Submitted:
23 May 2025
Posted:
26 May 2025
Read the latest preprint version here
Abstract
Background: Cigarette smoking remains a leading cause of death and illness in the US and globally. Electronic cigarettes (ECs) were introduced as a potentially less harmful alternative and are now used by approximately 20 million American adults. How scientific studies on ECs are reported can significantly influence perceptions of adults who smoke who might consider alternative products.A 2024 non peer-reviewed study by Medstar Health researchers who analyzed data from the All of Us NIH database found a 19% increased risk of heart failure (HF) among ever-users of ECs. This finding was announced by the American College of Cardiology (ACC) in a press release, and was reported on by over 30 news organizations in the US and England. Methods: This analysis investigated the translation frequency of Medstar study-related data across four stages: the original database, the researchers' analysis, the press release issued, and subsequent news media coverage. Instances of material omissions, unsupported claims, and confirmation bias throughout the dissemination process were identified and discussed. Results: The analytic sample (n=1,280) represented coverage (or omission) of material scientific content items (n=40) present in the abstract, poster and/or press release by general news sites (n=17) and science news sites (n=15). News reports on average, republished over half of the content items present in the press release, with direct quotes repeated 75% of the time in general news sites and 68% of the time in science news sites. Strikingly, content present only in the study's abstract and/or poster, but absent from the press release, was omitted by all general news sites and the majority of science news sites. Critical omissions included that exclusive EC use was not associated with a significant increase in HF, and the impact of combusted cigarette (CC) smoking in dual-users was discounted as having a minimal association with HF. These details were absent in the press release, as well as in almost all subsequent news reports. 94% of general news sites and 80% of science news sites didn’t mention that the study had not yet been peer-reviewed. Conclusion / Implications: The accuracy and precision of news reporting on the Medstar study could have been substantially improved if the press release had been clearer about the contradictions and limitations of the study findings, and if news outlets had thoroughly examined and reported the complete study findings, including the abstract and underlying data, rather than primarily transmitting quotations from the press release. This points to areas for improvement in science reporting quality, which could benefit public health literacy.
Keywords:
epidemiology
; public health
; e-cigarettes
; smoking
; news reporting
; harm reduction
Overview
On April 29, 2024, CBS News aired a health segment that stated “vaping, just once, could put you at risk of heart failure” (Figure 1). The claim stemmed from a study conducted by researchers at MedStar Health Baltimore and MedStar Georgetown University, presented at the American College of Cardiology (ACC) 74th Annual Meeting [1]. At first glance, the headline was alarming—an urgent warning to a public already believing that EC were equally or more dangerous than CC [2]. But a closer look reveals a more complex story: the study didn’t actually investigate the effects of vaping “just once.” Furthermore, key findings were omitted from the reporting of CBS and almost all of the 31 other news organizations which covered this story. These omissions included that the EC ever-use cohort smoked CC more than they vaped and 1.9x more than the EC non-use cohort, that smoking CC was modelled by the authors as having minimal impact—contrary to established research, and that vapers in the study population who didn’t smoke CC showed no significant effects on heart failure incidence. Revealingly, Fox News was explicit about confirmation bias in its reporting, stating “Let’s be honest here. It’s great news because sometimes we need to point to these studies to really hone this in on people” [3].
This case study examines how the MedStar study’s findings were communicated across four stages of translation: the underlying database, the primary analysis by the study authors, the ACC press release, and news media coverage (Figure 2). By tracing this chain, we can pinpoint where inaccuracies emerged and explore what fact-checking measures could have sharpened the precision and accuracy of the final reports. Cases of selective omission, ungrounded assertions, and expression of confirmation bias will be investigated.
Figure 3 illustrates the primary findings of this case study. On average, approximately half of the content which was included in the ACC press release was re-communicated in each subsequent news story. In particular, general news sites communicated 75% of press release direct quotations and 51% of non-quotation data items per news story. In contrast, material content which was not in the press release was completely omitted from all subsequent general news coverage and most science news coverage (0% and 13% inclusion frequency, respectively). The most salient omission, that vaping in never smokers was not associated with a significant increase in heart failure incidence, was mentioned in the initial abstract but then excluded in the poster and press release. Consequently, this result was omitted in all news reports, with the exception of Healio, which mentioned that HF incidence was attenuated in this population [5]. The Sun inaccurately asserted the opposite, that heart failure incidence was found in the study to significantly increase even in EC users who didn’t smoke [6].
Methods
The study by Bene-Alhasan et al., 2024 presented at ACC, was selected as a case study, because of its ubiquity and reach in the US and UK 2024 news cycles regarding the health impact of electronic cigarettes [1]. For the study itself, content which was generated in association with the ACC meeting was profiled; these included an abstract, poster presentation, and ACC-issued press release.[1,7] News reports were identified by searches on Google and Bing using keywords which included ([“electronic cigarette” OR “e-cig*” OR “vaping” OR “electronic nicotine”] OR [Bene-Alhasan OR Medstar]) AND “heart failure”), and combinations of subsets of these keywords, from a date of 4/1/2024 or later.
The press release was broken into contiguous sentences and phrases which represented the entirety of its content. Additional salient sentences and phrases which were present in the abstract and/or poster but not included in the press release were also identified. This matrix of (news reports) x (content) represented the analytic sample. Each news report was then scanned to capture the frequency of translation for each content element. In coverage of UK news sites, presentation of UK statistics on heart failure or tobacco use were counted as mirroring similar disclosures of US statistics in the Medstar / ACC content. A mention of the UK NHS supporting EC use for stopping smoking was not counted as evidence of mirroring the Medstar poster if the mention came in a section of the news report which was not discussing the Medstar study.
The lead author of the Medstar study was contacted four times with questions about the study over the course of a year, but did not respond. The lead author and the ACC were notified of the preprint on 4/28/25 and offered an opportunity to comment, but did not respond.
Stage I: The All Of Us Database was the Source of the Underlying Data
The underlying data analyzed by the Medstar team originated in the All of Us Research Program [8]. All of Us is a national multi-year database initiated in 2016, administered under the auspices of the National Institutes of Health (NIH). Participants are surveyed with questionnaires on demographics, lifestyle practices and health conditions, and for some participants, data can include electronic health records, blood samples, and digital health tracking.
The All of Us database measures CC use history comprehensively and precisely
The use of combusted cigarettes (CC) has been causally linked to subsequent cardiovascular disease. It has been shown that quantifying duration, timing and intensity of use are each important for precision and accuracy of assessment of risk associated with cigarette use; CC use-associated risk increases over years and decades of use and decreases over years after quitting [9].
The All of Us Lifestyle Questionnaire contains a sufficient dataset to precisely characterize exposure and associated cardiovascular risk for CC, but less precisely for EC (see Figure 4) [8].
At a minimum, pack-years of CC exposure are necessary for precision of the dose-response relationship between exposure and risk. For CC use, beyond generalized use status (current- former- and never-use) a comprehensive set of metrics are assessed by All of Us, including both current intensity of smoking as well as cumulative pack-year related data, and time started and stopped, for former smoking. As is typical for most studies, lifetime CC smoking of less than 100 times is classified as “never use.”
The All of Us database measures EC use history incompletely and imprecisely
In contrast to CC use, EC use is characterized in the All of Us database with a limited set of metrics indicative of current use status but not duration of use (see Figure 4). Subjects are classified based on current- former- or never-use. Current use is further sub-segmented into some-day and every-day use. Unlike CC use, duration of use or number of uses is not collected. In this respect, the All of Us study deviates from the PATH study, which does collect this more comprehensive information. The PATH study dataset, for instance, demonstrates that most adult ever-EC users and most current some-day users in their database had lifetime usage of fewer than 100 times (i.e., they would be classified as “never users” if assessed similarly to CC use) [9].
Stage II: The Medstar team studied a population of EC ever-users who smoked more than they vaped and found inconsistent results
The top-line finding was that heart failure incidence was 19% higher for EC ever-users vs. EC never-users, after adjusting for covariates.
The Medstar Health authors analyzed data from the All of Us database to assess the impact of EC exposure on heart failure (HF) risk. 175,667 adult participants were identified who had EC and CC usage data available, as well as subsequent medical electronic health records (EHR) tracking an average of 45 months (see Figure 5). These participants were segmented into two cohorts: 28,660 EC ever-users (n=28,660) and EC never-users (n=176,007). Participants with prior HF had been excluded, and 3,242 new HF diagnoses were reported in the EHR during the 45-month prospective health record period. In the raw data, the incidence of new diagnoses of heart failure were 36% lower in the EC ever-use group vs. the EC never-use group. After adjustments for covariates in the Medstar analysis, the final reported odds ratio was 19% higher in the EC ever-use group vs. the EC never-use group.
The Medstar authors incompletely characterized both CC and EC exposure
As shown in Figure 6, to characterize EC exposure, the authors tracked current usage status at a single time point (EC current-use, former-use, or never-use at the beginning of the prospective period; current-use was sub-segmented into every-day and some-day use). Duration of use or number of uses were not available in the All of Us data set and so were not tracked. To characterize CC exposure, the authors similarly captured current usage status at a single time point (CC current-use, former-use, or never-use.) Even though pack-year exposure and time quit data were available in the All of Us database, they were not utilized in the analysis. Lastly, CC and EC use were not tracked during the 45-month prospective period. In summary, duration of use was not tracked for CC as well as EC usage, therefore exposure quantification was incomplete and highly imprecise [9].
In the EC ever-use cohort, current smoking exceeded current vaping, and CC use was 1.9X higher than in the EC never-use cohort.
As previously mentioned, the All Of Us sample assessed by the Medstar authors were segmented into EC ever-users and never-users. In the EC ever-use group, prevalence of current smoking exceeded the prevalence of vaping (29% were CC current users vs. 26% current EC use). Furthermore, the CC smoking rate was 1.9x twice as high in the EC ever-use group vs. in the EC never use group (see Figure 7). Therefore, it was critical for the authors to disambiguate between the impact of smoking CC vs. vaping EC in these cohorts if they wished the results to be accurate.
In the raw data, EC users had 36% lower incidence of HF than non-EC users
As shown in Figure 5 and Table 1, the ~29k EC ever-users had 361 HF diagnoses, vs. 2,881 HF diagnoses for ~147k EC never-users, meaning that in the raw data the EC ever-use group had OR of 0.64 for HF relative to the EC never-use group.
In contrast to EC use, CC use was reported by the authors to contribute almost no HF risk, which is inconsistent with the literature
By definition, cross-sectional observational studies compare groups which are unbalanced, therefore odds ratios (OR) should be adjusted to balance out background differences in risk not associated with the exposure variable (EC use) [9]. The authors adjusted the relative risk of HF in the EC ever-use group vs. EC never-use group, from an unadjusted risk of 0.64, to an adjusted risk (aOR) of 1.19, in 3 sequential adjustment steps.
First, demographic factors were adjusted for, followed by smoking and substance use, and lastly by cardiovascular risk factors like diabetes and hypertension. When the authors adjusted for sociodemographic factors, such as a 14 year difference in ages between the EC use and non-use groups, the 0.64 OR was adjusted in a first model to aOR 1.19.
When a further adjustment for CC use was made (Model 2, see especially content highlighted in red), the aOR in a second, expanded, model was similar (1.17). In other words, the modeling approach which the authors used found that the almost doubling of prevalence of current and former CC use in the EC ever-use group was only associated with a 2% increase in HF risk. This result is highly inconsistent with the literature, which shows that CC use can cause a doubling or greater of cardiovascular risk [10,11].
Lastly, the EC ever-use group had lower rates of diabetes, hypertension, and hypercholesterolemia vs. the EC never-use group, therefore their HF adjusted odds ratio was increased to a final result of 1.19 to account for that imbalance between groups in their Model 3, which was the main (reported) model.
In summary, to account for imbalances, the OR were multiplied by adjustment factors which aggregated to a 190% adjustment to aOR 1.19, with a confidence interval of [1.04-1.34]. In other words, the authors asserted that their analysis of the impact of EC exposure was precise enough that its error was less than +/- 12.6%. This level of accuracy was asserted even though the characterization of CC and EC use was extremely incomplete and imprecise (pack-years of CC use were not reported, and duration of EC use was not tracked by the database). Based on comparable PATH study data, the current CC users likely had decades of CC use pack-years, while most of the vaping in the ever-use group was likely less than 100 lifetime uses [9].
The authors found no evidence for a dose-response association of EC use with HF and no effect in EC users who didn’t smoke CC
In the abstract, the authors mentioned that of the EC ever-users who didn’t smoke, there was no significant association with HF (aOR = 1.04 [0.57-1.89]) [7]. Furthermore, the authors reported that there was no difference seen between EC every-day and some-day current users (this was in contrast to an abstract published the previous year by these authors in which they reported an association of cannabis use with a 34% increase in HF incidence that was dependent on frequency of use) [12]. The authors did report that EC users who were also dual-users of CC had a 59% increase in HF incidence [13]. These results suggest that most or all of the risk in the EC ever-use group may have been due to CC smoking.
The authors reported a difference between two types of heart failure
The abstract and presentation indicated a difference in aOR for two types of heart failure, HFpEF (aOR 1.21 [1.01 - 1.47]) and HFrEF (aOR 1.11 [0.90-1.37]). The press release did not provide odds ratios, but highlighted that an association between EC use and HF was seen in one category of HF but not the other.
Stage III: The American College of Cardiology issued a press release days before the study was presented, which omitted key findings from the abstract and poster.
As shown in Table 2, an ACC press release was released in concert with a separate publication of the Medstar abstract on 4/2/24. A Medstar poster was presented five days after the press release, on 4/7/24.
The press release consisted of 24 key facts and quotations
As shown in Table 3 below, the press release, when segmented into contiguous sentences and phrases, contained 16 data points and 4 direct quotations and 5 indirect quotations summarizing the interpretation of the study authors. The abstract and poster contained at least 13 additional salient data points and two indirect quotations (conclusion statements).
Central information was omitted, modified, or obscured in the press release
The press release omitted or obscured mention of key caveats limiting the interpretability and generalizability of the results of the study, which were noted in the abstract and poster. A crucial omission was that the EC ever-use group smoked conventional cigarettes (CC) more than they vaped EC (29% current CC use versus 26% current EC use at the start of the 45-month study period). This EC ever-use group also smoked CC at 1.9 times the rate of the EC never-use group. Despite this substantial difference in CC use, the fully adjusted statistical model attributed only a 2% increase in HF risk attributable to this 1.9x difference. Furthermore, EC exclusive users (never smokers) showed a 4% increased risk that was not statistically significant. The press release also omitted the finding of a lack of a dose-response relationship, noting that there was no difference in HF incidence between everyday and some-day EC current users. These results call the central finding of the study into question.
Furthermore, the press release selectively highlighted a difference in aOR between two types of HF (1.21 vs. 1.11 respectively), suggesting that the study had the precision to identify a subtype of HF which was impacted by EC. However, it did not mention the larger and more salient difference in aOR between EC users who never smoked CC vs. those who did smoke CC (1.04 vs. 1.59, respectively).
Lastly, the more cautious conclusion of the poster, that “electronic nicotine product use should be discouraged among the youths while further studies are conducted” was replaced in the press release to a statement that EC are “not recommended for quitting smoking.”
Stage IV: The Medstar study was reported on by at least 17 general news sites and 15 science news sites. General news sites and most science news sites did not communicate salient data which was not in the press release.
Salient data and quotations which were not in the press release were omitted in all general news reports and most science news reports
The analytic sample for the current analysis represented (n=1280) data points, comprised of (n=40) possible content items per news report x (n=32) news reports. Of the (n=25) content items which were included in the ACC press release, on average, 51% were re-communicated in each general news site report (53% for science news sites; see Table 4 and Figure 3). In particular, general news sites on average communicated 75% of press release direct quotations, 31% of indirect quotations, and 51% of non-quotation data items per news story.
There were an additional (n=15) salient content items which were only included in the abstract and/or poster, and which were not included in the press release. This non press-release content was omitted in 100% of general news site reports. For science news sites, 13% of this content was included on average in each report. At the report level, 7 of the 15 science news sites included some content which was not in the press release, while 8 did not. In other words, data which was not in the press release was completely omitted from all subsequent general news coverage and the majority of science news coverage.
The most material omission, that vaping in never smokers was not associated with a significant increase in heart failure incidence, was mentioned in the initial abstract but then excluded in the poster and press release. Consequently, this result was omitted in all news reports, with the exception of Healio, which mentioned that HF incidence was attenuated in this population [5]. The Sun inaccurately asserted the opposite, that heart failure incidence was found in the study to significantly increase even in EC users who didn’t smoke [6].
Of positive note, 5 science news sites did include content which was only in the poster and not in the abstract or press release. This indicated an effort to review all the source materials, given that the poster data was the least easily accessible content. These sites included Health.com, Healthline, MedPage Today, ScienceAlert and TCTMD. [13,22,26,27,29] Healio and Patient Care referenced content which was in the abstract but not the press release, bringing the number of reports which cited content which was not in the press release to a total of 7. [5,17]
News site reporting included material omissions, unsupported claims, and acknowledgement of confirmation bias
As shown in Figure 8, omissions, unsupported claims, and acknowledgement of confirmation bias had multiple points of origination across the stages of information dissemination.
Material omissions centered on the HF impact of CC vs. EC use and appear to have originated from the study authors and/or ACC, as well as from news media not reporting on the abstract content
- Non-smoking EC users did not have a significant increase in heart failure incidence. As previously discussed, the press release and poster omitted this item which was only included in the abstract. Subsequently, all news reports but one omitted this finding, and one reported the opposite.
-
CC use was 1.9x higher in the EC use group, but CC use was surprisingly reported as having a minimal association with HF risk, calling the entire study into question. This data was omitted from the press release and most subsequent news reports.
- Medpage Today was the only site which reported that the EC group smoked CC 1.9X more than the non-EC group, and that the EC group smoked CC more than it vaped EC [13].
- Almost all news reports were not aware and/or did not question why the impact of the 1.9x difference in CC use was only a 2% increase in HF risk in the Medstar adjusted model. Two exceptions, reports by Health.com and Healthline, are discussed below.[22,26]
Unsupported claims / false conclusions were originated by news media and in one case repeated by another news report.
- 3.
-
Two news reports claimed that “vaping, even once, may raise the risk of heart failure. As discussed previously, the impact of a single use of EC product was not studied by the Medstar authors; moreover, the underlying All of Us database did not collect the duration of vaping (see Figure 5).
- Medical News Today originated this claim on 4/27/24 [32]. In an email communication, the Medical News Today author asserted that a statement in the ACC press release (“people who used e-cigarettes at any point had a 19% higher risk of heart failure”) validated their headline.
- This claim was then repeated two days later by CBS News [4].
- 4.
- The Sun reported “VAPING can damage your heart even if you have never smoked cigarettes, according to a study.” [6] As previously discussed, the Medstar authors in actuality reported the opposite, that there was no significant impact in the subset of EC users who didn’t use CC. However, this was disclosed only in the abstract and not the press release.
- 5.
- One news site reported that “one in five EC users went on to develop heart failure.” [24] This was likely a misunderstanding of the 19% increased adjusted risk of HF reported in the EC group (which was also correctly cited elsewhere in the news article). In actuality, 1.26% of EC ever-users were diagnosed with heart failure during the prospective period, vs. 1.96% of EC never-users in the unadjusted data.
One news report acknowledged confirmation bias
- 6.
- Dr. Nicotine Saphier, of Fox News, acknowledged, “This is not surprising… let’s be honest here. It’s great news because sometimes we need to point to these studies to really hone this in on people.” [3]
The news reports from Health.com and Healthline were the only 2 of 32 total studies which addressed the central question impacting the accuracy of the findings: what were the dose response relationships between smoking and vaping exposure and subsequent heart failure incidence, and to what level of precision were they accounted for in populations that used both products? Health.com cited a physician who said, “the supposed link between heart failure and e-cigarette use may, in reality, be an association between tobacco use and heart failure.” [26] Healthline likewise cited a physician who suggested that future studies should “look at the amount of e-cigarette use and the relative risk of heart failure with exposure levels. In comparison, the research that is currently available looked at a strict binary between those using these products and those who were not.”[22]
Some news reports did suggest caution in interpreting the results. One general news report (US News and World Report) and 3 science news reports (Science Alert, Healthline, and Medical News Today) identified that the Medstar study had not yet been peer-reviewed.[22,29,32] 29% of general news reports and 40% of science news reports noted that the study was observational, although this was usually caveated with the suggestion that one could infer likely causality due to the large size of the study and adjustments for covariates.
Multiple reports emphasized cause for alarm. The Times reported that the Medstar study was the “most conclusive evidence yet about potential harm of e-cigarettes.”[33] The Daily Mail announced a “shock study,” and Fox News likewise called the results “shocking.”[3,21] Forbes described a “threat”, and The Sun warned of a “deadly” risk.[6,14]
Physicians were cited in some of the news reports, and health care professionals, including physicians, pharmacists, and dentists, were the primary audience for many of the medical news sites. Several reports called for public health advisories based on the results of this study. Medical News Today interviewed the primary author of the Medstar study, a physician, who said, “doctors should make their patients aware of this association between e-cigarette use and increased heart failure risk…although more research is required, patients still need to know what we know about it now so they can make informed decisions.” Medical News Today also cited other physicians, who said, “this should really lead to more public outreach campaigns and public service announcements regarding the safety of e-cigarettes,” and, “this research (was) useful information to be able to share with patients, especially when trying to educate them about preventive measures for heart failure.”[32]
Discussion
Accurate scientific reporting on tobacco-related issues is critical for informing the public, including adults who smoke, clinical practice, and public health policy. This case study identified instances of omission, unsupported claims, and acknowledgement of confirmation bias in the course of dissemination of data from the underlying database to ultimate news reporting. The central finding was that content which was not in the press release, but only in the abstract or poster presentation, was primarily ignored in the news reporting.
The broadest qualitative conclusion of the Medstar authors regarded whether e-cigarettes had utility for quitting smoking. In the poster, the authors concluded that EC use should be discouraged among youth while further studies are conducted, but did not provide an opinion about the utility of e-cigarettes for harm reduction vs. continued smoking. This cautious tone was consistent with the lack of focus of the relative harm of EC use vs. CC use, and the acknowledgment that observational study designs can not prove causality. In the press release, however, this conclusion was expanded to a recommendation that EC not be used for quitting smoking. Consequently, the second quote was selectively communicated in general news reports and preferentially communicated in science news reports.
In their evaluation of the credibility of the Medstar study, science news sites relied heavily on an assertion that CC smoking was accounted for in the model (mentioned in 59% of reports). However, none of them noted that a 1.9X difference in CC smoking rates was only modelled as a 2% change in HF rates by the authors, and only 2 reports questioned the precision of the 2-product (CC and EC) dose-response assessment in a population which used both products. Of note, the Medstar study followed a case-control design. CC exclusive-users and CC + EC dual-users were not separately segmented out. Case control studies are especially susceptible to confounding, where the risk associated with one product can be artificially ascribed to the other product in modeling adjustments, which may explain why the risk associated with CC use was so low in the Medstar study [9].
Where Did It Go Wrong?
The errors which contributed to many of these news reports were distributed across all stages of the Medstar study, from the underlying database, to the work of the study authors, to the ACC, and finally in the news reporting.
- 1.
-
All of Us Study (NIH Database):
- Did not collect EC use duration data
- 2.
-
Abstract / Poster:
- a.
-
Imprecise measurement of EC and CC exposure
- Did not use CC use duration data available from the All of Us database.
- Did not measure EC and CC use during the prospective period.
- Used a case-control design which is especially subject to confounding if EC and CC use are not independent of each other.
- b.
- Omitted the finding that CC never use had a non-significant aOR of 1.04 in the poster.
- c.
- Did not directly report the aOR associated with CC use; rather, indirectly reported that 1.9X difference in CC use was accounted for by a 2% change in aOR.
- 3.
-
Press Release:
- Changed quote from “EC should not be used by youth” to “EC should not be used for stopping smoking” even though the study did not address this.
- Did not mention that the 1.9X increased CC smoking of the EC-ever-use group was “accounted for” as a 2% change in HF risk.
- Did however obscure this by stating that “smoking was accounted for.”
- Omitted that EC users who did not smoke did not show a significant increase in HF risk.
- Omitted that no dose response was found, in contrast to a previous year press release on the impact of cannabis by the same Medstar authors [12].
- 4.
-
News Reports
- All general news sites, and most science news sites, did not report content which was not in the press release.
- General news sites in particular relied heavily on quotations from the press release in their reporting.
- Even the science news sites did not question why CC use was viewed as harmless in this study.
- News media created and repeated a new claim that vaping even once could cause heart failure
- News media acknowledged confirmation bias in their reporting.
- Sensationalized headlines included characterization of the findings as “shocking” or indicating a “threat.” [3,14,21]
What Could Have Helped?
Science news journalists have a professional responsibility to review study content they report on, rather than relying on press releases, especially for non peer-reviewed studies. The Medstar abstract was available publicly online, and the poster presentation was available to journalists by request from the authors or the ACC. Effective fact-checking could have mitigated the impact of material omissions in the press release and provided a more accurate context for interpreting the data. Consultation of experts who could understand the underlying study design strengths and limitations was warranted. Epidemiologists could have clarified that vaping’s risks are dose-dependent and context-specific, and CC use and EC use were not measured precisely [9]. Unfortunately most (but not all) of the physicians who did provide commentary in the news reports did not critique the design limitations and result contradictions, most typically repeating from the press release that “this was one of the largest studies of its kind” and acknowledging confirmation bias in one case. Surveys have shown that most physicians are misinformed about nicotine, with the majority thinking incorrectly it is a primary reason smoking causes COPD and cancer, while only a minority believe it leads to birth defects [41]. Explanation of the non-smoking vapers’ null result and the fact that smoking was reported as near-harmless in this study would have painted a fuller picture, even if less sensational.
At the press release stage, the ACC could have highlighted nuance. Foregrounding the conflicting findings from the abstract and poster could have forced media to grapple with complexity.
Upstream, the authors could have preempted misinterpretation by not participating in the issuing of a press release with sensationalized quotes which were unsupported by their overall findings. Post-publication, they, as well as the news media, could still issue a statement correcting media distortions—a rare but impactful step.
Lessons Learned
This case illuminates the fragility of science communication when best practices are disregarded. Each stage of the data translation process, from the source NIH database, through the Medstar analysis, the ACC press release, and the subsequent news reporting decreased the precision and accuracy of the core data. Thorough fact-checking, using primary sources and experts who can understand the methodology of the study, is essential. Journalists have a responsibility to investigate thoroughly, and scientists and public health organizations likewise are entrusted by the public to be precise and accurate in their work. Truth is compromised when urgency and attention-seeking override careful scrutiny.
The net take: does EC use increase heart failure risk? Nicotine does have a well-established impact on the cardiovascular system, particularly in terms of acute biomarkers like blood pressure and heart rate. It has also been known for over a decade that EC, particularly when operated under extreme settings can emit high levels of toxicants [42]. E-cigarettes represent a broad category, and use of temperature-regulated and FDA-authorized vaping products can mitigate this.[9,43] The long term impact of EC use remains an important open question, both relative to continued smoking and relative to non-use of nicotine and tobacco products. The overall literature still points to EC use being more harmful than non-use, but dramatically less harmful than CC use, and helpful in quitting smoking.[9,44] Unfortunately, the Medstar study and its subsequent coverage have only muddied the water. The one optimistic note is that this study has shined a light on opportunities for the use of best practices to maximize the precision and accuracy of the analysis and reporting of future studies [9].
Postscript
As of one year after the ACC press release (5/17/2025), the Medstar study has been cited by at least 3 scientific papers but has still not yet been published in a peer-reviewed journal.[45,46,47]
However, a recent (April 2025) study with authors from the American Heart Association (AHA) and Johns Hopkins data-mined the same All of Us database and used a similar prospective approach, but segmented EC-exclusive users, CC-exclusive users, and EC+CC dual-users into separate cohorts [48]. As in the Medstar abstract, the AHA researchers reported that EC exclusive users did not have a significantly higher risk of heart failure compared to EC non-users (they reported a trend towards a 10-18% reduced risk in the EC exclusive users). Again, this material information was critically omitted from the Medstar presentation, the ACC press release, and 100% of news stories covering the Medstar study. Furthermore, in contrast to the Medstar study which modeled the impact of CC use as minimal, the AHA authors did report that exclusive CC use increased HF risk by 50%.
Lastly, however, both studies (Medstar and AHA), could have been more accurate in their analyses by factoring in duration of exposure to tobacco products in the sampled populations. In particular, the dual-use data from the AHA study is uninterpretable without adjusting for any differences in CC exposure in the dual-use vs. CC exclusive-use cohorts. In summary, observational studies of impact of exposure to tobacco and nicotine products should precisely measure the exposure if they wish their results to be accurate, and news reporters should verify this quantification as a standard course of their reporting on these types of studies [9].
Disclosures
G.C. is a salaried employee of Rose Research Center (RRC), an independent contract research organization that performs studies pertaining to smoking cessation and tobacco harm reduction. Dr. Jed Rose, the founder of RRC, invented the nicotine patch and performed the research which led to the development of varenicline (Chantix). RRC research support for other projects includes: National Institute on Drug Abuse; Global Action to End Smoking, Inc. (formerly Foundation for a Smoke-Free World, Inc.), a US nonprofit 501(c)(3) private foundation; Nicotine BRST LLC; JUUL Labs; Altria; Embera Neurotherapeutics, Inc.; Otsuka Pharmaceutical; Swedish Match, Philip Morris International. G.C. was previously a Principal Scientist at JUUL Labs. He also was employed at Nektar Therapeutics, whose pipeline included an inhaled NRT. Stock holdings in Qnovia, a developer of an inhaled NRT, and JUUL Labs. This review was not funded nor commissioned by any of these non-RRC entities.
Acknowledgments
Early analysis results were presented at the 2024 73rd TSRC conference [49]. The author thanks Saul Shiffman for comments on the abstract portion of this manuscript.
References
- American College of Cardiology (2024) Study Links E-Cigarette Use with Higher Risk of Heart Failure. ACC.org. [Online]. Available online: https://www.acc.org/About-ACC/Press-Releases/2024/04/01/21/51/study-links-e-cigarette-use-with-higher-risk-of-heart-failure (accessed on 11 April 2025).
- NIH, National Cancer Institute (2025) Compared to smoking cigarettes, would you say that using e-cigarettes that contain nicotine is…? | HINTS[Online]. Available online: https://hints.cancer.gov/view-questions/question-detail.aspx?PK_Cycle=14&qid=1929 (accessed on 15 April 2025).
- Penley, T. (2024) Smoking cigarettes can destroy lungs, but shocking new study reveals why vaping can harm the heart | Fox News. Fox News. [Online]. Available online: https://www.foxnews.com/media/smoking-cigarettes-destroy-lungs-shocking-new-study-vaping-harm-heart (accessed on 17 April 2025).
- Marshall, M. (2024) Could vaping one time put you at a higher risk of heart failure? - CBS Boston. CBS News. [Online]. Available online: https://www.cbsnews.com/boston/news/heart-failure-vaping-danger/ (accessed on 17 April 2025).
- Buzby, S. (2024) E-cigarette use could raise heart failure risk up to 19%. Healio. [Online]. Available online: https://www.healio.com/news/cardiology/20240417/ecigarette-use-could-raise-heart-failure-risk-up-to-19 (accessed on 15 May 2025).
- Blanchard, S. (2024) Vaping increases your risk of deadly heart failure by a fifth, study shows. The Sun. [Online]. Available online: https://www.thesun.co.uk/health/27074532/vaping-deadly-heart-failure-risk-health/ (accessed on 23 April 2025).
- Bene-Alhasan, Y. et al. (2024) ELECTRONIC NICOTINE PRODUCT USE IS ASSOCIATED WITH INCIDENT HEART FAILURE - THE ALL OF US RESEARCH PROGRAM. Journal of the American College of Cardiology 83, 695.
- All of Us Research Program (2025) Lifestyle Questionnaire[Online]. Available online: https://www.researchallofus.org/wp-content/themes/research-hub-wordpress-theme/media/surveys/Survey_Lifestyle_Eng_Src.pdf (accessed on 4 January 2025).
- Cohen, G. and Cook, S. (2025) Observational studies of exposure to tobacco and nicotine products: Best practices for maximizing statistical precision and accuracy. iScience 28, 111985.
- Farsalinos, K.E. et al. (2019) Is e-cigarette use associated with coronary heart disease and myocardial infarction? Insights from the 2016 and 2017 National Health Interview Surveys. Therapeutic Advances in Chronic Disease 10, 204062231987774.
- Lubin, J.H. et al. (2016) Risk of Cardiovascular Disease from Cumulative Cigarette Use and the Impact of Smoking Intensity: Epidemiology 27, 395–404.
- Bene-Alhasan, Y. et al. (2023) Abstract 13812: Daily Marijuana Use is Associated With Incident Heart Failure: “All of Us” Research Program. Circulation 148.
- Short, E. (2024) E-Cigarettes Tied to Heart Failure. Medpage Today. [Online]. Available online: https://www.medpagetoday.com/pulmonology/smoking/109470 (accessed on 18 April 2025).
- Johnson, A. (2024) Vaping Health Risks: Study Suggests Nearly 20% Increased Threat Of Heart Disease From E-Cigarette Use. Forbes. [Online]. Available online: https://www.forbes.com/sites/ariannajohnson/2024/04/02/vaping-health-risks-study-suggests-nearly-20-increased-threat-of-heart-disease-from-e-cigarette-use/ (accessed on 17 April 2025).
- DICardiology.com (2024) Study Links E-Cigarette Use with Higher Risk of Heart Failure. DAIC. [Online]. Available online: http://www.dicardiology.com/content/study-links-e-cigarette-use-higher-risk-heart-failure (accessed on 17 April 2025).
- Fortinsky, S. (2024) E-cigarette users 20 percent more likely to develop heart failure: Study. The Hill.
- Jennings, S. (2024) Vaping Associated with Increased Risk of Heart Failure, According to New Research. Patient Care Online. [Online]. Available online: https://www.patientcareonline.com/view/vaping-associated-with-increased-risk-of-heart-failure-according-to-new-research (accessed on 17 April 2025).
- Mundell, E. (2024) Vaping Could Raise Your Risk for Heart Failure. US News & World Report. [Online]. Available online: https://www.usnews.com/news/health-news/articles/2024-04-02/vaping-could-raise-your-risk-for-heart-failure (accessed on 17 April 2025).
- Ionescu, A. (2024) E-cigarettes linked to increased risk of heart failure. Earth.com. [Online]. Available online: https://www.earth.com/news/e-cigarettes-linked-to-increased-risk-of-heart-failure/ (accessed on 18 April 2025).
- Harris Bond, C. (2024) Vaping increases risk of heart failure by nearly 20%, study suggests. PhillyVoice. [Online]. Available online: https://www.phillyvoice.com/vaping-heart-failure-e-cigarettes-health-effects/ (accessed on 17 April 2025).
- Pickles, K. (2024) Fresh health warning over vaping as shock study finds e-cigarettes may raise risk of heart failure | Daily Mail Online. Daily Mail. [Online]. Available online: https://www.dailymail.co.uk/health/article-13263505/vaping-study-e-cigarettes-raise-risk-heart-failure.html (accessed on 17 April 2025).
- Loeppky, J. (2024) Heart Failure: E-Cigarettes Can Increase Risk By 21%. Healthline. [Online]. Available online: https://www.healthline.com/health-news/e-cigarettes-can-increase-heart-failure-risk-by-19 (accessed on 8 May 2025).
- Hampson, L. (2024) Vaping increases risk of heart failure by almost 20%, study finds. Yahoo Life!. [Online]. Available online: https://uk.style.yahoo.com/vape-heart-failure-study-110841496.html (accessed on 17 April 2025).
- Thomas, R. (2024) Vaping could increase heart failure by 19%, study says - Dentistry. Dentistry.co.uk.
- Howse, I. (2024) Vaping increases risk of heart failure by almost 20%. Metro. [Online]. Available online: https://metro.co.uk/2024/04/02/vaping-increases-risk-heart-failure-almost-20-20571960/ (accessed on 17 April 2025).
- Sullivan, K. (2024) Are E-Cigarettes Bad for Your Heart? New Research Suggests Vaping Could Raise Heart Failure Risk. Health.com. [Online]. Available online: https://www.health.com/study-vaping-e-cigarettes-heart-failure-8625237 (accessed on 18 April 2025).
- McKeown, L.A. (2024) Vaping Linked to Higher Risk of HFpEF, NIH Data Show. TCTMD.com. [Online]. Available online: https://www.tctmd.com/news/vaping-linked-higher-risk-hfpef-nih-data-show (accessed on 18 April 2025).
- Searles, M. (2024) Vaping causes substantial increase in risk of heart failure, study findsThe Telegraph.
- Watson, C. (2024) Massive Study Links Vaping to a Much Higher Risk of Heart Failure. ScienceAlert. [Online]. Available online: https://www.sciencealert.com/massive-study-links-vaping-to-a-much-higher-risk-of-heart-failure (accessed on 18 April 2025).
- Dewan, P. (2024) Vaping may cause “substantial” heart failure risk increase. Newsweek. [Online]. Available online: https://www.newsweek.com/vaping-cause-substantial-heart-failure-risk-1885920 (accessed on 17 April 2025).
- Massey, N. and Ahmed, J. (2024) Doctors reveal what vaping can do to your heart. The Independent. [Online]. Available online: https://www.independent.co.uk/news/science/vaping-vapes-heart-failure-smoking-b2522832.html (accessed on 17 April 2025).
- Pelc, C. (2024) Heart health: Vaping may raise heart failure risk by 19%. Medical News Today. [Online]. Available online: https://www.medicalnewstoday.com/articles/vaping-even-once-may-raise-risk-heart-failure-study-finds (accessed on 18 April 2025).
- Hayward, E. (2024) Vaping linked to increased risk of heart failure[Online]. Available online: https://www.thetimes.com/uk/article/vaping-increases-risk-of-heart-failure-researchers-find-n5bw36dms (accessed on 24 April 2025).
- Dillard, R. (2024) E-Cigarette Use Linked to Higher Risk of Heart Failure. Docwire News. [Online]. Available online: https://www.docwirenews.com/post/e-cigarette-use-linked-to-higher-risk-of-heart-failure (accessed on 18 April 2025).
- Geissler, H. (2024) Daily Express. One million facing health alert over “harmful effects” of vapes. [Online]. Available online: https://www.pressreader.com/uk/daily-express/20240403/281977497636261 (accessed on 24 April 2025).
- Cleveland Clinic News Service (2024) Vaping Linked to Heart Failure, Research Shows. Cleveland Clinic. [Online]. Available online: https://newsroom.clevelandclinic.org/2024/11/20/vaping-linked-to-heart-failure-research-shows (accessed on 18 April 2025).
- American College of Cardiology (2024) Heart failure risk of vapers 20% greater. Mirror. [Online]. Available online: https://www.pressreader.com/uk/daily-mirror/20240403/281943137898006/textview (accessed on 24 April 2025).
- ADA News Service (2024) Vaping increases risk of heart disease. ADA News. [Online]. Available online: https://adanews.ada.org/huddles/vaping-increases-risk-of-heart-disease/ (accessed on 18 April 2025).
- Massey, N. (2024) Vaping may increase the risk of heart failure, study suggests. The Standard. [Online]. Available online: https://www.standard.co.uk/news/science/vaping-people-uk-government-baltimore-nhs-b1149123.html (accessed on 24 April 2025).
- Hogue, M. (2024) Study links heart failure risk to e-cigarette use. American Pharmacists Association. [Online]. Available online: http://www.pharmacist.com/Blogs/CEO-Blog/Article/study-links-heart-failure-risk-to-e-cigarette-use (accessed on 15 May 2025).
- Steinberg, M.B. et al. (2021) Nicotine Risk Misperception Among US Physicians. J GEN INTERN MED 36, 3888–3890.
- Jensen, R.P. et al. (2015) Hidden Formaldehyde in E-Cigarette Aerosols. N Engl J Med 372, 392–394.
- FDA Center for Tobacco Products (2022) Technical Project Lead (TPL) Review of PMTAs: NJOY AceUS Food and Drug Administration.
- Rigotti, N.A. (2024) Electronic Cigarettes for Smoking Cessation — Have We Reached a Tipping Point? N Engl J Med 390, 664–665.
- Benam, K.H. (2024) Multidisciplinary approaches in electronic nicotine delivery systems pulmonary toxicology: emergence of living and non-living bioinspired engineered systems. Commun Eng 3, 123.
- Nagy, S.; et al. (2025) The Impacts of Vaping on the Cardiovascular System: A Systematic Review of Case Reports. Cureus. [CrossRef]
- Vaid, R.; et al. (2024) Asia’s Teen Vaping Surge: Unmasking Risks and Mobilizing Solutions. Asia Pac J Public Health 36, 646–647.
- Erhabor, J. et al. (2025) E-cigarette Use and Incident Cardiometabolic Conditions in the All of Us Research Program. Nicotine and Tobacco Research. [CrossRef]
- Cohen, G. (2024) “it’s good news”: case studies in the fact-checking of statistical bias in the scientific literature and its translation by the news media | CORESTACohen G. “it’s good news”: case studies in the fact-checking of statistical bias in the scientific literature and its translation by the news media | CORESTA [Internet]. 2024. Available online: https://www.coresta.org/abstracts/its-good-news-case-studies-fact-checking-statistical-bias-scientific-literature-and-its (accessed on 19 April 2025).
Figure 1.
News report indicating that vaping just once can cause heart failure. Source: © CBS News, reproduced under Fair Use [3]..
Figure 1.
News report indicating that vaping just once can cause heart failure. Source: © CBS News, reproduced under Fair Use [3]..
Figure 2.
Four stages of dissemination of information from underlying database to subsequent news reports.
Figure 2.
Four stages of dissemination of information from underlying database to subsequent news reports.
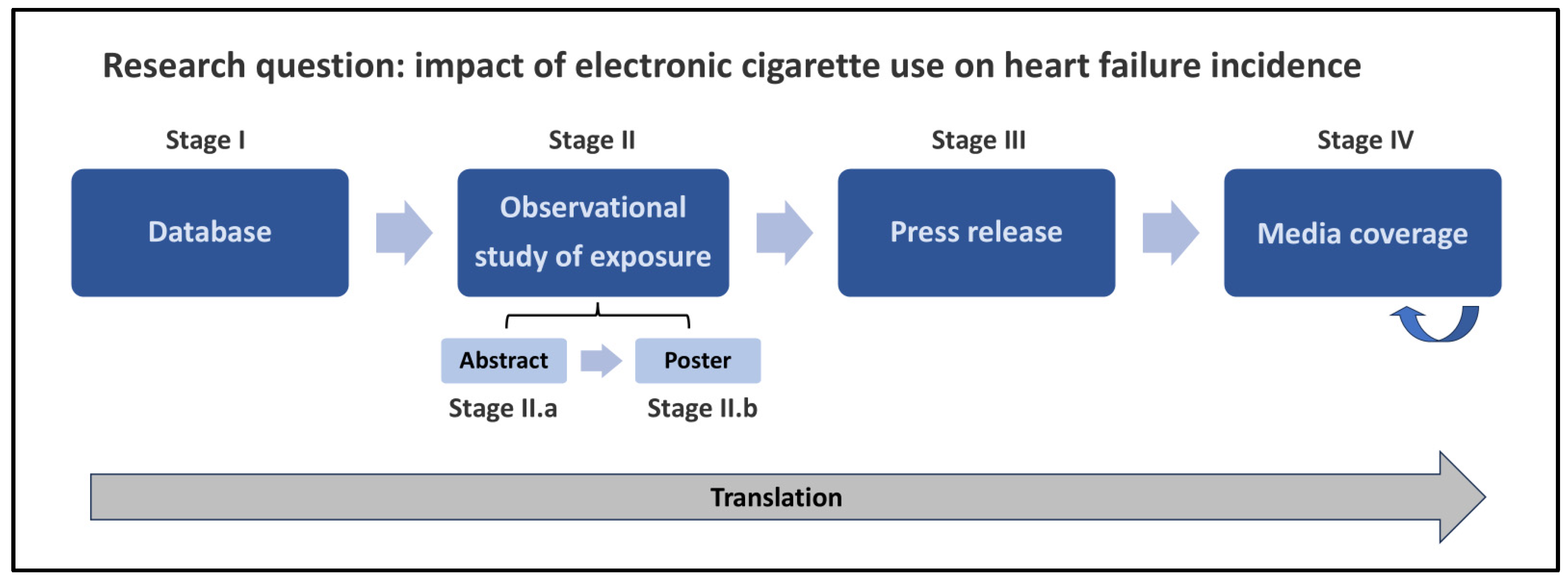
Figure 3.
(Graphical Abstract). Translation of content from primary study and press release to news sites. Logos are © of each news site and reproduced under Fair Use.
Figure 3.
(Graphical Abstract). Translation of content from primary study and press release to news sites. Logos are © of each news site and reproduced under Fair Use.
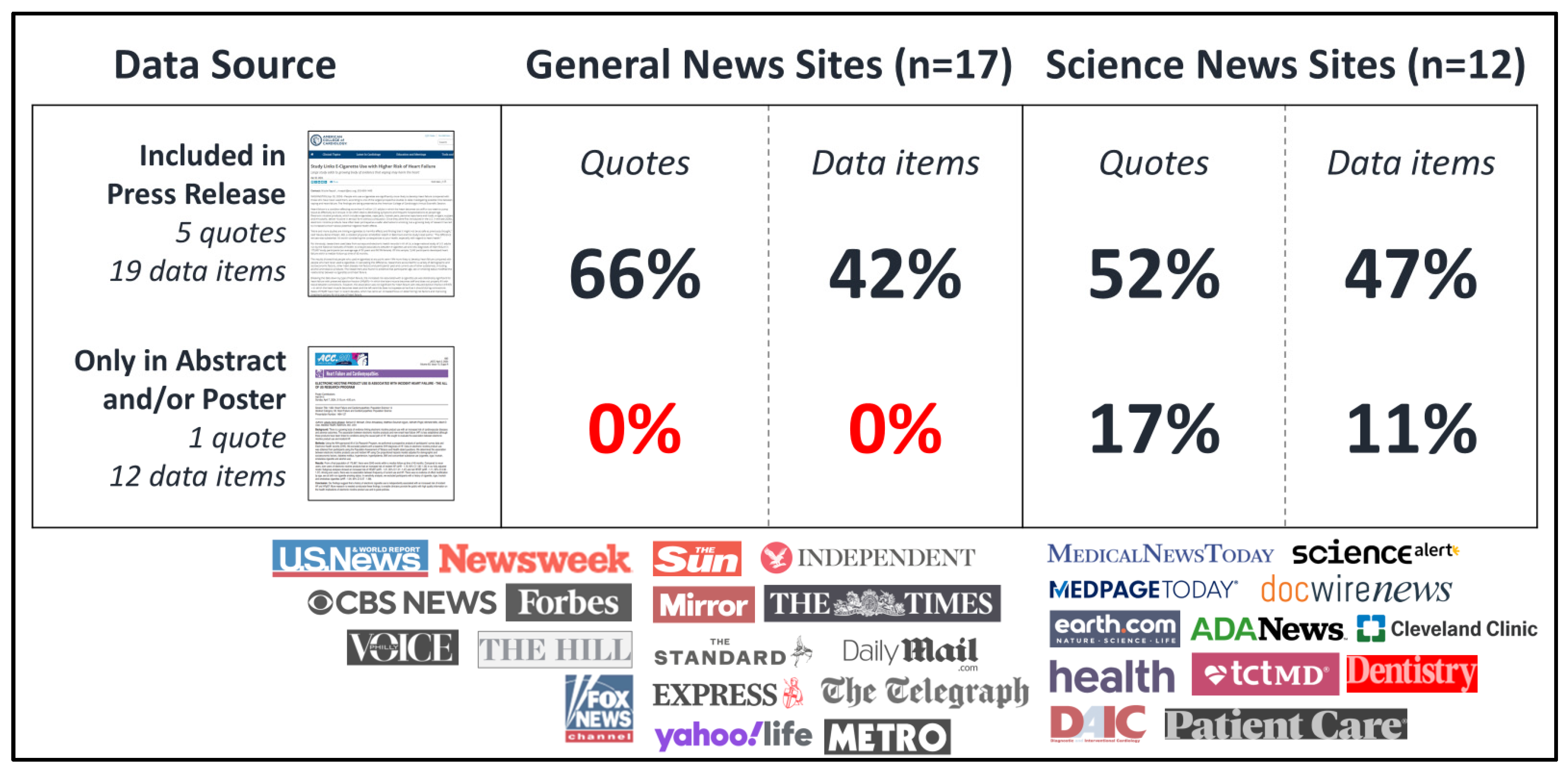
Figure 4.
Data fields pertaining to EC and CC use, All of Us Study. Data fields from the All of Us Lifestyle Questionnaire. Abbreviations: CC (cigarettes), EC (electronic cigarettes), CPD (cigarettes per day; 20 cigarettes = 1 pack).
Figure 4.
Data fields pertaining to EC and CC use, All of Us Study. Data fields from the All of Us Lifestyle Questionnaire. Abbreviations: CC (cigarettes), EC (electronic cigarettes), CPD (cigarettes per day; 20 cigarettes = 1 pack).
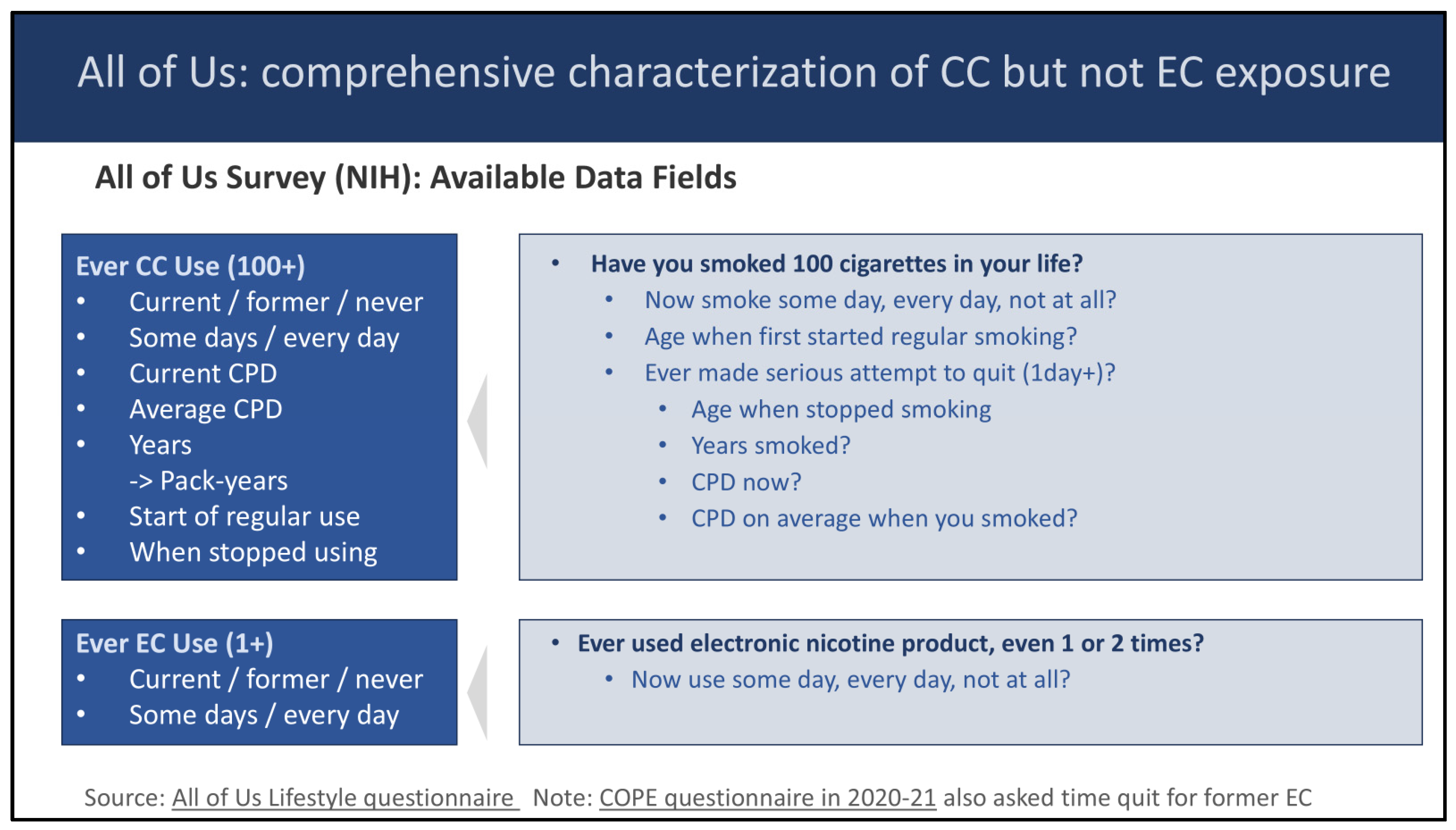
Figure 5.
Top-line results from the Medstar Study suggested that heart failure incidence was 19% higher in EC ever-users. Abbreviations: HF (heart failure), OR (odds ratio), aOR (adjusted odds ratio).
Figure 5.
Top-line results from the Medstar Study suggested that heart failure incidence was 19% higher in EC ever-users. Abbreviations: HF (heart failure), OR (odds ratio), aOR (adjusted odds ratio).
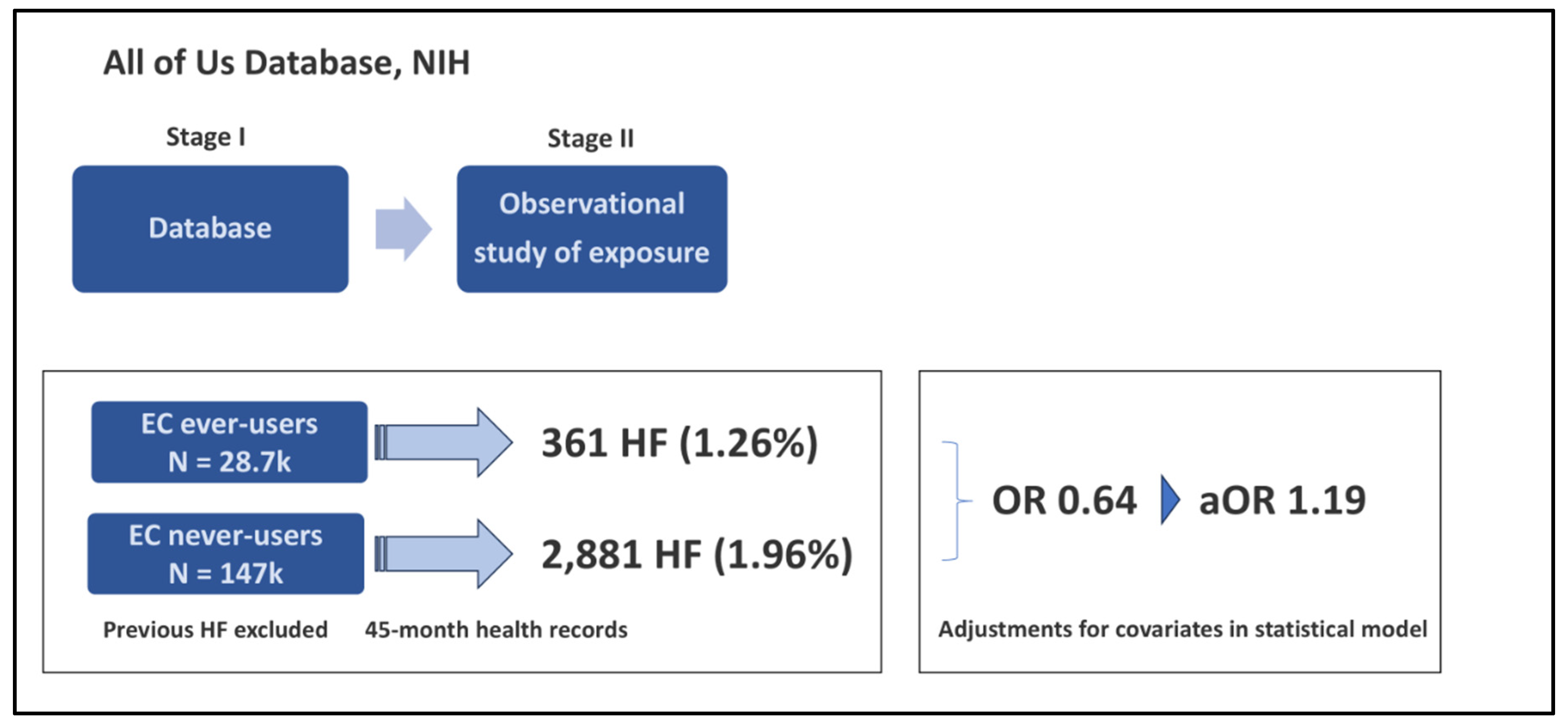
Figure 6.
The Medstar study utilized incomplete and imprecise EC and CC exposure metrics in their study of the impact of EC exposure. Left panel: CC use metrics. Right panel: EC use metrics. Abbreviations: CC (conventional cigarettes), EC (e-cigarettes), CPD (cigarettes per day).
Figure 6.
The Medstar study utilized incomplete and imprecise EC and CC exposure metrics in their study of the impact of EC exposure. Left panel: CC use metrics. Right panel: EC use metrics. Abbreviations: CC (conventional cigarettes), EC (e-cigarettes), CPD (cigarettes per day).
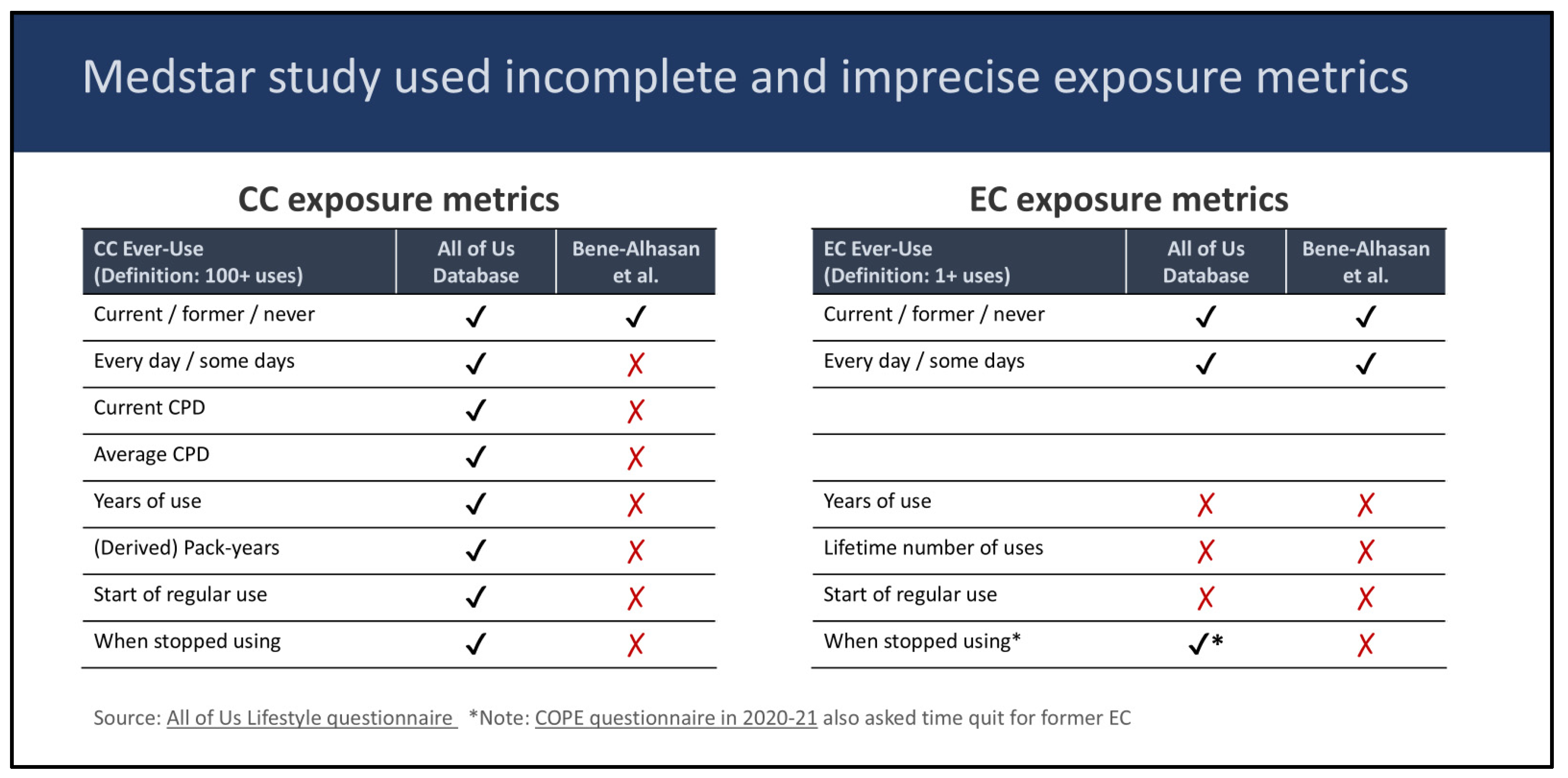
Figure 7.
EC and CC use histories, Medstar study. EC and CC use status at the start of the prospective period, EC ever-use cohort (left column) EC never-use cohort (middle column). Abbreviations: RR (relative risk), EC (electronic cigarette), CC (conventional combusted cigarette).
Figure 7.
EC and CC use histories, Medstar study. EC and CC use status at the start of the prospective period, EC ever-use cohort (left column) EC never-use cohort (middle column). Abbreviations: RR (relative risk), EC (electronic cigarette), CC (conventional combusted cigarette).
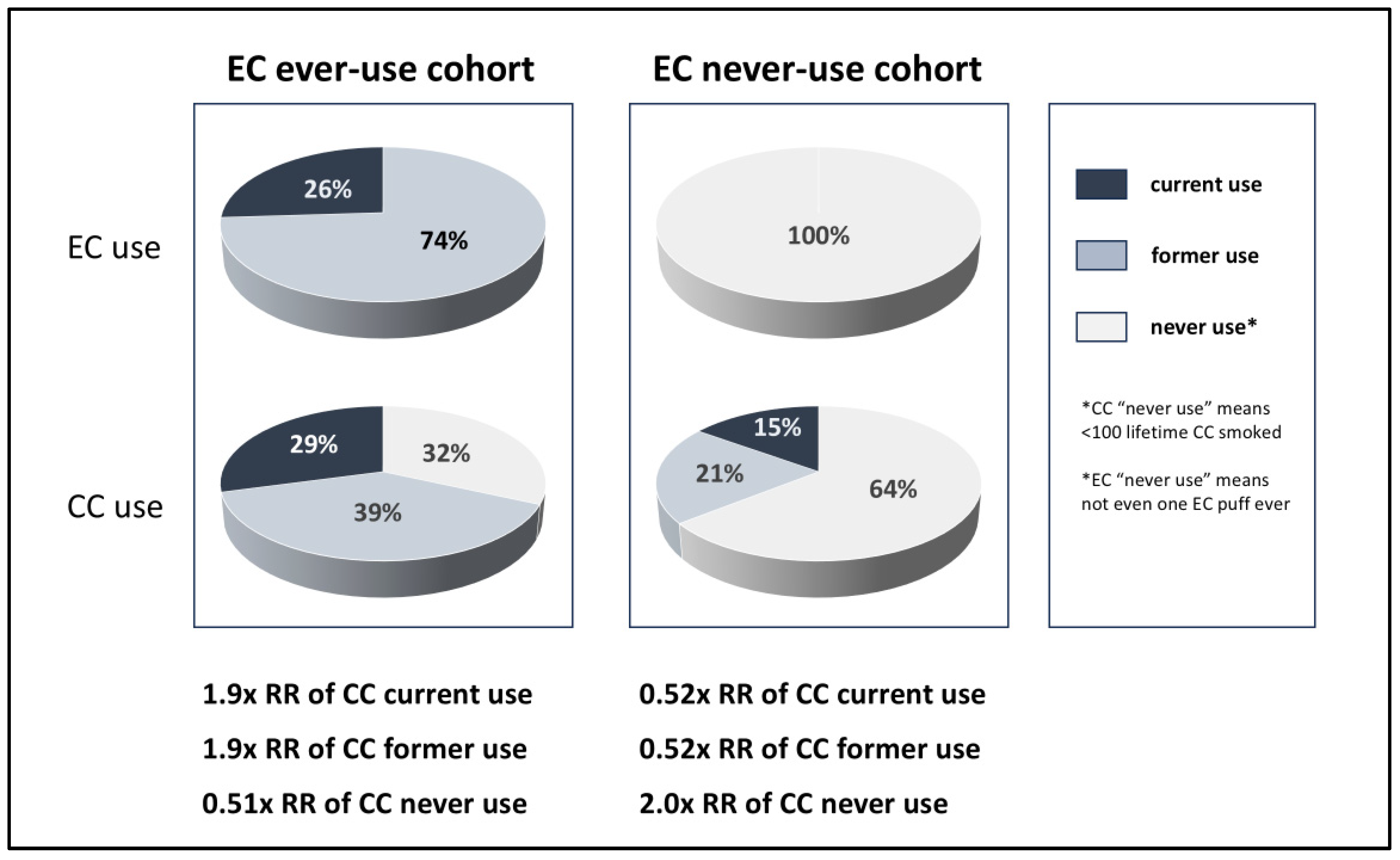
Figure 8.
Instances of material omissions, unsupported claims, and acknowledgment of confirmation bias. X represents omission, warning symbol represents unsupported claim or acknowledgment of confirmation bias.
Figure 8.
Instances of material omissions, unsupported claims, and acknowledgment of confirmation bias. X represents omission, warning symbol represents unsupported claim or acknowledgment of confirmation bias.


Table 1.
Characteristics of EC ever- and never-use groups, (Bene-Alhasan et al., 2024). OR (odds ratio), aOR (adjusted odds ratio, EC ever-users vs. never-users), HF (heart failure).
Table 1.
Characteristics of EC ever- and never-use groups, (Bene-Alhasan et al., 2024). OR (odds ratio), aOR (adjusted odds ratio, EC ever-users vs. never-users), HF (heart failure).
| EC Ever-Users | EC Never-Users | HF aOR | |
|---|---|---|---|
| Total sample | n=28,660 Age 40 (+/- 14) |
n=147,007 Age 54 (+/- 16) |
|
| HF Incident cases | 361 (1.26%) | 2,881 (1.96%) |
Risk of HF (unadjusted) OR = 0.64 |
| Odds ratio adjustments in the model - adjustments applied sequentially in 3 steps | |||
| Model 1 | Adjustments for age and demographic factors doubled the relative risk of HF associated with EC use in the model |
Risk of HF (adjusted) 0.64 -> 1.19 aOR of HF |
|
| Model 2 “accounted for the impact of CC smoking and substance use” |
Adjustments for tobacco and substance use reduced the EC group risk by only 2% (from 1.19 to 1.17) even though the EC group smoked CC almost twice as much as the EC non-use group | 1.19 - > 1.17 aOR of HF | |
| Model 3 (main model includes all 3 adjustments) |
Adjustments for diabetes, hypertension, hypercholesterolemia | 1.17 -> 1.19 aOR of HF aOR = 1.19 [1.04-1.34] |
|
Table 2.
Data releases by Medstar authors and the American College of Cardiology.
| Medstar / ACC data releases | Date | Comment |
|---|---|---|
| Abstract | 4/2/24 | Abstract published in Journal of ACC |
| Poster presentation | 4/7/24 | The 4/7 poster time of presentation was mentioned in the 4/2 press release; actual poster was released behind paywall or available from authors |
| Press release | 4/2/24 | Press release by ACC |
Table 3.
News sites which reported on the Medstar study included 17 general news sites and 15 science news sites.
Table 3.
News sites which reported on the Medstar study included 17 general news sites and 15 science news sites.
| Date | General news sites | Date | Science news sites | |
|---|---|---|---|---|
| 4/2/24 | Forbes [14] | 4/2/24 | DAIC [15] | |
| 4/2/24 | The Hill [16] | 4/2/24 | Patient Care [17] | |
| 4/2/24 | US News & World Report [18] | 4/2/24 | Earth.com [19] | |
| 4/2/24 | Philly Voice [20] | 4/2/24-3/24 | MedPage Today [13] | |
| 4/2/24 | Daily Mail (UK) [21] | 4/3/24 | Healthline [22] | |
| 4/2/24 | Yahoo Life! (UK) [23] | 4/4/24 | Dentistry (UK) [24] | |
| 4/2/24 | Metro (UK) [25] | 4/11/24 | Health [26] | |
| 4/2/24 | The Sun (UK) [6] | 4/12/24 | TCTMD [27] | |
| 4/2/24 | Telegraph (UK) [28] | 4/15/24 | Science Alert [29] | |
| 4/3/24 | Newsweek [30] | 4/17/24 | Healio [5] | |
| 4/3/24 | The Independent (UK) [31] | 4/27/24 | Medical News Today [32] | |
| 4/3/24 | The Times (UK) [33] | 7/24/24 | DocWire News [34] | |
| 4/3/24 | Daily Express (UK) [35] | 11/20/24 | Cleveland Clinic [36] | |
| 4/3/24 | Mirror (UK) [37] | Not disclosed | ADA News [38] | |
| 4/3/24 | Standard (UK) [39] | Not disclosed | Pharmacist.com [40] | |
| 4/7/24 | Fox News [3] | |||
| 4/29/24 | CBS News [4] |
Table 4.
Translation frequency of content items present in the abstract, poster and press release to general news and science news reports. Abstr. (abstract), Press Rel. (press release), News Rpt. (general news site report), Sci. Rpt. (science news site report).*UK or international prevalence statistics reported in UK papers.**A mention of the UK NHS supporting EC use for stopping smoking was sometimes also cited in UK papers, in segments following the discussion of the Medstar study.
Table 4.
Translation frequency of content items present in the abstract, poster and press release to general news and science news reports. Abstr. (abstract), Press Rel. (press release), News Rpt. (general news site report), Sci. Rpt. (science news site report).*UK or international prevalence statistics reported in UK papers.**A mention of the UK NHS supporting EC use for stopping smoking was sometimes also cited in UK papers, in segments following the discussion of the Medstar study.
| Inclusion in Abstract, Poster, Press Release | Translation Frequency |
|
|||
| Abstr. | Poster | Press Rel. |
News Rpt. n=17 |
Sci. Rpt. n=12 |
|
| ✔ | ✔ | ✔ | 100% | 100% | The results showed that people who used e-cigarettes at any point were 19% more likely to develop heart failure compared with people who had never used e-cigarettes. |
| ✔ | ✔ | ✔ | 100% | 93% | 175,667 study participants (an average age of 52 years and 60.5% female). |
| ✘ | ✘ | ✔ | 94% | 80% | “More and more studies are linking e-cigarettes to harmful effects and finding that it might not be as safe as previously thought,” said Yakubu Bene-Alhasan, MD, a resident physician at MedStar Health in Baltimore and the study’s lead author. |
| ✔ | ✔ | ✔ | 94% | 73% | Presented at the American College of Cardiology (ACC) annual scientific session |
| ✔ | ✔ | ✔ | 82% | 80% | Of this sample, 3,242 participants developed heart failure within a median follow-up time of 45 months. |
| ✘ | ✘ | ✔ | 76% | 73% | “The difference we saw was substantial. It’s worth considering the consequences to your health, especially with regard to heart health.” |
| ✘ | ✘ | ✔ | 71% | 40% | Heart failure affects 6M US adults, heart too stiff or weak |
| ✔ | ✔ | ✔ | 65% | 80% | Breaking the data down by type of heart failure, the increased risk associated with e-cigarette use was statistically significant for heart failure with preserved ejection fraction (HFpEF)—in which the heart muscle becomes stiff and does not properly fill with blood between contractions. |
| ✘ | ✘ | ✔ | 65% | 60% | “I think this research is long overdue, especially considering how much e-cigarettes have gained traction,” |
| ✘ | ✘ | ✔ | 65% | 60% | “We don’t want to wait too long to find out eventually that it might be harmful, and by that time a lot of harm might already have been done. With more research, we will get to uncover a lot more about the potential health consequences and improve the information out to the public.” |
| ✔ | ✘ | ✔ | 53% | 33% | EC have been portrayed as safer but growing research lead to increased concern |
| ✘ | ✘ | ✔ | 47% | 7% | 5-10% of teens and adults use EC. Surgeon General called youth EC use an epidemic* |
| ✔ | ✔ | ✔ | 35% | 73% | Accounted for demographic, socioeconomic, heart disease factors, and current use of other substances, including alcohol and tobacco products. |
| ✘ | ✘ | ✔ | 35% | 53% | Bene-Alhasan said EC are not recommended for quitting smoking*** |
| ✘ | ✘ | ✔ | 35% | 40% | Researchers said the new study findings point to a need for additional investigations of the potential impacts of vaping on heart health, especially considering the prevalence of e-cigarette use among younger people. |
| ✘ | ✘ | ✔ | 35% | 40% | Bene-Alhasan said this study was one of the most comprehensive / largest studies to date |
| ✔ | ✔ | ✔ | 35% | 40% | EC impact on HFrEF was not significant |
| ✔ | ✔ | ✔ | 29% | 67% | Study used the All of Us database from NIH |
| ✘ | ✘ | ✔ | 29% | 40% | Results align with previous studies in animals and humans, though some studies inconclusive |
| ✘ | ✘ | ✔ | 29% | 40% | Researchers said the observational design allows them to infer, but not conclusively determine a causal relationship |
| ✘ | ✘ | ✔ | 29% | 20% | Rates of HFpEF have risen in recent decades, increased focus on determining risk factors |
| ✔ | ✔ | ✔ | 18% | 47% | People who use e-cigarettes are significantly more likely to develop heart failure compared with those who have never used them (2nd mention, without 19% statistic) |
| ✔ | ✔ | ✔ | 18% | 47% | No evidence that age, sex or smoking status modified the relationship between EC and HF |
| ✘ | ✘ | ✔ | 18% | 20% | Bene-Alhasan said previous studies had limitations including smaller sizes |
| ✔ | ✘ | ✔ | 6% | 27% | Electronic nicotine products include e-cigarettes, and deliver nicotine in aerosol form without combustion. |
| ✔ | ✔ | ✘ | 0% | 33% | HFpEF aOR 1.21 [1.01-1.47], HFrEF aOR 1.11 CI [ 0.90-1.37] |
| ✘ | ✔ | ✘ | 0% | 27% | Dual users had 59% increased risk of incident HF |
| ✔ | ✘ | ✘ | 0% | 27% | PATH-styled questions on EC use. |
| ✔ | ✔ | ✘ | 0% | 27% | EC ever-use: aOR for HF 1.19, 95% CI [1.06 -1.35] in the fully adjusted model factoring in all covariates. |
| ✔ | ✔ | ✘ | 0% | 13% | Exclusion: patients with baseline HF diagnosis |
| ✘ | ✔ | ✘ | 0% | 13% | 70% were White, 20% were Black, and 10% were Asian or Hispanic |
| ✘ | ✔ | ✘ | 0% | 13% | Conclusion: Electronic nicotine product use should be discouraged among the youths while further studies are conducted |
| ✘ | ✔ | ✘ | 0% | 7% | Inclusion: Adults 18+ |
| ✘ | ✔ | ✘ | 0% | 7% | EC ever-user group: current EC use 27%, current CC use 29% (EC group smoked more than it vaped). |
| ✘ | ✔ | ✘ | 0% | 7% | EC never-use group: current CC use 15% |
| ✔ | ✘ | ✘ | 0% | 7% | No difference between EC current users who were every-day and some-day users (no dose-response) |
| ✔ | ✘ | ✘ | 0% | 7% | Conclusion: More research is needed to corroborate these findings, to enable clinicians to provide the public with high quality information on the health implications of electronic nicotine product use and to guide policies. |
| ✘ | ✔ | ✘ | 0% | 7% | EC ever-users n=28,660 EC never-users n=147,007 |
| ✔ | ✘ | ✘ | 0% | 7% | EC exclusive users (never smokers) had 4% increased risk, CI [0.57-1.89] (not significant). |
| ✘ | ✔ | ✘ | 0% | 0% | The impact of a 1.9x difference in CC use in the EC group was only a 2% increase in HF risk in the fully adjusted model |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



