Submitted:
27 April 2025
Posted:
29 April 2025
You are already at the latest version
Abstract
Complex Regional Pain Syndrome (CRPS) is a rare, chronic painful neurological debilitating disorder. Despite the substantial impact on quality of life, diagnosis remains challenging due to its complex pathophysiology and subjective clinical criteria. This integrative review aims to synthesize current research on potential diagnostic biomarkers for CRPS. A systematic search was conducted using PubMed and Scopus databases to identify relevant studies published until January 2025. Inclusion criteria focused on adult CRPS patients, with studies examining diagnostic or predictive biomarkers. Key findings highlight the role of inflammatory and immune-related biomarkers, such as elevated levels of cytokines (IL-6, TNF-α), immune cell infiltration, and specific autoantibodies. Neuropeptides, including substance P and calcitonin gene-related peptide, were associated with pain sensitization in acute phases, though their levels normalized in chronic stages. Additionally, genetic and epigenetic markers, brain imaging, and neurophysiological alterations provided insights into CRPS pathogenesis, emphasizing the dynamic nature of these biomarkers across disease stages. The review underscores the need for further research to integrate these biomarkers into diagnostic frameworks, which could enhance early diagnosis and treatment strategies for CRPS.
Keywords:
Complex Regional Pain Syndrome
; biomarkers
; cytokines
; neuropeptides
; inflammation
; immune response
1. Introduction
Complex regional pain syndrome (CRPS), formerly known as algodystrophy, causalgia (type 2 CRPS), reflex sympathetic dystrophy (type 1 CRPS), Sudeck’s atrophy, is a rare chronic neurologic condition which is frequently precipitated by trauma or elective surgery to the upper and lower limbs. CPRS causes significant morbidity and loss of quality of life [1]. The Budapest criteria for CRPS considers five categories of symptoms, pain disproportionate to any inciting event, sensory (allodynia, hyperalgesia), vasomotor changes (temperature asymmetry, skin color changes), sudomotor/edema changes (edema, sweating changes) and motor/trophic changes (decreased range of motion, muscle atrophy). A person with at least one symptom in three of the four categories is diagnosed with CRPS [2]. Management of CRPS is multimodal, often including a combination of free-radical scavengers, steroids and nonsteroidal anti-inflammatory medications, anti-depressants, gabapentinoids and physiotherapy [3]. These interventions are more effective in the early stages of the disease [3,4]. For unknown reasons, the clinical course of CRPS varies significantly with spontaneous resolution in one pole and aggressive refractory disease on the opposite pole, despite adequate management [4]. The uncertainty about clinical evolution reflects the complexity of the underlying pathophysiology that remains to be clarified. Nevertheless, there is consensus that CRPS results from aberrant peripheral and central responses to an injury which may involve multifactorial contribution of genetic predisposition, inflammation, immunological dysfunction, and brain plasticity adaptations [5,6,7]. Previous reviews were focused on brain imaging biomarkers [8] or other specific biomarkers such as inflammation [9,10] and some of the reviews are outdated in more than a decade [10,11]. The integration of different diagnostic biomarkers can reduce subjectiveness, anticipate diagnosis and treatment. For these reasons we sought to systematically review the available data on the potential diagnosis biomarkers of CRPS.
2. Materials and Methods
Methods Search Strategy: Pubmed and Scopus databases were used to search for relevant publications from interception to 30/01/2025 using the following terms Algoneurodystrophy, “Sudeck syndrome”, “causalgia” and “Complex Regional Pain Syndrome”, “reflex sympathetic dystrophy”, “reflex neurovascular dystrophy”. We have complemented this search by examining reference lists of the most relevant studies and the Open grey database (http://www.opengrey.eu/).
Study selection: We included prospective and retrospective studies published up to 30 January, 2025, containing information on one of the following domains under analysis: frequency and diagnostic or predictive associated factors. Only studies focusing on CRPS adult populations (≥ 18 years) and written in English were taken into consideration. Conference or seminar abstracts and/or studies with unclear inclusion criteria or convenience sampling, including very selective groups or mixed population with non CPRS patients, were excluded from the selection. Two authors independently screened abstracts obtained from the database search. Discrepancies were evaluated by a third investigator and resolved by the main investigator (RL). The full texts of potentially relevant articles were retrieved for further assessment. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist for systematic reviews was used to guide data extraction and report.
Quality Assessment of Literature
Two investigators independently evaluated the quality of the studies using the Newcastle-Ottawa Scale (NOS). The NOS includes three categories: selection of study groups, comparability of groups, and measurement of exposure, with a maximum score of 9. Scores of 0-4 are considered of low quality, 5-6 as moderate quality, and 7-9 as high quality [12].
Data extraction and synthesis:
Data were analyzed qualitatively. A posteriori, we divided biomarkers into inflammation and immune related potential biomarkers (cytokines, cells, autoantibodies, neuropeptides, others); genetic and epigenetic; brain imaging, and functional neurophysiological biomarkers. When appropriate data was described in terms of frequency, means and median. No meta-analysis was anticipated due to the expected marked heterogeneity and methodological variability of the studies. The study protocol was registered at Prospero (https://www.crd.york.ac.uk/ PROSPERO/) with number CRD4389417.
3. Results
We identified a total of 7901 (Pubmed) and 8799 (Scopus) publications using the predefined searching criteria. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart diagram (Figure 1) resumes the selection and inclusion process. A total of 66 [7,9,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76] studies, 2691 patients with CRPS were included in the systematic review.
The studies addressed different types of potential inflammation, immune, genetic, epigenetic, brain imaging and functional neurophysiological biomarkers associated of complex regional pain syndrome (Figure 2).
The list of inflammation and immune related potential biomarkers found in the literature are depicted in Table 1.
| Table 1. List of inflammation and immune related potential biomarkers associated with complex regional pain syndrome | ||||||
| Author, year | n | Cytocines | Cells | Autoantibodies | Neuropeptides | Others |
| Hartmannsberger et al, 2024 [32] | 25 | ↑Local mast cells and Langerhans cells (acute phase)± Local mast cells and Langerhans cells (chronic phase) | ||||
| Parkitny et al.,2022 [56] | 69 | ± immediate post fracture levels of IL** | ± immediate post fracture levels of T Cells | |||
| Bharwani et al, 2020 [19] | 23 | ↑sIL-2R | ||||
| Russo et al, 2020 [60] | 44 | ↓ IL-37, ↓GM-CSF | ||||
| Baerlecken et al, 2019 [17] | 36 | IgG to P29ING4 | ||||
| Russo et al, 2019 [61] | 14 | ↓ number of central memory CD8+, CD4+ T lymphocytes | ↑p38 signalling in CD1+ mDCs (dendritic cell type activation ?) | |||
| Bharwani et al, 2017 [9] | 80 | ↑sIL-2R | ||||
| Yetişgin et al,2016 [75] | 21 | ± blood cellular counts | ±: VS , CRP | |||
| Dirckx et al 2015 [27] | 66 | ↑ IL-6, TNF-a | ||||
| Dirckx et al, 2015 [28] | 296 | Antineuronal IgG | ||||
| Antinuclear IgG | ||||||
| Birklein et al,2014 [21] | 55 | ↑ local IL-6 | ↑Local mast cells | ↑ local tryptase | ||
| ↑ local TNF-α | ||||||
| Ritz et al, 2011 [59] | 25 | ± proinflammatory cytokines (IL-6, IL-8, TNF-a) | ↑ CD14+ CD16+ monocytes | |||
| ±IL-10 | ± T helper cells (CD4+ CD8- ), T cytotoxic cells (CD4- CD8+ ), NK cells (CD56+ ), B cells (CD19+ ), monocytes/macrophages (CD14+ ) | |||||
| Orlova et al, 2011 [55] | 41 | ↑interleukin1 receptor antagonist | ||||
| ↑ monocyte chemotactic protein-1 | ||||||
| ±IL-6, TNFα | ||||||
| ±Interferon-gamma, IL-1β, IL-2, IL-4, IL-5, IL-7, IL-8, IL-10 | ||||||
| Kohr et al, 2011 [47] | 20 | IgG to b2 adrenergic and/or the muscarinic-2 receptors | ||||
| Kaufmann et al,2009 [45] | 10 | ↑ anandamide | ||||
| Kohr et al, 2009 [48] | 30 | IgG to SH-SY5Y (inducible autonomic nervous system autoantigen) | ||||
| Schinkel et al, 2009 [62] | 25 | ± IL-4, IL-6, IL-8, IL-10, IL-11, IL-12 | ±White Blood Cell Count | ↑ Calcitonin Gene-Related Peptide | ↑Soluble TNF Receptor I and II | |
| ± TNF, IL6 | ↑ Substance P | ±CRP | ||||
| Wesseldijk et al,2009 [71] | 66 | ±IgE, tryptase | ||||
| Wesseldijk et al,2008 [74] | 12 | ↑ local TNF-α | ||||
| ↑ local IL-6 | ||||||
| Chronic phase | ± IL6, TNF-α | |||||
| Kaufmann et al, 2007 [44] | 15 | ± Lymphocites | ||||
| ↓cytotoxic CD8+ lymphocytes; IL-2-producing T cell | ||||||
| Uçeyler et al, 2007 [70] | 40 | ↓ IL-10, Transforming growth factor beta 1 | ± Whole blood counts | ± CPR | ||
| ↑IL-2 | ||||||
| ± TNF-α, IL-6 | ||||||
| ± IL-4 | ||||||
| Alexander et al, 2007 [14] | 22 | ↑ CSF IL-6 | ||||
| ↓ CSF IL-2, IL-10 | ||||||
| ↑ CSF Monocyte chemoattractant protein-1 | ||||||
| Heijmans-Antonissen et al 2006 [33] | 22 | ↑ local IL-6 | ||||
| ↑ local TNF-α | ||||||
| ± local IFNγ, IL-2, IL-2R, IL-4, IL-5, and IL-10 | ||||||
| ↓eotaxin | ||||||
| Schinkel et al, 2006 [63] | 25 | ↑ IL-8 | ± leukocytes | ↑ Subastance P | ↓soluble forms of selectins | |
| ±IL-6 | ± Neuropeptide Y | ±CRP | ||||
| ± CGRP | ↑soluble tumor necrosis factor receptor I/II | |||||
| Tan et al, 2005 [67] | 6 | ↑ Local leukocytes | ||||
| Alexander et al, 2005 [15] | 24 | ↑ CSF IL-6 / IL-1 | ||||
| ± CSF TNF-α | ||||||
| Munnikes et al, 2005 [54] | 25 | ↑ local IL-6 | ||||
| ↑ local TNF-α | ||||||
| Chronic phase | ± local IL-6 | |||||
| Chronic phase | ± local TNF-α | |||||
| Blaes et al, 2004 [22] | 12 | ↑IgG Myenteric plexus | ||||
| Huygen et al, 2004 [39] | 20 | ↑ local IL-6 | ↑tryptase | |||
| ↑ local TNF-α | ||||||
| Huygen et al, 2002 [38] | 9 | ↑ local IL-6 | ||||
| ↑ local TNF-α | ||||||
| ± local IL-1b , IL-1b | ||||||
| Birklein et al, 2001 [20] | 19 | ↑ Calcitonin Gene-Related Peptide | ||||
| Ribbers et al, 1998 [58] | 13 | ± Cell distribution (B and T lymphocyte populations) | ||||
| Blair et al, 1998 [23] | 61 | ↑ Calcitonin Gene-Related Peptide | ||||
| ± Neurokinin | ||||||
| ↑Bradykinin | ||||||
| CSF: Cerebrospinal fluid; IL: Interleukins; **: IL-1β, IL-10, IFN-α, IL-6, IL-12, RANTES, IL-13, IL-15, IL-17, MIP-1α, GM-CSF, MIP-1β; MCP-1, IL-5, IFN-γ, TNF-α, IL-1Ra, IL-2 , IL-7, IP-10 , IL-2r, MIG , IL-4 = interleukin-4, IL-8; GM-CSF: Granulocyte-macrophage colony-stimulating factor; tCr =total creatine levels; * N-acetylaspartate, tCr and potassium; TMS : transmagnetic strimulation; TNF: Tumor necrosis factor; AA: Aminoacids; ± No difference /correlation ; VS: erythrocyte sedimentation rate; CRP: C-reactive protein levels, | ||||||
Immune system cells
Most studies showed that the systemic distribution of immune system cells, namely B and T lymphocytes, natural killer, monocytes/macrophages is similar between CPRS patients and controls [44,58,59,62,63,70,75]. However, when comparing specific or subset of immune cells populations, an increased number proinflammatory CD14+ CD16+ monocytes [59] and reduction of cytotoxic CD8+ lymphocytes and IL-2-producing T cell [44] was demonstrated in CPRS patients. In studies based on cutaneous or subcutaneous tissue sample from the affected limb, an increased number of leukocytes [67] and mast cells [21] was demonstrated in patients with CPRS.
In addition, that the number of central memory CD8+, CD4+ T lymphocytes was found to be reduced in patients with CPRS in comparison to controls [61].
Autoantibodies
The prevalence of autoantibodies against the myenteric plexus [22], neurons [28], autonomic nervous system antigens [47,48], and tumor suppressor P29ING4 [17] was found to be elevated in CPRS patients. In addition, in a single study the frequency of anti-nuclear antibody was higher in CPRS patients in comparison to controls [28]. In none of these studies the pathogenicity was proven.
Cytokines
Table 1 shows that 14 studies evaluated the levels of different cytokines between CPRS patients and controls 14 with IL-6 and TNF-α being the most frequently studied. The systemic levels of IL-6 [55,62,63,70] and TNF-α [55,62,70] were comparable to controls. On the contrary, the systemic levels of IL-8 [63], IL-2 [70] were higher in patients with CPRS. The systemic levels of IL-10 and transforming growth factor beta 1 [70], granulocyte-macrophage colony-stimulating factor and IL-37, were decreased in CPRS [60] in comparison to controls. The systemic levels of IL-4, IL-8, IL-10, IL-11, IL-12 were also found to be similar between cases and controls [55,62].
In all studies evaluating behavior of cytokines in skin blisters, the levels of pro-inflammatory cytokines TNF-α and IL-6 [21,28,33,38,39,54,70,74] were found to be elevated in acute and intermediate stage, but not in the chronic phase [54,74]. The local levels of eotaxin, an eosinophilic chemokine, were found to be diminished in a single study [33]. No local differences for IL-1b , IL-1b [38], IFNγ, IL-2, IL-2R, IL-4, IL-5, and IL-10 [33].
In the cerebrospinal fluid, the levels of IL-1, IL-2, IL-6, IL-10 and monocyte chemotactic protein-1 were elevated [14,15], whereas the level of TNF-α was normal [15] in patients with CPRS.
Other inmune related proteins
The level of different proteins associated with specific immune cells activation such as the soluble IL receptor and selectins for activated T cells [9,62,63], and of local [21,39], but not the systemic [71] tryptase for mast cells was altered in CPRS patients. The C reactive protein level was normal in all studies [62,63,70,75] (Table 1).
Neuropeptides and neurogenic inflammation
In 4 studies (Table 1), the local and systemic levels of neuropeptides namely CGRP, substance P, neuropeptide Y, neurokinin, bradykinin side were higher in CPRS patients in comparison to controls or the contra-lateral healthy side [11,20,23,62]. The behavior of neuropeptides was found to change over time, with studies showing normalization CGRP associated with improvement of local inflammation [20], or absence of differences between CRPS and controls or even lower levels in patients with chronic CRPS [62,63]. For substance P, the shift was also demonstrated with increased levels in acute [62,63], and normal levels in chronic patients [62].
The level of different proteins associated with specific immune cells activation such as the soluble IL receptor and selectins for activated T cells [9,62,63]; and of local [21,39], but not the systemic [71] tryptase for mast cells was altered in CPRS patients. The C reactive protein level was normal in all studies [62,63,70,75]. The levels of anandamide which is synthesized by nucleated blood cells are higher in long-lasting CRPS suggesting an effort of the endogenous cannabinoid system to modulate neuropathic pain and pain memory [45].
Table 2. resumes depicts the genetic, epigenetic, brain imaging and functional neurophysiological biomarkers associated of complex regional pain syndrome.
| Table 2: Genetic, epigenetic, brain imaging and functional neurophysiological biomarkers associated of complex regional pain syndrome | ||||||
| Author, year | n | Genetic and epigenetics | Brain imaging | Functional neurophysiological | Other biomarkers | |
| Strutural | Metabolic | |||||
| Hok et al, 2024 [34] | 51 | ↓ antinociceptive modulation via the brainstem antinociceptive system | ||||
| Shaikh et al, 2024 [64] | Single-nucleotide polymorphism of genes ANO10, P2RX7, PRKAG1 and SLC12A9 | |||||
| Hotta et al.,2023 [37] | 17 | Sustained somatotopic alteration of the somatosensory cortex | ||||
| Delon-Martin et al.,2023 [25] | 11 | ↑ localized activation in the primary somatosensory cortex ( transcranial magnetic stimulation) | ||||
| Zhu et al.,2023 [7] | 9 | Five top five hub genes: MMP9, PTGS2, CXCL8, OSM, TLN1 | ||||
| Hong et al,,2023 [35] | 21 | ↑ functional connectivity in the somatosensory (S1) subnetworks | ||||
| ↓functional connectivity in the prefronto-parieto-cingulo-thalamic subnetworks | ||||||
| Lee et al., 2022 [51] | 15 | ↑ Basal ganglia infra-slow oscillations | ||||
| ↑ Basal ganglia resting connectivity | ||||||
| Domim et al, 2021 [29] | 24 | ↓ insula and bilateral grey matter medial thalamus. | ||||
| König et al, 2021 [49] | 25 | ↓ activity of angiotensin-converting enzyme | ||||
| Azqueta-Gavaldon et al, 2020 [16] | 20 | ↓gray matter density in the putamen/ functional connectivity increases amongst the putamen and pre-/postcentral gyri and cerebellum | ||||
| Russo et al, 2020 [60] | 44 | ↓ tryptophan | ||||
| Di Pietro et al., 2020 [26] | 15 | ↑ thalamo-S1 functional connectivity | ||||
| Bruehl et al 2019 [24] | 9 | Altered methylation of specific genes (COL11A1 and HLA-DRB6) | ||||
| Jung et al, 2019 [42] | 12 | Disruption of interactions between specific central and metabolic metabolites* in the thalamus | ||||
| Kohle et al,2019 [46] | 15 | ↓ activation of subthalamic nucleus, nucleus accumbens, and putamen | ||||
| Jung, et al, 2018 [43] | 12 | Anormal interactions of lipid13a and L f lipid 09 in the thalamus with peripheral tCr | ||||
| Hotta et al, 2017 [36] | 13 | Abnormal neural activity in sensorimotor and pain related areas | ||||
| Shokouhi et al, 2017 [66] | 28 | ↓grey matter in somatosensory cortex, and limbic system | ↓ perfusion in somatosensory cortex, and limbic system (early phase) | |||
| ↑ perfusion in somatosensory cortex, and limbic system (late phase) | ||||||
| Janicki et al, 2016 [40] | 230 | ±Common Single Nucleotide Polymorphisms |
||||
| Zhou et al, 2015 [76] | 35 | ↑ volume of choroid plexus | ||||
| Lee et al,2015 [52] | 25 | ↓ cortical thinning in the prefrontal cortex | ||||
| Pleger et al, 2014 [57] | 15 | ↑ in gray matter density in dorsomedial prefrontal | ||||
| ↑ in gray matter density located in the primary motor cortex (contralateral to the affected limb) | ||||||
| Krämer et al, 2014 [50] | 33 | ↑ Osteoprotegerin |
||||
| Barad et al, 2013 [18] | 15 | ↓ grey matter volume in pain related areas (dorsal insula, orbitofrontal cortex, cingulate cortex. | ||||
| Jin et al 2013 [41] | 24 | Increased expression of MMP9 | ||||
| Alexander et al, 2013 [13] | 160 | ↑ AA: L-Aspartate, L-glutamate, L-ornithine | ||||
| ↓ L-tryptophan and L-arginine | ||||||
| Lenz et al, 2011 [53] | 21 | ↓ Somatosensory cortex inhibition | ||||
| Orlova et al, 2011 [55] | 41 | ↑Specific microRNA: hsa-miR-532-3p | ↑ Vascular endothelial growth factor | |||
| Walton et al, 2010 [69] | 64 | Altered magneto-encephalographic imaging (thalamo-cortical Dysrhythmia) | ||||
| Wesseldijk et al, 2008 [73] | 64 | ↑ NMDA excitatory amino acids: glutamate, glutamine, glycine, taurine and arginine | ||||
| Wesseldijk et al, 2008 [72] | 35 | ↑ serotonin |
||||
| Geha et al, 2008 [31] | 26 | ↓ insula, ventromedial prefrontal cortex, nucleus accumbens; fractional anisotropy in cingulum-callosal bundle | ||||
| Turton et al,2007 [68] | 8 | ↓ motor response to TMS | ||||
| Alexander et al, 2007 [14] | 22 | ↑ CSF Calcium and glutamate | ||||
| ↑ CSF Glial fibrillary acidic protein | ||||||
| ↑ CSF Nitric oxide metabolites | ||||||
| Uçeyler et al, 2007 [70] | 40 | ↓ mRNA IL-4, IL-8, IL-10 | ||||
| ± transforming growth factor-b1mRNA | ||||||
| ↑ TNF and IL-2 mRNA level | ||||||
| Janicki et al, 2016 [40] | 230 | ±Common Single Nucleotide Polymorphisms | ||||
| Shiraishi et al, 2006 [65] | 18 | ↑ activity in somatosensory cortex | ||||
| ↓ contralateral activity in specific motor areas | ||||||
| Huygen et al, 2004 [39] | 20 | ± prostaglandin E2 | ||||
| Eisenberg et al, 2004 [30] | 38 | ±Endothelin-1 | ||||
| CSF: Cerebrospinal fluid; IL: Interleukins; GM-CSF: Granulocyte-macrophage colony-stimulating factor; tCr =total creatine levels; * N-acetylaspartate, tCr and potassium; TMS : transmagnetic strimulation;; AA: Aminoacids; ± No difference /correlation | ||||||
Genetic and epigenetics
In one study, five top hub genes: MMP9, PTGS2, CXCL8, OSM, TLN1 were identified to be correlated with the development of CRPS [7].
Specific microRNA, hsa-miR-532-3p were found in patients with increased Vascular endothelial growth factor [55] in patients with CRPS. In another study no correlation between transforming growth factor-b1mRNA and CRPS was found [70].
Brain structural and functional alterations
Volume reduction of grey matter in somatosensory cortex, limbic system prefrontal cortex and pain related areas in brain magnetic resonance was demonstrated in CPRS patients [18,29,31,52,66] (Table 2). In a single study it was demonstrated an increase volume of choroid plexus in patients with CRPS [76]. The density of gray matter in the dorsomedial prefrontal cortex was found to be increased in a single study [57].
Disruption of interactions between specific central and metabolic metabolites in the thalamus was reported in one study [42] (Table 2). A low perfusion in somatosensory cortex, and limbic system (early phase) and a high perfusion in somatosensory cortex, and limbic system (late phase) was shown in patients with CPRS [66] and high activity in somatosensory cortex and a low activity in specific motor areas was also described in CPRS patients [65] (Table 2). Table 2 shows that in 11 studies, functional brain alterations such as sustained somatotopic alteration of the somatosensory cortex [36,37]; high localized activation in the primary somatosensory cortex [25,53,68,69]; increased functional connectivity in the somatosensory subnetworks and low functional connectivity in the prefronto-parieto-cingulo-thalamic subnetworks [16,35]; high Basal ganglia infra-slow oscillations and resting connectivity [51]; increased thalami functional connectivity [26]; diminished activation of subthalamic nucleus, nucleus accumbens, and putamen [46].
Other biomarkers
The presence of high NMDA excitatory amino acids (glutamate, glutamine, glycine, taurine and arginine) and high level of serotonin were present in CRPS patients [73]; elevated pro-excitatory aminoacids such a L-Aspartate, L-glutamate, L-ornithine [13]; and vascular endothelial growth factor [55] was demonstrated in CPRS patients. Likewise, patients with CPRS also expressed increased levels of pro-excitatory cerebrospinal (CSF) calcium and glutamate [14] ( (Table 2). The presence of low activity of angiotensin-converting enzyme [49] and low tryptophan was found in CRPS patients [60]. In a single study, patients with CPRS expressed high levels of osteoprotegerin, a glycoprotein central to bone turnover [50].
Quality Assessment of the Studies
Eleven (19%) of the studies were cross-sectional (Table 3), while most studies were case-control (47/81%) (Table 4). No studies were classified as unsatisfactory based on the Newcastle-Ottawa Scale assessment. The majority were of good quality, with 87.2% (n=41) of case-control studies and 54.5% (n=6) of cross-sectional studies scoring ≥7. The main quality issues identified were the lack of satisfactory justifications and inappropriate selection of cases and controls.
| Table 3. Evaluation of the Quality of Cross-sectional Studies Based on the Newcastle-Ottawa Scale | |||||||
| Newcastle-Ottawa Scale Items | |||||||
| Study | S1 | S2 | S3 | S4 | C | O | Total |
| Hartmannsberger et al, 2024 [32] | * | - | * | ** | * | ** | 7 |
| Delon-Martin et al, 2024 [25] | * | - | * | ** | * | ** | 7 |
| Bharwani et al, 2020 [19] | * | - | * | ** | * | ** | 7 |
| Baerlecken et al, 2019 [17] | * | - | * | ** | * | *** | 9 |
| Dirckx et al, 2015 [28] | * | - | * | ** | * | ** | 7 |
| Kohr et al, 2011 [47] | * | - | * | ** | * | * | 6 |
| Alexander et al, 2007 [14] | * | - | * | ** | - | * | 5 |
| Heijmans-Antonissen et al, 2006 [33] | * | - | * | ** | * | * | 6 |
| Alexander et al,2005 [15] | * | - | * | ** | * | ** | 7 |
| Blaes et al, 2004 [22] | * | - | * | * | * | * | 5 |
| Blair et al, 1998 [23] | * | - | * | * | * | * | 5 |
| Abbreviations: S= Selection; S1, representativeness; S2, selection of the unexposed; S3,exposure determination; S4,outcome not present at the beginning of the study C: Comparability; B; O: OutcomesGreen 7(good); orange:5.6(satisfactory); red: 4(unsatisfactory). | |||||||
| Table 4. Evaluation of the Quality of Case Controls Based on the Newcastle-Ottawa Scale | |||||||
| Newcastle-Ottawa Scale Items | |||||||
| Study | S1 | S2 | S3 | S4 | C | E | Total |
| Shaikh et al,2024 [64] | * | * | * | * | ** | *** | 9 |
| Hok et al, 2024 [34] | * | * | - | * | ** | ** | 7 |
| Hotta et al, 2023 [37] | * | * | * | * | ** | ** | 8 |
| Hong et al, 2023 [35] | * | * | * | * | ** | ** | 8 |
| Zhu et al, 2023 [7] | * | * | * | * | ** | *** | 9 |
| Lee et al, 2022 [51] | * | * | * | * | ** | ** | 8 |
| Parkitny et al, 2022 [56] | * | * | - | * | ** | *** | 8 |
| Orlova et al 2011 [55] | * | * | - | * | ** | ** | 7 |
| König et al, 2021 [49] | * | * | - | * | ** | ** | 7 |
| Domim et al, 2021 [29] | |||||||
| Azqueta-Gavaldon et al, 2020 [16] | * | * | - | * | ** | ** | 7 |
| Russo et al, 2020 [60] | * | * | - | * | ** | ** | 7 |
| Di Pietro et al,2020 [26] | * | * | - | * | ** | ** | 7 |
| Russo et al, 2019 [61] | * | * | - | * | * | ** | 6 |
| Kohler et al, 2019 [46] | * | * | * | * | ** | ** | 8 |
| Jung et al, 2019 [42] | * | * | - | * | ** | ** | 7 |
| Jung et al, 2018 [43] | * | * | - | * | * | ** | 6 |
| Bruehl et al, 2019 [24] | * | * | - | * | ** | *** | 8 |
| Wesseldijk et al,2009 [71] | * | * | * | * | ** | *** | 9 |
| Wesseldijk et al,2008 [74] | * | * | - | * | ** | ** | 7 |
| Shokouhi et al 2017 [66] | * | * | - | * | ** | ** | 7 |
| Bharwani et al, 2017 [9] | * | * | - | * | ** | ** | 7 |
| Hotta et al, 2017 [36] | * | * | - | * | ** | * | 6 |
| Yetişgin et al, 2016 [75] | * | * | - | * | ** | ** | 7 |
| Zhou et al, 2015 [76] | * | * | - | * | ** | ** | 7 |
| Lee et al, 2015 [52] | * | * | * | * | ** | ** | 8 |
| Dirckx et al, 2015 [27] | * | * | - | * | ** | ** | 7 |
| Barad et al, 2014 [18] | * | * | - | * | ** | ** | 7 |
| Krämer et al, 2014 [50] | * | * | - | * | ** | ** | 7 |
| Birklein et al,2014 [21] | * | * | * | * | ** | ** | 8 |
| Pleger et al,2014 [57] | * | * | * | * | ** | ** | 8 |
| Jin et al, 2013 [41] | * | * | * | * | ** | *** | 9 |
| Alexander et al, 2013 [13] | * | - | - | * | ** | ** | 6 |
| Lenz et 2011 [53] | * | * | * | * | ** | *** | 9 |
| Ritz et al, 2011 [59] | * | * | * | * | ** | ** | 8 |
| Walton et al, 2010 [69] | * | * | - | * | ** | ** | 7 |
| Kaufmann et al, 2009 [45] | * | - | - | * | * | ** | 5 |
| Kohr et al, 2009 [48] | * | * | * | * | ** | ** | 8 |
| Schinkel et al, 2009 [62] | * | * | * | * | ** | ** | 8 |
| Geha et al, 2008 [31] | * | * | - | * | ** | ** | 7 |
| Wesseldijk et al, 2008 [73] | * | * | - | * | ** | ** | 7 |
| Wesseldijk et al, 2008 b)[72] | * | * | - | * | ** | ** | 7 |
| Kaufmann et al.,2007 [44] | * | - | - | * | * | *** | 6 |
| Uçeyler et al, 2007 [70] | * | * | - | * | ** | ** | 7 |
| Turton et al, 2007 [68] | * | * | - | * | ** | ** | 7 |
| Janicki et al, 2016 [40] | * | * | - | * | ** | ** | 7 |
| Schinkel et al,2006 [63] | * | * | * | * | ** | *** | 9 |
| Shiraishi et al,2006 [65] | * | * | - | * | ** | ** | 7 |
| Munnikes et al, 2005 [54] | * | - | - | * | ** | ** | 6 |
| Tan et al, 2005 [67] | * | * | - | * | ** | ** | 7 |
| Eisenberg et al,2004 [30] | * | * | - | * | ** | *** | 8 |
| Huygen et al, 2004 [39] | * | * | - | * | ** | ** | 7 |
| Huygen et al, 2002 [38] | * | * | - | * | ** | ** | 7 |
| Birklein et al, 2001 [20] | * | * | - | * | ** | ** | 7 |
| Ribbers et al, 1998 [58] | * | * | * | * | ** | ** | 8 |
| Abbreviations: S1 case definition; S2 case representativenes; S3 control seletion, S4 control definition; C: Comparability; E, Exposure.Green ≥7(good); Orange:5.6 (satisfactory); red: ≤4 (unsatisfactory). | |||||||
4. Discussion
The diagnosis of CRPS is supported by relatively subjective clinical criteria, with no single confirmatory test, which may lead to uncertainty and delays in the diagnosis. In addition, CRPS is heterogeneous with frequent discrepancy between clinical complains and findings in the physical exam [77]. The most frequently studied biomarkers were related to systemic [27,54,58,60], local [21,33,55,59,67,74] and CNS inflammation [14,15].
As in other predominantly localized inflammation conditions such as organ specific auto-immune diseases [78], in CRPS, the blood based general distribution of immune or inflammatory cells [44,58,59,62,63,70,75], and of non-specific inflammatory proteins such as C reactive protein, sedimentation velocity was comparable to controls [62,63,70,75].
On the other hand, our systematic review suggests the existence of distinct specific immune cellular signature, namely elevated proinflammatory CD14+ CD16+ monocytes [59], reduction of cytotoxic CD8+ lymphocytes and IL-2-producing T cell [44], and of central memory CD8+, CD4+ T lymphocytes [61] has been shown in CPRS. The documentation of elevated biomarkers of pathogenic T-cell activation such as serum soluble interleukin-2 receptor (sIL-2R) [9,19,62,63] dendritic cell tissue trafficking as p38 phosphorylation [61] further validates the role of specific cell activation in CPRS.
The results from studies aiming to evaluate the systemic levels of pro-inflammatory cytokines, mostly TNF-α, IL-6, IL-8, show contradictory results, with some showing higher levels [27,63] and other normal levels [55,56,59,62,70]. The intra and inter-variation of systemic levels of these pro-inflammatory biomarkers may be caused by inconsistent systemic spill of local inflammatory products [62]. This variation can impact the results in small studies. However in the CSF the levels of IL-6, IL-1, TNF-α were found to be elevated [14,15,70] in CRPS. The finding of increased pro-inflammatory cytokines, such as TNF-α, IL-6, and IL-1β, in local tissues [74] indicates an ongoing inflammatory response in CRPS. The local infiltration of immune cells [21,32,33,38,67] further reinforces the presence of local inflammation.
The presence of biomarkers of mast cell activation, infiltration [21,32] and elevation of tryptase [21,39] in some, but not all [71] noted in CRPS affected tissues, can also explain the disproportionate pain in CPRS patients. These biomarkers are not stable thorough the duration of disease, with the disappearance of mast cell infiltration with chronicity [32]. No differences between CPRS and controls were found for biomarkers such as vasoactive mediators (prostaglandin E2, endothelin-1) [30,39].
Indeed, our systematic review further validates the concept of a dynamic nature of diagnostic inflammatory biomarkers in CRPS [10]. In long lasting CRPS, the local and systemic levels of proinflammatory cytokines (TNF,IL6,IL-8) decreased with time, with dissipation or absence of the differences to controls in the intermediate to chronic stages [54,74]. The levels of proinflammatory biomarkers is similar among different severity degree of chronic CRPS [79] and treatment with prednisone caused reduction the level of the pro-inflammatory biomarker TNF-α and increasing of the anti-inflammatory IL-10 [80].
The contribution of inflammation is also demonstrated by the documentation of biomarkers of upregulation of mRNA expression levels related to pro-inflammatory cytokines, neuropeptides [55,70], expression of specific pro-inflammatory genes (MMP9, PTGS2, CXCL8, OSM, TLN1) [7,41]. Epigenetic modifications, such as altered DNA methylation of specific genes (COL11A1, HLA-DRB6) [24] may also be relevant in CRPS.
Of note, administration of infliximab, an TNF-alpha inhibitor in two patients with CRPS was associated with significant improvement in two patients. In both patients, it was documented a parallel local decline of TNF-alpha and IL-6 [81], suggesting that both interleukins can be biomarkers of clinical response. However, in a subsequent clinical trial the potential of rituximab as a treatment option for CRPS was not confirmed [82].
The levels of calcitonin Gene-Related Peptide, bradykinin, substance P but not neurokinin is consistent with ongoing peripheral nervous system inflammation [20,23,62,63]. CPRS can result from activation and sensitization of peripheral primary afferents by local pro-inflammatory environment. One can speculate that in susceptible patients, the initial inflammatory response is not suppressed or is amplified. Neuropeptides further sensitize primary peripheral afferent neurons as well ascending second order neurons in the spinal cord [20]. Peripheral sensitization of nociceptors [83] and CNS inflammation and functional adaptations may account for the persistence of hypersensitivity and pain at rest. Accordingly, quantitative sensory tests demonstrate the presence of decreased pain thresholds in the affected side by CPRS [84]. As for interleukins, the levels of neuropeptides change with chronification, with studies showing normalization CGRP associated with improvement of local inflammation [20], or absence of differences between CRPS and controls or even lower levels in patients with chronic CRPS [62,63]. For substance P, the shift was also demonstrated with increased levels in acute [62,63] and normal levels in chronic patients [62].
There are different sequential stages of CRPS, with stage I (first 3 months) characterized by predominant inflammation; stage II (3-6 months); and late stage or stage III (after 6 months) being characterized by trophic changes [77]. The normalization or decrease of pro-inflammatory biomarkers is in alignment with CRPS chronicity.
Few studies have addressed the possible role of imaging biomarkers in CRPS. Increased FDG uptake in the brain suggesting heightened neuroinflammatory activity in pain-processing regions, such as the thalamus and insular cortex [65]; and the evidence of local brain functioning or dysfunctional connectivity in the brain regions responsible for motor or sensory processing such as the anterior cingulate cortex, prefrontal cortex, thalamus and amygdala [25,26,35,36,37,46,51,53,66,68] suggest a secondary chronic process of brain maladaptive plasticity in CRPS. The demonstration of hyperactivated endocannabinoid system with origin in the periphery [45] at least in part, may justify the abnormalities found in CNS, particular the areas involved in sensory processing.
The possible role of autoimmunity is yet to be elucidated. The meaning and potential role as biomarkers of autoantibodies such as IgG anti-Myenteric plexus, IgG to SH-SY5Y (inducible autonomic nervous system autoantigen), IgG to P29ING4, IgG to b2 adrenergic and/or the muscarinic-2 receptors, antineuronal IgG , antinuclear IgG [17,22,28,47,48] need to be clarified.
Our review shows that integration of the different inflammatory, endothelial, epigenetic and brain potential diagnostic biomarkers in CRPS is complex as they most likely represent different disease mechanisms not necessary occurring at the same stage of phase CRPS.
5. Conclusions
Our review shows that integration of the different inflammatory, endothelial, epigenetic and brain potential diagnostic biomarkers in CRPS is complex as they most likely represent different disease mechanisms not necessary occurring at the same stage of phase CRPS. .
Author Contributions
Conceptualization, RL SP and H.N.; methodology, R.L.; validation, R.L., S.P. and H,B; formal analysis, R,L, H.N.; investigation, RL, AS, TG, JR, IR, BP, IN, DA, JB, HB, MB, resources, RL and HN; data curation, RL and HN; writing R.L, IN and HN; visualization, RL, AS, TG, JR, IR, BP, IN, DA, JB, HB, MB, SP, IN and HN.; supervision, R.L, H.N.;. All authors have read and agreed to the published version of the manuscript.”
Funding
This research was funded by the ALGARVE BIOMEDICAL CENTER and the Loulé municipality from Algarve. Município de Loulé.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Van Velzen, G.A.J.; Perez, R.S.G.M.; Van Gestel, M.A.; Huygen, F.J.P.M.; Van Kleef, M.; Van Eijs, F.; Dahan, A.; Van Hilten, J.J.; Marinus, J. Health-Related Quality of Life in 975 Patients with Complex Regional Pain Syndrome Type 1. Pain 2014, 155, 629–634. [Google Scholar] [CrossRef]
- Harden, R.N.; McCabe, C.S.; Goebel, A.; Massey, M.; Suvar, T.; Grieve, S.; Bruehl, S. Complex Regional Pain Syndrome: Practical Diagnostic and Treatment Guidelines, 5th Edition. Pain Med. 2022, 23, S1–S53. [Google Scholar] [CrossRef]
- Goebel, A.; Barker, C.; Birklein, F.; Brunner, F.; Casale, R.; Eccleston, C.; Eisenberg, E.; McCabe, C.S.; Moseley, G.L.; Perez, R.; et al. Standards for the Diagnosis and Management of Complex Regional Pain Syndrome: Results of a European Pain Federation Task Force. Eur. J. Pain 2019, 23, 641–651. [Google Scholar] [CrossRef]
- Limerick, G.; Christo, D.K.; Tram, J.; Moheimani, R.; Manor, J.; Chakravarthy, K.; Karri, J.; Christo, P.J. Complex Regional Pain Syndrome: Evidence-Based Advances in Concepts and Treatments. Curr. Pain Headache Rep. 2023, 27, 269–298. [Google Scholar] [CrossRef] [PubMed]
- Bruehl, S. Complex Regional Pain Syndrome. BMJ 2015, 351, h2730. [Google Scholar] [CrossRef]
- Mangnus, T.J.P.; Bharwani, K.D.; Dirckx, M.; Huygen, F.J.P.M. From a Symptom-Based to a Mechanism-Based Pharmacotherapeutic Treatment in Complex Regional Pain Syndrome. Drugs 2022, 82, 511–531. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Wen, B.; Xu, L.; Huang, Y. Identification of Potential Inflammation-Related Genes and Key Pathways Associated with Complex Regional Pain Syndrome. Biomolecules 2023, 13, 772. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.; Li, Z.-Y.; Yu, Y.; Yang, Y.; Ni, M.-H.; Xie, H.; Wang, W.; Huang, Y.-X.; Li, J.-L.; Cui, G.-B.; et al. Gray Matter Abnormalities in Patients with Complex Regional Pain Syndrome: A Systematic Review and Meta-Analysis of Voxel-Based Morphometry Studies. Brain Sci. 2022, 12, 1115. [Google Scholar] [CrossRef]
- Bharwani, K.D.; Dirckx, M.; Stronks, D.L.; Dik, W.A.; Schreurs, M.W.J.; Huygen, F.J.P.M. Elevated Plasma Levels of sIL-2R in Complex Regional Pain Syndrome: A Pathogenic Role for T-Lymphocytes? Mediators Inflamm. 2017, 2017, 2764261. [Google Scholar] [CrossRef]
- Parkitny, L.; McAuley, J.H.; Di Pietro, F.; Stanton, T.R.; O’Connell, N.E.; Marinus, J.; Van Hilten, J.J.; Moseley, G.L. Inflammation in Complex Regional Pain Syndrome: A Systematic Review and Meta-Analysis. Neurology 2013, 80, 106–117. [Google Scholar] [CrossRef]
- Birklein, F.; Schmelz, M. Neuropeptides, Neurogenic Inflammation and Complex Regional Pain Syndrome (CRPS). Neurosci. Lett. 2008, 437, 199–202. [Google Scholar] [CrossRef]
- Well, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The NewcastleOttawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analysis. Available online: https://www.ohri.ca/oxford (accessed on 11 January 2024).
- Alexander, G.M.; Reichenberger, E.; Peterlin, B.L.; Perreault, M.J.; Grothusen, J.R.; Schwartzman, R.J. Plasma Amino Acids Changes in Complex Regional Pain Syndrome. Pain Res. Treat. 2013, 2013, 742407. [Google Scholar] [CrossRef] [PubMed]
- Alexander, G.M.; Perreault, M.J.; Reichenberger, E.R.; Schwartzman, R.J. Changes in Immune and Glial Markers in the CSF of Patients with Complex Regional Pain Syndrome. Brain. Behav. Immun. 2007, 21, 668–676. [Google Scholar] [CrossRef]
- Alexander, G.M.; van Rijn, M.A.; van Hilten, J.J.; Perreault, M.J.; Schwartzman, R.J. Changes in Cerebrospinal Fluid Levels of Pro-Inflammatory Cytokines in CRPS. Pain 2005, 116, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Azqueta-Gavaldon, M.; Youssef, A.M.; Storz, C.; Lemme, J.; Schulte-Göcking, H.; Becerra, L.; Azad, S.C.; Reiners, A.; Ertl-Wagner, B.; Borsook, D.; et al. Implications of the Putamen in Pain and Motor Deficits in Complex Regional Pain Syndrome. Pain 2020, 161, 595–608. [Google Scholar] [CrossRef] [PubMed]
- Baerlecken, N.T.; Gaulke, R.; Pursche, N.; Witte, T.; Karst, M.; Bernateck, M. Autoantibodies against P29ING4 Are Associated with Complex Regional Pain Syndrome. Immunol. Res. 2019, 67, 461–468. [Google Scholar] [CrossRef]
- Barad, M.J.; Ueno, T.; Younger, J.; Chatterjee, N.; Mackey, S. Complex Regional Pain Syndrome Is Associated with Structural Abnormalities in Pain-Related Regions of the Human Brain. J. Pain 2014, 15, 197–203. [Google Scholar] [CrossRef]
- Bharwani, K.D.; Dirckx, M.; Stronks, D.L.; Dik, W.A.; Huygen, F.J.P.M.; Dozio, E. Serum Soluble Interleukin-2 Receptor Does Not Differentiate Complex Regional Pain Syndrome from Other Pain Conditions in a Tertiary Referral Setting. Mediators Inflamm. 2020, 2020, 1–10. [Google Scholar] [CrossRef]
- Birklein, F.; Schmelz, M.; Schifter, S.; Weber, M. The Important Role of Neuropeptides in Complex Regional Pain Syndrome. Neurology 2001, 57, 2179–2184. [Google Scholar] [CrossRef]
- Birklein, F.; Drummond, P.D.; Li, W.; Schlereth, T.; Albrecht, N.; Finch, P.M.; Dawson, L.F.; Clark, J.D.; Kingery, W.S. Activation of Cutaneous Immune Responses in Complex Regional Pain Syndrome. J. Pain 2014, 15, 485–495. [Google Scholar] [CrossRef]
- Blaes, F.; Schmitz, K.; Tschernatsch, M.; Kaps, M.; Krasenbrink, I.; Hempelmann, G.; Bräu, M.E. Autoimmune Etiology of Complex Regional Pain Syndrome (M. Sudeck). Neurology 2004, 63, 1734–1736. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.J.; Chinthagada, M.; Hoppenstehdt, D.; Kijowski, R.; Fareed, J. Role of Neuropeptides in Pathogenesis of Reflex Sympathetic Dystrophy. Acta Orthop. Belg. 1998, 64, 448–451. [Google Scholar]
- Bruehl, S.; Gamazon, E.R.; Van De Ven, T.; Buchheit, T.; Walsh, C.G.; Mishra, P.; Ramanujan, K.; Shaw, A. DNA Methylation Profiles Are Associated with Complex Regional Pain Syndrome after Traumatic Injury. Pain 2019, 160, 2328–2337. [Google Scholar] [CrossRef]
- Delon-Martin, C.; Lefaucheur, J.-P.; Hodaj, E.; Sorel, M.; Dumolard, A.; Payen, J.-F.; Hodaj, H. Neural Correlates of Pain-Autonomic Coupling in Patients With Complex Regional Pain Syndrome Treated by Repetitive Transcranial Magnetic Stimulation of the Motor Cortex. Neuromodulation J. Int. Neuromodulation Soc. 2024, 27, 188–199. [Google Scholar] [CrossRef]
- Di Pietro, F.; Lee, B.; Henderson, L.A. Altered Resting Activity Patterns and Connectivity in Individuals with Complex Regional Pain Syndrome. Hum. Brain Mapp. 2020, 41, 3781–3793. [Google Scholar] [CrossRef] [PubMed]
- Dirckx, M.; Stronks, D.L.; van Bodegraven-Hof, E. a. M.; Wesseldijk, F.; Groeneweg, J.G.; Huygen, F.J.P.M. Inflammation in Cold Complex Regional Pain Syndrome. Acta Anaesthesiol. Scand. 2015, 59, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Dirckx, M.; Schreurs, M.W.J.; de Mos, M.; Stronks, D.L.; Huygen, F.J.P.M. The Prevalence of Autoantibodies in Complex Regional Pain Syndrome Type I. Mediators Inflamm. 2015, 2015, 718201. [Google Scholar] [CrossRef]
- Domin, M.; Strauss, S.; McAuley, J.H.; Lotze, M. Complex Regional Pain Syndrome: Thalamic GMV Atrophy and Associations of Lower GMV With Clinical and Sensorimotor Performance Data. Front. Neurol. 2021, 12, 722334. [Google Scholar] [CrossRef]
- Eisenberg, E.; Erlich, T.; Zinder, O.; Lichinsky, S.; Diamond, E.; Pud, D.; Davar, G. Plasma Endothelin-1 Levels in Patients with Complex Regional Pain Syndrome. Eur. J. Pain Lond. Engl. 2004, 8, 533–538. [Google Scholar] [CrossRef]
- Geha, P.Y.; Baliki, M.N.; Harden, R.N.; Bauer, W.R.; Parrish, T.B.; Apkarian, A.V. The Brain in Chronic CRPS Pain: Abnormal Gray-White Matter Interactions in Emotional and Autonomic Regions. Neuron 2008, 60, 570–581. [Google Scholar] [CrossRef]
- Hartmannsberger, B.; Scriba, S.; Guidolin, C.; Becker, J.; Mehling, K.; Doppler, K.; Sommer, C.; Rittner, H.L. Transient Immune Activation without Loss of Intraepidermal Innervation and Associated Schwann Cells in Patients with Complex Regional Pain Syndrome. J. Neuroinflammation 2024, 21, 23. [Google Scholar] [CrossRef]
- Heijmans-Antonissen, C.; Wesseldijk, F.; Munnikes, R.J.; Huygen, F.J.; van der Meijden, P.; Hop, W.C.J.; Hooijkaas, H.; Zijlstra, F.J. Multiplex Bead Array Assay for Detection of 25 Soluble Cytokines in Blister Fluid of Patients with Complex Regional Pain Syndrome Type 1. Mediators Inflamm. 2006, 2006, 28398. [Google Scholar] [CrossRef] [PubMed]
- Hok, P.; Strauss, S.; McAuley, J.; Domin, M.; Wang, A.P.; Rae, C.; Moseley, G.L.; Lotze, M. Functional Connectivity in Complex Regional Pain Syndrome: A Bicentric Study. NeuroImage 2024, 301, 120886. [Google Scholar] [CrossRef]
- Hong, H.; Suh, C.; Namgung, E.; Ha, E.; Lee, S.; Kim, R.Y.; Song, Y.; Oh, S.; Lyoo, I.K.; Jeong, H.; et al. Aberrant Resting-State Functional Connectivity in Complex Regional Pain Syndrome: A Network-Based Statistics Analysis. Exp. Neurobiol. 2023, 32, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Hotta, J.; Saari, J.; Koskinen, M.; Hlushchuk, Y.; Forss, N.; Hari, R. Abnormal Brain Responses to Action Observation in Complex Regional Pain Syndrome. J. Pain 2017, 18, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Hotta, J.; Saari, J.; Harno, H.; Kalso, E.; Forss, N.; Hari, R. Somatotopic Disruption of the Functional Connectivity of the Primary Sensorimotor Cortex in Complex Regional Pain Syndrome Type 1. Hum. Brain Mapp. 2023, 44, 6258–6274. [Google Scholar] [CrossRef]
- Huygen, F.J.P.M.; De Bruijn, A.G.J.; De Bruin, M.T.; Groeneweg, J.G.; Klein, J.; Zijlstra, F.J. Evidence for Local Inflammation in Complex Regional Pain Syndrome Type 1. Mediators Inflamm. 2002, 11, 47–51. [Google Scholar] [CrossRef]
- Huygen, F.J.P.M.; Ramdhani, N.; van Toorenenbergen, A.; Klein, J.; Zijlstra, F.J. Mast Cells Are Involved in Inflammatory Reactions during Complex Regional Pain Syndrome Type 1. Immunol. Lett. 2004, 91, 147–154. [Google Scholar] [CrossRef]
- Janicki, P.K.; Alexander, G.M.; Eckert, J.; Postula, M.; Schwartzman, R.J. Analysis of Common Single Nucleotide Polymorphisms in Complex Regional Pain Syndrome: Genome Wide Association Study Approach and Pooled DNA Strategy. Pain Med. Malden Mass 2016, 17, 2344–2352. [Google Scholar] [CrossRef]
- Jin, E.-H.; Zhang, E.; Ko, Y.; Sim, W.S.; Moon, D.E.; Yoon, K.J.; Hong, J.H.; Lee, W.H. Genome-Wide Expression Profiling of Complex Regional Pain Syndrome. PLoS ONE 2013, 8, e79435. [Google Scholar] [CrossRef]
- Jung, Y.-H.; Kim, H.; Lee, D.; Lee, J.-Y.; Lee, W.J.; Moon, J.Y.; Kim, Y.C.; Choi, S.-H.; Kang, D.-H. Disruption of Homeostasis Based on the Right and Left Hemisphere in Patients with Complex Regional Pain Syndrome. Neuroimmunomodulation 2019, 26, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.-H.; Kim, H.; Jeon, S.Y.; Kwon, J.M.; Lee, D.; Choi, S.-H.; Kang, D.-H. Aberrant Interactions of Peripheral Measures and Neurometabolites with Lipids in Complex Regional Pain Syndrome Using Magnetic Resonance Spectroscopy: A Pilot Study. Mol. Pain 2018, 14, 1744806917751323. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, I.; Eisner, C.; Richter, P.; Huge, V.; Beyer, A.; Chouker, A.; Schelling, G.; Thiel, M. Lymphocyte Subsets and the Role of Th1/Th2 Balance in Stressed Chronic Pain Patients. Neuroimmunomodulation 2007, 14, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, I.; Hauer, D.; Huge, V.; Vogeser, M.; Campolongo, P.; Chouker, A.; Thiel, M.; Schelling, G. Enhanced Anandamide Plasma Levels in Patients with Complex Regional Pain Syndrome Following Traumatic Injury: A Preliminary Report. Eur. Surg. Res. Eur. Chir. Forsch. Rech. Chir. Eur. 2009, 43, 325–329. [Google Scholar] [CrossRef]
- Kohler, M.; Strauss, S.; Horn, U.; Langner, I.; Usichenko, T.; Neumann, N.; Lotze, M. Differences in Neuronal Representation of Mental Rotation in Patients With Complex Regional Pain Syndrome and Healthy Controls. J. Pain 2019, 20, 898–907. [Google Scholar] [CrossRef]
- Kohr, D.; Singh, P.; Tschernatsch, M.; Kaps, M.; Pouokam, E.; Diener, M.; Kummer, W.; Birklein, F.; Vincent, A.; Goebel, A.; et al. Autoimmunity against the Β2 Adrenergic Receptor and Muscarinic-2 Receptor in Complex Regional Pain Syndrome. Pain 2011, 152, 2690–2700. [Google Scholar] [CrossRef]
- Kohr, D.; Tschernatsch, M.; Schmitz, K.; Singh, P.; Kaps, M.; Schäfer, K.-H.; Diener, M.; Mathies, J.; Matz, O.; Kummer, W.; et al. Autoantibodies in Complex Regional Pain Syndrome Bind to a Differentiation-Dependent Neuronal Surface Autoantigen. Pain 2009, 143, 246–251. [Google Scholar] [CrossRef]
- König, S.; Steinebrey, N.; Herrnberger, M.; Escolano-Lozano, F.; Schlereth, T.; Rebhorn, C.; Birklein, F. Reduced Serum Protease Activity in Complex Regional Pain Syndrome: The Impact of Angiotensin-Converting Enzyme and Carboxypeptidases. J. Pharm. Biomed. Anal. 2021, 205, 114307. [Google Scholar] [CrossRef]
- Krämer, H.H.; Hofbauer, L.C.; Szalay, G.; Breimhorst, M.; Eberle, T.; Zieschang, K.; Rauner, M.; Schlereth, T.; Schreckenberger, M.; Birklein, F. Osteoprotegerin: A New Biomarker for Impaired Bone Metabolism in Complex Regional Pain Syndrome? Pain 2014, 155, 889–895. [Google Scholar] [CrossRef]
- Lee, B.; Di Pietro, F.; Henderson, L.A.; Austin, P.J. Altered Basal Ganglia Infraslow Oscillation and Resting Functional Connectivity in Complex Regional Pain Syndrome. J. Neurosci. Res. 2022, 100, 1487–1505. [Google Scholar] [CrossRef]
- Lee, D.-H.; Lee, K.-J.; Cho, K.I.K.; Noh, E.C.; Jang, J.H.; Kim, Y.C.; Kang, D.-H. Brain Alterations and Neurocognitive Dysfunction in Patients With Complex Regional Pain Syndrome. J. Pain 2015, 16, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Lenz, M.; Höffken, O.; Stude, P.; Lissek, S.; Schwenkreis, P.; Reinersmann, A.; Frettlöh, J.; Richter, H.; Tegenthoff, M.; Maier, C. Bilateral Somatosensory Cortex Disinhibition in Complex Regional Pain Syndrome Type I. Neurology 2011, 77, 1096–1101. [Google Scholar] [CrossRef] [PubMed]
- Munnikes, R.J.M.; Muis, C.; Boersma, M.; Heijmans-Antonissen, C.; Zijlstra, F.J.; Huygen, F.J.P.M. Intermediate Stage Complex Regional Pain Syndrome Type 1 Is Unrelated to Proinflammatory Cytokines. Mediators Inflamm. 2005, 2005, 366–372. [Google Scholar] [CrossRef]
- Orlova, I.A.; Alexander, G.M.; Qureshi, R.A.; Sacan, A.; Graziano, A.; Barrett, J.E.; Schwartzman, R.J.; Ajit, S.K. MicroRNA Modulation in Complex Regional Pain Syndrome. J. Transl. Med. 2011, 9, 195. [Google Scholar] [CrossRef] [PubMed]
- Parkitny, L.; McAuley, J.H.; Herbert, R.D.; Di Pietro, F.; Cashin, A.G.; Ferraro, M.C.; Moseley, G.L. Post-Fracture Serum Cytokine Levels Are Not Associated with a Later Diagnosis of Complex Regional Pain Syndrome: A Case-Control Study Nested in a Prospective Cohort Study. BMC Neurol. 2022, 22, 385. [Google Scholar] [CrossRef]
- Pleger, B.; Draganski, B.; Schwenkreis, P.; Lenz, M.; Nicolas, V.; Maier, C.; Tegenthoff, M. Complex Regional Pain Syndrome Type I Affects Brain Structure in Prefrontal and Motor Cortex. PLoS ONE 2014, 9, e85372. [Google Scholar] [CrossRef]
- Ribbers, G.M.; Oosterhuis, W.P.; van Limbeek, J.; de Metz, M. Reflex Sympathetic Dystrophy: Is the Immune System Involved? Arch. Phys. Med. Rehabil. 1998, 79, 1549–1552. [Google Scholar] [CrossRef]
- Ritz, B.W.; Alexander, G.M.; Nogusa, S.; Perreault, M.J.; Peterlin, B.L.; Grothusen, J.R.; Schwartzman, R.J. Elevated Blood Levels of Inflammatory Monocytes (CD14+ CD16+ ) in Patients with Complex Regional Pain Syndrome. Clin. Exp. Immunol. 2011, 164, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Russo, M.A.; Georgius, P.; Pires, A.S.; Heng, B.; Allwright, M.; Guennewig, B.; Santarelli, D.M.; Bailey, D.; Fiore, N.T.; Tan, V.X.; et al. Novel Immune Biomarkers in Complex Regional Pain Syndrome. J. Neuroimmunol. 2020, 347, 577330. [Google Scholar] [CrossRef]
- Russo, M.A.; Fiore, N.T.; Van Vreden, C.; Bailey, D.; Santarelli, D.M.; McGuire, H.M.; Fazekas De St Groth, B.; Austin, P.J. Expansion and Activation of Distinct Central Memory T Lymphocyte Subsets in Complex Regional Pain Syndrome. J. Neuroinflammation 2019, 16, 63. [Google Scholar] [CrossRef]
- Schinkel, C.; Scherens, A.; Köller, M.; Roellecke, G.; Muhr, G.; Maier, C. Systemic Inflammatory Mediators in Post-Traumatic Complex Regional Pain Syndrome (CRPS I) - Longitudinal Investigations and Differences to Control Groups. Eur. J. Med. Res. 2009, 14, 130–135. [Google Scholar] [CrossRef]
- Schinkel, C.; Gaertner, A.; Zaspel, J.; Zedler, S.; Faist, E.; Schuermann, M. Inflammatory Mediators Are Altered in the Acute Phase of Posttraumatic Complex Regional Pain Syndrome. Clin. J. Pain 2006, 22, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, S.S.; Goebel, A.; Lee, M.C.; Nahorski, M.S.; Shenker, N.; Pamela, Y.; Drissi, I.; Brown, C.; Ison, G.; Shaikh, M.F.; et al. Evidence of a Genetic Background Predisposing to Complex Regional Pain Syndrome Type 1. J. Med. Genet. 2024, 61, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Shiraishi, S.; Kobayashi, H.; Nihashi, T.; Kato, K.; Iwano, S.; Nishino, M.; Ishigaki, T.; Ikeda, M.; Kato, T.; Ito, K.; et al. Cerebral Glucose Metabolism Change in Patients with Complex Regional Pain Syndrome: A PET Study. Radiat. Med. 2006, 24, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Shokouhi, M.; Clarke, C.; Morley-Forster, P.; Moulin, D.E.; Davis, K.D.; St Lawrence, K. Structural and Functional Brain Changes at Early and Late Stages of Complex Regional Pain Syndrome. J. Pain 2018, 19, 146–157. [Google Scholar] [CrossRef]
- Tan, E.C.T.H.; Oyen, W.J.G.; Goris, R.J.A. Leukocytes in Complex Regional Pain Syndrome Type I. Inflammation 2005, 29, 182–186. [Google Scholar] [CrossRef]
- Turton, A.J.; McCabe, C.S.; Harris, N.; Filipovic, S.R. Sensorimotor Integration in Complex Regional Pain Syndrome: A Transcranial Magnetic Stimulation Study. Pain 2007, 127, 270–275. [Google Scholar] [CrossRef]
- Walton, K.D.; Dubois, M.; Llinás, R.R. Abnormal Thalamocortical Activity in Patients with Complex Regional Pain Syndrome (CRPS) Type I. Pain 2010, 150, 41–51. [Google Scholar] [CrossRef]
- Üçeyler, N.; Eberle, T.; Rolke, R.; Birklein, F.; Sommer, C. Differential Expression Patterns of Cytokines in Complex Regional Pain Syndrome. Pain 2007, 132, 195–205. [Google Scholar] [CrossRef]
- Wesseldijk, F.; van Toorenenbergen, A.W.; van Wijk, R.G.; Huygen, F.J.; Zijlstra, F.J. IgE-Mediated Hypersensitivity: Patients with Complex Regional Pain Syndrome Type 1 (CRPS1) vs the Dutch Population. A Retrospective Study. Pain Med. Malden Mass 2009, 10, 172–178. [Google Scholar] [CrossRef]
- Wesseldijk, F.; Fekkes, D.; Huygen, F.J.; Bogaerts-Taal, E.; Zijlstra, F.J. Increased Plasma Serotonin in Complex Regional Pain Syndrome Type 1. Anesth. Analg. 2008, 106, 1862–1867. [Google Scholar] [CrossRef]
- Wesseldijk, F.; Fekkes, D.; Huygen, F.J.P.M.; van de Heide-Mulder, M.; Zijlstra, F.J. Increased Plasma Glutamate, Glycine, and Arginine Levels in Complex Regional Pain Syndrome Type 1. Acta Anaesthesiol. Scand. 2008, 52, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Wesseldijk, F.; Huygen, F.J.P.M.; Heijmans-Antonissen, C.; Niehof, S.P.; Zijlstra, F.J. Six Years Follow-up of the Levels of TNF-Alpha and IL-6 in Patients with Complex Regional Pain Syndrome Type 1. Mediators Inflamm. 2008, 2008, 469439. [Google Scholar] [CrossRef]
- Yetişgin, A.; Tutoğlu, A.; Cinakli, A.; Kul, M.; Boyaci, A. Platelet and Erythrocyte Indexes in Complex Regional Pain Syndrome Type I. Arch. Rheumatol. 2016, 31, 359–362. [Google Scholar] [CrossRef] [PubMed]
- Zhou, G.; Hotta, J.; Lehtinen, M.K.; Forss, N.; Hari, R. Enlargement of Choroid Plexus in Complex Regional Pain Syndrome. Sci. Rep. 2015, 5, 14329. [Google Scholar] [CrossRef] [PubMed]
- Bruehl, S.; Harden, R.N.; Galer, B.S.; Saltz, S.; Backonja, M.; Stanton-Hicks, M. Complex Regional Pain Syndrome: Are There Distinct Subtypes and Sequential Stages of the Syndrome? Pain 2002, 95, 119–124. [Google Scholar] [CrossRef]
- Lesage, S.; Goodnow, C.C. Organ-Specific Autoimmune Disease. J. Exp. Med. 2001, 194, F31–F36. [Google Scholar] [CrossRef]
- Mangnus, T.J.P.; Bharwani, K.D.; Dik, W.A.; Baart, S.J.; Dirckx, M.; Huygen, F.J.P.M. Is There an Association between Serum Soluble Interleukin-2 Receptor Levels and Syndrome Severity in Persistent Complex Regional Pain Syndrome? Pain Med. 2023, 24, 1234–1243. [Google Scholar] [CrossRef]
- Kalita, J.; Shukla, R.; Pandey, P.C. Effect of Prednisolone on Clinical and Cytokine mRNA Profiling in Complex Regional Pain Syndrome. J. Mol. Neurosci. MN 2024, 74, 112. [Google Scholar] [CrossRef]
- Huygen, F.J.P.M.; Niehof, S.; Zijlstra, F.J.; van Hagen, P.M.; van Daele, P.L.A. Successful Treatment of CRPS 1 with Anti-TNF. J. Pain Symptom Manage. 2004, 27, 101–103. [Google Scholar] [CrossRef]
- Dirckx, M.; Groeneweg, G.; Wesseldijk, F.; Stronks, D.L.; Huygen, F.J.P.M. Report of a Preliminary Discontinued Double-Blind, Randomized, Placebo-Controlled Trial of the Anti-TNF-α Chimeric Monoclonal Antibody Infliximab in Complex Regional Pain Syndrome. Pain Pract. Off. J. World Inst. Pain 2013, 13, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Orstavik, K. Pathological C-Fibres in Patients with a Chronic Painful Condition. Brain 2003, 126, 567–578. [Google Scholar] [CrossRef] [PubMed]
- Tahmoush, A.J.; Schwartzman, R.J.; Hopp, J.L.; Grothusen, J.R. Quantitative Sensory Studies in Complex Regional Pain Syndrome Type 1/RSD: Clin. J. Pain 2000, 16, 340–344. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA-Pflow chart of the study inclusion process.
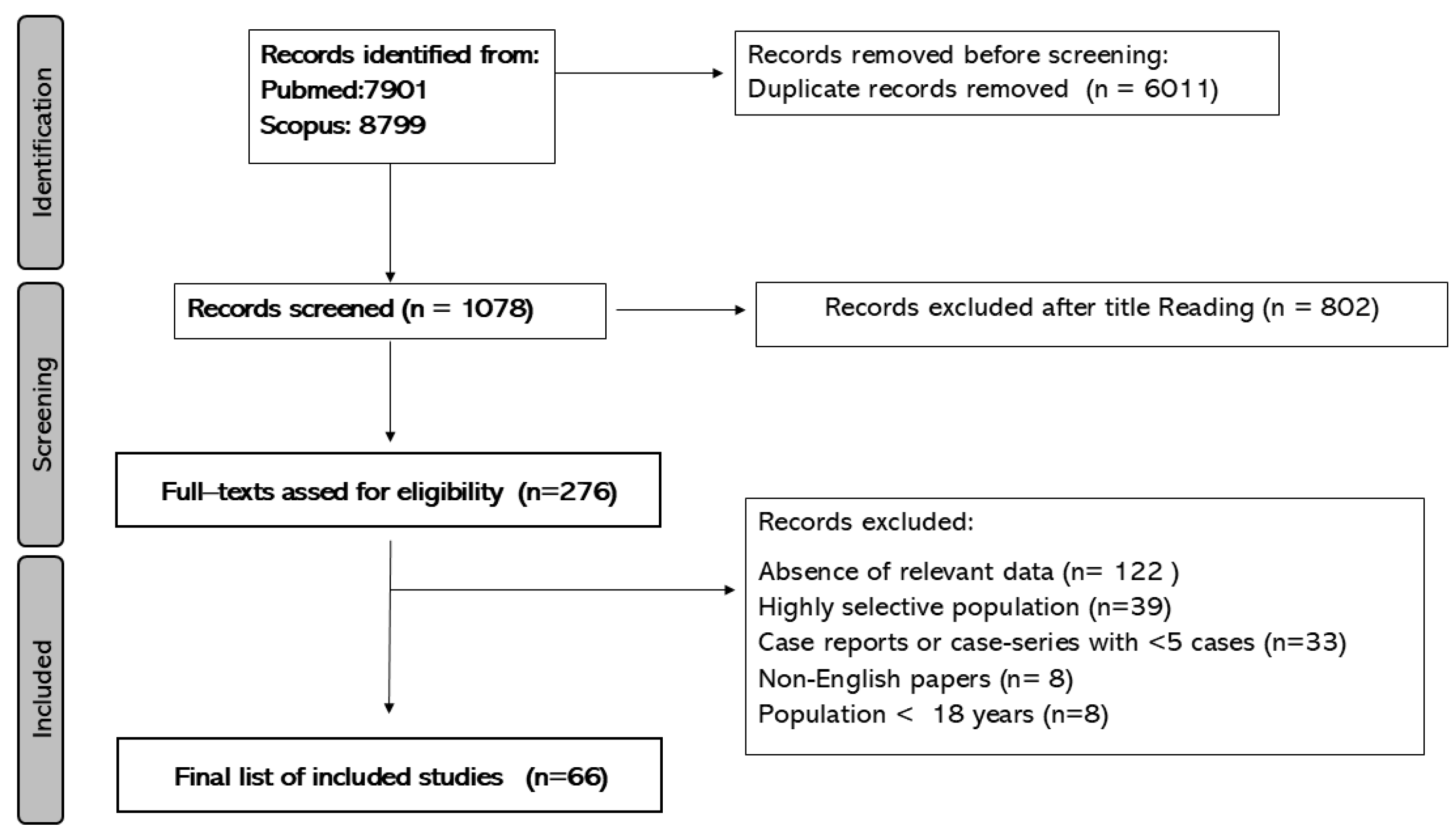
Figure 2.
List of potential diagnostic biomarkers for complex regional pain syndrome identified in the systematic review.
Figure 2.
List of potential diagnostic biomarkers for complex regional pain syndrome identified in the systematic review.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



