
Submitted:
22 April 2025
Posted:
23 April 2025
You are already at the latest version
Abstract
The paper investigates current and future pricing models in the European healthcare sector. European countries follow a universal healthcare system, whereas the United States rely on a mix of private insurers, government programmes, and private payments. It is becoming obvious that the European “free” healthcare systems are not sustainable in the long run. The authors propose a private Buy-Now-Pay-Later (BNPL) alternative. BNPL is common practice in retailing but highly unusual in healthcare. The authors suggest to enhancing BNPL further by adding AI and blockchain/crypto technology. However, there are three hurdles to overcome, namely, cryptocurrency volatility, regulatory uncertainty, and adoption barriers. Our field research investigated the acceptance barriers especially whether European medical service providers would accept cryptocurrency payments and the BNPL model in general. Our survey is based on 366 European medical service providers, mainly medical doctors. The results show that there is willingness to accept cryptocurrencies. As recommendation we outline how a fully integrated AI-powered BNPL model with cryptocurrency payments and smart contracts including BNPL Tokenisation in a decentralised financial market could work to the benefit of all stakeholders.
Keywords:
healthcare
; pricing models
; cryptocurrencies
; smart contracts
; tokenisation
; decentralised financial markets
1. Introduction
Pricing models are approaches how organisations determine their prices of products or services; these models are based on factors such as costs, market demand, competition, and perceived value (Kotler & Keller, 2016).
Pricing models in the healthcare sector play a crucial role in determining how medical services are billed and reimbursed. These models also influence the affordability/costs of care provided to patients. Over the years, different pricing models have evolved to balance cost efficiency and patient satisfaction. Among the various models, the most common ones are: Fee-for-Service (FFS), Capitation, Value-Based Pricing (VBP), Bundled Payments, and Subscription-Based models.
One of the most prevalent models in traditional healthcare is the Fee-for-Service (FFS) model. Under this system, healthcare providers are compensated for each individual service, test, or procedure. For example, a patient undergoing surgery would receive separate bills for the consultation, the procedure itself, hospital stay, and post-operative care. This model ensures that providers are reimbursed to the full extent of the care given. Critics argue that it incentivises excessive service utilisation and resulting in inflated medical costs (Cutler, 2020).
The Capitation model offers a fixed, prepaid amount to healthcare providers per patient over a specific period, regardless of the actual services utilised. While capitation encourages preventive care, there is concern that it might lead to under-treatment as providers may attempt to minimise services to stay within the budget (Glied & Smith, 2018).
The Value-Based Pricing (VBP) model, also known as Pay-for-Performance (P4P), seeks to address inefficiencies in traditional healthcare pricing by linking provider reimbursement to patient health outcomes. Instead of paying for the quantity of services rendered, insurers reward healthcare providers for improving a patient`s health. A major challenge is the accurate measurement of a patient`s health (Berenson & Rice, 2019).
Another approach, the Bundled Payments model, consolidates multiple services into a single payment for an entire episode of care. For instance, a hospital may charge a fixed price for a knee replacement procedure that includes pre-operative consultations, surgery, rehabilitation, and follow-up visits. By reducing administrative complexity and bundled payments it should lead to higher efficiency. However, it can be difficult to implement this model across multiple healthcare providers who need to agree on cost-sharing arrangements (Miller, 2021).
With the rise of telemedicine, Subscription-Based models have gained popularity. This approach allows patients to pay a recurring fee (monthly or annually) for unlimited access to healthcare services. Telehealth companies offer subscription-based plans that grant members virtual consultations and preventive care. This model ensures predictable costs and enhanced accessibility, though it may not cover all medical procedures, requiring additional out-of-pocket expenses for specialised care (Frogner, 2022). Predominant pricing models differ from country to country, see Table 1. Fee-for-Service remains the most common in the United States.
As the financial sector moves forward, Artificial Intelligence (AI) FinTech models are likely to play a greater role in future (Manta, 2025). AI in payment systems can be used for predictive analytics, fraud detection, and personalisation (Manta et al., 2025). For example, the benefits of AI-Driven Subscription Models are personalisation. Patients pay for what they use and making healthcare more affordable. In addition, cost efficiency in the form that providers reduce administrative costs by optimising pricing in real-time. Hopefully, this way patients stay motivated to follow healthier habits when rewarded with lower fees. AI could also flag high-risk patients, helping insurers and clinics to adjust their prices accordingly. AI could also track treatment progress, ensuring payments only trigger when health outcomes improve (e.g., improved blood sugar levels for diabetics). It could go that far that a patient pays nothing if a prescribed therapy does not show expected results. A model that the medical trade may disagree with.
AI-driven pricing models must analyse various data to calculate subscription fees, namely:
- Usage-Based Pricing: subscription costs adjust based on frequency of doctor visits, telehealth consultations, or prescription refills. Example: A patient who uses telehealth once a month pays less than someone who consults weekly.
- Predictive Health Risk Assessment: AI evaluates a patient’s health history and lifestyle to predict future healthcare needs and adjust pricing accordingly. Example: A diabetic patient who actively manages his/her/non-binary health may receive a lower subscription cost than one with unmanaged symptoms.
- Tiered and Dynamic Pricing: AI can segment patients into different pricing categories based on their engagement and risk profile. Example: A fitness-conscious user with a wearable health device showing high activity levels should pay less for a healthcare plan.
- Behaviour-Based Discounts: AI can track preventive care habits (e.g., regular exercises, diet tracking, medication adherence) and offer discounted subscription rates. Example: An app-linked smart scale or smartwatch can reward users who maintain a healthy weight or exercise regularly.
- Adaptive Payment Plans: AI can detect financial hardship patterns and offer flexible payment plans for patients struggling with payments. Example: If a patient’s income fluctuates (e.g. freelancer), AI can adjust monthly fees accordingly.
There are already real-world applications in form of Telehealth Platforms such as Teladoc and Babylon Health. Devices like Apple Watch and Fitbit can potentially integrate with insurers for dynamic premium adjustments. AI-powered diabetes management apps (e.g., Livongo) can tailor subscription fees based on a patient’s engagement. PayZen is a Fintech company specialising in providing "Care Now, Pay Later" (CNPL) solutions to address the growing challenge of medical debt in the United States. By leveraging AI, PayZen offers patients personalised, interest-free payment plans for their healthcare expenses, aiming to make medical treatments more accessible and affordable (FinMasters, 2023). This approach enhances the likelihood of repayment and increases acceptance rates among patients. In collaboration with Mastercard, PayZen introduced a Buy Now, Pay Later (BNPL) card specifically designed for medical expenses. This card, available in both physical and virtual forms, allows patients to manage their healthcare payments more flexibly (FinMasters, 2023).
BNPL is widely used in retailing to make purchases more accessible by allowing consumers to split payments into instalments. Lupșa-Tătaru et al. (2023) in their article “Buy Now Pay Later - A Fad or a Reality?” concluded that it is not a fad but there are overspending risks involved especially for young consumers. BNPL might be a new concept in healthcare but in sectors like retailing, where it is most common, prices are often quoted in instalments per month instead of the full price.
One may further argue that BNPL is applicable to the United States health care system only and has no relevance for Asian or European countries. However, all countries struggle to finance healthcare. In countries where healthcare is “free” (e.g. Canada, Portugal, Romania, Spain), the quality is generally poor. In addition, "free healthcare" does not mean that healthcare is completely without cost; most systems are funded through income taxes (e.g., Portugal) or social (national health) insurance (e.g., France, Germany, Romania, Switzerland). For example, in Germany one has to pay 14.6% of a normal (below EUR 5.500 per month) income for national health plus an additional 3.6% for compulsory care insurance (equally shared with employer) which is still not enough, so the government is forced to subsidise (BMG, 2025). The BNPL model could be advisable for countries like France, Germany and other European countries due to Europe's economic challenges and healthcare accessibility issues. Europe’s “free” public healthcare system faces long waiting times due to resource constraints, leading many patients to seek private care. In addition, not all services are free so patients have to co-finance but high inflation and cost of living pressures have reduced their disposable income. Studies show that financial concerns prevent people from seeking timely medical care, leading to worse health outcomes and higher long-term costs (Woolhandler, 2023). Implementing BNPL in Europe’s “free” healthcare sector could be a win-win solution by improving patient access to care, reducing financial stress, and supporting private healthcare providers in securing payments.
How AI could enhance BNPL in Healthcare:
- Personalised Payment Plans: AI customises repayment schedules based on income, medical history, and financial behaviour.
- Real-Time Credit Scoring: AI analyses non-traditional financial data (e.g., spending habits, employment stability) for instance BNPL approvals.
- Predictive Risk Assessment: AI detects potential late payments and proactively suggests adjustments (e.g., lower monthly payments).
- Automated Fraud Detection: AI identifies high-risk transactions and prevents fraudulent BNPL applications.
Khezr et al. (2019) outlined how blockchain technology can revolutionise healthcare. One could imagine an integration with cryptocurrencies and smart contracts. AI could automate subscription pricing using blockchain-based smart contracts including wearable BNPL Plans (AI analyses health data from smartwatches and fitness trackers to adjust payment options). Blockchain-powered BNPL will be secure and be decentralised medical financing with automatic payment tracking. By integrating these technologies, BNPL platforms can offer secure, transparent, and automated payment solutions while reducing fraud and operational costs. A potential addition could be the combination with the medical Internet of Things (IoT) as outlined by Sharma et al. (2020), which will not be further explored in the context of our research.
Features of Crypto and Smart Contracts BNPL are:
- Decentralised Payments: Patients can use stablecoins or healthcare-specific tokens to pay for medical services over time.
- Smart Contract Automation: Self-executing contracts ensure automatic payments, refunds, and compliance based on pre-decentralised financing rules.
- Transparent and Fraud-Proof Transactions: Blockchain records every BNPL transaction, reducing disputes and ensuring trust.
- Lower Processing Fees: Eliminates middlemen like banks, reducing transaction costs for both patients and providers.
However, there are three major Challenges:
1. Cryptocurrency Volatility: Using stablecoins (e.g., EUR Tether, EURS) instead of volatile cryptocurrencies, could be the answer. Even more secure would be a Fiat cryptocurrency as outlined by Salhout and Bechter (2018).
2. Regulatory Uncertainty: Boustani and Elisabetta (2022, p.306) rightly asked “How does a decentralized type of governance handle compliance and regulatory requirements? What happens if the majority of token owners in a decentralized voting system choose to abstain from voting for compliance upgrades or financial anti-money laundering requirements?” The answers can only lie in well-defined regulations regarding security and compliance. In other words, regulators must catch up and define clear rules. The deregulated community has to bite the bullet.
3. Adoption Barriers: Encourage practitioners and other medical services providers to accept crypto payments but nobody can be forced. This is the real bottleneck of a successful implementation. Our field research looked deeper into these barriers.
2. Materials and Methods
During the first quarter of 2025, 366 quantitative surveys were obtained from European practitioners and medical service providers. The aim of our field research was the evaluation of perceptions and state of knowledge in regard to cryptocurrencies, blockchain and smart contracts. In total 366 responses were analysed. Out of the 366 persons, 203 (55.5%) were medical doctors. The remaining ones were other healthcare specialists such as administrators. The demographics of the sample is listed in Table 2 and Table 3.
We also asked some lifestyle questions about how they relax and how they keep their knowledge updated, see Table 4 and Table 5.
The potential of cryptocurrencies and blockchains in financing healthcare are enormous but the implementation depends on the people involved, especially their perceptions, see Figure 1. Our research investigated the acceptance of BNPL contracts by asking whether the medical healthcare providers would accept instalment payments. For the acceptance of cryptocurrencies we asked whether they would be willing to run a pilot test accepting them as payment.
3. Results
We analysed the data by descriptive analyses as well as multivariate methods. Significant group differences were also extracted.
3.1. Descriptive Statistics
For all questions we used a 0 (totally disagree) to 10 (totally agree) Likert scale.
Most participants agree that AI will have an impact on healthcare (mean 7.6), see Table 6. The knowledge about cryptocurrencies is low and the perceived uncertainty of cryptocurrencies is high. The willingness to accept instalment payments or to run a crypto test is also more on the negative side.
3.2. Group Differences
We conducted a t-test to evaluate whether medical doctors working in the private sector have different views than the ones working in the public sector. The nullhyposesis that there is no difference at 95% confidence level could be rejected in two cases, namely, being replaced by AI and Telehealth, see Table 7. Medical experts working in the private sector (e.g. doctors having their own practice) fear more of being replaced by AI than their publicly employed colleagues. These, however, see a brighter future for telehealth than their private counterparts.
3.3. Major Factors and Correlations
A factor analysis extracted three major dimensions which in total can explain more than 60% of variance, see Table 8.
Factor (Component, Dimension) 1 showed four variables with high (>.6) loadings, see Table 9. The factor could be described as the “open to new ideas” because it includes willingness to learn more about cryptocurrencies, willing to run a pilot test with crypto payments, accepting instalments (BNPL), and existing knowledge about cryptocurrencies. These four attributes correlate significantly with each other, see Table 10.
3.4. Predicting
We conducted a regression analysis to predict who may be willing to run a pilot test with cryptocurrency as payment. The strongest influencing parameter is the willingness to learn more about cryptocurrencies. Unsurprisingly, doubts about cryptocurrencies (legality etc.) has a negative impact. Table 11 shows the Betas of the model. With an R square of 0.4 the fit of the model is good, see Table 12.
3.5. Grouping
We conducted a Clusteranalysis to group respondents. Two distinct clusters were identified. Looking at Table 15 we can see that Cluster 1 represents a more traditional lifestyle. A similar picture when looking at how respondents keep their knowledge updated, see Table 15. Cluster 2 is more into streaming than cluster 1 members who update their knowledge by reading printed journals, see Table 16.
However, the centroids (of willingness to run a pilot test) are not significantly different, see Table 17.
4. Discussion and Implementation
Our findings are in line with previous research conducted by Govindarajan et al. (2025) in the sense that there are many barriers to fully accept modern technologies such as cryptocurrencies in healthcare. AI is accepted as a force that will shape the years to come (Hua et al., 2004; Cornelissen et al., 2022). However, there are concerns about the legality of cryptocurrencies (Witkowski et al., 2004; Sahoo et al., 2025).
To fully integrate AI-powered BNPL with crypto payments and smart contracts, the system must include on-chain and off-chain components to ensure seamless financing, automation, and security. Below is a detailed breakdown of how it would work from a technical perspective.
System Architecture & Components:
- AI-Powered Credit and Risk Assessment uses machine learning algorithms to analyse:
- Patient's financial history (bank accounts, crypto wallets, spending patterns).
- On-chain activity (decentralised financing transactions, crypto staking, wallet balances).
- Healthcare history (frequency of doctor visits, medical insurance claims).
- AI generates a personalised BNPL plan with terms tailored to risk profile.
A smart contract is created to manage:
- Payment schedule (monthly or customised).
- Crypto collateral requirements (if needed).
- Automated penalties and rewards for early/late payments.
- Instant fund distribution to healthcare providers.
- Deployed on a public (e.g., Ethereum) or private (Hyperledger) blockchain.
- Crypto Payment Processing and Stablecoin Integration.
Healthcare BNPL could be tokenised into so-called NFTs (non-fungible tokens). Nunes et al. (2024) explored the potential applications of NFTs in healthcare, highlighting innovative solutions and challenges associated with integrating blockchain technology in the sector. As shown by Zhang et al. (2024) NFTs can effectively hedge against traditional financial assets when used as long positions. Patients could tokenise BNPL agreements as NFTs for trading on decentralised financing lending platforms and investors could fund BNPL pools in return for yield from patient repayments. Healthcare providers could then use BNPL-backed assets as collateral.
The integration of tokenised BNPL agreements with decentralised financing lending pools can revolutionise healthcare financing by transforming patient debt into tradeable assets. This model allows investors to fund medical loans, hospitals to gain liquidity, and patients to access care without upfront costs. Tokenisation converts BNPL agreements into digital assets (NFTs or security tokens) recorded on a blockchain. These assets represent a patient's outstanding medical balance and can be traded or used as collateral in decentralised finance lending markets. To implement tokenised BNPL for healthcare, it needs smart contracts that automate: loan issuance, payment tracking, default handling, and tokenisation. Tokenisation converts BNPL agreements into digital assets recorded on a blockchain. However, tokenising BNPL agreements in healthcare could introduce systemic financial risks, similar to those seen in the 2008 US mortgage crisis. Just like mortgage-backed securities bundled subprime loans, tokenised BNPL agreements could be packaged and traded as financial assets. If healthcare BNPL debts are issued to high-risk patients who struggle to repay, these tokenised assets could become overvalued and unstable. Lack of regulation in tokenised debt markets could lead to predatory lending, where patients are offered BNPL without proper risk assessment. If speculative trading increases, healthcare debt could be treated like a financial commodity rather than a human necessity. However, there is a long way to go before this risk factor may come into play.
There are limitations in our study. We surveyed medical professionals but not health insurance providers. These may have a more forward-looking perspective; nor did we include government officials. Like any other technology, blockchains (or distributed server systems) have to prove that they become mainstream and are manageable. The acceptance and tradability of BNPL NFTs has not been evaluated.
5. Conclusions
BNPL is an additional payment method and not a substitute for conventional methods. However, integrating AI-powered BNPL with cryptocurrencies and smart contracts could revolutionise medical financing, making healthcare more accessible, transparent, and automated. As blockchain adoption grows, decentralised BNPL financing solutions could provide patients with flexible, low-cost, and secure payment options worldwide to the extent of a global market for bundled BNPL tokens. Overall medical costs will be reduced because it will, at the same token, be financially incentivised to actively manage own health (preventing chronical diseases), and foster care habits (e.g., regular exercise, diet tracking) through AI. However, the stumbling block against changing the system are the people involved such as politicians and medical professionals. To incentivise politicians and medical practitioners to accept BNPL tokens in a decentralised financial environment, it will need a strategy that aligns with their interests i.e. economic benefits, risk reduction, regulatory alignment, and patient-centred incentives such as positioning BNPL tokens as a cost-reduction tool for national healthcare, collaboration with the European Central Bank to issue regulated stablecoin-backed BNPL tokens to avoid volatility concerns, and using pilot programmes in high-profile hospitals.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
Data are available from the corresponding author upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AI | Artificial Intelligence |
| BNPL | Buy Now Pay Later |
| NFT | Non-Fungible Token |
Appendix A. Survey
Dear Healthcare Practitioner,
We are conducting a survey to assess the challenges and barriers to adopting cryptocurrencies in healthcare. Your responses will help us understand medical industry perspectives and potential adoption strategies.
The survey should take 3 minutes to complete.
Your responses are anonymous and confidential.
Please answer using the Likert scale (0-10):0 Totally Disagree | 3 Disagree | 5.5 Neutral | 8 Agree | 10 Totally Agree
Thank you for your participation!
I have had prior exposure to cryptocurrencies like Bitcoin
I have heart about blockchain technology
Artificial Intelligence can enhance healthcare
I believe that most healthcare practitioners lack awareness of Artificial Intelligence
I believe that mosthealthcare practitioners lack awarenessof cryptocurrencies
I do not trust these new technologies like Artificial Intelligence and blockchains
I am too old for all these new technologies like Artificial Intelligence in healthcare
I worry about theregulatory uncertaintysurrounding cryptocurrencies in healthcare
I am interested in learning more abouthow cryptocurrencies could work in healthcare
I am familiar with healthcare financing systems in other countries
The current “free” healthcare should be replaced by a private healthcare system
I would accept payments in monthly instalments as it is common practice in retailing
I would be willing to pilot a small-scale crypto-based payment system in my practice/hospital
Age: below 30, 30-40, 40-50, above 50
I am a Medical Doc, other
References
- Berenson, R. A., & Rice, T. (2019). Beyond Fee-for-Service: Examining Alternative Payment Models in Healthcare. Health Affairs, 38(10), 1726-1733.
- BMG (2025). Minuistry of Health, Germany. Beiträge. Retrieved from https://www.bundesgesundheitsministerium.de/beitraege.html#:~:text=Der%20gesetzlich%20festgeschriebene%20allgemeine%20Beitragssatz,0%20Prozent%20der%20beitragspflichtigen%20Einnahmen 2. April 2025.
- Boustani, N. M., & Elisabetta, M. (2022). Smart Insurance Contracts Shielding Pandemic Business Disruption in Developing Countries and Blockchain Solution. FinTech, 1(4), 294-309.
- Cornelissen, L., Egher, C., Beek, V., Williamson, L., Hommes, D. (2022). The Drivers of Acceptance of Artificial Intelligence–Powered Care Pathways Among Medical Professionals: Web-Based Survey Study, JMIR Formative Research, 6(6).
- Cutler, D. (2020). The Costs of Care: Understanding Healthcare Pricing and Reimbursement. Journal of Health Economics, 39(4), 567-582.
- FinMasters. (2023). PayZen: A better way to finance medical bills. Retrieved from https://finmasters.com/payzen-a-better-way-to-finance-medical-bills/ 22. March 2025.
- Frogner, B. K. (2022). Telemedicine and the Rise of Subscription-Based Healthcare Services. Digital Health Review, 7(2), 112-126.
- Glied, S., & Smith, P. C. (2018). Healthcare Economics and Capitation Models: Balancing Cost and Care. Cambridge University Press.
- Govindarajan, U. H., Narang, G., Singh, D. K., Yadav, V. S. (2025). Blockchain technologies adoption in healthcare: Overcoming barriers amid the hype cycle to enhance patient care. Technological Forecasting and Social Change, 213, 124031.
- Hua, D., Petrina, N., Young, N., Cho, J.-G., Poon, S.K. (2004). Understanding the factors influencing acceptability of AI in medical imaging domains among healthcare professionals: A scoping review. Artificial Intelligence in Medicine, Volume 147, 102698.
- Khezr, S., Moniruzzaman, M., Yassine, A., & Benlamri, R. (2019). Blockchain Technology in Healthcare: A Comprehensive Review and Directions for Future Research. Applied Sciences, 9(9), 1736.
- Kotler, P., & Keller, K. L. (2016). Marketing management (15th ed.). Pearson.
- Lupșa-Tătaru, D. A., Nichifor, E., Dovleac, L., Chițu, I. B., Todor, R. D., & Brătucu, G. (2023). Buy Now Pay Later—A Fad or a Reality? A Perspective on Electronic Commerce. Economies, 11(8), 218.
- Manta, O.P. (2025). FinTech 2050: AI-powered transformation and innovation. LAP LAMBERT Academic Publishing.
- Manta, O.P., Vasile, V., & Rusu, E. (2025). Banking Transformation Through FinTech and the Integration of Artificial Intelligence in Payments. Preprints. Retrieved from https://www.preprints.org/manuscript/202502.1409 2. April 2025.
- Miller, H. D. (2021). Bundled Payments and Healthcare Reform: Cost Efficiency in a Changing Market. American Journal of Managed Care, 27(5), 253-261.
- Nunes, T., da Cunha, P. R., de Abreu, J. M., Duarte, J., & Corte-Real, A. (2024). Non-Fungible Tokens (NFTs) in Healthcare: A Systematic Review. International Journal of Environmental Research and Public Health, 21(8), 965.
- Salhout, S., Bechter, C. (2018). Visionizing a Fiat Cryptocurrency, Case Studies in Business and Management, 5(2), 1-12.
- Sharma, A., Dangi, S., Tomar, R., Chilamkurti, N., & Kim, B.-G. (2020). Blockchain Based Smart Contracts for Internet of Medical Things in e-Healthcare. Electronics, 9(10), 1609.
- Sahoo, R. K., Sahoo, K. C., Negi, S., Baliarsingh, S. K., Panda, B., Pati, S. (2025). Health professionals' perspectives on the use of Artificial Intelligence in healthcare: A systematic review, Patient Education and Counseling, 134, 108680.
- Statista (2025). Healthcare. Retrieved from https://www.statista.com/markets/412/topic/454/health-system 19. March 2025.
- Witkowski, K., Okhai, R. & Neely, S.R. (2004). Public perceptions of artificial intelligence in healthcare: ethical concerns and opportunities for patient-centered care. BMC Med Ethics 25, 74.
- Woolhandler, S., Himmelstein, D. U., & Gaffney, A. (2023). Financial barriers to care and unmet healthcare needs: A systematic review. Health Affairs Scholar, 1(5), Retrieved from https://academic.oup.com/healthaffairsscholar/article/1/5/qxad057/7338828 25. March 2025.
- Zhang, W., Liu, T., Zhang, Y., & Hamori, S. (2024). Can NFTs hedge the risk of traditional assets after the COVID-19 pandemic? The North American Journal of Economics and Finance, 72, 102149.
Figure 1.
Research Framework.
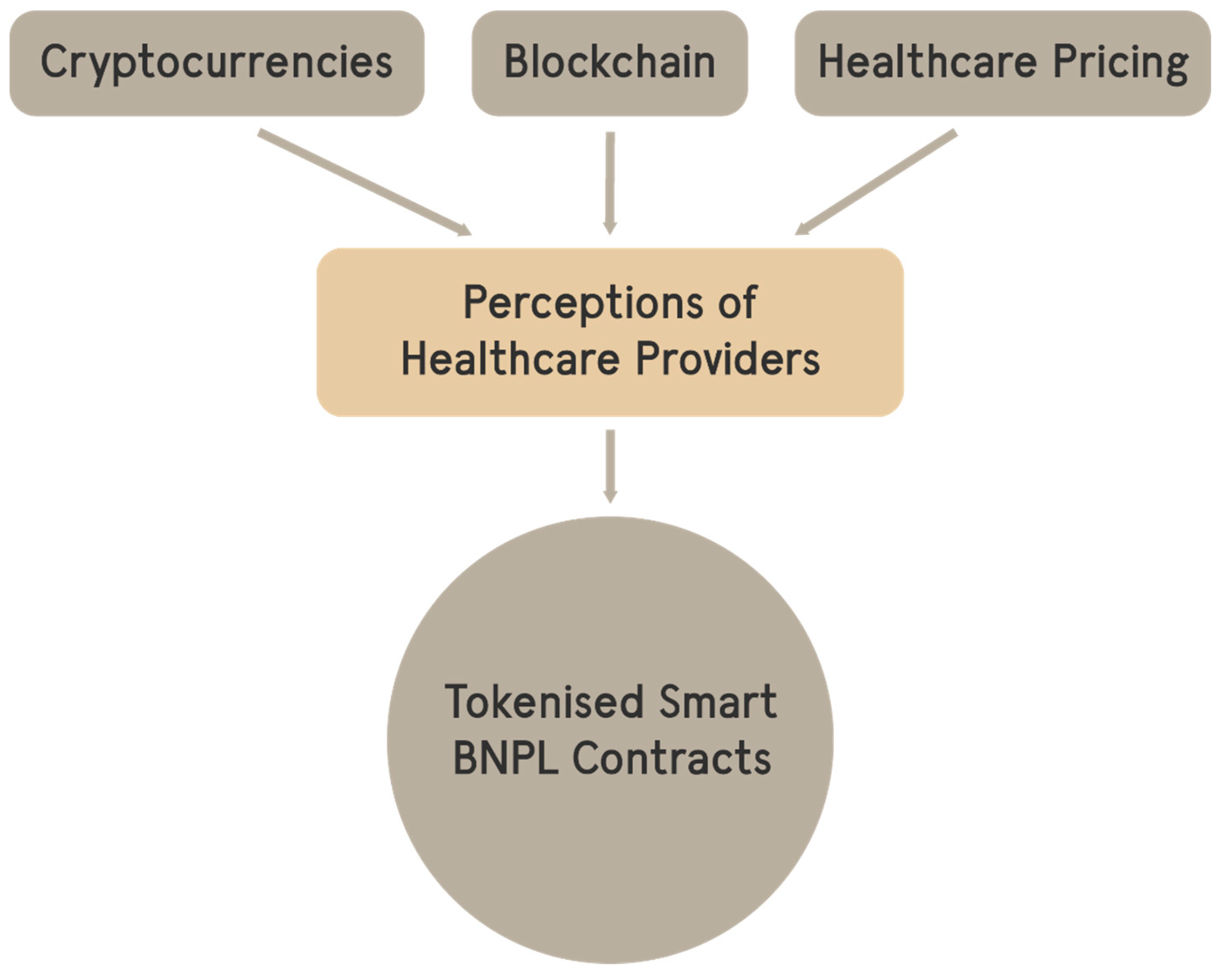

Table 1.
Pricing Models by selected countries.
| Predominant in | Pricing Model |
|---|---|
| U.S.A. | Fee-for-Service |
| UK | Capitation |
| Sweden | Value-Based Pricing |
| The Netherlands | Bundled Payments |
| Singapore | Subscription-Based |
Table 2.
Age.
| Age | Frequency | Percent |
|---|---|---|
| Below 30 years old | 83 | 22.7 |
| 30-40 years old | 122 | 33.3 |
| 40-50 years old | 101 | 27.6 |
| Above 50 years old | 60 | 16.4 |
| Total | 366 | 100.0 |
Table 3.
Employment Sector.
| Sector | Frequency | Percent |
|---|---|---|
| Government | 166 | 45.4 |
| Private Sector | 104 | 28.4 |
| Both | 96 | 26.2 |
| Total | 366 | 100.0 |
Table 4.
Relaxation.
| Relaxation | Frequency | Percent |
|---|---|---|
| Reading a book, classic radio, traditional relaxation | 83 | 22.7 |
| Streaming Netflix, social media, modern entertainment | 201 | 54.9 |
| Total | 366 | 100.0 |
Table 5.
Keeping Updated.
| Knowledge Update | Frequency | Percent |
|---|---|---|
| Online medical journals, webinars, and social media | 306 | 83.6 |
| Printed journals, books, and conferences | 45 | 12.3 |
| Total | 366 | 100.0 |
Table 6.
Descriptive Statistics.
| N | Mean | Std. Deviation | |
|---|---|---|---|
| AI healthcare | 366 | 7.60 | 2.21 |
| Telehealth | 366 | 6.69 | 2.62 |
| Crypto doubts | 366 | 5.55 | 3.16 |
| Learning | 366 | 4.81 | 3.38 |
| Rewarded | 366 | 4.58 | 3.22 |
| Replaced | 366 | 4.36 | 2.96 |
| Instalments | 366 | 3.77 | 2.94 |
| Pilot | 366 | 3.39 | 3.04 |
| Know crypto | 366 | 3.14 | 3.43 |
Table 7.
Group Differences.
| Question | Work | N | Mean |
|---|---|---|---|
| Replaced | private | 104 | 4.80 |
| public | 166 | 4.30 | |
| Telehealth | private | 104 | 6.00 |
| public | 166 | 6.70 |
Table 8.
Total Variance Explained.
| Rotation Sums of Squared Loadings | % of Variance |
|---|---|
| Factor 1 | 27.49 |
| Factor 2 | 20.23 |
| Factor 3 | 13.51 |
Table 9.
Rotated Component Matrix.
| Component | |||
|---|---|---|---|
| 1 | 2 | 3 | |
| Learning | .813 | .145 | .065 |
| Know crypto | .736 | -.083 | -.225 |
| Instalments | .696 | .160 | .175 |
| Pilot | .652 | .222 | .198 |
| Crypto doubts | .526 | .100 | .196 |
| Telehealth | .151 | .901 | .027 |
| AI healthcare | .184 | .861 | -.020 |
| Rewarded | .081 | .222 | .728 |
| Replaced | .149 | -.325 | .722 |
Extraction Method: Principal Component Analysis. Rotation Method: Varimax with Kaiser Normalization.
Table 10.
Correlations.
| Learning | Know Crypto | Instalments | Pilot | ||
|---|---|---|---|---|---|
| Learning | Pearson Correlation | 1 | .484 * | .451 * | .581 * |
| Know Crypto | N Pearson Correlation |
366 .484 * |
366 1 |
366 .283 * |
270 .329 * |
| Instalments | N Pearson Correlation |
366 .484 * |
366 .283 * |
366 1 |
270 .580 * |
| Pilot | N Pearson Correlation |
366 .581 * |
366 .329 * |
366 .580 * |
270 1 |
* Correlation is significant at the 0.01 level (2-tailed).
Table 11.
Coefficients - Dependent Variable: Pilot test cryptocurrency.
| Model | Unstandardized Coefficients B | Standardized Coefficients Beta |
|---|---|---|
| (Constant) | -.717 | |
| Learning | .462 | .532 |
| Crypto doubts | -.090 | -.094 |
| Rewarded | -.090 | .097 |
| Replaced | .127 | .123 |
| Telehealth | .219 | .200 |
Table 12.
Model Fit Pilot.
| R | R Square | Adjusted R Square |
|---|---|---|
| .63 | .40 | .39 |
Table 13.
Coefficients - Dependent Variable: Instalments.
| Model | Unstandardized Coefficients B | Standardized Coefficients Beta |
|---|---|---|
| Pilot | .457 | .455 |
Table 14.
Model Fit Instalments.
| Model R | R Square | Adjusted R Square |
|---|---|---|
| .606 | .368 | .363 |
Table 15.
Relaxation.
| Reading a book, classic radio, traditional relaxation | Streaming Netflix, social media, modern entertainment | ||||||
|---|---|---|---|---|---|---|---|
| Frequency | Percent | Frequency | Percent | ||||
| Cluster | 1 | 64 | 100.0% | 14 | 9.9% | ||
| 2 | 0 | 0.0% | 128 | 90.1% | |||
| Combined | 64 | 100.0% | 142 | 100.0% | |||
Table 16.
Keeping Updated.
| Online medical journals, webinars, and social media | Printed journals, books, and conferences | ||||||
|---|---|---|---|---|---|---|---|
| Frequency | Percent | Frequency | Percent | ||||
| Cluster | 1 | 90 | 41.3% | 41 | 100.0% | ||
| 2 | 128 | 58.7% | 0 | 0.0% | |||
| Combined | 218 | 100.0% | 41 | 100.0% | |||
Table 17.
Centroids.
| Pilot | |||
|---|---|---|---|
| Cluster | Mean | Std. Deviation | |
| 1 | 3.0986 | 3.05112 | |
| 2 | 3.7266 | 3.01104 | |
| Combined | 3.3963 | 3.04281 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



