Submitted:
09 May 2025
Posted:
09 May 2025
You are already at the latest version
Abstract
Deep Margin Elevation (DME) is a widely adopted technique for managing subgingival cervical proximal margins by repositioning them to a supragingival location. This approach enhances access, visibility, and control in these anatomically challenging areas. This review aims to consolidate existing literature on the indications/contraindications, materials, clinical application steps, and longterm clinical outcomes of DME. A variety of materials have been investigated for use as the intermediate layer, with composite resins of varying viscosities and filler compositions being preferred due to their favorable long-term mechanical properties. However, more randomized clinical studies with sufficient follow-up are needed to determine the longevity of such restorations and to evaluate their impact on periodontal health. Understanding the indications, limitations, and protocol of DME is critical for achieving biologically sound and predictably functional restorations.
Keywords:
deep margin elevation
; proximal box relocation
; cervical margin relocation
; dental caries
; subgingival margins
1. Introduction
Achieving optimal restoration in the presence of subgingival margins remains one of the most demanding challenges in restorative dentistry [1]. Subgingival margins complicate key clinical procedures such as rubber dam isolation, the placement and stabilization of matrix systems, and the proper adaptation of restorative materials [2]. Furthermore, they hinder the removal of excess material, compromise finishing and polishing in the cervical region, and complicate impression-taking, cementation, and bonding procedures, particularly for indirect restorations [3]. Failure to control these factors often leads to iatrogenic damage, plaque accumulation, gingival inflammation, violation of the supracrestal tissue attachment (STA), secondary caries, and eventual failure of the restoration [4]. Therefore, the clinical management of deep subgingival margins is critical to ensure both the biological health of the periodontium and the longevity of restorations [5].
Several strategies have been proposed to manage deep subgingival margins, including surgical crown lengthening and orthodontic extrusion [6,7,8]. While these methods can effectively reestablish a supragingival margin, they are associated with significant limitations. Surgical crown lengthening, although predictable, may compromise the periodontal support of adjacent teeth, negatively impact esthetics, particularly in the anterior region, and require substantial healing periods before final restoration [9]. Orthodontic extrusion, while preserving periodontal structures, necessitates patient compliance, demands extended treatment time, and may involve complex interdisciplinary coordination [10]. These drawbacks generally underline the need for a less invasive, more efficient approach that addresses deep margins without jeopardizing periodontal health or treatment timelines.
In this context, Deep Margin Elevation (DME) has emerged as a minimally invasive alternative that maintains the integrity of natural periodontal architecture [11,12]. Originally introduced by Dietschi and Spreafico in 1998 [13], DME involves the coronal relocation of subgingival cervical margins through the strategic placement of an intermediate layer of resin composite. Initially conceptualized for use with indirect adhesive restorations such as inlays, onlays, and overlays, the technique has since expanded to include its application in direct restorations and chairside-fabricated indirect restorations [14]. By elevating the margin to a more accessible supragingival position, DME facilitates critical restorative procedures such as isolation, matrix adaptation, composite layering, and finishing and polishing [15]. Furthermore, it reduces the risk of biological complications associated with subgingival margins, such as plaque retention and inflammation, thereby supporting long-term periodontal stability [16].
Despite the growing adoption of DME in clinical practice, the technique continues to raise several pertinent questions. Concerns remain regarding the material properties of the intermediate layer, the biological response of periodontal tissues to resin-based interfaces positioned near the supracrestal tissue attachment, and the long-term success rates of restorations involving margin elevation [17]. Moreover, current literature reveals considerable variation in clinical protocols, materials selection, and outcomes assessment, highlighting the absence of standardized guidelines for its implementation. Given the increasing reliance on adhesive restorations and the trend toward minimally invasive dentistry, a comprehensive review of the DME technique is both timely and necessary.
This article aims to critically analyze existing evidence on DME, outlining its historical development, clinical indications and contraindications, procedural steps, material choices, and periodontal considerations. In addition, it seeks to identify the current limitations within the body of research and suggest areas where future clinical studies are warranted to optimize and validate this promising restorative approach.
2. Materials and Methods
A comprehensive literature review was conducted to gather relevant studies on Deep Margin Elevation (DME) and related techniques. Electronic searches were performed across three major databases: PubMed, Cochrane Library, and Scopus. The search strategy employed the following keywords: "deep margin elevation," "proximal box relocation," and "cervical margin relocation," combined using Boolean operators ("AND", "OR") where appropriate to optimize search sensitivity.
Inclusion criteria were defined to select studies that addressed DME techniques, their clinical indications and contraindications, materials utilized, procedural approaches, and reported clinical or laboratory outcomes. Eligible publication types included meta-analyses, systematic reviews, clinical studies (both prospective and retrospective), case series, case reports, and in vivo/in vitro experimental research. Only articles published in the English language were considered, with a time frame set from January 1998, the year DME was first introduced, to December 2024. Abstracts were screened initially to determine relevance, followed by full-text review for final inclusion. Exclusion criteria were set to omit articles that did not specifically address DME or its clinical applications, studies focusing exclusively on surgical or orthodontic management of subgingival margins without reference to restorative techniques, and non-English publications.
The selection process and eligibility assessment are outlined in the relevant Prisma Flow diagram [18] (Figure 1)
The reviewed literature included various study types. Among the 74 items analyzed, 16 were clinical experimental studies. Additionally, the review comprised 33 in vitro studies, 14 systematic or narrative reviews, 3 case reports, 6 opinion articles, and 2 meta-analyses. The distribution of each type of evidence, along with its corresponding percentages, is presented in Figure 2.
3. Results.
3.1. Evolution of DME
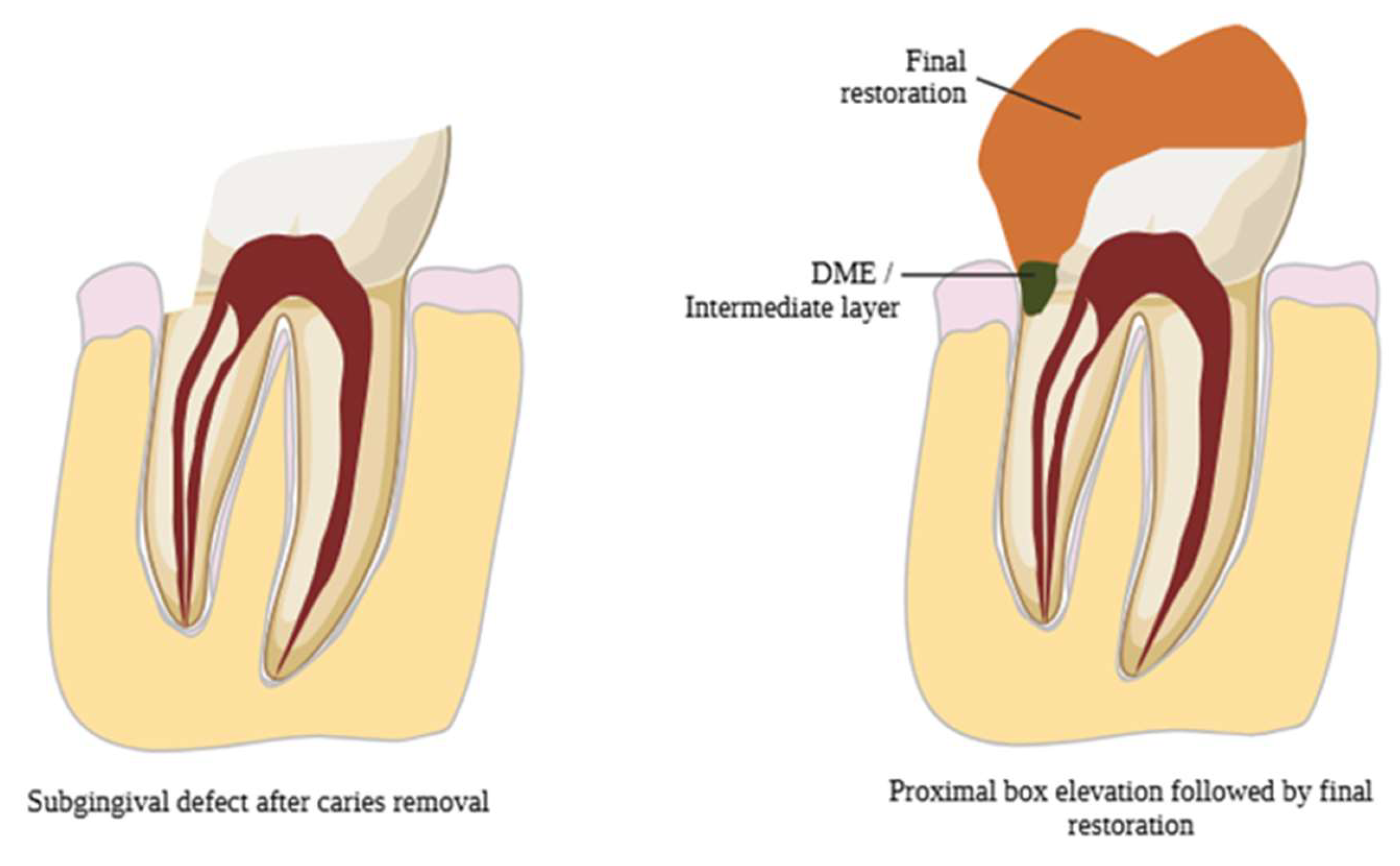
DME is based on relocating deep cervical margins coronally with an intermediate material layer, offering an alternative to surgical crown lengthening and orthodontic extrusion (Figure 3) [15.19]. Dietschi and Spreafico proposed using composite resin for this purpose [13]. The technique evolved from the open-sandwich technique, which used glass ionomer cement or resin-modified glass ionomer cement [20]. Today, composite resins of various viscosities with layered application options are predominantly used [21].
In 1998, Dietschi and Spreafico introduced the technique commonly referred to as deep margin relocation. This technique gained wider recognition in 2012 with the term “deep margin elevation”, which was proposed by Magne and Spreafico [14]. The goal of this technique is to elevate the cervical margin of a cavity coronally, either at or above the gingival level, using composite resin.
However, the article by Dietschi and Spreafico was not the first to reference the use of material for relocating the cervical margin of a cavity. As early as 1977, McLean and Wilson proposed the placement of a glass ionomer cement layer at the cervical margin of Class II restorations with subgingival margins, followed by overlaying this layer with composite resin. This method, widely known as the “open-sandwich technique”, demonstrated limited success due to the dissolution and mechanical degradation of conventional glass ionomer when exposed to the oral environment [22].
To address these limitations, resin-modified glass ionomer cement was introduced, offering improved mechanical properties, easier handling and significantly higher success rates compared to traditional glass ionomer. Nevertheless, advancements in composite resin materials and the ability to ensure proper isolation and moisture control, have shifted the focus of most researchers towards the exclusive use of various types of composite resins for cervical margin elevation [23,24].
Figure 2.
Basic principle of Deep Margin Elevation.
3.2. Indications for DME
DME is primarily indicated for clinical situations where deep cervical proximal margins extend subgingivally but still remain within the limits of the junctional epithelium [25]. Successful application of DME relies heavily on preserving the biological width, now more precisely termed the supracrestal tissue attachment (STA). To avoid STA violation, it is critical to ensure that the restorative margin is positioned at least 2.04 mm coronal to the alveolar bone crest, accounting for the dimensions of both the junctional epithelium and connective tissue attachment [5].
In addition, DME is particularly beneficial when managing deep margins during indirect restorative procedures such as inlays, onlays, and overlays. Elevating the margin to a supragingival or easily accessible location offers multiple clinical advantages. These include improved moisture control, enhanced visibility, facilitated impression-taking, more predictable bonding conditions, and easier removal of excess restorative material [2]. Achieving a supragingival margin significantly enhances the clinician’s ability to isolate the operative field, a crucial factor for the success of adhesive procedures. However, a fundamental prerequisite for performing DME is the ability to achieve complete and effective isolation of the operative field using a rubber dam [14]. Without adequate isolation, the risk of contamination increases, compromising the adhesive interface and the longevity of the restoration. Therefore, DME should only be considered in cases where proper rubber dam placement and stable isolation are feasible [26].
3.3. DME Technique
According to the protocol suggested by Magne et al [14], DME should be performed only when the field can be properly isolated with a rubber dam and the matrix system provides a firm seal.
After placing a rubber dam, old restorations and carious tissues are removed. Radiographic examination of the margin is essential to verify STA integrity and pulp involvement. Periodontal evaluation ensures predictable healing [27].
Tofflemire circumferential metal matrices are preferred, covering the cervical margin fully. In cases where the margin lies above the cemento-enamel junction (CEJ), conventional matrices suffice. For sub-CEJ margins, curved metal matrices, trimmed to 2–3 mm, slightly above the desired margin height- ensure proper adaptation and emergence profile (Figure 4) [14].
A critical focal point during DME is to ensure that neither the gingival tissues nor portions of the rubber dam interfere between the prepared margin and the matrix band. Proper matrix adaptation is essential for achieving an accurate restoration contour and an optimal seal [28]. Additionally, sufficient height and stability of the buccal and lingual walls are crucial, as these structures support the matrix system and maintain its proper positioning during composite placement [29]
Before proceeding with bonding procedures, Magne et al. [12] recommend the gentle re-preparation of the cavity margins using an ultrasonic instrument or a fine-grit diamond bur. This step aims to remove any debris or contamination that may have occurred during matrix placement, thereby optimizing the substrate for adhesive bonding.
For the adhesive protocol, the use of a three-step etch-and-rinse adhesive system combined with Immediate Dentin Sealing (IDS) is advised to enhance bond strength and long-term stability. Composite resin is then applied incrementally to elevate the margin by approximately 1.5 to 3 mm. Preheated composite resin (at approximately 55 °C) is preferred, as the increased temperature reduces the viscosity of the material, allowing for improved adaptation to cavity walls and minimizing the risk of void formation.
Following composite placement, excess material should be meticulously removed using a No. 12 surgical blade. Flossing between contacts and polishing with abrasive strips help refine the interproximal surfaces and ensure proper emergence profile. Radiographic confirmation, preferably using periapical X-rays, is a recommended final step to verify the correct adaptation of the material, absence of gaps or voids, and a harmonious emergence profile before proceeding with the final indirect restoration. (Figure 5).
Despite the emphasis given on rubber dam and matrix system placement, Frese et al described a technique that utilizes none: the R2-technique [27]. This approach relies on the principle that moisture control during the cervical margin relocation is confined within a small section of the defect, which is easily managed not to be contaminated by saliva, blood, and crevicular fluid. In the first step of this technique, after etching and bonding, a thin layer of flowable composite is placed on the surface, followed by a layer of nanohybrid composite without matrix (Figure 6). Both layers are light-cured simultaneously (snowplow technique). The inevitable excess is removed at this point using a No. 12 scalpel blade or a fine diamond bur. Afterwards, if a direct restoration is planned, a rubber dam, a sectional matrix, and a wedge are placed to shape the proximal surface. [27,30].
Even though the DME technique was first described for indirect restorations to facilitate impression taking, try-ins, cementation and excess removal, it can be a useful tool for defects that will be restored directly. In this way, rings are easily placed, a better emergence profile and tight proximal contacts are achieved.
3.4. Microleakage & Marginal Adaptation
Microleakage and proper marginal adaptation is a critical concern in DME due to the challenges of bonding to deep margins, as well as the difficulty in achieving a firm contact between the matrix and the cervical margin. Bulk-fill flowable and bioactive composites showed acceptable adaptation, while glass ionomer cement (GIC) exhibited poor mechanical properties over time. Flowable composites are beneficial in DME due to their low viscosity, which allows for excellent marginal adaptation [31]; however, evidence suggests that thicker layers of flowable composites are prone to polymerization shrinkage [32], making the snowplow technique particularly useful in DME scenarios by minimizing the thickness of the flowable layer and reducing the risk of long-term failure. Moreover, existing literature consistently indicates that self-curing resin cement generates a significantly higher number of microgaps, rendering it unsuitable for DME applications [33].

Table 1.
Microleakage & Marginal Adaptation
| Authors | Type of study | Bonding agent used | Means of evaluation | Results |
| Daghrery et al [34], 2024 | In vitro study | Total etch and 8th generation bonding agent | After thermal loading, marginal adaptation was assessed by measuring the vertical gaps between the lithium disilicate crown, the restorative material, and the underlying tooth structure. | Bulk fill flowable composite and bioactive composite demonstrated acceptable marginal adaptation. Glass ionomer cement produced the greatest change in vertical marginal adaptation. |
| Reddy et al [35], 2024 | In vitro study | Total etch and 5th generation bonding agent | Samples were examined for microleakage using confocal laser microscopy, and for interface integrity using scanning electron microscopy. | The use of glass ionomer cement (GIC) with hydroxyapatite addition ensures better marginal adaptation compared to flowable resins, but flowable resins create a more homogeneous surface. |
| Sadeghnezhad et al [1], 2024 | Meta-analysis | N/A | Data analysis was done by biostat software, 7 studies were included. | The use of DME had a positive effect in reducing microleakage compared to indirect restorations with subgingival extension. |
| Baldi et al [31], 2023 | In vitro study | Self-etch bonding agent | Specimens were scanned with micro-CT before after thermomechanical loading. | Flowable composites exhibited fewer interfacial gaps than nanohybrid composite. |
| Ismail HS et al [36], 2022 | Systematic review | N/A | Marginal adaptation was evaluated using a low vacuum scanning electron microscope. | Bulk-fill composites are recommended for proximal cavities with dentin/cementum margins, while RMGIs are better suited for poor moisture control or high caries risk. Despite bonding challenges, various adhesive protocols have shown comparable outcomes. |
| Vichitgomen et al [37], 2021 | In vitro study | 5th generation bonding agent | Marginal sealing ability at different interfaces was evaluated with a stereomicroscope at 40x magnification by scoring the depth of silver nitrate penetrating along the adhesive surfaces. | Microleakage was similar between DME and subgingival indirect restorations, but significantly higher with resin-modified glass ionomer cements. |
| Zhang et al [38], 2021 | In vitro study | Total etch | Specimens were coated with two layers of nail varnish extending 1 mm beyond the crown margins and immersed in a 0.55% methylene blue solution. Gingival microleakage was then evaluated under a stereomicroscope. | In endodontically treated teeth restored with an endocrown extending into the pulpal chamber, DME increased fracture resistance but did not reduce microleakage levels. |
| Jawaed et al [32], 2016 | In vitro study | Total etch | Specimens were sealed with acid-resistant varnish, leaving a 1 mm margin around the cervical area, and immersed in 2% buffered methylene blue solution for 24 hours. Microleakage was evaluated under a stereomicroscope, scored (0–4), and measured in millimeters. | The "snowplow" technique ensures lower microleakage in DME situations, because it reduces the thickness of the flowable resin at the base, which—due to its lower filler content—exhibits greater polymerization shrinkage. |
| Spreafico et al [21], 2016 | In vitro study | 4th generation bonding agent | Gold-sputtered epoxy replicas mounted on aluminum stubs were examined under SEM at 50X magnification. | No statistically significant differences in microleakage levels were found between margins with and without DME for indirect restorations. |
| Frankenberger et al [39], 2012 | In vitro study | Self-adhesive resin cements; | Microgaps were analyzed with SEM Analysis. | Direct bonding of glass ceramics to dentin showed the fewest microgaps (92%), followed by bonding to three-layered composite resin (84%), while repositioning with self-curing resin cement resulted in significantly more microgaps. |
| Stockton et al [33], 2007 | In vitro study | 5 groups: total etch; 6th generation; 7th generation; resin-modified-glass-ionomer-cement | Marginal integrity was measured by the percentage of surface area stained by silver nitrate solution. | On dentin, self-etch systems yielded lower microleakage rates. On enamel, they showed increased rates. |
3.5. Bond Strength & Layering
Securing a strong bond in the deep cervical margin is crucial to ensure long-term restoration stability. The literature remains inconclusive regarding the performance of flowable composites as an intermediate layer. Flowable and condensable composite resins demonstrated similar fracture resistance [40], with no significant impact observed from variations in DME layer height. Self-etching or universal adhesive systems are recommended for DME procedures, especially in cases when the tooth substrate is exclusively root dentin, or cementum. In an in vitro study by Magne et al [41], preheating the adhesive system (3-step etch-and-rinse) exhibited significantly increased μTBS between the composite resin and the underlying dentin. While this technique is still under investigation, it could be a valuable suggestion for further research, particularly in DME scenarios where bonding to dentin is a challenge, by potentially enhancing bond strength and improving long-term restoration performance.
Table 2.
Bond Strength & Layering
| Authors | Type of study | Bonding agent used | Means of evaluation | Results |
| Ismail et al [42], 2024 | In vitro study | 7th & 8th generation bonding agents | Specimens underwent μTBS testing after aging. | Light-cured adhesives showed the weakest μTBS to root-proximal dentin, while chemical and dual-cured agents performed comparably. |
| Balci et al [40], 2024 | In vitro study | Bonding agent N/A. Materials used for elevation: flowable composite, condensable composite. |
Static force was applied at an angle of 15° to the point of fracture. Fracture strength was measured and fracture types were examined under x6 magnification. | Flowable and condensable composite resin exhibited similar fracture resistance. |
| Juloski et al [43], 2020 | In vitro study | 7th generation bonding agent | SEM evaluation of marginal adaptation & microleakage evaluation with nail varnish | Self-etching or universal adhesives are recommended for DME to prevent dentin over-etching. |
| de Mattos Pimenta Vidal et al [44], 2012 | In vitro study | 5th generation b.a.; resin-modified-glass-ionomer | Two slabs per tooth were used for μTBS testing and two for nanoleakage assessment, based on penetration length (%) and silver nitrate deposition. | The presence of flowable composite significantly decreased micro tensile bond strength after aging simulation. |
3.6. Periodontal Response
The relationship between DME and periodontal health has long been a topic of debate, with heterogeneous results in literature. It is generally accepted that DME is contraindicated when the cervical margin is located less than 2 mm from the bone crest; in such instances, surgical crown lengthening should be considered (Figure 7 and Figure 8). Before determining the treatment plan, clinicians should carefully assess the distance from the bone crest through radiographic examination and bone sounding. When the supracrestal tissue attachment (STA) is preserved (more than 2.04 mm from the bone crest), DME can be compatible with periodontal health, provided that the patient maintains adequate oral hygiene (Figure 9). It is essential to establish an emergence profile that enables the patient to maintain effective oral hygiene. Undercontoured profiles and STA violation may result in open contact points, food traps, gingival inflammation, and ultimately, restoration failure (Figure 10). Additionally, the stages of excess removal, finishing, and polishing of the composite are critical, as only a perfectly smooth composite surface can facilitate the formation of a healthy junctional epithelium, thereby promoting periodontal health [25].
The relevant data on periodontal response are presented in Table 3.
3.7. Failure Rate
Deep Margin Elevation (DME) restorations demonstrate high survival rates, especially when combined with indirect restorations. Bresser et al. [50] reported a 95.9% five-year survival rate for partial-coverage restorations with prior DME, while Cieplik et al. [51] found comparable outcomes between restorations with and without DME. Similarly, Roggendorf et al. [52] observed no statistically significant differences in failure rates between DME and non-DME groups. Reported failure modes primarily include secondary caries, fractures, and pulpal complications [53,54,55]. However, existing studies differ in follow-up duration, sample size, and methodologies, which limits the strength of the conclusions. Although short- and medium-term data are favorable, further large-scale, long-term clinical trials are necessary to fully validate the longevity and reliability of DME restorations.
A critical factor in assessing the long-term performance of DME restorations is a comprehensive evaluation that includes not only the DME itself but also the overlying restoration. Although DME was initially introduced as a technique for indirect partial coverage restorations, the existing literature predominantly focuses on cases where the final restoration was direct composite resin. This discrepancy may influence the interpretation of results and the conclusions drawn regarding the long-term efficacy of DME. Therefore, future research should account for this limitation. Out of the included studies (in vitro or in vivo), 13 used exclusively direct composite resin restorations, 11 used indirect partial coverage restorations, 1 examined both and 4 used full coverage crowns. The distribution of final restoration types is presented in Figure 11 and relevant data of this section in Table 4.
4. Discussion
4.1. Material Selection for DME
Bonding to deep cervical margins presents significant clinical challenges, particularly when margins extend below the cementoenamel junction (CEJ). While residual enamel allows reliable bonding using total-etch techniques, adhesive protocols must be adapted when bonding to dentin or cementum to avoid over-etching and compromised adhesion [28,30]. In these cases, self-etch adhesives with selective enamel etching are recommended throughout the literature.
Early materials used for DME included glass-ionomer cements (GICs) and resin-modified glass-ionomer cements (RMGICs), often employed via the "open sandwich technique." Reddy et al. [35] evaluated DME using GIC, GIC with hydroxyapatite, and flowable resin composites. While RMGICs demonstrated lower microleakage due to their hydrophilic nature and fluoride release, they showed greater marginal integrity loss and a significantly weaker bond with overlying bulk-fill resin composites.
Recent studies have focused on flowable composites, highlighting the importance of material viscosity. Allegra Baldi et al. [60] reported that high-viscosity flowable resins exhibited superior marginal integrity compared to low-viscosity resins after cyclic loading. Flowable composites improve adaptation but, due to their lower filler content, may display greater polymerization shrinkage [61]. Limiting their thickness to 1–1.5 mm is therefore crucial, particularly when using the "snowplow" technique, where flowable and regular composite layers are polymerized simultaneously [62].
Preheated bulk-fill composites have also been proposed for DME, particularly for margins at or below the CEJ [15]. Their improved adaptation, reduced viscosity, and enhanced mechanical properties make them suitable for margin elevation. François et al. [63] demonstrated that high-filled flowable composites offer higher flexural strength and wear resistance compared to nanohybrids.
Regarding adhesive protocols, Roggendorf et al. [52] showed that applying three consecutive 1-mm layers of composite before ceramic bonding achieved marginal quality comparable to direct bonding to dentin. Furthermore, Cieplik et al. [51] reported similar performance between self-adhesive and conventional bulk-fill composites, suggesting a simplified protocol for future DME applications.
Polymerization shrinkage remains a critical factor influencing marginal stability. Lefever et al. [64] showed that self-etch adhesives failed to achieve ideal adaptation to enamel margins, supporting continued preference for fourth- and fifth-generation adhesives.
Dual-cure resin cements, despite offering handling convenience, provided unsatisfactory marginal adaptation [52,64,65]. Thus, their use for DME must be approached cautiously.
Finally, the mechanical demands on cervical margins cannot be ignored. Wu et al. [66] demonstrated that vertical forces concentrate on the cervical margin, especially where enamel height is reduced. Oblique forces increase stress even further, particularly in maxillary premolars [67]. Materials with an elastic modulus close to dentin, such as high-filled flowables or RMGICs, can act as stress absorbers, distributing occlusal forces more evenly and enhancing restoration longevity [68].
4.2. Long-Term Performance of DME
Despite increasing clinical use, long-term data for DME restorations remain limited. Bresser et al. [69] evaluated molars restored using bulk-fill composites, DME with lithium disilicate, and subgingival lithium disilicate extensions. DME cases showed more favorable outcomes in terms of repairability after fracture compared to subgingival ceramic extensions. In addition, material selection and adhesive protocols play critical roles in long-term success [64]. Silorane-based composites, due to their low polymerization shrinkage, have shown promising marginal adaptation. Ismail et al [36] also demonstrated that composite resins performed better than GIC-based materials regarding marginal integrity after thermomechanical loading.
Concerning secondary caries, Kuper et al. [53] reported no significant increase in caries risk for restorations extending below the CEJ. Bresser et al. [50] documented a 95.9% survival rate and a 2.5% secondary caries rate for indirect restorations with prior DME over five years. Finally, regarding fracture resistance, most studies support that DME does not compromise the strength of restorations [54,55] and in some cases, fracture resistance may even be enhanced [55].
4.3. Relationship Between DME and Periodontal Health
The biological response of periodontal tissues to DME remains a key concern. Ferrari et al. [25] observed increased bleeding on probing (BoP) and plaque index scores in DME cases, particularly when margins were placed less than 2 mm from the alveolar crest, violating the supracrestal tissue attachment (STA). Conversely, Sarfati et al. [70] noted that although connective tissue reattachment is not possible on resin surfaces, long epithelial adhesion can occur, provided plaque control is maintained. Van Dijken et al. [71] also found that while periodontal health remained stable after one year, gingival inflammation indicators increased slightly after 3–4 years, possibly due to early material deficiencies. Bertoldi et al. [47] further demonstrated that resin-based subgingival restorations may induce mild inflammation even in plaque-free environments, likely related to residual monomer release. However, when the STA is respected and margins are carefully polished, periodontal health can be preserved.
Therefore, for DME to remain biologically compatible, clinicians must ensure careful finishing and polishing of the restoration, perfect marginal integrity, and strict maintenance of >2 mm distance from the bone crest.
4.4. Alternative Techniques for Managing Subgingival Cervical Margins
Two primary alternatives to DME are surgical crown lengthening (SCL) and orthodontic extrusion (OE).
SCL involves apical repositioning of the STA through flap elevation. While effective, SCL carries significant drawbacks, including esthetic compromise, risk of hypersensitivity, altered crown-to-root ratio, and extended healing times [19]. Especially in the anterior region, SCL often necessitates more complex interventions to maintain symmetry.
OE offers a less invasive alternative by repositioning the tooth coronally. Strong forces (>0.6 N) achieve rapid extrusion without preserving the periodontal apparatus, while lighter forces (0.2–0.3 N) allow coordinated gingival and bone movement [72]. More aggressive surgical extrusion and intentional replantation are additional options but carry risks like root resorption and periodontal damage [73].
While both SCL and OE can manage deep margins, they are more invasive, costly, and time-consuming compared to DME.
4.5. Decision-Making and New Classifications
Recent classification systems help guide clinical decision-making. Veneziani [74] proposed a three-grade system based on isolation feasibility and margin proximity to bone: Grade 1: Full isolation possible; DME with flowable composite indicated, Grade 2: Isolation difficult; minimal surgical exposure needed, Grade 3: STA violation present; requires crown lengthening.
Ghezzi et al. [46] refined this system by correlating margin location with periodontal anatomy, emphasizing that margins ideally reside within the junctional epithelium, not connective tissue, for optimal outcomes.
4.6. Clinical Considerations
DME is a technique-sensitive procedure requiring precise case selection and execution. Ideal candidates must demonstrate excellent oral hygiene, as relocated margins are prone to plaque accumulation. Poor plaque control can exacerbate inflammation, leading to secondary caries and restoration failure [75]. Anatomical factors, such as thin biotypes and anterior esthetic demands, must be carefully evaluated. Minor STA violations in anterior teeth can cause recession and esthetic compromise [17]. Also, DME is well-suited for direct and indirect partial-coverage restorations but contraindicated for full-coverage crowns, where margins must be placed on natural tooth structure for mechanical durability [28].
Anatomical variations between the posterior and anterior regions influence the technique’s predictability. The flatter bone architecture of posterior regions provides greater resilience to minor epithelial attachment violations. In contrast, the scalloped anatomy of anterior regions makes them more susceptible to gingival recession when the supracrestal attachment is violated. This risk is highlighted in patients with a thin gingival biotype, where even minor disruptions can lead to significant esthetic consequences. Currently, the long-term outcomes of DME in anterior teeth remain unclear due to the limited availability of studies focused on this application. This knowledge gap underscores the need for further research to evaluate the technique's predictability and safety in esthetically demanding regions [17]. Finally, while DME offers a conservative, efficient solution for deep margins, meticulous isolation, correct adhesive selection, careful finishing, and continuous follow-up remain critical for long-term success.
4.7. Strengths and Limitations
This review offers a comprehensive and up-to-date synthesis of the available literature on Deep Margin Elevation (DME), incorporating both in vitro and clinical studies to provide a holistic understanding of adhesive protocols, material selection, mechanical behavior, periodontal outcomes, and clinical decision-making. A key strength is the integration of recent evidence, including publications through 2025, ensuring relevance to current practice. The review critically assesses the biological and mechanical aspects of DME rather than merely summarizing findings, and it offers practical clinical guidance by incorporating classifications and treatment algorithms. However, several limitations must be acknowledged. The included studies exhibit substantial heterogeneity in terms of design, methodology, and follow-up duration, which limits the generalizability of conclusions. Long-term clinical data specific to DME restorations remain sparse, particularly concerning indirect full-coverage restorations. Furthermore, inconsistencies among periodontal health assessments and a potential publication bias toward positive outcomes must be considered when interpreting the findings. Despite these limitations, this review provides a valuable, clinically oriented resource that highlights both the promise and the current gaps in the evidence surrounding Deep Margin Elevation.
5. Conclusions
The Deep Margin Elevation (DME) technique offers an effective, conservative solution for managing subgingival proximal cervical margins, improving access, visibility, and long-term restoration success. Composite resins remain the preferred material for margin relocation due to their superior mechanical properties, while self-adhesive resin cements and glass ionomer cements are less favorable. Success with DME depends on excellent moisture control, proper emergence profile, and meticulous removal of excess material to prevent plaque retention. Minor violations of the junctional epithelium are generally tolerated, but extension into connective tissue must be avoided.
Treatment planning should be individualized, considering periodontal health, anatomical risks, STA proximity, and patient compliance. Further large-scale, long-term clinical studies are essential to refine protocols and validate outcomes. A thorough understanding of DME indications, contraindications, and technique remains critical for achieving predictable, biologically sound restorations.
Author Contributions
Conceptualization, A.K., E.P.; methodology, A.K, E.P.; validation, A.K., M.F.; formal analysis, M.A.; investigation, A.K, M.F; data curation, A.K.; writing—original draft preparation, A.K.; writing—review and editing, M.F.,. M.A., E.P.; visualization, A.K.; supervision, M.F., M.A., E.P.; project administration, M.A., E.P.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| DME | Deep Margin Elevation |
| STA | Supracrestal Tissue Attachment |
| IDS | Immediate Dentin Sealing |
| PTFE | Polytetrafluoroethylene |
| GIC | Glass Ionomer Cement |
| μTBS | Micro Tensile Bond Strength |
| BoP | Bleeding on Probing |
| PI | Plaque Index |
| PPD | Probing Pocket Depth |
| GI | Gingival Index |
| SCL | Surgical Crown Lengthening |
| RMGIC | Resin Modified Glass Ionomer |
| OE | Orthodontic Extrusion |
References
- Sadeghnezhad P, Sarraf Shirazi A, Borouziniat A, Majidinia S, Soltaninezhad P, Nejat AH. Enhancing subgingival margin restoration: a comprehensive review and meta-analysis of deep margin elevation's impact on microleakage. Evid Based Dent. 2024 Jun 21. Epub ahead of print. PMID: 38907025. [CrossRef]
- Aldakheel M, Aldosary K, Alnafissah S, Alaamer R, Alqahtani A, Almuhtab N. Deep Margin Elevation: Current Concepts and Clinical Considerations: A Review. Medicina (Kaunas). 2022 Oct 18;58(10):1482. [CrossRef]
- Palma, P.J.; Neto, M.A.; Messias, A.; Amaro, A.M. Microtensile Bond Strength of Composite Restorations: Direct vs. Semi-Direct Technique Using the Same Adhesive System. J. Compos. Sci. 2025, 9, 203. [CrossRef]
- Alam MN, Ibraheem W, Ramalingam K, Sethuraman S, Basheer SN, Peeran SW. Identification, Evaluation, and Correction of Supracrestal Tissue Attachment (Previously Biologic Width) Violation: A Case Presentation with Literature Review. Cureus. 2024 Apr 12;16(4):e58128. [CrossRef]
- Felemban, M.F.; Khattak, O.; Alsharari, T.; Alzahrani, A.H.; Ganji, K.K.; Iqbal, A. Relationship between Deep Marginal Elevation and Periodontal Parameters: A Systematic Review. Medicina 2023, 59, 1948. [CrossRef]
- Fichera G., Mazzitelli C., Picciariello V., Maravic T., Josic U., Annalisa Mazzoni A., Breschi L. Structurally compromised teeth. Part II: A novel approach to peripheral build up procedures. J Esthet Rest Dent, 2023, 36, 1, 20-31. Special Annual Issue: Advances in Esthetic Dentistry 2024. [CrossRef]
- Lee, B., Shin, J., Jeong, T. et al. Combined treatment of surgical extrusion and crown lengthening procedure for severe crown-root fracture of a growing patient: a case report. BMC Oral Health 24, 1498 (2024). [CrossRef]
- Uravić Crljenica M., Perasso R., Imelio M., Viganoni C., Pozzan L. A systematic and comprehensive protocol for rapid orthodontic extrusion. J Esthet Rest Dent, 2024, 36, 6, 838-844. [CrossRef]
- Tu KW., Kuo CH, Hung CC., Yan DY., Mau JLP. Strategic sequencing of orthodontic treatment and periodontal regenerative surgery: A literature review. J Dent Sci. 2025.(In press). [CrossRef]
- Feu D. Orthodontic treatment of periodontal patients: challenges and solutions, from planning to retention. Dental Press J Orthod. 2020 Nov-Dec;25(6):79-116. [CrossRef]
- Bazos P, Magne P. Bio-Emulation: biomimetically emulating nature utilizing a histoanatomic approach; visual synthesis. Int J Esthet Dent. 2014;9(3):330-52.
- Magne PB. U Biomimetic restorative dentistry. Illinois: Quintessence; 2022.
- Dietschi D, Spreafico R. Current clinical concepts for adhesive cementation of tooth-colored posterior restorations. Pract Periodontics Aesthet Dent. 1998 Jan-Feb;10(1):47-54; quiz 56. PMID: 9582662.
- Magne, P., Harrington, S., & Spreafico, R. (2012). Deep Margin Elevation: A Paradigm Shift.
- Taylor A, Burns L. Deep margin elevation in restorative dentistry: A scoping review. J Dent. 2024 Jul;146:105066. Epub 2024 May 12. PMID: 38740249. [CrossRef]
- Kwon T, Lamster IB, Levin L. Current Concepts in the Management of Periodontitis. Int Dent J. 2021 Dec;71(6):462-476. Epub 2021 Feb 19. [CrossRef]
- Chun EP, de Andrade GS, Grassi EDA, Garaicoa J, Garaicoa-Pazmino C. Impact of Deep Margin Elevation Procedures Upon Periodontal Parameters: A Systematic Review. Eur J Prosthodont Restor Dent. 2023 Feb 28;31(1):10-21. PMID: 36446028. [CrossRef]
- University of Derby. Literature Reviews: systematic searching at various levels. Accessed on 28 April 2025 from https://libguides.derby.ac.uk/literature-reviews/prisma-lr.
- Mugri MH, Sayed ME, Nedumgottil BM, Bhandi S, Raj AT, Testarelli L, Khurshid Z, Jain S, Patil S. Treatment Prognosis of Restored Teeth with Crown Lengthening vs. Deep Margin Elevation: A Systematic Review. Materials (Basel). 2021 Nov 8;14(21):6733. [CrossRef]
- Loguercio AD, Alessandra R, Mazzocco KC, Dias AL, Busato AL, Singer Jda M, Rosa P. Microleakage in class II composite resin restorations: total bonding and open sandwich technique. J Adhes Dent. 2002 Summer;4(2):137-44.
- Spreafico R, Marchesi G, Turco G, Frassetto A, Di Lenarda R, Mazzoni A, Cadenaro M, Breschi L. Evaluation of the In Vitro Effects of Cervical Marginal Relocation Using Composite Resins on the Marginal Quality of CAD/CAM Crowns. J Adhes Dent. 2016;18(4):355-62. [CrossRef]
- Welbury RR, Murray JJ. A clinical trial of the glass-ionomer cement-composite resin "sandwich" technique in Class II cavities in permanent premolar and molar teeth. Quintessence Int. 1990, 6, 507-12.
- Andersson-Wenckert IE, van Dijken JW, Kieri C. Durability of extensive Class II open-sandwich restorations with a resin-modified glass ionomer cement after 6 years. Am J Dent. 2004 Feb;17(1):43-50.
- Da Silva Gonçalves D, Cura M, Ceballos L, Fuentes MV. Influence of proximal box elevation on bond strength of composite inlays. Clin Oral Investig. 2017 Jan;21(1):247-254. Epub 2016 Mar 11. PMID: 26969499. [CrossRef]
- Ferrari M, Koken S, Grandini S, Ferrari Cagidiaco E, Joda T, Discepoli N. Influence of cervical margin relocation (CMR) on periodontal health: 12-month results of a controlled trial. J Dent. 2018 Feb;69:70-76. Epub 2017 Oct 20. [CrossRef]
- Ismail EH, Ghazal SS, Alshehri RD, Albisher HN, Albishri RS, Balhaddad AA. Navigating the practical-knowledge gap in deep margin elevation: A step towards a structured case selection - a review. Saudi Dent J. 2024 May;36(5):674-681. Epub 2024 Mar 5. [CrossRef]
- Frese C, Wolff D, Staehle HJ. Proximal box elevation with resin composite and the dogma of biological width: clinical R2-technique and critical review. Oper Dent. 2014 Jan-Feb;39(1):22-31. Epub 2013 Jun 20. PMID: 23786609. [CrossRef]
- Samartzi TK, Papalexopoulos D, Ntovas P, Rahiotis C, Blatz MB. Deep Margin Elevation: A Literature Review. Dent J (Basel). 2022 Mar 14;10(3):48. PMID: 35323250; PMCID: PMC8947734. [CrossRef]
- Alizadeh Oskoee P, Dibazar S. Deep margin elevation; Indications and periodontal considerations. J Adv Periodontol Implant Dent. 2024 Nov 6;16(2):91-93. [CrossRef]
- Eggmann F, Ayub JM, Conejo J, Blatz MB. Deep margin elevation-Present status and future directions. J Esthet Restor Dent. 2023 Jan;35(1):26-47. Epub 2023 Jan 5. PMID: 36602272. [CrossRef]
- A Baldi, A Comba, T Rossi, L Monticone, E Berutti, N Scotti, 127 - Effect of flowable viscosities on deep margin elevation: a microCT study, Dental Materials,Volume 39, Supplement 1,2023,Pages e69-e70,ISSN 0109-5641. [CrossRef]
- Jawaed NU, Abidi SY, Qazi FU, Ahmed S. An In-VitroEvaluation of Microleakage at the Cervical Margin Between two Different Class II Restorative Techniques Using Dye Penetration Method. J Coll Physicians Surg Pak. 2016 Sep;26(9):748-52. PMID: 27671178.
- Stockton LW, Tsang ST. Microleakage of Class II posterior composite restorations with gingival margins placed entirely within dentin. J Can Dent Assoc. 2007 Apr;73(3):255. PMID: 17439712.
- Daghrery A, Jabarti E, Baras BH, Mitwalli H, Al Moaleem MM, Khojah MZ, Khayat W, Albar NH. Impact of Thermal Aging on Marginal Adaptation in Lithium Disilicate CAD/CAM Crowns with Deep Proximal Box Elevation. Med Sci Monit. 2025 Feb 3;31:e947191. PMID: 39895039; PMCID: PMC11804129. [CrossRef]
- Reddy KH, Priya BD, Malini DL, Mohan TM, Bollineni S, Gandhodi HC. Deep margin elevation in class II cavities: A comparative evaluation of microleakage and interface integrity using confocal laser microscopy and scanning electron microscopy. J Conserv Dent Endod. 2024 May;27(5):529-534. Epub 2024 May 10. PMID: 38939536; PMCID: PMC11205177. [CrossRef]
- Ismail HS, Ali AI, Mehesen RE, Juloski J, Garcia-Godoy F, Mahmoud SH. Deep proximal margin rebuilding with direct esthetic restorations: a systematic review of marginal adaptation and bond strength. Restor Dent Endod. 2022 Mar 4;47(2):e15. PMID: 35692223; PMCID: PMC9160765. [CrossRef]
- Vichitgomen J, Srisawasdi S. Deep margin elevation with resin composite and resin-modified glass-ionomer on marginal sealing of CAD-CAM ceramic inlays: An in vitro study. Am J Dent. 2021 Dec;34(6):327-332. PMID: 35051321.
- Zhang H, Li H, Cong Q, Zhang Z, Du A, Wang Y. Effect of proximal box elevation on fracture resistance and microleakage of premolars restored with ceramic endocrowns. PLoS One. 2021 May 26;16(5):e0252269. doi: 10.1371/journal.pone.0252269. Erratum in: PLoS One. 2021 Sep 23;16(9):e0258038. doi: 10.1371/journal.pone.0258038. PMID: 34038489; PMCID: PMC8153463.
- Frankenberger R, Hehn J, Hajtó J, Krämer N, Naumann M, Koch A, Roggendorf MJ. Effect of proximal box elevation with resin composite on marginal quality of ceramic inlays in vitro. Clin Oral Investig. 2013 Jan;17(1):177-83. Epub 2012 Feb 23. PMID: 22358378. [CrossRef]
- Balci ŞN, Tekçe N, Tuncer S, Demirci M. The effect of different deep margin elevation methods on the fracture strength of CAD-CAM restorations. Am J Dent. 2024 Jun;37(3):115-120. PMID: 38899989.
- Magne P, Mori Ubaldini AL. Thermal and bioactive optimization of a unidose 3-step etch-and-rinse dentin adhesive. J Prosthet Dent. 2020 Oct;124(4):487.e1-487.e7. Epub 2020 Jul 16. PMID: 32682525. [CrossRef]
- Ismail HS, Ali AI, Elawsya ME. Influence of curing mode and aging on the bonding performance of universal adhesives in coronal and root dentin. BMC Oral Health. 2024 Oct 5;24(1):1188. PMID: 39369181; PMCID: PMC11456248. [CrossRef]
- Juloski J, KÖken S, Ferrari M. No correlation between two methodological approaches applied to evaluate cervical margin relocation. Dent Mater J. 2020 Aug 2;39(4):624-632. Epub 2020 Apr 16. PMID: 32295986. [CrossRef]
- de Mattos Pimenta Vidal C, Pavan S, Briso AL, Bedran-Russo AK. Effects of three restorative techniques in the bond strength and nanoleakage at gingival wall of Class II restorations subjected to simulated aging. Clin Oral Investig. 2013 Mar;17(2):627-33. Epub 2012 May 11. PMID: 22576325. [CrossRef]
- Hausdörfer T, Lechte C, Kanzow P, Rödig T, Wiegand A. Periodontal health in teeth treated with deep-margin-elevation and CAD/CAM partial lithium disilicate restorations-a prospective controlled trial. Clin Oral Investig. 2024 Nov 30;28(12):670. PMID: 39613879; PMCID: PMC11606998. [CrossRef]
- Ghezzi C, Brambilla G, Conti A, Dosoli R, Ceroni F, Ferrantino L. Cervical margin relocation: case series and new classification system. Int J Esthet Dent. 2019;14(3):272-284. PMID: 31312813.
- Bertoldi C, Monari E, Cortellini P, Generali L, Lucchi A, Spinato S, Zaffe D. Clinical and histological reaction of periodontal tissues to subgingival resin composite restorations. Clin Oral Investig. 2020 Feb;24(2):1001-1011. Epub 2019 Jul 8. PMID: 31286261. [CrossRef]
- Oppermann RV, Gomes SC, Cavagni J, Cayana EG, Conceição EN. Response to Proximal Restorations Placed Either Subgingivally or Following Crown Lengthening in Patients with No History of Periodontal Disease. Int J Periodontics Restorative Dent. 2016 Jan-Feb;36(1):117-24. PMID: 26697548. [CrossRef]
- Padbury A Jr, Eber R, Wang HL. Interactions between the gingiva and the margin of restorations. J Clin Periodontol. 2003 May;30(5):379-85. PMID: 12716328. [CrossRef]
- Bresser RA, Gerdolle D, van den Heijkant IA, Sluiter-Pouwels LMA, Cune MS, Gresnigt MMM. Up to 12 years clinical evaluation of 197 partial indirect restorations with deep margin elevation in the posterior region. J Dent. 2019 Dec;91:103227. Epub 2019 Nov 4. PMID: 31697971. [CrossRef]
- Cieplik F, Hiller KA, Buchalla W, Federlin M, Scholz KJ. Randomized clinical split-mouth study on a novel self-adhesive bulk-fill restorative vs. a conventional bulk-fill composite for restoration of class II cavities - results after three years. J Dent. 2022 Oct;125:104275. Epub 2022 Aug 28. PMID: 36044948. [CrossRef]
- Roggendorf MJ, Krämer N, Dippold C, Vosen VE, Naumann M, Jablonski-Momeni A, Frankenberger R. Effect of proximal box elevation with resin composite on marginal quality of resin composite inlays in vitro. J Dent. 2012 Dec;40(12):1068-73. Epub 2012 Sep 7. PMID: 22960537. [CrossRef]
- Kuper NK, Opdam NJ, Bronkhorst EM, Huysmans MC. The influence of approximal restoration extension on the development of secondary caries. J Dent. 2012 Mar;40(3):241-7. Epub 2011 Dec 27. PMID: 22226997. [CrossRef]
- Amesti-Garaizabal A, Agustín-Panadero R, Verdejo-Solá B, Fons-Font A, Fernández-Estevan L, Montiel-Company J, Solá-Ruíz MF. Fracture Resistance of Partial Indirect Restorations Made With CAD/CAM Technology. A Systematic Review and Meta-analysis. J Clin Med. 2019 Nov 9;8(11):1932. PMID: 31717610; PMCID: PMC6912690. [CrossRef]
- Butt, Aftab. (2021). Cervical margin relocation and indirect restorations: Case report and literature review. Dental Update. 48. 93-97. [CrossRef]
- Onur Adson, Taha Yasin Sarıkaya, Bolay Şükran,,Margin Elevation for Posterior İndirect Restorations: 6-Month Clinical Outcomes, International Dental Journal, Volume 74, Supplement 1, 2024, Page S176, ISSN 0020-6539. [CrossRef]
- Gözetici-Çil B, Öztürk-Bozkurt F, Genç-Çalışkan G, Yılmaz B, Aksaka N, Özcan M. Clinical Performance of Posterior Indirect Resin Composite Restorations with the Proximal Box Elevation Technique: A Prospective Clinical Trial up to 3 Years. J Adhes Dent. 2024 Jan 26;26:19-30. PMID: 38276889; PMCID: PMC11740769. [CrossRef]
- Aziz AM, Suliman S, Sulaiman TA, Abdulmajeed A. Clinical and radiographical evaluation of CAD-CAM crowns with and without deep margin elevation: 10-year results. J Prosthet Dent. 2024 May 8:S0022-3913(24)00291-9. Epub ahead of print. PMID: 38724338 . [CrossRef]
- Muscholl C, Zamorska N, Schoilew K, Sekundo C, Meller C, Büsch C, Wolff D, Frese C. Retrospective Clinical Evaluation of Subgingival Composite Resin Restorations with Deep-Margin Elevation. J Adhes Dent. 2022 Aug 19;24:335-344. PMID: 35983705. [CrossRef]
- Baldi A, Rossi T, Comba A, Monticone L, Paolone G, Sannino I, Vichi A, Goracci C, Scotti N. Three-Dimensional Internal Voids and Marginal Adaptation in Deep Margin Elevation Technique: Efficiency of Highly Filled Flowable Composites. J Adhes Dent. 2024 Oct 14;26:223-230. PMID: 39397757. [CrossRef]
- De Goes MF, Giannini M, Di Hipólito V, Carrilho MR, Daronch M, Rueggeberg FA. Microtensile bond strength of adhesive systems to dentin with or without application of an intermediate flowable resin layer. Braz Dent J. 2008;19(1):51-6. PMID: 18438560. [CrossRef]
- Ölçer Us Y, Aydınoğlu A, Erşahan Ş, Erdem Hepşenoğlu Y, Sağır K, Üşümez A. A comparison of the effects of incremental and snowplow techniques on the mechanical properties of composite restorations. Aust Dent J. 2024 Mar;69(1):40-48. Epub 2023 Oct 9. PMID: 37814190. [CrossRef]
- Francois P, Attal JP, Fasham T, Troizier-Cheyne M, Gouze H, Abdel-Gawad S, Le Goff S, Dursun E, Ceinos R. Flexural Properties, Wear Resistance, and Microstructural Analysis of Highly Filled Flowable Resin Composites. Oper Dent. 2024 Sep 1;49(5):597-607. PMID: 39169507 . [CrossRef]
- Lefever D, Gregor L, Bortolotto T, Krejci I. Supragingival relocation of subgingivally located margins for adhesive inlays/onlays with different materials. J Adhes Dent. 2012 Dec;14(6):561-7. PMID: 22724114. [CrossRef]
- Juloski J, Köken S, Ferrari M. Cervical margin relocation in indirect adhesive restorations: A literature review. J Prosthodont Res. 2018 Jul;62(3):273-280. Epub 2017 Nov 15. [CrossRef]
- Wu F, Su X, Shi Y, Bai J, Feng J, Sun X, Wang X, Wang H, Wen J, Kang J. Comparison of the biomechanical effects of the post-core crown, endocrown and inlay crown after deep margin elevation and its clinical significance. BMC Oral Health. 2024 Aug 23;24(1):990. [CrossRef]
- Guo J, Wang Z, Li X, Sun C, Gao E, Li H. A comparison of the fracture resistances of endodontically treated mandibular premolars restored with endocrowns and glass fiber post-core retained conventional crowns. J Adv Prosthodont. 2016 Dec;8(6):489-493. Epub 2016 Dec 15. [CrossRef]
- Mahmoudi Yamchi F, Abbasi M, Atri F, Ahmadi E. Influence of Deep Margin Elevation Technique With Two Restorative Materials on Stress Distribution of e.max Endocrown Restorations: A Finite Element Analysis. Int J Dent. 2024 Nov 27;2024:6753069. [CrossRef]
- Bresser RA, Carvalho MA, Naves LZ, Melma H, Cune MS, Gresnigt MMM. Biomechanical behavior of molars restored with direct and indirect restorations in combination with deep margin elevation. J Mech Behav Biomed Mater. 2024 Apr;152:106459. Epub 2024 Feb 12. [CrossRef]
- Sarfati A, Tirlet G. Deep margin elevation versus crown lengthening: biologic width revisited. Int J Esthet Dent. 2018;13(3):334-356. PMID: 30073217.
- van Dijken JW, Sjöström S, Wing K. The effect of different types of composite resin fillings on marginal gingiva. J Clin Periodontol. 1987 Apr;14(4):185-9. [CrossRef]
- Reichardt E, Krug R, Bornstein MM, Tomasch J, Verna C, Krastl G. Orthodontic Forced Eruption of Permanent Anterior Teeth with Subgingival Fractures: A Systematic Review. Int J Environ Res Public Health. 2021 Nov 29;18(23):12580. PMID: 34886307; PMCID: PMC8656787. [CrossRef]
- Plotino G, Abella Sans F, Duggal MS, Grande NM, Krastl G, Nagendrababu V, Gambarini G. Present status and future directions: Surgical extrusion, intentional replantation and tooth autotransplantation. Int Endod J. 2022 May;55 Suppl 3:827-842. Epub 2022 Mar 30. [CrossRef]
- Veneziani M. Adhesive restorations in the posterior area with subgingival cervical margins: new classification and differentiated treatment approach. Eur J Esthet Dent. 2010 Spring;5(1):50-76.
- Dablanca-Blanco AB, Blanco-Carrión J, Martín-Biedma B, Varela-Patiño P, Bello-Castro A, Castelo-Baz P. Management of large class II lesions in molars: how to restore and when to perform surgical crown lengthening? Restor Dent Endod. 2017 Aug;42(3):240-252. Epub 2017 Aug 3. [CrossRef]
Figure 1.
Prisma Flow Diagram.
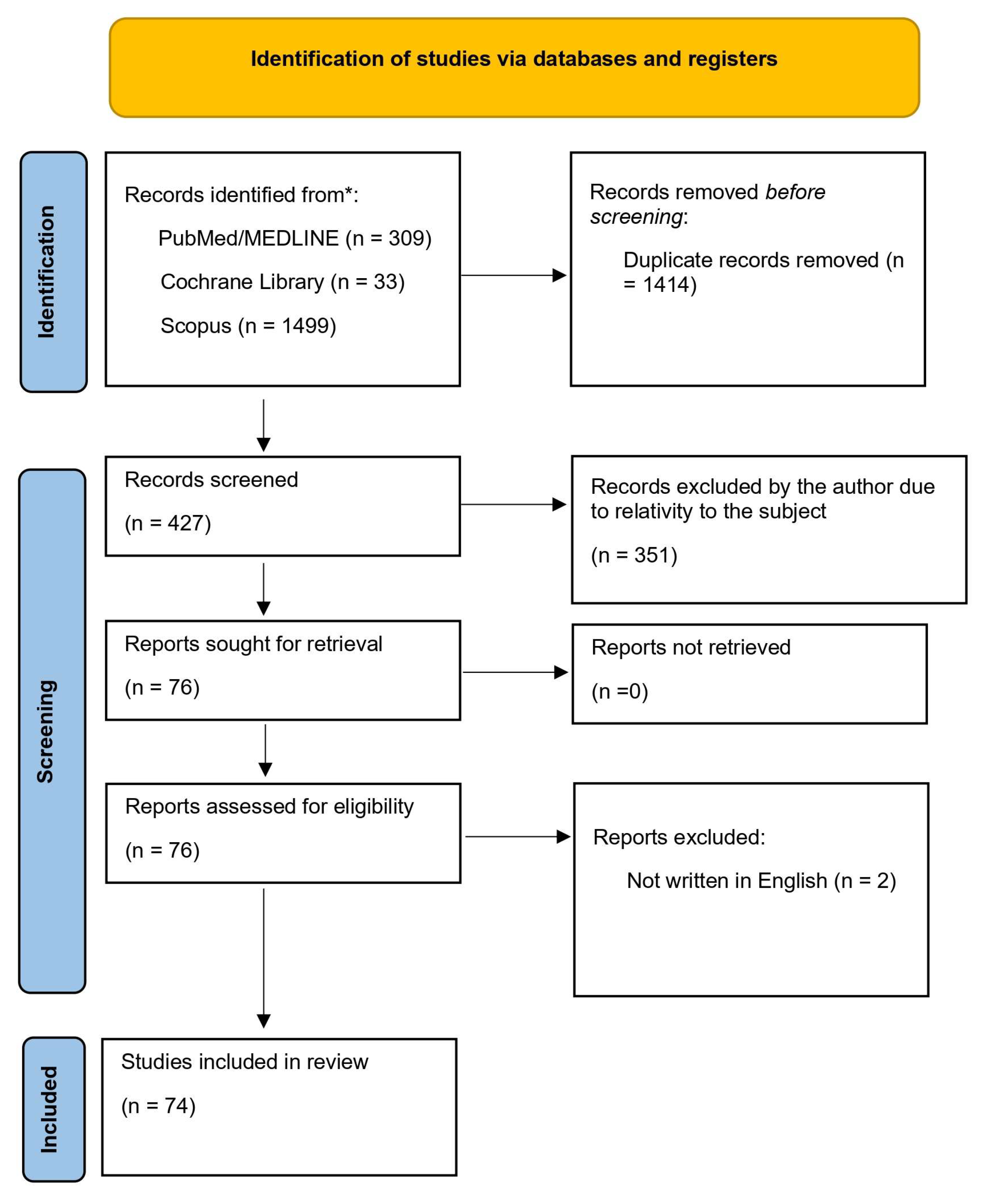
Figure 2.
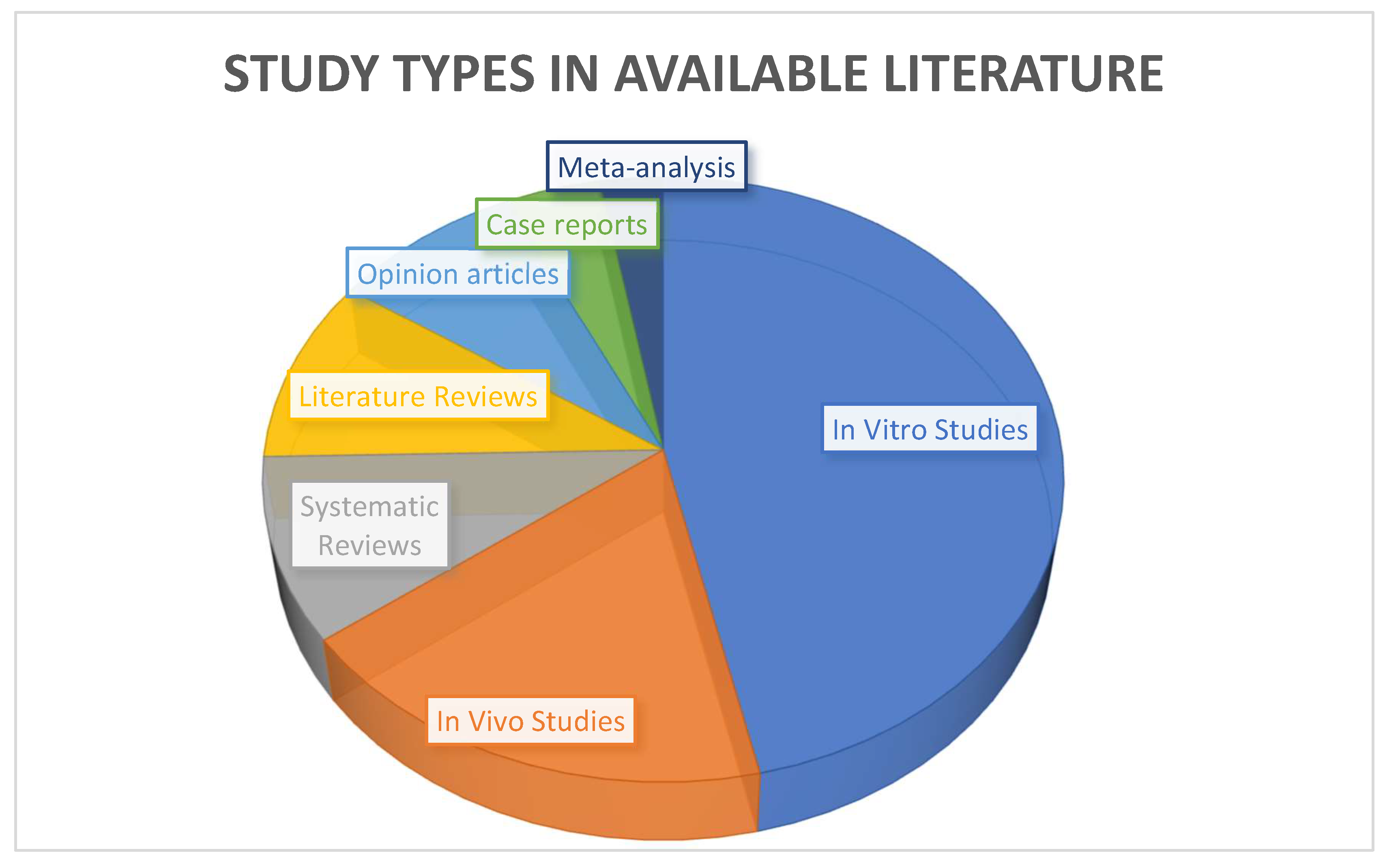
Figure 3.
DME with trimmed curved metal matrix.
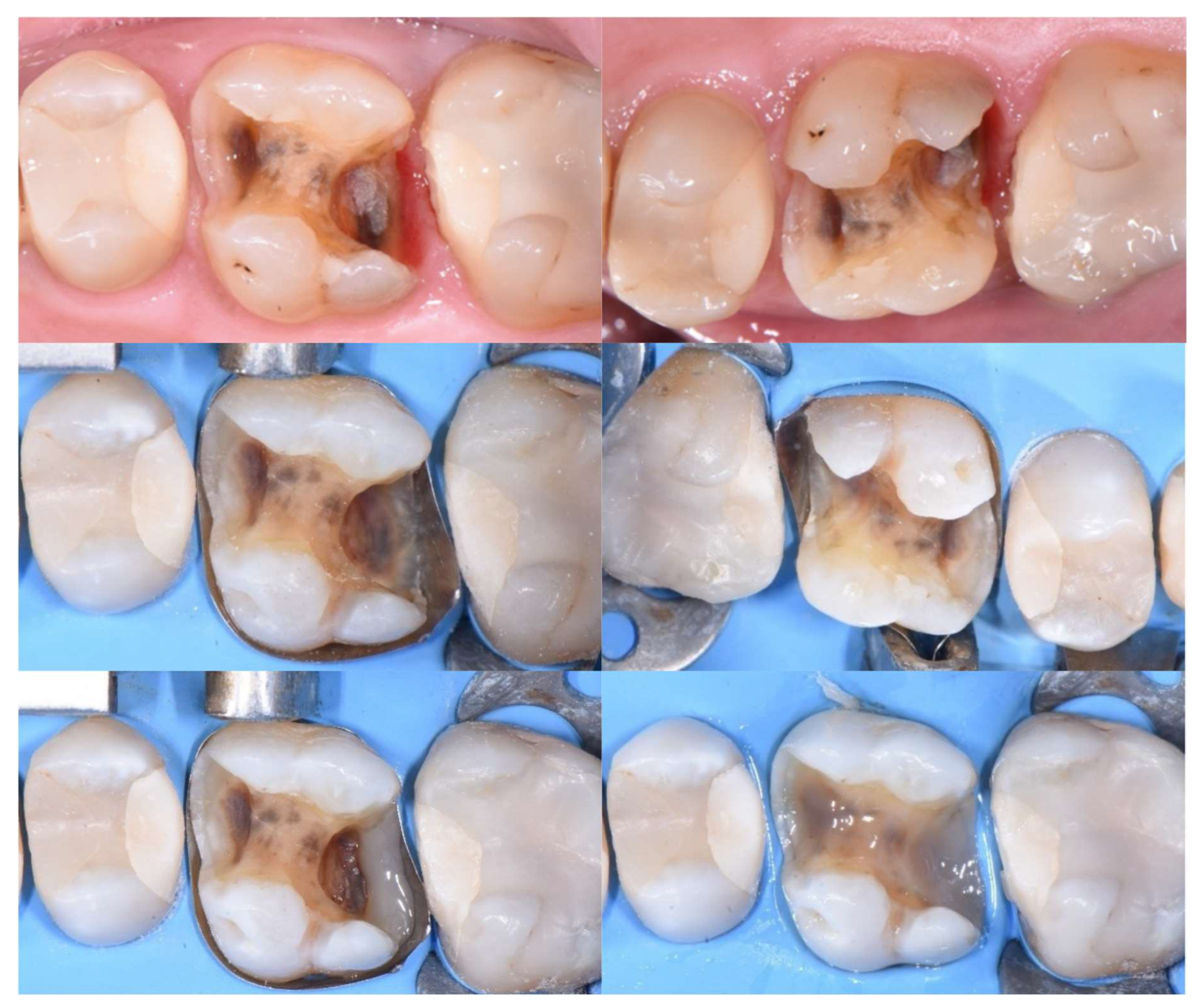
Figure 4.
Matrix-in-matrix technique.
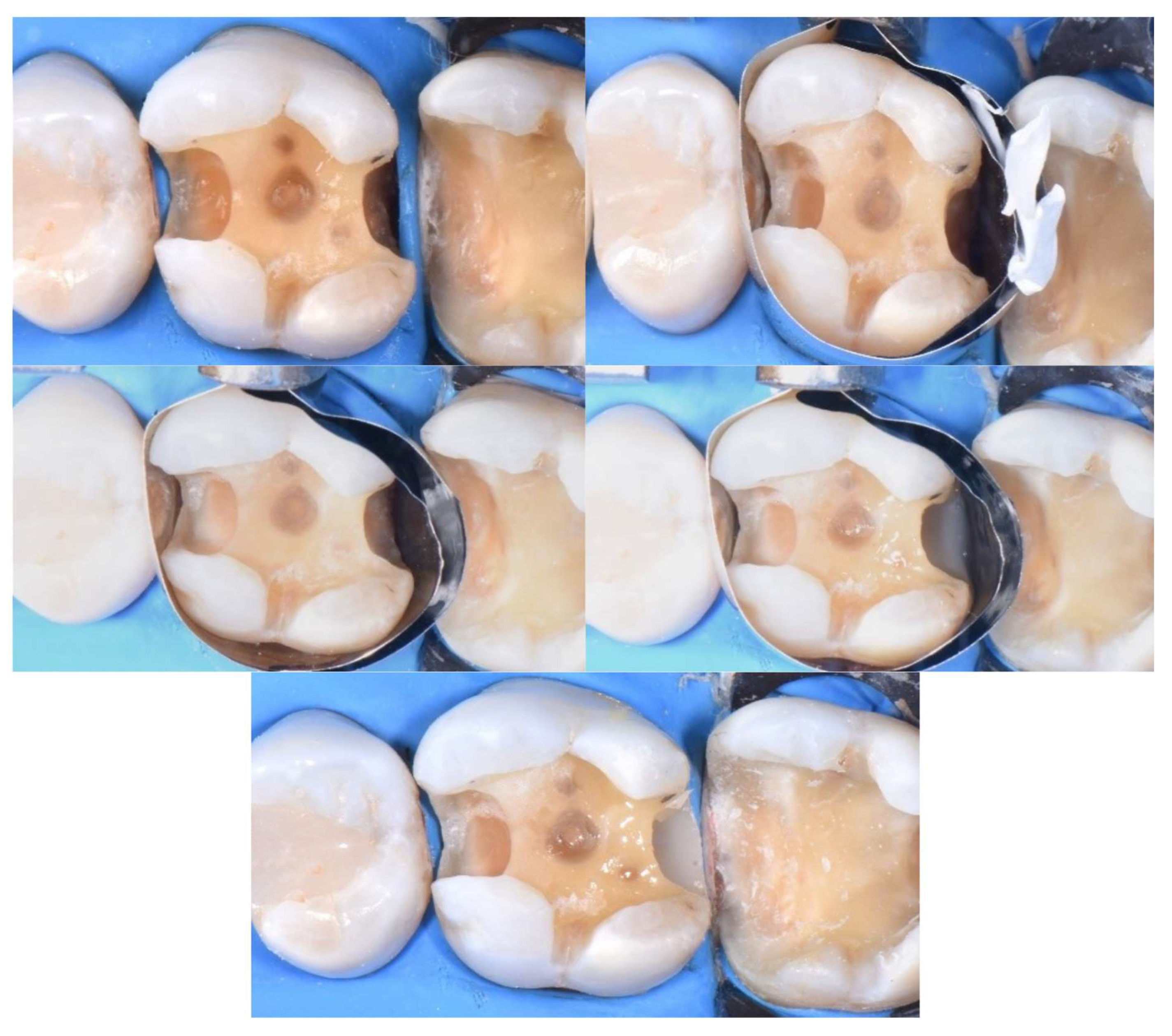
Figure 5.
Snowplow technique for DME: A thin layer (1 mm) of flowable composite is applied to the margin, followed by an increment of condensable composite resin, which is then directed toward the margin and polymerized simultaneously with the flowable layer.
Figure 5.
Snowplow technique for DME: A thin layer (1 mm) of flowable composite is applied to the margin, followed by an increment of condensable composite resin, which is then directed toward the margin and polymerized simultaneously with the flowable layer.
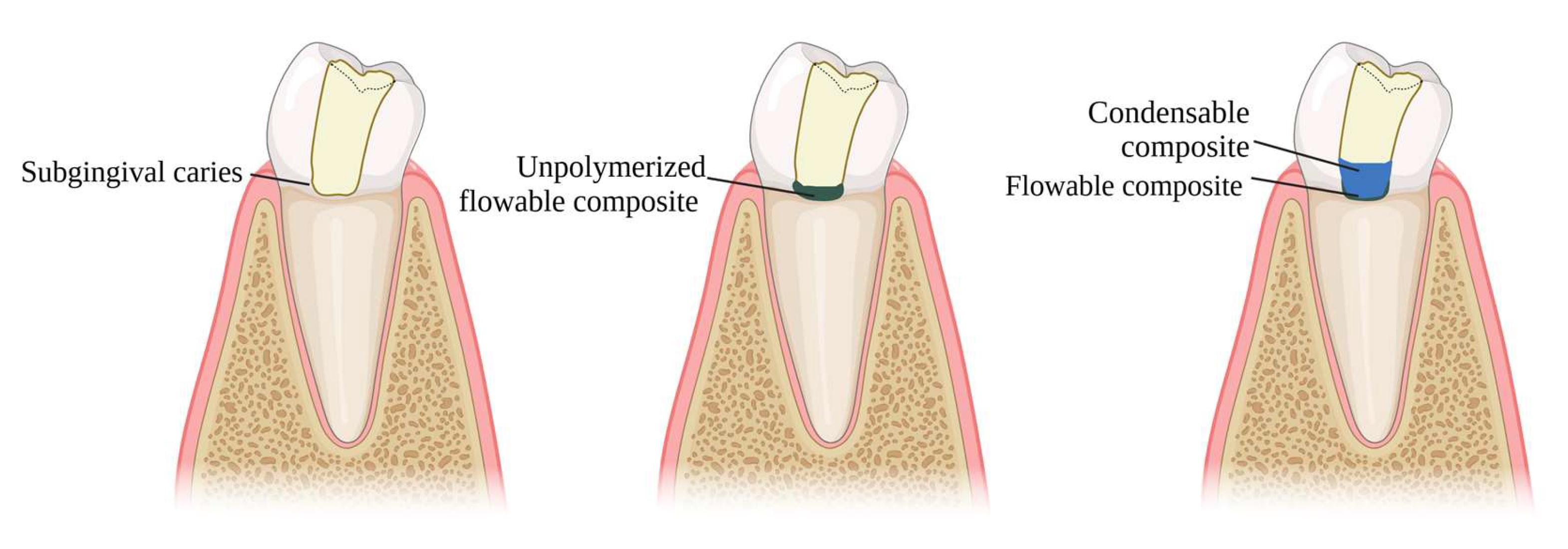
Figure 7.
DME with open flap.
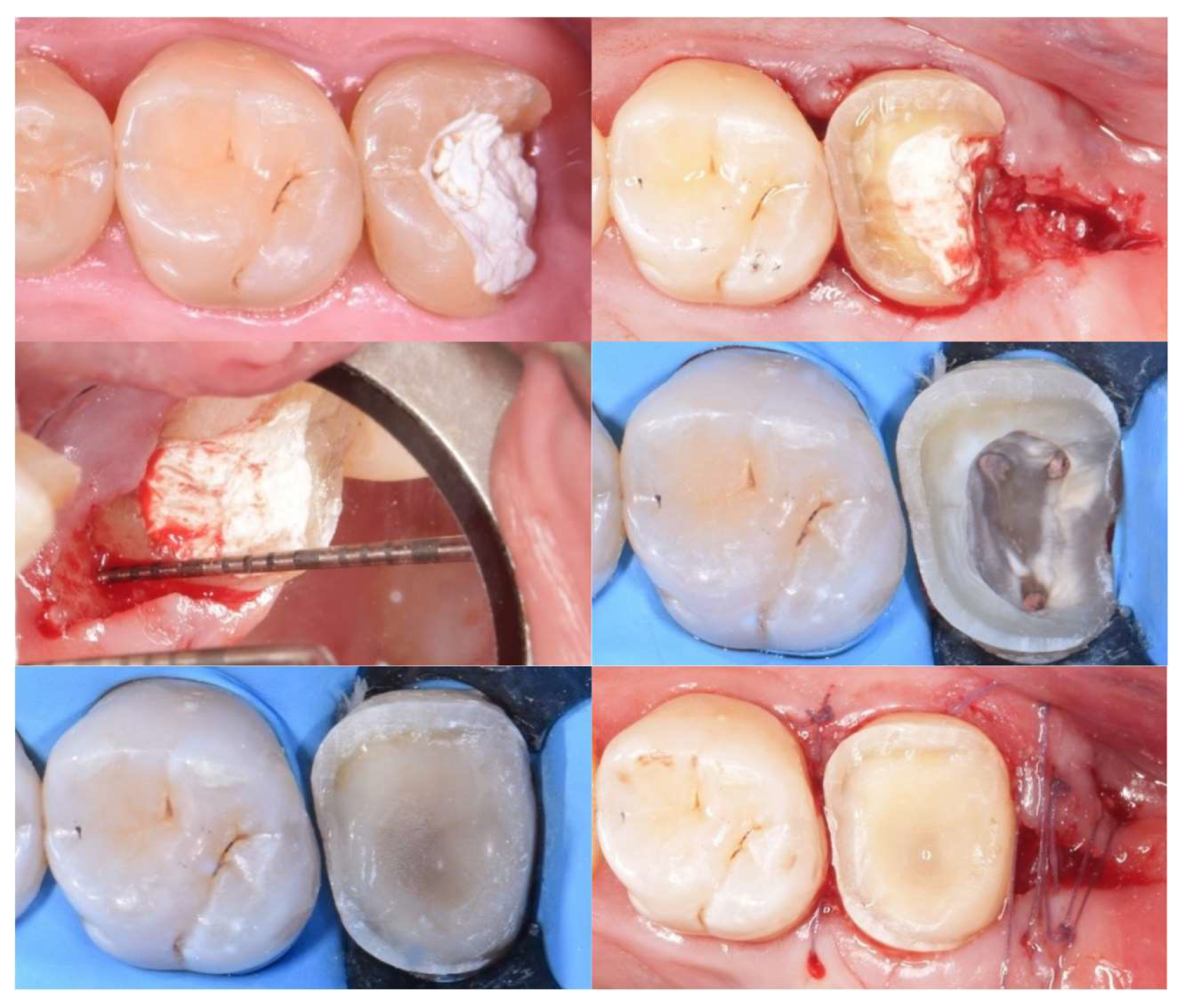
Figure 8.
Left: Subgingival caries in mesial surface of maxillary second molar. Right: Proper emergence profile after DME.
Figure 8.
Left: Subgingival caries in mesial surface of maxillary second molar. Right: Proper emergence profile after DME.
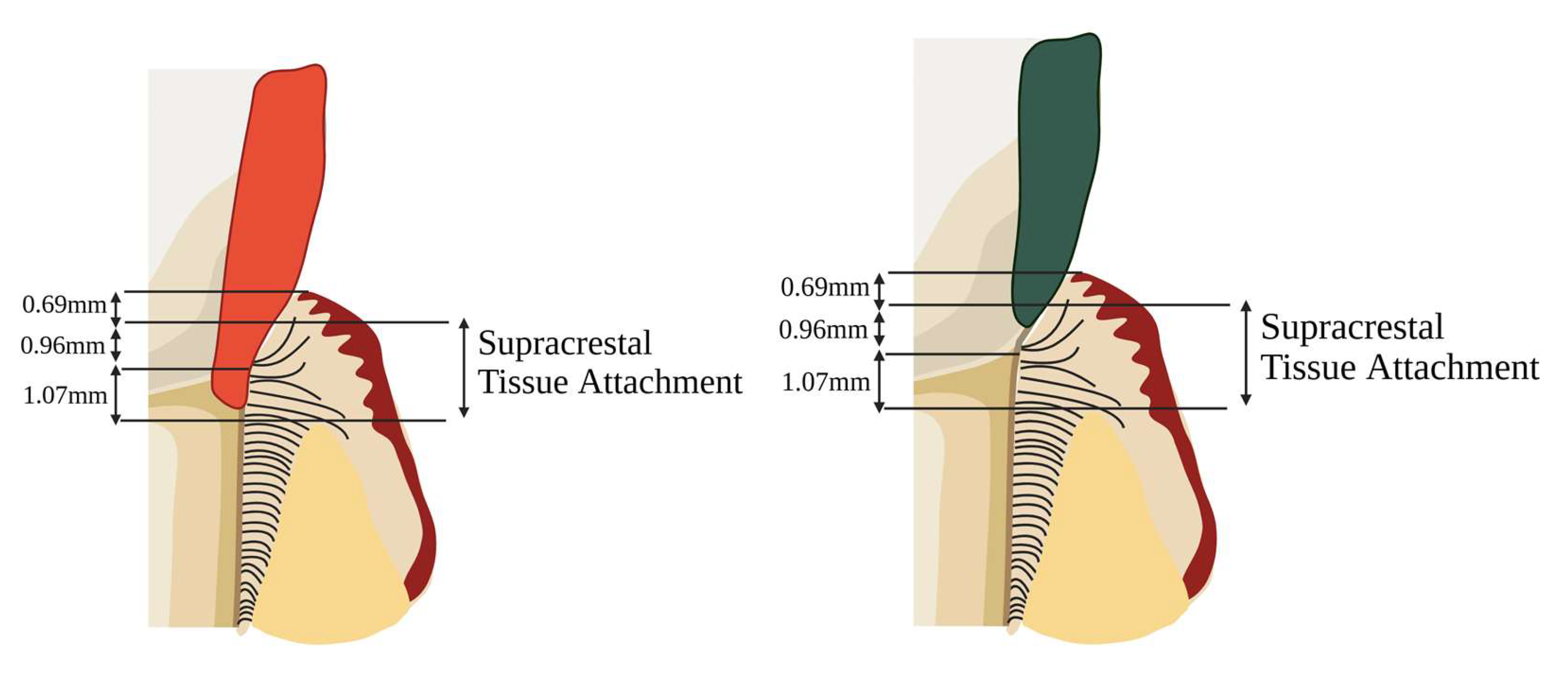
Figure 9.
Left: Subgingival margin with minor STA violation. DME can be tolerated in such cases. Right: Subgingival margin with deep STA violation. In such cases, crown lengthening should be considered.
Figure 9.
Left: Subgingival margin with minor STA violation. DME can be tolerated in such cases. Right: Subgingival margin with deep STA violation. In such cases, crown lengthening should be considered.

Figure 10.
Proper emergence profile of the intermediate layer allows for a tight contact point, preventing material overhangs and ensuring periodontal health.
Figure 10.
Proper emergence profile of the intermediate layer allows for a tight contact point, preventing material overhangs and ensuring periodontal health.
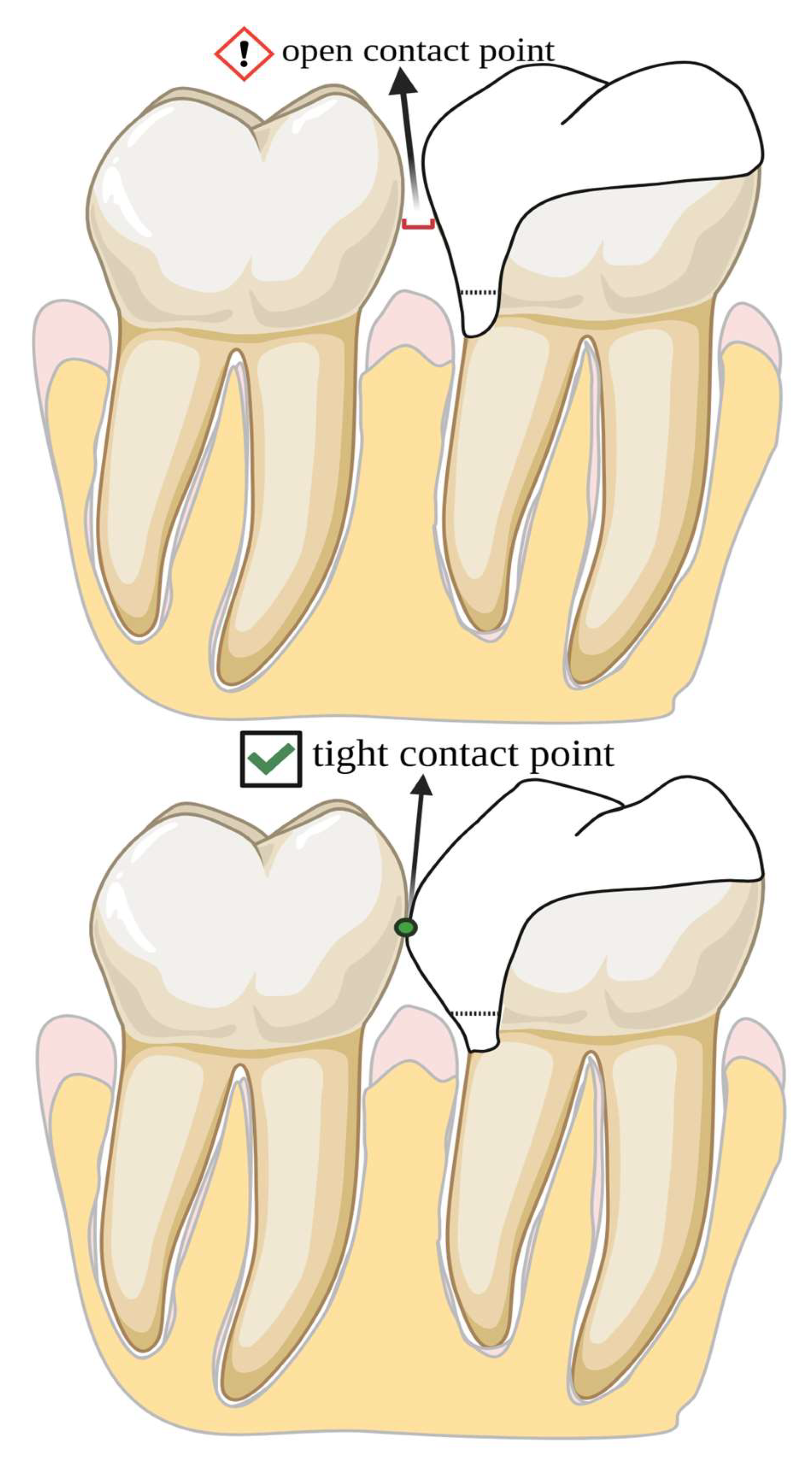
Figure 8.
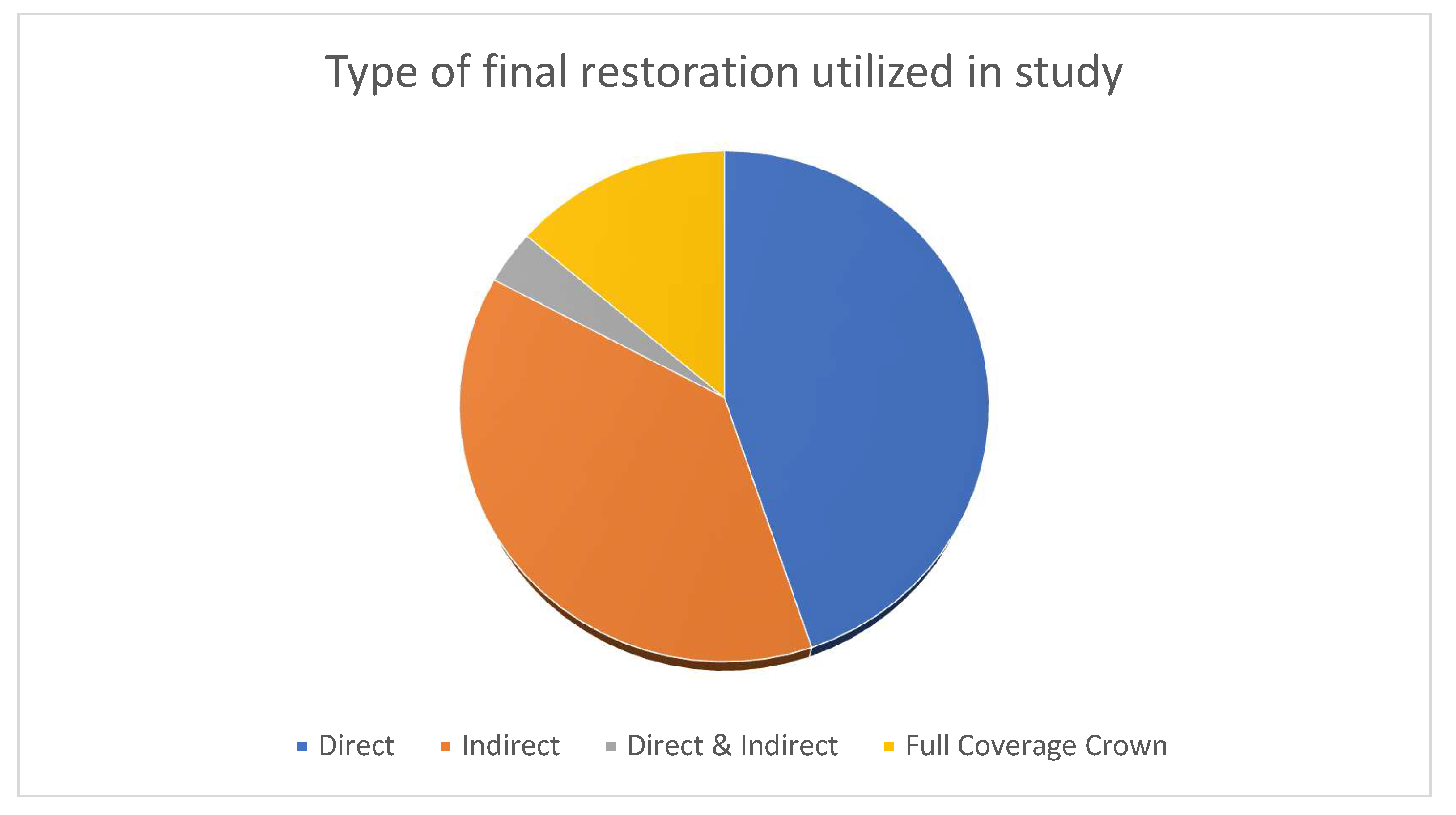
Table 3.
Periodontal Response
| Authors | Type of study | Means of evaluation | Results |
| Hausdörfer et al [45], 2024 | Prospective controlled clinical trial | Following DME combined with indirect restoration, periodontal response was assessed with BoP, PI, PPD with a follow-up of 1 year | Proximal boxes treated with DME were correlated with increased risk of gingival inflammation. |
| Felemban et al [5], 2023 | Systematic review | 68 articles were included | If the cervical margin is <2 mm from the bone crest, DME is contraindicated, and surgical crown lengthening (SCL) should be performed. |
| Ghezzi et al [46], 2019 | Case series | Periodontal response was assessed with BoP | When the supracrestal tissue attachment (STA) is respected (>2.04 mm from the bone crest), DME is compatible with periodontal health, with reduced bleeding on probing observed over 12 months. |
| Bertoldi et al [47], 2019 | Clinical study | Periodontal response was assessed with full-mouth plaque and bleeding score, focal probing depth. | The DME technique is compatible with periodontal health, at levels similar to intact tooth surfaces. |
| Ferrari et al [25], 2017 | Clinical study | Periodontal response was assessed with BoP, GI, and PI. | A flat contour of the intermediate layer after deep margin elevation (DME) has been associated with intense inflammatory infiltration and subsequent bone resorption, while clinical observations reported an increased incidence of bleeding on probing around DME-treated surfaces; however, although elevated bleeding on probing was also noted at 12 months post-treatment, no bone resorption was detected, likely due to the insufficient follow-up period. |
| Oppermann et al [48] | Clinical study | Periodontal response was assessed with BoP, GI, and PI. | It was observed that subgingivally placed restorations had comparable behavior to sites treated with crown lengthening. |
| Padbury et al [49], 2003 | Literature review | Periodontal response was assessed with BoP and probing depth. | Overextended material near soft tissues can severely compromise periodontal health. |
Table 4.
Failure Rate.
| Authors | Type of study | Type of failure | Results |
| Adson et al [56], 2024 | Retrospective clinical stydy | Failures included marginal integrity (n=1) | Out of 50 indirect partial restorations with DME, the 6-months survival rate was 98%. |
| Gözetici-Çil et al [57], 2024 | Retrospective clinical study | Failures included: partial loss (n=5), material chipping (n=4), secondary caries (n=1) | Out of 80 indirect partial composite restorations with DME, the 3-year survival rate was 93.8%. |
| Aziz et al [58], 2024 | Retrospective clinical study | Failures included: secondary caries (n=15), pulpal necrosis (n=4), crown fractures (n=4), loss of crown retention (n=3) | Out of 153 restorations with DME and CAD/CAM crowns, the 10-year survival rate was 95.8%, with no significant differences between groups with or without DME. |
| Muscholl et al [59], 2022 |
Retrospective clinical study | No failures were recorded. Periodontal parameters assessed included bleeding on probing, gingival bleeding index, and plaque control record. | Out of the 60 participants included, no failures were recorded in a follow-up range of 2.70 ± 1.90 years. |
| Bresser et al [50], 2019 | Retrospective clinical study | Failures included: secondary caries (n=5), pulpal necrosis (n=1), severe periodontal breakdown (n=1) and fracture (n=1) | Out of the 197 restorations with DME included, 8 failures occurred between 46-57 months. |
| Kuper et al [53], 2011 | Retrospective clinical study | Failures included: secondary caries (n=44), fracture tooth (n=6), fracture restoration (n=8), extraction (n=10), other/unknown (n=4) | Out of 344 composite restorations with margins apical to the CEJ, 72 failures were recorded, with no details provided on material selection or layering technique. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



