
Submitted:
23 April 2025
Posted:
24 April 2025
You are already at the latest version
Abstract
Background: Elexacaftor/tezacaftor/ivacaftor (ETI) treatment is showing remarkable beneficial effects in patients with Cystic Fibrosis (pwCF) harboring the F508del mutation in the Cystic Fibrosis Transmembrane conductance Regulator (CFTR) gene. Although this therapy is generally well tolerated in pwCF, some adverse events (AEs) have been recently described both in controlled studies and in post-marketing observations. Methods: We followed 414 pwCF carrying F508del CFTR that initiated ETI treatment, recording AEs for a period of 5 years. Results: A total of 142 AEs were reported. The most frequent AEs in the whole cohort were liver marker elevation, skin rush, epigastric pain, headache, and depression. Considering pediatric subjects, psychiatric and gastrointestinal disorders were the most frequent AEs. Only one patient reported a severe AE, leading to treatment discontinuation. In case of AEs, different decisions on ETI treatment were made, including temporary interruption and temporary or permanent dosage modification. Conclusions: Throughout the long-term observational period, almost 21% of pwCF experienced at least one AE. Psychiatric disorders, in particular attention deficit, were the most prevalent issue in our pediatric cohort, whereas adult patients mainly reported depression, anxiety and sleep disorders. This study therefore strengthen the recommendation of screening for changes in mental health during ETI treatment. AEs led to the permanent reduction of ETI dosage in 32% of cases, raising the issue of safety in relation to dosage reduction, efficacy, and minimum ETI levels. Eventually, this study highlights the need for a longitudinal monitoring of ETI safety since a significant number of AEs occurred after one year of treatment.
Keywords:
Cystic Fibrosis
; elexacaftor
; tezacaftor
; ivacaftor
; CFTR modulators
; drug safety
1. Introduction
Cystic fibrosis (CF) is an autosomal recessive disorder caused by mutations in the CF transmembrane conductance regulator (CFTR) gene, encoding a chloride and bicarbonate channel essential for the maintenance of the correct salt and water balance at the surface of epithelial cells [1,2].
Although more than 2000 mutations in CFTR have been reported so far, F508del is the most frequent pathogenic variant. This mutation causes misfolding of CFTR protein, leading to a defect in trafficking from the endoplasmic reticulum (ER). Over the past decade, the introduction of CFTR modulator therapies has transformed the CF clinical landscape. The first of these to be developed was the CFTR potentiator ivacaftor, improving CFTR protein function in the apical membrane of epithelial cells [3]. Other CFTR correctors improving the trafficking of unfolded F508del CFTR protein to the cell surface were subsequently developed. Currently, triple-combination elexacaftor-tezacaftor-ivacaftor (ETI) treatment has proved to be highly effective and safe when administered in clinical trials to patients with CF (pwCF), aged 2 years and older, harboring at least one F508del CFTR allele [3,4,5,6,7,8]. Recently, the Food and Drug Administration (FDA) expanded its ETI approval to a total of 272 CFTR mutations, allowing more pwCF to access this treatment.
ETI significantly improved lung function in pwCF, reducing the pulmonary exacerbation rate and decreasing hospitalizations [4]. It also increased body mass index, improved quality of life, decreased the sweat chloride concentration, and reduced infections. In addition, ETI was generally well tolerated in trials [5,7,9,10]: real-world data corroborate these findings, affording a valuable source of evidence on ETI’s tolerability and safety profile [10]. However, some adverse events (AEs) have been described both in controlled studies and in clinical practice. The most commonly reported AEs were increased liver marker levels and headache [3,5,9]. Post-marketing observations have highlighted additional AEs that were previously either not documented or under-reported [11,12,13,14,15], including neuropsychiatric symptoms and dermatologic reactions that required dosage modification or discontinuation of the treatment.
The aim of this study is to report potentially drug-related AEs in a large cohort of pwCF receiving long-term ETI treatment, and to assess their consequences in terms of temporary or permanent drug regimen modification.
2. Materials and Methods
2.1. Study Design and Study Participants
Between October 2019 and December 2024, 414 pwCF regularly attending the Verona Cystic Fibrosis Center initiated ETI treatment. The study was approved by the Ethics Committee of the Azienda Ospedaliera Universitaria Integrata, Verona (approval number 433CET), and informed consent was obtained from all subjects.
Dosage regimens were prescribed in compliance with the package leaflet and Italian Medicines Agency (AIFA) requirements (patients older than 6 years, weighing <30 kg, to receive elexacaftor 100 mg once daily, tezacaftor 50 mg once daily, ivacaftor 75 mg every 12 hours; patients weighing >30 kg to receive elexacaftor 200 mg once daily, tezacaftor 100 mg once daily, ivacaftor 150 mg every 12 hours).
AEs and pulmonary function were assessed quarterly, while a sweat chloride test was recorded annually; blood tests were done in accordance with AIFA guidelines (quarterly during the first year of treatment, then annually).
Percent predicted forced expiratory volume in 1 second (ppFEV1) was obtained by forced spirometry [15]. The parameter is expressed as the mean of measurements collected during consecutive 12-month periods (the year before ETI initiation, and every year of ETI treatment). Prevalence and type of AE were considered, regardless of the need for discontinuation of treatment. Serious AEs (SAEs) were defined in line with FDA and European Medicines Agency (EMA) criteria [16,17]. Identification of severe lung disease was based on ppFEV1 <40 and/or ongoing evaluation for lung transplantation.
2.2. Statistical Analysis
Descriptive statistics were used to summarize patient characteristics: continuous variables were described by median and min-max values, whilst categorical variables were reported by absolute and percentage frequencies. Baseline characteristics were compared between patients presenting AEs events and those with none. Chi-square and Mann-Whitney tests were used for categorical and continuous variables, respectively. The rate of AE occurrence during treatment was calculated, both for the overall period of ETI administration and for the first 30 days alone. Rates are reported as the number of AEs per 1000 days of treatment and were compared in relation to the main patient characteristics, using the Poisson exact test. A p-value <0.05 was considered statistically significant. All analyses were done with the R software (R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org)
3. Results
The evaluation comprised 414 patients older than 6 years (M 46%). One patient underwent lung transplantation after 3 months of treatment with ETI and was lost to follow-up. Patient characteristics are listed in Table 1.
Median duration of ETI treatment was 35.60 months [IQR 26.46 – 39.26]. During the period of observation, 142 AEs were reported, with 85 (20.53%) patients presenting at least one AE. Only one SAE was reported, consisting in epigastric pain which led to hospitalization and discontinuation of the drug. Characteristics of patients presenting AEs are shown in Table 2.
We observed no differences in age, sex, severe respiratory impairment, or genotype between patients with and without AEs (Table 1). AEs mostly occurred either early, within 2 weeks from the initiation of treatment (33%), or later, after 4 weeks of treatment (50.7%). They occurred earlier in PwCF with baseline severe respiratory impairment (35.5 % in patients with baseline ppFEV1 < 40, vs 28.8% in patients with ppFEV1 > 40); in relation to age, 47.6% and 29.46% of AEs occurred within the first 2 weeks in pediatric and adult patients, respectively (Table 2). The most frequent AEs were liver biomarker elevation (16.2%) and skin rash (11.27%), followed by epigastric pain (7.75%), headache (4.2%) and depression (4.2%). We harmonized AEs on the basis of System Organ Class (SOC) [19,20], categorizing anatomical or physiological systems involved: this ensured uniformity in reporting and analyzing data. The most frequent SOCs were psychiatric and investigations, followed by skin and subcutaneous tissue disorders and gastrointestinal disorders (Table 3).
Among the 24 psychiatric AEs as classified by SOC, 70.81% were first occurrences in the patients concerned. Pediatric subjects (n = 20) presented AEs mostly related to psychiatric disorders (7 patients), followed by gastrointestinal (4 patients), skin (4 patients), nervous system (2 patients), investigations (2 patients) and general (1 patient) disorders. Different decisions regarding ETI treatment were made for the 142 AEs reported.
Permanent discontinuation was rare (11% of all AEs), while temporary interruption, temporary dosage modification and permanent dosage modification were chosen in 17%, 25% and 32%, respectively (Figure 1).
Psychiatric disorders, investigation-related alterations, gastrointestinal, nervous system and musculoskeletal disorders most frequently resulted in permanent ETI dosage modification, whereas respiratory disorders, skin and subcutaneous tissue events mostly entailed only temporary dosage modification (Table 4).
4. Discussion
In this study we investigated potentially drug-related AEs in pwCF, treated with ETI in a real-life setting. Key strengths of this observational prospective study are that it encompasses a substantial patient cohort (414 subjects) and an extended follow-up period (median 35.6 months). A major limitation of the study is that it has been carried out in a single center; nevertheless, this also ensured consistency and reliability of the measurements.
Our findings show that 20.53% of the treated cohort experienced at least one AE, whereas a SAE occurred in only one patient (0.25%). Only a few (11%) AEs led to permanent discontinuation of the study treatment (8 pwCF, i.e. 1.9% of the treated cohort). These figures indicate that ETI was quite well tolerated. We observed that 33% and 47% of AEs occurred within 2 and 4 weeks from ETI initiation, respectively; FDA data indicate that the median time of AE onset is 70 days, with the majority occurring within 4 weeks. [21]
Earlier AEs in the pediatric population (2- to 5-year-old and 6- to 11-year-old subgroups) were described using the FDA reporting system, and speculatively attributed to the higher metabolic rate in these age groups [22]. Here, we found that the most frequent AEs were liver function marker elevation, skin rash, epigastric pain, headache and depression; the most frequently involved SOCs were investigations (mostly hepatic enzyme elevation), psychiatric, skin, gastrointestinal and musculoskeletal disorders.
The prevalence of AEs did not differ in pediatric and adult pwCF, regardless of sex, severity of respiratory function impairment, or genotype, this trend being consistent with previously described pediatric data [14]. When considering pediatric pwCF, psychiatric disorders were the most prevalent (35% in our cohort), with the majority of cases involving attention deficit. Conversely, in adult subjects, psychiatric disorders were primarily depression, anxiety and sleep disorders. A recent analysis of the UK adverse drug reaction reporting system for psychiatric events found that the proportion of reported AEs categorised as psychiatric increased in the post-ETI period [23].
Taken together, our data and previous reports suggest that systematic screening of psychiatric conditions needs to be taken into account. The high background prevalence of psychiatric disorders in pwCF has already been described. Although data from the US and German registries showed that patterns of depression prevalence did not change upon ETI treatment in adults [24], accurate evaluation of psychiatric symptoms through standardized questionnaires should be carried out for the pediatric population. Concerns may extend beyond psychiatric conditions, to encompass neurodevelopmental issues [24]. It should be borne in mind that screening for changes in mental health during the first 3 months of ETI is recommended in the European Cystic Fibrosis Society (ECFS) Standards of Care guidelines [26].
We found that AEs led to permanent dosage adjustments in 32% of cases; this raises the issue of safety in relation to dosage reduction, efficacy and minimum ETI levels. A recent case series [27] correlated AEs with ETI dosage, showing that dose reduction mitigated AEs while maintaining efficacy in terms of sweat chloride concentration. Nevertheless, the optimal dose adjustment strategy has not yet been identified and the long-term efficacy of different dosing strategies needs to be demonstrated.
In relation to permanent ETI treatment modification, whether by dosage adjustment or discontinuation, the causative AEs in most cases comprised liver marker elevation. This is not unexpected: one clinical trial found a higher incidence of liver involvement in comparison to placebo [5], albeit not resulting in the study treatment's discontinuation. Longitudinal real-world data showed a non-significant increase in median ALT, AST, and total bilirubin values after 3 months of treatment [27].
5. Conclusions
Our study shows good tolerability for ETI, with almost 80% of patients experiencing no AEs during observation. Potentially treatment-related AEs were recorded, leading to permanent discontinuation of treatment in only 11% of cases (1.9% of the entire treated population). Psychiatric disorders, liver function marker elevation, gastrointestinal and skin disorders are the most prevalent AEs in our cohort, in line with the current literature. Special attention to long-term assessment in pediatric patients is a crucial point. Since a significant number of AEs occur after one year of treatment [21], longitudinal monitoring appears to be essential. National registries might provide a useful complement with a view to AE data collection, including occurrences related to mental health issues.
Author Contributions
Conceptualization,. F.L and M.C.; methodology, G.T. and M.C.; software, G.T.; validation, F.L. and I.M.; formal analysis, I.M. and G.T.; investigation, F.B., G.C., S.V., and E.P.; resources, M.C.; data curation, F.L., I.M., and G.T.; writing—original draft preparation, F.L. and V.B.; writing—review and editing, M.C.; supervision, V.B. and M.C.; project administration, M.C.; funding acquisition, V.B. and M.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by The Cystic Fibrosis Foundation (CFF, Bethesda, MD, USA), grant 005009122.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Azienda Ospedaliera Universitaria Integrata, Verona (number 433CET, approval date December 3rd, 2024 ).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
We are grateful to Peter Mead for English language editing and to the Lega Italiana Fibrosi Cistica - Veneto for supporting our activities.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CF | Cystic Fibrosis |
| pwCF | Patients with Cystic Fibrosis |
| F508del | F508del mutant CFTR |
| AE | Adverse event |
| ETI | Elexacaftor/tezacaftor/ivacaftor |
| SOC | System Organ Class |
References
- Riordan JR, Rommens JM, Kerem B, Alon N, Rozmahel R, Grzelczak Z, et al. Identification of the cystic fibrosis gene: cloning and characterization of complementary DNA. Science. 1989;245:1066–1073. [CrossRef]
- Ratjen F, Bell SC, Rowe SM, Goss CH, Quittner AL, Bush A. Cystic fibrosis. Nat Rev Dis Primers. 2015;1:15010. [CrossRef]
- Van Goor F, Straley KS, Cao D, González J, Hadida S, Hazlewood A, Joubran J, Knapp T, Makings LR, Miller M, Neuberger T, Olson E, Panchenko V, Rader J, Singh A, Stack JH, Tung R, Grootenhuis PD, Negulescu P. Rescue of DeltaF508-CFTR trafficking and gating in human cystic fibrosis airway primary cultures by small molecules. Am J Physiol Lung Cell Mol Physiol. 2006 Jun;290(6):L1117-30. [CrossRef] [PubMed]
- Taylor-Cousar JL, Robinson PD, Shteinberg M, Downey DG. CFTR modulator therapy: transforming the landscape of clinical care in cystic fibrosis. Lancet. 2023 Sep 30;402(10408):1171-1184. [CrossRef] [PubMed]
- Heijerman HGM, McKone EF, Downey DG, et al. Efficacy and safety of the elexacaftor plus tezacaftor plus ivacaftor combination regiment in people with cystic fibrosis homozygous for the F508del mutation: a double-blind, randomised, phase 3 trial. Lancet 2019;394:1940–8.
- Keating D, Marigowda G, Burr L, et al. VX-445-Tezacaftor-Ivacaftor in patients with cystic fibrosis and one or two Phe508del alleles. N Engl J Med 2018;379:1612–20.
- Middleton PG, Mall MA, Drevinek P, et al. Elexacaftor-Tezacaftor-Ivacaftor for cystic fibrosis with a single Phe508del allele. N Engl J Med 2019;381:1809–19.
- Goralski JL, Hoppe JE, Mall MA, McColley SA, McKone E, Ramsey B, Rayment JH, Robinson P, Stehling F, Taylor-Cousar JL, Tullis E, Ahluwalia N, Chin A, Chu C, Lu M, Niu T, Weinstock T, Ratjen F, Rosenfeld M. Phase 3 Open-Label Clinical Trial of Elexacaftor/Tezacaftor/Ivacaftor in Children Aged 2-5 Years with Cystic Fibrosis and at Least One F508del Allele. Am J Respir Crit Care Med. 2023 Jul 1;208(1):59-67. [CrossRef] [PubMed] [PubMed Central]
- McNally P, Lester K, Stone G, Elnazir B, Williamson M, Cox D, Linnane B, Kirwan L, Rea D, O'Regan P, Semple T, Saunders C, Tiddens HAWM, McKone E, Davies JC; RECOVER Study Group. Improvement in Lung Clearance Index and Chest Computed Tomography Scores with Elexacaftor/Tezacaftor/Ivacaftor Treatment in People with Cystic Fibrosis Aged 12 Years and Older - The RECOVER Trial. Am J Respir Crit Care Med. 2023 Nov 1;208(9):917-929. [CrossRef] [PubMed]
- Daines CL, Tullis E, Costa S, Linnemann RW, Mall MA, McKone EF, Polineni D, Quon BS, Ringshausen FC, Rowe SM, Selvadurai H, Taylor-Cousar JL, Withers NJ, Ahluwalia N, Moskowitz SM, Prieto-Centurion V, Tan YV, Tian S, Weinstock T, Xuan F, Zhang Y, Ramsey B, Griese M; VX17-445-105 Study Group. Long-term safety and efficacy of elexacaftor/tezacaftor/ivacaftor in people with cystic fibrosis and at least one F508del allele: 144-week interim results from a 192-week open-label extension study. Eur Respir J. 2023 Dec 7;62(6):2202029. [CrossRef] [PubMed] [PubMed Central]
- Bower JK, Volkova N, Ahluwalia N, Sahota G, Xuan F, Chin A, Weinstock TG, Ostrenga J, Elbert A. Real-world safety and effectiveness of elexacaftor/tezacaftor/ivacaftor in people with cystic fibrosis: Interim results of a long-term registry-based study. J Cyst Fibros. 2023 Jul;22(4):730-737. [CrossRef] [PubMed]
- Heo S, Young DC, Safirstein J, Bourque B, Antell MH, Diloreto S, Rotolo SM. Mental status changes during Elexacaftor/Tezacaftor /Ivacaftor therapy. J Cyst Fibros 2021.
- Spoletini G, Gillgrass L, Pollard K, Shaw N, Williams E, Etherington C, Clifton IJ, Peckham DG. Dose adjustments of Elexacaftor/Tezacaftor/Ivacaftor in response to mental health side effects in adults with cystic fibrosis. J Cyst Fibros. 2022 Nov;21(6):1061-1065. [CrossRef] [PubMed]
- Papadakis L, Stander T, Mombourquette J, Richards CJ, Yonker LM, Lawton B, Hardcastle M, Zweifach J, Sicilian L, Bringhurst L, Neuringer IP. Heterogeneity in Reported Side Effects Following Initiation of Elexacaftor-Tezacaftor-Ivacaftor: Experiences at a Quaternary CF Care Center. Pediatr Pulmonol. 2025 Jan;60(1):e27382. [CrossRef] [PubMed]
- Terlizzi V, Fevola C, Presti S, Castaldo A, Daccò V, Claut L, Sepe A, Majo F, Casciaro R, Esposito I, Vitullo P, Salvi M, Troiani P, Ficili F, Parisi GF, Pantano S, Costa S, Leonetti G, Palladino N, Taccetti G, Bonomi P, Salvatore D. Reported Adverse Events in a Multicenter Cohort of Patients Ages 6-18 Years with Cystic Fibrosis and at Least One F508del Allele Receiving Elexacaftor/Tezacaftor/Ivacaftor. J Pediatr. 2024 Nov;274:114176. doi: 10.1016/j.jpeds.2024.114176. Epub 2024 Jun 28. Erratum in: J Pediatr. 2024 Nov;274:114228. [CrossRef] [PubMed]
- Graham BL, Steenbruggen I, Miller MR, Barjaktarevic IZ, Cooper BG, Hall GL, Hallstrand TS, Kaminsky DA, McCarthy K, McCormack MC, Oropez CE, Rosenfeld M, Stanojevic S, Swanney MP, Thompson BR. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am J Respir Crit Care Med. 2019 Oct 15;200(8):e70-e88. [CrossRef] [PubMed] [PubMed Central]
- What is a serious adverse event? FDA. 2023. https://www.fda.gov/safety/reporting-serious-problems-fda/what-serious-adverse-event. (Accessed March 24, 2025).
- Serious adverse reaction. European medicines agency. https://www.ema.europa.eu/en/glossary-terms/serious-adverse-reaction (Accessed March 24, 2025).
- Bousquet C, Lagier G, Lillo-Le Louët A, Le Beller C, Venot A, Jaulent MC. Appraisal of the MedDRA conceptual structure for describing and grouping adverse drug reactions. Drug Saf. 2005;28(1):19-34. [CrossRef] [PubMed]
- Common Terminology Criteria for Adverse Events (CTCAE) Version 5. https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf (accessed on April 14th 2025).
- Zhu C, Cui Z, Liu T, Lou S, Zhou L, Chen J, Zhao R, Wang L, Ou Y and Zou F (2025) Realworld safety profile of elexacaftor/tezacaftor/ ivacaftor: a disproportionality analysis using the U.S. FDA adverse event reporting system. Front. Pharmacol. 16:1531514. [CrossRef]
- Mangoni, A. A. , and Jackson, S. H. (2004). Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br. J. Clin. Pharmacol. 57 (1), 6–14. [CrossRef]
- O'Connor J, Nazareth D, Wat D, Southern KW, Frost F. Regulatory adverse drug reaction analyses support a temporal increase in psychiatric reactions after initiation of cystic fibrosis combination modulator therapies. J Cyst Fibros. 2025 Jan;24(1):30-32. [CrossRef] [PubMed]
- Ramsey B, Correll CU, DeMaso DR, McKone E, Tullis E, Taylor-Cousar JL, Chu C, Volkova N, Ahluwalia N, Waltz D, Tian S, Mall MA. Elexacaftor/Tezacaftor/Ivacaftor Treatment and Depression-related Events. Am J Respir Crit Care Med. 2024 Feb 1;209(3):299-306. [CrossRef] [PubMed] [PubMed Central]
- Kolski-Andreaco A, Taiclet S, Myerburg MM, Sembrat J, Bridges RJ, Straub AC, Wills ZP, Butterworth MB, Devor DC. Potentiation of BKCa channels by cystic fibrosis transmembrane conductance regulator correctors VX-445 and VX-121. J Clin Invest. 2024 Jul 2;134(16):e176328. [CrossRef] [PubMed] [PubMed Central]
- Southern KW, Addy C, Bell SC, Bevan A, Borawska U, Brown C, Burgel PR, Button B, Castellani C, Chansard A, Chilvers MA, Davies G, Davies JC, De Boeck K, Declercq D, Doumit M, Drevinek P, Fajac I, Gartner S, Georgiopoulos AM, Gursli S, Gramegna A, Hansen CM, Hug MJ, Lammertyn E, Landau EEC, Langley R, Mayer- Hamblett N, Middleton A, Middleton PG, Mielus M, Morrison L, Munck A, Plant B, Ploeger M, Bertrand DP, Pressler T, Quon BS, Radtke T, Saynor ZL, Shufer I, Smyth AR, Smith C, van Koningsbruggen-Rietschel S. Standards for the care of people with cystic fibrosis; establishing and maintaining health. J Cyst Fibros 2024;23(1):12–28.
- Baromeo SBC, van der Meer R, van Rossen RCJM, Wilms EB. Adverse events to elexacaftor/tezacaftor/ivacaftor in people with cystic fibrosis due to elevated drug exposure?: A case series. J Cyst Fibros. 2025 Mar 10:S1569-1993(25)00061-X. [CrossRef] [PubMed]
- Tewkesbury DH, Athwal V, Bright-Thomas RJ, Jones AM, Barry PJ. Longitudinal effects of elexacaftor/tezacaftor/ivacaftor on liver tests at a large single adult cystic fibrosis centre. J Cyst Fibros. 2023 Mar;22(2):256-262. [CrossRef] [PubMed]
Figure 1.
ETI treatment adjustments in response to AEs for each SOC.
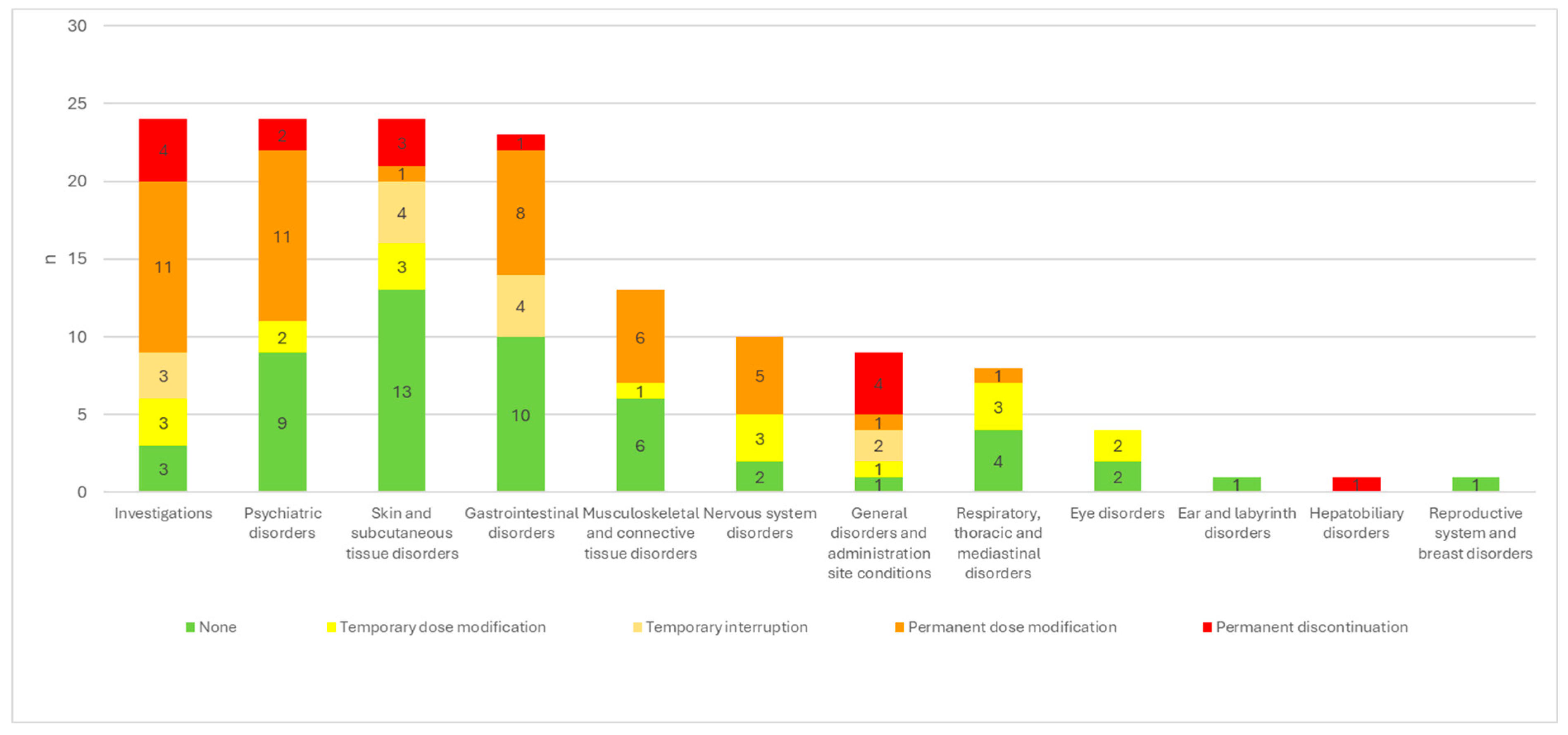

Table 1.
Comparison of baseline characteristics for overall population, pwCF presenting at least 1 AE, and pwCF not presenting AEs.
Table 1.
Comparison of baseline characteristics for overall population, pwCF presenting at least 1 AE, and pwCF not presenting AEs.
| Variable | Overall population (N=414) |
pwCF not presenting AE (N=329) |
pwCF presenting at least 1 AE (N=85) (21%) |
p-value |
|---|---|---|---|---|
| Age | 329 | 85 | 0.4 | |
| Median (Min, Max) | 27 (2, 68) | 27 (2, 59) | 28 (5, 68) | |
| Mean (SD) | 28 (13) | 28 (13) | 29 (14) | |
| Age | 0.7 | |||
| Adult | 310 (75%) | 245 (79%) | 65 (21%) | |
| Ped | 104 (25%) | 84 (81%) | 20 (19%) | |
| Sex | 0.6 | |||
| F | 222 (54%) | 174 (78%) | 48 (22%) | |
| M | 192 (46%) | 155 (81%) | 37 (19%) | |
| Baseline ppFEV1 (N=401) | 401 | 320 | 81 | 0.2 |
| Median (Min, Max) | 77 (19, 121) | 77 (19, 121) | 75 (25, 118) | |
| Mean (SD) | 74 (22) | 75 (22) | 71 (22) | |
| Baseline ppFEV1 (N=401) | 0.082 | |||
| <40 | 31 (7.7%) | 21 (68%) | 10 (32%) | |
| >40 | 370 (92%) | 299 (81%) | 71 (19%) | |
| Genotype | 0.4 | |||
| F508del/other | 274 (66%) | 221 (81%) | 53 (19%) | |
| F508del/ F508del | 140 (34%) | 108 (77%) | 32 (23%) | |
| Cl at sweat test in mmol/L (N=405) | 405 | 320 | 85 | 0.5 |
| Median (Min, Max) | 96 (12, 188) | 96 (12, 188) | 92 (47, 156) | |
| Mean (SD) | 93 (21) | 93 (22) | 93 (19) |
Table 2.
Rate of AEs throughout the entire treatment period (Part A) and in the first 30 days alone (Part B). Comparison of rates in relation to the main patient characteristics.
Table 2.
Rate of AEs throughout the entire treatment period (Part A) and in the first 30 days alone (Part B). Comparison of rates in relation to the main patient characteristics.
| AE (n) | ETI treatment days (n) | AE/1000 days ETI | p | |||||
|---|---|---|---|---|---|---|---|---|
| Part A | Entire period of observation | |||||||
| Total | 142 | 488889 | 0.290 | |||||
| Sex | M | 64 | 224985 | 0.284 | 0.9 | |||
| F | 78 | 263904 | 0.296 | |||||
| Genotype | F508del/F508del | 45 | 152652 | 0.295 | 0.9 | |||
| F508del/other | 97 | 336237 | 0.288 | |||||
| ppFEV1 | ppFEV1 <40 | 16 | 52932 | 0.302 | 0.8 | |||
| ppFEV1 ≥40 | 118 | 415512 | 0.284 | |||||
| Sweat test | Cl < median (95.5) | 76 | 232524 | 0.327 | 0.3 | |||
| Cl ≥ median (95.5) | 66 | 244858 | 0.270 | |||||
| Age | Age < 18 y | 30 | 93983 | 0.319 | 0.6 | |||
| Age ≥ 18 y | 112 | 394907 | 0.284 | |||||
| Part B | 0-30 days | |||||||
| Total | 62 | 14062 | 4.409 | |||||
| Sex | M | 24 | 6549 | 3.665 | 0.3 | |||
| F | 38 | 7513 | 5.058 | |||||
| Genotype | F508del/F508del | 19 | 4590 | 4.139 | 0.8 | |||
| F508del/other | 43 | 9472 | 4.540 | |||||
| ppFEV1 | ppFEV1 <40 | 11 | 1110 | 9.910 | 0.01 | |||
| ppFEV1 ≥40 | 49 | 12442 | 3.938 | |||||
| Sweat test | Cl < median (95.5) | 33 | 6772 | 4.873 | 0.5 | |||
| Cl ≥ median (95.5) | 29 | 7020 | 4.131 | |||||
| Age | Age < 18 y | 15 | 3363 | 4.460 | 1 | |||
| Age >= 18 y | 47 | 10699 | 4.393 | |||||
Table 3.
System Organ Class (SOC) for reported AEs.
| SOC | AEs | |
| n | (%) | |
| Investigations | 24 | 16.90 |
| Liver function marker elevations | 22 | |
| Pancreatic enzyme elevation | 1 | |
| Hypercholesterolemia | 1 | |
| Psychiatric disorders | 24 | 16.90 |
| Depression | 6 | |
| Anxiety | 3 | |
| Brain fog | 3 | |
| Insomnia | 3 | |
| Low mood | 3 | |
| Behavioral alterations | 3 | |
| Attention deficit | 2 | |
| Agitation | 1 | |
| Skin and subcutaneous tissue disorders | 24 | 16.90 |
| Skin rash | 16 | |
| Itching | 3 | |
| Erythema | 2 | |
| Acne | 1 | |
| Mucosal dryness | 1 | |
| Desquamation of the palms | 1 | |
| Gastrointestinal disorders | 23 | 16.20 |
| Epigastric pain | 11 | |
| Diarrhea | 4 | |
| Abdominal pain | 2 | |
| Nausea | 2 | |
| Dyspeptic disorders | 2 | |
| Abdominal swelling | 1 | |
| Odontologic symptoms | 1 | |
| Musculoskeletal and connective tissue disorders | 13 | 9.15 |
| Myalgia | 6 | |
| Articular pain | 4 | |
| Muscle weakness | 2 | |
| Low back pain | 1 | |
| Nervous system disorders | 10 | 7.04 |
| Headache | 6 | |
| Drowsiness | 1 | |
| School difficulties | 1 | |
| Episodes of absence | 1 | |
| Tic | 1 | |
| General disorders and administration site conditions | 9 | 6.34 |
| Asthenia | 4 | |
| Fever | 2 | |
| Generalized edema | 1 | |
| Hyperpyrexia | 1 | |
| Tiredness | 1 | |
| Respiratory, thoracic and mediastinal disorders | 8 | 5.63 |
| Chest tightness | 3 | |
| Chest heaviness | 2 | |
| Blood in sputum | 2 | |
| Dysphonia | 1 | |
| Eye disorders | 4 | 2.82 |
| Dry eyes | 2 | |
| Decrease in visual acuity | 1 | |
| Eye swelling | 1 | |
| Ear and labyrinth disorders | 1 | 0.70 |
| Hepatobiliary disorders | 1 | 0.70 |
| Reproductive system and breast disorders | 1 | 0.70 |
Table 4.
Modifications of ETI therapy in response to AEs, broken down by SOC. The frequency of the worst outcome is reported for each SOC.
Table 4.
Modifications of ETI therapy in response to AEs, broken down by SOC. The frequency of the worst outcome is reported for each SOC.
| None | Temporary dosage modification | Temporary interruption | Permanent dosage modification | Permanent discontinuation |
||
| Investigations | 24 | 3/24 (12.5%) | 3/24 (12.5%) | 3/24 (12.5%) | 11/24 (45.8%) | 4/24 (16.7%) |
| Psychiatric disorders | 24 | 9/24 (37.5%) | 2/24 (8.3%) | 11/24 (45.8%) | 2/24 (8.3%) | |
| Skin and subcutaneous tissue disorders | 24 | 13/24 (54.2%) | 3/24 (12.5%) | 4/24 (16.7%) | 1/24 (4.2%) | 3/24 (12.5%) |
| Gastrointestinal disorders | 23 | 10/23 (43.5%) | 4/23 (17.4%) | 8/23 (34.8%) | 1/23 (4.3%) | |
| Musculoskeletal and connective tissue disorders | 13 | 6/13 (46.2%) | 1/13 (7.7%) | 6/13 (46.2%) | ||
| Nervous system disorders | 10 | 2/10 (20.0%) | 3/10 (30.0%) | 5/10 (50.0%) | ||
| General disorders and administration site conditions | 9 | 1/9 (11.1%) | 1/9 (11.1%) | 2/9 (22.2%) | 1/9 (11.1%) | 4/9 (44.4%) |
| Respiratory, thoracic and mediastinal disorders | 8 | 4/8 (50.0%) | 3/8 (37.5%) | 1/8 (12.5%) | ||
| Eye disorders | 4 | 2/4 (50.0%) | 2/4 (50.0%) | |||
| Ear and labyrinth disorders | 1 | 1/1 | ||||
| Hepatobiliary disorders | 1 | 1/1 | ||||
| Reproductive system and breast disorders | 1 | 1/1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



