Submitted:
30 April 2025
Posted:
02 May 2025
You are already at the latest version
Abstract
Background and objectives: The prognostic immune and nutritional index (PINI) was reported to be clinically relevant for colorectal cancer prognosis. Herein, the utility of PINI as a prognostic factor for the survival of patients with gastric cancer (GC) was investigated. Methods: We retrospectively analyzed 492 patients with stage I–III GC, predominantly of Asian descent, who underwent curative-intent gastrectomy. Multivariate Cox regression analysis identified independent predictors of overall survival (OS). Model performance was evaluated using the concordance index (C-index), integrated area under the curve (iAUC), time-dependent AUC, integrated discrimination improvement (IDI), and continuous net reclassification improvement (cNRI). Results: The PINI score—calculated as [albumin (g/dL) × 0.9] − [absolute monocyte count (/μL) × 0.0007]—was found to be independently associated with OS (p < 0.001). Additional independent prognostic factors included age, body mass index, 5-factor modified frailty index, tumor–node–metastasis (TMN) stage, gastrectomy type, and anemia. The full model that included all significant covariates outperformed the baseline TNM model, showing significantly higher C-index and iAUC values (both p < 0.001). Compared with an intermediate model, which excluded PINI, the full model demonstrated a superior C-index and iAUC (both p = 0.004). Although the observed improvements in AUC, IDI, and cNRI at 3 years were not statistically significant, the full model achieved significant gains in all three metrics at 5 years, underscoring the added long-term prognostic value of the PINI score. Conclusion: PINI score is a significant independent predictor of survival in patients with GC who underwent curative-intent surgery. Its inclusion in prognostic models enhances the long-term predictive accuracy for survival, supporting its potential role in guiding personalized postoperative management. External validation in larger multi-ethnic prospective cohorts is essential to confirm its generalizability and to establish its role in routine clinical practice.
Keywords:
gastrectomy
; monocytes
; serum albumin
; stomach neoplasm
1. Introduction
Gastrectomy is the primary curative treatment for patients with tumor–node–metastasis (TNM) stage I–III gastric cancer (GC); however, these patients are still at risk of recurrence and death. While the TNM staging system remains the cornerstone for predicting survival in patients with cancer, it does not fully account for biological variability among individuals. Factors such as tumor heterogeneity, differential treatment responses, and patient-specific characteristics can lead to substantial differences in outcomes among patients classified within the same TNM stage [1,2]. Thus, identifying reliable biomarkers to accurately predict survival is still warranted, as they may offer valuable prognostic insights to clinicians, enhance decision-making both before and after surgery, and ultimately improve patient outcomes.
Serum albumin levels have long been considered a crucial prognostic marker in cancer. Hypoalbuminemia, a well-established sign of poor nutritional status, is associated with high risk for postoperative infectious complications and poor survival outcomes in patients with GC [3,4]. Additionally, various nutritional indices that include albumin have demonstrated prognostic significance. The prognostic nutritional index (PNI), which combines albumin levels with absolute lymphocyte count (ALC), was reported to be strongly associated with overall survival (OS) of patients with GC [5]. Similarly, the geriatric nutritional risk index, which incorporates albumin levels, body weight, and height, has gained recognition for its role in predicting outcomes in patients with cancer, including those with GC [5]. The controlling nutritional status score, which evaluates albumin, total cholesterol, and ALC levels, is an established tool for assessing nutritional and immune status, with its prognostic value for GC being supported by multiple studies [6]. Furthermore, several other markers were combined with albumin levels aiming to improve cancer prognosis, namely bilirubin [7], globulin [8], fibrinogen [9], C-reactive protein (CRP) [10], carcinoembryonic antigen [11], neutrophil-to-lymphocyte ratio (NLR) [12], and platelet count [13]. More complex indices such as the CALLY index (CRP, albumin, and ALC) [14] and HALP score (hemoglobin, albumin, ALC, and platelet count) [15] have also emerged as comprehensive tools that reflect both nutritional and inflammatory states.
Monocyte-based markers have also attracted significant attention because of their relevance in cancer progression. For example, an elevated absolute monocyte count (AMC) was implicated in promoting tumor growth and angiogenesis, supporting immune evasion, and facilitating the formation of tumor-associated macrophages (TAMs) via chemokine-driven differentiation at the tumor site [16,17,18]. Composite indices incorporating AMC, such as the lymphocyte-to-monocyte ratio [19], monocyte-to-lymphocyte ratio (MLR) [20], monocyte and lymphocyte count prognostic score [21], and systemic inflammatory response index (SIRI; comprising absolute neutrophil count [ANC], AMC, and ALC) [22], were also associated with prognosis in various cancers, including GC. Nevertheless, the prognostic significance of the AMC and AMC-based indices remains underexplored, and no consensus has been reached regarding their clinical applicability, highlighting the need for further validation.
The prognostic inflammatory and nutritional index (PINI), which is calculated as [albumin (g/dL) × 0.9] − [AMC (/μL) × 0.0007], was recently demonstrated to hold potential for predicting survival outcomes in colorectal cancer [23]. Subsequent studies validated its predictive utility in patients with stage I–III colorectal cancer [24,25]. This study aimed to assess the prognostic significance of the PINI score in patients with stage I–III GC who underwent curative gastrectomy.
2. Materials and Methods
2.1. Study Population
This retrospective study included patients who underwent curative-intent gastrectomy for GC at the Kyung Hee University Hospital (Gangdong, Korea), between October 2006 and July 2018. Eligible patients met the following criteria: (i) histologically confirmed primary GC according to the Lauren classification [26]; (ii) stage I–III disease as defined by the 8th edition of the American Joint Committee on Cancer TNM staging system [27]; and (iii) complete (R0) resection with microscopically negative margins. Patients were excluded if they had a history of other malignancies within the previous 5 years, had received prior anticancer therapy, had active infections or autoimmune disorders, or lacked available preoperative blood counts or serum albumin data.
2.2. Baseline Clinical Characteristics
The collected clinicopathological parameters included age, sex, body mass index (BMI), American Society of Anesthesiologists physical status (ASA-PS) classification [28], and the 5-factor modified frailty index (mFI-5) [29,30]. Tumor characteristics included the extent of the primary tumor (T stage), regional lymph node involvement (N stage), TNM stage, and histological type. Additional pathological features included identification of lymphatic, vascular, and perineural invasion. Surgical and treatment-related variables included the type of gastrectomy (TOG), administration of adjuvant therapy, and length of stay (LOS).
Laboratory parameters assessed were serum albumin, white blood cell count (WBC), ANC, ALC, AMC, hemoglobin levels, mean corpuscular volume (MCV), and platelet count.
PINI was calculated using the following formula: [albumin (g/dL) × 0.9] − [AMC (/μL) × 0.0007] [23]. Other albumin- or AMC-based indices included the PNI, MLR, SIRI, and HALP score. PNI was determined as 10 × albumin (g/dL) + 0.005 × ALC (/μL) [5]. MLR was calculated as AMC / ALC [20]; SIRI as (ANC × AMC) / ALC [22]; and HALP score as (hemoglobin × albumin × ALC) / platelet count [15].
Additionally, several inflammation-based indices that excluded albumin and AMC were evaluated, including the NLR, platelet-to-lymphocyte ratio (PLR), and systemic immune-inflammation index (SII). NLR was calculated as ANC / ALC [19]; PLR as platelet count / ALC [31]; and SII as (platelet count × ANC) / ALC [32].
2.3. Statistical Analysis
Overall survival (OS) was defined as the time from the date of gastrectomy to death from any cause. To reduce potential bias and preserve data integrity, continuous variables were analyzed in their original form rather than categorized. These variables are summarized using medians and interquartile ranges (IQRs) to reflect their distribution.
In addition to being analyzed as continuous variables, both age and hemoglobin levels were categorized for specific subgroup analyses. Age was dichotomized at 50 years, which is a threshold commonly used to define early-onset gastric cancer [33]. Hemoglobin levels were classified into anemia and non-anemia according to the following cutoff values for anemia: <12 g/dL for women and <13 g/dL for men [34].
Kaplan–Meier survival curves were constructed to estimate the 5-year OS and visualize survival probabilities for key prognostic variables, where applicable. Hazard ratios (HRs) and their corresponding 95% confidence intervals (CIs) were calculated using univariate Cox proportional hazards regression. Variables with a p-value < 0.05 in univariate analysis were further evaluated in a multivariate Cox regression model. Variables violating the proportional hazards assumption were excluded from the multivariate analysis. Multicollinearity was assessed using the variance inflation factor and only variables without significant collinearity were retained in the final model. For key continuous variables with significant prognostic value, their association with log relative hazard was explored using fractional polynomial modeling to account for potential non-linear effects.
The discriminatory performance of each model was assessed using the concordance index (C-index). Statistical comparisons of model performance were conducted using 1,000 bootstrap resamples. To evaluate the stability of the predictive model over time, time-dependent C-indices were estimated and plotted across a 10-year follow-up period using bootstrap cross-validation with 1,000 repetitions.
Time-dependent area under the curve (AUC) analyses were also conducted to evaluate and compare the predictive accuracy of the models for OS at 3 and 5 years post-surgery using 1,000 bootstrap resamples to ensure robust estimation. To provide a comprehensive summary measure of the model discrimination over time, the integrated AUC (iAUC), which quantifies the average AUC across the follow-up period, was computed.
Additionally, integrated discrimination improvement (IDI) and continuous net reclassification improvement (cNRI) were employed to assess the enhancement in OS prediction between models at 3 and 5 years after surgery [35,36,37].
Prognostic nomograms were constructed based on the finalized multivariable models to estimate OS probabilities for individual patients. Each predictor was assigned a score on the “Points” scale at the top of the nomogram according to its prognostic contribution. The total score was calculated by summing the points for all individual variables. The “Total Points” axis at the bottom of the nomogram allowed for summing all variable-specific points and estimate individualized 3-year and 5-year OS probabilities using the corresponding survival probability scales. Internal validation of the nomograms was performed using calibration curves generated from 1,000 bootstrap resamples to assess model accuracy and mitigate overfitting.
Spearman’s rank correlation was used to assess the strength and direction of associations between continuous variables. Strong correlations (r > 0.5 or r < −0.5) were visualized using a chord diagram to illustrate the key interrelationships. To further explore non-linear effects, generalized additive models with a gamma distribution were applied, incorporating predictors selected through least absolute shrinkage and selection operator (Lasso) regression.
To evaluate the potential interaction between serum albumin levels and AMC in predicting OS of patients with GC, we constructed a base model comprising albumin and AMC as independent variables. To assess whether the effect of albumin on OS was modified by AMC levels, we extended this model by adding an interaction term (albumin × AMC), resulting in an extended model. A likelihood ratio test, which evaluates whether the addition of an interaction term significantly improves the model fit, was used to compare the base and extended models. The predictive accuracy and fitting of the model were evaluated by calculating the C-index and the Akaike Information Criterion (AIC). To visualize the relationship between albumin levels and OS across different AMC levels, we generated plots of the predicted HRs from the Cox model with the interaction term, fixing AMC at the 25th, 50th, and 75th percentiles. This graphical analysis supported the statistical findings, reinforcing the idea that any interaction between albumin and AMC was negligible.
The p-values were two-sided, with statistical significance set at p < 0.05. All statistical analyses were performed using MedCalc (version 23.0.2) and R software (version 4.1.2).
3. Results
3.1. Clinical Characterization of the Study Cohort
The study included 492 patients diagnosed with GC, comprising predominantly Asian individuals (96.1%, n = 473), with a small proportion of Caucasians (3.9%, n = 19). The median age of the participants was 60.5 years (IQR: 52.0–70.0). The tumor location was most common in the lower region (54.3%, n = 267), followed by the middle (34.1%, n = 168), upper (10.0%, n = 49), and diffuse (1.6%, n = 8) regions. The TNM stage distribution was as follows: stage I (61.4%, n = 302), stage II (18.5%, n = 91), and stage III (20.1%, n = 99). Concerning the ASA-PS scores, 42 patients had a score of 1, 394 patients had a score of 2, and 56 patients had a score of 3. For the mFI-5 score, 199 patients scored 0, 182 scored 1, 79 scored 2, 26 scored 3, and 6 patients scored 4. Most patients underwent partial gastrectomy (79.1%, n = 389), whereas 20.9% (n = 103) underwent total gastrectomy. The median LOS was 9 days (IQR: 8–11). The median PINI score was 3.38 (IQR: 3.15–3.59) (Table 1).
3.2. Identification of Risk Factors for OS of Patients with GC
The median follow-up period was 107.5 months (IQR: 58.0–140.9 months). Kaplan–Meier survival analysis showed 5-year OS rates of 92.3%, 76.2%, and 47.4% for patients with cancer at stages I, II, and III, respectively. Univariate Cox regression analysis identified significant associations between OS and variables, including age, sex, BMI, ASA-PS, mFI-5, TNM stage, lymphatic/vascular/perineural invasion, tumor size, TOG, LOS, adjuvant chemotherapy, AMC, anemia, MCV, albumin, NLR, PLR, MLR, SII, SIRI, PNI, HALP score, and PINI scores. In multivariate analysis, when the NLR, PLR, MLR, SII, SIRI, PNI, HALP, and PINI were introduced sequentially, the model incorporating the PINI score yielded the highest C-index of 0.815 (0.784–0.846). The C-indices for models incorporating each of the other markers were as follows: 0.801 (95% CI, 0.768–0.834) for NLR, 0.801 (95% CI, 0.768–0.834) for PLR, 0.806 (95% CI, 0.774–0.838) for MLR, 0.801 (95% CI, 0.768–0.834) for SII, 0.801 (95% CI, 0.768–0.834) for SIRI, and 0.801 (95% CI, 0.768–0.834) for HALP score. Moreover, when all these variables were included simultaneously, only PINI score remained significant, underscoring its strength as an independent predictor of OS in patients with GC.
The final full model included the following significant predictors: age, BMI, mFI-5, TNM stage, TOG, anemia, and PINI score. The variance inflation factor for the included variables were: 1.06 for age, 1.17 for BMI, 1.20 for mFI5, 1.16 for TNM stage, 1.03 for TOG, 1.29 for anemia, and 1.28 for PINI, indicating negligible multicollinearity among the variables. All the significant variables adhered to the proportional hazards assumption (Table 2).
Fractional polynomial analysis demonstrated a linear association between log relative hazard and the PINI score in predicting OS (Figure 1).
3.3. Comparison of Different OS Predictive Models
The full model, which included all significant variables identified in the Cox regression analysis (age, BMI, mFI-5, TNM stage, TOG, anemia, and PINI score), exhibited enhanced predictive accuracy compared with both the baseline (based solely on TNM stage) and intermediate (incorporated all variables from the full model except for the PINI score) models. Compared with the baseline model, the full model demonstrated a significantly higher C-index for OS (0.815 vs. 0.659, p < 0.001). Similarly, the full model achieved substantially higher iAUC values for OS (0.791 vs. 0.640, p < 0.001), indicating an improved predictive performance over time. In addition, the full model achieved substantially higher AUC values for 3- and 5-year OS (all p < 0.001), indicating an enhanced discrimination. IDI and cNRI analyses also confirmed significant improvements for postoperatively predictive accuracy and risk stratification with the full model at both 3 and 5 years (all p < 0.001). Compared with the intermediate model, the full model achieved a notably higher C-index (0.815 vs. 0.797, p = 0.004), highlighting the added prognostic value of including PINI for survival prediction. Similarly, the full model achieved substantially higher iAUC values for OS (0.791 vs. 0.776, p = 0.004), indicating improved predictive performance over time. For the 3-year OS, the full model demonstrated higher AUC, IDI, and cNRI values; however, these differences were not statistically significant. Regarding the 5-year OS, the full model exhibited statistically significant improvements in AUC (p = 0.012), IDI (p = 0.032), and cNRI (p = 0.012), indicating the added long-term prognostic value of the PINI score. Collectively, these findings underscore the enhanced predictive capacity of the full model, particularly during long-term follow up (Table 3).
The predictive advantage of the full model was consistently maintained over the 10-year follow-up period, as illustrated by the time-dependent concordance index plot (Figure 2), which represents the discriminatory ability of each model to predict OS at different time points. The full model consistently achieved the highest C-index across the entire follow-up period, maintaining stable and superior predictive accuracy (approximately 0.80–0.82). Excluding PINI (intermediate model) led to a slightly lower, but still robust discrimination performance. In contrast, the baseline model, which included only the TNM stage, showed substantially lower C-index values (approximately 0.65–0.70), indicating limited predictive capability. Notably, although all three models performed significantly better than chance, the sustained advantage of the full model highlights the additive value of including comprehensive clinical, functional, and nutritional parameters, particularly the PINI score. These results confirm that the full model offers a more accurate and consistent survival prediction across long-term follow up, supporting its clinical utility in postoperative risk stratification (Figure 2).
3.4. Establishment and Validation of the Constructed Nomogram
A prognostic nomogram for OS in patients with GC was developed using the full model. Overall, older age, lower BMI, higher mFI-5 score, advanced stage (stage III), total gastrectomy, presence of anemia, and lower PINI scores contributed to a higher total score, reflecting a worse prognosis (Figure 3).
Calibration plots were generated for 3-year and 5-year OS probabilities, showing excellent concordance between the predicted and observed survival outcomes, with a particularly strong alignment in patients with higher predicted survival probabilities (Figure 4).
3.5. Evaluation of Predictors for PINI Score
Spearman’s correlation analysis was performed across multiple clinical and laboratory parameters. The PINI score demonstrated a strong positive correlation with albumin (r = 0.94) and PNI (r = 0.71), indicating a substantial overlap in the nutritional and inflammatory information captured by these indices. In contrast, the PINI score exhibited only weak correlations (∣r∣ < 0.5) with the remaining variables, suggesting that it provides distinct prognostic information relative to other common clinical markers (Figure 5).
To explore the determinants of PINI score, Lasso regression analysis was conducted using a comprehensive set of clinical, pathological, and laboratory variables. Candidate predictors included categorical variables such as age group (≤50 vs. >50 years), sex, ASA-PS, mFI-5, T stage, N stage, overall TNM stage, histologic type, lymphatic, vascular, and perineural invasion, type of gastrectomy (total vs. partial), receipt of adjuvant therapy (yes vs. no), anemia status (based on sex-specific hemoglobin thresholds), and tumor location. Additionally, continuous variables from routine blood tests and nutritional markers were incorporated to capture a broad range of potential influences on PINI scores.
Using LASSO for variable selection, the final model retained serum albumin (coefficient = 0.8804) and AMC (coefficient = –0.00065) as the only predictors of PINI. The model demonstrated excellent performance, with an R² value of 0.9992 and a root mean square error of 0.0112 on the test set, indicating an exceptionally strong fit. These findings suggest that albumin and AMC are the primary determinants of PINI expression.
To further refine the model, a generalized additive models with gamma distribution was fitted (intercept at 1.196; p < 0.001), confirming the significance of both albumin and AMC. The smooth terms for s(albumin) and s(AMC) had 8.744 and 6.083 estimated degrees of freedom, respectively, within the predefined basis dimensions (k = 9), supporting adequate model flexibility. Both predictors remained highly significant (p < 0.001) and the model showed excellent calibration, with an adjusted R² of 0.999 and 99.8% deviance. Residual diagnostics confirmed the appropriateness of the gamma distribution, with no evidence of model misspecification. In summary, the PINI score demonstrated a strong correlation with its constituent components—serum albumin and AMC—while showing no substantial associations with demographic factors, tumor pathology, or other clinical parameters, highlighting its specificity as a composite inflammatory and nutritional biomarker.
3.6. Comparison of the Prognostic Discriminatory Ability of the PINI Score vs. Albumin and AMC
Based on the iAUC analysis, the PINI score demonstrated a slightly better discriminatory ability than the albumin levels (iAUC: 0.699 vs. 0.691), although the difference was not statistically significant (p = 0.142). In contrast, PINI showed significantly superior performance compared with AMC (iAUC: 0.699 vs. 0.564, p < 0.001). These results suggest that, while PINI and albumin perform similarly, PINI offers a clear advantage over AMC in predicting patient outcomes. Pointwise time-dependent differences in the AUC between the PINI and albumin over a 120-month follow-up period further showed a slight, yet sustained, improvement in the discriminatory ability of PINI (orange line). In contrast, the AUC difference between PINI and AMC (purple line) was substantially higher, particularly within the first 60 months and remained favorable thereafter (Figure 6).
To further evaluate the predictive performance of PINI, we developed the albumin model by substituting the PINI score with serum albumin while retaining other covariates. Of note, BMI was excluded from this model because of its lack of statistical significance in the multivariate analysis. Thus, the significant variables in the albumin model were age (HR, 0.32; p = 0.004), mFI-5 (HR, 1.26; p = 0.005), TNM stage (HR, 2.96; p < 0.001), TOG (HR, 1.60; p = 0.010), anemia (HR, 1.79; p = 0.002), and albumin level (HR, 0.38; p < 0.001). No significant multicollinearity was observed between the variables.
When comparing model discrimination, the full model demonstrated a slightly higher C-index than the albumin model (0.815 vs. 0.810, p = 0.280), suggesting a modest improvement in predictive accuracy. A similar result was observed when comparing model discrimination, with the full model demonstrating a slightly higher iAUC than the albumin model (0.791 vs. 0.787; p = 0.180) (Table 4).
3.7. Evaluation of Possible Interaction Between Albumin and AMC
To evaluate the potential interaction between serum albumin levels and AMC in predicting OS in patients with GC, we constructed two Cox proportional hazards models. The base model included albumin level and AMC as independent variables, whereas the extended model included an interaction term (albumin × AMC). We compared these nested models using the likelihood ratio test, which yielded a non-significant result (p = 0.990), indicating that the interaction term did not enhance the explanatory power of the model. Consequently, a simpler model (without the interaction term) was deemed sufficient to describe the relationship among albumin level, AMC, and OS in this GC cohort. The performance metrics consistently showed that the base model had a slightly better C-index (0.4665 vs. 0.4629) and a lower AIC (1577.4 vs. 1579.4) than the interaction model. Overall, the interaction between the two variables was statistically negligible.
The predicted HRs from a Cox proportional hazards model that included an interaction term between albumin levels and AMC (fixed at the 25th, 50th, and 75th percentiles further revealed that higher albumin levels were associated with significantly lower HRs regardless of the AMC value. The slope was the steepest at lower albumin concentrations, indicating a disproportionately high risk in patients with hypoalbuminemia. Moreover, no meaningful divergence in the albumin–hazard relationship was observed across the different AMC strata, as denoted by the nearly superimposed curves. This supports the earlier interaction test result (p = 0.990), reinforcing that any statistical interaction between albumin levels and AMC was negligible or nonexistent (Figure 7).
4. Discussion
In our study, the PINI score emerged as an important prognostic factor for OS in patients with GC who underwent curative-intent gastric resection. The PINI stands out as a robust tool for prognostic assessment owing to its simplicity and reliance on two fundamental components, serum albumin level and peripheral AMC count, both of which are readily available without additional expenses. Moreover, our comprehensive full model, which integrates the PINI score with other significant variables, demonstrated superior predictive accuracy compared with conventional models, such as those based solely on the TNM stage. Since the PINI score encompasses the critical aspects of immune function and nutritional status, it offers a holistic approach to prognostic evaluation with more nuanced risk stratification for patients with GC.
In the present study, PINI was found to be significantly correlated with albumin and AMC, but not with other variables (including demographic and pathological variables), suggesting the independence of these variables. Serum albumin, a core component of the PINI score, reflects both nutritional reserves and the systemic inflammatory state, and plays a pivotal role in GC prognosis [3,4]. Numerous prognostic indices that incorporate albumin were associated with poor survival in patients with GC, including the PNI [5], geriatric nutritional risk index [5], controlling nutritional status score [6], albumin-bilirubin score [7], albumin-to-globulin ratio [8], albumin-to-fibrinogen ratio [9], CRP-to-albumin ratio [10], carcinoembryonic antigen-to-albumin ratio [11], neutrophil-to-albumin ratio [12], platelet-to-albumin ratio [13], the CALLY index [14], and the HALP score [15]. These composite biomarkers further underscore the multifaceted prognostic value of albumin levels in patients with GC. Factors such as tumor necrosis factor-α and interleukin-6 can suppress albumin production, resulting in lower levels [38]. This reduction was associated with a higher risk of postoperative complications and poorer survival outcomes in patients with GC [3,4,39,40,41]. Monocyte-based markers have garnered significant attention owing to their crucial roles in cancer progression. The inclusion of AMC in PINI underscores its role in fostering a microenvironment conducive to tumor progression [16,17,18].
In addition to PINI, multivariate analysis herein identified age, BMI, mFI-5, TNM stage, TOG, and anemia as significant independent determinants of OS. Our findings show that patients with late-onset GC (> 50 years) had significantly poorer survival outcomes than those with early onset GC. This observation is consistent with a previous study by He et al., who reported higher mortality in late-onset GC, potentially due to age-related factors such as increased comorbidity burden and cumulative exposure to carcinogens [33]. Regarding the prognostic effect of BMI on GC, Wada et al. demonstrated that patients with low BMI exhibited worse OS outcomes than those in the normal- or high-BMI groups [42]. The TNM staging system remains the gold standard for the prognostic assessment of cancer patients and its prognostic value has been well established for GC survival outcomes [1,43,44,45,46]. In the present study, TNM stage was found to be a significant predictor of OS, even after adjusting for other variables, reinforcing its critical role in GC prognosis [47]. Patients who undergo total gastrectomy have historically experienced higher 30-day morbidity and readmission rates because of nutritional complications [48,49]. Additionally, total gastrectomy has been shown to affect OS in patients with GC [46], which was confirmed in our study, where total gastrectomy remained a significant predictor of OS. Furthermore, preoperative anemia is recognized as an important prognostic factor of OS in patients with GC. A meta-analysis of 17 studies involving 13,154 patients with GC found that 36% of patients had preoperative anemia, who experienced worse OS (HR = 1.33) compared with those without anemia [50].
We included NLR, PLR, MLR, SII, SIRI, HALP, and PNI when constituting the comprehensive full predictive model, but excluded these variables from the final model because of their lack of statistical significance in the multivariate analysis. The variability in findings across studies may be attributed to differences in methodological approaches, such as the use of categorical vs. continuous variable analyses, which can affect the detection of prognostic associations. Additionally, the heterogeneity in patient cohorts, including demographic and clinical characteristics, may influence the prognostic value of these markers. Therefore, although we did not identify these markers as independent prognostic factors within our specific cohort or analytical framework, their potential utility in other contexts remains valid and warrants further investigation.
The full model, which included age, BMI, mFI-5, TNM stage, TOG, anemia, and PINI score, outperformed both the baseline and intermediate models in predicting OS. Specifically, when compared with the baseline model (relying solely on TNM stage), the full model yielded a significantly higher concordance index (p < 0.001) and improved iAUC (p < 0.001), reflecting enhanced discriminatory ability across the follow-up period. In addition, the full model showed higher AUCs for 3- and 5-year OS (p < 0.001 for both). The IDI and cNRI analyses also confirmed improved risk discrimination and reclassification at both time points (p < 0.001), and the calibration curves showed good agreement between the predicted and observed outcomes. Moreover, the full model achieved higher C-index (p = 0.004) and iAUC (p = 0.004) as compared with the intermediate model. While differences in the 3-year AUC, IDI, and cNRI were not statistically significant, the full model showed significant improvements in all three metrics for 5-year OS (p = 0.012, 0.032, and 0.012, respectively), highlighting the added prognostic value of PINI over the long-term follow-up. Taken together, these results confirm that the full model offers enhanced discrimination, calibration, and clinical utility in predicting long-term survival.
The predictive advantage of the full model was consistently maintained throughout the 10-year follow-up period, as shown in the time-dependent C-index plot. The full model demonstrated the highest concordance index across all time points, indicating stable and superior discriminatory ability for OS. The intermediate model, which excluded the PINI score, showed a slightly lower but still acceptable performance, whereas the baseline model, based solely on the TNM stage, had notably lower C-indices, reflecting limited predictive power. All models performed above the chance level; however, the sustained advantage of the full model underscores the value of integrating clinical, functional, and nutritional factors, particularly PINI, for accurate long-term survival prediction and postoperative risk stratification.
In this study, we evaluated whether there was a statistically and clinically meaningful interaction between the components of the PINI (serum albumin and AMC) in predicting OS among patients with GC. The base model included albumin level and AMC as independent variables, whereas the extended model included an interaction term (albumin × AMC). Model performance metrics, including the C-index and AIC, consistently indicated that the base model either outperformed or matched the extended model, suggesting that the interaction between albumin and AMC was negligible. Moreover, the prognostic impact of serum albumin levels remained stable across varying AMC levels, reinforcing its independent predictive value.
Although albumin was confirmed as a strong and independent prognostic factor, the PINI score demonstrated a slightly higher iAUC than albumin alone, although these differences were not statistically significant. Moreover, over the entire 10-year follow-up period, the PINI score consistently showed superior discriminative performance in terms of AUC relative to albumin levels, suggesting a potential incremental benefit in long-term prognostic assessment. Comparison of the models also revealed that the full model incorporating PINI achieved marginally higher C-index and iAUC values than the albumin model, further suggesting a modest enhancement in predictive accuracy. These findings imply that, while albumin captures a substantial portion of the prognostic signal, PINI may offer incremental value by incorporating inflammatory information via AMC. By encompassing a broader spectrum of nutritional and inflammatory statuses, the PINI provides a new platform for personalized treatment for patients with GC.
This study had several strengths. To the best of our knowledge, this is the first study to evaluate the prognostic significance of PINI in patients with GC undergoing curative-intent resection. The PINI score, derived from readily available and cost-effective parameters, such as serum albumin and AMC, serves as a simple yet powerful tool for risk stratification. By incorporating the PINI as a continuous variable, we preserved data granularity, enhanced statistical power, and improved model generalizability. This approach facilitated the identification of a linear relationship between PINI and mortality risk through fractional polynomial modeling, which may have been obscured by categorization. Importantly, we conducted a thorough evaluation of the potential interaction between serum albumin and AMC for predicting OS, which revealed no statistically significant interaction effect and that the prognostic impact of serum albumin was consistent across varying AMC levels. The comprehensive model integrating PINI with clinical and functional parameters demonstrated superior predictive performance across multiple statistical metrics, including the C-index, iAUC, AUC, IDI, and cNRI, particularly for long-term survival prediction. These findings were further corroborated by a time-dependent C-index analysis. Building upon these results, we developed a nomogram incorporating PINI along with other significant clinical variables to predict the 3- and 5-year OS probabilities for GC patients after curative resection. The nomogram exhibited accurate calibration and reasonable discrimination, offering a practical tool for individualized prognostic assessment and aiding clinicians in tailoring postoperative management strategies.
Despite its strengths, this study had several limitations. First, its retrospective design introduces the potential for selection bias and residual confounding, as not all clinical or biological variables can be fully accounted for. Second, the study was conducted at a single clinical center in East Asia, with a predominantly Asian population (96.1%). Although this enhances the internal validity, it limits the generalizability of the findings to more diverse or multiethnic populations. Ethnic differences in genetic background, environmental exposure, and nutritional status may influence the prognostic value of PINI. Third, although the sample size was adequate for model development, external validation in larger multicenter cohorts is essential to confirm reproducibility and clinical utility. Finally, as with all observational studies, causal relationships cannot be established and unmeasured confounders may have affected the results. Future prospective studies involving diverse populations are needed to validate and refine the role of PINI in personalized prognostication of GC.
5. Conclusions
In conclusion, our study demonstrated that PINI is a valuable and accessible tool for predicting OS in patients with GC undergoing curative intent resection. By integrating serum albumin levels and AMC, PINI reflects both the nutritional and inflammatory statuses of patients, which are critical determinants of cancer prognosis. Albumin serves as a marker of nutritional reserves and systemic inflammation, whereas monocytes may promote tumor progression through immunosuppressive and proangiogenic pathways. Collectively, these components provide a biologically plausible basis for the prognostic relevance of this index.
The simplicity, low cost, and routine availability of the variables used to calculate the PINI make it an attractive candidate for widespread clinical use, particularly in resource-limited settings. This may aid clinicians in stratifying risks, tailoring perioperative care, and identifying patients who can benefit from closer surveillance or additional supportive interventions. Future research should elucidate the biological mechanisms underlying the prognostic value of PINI and evaluate its role in guiding individualized treatment strategies.
Author Contributions
Conceptualization, Soomin An (S. An), Wankyu Eo (W. Eo), and Sookyung Lee (S. Lee); methodology, S. An, W. Eo, and S. Lee; resources, S. An, W. Eo, and S. Lee; formal analysis, S. An, W. Eo, and S. Lee; investigation, S. An, W. Eo, and S. Lee; resources, S. An, W. Eo, and S. Lee; data curation, S. An, W. Eo, and S. Lee; writing—original draft preparation, S. An, W. Eo, and S. Lee; writing— original draft preparation, S. An, W. Eo, and S. All the authors have read and agreed to the published version of this manuscript.
Funding
This study was funded by a grant from Dongyang University in 2024.
Institutional Review Board Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki. This study was approved by the Institutional Review Board of Kyung Hee University Hospital (2024-05-005).
Informed Consent Statement
Informed patient consent was waived owing the retrospective nature of the study.
Data Availability Statement
The data sets presented in this study are available upon request from the corresponding author due to ethical reasons.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the study design, collection, analyses, interpretation of data, writing of the manuscript, or decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| AIC | Akaike Information Criterion |
| ALC | Absolute lymphocyte count |
| AMC | Absolute monocyte count |
| ANC | Absolute neutrophil count |
| ASA-PS | American Society of Anesthesiologists physical status |
| AUC | Area under the curve |
| BMI | Body mass index |
| CALLY | CRP-albumin-lymphocyte index |
| C-index | Concordance index |
| CI | Confidence interval |
| cNRI | Continuous net reclassification improvement |
| CRP | C-reactive protein |
| GC | Gastric cancer |
| HALP | Hemoglobin, albumin, lymphocyte, and platelet |
| HR | Hazard ratio |
| iAUC | Integrated AUC |
| IDI | Integrated discrimination improvement |
| IQR | Interquartile range |
| Lasso | Least absolute shrinkage and selection operator |
| LOS | Length of stay |
| MCV | Mean corpuscular volume |
| mFI-5 | Five-factor modified frail index |
| NLR | Neutrophil-to-lymphocyte ratio |
| OS | Overall survival |
| PINI | Prognostic immune nutritional index |
| PLR | Platelet-to-lymphocyte ratio |
| PNI | Prognostic nutritional index |
| SII | Systemic immune-inflammation index |
| SIRI | Systemic inflammation response index |
| TAM | Tumor-associated macrophage |
| TNM | Tumor–node–metastasis |
| TOG | Type of gastrectomy |
References
- Balachandran, V.P.; Gonen, M.; Smith, J.J.; DeMatteo, R.P. Nomograms in oncology: more than meets the eye. The Lancet. Oncology 2015, 16, e173–e180. [Google Scholar] [CrossRef] [PubMed]
- Oñate-Ocaña, L.F.; Aiello-Crocifoglio, V.; Gallardo-Rincón, D.; Herrera-Goepfert, R.; Brom-Valladares, R.; Carrillo, J.F.; Cervera, E.; Mohar-Betancourt, A. Serum albumin as a significant prognostic factor for patients with gastric carcinoma. Annals of surgical oncology 2007, 14, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Crumley, A.B.; Stuart, R.C.; McKernan, M.; McMillan, D.C. Is hypoalbuminemia an independent prognostic factor in patients with gastric cancer? World journal of surgery 2010, 34, 2393–2398. [Google Scholar] [CrossRef] [PubMed]
- Akula, B.; Doctor, N. A Prospective Review of Preoperative Nutritional Status and Its Influence on the Outcome of Abdominal Surgery. Cureus 2021, 13, e19948. [Google Scholar] [CrossRef]
- An, S.; Eo, W.; Lee, S. Comparison of the Clinical Value of the Geriatric Nutritional Risk Index and Prognostic Nutritional Index as Determinants of Survival Outcome in Patients with Gastric Cancer. Journal of Cancer 2022, 13, 3348–3357. [Google Scholar] [CrossRef]
- Esashi, R.; Aoyama, T.; Yamamoto, S.; Maezawa, Y.; Hashimoto, I.; Kazama, K.; Morita, J.; Kawahara, S.; Otani, K.; Komori, K.; et al. The CONUT Score Can Predict the Prognosis of Gastric Cancer Patients After Curative Treatment. Anticancer research 2025, 45, 1251–1260. [Google Scholar] [CrossRef]
- Ju, M.; Aoyama, T.; Komori, K.; Tamagawa, H.; Tamagawa, A.; Maezawa, Y.; Morita, J.; Onodera, A.; Endo, K.; Hashimoto, I.; et al. The Albumin-Bilirubin Score Is a Prognostic Factor for Gastric Cancer Patients Who Receive Curative Treatment. Anticancer research 2022, 42, 3929–3935. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhu, J.Y.; Zhou, L.N.; Tang, M.; Chen, M.B.; Tao, M. Predicting the Prognosis of Gastric Cancer by Albumin/Globulin Ratio and the Prognostic Nutritional Index. Nutrition and cancer 2020, 72, 635–644. [Google Scholar] [CrossRef]
- Zhao, G. Albumin/fibrinogen ratio, a predictor of chemotherapy resistance and prognostic factor for advanced gastric cancer patients following radical gastrectomy. BMC Surg 2022, 22, 207. [Google Scholar] [CrossRef]
- Li, C.; Yang, X.; Li, H.; Fu, Y.; Wang, W.; Jin, X.; Bian, L.; Peng, L. Postoperative ratio of C-reactive protein to albumin is an independent prognostic factor for gastric cancer. Eur J Med Res 2023, 28, 360. [Google Scholar] [CrossRef]
- Culcu, S.; Yuksel, C.; Aydin, F.; Bakirarar, B.; Aksel, B.; Dogan, L. The effect of CEA/Albumin ratio in gastric cancer patient on prognostic factors. Ann Ital Chir 2022, 93, 447–452. [Google Scholar]
- Hashimoto, I.; Kano, K.; Onuma, S.; Suematsu, H.; Nagasawa, S.; Kanematsu, K.; Furusawa, K.; Hamaguchi, T.; Watanabe, M.; Hayashi, K.; et al. Clinical Significance of Neutrophil-to-Lymphocyte Ratio/Serum Albumin Ratio in Patients With Metastatic Gastric or Gastroesophageal Junction Cancer Administered Trifluridine/Tipiracil. Anticancer research 2023, 43, 1689–1697. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Xia, Y.Q.; Xiao, L.; Huang, J.; Zhu, Z.M. Combining the platelet-to-albumin ratio with serum and pathologic variables to establish a risk assessment model for lymph node metastasis of gastric cancer. J Biol Regul Homeost Agents 2021, 35, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhang, S.; Hu, X.; Huang, T.; Chen, M. Correlation between the C-reactive protein (CRP)-albumin-lymphocyte (CALLY) index and the prognosis of gastric cancer patients after gastrectomy: a systematic review and meta-analysis. Surgery today 2025, 55, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Sargin, Z.G.; Dusunceli, I. The Effect of HALP Score on the Prognosis of Gastric Adenocarcinoma. J Coll Physicians Surg Pak 2022, 32, 1154–1159. [Google Scholar] [CrossRef]
- Kiss, M.; Caro, A.A.; Raes, G.; Laoui, D. Systemic Reprogramming of Monocytes in Cancer. Front Oncol 2020, 10, 1399. [Google Scholar] [CrossRef]
- Huang, B.; Lei, Z.; Zhao, J.; Gong, W.; Liu, J.; Chen, Z.; Liu, Y.; Li, D.; Yuan, Y.; Zhang, G.M.; et al. CCL2/CCR2 pathway mediates recruitment of myeloid suppressor cells to cancers. Cancer Lett 2007, 252, 86–92. [Google Scholar] [CrossRef]
- Cassetta, L.; Pollard, J.W. Targeting macrophages: therapeutic approaches in cancer. Nat Rev Drug Discov 2018, 17, 887–904. [Google Scholar] [CrossRef]
- Schiefer, S.; Wirsik, N.M.; Kalkum, E.; Seide, S.E.; Nienhüser, H.; Müller, B.; Billeter, A.; Büchler, M.W.; Schmidt, T.; Probst, P. Systematic Review of Prognostic Role of Blood Cell Ratios in Patients with Gastric Cancer Undergoing Surgery. Diagnostics 2022, 12, 593. [Google Scholar] [CrossRef]
- An, S.; Eo, W.; Lee, S.; Lee, Y.J. Monocyte-to-lymphocyte ratio as a determinant of survival in patients with gastric cancer undergoing gastrectomy: A cohort study. Medicine 2023, 102, e33930. [Google Scholar] [CrossRef]
- Eo, W.K.; Jeong, D.W.; Chang, H.J.; Won, K.Y.; Choi, S.I.; Kim, S.H.; Chun, S.W.; Oh, Y.L.; Lee, T.H.; Kim, Y.O.; et al. Absolute monocyte and lymphocyte count prognostic score for patients with gastric cancer. World journal of gastroenterology 2015, 21, 2668–2676. [Google Scholar] [CrossRef] [PubMed]
- Yazici, H.; Yegen, S.C. Is Systemic Inflammatory Response Index (SIRI) a Reliable Tool for Prognosis of Gastric Cancer Patients Without Neoadjuvant Therapy? Cureus 2023, 15, e36597. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.H.; Hao, J.; Shivakumar, M.; Nam, Y.; Kim, J.; Kim, M.J.; Ryoo, S.B.; Choe, E.K.; Jeong, S.Y.; Park, K.J.; et al. Development and validation of a novel strong prognostic index for colon cancer through a robust combination of laboratory features for systemic inflammation: a prognostic immune nutritional index. British journal of cancer 2022, 126, 1539–1547. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.; Wei, L.; Liu, M.; Liang, Y.; Yuan, G.; Gao, S.; Wang, Q.; Lin, X.; Tang, S.; Gan, J. Prognostic significance of preoperative prognostic immune and nutritional index in patients with stage I-III colorectal cancer. BMC cancer 2022, 22, 1316. [Google Scholar] [CrossRef]
- Shibutani, M.; Kashiwagi, S.; Fukuoka, T.; Iseki, Y.; Kasashima, H.; Maeda, K. Significance of the Prognostic Immune and Nutritional Index in Patients With Stage I-III Colorectal Cancer. Cancer Diagn Progn 2023, 3, 354–359. [Google Scholar] [CrossRef]
- Lauren, P. THE TWO HISTOLOGICAL MAIN TYPES OF GASTRIC CARCINOMA: DIFFUSE AND SO-CALLED INTESTINAL-TYPE CARCINOMA. AN ATTEMPT AT A HISTO-CLINICAL CLASSIFICATION. Acta pathologica et microbiologica Scandinavica 1965, 64, 31–49. [Google Scholar] [CrossRef]
- Mranda, G.M.; Xue, Y.; Zhou, X.G.; Yu, W.; Wei, T.; Xiang, Z.P.; Liu, J.J.; Ding, Y.L. Revisiting the 8th AJCC system for gastric cancer: A review on validations, nomograms, lymph nodes impact, and proposed modifications. Ann Med Surg (Lond) 2022, 75, 103411. [Google Scholar] [CrossRef]
- Foley, C.; Kendall, M.C.; Apruzzese, P.; De Oliveira, G.S. American Society of Anesthesiologists Physical Status Classification as a reliable predictor of postoperative medical complications and mortality following ambulatory surgery: an analysis of 2,089,830 ACS-NSQIP outpatient cases. BMC Surg 2021, 21, 253. [Google Scholar] [CrossRef]
- Tracy, B.M.; Adams, M.A.; Schenker, M.L.; Gelbard, R.B. The 5 and 11 Factor Modified Frailty Indices are Equally Effective at Outcome Prediction Using TQIP. J Surg Res 2020, 255, 456–462. [Google Scholar] [CrossRef]
- Subramaniam, S.; Aalberg, J.J.; Soriano, R.P.; Divino, C.M. New 5-Factor Modified Frailty Index Using American College of Surgeons NSQIP Data. Journal of the American College of Surgeons 2018, 226, 173–181.e178. [Google Scholar] [CrossRef]
- Cao, W.; Yao, X.; Cen, D.; Zhi, Y.; Zhu, N.; Xu, L. The prognostic role of platelet-to-lymphocyte ratio on overall survival in gastric cancer: a systematic review and meta-analysis. BMC Gastroenterol 2020, 20, 16. [Google Scholar] [CrossRef] [PubMed]
- Hirahara, N.; Tajima, Y.; Matsubara, T.; Fujii, Y.; Kaji, S.; Kawabata, Y.; Hyakudomi, R.; Yamamoto, T.; Uchida, Y.; Taniura, T. Systemic Immune-Inflammation Index Predicts Overall Survival in Patients with Gastric Cancer: a Propensity Score-Matched Analysis. Journal of gastrointestinal surgery: official journal of the Society for Surgery of the Alimentary Tract 2021, 25, 1124–1133. [Google Scholar] [CrossRef] [PubMed]
- He, M.J.; Ji, L.D.; Lian, L.; Ma, Z.F.; Luo, Y.T.; Lai, J.L.; Wang, K.J. [Epidemiological trend of early-onset gastric cancer and late-onset gastric cancer in China from 2000 to 2019]. Zhonghua Liu Xing Bing Xue Za Zhi 2023, 44, 1198–1202. [Google Scholar] [CrossRef]
- Cappellini, M.D.; Motta, I. Anemia in Clinical Practice-Definition and Classification: Does Hemoglobin Change With Aging? Seminars in hematology 2015, 52, 261–269. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models: a framework for traditional and novel measures. Epidemiology (Cambridge, Mass.) 2010, 21, 128–138. [Google Scholar] [CrossRef]
- Chipman, J.; Braun, D. Simpson’s paradox in the integrated discrimination improvement. Stat Med 2017, 36, 4468–4481. [Google Scholar] [CrossRef]
- Cook, N.R.; Demler, O.V.; Paynter, N.P. Clinical risk reclassification at 10 years. Stat Med 2017, 36, 4498–4502. [Google Scholar] [CrossRef]
- Rothschild, M.A.; Oratz, M.; Schreiber, S.S. Serum albumin. Hepatology 1988, 8, 385–401. [Google Scholar] [CrossRef]
- Tamai, K.; Okamura, S.; Makino, S.; Yamamura, N.; Fukuchi, N.; Ebisui, C.; Inoue, A.; Yano, M. C-reactive protein/albumin ratio predicts survival after curative surgery in elderly patients with colorectal cancer. Updates Surg 2021. [Google Scholar] [CrossRef]
- Forones, N.M.; Mandowsky, S.V.; Lourenço, L.G. Serum levels of interleukin-2 and tumor necrosis factor-alpha correlate to tumor progression in gastric cancer. Hepato-gastroenterology 2001, 48, 1199–1201. [Google Scholar]
- Ishida, S.; Hashimoto, I.; Seike, T.; Abe, Y.; Nakaya, Y.; Nakanishi, H. Serum albumin levels correlate with inflammation rather than nutrition supply in burns patients: a retrospective study. The journal of medical investigation: JMI 2014, 61, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Wada, T.; Kunisaki, C.; Ono, H.A.; Makino, H.; Akiyama, H.; Endo, I. Implications of BMI for the Prognosis of Gastric Cancer among the Japanese Population. Digestive surgery 2015, 32, 480–486. [Google Scholar] [CrossRef] [PubMed]
- An, S.; Eo, W.; Kim, Y.J. Muscle-Related Parameters as Determinants of Survival in Patients with Stage I-III Gastric Cancer Undergoing Gastrectomy. Journal of Cancer 2021, 12, 5664–5673. [Google Scholar] [CrossRef]
- Furuke, H.; Matsubara, D.; Kubota, T.; Kiuchi, J.; Kubo, H.; Ohashi, T.; Shimizu, H.; Arita, T.; Yamamoto, Y.; Konishi, H.; et al. Geriatric Nutritional Risk Index Predicts Poor Prognosis of Patients After Curative Surgery for Gastric Cancer. Cancer Diagn Progn 2021, 1, 43–52. [Google Scholar] [CrossRef]
- Hirahara, N.; Tajima, Y.; Fujii, Y.; Kaji, S.; Kawabata, Y.; Hyakudomi, R.; Yamamoto, T.; Taniura, T. Prediction of postoperative complications and survival after laparoscopic gastrectomy using preoperative Geriatric Nutritional Risk Index in elderly gastric cancer patients. Surgical endoscopy 2021, 35, 1202–1209. [Google Scholar] [CrossRef]
- Sugawara, K.; Yamashita, H.; Urabe, M.; Okumura, Y.; Yagi, K.; Aikou, S.; Seto, Y. Geriatric Nutrition Index Influences Survival Outcomes in Gastric Carcinoma Patients Undergoing Radical Surgery. JPEN. Journal of parenteral and enteral nutrition 2021, 45, 1042–1051. [Google Scholar] [CrossRef]
- An, S.; Eo, W.; Lee, S. Prognostic significance of a five-factor modified frailty index in patients with gastric cancer undergoing curative-intent resection: A cohort study. Medicine 2023, 102, e36065. [Google Scholar] [CrossRef]
- Osaki, T.; Saito, H.; Miyauchi, W.; Shishido, Y.; Miyatani, K.; Matsunaga, T.; Tatebe, S.; Fujiwara, Y. The type of gastrectomy and modified frailty index as useful predictive indicators for 1-year readmission due to nutritional difficulty in patients who undergo gastrectomy for gastric cancer. BMC Surg 2021, 21, 445. [Google Scholar] [CrossRef]
- Martin, A.N.; Das, D.; Turrentine, F.E.; Bauer, T.W.; Adams, R.B.; Zaydfudim, V.M. Morbidity and Mortality After Gastrectomy: Identification of Modifiable Risk Factors. Journal of gastrointestinal surgery: official journal of the Society for Surgery of the Alimentary Tract 2016, 20, 1554–1564. [Google Scholar] [CrossRef]
- Huang, X.Z.; Yang, Y.C.; Chen, Y.; Wu, C.C.; Lin, R.F.; Wang, Z.N.; Zhang, X. Preoperative Anemia or Low Hemoglobin Predicts Poor Prognosis in Gastric Cancer Patients: A Meta-Analysis. Disease markers 2019, 2019, 7606128. [Google Scholar] [CrossRef]
Figure 1.
Fractional polynomial model of log relative hazard for the prognostic immune nutritional index (PINI) for overall survival (OS) in patients with gastric cancer (GC) with 95% confidence intervals.
Figure 1.
Fractional polynomial model of log relative hazard for the prognostic immune nutritional index (PINI) for overall survival (OS) in patients with gastric cancer (GC) with 95% confidence intervals.
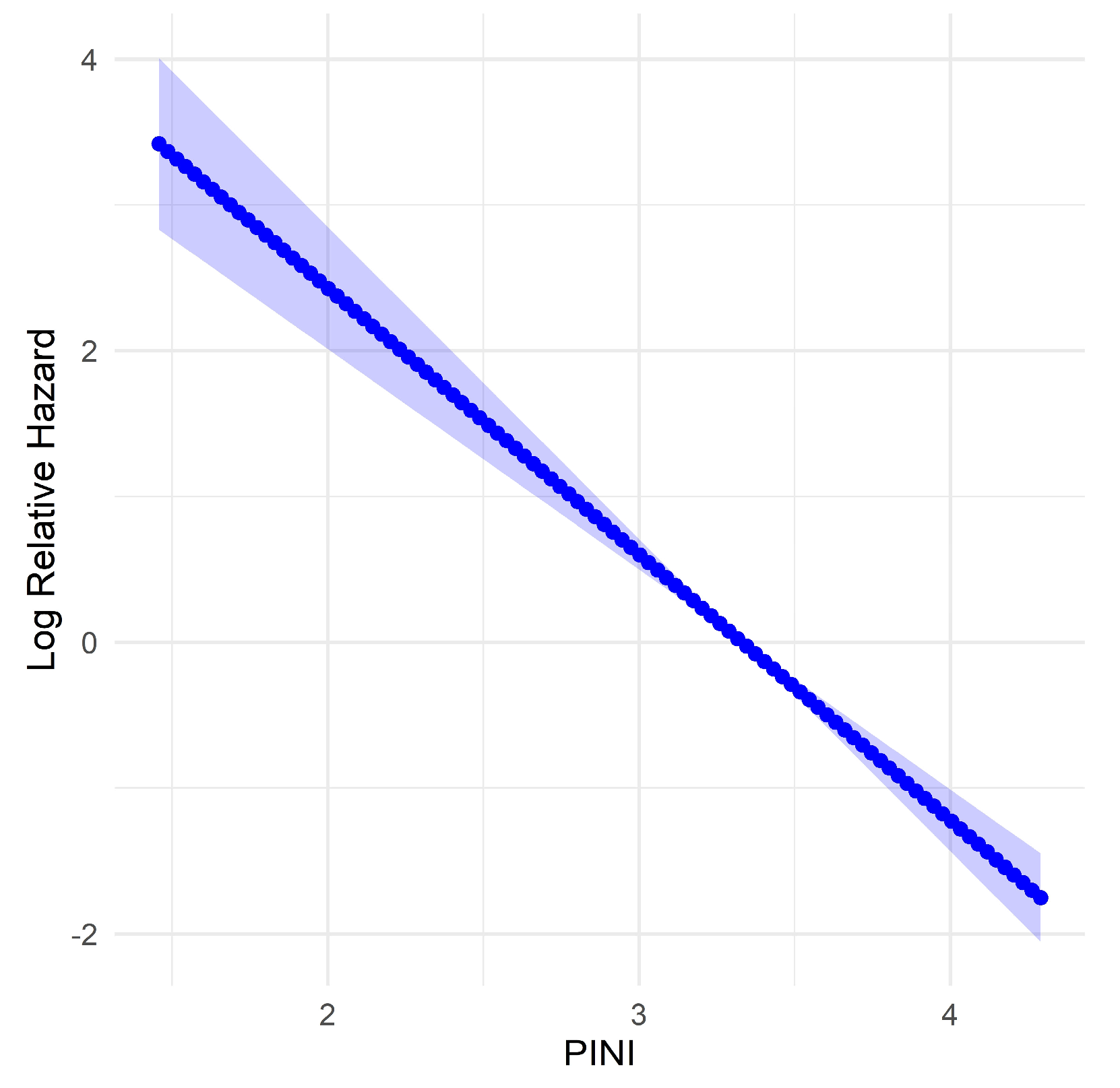
Figure 2.
Concordance indices of the predictive models designed to assess OS outcomes in patients with GC for over a 10-year period. The full model for OS incorporated age, BMI, mFI-5, stage, TOG, anemia, and the PINI. The intermediate model consisted of the same variables as those of the full model, excluding PINI. The baseline model relied solely on cancer stage.
Figure 2.
Concordance indices of the predictive models designed to assess OS outcomes in patients with GC for over a 10-year period. The full model for OS incorporated age, BMI, mFI-5, stage, TOG, anemia, and the PINI. The intermediate model consisted of the same variables as those of the full model, excluding PINI. The baseline model relied solely on cancer stage.
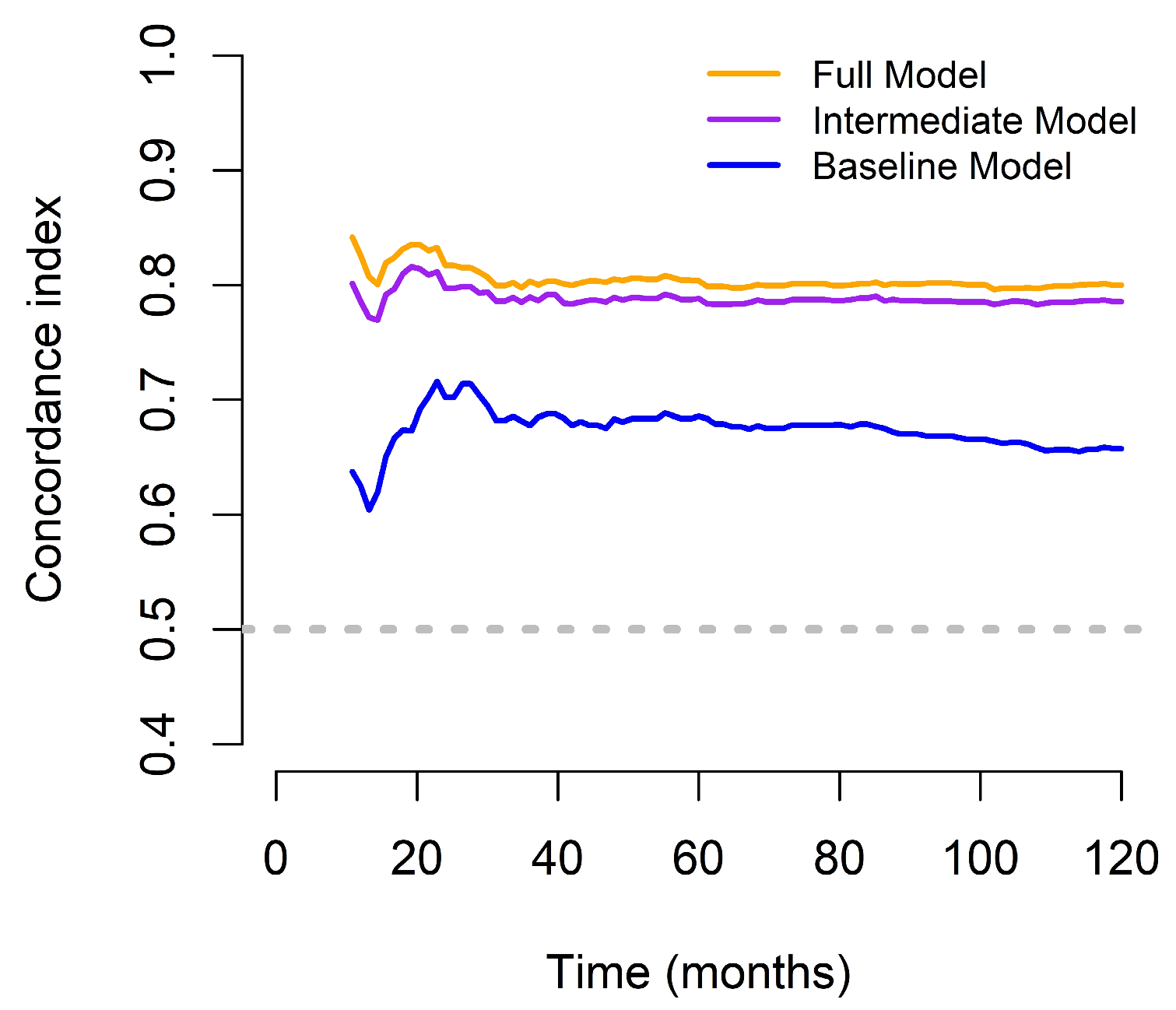
Figure 3.
Nomograms predicting 3-year and 5-year OS based on the full model. The full model for OS incorporates age, BMI, mFI-5, stage, TOG, anemia, and the PINI.
Figure 3.
Nomograms predicting 3-year and 5-year OS based on the full model. The full model for OS incorporates age, BMI, mFI-5, stage, TOG, anemia, and the PINI.
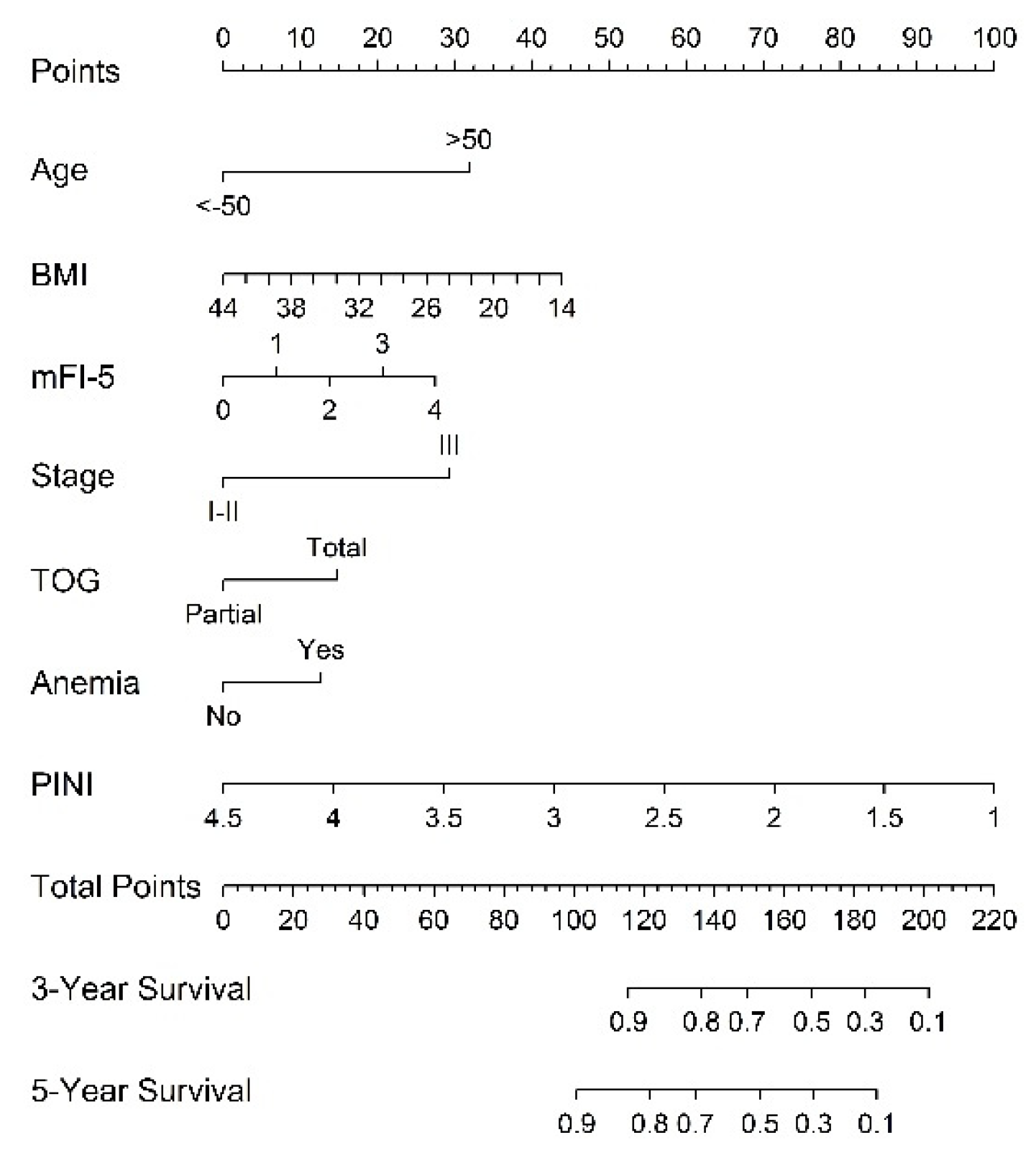
Figure 4.
Calibration curves of the designed nomogram for predicting (A) 3- and (B) 5-year OS. Each point on the plot represents a subgroup of the predicted survival obtained by dividing the data into five groups. Vertical error bars denote the 95% confidence intervals for the observed survival within each subgroup, centered on the predicted survival values along the x-axis. A grouping parameter (m = 100) and bootstrap parameter (B = 1000) were employed, referring to the use of 1,000 bootstrap resamples to enhance the robustness and precision of the calibration estimates.
Figure 4.
Calibration curves of the designed nomogram for predicting (A) 3- and (B) 5-year OS. Each point on the plot represents a subgroup of the predicted survival obtained by dividing the data into five groups. Vertical error bars denote the 95% confidence intervals for the observed survival within each subgroup, centered on the predicted survival values along the x-axis. A grouping parameter (m = 100) and bootstrap parameter (B = 1000) were employed, referring to the use of 1,000 bootstrap resamples to enhance the robustness and precision of the calibration estimates.
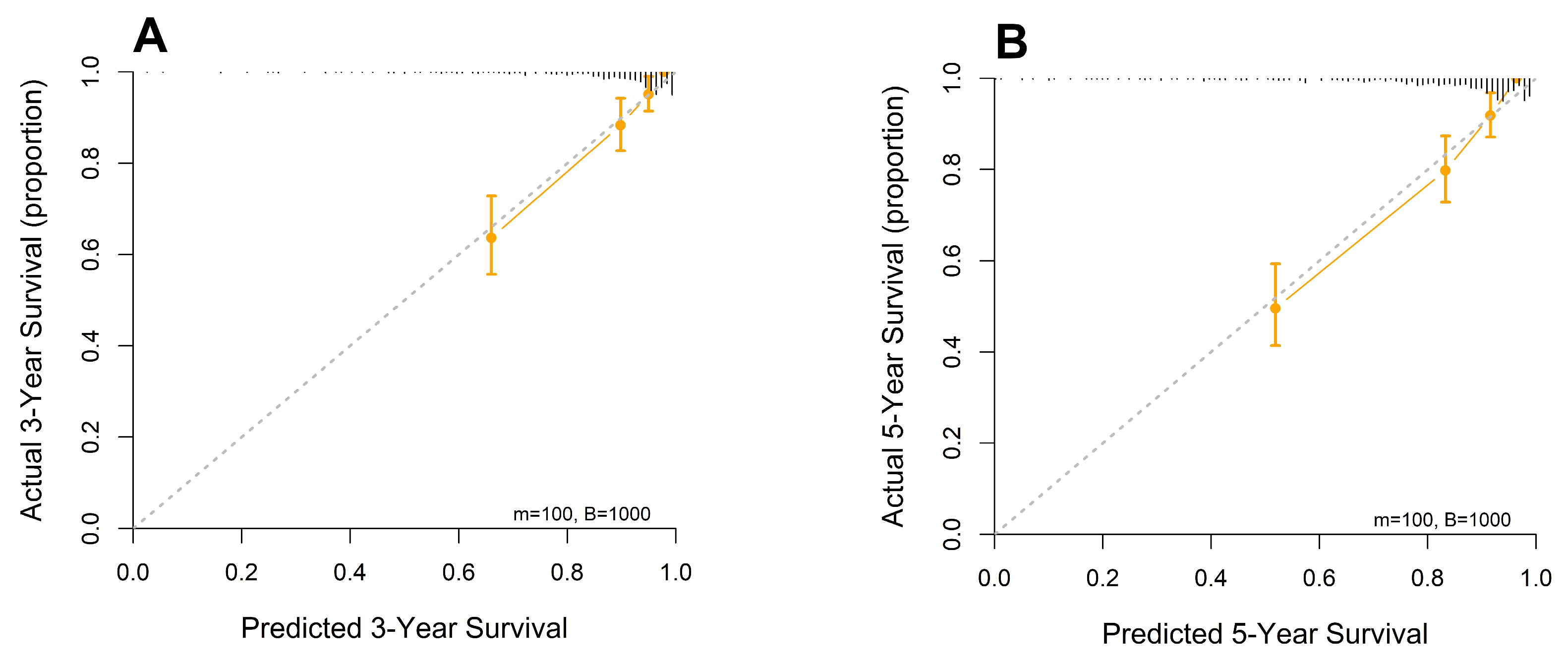
Figure 5.
Chord diagram of correlations among variables. Correlation coefficients of > 0.5 or < −0.5 between variable pairs are represented.
Figure 5.
Chord diagram of correlations among variables. Correlation coefficients of > 0.5 or < −0.5 between variable pairs are represented.
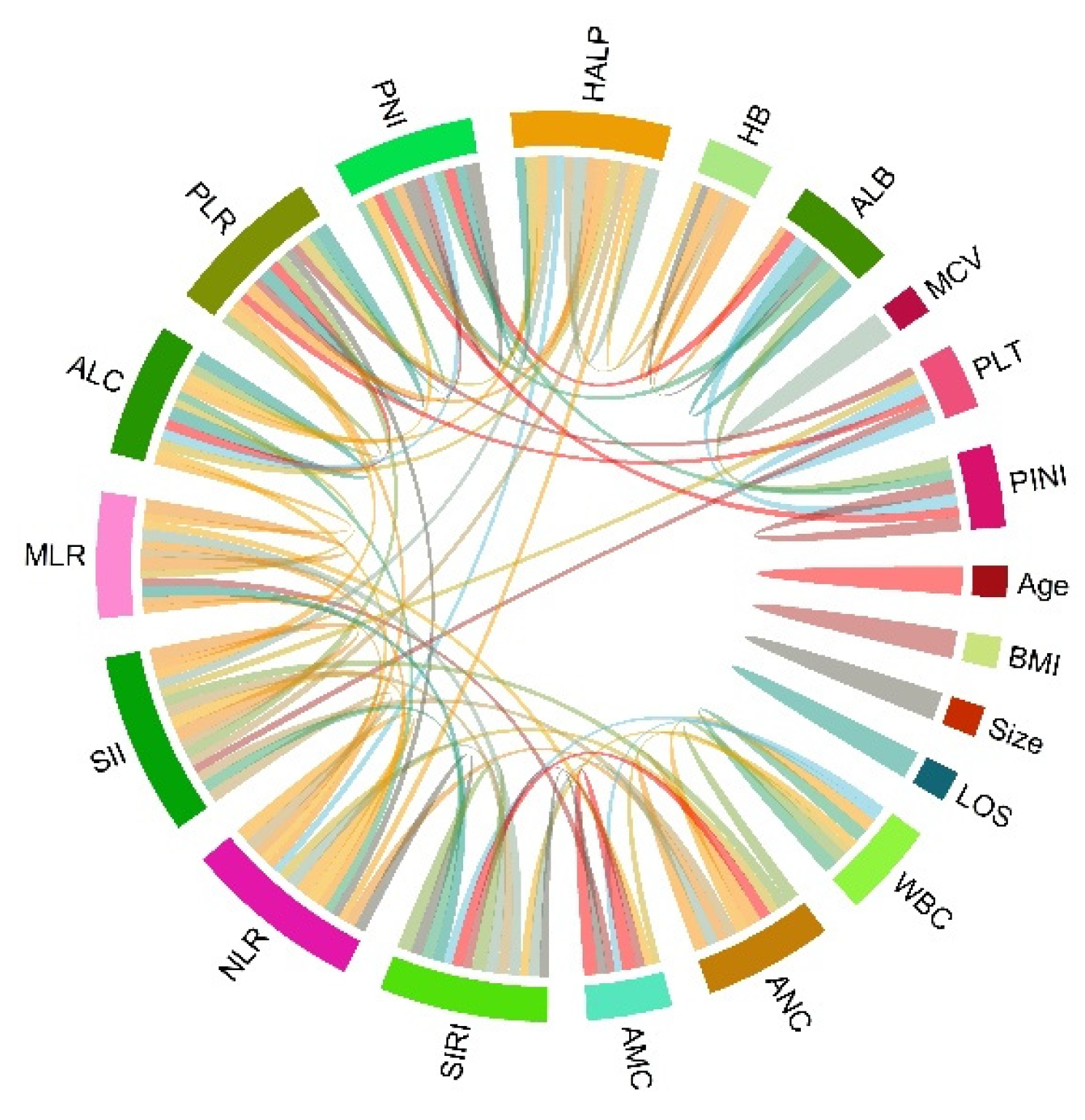
Figure 6.
Time-dependent area under the curve (AUC) differences between PINI vs. albumin plus absolute monocyte count (AMC). The horizontal dashed line at 0 marks the reference.
Figure 6.
Time-dependent area under the curve (AUC) differences between PINI vs. albumin plus absolute monocyte count (AMC). The horizontal dashed line at 0 marks the reference.
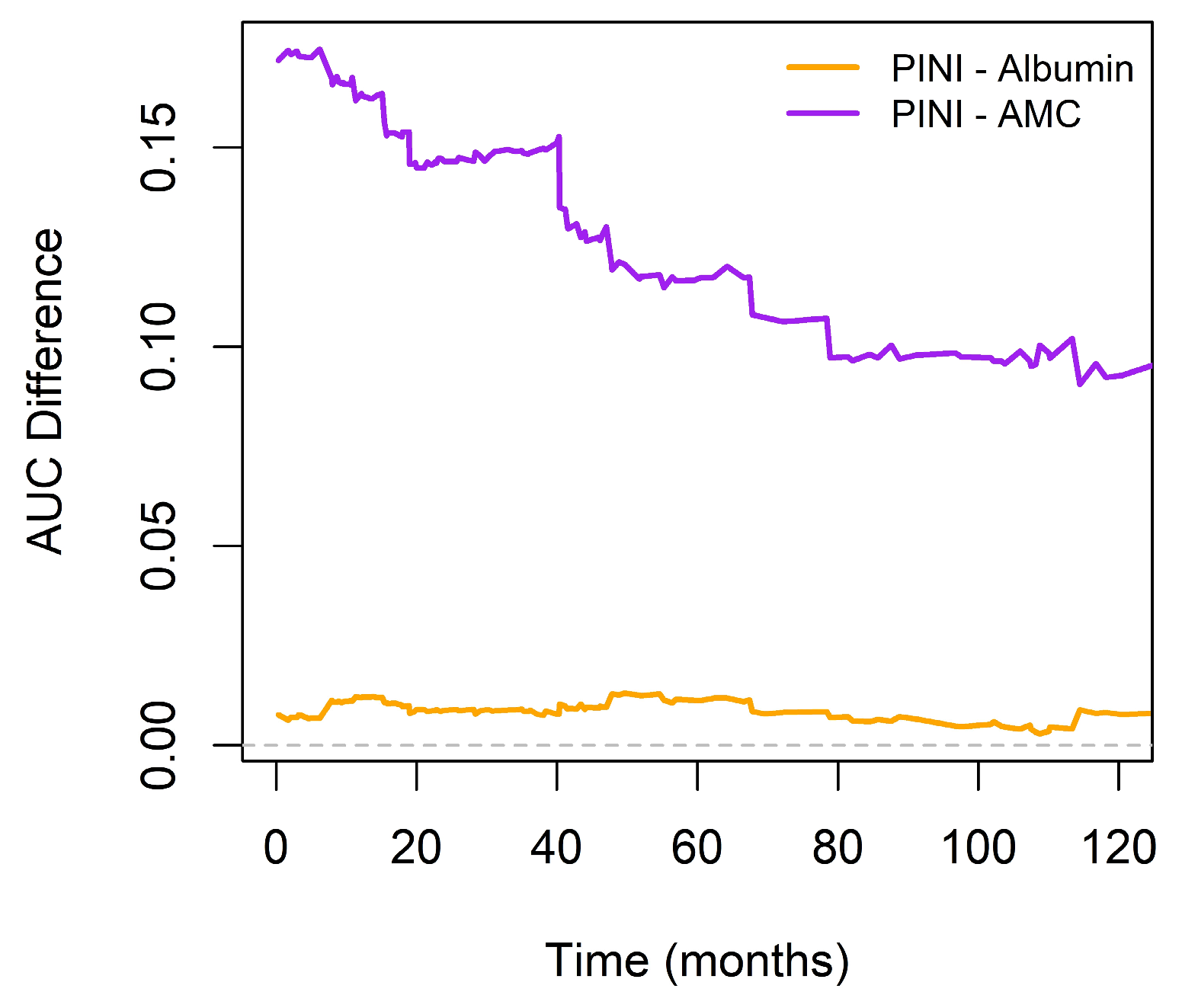
Figure 7.
Relationship between albumin and predicted hazard ratio across different AMC levels. AMC was fixed at the 25th, 50th, and 75th percentiles (367, 465, and 573 cells/µL). Linear predictors of the model were transformed into hazard ratios via exponentiation.
Figure 7.
Relationship between albumin and predicted hazard ratio across different AMC levels. AMC was fixed at the 25th, 50th, and 75th percentiles (367, 465, and 573 cells/µL). Linear predictors of the model were transformed into hazard ratios via exponentiation.
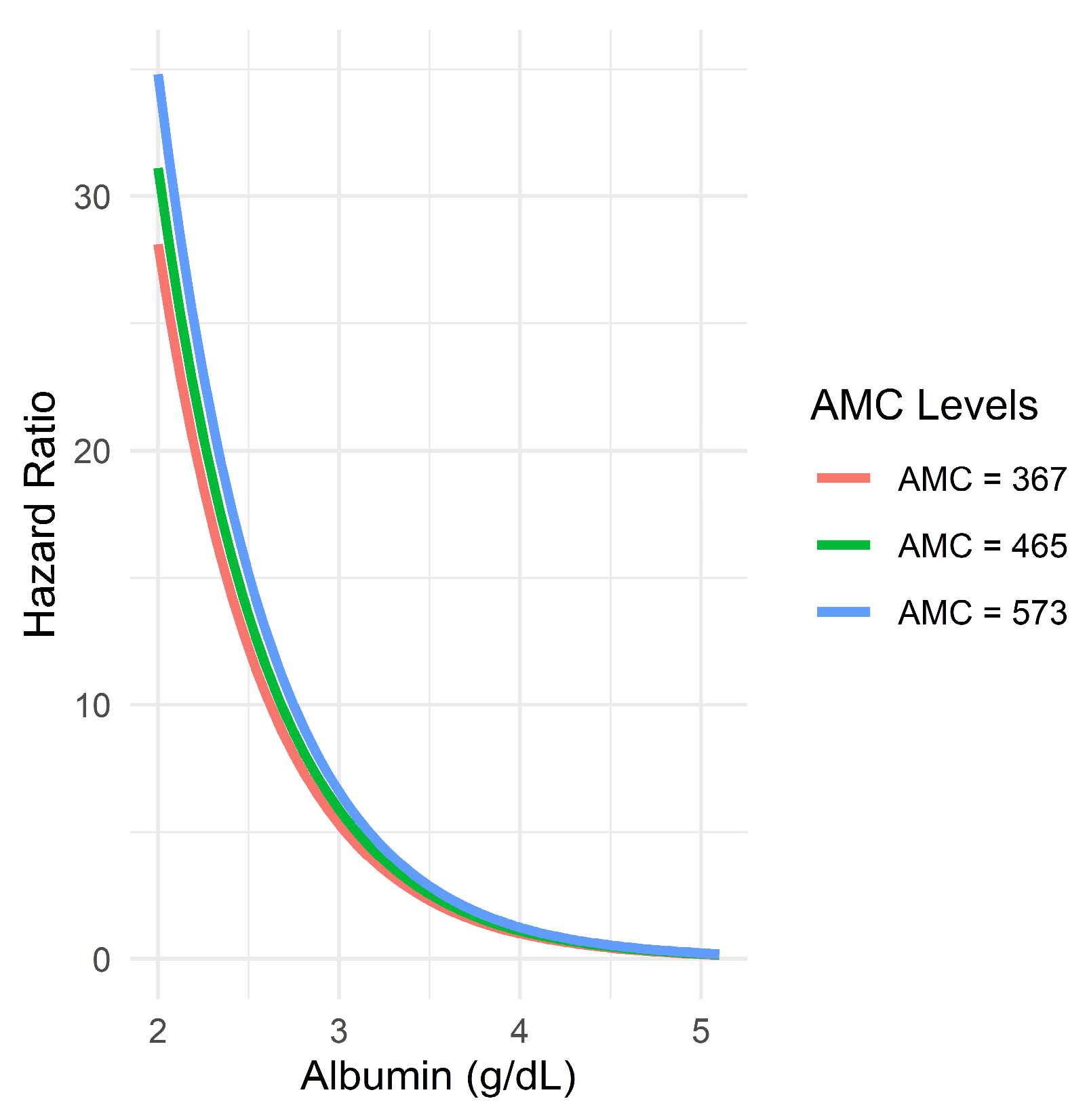

Table 1.
Baseline characteristics of study population with gastric cancer (GC).
| Variables | % or median (IQR) | Variables | % or median (IQR) |
|---|---|---|---|
| Age, years | 60.5 (52.0–70.0) | Tumor size, cm | 3.0 (2.0–5.5) |
| Sex | Lymphatic invasion | ||
| Men | 330 (67.1) | No | 325 (66.1) |
| Women | 162 (32.9) | Yes | 167 (33.9) |
| ASA-PS | Vascular invasion | ||
| I/II | 436 (88.6) | No | 466 (94.7) |
| III | 56 (11.4) | Yes | 26 (5.3) |
| mFI-5 score | Perineural invasion | ||
| 0–1 | 381 (77.4) | No | 442 (89.8) |
| 2–4 | 111 (22.6) | Yes | 50 (10.2) |
| BMI, kg/m2 | 23.7 (21.4–26.0) | Length of stay, days | 9 (8–11) |
| Location | Adjuvant therapy | ||
| Upper | 49 (10.0) | No | 320 (65.0) |
| Middle | 168 (34.1) | Yes | 172 (35.0) |
| Lower | 267 (54.3) | WBC, per μL | 6500 (5345–7850) |
| Diffuse | 8 (1.6) | ANC, per μL | 3660.5 (2899.5–4806.0) |
| T stage | ALC, per μL | 1907.5 (1534.5–2326.0) | |
| 0–1 | 334 (67.9) | AMC, per μL | 465.0 (367.0–573.5) |
| 2–4 | 158 (32.1) | Hemoglobin, g/dL | 13.1 (11.3–14.2) |
| N stage | MCV, fL | 92.2 (88.5–95.5) | |
| 0 | 320 (65.0) | Platelet, × 103 per μL | 238.0 (204.5–281.0) |
| 1–3 | 172 (35.0) | NLR | 1.9 (1.4–2.7) |
| TNM stage | PLR | 122.8 (96.7–159.1) | |
| I–II | 393 (79.9) | MLR | 2.3 (1.8–3.1) |
| III | 99 (20.1) | SII | 459.4 (303.8–682.7) |
| Histology | SIRI | 0.9 (0.6–1.3) | |
| Intestinal | 243 (49.4) | Albumin, g/dL | 4.1 (3.9–4.3) |
| Others | 249 (50.6) | PNI | 51.2 (47.2–54.7) |
| Type of gastrectomy | HALP score | 44.5 (30.4–58.5) | |
| Patial | 389 (79.1) | PINI score | 3.4 (3.2–3.6) |
| Total | 103 (20.9) |
Table 2.
Cox regression analysis for overall survival (OS) of patients with GC.
| Covariate | Univariate HR (95% CI) |
p-value | Multivariate HR (95% CI) |
p-value |
|---|---|---|---|---|
| Age, years (≤50 vs. >50) | 0.16 (0.08–0.35) | < 0.001 | 0.32 (0.15–0.69) | 0.004 |
| Sex (female vs. male) | 0.59 (0.40–0.87) | 0.008 | ||
| BMI, kg/m2 | 0.91 (0.87–0.96) | < 0.001 | 0.95 (0.90–1.00) | 0.044 |
| ASA-PS score† | 2.04 (1.42–2.91) | < 0.001 | ||
| mFI-5† | 1.50 (1.28–1.76) | < 0.001 | 1.28 (1.08–1.52) | 0.004 |
| TNM stage (IIIA vs. I/II) | 4.51 (3.23–6.31) | < 0.001 | 2.87 (1.99–4.13) | < 0.001 |
| Histology (intestinal vs. others) | 1.05 (0.75–1.45) | 0.787 | ||
| Lymphatic invasion (yes vs. no) | 2.79 (2.01–3.89) | < 0.001 | ||
| Vascular invasion (yes vs. no) | 3.32 (1.97–5.59) | < 0.001 | ||
| Perineural invasion (yes vs. no) | 1.99 (1.25–3.17) | 0.004 | ||
| Tumor size | 1.18 (1.14–1.22) | < 0.001 | ||
| TOG (total vs. partial) | 2.35 (1.66–3.33) | < 0.001 | 1.70 (1.19–2.42) | 0.003 |
| LOS, days | 1.02 (1.01–1.04) | < 0.001 | ||
| Adjuvant therapy (yes vs. no) | 2.48 (1.78–3.45) | < 0.001 | ||
| WBC | 1.00 (1.00–1.00) | 0.829 | ||
| AMC | 1.00 (1.00–1.00) | 0.003 | ||
| Anemia (yes vs. no) | 3.57 (2.55–5.01) | < 0.001 | 1.58 (1.07–2.32) | 0.020 |
| MCV | 0.97 (0.95–0.99) | 0.008 | ||
| Platelet | 1.00 (1.00–1.00) | 0.126 | ||
| Albumin | 0.18 (0.14–0.25) | < 0.001 | ||
| NLR | 1.16 (1.09–1.23) | < 0.001 | ||
| PLR | 1.01 (1.00–1.09) | < 0.001 | ||
| MLR | 1.42 (1.29–1.57) | < 0.001 | ||
| SII | 1.00 (1.00–1.00) | < 0.001 | ||
| SIRI | 1.21 (1.11–1.32) | < 0.001 | ||
| PNI | 0.87 (0.85–0.90) | < 0.001 | ||
| HALP score | 0.97 (0.96–0.98) | < 0.001 | ||
| PINI score | 0.16 (0.11–0.22) | < 0.001 | 0.36 (0.25–0.52) | < 0.001 |
† Ordinal variable.
Table 3.
Model comparisons for predicting OS in patients with GC.
| Metrics | Full model (FM)a | Intermediate model (IM)b | Baseline model (BM)c | FM vs. BM Difference (SE) | p-value | FM vs. IM Difference (SE) | p-value |
|---|---|---|---|---|---|---|---|
| C-index | 0.815 (0.017) | 0.797 (0.017) | 0.659 (0.020) | 0.159 (0.018) | < 0.001 | 0.018 (0.007) | 0.004 |
| iAUC | 0.791 (0.015) | 0.776 (0.017) | 0.640 (0.019) | 0.144 (0.019) | < 0.001 | 0.014 (0.006) | 0.004 |
| 3-year OS | |||||||
| AUC | 0.835 (0.024) | 0.821 (0.026) | 0.690 (0.032) | 0.144 (0.027) | < 0.001 | 0.013 (0.011) | 0.156 |
| IDI | 0.106 (0.027) | < 0.001 | 0.018 (0.016) | 0.206 | |||
| cNRI | 0.394 (0.066) | < 0.001 | 0.134 (0.072) | 0.054 | |||
| 5-year OS | |||||||
| AUC | 0.857 (0.020) | 0.839 (0.022) | 0.711 (0.027) | 0.146 (0.022) | < 0.001 | 0.019 (0.009) | 0.012 |
| IDI | 0.141 (0.029) | < 0.001 | 0.031 (0.016) | 0.032 | |||
| cNRI | 0.383 (0.054) | < 0.001 | 0.171 (0.062) | 0.012 |
aIncorporated age, BMI, mFI-5, stage, TOG, anemia, and the PINI. bConsisted of the same variables as those of the full model, excluding PINI. cRelied solely on cancer staging.
Table 4.
Model comparisons for predicting survival outcomes in patients with GC.
| Metrics | Full model (FM)a | Albumin model (AM)b | FM vs. AM Difference (SE) |
p-value |
|---|---|---|---|---|
| C-index | 0.815 (0.017) | 0.810 (0.025) | 0.005 (0.005) | 0.280 |
| iAUC | 0.791 (0.015) | 0.787 (0.015) | 0.003 (0.004) | 0.180 |
| AUC | ||||
| 3-year OS | 0.835 (0.024) | 0.833 (0.025) | 0.002 (0.007) | 0.872 |
| 5-yerar OS | 0.857 (0.020) | 0.851 (0.021) | 0.006 (0.006) | 0.412 |
aIncorporated age, BMI, mFI-5, stage, TOG, anemia, and the PINI. bConsisted of the age, mFI-5, stage, TOG, anemia, and serum albumin level.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



