Submitted:
28 April 2025
Posted:
29 April 2025
You are already at the latest version
Abstract
Hypertrophic cardiomyopathy (HCM) is often associated with left ventricular outflow tract (LVOT) obstruction, which affects a substantial proportion of patients. This obstruction results from a range of anatomical abnormalities involving both the valvular and subvalvular structures. Pharmacological therapies play a pivotal role in the management of LVOT obstruction, with a range of drug classes exhibiting distinct mechanisms of action. Beta-blockers, including atenolol and nadolol, are considered the first-line treatment due to their ability to reduce heart rate, myocardial contractility, and enhance diastolic filling. Non-dihydropyridine calcium channel blockers, such as verapamil and diltiazem, are utilized as second-line agents when beta-blockers are ineffective or contraindicated. These agents inhibit calcium influx and improve diastolic function. Disopyramid, a Class 1A antiarrhythmic agent, is employed for patients who do not respond to initial therapeutic interventions and can reduce LVOT gradients. Recent advancements in cardiac myosin modulators, such as Mavacamten and Aficamten, offer targeted therapies by modulating myosin-actin interactions to reduce LVOT gradients and improve symptoms, with promising results from clinical trials. Although gene therapy is still in its nascent stages, it has the potential to address the genetic basis of HCM by employing techniques such as genome editing, gene replacement, and modulation of signaling pathways. Despite the encouraging developments in these fields, further research is necessary to optimize the clinical application of these therapies. For patients exhibiting severe symptoms or demonstrating unresponsiveness to medical treatment, invasive therapies, such as septal reduction therapy (SRT) and alcohol septal ablation (ASA), are considered. SRT, which involves surgical myectomy, offers a comprehensive solution by addressing anatomical anomalies, while ASA provides a less invasive option with similar gradient reduction outcomes. This review aims to provide an overview of current pharmacological and invasive strategies, as well as emerging therapies, in the management of HCM.
Keywords:
Hypertrophic cardiomyopathy (HCM)
; Left ventricular outflow tract (LVOT) obstruction
; Phar-macological therapy
; Beta-blockers
; Calcium channel blockers
; Disopyramide
; Cardiac myosin modulators
; Mavacamten
; Gene therapy
; Septal reduction therapy (SRT)
1. Introduction
Hypertrophic cardiomyopathy (HCM) is a genetic heart disease characterized by marked wall thickness that is unexplained by overload conditions. Despite its historical prevalence, the efficacy of standard pharmacological therapy remains uncertain due to the paucity of randomized clinical trials demonstrating its effectiveness[1]. The natural history of HCM is marked by the development of heart failure (HF), arrhythmias, and sudden cardiac death (SCD), exhibiting clinical presentation heterogeneity ranging from asymptomatic conditions to severe manifestations. The initial step in the therapeutic approach is the identification of left ventricular outflow tract (LVOT) obstruction. In obstructive forms, defined by a LVOT gradient >30 mmHg, symptoms manifest as exertional dyspnea/fatigue, chest pain (angina), syncope/presyncope, and HF. In obstructive forms, the therapeutic objective is to reduce LVOT obstruction. In non-obstructive forms, treatment objectives include the reduction of HF and the occurrence of atrial fibrillation, as well as the prevention of cardioembolic events[2,3]. Diagnostic progress has recently led to a precise distinction between obstructive and non-obstructive forms and between HCM and phenocopies such as cardiac amyloidosis[4,5,6,7,8,9,10,11]. This aspect is crucial for the effective implementation of the pharmacological therapy[12,13]. In this regard, ATPase inhibitors have exhibited the capacity to modify the natural progression of the disease, exerting their effects on the heightened contractility of the myocardium[1]. These novel pharmacotherapeutic agents have marked a pivotal shift in the therapeutic approach for HCM. Furthermore, gene therapy constitutes a novel approach that aims to precisely modify specific DNA sequences through various techniques, such as genome editing. These treatments offer significant potential, though further research is required to fully realize their clinical applicability[14]. Invasive strategies for treating LVOT obstruction include septal reduction therapy, which encompasses ventricular septal myectomy and alcohol septal ablation[1]. The objective of this review is to analyze the different therapeutic approaches, from those that have been demonstrated to be effective to those that are emerging, in the context of HCM. It is imperative to comprehend such a multifaceted approach, particularly in a pathology such as HCM, which exhibits a wide range of phenotypes and grades of severity and necessitates comprehensive treatment strategies.
2. Pharmacological Therapy in Obstructive Forms
LVOT obstruction is present in 1/3 of patients[15], is caused by many factors e by anoumalous anatomy of valvular and subvalvular apparatus. Describing the pathophysiological mechanisms of LVOT obstruction is beyond the scope of this review. The drugs for the managment of LVOT obstruction are various, with different characteristics[1,3].
2.1. Beta-Blockers and Non-Dihydropiridine Calcium Channel Blockers
Beta-blockers (BB) represent the most prevalent class of drugs employed in the treatment of HCM, with their utilization being predicated on the attenuation of sympathetic activity, culminating in a reduction of heart rate and ventricular contractility. This, in turn, engenders an enhancement of diastolic filling, a diminution of oxygen demand, and a reduction of exercise-induced LVOT gradient[16]. The first beta-blocker utilized was propanolol, as evidenced by a small non-randomized study demonstrating a reduction in gradient and an improvement in symptoms[15]. Its efficacy in the treatment of angina and the control of heart rate has led to its frequent use in pediatric patients diagnosed with obstructive HCM (OHCM)[17]. However, it should be noted that propanolol is not the drug of choice for adult patients. Atenolol, with doses up to 150 mg, is the recommended treatment for adults with obstructive HCM and hypertension. Similar to propanolol, it is effective in managing angina and effort dyspnea, and it is more potent in regulating heart rate. Nadolol, similar to atenolol, is effective in managing LVOT obstruction and reducing non-sustained ventricular tachycardia (NSVT) episodes[18]. Bisoprolol and metoprolol are the drugs of choice in cases of HCM with heart failure and in end-stage HCM. However, Dybro et al. has showed that metoprolol reduced LVOT obstruction at rest and during exercise, provided symptom relief, and improved quality of life also in patients with OHCM[19]. It is imperative to note that the dosage of these medications must be gradually increased until they are tolerated by the patient. The primary constraints associated with the utilization of BB pertain to their adverse effects, which include bradycardia, hypotension, and airway reactions[20]. Non-dihydropiridine calcium channel blockers (ND-CCB) are utilized when beta-blockers are contraindicated or not tolerated. These agents represent a second-line treatment option due to their reduced efficacy compared to beta-blockers. The rationale for using this class of drugs is, once again, the negative inotropic effect, obtained with a different mechanism than BB: the reduction of calcium (Ca++) intracellular inflow by blocking calcium channel[21]. In animal models, calcium channel blockers have demonstrated efficacy in treating alterations associated with the R403Q mutation in the MHY6 gene, even in the absence of hypertrophy[22]. The negative chronotropic effect of calcium channel blockers leads to improved diastolic filling, reduced oxygen demand, and improved symptoms. However, the vasodilation caused by these drugs can lead to dangerous effects, including increased left ventricular (LV) outflow tract obstruction and peripheral edema[3,21]. The natural history of patients with HCM is characterized by events such as atrial fibrillation occurrence, hospitalizations for HF, and SCD[23]. For these reasons it is important to use drugs that have also a prognostic impact. So far, BBs and ND-CCBs have not provided any evidence of improving prognosis in patients with HCM, either with an obstructive phenotype or not. Of note, numerous studies have highlighted the possibility of severe adverse effects with verapamil, leading to its limited use in patients with severe obstruction or increased ventricular filling pressure[24]. In this scenario a recent study has showed that in a real-world cohort of low-risk patients with HCM, either obstructive or not, verapamil therapy was not associated with a higher incidence of CV events than BB therapy[25]. Considering these results, verapamil appears to be an effective and safe alternative to BBs in the therapeutic algorithm of HCM.
2.2. Disopyramid
The utilization of disopyramid is recommended by European Guidelines (Class I) for patients who continue to experience symptoms or demonstrate non-responsiveness to beta-blockers or calcium channel blockers[3]. Disopyramid is classified as a Class 1A antiarrhythmic agent, exhibiting a negative inotropic effect. This cardiac effect of disopyramid has been demonstrated to improve symptoms and reduce LVOT gradient[26,27]. Disopyramid is administered in conjunction with beta-blockers or calcium channel blockers, as it can facilitate the AV conduction and increase the risk of high-rate atrial fibrillation (AF) episodes. It is imperative to inform patients of the necessity to avoid the use of concomitant medications associated with QTc prolongation[28]. The limitations of disopyramid include its gradual loss of efficacy over time[29,30], the absence of a long-acting formulation, necessitating frequent dosing (every 6-8 hours), which can cause patient discomfort, the potential for QTc prolongation requiring ECG monitoring, anticholinergic effects (e.g., xerostomia), and, in male patients, prostatism and urinary tract symptoms[27]. In instances of disopyramide intolerance, cibenzoline, a class Ia antiarrhythmic agent, has been employed, demonstrating efficacy in reducing LVOT obstruction and enhancing diastolic function[31]. In a recent real-world study, Maurizi et al.[32] demonstrated that the best responders to disopyramid therapy were younger, had a smaller left atrium, less severe LVOT gradient, and a higher LV ejection fraction, with a safe arrhythmic profile. These findings are in line with the drug physiopathological effect, mainly driven by its negative inotropic effect, which is the main mechanistic driver of reduction in LVOT gradients. This evidence suggests that clinicians should not be discouraged from trying disopyramide in patients who are symptomatic and have high LVOT gradients despite administering the maximum doses of other negative inotropic drugs[32]. In Figure 1 and Table 1 the mechanism of action and properties of the principal drugs used in the management of OHCM are represented.
2.3. Cardiac Myosin Modulators: Mavacamten and Aficamten
Mavacamten and Aficamten are two new drugs used to treat LVOTO in OHCM. These treatments represent a turning point in the scenario of cardiomyopathies management, because able to change the natural history of the pathology[33]. HCM is characterized by an exaggerated interaction between myosin and actin filaments in the heart muscle. The mechanism of action Mavacamten works by reducing ATP hydrolysis, which decreases the number of myosin heads available to interact with actin filaments. It stabilizes myosin in a super-relaxed state, preventing cross-bridge formation. This effect can also downregulate the metabolic pathway linked to hypertrophy and fibrosis in HCM. Early animal testing of Mavacamten led to successful Phase 1 and 2 clinical trials. The PIONEER-HCM trial[34], a Phase 2 study, demonstrated that Mavacamten reduced the LVOT gradient, improved symptoms, NYHA class, oxygen demand, and pro-BNP levels. The EXPLORER-HCM trial[35], a Phase 3 study, involved 251 patients with HCM and LVOT gradients >50 mmHg. Mavacamten treatment led to a reduction in LVOT gradient, improved diastolic function, left atrial volume, and LV mass index. However, 6% of patients had reduced left ventricular function, which improved after stopping treatment. About one-third of patients did not respond to Mavacamten, suggesting varying responses among patients, unrelated to genotype. The VALOR-HCM trial[36], focused on patients eligible for septal reduction therapy (SRT), showed that only 18% of Mavacamten-treated patients maintained eligibility for SRT after 16 weeks, indicating improvement in symptoms. Results from the ongoing MAVA-LTE trial[37] suggest that Mavacamten remains effective in the medium term. A recent study by Wheeler et al. demonstrated that Mavacamten was effective in improving functional capacity, LVOTO, symptom burden, and biomarkers, independent of the use of beta-blockers[38]. Subsequent meta-analyses have confirmed the safety and efficacy of this drug in OHCM[39,40]. Mavacamten has been recently tested also on symptomatic HCM patients without LVOTO. The medication was found to be well tolerated by the majority of subjects, resulting in a significant decrease in biomarkers (NT-proBNP and troponin levels)[41]. These findings provide a foundation for additional research targeting non-obstructive HCM population. The second cardiac myosin inhibitor, Aficamten, has a shorter half-life (3-4 days) compared to Mavacamten (6-8 days) and reaches the steady state more quickly (2 weeks vs. 6-8 weeks for Mavacamten). Aficamten does not interact with CYP450 enzymes, differently from Mavacamten which affects CYP2B6 and CYP3A4. The REDWOOD-HCM trial[42] demonstrated that Aficamten effectively reduced LVOT gradients in patients with NYHA class II or III symptoms, with no significant adverse effects, except for one patient who discontinued treatment due to reduced left ventricular function. REDWOOD-HCM cohorts 1 and 2 showed that Aficamten may reduce LVOT gradient safely in patients already in treatment with BB and/or ND-CCB. On the other hand, in REDWOOD-HCM cohort 3 Aficamten demonstrated to be an effective add-on treatment in patients who do not respond to all other medical therapies[43]. Aficamten has been demonstrated to be effective in improving peak oxygen uptake, symptoms, exercise capacity, and NT-pro-BNP levels[44,45]. A substudy of the SEQUOIA-HCM trial has demonstrated also the efficacy of Aficamten in improving cardiac remodeling, particularly with regard to left ventricular mass, wall thickness, and left atrial size[46]. The ongoing phase 3 MAPLE-HCM trial is evaluating Aficamten as both first-line therapy for newly diagnosed OHCM and as an alternative to standard drugs (BB and CCB)[47]. Both cardiac myosin ATPase inhibitors have shown promise in clinical trials, with continued research needed to optimize their use. The mechanism of action of ATPase inhibitors is illustrated in Figure 2.
3. Gene Therapy
HCM is an autosomal dominant disorder that is genetically heterogeneous. It results from over 1,500 identified mutations across at least 15 distinct genes[48]. Since advancements in DNA sequencing technology have been made, genetic testing and counseling are now strongly recommended[3,49]. Given the genetic basis of HCM, novel therapeutic opportunities have emerged, including gene therapy. This approach entails the precise modification of specific DNA sequences. Gene therapy is predicated on several methodologies. One of the first tested techniques was genome editing, which involves the precise modification of specific DNA nucleotides using cluster regularly interspaced short palindromic repeats (CRISPR)-Cas9 endonucleases. These endonucleases can cleave DNA at specific sites, allowing for the precise alteration of genetic material[50]. The first application of genome editing was in a study involving human embryos. In this study, human sperm carrying a pathological MYBPC3 mutation were injected into oocytes with a normal MYBPC3 allele. The study demonstrated the remarkable capacity of CRISPR-Cas9 to produce a normal MYBPC3 allele in 72% of the embryos[51]. Subsequent studies employing genome editing in animal models yielded encouraging results, underscoring its potential for therapeutic applications[52,53]. Another technique is gene replacement, which is used when the mutation causes deficiency or complete absence of the protein, as in the case of haploinsufficiency. This technique is particularly suitable for MYBPC3, the most common mutation in HCM. The objective of this approach is to introduce a functional gene copy that can synthesize a functional protein. This approach does not directly address the mutation; rather, it provides an exact copy of the gene, thereby reducing the production of the abnormal protein[22]. Two strategies are employed to achieve this objective. The first strategy involves the introduction of a wild-type MYBPC3 DNA copy (cDNA) by viral vectors, resulting in an increase in mRNA and wild-type myosin-binding protein C levels in animal models, with this increase being dose-dependent[54]. The second strategy utilizes RNA transcription, wherein the pre-RNA is spliced together with gene therapy products, which consist of sequences of wild-type exons, to create a repaired mRNA. Allelic Specific Silencing is another possible approach in this setting. It consists of modifying the mRNA, emulating the mRNA alteration system that is inherently present in cells. It involves exon skipping, which entails the introduction of oligonucleotides that are complementary to specific sequences of the pre-RNA into cells by viral vectors. These oligonucleotides attach themselves to these sequences, impeding the action of the splicing regulatory protein and preventing the sequences from being inserted into the mature RNA. This results in the formation of an RNA devoid of the mutation[55]. This technique finds application when an allele of a gene carries a mutation and the other allele is normal[50]. RNA interference is particularly well-suited for conditions driven by gain-of-function mutations, such as MYH7, but its applicability to the entire spectrum of HCM, including MYBPC3-related cases, is not yet clear[1]. Modulation of signaling pathways is another technique that involves the interference with the pathways that regulate the contraction and relaxation of the cardiac muscle. Two therapeutic targets have been identified for HCM: sarcoplasmic/endoplasmic reticulum Ca2+ ATPase 2a (SERCA2) and myosin regulatory light chain (myosin RLC). In HCM, a reduction in SERCA2 levels has been observed, suggesting that the introduction of this mutation by viral vectors may prove beneficial[14]. The mutation of myosin RLC has been linked to an aggressive form of HCM. In animal models, the introduction of the aforementioned viral vectors has been demonstrated to result in a reduction in left ventricular hypertrophy and an enhancement in cardiac function[56,57,58]. Figure 3 resumes the novel gene therapy approaches previously described.
Notwithstanding the encouraging results, there are numerous limitations and challenges that must be considered. The utilization of viral vectors, which are innocuous, has the potential to stimulate the immune system. However, many patients may possess neutralizing antibodies that could render the vectors ineffective. The CRISPR/Cas9 system, in particular, poses a series of challenges due to its potential for off-target activity and the induction of unintended mutations. This potential for off-target effects is a subject of intensive research, with the development of selective RNA guides aimed at mitigating these risks. Despite the encouraging results, the translation of these findings into clinical practice remains in its nascent stages, with the safety and ethical considerations being paramount[14].
4. Invasive Strategies: Surgery and Alcohol Septal Ablation
LVOTO is defined as a peak LVOT gradient of ≥30 mmHg. However, the threshold for invasive treatment is generally considered to be ≥50 mmHg (resting or provoked by exercise or Valsalva) in patients with severe symptoms (NYHA functional class III-IV) despite maximally tolerated pharmacological treatment[3]. Invasive therapy may be considered also for patients with mild symptoms (NYHA class II) who do not respond to medical therapy. This therapy is recommended in expert centers with demonstrable low procedural complication rates[59]. Invasive treatment for LVOTO involves septal reduction therapy (SRT) when the anterior septal thickness is equal to or greater than 15 mm. The two main techniques for SRT are ventricular septal myectomy and alcohol septal ablation (ASA). An assessment checklist is crucial for the evaluation of candidates for invasive treatment. It is imperative to assess alternative causes that can explain symptoms (e.g., obesity, respiratory disease, coronary artery disease, anemia, thyroid disease, arrhythmia, amyloid, right-ventricular outflow tract obstruction). Imaging plays a pivotal role in evaluating the underlying mechanism of obstruction (e.g., SAM-related, sub-aortic membrane, anomalous papillary muscle insertion, accessory mitral valve tissue), the function of the mitral valve (MV), and the distribution and severity of hypertrophy[3]. Surgical myectomy has long been regarded as the gold standard for treating symptomatic patients with significant LVOTO. It effectively reduces symptoms, maintains long-term survival rates, and can improve left ventricular function by alleviating the obstruction caused by muscle hypertrophy[60,61]. Notably, a systematic review indicated that the five-year survival rates post-myectomy are high, reportedly around 98.9%[60]. In contrast, alcohol septal ablation, a less invasive technique, has also gained recognition for its safety and efficacy. Studies indicate that ASA can provide similar symptomatic relief and improve LVOT gradient comparable to myectomy, yielding notable long-term benefits and survival rates that align with those of surgical myectomy[61,62]. Comparative analyses suggest that both procedures offer comparable outcomes regarding mortality and functional status post-operation. A systematic review concluded that recent evidence shows no significant difference in cumulative outcomes, including survival and stroke incidence, between the two interventions[60,61]. Furthermore, ASA has emerged as a prudent option for older patients or those with comorbidities that may render them unfit for surgical intervention, highlighting its importance in a diverse patient population struggling with HCM[62,63]. Recent case reports and analyses have demonstrated the nuanced decision-making involved in choosing between these two approaches. For instance, ASA is often considered for patients who are not ideal candidates for myectomy due to anatomical variations or significant comorbidities[64,65]. In adult patients with symptomatic OHCM in whom surgery is contraindicated or the risk is considered unacceptably high because of serious comorbidities or advanced age, ASA when feasible and performed in experienced centers becomes the preferred invasive strategy for relief of LVOTO[66]. In patients who have associated cardiac disease requiring surgical treatment (e.g. associated anomalous papillary muscle, markedly elongated anterior mitral leaflet, intrinsic MV disease, coronary artery disease, valvular aortic stenosis), the surgical intervention performed by experienced operators provides the opportunity to correct all structural and anatomic issues with a single procedure[66]. Additionally, procedural advancements, such as the use of high-precision imaging and mapping techniques, have enhanced the efficacy and safety profiles of ASA, aligning well with contemporary surgical goals of minimally invasive practices[67]. Furthermore, ongoing investigations aim to explore combined approaches or novel pharmacological adjuncts that may aid in the management of HCM and influence decisions regarding surgical interventions[68]. Despite there are no randomized trials comparing surgery and ASA, meta-analyses have shown that both procedures improve functional status with a similar procedural mortality[3,69,70]. From these studies emerged that ASA was associated with a higher rate of reoperation and less reduction of LVOT gradient[71], with a higher risk of atrio-ventricular (AV) block, requiring permanent pacemaker (PM) implantation. The risk of AV block following surgery and ASA is higher in patients with pre-existing conduction disease although recent data suggest that the long-term outcome of patients after ASA with implanted permanent PM is similar to those without PM[69,70]. Conclusively, both surgical myectomy and alcohol septal ablation represent critical elements of the therapeutic landscape for hypertrophic cardiomyopathy. A clear understanding of the distinctions, advancements, and practical applications of these interventions enables healthcare providers to develop tailored, patient-centric management strategies.
Ventricular septal myectomy. This procedure consists of creating a rectangular trough in the basal septum below the aortic valve, then extended distally to beyond the point of the mitral leaflet–septal contact. The classic Morrow myectomy was described for the first time in 1975[72]. In the classic Morrow procedure, LVOTO is relieved by resecting relatively small sections of muscle tissue in the proximal ventricular septum, which widens LVOT and partially decreases the hydrodynamic drag forces along with a “Venturi” effect resulting in SAM (Figure 4A-5B). Many variations of this procedure have been reported with varied efficacy[73,74]. For the modified Morrow procedure, the incision was made by extending the classic incision with a midventricular resection, beginning with continued resection leftward toward the MV annulus and apically to the bases of the papillary muscles (Figure 4C). All areas of papillary muscle fusion to the septum or ventricular free wall were divided, and anomalous chordal structures, muscle bundles, and fibrous attachments of the mitral leaflets to the ventricular septum or free wall were divided or excised. Extensive myectomy results in enlargement of the LVOT area and redirection of forward flow with loss of the drag and Venturi effects on the mitral valve[75]. Pre-operative determinants of a good long-term outcome are age <50 years, left atrial size <46 mm, absence of AF, male sex[3]. Typically, septal myectomy is approached by transaortic route. Transaortic septal myectomy is a well-tried procedure, with wide and long follow-up, in addition the aorta incision is not arrhythmogenic[73,74,76]. On the other hand, transaortic septal myectomy is characterized by a limited operating field, with limited visualization of the MV[66]. This makes this procedure prohibitive in case of small aortic annulus (i.e. infants and young children); in such instances, the modified Konno procedure has been reported to provide equally satisfactory long-term results for basal obstruction[77,78,79]. Therefore, other surgical approaches are being tested as transapical and trans-mitral exposure. Transapical approach is a safe and effective approach for relief of midventricular obstruction[80,81]. The technique can be combined with transaortic myectomy for patients with left ventricular outflow obstruction at both levels[81]. Trans-mitral approach is feasible and reliable for the treatment of certain types of OHCM cases. Potential advantages of transmitral myectomy include a panoramic view of the septum and mitral subvalvular apparatus and the ability to simultaneously address MV pathology[82]. The latter is preferable in patients with diffuse hypertrophy, abnormal papillary muscle orientation and MV abnormality. Transmitral approach allows aggressive papillary muscle reorientation[83], enlargement of LVOT using an autologous pericardial patch for anterior MV leaflet (Figure 4D)[84], MV repair or replacement. Cardiac imaging provides key information for planning surgery: small aortic root, anterior mitral leaflet length > 30 mm, intraventricular septum thickness <19 mm or neutral septum and mitro-aortic angle <120° lean to transmitral approach. Management of MV is a big challenge to HCM surgery. MV replacement is more common in non-specialized HCM centers than in specialized HCM centers. Valve replacement eliminates SAM and associated mitral regurgitation as well as the outflow tract gradient but the addition of MV replacement with or without myectomy increases the hospital mortality rate (>10-fold) and length of hospitalization compared with patients undergoing isolated septal myectomy. Further, when intervention on the valve at the time of myectomy is needed because of intrinsic mitral disease, every effort should be made to repair the valve because early and long-term mortality is worse in patients with prosthetic replacement compared with patients who have septal myectomy and MV repair[66]. A very complex category of OHCM patients are those affected by mitral annular calcium (MAC), who represents about the 1/10 of OHCM population: MAC is associated with anterior displacement of mitral coaptation and contributes to the pathophysiology of LVOTO[85]. These patients have worse prognosis and more recurrent MV regurgitation than those without MAC after septal myectomy. Furthermore, a paravalvular leak is often present after replacement[86]. In patients with AF, concomitant ablation using the Cox– Maze procedure can also be performed[3].
Alcohol septal ablation and alternative methods. ASA involves the percutaneous injection of absolute alcohol into the septal arteries supplying the hypertrophied myocardium, resulting in a controlled myocardial infarction that reduces LVOTO and alleviates symptoms[87,88]. The outcomes of this procedure are similar to surgery in terms of gradient reduction, symptom improvement, and exercise capacity, including also younger adults[3,89]. Due to the variability of the septal blood supply, myocardial contrast echocardiography is essential prior to alcohol injection. Injection of large volumes of alcohol in multiple septal branches—with the aim of gradient reduction—in the catheter laboratory is generally not recommended, as it can be associated with a high risk of complications and arrhythmic events[90,91]. However, the procedure is not without complications. The primary risks associated with ASA include the potential for complete heart block, necessitating pacemaker implantation in 10-12% of patients[65]. Notably, careful patient selection and planning, such as considering the distribution of coronary arteries, are crucial for minimizing complications associated with this technique[92]. Variations in alcohol dosage have also been implicated in outcomes, as lower doses may be associated with higher rates of repeat septal reduction therapies due to inadequate myocardial necrosis[61,93]. The decision-making process regarding the use of ASA versus other treatment modalities relies on an interdisciplinary approach, incorporating cardiologists’ insights on the individual patient’s pathology, risks, and expected outcomes [88,91]. Alternative methods have been reported in small numbers of patients[94,95], including non-ASA techniques (coils, polyvinyl alcohol foam particles, cyanoacrylate) and direct endocavitary and intramuscular ablation (radiofrequency, cryotherapy). Glue septal ablation (GSA) is a promising approach. Its main advantage is the immediate polymerization, which prevents leakage into the left anterior descending coronary artery. This characteristic renders GSA particularly beneficial for patients with collateral circulation to the right coronary artery, for whom alcohol ablation is contraindicated. No significant complications in the clinical experience of this technique have been reported. The procedure leads to an immediate reduction of LVOT gradient, and this improvement has been demonstrated to be maintained throughout 12 months of follow-up[95]. Furthermore, GSA has been shown to enhance functional capacity according to the NYHA classification and to reduce interventricular septal wall thickness. However, further research is necessary to assess the long-term efficacy and safety of this technique. Also microcoil embolisation has produced promising results, avoiding the toxic effects of alcohol[96]. A lower percentage of complications (e.g. need for PM implantation, ethanol flow to other myocardial regions) has also been reported[97]. These alternative methods have not been directly compared with other septal reduction therapies and long-term outcome/safety data are not available[95].
5. Management of Non-Obstructive Forms
In patients without obstruction in LVOT and with a normal ejection fraction, symptoms are secondary to diastolic dysfunction due to LV hypertrophy, stiffness of the wall, a small cavity, and myocardial fibrosis[98]. The initial step in the diagnostic process is the evaluation of LVEF. If the EF is equal to or greater than 50%, the administration of beta-blockers or calcium channel blockers (e.g., verapamil or diltiazem) is recommended[3]. These medications have been shown to enhance quality of life, alleviate symptoms, extend diastolic filling time, and mitigate the severity of chest pain[99]. Nitrates represent a second-line therapeutic option, unless concomitant coronary disease is present. When LVEF is equal to or less than 50%, the therapeutic approach for HF remains consistent, involving the administration of beta-blockers, angiotensin-converting enzyme inhibitors (ACEi), angiotensin receptor blockers (ARB), mineralocorticoid receptor antagonists (MRA), sodium-glucose cotransporter 2 inhibitors (SGLT2i), and low-dose diuretics (Figure 5)[3,16,100,101]. Other studies focused on the role of different drugs in non-obstructive HCM with preserved left ventricular ejection fraction. The use of sacubitril/valsartan in symptomatic patients with non-obstructive HCM is currently under study[102]. However, initial findings indicate that a 16-week treatment period with this pharmaceutical agent, while generally well-tolerated, does not demonstrate substantial enhancement of exercise capacity or cardiac structure and function. The impact of losartan has been thoroughly investigated in several randomized controlled trials. First reports indicated the efficacy of the drug in halting the progression of hypertrophy and fibrosis[103]. However, this finding was contradicted by subsequent research[104]. Another study demonstrated the beneficial effect of valsartan in improving cardiac remodeling in individuals with sarcomeric HCM[105]. Also the role of ranolazine in this context remains a subject of debate[106]. Recent trials have not demonstrated any beneficial effects in non-obstructive HCM[107].
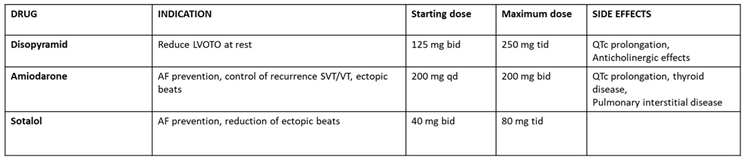
Patients with HCM who are completely asymptomatic, devoid of signs of HF, and exhibiting no symptoms due to arrhythmias do not require treatment. However, some patients classified as "asymptomatic" derive benefit from low-dose beta-blockers, particularly during periods of physical exertion. It is imperative to inquire about the presence of symptoms in patients, as they may exhibit self-limiting daily activities. In young patients who engage in regular physical activity, the administration of beta-blockers is recommended to mitigate the potential for an increase in heart rate[108]. Routine ambulatory visits are necessary to monitor the progression of the pathology and to promptly intervene as required[109]. Given the prevalence of atrial fibrillation (AF) as the most commonly observed arrhythmia in patients with HCM, a discussion of its treatment is pertinent. In patients with LVOTO, the presence of AF often results in a more unfavorable prognosis if not addressed promptly[110]. In cases of paroxysmal AF, restoring sinus rhythm is reasonable, given the atrial contribution to ventricular filling. According to established guidelines, amiodarone is recommended as the initial treatment, with subsequent electrical cardioversion. In the long term, sotalol and disopyramid are the drugs of first choice for the prevention of AF recurrences, particularly in patients with LVOTO[111]. It is imperative to avoid other antiarrhythmic class IC drugs, such as flecainide and propafenone, due to their proarrhythmic potential. In cases where restoration of sinus rhythm is not feasible, it is imperative to implement rate control with beta-blockers (even in cases of reduced ejection fraction) or calcium channel blockers (only if ejection fraction is preserved)[111]. The use of digoxin is contraindicated; it may be utilized only in advanced, end-stage HF. According to European Guidelines[3], oral anticoagulation is recommended to reduce the risk of stroke and thromboembolic events in all patients with HCM and AF or atrial flutter (unless contraindicated), independent of the CHADS-Va score[112] (Table 2).
6. Conclusions
HCM with LVOTO represents a complex clinical challenge, requiring a multifaceted therapeutic approach. Pharmacological treatments, including beta-blockers, calcium channel blockers, and disopyramide, remain fundamental in the management of symptoms and the reduction of LVOT gradients. The advent of cardiac myosin modulators has emerged as a pivotal development, with the potential to transform the natural progression of the pathology. While gene therapy is still in its nascent stages, its potential to revolutionize the field by addressing the underlying genetic causes of HCM is a promising avenue for future research. For patients exhibiting refractory symptoms, invasive treatments such as septal reduction therapy and alcohol septal ablation offer viable alternatives. However, ongoing research and clinical trials are imperative to refine these strategies, optimize their use, and explore novel therapies for enhanced patient outcomes. A personalized multimodal treatment approach, incorporating both established and emerging therapies, will be pivotal in managing the diverse manifestations of HCM with and without LVOTO.
Author Contributions
Conceptualization, M.M.D. and I.D..; methodology, M.M.D., I.D. and A.I.G.; writing—original draft preparation, M.M.D., G.C., F.M., R.A., M.A. and C.A.G.; writing—review and editing, G.C., P.B., S.C., M.C.C. and C.F.; visualization, M.C.C., A.I.G., S.C., C.F.; supervision, C.F., M.M.C., A.I.G. and I.D.; project administration, I.D. and A.I.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tuohy, C.V.; Kaul, S.; Song, H.K.; Nazer, B.; Heitner, S.B. Hypertrophic cardiomyopathy: the future of treatment. Eur J Heart Fail 2020, 22, 228–240. [Google Scholar] [CrossRef] [PubMed]
- Ammirati, E.; Contri, R.; Coppini, R.; Cecchi, F.; Frigerio, M.; Olivotto, I. Pharmacological treatment of hypertrophic cardiomyopathy: current practice and novel perspectives. Eur J Heart Fail 2016, 18, 1106–1118. [Google Scholar] [CrossRef] [PubMed]
- Arbelo, E.; Protonotarios, A.; Gimeno, J.R.; Arbustini, E.; Barriales-Villa, R.; Basso, C.; Bezzina, C.R.; Biagini, E.; Blom, N.A.; de Boer, R.A.; et al. 2023 ESC Guidelines for the management of cardiomyopathies. Eur Heart J 2023, 44, 3503–3626. [Google Scholar] [CrossRef] [PubMed]
- Merlo, M.; Gagno, G.; Baritussio, A.; Bauce, B.; Biagini, E.; Canepa, M.; Cipriani, A.; Castelletti, S.; Dellegrottaglie, S.; Guaricci, A.I.; et al. Clinical application of CMR in cardiomyopathies: evolving concepts and techniques : A position paper of myocardial and pericardial diseases and cardiac magnetic resonance working groups of Italian society of cardiology. Heart Fail Rev 2023, 28, 77–95. [Google Scholar] [CrossRef]
- Forleo, C.; D'Erchia, A.M.; Sorrentino, S.; Manzari, C.; Chiara, M.; Iacoviello, M.; Guaricci, A.I.; De Santis, D.; Musci, R.L.; La Spada, A.; et al. Targeted next-generation sequencing detects novel gene-phenotype associations and expands the mutational spectrum in cardiomyopathies. PLoS One 2017, 12, e0181842. [Google Scholar] [CrossRef]
- Merlo, M.; Porcari, A.; Pagura, L.; Cameli, M.; Vergaro, G.; Musumeci, B.; Biagini, E.; Canepa, M.; Crotti, L.; Imazio, M.; et al. A national survey on prevalence of possible echocardiographic red flags of amyloid cardiomyopathy in consecutive patients undergoing routine echocardiography: study design and patients characterization-the first insight from the AC-TIVE Study. Eur J Prev Cardiol 2021. [Google Scholar] [CrossRef]
- Ghanbari, F.; Joyce, T.; Lorenzoni, V.; Guaricci, A.I.; Pavon, A.G.; Fusini, L.; Andreini, D.; Rabbat, M.G.; Aquaro, G.D.; Abete, R.; et al. AI Cardiac MRI Scar Analysis Aids Prediction of Major Arrhythmic Events in the Multicenter DERIVATE Registry. Radiology 2023, 307, e222239. [Google Scholar] [CrossRef]
- Baggiano, A.; Del Torto, A.; Guglielmo, M.; Muscogiuri, G.; Fusini, L.; Babbaro, M.; Collevecchio, A.; Mollace, R.; Scafuri, S.; Mushtaq, S.; et al. Role of CMR Mapping Techniques in Cardiac Hypertrophic Phenotype. Diagnostics (Basel) 2020, 10. [Google Scholar] [CrossRef]
- Mushtaq, S.; Chiesa, M.; Novelli, V.; Sommariva, E.; Biondi, M.L.; Manzoni, M.; Florio, A.; Lampus, M.L.; Avallone, C.; Zocchi, C.; et al. Role of advanced CMR features in identifying a positive genotype of hypertrophic cardiomyopathy. Int J Cardiol 2024, 417, 132554. [Google Scholar] [CrossRef]
- Pagura, L.; Porcari, A.; Cameli, M.; Biagini, E.; Canepa, M.; Crotti, L.; Imazio, M.; Forleo, C.; Pavasini, R.; Limongelli, G.; et al. ECG/echo indexes in the diagnostic approach to amyloid cardiomyopathy: A head-to-head comparison from the AC-TIVE study. Eur J Intern Med 2023. [Google Scholar] [CrossRef]
- Carrabba, N.; Amico, M.A.; Guaricci, A.I.; Carella, M.C.; Maestrini, V.; Monosilio, S.; Pedrotti, P.; Ricci, F.; Monti, L.; Figliozzi, S.; et al. CMR Mapping: The 4th-Era Revolution in Cardiac Imaging. J Clin Med 2024, 13. [Google Scholar] [CrossRef] [PubMed]
- Dicorato, M.M.; Basile, P.; Muscogiuri, G.; Carella, M.C.; Naccarati, M.L.; Dentamaro, I.; Guglielmo, M.; Baggiano, A.; Mushtaq, S.; Fusini, L.; et al. Novel Insights into Non-Invasive Diagnostic Techniques for Cardiac Amyloidosis: A Critical Review. Diagnostics (Basel) 2024, 14. [Google Scholar] [CrossRef] [PubMed]
- Carella, M.C.; Forleo, C.; Caretto, P.; Naccarati, M.L.; Dentamaro, I.; Dicorato, M.M.; Basile, P.; Carulli, E.; Latorre, M.D.; Baggiano, A.; et al. Overcoming Resistance in Anderson-Fabry Disease: Current Therapeutic Challenges and Future Perspectives. J Clin Med 2024, 13. [Google Scholar] [CrossRef]
- Prondzynski, M.; Mearini, G.; Carrier, L. Gene therapy strategies in the treatment of hypertrophic cardiomyopathy. Pflugers Arch 2019, 471, 807–815. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.W.; Lumish, H.S.; Sewanan, L.R.; Shimada, Y.J.; Maurer, M.S.; Weiner, S.D.; Clerkin, K.J. Evolving Strategies for the Management of Obstructive Hypertrophic Cardiomyopathy. J Card Fail 2024, 30, 1136–1153. [Google Scholar] [CrossRef]
- Maron, B.J.; Desai, M.Y.; Nishimura, R.A.; Spirito, P.; Rakowski, H.; Towbin, J.A.; Dearani, J.A.; Rowin, E.J.; Maron, M.S.; Sherrid, M.V. Management of Hypertrophic Cardiomyopathy: JACC State-of-the-Art Review. J Am Coll Cardiol 2022, 79, 390–414. [Google Scholar] [CrossRef]
- Colan, S.D. Hypertrophic cardiomyopathy in childhood. Heart Fail Clin 2010, 6, 433–444. [Google Scholar] [CrossRef]
- Yoerger, D.M.; Weyman, A.E. Hypertrophic obstructive cardiomyopathy: mechanism of obstruction and response to therapy. Rev Cardiovasc Med 2003, 4, 199–215. [Google Scholar]
- Dybro, A.M.; Rasmussen, T.B.; Nielsen, R.R.; Andersen, M.J.; Jensen, M.K.; Poulsen, S.H. Randomized Trial of Metoprolol in Patients With Obstructive Hypertrophic Cardiomyopathy. J Am Coll Cardiol 2021, 78, 2505–2517. [Google Scholar] [CrossRef]
- Borlaug, B.A.; Omote, K. Beta-Blockers and Exercise Hemodynamics in Hypertrophic Cardiomyopathy. J Am Coll Cardiol 2022, 79, 1576–1578. [Google Scholar] [CrossRef]
- Rosing, D.R.; Idanpaan-Heikkila, U.; Maron, B.J.; Bonow, R.O.; Epstein, S.E. Use of calcium-channel blocking drugs in hypertrophic cardiomyopathy. Am J Cardiol 1985, 55, 185B–195B. [Google Scholar] [CrossRef] [PubMed]
- Maltes, S.; Lopes, L.R. New perspectives in the pharmacological treatment of hypertrophic cardiomyopathy. Rev Port Cardiol (Engl Ed) 2020, 39, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Maron, M.S.; Rowin, E.J.; Olivotto, I.; Casey, S.A.; Arretini, A.; Tomberli, B.; Garberich, R.F.; Link, M.S.; Chan, R.H.M.; Lesser, J.R.; et al. Contemporary Natural History and Management of Nonobstructive Hypertrophic Cardiomyopathy. J Am Coll Cardiol 2016, 67, 1399–1409. [Google Scholar] [CrossRef]
- Epstein, S.E.; Rosing, D.R. Verapamil: its potential for causing serious complications in patients with hypertrophic cardiomyopathy. Circulation 1981, 64, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Pinto, G.; Chiarito, M.; Puscas, T.; Bacher, A.; Donal, E.; Reant, P.; Condorelli, G.; Hagege, A.; Cardiology, R.w.g.o.t.F.S.o. Comparative Influences of Beta blockers and Verapamil on Cardiac Outcomes in Hypertrophic Cardiomyopathy. Am J Cardiol 2025, 235, 9–15. [Google Scholar] [CrossRef]
- Sanchez-Nadales, A.; Anampa-Guzman, A.; Khan, A. Disopyramide for Hypertrophic Cardiomyopathy. Cureus 2019, 11, e4526. [Google Scholar] [CrossRef]
- Verlinden, N.J.; Coons, J.C. Disopyramide for Hypertrophic Cardiomyopathy: A Pragmatic Reappraisal of an Old Drug. Pharmacotherapy 2015, 35, 1164–1172. [Google Scholar] [CrossRef]
- Sherrid, M.V.; Massera, D. Disopyramide for symptomatic obstructive hypertrophic cardiomyopathy. Int J Cardiol 2025, 423, 133030. [Google Scholar] [CrossRef]
- Sherrid, M.V.; Barac, I.; McKenna, W.J.; Elliott, P.M.; Dickie, S.; Chojnowska, L.; Casey, S.; Maron, B.J. Multicenter study of the efficacy and safety of disopyramide in obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol 2005, 45, 1251–1258. [Google Scholar] [CrossRef]
- Sherrid, M.V.; Shetty, A.; Winson, G.; Kim, B.; Musat, D.; Alviar, C.L.; Homel, P.; Balaram, S.K.; Swistel, D.G. Treatment of obstructive hypertrophic cardiomyopathy symptoms and gradient resistant to first-line therapy with beta-blockade or verapamil. Circ Heart Fail 2013, 6, 694–702. [Google Scholar] [CrossRef]
- Hamada, M.; Ikeda, S.; Shigematsu, Y. Advances in medical treatment of hypertrophic cardiomyopathy. J Cardiol 2014, 64, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Maurizi, N.; Chiriatti, C.; Fumagalli, C.; Targetti, M.; Passantino, S.; Antiochos, P.; Skalidis, I.; Chiti, C.; Biagioni, G.; Tomberli, A.; et al. Real-World Use and Predictors of Response to Disopyramide in Patients with Obstructive Hypertrophic Cardiomyopathy. J Clin Med 2023, 12. [Google Scholar] [CrossRef]
- Forleo, C.; Carella, M.C.; Basile, P.; Mandunzio, D.; Greco, G.; Napoli, G.; Carulli, E.; Dicorato, M.M.; Dentamaro, I.; Santobuono, V.E.; et al. The Role of Magnetic Resonance Imaging in Cardiomyopathies in the Light of New Guidelines: A Focus on Tissue Mapping. J Clin Med 2024, 13. [Google Scholar] [CrossRef] [PubMed]
- Masri, A.; Lester, S.J.; Stendahl, J.C.; Hegde, S.M.; Sehnert, A.J.; Balaratnam, G.; Shah, A.; Fox, S.; Wang, A. Long-Term Safety and Efficacy of Mavacamten in Symptomatic Obstructive Hypertrophic Cardiomyopathy: Interim Results of the PIONEER-OLE Study. J Am Heart Assoc 2024, 13, e030607. [Google Scholar] [CrossRef] [PubMed]
- Olivotto, I.; Oreziak, A.; Barriales-Villa, R.; Abraham, T.P.; Masri, A.; Garcia-Pavia, P.; Saberi, S.; Lakdawala, N.K.; Wheeler, M.T.; Owens, A.; et al. Mavacamten for treatment of symptomatic obstructive hypertrophic cardiomyopathy (EXPLORER-HCM): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2020, 396, 759–769. [Google Scholar] [CrossRef]
- Desai, M.Y.; Owens, A.; Wolski, K.; Geske, J.B.; Saberi, S.; Wang, A.; Sherrid, M.; Cremer, P.C.; Lakdawala, N.K.; Tower-Rader, A.; et al. Mavacamten in Patients With Hypertrophic Cardiomyopathy Referred for Septal Reduction: Week 56 Results From the VALOR-HCM Randomized Clinical Trial. JAMA Cardiol 2023, 8, 968–977. [Google Scholar] [CrossRef]
- Rader, F.; Oreziak, A.; Choudhury, L.; Saberi, S.; Fermin, D.; Wheeler, M.T.; Abraham, T.P.; Garcia-Pavia, P.; Zwas, D.R.; Masri, A.; et al. Mavacamten Treatment for Symptomatic Obstructive Hypertrophic Cardiomyopathy: Interim Results From the MAVA-LTE Study, EXPLORER-LTE Cohort. JACC Heart Fail 2024, 12, 164–177. [Google Scholar] [CrossRef]
- Wheeler, M.T.; Jacoby, D.; Elliott, P.M.; Saberi, S.; Hegde, S.M.; Lakdawala, N.K.; Myers, J.; Sehnert, A.J.; Edelberg, J.M.; Li, W.; et al. Effect of beta-blocker therapy on the response to mavacamten in patients with symptomatic obstructive hypertrophic cardiomyopathy. Eur J Heart Fail 2023, 25, 260–270. [Google Scholar] [CrossRef]
- Ismayl, M.; Abbasi, M.A.; Marar, R.; Geske, J.B.; Gersh, B.J.; Anavekar, N.S. Mavacamten Treatment for Hypertrophic Cardiomyopathy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Curr Probl Cardiol 2023, 48, 101429. [Google Scholar] [CrossRef]
- Bishev, D.; Fabara, S.; Loseke, I.; Alok, A.; Al-Ani, H.; Bazikian, Y. Efficacy and Safety of Mavacamten in the Treatment of Hypertrophic Cardiomyopathy: A Systematic Review. Heart Lung Circ 2023, 32, 1049–1056. [Google Scholar] [CrossRef]
- Ho, C.Y.; Mealiffe, M.E.; Bach, R.G.; Bhattacharya, M.; Choudhury, L.; Edelberg, J.M.; Hegde, S.M.; Jacoby, D.; Lakdawala, N.K.; Lester, S.J.; et al. Evaluation of Mavacamten in Symptomatic Patients With Nonobstructive Hypertrophic Cardiomyopathy. J Am Coll Cardiol 2020, 75, 2649–2660. [Google Scholar] [CrossRef]
- Maron, M.S.; Masri, A.; Choudhury, L.; Olivotto, I.; Saberi, S.; Wang, A.; Garcia-Pavia, P.; Lakdawala, N.K.; Nagueh, S.F.; Rader, F.; et al. Phase 2 Study of Aficamten in Patients With Obstructive Hypertrophic Cardiomyopathy. J Am Coll Cardiol 2023, 81, 34–45. [Google Scholar] [CrossRef]
- Owens, A.T.; Masri, A.; Abraham, T.P.; Choudhury, L.; Rader, F.; Symanski, J.D.; Turer, A.T.; Wong, T.C.; Tower-Rader, A.; Coats, C.J.; et al. Aficamten for Drug-Refractory Severe Obstructive Hypertrophic Cardiomyopathy in Patients Receiving Disopyramide: REDWOOD-HCM Cohort 3. J Card Fail 2023, 29, 1576–1582. [Google Scholar] [CrossRef]
- Maron, M.S.; Masri, A.; Nassif, M.E.; Barriales-Villa, R.; Abraham, T.P.; Arad, M.; Cardim, N.; Choudhury, L.; Claggett, B.; Coats, C.J.; et al. Impact of Aficamten on Disease and Symptom Burden in Obstructive Hypertrophic Cardiomyopathy: Results From SEQUOIA-HCM. J Am Coll Cardiol 2024, 84, 1821–1831. [Google Scholar] [CrossRef] [PubMed]
- Maron, M.S.; Masri, A.; Nassif, M.E.; Barriales-Villa, R.; Arad, M.; Cardim, N.; Choudhury, L.; Claggett, B.; Coats, C.J.; Dungen, H.D.; et al. Aficamten for Symptomatic Obstructive Hypertrophic Cardiomyopathy. N Engl J Med 2024, 390, 1849–1861. [Google Scholar] [CrossRef] [PubMed]
- Masri, A.; Cardoso, R.N.; Abraham, T.P.; Claggett, B.L.; Coats, C.J.; Hegde, S.M.; Kulac, I.J.; Lee, M.M.Y.; Maron, M.S.; Merkely, B.; et al. Effect of Aficamten on Cardiac Structure and Function in Obstructive Hypertrophic Cardiomyopathy: SEQUOIA-HCM CMR Substudy. J Am Coll Cardiol 2024, 84, 1806–1817. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Pavia, P.; Bilen, O.; Burroughs, M.; Costabel, J.P.; de Barros Correia, E.; Dybro, A.M.; Elliott, P.; Lakdawala, N.K.; Mann, A.; Nair, A.; et al. Aficamten vs Metoprolol for Obstructive Hypertrophic Cardiomyopathy: MAPLE-HCM Rationale, Study Design, and Baseline Characteristics. JACC Heart Fail 2025, 13, 346–357. [Google Scholar] [CrossRef]
- Maron, B.J.; Maron, M.S.; Semsarian, C. Genetics of hypertrophic cardiomyopathy after 20 years: clinical perspectives. J Am Coll Cardiol 2012, 60, 705–715. [Google Scholar] [CrossRef]
- Forleo, C.; Carella, M.C.; Basile, P.; Carulli, E.; Dadamo, M.L.; Amati, F.; Loizzi, F.; Sorrentino, S.; Dentamaro, I.; Dicorato, M.M.; et al. Missense and Non-Missense Lamin A/C Gene Mutations Are Similarly Associated with Major Arrhythmic Cardiac Events: A 20-Year Single-Centre Experience. Biomedicines 2024, 12. [Google Scholar] [CrossRef]
- Paratz, E.D.; Mundisugih, J.; Rowe, S.J.; Kizana, E.; Semsarian, C. Gene Therapy in Cardiology: Is a Cure for Hypertrophic Cardiomyopathy on the Horizon? Can J Cardiol 2024, 40, 777–788. [Google Scholar] [CrossRef]
- Ma, H.; Marti-Gutierrez, N.; Park, S.W.; Wu, J.; Lee, Y.; Suzuki, K.; Koski, A.; Ji, D.; Hayama, T.; Ahmed, R.; et al. Correction of a pathogenic gene mutation in human embryos. Nature 2017, 548, 413–419. [Google Scholar] [CrossRef]
- Chai, A.C.; Cui, M.; Chemello, F.; Li, H.; Chen, K.; Tan, W.; Atmanli, A.; McAnally, J.R.; Zhang, Y.; Xu, L.; et al. Base editing correction of hypertrophic cardiomyopathy in human cardiomyocytes and humanized mice. Nat Med 2023, 29, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Reichart, D.; Newby, G.A.; Wakimoto, H.; Lun, M.; Gorham, J.M.; Curran, J.J.; Raguram, A.; DeLaughter, D.M.; Conner, D.A.; Marsiglia, J.D.C.; et al. Efficient in vivo genome editing prevents hypertrophic cardiomyopathy in mice. Nat Med 2023, 29, 412–421. [Google Scholar] [CrossRef]
- Mearini, G.; Stimpel, D.; Geertz, B.; Weinberger, F.; Kramer, E.; Schlossarek, S.; Mourot-Filiatre, J.; Stoehr, A.; Dutsch, A.; Wijnker, P.J.; et al. Mybpc3 gene therapy for neonatal cardiomyopathy enables long-term disease prevention in mice. Nat Commun 2014, 5, 5515. [Google Scholar] [CrossRef]
- Jiang, J.; Wakimoto, H.; Seidman, J.G.; Seidman, C.E. Allele-specific silencing of mutant Myh6 transcripts in mice suppresses hypertrophic cardiomyopathy. Science 2013, 342, 111–114. [Google Scholar] [CrossRef]
- Helms, A.S.; Thompson, A.D.; Day, S.M. Translation of New and Emerging Therapies for Genetic Cardiomyopathies. JACC Basic Transl Sci 2022, 7, 70–83. [Google Scholar] [CrossRef] [PubMed]
- Jaski, B.E.; Jessup, M.L.; Mancini, D.M.; Cappola, T.P.; Pauly, D.F.; Greenberg, B.; Borow, K.; Dittrich, H.; Zsebo, K.M.; Hajjar, R.J.; et al. Calcium upregulation by percutaneous administration of gene therapy in cardiac disease (CUPID Trial), a first-in-human phase 1/2 clinical trial. J Card Fail 2009, 15, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, B.; Butler, J.; Felker, G.M.; Ponikowski, P.; Voors, A.A.; Desai, A.S.; Barnard, D.; Bouchard, A.; Jaski, B.; Lyon, A.R.; et al. Calcium upregulation by percutaneous administration of gene therapy in patients with cardiac disease (CUPID 2): a randomised, multinational, double-blind, placebo-controlled, phase 2b trial. Lancet 2016, 387, 1178–1186. [Google Scholar] [CrossRef]
- Menon, S.C.; Ackerman, M.J.; Ommen, S.R.; Cabalka, A.K.; Hagler, D.J.; O'Leary, P.W.; Dearani, J.A.; Cetta, F.; Eidem, B.W. Impact of septal myectomy on left atrial volume and left ventricular diastolic filling patterns: an echocardiographic study of young patients with obstructive hypertrophic cardiomyopathy. J Am Soc Echocardiogr 2008, 21, 684–688. [Google Scholar] [CrossRef]
- Bytyci, I.; Nistri, S.; Morner, S.; Henein, M.Y. Alcohol Septal Ablation versus Septal Myectomy Treatment of Obstructive Hypertrophic Cardiomyopathy: A Systematic Review and Meta-Analysis. J Clin Med 2020, 9. [Google Scholar] [CrossRef]
- Karabulut, U.; Yilmaz Can, Y.; Duygu, E.; Karabulut, D.; Keskin, K.; Okay, T. Periprocedural, Short-Term, and Long-Term Outcomes of Alcohol Septal Ablation in Patients with Hypertrophic Obstructive Cardiomyopathy: A 20-Year Single-Center Experience. Anatol J Cardiol 2022, 26, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Kimmelstiel, C.; Rowin, E.J. Fixed, high-volume alcohol dose for septal ablation: High risk with no benefit. Catheter Cardiovasc Interv 2020, 95, 1219–1220. [Google Scholar] [CrossRef] [PubMed]
- Lawin, D.; Lawrenz, T.; Marx, K.; Danielsmeier, N.B.; Poudel, M.R.; Stellbrink, C. Gender disparities in alcohol septal ablation for hypertrophic obstructive cardiomyopathy. Heart 2022, 108, 1623–1628. [Google Scholar] [CrossRef]
- Sasahira, Y.; Yamada, R.; Doi, N.; Uemura, S. Urgent percutaneous transluminal septal myocardial ablation for left ventricular outflow tract obstruction exacerbated after surgical aortic valve replacement. Clin Case Rep 2021, 9, e04789. [Google Scholar] [CrossRef]
- Buchel, J.; Leibundgut, G.; Badertscher, P.; Kuhne, M.; Krisai, P. Radiofrequency ablation in obstructive hypertrophic cardiomyopathy: a case report. Eur Heart J Case Rep 2024, 8, ytae359. [Google Scholar] [CrossRef]
- Ommen, S.R.; Ho, C.Y.; Asif, I.M.; Balaji, S.; Burke, M.A.; Day, S.M.; Dearani, J.A.; Epps, K.C.; Evanovich, L.; Ferrari, V.A.; et al. 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR Guideline for the Management of Hypertrophic Cardiomyopathy: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2024, 149, e1239–e1311. [Google Scholar] [CrossRef] [PubMed]
- da Silva Menezes Junior, A.; de Oliveira, A.L.V.; Maia, T.A.; Botelho, S.M. A Narrative Review of Emerging Therapies for Hypertrophic Obstructive Cardiomyopathy. Curr Cardiol Rev 2023, 19, e240323214927. [Google Scholar] [CrossRef]
- Maron, B.J.; Rowin, E.J.; Maron, M.S. Evolution of risk stratification and sudden death prevention in hypertrophic cardiomyopathy: Twenty years with the implantable cardioverter-defibrillator. Heart Rhythm 2021, 18, 1012–1023. [Google Scholar] [CrossRef]
- Ullah, W.; Warner, E.; Khandait, H.; Sachdeva, S.; Abdalla, A.S.; Shafique, M.; Khan, M.A.; Roomi, S.; Khattak, F.; Alraies, M.C. Septal Myectomy or Alcohol Ablation for Hypertrophic Cardiomyopathy: A Nationwide Inpatient Sample (NIS) Database Analysis. Cardiovasc Revasc Med 2023, 50, 54–58. [Google Scholar] [CrossRef]
- Afanasyev, A.V.; Bogachev-Prokophiev, A.V.; Zheleznev, S.I.; Zalesov, A.S.; Budagaev, S.A.; Shajahmetova, S.V.; Nazarov, V.M.; Demin, II; Sharifulin, R.M.; Pivkin, A.N.; et al. Early post-septal myectomy outcomes for hypertrophic obstructive cardiomyopathy. Asian Cardiovasc Thorac Ann 2022, 30, 74–83. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Shimoda, T.; Shimada, Y.J.; Shimamura, J.; Akita, K.; Yasuda, R.; Takayama, H.; Kuno, T. Alcohol septal ablation versus surgical septal myectomy of obstructive hypertrophic cardiomyopathy: systematic review and meta-analysis. Eur J Cardiothorac Surg 2023, 63. [Google Scholar] [CrossRef] [PubMed]
- Morrow, A.G.; Reitz, B.A.; Epstein, S.E.; Henry, W.L.; Conkle, D.M.; Itscoitz, S.B.; Redwood, D.R. Operative treatment in hypertrophic subaortic stenosis. Techniques, and the results of pre and postoperative assessments in 83 patients. Circulation 1975, 52, 88–102. [Google Scholar] [CrossRef]
- Tan, T.; Zhu, W.; Ma, J.; Fu, B.; Zeng, X.; Wang, R.; Li, X.; Liu, J.; Zhuang, J.; Chen, J.; et al. Clinical Effect of the Modified Morrow Septal Myectomy Procedure for Biventricular Hypertrophic Cardiomyopathy. Rev Cardiovasc Med 2024, 25, 21. [Google Scholar] [CrossRef]
- Stefano, P.; Argiro, A.; Bacchi, B.; Iannone, L.; Bertini, A.; Zampieri, M.; Cerillo, A.; Olivotto, I. Does a standard myectomy exist for obstructive hypertrophic cardiomyopathy? From the Morrow variations to precision surgery. Int J Cardiol 2023, 371, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.; Guo, H.; Li, J.; Dai, J.; Ren, C.; Wang, Y. Comparison of surgical results in patients with hypertrophic obstructive cardiomyopathy after classic or modified morrow septal myectomy. Medicine (Baltimore) 2017, 96, e9371. [Google Scholar] [CrossRef] [PubMed]
- Reis, R.L.; Hannah, H., 3rd; Carley, J.E.; Pugh, D.M. Surgical treatment of idiopathic hypertrophic subaortic stenosis (IHSS). Postoperative results in 30 patients following ventricular septal myotomy and myectomy (Morrow procedure). Circulation 1977, 56, II128–132. [Google Scholar]
- Quinones, J.A.; DeLeon, S.Y.; Vitullo, D.A.; Hofstra, J.; Cziperle, D.J.; Shenoy, K.P.; Bell, T.J.; Fisher, E.A. Regression of hypertrophic cardiomyopathy after modified Konno procedure. Ann Thorac Surg 1995, 60, 1250–1254. [Google Scholar] [CrossRef]
- Laredo, M.; Khraiche, D.; Raisky, O.; Gaudin, R.; Bajolle, F.; Maltret, A.; Chevret, S.; Bonnet, D.; Vouhe, P.R. Long-term results of the modified Konno procedure in high-risk children with obstructive hypertrophic cardiomyopathy. J Thorac Cardiovasc Surg 2018, 156, 2285–2294. [Google Scholar] [CrossRef]
- Nguyen, S.N.; Chung, M.M.; Vinogradsky, A.V.; Richmond, M.E.; Zuckerman, W.A.; Goldstone, A.B.; Bacha, E.A. Long-term outcomes of surgery for obstructive hypertrophic cardiomyopathy in a pediatric cohort. JTCVS Open 2023, 16, 726–738. [Google Scholar] [CrossRef]
- Kunkala, M.R.; Schaff, H.V.; Nishimura, R.A.; Abel, M.D.; Sorajja, P.; Dearani, J.A.; Ommen, S.R. Transapical approach to myectomy for midventricular obstruction in hypertrophic cardiomyopathy. Ann Thorac Surg 2013, 96, 564–570. [Google Scholar] [CrossRef]
- Sun, D.; Schaff, H.V.; Nishimura, R.A.; Geske, J.B.; Dearani, J.A.; Ommen, S.R. Transapical Septal Myectomy for Hypertrophic Cardiomyopathy With Midventricular Obstruction. Ann Thorac Surg 2021, 111, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Wehman, B.; Ghoreishi, M.; Foster, N.; Wang, L.; D'Ambra, M.N.; Maassel, N.; Maghami, S.; Quinn, R.; Dawood, M.; Fisher, S.; et al. Transmitral Septal Myectomy for Hypertrophic Obstructive Cardiomyopathy. Ann Thorac Surg 2018, 105, 1102–1108. [Google Scholar] [CrossRef]
- Sakaguchi, T.; Totsugawa, T.; Tamura, K.; Hiraoka, A.; Chikazawa, G.; Yoshitaka, H. Minimally invasive trans-mitral septal myectomy for diffuse-type hypertrophic obstructive cardiomyopathy. Gen Thorac Cardiovasc Surg 2018, 66, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhu, K.; Wang, F.; Yang, Z.; Yang, S.; Wang, C. Enlargement of left ventricular outflow tract using an autologous pericardial patch for anterior mitral valve leaflet and septal myectomy through trans-mitral approach for the treatment of hypertrophic obstructive cardiomyopathy. J Card Surg 2021, 36, 4198–4202. [Google Scholar] [CrossRef]
- Massera, D.; Xia, Y.; Li, B.; Riedy, K.; Swistel, D.G.; Sherrid, M.V. Mitral annular calcification in hypertrophic cardiomyopathy. Int J Cardiol 2022, 349, 83–89. [Google Scholar] [CrossRef]
- Wu, Z.; Nie, C.; Zhu, C.; Meng, Y.; Yang, Q.; Lu, T.; Lu, Z.; Liu, X.; Wang, S. Mitral annular calcification in obstructive hypertrophic cardiomyopathy: Incidence, risk factors, and prognostic value after myectomy. Int J Cardiol 2023, 391, 131266. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, H.; Seggewiss, H.; Gietzen, F.H.; Boekstegers, P.; Neuhaus, L.; Seipel, L. Catheter-based therapy for hypertrophic obstructive cardiomyopathy. First in-hospital outcome analysis of the German TASH Registry. Z Kardiol 2004, 93, 23–31. [Google Scholar] [CrossRef]
- Douglas, J.S., Jr. Current state of the roles of alcohol septal ablation and surgical myectomy in the treatment of hypertrophic obstructive cardiomyopathy. Cardiovasc Diagn Ther 2020, 10, 36–44. [Google Scholar] [CrossRef]
- O'Mahony, C.; Mohiddin, S.A.; Knight, C. Alcohol Septal Ablation for the Treatment of Hypertrophic Obstructive Cardiomyopathy. Interv Cardiol 2014, 9, 108–114. [Google Scholar] [CrossRef]
- Gragnano, F.; Pelliccia, F.; Guarnaccia, N.; Niccoli, G.; De Rosa, S.; Piccolo, R.; Moscarella, E.; Fabris, E.; Montone, R.A.; Cesaro, A.; et al. Alcohol Septal Ablation in Patients with Hypertrophic Obstructive Cardiomyopathy: A Contemporary Perspective. J Clin Med 2023, 12. [Google Scholar] [CrossRef]
- Bataiosu, D.R.; Rakowski, H. Septal Reduction Strategies in Hypertrophic Cardiomyopathy-The Scalpel, Catheter, or Wire? JAMA Cardiol 2022, 7, 538–539. [Google Scholar] [CrossRef] [PubMed]
- Bode, M.F.; Ahmed, A.A.; Baron, S.J.; Labib, S.B.; Gadey, G. The use of MitraClip to prevent posttranscatheter aortic valve replacement left ventricular "suicide". Catheter Cardiovasc Interv 2021, 97, 369–372. [Google Scholar] [CrossRef] [PubMed]
- Veselka, J.; Faber, L.; Liebregts, M.; Cooper, R.; Januska, J.; Kashtanov, M.; Dabrowski, M.; Hansen, P.R.; Seggewiss, H.; Bonaventura, J.; et al. Alcohol dose in septal ablation for hypertrophic obstructive cardiomyopathy. Int J Cardiol 2021, 333, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Raimondo, C.; Balsam, P. Alternative Management Options for Hypertrophic Cardiomyopathy: Feasible? JACC Case Rep 2020, 2, 389–391. [Google Scholar] [CrossRef]
- Okutucu, S.; Aytemir, K.; Oto, A. Glue septal ablation: A promising alternative to alcohol septal ablation. JRSM Cardiovasc Dis 2016, 5, 2048004016636313. [Google Scholar] [CrossRef]
- Iacob, M.; Pinte, F.; Tintoiu, I.; Cotuna, L.; Caroescu, M.; Popa, A.; Cristian, G.; Goleanu, V.; Greere, V.; Moscaliuc, I.; et al. Microcoil embolisation for ablation of septal hypertrophy in hypertrophic obstructive cardiomyopathy. Kardiol Pol 2004, 61, 350–355. [Google Scholar]
- Iacob, M.; Pinte, F.; Tintoiu, I.; Cotuna, L.; Coroescu, M.; Filip, S.; Popa, A.; Cristian, G.; Goleanu, V.; Greere, V.; et al. Microcoil embolization for ablation of septal hypertrophy in hypertrophic obstructive cardiomyopathy. EuroIntervention 2005, 1, 93–97. [Google Scholar] [CrossRef]
- Banthiya, S.; Check, L.; Atkins, J. Hypertrophic Cardiomyopathy as a Form of Heart Failure with Preserved Ejection Fraction: Diagnosis, Drugs, and Procedures. US Cardiol 2024, 18, e17. [Google Scholar] [CrossRef]
- Udelson, J.E.; Bonow, R.O.; O'Gara, P.T.; Maron, B.J.; Van Lingen, A.; Bacharach, S.L.; Epstein, S.E. Verapamil prevents silent myocardial perfusion abnormalities during exercise in asymptomatic patients with hypertrophic cardiomyopathy. Circulation 1989, 79, 1052–1060. [Google Scholar] [CrossRef]
- Ommen, S.R.; Mital, S.; Burke, M.A.; Day, S.M.; Deswal, A.; Elliott, P.; Evanovich, L.L.; Hung, J.; Joglar, J.A.; Kantor, P.; et al. 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients With Hypertrophic Cardiomyopathy: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2020, 142, e558–e631. [Google Scholar] [CrossRef]
- Basile, P.; Monitillo, F.; Santoro, D.; Falco, G.; Carella, M.C.; Khan, Y.; Moretti, A.; Santobuono, V.E.; Memeo, R.; Pontone, G.; et al. Impact on ventricular arrhythmic burden of SGLT2 inhibitors in patients with chronic heart failure evaluated with cardiac implantable electronic device monitoring. J Cardiol 2024. [Google Scholar] [CrossRef] [PubMed]
- Velicki, L.; Popovic, D.; Okwose, N.C.; Preveden, A.; Tesic, M.; Tafelmeier, M.; Charman, S.J.; Barlocco, F.; MacGowan, G.A.; Seferovic, P.M.; et al. Sacubitril/valsartan for the treatment of non-obstructive hypertrophic cardiomyopathy: An open label randomized controlled trial (SILICOFCM). Eur J Heart Fail 2024, 26, 1361–1368. [Google Scholar] [CrossRef]
- Shimada, Y.J.; Passeri, J.J.; Baggish, A.L.; O'Callaghan, C.; Lowry, P.A.; Yannekis, G.; Abbara, S.; Ghoshhajra, B.B.; Rothman, R.D.; Ho, C.Y.; et al. Effects of losartan on left ventricular hypertrophy and fibrosis in patients with nonobstructive hypertrophic cardiomyopathy. JACC Heart Fail 2013, 1, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Olivotto, I.; Ashley, E.A. INHERIT (INHibition of the renin angiotensin system in hypertrophic cardiomyopathy and the Effect on hypertrophy-a Randomised Intervention Trial with losartan). Glob Cardiol Sci Pract 2015, 2015, 7. [Google Scholar] [CrossRef]
- Ho, C.Y.; Day, S.M.; Axelsson, A.; Russell, M.W.; Zahka, K.; Lever, H.M.; Pereira, A.C.; Colan, S.D.; Margossian, R.; Murphy, A.M.; et al. Valsartan in early-stage hypertrophic cardiomyopathy: a randomized phase 2 trial. Nat Med 2021, 27, 1818–1824. [Google Scholar] [CrossRef]
- Coats, C.J.; Pavlou, M.; Watkinson, O.T.; Protonotarios, A.; Moss, L.; Hyland, R.; Rantell, K.; Pantazis, A.A.; Tome, M.; McKenna, W.J.; et al. Effect of Trimetazidine Dihydrochloride Therapy on Exercise Capacity in Patients With Nonobstructive Hypertrophic Cardiomyopathy: A Randomized Clinical Trial. JAMA Cardiol 2019, 4, 230–235. [Google Scholar] [CrossRef]
- Olivotto, I.; Camici, P.G.; Merlini, P.A.; Rapezzi, C.; Patten, M.; Climent, V.; Sinagra, G.; Tomberli, B.; Marin, F.; Ehlermann, P.; et al. Efficacy of Ranolazine in Patients With Symptomatic Hypertrophic Cardiomyopathy: The RESTYLE-HCM Randomized, Double-Blind, Placebo-Controlled Study. Circ Heart Fail 2018, 11, e004124. [Google Scholar] [CrossRef] [PubMed]
- Sherrid, M.V. Drug Therapy for Hypertrophic Cardiomypathy: Physiology and Practice. Curr Cardiol Rev 2016, 12, 52–65. [Google Scholar] [CrossRef]
- Iavarone, M.; Monda, E.; Vritz, O.; Calila Albert, D.; Rubino, M.; Verrillo, F.; Caiazza, M.; Lioncino, M.; Amodio, F.; Guarnaccia, N.; et al. Medical treatment of patients with hypertrophic cardiomyopathy: An overview of current and emerging therapy. Arch Cardiovasc Dis 2022, 115, 529–537. [Google Scholar] [CrossRef]
- Dicorato, M.M.; Basile, P.; Naccarati, M.L.; Carella, M.C.; Dentamaro, I.; Falagario, A.; Cicco, S.; Forleo, C.; Guaricci, A.I.; Ciccone, M.M.; et al. Predicting New-Onset Atrial Fibrillation in Hypertrophic Cardiomyopathy: A Review. J Clin Med 2025, 14. [Google Scholar] [CrossRef]
- Garg, L.; Gupta, M.; Sabzwari, S.R.A.; Agrawal, S.; Agarwal, M.; Nazir, T.; Gordon, J.; Bozorgnia, B.; Martinez, M.W. Atrial fibrillation in hypertrophic cardiomyopathy: prevalence, clinical impact, and management. Heart Fail Rev 2019, 24, 189–197. [Google Scholar] [CrossRef]
- Oliveri, F.; Pepe, A.; Bongiorno, A.; Fasolino, A.; Gentile, F.R.; Schirinzi, S.; Colombo, D.; Breviario, F.; Greco, A.; Turco, A.; et al. Hypertrophic Cardiomyopathy and Atrial Fibrillation: A Systematic Review and Meta-analysis of Anticoagulation Strategy. Am J Cardiovasc Drugs 2023, 23, 269–276. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
mechanism of action of the main studied drugs used in the management of hypertrophic cardiomyopathy.
Figure 1.
mechanism of action of the main studied drugs used in the management of hypertrophic cardiomyopathy.
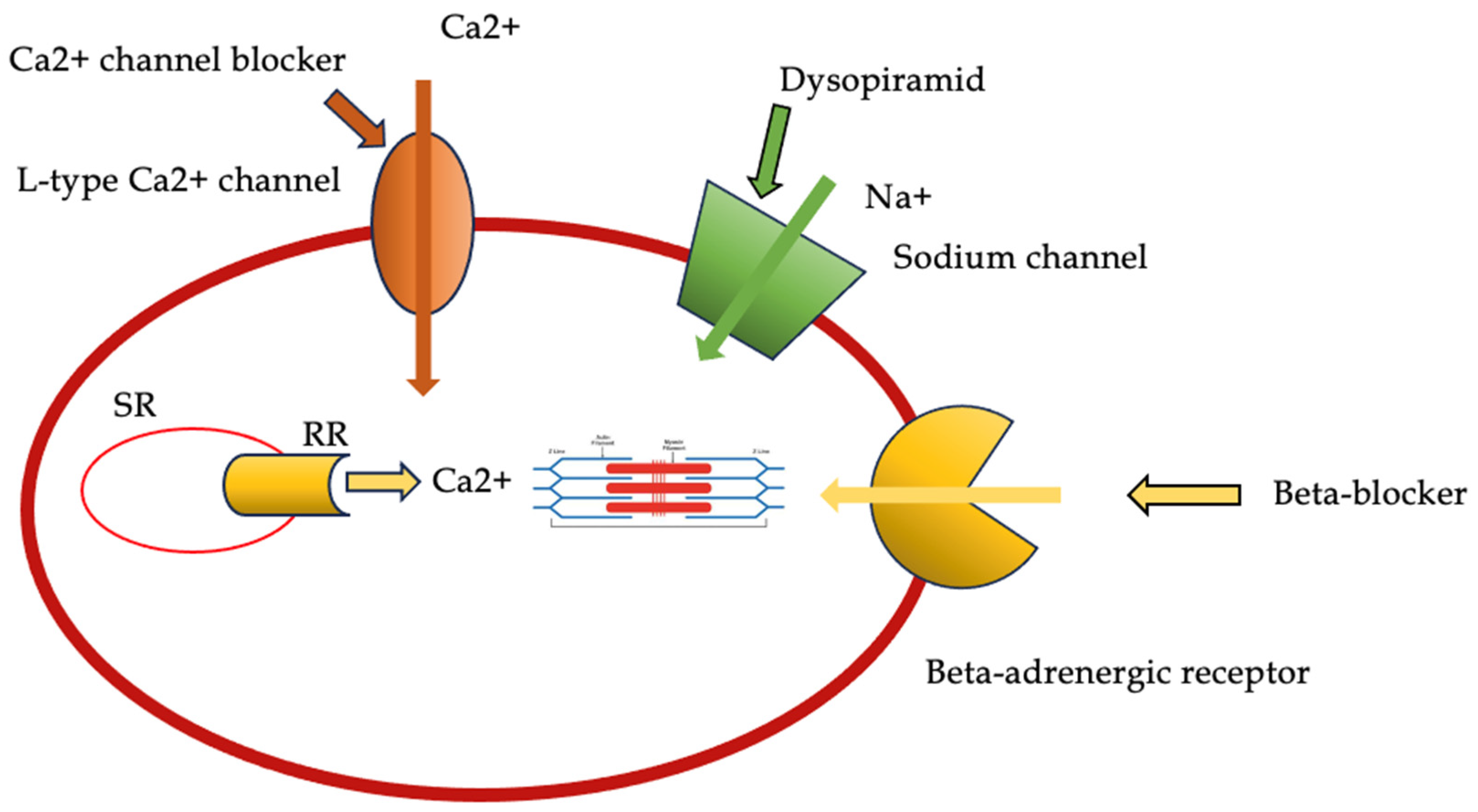
Figure 2.
Representation of the mechanism of action of cardiac myosin ATPase inhibitors.
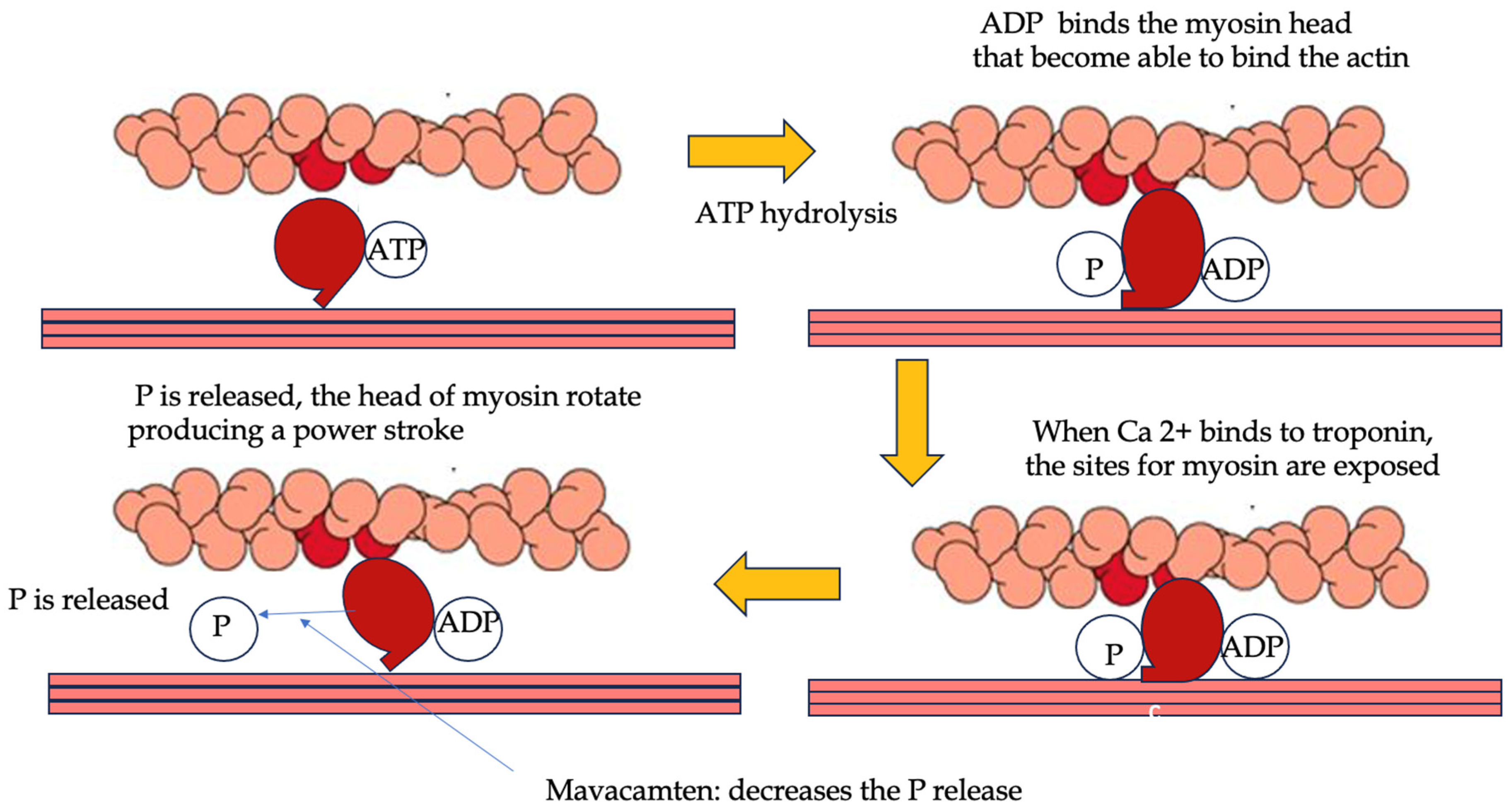
Figure 3.
Different gene therapy approaches for hypertrophic cardiomyopathy.
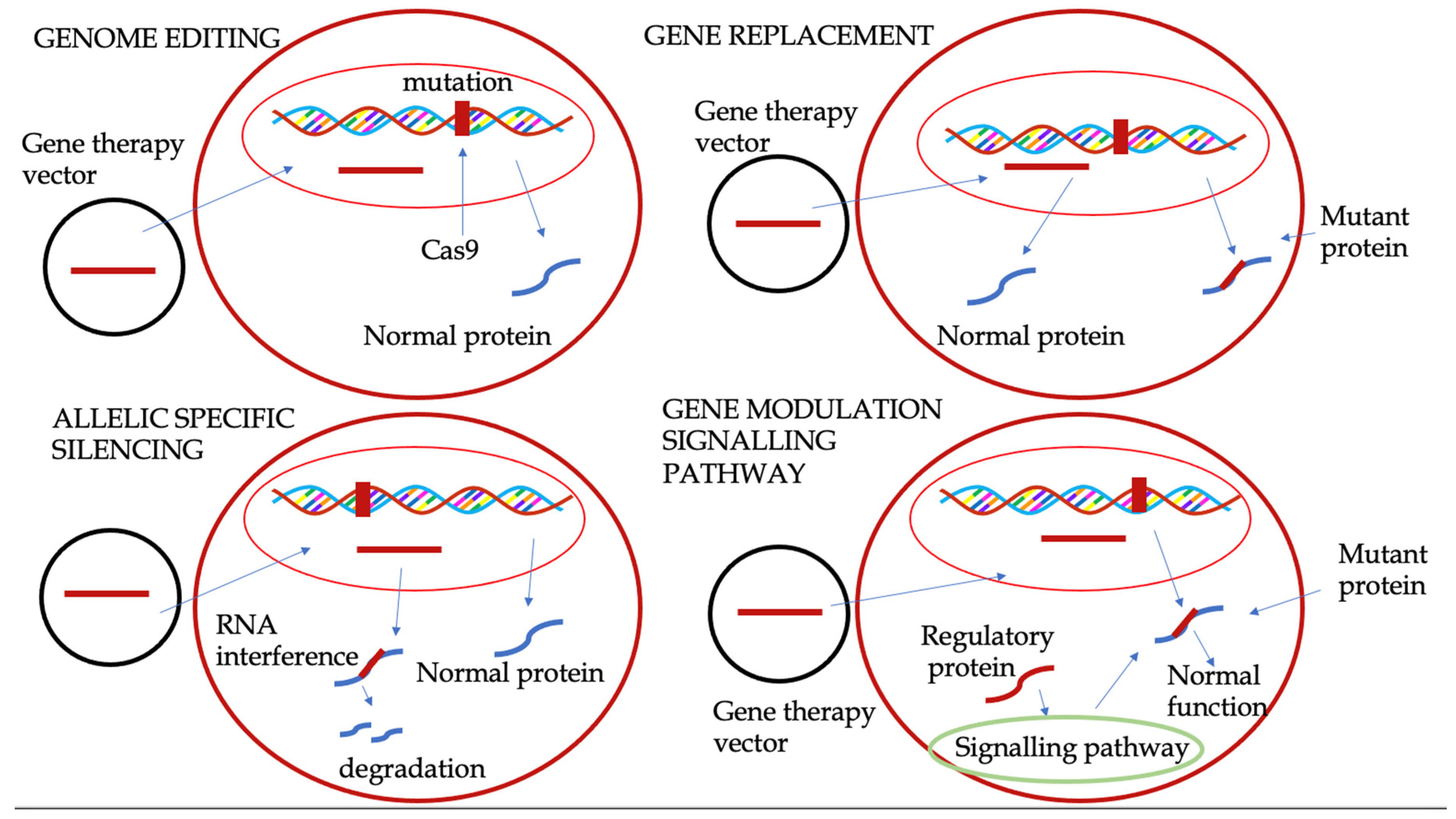
Figure 4.
Surgical approach used in hypertrophic cardiomyopathy. 4A. The hydrodynamic drag forces, in conjunction with the Venturi effect, result in the occurrence of SAM in OHCM. 4B. The classic Morrow procedure entails the resection of relatively small muscle tissue sections in the proximal ventricular septum, thereby widening the LVOT. However, this procedure does not alter the orientation of resistance forces, resulting in the persistence of SAM. 4C. The modified Morrow procedure involves extending the classic incision with a midventricular resection, which results in the widening of the LVOT and a concomitant alteration in the orientation of forces, leading to the dissolution of SAM. 4D. The LVOT is enlarged using an autologous pericardial patch for the anterior MV leaflet. OHCM: obstructive hypertrophic cardiomyopathy; SAM: systolic anterior motion; LVOTO: left ventricular outflow tract obstruction; LVOT: left ventricular outflow tract; MV: mitral valve.
Figure 4.
Surgical approach used in hypertrophic cardiomyopathy. 4A. The hydrodynamic drag forces, in conjunction with the Venturi effect, result in the occurrence of SAM in OHCM. 4B. The classic Morrow procedure entails the resection of relatively small muscle tissue sections in the proximal ventricular septum, thereby widening the LVOT. However, this procedure does not alter the orientation of resistance forces, resulting in the persistence of SAM. 4C. The modified Morrow procedure involves extending the classic incision with a midventricular resection, which results in the widening of the LVOT and a concomitant alteration in the orientation of forces, leading to the dissolution of SAM. 4D. The LVOT is enlarged using an autologous pericardial patch for the anterior MV leaflet. OHCM: obstructive hypertrophic cardiomyopathy; SAM: systolic anterior motion; LVOTO: left ventricular outflow tract obstruction; LVOT: left ventricular outflow tract; MV: mitral valve.
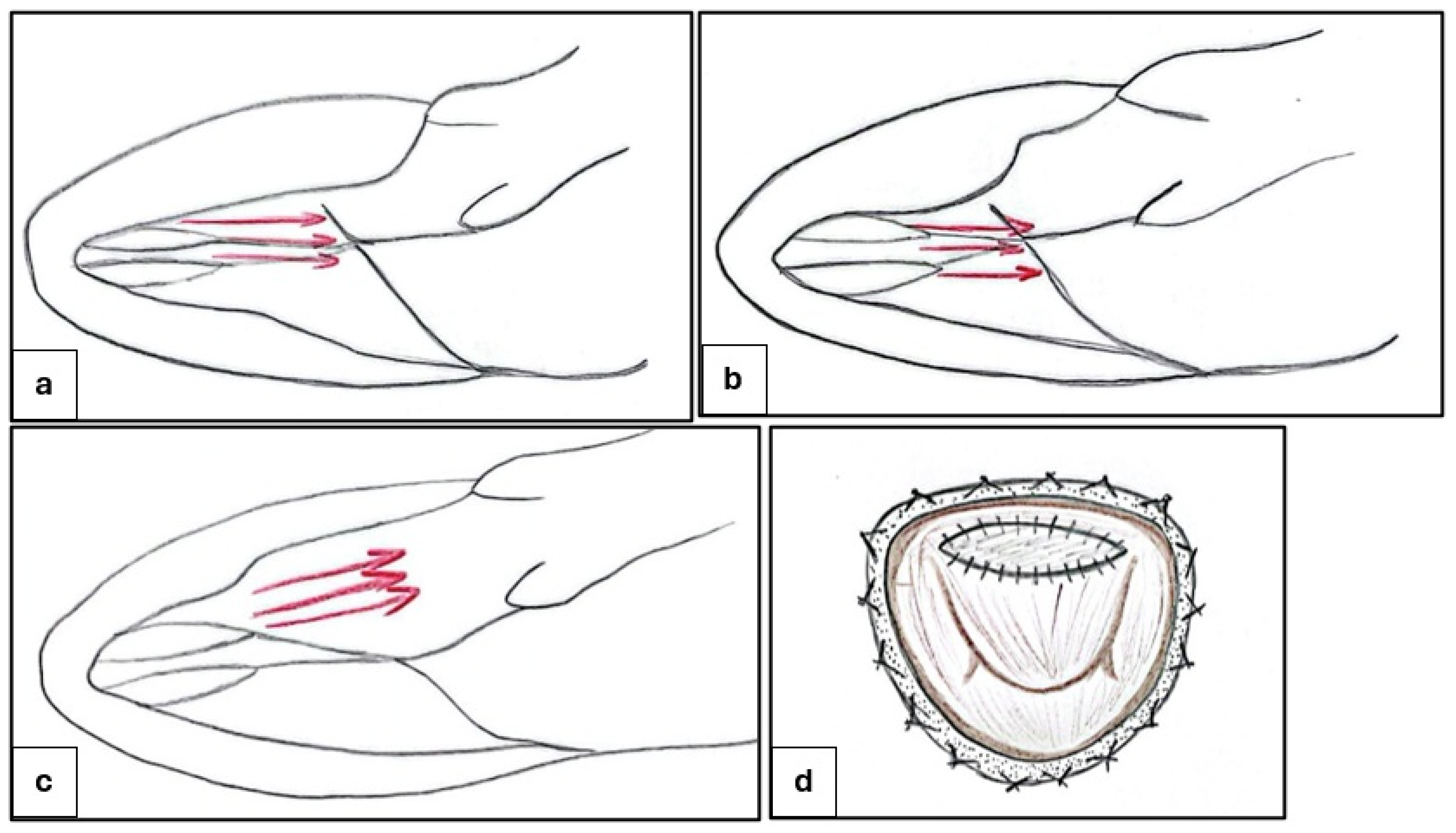
Figure 5.
Management of patients with non-obstructive hypertrophic cardiomyopathy.
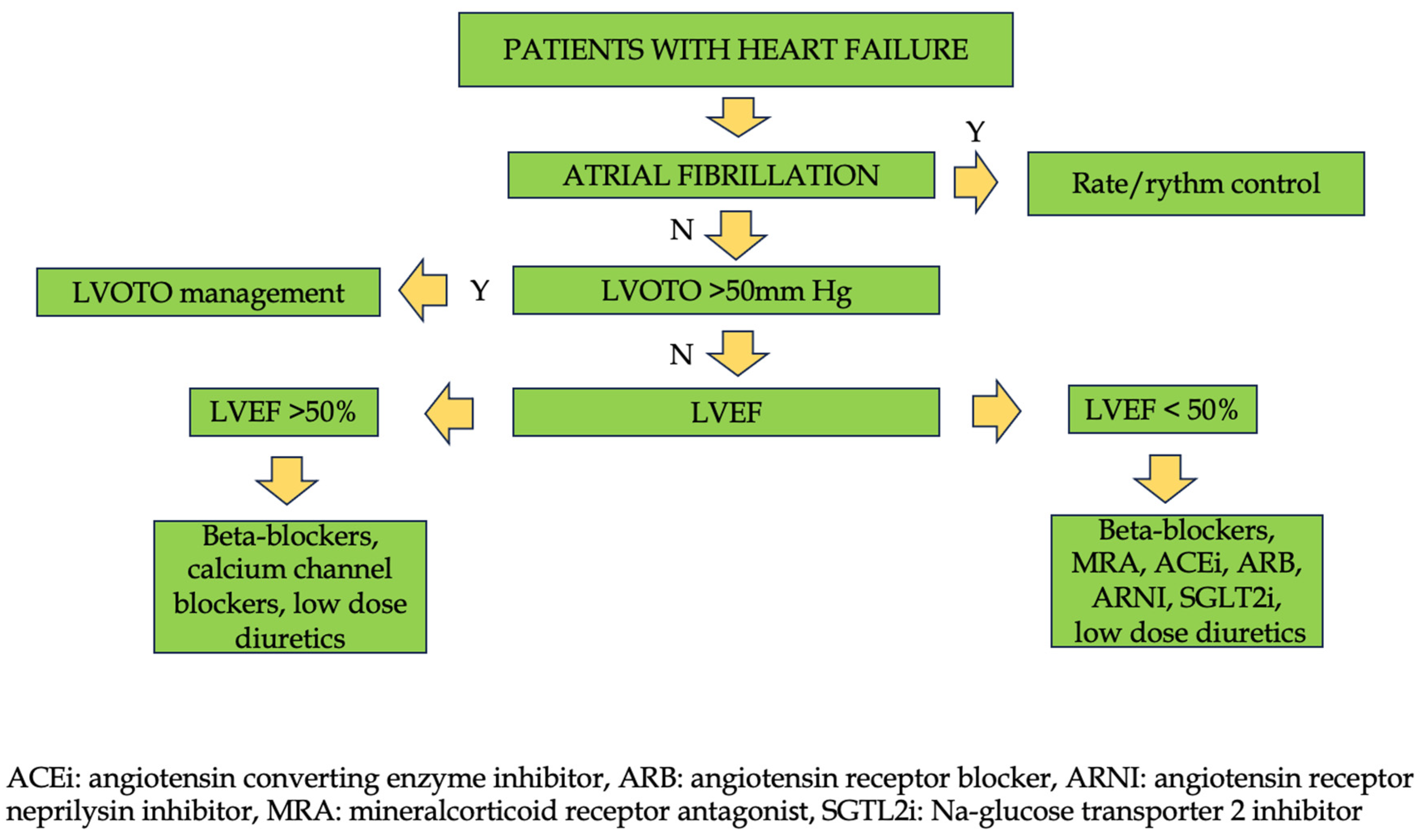

Table 1.
clinical properties of the main drugs used in the management of obstructive hypertrophic cardiomyopathy.
Table 1.
clinical properties of the main drugs used in the management of obstructive hypertrophic cardiomyopathy.
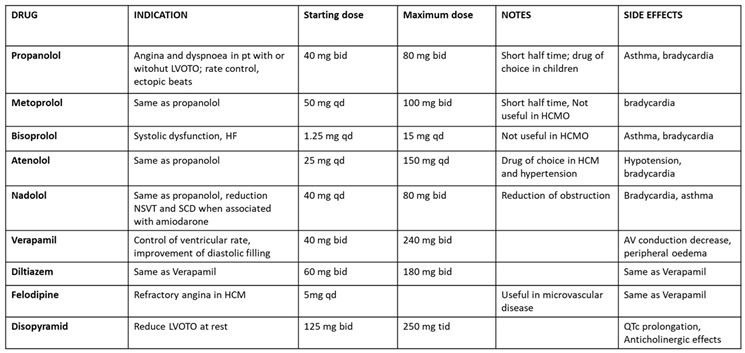 |
Table 2.
Main drugs used in the management of atrial fibrillation in hypertrophic cardiomyopathy.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



