
Submitted:
01 May 2025
Posted:
05 May 2025
You are already at the latest version
Abstract
Background: Reproductive, maternal, newborn, and child health (RMNCH) remains a key priority for official development assistance and private voluntary assistance (ODA+) in low-income countries. In Guinea-Bissau, maternal and child mortality rates remain high, with the healthcare system heavily dependent on foreign aid. This study analyzes ODA+ trends for RMNCH in Guinea-Bissau from 2002 to 2018 and assesses its impact on maternal, neonatal, infant, and under-five mortality rates. Methods: We used data from the OECD Creditor Reporting System and applied the Muskoka2 methodology to estimate RMNCH-related disbursements. Funding trends were categorized by donor type and RMNCH subsectors. A longitudinal analysis used regression models to assess the relationship between aid categories and mortality outcomes. Results: RMNCH funding accounted for 8.9% of total ODA+ to Guinea-Bissau, with most aid directed toward child health. Models revealed a negative association between child health funding and under-five and infant mortality, while reproductive health funding showed no significant correlation with maternal or neonatal mortality. Conclusions: Although variable, ODA+ for RMNCH in Guinea-Bissau has helped reduce child mortality. However, maternal and neonatal mortality require targeted interventions and improved coordination. Fluctuating aid disbursements emphasize the need for sustainable health financing and stronger donor alignment with national priorities.
Keywords:
reproductive health
; maternal health
; newborn health
; child health
; foreign aid
; official development assistance
; private voluntary support
; Muskoka2 methodology
; Guinea-Bissau
; West Africa
1. Introduction
Reproductive, maternal, newborn, and child health (RMNCH) has deserved special attention from the international community over the years, being one of the prioritized areas for foreign aid, especially in low-income countries [1,2,3] . It played a central role in the Millennium Development Goals (MDGs) and remains crucial to the Sustainable Development Goals (SDGs), especially SDG 3.8 - which aims to achieve universal health coverage (UHC), including financial risk protection [4,5,6].
Foreign aid, as defined by the Organization for Economic Cooperation and Development (OECD), includes financial flows, technical assistance, and commodities intended to promote economic development and welfare [7]. It is typically provided as grants or subsidized loans [7] . Foreign aid comprises official development assistance (ODA), official assistance (OA), and private voluntary assistance (PVA), including contributions from non-governmental organizations and private entities [7,8] .
While foreign aid has played a positive role in global development [8,9,10], it has also been met with criticism, particularly in Africa, where weak institutions and unstable governance have raised questions about its effectiveness [11,12] . In the health sector, the impact of foreign aid remains debated [13,14]. Some studies highlight its success in addressing specific health challenges—such as reducing malaria, HIV, and tuberculosis and improving maternal and child mortality rates( [15,16,17,18] . Others suggest that foreign aid has little to no effect on broader health outcomes, particularly in reducing child mortality [19,20]. Some aid critics argue that while health aid has caused measurable improvements in health outcomes, the frequency of poor implementation and lack of donor coordination has often led to duplicate efforts and corruption, causing aid funds to disappear [18,21] , thus, suggesting that factors—such as domestic health expenditures, economic growth, and governance quality—are the key drivers of improvements in health outcomes [18,22,23].
Motivations for foreign aid vary widely, ranging from geopolitical and economic interests to philanthropic and humanitarian goals [10,24,25,26]. Some authors argue that while development-oriented assistance is often channeled through multilateral institutions, bilateral aid is frequently aligned with donor countries’ strategic priorities, concentrating on nations of geopolitical significance [27,28,29] .
Guinea-Bissau, a West African nation with a population of 2.15 million [30] , ranks among the poorest in the world, with a per capita GDP of $1,880 (PPP, 2017) and a Human Development Index (HDI) of 0.483, placing it 179th out of 193 countries [31] . Since gaining independence from Portugal in 1974, Guinea-Bissau has experienced persistent political instability, including multiple coups d’état, weak institutions, and its emergence as a hub for international drug trafficking [32,33,34,35] .
As a fragile context, Guinea-Bissau relies heavily on foreign aid to sustain its healthcare system and provide essential services. Despite some progress, maternal and child health indicators remain concerning [36] . The country failed to meet the Millennium Development Goals (MDGs) - MDG 4 (reducing child mortality by two-thirds) and MDG 5 (reducing maternal mortality by three-quarters) by 2015 [36]. Between 2002 and 2018, domestic general government health expenditure remained consistently low, accounting for 0.4% to 0.6% of Gross Domestic Product (GDP) [36,37] .
Few studies [38,39] have been conducted on official development assistance in conflict-affected countries (including Guinea-Bissau), but they were primarily focused on tracking reproductive health activities to which such support was allocated or assessing the link between development assistance for health and disease burden. With limited evidence available on this topic, this study aims to examine Official Development Assistance and Private Voluntary Assistance (ODA+) trends for RMNCH in Guinea-Bissau from 2002 to 2018 and evaluate their impact on maternal, neonatal, infant, and under-five mortality rates.
2. Materials and Methods
2.1. Study design
We analyzed ODA+ disbursement data from all donors reporting aid disbursements to the Creditor Reporting System (CRS) of the Organization for Economic Cooperation (OECD) and Development as of May 6, 2021.
2.2. Data gathering
We gathered ODA+ disbursement data from all donors reporting aid disbursements to the creditor reporting system (CRS) of the Organization for Economic Cooperation and Development (OECD). The Creditor Reporting System was established in 1973 by the OECD to collect information on individual aid loans and, later, grants, complementing the recording of aggregate flows of ODA [40] . This dataset included 148 donors (55 bilateral, 65 multilateral, and 28 private donors) covering 2002–2018. Data from the Muskoka2 initiative was also incorporated [41,42] . Muskoka2 consists of an automated algorithm applied to aid data reported to the OECD’s CRS aid activities database, which estimates the monetary value of funding that directly influences RMNCH outcomes globally, by year, by recipient country, and by the donor, rather than only funding earmarked for RMNCH, including funding targeted at specific diseases, such as HIV and malaria, health system strengthening, water and sanitation sector and shares of funding for the humanitarian sector [41].
2.3. Data disbursement classification
In line with the OECD definitions (OECD, 2019), disbursements were categorized based on donor type. Specifically, we classified disbursements into three main categories: (1) bilateral aid from individual countries, (2) multilateral aid from international institutions, including Global Health Initiatives, and (3) private voluntary assistance from non-governmental organizations, religious groups, charities, foundations, and private companies. Our analysis focused on disbursements that the OECD identifies as most accurately reflecting actual international transfers of financial resources, goods, or services [7].
2.4. Data estimations and coding
We applied the Muskoka2 methodology [41,42] to the CRS database to estimate RMNCH disbursements to Guinea-Bissau from 2002 to 2018.
RMNCH disbursements include activities that improve access for women and children to integrated health interventions, strengthen health systems, and build RMNCH-specific workforce capacity [43]. Expenditures were categorized as follows:
- Reproductive Health (RH): Activities focused on reproductive and sexual health for non-pregnant women, including family planning and population policies [41,44].
- Maternal and Neonatal Health (MNH): Interventions focused on the health of pregnant women and their newborns during pregnancy, childbirth, and the one-month postnatal period [41,45].
- Child Health (CH): Activities aimed at improving children’s health from one month to five years [41,45].
Additional funding categories, such as health system strengthening, general healthcare, humanitarian health, and condition-specific funding (e.g., HIV/AIDS, malaria), were proportionally allocated to RMNCH based on CRS purpose codes and refined using data on disease burden, demographics, and government health expenditure [41,46,47]. Percentages (0–100%) were assigned to CRS disbursements by purpose code, with 25 out of 223 codes identified as contributing to RMNCH [41] (Supplementary Tables A1, A2, and A3).
In this study, ODA+ for the Health Sector (HS) was defined as the sum of categories I.2 (Health, Total) and I.3 (Population Policies/ Programmes & Reproductive Health) from the CRS database [48] and ODA+ to all sectors (AS) represents the total ODA+ to Guinea-Bissau.
2.5. Data categorization and Study variables
Data categorization
Annual RMNCH assistance was disaggregated by donor type (bilateral, multilateral, private) and RMNCH category (RH, MNH, CH) for 2002–2018. Disbursement data are presented, unless otherwise specified, in constant 2018 US dollars using the Development Assistance Committee deflators, with data management performed in Microsoft Excel (version 16) [49].
Study variables
We used four mortality rates as dependent variables to assess the effectiveness of aid: 1) Neonatal mortality rate -deaths per 1,000 live births during the first 28 days of life, 2) Infant mortality rate -deaths per 1,000 live births of children under one year of age; 3) Under-five mortality rate -deaths per 1,000 live births of children under five and 4) Maternal mortality rate - deaths per 100,000 live births due to complications of pregnancy or childbirth [37,50]. These indicators represent specific demographic groups and health outcomes related to maternal and reproductive health, childbirth, and child growth and were sourced from the World Development Indicators Database [37] .
Based on current literature, we incorporated several control variables known to influence mortality rates, including Gross Domestic Product (GDP) per capita, life expectancy at birth, sanitation rate, fertility rate, use of modern contraceptives, and vaccination coverage against measles and Diphtheria, Tetanus, and Pertussis (DTP) [30,37,51]. More details on these variables are available in Supplementary Table A4.
Primary independent variables included four ODA+ categories: RMNCH, CH, RH, and MNH, along with an additional category, HS (Figure 1). This study controlled RMNCH, CH, and MNH variables using GDP per capita, life expectancy, sanitation rate, and vaccination coverage (measles and DTP). Meanwhile, RH was controlled using GDP per capita (PPP), fertility rate, and the prevalence of modern contraceptive use. HS was controlled using GDP per capita, life expectancy, sanitation rate, vaccination coverage (measles and DTP), and fertility rate.
Figure A1.
Primary independent variables.
2.6. Data modelling and analysis
2.6.1. Study hypothesis
The hypothesis proposed in this study is that Official Development Assistance and private voluntary assistance (ODA +) significantly predict maternal, newborn, infant, and under-five mortality rates, with an expected negative correlation between aid disbursements and mortality rates.
2.6.2. Model development
We designed a quasi-experimental longitudinal analysis [52,53], developing fifteen models after excluding control variables exhibiting multicollinearity (Supplementary Table A5).
Each model assessed the relationship between a specific independent variable and a health-related mortality outcome, controlling for relevant covariates. Model 1 examined newborn mortality as the dependent variable and HS (Health-sector-specific ODA+) as the independent variable. Control variables included GDP per capita, DTP and measles coverage, life expectancy, sanitation, and fertility rate. Model 2 included infant mortality as the dependent variable and HS as the independent variable. Control variables included GDP per capita, DTP and measles coverage, life expectancy, and sanitation. Model 3 used under-5 mortality as the dependent variable, with HS as the independent variable, and control variables remained the same as in Model 2. Model 4 examined maternal mortality as the dependent variable, with HS as the independent variable, and the control variables were GDP per capita and fertility rate. Model 5 included newborn mortality as the dependent variable, RMNCH as the independent variable, and retained control variables from Model 1. Model 6 used infant mortality as the dependent variable and retained RMNCH as the independent variable and control variables from Model 2. Model 7 included under-5 mortality as the dependent variable, retained RMNCH as the independent variable, and control variables were the same as those applied in Model 3. Model 8 examined maternal mortality as the dependent variable, retained RMNCH as the independent variable and control variables were the same as those applied in Model 4. Model 9 included newborn mortality as the dependent variable, retained CH as the independent variable, and control variables from Model 1. Model 10 used infant mortality as the dependent variable, retained CH as the independent variable, and control variables from Model 2. Model 11 included under-5 mortality as the dependent variable, retained CH as the independent variable, and control variables from Model 3. Model 12 included newborn mortality as the dependent variable, retained RH as the independent variable, and control variables from Model 1. Model 13 examined maternal mortality as the dependent variable, retained RH as the independent variable, and the control variables were the same as in Model 4. Model 14 included newborn mortality as the dependent variable, retained MNH as the independent variable, and control variables from Model 1. Model 15 included maternal mortality as the dependent variable, retained MNH as the independent variable, and control variables were the same as those applied in Model 4.
2.6.3. Data analysis
Multiple regression analysis was performed to assess this relationship, focusing on the β2 coefficient to measure the impact of ODA+ on mortality rates. Several statistical tests were conducted to validate the linear regression assumptions, including a correlation matrix to identify multicollinearity, the Breusch-Pagan/Cook-Weisberg test for homoscedasticity, the Breusch-Godfrey LM test for autocorrelation, and the Shapiro-Wilk W test to assess the distribution type. Multicollinearity was addressed by excluding all control variables except GDP per capita. Quadratic terms were introduced in the eighth, ninth, and eleventh models to address the non-linear effects identified. Homoscedasticity was not observed in any model, and a non-normal distribution was identified in the ninth model. All variables were logarithmically transformed to interpret regression coefficients as percentages. A significance level of α=0.05 was applied. Data analysis was conducted using Stata Statistical Software [54] .
3. Results
3.1. Flows of ODA+ Funding in Guinea-Bissau
Between 2002 and 2018, Guinea-Bissau received ODA+ disbursements totaling approximately $2.3 billion across various sectors, including social and economic infrastructure, production, commodity aid, and humanitarian assistance. These disbursements represented between 7.6% and 26.7% of the country’s Gross National Income (GNI). During this period, a total of $364 million was allocated to the health sector, encompassing health and population policies as well as reproductive health. This accounted for 16.4% of total ODA+, translating to $6.6 and $23.6 per capita. Of this health sector funding, $197.4 million (8.9% of total ODA+) was directed to Reproductive, Maternal, Newborn, and Child Health (RMNCH) activities. RMNCH funding experienced a 237% increase, rising from $4.1 million in 2002 to $13.8 million in 2018, significantly outpacing the 101% growth in overall ODA+. The average annual growth rates for total ODA+ and RMNCH-specific funding were 15.8% and 14.8%, respectively. Overall, total ODA+, health sector aid, and RMNCH-specific funding financing patterns varied throughout the study period (Table A1).

Table A1.
Descriptive statistics of the sample for the period 2002–2018.
| Dependent variables | Min. | Mean | Median | Máx. | SD | Annual Average Trend | N |
|---|---|---|---|---|---|---|---|
| Neonatal mortality | 36.70 | 45.08 | 45,10 | 53.20 | 5.58 | ↓ 2.29 % | 17 |
| Infant mortality | 54,60 | 74.48 | 72.60 | 99.50 | 14.72 | ↓ 3.68 % | 17 |
| Under-five mortality | 82.40 | 118.01 | 114.40 | 163.40 | 26.50 | ↓ 4.19 % | 17 |
| Maternal mortality | 648.00 | 830.59 | 795.00 | 1136.00 | 145.23 | ↓ 3.38 % | 17 |
| Funding (US $, Millions, 2018) | |||||||
| ODA+ all sectors | 77.27 | 130.74 | 113.07 | 273.83 | 50.56 | ↑15.84% | 17 |
| ODA+ Health | 8.71 | 21.43 | 19.89 | 40.15 | 31.44 | ↑ 13.83 % | 17 |
| ODA+ RMNCH | 4.10 | 11.61 | 10.89 | 23.69 | 5.78 | ↑ 14.83% | 17 |
| ODA+ CH | 1.90 | 6.51 | 4.94 | 15.10 | 3.84 | ↑ 23.46 % | 17 |
| ODA+ RH | 0.53 | 1.94 | 1.50 | 4.77 | 1.40 | ↑ 33.18% | 17 |
| ODA+ MNH | 1.34 | 3.17 | 2.53 | 8.03 | 1.87 | ↑ 17.24% | 17 |
| Control variables | |||||||
| GDP per capita | 1600.65 | 1703.08 | 1690.09 | 1872.31 | 84.58 | ↑ 0.83 | 17 |
| Average life expectancy at birth | 50.98 | 55.98 | 56.23 | 60.50 | 3.19 | ↑ 1.08 | 17 |
| Basic sanitation rate (%) | 3.01 | 7.88 | 7.80 | 3.20 | 13.03 | ↑ 11.11 | 17 |
| Fertility rate | 4.26 | 5.61 | 5.06 | 5.06 | 0.42 | ↓1.70 | 17 |
| Modern contraception (%) | 0.059 | 0.098 | 0.094 | 0.154 | 0.031 | ↑ 6.20 | 17 |
| Measles vaccination (%) | 66.00 | 76.00 | 76.00 | 83.00 | 4.78 | ↑ 0.78 | 17 |
| DTP vaccination coverage (%) | 57.00 | 77.18 | 80.00 | 87.00 | 9.89 | ↑ 2.36 | 17 |
Abbreviations: DTP-diphtheria, tetanus and polio; SD - standard deviation; ODA+ - Official Development Assistance and Private Voluntary Assistance; RMNCH – Reproductive, Maternal, Neonatal, and Child Health; CH - Child Health; RH - Reproductive Health; MNH - Maternal and neonatal health; GDP per capita – gross domestic product per capita (PPP (constant 2017 international $); Neonatal mortality: deaths per 1,000 live births during the first 28 days of life; Under-five mortality: deaths per 1,000 live births of children under five; Infant Mortality: deaths per 1. 000 live births of children under one year of age; Maternal mortality: number of maternal deaths per 100,000 live births due to complications of pregnancy or childbirth; Fertility rate, total: births per woman. Sources: [37,41,42,48].
3.2. Donor Variability and Growth Rates
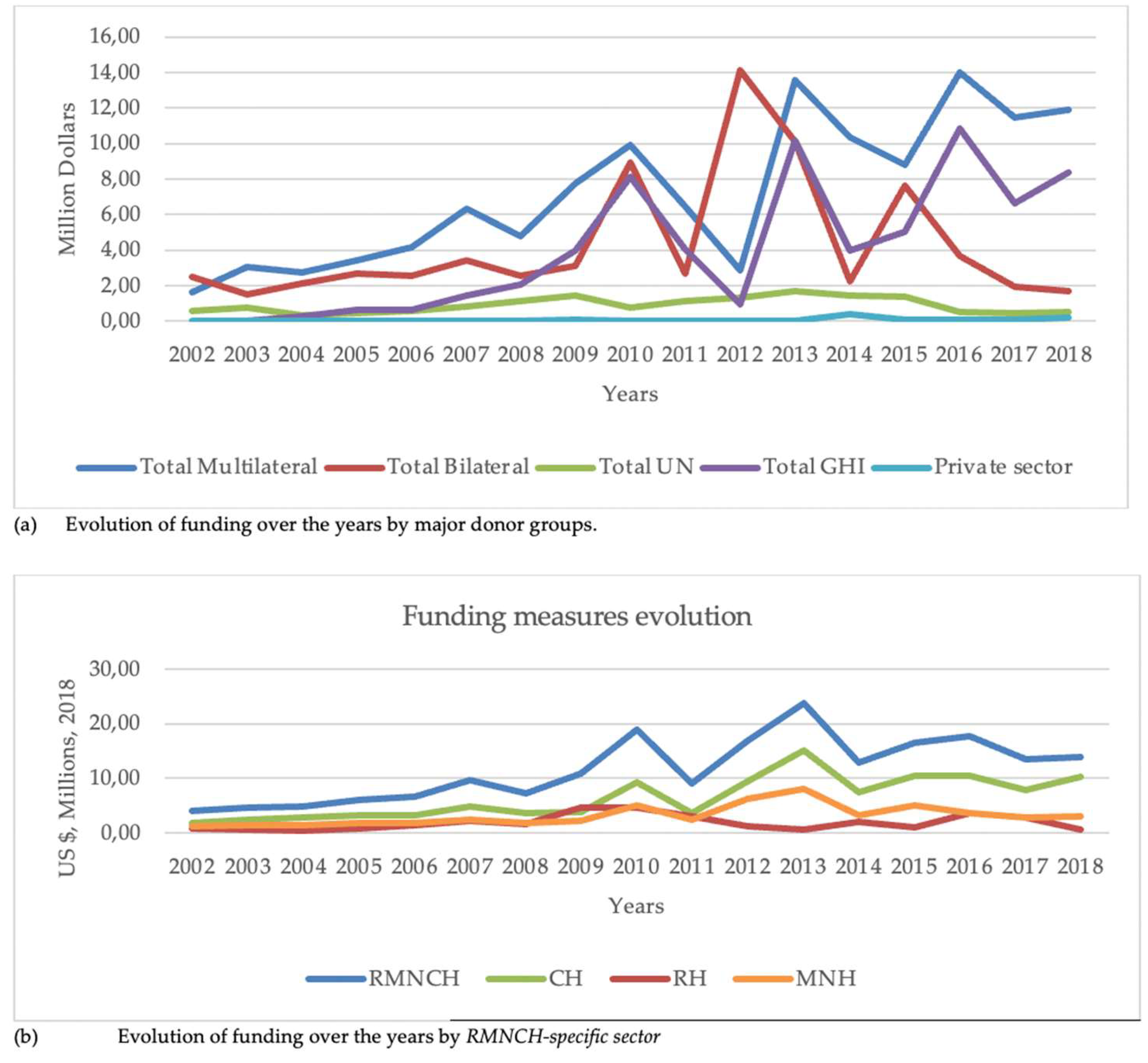
Funding patterns from different donors exhibited significant variability over the years (Figure A2; Supplementary Figure A1). The largest bilateral and multilateral donors were the USA (17.4%; $34.4 million), Portugal (11,3 %; $22.4 million) and the International Development Association (6%; $11.8 million), while the only private donor was the Bill & Melinda Gates Foundation (0.5%; $0.99 million). Among major donor groups, Global Health Initiatives, particularly the Global Fund, recorded the highest average annual growth rate (102.2% in 2004–2018), followed by bilateral donors, with an annual growth rate of 38.7%.
Figure A2.
Evolution of funding over the years by major donor groups (a) and RMNCH-specific sector (b). Abbreviations: UN- United Nations; GHI- Global Health Initiatives; RMNCH – Reproductive, Maternal, Neonatal, and Child Health; CH - Child Health; RH - Reproductive Health; MNH - Maternal and neonatal health.
Figure A2.
Evolution of funding over the years by major donor groups (a) and RMNCH-specific sector (b). Abbreviations: UN- United Nations; GHI- Global Health Initiatives; RMNCH – Reproductive, Maternal, Neonatal, and Child Health; CH - Child Health; RH - Reproductive Health; MNH - Maternal and neonatal health.
3. RMNCH-specific Funding Allocation
RMNCH-specific funding was primarily directed to child health (56.0%; $110.6 million), followed by maternal and neonatal health (27.3%; $53.9 million) and reproductive health (16.7%; $32.9 million). Multilateral donors provided most of the funding (62.4%; $123.1 million), with bilateral donors contributing 37.1% ($73.3 million) and the private sector 0.5% ($0.99 million). The top donors included the Global Fund ($55.4 million), the United States of America (USA) ($34.4 million), Portugal ($22.4 million), European Union (EU) Institutions ($18.5 million), and the International Development Association ($11.8 million) (Supplementary Figure A1).
3.4. Child Health Funding
Child health support received substantial contributions from key donors, including the Global Fund (25.0% of total child health aid, $27.7 million), the USA (19.5%; $21.6 million), EU Institutions (11.4%; $12.6 million), Portugal (10.7%; $11.8 million), and the Global Alliance for Vaccines and Immunization (GAVI) (10.3%; $11.4 million). Funding primarily targeted three key areas: basic healthcare (21.9%; $24.2 million), which included primary healthcare programs, paramedical and nursing care, and essential medicines and vaccines; malaria control and prevention (20.9; $23.1 million); and basic nutrition (20%; $22.1 million).
3.5. Maternal and Neonatal Health Funding
Maternal and neonatal health funding was predominantly supported by the USA (23.0%, $12.4 million), the Global Fund (19.5%, $10.5 million), and Portugal (16.6%, $9.0 million). Focus areas included basic nutrition (25.1%; $13.5 million), malaria control ($10.32 million, 19.1%), and reproductive healthcare ($7.05 million, 13.1%).
3.6. Reproductive Health Funding
Reproductive health funding was primarily supported by the Global Fund (52.4%, $17.3 million), Spain (8.5%, $2.8 million), and EU Institutions (6.7%, $2.2 million). Most of the funding was allocated to sexually transmitted diseases (STD) and HIV control (71.0%; $23.4 million), followed by general budget support (8.9%; $2.9 million) and reproductive healthcare (6.2%; $2.1 million). The reproductive healthcare allocation covered initiatives of RH according to OECD [43], such as reproductive health promotion, prenatal and postnatal care (including delivery), infertility prevention and treatment, as well as the prevention and management of abortion-related complications and safe motherhood programs.
3.7. ODA+ Funding Allocation
Most ODA+ funding for RMNCH—totaling $192.5 million (97.5%)—was allocated to health and population sectors, water and sanitation, and humanitarian initiatives during this period. Only a small portion, $5 million (2.5%), was designated for general budget support. Among RMNCH support categories, basic nutrition received the largest share at 18.1% ($35.8 million), followed closely by malaria prevention and control at 16.9% ($33.4 million), basic healthcare at 14.5% ($28.7 million), sexually transmitted disease (STD) and HIV control at 12.1% ($23.9 million), and medical services at 9.0% ($17.8 million).
3.8. Funding and Mortality Trends
Table A2 and Table A3 illustrates trends in mortality rates and funding measures over the study period. While all mortality rates declined, maternal mortality showed an exception in 2017 (Table A3). The most substantial reductions occurred during the first decade of the study, with annual declines surpassing the average annual reduction (Table A3).
Despite overall growth in aid measures, certain years saw reductions in financial assistance, particularly in the RH aid category. Nevertheless, RH aid exhibited the highest average annual increase among all aid measures, rising by 33.18% per year.
Table A3.
Trends in funding measures 2002-.
| Year | RMNCH | AAGR (%) | RH | AAGR (%) | CH | AAGR (%) | MNH | AAGR (%) |
|---|---|---|---|---|---|---|---|---|
| 2002 | 4.1 | 0.9 | 1.9 | 1.3 | ||||
| 2003 | 4.6 | 11.4 | 0.7 | 22.8 | 2.5 | 29.9 | 1.4 | 7.2 |
| 2004 | 4.8 | 5.7 | 0.5 | 21.2 | 2.9 | 15.5 | 1.5 | 1.3 |
| 2005 | 6.1 | 25.6 | 0.9 | 73.9 | 3.3 | 15.4 | 1.9 | 28.0 |
| 2006 | 6.7 | 10.3 | 1.5 | 63.8 | 3.3 | 0.7 | 1.9 | 0.8 |
| 2007 | 9.7 | 45.6 | 2.3 | 50.8 | 5.0 | 49.5 | 2.5 | 34.5 |
| 2008 | 7.3 | 24.9 | 1.7 | 25.2 | 3.7 | 24.7 | 1.9 | 25.0 |
| 2009 | 10.9 | 48.9 | 4.8 | 181.7 | 3.9 | 4.4 | 2.2 | 17.7 |
| 2010 | 18.9 | 73.2 | 4.6 | 3.1 | 9.3 | 137.9 | 5.0 | 123.5 |
| 2011 | 9.2 | 51.5 | 3.0 | 34.4 | 3.8 | 59.4 | 2.4 | 52.6 |
| 2012 | 17.0 | 85.5 | 1.3 | 58.5 | 9.5 | 153.8 | 6.2 | 161.5 |
| 2013 | 23.7 | 39.6 | 0.6 | 54.7 | 15.1 | 58.7 | 8.0 | 29.3 |
| 2014 | 13.0 | 45.4 | 2.1 | 264.0 | 7.6 | 49.9 | 3.3 | 58.7 |
| 2015 | 16.6 | 27.8 | 1.0 | 51.7 | 10.6 | 39.8 | 5.0 | 50.1 |
| 2016 | 17.7 | 7.1 | 3.7 | 268.7 | 10.5 | 0.9 | 3.6 | 28.5 |
| 2017 | 13.5 | 23.6 | 2.9 | 21.4 | 7.9 | 24.8 | 2.8 | 22.5 |
| 2018 | 13.8 | 2.0 | 0.6 | 79.0 | 10.2 | 29.5 | 3.0 | 9.0 |
Abbreviations: AAGR - Average annual growth rate; AARR - Average Annual Rate of Reduction; RMNCH – Reproductive, Maternal, Neonatal, and Child Health; CH - Child Health; RH - Reproductive Health; MNH - Maternal and neonatal health.
3.9. Aid measures and Mortality rate Associations
Regression models demonstrated a negative association between aid measures and corresponding mortality rates, except for ODA+ for reproductive health (RH), which showed no correlation with neonatal and maternal mortality. GDP per capita emerged as the most influential control variable, consistently predicting significant reductions in mortality rates across all models. Regarding ODA+ to all sectors, no significant correlation was found with any of the mortality rates (p > 0.05). Health-sector-specific ODA+ and GDP per capita explained 88.0%–93.0% of the decrease in mortality rates, particularly for infant and under-five mortality (Models 1–4). Similarly, RMNCH funding, combined with GDP per capita, explained 89.0%–93.0% of the reductions in mortality rates (Models 5–8).
Models 9–11 demonstrated that funding for Child Health (CH), combined with GDP per capita, explained 94.0% of the reductions in neonatal, infant, and under-five mortality rates. A 1.0% increase in Child Health funding was associated with decreases of 0.16% in infant mortality and 0.17% in under-five mortality. However, the impact on neonatal mortality was less pronounced, showing a less favorable regression coefficient. Although Reproductive Health (RH) funding experienced substantial financial growth, no correlation with neonatal or maternal mortality was observed (Models 12–13) (p > 0.05). Models 14–15 showed that Maternal and Newborn Health (MNH) funding and GDP per capita explained 81.0% and 93.0% of the reductions in neonatal and maternal mortality rates, respectively, with a less favorable regression coefficient for neonatal mortality (Table A2 and Table A3).
4. Discussion
Our study presents a comprehensive analysis of Official Development Assistance (ODA+) disbursements for Reproductive, Maternal, Newborn, and Child Health (RMNCH) and their impact on maternal, neonatal, infant, and under-five mortality rates in Guinea-Bissau from 2002 to 2018. Our findings highlight significant financial contributions to RMNCH, with notable increases in child health funding and strong donor participation. However, aid effectiveness varied across categories, with reproductive health (RH) funding showing no significant impact on neonatal and maternal mortality reductions over time. Some authors [55] suggest that higher public spending improves healthcare for pregnant women, thereby reducing maternal mortality rates. Foreign aid might not increase public expenditure in the health sector, such as expanding the healthcare ecosystem and care networks. As a result, financial bottlenecks persist, preventing improvements for these women [55,56].
Trends RMNCH Funding
Between 2002 and 2018, donors prioritized the reproductive, maternal, newborn, and child health (RMNCH) sectors within the broader context of overall ODA+. The increase in ODA+ funding for RMNCH mirrored the growth in ODA+ across all sectors during this period. This trend reflects global efforts to improve maternal, neonatal, and child health outcomes through concerted donor support and health systems strengthening [57,58,59,60,61] . In the same period under analysis, children aged between 1 month and five years benefited from more than half of the funding for reproductive, maternal, newborn, and child health due to increased funding from donors to immunization projects and malaria control programs, as observed in other studies [62,63] .
RMNCH Funding and Mortality rates
Our regression models demonstrated a strong negative association between CH funding and infant and under-five mortality rates, suggesting that targeted investments in child health interventions significantly contributed to mortality reduction in Guinea-Bissau. Funding directed at child health demonstrated the strongest associations, explaining 94.0% of reductions in neonatal, infant, and under-five mortality combined with GDP per capita. This highlights the effectiveness of investments in primary healthcare, malaria prevention, and basic nutrition, which accounted for a significant share of child health funding. Similarly, maternal and newborn health (MHN) funding and GDP per capita explained 81.0% and 93.0% of the reduction in the neonatal and maternal mortality rate, respectively, with a less favorable regression coefficient for neonatal mortality in Guinea-Bissau. In contrast, reproductive health (RH) funding showed the highest annual financial growth with no correlation with neonatal or maternal mortality reductions. This suggests potential inefficiencies in RH aid allocation, limitations in its short-term impact, or that funding levels remain insufficient to address the complex drivers of maternal and neonatal mortality. The lack of correlation may also stem from the nature of RH interventions, which primarily focus on long-term behavioral and systemic changes (such as contraception use and family planning policies) rather than immediate life-saving measures like emergency obstetric care, neonatal resuscitation, or treatment for severe pregnancy complications like eclampsia or hemorrhage [64,65] .
Donor Contributions and Funding Variability
Our findings revealed that multilateral donors were the primary contributors to RMNCH funding in Guinea-Bissau, accounting for 62.4%, while bilateral donors also played a significant role, contributing 37.1%. The growing involvement of Global Health Initiatives, including the Global Fund, in Guinea-Bissau since 2004 has influenced the funding trends. Notably, there has been a substantial increase in funding since 2009. Additionally, GAVI has played a significant role in financing projects to improve reproductive, maternal, newborn, and child health, a trend observed by other researchers [63,66]. Notably, private sector contributions were minimal, highlighting an opportunity to engage more non-state actors in health financing for Guinea-Bissau. Since 2009, private foundations, represented by the Bill and Melinda Gates Foundation, have provided a modest but steady share of RMNCH funding.
This study verified that donors maintained constant support for RMNCH despite the fragile context and periods of significant governance disruptions in Guinea-Bissau between 2002 and 2018 [32,33]. Our study revealed peaks in aid disbursements for RMNCH in 2007, 2010, 2014, and 2016. These years were marked by intense political and military instability in Guinea-Bissau. In 2007, the country witnessed the assassination of a high-ranking military officer and the passage of a no-confidence motion against the government. In 2010, a mutiny within the armed forces led to the arrest of the acting prime minister. The 2014 legislative and presidential elections were followed by institutional conflict between the presidency and the government. In 2016, a parliamentary censure motion against the government further deepened political strife. These surges in disbursement likely reflect the increased reliance on external aid during periods of significant domestic instability, when the state faced substantial constraints in fulfilling its financial responsibilities in the health sector.
Our findings reveal significant annual fluctuations in the disbursement of donor assistance across various areas, a trend observed in similar studies conducted in Kenya, Tanzania, Uganda, and Zambia [62,67]. This can be explained by multiple allocation policies of foreign donors and country-specific characteristics [68,69,70] .
Similarly, to previous studies [41], we observed that RMNCH funding was highly concentrated among a few donors, notably the Global Fund, USA, Portugal, EU Institutions, International Development Association, and GAVI. We also observed that the priority of funding was given to basic nutrition, malaria prevention, and control, and basic health before the control of sexually transmitted diseases, including HIV, which was reported as a priority area in other studies [63]. While significant, maternal and neonatal health funding appears to have less impact on neonatal mortality in Guinea-Bissau, suggesting that targeted interventions in this area require further strengthening. Investments in maternal nutrition, skilled birth attendance, and postnatal care should be prioritized to address persistent gaps.
Similarly, to previous studies [71,72] , the overwhelming focus of reproductive health funding on sexually transmitted diseases and HIV control (71.0% of total reproductive health aid) may have overshadowed other critical areas, such as safe motherhood initiatives and access to family planning services. Thus, balancing investments across these areas could enhance the overall impact of reproductive health aid. Almost all ODA+ to RMNCH in this period was channeled as projects rather than general budget support, as observed in other studies [62,63] , which displays a pattern of health financing that could raise questions about national ownership and long-term sustainability. The question of ownership was raised in the Paris Declaration, reinforced by the Accra Agenda in 2008 [73] and the Busan Partnership for Effective Development Cooperation in 2011, in which donors and partners were encouraged to adhere to the principles of national ownership of development strategies, alignment of aid with national priorities, harmonization of donor activities, focus on results, mutual accountability, predictability, and transparency [74]. This issue was reinforced by UHC 2030, which resulted from the transformation of the International Health Partnership + (IHP +), whose role in cooperation and national ownership was reaffirmed in the Political declaration of the high-level meeting on universal health coverage in 2019 [75]. Based on our data, considering the annual variations in funding and its distribution across different areas, it is unclear whether there is a real effort to harmonize priorities between the multiple donors and the national authorities of Guinea-Bissau. This fact also suggests the need to explore and develop new strategies and actions that can contribute to this harmonization by engaging all relevant stakeholders involved in foreign aid in a participatory and collaborative process.
Influence of Socioeconomic Factors on Mortality Reduction
Beyond ODA+ disbursements, our findings highlight the crucial role of economic and social determinants in shaping health outcomes in Guinea-Bissau. Among these, GDP per capita emerged as the most significant predictor of mortality reduction across all models, underscoring the broader impact of economic growth on health improvements. This suggests that integrating health financing with strategies that promote economic stability, and growth seems essential for long-term health improvements [76,77,78]. Additionally, variables such as sanitation access, fertility rates, and vaccination coverage played essential roles in influencing maternal and child health outcomes. Improved sanitation and immunization coverage are strongly associated with better maternal and child health outcomes. Cross-country studies have shown that expanded access to sanitation significantly reduces neonatal and under-five mortality [79,80,81], while vaccination programs play a critical role in lowering the burden of infectious diseases and enhancing child survival [82,83] These findings underscore the importance of integrated, multisectoral strategies for advancing maternal and child health [76,84]. While foreign aid remains essential, it should be complemented by broader socioeconomic development policies and a robust framework addressing the social determinants of health—particularly the structural factors—to ensure sustainable improvements.
5. Conclusions
This study highlights the significant progress achieved through RMNCH funding in Guinea-Bissau, particularly in reducing child mortality. However, persistent gaps in maternal and neonatal health outcomes call for targeted strategies to address these challenges. By aligning donor priorities with national health needs and integrating economic growth strategies, Guinea-Bissau can continue to build on these gains and advance towards achieving SDG health targets.
Strengthening financial sustainability by promoting domestic resource mobilization can mitigate fluctuations in donor contributions and enhance program stability.
Ensuring the efficient allocation of RH funding is crucial, as its lack of correlation with mortality reductions suggests a need to reassess intervention strategies.
Policymakers should prioritize scaling up successful interventions in child health and strengthening maternal and neonatal health programs. Greater engagement with the private sector and innovative financing mechanisms could diversify funding sources and enhance sustainability. Finally, ensuring that aid aligns with national health priorities and is effectively implemented is crucial to maximizing its impact. Integrating RMNCH investments with broader health system strengthening efforts will be key to achieving lasting improvements, particularly in maternal and neonatal health outcomes.
Future research should explore qualitative dimensions of aid effectiveness, including governance, healthcare infrastructure, and community engagement in RMNCH programs, while also investigating the impact of donor coordination and alignment with national health priorities to provide further insights into optimizing development assistance for maternal and child health.
Strengths and Limitations
To our knowledge, this is the first study to examine comprehensively the official development assistance and private voluntary assistance (ODA+) trends for RMNCH in Guinea-Bissau and evaluate their impact on maternal, neonatal, infant, and under-five mortality rates.
Our study has several limitations. First, we used data from the creditor reporting system database that does not capture all aid flows, namely from donors such as China, Brazil, or India. These countries have supported Guinea-Bissau in the health sector over the years, and it would be interesting to analyze their contribution to RMNCH over the years under study. However, as these countries do not report to the DAC of OECD, their assistance was not considered for this work. Second, as allocation to purpose codes in the database depends on the information provided to OECD by countries, there is a possibility of some inconsistency with the project descriptions over the years. Third, our data should be interpreted with caution, considering the short observation period, the limitations of existing data, the macro-level perspective that does not explore the micro-level specifics of projects or their geographical distribution, and the absence of comparative analysis with similar countries. While this represents an initial step toward addressing this issue in Guinea-Bissau, further research is necessary to explore this reality in-depth.
Author Contributions
Conceptualization, A.C, L.V, and I.C.; methodology, A.C and J.B.; software, A.C, and J.B.; formal analysis A.C and J.B.; investigation, A.C.; resources, A.C.; data curation, A.C, and J.B.; writing - original draft preparation, A.C; writing, review and editing-second draft, A.C, R.M.C and M.J.; visualization, A.C, J.B, R.M.C and M.J; supervision, L.V. and I.C. All authors read and approved the final manuscript.
Funding
A.C., R.M.C., L.V., and I.C. were supported by Fundação para a Ciência e a Tecnologia for funds to GHTM—UID/04413/2020 and LA-REAL—LA/P/0117/2020. The authors’ views expressed in this publication do not necessarily reflect the views of institutions and funders.
Ethics approval
The National Committee for Ethics in Research in Health Research of Guinea-Bissau approved the research (Ref. No. 022/CNES/INASA/2021, approved on 18/05/2021).
Acknowledgements
The authors gratefully acknowledge the valuable contributions and suggestions of Professors Cláudia Conceição and José Pereirinha, as well as Prof. Ana Papoila and Marta Alves from the Epidemiology and Statistics Office of the Research Unit at Unidade Local de Saúde de São José, Lisbon, Portugal. We also thank Daisy Carlos and Isabel Pataca for their support.
Conflicts of Interest
The authors declare that they have no competing interests
Abbreviations
AS, All Sector Aid; CH, Child Health; DAC, Development Assistance Committee; DAH, Development Assistance for Health; GNI, gross domestic product; HS, Health Sector Aid; MDG, Millennium Development Goals; MNH, Maternal and neonatal health; ODA, Official Development Assistance; OECD, Organization for Economic Cooperation and Development; RMNCH, Reproductive, maternal, newborn, and child health; RH, Reproductive Health; SDG, Sustainable Development Goals; USD, US dollars.
References
- Rahman, M.; Rouyard, T.; Khan, S.T.; Nakamura, R.; Islam, R.; Hossain, S.; Akter, S.; Lohan, M.; Ali, M.; Sato, M. Reproductive, maternal, newborn, and child health intervention coverage in 70 low-income and middle-income countries, 2000–30: trends, projections, and inequities. Lancet Glob. Heal. 2023, 11, e1531–e1543. [Google Scholar] [CrossRef] [PubMed]
- Marchant, T.; A Bhutta, Z.; Black, R.; Grove, J.; Kyobutungi, C.; Peterson, S. Advancing measurement and monitoring of reproductive, maternal, newborn and child health and nutrition: global and country perspectives. BMJ Glob. Heal. 2019, 4, e001512. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Public spending on health: a closer look at global trends. Geneva; 2018.
- World Health Organization. Targets of Sustainable Development Goal 3 [Internet]. 2025 [cited 2025 Feb 1]. Available from: https://www.who.int/europe/about-us/our-work/sustainable-development-goals/targets-of-sustainable-development-goal-3.
- Costello, A.; Naimy, Z. Maternal, newborn, child and adolescent health: challenges for the next decade. Int. Heal. 2019, 11, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Engmann CM, Khan S, Moyer CA, Coffey PS, Bhutta ZA. Transformative Innovations in Reproductive, Maternal, Newborn, and Child Health over the Next 20 Years. PLoS Med. 2016 Mar 2;13(3):e1001969.
- OECD. DAC glossary of key terms and concepts [Internet]. 2019 [cited 2021 Apr 26]. Available from: https://www.oecd.org/dac/dac-glossary.htm.
- Radelet S. A Primer on Foreign Aid. SSRN Electronic Journal [Internet]. 2006; Available from: http://www.ssrn.com/abstract=983122.
- Khan, R.; Zeeshan, *!!! REPLACE !!!*; Haque, M.I.; Gupta, N.; Tausif, M.R.; Kaushik, I. How foreign aid and remittances affect poverty in MENA countries? PLOS ONE 2022, 17, e0261510. [Google Scholar] [CrossRef]
- Staicu, G.; Barbulescu, R. A Study of the Relationship between Foreign Aid and Human Development in Africa. In: International Development. InTech; 2017. p. 1689–99.
- Easterly, W. Was Development Assistance a Mistake? American Economic Review. 2007 Apr 1;97(2):328–32.
- Moyo, D. Dead Aid: Why Aid Is Not Working and How There Is a Better Way for Africa. Penguin; 2010.
- Negeri, K.G. The long-run effects of health aid in low-income countries. J. Public Heal. Afr. 2023, 14, 2219. [Google Scholar] [CrossRef]
- Odokonyero, T.; Marty, R.; Muhumuza, T.; Ijjo, A.T.; Moses, G.O. The impact of aid on health outcomes in Uganda. Heal. Econ. 2017, 27, 733–745. [Google Scholar] [CrossRef]
- Abraham R, Tao Z. Funding health in developing countries: foreign aid, FDI, or personal remittances? Int J Soc Econ. 2021 Oct 28;48(12):1826–51.
- Bendavid, E.; Bhattacharya, J. The Relationship of Health Aid to Population Health Improvements. JAMA Intern. Med. 2014, 174, 881–887. [Google Scholar] [CrossRef]
- Mishra P, Newhouse D. Does health aid matter? J Health Econ [Internet]. 2009 Jul;28(4):855–72. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0167629609000563.
- Marty, R.; Dolan, C.B.; Leu, M.; Runfola, D. Taking the health aid debate to the subnational level: the impact and allocation of foreign health aid in Malawi. BMJ Glob. Heal. 2017, 2, e000129. [Google Scholar] [CrossRef]
- Toseef MU, Jensen GA, Tarraf W. How Effective Is Foreign Aid at Improving Health Outcomes in Recipient Countries? Atlantic Economic Journal. 2019 Dec 14;47(4):429–44.
- Williamson, C.R. Foreign Aid and Human Development: The Impact of Foreign Aid to the Health Sector. South. Econ. J. 2008, 75, 188–207. [Google Scholar] [CrossRef]
- Pallas, S.W.; Ruger, J.P. Effects of donor proliferation in development aid for health on health program performance: A conceptual framework. Soc. Sci. Med. 2017, 175, 177–186. [Google Scholar] [CrossRef]
- Leunig, I.; Dijkstra, G.; Tuytens, P. The Relationship Between Health aid and Health Outcomes and the Role of Domestic Healthcare Expenditure in Developing Countries. Forum Dev. Stud. 2024, 51, 211–234. [Google Scholar] [CrossRef]
- Hu, B.; Mendoza, R.U. Public Health Spending, Governance and Child Health Outcomes: Revisiting the Links. J. Hum. Dev. Capab. 2013, 14, 285–311. [Google Scholar] [CrossRef]
- Dreher, A.; Lang, V.; Reinsberg, B. Aid effectiveness and donor motives. World Dev. 2024, 176. [Google Scholar] [CrossRef]
- Francisco, P.; Moreira, S.B.; Caiado, J. Identifying differences and similarities between donors regarding the long-term allocation of official development assistance. Dev. Stud. Res. 2021, 8, 181–198. [Google Scholar] [CrossRef]
- Keeley B. From Aid to Development [Internet]. OECD; 2012 [cited 2021 Mar 25]. (OECD Insights). Available from: https://www.oecd-ilibrary.org/agriculture-and-food/development-and-aid_9789264123571-en.
- Elayah, M.; Al-Awami, H. Exploring the preference for bilateral aid: Gulf oil states’ aid to Yemen. Third World Q. 2024, 45, 2266–2286. [Google Scholar] [CrossRef]
- Apodaca C. Foreign Aid as Foreign Policy Tool. In: Oxford Research Encyclopedia of Politics [Internet]. Oxford University Press; 2017. Available from: http://politics.oxfordre.com/view/10.1093/acrefore/9780190228637.001.0001/acrefore-9780190228637-e-332.
- Headey, D. Geopolitics and the effect of foreign aid on economic growth: 1970–2001. J. Int. Dev. 2007, 20, 161–180. [Google Scholar] [CrossRef]
- United Nations Dof, E.; SAPD World Population Prospects 2024, Online Edition. [Internet]. 2024 [cited 2024 Aug 4]. Available from: https://population.un.org/wpp/Download/Standard/Population/.
- UNDP (United Nations Development Programme). Human Development Report 2023/2024: Breaking the Gridlock - Reimagining Cooperation in a Polarized World. 2024.
- Sangreman, C. A Política Económica e Social na Guiné-Bissau. CEsA/ CSG - Documentos de Trabalho no 146/ 2016. 2016;(1):1–35.
- Barros M De, Gomes PG, Correia D. Les conséquences du narcotrafic sur un État fragile : le cas de la Guinée-Bissau. Alternatives Sud. 2013;20:145–58.
- Nóbrega, Á. A Luta pelo Poder na Guiné-Bissau. Lisbon: Universidade técnica de Lisboa, Instituto superior de ciências sociais e políticas; 2003.
- Koudawo, F. Cabo Verde e Guiné-Bissau: da democracia revolucionária a democracia liberal. Bissau: Instituto Nacional de Estudos e Pesquisa; 2001.
- United Nations Inter-agency Group for Child Mortality Estimation (UN IGME). Levels and Trends in Child Mortality: Report 2024. 2025.
- World Bank. WDI [World Development Indicators]. 2020. Available online: https://databank.worldbank.org/source/world-development-indicators# (accessed on 2 December 2020).
- Patel, P.; Roberts, B.; Guy, S.; Lee-Jones, L.; Conteh, L. Tracking Official Development Assistance for Reproductive Health in Conflict-Affected Countries. PLOS Med. 2009, 6, e1000090. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Tadesse, E.; Jin, Y.; Cha, S. Association between Development Assistance for Health and Disease Burden: A Longitudinal Analysis on Official Development Assistance for HIV/AIDS, Tuberculosis, and Malaria in 2005–2017. Int. J. Environ. Res. Public Heal. 2022, 19, 14091. [Google Scholar] [CrossRef]
- International Aid Transparency Initiative. The Relationship between IATI and CRS [Internet]. 2025 [cited 2025 Mar 12]. Available from: https://iatistandard.org/documents/63/The-relationship-between-IATI-and-CRS.doc.
- Dingle, A.; Schäferhoff, M.; Borghi, J.; Sabin, M.L.; Arregoces, L.; Martinez-Alvarez, M.; Pitt, C. Estimates of aid for reproductive, maternal, newborn, and child health: findings from application of the Muskoka2 method, 2002–17. Lancet Glob. Heal. 2020, 8, e374–e386. [Google Scholar] [CrossRef]
- Pitt, C.; Bath, D.; Binyaruka, P.; Borghi, J.; Martinez-Alvarez, M. Falling aid for reproductive, maternal, newborn and child health in the lead-up to the COVID-19 pandemic. BMJ Glob. Heal. 2021, 6, e006089. [Google Scholar] [CrossRef]
- OECD. Aid to Health [Internet]. 2018 [cited 2021 Sep 20]. Available from: https://www.oecd.org/development/stats/aidtohealth.htm.
- Hsu, J.; Berman, P.; Mills, A. Reproductive health priorities: evidence from a resource tracking analysis of official development assistance in 2009 and 2010. Lancet 2013, 381, 1772–1782. [Google Scholar] [CrossRef] [PubMed]
- Powell-Jackson, T.; Borghi, J.; Mueller, D.H.; Patouillard, E.; Mills, A. Countdown to 2015: tracking donor assistance to maternal, newborn, and child health. Lancet 2006, 368, 1077–1087. [Google Scholar] [CrossRef]
- United Nations—Population Division. World Population Prospects 2017. Available online: https://population.un.org/wpp/ (accessed on 17 February 2019).
- Department of Economic Social Affairs, U.N. World Population Prospects 2019 [Internet]. 2021 [cited 2021 Apr 26]. Available from: https://population.un.org/wpp/.
- OECD. Creditor Reporting System: Aid activities. OECD International Development Statistics (Database). [Internet]. 2024. Available from: https://www.oecd-ilibrary.org/development/data/creditor-reporting-system/aid-activities_data-00061-en.
- Microsoft Corporation. Microsoft Excel. Version 16,. 2016.
- UNICEF, WHO. A Decade of Tracking Progress for Maternal, Newborn and Child Survival: the 2015 Report [Internet]. 2015. Available from: https://www.countdown2015mnch.org/documents/2015Report/Countdown_to_2015-A_Decade_of_Tracking_Progress_for_Maternal_Newborn_and_Child_Survival-The2015Report-Conference_Draft.
- WHO. World health statistics 2024 [Internet]. 2024 [cited 2024 May 25]. Available from: https://data.who.int.
- Winkleman, T.F.; Adams, G.B. An empirical assessment of the relationship between Official Development Aid and child mortality, 2000–2015. Int. J. Public Heal. 2017, 62, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Banchani, E.; Swiss, L. The Impact of Foreign Aid on Maternal Mortality. Politi- Gov. 2019, 7, 53–67. [Google Scholar] [CrossRef]
- StataCorp LLC. Stata Statistical Software: Release 18. 2023.
- Boundioa, J.; Thiombiano, N. Effect of public health expenditure on maternal mortality ratio in the West African Economic and Monetary Union. BMC Women's Heal. 2024, 24, 1–10. [Google Scholar] [CrossRef]
- Souza, J.P.; Day, L.T.; Rezende-Gomes, A.C.; Zhang, J.; Mori, R.; Baguiya, A.; Jayaratne, K.; Osoti, A.; Vogel, J.P.; Campbell, O.; et al. A global analysis of the determinants of maternal health and transitions in maternal mortality. Lancet Glob. Heal. 2023, 12, e306–e316. [Google Scholar] [CrossRef] [PubMed]
- Annan, K. We the peoples: the role of the United Nations in the 21st century. New York; 2000.
- Countdown to 2030. Fulfilling the Health Agenda for Women and Children [Internet]. 2014. Available from: https://www.countdown2030.org/wp-content/uploads/2014/06/Countdown_2014_Report_No_Profiles_final.pdf.
- Kirton J, Kulik J, Bracht C. The political process in global health and nutrition governance: the G8’s 2010 Muskoka Initiative on Maternal, Child, and Newborn Health. Ann N Y Acad Sci. 2014 Dec 21;1331(1):186–200.
- UKAid. The London summit on family planning [Internet]. 2012 [cited 2021 Apr 26]. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/67328/london-summit-family-planning-commitments.pdf.
- United Nations. Global Strategy for Women’s and Children’s health [Internet]. Publisher/Organizer: The Partnership for Maternal, Newborn and Child Health; 2010. Available from: https://www.who.int/pmnch/knowledge/publications/fulldocument_globalstrategy/en/.
- Greco, G.; Powell-Jackson, T.; Borghi, J.; Mills, A. Countdown to 2015: assessment of donor assistance to maternal, newborn, and child health between 2003 and 2006. Lancet 2008, 371, 1268–1275. [Google Scholar] [CrossRef]
- Grollman C, Arregoces L, Martínez-Álvarez M, Pitt C, Mills A, Borghi J. 11 years of tracking aid to reproductive, maternal, newborn, and child health: estimates and analysis for 2003–13 from the Countdown to 2015. Lancet Glob Health [Internet]. 2017 Jan;5(1):e104–14. Available from: https://linkinghub.elsevier.com/retrieve/pii/S2214109X16303047.
- Bhutta ZA, Lassi ZS, Blanc A, Donnay F. Linkages Among Reproductive Health, Maternal Health, and Perinatal Outcomes. Semin Perinatol. 2010 Dec;34(6):434–45.
- Pasha O, McClure EM, Wright LL, Saleem S, Goudar SS, Chomba E, et al. A combined community- and facility-based approach to improve pregnancy outcomes in low-resource settings: a Global Network cluster randomized trial. BMC Med. 2013 Dec 3;11(1):215.
- Hsu, J.; Pitt, C.; Greco, G.; Berman, P.; Mills, A. Countdown to 2015: changes in official development assistance to maternal, newborn, and child health in 2009–10, and assessment of progress since 2003. Lancet 2012, 380, 1157–1168. [Google Scholar] [CrossRef]
- Kibira, D.; Asiimwe, C.; Muwonge, M.; Ham, H.A.v.D.; Reed, T.; Leufkens, H.G.; Mantel-Teeuwisse, A.K. Donor Commitments and Disbursements for Sexual and Reproductive Health Aid in Kenya, Tanzania, Uganda and Zambia. Front. Public Heal. 2021, 9. [Google Scholar] [CrossRef]
- A Grépin, K.; Pinkstaff, C.B.; Hole, A.R.; Henderson, K.; Norheim, O.F.; Røttingen, J.-A.; Ottersen, T. Allocating external financing for health: a discrete choice experiment of stakeholder preferences. Heal. Policy Plan. 2018, 33, i24–i30. [Google Scholar] [CrossRef]
- Ottersen T, Kamath A, Moon S, Martinsen L, Røttingen JA. Development assistance for health: what criteria do multi- and bilateral funders use? Health Econ Policy Law. 2017 Apr 23;12(2):223–44.
- Ottersen, T.; A Grépin, K.; Henderson, K.; Pinkstaff, C.B.; Norheim, O.F.; Røttingen, J.-A. New approaches to ranking countries for the allocation of development assistance for health: choices, indicators and implications. Heal. Policy Plan. 2018, 33, i31–i46. [Google Scholar] [CrossRef]
- Chersich, M.F.; Martin, G. Priority gaps and promising areas in maternal health research in low- and middle-income countries: summary findings of a mapping of 2292 publications between 2000 and 2012. Glob. Heal. 2017, 13, 6. [Google Scholar] [CrossRef]
- Mishra, S.K. Addressing reproductive and maternal health in Latin America and the caribbean – initiatives underway. Obstet. Gynecol. Int. J. 2018, 9, 423–430. [Google Scholar] [CrossRef]
- OECD. Accra Agenda for Action [Internet]. Paris: OECD; 2008 [cited 2022 Feb 13]. Available from: https://www.oecd-ilibrary.org/development/accra-agenda-for-action_9789264098107-en.
- OECD. Declaration of the Fourth High Level Forum on Aid Effectiveness. In: OECD [Internet]. 2011 [cited 2022 Feb 13]. Available from: https://www.oecd.org/development/effectiveness/49650173.pdf.
- General Assembly UN. General Assembly. 2019;65106(December). Available from: https://generalassemb.ly/design.
- Bishai, D.M.; Cohen, R.; Alfonso, Y.N.; Adam, T.; Kuruvilla, S.; Schweitzer, J. Factors Contributing to Maternal and Child Mortality Reductions in 146 Low- and Middle-Income Countries between 1990 and 2010. PLOS ONE 2016, 11, e0144908–e0144908. [Google Scholar] [CrossRef] [PubMed]
- DerSarkissian, M.; A Thompson, C.; A Arah, O. Time series analysis of maternal mortality in Africa from 1990 to 2005. J. Epidemiology Community Heal. 2013, 67, 992–998. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Qu, H.; Xia, J.; Hui, X.; Shi, C.; Xu, F.; He, J.; Cao, Y.; Hu, M. Trends, influencing factors and prediction analysis of under-five and maternal mortality rates in China from 1991 to 2020. Front. Public Heal. 2023, 11, 1198356. [Google Scholar] [CrossRef] [PubMed]
- A Fuller, J.; Villamor, E.; Cevallos, W.; Trostle, J.; Eisenberg, J.N. I get height with a little help from my friends: herd protection from sanitation on child growth in rural Ecuador. Leuk. Res. 2016, 45, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Kmush, B.L.; Walia, B.; Neupane, A.; Frances, C.; Mohamed, I.A.; Iqbal, M.; A Larsen, D. Community-level impacts of sanitation coverage on maternal and neonatal health: a retrospective cohort of survey data. BMJ Glob. Heal. 2021, 6, e005674. [Google Scholar] [CrossRef]
- Ummalla, M.; Samal, A.; Zakari, A.; Lingamurthy, S. The effect of sanitation and safe drinking water on child mortality and life expectancy: Evidence from a global sample of 100 countries. Aust. Econ. Pap. 2022, 61, 778–797. [Google Scholar] [CrossRef]
- Kumari P, . S. Investigating The Importance of Vaccines and Childhood Nutrition on Improving Maternal and Child Health. International Journal of Multidisciplinary Research in Science, Engineering and Technology [Internet]. 2024 May 22;7(05):10275–7. Available from: https://ijmrset.com/upload/111_Investigating.pdf.
- Karaut, T.S. Evaluating the Effectiveness and Coverage of Vaccination Programs in Reducing the Incidence of Paediatric Infectious Diseases. Asian J. Pediatr. Res. 2024, 14, 29–36. [Google Scholar] [CrossRef]
- Bijleveld, P.; Maliqi, B.; Pronyk, P.; Franz-Vasdeki, J.; Nemser, B.; Sera, D.; van de Weerdt, R.; Walter, B. Country perspectives on integrated approaches to maternal and child health: the need for alignment and coordination. Bull. World Heal. Organ. 2016, 94, 401–404. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



