Submitted:
02 May 2025
Posted:
06 May 2025
You are already at the latest version
Abstract
About a quarter of the world’s population is infected with Mycobacterium tuberculosis. Growing antibiotic resistance by the microorganism is a major problem in the therapy of the disease. M. avium‐M. intracellulare that emerged as a major opportunistic infection of HIV/AIDS continues to afflict immunocompromised individuals. Here we briefly describe the various methods for liposome preparation, and the use of liposome‐encapsulated antibiotics in the experimental and clinical therapy of mycobacterial and other bacterial infections. We also review recent experimental liposomal vaccines against tuberculosis.
Keywords:
liposomes
; tuberculosis
; antibiotics
; antimycobacterial agents
; bacterial infections
; tuberculosis vaccines
1. Mycobacteria
Mycobacteria are aerobic bacteria with a diameter of approximately 0.2–0.6 µm and they vary in length between 1–10 µm. Owing to the long-chain lipids, termed mycolic acids, in the bacterial membrane, the surface of the microorganism presents a hydrophobic interface, which resists the entry of many disinfectants as well as the Gram and Giemsa stains. A major characteristic of mycobacteria is that after incubation with the Ziehl-Neelsen stain, they are resistant to the decolorizing effect of an ethanol-hydrochloric acid solution (which can remove the stain from many other bacteria), and are thus termed acid-fast bacteria. Nevertheless, under some conditions, for example, after treatment with the mycolic acid synthesis inhibitor, isoniazid, or when it is in a metabolically inactive state in the host, M. tuberculosis may become acid-fast-negative [1]. Mycobacteria grow very slowly. The doubling time for Mycobacterium tuberculosis may be as long as 1676 h in the chronic infection phase in infected mice, and about 25 h during acute infection [2]. During the Industrial Revolution in the 18th and 19th centuries in Europe, tuberculosis became an epidemic, exacerbated by the crowding of urbanization and economic depression [3]. One quarter of the population of Europe in the 19th Century is thought to have died of “consumption,” as tuberculosis was called at the time. The victims included Goethe, Rousseau, Thoreau, Keats, Paganini, and Chopin. It is estimated that even in the 21st Century, one in four people in the world are infected with M. tuberculosis. According to the World Health Organization, the bacterium infected 10.8 million people in 2023, and killed about 1.25 million people. Among these, 161,000 were HIV-1-infected people. It is estimated that between 5 and 10% of individuals infected with the mycobacterium will eventually develop tuberculosis. The incidence is highest in Southeast Asia (45%), Africa (24%) and the Western Pacific (17%). Tuberculosis is prevalent in areas with poverty, malnutrition and poor housing. Mycobacteria have a complex cell wall, composed of the peptidoglycan layer linked with arabinose-galactose-mycolic acid [3]. Long chain mycolic acids, in the range of 70 to 90 carbon atoms, are the major lipids in the mycobacterial cell wall. Free lipids are located on the outer layers, including waxes, mycosides, which are complex saturated glycolipids, and 6,6'-dimycolate of trehalose, known as cord factor, one of the virulence factors of mycobacteria. The tubercle bacillus is transmitted by via inhalation of infectious aerosols, generally involving person-to-person contact in close quarters, and occasionally by ingestion and skin trauma. Large aerosol particles are usually trapped by the lung mucosal surfaces and removed by the mucociliary escalator. Smaller aerosol particles with 1–3 mycobacteria can reach the alveoli and are phagocytosed by alveolar macrophages, where they replicate and may destroy their host cell. Infected macrophages may migrate to local lymph nodes, the bloodstream, bone marrow, spleen, kidneys, and the central nervous system [3]. According to American Thoracic Society recommendations, the initial treatment regimen involves isoniazid (and inhibitor of mycolic acid biosynthesis), rifampin (an inhibitor of bacterial RNA synthesis), pyrazinamide (an inhibitor of fatty acid synthase type I), and ethambutol (an inhibitor of arabinogalactan synthesis) for 2 months. This is followed by isoniazid and rifampin therapy for 4–6 months. Noncompliance is known to cause the emergence of multi-drug-resistant (MDR) strains; thus, in many countries, directly observed therapy (DOT) is employed to ensure compliance.
MDR strains that are resistant to at least isoniazid and rifampin have become a worldwide problem [4]. The resistance is attributed to one or more chromosomal mutations. One of these mutations is in a gene for mycolic acid synthesis, and another in a gene for catalase-peroxidase, an enzyme required to activate isoniazid within the bacterium [3]. Previous treatment for tuberculosis predisposes the patient to the selection of MDR organisms. In addition to MDR tuberculosis, extensively drug resistant (XDR) M. tuberculosis strains have emerged throughout the world [5]. These bacteria are MDR- M. tuberculosis strains that are resistant to fluoroqinolones and at least one of the second line drugs, such as kanamycin, capreomycin and amikacin.
M. avium and M. intracellulare (MAC) are difficult to differentiate physiologically, and cause identical diseases, and are thus grouped together as the M. avium-M. intracellulare Complex, abbreviated as MAC [3]. They cause disseminated disease, where tissue macrophages are inundated with the microorganisms, especially in advanced HIV/AIDS patients, and the blood contains large numbers of organisms. M. abscessus has been recogized recently as a pathogen that can colonize the lungs of patients with cystic fibrosis, chronic obstructive pulmonary disease, or bronchiectasis, and that can grow in macrophages and free-living amoebae [6]. The mycobacterium has intrinsic and acquire mechanisms of resistance to therapeutics [7].
2. Early Studies on Liposome-Encapsulated Antibiotics for Tuberculosis Therapy
The first English-language publications on the use of liposome-encapsulated antibiotics appeared in 1982. Vladimirsky and Ladigina [8] treated mice infected with M. tuberculosis strain H37Rv by intravenous injection of streptomycin sulfate encapsulated in liposomes composed of lecithin (phosphatidylcholine with various acyl chains). There was a statistically different decrease in mycobacterial counts in the spleen compared to an equivalent concentration free streptomycin, which translated into prolonged survival in the liposomal antibiotic group, and reduced antibiotic toxicity. In a subsequent study, Ladigina & Vladimirsky [9] showed that the total area under the serum concentration-time curve (“AUC”) of liposomal 3H-dihydrostreptomycin was 8.8 times higher in uninfected mice than the free antibiotic, and 5.9 times higher in mice with advanced tuberculosis. The total amounts of liposome-delivered antibiotic in the spleen and liver of infected mice were 9.2 and 7.3 times higher, respectively than that achieved with the free antibiotic. Orozco et al. reported that mice with severe tuberculosis treated with rifampicin and isoniazid in free and liposome-encapsulated form, together, had a higher survival rate (about 85%) after 30 days, the lowest colony-forming units (CFU) of the bacteria, and less inflammation in the lungs [10]. These early experiments were followed by the impressive results obtained by Agarwal et al. who employed rifampin-loaded phosphatidylcholine liposomes to which the macrophage activating tetrapeptide, tuftsin (Thr-Lys-Pro-Arg), was coupled covalently via its C-terminus, using an ethylene diamine spacer. The liposomes delivered twice weekly for 2 weeks were several orders of magnitude more effective effective than the free drug in lowering the CFU in the lungs, liver and spleen of mice that had been infected for 13-16 days with the H37Rv strain of M. tuberculosis [11].
3. Early Studies on Liposomal Antibiotic Therapy of Mycobacterium Avium-Mycobacterium Intracellulare Infections
The first report on the use of liposome-encapsulated antibiotics against experimental MAC infections in beige mice employed amikacin in phosphatidylglycerol-phosphatidlycholine-cholesterol (1:1:1) liposomes prepared by reverse-phase evaporation followed by extrusion through polycarbonate membranes [12]. This formulation arrested the growth of MAC in the liver, and reduced the CFU counts by about 1,000-fold in the spleen and kidneys, compared with those of both untreated controls and free-drug-treated mice. Using a much higher dose of amikacin, either free or encapsulated in phosphatidylcholine liposomes, Cynamon et al. obtained similar results in the liver and spleen; however, they also found a significant reduction in CFU in the lungs with both free and liposomal amikacin [13]. Relatively low concentrations of amikacin and gentamicin in liposomes reduced significantly the MAC CFU in blood, liver, and spleen [14]. Klemens et al. found that both encapsulated and free gentamicin reduced viable MAC counts in the liver, spleen and lungs compared with no treatment [15]. Encapsulated gentamicin was more effective than the free antibiotic in reducing the viable cell counts in the spleen and liver. Liposomal amikacin was also more effective than the free drug when administered to MAC-infected murine peritoneal macrophages [16].
Intraperitoneal administration of rifampin-incorporating multilamellar liposomes resulted in a larger reduction in bacterial growth in the lungs and spleen of infected ddY mice than did free rifampin [17]. Liposome-encapsulated streptomycin, administered intravenously in weekly doses (15 mg/kg) for 4 weeks, reduced the CFU in the liver and spleen of MAC-infected beige mice by an extent similar to that of a 50- to 100-fold higher dose of the free drug [18]. With this injection schedule, the CFU in the liver and spleen were lower by 2.4 and 2.9 log units, respectively, compared to untreated controls, even by the end of 12 weeks, suggesting that the liposomal formulation also increases the residual activity of the drug in these organs. In a parallel study, the effect of free streptomycin at 150 mg/kg given im five days a week for 8 weeks was compared with 15 mg/kg of streptomycin in unilamellar liposomes administered intravenously in 4 injections, with no further treatment up to 8 weeks [19]. The chemotherapeutic efficacy, expressed as the reduction in CFU/unit dose of the antibiotic, was several fold higher for the liposomal drug.
4. Encapsulation of Antibiotics in Liposomes
Various drug delivery systems, including metallic, polymeric, carbon-based, and dendrimeric carriers, as well as liposomes, have been utilized to overcome the limitations of antibiotics, such as low aqueous solubility, drug degradation, and antibiotic resistance, while simultaneously enhancing their bioavailability and minimizing adverse effects [20]. Liposomes offer advantages such as biocompatibility, capacity for self-assembly, low immunogenicity, passive and active targetability, prolonged half-life of the loaded drug, protection of sensitive molecules, and enhanced bioavailability [21].
Liposomes are generally classified based on their size, with small unilamellar vesicles (SUVs) being <100 nm and large unilamellar vesicles (LUVs) being >100 nm, as well as by the number of lamellae (unilamellar or multilamellar vesicles). In the preparation of liposomal formulations, the composition and charge—neutral, anionic, or cationic—can be tailored according to the therapeutic target [22]. This is particularly important for the interaction of liposomes with bacteria and their uptake by eukaryotic cells [23] . Additionally, liposomal formulations offer significant advantages in the optimal treatment of infections, as they can be administered through various routes, including intravenous [24], transdermal [25], oral [26], inhalational [27,28], and nasal delivery [29].
The encapsulation of antibiotics in liposomes can be achieved through two main approaches: active and passive loading. Passive loading techniques include mechanical dispersion, solvent dispersion, and detergent removal methods, whereas active loading techniques involve approaches such as detergent dialysis and microfluidic methods. These techniques are used to load drugs into preformed liposomes, ensuring minimal drug loss during the loading process [30].
Hydrophilic antibiotics are incorporated into the aqueous core, whereas hydrophobic antibiotics are naturally embedded within the lipid bilayer. The development of antibiotic-loaded liposomes depends on multiple factors, including the physicochemical properties of the drug, formulation stability, drug leakage, and retention [31]. In general, liposomes are prepared by dissolving lipid components in an organic solvent, forming a lipid film, which is then redispersed in an aqueous medium, followed by sizing and purification. Various techniques have been utilized for liposome synthesis and antibiotic encapsulation, including sonication, thin-film hydration, freeze-thawing, micro-emulsification, solvent injection, reverse-phase evaporation, dehydration-rehydration, hydration in a packed bed of colloidal particles, pH jumping, detergent removal, and extrusion [32,33].
One of the distinguishing factors that set liposomes apart from other drug carriers in antibiotic delivery is the flexibility of their surface modification. The frequently employed polyethylene glycol (PEG)-conjugated lipids can be used to confer to liposomes incorporating them the property of prolonged circulation after intravenous administration [34,35]. These “PEGylated” liposomes can be further functionalized on their surface with antibodies, peptides, proteins, or carbohydrates [36]. This surface modification enhances drug efficacy while correspondingly improving therapeutic effectiveness [37-39].
Bacteria can develop resistance mechanisms against drugs through various pathways, such as enzymatic inactivation of the drug and active efflux pumping, which expels the drug from the cell [40]. Numerous studies have demonstrated that liposome-based antibiotic formulations can be effective in treating antibiotic-resistant bacteria (Figure 1) [41].
Antibiotics encapsulated within liposomes can target both Gram-negative and Gram-positive bacteria, which often produce enzymes that degrade antimicrobial agents. Additionally, for an antibiotic to exert its effect, it must penetrate the bacterial membrane and enter the cell. However, mutations can lead to alterations in outer membrane porins, reducing permeability [42]. In Gram-negative bacteria, the complex structure of the outer membrane further hinders antibiotic penetration, contributing to resistance. Moreover, active efflux pump proteins, which play a crucial role in bacterial physiology, can also contribute to resistance by expelling antibiotics before they reach their target. During the formulation of liposomes, the use of potentially fusogenic phospholipids may help overcome this challenge by facilitating membrane penetration. These phospholipids enhance the fusion of liposomes with bacterial membranes, improving drug delivery and increasing the intracellular uptake of antibiotics, thereby enhancing their therapeutic efficacy against resistant bacterial strains [43].
Given these challenges, liposomal antibiotic formulations have been widely explored as a potential strategy to enhance the efficacy of antibiotics against resistant bacterial strains (Table 1). In a study targeting Staphylococcus aureus biofilms, negatively charged liposomes encapsulating Levofloxacin and Vancomycin were prepared using the dehydration-rehydration technique, enabling in situ antibiotic release within the biofilm [44]. Additionally, Nafcillin-loaded PEG-grafted liposomes, prepared via the reverse-phase evaporation method with an average size of 253 nm, exhibited a fourfold reduction in the minimum inhibitory concentration (MIC) against Methicillin-susceptible Staphylococcus aureus (MSSA) compared to free Nafcillin [45].
For the treatment both Gram-positive and Gram-negative bacterial infections, amoxicillin, β-lactam antibiotic, was successfully encapsulated into liposomes (~200 nm in size) using the Supercritical Assisted Liposome Formation (SuperLip) method. In this technique, liposomes are prepared by spraying water droplets into an expanded phase composed of phospholipids, ethanol, and carbon dioxide (CO₂) under high pressure. During the process, the water droplets are rapidly surrounded by a lipid layer, and upon falling into the water pool located at the bottom of the vessel, liposomes are formed. Using this approach, an encapsulation efficiency of 84% was achieved [46]. Furthermore, pH-sensitive liposomes loaded with a silver-tinidazole complex effectively eradicated tumor-associated bacteria from primary tumors.
5. Therapy of Mycobacterium tuberculosis Infection
Airborne and primarily affecting the lungs, tuberculosis is a highly lethal disease caused by Mycobacterium tuberculosis. According to WHO data, tuberculosis affects approximately 10 million people annually and results in about 1.3 million deaths worldwide [57]. The treatment of this disease commonly involves Rifampicin (RIF), Isoniazid (INH), Pyrazinamide (PZA), and Ethambutol (EMB). However, due to the potential development of resistance to these drugs, novel and more effective therapeutic strategies are needed urgently [58].
Formulations of various drugs prepared using liposomal delivery systems not only enhance therapeutic efficacy but also serve as promising platforms for the development of vaccines against tuberculosis infections [59]. A novel vaccine strategy has been explored by combining Poly:IC adjuvant with liposomes containing the Ag85B and ESAT-6 antigens [60]. To induce a stronger immune response, fusion proteins such as Hspx, PPE44, and EsxV have been loaded into liposomes for the development of a tubeculosis vaccine [61].
The FDA approval of liposome-based drug formulations and the widespread utilization of this nanocarrir system highlight its significance in advancing next-generation anti-tuberculosis treatment approaches [62]. Thanks to remarkable advancements in liposome technology, the development of inhalable antibiotic-loaded liposomes, in addition to those administered via the intravenous [63] or oral route [37], has been made possible. Additionally, targeted drug delivery systems help reduce the degradation of drugs in the body compared to their free forms, allowing for the administration of lower doses while maintaining therapeutic efficacy. As a result, the toxic effects of the drugs are minimized, leading to a more effective treatment.
These formulations hold potential for clinical applications and patent acquisition, ultimately making them available for human use [64]. This characteristic provides a significant advantage in the treatment of tuberculosis, which is primarily localized in the lungs [65]. Although oral administration of rutin-based drugs is more frequent and cost-effective, their low gastrointestinal absorption and rapid hepatic first-pass metabolism necessitate high-dose administration. Therefore, parenteral and pulmonary delivery of rutin-based drugs offers a higher bioavailability, as they bypass the first-pass metabolism. M. tuberculosis evades macrophage-mediated bactericidal mechanisms by inhibiting the formation of phagolysosomes [66]. Liposomes can be administered via inhalation depending on their size. Liposomes with a particle size ranging from 0.1 to 2 µm can reach the alveoli, whereas those larger than 15 µm cannot penetrate the respiratory barrier [67].
For the treatment of tuberculosis, liposomes have been designed to encapsulate antibiotics such as RIF [68], INH [69], PZA [70], and EMB [71], either individually or in combination [72,73]. Additionally, potential compounds with anti- tuberculosis activity [19] have also been loaded into liposomes for therapeutic applications, including theranostic approaches. Furthermore, increasing the particle size can influence the therapeutic effect. (Figure 2).
For targeted applications, if the aim is to reduce the immunogenicity of liposomes and decrease their uptake by the mononuclear phagocyte system, their surface can be modified with PEG [74]. PEGylated liposomes have been developed for the co-delivery of antitubercular drugs and TGF-β1 siRNA for tuberculosis treatment. The formulated liposomes exhibited minimal toxicity to human macrophages while demonstrating good selectivity [75].
The conjugation of various polysaccharides, including chitosan, dextran, and fucoidan, to the surface of liposomes can enhance their stability while also imparting mucoadhesive properties. Additionally, these formulations not only improve cellular uptake but also interact with carbohydrate receptors expressed on the surface of macrophages [76]. Fucoidan-based surface modifications have been applied to enhance the activity of usnic acid-loaded liposomes in tuberculosis treatment [77]. The use of cationic pH-sensitive liposome-based delivery systems facilitates the passage through the endosomal membrane under low pH conditions, enabling the release of the encapsulated content into the cytosol. This prevents the degradation of delivered antigens and, consequently, enhances cytotoxic CD8+ T-cell responses [78]. In tuberculosis treatment, to overcome local and systemic toxicity, liposomes encapsulating anti- tuberculosis drugs can be surface-modified with macrophage-specific ligands. To facilitate the delivery of RIF-loaded liposomes to alveolar macrophages, liposomal formulations coated with maleylated bovine serum albumin and O-stearoyl amylopectin were developed. Based on drug localization index data, ligand-functionalized drug-loaded liposomes exhibited a 1.4- to 3.5-fold higher localization compared to non-ligand-modified counterparts. These findings indicate that the ligand-modified liposomes enable rapid drug delivery to the lungs and achieve high drug concentrations at the target site [79].
6. Therapy of Non-Tuberculous Mycobacterial Infections
The most common appearance of non-tuberculous mycobacteria (NTM) infections is lung disease [94]. These bacteria, which include M. avium, M. intracellulare and M. chimaera, are present in the environment and can cause pulmonary infections in immunocompromised individuals or persons who have lung damage. NTM may present as biofilms attached to the alveolar wall or intracellularly in monocytes and macrophages. Ehlers et al. [95] found that long-term intravenous administration of liposomal amikacin was not effective against lung infections in M. avium-infected mice. As an approach to this problem Zhang et al. [96] aerosolized amikacin-liposomes (dipalmitoylphosphatidylcholine-choesterol (2:1)) into rats infected with NTM, and observed a large increase in the mean area under the concentration-time curve in the lungs and lung macrophages compared to intravenous free amikacin .
A retrospective analysis of 17 patients undergoing treatment with amikacin-liposomes (“Amikacin Liposomal Inhalation Suspension”) for NTM lung infection showed that at 6 months, 86% of the patients had clinical, microbiological, and radiological improvement. Twenty five percent of the treated patients, some of whom were coinfected with M. abscessus, relapsed after the therapy was completed [97].
Rifampicin embedded in the membrane of hydrogenated soy phosphatidylcholine-dipalmitoylphosphatidylcholine (1:1) liposomes reduced the viability of M. abscessus in infected, differentiated THP-1 human monocytic leukemia cells, significantly more than the free drug [84].
7. Future Directions, Challenges and Limitations
Liposomes, in addition to being biocompatible and undergoing natural degradation, offer the advantages of easy synthesis and modification with various agents. Their ability to encapsulate both hydrophilic and hydrophobic first-line anti-tuberculosis drugs, as well as other potential therapeutic compounds, further enhances their versatility. Additionally, liposomes can be utilized as vaccine carriers against tuberculosis. In the near future, formulations developed with liposomal technology hold promise for patentability, while providing effective solutions in tuberculosis treatment, ultimately improving patients' quality of life and minimizing the adverse impacts of the disease on public health. One of the major challenges associated with liposomes is drug leakage, which can significantly impact their efficacy. The high production cost of this carrier system poses another limitation. Moreover, liposomes are prone to lipid oxidation and hydrolysis, leading to potential instability. To enhance their stability and prolong their therapeutic effect, liposomal formulations often require polymeric coating. However, this coating process further increases the complexity of synthesis and production costs, making large-scale application more challenging.
Author Contributions
Conceptualization: ND and MY; Writing, Review and Editing: MY and ND. All authors have read and agreed to the published version of the manuscript.
Funding
No extramural funding was available for this project.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statetment: Not applicable. No new data have been generated for this review.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Vilchèze, C.; Kremer, L. Acid-fast positive and acid-fast negative Mycobacterium tuberculosis: The Koch paradox. Microbiology Spectrum 2017, 5, 10.1128. [Google Scholar] [CrossRef]
- Muñoz-Elías, E.J.; Timm, J.; Botha, T.; Chan, W.-T.; Gomez, J.E.; McKinney, J.D. Replication dynamics of Mycobacterium tuberculosis in chronically infected mice. Infection and Immunity 2005, 73, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Düzgüneş, N. Medical microbiology and immunology for dentistry. 2015.
- Daley, C.L.; Caminero, J.A. Management of multidrug-resistant tuberculosis. In Proceedings of the Seminars in Respiratory and Critical Care Medicine; 2018; pp. 310–324. [Google Scholar]
- Matteelli, A.; Lovatti, S.; Rossi, B.; Rossi, L. Update on multidrug-resistant tuberculosis preventive therapy toward the global tuberculosis elimination. International Journal of Infectious Diseases 2025. [Google Scholar] [CrossRef] [PubMed]
- Cocorullo, M.; Stamilla, A.; Recchia, D.; Marturano, M.C.; Maci, L.; Stelitano, G. Mycobacterium abscessus Virulence Factors: An Overview of Un-Explored Therapeutic Options. International Journal of Molecular Sciences 2025, 26, 3247. [Google Scholar] [CrossRef]
- Palucci, I.; Delogu, G. Alternative therapies against Mycobacterium abscessus infections. Clinical Microbiology and Infection 2024, 30, 732–737. [Google Scholar] [CrossRef]
- Vladimirsky, M.; Ladigina, G. Antibacterial activity of liposome-entrapped streptomycin in mice infected with Mycobacterium tuberculosis. Biomedicine & Pharmacotherapy 1982, 36, 375–377. [Google Scholar]
- Ladigina, G.; Vladimirsky, M. The comparative pharmacokinetics of 3H-dihydrostreptomycin in solution and liposomal form in normal and Mycobacterium tuberculosis infected mice. Biomedicine & Pharmacotherapy 1986, 40, 416–420. [Google Scholar]
- Orozco, L.C.; Quintana, F.O.; Beltrán, R.M.; de Moreno, I.; Wasserman, M.; Rodriguez, G. The use of rifampicin and isoniazid entrapped in liposomes for the treatment of murine tuberculosis. Tubercle 1986, 67, 91–97. [Google Scholar] [CrossRef]
- Agarwal, A.; Kandpal, H.; Gupta, H.; Singh, N.; Gupta, C. Tuftsin-bearing liposomes as rifampin vehicles in treatment of tuberculosis in mice. Antimicrobial Agents and Chemotherapy 1994, 38, 588–593. [Google Scholar] [CrossRef]
- Düzgüneş, N.; Perumal, V.K.; Kesavalu, L.; Goldstein, J.A.; Debs, R.J.; Gangadharam, P. Enhanced effect of liposome-encapsulated amikacin on Mycobacterium avium-M. intracellulare complex infection in beige mice. Antimicrobial Agents and Chemotherapy 1988, 32, 1404–1411. [Google Scholar] [CrossRef]
- Cynamon, M.; Swenson, C.; Palmer, G.; Ginsberg, R. Liposome-encapsulated-amikacin therapy of Mycobacterium avium complex infection in beige mice. Antimicrobial Agents and Chemotherapy 1989, 33, 1179–1183. [Google Scholar] [CrossRef] [PubMed]
- Bermudez, L.E.; Vau-Young, A.O.; Lin, J.-P.; Cogger, J.; Young, L.S. Treatment of disseminated Mycobacterium avium complex infection of beige mice with liposome-encapsulated aminoglycosides. Journal of Infectious Diseases 1990, 161, 1262–1268. [Google Scholar] [CrossRef] [PubMed]
- Klemens, S.; Cynamon, M.; Swenson, C.; Ginsberg, R. Liposome-encapsulated-gentamicin therapy of Mycobacterium avium complex infection in beige mice. Antimicrobial Agents and Chemotherapy 1990, 34, 967–970. [Google Scholar] [CrossRef]
- Kesavalu, L.; Goldstein, J.A.; Debs, R.J.; Düzgüneş, N.; Gangadharam, P.R. Differential effects of free and liposome encapsulated amikacin on the survival of Mycobacterium avium complex in mouse peritoneal macrophages. Tubercle 1990, 71, 215–217. [Google Scholar] [CrossRef]
- Saito, H.; Tomioka, H. Therapeutic efficacy of liposome-entrapped rifampin against Mycobacterium avium complex infection induced in mice. Antimicrobial \Agents and Chemotherapy 1989, 33, 429–433. [Google Scholar] [CrossRef] [PubMed]
- Düzgüneş, N.; Ashtekar, D.R.; Flasher, D.L.; Ghori, N.; Debs, R.J.; Friend, D.S.; Gangadharam, P.R. Treatment of Mycobacterium avium-intracellulare complex infection in beige mice with free and liposome-encapsulated streptomycin: role of liposome type and duration of treatment. Journal of Infectious Diseases 1991, 164, 143–151. [Google Scholar] [CrossRef]
- Gangadharam, P.R.; Ashtekar, D.A.; Ghori, N.; Goldstein, J.A.; Debs, R.J.; Düzgüneş, N. Chemotherapeutic potential of free and liposome encapsulated streptomycin against experimental Mycobacterium avium complex infections in beige mice. Journal of Antimicrobial Chemotherapy 1991, 28, 425–435. [Google Scholar] [CrossRef]
- Bozzuto, G.; Molinari, A. Liposomes as nanomedical devices. International Journal of Nanomedicine 2015. [Google Scholar] [CrossRef]
- Pande, S. Liposomes for drug delivery: review of vesicular composition, factors affecting drug release and drug loading in liposomes. Artificial Cells, Nanomedicine, and Biotechnology 2023, 51, 428–440. [Google Scholar] [CrossRef]
- Daraee, H.; Etemadi, A.; Kouhi, M.; Alimirzalu, S.; Akbarzadeh, A. Application of liposomes in medicine and drug delivery. Artificial Cells, Nanomedicine, and Biotechnology 2014, 44, 381–391. [Google Scholar] [CrossRef]
- Düzgüneş, N.; Nir, S. Mechanisms and kinetics of liposome–cell interactions. Advanced Drug Delivery Reviews 1999, 40, 3–18. [Google Scholar] [CrossRef]
- Karimi, M.; Aslanabadi, A.; Atkinson, B.; Hojabri, M.; Munawwar, A.; Zareidoodeji, R.; Ray, K.; Habibzadeh, P.; Parlayan, H.N.K.; DeVico, A.; et al. Subcutaneous liposomal delivery improves monoclonal antibody pharmacokinetics in vivo. Acta Biomaterialia 2025. [Google Scholar] [CrossRef] [PubMed]
- Xing, H.; Pan, X.; Hu, Y.; Yang, Y.; Zhao, Z.; Peng, H.; Wang, J.; Li, S.; Hu, Y.; Li, G.; et al. High molecular weight hyaluronic acid-liposome delivery system for efficient transdermal treatment of acute and chronic skin photodamage. Acta Biomaterialia 2024, 182, 171–187. [Google Scholar] [CrossRef]
- Xiao, P.; Wang, H.; Liu, H.; Yuan, H.; Guo, C.; Feng, Y.; Qi, P.; Yin, T.; Zhang, Y.; He, H.; et al. Milk exosome–liposome hybrid vesicles with self-adapting surface properties overcome the sequential absorption barriers for oral delivery of peptides. ACS Nano 2024, 18, 21091–21111. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Huang, Y.; Shen, W.; Zeng, Y.; Miao, Y.; Feng, N.; Ci, T. Effects of surface charge of inhaled liposomes on drug efficacy and biocompatibility. Pharmaceutics 2025, 17. [Google Scholar] [CrossRef] [PubMed]
- Konduri, K.S.; Nandedkar, S.; Düzgüneş, N.; Suzara, V.; Artwohl, J.; Bunte, R.; Gangadharam, P.R. Efficacy of liposomal budesonide in experimental asthma. Journal of Allergy and Clinical Immunology 2003, 111, 321–327. [Google Scholar] [CrossRef]
- Heurtault, B.; Frisch, B.; Pons, F. Liposomes as delivery systems for nasal vaccination: strategies and outcomes. Expert Opinion on Drug Delivery 2010, 7, 829–844. [Google Scholar] [CrossRef]
- Pande, S. Factors affecting response variables with emphasis on drug release and loading for optimization of liposomes. Artificial Cells, Nanomedicine, and Biotechnology 2024, 52, 334–344. [Google Scholar] [CrossRef]
- Izadiyan, Z.; Misran, M.; Kalantari, K.; Webster, T.; Kia, P.; Basrowi, N.; Rasouli, E.; Shameli, K. Advancements in liposomal nanomedicines: innovative formulations, therapeutic applications, and future directions in precision medicine. International Journal of Nanomedicine 2025, Volume 20, 1213–1262. [Google Scholar] [CrossRef]
- Chai, C.; Park, J. Food liposomes: Structures, components, preparations, and applications. Food Chemistry 2024, 432. [Google Scholar] [CrossRef]
- Düzgüneş, N. Liposomes, Part G; Academic Press: 2009; Volume 465.
- Awasthi, V.D.; Garcia, D.; Goins, B.A.; Phillips, W.T. Circulation and biodistribution profiles of long-circulating PEG-liposomes of various sizes in rabbits. International Journal of Pharmaceutics 2003, 253, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Lian, J.; Tang, X.; Gui, Y.; Lu, S.; Song, Y.; Deng, Y. Impact of formulation parameters and circulation time on PEGylated liposomal doxorubicin related hand-foot syndrome. International Journal of Pharmaceutics 2024, 665. [Google Scholar] [CrossRef]
- Du, Q.; Liu, Y.; Fan, M.; Wei, S.; Ismail, M.; Zheng, M. PEG length effect of peptide-functional liposome for blood brain barrier (BBB) penetration and brain targeting. Journal of Controlled Release 2024, 372, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Werner, J.; Umstätter, F.; Hertlein, T.; Mühlberg, E.; Beijer, B.; Wohlfart, S.; Zimmermann, S.; Haberkorn, U.; Ohlsen, K.; Fricker, G.; et al. Oral delivery of the vancomycin derivative FU002 by a surface-modified liposomal nanocarrier. Advanced Healthcare Materials 2024, 13. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Yu, Q.; Liu, Y.; Sheng, Q.; Shi, K.; Wang, Y.; Li, M.; Zhang, Z.; He, Q. Synergistic cytotoxicity and co-autophagy inhibition in pancreatic tumor cells and cancer-associated fibroblasts by dual functional peptide-modified liposomes. Acta Biomaterialia 2019, 99, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Khorshid, S.; Montanari, M.; Benedetti, S.; Moroni, S.; Aluigi, A.; Canonico, B.; Papa, S.; Tiboni, M.; Casettari, L. A microfluidic approach to fabricate sucrose decorated liposomes with increased uptake in breast cancer cells. European Journal of Pharmaceutics and Biopharmaceutics 2022, 178, 53–64. [Google Scholar] [CrossRef]
- Urban-Chmiel, R.; Marek, A.; Stępień-Pyśniak, D.; Wieczorek, K.; Dec, M.; Nowaczek, A.; Osek, J. Antibiotic resistance in bacteria—a review. Antibiotics 2022, 11. [Google Scholar] [CrossRef]
- Ferreira, M.; Ogren, M.; Dias, J.N.R.; Silva, M.; Gil, S.; Tavares, L.; Aires-da-Silva, F.; Gaspar, M.M.; Aguiar, S.I. Liposomes as antibiotic delivery systems: a promising nanotechnological strategy against antimicrobial resistance. Molecules 2021, 26. [Google Scholar] [CrossRef]
- Ghosh, R.; De, M. Liposome-based antibacterial delivery: an emergent approach to combat bacterial infections. ACS Omega 2023, 8, 35442–35451. [Google Scholar] [CrossRef]
- Singh, I.; Kumar, S.; Singh, S.; Wani, M.Y. Overcoming resistance: Chitosan-modified liposomes as targeted drug carriers in the fight against multidrug resistant bacteria–a review. International Journal of Biological Macromolecules 2024, 278. [Google Scholar] [CrossRef]
- Ferreira, M.; Pinto, S.N.; Aires-da-Silva, F.; Bettencourt, A.; Aguiar, S.I.; Gaspar, M.M. Liposomes as a nanoplatform to improve the delivery of antibiotics into Staphylococcus aureus biofilms. Pharmaceutics 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Alavi, S.E.; Koohi Moftakhari Esfahani, M.; Raza, A.; Adelnia, H.; Ebrahimi Shahmabadi, H. PEG-grafted liposomes for enhanced antibacterial and antibiotic activities: An in vivo study. NanoImpact 2022, 25. [Google Scholar] [CrossRef] [PubMed]
- Trucillo, P.; Ferrari, P.F.; Campardelli, R.; Reverchon, E.; Perego, P. A supercritical assisted process for the production of amoxicillin-loaded liposomes for antimicrobial applications. The Journal of Supercritical Fluids 2020, 163. [Google Scholar] [CrossRef]
- Coelho, M.P.; Pinho, J.O.; Pinto, S.N.; Gaspar, M.M. A step forwarded on the in vitro and in vivo validation of rifabutin-loaded liposomes for the management of highly virulent MRSA infections. Journal of Controlled Release 2025, 380, 348–361. [Google Scholar] [CrossRef]
- Patel, A.; Dey, S.; Shokeen, K.; Karpiński, T.M.; Sivaprakasam, S.; Kumar, S.; Manna, D. Sulfonium-based liposome-encapsulated antibiotics deliver a synergistic antibacterial activity. RSC Medicinal Chemistry 2021, 12, 1005–1015. [Google Scholar] [CrossRef] [PubMed]
- Karpuz, M.; Temel, A.; Özgenç, E.; Tekintaş, Y.; Erel-Akbaba, G.; şenyigit, Z.; Atlıhan-Gündogdu, E. 99mTc-labeled, colistin encapsulated, theranostic liposomes for Pseudomonas aeruginosa infection. AAPS PharmSciTech 2023, 24. [Google Scholar] [CrossRef]
- Wang, S.; Wang, Z.; Xu, C.; Cui, L.; Meng, G.; Yang, S.; Wu, J.; Liu, Z.; Guo, X. PEG-α-CD/AM/liposome@ amoxicillin double network hydrogel wound dressing–multiple barriers for long-term drug release. Journal of Biomaterials Applications 2021, 35, 1085–1095. [Google Scholar] [CrossRef]
- Fesendouz, S.A.; Hamishehkar, H.; Alizadeh, E.; Rahbarghazi, R.; Akbarzadeh, A.; Yousefi, S.; Milani, M. Bactericidal activity and biofilm eradication of Pseudomonas aeruginosa by liposome-encapsulated piperacillin/tazobactam. BioNanoScience 2024, 15. [Google Scholar] [CrossRef]
- Erdene, E.; Munkhjargal, O.; Batnasan, G.; Dorjbal, E.; Oidov, B.; Byambaa, A. Evaluation of liposome-encapsulated vancomycin against methicillin-resistant Staphylococcus aureus. Biomedicines 2025, 13. [Google Scholar] [CrossRef]
- Trucillo, P.; Cardea, S.; Baldino, L.; Reverchon, E. Production of liposomes loaded alginate aerogels using two supercritical CO2 assisted techniques. Journal of CO2 Utilization 2020, 39. [Google Scholar] [CrossRef]
- Bogdanov, A.; Janovák, L.; Vraneš, J.; Meštrović, T.; Ljubin-Sternak, S.; Cseh, Z.; Endrész, V.; Burián, K.; Vanić, Ž.; Virok, D.P. Liposomal encapsulation increases the efficacy of azithromycin against Chlamydia trachomatis. Pharmaceutics 2021, 14. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Wang, S.; Zou, P.; Chai, G.; Lin, Y.-W.; Velkov, T.; Li, J.; Pan, W.; Zhou, Q.T. Inhalable liposomal powder formulations for co-delivery of synergistic ciprofloxacin and colistin against multi-drug resistant Gram-negative lung infections. International Journal of Pharmaceutics 2020, 575. [Google Scholar] [CrossRef]
- Dong, Y.; Wu, T.; Jiang, T.; Zhu, W.; Chen, L.; Cao, Y.; Xiao, Y.; Peng, Y.; Wang, L.; Yu, X.; et al. Chitosan-coated liposome with lysozyme-responsive properties for on-demand release of levofloxacin. International Journal of Biological Macromolecules 2024, 269. [Google Scholar] [CrossRef]
- Nieto Ramirez, L.M.; Mehaffy, C.; Dobos, K.M. Systematic review of innate immune responses against Mycobacterium tuberculosis complex infection in animal models. Frontiers in Immunology 2025, 15. [Google Scholar] [CrossRef] [PubMed]
- Alsayed, S.S.R.; Gunosewoyo, H. Tuberculosis: pathogenesis, current treatment regimens and new drug targets. International Journal of Molecular Sciences 2023, 24. [Google Scholar] [CrossRef] [PubMed]
- Tretiakova, D.S.; Vodovozova, E.L. Liposomes as adjuvants and vaccine delivery systems. Biochemistry (Moscow), Supplement Series A: Membrane and Cell Biology 2022, 16, 1–20. [Google Scholar] [CrossRef]
- Diogo, G.R.; Hart, P.; Copland, A.; Kim, M.-Y.; Tran, A.C.; Poerio, N.; Singh, M.; Paul, M.J.; Fraziano, M.; Reljic, R. Immunization with Mycobacterium tuberculosis antigens encapsulated in phosphatidylserine liposomes improves protection afforded by BCG. Frontiers in Immunology 2019, 10. [Google Scholar] [CrossRef]
- Mansury, D.; Ghazvini, K.; Jamehdar, S.A.; Badiee, A.; Tafaghodi, M.; Nikpoor, A.R.; Amini, Y.; Jaafari, M.R. Increasing cellular immune response in liposomal formulations of DOTAP encapsulated by fusion protein Hspx, PPE44, and Esxv, as a potential tuberculosis vaccine candidate. Reports of Biochemistry & Molecular Biology 2019, 7, 156. [Google Scholar]
- Zhou, S.; Luo, Y.; Lovell, J.F. Vaccine approaches for antigen capture by liposomes. Expert Review of Vaccines 2023, 22, 1022–1040. [Google Scholar] [CrossRef]
- Panthi, V.K.; Fairfull-Smith, K.E.; Islam, N. Antibiotic loaded inhalable liposomal nanoparticles against lower respiratory tract infections: challenges, recent advances, and future perspectives. Journal of Drug Delivery Science and Technology 2024, 94. [Google Scholar] [CrossRef]
- Sang, N.; Jiang, L.; Wang, Z.; Zhu, Y.; Lin, G.; Li, R.; Zhang, J. Bacteria-targeting liposomes for enhanced delivery of cinnamaldehyde and infection management. International Journal of Pharmaceutics 2022, 612. [Google Scholar] [CrossRef] [PubMed]
- Justo, O.R.; Moraes, Â.M. Incorporation of antibiotics in liposomes designed for tuberculosis therapy by inhalation. Drug Delivery 2003, 10, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim Bekraki, A. Liposomes-and niosomes-based drug delivery systems for tuberculosis treatment. In Nanotechnology Based Approaches for Tuberculosis Treatment; 2020; pp. 107-122.
- Al-Jipouri, A.; Almurisi, S.H.; Al-Japairai, K.; Bakar, L.M.; Doolaanea, A.A. Liposomes or extracellular vesicles: a comprehensive comparison of both lipid bilayer vesicles for pulmonary drug delivery. Polymers 2023, 15. [Google Scholar] [CrossRef]
- Kaul, A.; Chaturvedi, S.; Attri, A.; Kalra, M.; Mishra, A.K. Targeted theranostic liposomes: rifampicin and ofloxacin loaded pegylated liposomes for theranostic application in mycobacterial infections. RSC Advances 2016, 6, 28919–28926. [Google Scholar] [CrossRef]
- Altamimi, M.A.; Hussain, A.; Imam, S.S.; Alshehri, S.; Singh, S.K.; Webster, T.J. Transdermal delivery of isoniazid loaded elastic liposomes to control cutaneous and systemic tuberculosis. Journal of Drug Delivery Science and Technology 2020, 59. [Google Scholar] [CrossRef]
- El-Ridy, M.S.; Mostafa, D.M.; Shehab, A.; Nasr, E.A.; Abd El-Alim, S. Biological evaluation of pyrazinamide liposomes for treatment of Mycobacterium tuberculosis. International Journal of Pharmaceutics 2007, 330, 82–88. [Google Scholar] [CrossRef]
- Chimote, G.; Banerjee, R. Evaluation of antitubercular drug-loaded surfactants as inhalable drug-delivery systems for pulmonary tuberculosis. Journal of Biomedical Materials Research Part A 2008, 89A, 281–292. [Google Scholar] [CrossRef]
- Nongkhlaw, R.; Nongrum, R.; Arunachalam, J.; Kalia, N.P.; Agnivesh, P.K.; Nongkhlaw, R. Drug-loaded liposomes for macrophage targeting in Mycobacterium tuberculosis: development, characterization and macrophage infection study. 3 Biotech 2025, 15. [Google Scholar] [CrossRef]
- Shrivastava, P.; Gautam, L.; Sharma, R.; Dube, D.; Vyas, S.; Vyas, S.P. Dual antitubercular drug loaded liposomes for macrophage targeting: development, characterisation, ex vivo and in vivo assessment. Journal of Microencapsulation 2020, 38, 108–123. [Google Scholar] [CrossRef]
- Kósa, N.; Zolcsák, Á.; Voszka, I.; Csík, G.; Horváti, K.; Horváth, L.; Bősze, S.; Herenyi, L. Comparison of the efficacy of two novel antitubercular agents in free and liposome-encapsulated formulations. International Journal of Molecular Sciences 2021, 22. [Google Scholar] [CrossRef]
- Zhou, S.-F.; Niu, N.-K.; Yin, J.; Yang, Y.; Wang, Z.-L.; Zhou, Z.-W.; He, Z.-X.; Chen, X.-W.; Zhang, X.; Duan, W.; et al. Novel targeting of PEGylated liposomes for codelivery of TGF-β1 siRNA and four antitubercular drugs to human macrophages for the treatment of mycobacterial infection: a quantitative proteomic study. Drug Design, Development and Therapy 2015. [CrossRef]
- Obiedallah, M.M.; Melekhin, V.V.; Menzorova, Y.A.; Bulya, E.T.; Minin, A.S.; Mironov, M.A. Fucoidan coated liposomes loaded with novel antituberculosis agent: preparation, evaluation, and cytotoxicity study. Pharmaceutical Development and Technology 2024, 29, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Lima Salviano, T.; dos Santos Macedo, D.C.; de Siqueira Ferraz Carvalho, R.; Pereira, M.A.; de Arruda Barbosa, V.S.; dos Santos Aguiar, J.; Souto, F.O.; Carvalho da Silva, M.d.P.; Lapa Montenegro Pimentel, L.M.; Correia de Sousa, L.d.Â.; et al. Fucoidan-coated liposomes: a target system to deliver the antimicrobial drug usnic Acid to macrophages infected with mycobacterium tuberculosis. Journal of Biomedical Nanotechnology 2021, 17, 1699–1710. [Google Scholar] [CrossRef] [PubMed]
- Szachniewicz, M.M.; van den Eeden, S.J.F.; van Meijgaarden, K.E.; Franken, K.L.M.C.; van Veen, S.; Geluk, A.; Bouwstra, J.A.; Ottenhoff, T.H.M. Cationic pH-sensitive liposome-based subunit tuberculosis vaccine induces protection in mice challenged with Mycobacterium tuberculosis. European Journal of Pharmaceutics and Biopharmaceutics 2024, 203. [Google Scholar] [CrossRef]
- Vyas, S.P.; Kannan, M.E.; Jain, S.; Mishra, V.; Singh, P. Design of liposomal aerosols for improved delivery of rifampicin to alveolar macrophages. International Journal of Pharmaceutics 2004, 269, 37–49. [Google Scholar] [CrossRef]
- Avdeev, V.V.; Kuzin, V.V.; Vladimirsky, M.A.; Vasilieva, I.A.E. Experimental studies of the liposomal form of lytic mycobacteriophage D29 for the treatment of tuberculosis infection. Microorganisms 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, S.L.; Reese, V.A.; Larsen, S.E.; Pecor, T.; Brown, B.P.; Granger, B.; Podell, B.K.; Fox, C.B.; Reed, S.G.; Coler, R.N. Therapeutic efficacy against Mycobacterium tuberculosis using ID93 and liposomal adjuvant formulations. Frontiers in Microbiology 2022, 13. [Google Scholar] [CrossRef]
- Maringolo Ribeiro, C.; Augusto Roque-Borda, C.; Carolina Franzini, M.; Fernanda Manieri, K.; Manaia Demarqui, F.; Leite Campos, D.; Temperani Amaral Machado, R.; Cristiane da Silva, I.; Tavares Luiz, M.; Delello Di Filippo, L.; et al. Liposome-siderophore conjugates loaded with moxifloxacin serve as a model for drug delivery against Mycobacterium tuberculosis. International Journal of Pharmaceutics 2024, 655. [Google Scholar] [CrossRef]
- Pires, D.; Mandal, M.; Pinho, J.; Catalão, M.J.; Almeida, A.J.; Azevedo-Pereira, J.M.; Gaspar, M.M.; Anes, E. Liposomal delivery of saquinavir to macrophages overcomes cathepsin blockade by Mycobacterium tuberculosis and helps control the phagosomal replicative niches. International Journal of Molecular Sciences 2023, 24. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, F.; Hanieh, P.N.; Sennato, S.; De Santis, F.; Forte, J.; Fraziano, M.; Casciardi, S.; Marianecci, C.; Bordi, F.; Carafa, M. Rifampicin-liposomes for Mycobacterium abscessus infection treatment: intracellular uptake and antibacterial activity evaluation. Pharmaceutics 2021, 13. [Google Scholar] [CrossRef]
- To, K.; Cao, R.; Yegiazaryan, A.; Owens, J.; Nguyen, T.; Sasaninia, K.; Vaughn, C.; Singh, M.; Truong, E.; Medina, A.; et al. Effects of oral liposomal glutathione in altering the immune responses against Mycobacterium tuberculosis and the Mycobacterium bovis BCG strain in individuals with type 2 diabetes. Frontiers in Cellular and Infection Microbiology 2021, 11. [Google Scholar] [CrossRef]
- Mehnath, S.; Rajan, M.; Jeyaraj, M. Immunomodulating polyorganophosphazene-arginine layered liposome antibiotic delivery vehicle against pulmonary tuberculosis. Journal of Drug Delivery Science and Technology 2021, 66. [Google Scholar] [CrossRef]
- Liu, P.; Guo, B.; Wang, S.; Ding, J.; Zhou, W. A thermo-responsive and self-healing liposome-in-hydrogel system as an antitubercular drug carrier for localized bone tuberculosis therapy. International Journal of Pharmaceutics 2019, 558, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Miretti, M.; Juri, L.; Cosiansi, M.C.; Tempesti, T.C.; Baumgartner, M.T. Antimicrobial effects of ZnPc delivered into liposomes on multidrug resistant (MDR)-Mycobacterium tuberculosis. ChemistrySelect 2019, 4, 9726–9730. [Google Scholar] [CrossRef]
- Sciolla, F.; Truzzolillo, D.; Chauveau, E.; Trabalzini, S.; Di Marzio, L.; Carafa, M.; Marianecci, C.; Sarra, A.; Bordi, F.; Sennato, S. Influence of drug/lipid interaction on the entrapment efficiency of isoniazid in liposomes for antitubercular therapy: a multi-faced investigation. Colloids and Surfaces B: Biointerfaces 2021, 208. [Google Scholar] [CrossRef]
- Izzo, A.A.; Baldwin, S.L.; Reese, V.A.; Larsen, S.E.; Beebe, E.; Guderian, J.; Orr, M.T.; Fox, C.B.; Reed, S.G.; Coler, R.N. Prophylactic efficacy against Mycobacterium tuberculosis using ID93 and lipid-based adjuvant formulations in the mouse model. Plos One 2021, 16. [Google Scholar] [CrossRef]
- van Zyl, L.; Viljoen, J.M.; Haynes, R.K.; Aucamp, M.; Ngwane, A.H.; du Plessis, J. Topical delivery of artemisone, clofazimine and decoquinate encapsulated in vesicles and their in vitro efficacy against Mycobacterium tuberculosis. AAPS PharmSciTech 2019, 20. [Google Scholar] [CrossRef]
- Nkanga, C.I.; Krause, R.W.M. Encapsulation of Isoniazid-conjugated phthalocyanine-in-cyclodextrin-In-Liposomes Using Heating Method. Scientific Reports 2019, 9. [Google Scholar] [CrossRef] [PubMed]
- Truzzi, E.; Meneghetti, F.; Mori, M.; Costantino, L.; Iannuccelli, V.; Maretti, E.; Domenici, F.; Castellano, C.; Rogers, S.; Capocefalo, A.; et al. Drugs/lamellae interface influences the inner structure of double-loaded liposomes for inhaled anti-TB therapy: An in-depth small-angle neutron scattering investigation. Journal of Colloid and Interface Science 2019, 541, 399–406. [Google Scholar] [CrossRef]
- Johnson, M.M.; Odell, J.A. Nontuberculous mycobacterial pulmonary infections. Journal of thoracic disease 2014, 6, 210. [Google Scholar]
- Ehlers, S.; Bucke, W.; Leitzke, S.; Fortmann, L.; Smith, D.; Hänsch, H.; Hahn, H.; Bancroff, G.; Müller, R. Liposomal amikacin for treatment of M. avium infections in clinically relevant experimental settings. Zentralblatt für Bakteriologie 1996, 284, 218–231. [Google Scholar] [CrossRef]
- Zhang, J.; Leifer, F.; Rose, S.; Chun, D.Y.; Thaisz, J.; Herr, T.; Nashed, M.; Joseph, J.; Perkins, W.R.; DiPetrillo, K. Amikacin liposome inhalation suspension (ALIS) penetrates non-tuberculous mycobacterial biofilms and enhances amikacin uptake into macrophages. Frontiers in Microbiology 2018, 9, 915. [Google Scholar] [CrossRef] [PubMed]
- Loukeri, A.A.; Papathanassiou, E.; Kavvada, A.; Kampolis, C.F.; Pantazopoulos, I.; Moschos, C.; Papavasileiou, A. Amikacin liposomal inhalation suspension for non-tuberculous mycobacteria lung infection: a Greek observational study. Medicina 2024, 60, 1620. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Treatment pathways of antibacterial drug-loaded liposomes against bacteria. (Reproduced from [42]).
Figure 1.
Treatment pathways of antibacterial drug-loaded liposomes against bacteria. (Reproduced from [42]).
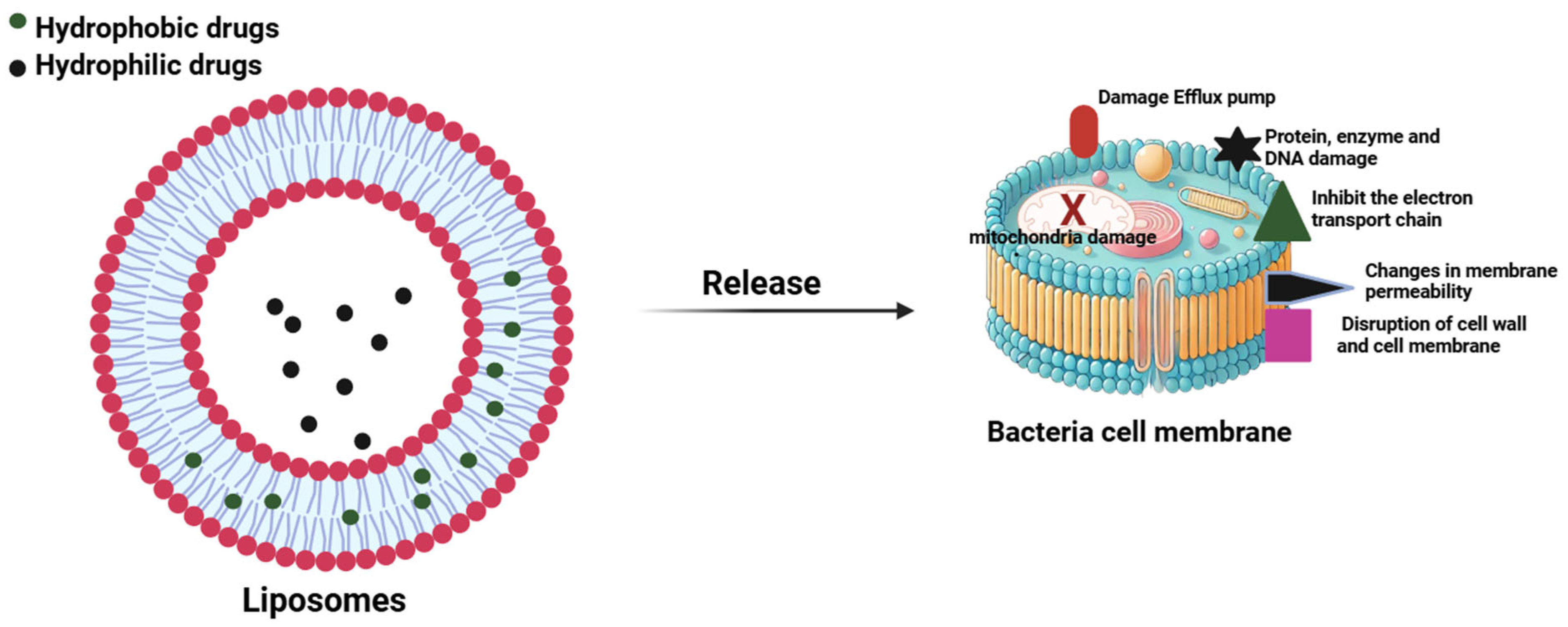
Figure 2.
Antibiotic-loaded liposomes as a strategy to overcome tuberculosis resistance and enhance treatment efficacy.
Figure 2.
Antibiotic-loaded liposomes as a strategy to overcome tuberculosis resistance and enhance treatment efficacy.
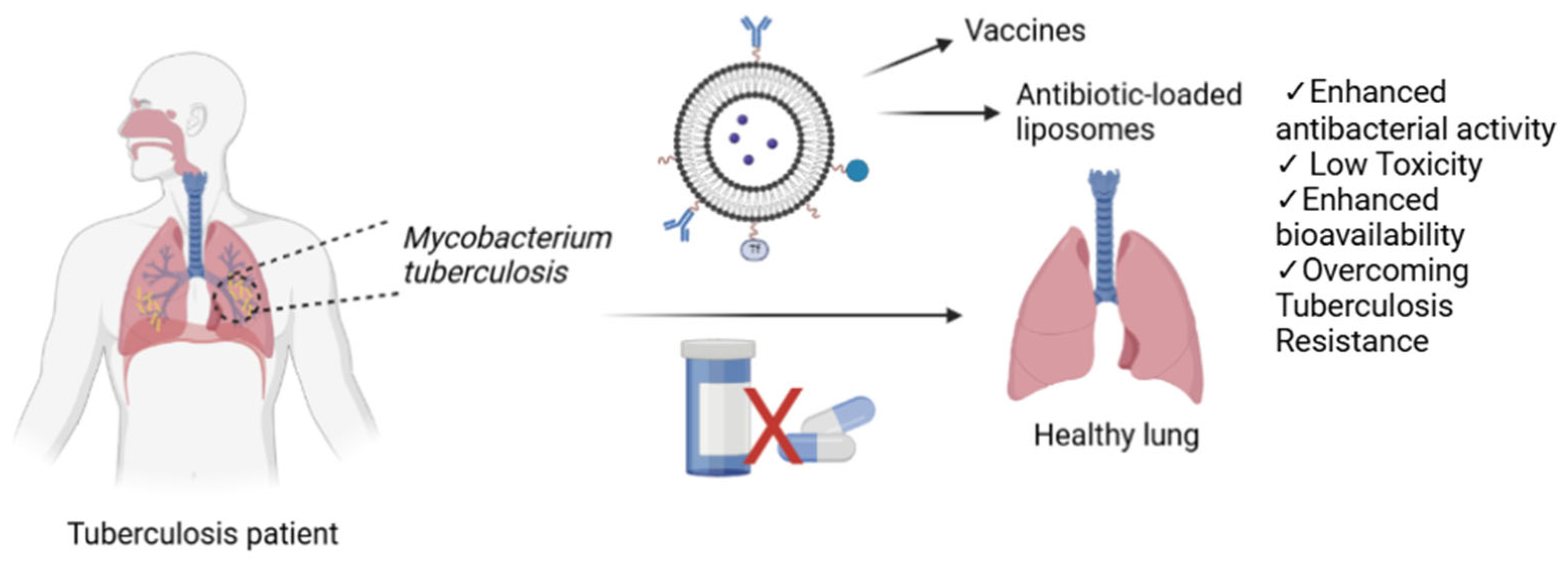

Table 1.
Overview of the Effect of Antibiotic-Loaded Liposomes Against Bacterial Infections.
| Drug | Method | Size | Target | Remarks | References |
| Rifabutin | Dehydration-rehydration | 100–115 nm | MRSA biofilm | Rifabutin-loaded liposomal formulations demonstrated superior efficacy compared to free vancomycin | [47] |
| Tetracycline, Amoxicillin | - | 270–340 nm | MRSA | Drug-loaded liposomes enhance the cellular uptake of antibiotics, thereby providing more effective treatment compared to their free forms. | [48] |
| Colistin | Thin layer hydration | 73–217 nm | Pseudomonas aeruginosa infection | Colistin-loaded cationic liposomes, with an encapsulation efficiency of 77%, had low MIC values against Pseudomonas aeruginosa. | [49] |
| Amoxicillin | Film hydration method | 210 nm | Staphylococcus aureus infection | Amoxicillin-loaded PEG--cyclodextrin- acrylamide-liposomes were incorporated into biocompatible hydrogels to prepare a wound dressing. The formulation demonstrated controlled drug release and effective antibacterial activity. | [50] |
| Piperacillin sodium | Film hydration method | 94.49 nm | Antibiotic resistance of clinical isolates of Pseudomonas aeruginosa | Liposome-loaded Piperacillin exhibited superior antibacterial activity at a lower MIC value compared to its free form. | [51] |
| Vancomycin | Freeze–thaw method | 157 nm | MRSA | At a 1:102 dilution, free vancomycin failed to inhibit bacterial growth, whereas the liposome-loaded form achieved 100% inhibition. | [52] |
| Ampicillin | SuperLip | 200 nm | - | Ampicillin-loaded liposomes were entrapped in alginate gels. This method resulted in enhanced encapsulation efficiency and improved polydispersity index values, indicating a more effective formulation. | [53] |
| Azithromycin | Proliposome | 164- 187 nm | Chlamydia trachomatis | The formulations exhibited at least twofold higher activity compared to the free form against both clinical isolates and bacterial strains. | [54] |
| Ciprofloxacin and colistin | Thin film evaporation and sonication | 102.1- 119.7 nm | Clinical isolates of Pseudomonas aeruginosa H131300444 and P. aeruginosa H133880624 | The formulation exhibited effective antibacterial properties against Pseudomonas aeruginosa, a multidrug-resistant Gram-negative bacterium responsible for pulmonary infections, while showing no cytotoxic effects on A549 cells. However, the encapsulation efficiency for both drugs remained below 50%. | [55] |
| Levofloxacin | Film hydration method | 127.6 nm | Staphylococcus aureus | Levofloxacin-loaded liposome formulations were coated with chitosan (CS). Following CS coating, an increase in particle size was observed, along with an enhancement in antibacterial activity. | [56] |
Table 2.
New Liposomal Strategies Against Tuberculosis.
| Drug | Method | Size | Remarks | References |
| Cationic pH-sensitive liposome | Thin-film hydration | 164.6 nm | pH-sensitive cationic liposomes formulated with the Ag85B-ESAT6-Rv2034 fusion antigen and CpG and MPLA adjuvants have been shown to induce potent polyfunctional CD4⁺ and CD8⁺ T-cell responses. Additionally, an increase in CD69⁺ B-cell sub-populations was observed. | [78] |
| Anionic and neutral liposomes | - | For improved pulmonary TB treatment, ID93 plus GLA-containing liposomal adjuvant formulations were developed. However, the anionic or neutral liposome + QS-21 liposomal formulations did not result in a significant reduction in M. tuberculosis bacterial load. Nevertheless, these formulations were observed to induce distinct immune responses. | [81] | |
| Moxifloxacin loaded liposome-siderophore conjugates | Film hydration technique | 200 nm | Liposome formulations with a spherical shape had an encapsulation efficiency of 46 % and demonstrated anti-TB activity with a MIC value of 0.32 µg/mL. | [82] |
| Saquinavir | Thin-film hydration | 116 nm | In the treatment of multidrug- and extensively drug-resistant M. tuberculosis strains, negatively charged Saquinavir-loaded liposomes were shown to enhance intracellular killing activity by human macrophages. | [83] |
| Rifampicin | Thin-Layer Evaporation | 117 nm | The prepared formulation demonstrated a greater reduction in intracellular M. abscessus viability compared to the free form of the drug. | [84] |
| Oral liposomal glutathione supplementation | - | - | Commercially available liposomal glutathione supplementation (L-GSH) has been shown to reduce oxidative stress in patients with type 2 diabetes mellitus (T2DM). In vitro models have demonstrated its ability to decrease intracellular mycobacteria. | [85] |
| Rifampicin and isoniazid |
Lipid film hydration, sonication and extrusion | - | Antibiotic loaded, polyorganophosphazene-arginine-grafted liposomes exhibited a 73% RIF and 80% IZN release at endosomal pH. The liposomes demonstrated a dose-dependent inhibition of M. tuberculosis growth in culture medium. | [86] |
| N′-Dodecanoylisonicotinohydrazide | ∼130 nm | For use in localized tuberculosis treatment, the Isoniazid derivative N′dodecanoylisonicotinohydrazide, a commonly used agent in tuberculosis therapy, was loaded into liposomes. PLGA-PEG-PLGA systems were incorporated to develop thermosensitive and self-healing hydrogel systems. Data obtained from in vivo microdialysis studies demonstrated the rapid release of the drug into the synovial fluid. | [87] | |
| Coumaran (2,3-dihydrobenzofuran) derivatives—TB501 and TB515— | Thin film hydration | ∼60 nm | The liposome formulation prepared with TB515 exhibited high encapsulation efficiency. Multicomponent pH-sensitive stealth liposomes encapsulating TB501 were highly effective against M. tuberculosis in macrophage cell lines. | [74] |
| Zn-phthalocyanine | Ethanol injection | 134 nm | ZnPC-loaded liposomes, prepared for the treatment of Rifampin-Isoniazid-resistant M. tuberculosis strains, achieved a 99.9% cell death rate in vitro through photodynamic therapy (PDT). | [88] |
| Isoniazid | Thin-film hydration | 37–45 nm | Biocompatible hydrogenated soy phosphatidylcholine-phosphatidylglycerol liposomes were developed as isoniazid carriers. The encapsulation efficiency was determined using UV and Laser Transmission Spectroscopy. | [89] |
| Glucopyranosyl lipid adjuvant (GLA) and the experimental tuberculosis vaccine, ID93, composed of four M. tuberculosis antigens |
Thin-film hydration, sonication, homogenization | 50–87 nm | For use as a vaccine in the treatment of Mycobacterium tuberculosis, formulations containing a TLR4 agonist (GLA) and QS21, in combination with ID93, were developed. In an in vivo model, these formulations demonstrated a reduction in bacterial load in the lungs of mice infected with M. tuberculosis. Clinical studies involving human participants are ongoing to evaluate the safety, tolerability, and immunogenicity of the developed formulations. | [90] |
| Artemisone, Clofazimine and Decoquinate | Thin-film hydration | 147, 482, 253 nm |
Drug-loaded liposomes, synthesized in various sizes, exhibited 32–42% inhibition of M. tuberculosis growth in culture medium. By contrast, drug-free liposomes induced only 12% inhibition. | [91] |
| Isoniazid-conjugated Phthalocyanine | “Heating Method” | 150–650 nm | A complex of γ-Cyclodextrin with Isoniazid-conjugated Phthalocyanine, was incorporated into crude soybean lecithin liposomes using a simple and measurable heating method. This pH-sensitive formulation exhibited 100% drug release at pH 4.4, while releasing only 40% at pH 7.4, demonstrating its potential applicability in targeted therapies. | [92] |
| Isoniazid and Rifampicin | Reverse Phase Evaporation | 332 - 361 nm | Liposomal formulations loaded with anti-TB drugs Isoniazid, Rifampicin, and their combination were developed for inhaled therapy. Isoniazid formulations exhibited a faster release compared to Rifampicin formulations, while their encapsulation efficiencies were found to be similar. | [93] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



