chemoproteomic loops for COVID-19 prophylaxis, while Drug Farm's IDInVivo platform enabled in vivo gene targeting for Hepatitis B. In neurology and immunology, platforms such as Magellan™ (Gain Therapeutics) and DeepCure’s AI-driven compound design system illustrate how AI is pushing the frontier of precision medicine. In rheumatology, Formation Bio used AI to automate MRI segmentation and analyze cartilage degradation in osteoarthritis. Such examples show how AI is revolutionizing both molecular-level innovations and system-level clinical decision-making processes. The diversity of AI techniques employed across these case studies reflects the maturity and versatility of the field. Methods range from knowledge graphs and Bayesian modeling to convolutional neural networks and reinforcement learning. For example, a study leveraged knowledge graphs for target prioritization in ulcerative colitis [48], while another study used generative AI and reinforcement learning for chemical space exploration in rheumatoid arthritis [57]. Integration with supercomputing resources, as seen in BERG’s use of the Oak Ridge supercomputer, and the construction of AI-driven lipid nanoparticle optimization (AiLNP) platforms by METiS Pharmaceuticals, exemplify cross-disciplinary innovation between AI, physics, and pharmaceutical sciences.
Figure 4 comprehensively depicts the current focus and molecular strategies of AI-driven drug discovery initiatives. Figure 4A reveals a significant concentration of AI applications in oncology, which accounts for 126 studies (72.83%), far surpassing all other therapeutic areas. This outsized focus reflects the urgent unmet needs in cancer treatment and the availability of robust datasets in oncology, which are essential for training and validating AI models. The nature of cancer, characterized by genomic complexity and high inter-patient variability, makes it a fertile ground for AI applications that can sift through large-scale omics data, identify novel biomarkers, and propose tailored therapeutic strategies. Furthermore, oncology's historically high rate of drug development investment likely incentivizes AI startups and pharmaceutical companies to focus on this domain, where the return on innovation can be particularly high. Beyond oncology, the distribution of studies across other disease areas shows a sharp drop. Dermatology ranks second with only 10 studies (5.78%), followed by gastroenterology and neurology with nine studies each (5.20%). These numbers indicate a nascent expansion of AI efforts into non-cancer areas, though the pace remains cautious. Dermatology, for example, benefits from the abundance of image-based data, which aligns well with AI tools such as convolutional neural networks. Neurology and gastroenterology, despite being rich in research potential, pose unique challenges such as limited biomarker availability and the complexity of brain–gut interactions, which might explain their relatively modest representation. Immunology accounts for seven studies (4.05%) and infectious diseases for five studies (2.89%), which gradually incorporate AI, particularly in areas like immune profiling, vaccine design, and antibiotic resistance prediction. Meanwhile, pulmonary and endocrinology have three studies each (1.73%), and rheumatology is the least represented with only 1 study (0.58%), underscoring their current underrepresentation, possibly due to insufficient data infrastructure or less immediate commercial incentive.
Figure 4B complements this therapeutic overview with a flower plot that maps the molecular targets pursued by leading AI-powered drug discovery companies. This visualization illustrates how AI is being used to expand therapeutic areas and diversify molecular strategies. The flower's petals are divided among six prominent AI-driven biopharmaceutical firms: Insilico Medicine, Compugen, Schrödinger, Lantern Pharma, HiFiBiO Therapeutics, and Relay Therapeutics. Each sector's molecular targets are placed according to their development phase, ranging from preclinical (light blue) to clinical phases I through III (in increasingly darker shades of blue). Notably, specific targets such as PD-1, PD-L1, TYK2, and EGFR appear in multiple petals, signaling their importance across company pipelines and suggesting convergence on high-value targets in immuno-oncology and precision medicine. The recurrence of targets like PD-1 and PD-L1, central to immune checkpoint inhibition therapies, indicates that AI is used to identify new molecules and optimize well-known mechanisms of action. Their widespread inclusion across companies and development stages signals intense competition and the strategic prioritization of validated but improvable pathways. Similarly, TYK2 and EGFR represent attractive targets with known therapeutic relevance in autoimmune and oncologic conditions [95,96], further reinforcing that AI enhances and accelerates drug discovery within proven biological frameworks. Additionally, more specialized or emerging targets, such as pan-TEAD, CDC7, and MALT1, demonstrate that AI is also facilitating novel hypothesis generation and target validation, which may yield first-in-class therapies.
3. Discussion
3.1. Main Findings and Comparison with Prior Works
This systematic review presents a comprehensive landscape of how AI is applied in the drug discovery and development (DDD) pipeline. The main findings reveal that AI adoption is predominantly concentrated in the early stages of drug discovery, specifically in target identification, validation, and compound screening, with a gradual extension into preclinical and early clinical development. Oncology emerges as the principal therapeutic area of AI activity, representing nearly 73% of identified studies, followed by dermatology, gastroenterology, and neurology. This distribution highlights a strategic focus by AI developers and pharmaceutical companies on high-burden, data-rich therapeutic domains. Additionally, AI technologies such as ML, DL, NLP, and reinforcement learning were frequently reported, each employed according to task-specific requirements, such as image analysis, biomarker discovery, structure-based drug design, and patient stratification. This study aligns with and extends the existing body of knowledge compared to prior reviews in this domain. For instance, several findings highlighted the growing role of ML algorithms in streamlining target discovery and virtual screening [97,98,99]. However, these earlier reviews primarily focused on the promise of AI technologies, emphasizing algorithmic performance and proof-of-concept studies. In contrast, the present review integrates real-world implementation trends, industry partnerships, and clinical translation efforts, thereby offering a more grounded assessment of AI’s practical impact across the pharmaceutical value chain. Additionally, by disaggregating findings by disease area, development phase, and molecular strategy, this review reveals specific bottlenecks in underrepresented domains (e.g., rheumatology and endocrinology), which prior works only mentioned anecdotally.
One unique aspect of this review is its granular mapping of AI-driven pipelines at the company level, particularly through visualizations like the flower plot of molecular targets. This approach offers novel insights into how leading AI-powered biopharmaceutical firms prioritize molecular targets such as PD-1, PD-L1, EGFR, and TYK2, and how these targets are being pursued across different stages of development. While previous reviews acknowledged the theoretical ability of AI to identify novel targets, they rarely tracked how these insights translated into pipeline activities or advanced to clinical trials [100]. Identifying first-in-class targets (e.g., CDC7, pan-TEAD, and MALT1) further underscores AI's growing role in hypothesis generation and mechanistic innovation, an aspect only sparsely covered in older literature. Moreover, this review distinguishes itself by explicitly analyzing global trends in AI-related research output, highlighting geographic disparities in AI adoption and institutional investment. The dominance of studies from the United States, China, and select European countries reflects a concentration of technical and financial resources, which may perpetuate regional inequalities in AI access and infrastructure.
3.2. Limitations and Future Works
While this systematic review provides a comprehensive overview of AI applications in drug discovery, several limitations must be addressed. One limitation is the strict inclusion and exclusion criteria, which may have excluded valuable studies, particularly those indirectly discussing AI in drug discovery. The scope of therapeutic areas analyzed is another limitation, with oncology receiving disproportionate attention, potentially overlooking emerging uses of AI in other fields such as dermatology, immunology, and gastroenterology. Additionally, the geographic distribution of studies, predominantly from North America, Europe, and East Asia, may not fully represent global trends, and the review's temporal focus may have missed earlier foundational work. Furthermore, while the review addresses AI's application across various stages of drug discovery, it lacks a detailed discussion on the regulatory challenges and clinical translation of AI technologies, which are critical to understanding their real-world impact.
Future work in systematic reviews could benefit from expanding the scope to include a broader range of therapeutic areas, more diverse geographic sources, and more extended temporal periods. Additionally, incorporating a wider range of metrics for assessing success, such as cost-effectiveness, real-world clinical efficacy, and post-market surveillance, would provide a more nuanced understanding of AI’s value in drug development. Future reviews could also explore AI's effectiveness in predicting drug-drug interactions and real-world clinical outcomes, essential for evaluating AI’s full potential in therapeutic development. Considering diverse AI techniques, regulatory considerations, and clinical trial outcomes, a more inclusive approach would offer a more comprehensive perspective on AI’s transformative role in drug discovery.
4. Materials and Methods
4.1. Eligibility Criteria
This systematic review focused on identifying and analyzing scholarly and professional works that reflect the real-world application and downstream impact of AI in drug discovery and development. To ensure the relevance and rigor of the selected literature, only studies and reports demonstrating meaningful contributions to the AI-driven drug development pipeline were considered. Specifically, the review encompassed original research articles, comprehensive reviews, white papers, and technical or industry reports that detailed the use of AI in advancing one or more stages of the drug discovery process. These stages included, but were not limited to, target identification, compound screening, hit-to-lead optimization, and the progression of candidates into preclinical studies and clinical trials. Documents were prioritized if they described tangible outputs from AI-driven pipelines, such as successful candidate nominations, IND filings, or the initiation of clinical trials. Emphasis was placed on works that provided evidence of accelerated timelines, improved molecular profiling, or enhanced pipeline productivity resulting from AI integration. Conversely, studies were not considered if they focused solely on computational or algorithmic model development without any application to real-world pharmaceutical pipelines. Likewise, literature discussing AI applications in areas unrelated to the core drug discovery lifecycle, such as marketing, supply chain logistics, sales analytics, or pharmacovigilance, was excluded from consideration. This delineation ensured that the review remained centered on evaluating AI’s tangible contributions to therapeutic innovation, translational science, and clinical readiness.
4.2. Information Sources
Multiple information sources were systematically searched to ensure a comprehensive and representative collection of relevant literature. The primary bibliographic databases consulted included PubMed, Web of Science, Scopus, and Cochrane Library. These platforms were selected due to their extensive indexing of peer-reviewed journals and conference proceedings across the domains of biomedical sciences, pharmaceutical innovation, artificial intelligence, and computational modeling. They offered broad and complementary coverage of academic research and industry-driven applications. In addition to scientific databases, the clinical trials registry ClinicalTrials.gov was queried to identify records of ongoing or completed trials involving AI-assisted drug development. This source provided insights into the translational impact of AI on candidate advancement and regulatory readiness, particularly those that have reached investigational or therapeutic stages.
4.3. Search Strategy
A comprehensive search strategy was developed to capture literature at the intersection of AI and drug discovery and development. This strategy combined free-text keywords and controlled vocabularies, including MeSH terms in PubMed, to ensure broad and precise retrieval of relevant studies. The search queries were constructed around five core conceptual domains: (1) AI technologies (e.g., "artificial intelligence," "machine learning," "deep learning," "neural networks"); (2) Drug discovery and development stages (e.g., "target identification," "compound screening," "preclinical development," "clinical trials"); (3) Outcomes and impact metrics (e.g., "timeline reduction," "pipeline productivity," "time-to-IND," "regulatory approval"); (4) Industry and commercial adoption (e.g., "pharmaceutical industry," "venture capital," "strategic partnerships," "AI integration"); and (5) AI-based pharmaceutical and biotechnology companies (e.g., "Insilico Medicine," "BenevolentAI," "Exscientia," "Recursion Pharmaceuticals," "Relay Therapeutics," "Generate Biomedicines," among others). Boolean operators (AND/OR) were used to link these concepts effectively, and advanced syntax such as truncation and phrase searching was applied to optimize term variation capture. A representative query included terms such as: ("artificial intelligence" OR "machine learning") AND ("drug discovery" OR "drug development") AND ("timeline reduction" OR "pipeline performance") AND ("pharmaceutical industry" OR "venture capital") AND ("Insilico Medicine" OR "BenevolentAI" OR "Exscientia").
Searches were executed across multiple bibliographic databases, including PubMed, Web of Science, Scopus, and the Cochrane Library. To supplement peer-reviewed sources, grey literature was identified through targeted searches in Google Scholar and manual retrieval of documents recommended by domain experts. Additionally, ClinicalTrials.gov was searched to identify ongoing or completed trials involving AI-developed drug candidates. Only English-language publications were considered. To enhance transparency and reproducibility, the complete search strategy, including specific database queries and applied search filters, is provided in Supplementary Data S2.
4.4. Study Selection
The study selection process was conducted using a two-phase approach designed to rigorously identify publications relevant to the application of AI in drug discovery and development. In the first phase, two independent reviewers screened the titles and abstracts of all retrieved records. This initial screening was guided by a predefined set of criteria, focusing on the relevance of AI methods to drug development pipelines and the presence of tangible outcomes. Records that clearly did not meet the criteria were excluded at this stage, while those deemed potentially relevant were moved to the next phase. During the second phase, full-text articles were reviewed in detail by the same two reviewers to assess their eligibility. This phase involved careful evaluation of the AI methodology employed, the specific application stage within the drug discovery pipeline, and the outcome measures reported. Studies that did not provide concrete results, such as candidate identification, IND filing, or progression into clinical trials, were excluded. Similarly, studies that applied AI to areas unrelated to drug discovery (e.g., diagnostic imaging, electronic health record analysis, or marketing) were also excluded. Discrepancies between reviewers were addressed through structured discussion; in cases where consensus could not be reached, a third reviewer provided arbitration to ensure objectivity. The selection workflow followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [101,102] to enhance methodological transparency and reproducibility. The PRISMA checklist can be seen in Supplementary Data S3. Additionally, Table 2 summarizes the detailed criteria used to guide study inclusion and exclusion, which were aligned with the review’s objective of assessing AI's impact on accelerating drug development timelines and improving productivity metrics across preclinical and clinical stages.
4.5. Data Extraction
A standardized data extraction form was meticulously developed and pilot-tested prior to formal data collection to ensure consistency and accuracy in capturing relevant information. The form encompassed a comprehensive set of variables, including bibliographic details (publication year, authors, journal, database), methodological features (study type, AI technique applied), and contextual information (drug discovery stage targeted, therapeutic area, geographic origin). Additionally, outcomes of interest were systematically recorded, such as key performance indicators (e.g., time-to-IND reduction, development timeline acceleration, clinical success rates), commercial outcomes (e.g., funding mechanisms, industry partnerships, licensing agreements), and any reported limitations. Two reviewers independently reviewed each article to minimize bias and discrepancies during data extraction. Any discrepancies were resolved through discussion and consensus between the reviewers. The data extraction framework also included binary indicators (Yes/No) for key metrics such as whether the study demonstrated timeline impact, reported clinical outcomes, or involved industry collaboration. This detailed approach allowed for systematically comparing AI applications across various stages of drug development and therapeutic areas.
4.6. Data Synthesis and Interpretations
The extracted data were synthesized using a qualitative narrative approach complemented by descriptive statistics. Studies were grouped based on the type of AI technique employed (e.g., deep learning, reinforcement learning, machine learning), the stage of drug development targeted (e.g., target identification, lead optimization, preclinical or clinical phases), and the therapeutic area (e.g., oncology, neurology, infectious diseases). Frequency counts and proportions were used to summarize categorical variables such as AI method usage, therapeutic focus, and geographic origin. Key performance indicators, such as time-to-IND reduction, success rates, and commercial outcomes, were compared across studies to identify trends and outliers. Studies reporting similar metrics were narratively compared to highlight the magnitude of AI-driven impact on drug development efficiency and productivity. Where available, industry partnerships, external funding, and licensing agreements were also examined to assess real-world translational potential. Findings were interpreted in the context of methodological quality, generalizability, and limitations noted within the included studies. This synthesis enabled a multi-dimensional understanding of how AI technologies reshape modern drug discovery pipelines across research and commercial domains.
5. Conclusions
This systematic review demonstrates that artificial intelligence is rapidly reshaping the drug discovery and development landscape by streamlining early-stage research, improving target identification, and enhancing decision-making across clinical phases. AI technologies, particularly machine learning, molecular modeling, and deep learning, are instrumental in accelerating compound selection, optimizing lead candidates, and supporting personalized therapeutic strategies. The field strongly emphasizes oncology due to data availability and commercial viability, though AI applications are gradually expanding into other therapeutic areas. A significant translational gap remains, as many studies have yet to report clinical outcomes, highlighting the need for deeper clinical integration and validation of AI-derived insights. Nevertheless, the high prevalence of industry collaborations underscores growing confidence in AI as a strategic tool for pharmaceutical innovation. The findings suggest that AI is transitioning from experimental utility to a core component of modern drug development pipelines, with future efforts needed to improve data interoperability, model interpretability, and broader application in underrepresented disease domains.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Supplementary Data S1: Dataset of included studies; Supplementary Data S2: Full search strategy; Supplementary Data S3: PRISMA checklist.
Author Contributions
Conceptualization, Nasser Alotaiq and Doni Dermawan; Data curation, Nasser Alotaiq; Formal analysis, Doni Dermawan; Funding acquisition, Nasser Alotaiq; Investigation, Doni Dermawan; Methodology, Nasser Alotaiq and Doni Dermawan; Project administration, Nasser Alotaiq; Resources, Nasser Alotaiq; Software, Doni Dermawan; Supervision, Nasser Alotaiq; Validation, Nasser Alotaiq and Doni Dermawan; Visualization, Doni Dermawan; Writing – original draft, Nasser Alotaiq and Doni Dermawan; Writing – review & editing, Nasser Alotaiq and Doni Dermawan.
Funding
This work was supported and funded by the Deanship of Scientific Research at Imam Mohammad Ibn Saud Islamic University (IMSIU) (grant number IMSIU-DDRSP2501).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author(s).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ADMET | Absorption, distribution, metabolism, excretion, and toxicity |
| AI | Artificial intelligence |
| AML | Acute myeloid leukemia |
| CV | Computer vision |
| DDD | Drug discovery and development |
| DL | Deep learning |
| GM | Generative model |
| HGSOC | High-grade serous ovarian cancer |
| HTS | High-throughput screening |
| IBD | Inflammatory bowel disease |
| IND | Investigational new drug |
| IPF | Idiopathic pulmonary fibrosis |
| KG | Knowledge graph |
| ML | Machine learning |
| MMS | Molecular modeling and simulation |
| NLP | Natural language processing |
| NSCLC | Non-small cell lung cancer |
| OCD | Obsessive-compulsive disorder |
| OM | Omics integration |
| PBM | Physics-based modeling |
| PK/PD | Pharmacokinetics/pharmacodynamics |
| PRISMA | Preferred reporting items for systematic reviews and meta-analyses |
| QSAR | Quantitative structure–activity relationship |
| R&D | Research and development |
| RL | Reinforcement learning |
| SBDD | Structure-based drug design |
| SLE | Systemic lupus erythematosus |
| TNBC | Triple-negative breast cancer |
References
- Paul, S.M. , et al., How to improve R&D productivity: the pharmaceutical industry's grand challenge. Nature Reviews Drug Discovery, 2010. 9(3): p. 203-214.
- DiMasi, J.A. H.G. Grabowski, and R.W. Hansen, Innovation in the pharmaceutical industry: New estimates of R&D costs. J Health Econ, 2016. 47: p. 20-33.
- Berdigaliyev, N. and M. Aljofan, An overview of drug discovery and development. Future Med Chem, 2020. 12(10): p. 939-947.
- Hay, M. , et al., Clinical development success rates for investigational drugs. Nat Biotechnol, 2014. 32(1): p. 40-51.
- Wong, C.H. K.W. Siah, and A.W. Lo, Estimation of clinical trial success rates and related parameters. Biostatistics, 2019. 20(2): p. 273-286.
- Scannell, J.W. , et al., Diagnosing the decline in pharmaceutical R&D efficiency. Nat Rev Drug Discov, 2012. 11(3): p. 191-200.
- Mak, K.K. and M.R. Pichika, Artificial intelligence in drug development: present status and future prospects. Drug Discov Today, 2019. 24(3): p. 773-780.
- Ekins, S. , et al., Exploiting machine learning for end-to-end drug discovery and development. Nat Mater, 2019. 18(5): p. 435-441.
- Wu, Y. and L. Xie, AI-driven multi-omics integration for multi-scale predictive modeling of genotype-environment-phenotype relationships. Comput Struct Biotechnol J, 2025. 27: p. 265-277.
- Vamathevan, J. , et al., Applications of machine learning in drug discovery and development. Nat Rev Drug Discov, 2019. 18(6): p. 463-477.
- Zhavoronkov, A. From Start to Phase 1 in 30 Months: AI-discovered and AI-designed Anti-fibrotic Drug Enters Phase I Clinical Trial. 2022 [cited 2025 10 March]; Available from: https://insilico.com/phase1.
- Burki, T. , A new paradigm for drug development. Lancet Digit Health, 2020. 2(5): p. e226-e227.
- Serrano, D.R. , et al., Artificial Intelligence (AI) Applications in Drug Discovery and Drug Delivery: Revolutionizing Personalized Medicine. Pharmaceutics, 2024. 16(10).
- Andy, A. and C. James, Hybrid Physics-AI Approaches for Protein-Ligand Docking and Scoring. 2025.
- Niazi, S.K. and Z. Mariam, Computer-Aided Drug Design and Drug Discovery: A Prospective Analysis. Pharmaceuticals (Basel), 2023. 17(1).
- Ren, F. , et al., A small-molecule TNIK inhibitor targets fibrosis in preclinical and clinical models. Nat Biotechnol, 2025. 43(1): p. 63-75.
- Waldron, J. Sanofi signs $1.2B pact with Atomwise in latest high-value AI drug discovery deal. 2022 [cited 2025 15th April]; Available from: https://www.fiercebiotech.com/biotech/sanofi-signs-12b-pact-atomwise-latest-high-value-ai-drug-discovery-deal.
- AstraZeneca. AstraZeneca starts artificial intelligence collaboration to accelerate drug discovery, /: 2025 15th April]; Available from: https, 2025.
- Al-Idrus, A. AI drug prospector Recursion bumps IPO up (again) to $374M. 2021 [cited 2025 15th April]; Available from: https://www.fiercebiotech.com/biotech/ai-drug-prospector-recursion-bumps-ipo-up-again-to-374m.
- Robinson, R. The Uptick in AI Use Will Bring Pharma Into the Future Faster. 2019 [cited 2025 15th April]; Available from: https://www.pharmavoice.com/news/2019-11-ai/612372/.
- Roche. Roche to acquire Flatiron Health to accelerate industry-wide development and delivery of breakthrough medicines for patients with cancer, /: 2025 16th April]; Available from: https, 2025.
- Novartis. Novartis and Microsoft announce collaboration to transform medicine with artificial intelligence, /: 2025 16th April]; Available from: https, 2025.
- Vatansever, S. , et al., Artificial intelligence and machine learning-aided drug discovery in central nervous system diseases: State-of-the-arts and future directions. Med Res Rev, 2021. 41(3): p. 1427-1473.
- Bera, I. and P.V. Payghan, Use of Molecular Dynamics Simulations in Structure-Based Drug Discovery. Curr Pharm Des, 2019. 25(31): p. 3339-3349.
- Alotaiq, N. D. Dermawan, and N.E. Elwali, Leveraging Therapeutic Proteins and Peptides from Lumbricus Earthworms: Targeting SOCS2 E3 Ligase for Cardiovascular Therapy through Molecular Dynamics Simulations. International Journal of Molecular Sciences, 2024. 25(19): p. 10818.
- Musliha, A. , et al., Unraveling modulation effects on albumin synthesis and inflammation by Striatin, a bioactive protein fraction isolated from Channa striata: In silico proteomics and in vitro approaches. Heliyon, 2024. 10(19): p. e38386.
- Choudhary, K. , et al., Recent advances and applications of deep learning methods in materials science. npj Computational Materials, 2022. 8(1): p. 59.
- Fu, C. and Q. Chen, The future of pharmaceuticals: Artificial intelligence in drug discovery and development. Journal of Pharmaceutical Analysis, 2025: p. 101248.
- Tong, X. , et al., Generative Models for De Novo Drug Design. Journal of Medicinal Chemistry, 2021. 64.
- Gangwal, A. and A. Lavecchia, Unleashing the power of generative AI in drug discovery. Drug Discovery Today, 2024. 29(6): p. 103992.
- Ataeinia, B. and P. Heidari, Artificial Intelligence and the Future of Diagnostic and Therapeutic Radiopharmaceutical Development:: In Silico Smart Molecular Design. PET Clin, 2021. 16(4): p. 513-523.
- Alotaiq, N. and D. Dermawan Computational Investigation of Montelukast and Its Structural Derivatives for Binding Affinity to Dopaminergic and Serotonergic Receptors: Insights from a Comprehensive Molecular Simulation. Pharmaceuticals, 2025. 18,. [CrossRef]
- Popova, M. O. Isayev, and A. Tropsha, Deep reinforcement learning for de novo drug design. Sci Adv, 2018. 4(7): p. eaap7885.
- Tan, R.K., Y. Liu, and L. Xie, Reinforcement learning for systems pharmacology-oriented and personalized drug design. Expert Opin Drug Discov, 2022. 17(8): p. 849-863.
- Lindroth, H. , et al. Applied Artificial Intelligence in Healthcare: A Review of Computer Vision Technology Application in Hospital Settings, 2024; 10. [Google Scholar] [CrossRef]
- Zhang, Y. , et al., A comprehensive large scale biomedical knowledge graph for AI powered data driven biomedical research. bioRxiv, 2025.
- Perdomo-Quinteiro, P. and A. Belmonte-Hernández, Knowledge Graphs for drug repurposing: a review of databases and methods. Briefings in Bioinformatics, 2024. 25(6): p. bbae461.
- Jang, H. and B. Yoon, An explainable artificial intelligence – human collaborative model for. investigating patent novelty. Engineering Applications of Artificial Intelligence, 2025. [Google Scholar]
- Just, J. , Natural language processing for innovation search – Reviewing an emerging non-human innovation intermediary. Technovation, 2024. 129: p. 102883.
- Ivanenkov, Y.A. , et al., Chemistry42: An AI-Driven Platform for Molecular Design and Optimization. Journal of Chemical Information and Modeling, 2023. 63(3): p. 695-701.
- Kathad, U. , et al., Development and clinical validation of Lantern Pharma’s AI engine: Response algorithm for drug positioning and rescue (RADR). Journal of Clinical Oncology. 37(15_suppl): p. 3114-3114.
- Alexandrov, V. , et al., High-throughput analysis of behavior for drug discovery. European Journal of Pharmacology, 2015. 750: p. 82-89.
- Long, G.V. , et al., KEYNOTE – D36: Personalized Immunotherapy with a Neoepitope Vaccine, EVX-01 and Pembrolizumab in Advanced Melanoma. Future Oncology, 2022. 18(31): p. 3473-3480.
- Dumbrava, E.E. , et al., A first-in-human, phase 1 study evaluating oral TACC3 inhibitor, AO-252, in advanced solid tumors. Journal of Clinical Oncology, 2024. 42(16_suppl): p. TPS3176-TPS3176.
- Patel, M.R. , et al., Preliminary results from a phase 1 study of AC699, an orally bioavailable chimeric estrogen receptor degrader, in patients with advanced or metastatic breast cancer. Journal of Clinical Oncology, 2024. 42(16_suppl): p. 3074-3074.
- Niewiarowska, A. , et al., Phase 2 clinical investigation of BPM31510 (ubidecarenone) alone and in combination with gemcitabine in patients with advanced pancreatic cancer. Annals of Oncology, 2017. 28: p. v157.
- Xia, S. , et al., BSI-001, a novel anti-HER2 antibody exhibiting potent synergistic efficacy with trastuzumab. Cancer Research, 2022. 82(12_Supplement): p. 5290-5290.
- Molnar, J. , et al., DOP098 Development of BEN8744, a phase 2 ready, peripherally restricted PDE10 inhibitor targeting a new mechanism of action for the treatment of ulcerative colitis. Journal of Crohn's and Colitis, 2025. 19(Supplement_1): p. i263-i263.
- Hartman, G. , et al., The discovery of novel and potent indazole NLRP3 inhibitors enabled by DNA-encoded library screening. Bioorg Med Chem Lett, 2024. 102: p. 129675.
- Risinger, R., L. Rajachandran, and H. Robinson, A Phase Ib/II Study of BXCL501 in Agitation Associated with Dementia. Alzheimer's & Dementia, 2025. 20.
- Rotta, M. , et al., Covalent-103: A phase 1, open-label, dose-escalation and expansion study of BMF-500, an oral covalent FLT3 inhibitor, in adults with acute leukemia (AL). Journal of Clinical Oncology, 2024. 42(16_suppl): p. TPS6589-TPS6589.
- Patel, J. , et al., EP.12H.01 A Phase 2 Study to Assess BDTX-1535, An Oral EGFR Inhibitor, in Patients with Non-Small Cell Lung Cancer. Journal of Thoracic Oncology, 2024. 19(10, Supplement): p. S657.
- Idowu, O. , et al., 688P Pharmacokinetics of HMBD-001, a human monoclonal antibody targeting HER3, a CRUK first-in-human phase I trial in patients with advanced solid tumours. Annals of Oncology, 2023. 34: p. S480.
- Grant, S. , et al., DOP02 Single cell RNA sequencing of Ulcerative Colitis and Crohn's Disease tissue samples informs the selection of Triggering Receptors Expressed on Myeloid Cells 1 (TREM1) as a target for the treatment of Inflammatory Bowel Diseases. Journal of Crohn's and Colitis, 2023. 17(Supplement_1): p. i59-i60.
- Dumbrava, E. , et al., 477 COM902 (Anti-TIGIT antibody) monotherapy – preliminary evaluation of safety, tolerability, pharmacokinetics and receptor occupancy in patients with advanced solid tumors (NCT04354246). Journal for ImmunoTherapy of Cancer, 2021. 9(Suppl 2): p. A507.
- Khairnar, V. , et al., CYT-338 NK Cell Engager Mutispecific Antibody Engagement of NKp46 Activation Receptor Overcomes Anti-CD38 Mab Mediated Fratricide of NK Cells and Accords Enhanced Cancer Immunotherapy. Blood, 2023. 142: p. 6725.
- Segal Salto, M. , et al., DC-9476, a Novel Selective BRD4(BD2) Inhibitor, Improves Arthritis Scores in Preclinical Models of Rheumatoid Arthritis by Regulating Key Inflammatory Pathways. Arthritis Rheumatol., 2024. 76(suppl 9).
- Xu, C. , et al., Alpha-kinase 1 (ALPK1) agonist DF-006 demonstrates potent efficacy in mouse and primary human hepatocyte (PHH) models of hepatitis B. Hepatology, 2023. 77(1): p. 275-289.
- Wong, G. , A Randomised, Double-Blind, Placebo-Controlled, Ascending Dose Study to Assess the Safety, Tolerability, Pharmacokinetics, and Pharmacodynamics of a Single Dose of EMP-012 for Injection Administered Subcutaneously to Healthy Volunteers, in CENTRAL 2024 Issue 6. 2024.
- Khattak, A. , et al., 782-H Effects of an AI generated personalized neopeptide-based immunotherapy, EVX-01, in combination with pembrolizumab in patients with metastatic melanoma: a clinical trial update. Journal for ImmunoTherapy of Cancer, 2023. 11(Suppl 2): p. A1818.
- Diaz, N. , et al., Data from first-in-human study of EXS21546, an A2A receptor antagonist, now progressing into phase 1 in RCC/NSCLC. Cancer Research, 2023. 83(8_Supplement): p. CT114-CT114.
- Eckstein, F. , et al., Long-term efficacy and safety of intra-articular sprifermin in patients with knee osteoarthritis: results from the 5-year forward study. Osteoarthritis and Cartilage, 2020. 28: p. S77-S78.
- Keating, A.T. , et al., Phase 1/2 study of FMC-376 an oral KRAS G12C dual inhibitor in participants with locally advanced unresectable or metastatic solid tumors (PROSPER). Journal of Clinical Oncology, 2024. 42(16_suppl): p. TPS3184-TPS3184.
- Wentzel, K. , et al., A phase I/II, open-label study of the novel checkpoint IGSF8 inhibitor GV20-0251 in patients with advanced solid tumors. Annals of Oncology, 2024. 35: p. S680-S681.
- Guzman, B. , et al., GT-02287, a brain-penetrant structurally targeted allosteric regulator for glucocerebrosidase show evidence of pharmacological efficacy in models of Parkinson’s disease. Parkinsonism & Related Disorders, 2023. 113.
- De Alwis, D. , et al., First-in-human study of a novel half-life extended monoclonal antibody (GB-0669) against SARS-CoV2 and related sarbecoviruses. Open Forum Infectious Diseases, 2025. 12(Supplement_1): p. ofae631.026.
- Spira, A.I. , et al., Phase I study of HFB200301, a first-in-class TNFR2 agonist monoclonal antibody in patients with solid tumors selected via Drug Intelligent Science (DIS). Journal of Clinical Oncology, 2022. 40(16_suppl): p. TPS2670-TPS2670.
- Sanborn, R.E. , et al., First-in-human (FIH) phase I data of HST-1011, an oral CBL-B inhibitor, in patients with advanced solid tumors. Annals of Oncology, 2024. 35: p. S675-S676.
- Rodon Ahnert, J. , et al., A phase 1 first-in-human clinical trial of HMBD-002, an IgG4 monoclonal antibody targeting VISTA, in advanced solid tumors. Journal of Clinical Oncology, 2023. 41(16_suppl): p. TPS2664-TPS2664.
- Adjei, A.A. , et al., IAM1363-01: A phase 1/1b study of a selective and brain-penetrant HER2 inhibitor for HER2-driven solid tumors. Journal of Clinical Oncology, 2024. 42(16_suppl): p. TPS3186-TPS3186.
- Ren, F. , et al., A small-molecule TNIK inhibitor targets fibrosis in preclinical and clinical models. Nature Biotechnology, 2025. 43(1): p. 63-75.
- Kim, H. , et al., Development of a novel fusion protein, JUV-161, that enhances muscle regeneration for treatment of myotonic dystrophy type 1. Neuromuscular Disorders, 2024. 43: p. 104441.516.
- Leber, A. , et al., Efficacy and Safety of Omilancor in a Phase 2 Randomized, Double-Blind, Placebo-Controlled Trial of Patients With Ulcerative Colitis. Official journal of the American College of Gastroenterology | ACG, 2023. 118(10S).
- McKean, W. , et al., Phase 1 Clinical Trial of LP-284, a Novel Synthetically Lethal Small Molecule, in Relapsed or Refractory B-Cell Non-Hodgkin Lymphomas and Solid Tumors. Clinical Lymphoma, Myeloma and Leukemia, 2024. 24: p. S482-S483.
- Huang, Y. , et al., Organ-specific delivery of a mRNA-encoded bispecific T cell engager targeting Glypican-3 in hepatocellular carcinoma. Journal for ImmunoTherapy of Cancer, 2024. 12(Suppl 2): p. A1499.
- Wang, S. , et al., Halicin: A New Horizon in Antibacterial Therapy against Veterinary Pathogens. Antibiotics (Basel), 2024. 13(6).
- Verstockt, B. , et al., The Safety, Tolerability, Pharmacokinetics, and Clinical Efficacy of the NLRX1 agonist NX-13 in Active Ulcerative Colitis: Results of a Phase 1b Study. Journal of Crohn's and Colitis, 2024. 18(5): p. 762-772.
- Khanna, D. , et al., BASELINE DEMOGRAPHICS AND DISEASE CHARACTERISTICS IN SUBJECTS WITH ILD IN A PHASE 2 STUDY TO EVALUATE EFFICACY, SAFETY, AND TOLERABILITY OF MT-7117 IN DIFFUSE CUTANEOUS SYSTEMIC SCLEROSIS. Annals of the Rheumatic Diseases, 2024. 83: p. 1934-1935.
- Hussain, A. , et al., Changes in circulating lymphocyte subsets and CCR9 transcripts as mechanistic biomarkers of the small molecule α4β7 inhibitor MORF-057 in patients with Ulcerative Colitis. Journal of Crohn's and Colitis, 2025. 19(Supplement_1): p. i1854-i1855.
- Leber, A. , et al., Safety, Tolerability, and Pharmacokinetics of NIM-1324 an Oral LANCL2 Agonist in a Randomized, Double-Blind, Placebo-Controlled Phase I Clinical Trial. Clin Transl Sci, 2025. 18(1): p. e70129.
- Wu, R. , et al., Discovery and characterization of NXV01c, an EGFR × cMET bispecific nanobody drug conjugate with potent anti-tumor activity. Cancer Research, 2024. 84(6_Supplement): p. 1871-1871.
- Noel, M.S. , et al., Phase 1/2 trial of the HPK1 inhibitor NDI-101150 as monotherapy and in combination with pembrolizumab: Clinical update. Journal of Clinical Oncology, 2024. 42(16_suppl): p. 3083-3083.
- Papadopoulos, K.P. , et al., Phase 1/2 study of FOG-001, a first-in-class direct β-catenin:TCF inhibitor, in patients with colorectal cancer, hepatocellular carcinoma, and other locally advanced or metastatic solid tumors. Journal of Clinical Oncology, 2025. 43(4_suppl): p. TPS322-TPS322.
- Shin, D.-Y. , et al., PHI-101, a Novel FLT3 TKI, Shows Clinical Efficacy in Relapsed/Refractory FLT3-Mutated AML. Blood, 2024. 144: p. 1495.
- Alfa, R. , et al., Clinical pharmacology and tolerability of REC-994, a redox-cycling nitroxide compound, in randomized phase 1 dose-finding studies. Pharmacol Res Perspect, 2024. 12(3): p. e1200.
- Schönherr, H. , et al., Discovery of lirafugratinib (RLY-4008), a highly selective irreversible small-molecule inhibitor of FGFR2. Proceedings of the National Academy of Sciences, 2024. 121(6): p. e2317756121.
- Gamez, J. , et al., A proof-of-concept study with SOM3355 (bevantolol hydrochloride) for reducing chorea in Huntington's disease. Br J Clin Pharmacol, 2023. 89(5): p. 1656-1664.
- Krueger, J.G. , et al., Clinical efficacy of TAK-279, a highly selective oral tyrosine kinase 2 (TYK2) inhibitor, is associated with modulation of disease and TYK2 pathway biomarkers in patients with moderate-to-severe psoriasis. Journal of the American Academy of Dermatology, 2024. 91(3): p. AB159.
- Manasson, J. , et al., Preclinical Polypharmacology of S-1117, a Novel Engineered Fc-Fused IgG Degrading Enzyme, for Chronic Treatment of Autoantibody-Mediated Diseases. Blood, 2024. 144(Supplement 1): p. 2562-2562.
- Rao, S. , et al., Therapeutic potential of ISM8207: A novel QPCTL inhibitor, in triple-negative breast cancer and B-cell non-Hodgkin lymphoma. Annals of Oncology, 2023. 34: p. S201.
- Dedic, N. , et al., SEP-363856, a Novel Psychotropic Agent with a Unique, Non-D(2) Receptor Mechanism of Action. J Pharmacol Exp Ther, 2019. 371(1): p. 1-14.
- Koblan, K.S. , et al., Efficacy and Safety of SEP-363856, a Novel Psychotropic Agent with a Non-D2 Mechanism of Action, in the Treatment of Schizophrenia. CNS Spectrums, 2020. 25(2): p. 287-288.
- Sowell, R.T. , et al., STX-001, a locally administered LNP-formulated self-replicating mRNA that encodes the therapeutic payload IL-12, induces deep systemic immune responses to solid tumors. Cancer Research, 2023. 83(7_Supplement): p. 2731-2731.
- Fakih, M. , et al., Initial results from the phase I, first-in-human study of the covalent, PI3Kα inhibitor TOS-358 in patients with solid tumors, expressing PI3Kα mutations or amplifications. Annals of Oncology, 2024. 35: p. S499-S500.
- Gonciarz, M. , et al., TYK2 as a therapeutic target in the treatment of autoimmune and inflammatory diseases. Immunotherapy, 2021. 13(13): p. 1135-1150.
- Ubel, C. , et al., Establishing the role of tyrosine kinase 2 in cancer. Oncoimmunology, 2013. 2(1): p. e22840.
- Chen, H. , et al., The rise of deep learning in drug discovery. Drug Discovery Today, 2018. 23(6): p. 1241-1250.
- Vamathevan, J. , et al., Applications of machine learning in drug discovery and development. Nature Reviews Drug Discovery, 2019. 18(6): p. 463-477.
- Mak, K.-K. and M.R. Pichika, Artificial intelligence in drug development: present status and future prospects. Drug Discovery Today, 2019. 24(3): p. 773-780.
- Patel, V. and M. Shah, Artificial intelligence and machine learning in drug discovery and development. Intelligent Medicine, 2022. 02(03): p. 134-140.
- Moher, D. , et al., Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med, 2009. 6(7): p. e1000097.
- Alotaiq, N. and D. Dermawan, Advancements in Virtual Bioequivalence: A Systematic Review of Computational Methods and Regulatory Perspectives in the Pharmaceutical Industry. Pharmaceutics, 2024. 16(11): p. 1414.
Figure 1.
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram illustrates the process of selecting studies, showing how records were identified, screened, excluded, and finally included in the scoping review.
Figure 1.
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram illustrates the process of selecting studies, showing how records were identified, screened, excluded, and finally included in the scoping review.
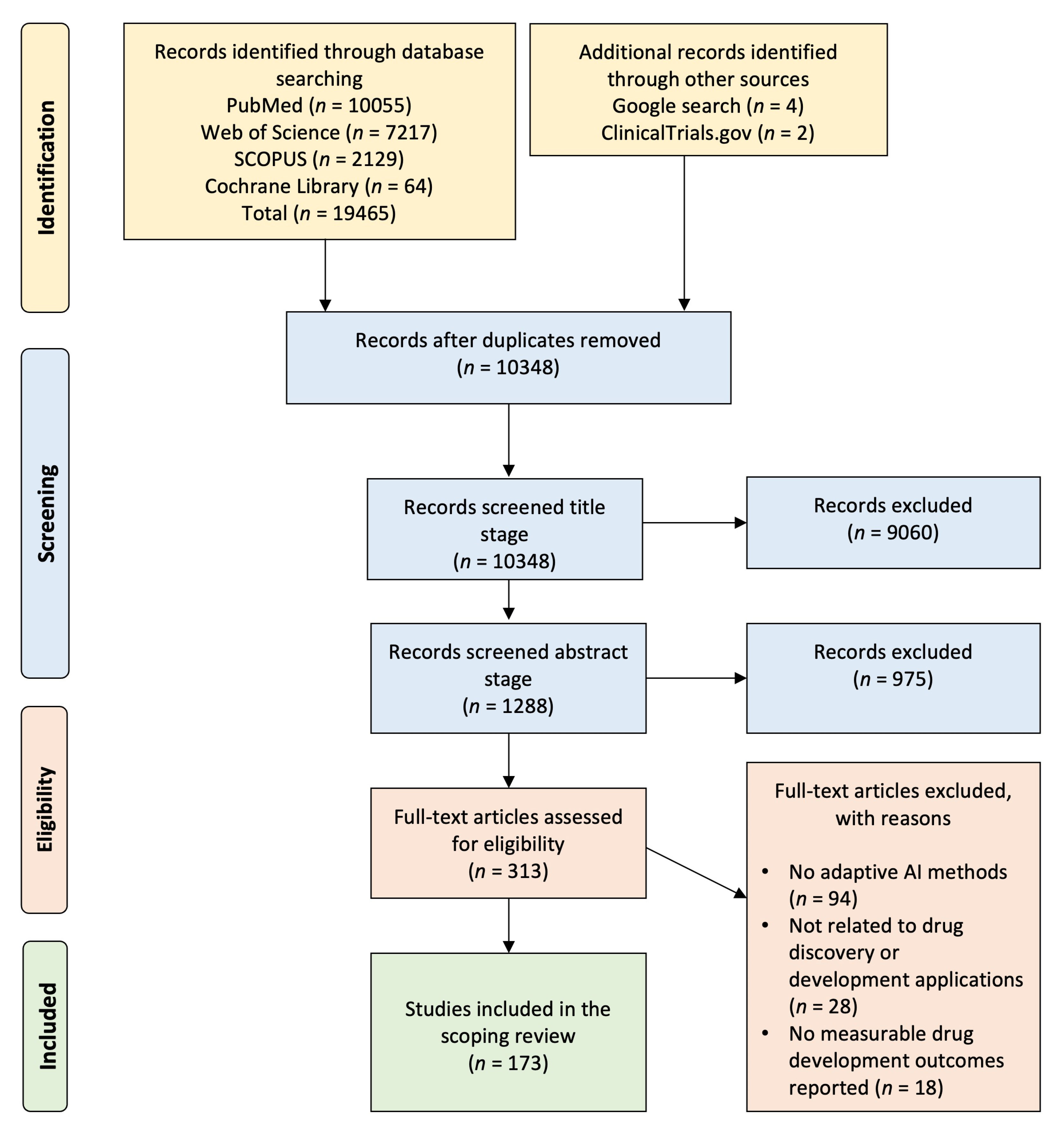
Figure 2.
Comprehensive analysis of AI-driven drug discovery studies: distribution across drug development stages, global research activity by country, industry collaboration, clinical reporting, and utilization of artificial intelligence methodologies. (A) A horizontal bar graph showing the number of AI-driven drug discovery studies categorized by their developmental stage, from preclinical research through various phases of clinical trials. (B) A world map indicating the number of AI-driven drug discovery studies conducted by country. (C) A series of bar graphs illustrating the percentage of studies reporting (1) industry partnerships, (2) clinical outcomes, and (3) translational impact. (D) A pie chart depicting the proportion of various AI technologies used in the studies. Machine Learning (ML) and Deep Learning (DL) dominate the field, accounting for 40.9% and 20.7% of studies, respectively.
Figure 2.
Comprehensive analysis of AI-driven drug discovery studies: distribution across drug development stages, global research activity by country, industry collaboration, clinical reporting, and utilization of artificial intelligence methodologies. (A) A horizontal bar graph showing the number of AI-driven drug discovery studies categorized by their developmental stage, from preclinical research through various phases of clinical trials. (B) A world map indicating the number of AI-driven drug discovery studies conducted by country. (C) A series of bar graphs illustrating the percentage of studies reporting (1) industry partnerships, (2) clinical outcomes, and (3) translational impact. (D) A pie chart depicting the proportion of various AI technologies used in the studies. Machine Learning (ML) and Deep Learning (DL) dominate the field, accounting for 40.9% and 20.7% of studies, respectively.
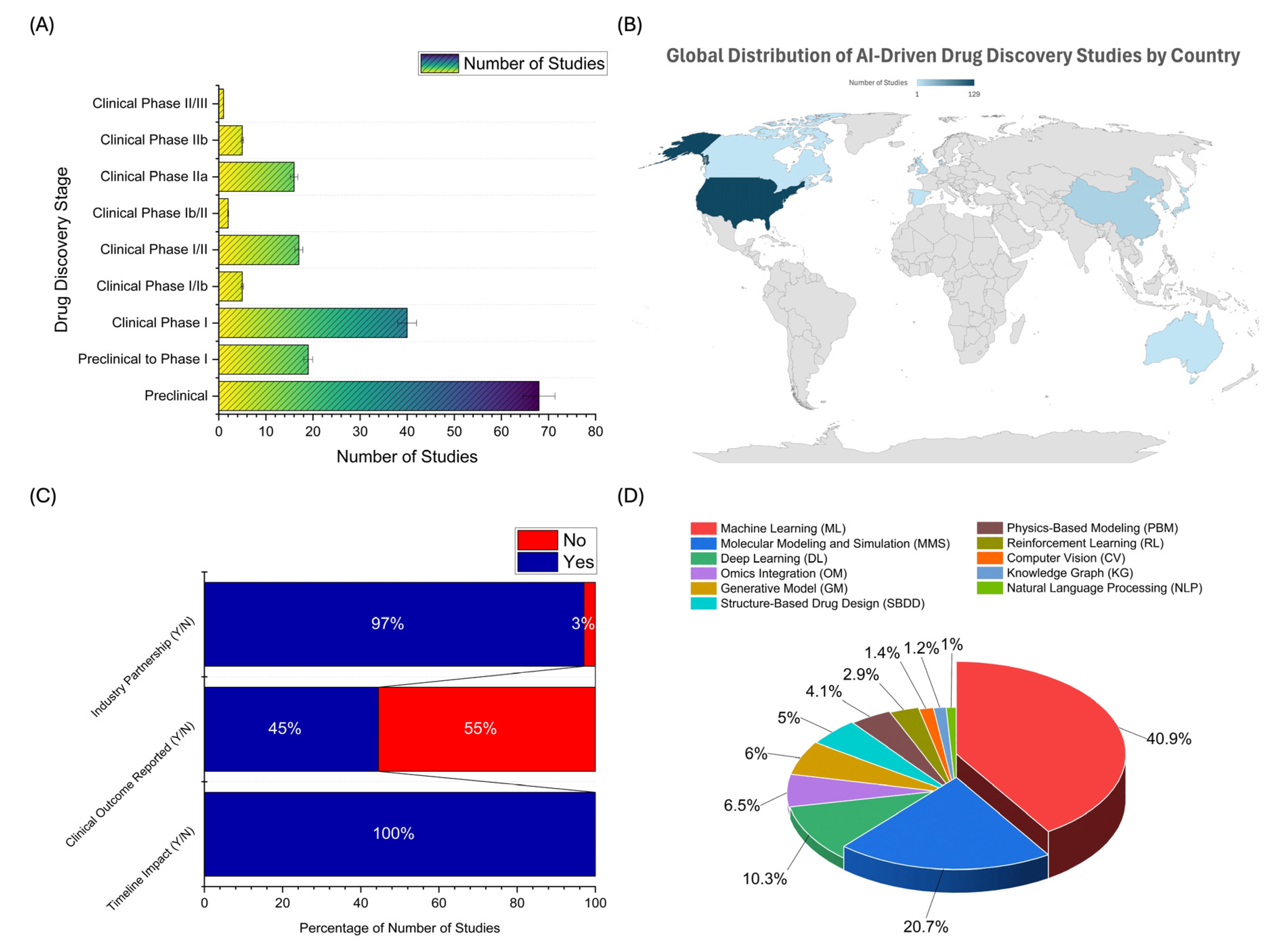
Figure 3.
Diversity of artificial intelligence (AI) techniques utilized across leading AI drug discovery platforms. This figure presents a comparative analysis of the number and variety of artificial intelligence (AI) techniques implemented by major AI platforms in drug discovery. Each bar represents a distinct AI platform, and each colored segment within the bars corresponds to a specific AI technique. These include: Single-cell Analysis (purple); Motion Simulation (light purple); Structural Biology (orange); Physics-based Modeling (gold); Big Data Analytics (red); Ensemble Machine Learning (pink); Predictive Machine Learning (green); Reinforcement Learning (lime green); Deep Learning (blue); and Generative Artificial Intelligence (light blue).
Figure 3.
Diversity of artificial intelligence (AI) techniques utilized across leading AI drug discovery platforms. This figure presents a comparative analysis of the number and variety of artificial intelligence (AI) techniques implemented by major AI platforms in drug discovery. Each bar represents a distinct AI platform, and each colored segment within the bars corresponds to a specific AI technique. These include: Single-cell Analysis (purple); Motion Simulation (light purple); Structural Biology (orange); Physics-based Modeling (gold); Big Data Analytics (red); Ensemble Machine Learning (pink); Predictive Machine Learning (green); Reinforcement Learning (lime green); Deep Learning (blue); and Generative Artificial Intelligence (light blue).
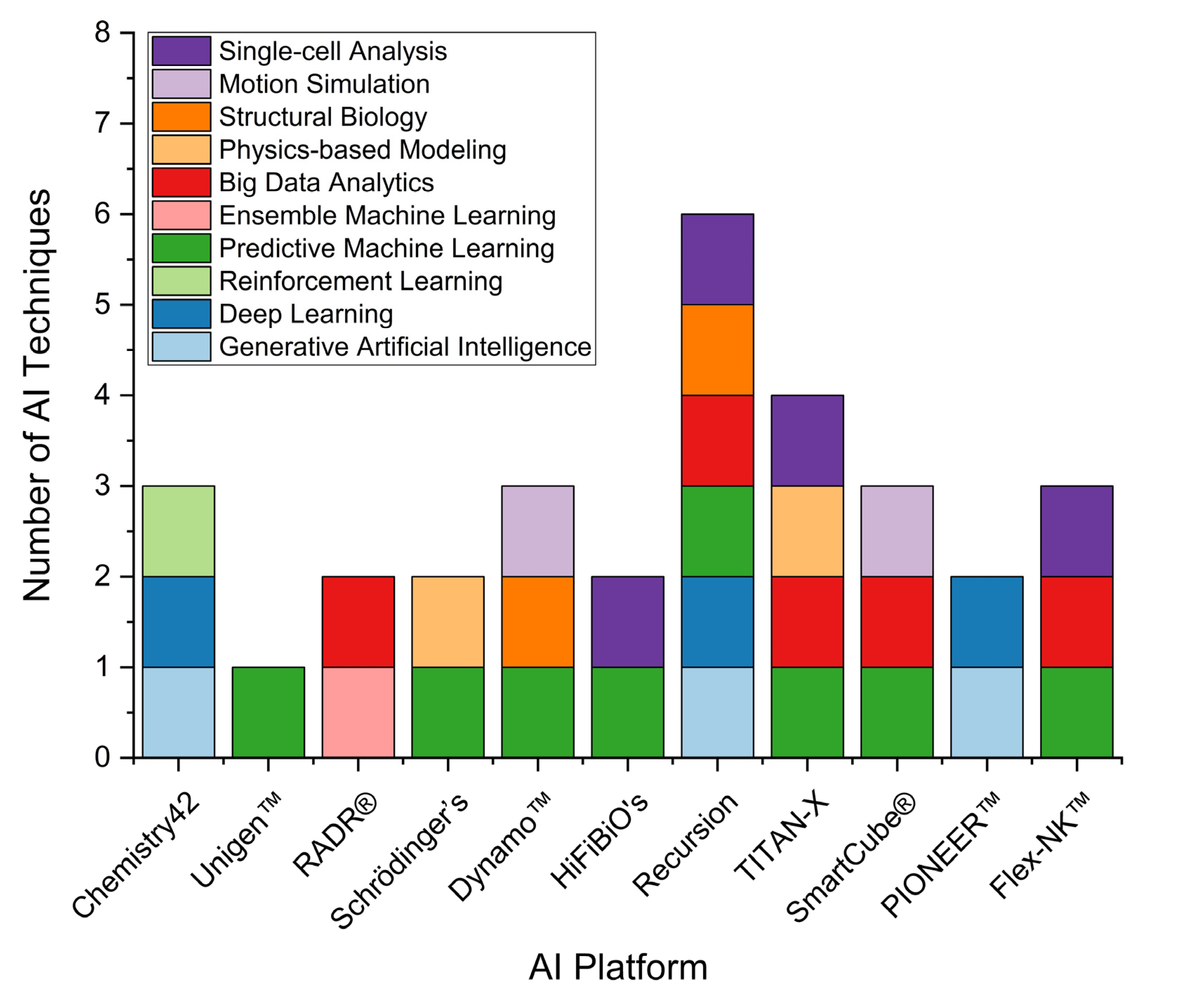
Figure 4.
Therapeutic focus and molecular target distribution in AI-driven drug discovery. (A) Bar chart showing the number of studies across various therapeutic areas. Oncology dominates with 126 studies, followed by dermatology (10), gastroenterology (9), neurology (9), and immunology (7), indicating a primary focus on cancer treatment in AI-based drug development. (B) Flower plot illustrating target molecules pursued by major AI-driven pharmaceutical companies (e.g., Insilico Medicine, Compugen, Schrödinger, Lantern Pharma, HiFiBiO Therapeutics, and Relay Therapeutics). Target labels are color-coded by development phase: preclinical (light blue), clinical phase I (moderate blue), phase II (darker blue), and phase III (darkest blue). Shared and high-priority targets such as PD-1, PD-L1, TYK2, and EGFR are visible across companies and development stages.
Figure 4.
Therapeutic focus and molecular target distribution in AI-driven drug discovery. (A) Bar chart showing the number of studies across various therapeutic areas. Oncology dominates with 126 studies, followed by dermatology (10), gastroenterology (9), neurology (9), and immunology (7), indicating a primary focus on cancer treatment in AI-based drug development. (B) Flower plot illustrating target molecules pursued by major AI-driven pharmaceutical companies (e.g., Insilico Medicine, Compugen, Schrödinger, Lantern Pharma, HiFiBiO Therapeutics, and Relay Therapeutics). Target labels are color-coded by development phase: preclinical (light blue), clinical phase I (moderate blue), phase II (darker blue), and phase III (darkest blue). Shared and high-priority targets such as PD-1, PD-L1, TYK2, and EGFR are visible across companies and development stages.
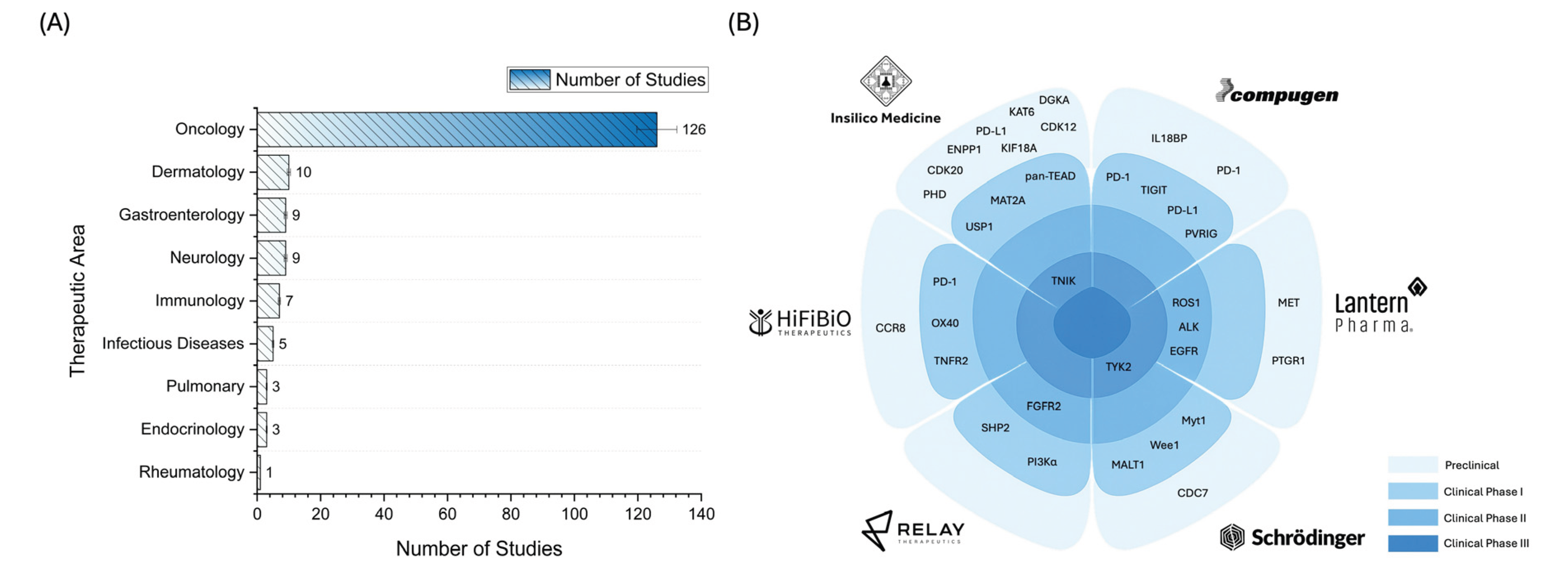

Table 1.
Recent applications of Artificial Intelligence (AI) techniques in drug discovery across therapeutic areas and development stages (2015 – 2025). This table presents data from a single study conducted by one pharmaceutical or AI company, showcasing the application of AI techniques in drug discovery and development across various therapeutic domains. The complete dataset, comprising 173 studies from multiple companies and research groups, is available in Supplementary Data S1.
Table 1.
Recent applications of Artificial Intelligence (AI) techniques in drug discovery across therapeutic areas and development stages (2015 – 2025). This table presents data from a single study conducted by one pharmaceutical or AI company, showcasing the application of AI techniques in drug discovery and development across various therapeutic domains. The complete dataset, comprising 173 studies from multiple companies and research groups, is available in Supplementary Data S1.
| Study; Year | AI Technique Used | Drug Discovery Stage | Therapeutic Area | Company/Funding Source |
|---|---|---|---|---|
| Dumbrava, EE. et al [44]; 2024 | Structure-Based Drug Design, Virtual Screening, ADMET Prediction, Biomarker Identification | Clinical Phase I | Oncology (TNBC, HGSOC, Endometrial Cancer with TP53 mutation/loss) |
A2A Pharmaceuticals |
| Patel, MR. et al [45]; 2024 | ChemiRise, Orbital Virtual Screening, Intelligent-SAR, Chemi-Net (AI-driven computational drug design, virtual screening, PK/PD prediction) | Clinical Phase I | Oncology (ER+/HER2- Breast Cancer) |
Accutar Biotechnology Inc |
| Niewiarowska, A. et al [46]; 2017 | BERG’s Interrogative Biology® platform + Oak Ridge Frontier supercomputer: Bayesian AI Modeling, Multi-Omics Data Integration, Supercomputing | Clinical Phase II | Oncology (Pancreatic Cancer) |
BERG LLC |
| Xia, S. et al [47]; 2022 | Deep learning for epitope mapping and functional screening, synthetic antigen design, multi-modal AI for antibody optimization | Preclinical | Oncology (HER2+ Breast Cancer) |
Baseimmune |
| Molnar, J. et al [48]; 2025 | Knowledge Graph and Machine Learning for Target Prioritization | Clinical Phase I | Gastroenterology (Ulcerative Colitis) |
BenevolentAI |
| Hartman, G. et al [49]; 2024 | DNA-Encoded Library (DEL) Screening, Computational Modeling, and Structure-Activity Relationship (SAR) Analysis | Preclinical | Immunology (NLRP3-related) |
BioAge Labs |
| Risinger, R. et al [50]; 2025 | NovareAI: Drug repurposing via big data integration, ML-based target identification, predictive modeling for trial design | Clinical Phase Ib/II | Neuropsychiatry (Dementia/Agitation) |
BioXcel Therapeutics |
| Rotta, M. et al [51]; 2024 | AI-driven FUSION™ System: Target ID, molecular modeling, PK/PD modeling, biomarker stratification | Clinical Phase I | Oncology (Acute myeloid leukemia/AML) |
Biomea Fusion Inc |
| Patel, J. et al [52]; 2024 | AI-based MAP platform for mutation analysis, allosteric site prediction, compound optimization, PK/PD modeling | Clinical Phase II | Oncology (Glioblastoma, non-small cell lung cancer/NSCLC) |
Black Diamond Therapeutics |
| Idowu, O. et al [53]; 2023 | AI-driven epitope prediction, multi-omic integration, biomarker stratification, and predictive modeling via RAD platform | Clinical Phase I/II | Oncology (Advanced solid tumors) | Cancer Research UK |
| Grant, S. et al [54]; 2023 | Machine Learning (target identification from scRNA-seq data via SCOPE platform) | Preclinical to Clinical Phase I | Gastroenterology (Ulcerative Colitis and Crohn’s Disease) |
Celsius Therapeutics |
| Dumbrava, E. et al [55]; 2021 | Unigen™: Machine learning–based predictive target discovery, AI-driven antibody design, spatial transcriptomics integration, and combination therapy modeling | Clinical Phase I | Oncology (Advanced Solid Tumors) |
Compugen Ltd |
| Khairnar, V. et al [56]; 2023 | Flex-NK™ platform: Computational antibody design, gene expression profiling, in vitro and in vivo modeling, combination therapy optimization using AI-driven analyses and structural modeling | Preclinical | Oncology (Multiple Myeloma) |
Cytovia Therapeutics |
| Salto, MS. et al [57]; 2024 | Generative AI for compound design, reinforcement learning for chemical space exploration, physics-based simulations for binding affinity optimization, automated synthesis and screening | Preclinical | Immunology (Rheumatoid Arthritis) |
DeepCure Inc |
| Xu, C. et al [58]; 2023 | IDInVivo platform: AI-driven in vivo gene targeting, preclinical efficacy modeling, PK/PD prediction, biomarker identification | Preclinical | Infectious Diseases (Hepatitis B) | Drug Farm |
| Wong, G [59]; 2024 | AI-driven target discovery (Precision Insights), siRNA design (siRCH), pharmacokinetics modeling, biomarker-based stratification | Preclinical to Clinical Phase I | Pulmonary (Chronic Lung Disease) |
Empirico |
| Khattak, A. et al [60]; 2023 | AI-Immunology™ platform (PIONEER™): Neoantigen prediction, ML, immune response modeling | Clinical Phase II | Oncology (Melanoma) |
Evaxion Biotech |
| Diaz, N. et al [61]; 2023 | Generative design, machine learning for predictive modeling, simulation-guided clinical trial design | Clinical Phase I | Oncology (Renal cell carcinoma/RCC, NSCLC) |
Exscientia and Evotec |
| Eckstein, F. et al [62]; 2020 | AI-assisted MRI segmentation and quantitative MRI (qMRI) analysis, location-independent cartilage change analysis, post-hoc data analysis | Clinical Phase II | Rheumatology (Knee Osteoarthritis) |
Formation Bio |
| Keating, AT. et al [63]; 2024 | AI-driven chemoproteomics, Druggability Atlas™ construction, covalent fragment-based drug discovery, machine learning, predictive modeling of resistance mechanisms | Clinical Phase I/II | Oncology (KRASG12C Mutant Tumors: NSCLC, PDAC, CRC) |
Frontier Medicines |
| Wentzel, K. et al [64]; 2024 | GV20's STEAD platform: AI-driven target discovery, antibody sequence prediction, and functional genomics integration | Clinical Phase I/II | Oncology (Advanced solid tumors) |
GV20 Therapeutics |
| Guzman, B. et al [65]; 2023 | Magellan™ AI platform for allosteric modulator discovery, Structural modeling, Predictive modeling (PK/PD), Biomarker identification | Preclinical | Neurology (Parkinson’s Disease) |
Gain Therapeutics |
| Alwis, DD. et al [66]; 2025 | Machine learning (Generate Platform) + iterative computation-experimentation loop | Clinical Phase I | Infectious Diseases (COVID-19 prophylaxis) | Generate Biomedicines |
| Spira, AI. et al [67]; 2022 | Generative AI, Multi-Modal Predictive Modeling, Convolutional Neural Networks | Clinical Phase I | Oncology (Solid tumors including EBV+ gastric cancer, ccRCC, melanoma, mesothelioma) | HiFiBiO Therapeutics |
| Sanborn, RE. et al [68]; 2024 | Smart Allostery™ platform: AI-driven data mining, computational modeling | Clinical Phase I/II | Oncology (Advanced solid tumors) | HotSpot Therapeutics |
| Ahnert, JR. et al [69]; 2023 | RAD platform (AI-driven epitope prediction), mAbPredictAI (AI-guided antibody design), cross-species AI analysis, systems biology integration | Clinical Phase I | Oncology (TNBC, NSCLC, other solid tumors) | Hummingbird Bioscience |
| Adjei, AA. et al [70]; 2024 | Iambic AI: Physics-informed AI drug discovery platform | Clinical Phase I/Ib | Oncology (HER2-driven solid tumors) |
Iambic Therapeutics |
| Ren, F. et al [71]; 2025 | Chemistry42: Generative Models and Reinforcement Learning | Clinical Phase III | Pulmonary (Idiopathic pulmonary fibrosis /IPF) |
Insilico Medicine |
| Kim, H. et al [72]; 2024 | AI-driven secretome mining, quantitative proteomics, and phenotypic validation | Preclinical | Endocrinology (Diabetes Type 1) |
Juvena Therapeutics |
| Leber, A. et al [73]; 2023 | LANCE® AI Platform, TITAN-X AI Platform: machine learning, multiscale modeling, predictive analytics, and bioinformatics | Clinical Phase II | Gastroenterology (Ulcerative Colitis and Inflammatory Bowel Disease/IBD) |
Landos Biopharma |
| McKean, W. et al [74]; 2024 | RADR® AI platform for identifying DNA repair vulnerabilities, biomarker signatures, and mechanism of action of LP-284 | Clinical Phase I/Ib | Oncology (Relapsed/Refractory B-cell NHL, Solid Tumors) |
Lantern Pharma Inc |
| Huang, Y. et al [75]; 2024 | AiLNP (Artificial Intelligence Lipid Nanoparticle) platform for lipid formulation optimization; AiTEM (Artificial Intelligence Therapeutic Engine for mRNA) for mRNA therapeutic candidate optimization. | Preclinical | Oncology (Hepatocellular Carcinoma) |
METiS Pharmaceuticals |
| Wang, S. et al [76]; 2024 | Deep learning, AI-based identification, and screening using IBM Watson | Preclinical | Infectious Diseases (Veterinary Bacterial Infections) | MIT and IBM Watson |
| Verstockt, B. et al [77]; 2024 | AI-powered precision medicine (TITAN-X Platform) for target discovery, biomarker identification, and trial optimization | Clinical Phase I/Ib | Gastroenterology (Ulcerative Colitis) |
MedChemExpress, NIMML Institute |
| Khanna, D. et al [78]; 2024 | Machine learning, QSAR models | Clinical Phase II | Dermatology (Skin diseases, autoimmune, fibrotic disorders) |
Medi-Tate and Medidata AI |
| Hussain, A. et al [79]; 2025 | Schrödinger LiveDesign platform: Computational modeling, structural biology, machine learning | Clinical Phase IIa | Gastroenterology (Ulcerative Colitis) | Morphic Therapeutic, Schrödinger, Lilly |
| Leber, A. et al [80]; 2025 | TITAN-X Precision Medicine Platform: Gene expression analysis, Predictive modeling, Multiomics data integration, Mechanistic modeling, Pharmacokinetic simulations | Clinical Phase I | Immunology (Systemic Lupus Erythematosus/SLE) |
NImmune, MedPath, BioSpace |
| Wu, R. et al [81]; 2024 | neoBiologics™ and neoDegrader™ (AI for antibody design, protein degradation, PPI analysis, and immunogenicity prediction) | Preclinical to Clinical Phase I | Oncology (NSCLC, gastric, liver, esophageal tumors) |
NeoX Biotech |
| Noel, MS. et al [82]; 2024 | Structure-based drug design, machine learning-based predictive modeling, medicinal chemistry optimization | Clinical Phase I/II | Oncology (Solid tumors) |
Nimbus Therapeutics |
| Papadopoulos, KP. et al [83]; 2025 | AI-Driven Helicon Design, Computational Physics Integration, Data Science for Trial Optimization | Clinical Phase I/II | Oncology (Solid tumors) |
Parabilis Medicines |
| Shin, DY. et al [84]; 2024 | AI-driven Chemiverse Platform: Target Identification, Compound Screening, ADMET Prediction | Clinical Phase I/II | Oncology (Acute Myeloid Leukemia) |
Pharos iBio |
| Alfa, R. et al [85]; 2024 | Recursion OS: AI-driven drug discovery (deep learning, machine vision, predictive modeling, computational chemistry) | Clinical Phase I | Neurology (Cerebral Cavernous Malformations) |
Recursion Pharmaceuticals |
| Schönherr, H. et al [86]; 2024 | Dynamo™ platform: Motion-Based Drug Design (MBDD), Molecular Dynamics Simulations, Machine Learning, AI-Driven Modeling | Clinical Phase I | Oncology (Solid Tumors, Intrahepatic Cholangiocarcinoma) |
Relay Therapeutics |
| Gamez, J. et al [87]; 2023 | SOMAIPRO platform: AI-driven computational techniques to identify new mechanisms of action, predict drug-target interactions, and repurpose existing drugs for new indications | Clinical Phase II | Neurology (Huntington’s Disease) |
SOM Biotech |
| Krueger, JG. et al [88]; 2024 | Deep learning, molecular dynamics simulations, free energy perturbation (FEP) | Clinical Phase III | Dermatology (Psoriasis) |
Schrödinger Inc |
| Manasson, J. et al [89]; 2024 | IMPACT platform: Machine learning-driven AI for IgG protease design, Deimmunization (epitope elimination), Pharmacokinetic/Pharmacodynamic (PK/PD) modeling, and multi-mechanistic targeting for optimal drug performance | Preclinical | Immuno-oncology (Thrombocytopenia/ITP and Evans syndrome) | Seismic Therapeutic |
| Rao, S. et al [90]; 2023 | Pharma.AI: Deep Learning, Reinforcement Learning, and Generative Chemistry | Preclinical | Oncology (Triple-negative breast cancer, B-cell non-Hodgkin lymphoma) |
Shanghai Fosun Pharmaceutical Development Co. Ltd, Insilico Medicine |
| Dedic, N. et al [91]; 2019 | SmartCube® platform (phenotypic screening, computer vision, machine learning) | Preclinical to Clinical Phase I | Neurology (Schizophrenia) |
Sumitomo Pharma and PsychoGenics |
| Koblan, KS. et al [92]; 2020 | SmartCube® platform (phenotypic screening, computer vision, machine learning) | Clinical Phase II | Neurology (Schizophrenia) |
Sunovion Pharmaceuticals Inc |
| Sowell, RT. et al [93]; 2023 | AI/ML-enabled target discovery, compound generation, and ADMET prediction | Preclinical | Oncology (Solid Tumors) |
Supercede Therapeutics |
| Fakih, M. et al [94]; 2024 | DNA-Encoded Library Screening, Machine Learning | Clinical Phase I | Oncology (Cancer) |
Totus Medicines |
Table 2.
Inclusion and exclusion criteria were used in study selection. This table outlines the detailed eligibility criteria applied during the selection of studies included in this systematic review. The criteria were established a priori to ensure consistency and relevance in capturing studies focused on the application of artificial intelligence (AI) in drug discovery and development.
Table 2.
Inclusion and exclusion criteria were used in study selection. This table outlines the detailed eligibility criteria applied during the selection of studies included in this systematic review. The criteria were established a priori to ensure consistency and relevance in capturing studies focused on the application of artificial intelligence (AI) in drug discovery and development.
| Criteria Type | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Study Type | Peer-reviewed original research articles, white papers, or technical reports focusing on AI-driven drug discovery or development | Editorials, opinion pieces, reviews, commentaries, preprints, general reviews without AI focus, or unverified grey literature |
| AI Method | Studies applying machine learning, deep learning, natural language processing, generative AI, reinforcement learning, or knowledge graph-based models | Studies based solely on rule-based systems, deterministic algorithms, or expert systems without adaptive or learning capabilities |
| Application Focus | Application of AI in drug discovery pipeline stages: target identification, hit/lead optimization, compound screening, preclinical evaluation, IND submission | Studies focused on AI in diagnostics, radiology, electronic health records, hospital operations, marketing, or unrelated computational biology applications |
| Outcome Measures | Studies reporting on outcomes such as candidate nomination, time-to-lead, IND approval acceleration, development timeline reduction, or pipeline productivity | Studies lacking measurable outcomes or reporting only theoretical models without downstream drug development relevance |
| Language | Published in English | Published in languages other than English |
| Publication Date | Published between January 2015 and April 2025 | Published before January 2015 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



